-
7/30/2019 Hypertensive Retinopathy - Yanoff and Duker
1/13
Yanoff & Duker: Ophthalmology, 3rd ed.
Copyright 2008 Mosby, An Imprint of Elsevier
section5 VASCULAR DISORDERS
Chapter 6.15 Hypertensive Retinopathy
Adam H. Rogers
CHRONIC HYPERTENSIVE RETINOPATHY
MALIGNANT ACUTE HYPERTENSIVE RETINOPATHY
Definition: Retinal vascular changes occurring from chronically
elevated systemic arterialhypertension.
Key features
Narrowing and irregularity of retinal arteries.
Arteriovenous nicking (narrowing of retinal veins at
arteriovenous crossing sites).
Blot retinal hemorrhages.
Microaneurysms.
Cotton-wool spots.
Associated features
Retinal venous obstruction.
Retinal neovascularization.
Retinal arterial emboli.
Definition: Retinal, choroidal, and optic nerve changes
secondary to acutely elevated
systemic arterial blood pressure.
Key features
Retinal arteriolar spasm.
Superficial retinal hemorrhages.
Cotton-wool spots.
Serous retinal detachment.
Optic disc edema.
Page 1 of 13Section 5 - VASCULAR DISORDERS from Yanoff &
Duker: Ophthalmology on M...
16/02/2011mk: MSITStore:C:\Documents%20and%20Settin
s\Administrador\Mis%20docume...
-
7/30/2019 Hypertensive Retinopathy - Yanoff and Duker
2/13
INTRODUCTION
Hypertensive retinopathy represents the ophthalmic findings of
end-organ damage secondary to
systemic arterial hypertension. Although its name implies only
retinal involvement, changes inboth the choroid and the optic nerve
are observed, depending on the chronicity and severity of
the disease. Ocular changes in malignant hypertension can be
striking, with optic neuropathy,choroidopathy, and retinopathy.
Changes from essential hypertension are subtler, affecting
primarily the retinal vasculature. Because hypertension is so
prevalent in industrialized countries,hypertensive retinopathy is a
common condition encountered by all ophthalmologists and
health-
care professionals.
EPIDEMIOLOGY AND PATHOGENESIS
Systemic arterial hypertension is one of the most common
diseases of adults in industrializedcountries. Although the medical
literature subdivides hypertension into multiple groups, only
essential (primary) and malignant hypertension are relevant to a
discussion of hypertensiveretinopathy. Essential hypertension is of
unknown cause and is diagnosed when the average
blood pressure measures greater than 140mmHg systolic or 90mmHg
diastolic on at least two
subsequent visits. In the United States alone, it is estimated
that more than 25% of all adults and
60% of persons older than 60years are affected. Blacks have a
higher prevalence ofhypertension than whites, and men are affected
more than women. [1] However, over age 50,women have a higher
prevalence than men. [2] Elevated blood pressure is rare in
agrarian
societies and in individuals who are physically active. [1]
Because high blood pressure is an asymptomatic disease, most
patients remain undiagnosed or
inadequately treated despite the relative ease of detection. In
the National Health and NutritionStudy (NHANES III) that evaluated
hypertensive adults aged 18-74years, 68.4% were aware of
their hypertension, 53.6% were receiving treatment, and only
27.4% had their hypertension under
control. [3] Untreated or inadequately treated hypertension
carries significant cardiovascular
mortality. In patients with borderline hypertension, the
relative risk of cardiovascular disease and
end-stage renal disease is nearly double compared with patients
with optimal blood pressure. [4]
The incidence of hypertensive retinal changes is variable and is
often confounded by thepresence of other retinal vascular disease,
such as diabetes. In the Beaver Dam Eye Study, [5]
which evaluated hypertensive patients without coexisting,
confounding vascular diseases, the
overall incidence of hypertensive retinopathy was about 15%;
specifically, 8% showedretinopathy, 13% showed arteriolar
narrowing, and 2% showed arteriovenous nicking. The
predictive value of diagnosing systemic hypertension from
ophthalmic findings on examinationwas only 4753%, demonstrating
that measurement of blood pressure is a more accurate means
of diagnosis. The highest frequency of hypertensive retinopathy
in the study population was
identified in subjects with poor blood pressure control
Malignant hypertension is a rare syndrome consisting of rapid
and severe elevation of blood
pressure, with the systolic component above 200mmHg or the
diastolic blood pressure greaterthan 140mmHg. Although the absolute
blood pressure measurement is important, the presence
of systemic findings defines malignant hypertension. These
include ocular, cardiac, renal, andcerebral injury. Persistently
elevated malignant hypertension can lead to a rapidly fatal
course,
Associated features
Choroidal ischemia.
