Embed Size (px)
Citation preview

Biomedical Informatics1
Initial progress on the journey toward an open source potential drug-drug interaction knowledge base
Richard D. Boyce, PhDUniversity of Pittsburgh
33rd VistA Community MeetingMay 24th 2016

Biomedical Informatics2
Disclosures• Neither myself or my spouse have
any relevant financial relationships with commercial interests

Biomedical Informatics3
Key point from my last VistA Community talk in January…• Many drug information systems
disagree about potential drug-drug interactions (PDDIs)– the specific ones that exist– their potential to cause harm
• This leads to– confusion and frustration for clinicians– greater risks of harm to patients

Biomedical Informatics4
The danger of incomplete drug-drug interaction knowledge

Evidence of drug compendia problems• Three PDDI information sources agreed upon
only 25% of 59 contraindicated drug pairs found in black box warnings
• 18 (28%) of 64 pharmacy information and clinical decisions support systems correctly identified 13 clinically significant DDIs
• Four sources agreed on only 2.2% of 406 PDDIs considered to be “major” by at least one source
Wang LM, Wong M, Lightwood JM, Cheng CM. Black box warning contraindicated comedications: concordance among three major drug interaction screening programs. Ann Pharmacother. 2010;44(1):28–34. doi:10.1345/aph.1M475.
Saverno KR, Hines LE, Warholak TL, et al. Ability of pharmacy clinical decision-support software to alert users about clinically important drug-drug interactions. J Am Med Inform Assoc. 2011;18(1):32–37. doi:10.1136/jamia.2010.007609.
Abarca J, Malone DC, Armstrong EP, et al. Concordance of severity ratings provided in four drug interaction compendia. J Am Pharm Assoc (2003). 2004;44(2):136–141.

Biomedical Informatics6
Problems with drug compendia extend to non-commercial sources
“our investigation of NDF-RT and DrugBank as sources of DDIs for our API provides a mixed picture. Not only do they both provide incomplete coverage of the reference set (about 60% each), but their overlap is also limited (42%)”.
Peters, Lee B., Nathan Bahr, and Olivier Bodenreider. "Evaluating drug-drug interaction information in NDF-RT and DrugBank." Journal of biomedical semantics 6.1 (2015): 19.

Is this true of the translated French PDDI dataset?
• Free online: http://ansm.sante.fr/Dossiers/Interactions-medicamenteuses/Interactions-medicamenteuses/%28offset%29/0
• Potentially interacting drugs and drug groups– Ingredients X drug groups : ~3,000– Expands to ~ 116,000 ingredient pairs

Examples interactionsDIGOXIN RxNorm: 3407ATC: C01AA05
CLARITHROMYCINRxNorm: 21212 ATC:J01FA09 A02BD04 A02BD05 A02BD06 A02BD07
Increase of the digoxinemia due to increase of its absorption
Precaution for useClinical monitoring and possibly monitoring of the digoxinemia during the treatment with the clarithromycin and after it is stopped. DIGOXIN
RxNorm: 3407ATC: C01AA05
RITONAVIR BOOSTED PROTEASE INHIBITORSCLASS CODE: J05AE-002
Increase of the digoxinemia, more marked for IV route, due to increase of the absorption of the digoxin or decrease of its renal clearance.
Precaution for useClinical monitoring and, if there is reason for them, EKG and monitoring of the digoxinemia, with possible adjustment of the dosage of digoxin.

Biomedical Informatics9
Extending our overlap comparison to the translated French PDDI dataset• Methods
– Map the drug mentions in the French PDDI to DrugBank • using an RxNorm to DrugBank mapping table
– Compared the drug pairs with other sources• Focused on clinically oriented datasets• Pair-wise matching at the drug ingredient level• Comparison of the information items provided
– Code: https://github.com/dbmi-pitt/public-PDDI-analysis/

