Embed Size (px)
DESCRIPTION
short presentation describing the danger of vitamin D in overdose.
Citation preview

1
Vitamin D intoxication in infant:
a growing concern in Switzerland
from Case Report to Physiology to Prevention
Moullet F, Hassib C, Humbert M, Cachat F
Department of Pediatrics, Pediatric Nephrology Unit
University Hospital, Lausanne, Switzerland
4/20/2011

Case presentation
• 1er enfant d’un couple kosovare
• NNT, RCIU dysharmonieux
• Multiples signes dysmorphiques
• Bilan malformatif:- US abdominal: Rein G ectopique fusionné
- Caryotype: Trisomie partielle du chromosome 2
24/20/2011 vitamin D intoxication

Case presentation
• Follow up 1 année
- TA: normale
- US: rein G ectopique fusionné, rein D normal, pas de
dilatation pyélo-calicielle, bonne croissance
- CUM: RVU grade 1 ddc
- Scintigraphie rénale: bonne fonction
34/20/2011 vitamin D intoxication

Case presentation
Bilan fonction rénale:Plasma : Na, K, P, Mg, créatinine, urée, urate dans la
norme, Ca tot 2.94 mmol/l (N 2.15-2.70), PTH 42 ng/l (N 10-
70)
Urine: natriurie, phosphaturie, magnésurie dans la norme, pas
de protéinurie, rapport Ca/créatinine: 2.23 mol/mol (N 0,07-
1.50)
44/20/2011 vitamin D intoxication

Que faites-vous (chez un enfant asymptomatique)?
54/20/2011 vitamin D intoxication

Case presentation
• Recontrôle 2 semaines plus tard
Persistance de:
hypercalcémie (Ca tot. 2.82 mmol/l)
hypercalciurie (Ca/créatinine 2.65 mol/mol)
64/20/2011 vitamin D intoxication

Suite de la prise en charge?
74/20/2011 vitamin D intoxication

Case presentation
• 25-OH Vitamine D : 238 µg/l (N 8.4-52.3)
• 1,25 dihydroxy-vit D3 : 90 pmol/l (N 48-160)
• PTH 42 ng/l (N 10-70) il y a 2 semaines
• PO4 1.28 mmol/l (N); PAL 130 UI/l (N), Mg 0.76
mmol/l (N)
84/20/2011 vitamin D intoxication

Attitude?
Arrêt de la supplémentation en Vitamine D
94/20/2011 vitamin D intoxication

Case presentation
Contrôle 3 semaines après arrêt de la Vitamine D
• Plasma: Ca tot. 3.28 mmol/l, Ca ionisé 1.68 mmol/l
• Urine: Ca /créat: 2.66 mol/mol
104/20/2011 vitamin D intoxication

Case presentation
Hospitalisation pour prise en charge.
Bilan:
25-OH Vitamine D: 179 µg/l ( N 8,4-52.3)
1,25-Dihydroxy-Vit D3: 31 pmol/l (N 48-160)
PTH: <3 ng/l
114/20/2011 vitamin D intoxication

Case presentation
• Reprise d’anamnèse
Maman donne de l’Oleovit : 1 gtte = 400 U Vit D3 (4x plus
concentré que le Vide*), entre 4 gttes et une pipette (=
env. 25 gttes)/j
Apport de Vit D3 (Cholécalciférol) : entre 1600 U et
10’000 U/j + apports laitiers: Aptamil 3 450 U Vit D/j
124/20/2011 vitamin D intoxication

Case presentation
hospitalisation du 31.03 au 02.04 puis du 04 au
06.04
• Hydratation iv
• Régime sans Ca
• Pas apport Vit D po
Normalisation lente et progressive de la calcémie
Enfant cliniquement asymptomatique13

Definition of hypercalcemia
• Ionized calcium > 1.35 mmol/l (5.4 mg/dl) or
total calcium > 2.7 mmol/l (10.8 mg/dl)
• Repeated at least twice
• Rule out extremely high albumin, total
protein, paraprotein level (pseudo-hypercalcemia)
(increased protein-bound calcium, normal ionized calcium!)14

Symptoms of hypercalcemia
• GI: nausea, vomiting, constipation, anorexia, abdominal pain, pancreatitis
• Neurologic: pseudo-tumor cerebri, depression, confusion, fatigue, coma,
hypotonia
• Cardiovascular: hypertension, bradycardia, cardiac arrest, vascular
calcification
• Renal: polyuria, dehydration, nephrocalcinosis
Kidney stones
Symptoms related to the severity of hypercalcemia
often asymptomatic if total Ca < 3 mmol/l

From: Plum L. Vitamin D, diseases, and therapeutic opportunities. Nature Rev Drug Discovery 2010;9:948-961
Physiological
controls of calcium
and phosphate
metabolism
Which actors are
Important?

