Embed Size (px)
DESCRIPTION
Management of Snake bite in Children
Citation preview

Dr.Padmesh. V
Snake bite Management
Dr.Padmesh .V,Dept of Pediatrics,
Dr.SMCSI MCH, Karakonam.
Dr.Padmesh. V
• Pediatric snakebite mortality and morbidity remains significant.
• National Snakebite Conference was convened in July 2006 which developed national protocols for first aid and treatment.
Dr.Padmesh. V
• Of the >3,000 known species of snakes, only 200 are poisonous to humans.
• Of the poisonous snakes, 90% are members of one of three families:
• Hydrophidae - poisonous sea snakes• Elapidae - cobras, kraits, coral snakes • Viperidae – vipers
Dr.Padmesh. V
V
V
VV ..
..
..
.
Dr.Padmesh. V
PATHOGENESIS. • Snake venom is a mixture of polypeptides, proteolytic enzymes, and
toxins, which are species-specific.
• Hydrophidae - poisonous sea snakes• Elapidae - cobras, kraits, coral snakes
• Venom have a curare-like effect by blocking neurotransmission at neuromuscular junction.
• Death results from respiratory depression.
Primarily neurotoxic
Dr.Padmesh. V
PATHOGENESIS. • Snake venom is a mixture of polypeptides, proteolytic enzymes, and
toxins, which are species-specific.
• Viperidae – vipers • Crotalidae (sub family of viperidae) :
• Tissue necrosis, vascular leak, and coagulopathies.
• Death from pit viper bites results from hemorrhagic shock, adult respiratory distress syndrome, and renal failure.
Cytolytic
Dr.Padmesh. V• Clinical Manifestations.
• Bites of most Elapidae are minimally painful because venom has no cytotoxin.
• However, lack of immediate symptoms should not be mistaken for absence of serious envenomation.
• Neurotoxic symptoms can progress rapidly in a few hours from mild drowsiness to cranial nerve palsies, weakness, and death from respiratory failure.
Dr.Padmesh. V
• Clinical Manifestations.
• Pit viper bites usually occur on extremities; pain and swelling occur at site within minutes.
• As venom moves proximally, edema and ecchymosis advance;
• In severe cases: Bulla formation and tissue necrosis.
• Systemic symptoms: nausea, vomiting, diaphoresis, weakness, tingling around face, and muscle fasciculations.
• Rarely, patients may present in shock with generalized edema or cardiac arrhythmias.
• Complex clotting abnormalities often occur.
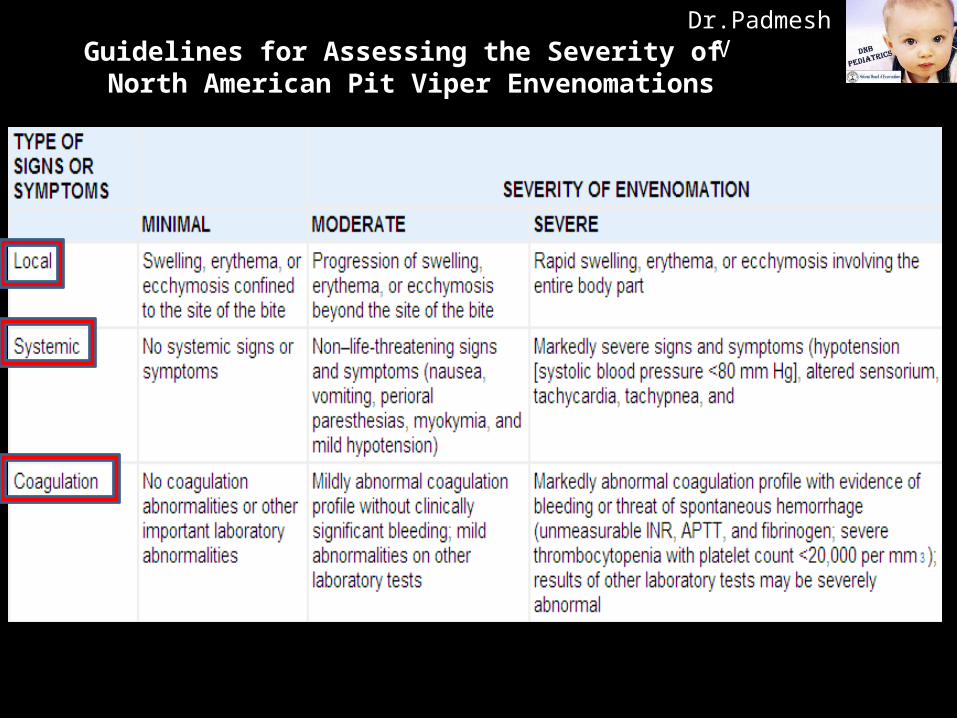
Dr.Padmesh. VGuidelines for Assessing the Severity of
North American Pit Viper Envenomations
Dr.Padmesh. V
• Treatment: First aid recommended : “Do it R.I.G.H.T.”
