Embed Size (px)
Citation preview
Edward H. AngleExtractions for crowding were common until
late 1800sAs a prosthodontist, Edward H. Angle
developed the concept of occlusion
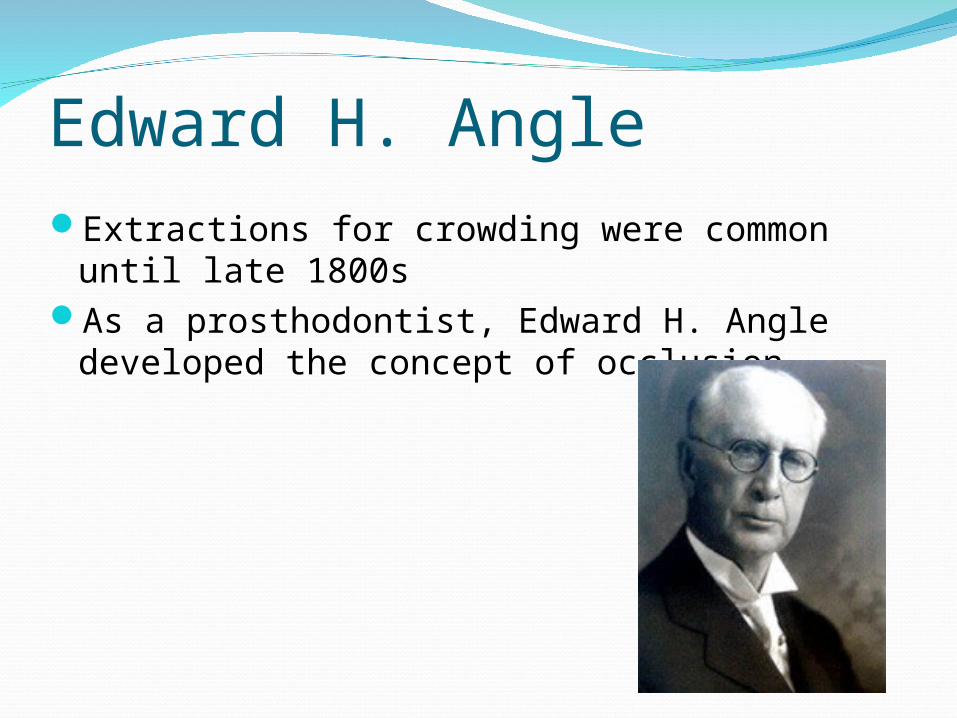
Edward H. AngleGave the first clear and simple classification of
malocclusionThe upper first molars were the key to
occlusion
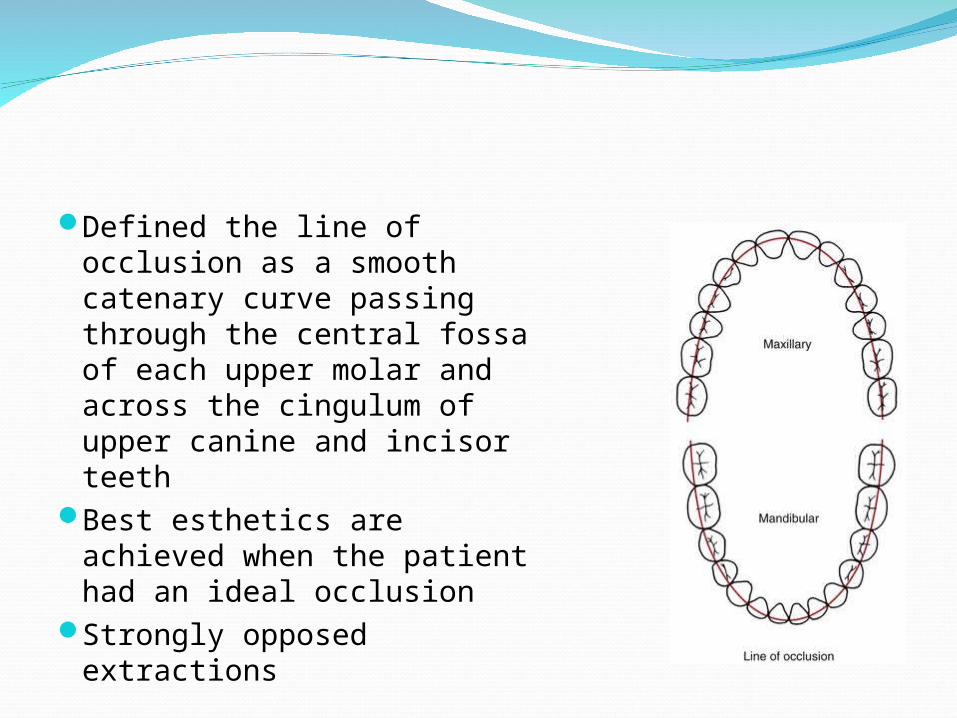
Defined the line of occlusion as a smooth catenary curve passing through the central fossa of each upper molar and across the cingulum of upper canine and incisor teeth
Best esthetics are achieved when the patient had an ideal occlusion
Strongly opposed extractions
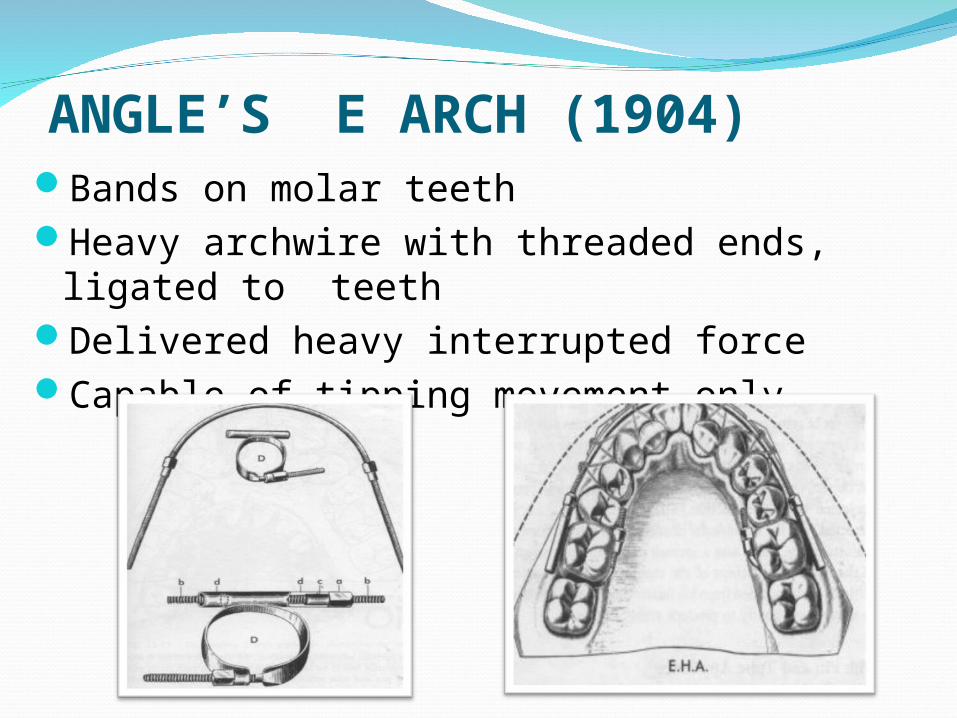
ANGLE’S E ARCH (1904)Bands on molar teethHeavy archwire with threaded ends, ligated
to teethDelivered heavy interrupted forceCapable of tipping movement only
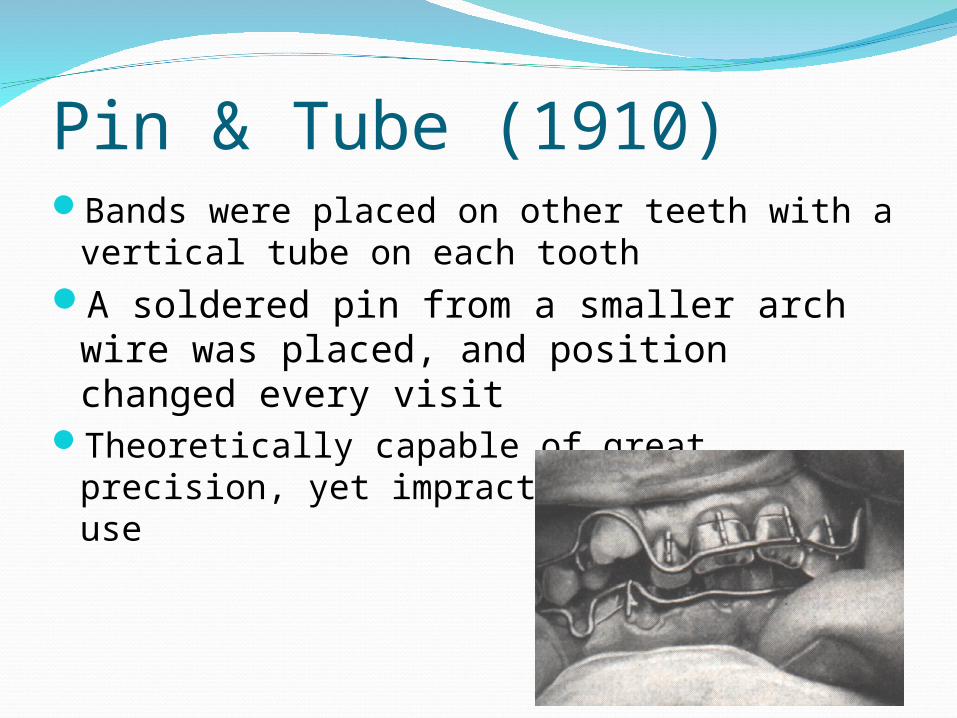
Pin & Tube (1910)Bands were placed on other teeth with a
vertical tube on each toothA soldered pin from a smaller arch wire
was placed, and position changed every visit
Theoretically capable of great precision, yet impractical in clinical use
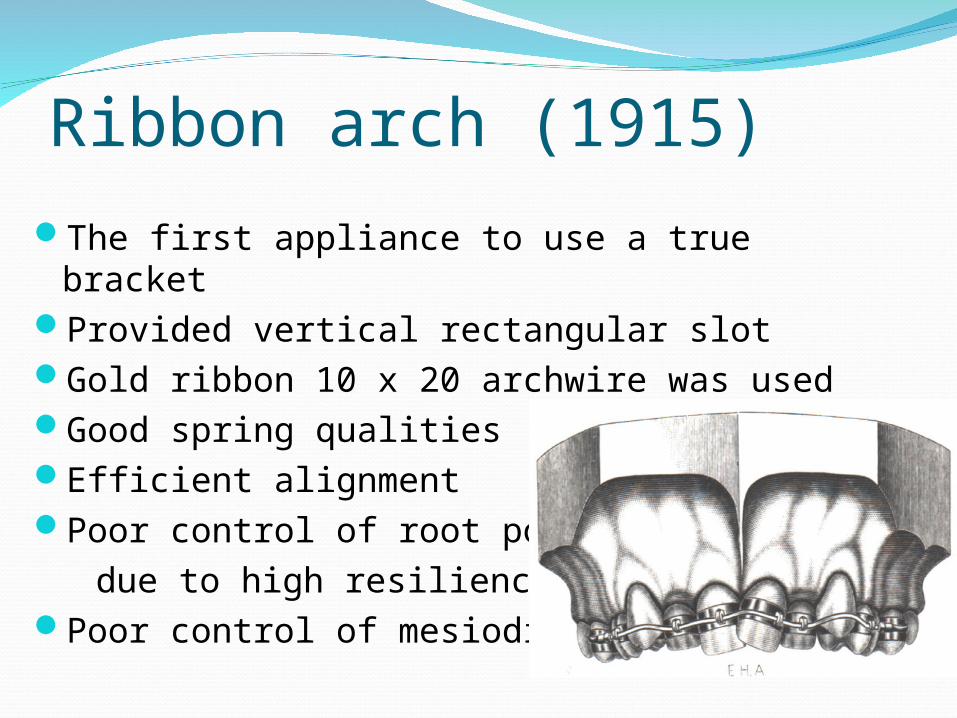
Ribbon arch (1915)The first appliance to use a true bracket Provided vertical rectangular slot Gold ribbon 10 x 20 archwire was usedGood spring qualitiesEfficient alignmentPoor control of root position due to high resiliency of wirePoor control of mesiodistal tip
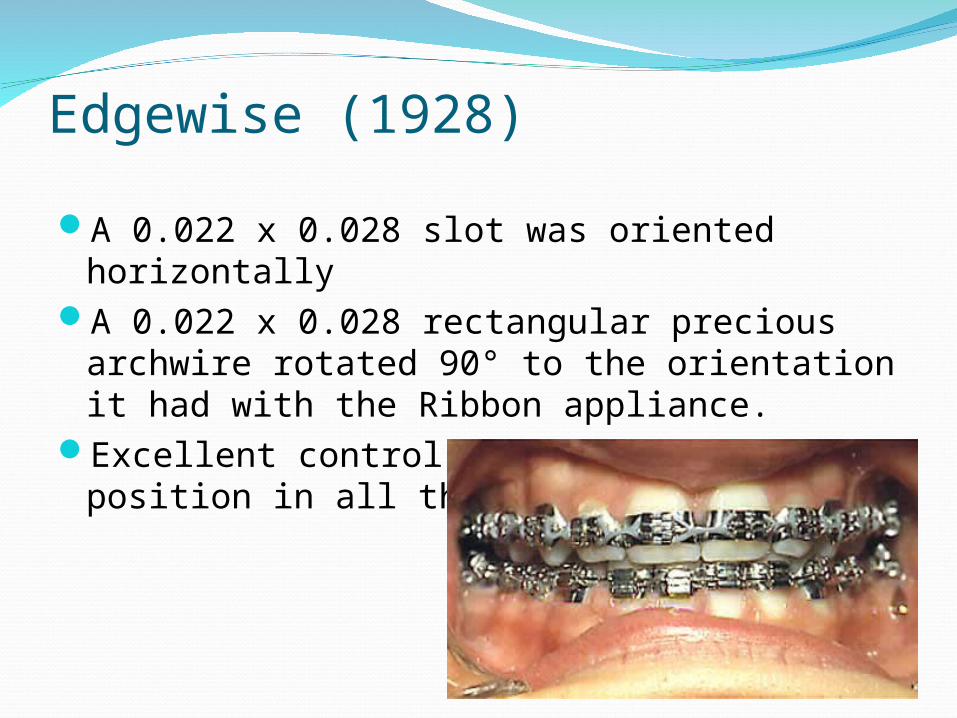
Edgewise (1928)
A 0.022 x 0.028 slot was oriented horizontallyA 0.022 x 0.028 rectangular precious
archwire rotated 90° to the orientation it had with the Ribbon appliance.
Excellent control of crown & root position in all three planes
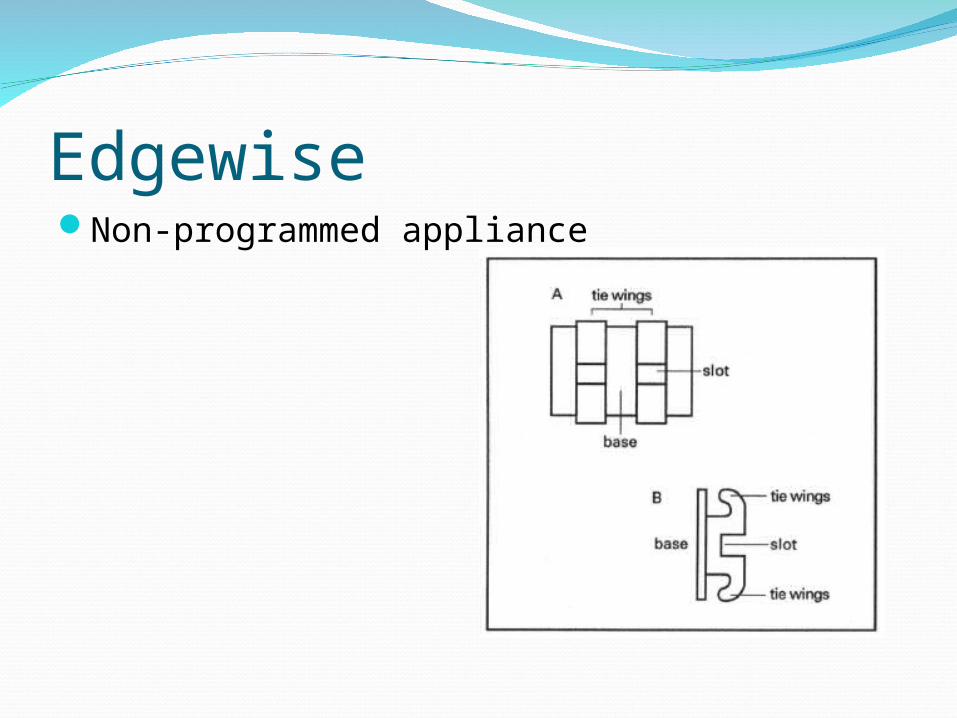
EdgewiseNon-programmed appliance
