Embed Size (px)
Citation preview

Anticoagulation Update: DOACs, VTE Guidelines, “Bridging”
and iCentra (whew!)
Scott C. Woller, MD Co-Director, Thrombosis Program Intermountain Medical Center Professor of Medicine University of Utah School of Medicine
Clinical Learning Day 2016

Disclosures
• Investigator initiated grant recipient: Bristol-
Myers-Squibb (paid to Intermountain Healthcare)
• Panelist American College of Chest Physicians (ACCP) Clinical Practice Guideline: Antithrombotic therapy for venous thromboembolic disease (AT10)

Objectives • DOAC limitations & use in routine clinical care
– Special populations
• AT10 Updates: Venous Thromboembolism • Anticoagulation procedural interruption (“bridging”)
– Warfarin – DOACs
• Why & how to manage anticoagulation in iCentra

The Direct Oral Anticoagulants

The Direct Oral Anticoagulants Rivaroxaban Apixaban Edoxaban Dabigatran
BRAND NAME PHARMACEUTICAL
Xarleto™ Bayer
Eliquis™ BMS & Pfizer
Savaysa™
Daiichi Sankyo Pradaxa™
Boehringer Ingelheim
TARGET Factor Xa Factor Xa Factor Xa Factor IIa
BIOAVAILABILITY (%) ~80 ~50 62 6–7
TIME TO PEAK (h) 2–3 1–2 1-2 1.5
HALF-LIFE (h) 9-13 8-15 9-10 12-14
RENAL EXCRETION (%) 33 25 35 >80
EFFECT ON aPTT/PT* 1.8/2.6 1.2/~2 yes 2.3/NR
EFFECT ON Xa 68% NR NR No Effect
DRUG INTERACTIONS CYP3A4 IND/INH CYP3A4 INH P-gp INH/CYP3A4 Verapamil/rifampin
Derived from: Crowther. Blood. 2008;111:4871-4879; Garcia, D. Blood. 2010;115:15-20; http://www.eliquis.com/PDF/ELIQUIS%20%C2%AE%20(apixaban)%20SmPC.pdf Schulman Thromb Haemost 2014; 111:

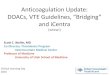
Choosing a DOAC vs. warfarin in AF
Ruff CT et al. Lancet 2014; 383: 955–62

Choosing a DOAC vs. warfarin in AF
Ruff CT et al. Lancet 2014; 383: 955–62 *TTR > 66%
*

AT10 Summary of evidence: Recurrent VTE
QUESTION: Should a DOAC or warfarin be used for acute and long-term treatment of VTE ? Quality assessment Summary of Findings
NOAC n (studies)
Risk of bias Overall quality of evidence
Study event rates (%) Relative effect
(95% CI)
Anticipated absolute effects With LMWH
and VKA With NOAC Risk w/
LMWH &VKA
Risk difference with NOACs
(95% CI)
Recurrent VTE RIVAROXABAN 8281 (2 studies)
no serious risk of bias
⊕⊕⊕⊝ MODERATE
due to imprecision
95/4131 (2.3%)
86/4150 (2.1%)
RR 0.90 (0.68 to 1.2)
23 per 1000 2 fewer per 1000 (from 7 fewer
to 5 more)
DABIGATRAN 5107 (2 studies)
no serious risk of bias
⊕⊕⊕⊝ MODERATE
due to imprecision
55/2554 (2.2%)2
60/2553 (2.4%)
RR 1.12 (0.77 to
1.62)
22 per 1000 3 more per 1000 (from 5 fewer to 13 more)
APIXABAN 5244 (1 study)
no serious risk of bias
⊕⊕⊕⊝ MODERATE
due to imprecision
71/2635 (2.7%)
59/2609 (2.3%)
RR 0.84 (0.6 to 1.18)
27 per 1000 4 fewer per 1000 (from 11 fewer
to 5 more)
EDOXABAN 8240 (1 study)
no serious risk of bias
⊕⊕⊕⊝ MODERATE
due to imprecision
146/4122 (3.5%)3
130/4118 (3.2%)
RR 0.83 (0.57 to
1.21)
35 per 1000 6 fewer per 1000 (from 15 fewer
to 7 more)

