Embed Size (px)
Citation preview

G I Toxicity of NSAIDs
Mohmeet Singh BrarPG resident

NSAIDs
• Analgesics• Antipyretic (fever-reducing) • Anti-inflammatory(higher doses)

CYCLOOXYGENASE PATHWAY

• PGI2 and PGE2 : vasodilator cytoprotective on GI mucosa.
• 5-lipoxygenase forms leukotrienes (LT) LTB4, a potent chemotaxin, LTC4, LTD4, LTDE4, :constriction of bronchial tissue and edema

CONSTITUTIVE AND INDUCIBLE CYCLOOXYGENASES
• Three forms• COX-1 :constitutive enzyme in most cells of the body mucosal-protective• COX-2: inducible TNFa or IL-1b, or growth factors bacterial polysaccharide

COX Contd..
• COX-3 : expressed in brain target of acetaminophen (paracetamol)

COX Contd..
• Non selective NSAIDs: block COX-1 and COX-2 impair PG production at low (<1µM) concentrations
• Selective inhibitors of COX-2,COX–3 inhibitors: less of COX1 inhibition
preserve GI mucosal protection


MECHANISMS OF GASTRODUODENAL PROTECTION BY ENDOGENOUS PGS
• Major effect: hypochlorhydria• Other cytoprotective mechanisms : Stimulation of glycoprotein (mucin) secretion by epithelial cells Stimulation of bicarbonate secretion by epithelial cells

• Stimulation of phospholipid secretion by epithelial cells
• Enhancement of mucosal blood flow and oxygen delivery to epithelial cells via local vasodilation
• Increased epithelial cell migration towards the luminal surface (restitution)
• Enhanced epithelial cell proliferation

• Injury occurs when the protective functions are compromised.
• lead to gastric and/or duodenal ulcer formation,
• ulcer complications (bleeding, perforation, and obstruction).

ROLE OF NITRIC OXIDE
• Constitutive NO synthase (NOS): maintenance of an intact mucosal lining.
• Two enzymes : neuronal NOS (nNOS, type I) endothelial NOS (eNOS, type III).
• Cytoprotective mechanisms include:

NO Contd..
Mediation of the release of gastric mucinStimulation of alkaline fluid secretionMaintenance of epithelial barrier functionEnhancement of mucosal blood flow

Topical effects of NSAIDs
• Carboxylic acid derivatives.• Not ionized at the acidic pH • Absorbed across the gastric mucosa. • In the pH–neutral mucosa, the drug ionizes
and is trapped temporarily in epithelial cells where it may damage these cells.

• Is the topical effect sufficient??
• Do I/V or I/M NSAIDs cause gastric damage??

• The topical epithelial injury: not the only factor for symptomatic ulcers
• Systemic (post-absorptive) effects: inhibition of GI mucosal cyclooxygenase (COX) activity.
• Even I/V or I/M administration of NSAIDs can cause gastric or duodenal ulcers
Clin Gastroenterol Hepatol 2008; 6:309


SPECTRUM OF GASTRODUODENAL MUCOSAL INJURY
• Alterations in gastric mucosal barrier function through microscopic damage to an ulcer complication.
• Increased mucosal permeability to hydrogen and sodium ions.

• Macroscopic injury by NSAIDs : edema, erythema, subepithelial hemorrhage, erosions (mucosal breaks, without visible depth to the lesion) ulcers (mucosal breaks, with visible depth to the lesion).

• GASTRIC DAMAGE: Aspirin doses as low as 10 mg/day inhibit gastric PG generation considerably and can damage the stomach.
• Epidemiologic and placebo-controlled studies indicate that the risk of serious, clinically-relevant GI damage increases as the aspirin dose is raised
Am J Physiol Gastrointest Liver Physiol 2000; 279:G1113.

• In contrast to aspirin, which acetylates COX irreversibly, most NSAIDs inhibit COX-1 and COX–2 reversibly
• even transient COX-1 inhibition in the gastric mucosa by an NSAID is sufficient to predispose the stomach to injury
• It is supported by the observation that NSAID-related gastric damage is prevented by PGE analogs such as misoprostol
JAMA 2000; 284:1247

• Duodenal damage — Aspirin doses as low as 325 mg every other day increase the risk of duodenal ulcers.
• In contrast to the stomach, damage to the duodenal mucosa by aspirin and NSAIDs seems to depend highly upon gastric acid
N Engl J Med 1989; 321:129

ROLE OF H. PYLORI INFECTION
• The risk of uncomplicated peptic ulcer disease was significantly higher among H. pylori positive
• Ulcers were common in H. pylori positive compared with H. pylori negative patients irrespective of NSAID use
Clin Gastroenterol Hepatol 2006; 4:130

RISK OF GASTROINTESTINAL COMPLICATIONS
• A number of factors are associated with an increased risk of gastroduodenal toxicity and complications from NSAIDs
• An important determinant is the DURATION OF THERAPY.
• The administration of NSAIDs for a short period of time (less than one week) is unlikely to result in any significant gastroduodenal toxicity.