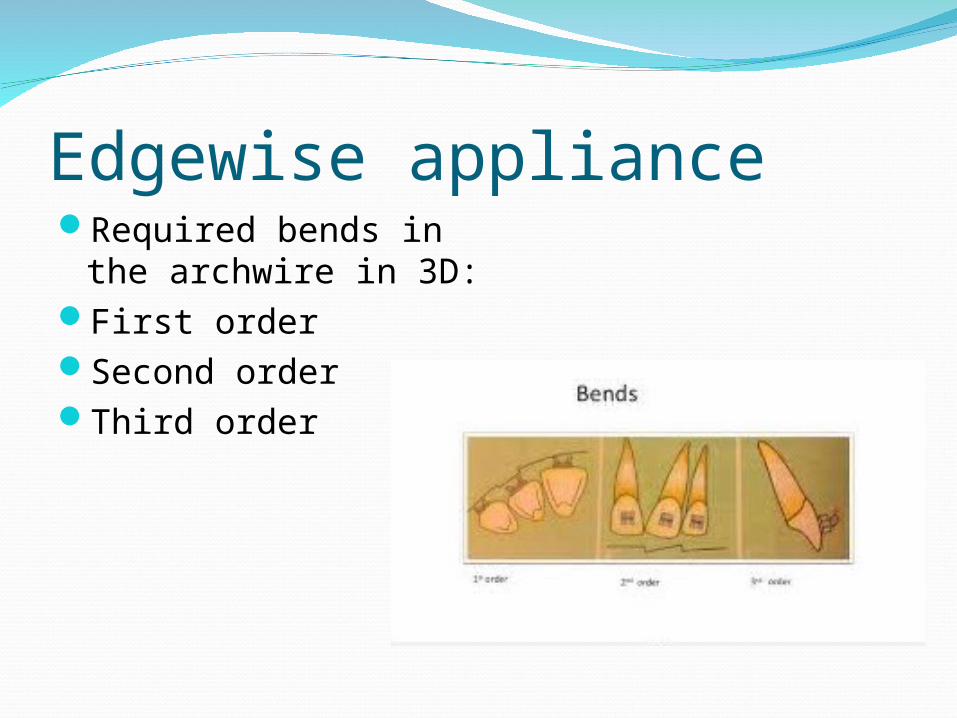
Edgewise applianceRequired bends in the
archwire in 3D:First order Second orderThird order
Edgewise applianceTreatment phases:Correction of interarch relationship, leveling
and alignmentOpening or closing spacesFinishing
Edgewise applianceAdvantages:
Precision Mechanical simplicityCleanlinessVersatility
DisadvantagesLack of system and number of variantsDependence on wire bendingFrictionAnchorage demands
EdgewiseModifications to Edgewise (Partially
programmed):Angle: angulation of brackets on the bandJarabak and Fizzel: “building treatment into
the appliance” Incorporation of tip and torqueHoldaway: increase bracket angulation next to
extraction siteRaising upper lateral base: To eliminate need
for offset bend
Charles TweedReintroduced tooth extraction
due to facial esthetics and occlusal stability
Philosophy: malocclusion was genetically determined due to tooth and jaw mismatch in sizes
Adapted the edgewise appliance for extraction treatment
Used the subdivision approach for anchorage control by moving the canines distally then retracting the incisors
Charles Tweed Modified Edgewise appliance by using the
0.022” in different widthsDouble width for anteriors, intermediate for
PM, twin slot in 6s, tubes on 7s
Reymond Begg At first a follower of
Angle’s non-extraction After cases of poor profile
esthetics and relapse, he advocated for tooth extraction
Philosophy: tooth size reduction is required to compensate for dietary changes
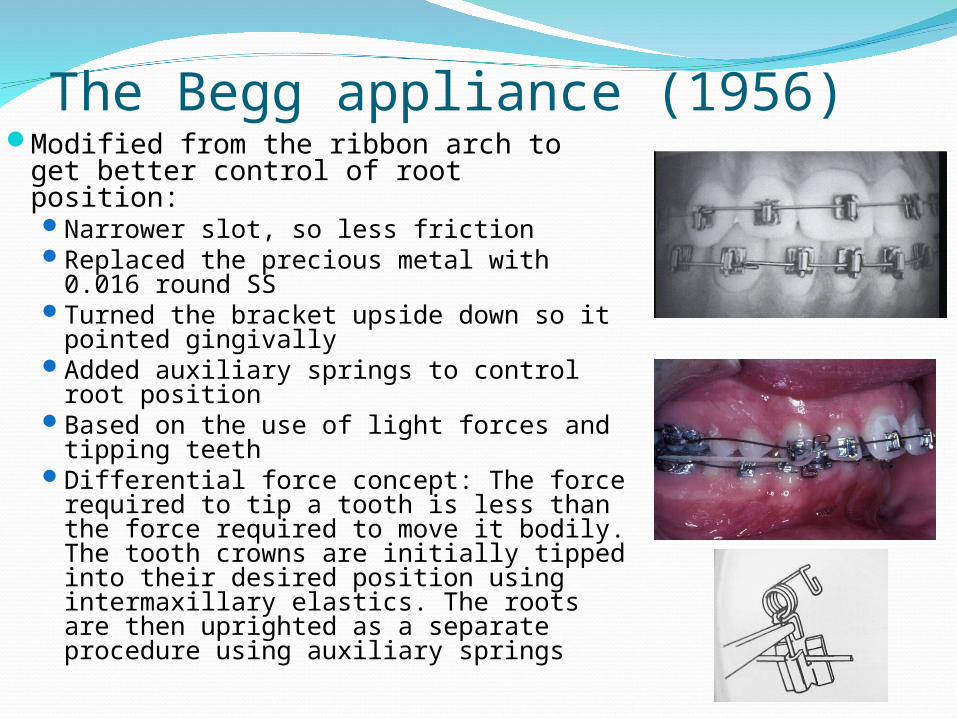
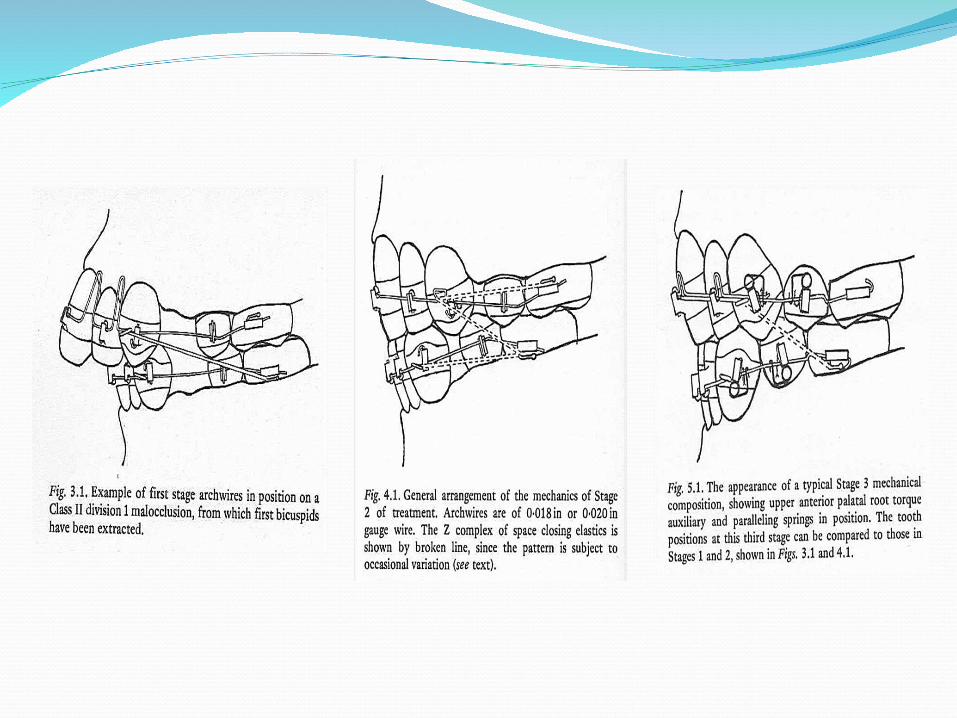
The Begg appliance (1956)Modified from the ribbon arch to get
better control of root position:Narrower slot, so less frictionReplaced the precious metal with
0.016 round SSTurned the bracket upside down so it
pointed gingivallyAdded auxiliary springs to control root