From the clinical trials:
• Need for thrombolytic therapy • An indication for anticoagulation for which no DOAC approval exists • High risk of bleeding • Significant liver disease (hepatitis, cirrhosis, or AST/ALT ≥ 3x ULN) • Creatinine clearance 30 mL/min (apixaban threshold was 25 mL/min) • Aspirin use (100 mg/day) • Concomitant use of interacting medications • Uncontrolled hypertension
Who is not?
Who is a candidate for a DOAC therapy to treat VTE?
Schulman S (2013) N Engl J Med 368:709–718. EINSTEIN Investigators (2010) N Engl J Med 363:2499–2510. Agnelli G (2013) N Engl J Med 368:699–708. Schulman S (2009) N Engl J Med 361:2342–2352. Schulman S (2014) Circulation 129:764–772 EINSTEIN–PE Investigators (2012). N Engl J Med 366:1287–1297. Agnelli G (2013) N Engl J Med 369:799–808. Hokusai-VTE Investigators (2013) N Engl J Med 369:1406–1415.

From the school of hard knocks:
• Patients who struggle with compliance (unless related to transportation for INRs) • Warfarin is likely favorable to allow ascertainment of and
anticoagulant effect
• Financial barriers to longitudinal compliance • After 1.1 year f/u <50% prescribed DOAC picked up adequate
drug to cover 80% days
Who is not?
Who is a candidate for a DOAC therapy to treat VTE?
Kearon C AT10 Chest 2016; Yao, X Chest Physician Vol. 11, No. 2 Feb. 2016

DOAC therapy: Special populations

Pregnancy
Candidates for a DOAC therapy: Special populations
XARELTO-PM-ENG-10JUL2014-172618.pdf. http://www.bayer Boehringer Ingelheim Canada Ltd (2014) Pradaxa product monograph. http://www.boehringeringelheim.ca; images from: colorbox.com; dailykos.com; Bapat P et al.. J Thromb Haemost 2016; 14: 1436–41.; Bapat P etal. Obstet Gynecol 2014; 123: 1256; 15 Bapat P etal. Am J Obstet Gynecol 2015; 213: 710.e1–6.
+ Dabigatran or rivaroxaban =
• Apixaban has no human data in pregnancy, but showed no maternal or fetal harm in animal studies • Ex vivo drug concentration across placenta F:M ratio 0.9
• Edoxaban animal studies demonstrated no fetal harm
• DOAC excretion in breast milk is not known.

Pregnancy
Candidates for a DOAC therapy: Special populations
dailykos.com

Extremes of weight
Candidates for a DOAC therapy: Special populations
• Evidence is limited • Patients <50–60 kg were 2–13 % of DOAC study populations &
16 % of patients were >100 kg • 1 meta-analysis showed that for patients >100kg recurrent VTE
risk was 0.9 (95% CI 0.77-1.06) • Dabigatran does not appear to be affected by extremes of weight • Weight may affect kinetics of anti-Xa’s but the clinical significance
is unknown. • ISTH and AC Forum suggest against use based on PK/PD in obese
Schulman NEJM 2009; EINSTEIN Investigators NEJM 2010; AMPLIFY NEJM 2013; HOKUSAI NEJM 2013; Stangier DJ Clin Pharmacokinet 2008; Frost J. thromb Haemost 2009; Upreti VV 2013 Br J Clin Pharmacol; Kubitza D 2007 J Clin Pharmacol; clipartbest.com; van Es Blood. 2014; Martin K etal. J Thromb Haemost 2016; 14: 1308–13.; Burnett etal. J Thromb Thrombolysis (2016) 41:206–232

Extremes of weight
Candidates for a DOAC therapy: Special populations
dailykos.com

Elderly
Candidates for a DOAC therapy: Special populations
• Evidence from a meta-analysis of the Phase 3 trials studying VTE
• Pooled DOAC vs. VKA for age ≥ 75 years for recurrent VTE or VTE-related death: HR 0.56 (95% CI 0.38-0.82) p=0.003
• Pooled DOAC vs. VKA for age ≥ 75 years for Major bleeding: HR 0.49 (95% CI 0.25-0.96) p=0.04
van Es N. Blood. 2014; pintrest.com

Elderly
Candidates for a DOAC therapy: Special populations
van Es N. Blood. 2014; pintrest.com