Retinal pigment epithelial changes.
Optic neuropathy.
Cortical blindness.
Proteinuria, stroke, kidney failure, encephalopathy.
Page 2 of 13Section 5 - VASCULAR DISORDERS from Yanoff &
Duker: Ophthalmology on M...
16/02/2011mk: MSITStore:C:\Documents%20and%20Settin
s\Administrador\Mis%20docume...
-
7/30/2019 Hypertensive Retinopathy - Yanoff and Duker
3/13
with heart failure, myocardial infarction, stroke, or renal
failure. [1]
Nearly 1% of hypertensive patients develop malignant
hypertension, and it is rare for patients topresent initially with
this form of elevated blood pressure. Most have a pre-existing
diagnosis of
either primary or secondary hypertension. Malignant hypertension
rarely occurs in individuals
receiving treatment for hypertension. The average age at
diagnosis is 40years, with men affected
more than women. With the advent of effective antihypertensive
treatment, nearly 50% of
patients survive more than 5years. [6]
Heredity and environmental factors have been implicated in the
pathogenesis of essentialhypertension. In the elderly, an increase
in basal smooth muscle tone occurs as a result of
sympathetic overactivity with increases in the renin-angiotensin
system. Other factors include salt
sensitivity, low systemic calcium, and insulin resistance with
hyperinsulinemia. [7] Secondaryhypertension is due to an
identifiable cause, usually related to an alteration in hormone
secretion
or renal function. With correction of the underlying cause, this
form of hypertension can be cured.[6] The pathogenesis of malignant
hypertension, similar to essential hypertension, is unknown.
Research has focused on overactivity of the
renin-angiotensin-aldosterone system, with high
plasma renin-angiotensin levels as the cause. [7]
OCULAR MANIFESTATIONS
Chronic Hypertensive Retinopathy
Patients with hypertensive retinopathy are usually asymptomatic.
Common clinical findings
include focal constriction and dilatation of the retinal
arterioles, tortuosity of the retinal arterioles,
an increase in the arteriolar light reflex, and loss of
transparency of the intra-arterial blood column( Fig. 6-15-1 ).
Arteriovenous nicking is a highly specific finding and the hallmark
of chronic
hypertensive retinopathy. At the arteriovenous crossings in the
retina, the vessels share acommon adventitial sheath. Arteriovenous
nicking is diagnosed when the crossing retinal vein
becomes less apparent or even disappears on either side of the
artery ( Fig. 6-15-2 ). The course
of the vein may change to a more perpendicular direction as
well. If there is impedance to flow,
the segment of the vein distal to the constriction appears
larger, darker, and more tortuous.Additional signs of impedance to
flow are retinal hemorrhages, macular edema, and cotton-woolspots (
Fig. 6-15-3 ). In areas of frank obstruction, the presence of
venous-venous collaterals
may be long standing. Secondary ocular complications of chronic
systemic arterial hypertensioninclude retinal vascular occlusive
disease, macroaneurysm formation, and nonarteritic anterior
ischemic optic neuropathy. [8] For the differential diagnosis,
see Box 6-15-1 .
Page 3 of 13Section 5 - VASCULAR DISORDERS from Yanoff &
Duker: Ophthalmology on M...
16/02/2011mk: MSITStore:C:\Documents%20and%20Settin
s\Administrador\Mis%20docume...
-
7/30/2019 Hypertensive Retinopathy - Yanoff and Duker
4/13
Fig. 6-15-1 Mild to moderate chronic hypertensive retinopathy.