positionBased on the use of light forces and
tipping teeth Differential force concept: The force
required to tip a tooth is less than the force required to move it bodily. The tooth crowns are initially tipped into their desired position using intermaxillary elastics. The roots are then uprighted as a separate procedure using auxiliary springs
Treatment stages:Stage I: Alignment and levelingClosure of spacesOvercorrection of rotationsOvercorrection of OB and OJCorrection of inter arch relationships
Stage II:All extraction spaces closedThe objectives achieved in stage 1 maintained
Stage III: Correction of tooth angulations and inclinationsThe objectives achieved in stage 1 and 2 maintained
The Begg appliance (1956)
Begg applianceAdvantages:
Systemic approach of stagesBetter anchorageLack of frictionFree tippingSpeed of tooth movementDifferential tooth movementMinimal wire binding through use of auxiliariesMinimal post-treatment relapse
Begg applianceDisadvantages:
Emphasis on extractionsReliance on elasticsComplexity in finishingOral hygiene difficultiesBreakagesLack of precisionLack of flexibility
Larry AndrewsDeveloped preadjusted edgewise
based on his “6 keys of occlusion”Studied 120 subjects with ideal
occlusion with no history of orthodontic treatment
His appliance eliminated the need for wire bending
Proper bracket position allows the teeth to be placed with a straight wire into an occlusal contact with an excellent mesiodistal inclination (tip) and excellent faciolingual inclination (torque)
The brackets placed at the midpoint of the facial axis of the clinical crown (FACC)
Andrews’ 6 keys of occlusion (1972)
Correct interarch relationship.Correct crown Angulation (Tip).Correct crown Inclination (Torque).No Rotations.Tight Contacts.Flat Curve of Spee.