Thrombophilias
Candidates for a DOAC therapy: Special populations
• Evidence is limited • Patients with thrombophilias comprised 2-18% of those
enrolled in DOAC trials
• Post-hoc dabigatran data shows no difference in recurrent VTE
• Exception: APS--3 ongoing studies • RAPS (Canada), TRAPS (Italy), ASTRO-APS (USA)
Schulman S (2013) N Engl J Med 368:709–718. EINSTEIN Investigators (2010) N Engl J Med 363:2499–2510. Agnelli G (2013) N Engl J Med 368:699–708. Schulman S (2009) N Engl J Med 361:2342–2352. Schulman S (2014) Circulation 129:764–772 EINSTEIN–PE Investigators (2012). N Engl J Med 366:1287–1297. Agnelli G (2013) N Engl J Med 369:799–808. Hokusai-VTE Investigators (2013) N Engl J Med 369:1406–1415; Schulman S et al (2014) ASH 56th annual meeting Dec 2014, session 332 abstract 1544

Thrombophilias
Candidates for a DOAC therapy: Special populations
dailykos.com

Thrombophilias
Candidates for a DOAC therapy: Special populations
APS =
dailykos.com

Cancer
Candidates for a DOAC therapy: Special populations
• No dedicated RCT evidence for cancer patients exists • Systematic reviews of the cancer subgroup from the clinical
trials suggest DOACs are similar to VKA for VTE recurrence risk reduction and no difference in MB/CRNMB
• 1 meta-analysis suggested for VTE recurrence RR 0.57 (95% CI
0.36-0.91; p=0.02)
Schulman S 2013 NEJM EINSTEIN Investigators 2010 NEJM ; Agnelli G 2013 NEJM; Schulman S 2009 NEJM; Schulman S 2014 Circulation; EINSTEIN–PE Investigators 2012 NEJM; Agnelli G 2013 NEJM; Hokusai-VTE Investigators 2013 NEJM; Castellucci LA. 2014 JAMA; Carrier M. 2014 Thromb Res; Vedovati MC. 2015 Chest; Di Minno MN. 2014 J Thromb Haemost; Franchini M.2015 Thromb Res

Cancer
Candidates for a DOAC therapy: Special populations
Schulman S 2013 NEJM EINSTEIN Investigators 2010 NEJM ; Agnelli G 2013 NEJM; Schulman S 2009 NEJM; Schulman S 2014 Circulation; EINSTEIN–PE Investigators 2012 NEJM; Agnelli G 2013 NEJM; Hokusai-VTE Investigators 2013 NEJM; Castellucci LA. 2014 JAMA; Carrier M. 2014 Thromb Res; Vedovati MC. 2015 Chest; Di Minno MN. 2014 J Thromb Haemost; Franchini M.2015 Thromb Res; va Es 2015; Kearon C AT10 2016

• AT10 states that “For VTE and cancer, we suggest LMWH over VKA
(Grade 2B), dabigatran (Grade 2C), rivaroxaban (Grade 2C), apixaban (Grade 2C), or edoxaban (Grade 2C).”
• No comparison of DOAC with LMWH to date • 5 ongoing trials (rivaroxaban=2, apixaban=2, edoxaban=1)
clinicaltrials.gov accessed 12 MAR 2016
Cancer
Candidates for a DOAC therapy: Special populations
Kearon C AT10 2016

Cancer
Candidates for a DOAC therapy: Special populations
dailykos.com

Choosing between DOACs: Summary
Warfarin Dabigatran Rivaroxaban Apixaban Edoxaban
Cost +++ + + + + Compliance +++ + ++ + ++ Bleeding risk
+ ++ ++ +++ +++ Renal Dysfunction
+++ + + ++ + QOL + ++ +++ ++ +++ +: Less favorable +++: More favorable

Treatment updates for Venous Thromboembolism
Kearon C. CHEST 2016; 149(2):315-352

Evaluation of Individuals with Pulmonary Nodules: General Approach
Of the 53 recommendations in this update, 20 (38%) are strong recommendations (Grade 1) and none are based on high quality (Grade A) evidence. AT LGM represents the first endeavor to transition to a continually updated “Living Guideline” with a format designed to facilitate updates as new evidence becomes available.
AT living guideline model

Evaluation of Individuals with Pulmonary Nodules: General Approach
AT10 Guideline Statement:
AT10 Choice of anticoagulant for long-term treatment of DVT and PE: DOAC vs. warfarin
In patients with DVT of the leg or PE and no cancer, as long-term (first 3 months) anticoagulant therapy, we suggest apixaban or edoxaban or rivaroxaban or dabigatran over VKA therapy (Grade 2B). Remarks: Acute therapy with parenteral anticoagulation is given before dabigatran and edoxaban.
Kearon C. Chest. 2016. doi:10.1016/j.chest.2015.11.026
For the first time an alternative to usual care with low molecular weight heparin and warfarin has been suggested for the long-term treatment of PE and DVT.

