Embed Size (px)
Citation preview

HYPERCALCEMIA
Dow University of Health SciencesDow College of PharmacyANEELA PASHA Final year Clinicals.

HYPERCALCEMIA
• Serum calcium > 10.5 mg/dl
• Mild: total CA : 10.5-11.9 mg/dl
• Moderate: total CA : 12-13.9 mg/dl
• Severe: total CA: 14-16 mg/dl
• Calcium enters extra cellular fluid from intestine and bone and excreted through kidney.
• Calcium is tightly controlled by hormones (PTH, calcitriol , calcitonin).

CALCIUM and its three forms
• Ionized (physiological form) (40%)
• Protein bound (50%), mainly to albumin
• Non ionized or Complexes to citrate and phosphate (10%)

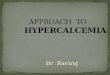
CALCIUM
ECF8.5-10.6 mg/dl
2.25-2.65 nmol/l
ICFCYTOPLASMIC FREE
50-100 nmol/l
PROTIEN BOUND
45%
DIFFUSIBLEULTRAFILTRABLE
55%
90% ALBUMIN
10% GLOBULUIN
IONIZED45%
COMPLEXED10%

FUNCTIONS
• Muscle contraction
• Neuromuscular/ nerve conduction
• Intracellular signaling
• Bone formation
• Coagulation
• Enzyme regulation

VITAMIN D

Causes of hypercalcemiaEndocrine:• Hyperparathyroidism
• MEN Type 1 (parathyroid adenoma , pituitary adenoma , pancreatic islet cell tumor)
• Familial hypocalciuric hypercalcemia
Malignancy:• Metastases
• PTHrP
• Breast caner, lung cancer , bone cancer.
Granulomatous Disease:• Sarcoidosis
• TB
Miscellaneous:• Acute kidney failure
• Milk-alkali syndrome
Medications:• Lithium therapy
• Thiazides ( inc. Na, water absorp and inc ca concentration)
• Vit D

Causes of hypercalcemia
C calcium supplements
H hyperparathyroidism
I immobilization
M MEN, milk-alkali syndrome, medication
P parathyroid hyperplasia or adenoma
A alcohol
N neoplasm (breast, lung, kidney)
Z Zollinger ellison syndrome
E excessive vit D
E excessive vit A
S Sarcoidosis

THYROTOXICOSIS
• Sever thyrotoxicosis
• Increased calcium release from bone (thyroxine acts on bone)
• PTH is normal
• Takes 4-6 weeks to resolve with antithyroid treatment

Clinical presentation
• The famous mnemonic ;• Stone• Bones• Abdominal moans• thrones• Psychic groans• Others: anorexia, n/v , weakness, renal failure cardiac
arrest , stupor or coma .• Hypocalcaemia can increase gastrin production,
leading to increased acidity so peptic ulcer may also occur.

INVESTIGATIONS
• History
• Examination
• ECG
• Blood levels.

INVESTIGATIONS
• History + PTH levels are essential for diagnosis.
• Blood tests: calcium, phosphate, magnesium, creatinine, U&E, PTH.
• CXR (bones ,lungs etc. )
• CT scan / MRI
• Mammogram
• ECG = short QT interval

MANAGEMENT
• Persistent high levels of calcium.

MANAGEMENT
• Acute management focuses on hydration the other medications
• Chronic management focuses on the underlying etiology.
• Hypercalcemia crisis = aggressive TX

MANAGEMENT
• Rehydration:
• Monitor for fluid overload if renal impairment or elderly.
• Loop diuretics rarely used and only if fluid overload develops; not effective for reducing serum calcium
• furosemide 40mg/12h PO/IV.
Intravenous 0.9% saline 4-6 litres in 24h

MANAGEMENT• After rehydration: intravenous bisphosphonates
(inhibits osteoclast. )
Or Pamidronate 30 to 90mg (depending on severity of hypocalcaemia) at 20mg/hrOr Ibandronic acid 2 to 4mg
• Give more slowly and consider dose reduction in renal impairment • Monitor serum calcium response -after at 2 to 4 days • Can cause hypocalcaemia if vitamin D deficiency or suppressed PTH• Max effects in 1W.
Zoledronic acid 4mg over 15 mins

MANAGEMENT
• Second line treatments:
• Glucocorticoids (inhibit VIT D production)
• In lymphoma, other granulomatous diseases or Vit D poisoning, sarcoidosis.
• Prednisolone 20-40mg daily
• Usually effective in 2 to 4 days

MANAGEMENT
• Calcitonin :
• Can be considered if poor response to Bisphosphonates
• Dose 4U/kg S/C or IM 12h
• Calcimimetics :
• Licensed for hypocalcaemia due to primary hyperparathyroidism, parathyroid carcinoma or renal failure.
• only cinacalcet is currently available

• DIALYSIS
• In cases life-threatening hypercalcemia, dialysis to get rid your blood of extra calcium and waste and lowering serum calcium levels.
• Only when other treatment methods not works.

MANAGEMENT
• SURGERY
• Parathyroidectomy
• Can be considered in acute presentation of primary hyperparathyroidism if severe hypercalcaemia and poor response to other measures.
• Chemotherapy in malignancy.

LIFESTYLE CHANGES
• Healthier lifestyle
• Drink plenty of water
• Exercise .

Complications (if untreated)
• Osteoporosis
• Kidney stones
• Kidney failure
• Nervous system dysfunction
• Arrhythmia
• Cardiac arrest

REFERENCE
• Society for Endocrinology, Endocrine guidance.
• Kumar and Clark medicine 2009
• Emedicine.medscape.com
• Dipiro Pharmacotherapy Handbook 8th Edition
(Pg. 988-989)