Physiological control of calcium (and
phosphorus)
Hormone Blood Bone Gut Kidney
PTH Ca, PO4 osteoclast indirect effect Ca excretion
resorbtion through PO4 excretion
calcitriol
Calcitriol Ca, PO4 no direct Ca and PO4 no direct effect
effect absorption
Calcitonin Ca, PO4 osteoclast no direct Ca excretion
resorbtion effect PO4 excretion
From: Carroll M. A practical approach to hypercalcemia. Am Fam Phys 2003;67:1959-1966

Physiopathological mechanisms
leading to (sustained) hypercalcemia
Initiation of hypercalcemia
Maintenance of hypercalcemia
4/20/2011 18vitamin D intoxication

19
1. Initiation of hypercalcemia
Calcium intoxication
Vitamin D intoxication
Granulomatous liver
disease
Vitamin D intoxication
Bone metastasis
Bone disease
Overdose of calcium
Overdose of vitamin D
Williams syndrome4/20/2011

Slow release of vitamin
D from fat tissue(days to weeks) Continuous vitamin D
Exposure(variable)
Renal failure
chronic acidosis(variable)
2. Maintenance of hypercalcemia
20

214/20/2011

In summary: the questions (you should ask
yourself) at this point (from the history point of
view):
• Does my patient take vitamin D?
• Vitamin D intoxication
• Does my patient produce vitamin D?
• Granulomatous diseases, sarcoidosis
• Does my patient take calcium?
• Calcium intoxication
• Does my patient release calcium?
• Bone diseases
22

Laboratory approach to
hypercalcemia
with a good understanding of the physiology controlling
calcium metabolism
234/20/2011 vitamin D intoxication

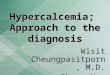
Hypercalcemia
PTH
25(OH)D 1,25(OH)D
Increased Normal/decreased
Loss of function CaSR(Severe neonatal hyperPTH, FHH)
Vitamin D
intoxication
Sarcoidosis
Granulomatosis
Fat necrosis
Hypophophatasia
Heterogenous
Williams syndrome
25(OH)D
Janssen
PTHrP
Malignancy
Vitamin A intox.

• What is the PTH level of my patient?
• What is the 25(OH)Vitamin D level of my
patient?
• Expected low PTH, high 25(OH)D and normal (/high)1,25(OH)D
levels in case of hypervitaminosis D
In summary: the questions (you should ask
yourself) at this point (from the laboratory point
of view):
25

26
Vitamin D intoxication:
How does that happen?
How can we prevent it?
4/20/2011 26vitamin D intoxication

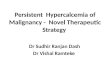
Vitamin D intoxication: how common is
it?
0
20
40
60
80
100
120
140
160
180
200
2000 2002 2004 2006 2008 2010
aigu (flacon)
aigu (posologie)
chronique
Number of cases reported to the ToxZentrum Zurich
with acute or chronic vitamin D3 intoxication
Sharp increase of
both acute and
chronic VitD3
intoxication over
the last decade
Related to the different currently
available forms of vitamin D?