Evaluation of Individuals with Pulmonary Nodules: General Approach
Recommended therapy for VTE takes into consideration efficacy, safety, and burden of treatment (can also include cost). Is there evidence to recommend 1 DOAC over another? DOACs have not been compared head-to-head for patient-important outcomes. Based on indirect comparisons these outcomes appear to be similar with all of the NOACs Individual patient characteristics (including cost and insurance coverage) will likely drive choice of anticoagulant for the initial 3 months of therapy
AT10 Choice of anticoagulant for long-term treatment of DVT and PE: DOAC vs. warfarin

AT10 Guideline Statement:
In patients with subsegmental PE (no involvement of more proximal pulmonary arteries), no proximal DVT in the legs, and a low risk for recurrent VTE (see text), we suggest clinical surveillance over anticoagulation (Grade 2C).
Whether to Anticoagulate Subsegmental Pulmonary Embolism NEW TOPIC!
Kearon C. CHEST 2016; 149(2):315-352

Evaluation of Individuals with Pulmonary Nodules: General Approach Definition: Subsegmental PE (SSPE) refers to PE that is confined to the subsegmental pulmonary arteries (and may occur bilaterally). SSPE has become important because improvements in computerized tomography pulmonary angiography (CTPA) have increased how often subsegmental PE is diagnosed. Now SSPE constitutes about 10% of all PE cases.
Whether to Anticoagulate Subsegmental Pulmonary Embolism NEW TOPIC!

Evaluation of Individuals with Pulmonary Nodules: General Approach
No RCTs exist to direct treatment of SSPE however high quality evidence supports anticoagulation for treatment of larger PE Whether the risk of progressive or recurrent VTE is high enough to justify anticoagulation in patients with SSPE is uncertain
Whether to Anticoagulate Subsegmental Pulmonary Embolism NEW TOPIC!

Evaluation of Individuals with Pulmonary Nodules: General Approach
What considerations are important upon weighing SSPE treatment options?
1. Consider certainty of true thrombosis being present (evaluate
likelihood of observed thrombosis being a false positive result) SSPE is more likely a true-positive if…
CTPA characteristics (quality, multiple defects, multiple projections, etc.)
Patients are symptomatic (as opposed to PE being an incidental finding)
There is a high clinical pre-test probability for PE
Elevated D-Dimer that’s otherwise unexplained
Whether to Anticoagulate Subsegmental Pulmonary Embolism NEW TOPIC!

Evaluation of Individuals with Pulmonary Nodules: General Approach
What considerations are important upon weighing SSPE treatment options?
2. Assess the patient for risk factors for progressive thrombosis and risk of anticoagulation.
Favors Anticoagulation Favors No Anticoagulation Active cancer (particularly if metastatic or on chemotherapy)
High bleeding risk
No reversible VTE risks (e.g. recent surgery) Patient prefers to avoid anticoagulation
Marked symptoms without another cause Patient prefers anticoagulation Hospitalized or immobilized
Whether to Anticoagulate Subsegmental Pulmonary Embolism NEW TOPIC!

What additional testing and follow-up is recommended if the decision is to not anticoagulate SSPE?
Additional testing recommended Additional follow-up
Bilateral US to exclude proximal DVT of the legs
Assure patient literacy surrounding signs and symptoms of progressive thrombosis
Exclude DVT in other high risk locations (e.g. upper extremities if a central line is present)
Perform one or more follow-up US of the legs to detect (and then treat) evolving proximal DVT
Whether to Anticoagulate Subsegmental Pulmonary Embolism NEW TOPIC!

SUMMARY With a weak recommendation based on low quality evidence (Grade 2C), clinical surveillance is suggested over anticoagulation in patients with isolated subsegmental PE If clinical surveillance is chosen, it should be assured that no proximal DVT in the legs exists, and that the patient is at a low risk for recurrent VTE Upon clinical surveillance perform serial ultrasound of the legs to detect evolving DVT (e.g. repeating ultrasound weekly x 2 weeks)
Whether to Anticoagulate Subsegmental Pulmonary Embolism NEW TOPIC!