The examined datasets Source Description Mapped/
OriginalCategory Data
owner/ Maintainer
Frequency of updates
Crediblemeds.org
A list of clinically important drug-drug interactions
82/83 Clinically-oriented
Crediblemeds.org
As needed
VA NDF- RT PDDIs used until 2014 by the Veteran’s Administration health care system
2,598/5,265 Clinically-oriented
Veterans Health Administration
No future updates. Discontinued
ONC High Priority
A consensus list of PDDIs that are recommended by the Office of the National Coordinator as high priority for inclusion in alerting systems
1,150/1,150 Clinically-oriented
ONC One-time
ONC Non-interruptive
A consensus list of PDDIs that are recommended by the Office of the National Coordinator for use in non-interruptive alerts
2,101/2,101 Clinically-oriented
ONC One-time
DrugBank Comprehensive drug information resource
12,113 Bioinformatics- Pharmacovigilance
DrugBank.ca Roughly bi-annual
WorldVista Comprehensive list of clinically important drug-drug interactions
16,202/44,758
Clinically-oriented
WordVista Twice per year

Biomedical Informatics11
PDDI comparison caveats• Comparisons were with versions of the other
database that were current in late 2014 – might not reflect the current state (though the
ONC data is static and DrugBank and NDF-RT should not have changed much since then)
• Analysis was done using our existing pipeline for expediency [1]. – comparing the PDDIs with the NDF-RT dataset
using RxNorm directly was not feasible due to time restrictions1. Ayvaz S, Horn J, Hassanzadeh O, Zhu Q, Stan J, Tatonetti NP, Vilar S, Brochhausen M, Samwald M,
Rastegar-Mojarad M, Dumontier M, Boyce RD, Toward a complete dataset of drug-drug interaction information from publicly available sources, Journal of Biomedical Informatics. 55 (2015), 206-217. DOI:10.1016/j.jbi.2015.04.006. http://www.sciencedirect.com/science/article/pii/S1532046415000738# PMCID: PMC4464899

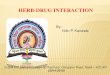
Results – Simple overlapCredibleMeds
Credible Meds
NDF-RT16
(0.6%, 19.5%)
NDF-RT ONC High Priority
8(0.7%, 9.8%)
225(19.6%, 8.7%)
ONC High Priority
ONC Non-interruptive
4(0.2%, 4.9%)
27(1.3%, 1.0%)
2(0.1%, 0.2%)
ONC Non-interruptive
DRUGBANK
57(0.5%, 69.5%)
1296(10.7%, 49.9%)
319(2.6%, 27.7%)
180(1.5%, 8.6%)
DRUGBANK
WordVista16
(0.1%,19.5%)
1024(6.3%,39.4%)
282(1.7%,24.5
%)
326(2.0%,15.5%)
1918(11.8%,15.8
%)https://raw.githubusercontent.com/dbmi-pitt/public-PDDI-analysis/master/analysis-results/WorldVista-analysis-02152016/log-output-OR-analysis.txt

Thinking through these results• WorldVista DrugBank : ~16% – Similar to NDF-RT : ~11%
• DrugBank WorldVista ~12% – Interactions in DrugBank are not listed at the class
level
• WorldVista NDF-RT : ~40%– Comparable to DrugBank : ~50%
• WorldVista ONC High Priority : ~25%– Comparable to DrugBank : ~28%– Comparable to NDF-RT : ~20%

Information needsDrug Information• Pharmacology• Mechanism of action• Formulation • Timing• …
Evidence• Study design• Reporting information
(e.g., funding agency)• Causality assessment
(case reports)• …
Clinical Information• Seriousness• Severity• Time of onset• Manageability• …
Consequences• Adverse effect(s)• Reversibility• Frequency • Modifying and
mitigating factors• …
Recommendation• Monitor, change
drugs, modify strength, adjust timing, etc
• Strength of recommendation

What information in the French PDDI data?Data element CredibleMeds ONC High
PriorityONC Non-interruptiv
e
Drug-Bank
WorldVista
clinical consequences
x* x* x*
Frequency of harm and exposure
Contextual information/modify
ing factors
Drugs involved (terminology code)
x x
Evidence
mechanism x* x† x‡
Recommended actions
x* x*
Seriousness rating x x x
* Provided as unstructured text. †Available on the public website but not explicitly in the downloadable data. ‡ Only computable for CYP3A4 inhibition.

