Embed Size (px)
Citation preview

1

Indian health systemOverview, issues & challenges
Prashanth N S MBBS, MPH, PhD
Institute of Public Health, Bengaluru

3
Outline• Part 1: Introduction, human resources in health in India, health
(in)equity patterns in India and social determinants of health
• Part 2: Structure and functioning of the health system and services in India with respect to – Health Services– The disease burden– Human resources– Medicines– Governance– Financing of Indian health services
• Part 3: Bringing it together – health system frameworks

4
India• India is a
– Sovereign– Socialist– Secular– Democratic– Republic
• Promote – Justice– Liberty– Equality– Fraternity

5
India - Demography
• 1.21 billion people• 74% literacy; 65 F literacy• 30% of population live in urban area• 940 females per 1000 males• 47% of population are below 25 years

6
India - Social
• Secular – Hindus (83%), Muslims (13%), Christians (2%), Others (2%)
• Social stratification along caste lines though the system is abolished
• 38% of population classified as socially vulnerable

Do health workers save lives? More health workers, more health. True?

Do health workers save lives?
• Doctor anomaly
• Cardiologists’ holiday paradox

WHR 2006

WHR 2006

WHR 2006

Karnataka state– Regional/sub-regional disparitiesRole of (mis)management?
For example, in 2006Immunisation coverage – 96% in Kodagu district and <50% in Raichur.
114 ‘backward’ talukas, nearly half in ‘forward’ districts
“Systemic failure” as a cause? (George, 2007&2009), Sen (2006)

NS Prashanth, PhD Committee meeting, UCL
13
What is capacity?
Brown, L., LaFond, A., & Macintyre, K. (2001). Measuring capacity building. Chapel Hill: MEASURE Evaluation.
06/12/13

A few characteristics of HR/health systems

So, then what is a system? Is it called a system because it works “systematically”?
-> Systems thinking

Complexity
• Simple, complicated and complex problems• Health service versus a health system…& HR (& health) systems are complex…

WHO – Alliance for Health Policy and Systems Research

Layered dimensions of HRM in a system
• Individual• Institutional (workplace)• Meso/Macro policy level factors• Environmental, societal, socio-political

19
Inequities

20
India – a land of contrasts

21
India – a land of contrasts

22
India – a land of contrasts

23
Layered inequalities• Economic
inequalities most well researched & possibly most “obvious”
• Economic inequalities: income, wealth and consumption (also applies to health)
Barton and Grant (2006) adaptation of Dahlgren and Whitehead (1991)

24
Indian health system worsens income/class inequity
• Healthcare expenditure financed by people out of pocket, at the point of service delivery (high OOPs)
• Poor social protection: Neither universal nor well targeted
Oxfam

25
Class/income inequalities
• Income positively correlated with health outcomes globally
• Income as one of the drivers of health
• The poor cannot buy into health

26
Equity ≠ Equality• Absence of particularly unfair
differences; Social and political disadvantages -> adverse societal conditions that prevent these populations/population sub-groups from realising individual measures to overcome health or social inequalities.
• “ (lack of) social justice is killing people on a grand scale”
• “inequitable distribution of power, money and resources as one of the underlying causes of inequities in health”.

27
Broad patterns and correlates• Clear income gradient in public health across states and districts with positive associations with
literacy and rural residence. Wealth strongest marker of anaemia status, more so than education and caste
• Economic constraints influence choice of various health services, in several contexts public services “a lesser good” (cf. childbirth, inpatient care, skilled birth attendance)
• Unequal access to a variety of services, schemes and programmes for poorer sections
• Somewhat a pattern of rich seeking care in for-profit organised private while the poor delaying care or at public (although not generalisable)
• Postnatal care most unequal among maternal health services (cf. discrimination)
• Although inequalities generally lower in economically better-off states (many of them in south India), paradoxically being in a “better-off” state not always good for the poor in these states. Similar patterns in outcomes (cf. U-5 mortality inequalities better in “poorer” states, but…)
IPH/Shree Chitra Equity mapping 2015