• R = Reassure the patient. 70% of all snakebites are from non venomous species. Only 50% of bites by venomous species actually envenomate the patient.
• I = Immobilise in the same way as a fractured limb. Children can be carried. Use bandages or cloth to hold the splints, not to block the blood supply or apply pressure. Do not apply any compression in the form of tight ligatures.
• G.H = Get to Hospital immediately. Traditional remedies have NO PROVEN benefit in treating snakebite.
• T = Tell the doctor of any systemic symptoms such as ptosis that manifest on the way to hospital.
Dr.Padmesh. V
• Treatment:
• First task: Determine whether bite was by a poisonous snake and if envenomation occurred.
• If snake has been killed, it should be brought to emergency department for identification.
• Immediate care : Immobilize the bitten extremity and transport the patient to hospital.
• Expert view: Constricting bands increase risk of ischemia exacerbate local tissue damage. Therefore do not apply tourniquet.
• Applying ice to bite site or using excision & suction causes more tissue damage than benefit – to be avoided.
Dr.Padmesh. V
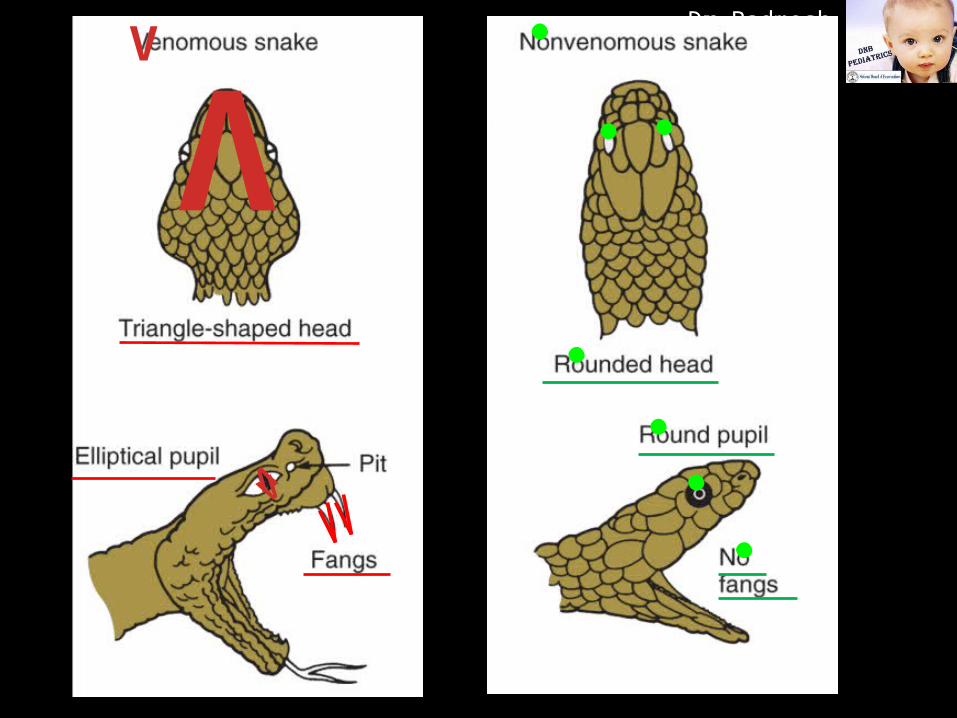
• Treatment: Diagnosis and testing
• Bite marks to determine whether the snake was venomous or non venomous are of no use.