Andrews’ 6 keys of occlusionInterarch relationships:The distal surface of the distobuccal cusp of the
upper first permanent molar made contact and occluded with the mesial surface of the mesiobuccal cusp of the lower second molar. The mesiodistal cusp of the upper first permanent molar fell within the groove between the mesial and middle cusps of the lower first permanent molar
Canines and premolars occlude in a cusp-embrasure way buccally, and cusp-fossa lingually
Andrews’ 6 keys of occlusion
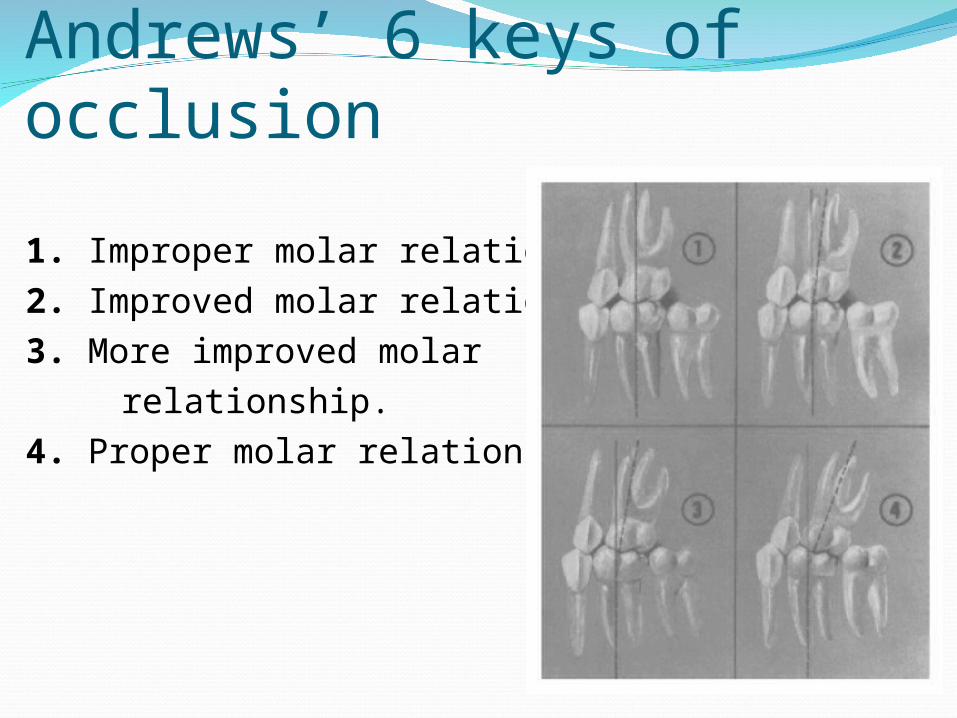
1. Improper molar relationship. 2. Improved molar relationship. 3. More improved molar
relationship.4. Proper molar relationship.
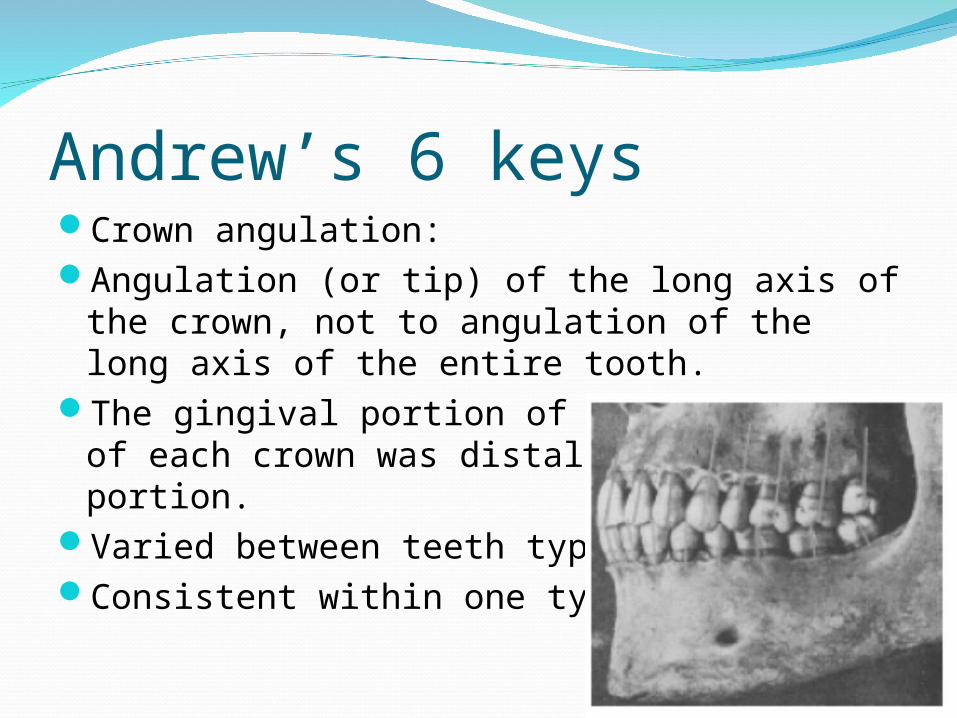
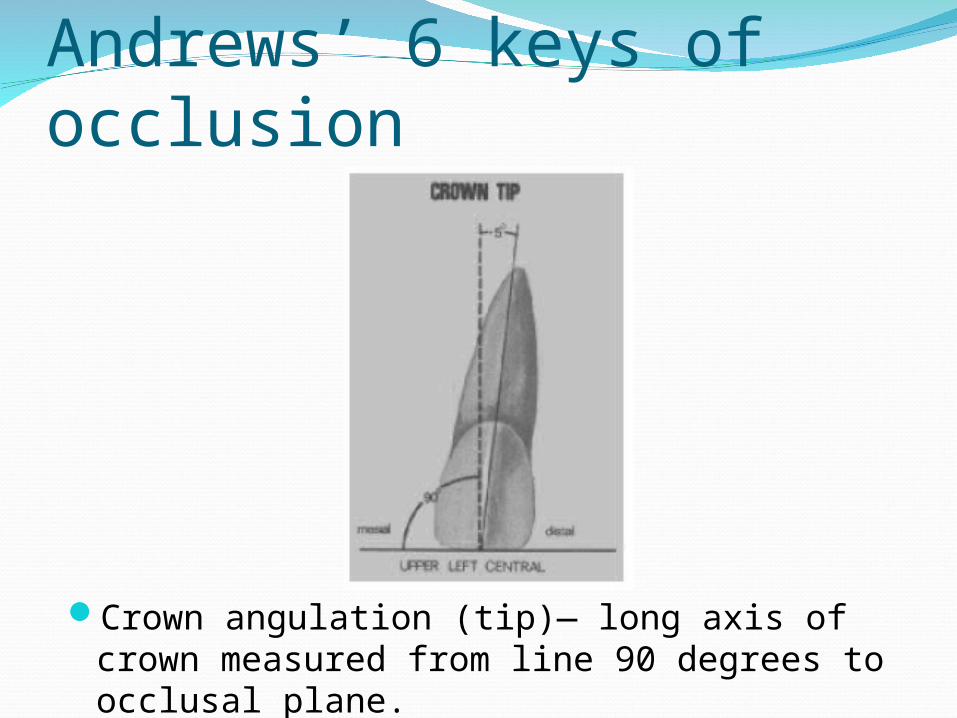
Andrew’s 6 keysCrown angulation:Angulation (or tip) of the long axis of the
crown, not to angulation of the long axis of the entire tooth.
The gingival portion of the long axis of each crown was distal to the incisal portion.
Varied between teeth typesConsistent within one type
Andrews’ 6 keys of occlusion
Crown angulation (tip)— long axis of crown measured from line 90 degrees to occlusal plane.
