Embed Size (px)
Citation preview

In the NOACs era , how to deal with liver cirrhosis needing anticoagulation?
Magdy El-Masry.Prof. of Cardiology , Tanta University. “CardioEgypt 2017”

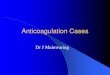
The liver is responsible for a plethora of processes

The coagulation network.
APC: Activated protein C; AT-III: Antithrombin III; CA: Contact activator; F: Fibrin; PC: Protein C; PS: Protein S; TF: Tissue factor; Tmod: Thrombomodulin; VKO: Vitamin K epoxide; XF: Cross-linked fibrin

The liver is responsible for a plethora of processes
Hepatic dysfunction affects all of these processes; however, various models of liver disease severity focus on only a select few.

Indeed, the Model for End-stage Liver Disease (MELD) incorporates only the bilirubin, INR, and creatinine , with the largest weight
given to the INR.

Is My Cirrhotic Patient Auto-anticoagulated?Cirrhotic patients often present with elevated
INR as a result of coagulopathy
Does "Auto-anticoagulation" Protect Against thrombosis in Patients with Liver Disease?
The "auto-anticoagulation" does not protect against thrombosis.
This is a case of "bad news and more bad news": An elevated INR in a patient with cirrhosis
predisposes to bleeding and also does not protect against thrombosis.

Coagulation Levels
INR aPTT Anti-Xa
Effect of cirrhosis
↑ ↑ ↓
Cirrhosis and Coagulation Tests
Cirrhosis affects production of both procoagulant and anticoagulant factors , thus resulting in increased INR
and aPTT levels and decreased anti-Xa levels.

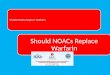
The normal balance of hemostasis and rebalanced hemostasis in liver disease:
Because of the relative deficiency of both procoagulantand anticoagulant factors in chronic liver disease, the balance is more fragile and more easily tipped toward bleeding or thrombosis.
Hemostatic stability
Hemostatic instability

Primary hemostasis: high VWF levels and low ADAMTS 13 levels counteract defects in primary hemostasis. Coagulation: reduced levels of procoagulant factors are balanced by a parallel decline in anticoagulant factors. Fibrinolysis: fibrinolysis is rebalanced by parallel changes in profibrinolytic and antifibrinolytis proteins. VWF indicates von Willibrand factor; ADAMTS 13, a disintegrin & metalloproteinase with thrombospondin type 1 motif 13; PC, protein C; PS, protein S; AT,antithrombin; * does not occur consistently in chronic liver disease; and **end-stage liver disease .
Promoting bleeding Promoting clotting
Thrombosis Bleeding
Rebalanced hemostasis in chronic liver
disease.

Should we anti-coagulate patients with cirrhosis?Cardiologist
Stroke prevention in AF
prevention & treatment
of VTE (DVT/PE)Hepatologist
Risk of portal vein thrombosis
Crosstalk Between the Hepatologist and the Cardiologist:Risk of Bleeding

How safe is anticoagulation therapy to use in those with chronic liver disease?
No studies have been conducted examining anticoagulation in cirrhosis patients for VTE or atrial fibrillation.
Unfortunately, RCTs universally exclude cirrhosis patients.
Anticoagulation In Difficult Clinical Scenarios.
Anticoagulation in Patients With Cirrhosis.

“Caught between a rock and a hard place"
A hard place A rock

The Search for the "Ideal" Anticoagulant: Where Are We Now?
The ideal anticoagulant does not exist.
In all likelihood it will never exist.


Pros and Cons of Anticoagulants in Cirrhotic Patients.
Annals of Pharmacotherapy.2016,vol.50(5)402-409

Summary of Pros and Cons of Anticoagulants in Cirrhotic Patients.
Low-molecular-weight heparin (LMWH)
ProsGood safety profile in patients with cirrhosis and DVT/PVT Experience up to 2 years in prophylaxis treatment for PVTAnticoagulant effect is rapidly reversible in case of
hemorrhagic complications
Cons Inconvenient and associated with poor complianceRenal adjustments may be tricky (serum creatinine may be falsely low)Acts on antithrombinHeparin-induced thrombocytopenia (HIT)Cannot use anti-Xa to estimate therapeutic effect

Summary of Pros and Cons of Anticoagulants in Cirrhotic Patients.
Unfractionated heparin (UFH)
ProsPotential option in patients with concomitant renal failureAnticoagulant effect is rapidly reversible in case of
hemorrhagic complications
ConsCannot be used practically and conveniently for long-term
treatmentHigher potential for HIT

Summary of Pros and Cons of Anticoagulants in Cirrhotic Patients.
Fondaparinux
ProsOption for patients with HIT
ConsActs on antithrombinAccumulation in renal and liver disease Inconvenient and associated with poor compliance Limited data exist in the use of fondaparinux in
cirrhotic patients