-Many venomous species have more than one set of fangs.
-Non venomous species can leave just two punctures from
enlarged teeth, which can appear to be fang-like.
Dr.Padmesh. V
• Treatment: Diagnosis and testing• The 20 Minute Whole Blood Clotting Test (20 WBCT) : • Standard test for coagulopathy.
• Simple,but requires a clean, new and dry test tube.
• A few mL of fresh venous blood is left undisturbed for 20 minutes, and then gently tilted.
• If the blood is still liquid this is evidence of coagulopathy and confirms that the biting species is Viperine.
• Cobras or Kraits do not cause anti-hemostatic symptoms.
Dr.Padmesh. V
• Treatment. • Emergency department: • Insert large-bore intravenous line.
• Draw blood for baseline laboratory studies: Initial blood tests: -Type and cross-match.-Complete blood count and platelet counts; -Prothrombin Time, Partial Thromboplastin Times; -Fibrinogen and fibrin degradation products; -Blood urea nitrogen, creatinine, creatine phosphokinase
levels.
Dr.Padmesh. V
• Treatment. • Tests repeated at intervals, depending on severity of envenomation.
• Baseline vital signs – Recorded.
• Circumference of bitten extremity - Recorded.
• Demarcation of ecchymosis and swelling should be marked on the limb so progression can be monitored.
• Wound should be cleansed.
• Tetanus toxoid given if appropriate.