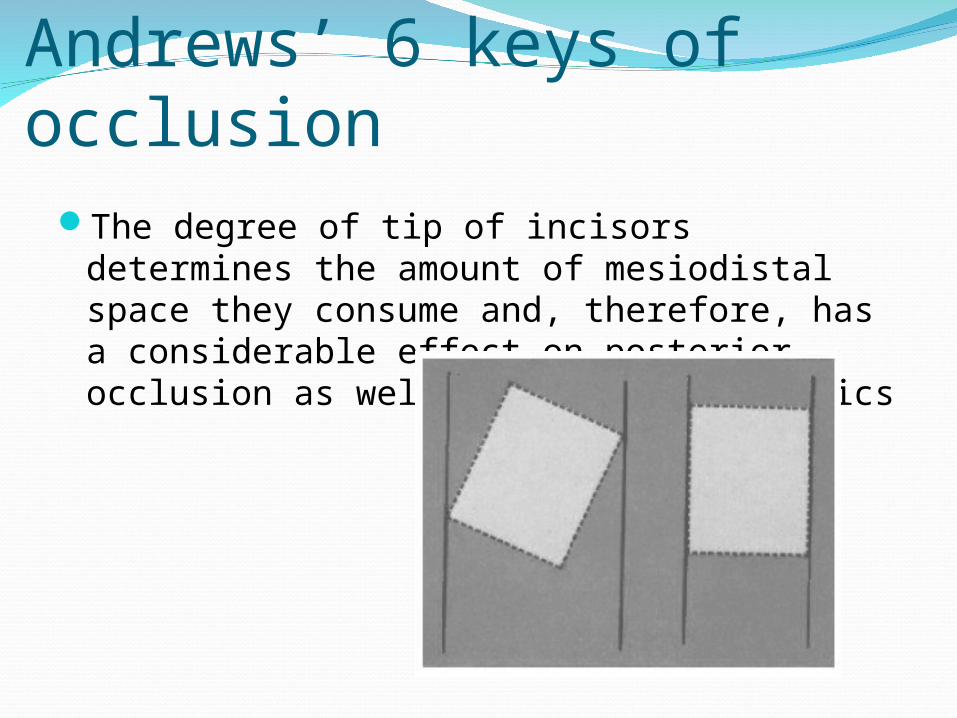
Andrews’ 6 keys of occlusionThe degree of tip of incisors determines the
amount of mesiodistal space they consume and, therefore, has a considerable effect on posterior occlusion as well as anterior esthetics
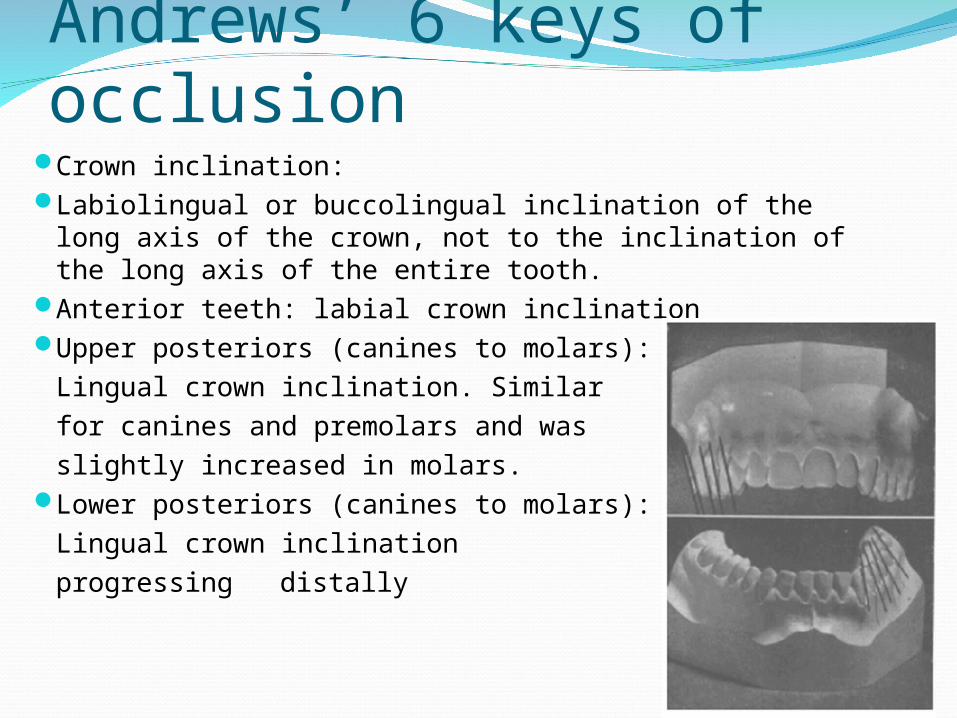
Andrews’ 6 keys of occlusionCrown inclination:Labiolingual or buccolingual inclination of the long axis of
the crown, not to the inclination of the long axis of the entire tooth.
Anterior teeth: labial crown inclination Upper posteriors (canines to molars):
Lingual crown inclination. Similarfor canines and premolars and was slightly increased in molars.
Lower posteriors (canines to molars): Lingual crown inclinationprogressing distally
Andrews’ 6 keys of occlusion
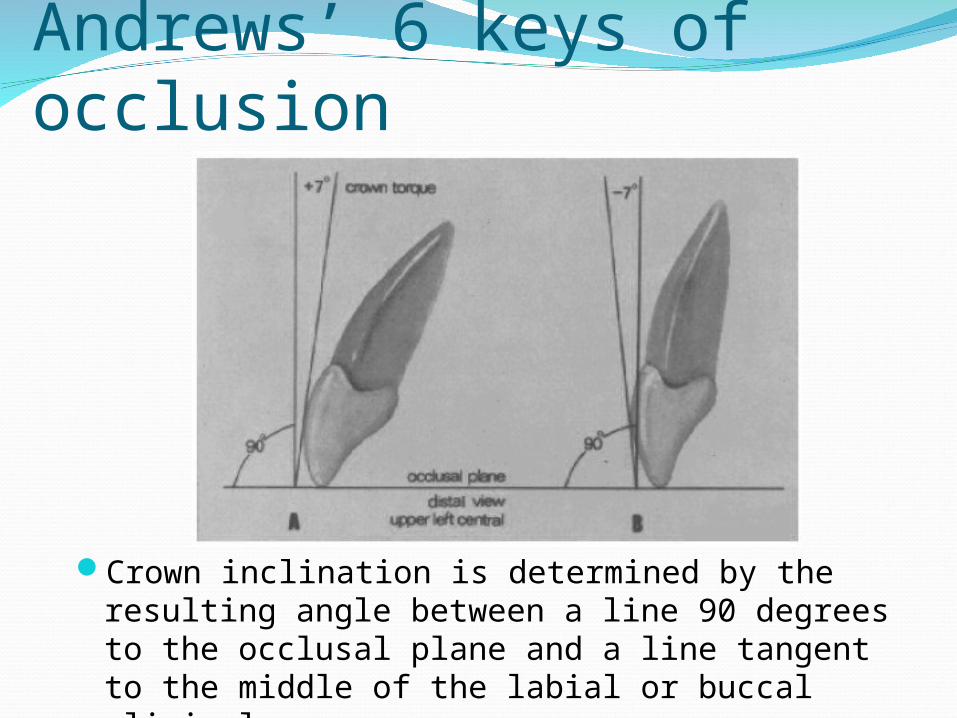
Crown inclination is determined by the resulting angle between a line 90 degrees to the occlusal plane and a line tangent to the middle of the labial or buccal clinical crown.
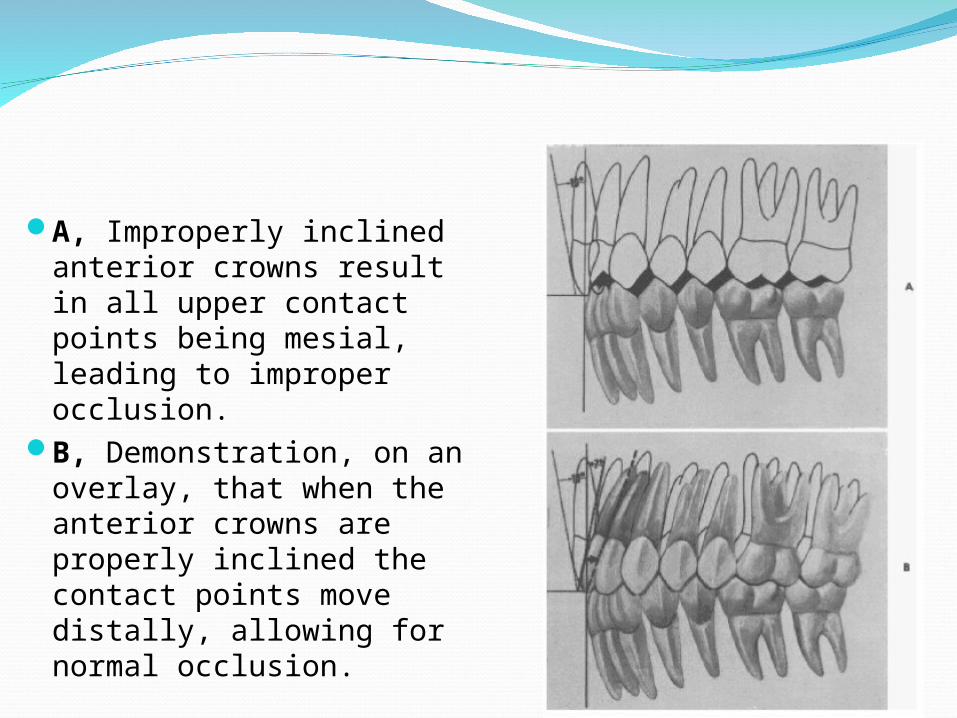
A, Improperly inclined anterior crowns result in all upper contact points being mesial, leading to improper occlusion.
