Embed Size (px)
Citation preview

QURAT KHAN, M.D.
Epilepsy, Stroke

• BRIEF OVERVIEW• TLE
Epilepsy

Epilepsy
• Chronic disorder of brain characterized by recurrent seizures due to excessive electrical discharges in a group of brain cells
• Two or more unprovoked seizures• Seizures are brief episodes of involuntary
shaking which may involve a part of the body (partial) or the entire body (generalized) and may cause LOC and control of bowel or bladder.
Idiopathic Epilepsy
Is the most common typeHas no identifiable causeOften underlying genetic basis
Secondary Epilepsy
• Epilepsy with a known cause• Possible causes:• brain damage from prenatal or perinatal injuries
(hypoxia or trauma during birth, low birth weight) • Congenital abnormalities or genetic conditions
with associated brain malformations• TBI• Stroke • Brain infection • Certain genetic syndromes• Brain tumor and vascular lesions • Neurodegenerative conditions
COMPLEX PARTIAL SEIZURES
Temporal Lobe Epilepsy (TLE)
• The most common form of adult epilepsy• Symptomatic localization-related epilepsy• Epileptogenic abnormalities in mesial
temporal limbic structures • The associated pathological substrate is
usually hippocampal sclerosis• One of the most medically refractory forms
of human epilepsy
Clinical Features
History
• Higher incidence of complicated febrile convulsions or other cerebral insults in the first 5 years of life
• Family history of epilepsy common• Onset of habitual seizures usually in latter half of
first decade of life.• Auras commonly occur in isolation.• Infrequent secondarily generalized seizures.• Seizures often remit for several years until
adolescence or early adulthood.• Seizures often become medically intractable.• Interictal behavioral disturbances can develop,
most commonly depression.

Clinical Presentation
• Aura is usually present. The most common is epigastric, often with other autonomic or psychic symptoms, including emotion (e.g., fear). Olfactory or gustatory sensations can occur. Last several seconds
• Often begin with arrest and stare; oroalimentary automatisms and complex automatisms are common
• Posturing of one arm may occur contralateral to the ictal discharge. Seizure lasts 1 to 2 minutes
• Postictal phase: disorientation, recent-memory deficit, amnesia for the event, and dysphasia if seizures begin in the language-dominant hemisphere. Lasts several minutes

Neurologic and Laboratory features
• Neurologic examination usually normal • Memory dysfunction on neuropsychological testing and amnesia with
contralateral intracarotid injection of amobarbital.EEG• Interictal EEG: anterior temporal spikes with maximal amplitude in
basal electrodes.• Ictal EEG: 5 to 8 Hz rhythmic discharge beginning in one mesial
temporal area, either initially or within 30 seconds of a more generalized electrographic change
MRI• Hippocampal atrophy on T1 and mesial temporal increased signal on
T2-weighted MRIFunctional MRI• Temporal-lobe hypometabolism on interictal FDG-PET • Hypoperfusion on ictal SPECT• Decreased n-acetyl aspartate on magnetic resonance spectroscopy

• Frequently misdiagnosed with psychiatric illnesses.
• Often symptoms have unusual qualities atypical for primary psychiatric syndromes such as gustatory and olfactory hallucinations; micropsia or macropsia; intense delusions involving bodily harm, déjà vu, or “out-of-body” experiences.
• Personality features: moral rigidity, hyperreligiosity, hypergraphia, and viscosity

Anterior Temporal Lobectomy (ATL) for medically refractory medial temporal lobe epilepsy due to medial temporal sclerosis (MTS) is the most commonly performed surgical procedure in the comprehensive epilepsy management centres.
Surgery is ideally directed towards complete seizure freedom without or with very minimal cognitive or functional deficits.