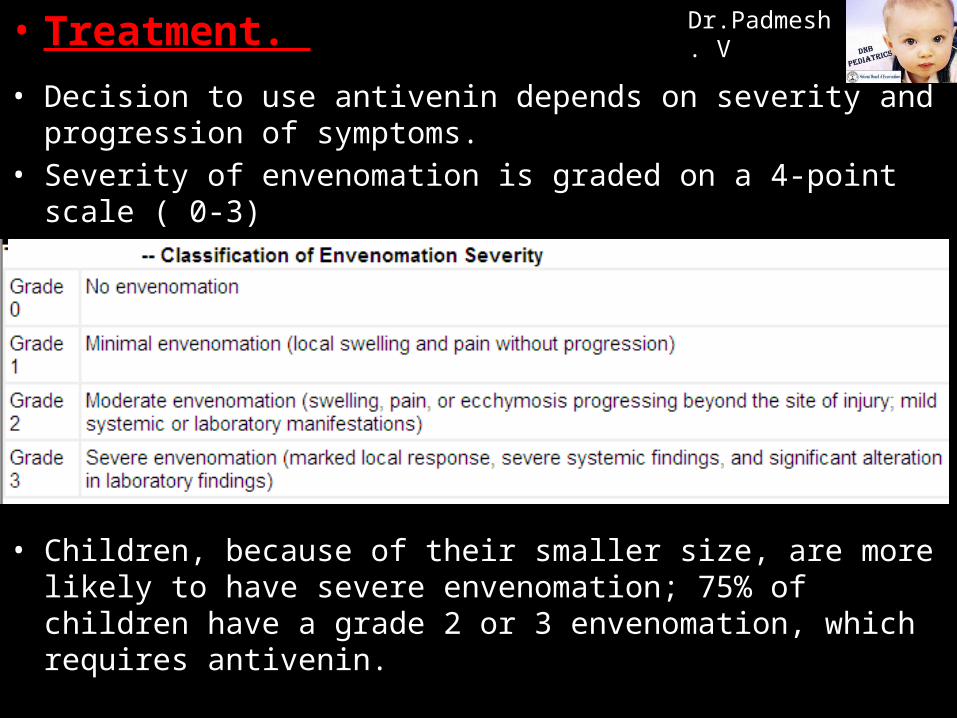
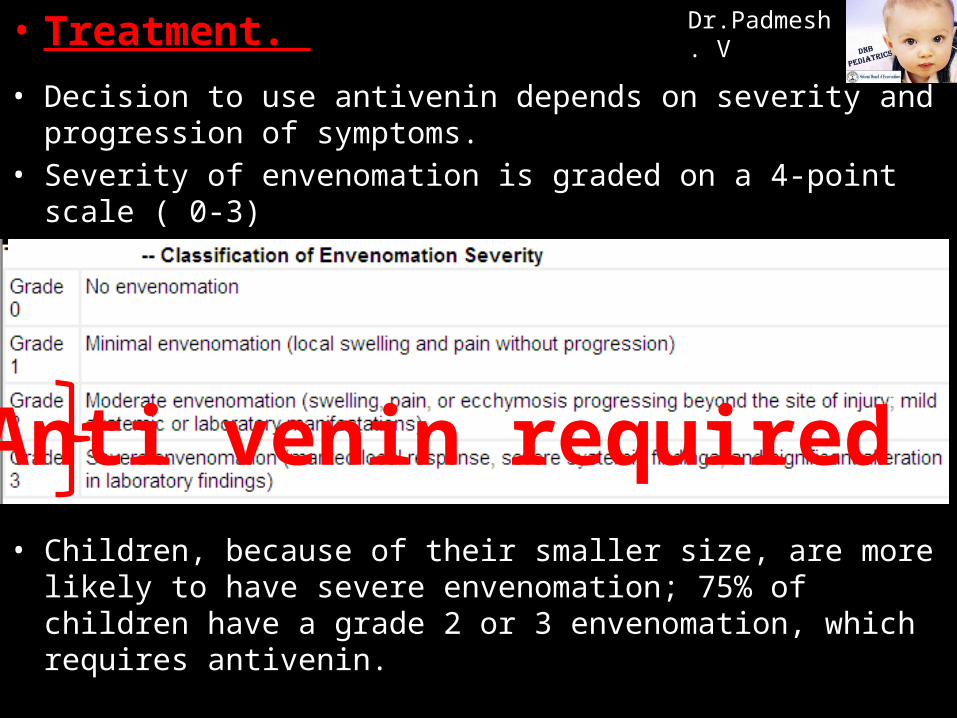
Dr.Padmesh. V• Treatment. • Decision to use antivenin depends on severity and progression of
symptoms. • Severity of envenomation is graded on a 4-point scale ( 0-3)
• Children, because of their smaller size, are more likely to have severe envenomation; 75% of children have a grade 2 or 3 envenomation, which requires antivenin.
Dr.Padmesh. V• Treatment. • Decision to use antivenin depends on severity and progression of
symptoms. • Severity of envenomation is graded on a 4-point scale ( 0-3)
• Children, because of their smaller size, are more likely to have severe envenomation; 75% of children have a grade 2 or 3 envenomation, which requires antivenin.
Anti venin required
Dr.Padmesh. V
• ASV administration criteria
• Antivenin is most effective if delivered within 4 hr of bite.
• Is of little value if administration is delayed beyond 12 hr.
Dr.Padmesh. V• ASV administration criteria
• ASV should not be used without evidence of Systemic envenomation or Severe local swelling.
• Systemic envenomation will be evident from -20WBCT, -Signs of spontaneous bleeding -Neurological impairment such as ptosis.
Dr.Padmesh. V• ASV administration criteria
• ASV should not be used without evidence of Systemic envenomation or Severe local swelling.