Biomedical Informatics16
What about agreement across sources?1) NDF-RT (2,598), WorldVista (16,202), DrugBank (12,113)
Overlap: 327 -- https://goo.gl/9JpNhZ
2) ONC High Priority (1,150), CredibleMeds (82), WorldVista (16,202)
Overlap: 2 -- https://goo.gl/21aiKz

Biomedical Informatics17
Thoughts about the overlap analysis…• Not surprisingly – pairwise overlap is
fairly poor– Does not really say anything about the
quality of the French dataset – disagreement is common
• Positives– The French dataset is comparable in terms
of overlap to DrugBank and NDF-RT – More frequently updated – Provides more information that can be
structured to aid with decision support

Biomedical Informatics18
Take home point• The WorldVista translation of the French
PDDI dataset is very promising as a “kernel” for a public PDDI knowledge base– To my knowledge, the only truly clinically-
oriented dataset that is actively maintained
• But, more work to be done…– Better structuring of the information to
meet clinical information needs– Connections to evidence

Biomedical Informatics19
Contributions my lab plans to make toward converting the French PDDI dataset to a public drug-drug interaction knowledge base
• Better structuring of the information to meet clinical information needs
• Connections to evidence

Biomedical Informatics20
Better structuring of the information to meet clinical information needs• drugs involved,
• seriousness,
• clinical consequences,
• mechanism of the interaction,
• contextual information/modifying factors,
• recommended action(s), and
• evidence

Biomedical Informatics21
Example• Warfarin – NSAIDs
– Current example• http://goo.gl/1W0k6A • https://www.dikb.org/Merged-PDDI
– Decision tree• See PDF

Data element Valueclinical
consequences Increase of the oral anticoagulant’s risk of hemorrhage, especially
upper gastrointestinal bleeding (UGIB)
Frequency of harm and exposure
INFORMATION NEEDED
Contextual information/modi
fying factors
Mitigating: topical diclofenac [1], patient also taking on proton pump inhibitor or misoprostol
Predisposing: history of UGIB or peptic ulcer, > 65 years old, systemic corticosteroids, aldosterone antagonist [2], high dose or multiple NSAIDs
Drugs involved (terminology
code)
NSAIDS: http://goo.gl/E9yNiY Oral Anticoagulants: http://goo.gl/BdMvZt
Evidence 1. In one study a topical gel (16 g/day) produced about 6% of the absorption seen with systemic administration of 150 mg/day. A higher than recommended dose of topical gel (48 g/day) produced 20% of a systemic dose of diclofenac.
2. Both corticosteroids and aldosterone antagonists have been shown to substantially increase the risk of UGIB in patients on NSAIDs, with relative risks of 12.8 and 11 respectively compared to a risk of 4.3 with NSAIDs alone (Masclee et al. Gastroenterology 2014;147:784-92.)
mechanism Non-steroidal anti-inflammatory drugs (NSAIDs) have antiplatelet effects which increase the bleeding risk when combined with oral anticoagulants such as warfarin. The antiplatelet effect of NSAIDs lasts only as long as the NSAID is present in the circulation, unlike aspirin’s antiplatelet effect, which lasts for up to 2 weeks after aspirin is discontinued. NSAIDs also can cause peptic ulcers and most of the evidence for increased bleeding risk with NSAIDs plus warfarin is due to upper gastrointestinal bleeding (UGIB).
Recommended actions
With only mitigating factors present: Assess risk and take action if necessary
With one or more predisposing factors present: Use only if benefit outweighs risk
Seriousness rating
If the NSAID is topical diclofenac then Clinically inconsequential, otherwise Interruptive

Biomedical Informatics23
PDDI Minimum Information Task Force• Formed to create broad consensus
on the definitions and content of information to be structured– https://goo.gl/MDq2Ye

Biomedical Informatics24
Meet the PDDI Minimum Information Task Force:• volunteer-based – currently ~40
participants– WorldVista, W3C, AMIA
Pharmacoinformatics, ISPE, and academics
• broad stakeholder involvement– NLM, ASHP, industry, academic
institutions • Open public participation
– formed within the Health Care and Life Sciences Interest Group that operates publicly through the World Wide Web Consortium (W3C)

Task force objective and deliverables• Objective: Develop a minimal information
model for drug interaction evidence and knowledge as part of an HIT standard like HL7
• Deliverables: using an interesting and non-trivial set of potential drug-drug interactions:– Data Model: A data model (schema) for potential
drug interaction knowledge and evidence– Vocabulary: A precise vocabulary
describing/defining the data model– Serializations: one or more serialization formats of
the abstract data model, such as Structured Product Labeling (HL7 CDA), JSON/JSON-LD)
– Demonstration of how the minimum information model can support medication reconciliation