B, Demonstration, on an overlay, that when the anterior crowns are properly inclined the contact points move distally, allowing for normal occlusion.
Andrews’ 6 keys of occlusionRelationship between tip and torque:The more we torque the anterior portion of
an upper rectangular arch wire, a proportional amount of mesial tip of the anterior crowns is lost.
The ratio is approximately 4:1. For every 4 degrees of lingual crown torque, there is 1 degree of mesial convergence of the gingival portion of the central and lateral crowns
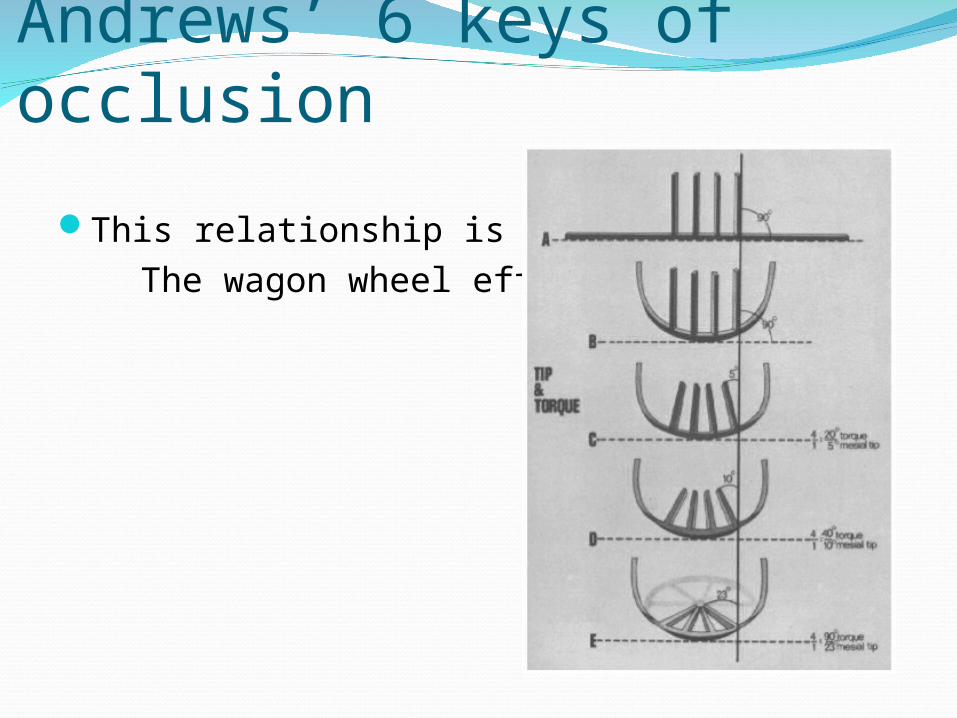
Andrews’ 6 keys of occlusion
This relationship is called The wagon wheel effect
Andrew’s 6 keysRotations
Teeth should be free of undesirable rotationsRotated posterior teeth would occupy more space
Tight contactsNo spacesTooth size discrepancy should be corrected, so that space closure would not affect occlusion
Andrews’ 6 keys of occlusion
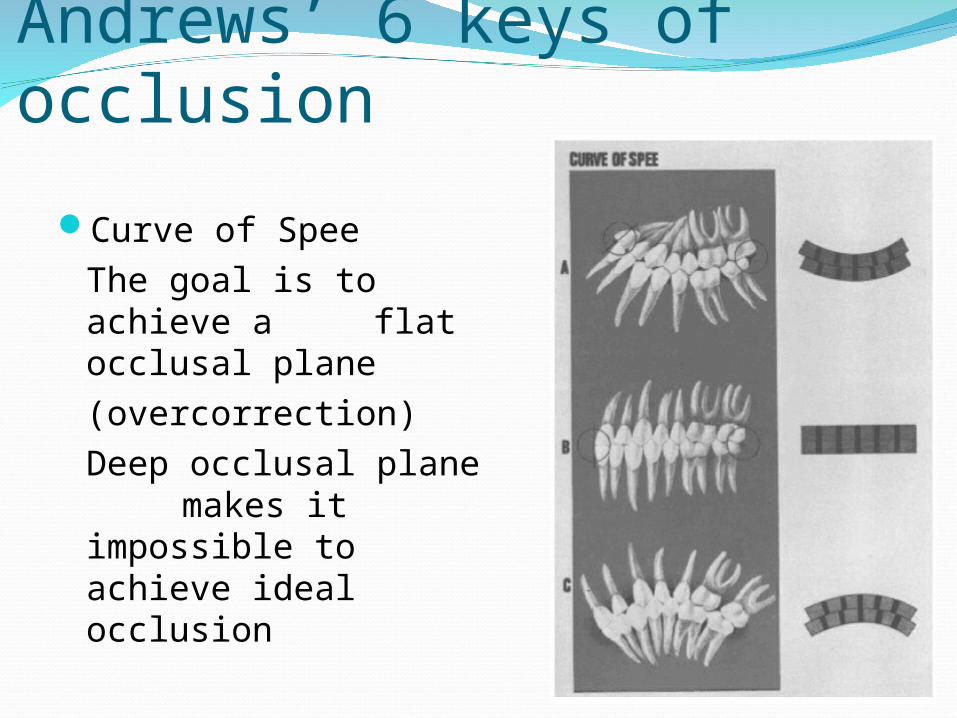
Curve of SpeeThe goal is to achieve a
flat occlusal plane (overcorrection)Deep occlusal plane makes it impossible to
achieve ideal occlusion
The Straight Wire Appliance
Theoretical basis: Most individuals have normal teeth regardless of occlusal typeThe size of normal crowns has no effect on their ability to achieve optimal occlusionJaws must be normal and correctly related to allow teeth to be correctly positioned and relatedDentitions with normal teeth in jaws that are correctly related can be brought to optimal occlusal standards
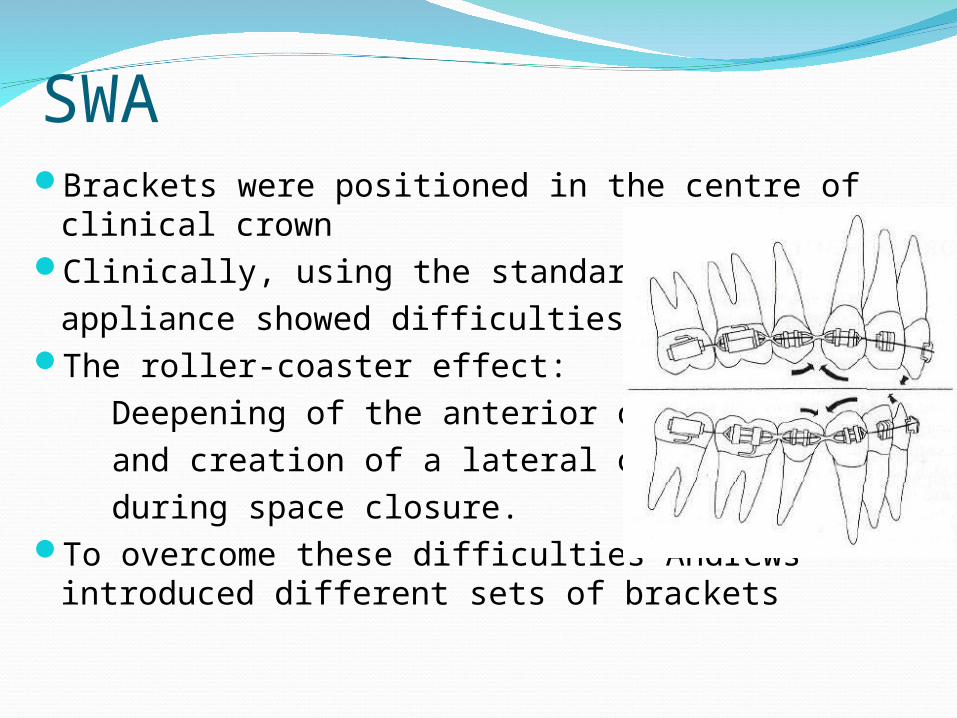
SWABrackets were positioned in the centre of
clinical crownClinically, using the standard
appliance showed difficulties.The roller-coaster effect: Deepening of the anterior over bite and creation of a lateral open bite during space closure.To overcome these difficulties Andrews
introduced different sets of brackets
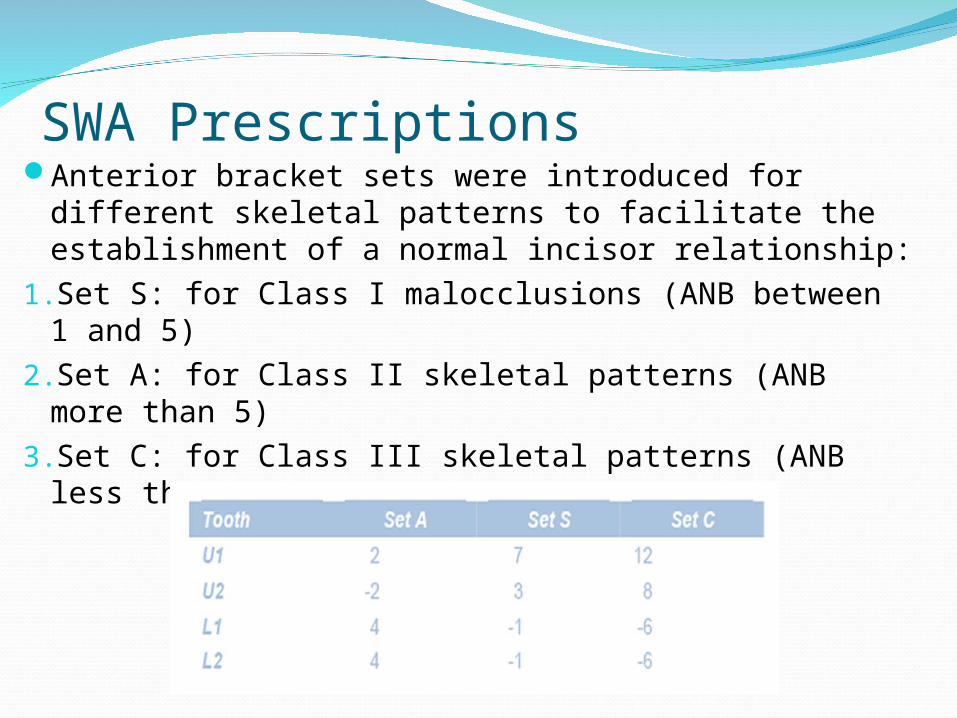
SWA PrescriptionsAnterior bracket sets were introduced for different
skeletal patterns to facilitate the establishment of a normal incisor relationship:
1.Set S: for Class I malocclusions (ANB between 1 and 5)
2.Set A: for Class II skeletal patterns (ANB more than 5)
3.Set C: for Class III skeletal patterns (ANB less than 1)
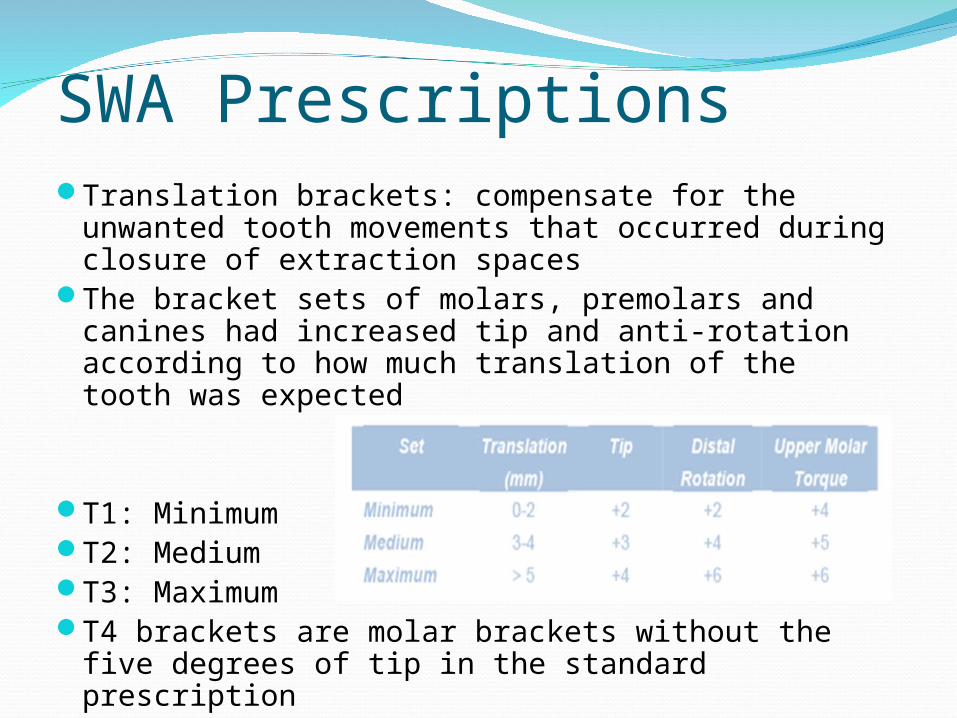
Translation brackets: compensate for the unwanted tooth movements that occurred during closure of extraction spaces
The bracket sets of molars, premolars and canines had increased tip and anti-rotation according to how much translation of the tooth was expected
T1: MinimumT2: MediumT3: MaximumT4 brackets are molar brackets without the five
degrees of tip in the standard prescription
SWA Prescriptions
Ronald RothRecognized the importance of
Andrew’s concept, but only in harmony with properly functioning temporomandibular joint
Incorporated “The six keys to normal occlusion with mandible in gnathologic centric relation”
Introduced the repositioning splint to find CR
Ideal Functional Occlusion
Coincident CR and COOcclusal forces directed down the long axis of
teeth.0.005” between the anterior teeth in occlusion.In lateral excursion and protrusion the incisors
and canines disocclude the posterior teeth.Protrusion with dis-occlusion of posterior teeth.Working side ‘canine guided’Non-working
Roth’s modificationsOvercorrection, due to:High relapseCompensate for play between archwire and the bracketCurve of Spee deepens after treatmentTeeth adjacent to extraction site tend to rotate and tip towards the extraction site (rollercoaster effect)As teeth in the buccal segments settle they will rotate and tip mesially, so by overcorrection they will settle better than teeth that are already mesially inclinedAs band spaces close, there is a corresponding loss of torque of the anterior teeth
Roth’s prescription One appliance fits allAvailable in 0.018”, 0.022” slotsBracket positioning: Andrew’s FA point is the
reference:Incisors: more incisally Lower canines: more gingivally

Bennett-Mclaughlin
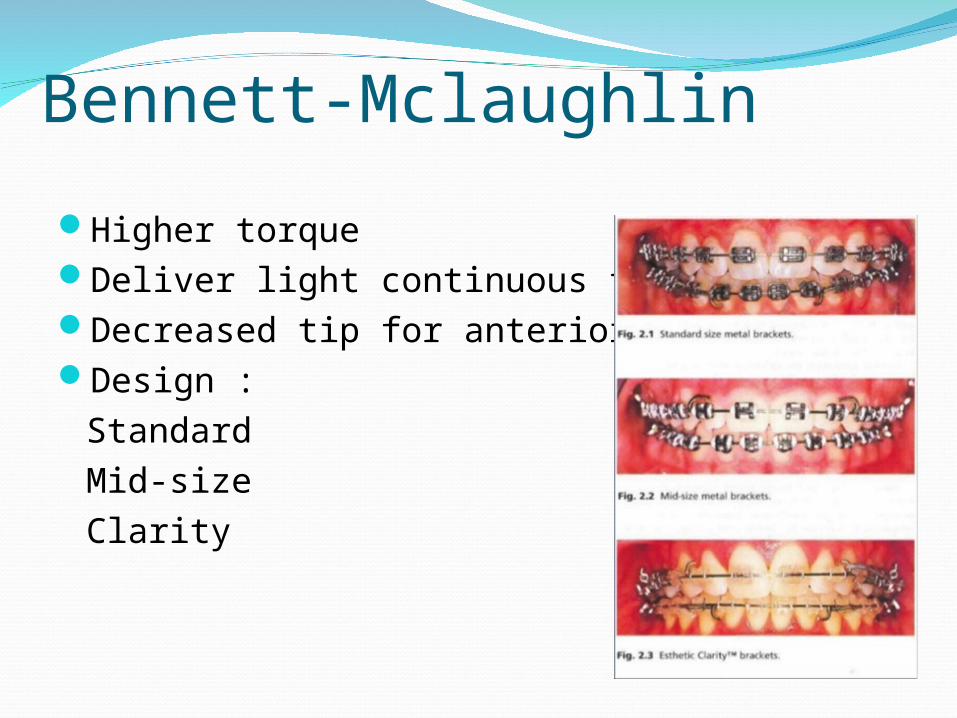