Vitamin D intoxication: summary of
reported cases in the literature
Age cummulative dose duration of intoxication calcium level (mmol/l)
IU
7 w 6 millions 200’000 IU/d x 30 d 4.05
3 m 1.2 millions 3000’000 IU/d x 4 d 4.6
3 m 2.56 millions 302’000 IU/d x 8 days 4.5
6 m 3 millions 300’000 IU/d x 10 d 4.2
2 y 2.4 millions 600’000 IU/d x 4 d 3.6
11 m 1.34 millions 300’000 IU/m x 3 m 4.5
400 IU/d x 11 m
4 m 600’000 600’000 IU in 3 w 3.7
7 y 4.5 millions 300’000 IU x 15 d
7 m 1.8 millions 600’000 IU x 3 8.8
4 m 333’240 unclear 4.28
From: Chambellan-Tison C. Hypercalcemie majeure secondaire à une intoxication par la vitamine D. Arch Péd 2007;14:1328-1332

• Acute intoxication: • Relatively well described
• From 40’000 IU per day for 3 to 4 months (= 3.6 millions to 4.8
millions)
• Most of the time > 1-2 million IU cummulative dose (see French
experience) for symptoms to develop
• Chronic intoxication: • Relatively unclear
• From 2’000 to 4’000 IU per day for years29
Vitamin D intoxication: beware of the
level, beware of the duration!
29

Vitamin D intoxication: why does that
happen?
Multitude of vitamin D
available with different
dispensers and concentration 30
Double cause for
medication error

How can we prevent it?
• What has been done?• Medical Information (Forum médical suisse Journal) (2010)
• Pharmacist Information (pharmajournal) (2008 and 2010)
• Implementation of recommendations difficult• Multitude of different concentrations and dispensers available
– CONFUSION!
• Over the counter vitamins– CONFUSION!
• Effective and presumed beneficial effects of vitamin D reported in the literature
– CONFUSION!
BUT errors still occurs !
31

Real and presumed beneficial effects of
vitamin as of 2010
Vitamin D
02000400060008000
100001200014000160001800020000
1960-
1970
1970-
1980
1980-
1990
1990-
2000
2000-
2010
Vitamin D

What have we done so far?
How can we improve public safety?
4/20/2011 33vitamin D intoxication

Contexte : Depuis 2000 en Suisse, les cas de surdosages par solutions de vitamine D3 chez l’enfant sont en
constante augmentation1.
Rappels : Indications : Prévention et traitement du rachitisme.
Posologies usuelles :
Prévention rachitisme : Nouveau né : 400 UI/jour et Prématurés : 400 à 800 UI /jour jusqu’à la fin de la
1ère
année de vie.
Traitement du rachitisme : 5000 UI à 10 000 UI/jour 1 semaine, puis 5000 UI/jour 6 semaines, puis 200 à
5000 UI /jour plusieurs mois (avec suppléments calciques si nécessaire).
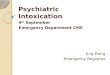
VITAMINE D3 buvables chez l’enfant :
Eviter les surdosages
Ces spécialités sont souvent présentes dans les pharmacies internationales.4
En Suisse2,3
VIDE 3 Vitamine D3 Streuli Vitamine D3 Wild
Principe Actif Cholécalciférol
(4500 UI/ml)°
1 goutte = 100 UI
Cholécalciférol
(4000 UI/ml)°
1 goutte = 100 UI
Cholécalciférol
(20 000 UI/ml)
1 goutte = 667 UI
Excipient Ethanol 65% Ethanol 49% Huile (triglycéride
chaine moyenne)
Forme galénique Flacon compte-goutte
10 ml
Flacon compte-goutte
10 ml
Flacon avec Pipette
compte-goutte 10 ml
Prix (Chf)
/Remboursé (Ass. de base)
4.60
OUI
3.85
NON
22.50
NON
Posologie usuelle en
prévention du rachitisme 4 gouttes/jour 4 gouttes/jour 1 goutte/jour
Administration Mélanger avec une
boisson/aliment.
Mélanger avec
liquide.
Mélanger au lait/
bouillie.
Présentation
Version: 1.0
Date : 07.04.2011 (MHC )
Improving implementation / error
prevention
1. Leaflet for medical doctors
and nurses and midwifes for
the prevention of vitamin D
intoxication
In close collaboration with the
Central Pharmacy of the
Hospital
2. Ward round together with a
pharmacist twice a week

• Thanks to
– Marie Humbert, PharmD, PHEL, Central PharmacyVevey, for careful literature review and leafletconception and writing
– Christian Schaeli, PharmD, PHEL, for providingexcellent service with a pharmacist for weekly wardround in the pediatric department
– All pediatricians for anouncing all cases of hypervitaminosis in their patients
4/20/2011 35vitamin D intoxication