NEUROPSYCHIATRY OF STROKE
Stroke
Definition of Stroke
Rapidly developing clinical signs of focal (or global) disturbance of cerebral function, with sx lasting 24 hours or longer or leading to death, with no apparent cause other than of vascular origin.
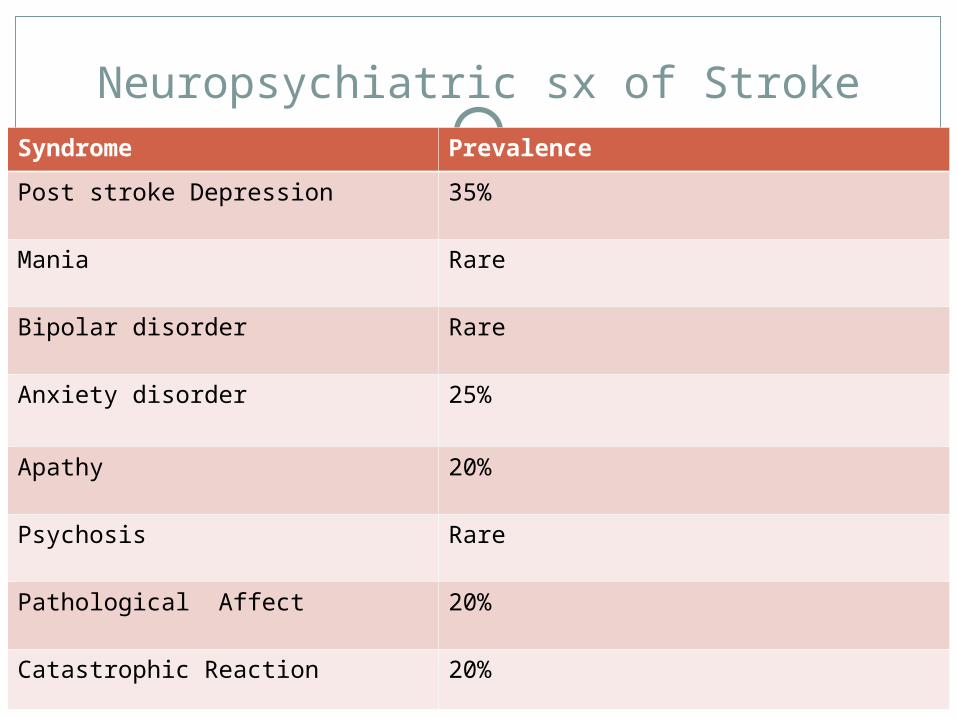
Neuropsychiatric sx of StrokeSyndrome Prevalence
Post stroke Depression 35%
Mania Rare
Bipolar disorder Rare
Anxiety disorder 25%
Apathy 20%
Psychosis Rare
Pathological Affect 20%
Catastrophic Reaction 20%
Post stroke Depression (PSD)
• DSM-IV criteria for “mood disorders due to medical condition” are used for diagnosis
• Loss of energy and appetite, insomnia• Mean duration of depression appears to be 9
months but significant number of patients remain depressed for several years after stroke
• Anatomical Correlates: L>R, frontal, parietal• Mechanism: depletion of monoaminergic
amines after lesions of frontal lobe or basal ganglia
Association Between Physical Impairment and PSD
Association Between Cognitive Impairment and PSD- L hemisphere strokes
Treatment: anti depressants, stimulants, ECT
Post stroke Anxiety Disorder
Significant comorbidity with PSDAnatomical Correlates: L or R cortical
lesionsADL impairment is associated with GADTreatment

Catastrophic Reaction
• In 1939, Goldstein created the term to describe a series of symptoms (i.e., anxiety, aggressiveness, refusal, and renouncement) in patients with TBI
• Appear to be due to the “inability of the organism to cope with physical or cognitive deficits”
• Common in patients with nonfluent aphasia after stroke

Pathological Affect
Characterized by frequent and easily provoked episodes of crying and/or laughing not appropriate to the situation or in excess of the underlying emotion
Treatment
Post stroke Psychosis
Rare complication of strokeAnatomical correlate: R frontoparietal
lesionsTreatment

EID MUBARAK
Thank you and




![TLE ANALYSER · TLE ANALYSER User Manual v2.8 TLE analysis ... TLE ANALYSER Version 2.8 - 2013 TLE ANALYSER - User Manual [4] 2. TLE Analyser Setup and Options TLE Updater allow to](https://img.pdfslide.us/doc/110x75/5aa68a5c7f8b9a517d8ea13c/tle-analyser-analyser-user-manual-v28-tle-analysis-tle-analyser-version-28.jpg)