28

29
Part 2: System vs services
• What is Indian health services like? • How is it perceived and utilised by different
sections of the population?• What is the disease burden and how is it
financed?• How does the Indian health system perform
with respect to enabling health and social protection?
30
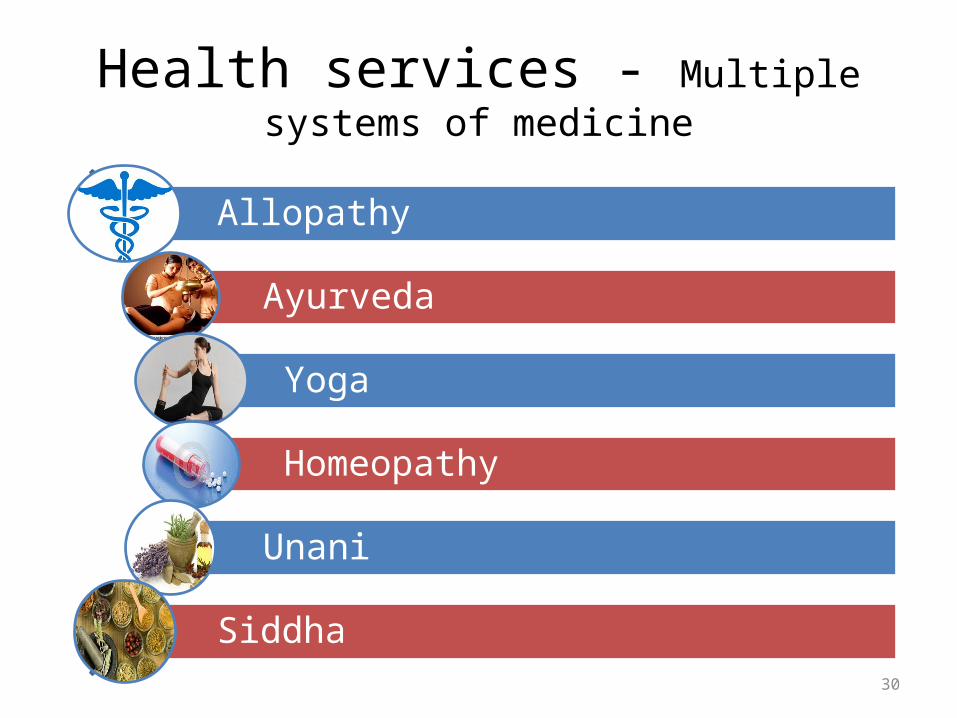
Health services - Multiple systems of medicine
Allopathy
Ayurveda
Yoga
Homeopathy
Unani
Siddha

31
Health services – multiple providers
• Certified / Uncertified
• Government / Private / Private not-for-profit

32
Health services – multiple facilities

33

34

35

36
Organisation of Health services

37
Health services – Govt. & Private
G - U
G - R
P -U
P -R
NSSO

38
Provision of health services
Outpatient care Inpatient care Deliveries0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
22%
42%
Government; 52%
Private , 78%
58%38%
NSSO data

39
India – disease burden
IHME2010India

40
Medicines
• Under Ministry of Chemicals• Largest producer of generics in the world• Multi billion dollar industry• Regulatory policies exist, but not implemented• Medicines freely available – over the counter• Government spends just € 0.10 cents per
person on medicine

41
Financing of health care
Mostly through out of pocket payments by
individual patients at the time of illness

42
Sources of financing for health
State Govt; 12%
Federal Govt; 7%
Local Govt; 1%
OOP; 71%
Firms; 6%
Insurance; 1% External aid; 2%

43
Health financing – source of funds
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 20100
10
20
30
40
50
60
70
80
90
100
Government
39
Out-of-pocket
94
Int.
$ PP
P

44
Health insurance in IndiaNumber of people covered (millions)
Social health insurance*
Private health insurance #
Government health insurance ^
Outpatient 58
Secondary care 58 55 130
Tertiary care 58 117
TOTAL 58 55 147
* - Civil servants
# - Mostly the formal sector high & middle-income groups
^ - Those below the poverty line

45
Effect of this
• Inadequate health staff in the government sector– 0.6 doctors per 1000 population– 1 doctor to 1.3 nurses
• Inadequate medicines in the government sector

46
Effect of this ….
Financial barrier
Do not seek care
Seek sub standard care Seek care
Manage with savings Borrow Sell Asset Labour
substitution

