Embed Size (px)
Citation preview


Sahar yusuf Alkadi
Prepared by:

Lecture Outline• Headaches Introduction• Sensitive structures in the skull• Headache ‘red flags’Diagnosis• Patho-physiology• Etiology• Classification of headaches
•History : Profile of HA• Home care for headaches • Material to read later-Case StudyMaterial to read later-Case Study


Definition:
Pain or discomfort from the level of the brows to the suboccipital region


WhyWhy????

Sensitive structures in the skull
1. All the tissue covering the bone except the hair2. Cerebral arteries3. Venous sinuses4. Cranial nerves: 5,9,10 & upper 3 cervical nerves5. Meninges: especially the basal
N.B: the Brain itself is insensitive

Origins of Pain in the HeadExtra-cranial pain sensitive structures:
Intra-cranial pain sensitive structures:
SinusesEyes/orbitsEarsTeethTMJ Blood vessels
ArteriesVeinsMeningesDura

Headache ‘red flags’New onset headache in middle age or
later ;and progressive headache, especially in middle-age >50 (giant cell arteritis)
New or progressive headache that lasts for days
Headache with neurologic symptomsSystemic symptoms (neck stiffness, fever,
nausea, Vomiting, weight loss ,blurry or double vision ) or Secondary risk factors (HIV, systemic cancer)



Nerve involved :
- Trigeminal nerve- First 3 cervical nerve- Facial nerve- Glosso-pharyngeal & vagus nerve

Etiology
1) Vascular headache : (V.D.)MigraineHypertension & Hypoxia & HypoglycemiaArteritis & AneurysmToxic: Caffeine withdrawal & Alcohol renal and hepatic failure2) Traction Headache: (Space occupying lesion )due to stretch of Meninges as in brain tumors

3) Tension Headache: (Psychogenic headache )Cap-like constriction (Ache pain)Not localized & Not throbbing & Don’t increase with StrainingUsually associated with depression, neurosis & stress4) Meningeal irritation:MeningitisSubarachnoid hemorrhage5) Muscle contraction headache:Prolonged contraction of the muscles of the head and neck e.g: prolonged driving

6) Neuritis and neuralgia:Of the sensory nerves of the scalp e.g.: trigeminal neuralgia7) Referred headache: may be very severEye: iritis, glaucomaEar: middle ear diseasesNasal sinuses diseasesTeeth diseases and Tongue diseases

Classification of headachesPrimary headachesOR Idiopathic headaches
THE HEADACHE IS ITSELF THE DISEASE
NO ORGANIC LESION IN THE BEACKGROUND
TREAT THE HEADACHE!
Secondary headachesOR Symptomatic headaches
THE HEADACHE IS ONLY A SYMPTOM OF AN OTHER UNDERLYING DISEASE
TREAT THE UNDERLYING DISEASE!
The differentiation between 1 and 2 is critical as it dictates diagostic approach and guides treatment and prognosis.

*Migraine
*Thunderclap headache (TCH)-sudden onset
Exertional headache
Cough headache*Tension type of
headache*Cluster headache
Other, rare types of primary headaches
*Sexual headache (Coital Cephalgia)
deBruijn, SF, et al. Lancet. 1996; Lancet. 1998.

Episodic headache disorder characterised by combinations of changes:Neurological, Gastrointestinal, Autonomic
Definition A neurologic disorder characterised by idiopathic,
paroxysmal, recurrent attacks of headache lasting from 2-72 hours
Typical characteristics: Unilateral (sometimes bilateral) pulsating qualitymod or severe intensitymay be accompanied by either nausea & vomiting or
photophobia & phonophobiaaggravated by physical activitymay be preceded by an aura
Definition of Migraine headache


.The Most common type of 1ry headache, TTH accounts for nearly 90% of all headaches. Approximately 3% of the population has chronic tension-type headaches .
.lasting 30 min to 7 days.
.The pain not only occurs in the head and neck, but also radiates around the face and scalp muscles.
.This is a type of muscle contraction pain.
.It is more in females than males.