Summary of Pros and Cons of Anticoagulants in Cirrhotic Patients.
Warfarin
ProsOral mode of administration Supratherapeutic level is reversible
ConsRequires close monitoringCannot distinguish between INR resulting from warfarin vs
cirrhosisAltered metabolism as a result of liver dysfunctionDrug-drug interactionsDrug-food interactions

Summary of Pros and Cons of Anticoagulants in Cirrhotic Patients.
Novel Oral Anticoagulants (NOACs)
ProsNo monitoring requiredOral mode of administration
ConsContraindicated because of lack of data
(Patients with cirrhosis were excluded from RE-LY, ROCKET AF,
and ARISTOTLE )

Matching the NOAC to the Patient

Which NOAC for Which Patient?

Because all NOACs are dependent on the liver for metabolism to some degree, patients with hepatic dysfunction are not ideal candidates for these agents, especially if there is pre-existent
evidence of coagulopathy (an elevated INR ).
Restrictions for the use of NOACs in patients with liver disease are based on the Child-Pugh classification system
and exclusion criteria applied in pivotal trials.
NOACs in liver disease – is there a problem?


Sydney , Australia
No current guidelines exist to guide clinicians,when caring for cirrhosis patients with thrombosis or other indications for anticoagulation

Considerations prior to commencing NOAC therapy
Hepatic impairment : Child-Pugh estimates cirrhosis severity
Dabigatran (Pradaxa® )
Contraindicated - Child-Pugh C Use with caution - Child-Pugh A or B
Apixaban (Eliquis® )
Contraindicated in hepatic disease associated with coagulopathy and clinically relevant bleeding risk, including severe hepatic impairment (Child-Pugh C)
May be used with caution in patients with mild or moderate hepatic impairment (Child-Pugh A or B)
Rivaroxaban (Xarelto® )
Contraindicated - Child-Pugh B or C Use with caution - Child-Pugh A

Monitoring in patients with chronic liver disease
Unfractionated heparin Monitor by APTT as the test for dose adjustment; aim for
therapeutic interval of 1.5-2.5 prolongation over the normal value. However, recognise that the decreased antithrombin levels in the
plasma of patients with CLD may lead to falsely elevated APTT in cirrhotics treated with heparin ; interpret APTT levels with caution.
Low-molecular-weight heparin No routine laboratory monitoring required; anti-Factor Xa is
probably a poor measure of the anticoagulation effect of LMWH in those with cirrhosis.

Monitoring in patients with chronic liver disease
WarfarinAim for INR in therapeutic interval of 2.0 – 3.0, but recognise the limitations of the use of INR for this purpose in those with chronic liver disease
Novel Oral Anticoagulants Very limited experience in chronic liver disease, but no routine
laboratory testing used.

Potential complications specific to those with chronic liver disease
Unfractionated heparin*In vitro data suggest that cirrhotics may have increased sensitivity to the anticoagulant effect of unfractionated heparin *Increased risk of thrombocytopenia (potentially because of heparin-induced thrombocytopenia) when used in cirrhotic patient
Low-molecular-weight heparin In vitro data suggest that cirrhotics may have increased sensitivity to the anticoagulant effect of LMWH

WarfarinNo potential complications specific to those with chronic liver disease beyond those with VKA in general.
Novel Oral Anticoagulants Dabigatran
In vitro data suggest that cirrhotics may have much increased sensitivity to the anticoagulant effect of dabigatran
Rivaroxaban, apixiban In vitro data suggest that cirrhotics may have reduced sensitivity to the anticoagulant effect of these agents
Potential complications specific to those with chronic liver disease

Reversal agentsUnfractionated heparin & Low-molecular-weight heparin Protamine-sulphate
WarfarinOptions including vitamin K, prothrombin complex concentrate and fresh frozen plasma, depending upon urgency and/ or product availability
Novel Oral Anticoagulants Dabigatran : Idarucizumab(Praxbind)Rivaroxaban, apixiban :Antidotes still at trial stage but likely to come to market soon, e.g. andexanetConsider prothrombin complex concentrates , antifibrinolytics

Conclusions : NOACs are not associated with an increased risk of DILI.
Risks of hepatoxicity with NOACs


Adequately powered studies examining safety and efficacy of these NOACs in a wider variety of cirrhosis patients are now needed.
Cirrhotic patients are not absolutely protected from thrombotic events despite their elevated INR and auto-anticoagulation.
Several anticoagulation drugs are available for clinical use including several NOACs.
Each drug has its own advantages and disadvantages.
Still no consensus is available regarding the preferred anticoagulant agents used in cirrhosis.
Conclusions