Note the color change in the retinal arterioles and the
early arteriovenous crossing changes.
Fig. 6-15-2 In this 15 view, note the arteriovenous crossing
changes, presence of collateral vessels, and dilated
capillary bed.
Page 4 of 13Section 5 - VASCULAR DISORDERS from Yanoff &
Duker: Ophthalmology on M...
16/02/2011mk: MSITStore:C:\Documents%20and%20Settin
s\Administrador\Mis%20docume...
-
7/30/2019 Hypertensive Retinopathy - Yanoff and Duker
5/13
BOX 6-15-1
The appearance of the ocular fundus in hypertension is related
directly to the status of the retinalarteries and the rate of rise
and degree of systemic blood pressure. The age of the patient
maycomplicate interpretation of the clinical fundus changes.
Although arteriolar sclerosis is a finding
of long-standing hypertension, these changes, categorized as
involutional sclerosis, also occur in
the normal aging population. [9] With atherosclerosis alone,
mild thickening of the arteriolar wall
occurs. Clinically, focal narrowing and straightening of the
retinal arterioles are seen in the
absence of arteriovenous crossing changes. [10] Because the
chronic effects of elevated systemicblood pressure occur along with
arteriosclerotic thickening of the blood vessel walls, it can
be
difficult to categorize fundus changes solely on the basis of
elevated blood pressure.
Malignant Hypertensive Retinopathy
Visual disturbances are common in malignant hypertension.
Symptoms include headache,scotoma, diplopia, dimness in vision, and
photopsia. [11] Ocular findings in malignant arterial
hypertension are divided into three distinct categories:
hypertensive retinopathy, hypertensivechoroidopathy, and
hypertensive optic neuropathy. The causes of these clinical
findings includes
Fig. 6-15-3 A 60 view of the same patient as shown in Fig.
6-15-2 . Note the telangiectatic vessels on the optic nerve
head and intraretinal hemorrhages temporal to the macula.
Differential Diagnosis of Chronic Hypertensive Retinopathy
Diabetic retinopathy
Retinal venous obstruction
Hyperviscosity syndromes
Congenital hereditary retinal arterial tortuosity
Ocular ischemic syndrome
Radiation retinopathy
Page 5 of 13Section 5 - VASCULAR DISORDERS from Yanoff &
Duker: Ophthalmology on M...
16/02/2011mk: MSITStore:C:\Documents%20and%20Settin
s\Administrador\Mis%20docume...
-
7/30/2019 Hypertensive Retinopathy - Yanoff and Duker
6/13
constriction of vascular beds from circulating catecholamines,
obstruction of arterioles, and
breakdown in the blood-retina barrier. Ophthalmic findings in
acute malignant hypertensive
retinopathy include focal arteriolar narrowing, cotton-wool
spots, intraretinal transudates, macular
edema, and retinal hemorrhages. Retinal hemorrhages are linear,
occurring in the nerve fiber
layer in the peripapillary region. Cystoid macular edema, lipid
deposits, and arteriolar changesare signs of more chronic malignant
hypertensive retinopathy. [12]
Arteriolar narrowing observed on ophthalmoscopy has been
challenged by Hayreh, who refers tothis clinical finding as
pseudonarrowing secondary to retinal edema creating a visual effect
of
narrowing of the retinal arteriole. Fluorescein angiography
performed in rhesus monkeys withacute malignant hypertension has
demonstrated normal retinal arteriolar caliber, casting doubt
on
the long-standing belief that arteriolar spasm occurs. [13]
Cotton-wool spots are fluffy, elevated,
tanwhite areas of retinal opacity occurring within a few disc
diameters of the optic nerve, causedby occlusion of terminal
retinal arterioles. Capillary nonperfusion is present on
angiography ( Fig.
6-15-4 ). Cotton-wool spots typically resolve in 36weeks and are
associated with permanentnerve fiber layer loss in the vicinity of
the lesion. [12] Periarteriolar intraretinal transudates are
tan
white retinal lesions occurring in the vicinity of an arteriole.