Higher torqueDeliver light continuous forceDecreased tip for anterior teethDesign :
Standard Mid-sizeClarity
MBTBracket design :Mid-size metal bracketsRhomboidal shape Torque in baseThe 0.022 not the 0.018 slot Thicker 0.5 mm bracket on upper second premolar if they are small
MBT
Versatility of bracket system: to avoid wire binding
Bracket positioningAnchorage control early in treatmentGroup movement where possibleCanine laceback: retraction, prevent mesial
movementcorrect midline, protect flexible archwire
Bendback: to prevent mesial movement
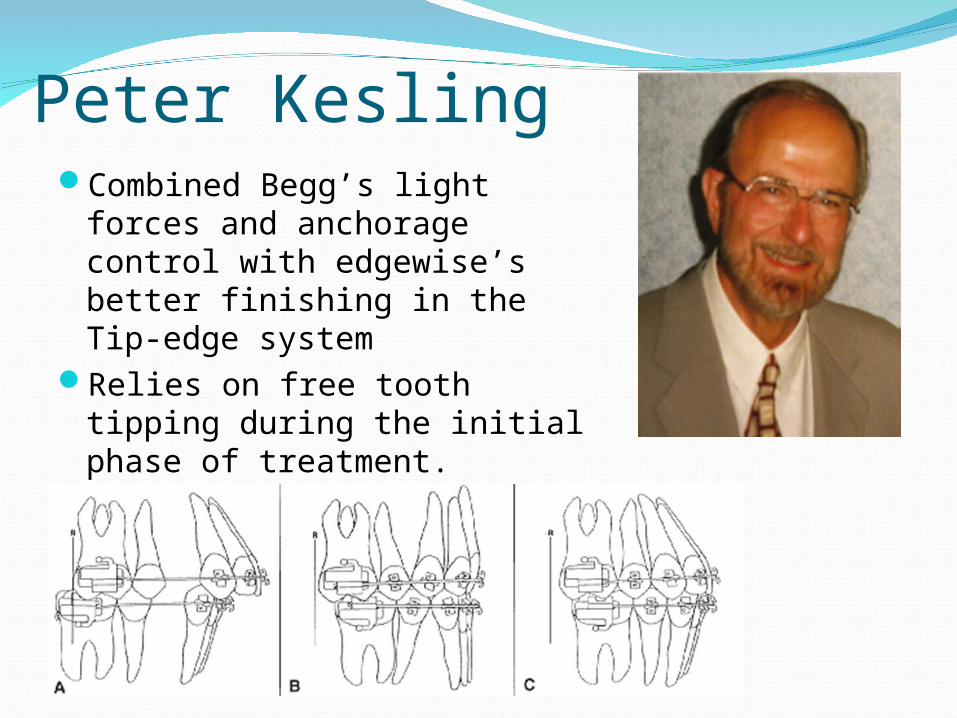
Peter KeslingCombined Begg’s light forces
and anchorage control with edgewise’s better finishing in the Tip-edge system
Relies on free tooth tipping during the initial phase of treatment.
Using rigid rectangular archwires to upright teeth later
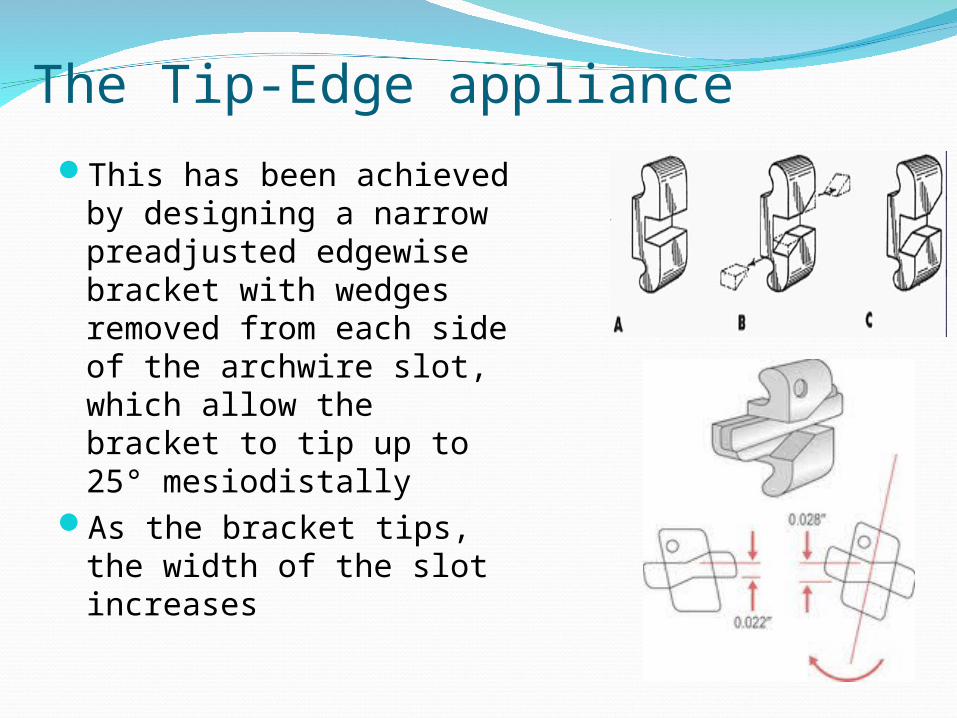
The Tip-Edge applianceThis has been achieved by
designing a narrow preadjusted edgewise bracket with wedges removed from each side of the archwire slot, which allow the bracket to tip up to 25° mesiodistally
As the bracket tips, the width of the slot increases
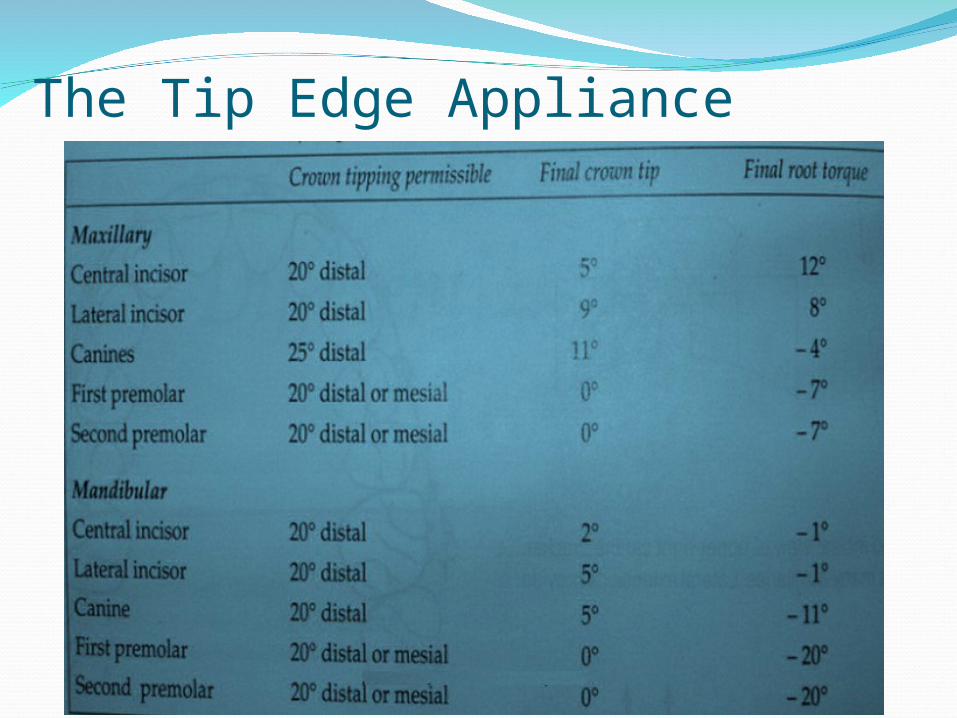
The Tip Edge Appliance
Advantages:Permits tooth tipping in early stages of treatmentProgressive torque applicationImproved precision and finishing Versatility is increasedExpresses all the treatment built into the bracketOvertreatment
The Tip Edge Appliance
The Tip Edge ApplianceDisadvantages:A relatively poor rotational control due to narrow single wing bracket Friction (due to elastomeric ligation)Dependence on intermaxillary elastics Relative complexity in finishing stageRigid designDependence on extraction treatment
Thank you









![Pain level between clear aligners and fixed appliances: a ......with fixed appliances, it is common to feel pain and dis-comfort [6], reaching its peak 24h after arch insertion, and](https://img.pdfslide.us/doc/110x75/5f88505305ea577cf73ee39c/pain-level-between-clear-aligners-and-fixed-appliances-a-with-fixed-appliances.jpg)