- The exact cause of tension headache is unknown.
- it’s thought to occur due to stress, tension, depression, bad posture, staying in one position for long time, or caffeine.

. Adult or tightness pain around the head , band like. Pain radiates down to the neck.. The pain is bilateral, vary in intensity.. Not associated with aura, nausea, vomiting, or light or sound sensitivity..sever in early part of the day and less as day goes..continue for weeks or months without interruption



..Tension headache is usually treated with the help of over-the counter medications(pain-killers) as: aspirin ,acetaminophen or naproxen .
..If these fail , other supportive ttt are available as: massage & stress management.
..If recurrent headache , should seek for medical help.

Prophylactic treatment of the chronic tension type of headache
Tricyclic antidepressantsGuidelines:
Start with low dose (10-25 mg) and increase the dose if no beneficial effect after 1-2 weeks
Maximal dose should not be more than 75 mg/day Change to other tricyclic antidepressant only after 6-8
weeks Ask the patient to use headache diary Use the tricyclic antidepressant for 6-9 months Decrease the dose gradually

Prophylactic treatment of the chronic tension type of headache
First choice of drug: Amitryptiline or Mirtazapine1st week: 25 mg in the evening2nd week: 50 mg in the evening3rd week: 75 mg in the evening continuouslyChange to other drug (e.g. clomipramine) if no
beneficial effect within 6 weeks

is one of the most painful types of headache..- Is avascular headache that causes extreme pain.- Occur for several days or weeks at the same time of the day.- It’s more common in men, especially smokers.- It begins in adolescence but can extend to middle age.- There are 2 types of cluster headache:
. Episodic
. Chronic

Causes of cluster headache:. the cause of cluster headache is unknown..it’s brought to occur due to:1- dilation of blood vessels.2- inflammation of the nerves present behind eyes.3- bright sunlight, smoking, drinking alcohol and some foods as: chocolate or foods high in nitrites like smoked meats may trigger cluster headache. 4- tend to run in families& this suggest that there may be areole for genetics.5- may be due to changes in sleep patterns.6- may be triggered by medication as: nitroglycerin which used for heart disease.

Symptoms of cluster headache:1- sever unilateral per orbital pain accompanied by: unilateral lacrimation , nasal congestion..(dull, steady pain ,some pt. describe the pain as feeling like a hot poker in the eye, the affected eye may become red, inflamed and watery ,also the nose of the affected side may become congested and runny).2- attack occur at the same time every day , lasting for 30 to 90 min , often awaken the pt. at night from a sleep.3- once or twice daily or more than twice followed by respite for months before another cluster occur — known as cluster periods .4- tend to be restless which make the pt. to pace the floor or bang their head against a wall.5- nausea and vomiting rarely occur. 6-symptoms develop in early hours of morning


- There’s no specific ttt for cluster headache.-- However ttt help in reliving the symptoms as well as help prevent more attacks.
Some of these ttt include:
1. Inhalation of high concentration oxygen: the pt. is required to wear an oxygen mask that help increase the amount of oxygen in blood , thus relaxing the blood vessels and providing pain relief.

2. Injection of triptan medication as, sumatriptan which is common migraine medication.
3. Injection of lidocaine ,local anasthetic into the nostril.
4. caffine.

Prevention of the next cluster headache include the following:
1- calcium channel blocker as verapamil.2- prednisolone.3- antidepressant medication.4- lithium.5- antiseziure medication as valproic acid..also life style changes may help to minimize the risk of cluster headache as stop smoking and alcohol.