Biomedical Informatics26
Possibly one of the most important deliverables….• Create a foundation for further
collaborative work by disseminating results through an interest group note, a website, and an online discussion forum– https://forums.dikb.org

Progress so far…• Selected most of the PDDIs to focus on
– https://goo.gl/rYpmjt– Decision trees developed for:
• Warfarin - NSAIDs• KCL – K-sparing diuretcs• Beta-blocker – Epinephrine
• Agreement on the scope of knowledge representation
• Definitions for major categories in process• Initial format of draft W3C Interest Group
Note– http://goo.gl/DkKSwj

Biomedical Informatics28
Contributions my lab plans to make toward converting the French PDDI dataset to a public drug-drug interaction knowledge base
• Better structuring of the information to meet clinical information needs
• Connections to evidence

Data element Valueclinical
consequences Increase of the oral anticoagulant’s risk of hemorrhage, especially
upper gastrointestinal bleeding (UGIB)
Frequency of harm and exposure
INFORMATION NEEDED
Contextual information/modi
fying factors
Mitigating: topical diclofenac [1], patient also taking on proton pump inhibitor or misoprostol
Predisposing: history of UGIB or peptic ulcer, > 65 years old, systemic corticosteroids, aldosterone antagonist [2], high dose or multiple NSAIDs
Drugs involved (terminology
code)
NSAIDS: http://goo.gl/E9yNiY Oral Anticoagulants: http://goo.gl/BdMvZt
Evidence 1. In one study a topical gel (16 g/day) produced about 6% of the absorption seen with systemic administration of 150 mg/day. A higher than recommended dose of topical gel (48 g/day) produced 20% of a systemic dose of diclofenac.
2. Both corticosteroids and aldosterone antagonists have been shown to substantially increase the risk of UGIB in patients on NSAIDs, with relative risks of 12.8 and 11 respectively compared to a risk of 4.3 with NSAIDs alone (Masclee et al. Gastroenterology 2014;147:784-92.)
mechanism Non-steroidal anti-inflammatory drugs (NSAIDs) have antiplatelet effects which increase the bleeding risk when combined with oral anticoagulants such as warfarin. The antiplatelet effect of NSAIDs lasts only as long as the NSAID is present in the circulation, unlike aspirin’s antiplatelet effect, which lasts for up to 2 weeks after aspirin is discontinued. NSAIDs also can cause peptic ulcers and most of the evidence for increased bleeding risk with NSAIDs plus warfarin is due to upper gastrointestinal bleeding (UGIB).
Recommended actions
With only mitigating factors present: Assess risk and take action if necessary
With one or more predisposing factors present: Use only if benefit outweighs risk
Seriousness rating
If the NSAID is topical diclofenac then Clinically inconsequential, otherwise Interruptive

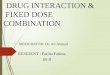
Example of the need to connect evidence
ATORVASTATINRxNorm: 83367 ATC: C10AA05
CLARITHROMYCINRxNorm: 21212 ATC:J01FA09 A02BD06 A02BD07 A02BD05 A02BD04
Increased risk of undesirable effects (concentration-dependant) of the rhabodmyolysis type due to decrease of the hepatic metabolism of the cholesterol-lowering drug
Precaution for useAdminister weaker doses of cholesterol-lowering agent. If the therapeutic objective is not reached, use another statin not affected by this type of interaction
DrugBank: “The macrolide, clarithromycin, may increase the toxicity of the statin, atorvastatin.”
WorldVista:

Biomedical Informatics31
Questions about clarithromycin – atorvastatin PDDI• What is the mechanism – pharmacokinetic
or pharmacodynamic?• What is the expected magnitude of
pharmacokinetic effect?• What potential frequency of the adverse
event (rhabdomyolysis) relative to other statins w/ and w/out clarithromycin?
• What are factors that increase or decrease those risks?