Management of Recurrent Venous Thromboembolism on Anticoagulant Therapy New TOPIC!
In patients who have recurrent VTE on VKA therapy (in the therapeutic range) or on dabigatran, rivaroxaban, apixaban or edoxaban (and are believed to be compliant), we suggest switching to treatment with LMWH at least temporarily (Grade 2C).
AT10 Guideline Statement:
Kearon C. CHEST 2016; 149(2):315-352

Risk factors for recurrent VTE while on anticoagulant therapy can be divided into two broad categories:
(1) Treatment factors (2) Patient intrinsic risk of recurrence
Management of Recurrent Venous Thromboembolism on Anticoagulant Therapy New TOPIC!

TREATMENT FACTORS Important initial considerations when assessing for
recurrent VTE on anticoagulant therapy (1) Was the patient adherent (2) Was warfarin sub-therapeutic (3) Was anticoagulant therapy prescribed correctly (4) Was the patient taking a NOAC and a drug that reduced anticoagulant effect (5) Had anticoagulant dose been reduced (drugs other than warfarin)
Management of Recurrent Venous Thromboembolism on Anticoagulant Therapy New TOPIC!

INTRINSIC PATIENT RISK FACTORS FOR RECURRENCE Important considerations when assessing for
recurrent VTE on anticoagulant therapy (1) Active cancer (occult disease should always be considered)
(2) Antiphospholipid Syndrome
i. Associated with recurrence ii. LA can interfere with the INR (spurious results)
(3) Concomitant use of medications that increase risk of thrombosis
Management of Recurrent Venous Thromboembolism on Anticoagulant Therapy New TOPIC!

SUMMARY If a patient is on warfarin, then it is recommended to switch to treatment-dose LMWH If a patient is on LMWH, then it is recommended to increase the dose by about 25% If anticoagulant intensity cannot be increased because of risk of bleeding, an IVC can be inserted to prevent PE This is a least favorable option of last resort
Management of Recurrent Venous Thromboembolism on Anticoagulant Therapy New TOPIC!

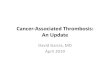
Aspirin for extended treatment VTE?

Aspirin for the secondary prevention of VTE
In patients with an unprovoked proximal DVT or PE who are stopping anticoagulant therapy and do not have a contraindication to aspirin, we suggest aspirin over no aspirin to prevent recurrent VTE (Grade 2B)
AT10 Guideline Statement:
Kearon C. CHEST 2016; 149(2):315-352

Quality Evidence (GRADE)
Hazard Ratio
Difference Per 1,000
VTE
Major Bleeding
Mortality
Studies: 2 Participants: 1,224
Aspirin for the secondary prevention of VTE

• Anticoagulants reduce VTE >90% • DOACS suggested if unprovoked & low risk bleeding • Bleeding may be similar with ASA & DOACs
SUMMARY
Unprovoked proximal DVT or PE and stop AC & no contraindication then aspirin over no aspirin (Grade 2B)
Aspirin for the secondary prevention of VTE

Bridge therapy
www.bridge1980.com; www.istockphoto.com; en.wikipedia.org

Anderson M Clev. Clin J Med, 2014, 8; 629;
About 2.5M Americans require long-term anticoagulation
About 10% require interruption annually

Warfarin interruption for procedures “Bridging”
Bridge Trial: Atrial Fibrillation • RDBPCT 1884 pts. with AF Dalteparin or Placebo
– From 3 days before until AM before the procedure and then for 5-10 days after
– Demographics: mean age 72; 97.2% with CHADS ≤ 4 – Time to first post-procedure dose: 53h (H) 21h (L) – Mean # Post-Procedure doses: 16
Douketis JD etal. NEJM online 22 June 2014

Warfarin interruption for procedures “Bridging” Bridge Trial
• Results – The incidence of arterial TE 0.4% in the no-bridging
group and 0.3% in the bridging group (95% CI −0.6-0.8; P = 0.01 for noninferiority).
– The incidence of major bleeding was 1.3% in the no-bridging group and 3.2% in the bridging group RR 0.41 (95% CI 0.20-0.78; p= 0.005 for superiority).
• Conclusion: Forgoing bridging in AF patients was noninferior to bridging for stroke and decreased the risk of major bleeding.
Douketis JD etal. NEJM online 22 June 2014