The lesions measure about onequarter of the disc area but are
clinically larger, as they coalesce with adjacent lesions.
Intraretinal transudates occur secondary to focal areas of
arteriolar leakage identified on
angiography and resolve without residual retinal damage in
23weeks. [14] Macular edema andsubretinal fluid are retinal
findings related to hypertensive choroidal changes affecting the
retinal
pigment epithelium (RPE), with alterations in the blood-retina
barrier.
Page 6 of 13Section 5 - VASCULAR DISORDERS from Yanoff &
Duker: Ophthalmology on M...
16/02/2011mk: MSITStore:C:\Documents%20and%20Settin
s\Administrador\Mis%20docume...
-
7/30/2019 Hypertensive Retinopathy - Yanoff and Duker
7/13
Clinical changes from hypertensive choroidopathy are directly
related to the release ofendogenous vasoconstrictor agents (e.g.,
angiotensin II, epinephrine, vasopressin) duringsystemic
hypertension. Angiographically, there is delayed, patchy choroidal
filling. [12] Gitter et al.
[15] demonstrated through the use of fluorescein angiography
that the delay in choroidal filling isfollowed by late leakage from
choroidal vessels into the subretinal space. The leakage is
enhanced by infarction and damage to the RPE cells or
transudation of fluid into the subretinal
space in response to increased pressure in the choroidal
vessels. [16] [17] Focal occlusion of the
choriocapillaris leads to necrosis and atrophy of the RPE,
forming Elschnigs spots ( Fig. 6-15-
5 ). [18] [ 19] Acutely, Elschnigs spots are punctate, tanwhite
lesions that leak on fluorescein andindocyanine green angiography
from breakdown in the bloodretina barrier. Subretinal fluid
accumulates, with the eventual formation of macular edema, a
common finding associated withhypertensive choroidopathy [14] (
Fig. 6-15-6 ). With time, the focal RPE lesions become
confluent
and more extensive. Diffuse pigmentary changes with atrophy give
a mottled appearance onophthalmoscopy. Linear configurations of
pigmentation along choroidal arteries are known asSiegrists
streaks. [19]
Fig. 6-15-4 The right eye of the same patient as shown in Figs.
6-15-2 and Fig. 6-15-3 . (A) A prominent cotton-wool spot
in the papillomacular bundle is seen, with an adjacent
intraretinal hemorrhage. (B) Fluorescein angiography shows
capillary
nonperfusion in the area corresponding to the cotton-wool patch;
note the hypofluorescence of the intraretinal hemorrhage,
caused by blockage.
Fig. 6-15-5 Elschnigs spots.
Page 7 of 13Section 5 - VASCULAR DISORDERS from Yanoff &
Duker: Ophthalmology on M...
16/02/2011mk: MSITStore:C:\Documents%20and%20Settin
s\Administrador\Mis%20docume...
-
7/30/2019 Hypertensive Retinopathy - Yanoff and Duker
8/13
Hypertensive optic neuropathy presents clinically as disc edema
( Fig. 6-15-7 ). This occurs from
vasoconstriction of the posterior ciliary arteries supplying the
optic nerve head, resulting from the
release of angiotensin II and other vasoconstricting agents.
Ischemia occurs in the optic nerve,leading to stasis of axoplasmic
flow, which is a form of anterior ischemic optic neuropathy. [20]
Forthe differential diagnosis, see Box 6-15-2 .
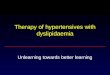
Fig. 6-15-6 Serous detachment of the retina in a 27- ear-old
patient who has pregnancy-induced hypertension, 3
days post partum. Blood pressure measured 158/100 mmHg. Note the
subretinal fibrin and folds in the retina. (Courtesy of
Franklin L. Myers.)
Page 8 of 13Section 5 - VASCULAR DISORDERS from Yanoff &
Duker: Ophthalmology on M...
16/02/2011mk: MSITStore:C:\Documents%20and%20Settin
s\Administrador\Mis%20docume...