Primary data
Authors using annotation toolsNew evidence
items
Existing evidence items
Argument graphs
Product label,Journal article,Other…
Claim
Support
Reference
• “drug X interacts with drug Y
• drug X inhibits enzyme Q
• Data• Materials• Methods
• Literature• Product label• Other…
Authors using annotation tools

Evidence annotation example

Evidence annotation example…

Biomedical Informatics35
Progress so far…• Annotated pharmacokinetic interactions
for 65 drugs – The evidence board for my R01 project
Addressing gaps in clinically useful evidence on drug-drug interactions" (R01LM011838)
– All drug product labeling completed• Plan to release this fall
– ~300 full text articles screened • Complete annotation beginning this summer• Plan to release next Spring

Biomedical Informatics36
Progress so far…• A proposed standard approach for
assessing the existence of an interaction– Based on two AHRQ-funded
conference series have brought together a wide spectrum of stakeholders
Scheife RT, Hines LE, Boyce RD, Chung SP, Momper JD, Sommer CD, Abernethy DR, Horn JR, Sklar SJ, Wong SK, Jones G, Brown ML, Grizzle AJ, Comes S, Wilkins TL, Borst C, Wittie MA, Malone DC. Consensus Recommendations for Systematic Evaluation of Drug-Drug Interaction Evidence for Clinical Decision Support. Drug Saf. 2015 Feb. 38(2):197-206 http://link.springer.com/article/10.1007%2Fs40264-014-0262-8. PubMed PMID: 25556085.

PDDI evidence assessment
Sufficient Evidence?
• Conflicting evidence• Magnitude of effect• Biological
plausibility
Clinically Relevant?
• Clinical Consequences• Frequency• Modifying factors• Seriousness
How to Present DDI Information
?
• Seriousness• Recommended
actions• Strength of
evidence • Strength of
recommendations

The DRug Interaction eVidence Evaluation (DRIVE) Instrument (being tested)
Category Evidence
Sufficient evidence that a drug interaction exists and can be evaluated for clinical relevance
One or more of the following: Well-designed and executed, prospective controlled studies Well-designed and executed, observational studies Case reports or series demonstrating probable or highly
probable causality of an interaction (Drug Interaction Probability Score of 5-10)
Reasonable extrapolation on the basis of studies of drugs with similar pharmacologic properties
Reasonable extrapolation on the basis of studies with in vitro substrate data
Reasonable extrapolation on the basis of human genetic polymorphism studies
Insufficient evidence that a drug interaction exists
One or more of the following, without supporting evidence from the “sufficient” category: Extrapolation on the basis of studies with in vitro inhibitor or
inducer data Case reports or series demonstrating only possible or doubtful
causality of an interaction (Drug Interaction Probability Score of <5)
Studies of poor design or execution Hypothesis-generating research methods Animal data Unsubstantiated statements in product labeling and regulatory
documents “Data on file” from product sponsors/manufacturers

Biomedical Informatics39
Evaluating DRIVE• Phase 1: “usability” evaluation
– Completed
• Phase 2a: interrater reliability– In progress! – 15 participants enrolled
• Phase 2b: empirical evaluation of in vitro data– In process

Biomedical Informatics40
Conclusions• While challenging, progress is being
made toward a high quality, open source, PDDI knowledge base– But it will require sustained involvement by
a broad group of stakeholders

Biomedical Informatics42
Acknowledgements - Funding• The American taxpayers via:
– NLM (R01LM011838 and T15 LM007059-24)– NIH/NIA (K01AG044433, K07AG033174)– Agency for Healthcare Research and Quality
(K12HS019461 and R01HS018721) – NIH/NCATS (KL2TR000146)– NIH/NIGMS (U19 GM61388; the
Pharmacogenomic Research Network)

Biomedical Informatics43
Acknowledgements - People• Co-investigators: Harry Hochheiser, Phil Empey, Carol
Collins (UW Seattle), John Horn (UW Seattle), Dan Malone (U of A), Lisa Hines (U of A), William Hogan (UAMS), Mathias Brochhausen (UAMS)
• Programmers, staff, postdocs: Yifan Ning, Wen Zhang, Katrina Romagnoli, Jodi Schneider (U of Pitt), Amy Grizzle (U of Arizona), Scott Nelson (Vanderbilt)
• Students and Research assistants: Sam Rosko, Steven DeMarco (U of Pitt), Nikolas Milosevec (U of Manchester)
• Advisors: Rebecca Crowley, Michel Dumontier (Stanford, W3C), Matthias Samwald (Medical U of Vienna), Tim Clark and Paulo Ciccarese (Harvard), Robert Freimuth (Mayo, PGRN)
• Additional stakeholders: FDA, Cochrane, W3C Health Care and Life Sciences Interest Group, ASHP, IBM Research, OHDSI

Biomedical Informatics44
Discussion