Prophylactic treatment of the episodic form of cluster headache
Episodic form: prednisoloneTreatment:
1-5. days 40 mg6-10. days daily 30 mg 10-15. days daily 20 mg 16-20. days daily 15 mg21-25. days daily 10 mg26-30. days daily 5 mgNothingIntravenous magnesium sulfate relieves cluster headaches in about 40% of patients with low
serum ionized magnesium levels. Melatonin has also been demonstrated to bring significant improvement in approximately half of episodic patients

Prophylactic treatment of the chronic form of cluster headache
Lithium carbonate Daily 600-700 mgCan be decreased after 2 weeks remissionControl of serum level is necessary (0,4 - 0,8
mmol/l)
Methysergide (synthetic ergot alkaloid), and the anticonvulsant topiramate are alternative treatments.

Dubose Dubose et alet al (1995); Goadsby (1999); Marks and Rapoport (1997) (1995); Goadsby (1999); Marks and Rapoport (1997)
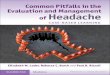
Family historyFamily history YesYes
SexSex More femalesMore females
OnsetOnset Variable Variable
LocationLocation Usually unilateralUsually unilateralin adultsin adults
Character/severityCharacter/severity PulsatilePulsatileThrobbingThrobbing
Frequency/Frequency/ 2–72 h/attack2–72 h/attack durationduration 1 attack/year to1 attack/year to
>8 per month>8 per month
AssociatedAssociated Visual auraVisual aurasymptomssymptoms PhonophobiaPhonophobia
PhotophobiaPhotophobiaPallorPallorNausea/vomitingNausea/vomiting
Clinical featureClinical feature MigraineMigraine
NoNo
More malesMore males
During sleepDuring sleep
Behind/aroundBehind/aroundone eyeone eye
Excruciating/Excruciating/sharpsharpSteadySteady
15–90 min/attack15–90 min/attack1–8 attacks/day1–8 attacks/dayfor 3–16 weeks for 3–16 weeks 1–2 bouts/year1–2 bouts/year
SweatingSweatingFacial flushingFacial flushingNasal congestionNasal congestionPtosisPtosisLacrimationLacrimationConjunctival injectionConjunctival injectionPupillary changesPupillary changes
Cluster headacheCluster headache
YesYes
More femalesMore females
Under stressUnder stress
Bilateral in bandBilateral in bandaround headaround head
DullDullPersistent Tightening/pressingPersistent Tightening/pressing
30 min to 7 days 30 min to 7 days 3–4 attacks/week3–4 attacks/weekto 1–2 attacks/yearto 1–2 attacks/year
Mild photophobiaMild photophobiaMild phonophobiaMild phonophobiaAnorexiaAnorexia
Tension headacheTension headache


refers to a severe headache of sudden onset. Its explosive and unexpected nature is likened to a "clap of thunder.”


- are headaches brought on by sexual activity. - You may notice a dull ache in your head and neck that builds up as sexual excitement increases- you may experience a sudden, severe headache just before or during orgasm.( Obviously, sex raises the blood pressure. This in turn raises the pressure in the head. Also, sex causes muscle tightening and tension.) Sex headaches are a combination of the blood pressure and muscle tension, for most people.



Trigeminal neuralgiaLancinating pain in 2nd ,3rd division of trigeminal nerve
Usually in pt. over the 50 yrs.

Clinical featuresSever, very brief but repetitive
Precipitated by touching trigger zones within the trigeminal territory by cold wind blowing on the face or by eating

Management1-Carbamazepine more than 1200mg/daily
2-Gabapentin or pregabalin

Hypnic headaches
Tend to occur in the elderly, women>men. Occur particularly at night, waking patient during REM stages of sleep. Characterized by throbbing, without autonomic features, may last upto 1 hr and reoccur through the night.