-
7/30/2019 Hypertensive Retinopathy - Yanoff and Duker
9/13
-
7/30/2019 Hypertensive Retinopathy - Yanoff and Duker
10/13
described earlier are more common in malignant hypertension.
Measurement of systemic blood
pressure is necessary to rule out other causes with similar
clinical pictures.
Several classification schemes have been used to stage
hypertensive retinal changes. The two
most widely accepted are the Keith-Wagener-Barker classification
and the Scheie classification.
The Keith-Wagener-Barker scheme ( Table 6-15-1 ) combines the
clinical findings of
hypertension and atherosclerosis. [21] The Scheie classification
( Table 6-15-2 ) keeps the two
disease processes separate. [22] Unfortunately, no
classification is satisfactory because of thehigh variability of
clinical findings. [23] They are of historical value only and are
not used clinically;
accurate description of the ocular findings is more valuable
than any classification system.
Table 6-15-1 -- KEITH-WAGENER-BARKER CLASSIFICATION
Group 1 Mild-to-moderate narrowing or sclerosis of the
arterioles
Group 2 Moderate to marked narrowing of the arterioles
Local and/or generalized narrowing of arterioles
Exaggeration of the light reflex Arteriovenous crossing
changes
Group 3 Retinal arteriolar narrowing and focal constriction
Retinal edema Cotton-wool patches
Hemorrhage
Group 4 As for Group 3, plus papilledema
(Adapted from Walsh JB. Hypertensive retinopathy. Description,
classification and prognosis.Ophthalmology. 1981;89:112731.)
Table 6-15-2 -- SCHEIE CLASSIFICATION
Although newer imaging techniques, such as scanning laser
ophthalmoscopy, allow
quantification of retinal capillary density and flow velocity in
patients who have essentialhypertension, these results are still
preliminary in terms of their application to the long-term
prevention of retinal disease. [21] Optical coherence tomography
may be used to evaluate cross-
sectional images of the retina and subretinal fluid collections.
[24]
SYSTEMIC ASSOCIATIONS
HYPERTENSION
Grade 0 No changes
Grade 1 Barely detectable arteriolar narrowing
Grade 2 Obvious arteriolar narrowing with focal
irregularities
Grade 3 Grade 2 plus retinal hemorrhages and/or exudates
Grade 4 Grade 3 plus papilledema
ARTERIOLAR SCLEROSIS
Grade 0 NormalGrade 1 Barely detectable light reflex changes
Grade 2 Obvious increased light reflex changes
Grade 3 Copper-wire arterioles
Grade 4 Silver-wire arterioles
Page 10 of 13Section 5 - VASCULAR DISORDERS from Yanoff &
Duker: Ophthalmology on ...
16/02/2011mk: MSITStore:C:\Documents%20and%20Settin
s\Administrador\Mis%20docume...
-
7/30/2019 Hypertensive Retinopathy - Yanoff and Duker
11/13
Essential hypertension is the most common cause of chronically
elevated blood pressure and is
typically of unknown cause. Screening for secondary systemic
causes is not pursued unlessother symptoms are present or the
hypertension is resistant to treatment. The causes of
secondary hypertension include pheochromocytoma, renovascular
stenosis, and primary
hyperaldosteronism. [1] [7]
In nearly all cases of malignant hypertension, a systemic cause
can be elucidated via systemicevaluation. Potential causes include
renal disease, such as polycystic kidney or renovascular
stenosis; pheochromocytoma; and pregnancy. Rarely, untreated
essential hypertension may leadto an acute hypertensive crisis.
Systemic abnormalities accompany accelerated hypertension
with evidence of end-organ damage, including acute left
ventricular heart failure, myocardial
infarction, pulmonary edema, dissecting aortic aneurysm, stroke,
encephalopathy, andintracranial hemorrhage. [1] [7]
PATHOLOGY
Microscopically, early changes from hypertension demonstrate
sclerosis and thickening of thearteriolar walls with luminal
narrowing. These findings become more prominent with long-
standing systemic hypertension. Arteriole thickening in the
choroidal vessels is typically moresevere than in the retinal
arterioles and more closely resembles systemic arterial changes.