Warfarin interruption for procedures “Bridging”
Warehouse Study: VTE • Retrospective cohort study at Kaiser Colorado • 1187 pts. on indefinite anticoagulation for VTE
– Demographics: • mean age 66; 46% M • 56% DVT 44% PE • 79% “low risk for recurrence” at time of interruption • 98.7% with VTE ≥ 3 mo. prior • Procedures: GI Endo (37%) ortho (14%) spine (10%) abd sx (9%)
• Outcome: 30-d clinically relevant bleeding, recurrent VTE, and all-cause mortality.
Clark NP etal. JAMA Intern Med. Online May 26, 2015.

Warfarin interruption for procedures “Bridging”
Warehouse Study • Results
– There was no significant difference in the rate of recurrent VTE between groups (0 vs 3; P = .56).
– 30d bleeding in the bridge therapy and non–bridge groups occurred in 15 patients (2.7%) and 2 patients (0.2%), respectively (hazard ratio, 17.2; 95%CI 3.9-75.1).
• Conclusion: Bridge therapy was associated with an
increased risk of bleeding during warfarin interruption among VTE patients and is likely unnecessary for most.
Clark NP etal. JAMA Intern Med. Online May 26, 2015.





Anderson M Clev. Clin J Med, 2014, 8; 629;
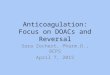
Generally, interrupt 4-5 half-lives before HBR procedure
OK to interrupt 2-3 half-lives before LBR procedure
Half-life increases as renal function worsens

Pre-procedural interruption of DOACs
Adapted from Gladstone DJ Ann Intern Med. 2015;163:382-385.

Douketis J. Current Pharmaceutical Design, 2010, 16, 3436-3441

Why use warfarin decision-support?

Anticoagulation management: iCentra
Why Clinical Decision Support in iCentra? AT 9 Guideline “For dosing decisions during maintenance VKA therapy, we suggest using validated decision support (e.g. computerized programs) rather than no decision support.” Anticoagulation Forum “When determining warfarin doses during VTE treatment we suggest using computer-aided warfarin dosing programs over an ad hoc approach.”
Holbrook CHEST 2012; 141(2)(Suppl):e152S–e184S; Witt D etal. J Thromb Thrombolysis (2016) 41:187–205

CDS outcomes within Intermountain

Time that the patient is taking warfarin
Pre-Post warfarin management with CAC CDS
Patient enrolled in
CAC
INRs before CDS
INRs after CDS
n=2591
Woller, SC et al. Clin Appl Thromb Hemost. 2015 Apr;21(3):197-20

Results
TTR=64% TTR=65.1%
Woller, SC et al. Clin Appl Thromb Hemost. 2015 Apr;21(3):197-20

Results: Secondary Outcomes
Major Complications
Percent Δ
p-value BEFORE CDS AFTER CDS
Events, n Events/
100 Pt. yrs. Events, n
Events/ 100 Pt. yrs.
PE 59 0.85 23 0.27 -68% <0.0001
VTE with hospitalization
96 1.38 47 0.56 -59% <0.0001
Stroke 2 0.02 1 0.01 NA 0.7365
Major Bleed 77 0.91 94 1.30 +30% 0.0106
ED visit 3831 55 2876 34 -38% <0.0001
Hospitalization 2943 42 2221 26 -44% <0.0001
Woller, SC et al. Clin Appl Thromb Hemost. 2015 Apr;21(3):197-20

Comprehensive Anticoagulation CDS in iCentra
• Initiation protocol
• Chronic protocol
• Bridging protocol
• DOAC Management*
*Coming soon….

Anticoagulation CDS in iCentra: workflow

Routine warfarin management in iCentra
Workflow for chronic anticoagulation management

Anticoagulation CDS in iCentra: workflow

Anticoagulation CDS in iCentra: workflow
Clinician summary report

Anticoagulation CDS in iCentra: workflow

Anticoagulation CDS in iCentra: workflow

Anticoagulation CDS in iCentra: workflow
Patient Summary Report

Summary • DOAC limitations & use in routine clinical care
– Special populations
• AT10 Updates: Venous Thromboembolism • Anticoagulation procedural interruption
(“bridging”) – Warfarin – DOACs
• Why & how to manage anticoagulation in iCentra

QUESTIONS?