Cluster headache Short, excruciating (15 min-3 hrs) Usually occur in the middle of the night unilateral pain behind eye occur daily for 2-3mths then remit for months-years Red, watering eyes, blocked nose
Tension headache diffuse pain in tight head-band pattern bilateral, non-pulsating no prodrome/aura No nausea and vomiting 10 attacks lasting 30 min–7 days 2 of the following 4 Bilateral Not pulsating Mild or moderate intensity Not aggravated by routine physical activity No nausea or vomiting One or neither photophobia or phonophobia Not attributable to another disorder
Sinus headache Evidence of purulent discharge from the nose constant dull ache in cheek area accompanied by sinusitis worsens with bending over or blowing nose
Differential diagnosis of primary headaches


SECONDARY – (structural or metabolic abnormality):• Extra-cranial: sinusitis, otitis
media, glaucoma, TMJ ds• Intra-cranial: SAH, vasculitis,
dissection, central vein thrombosis, tumor, abscess, meningitis
• Metabolic disorders: CO2 retention, CO poisoing

History : Profile of HAtime from onset to peakusual time of onset
(week , month, season, hour of day)
frequency & durationchange over lifetimedescription : pulsating,
pressing, sharplocation : unilateral or
bilateral or changing
severity precipitating factors Aggravating factorsfactors that relieve the
headacheeffectiveness of
pharmacological or non-pharmacological treatments
Aura

Giant cell arteritis syn Arteriitis temporalis syn temporal arteritis • Giant cell arteritis (GCA or temporal arteritis) is an
autoimmune disease, granulomatose inflammation of branches of External Carotid Artery that supply the head eyes, and optic nerves . It is a form of vasculitis.
• The name (giant cell arteritis) reflects the type of inflammatory cell that is involved (as seen on biopsy).
• The terms "giant cell arteritis" and "temporal arteritis" are sometimes used interchangeably, because of the frequent involvement of the temporal artery.

Epidemiology:
It is more common in females than males by a ratio of 3:1. The mean age of onset is about 70 years, and it is rare in those less than 50 years of age. The incidence is 24.2 per 100,000 women over 50 and 8.2 per 100,000 men over 50

Clinical Presentation:•Unilateral headache, pulsating pain more sever at night•Fever •Tenderness and sensitivity on the scalp •Jaw claudication (pain in jaw when chewing) inflammation of internal maxillary artery•Tongue claudication (pain in tongue when chewing) and necrosis•Reduced visual acuity (blurred vision) •Acute visual loss (sudden blindness) •Diplopia (double vision) •Acute tinnitus (ringing in the ears) •Approximately 50% of GCA patients also have polymyalgia rhematica (PMR), which is characterized by muscle pain and stiffness.•The inflammation may affect blood supply to the eye and blurred vision or sudden blindness may occur. In 76% of cases involving the eye, the ophthalmic artery is involved causing anterior ischemic optic neuropathy. Loss of vision in both eyes may occur very abruptly and this disease is therefore a medical emergency. Amaurosis fugax may precede the blindness

TreatmentCorticosteroids, typically high-dose prednisone (40–60 mg bd), must be started as soon as the diagnosis is suspected (even before the diagnosis is confirmed by biopsy) to prevent irreversible blindness secondary to ophthalmic artery occlusion. The dose of prednisone is lowered after a 2–4 weeks, and slowly tapered over the course of 9–12 months. Oral steroids are at least as effective as iv steroids, except in the treatment of acute visual loss where iv steroids appear to offer significant benefit over oral steroids

Home care for headaches :Headaches make life difficult , those who suffer from
regular headaches ,will agree with this statement . .. When a headache strikes , one should follow some
simple home care tips that help relieve the symptoms to some extent .
These include : - First and foremost , if possible , rest , it is very important
that you leave all works aside & rest in a quiet dark room . - At times , a light sleep helps relieve the stress that
causes headaches . - You can place a light , cool cloth over the head as it
helps you relax . - Use painkiller .


Material to read later-Case Study 17 yr old femaleL-sided pulsatile headache recurring 3-4x monthlyheadache preceded by loss of visual fieldsheadache is accompanied by nausea, vomiting and
photophobiaheadache lasts all day unless able to lie in a dark room &
sleepaffects ability to work/studypast medical history unremarkable - no other medical
problemsgeneral physical & neurologic exam -normal

Thank you