[19] In
malignant hypertension, the arterioles are similarly thickened,
but necrosis and fibrinoid
deposition in the vessel wall occur. Electron micrographs of
retinal arterioles in malignanthypertension eventually demonstrate
dilatation of the lumen, with focal breaks in the endothelium
surrounded by lipid and fibrin, as the autoregulatory mechanisms
of the arterioles areexceeded. [14] [ 19] Other pathological
findings include optic nerve edema, cotton-wool spots,
microaneurysms, and focal infarcts. [19]
TREATMENT, COURSE, AND OUTCOME
By itself, chronic hypertensive retinopathy rarely, if ever,
results in significant loss of vision.Treatment of the underlying
systemic condition can halt the progress of the retinal changes,
but
arteriolar narrowing and arteriovenous nicking usually are
permanent.
Treatment of malignant hypertensive retinopathy, choroidopathy,
and optic neuropathy consists
of lowering blood pressure in a controlled fashion to a level
that minimizes end-organ damage.The actual level of blood pressure
is less important in gauging the urgency of the situation than
is
the ongoing end-organ damage. In hypertensive patients, the
autoregulatory mechanism thatmaintains constant blood flow to
tissues is elevated to a higher level. This allows for the
tolerance
of higher blood pressures, and lowering blood pressure below the
regulatory range can prevent
adequate blood flow from reaching vital organs. [12] Therefore,
blood pressure should be loweredin a slow, deliberate, controlled
fashion to prevent end-organ damage. Too rapid a decline can
lead to ischemia of the optic nerve head, brain, and other vital
organs, resulting in permanentdamage. Medications used to treat
hypertensive emergencies include sodium nitroprusside,
nitroglycerin, calcium channel blockers, beta blockers, and
angiotensin-converting enzymeinhibitors. Treatment should be
initiated in a controlled, monitored setting under the auspices of
a
physician skilled in the use of antihypertensive
medications.
From a systemic viewpoint, the diagnosis of a malignant
hypertensive crisis represents a medical
emergency. Untreated, the mortality rate is 50% at 2 months and
90% at 1 year. [25] [ 26] Most
patients resume normal vision. On the rare occasion when vision
loss occurs, this may resultfrom retinal pigment changes secondary
to retinal detachment or from optic atrophy due to
prolonged papilledema.
REFERENCES
1.. Oparil S.: Arterial hypertension. In: Goldman L., Bennett
J.C., ed. Cecil textbook of medicine,Philadelphia: Saunders;
2000:258-273.
2.. Joint National Committee on Prevention, Detection,
Evaluation, and Treatment of High Blood
Page 11 of 13Section 5 - VASCULAR DISORDERS from Yanoff &
Duker: Ophthalmology on ...
16/02/2011mk: MSITStore:C:\Documents%20and%20Settin
s\Administrador\Mis%20docume...
-
7/30/2019 Hypertensive Retinopathy - Yanoff and Duker
12/13
Pressure. Sixth report of the Joint National Committee on
Prevention, Detection, Evaluation, and
Treatment of High Blood Pressure (JNC VI). Arch Intern Med 1997;
157:2413.
3.. Burt V.L., Cutler J.A., Higgins M.: Trends in the
prevalence, awareness, treatment and control of
hypertension in the adult US population: data from the Health
Examination Surveys, 19601991.
Hypertension 1995; 26:60.
4.. National High Blood Pressure Education Program Working Group
: Report on primary preventionof hypertension. Arch Intern Med
1993; 153:186.
5.. Klein R., Klein B.E., Moss S.E., Wang Q.: Hypertension and
retinopathy, arteriolar narrowing, andarteriovenous nicking in a
population. Arch Ophthalmol 1994; 112:92-98.
6.. Laragh J.: Laraghs lessons in pathophysiology and clinical
pearls for treating hypertension. Am J
Hypertens 2001; 14:186-194.
7.. Williams G.H.: Hypertensive vascular disease. In: Iselbacher
K.J., et al ed. Harrisons textbook of
internal medicine, New York: McGraw-Hill; 1994:1116-1131.
