Embed Size (px)
DESCRIPTION
Hearing Screening in Newborns
Citation preview

Dr.Padmesh
HEARING SCREENING IN NEWBORNS

Dr.Padmesh. V
UNIVERSAL Screening is the ideal method.
Atleast HIGH RISK Screening is mandatory.
High risk factors: Genetic abnormalities (next slide), In-utero infections, including cytomegalovirus,
herpes, rubella, syphilis, and toxoplasmosis , Asphyxia, Hyperbilirubinemia, Meningitis/sepsis Premature infants in the neonatal intensive
care unit.

Dr.Padmesh. V
Syndromes associated with hearing loss:
Neurofibromatosis Osteopetrosis Waardenburg syndrome Pendred syndrome Jervell syndrome Lange-Nielsen syndrome Alport syndrome Usher syndrome Treacher-Collins syndrome

Dr.Padmesh. V
Modalities for performing hearing screening
Evoked Oto acoustic emissions (EOAEs).
Auditory brainstem response (ABR) & Automated ABR (AABR) testing .

Dr.Padmesh. V
THRESHOLD OF >= 35 Db has been established as a
cut-off for abnormal screening test, and prompts further testing.

Dr.Padmesh. VEOAE
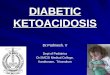
OAEs are used to assess cochlear integrity.
Fast objective screening test to evaluate the function of the peripheral auditory system, primarily the cochlea, which is the area most often involved in sensorineural hearing loss.
The presence of evoked OAE responses indicates hearing sensitivity in the normal to near-normal range.
Quicker to perform than ABR.
However,maybe affected by debris/fluid in external or middle ear.
OAE are unable to detect some forms of Sensory neural hearing loss,including auditory dyssynchrony.
Coaechlear!

Dr.Padmesh. VEOAE

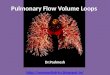
Dr.Padmesh. VABR / BERA
Synonyms: Brain stem evoked response audiometry, Auditory brain stem response, ABR audiometry, BAER (Brainstem auditory evoked response audiometry).
Neural signals are generated in VIII Cranial nerve & brain stem in response to auditory stimuli.
Objective way of eliciting brain stem potentials in response to audiological click stimuli. Electro encephalographic waves are recorded by electrodes placed over the scalp.
ABR is reliable after 34 wks postnatal age.
ABR is the preferred screening method to evaluate hearing loss in NICU graduate.

Dr.Padmesh. VABR / BERA
BERA

Dr.Padmesh. V
Recommendations:
The initial screening can be performed using OAE/ AABR or both.
OAEs alone are not a sufficient screening tool in infants who are at risk for neural hearing loss (e.g., auditory neuropathy/dyssynchrony, infants with jaundice/ asphyxia).
Hence, any infant in the NICU or in the hospital for more than 5 days should undergo an ABR screening also, so that the presence of auditory neuropathy is not missed.

Dr.Padmesh. V
Recommendations:
Both ears should be screened individually.
The initial screening should consist of 2 attempts maximum on each ear.
The re-screening is a second hearing screening that can be performed if an infant does not pass the initial hearing screening in one or both ears and it should be performed prior to 1 month of age.
In India, it would be practical to do the second test at 6 weeks when the infant comes for immunization.
If an infant does not pass the re-screening or if results cannot be obtained in one or both ears, he should be referred for diagnostic audiological evaluation which should involve diagnostic BERA.

Dr.Padmesh. V
Recommendations:
When to screen : a. Testing should be done as close to discharge as
possible b. It is preferable to screen between 24 – 72 Hrs of life. c. False positive rates decreases after 12 – 24 hrs of life d. After infant completes nursing or feeding e. Screen after 34 week of gestation. f. Antibiotic therapy should not be reason for missed
screen. g. Screen can be done during phototherapy. h. Test time, 3–6 min per baby depending on type of
equipment and co-operation. i. Should return for 2nd screen within 6 weeks

Dr.Padmesh. V
Recommendations: Neonatal Intensive Care unit babies: a. AABR is preferred method of screening for all NICU infants;
OAE an alternative b. Initial screen: Two attempts may be conducted on each ear
before considering referral c. Second screen: Separate time of the day than the initial
screen. Two attempts may be conducted on each ear before referral.
d. Maximum: Do not screen more than 2 times in each ear at either the initial or second screen.
e. NICU infants admitted for greater than 5 days should have auditory brainstem response (ABR) included as part of their hearing screening so that neural hearing loss will not be missed.
f. Infants who do not pass the automated ABR should be referred directly to an audiologist for re – screening/ diagnostic ABR .

Dr.Padmesh. V
Protocol for Newborn Hearing Screening Program [(Based on NHS (UK) Newborn Hearing Screening Program)]
Portable handy equipment (OTOPORT, Otodynamics, UK).
If abnormal result (no response)
Test repeated after 2 weeks.
If again no response
BEARA test
(Done for confirmation & quantification of hearing loss)
If BERA abnormal
Do comprehensive hearing evaluation.
If abnormal
Hearing Aid usage at the earliest.

Dr.Padmesh. V
Protocol for Newborn Hearing Screening Program [(Based on NHS (UK) Newborn Hearing Screening Program)]
Hearing aids may be fitted for infants as early as 2 months of age.
This should be followed with auditory training and speech therapy.
Children with profound deafness who drive negligible benefit from
conventional amplification with hearing aids may be considered for
cochlear implants.
Identification and intervention for hearing impairment should occur before 6 months of age.

Dr.Padmesh. V
Reference:
NNF Clinical Practice Guidelines
Manual of Neonatal Care –Cloherty
Indian Pediatrics 2011;48: 351-353

Dr.Padmesh. V
THANK YOU!