• Severe local symptoms:-Swelling rapidly crossing a joint or involving half the bitten
limb, in the absence of a tourniquet.
-If the swelling rapidly continues once the tourniquet has been removed for more than one hour, this should be viewed as due to venom and not due to continuing effect of the tourniquet.
-Purely local swelling is not grounds for administering ASV.
Dr.Padmesh. V
• Anti-snake venom doses and administration• Initial dose of ASV to be given has been subject of debate.
• Symptomology is of no help to determine severity of envenomation as it is too dynamic and constantly evolving.
• Russells Viper injects on average 63 mg ( SD 7 mg) venom in 1st bite.
• Initial dose calculated to neutralise average dose of venom injected.
• Each vial of polyvalent ASV neutralises 6 mg of Russells viper venom
Initial dose is 8-10 vials for both adults and children.
Dr.Padmesh. V
• Anti-snake venom doses and administration
• Range of venom injected is 5 mg- 147 mg.
• This would imply a maximum ASV dose of around 25 vials.
• Those envenomated with more than 60 mg will be addressed in repeat doses at the appropriate time.
• ASV should be administered over one hour.
• There is no benefit in administering each dose over longer periods.
Dr.Padmesh. V
• Adverse reactions to anti-snake venom
• Fear of potentially life threatening adverse reactions causes reluctance amongst some to treat snakebite.
• However, if handled early and with the primary drug of choice, these reactions are easily managed.
• Patients should be monitored closely as there is evidence that many anaphylactoid reactions go unnoticed.
Dr.Padmesh. V
• Adverse reactions to anti-snake venom
• At the first sign of any of the following:• Urticaria, itching, fever, shaking chills, nausea, vomiting, diarrhea,
abdominal cramps, tachycardia, hypotension, bronchospasm and angio-oedema:
• 1. ASV should be discontinued
• 2. Adrenaline should be given I.M
• Evidence shows that adrenaline reaches necessary blood plasma levels in 8 minutes via the IM route, but up to 34 minutes in the subcutaneous route.
Dr.Padmesh. V
• Adverse reactions to anti-snake venom
• In addition, to provide longer term protection against anaphylactoid reactions:
• Hydrocortisone and
• Antihistamine.
• If after 10 to 15 minutes the patient’s condition has not improved or
is worsening, REPEAT Adrenaline IM.
Dr.Padmesh. V
Once the patient has recovered
ASV can be restarted
Given slowly for 10-15 minutes (under close monitoring)
Then the normal drip rate should be resumed
• ASV test doses have been abandoned:• Have no predictive value in anaphylactoid or late serum reactions.• May pre-sensitise the patient to the protein.
Dr.Padmesh. V• Repeat doses of ASV:• In anti-hemostatic bites:
• Once initial dose has been administered over one hour, no further ASV is given for 6 hours.
• Twenty WBCT test every 6 hours will determine if additional ASV is required.
• This reflects the period the liver requires to restore clotting factors.
Dr.Padmesh. V• Repeat doses of ASV:• In Neurotoxic bites:
• Once the first dose has been administered, and a Neostigmine test given, the victim is closely monitored.
• If after 1-2 hours the victim has not improved or has worsened then a second and final dose should be given.
• At this point the victim will have received sufficient neutralising capacity from the ASV, and will either recover or require mechanical ventilation;
• In either event further ASV will achieve nothing.
Dr.Padmesh. V• PROGNOSIS.
• Despite the potential for mortality and severe morbidity with poisonous snakebites, both can be minimized by early and judicious use of appropriate antivenin.
• Even extremities with marked tissue necrosis from rattlesnake bites will return to full function with the resolution of swelling.
Dr.Padmesh. V
Reference:
• INDIAN PEDIATRICS, VOLUME 44 -MARCH 17, 2007.
• NELSON TEXTBOOK OF PEDIATRICS

Dr.Padmesh. V
Thank you!