8.. Panton R.W., Goldberg M.F., Farber M.D.: Retinal arterial
macroaneurysm: risk factors and natural
history. Br J Ophthalmol 1990; 74:595-660.
9.. Leishman R.: The eye in general vascular disease:
hypertension and arteriosclerosis. Br J
Ophthalmol 1957; 41:641-701.
10.. Stokoe N.L.: Fundus changes in hypertension: a long-term
clinical study. In: Cant J.S., ed. The
William Mackenzie centenary symposium on the ocular circulation
in health and disease,
London: Kimpton; 1969:117-135.
11.. Bosco J.A.: Spontaneous nontraumatic retinal detachment in
pregnancy. Am J Obstet
Gynecol 1961; 82:208-212.
12.. Hayreh S.S.: Hypertensive fundus changes. In: Guyer D.R.,
ed. Retina-vitreous-macula ,Philadelphia: Saunders;
1999:345-371.
13.. Hayreh S.S., Servais G.E., Virdi P.S.: Retinal arteriolar
changes in malignant arterial
hypertension. Ophthalmologica 1989; 198:178-196.
14.. Hayreh S.S., Servais G.E., Virdi P.S.: Fundus lesions in
malignant hypertension. IV. Focalintraretinal periarteriolar
transudates. Ophthalmology 1986; 93:60-73.
15.. Gitter K.A., Houser B.P., Sarin L.K., Justice J.: Toxemia
of pregnancy. An angiographicinterpretation of fundus changes. Arch
Ophthalmol 1968; 80:449-454.
16.. Fastenberg D.M., Fetkenhour C.L., Choromolos E., Shoch
D.E.: Choroidal vascular changes intoxemia of pregnancy. Am J
Ophthalmol 1980; 89:362-368.
17.. Kenny G.S., Cerasoli J.R.: Color fundus angiography in
toxemia of pregnancy. ArchOphthalmol 1972; 87:383-388.
18.. Schmidt D., Loffler K.U.: Elschnigs spots as a sign of
severe hypertension.
Ophthalmologica 1993; 206:24-28.
19.. Green W.R.: Systemic diseases with retinal involvement. In:
Spencer W.H., ed. Ophthalmic
pathology, an atlas and textbook, Philadelphia: Saunders;
1985:1034-1045.
20.. Hayreh S.S., Servais G.E., Virdi P.S.: Fundus lesions in
malignant hypertension V. Hypertensive
optic neuropathy. Ophthalmology 1986; 93:74-87.
21.. Wolf S., Arind O., Schulte K., et al: Quantification of
retinal capillary density and flow velocity in
Page 12 of 13Section 5 - VASCULAR DISORDERS from Yanoff &
Duker: Ophthalmology on ...
16/02/2011mk: MSITStore:C:\Documents%20and%20Settin
s\Administrador\Mis%20docume...
-
7/30/2019 Hypertensive Retinopathy - Yanoff and Duker
13/13
patients with essential hypertension. Hypertension 1994;
23:464-467.
22.. Sheie H.G.: Evaluation of ophthalmoscopic changes of
hypertension and arteriolar sclerosis.Arch Ophthalmol 1953;
49:117-138.
23.. Walsh J.B.: Hypertensive retinopathy. Description,
classification and prognosis.Ophthalmology 1982; 89:1127-1131.
24.. Puliafito C.A., Hee M.R., Lin C.P., et al: Imaging of
macular disease with optical coherence
tomography. Ophthalmology 1995; 102:217-229.
25.. Keith N.M., Wagener H.P., Barker N.W.: Some different types
of essential hypertension: their
course and prognosis. Am J Med Sci. 1939; 197:332-343.
26.. Kincaid-Smith P., McMichael J., Murphy E.A.: The clinical
course and pathology of hypertension
with papilloedema (malignant hypertension). Q J Med 1958;
27:117-153.
Copyright 2009 Elsevier Inc. All rights reserved. -
www.mdconsult.com
Page 13 of 13Section 5 - VASCULAR DISORDERS from Yanoff &
Duker: Ophthalmology on ...