47
Effect of this …
63 Million Indians are impoverished every year
because of medical expenses
48
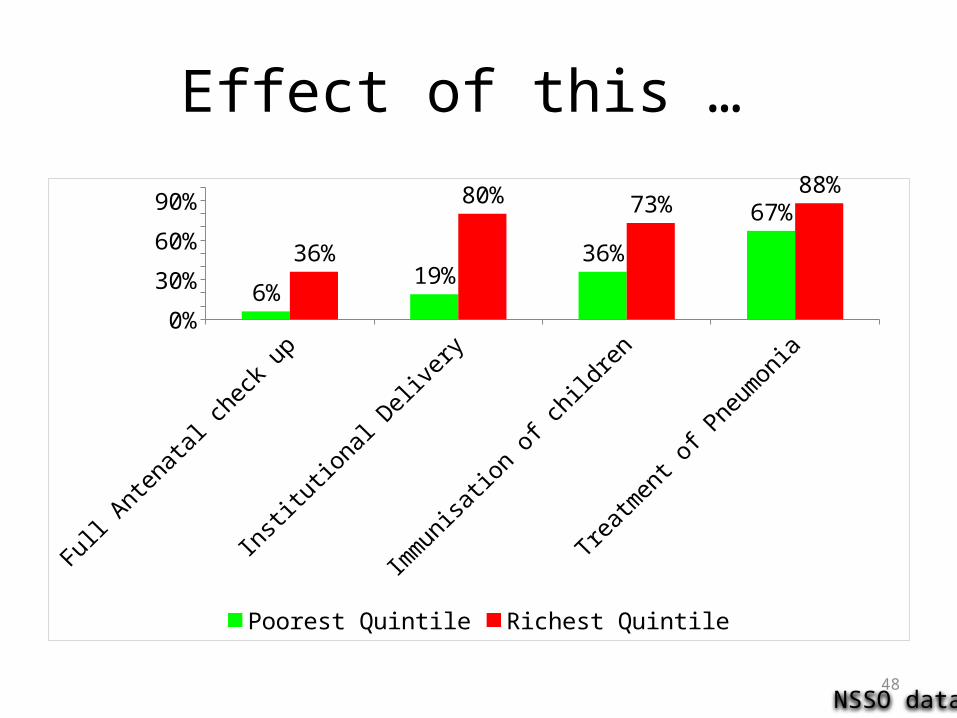
Effect of this …
Full A
ntenatal ch
eck up
Institutional
Delivery
Immunisa
tion of child
ren
Treatment o
f Pneumonia
0%
20%
40%
60%
80%
100%
6%19%
36%
67%
36%
80% 73%88%
Poorest Quintile Richest Quintile
NSSO data

49
Effect of this …
• Multi billion dollar industry – US$ 80 billion and growing @ 17%
http://www.ibef.org/industry/healthcare-india.aspx

50
Government response
• 2005 – National Rural Health Mission
• 2008 – National Health Insurance Scheme
• 2015 – Subsidised medicines to all
But Government health expenditure still remains at 1.1% of GDP

51
Governance• Many regulations
– Drugs– Medical practice– Infrastructure– Certification of health staff– Medical negligence– Food safety– Pollution control
• Many ministries – Health, Medical education, Chemicals, Environment, Food and Civil Supplies, Water and Sanitation, Women and Child Welfare, etc.
But poorly implemented

52
Health status - Life expectancy (in years)
18001813182618391852186518781891190419171930194319561969198219952008-5
5
15
25
35
45
55
65
75
85
India
66
Sri Lanka
74
UK
81
Year
s

53
Health status – under nutrition
54
Part 3
• Assessing a health system: frameworks

55
Eg framework:Building Blocks & Systems Thinking
WHO 2007, WHO 2009

56
Eg: Reform/Control Knobs framework
Roberts et al, 2004

57
Framework – a full overview?
• Who are actors in the Health System?• What are issues in the Health System?
Leadership & governance:* policy – making
* regulation* coordination
Organisation and delivery of health care services:
* primary health care – specialised * health problem specific – general
* prevention – curative care* public – private, for profit – not for profit,
formal - informat
Guiding by values and principles:* health care as a right* autonomy <> security
* protection of public <> response to individual suffering * effectiveness <> efficiency
* participation, accountability, trust* social justice and equity
* global social responsibility* sustainability: at which level?
Outcomes:* universal access
* quality of care
Goals:* improved health* responsiveness * social & financial
protection
Interaction with context:* with national policies, culture, values
* with international context* with other sectors and actors
Interaction with population:* demand generation
* participation of individuals and groups in community* accountability
human resources
Organisation of resources:
financing
Medical supplies & technologies
Monitoring & evaluation / information
1
2
3
4 56 7
8
9
10
1
Van Olmen et al, Institute of Tropical Medicine, Antwerp

58
Conclusion• A complex health system
– Pluralistic providers– A strong and unregulated private sector– Financed mostly by individual households at the point of care– Wide range of services, quality and access– Government trying hard to regain control
• Double burden of CD and NCD
• Inadequate and inefficient expenditure by the government on health services

59
Conclusions
Has money?YES NO
Reasonable to high quality of care in
private health sector
Reasonable to poor quality of care in
government / private health sector

With inputs of Dr. Devadasan, IPH
Assistant Director (Research), IPHChairperson, Emerging Voices for Global Health
web @daktre.comedits @Wikipedia/User:Prashanthns
Researchgate ORCID Goodreads Scholar