• Longer duration : increased risk of developing complications
• Most common within the first three months after the initiation of therapy
• Other factors include increasing age, higher NSAID dose a past history of gastroduodenal toxicity from NSAIDs

• past history of PUD• Concurrent use of corticosteroids SSRI clopidogrel bisphosphonates
Circulation 2011; 123:1108

Patients at increased risk


Bleeding duodenal ulcer

Treatment of gastroduodenal toxicity
• STOP NSAID• Ulcer therapy with a PPI or an H2 antagonist• PPIs preferred :: more rapid ulcer healing ( Acid
Suppression Trial: Ranitidine versus Omeprazole for NSAID-associated Ulcer Treatment (ASTRONAUT) Study Group. N Engl J Med 1998; 338:719. )
• Patient's H. pylori status should also be assessed (if not done previously)
• If positive, appropriate therapy for H. pylori should be instituted

Treatment contd..
• For patients who must remain on low-dose aspirin or NSAID therapy, randomized trials have shown that ulcer healing occurs more rapidly with a proton pump inhibitor than an H2 antagonist, misoprostol or sucralfate.

Treatment contd..
• Treatment continued for four (duodenal ulcer) to eight weeks( gastric ulcer),
• Endoscopic follow-up to assess ulcer healing is usually unnecessary for duodenal ulcers,
• performed to assess healing of gastric ulcers if malignancy had not been excluded at the initial endoscopy.

• MISOPROSTOL: prostaglandin analogue• Efficacy similar to PPIs (Arch Int Med 2002;162)• 200 mg Qid• Limited by adverse effects- diarrhea,
cramping, poor compliance

Secondary prevention of NSAIDs induced ulcers
• For patients who must continue (NSAID) or aspirin therapy, treatment with a PPI for as long as the NSAID or aspirin is used.
• H. pylori infection must be eradicated, if known to be present

COXIBS
• In patients with high risk for peptic ulcer disease: combine a selective COX-2 inhibitor with a PPI
• Associated with low risk as compared to non selective NSAIDs
• Less beneficial in patients also taking low dose aspirin

COXIBS contd..
• Downsize: increased incidence of MI and other thrombotic events
• Higher incidence of CV risk- non inhibition of thromboxanes.
• Rofecoxib(2004) and valdecoxib(2005) withdrawn by FDA

COXIBS Contd..
• CLASS trial: no difference with celecoxib (JAMA 2000;284)
• APC trial: high incidence with celecoxib Can be reduced by lowering the dose to 200 mg BD (N Engl J Med 2005;352)

COXIBS Contd..
• TARGET study: same incidence with Lumiracoxib and ibuprofen but less then naproxen (Ann Rheum Dis 2007;66)
• Celecoxib is currently approved by the Food and Drug Administration (FDA). Parecoxib, etoricoxib, are also available.

Recommendations for prevention of NSAIDs related ulcers
GI RISK LOW MODERATE HIGH
Low Risk NSAIDs alone
NSAIDs +PPI/ Misoprostol
Alternative RxCOX 2 inhibitor +PPI/ Misoprostol
High Risk Naproxen +PPI/ Misoprostol
Naproxen +PPI/ Misoprostol
Avoid NSAIDs or COX 2 Inhibitors.

Adverse effects on the distal small bowel and colon
• The distal small bowel and colon are susceptible to the deleterious effects of NSAIDs.
• ILEOCECAL REGION: most common site• Include erosions, ulcers, strictures, perforation,

formation of diaphragms, bowel obstruction exacerbate preexisting IBD, bleeding

PATHOGENESIS
• The attempts to decrease gastro duodenal side effects by
the use of enteric-coated, sustained-release, or slow-release(NSAIDs)• Shifted the damage to the distal small
intestine and colon.

PATHOGENESIS Contd..
High local concentration following ingestion
biliary excretion
Increased intestinal permeability

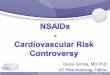
• Intestinal diaphragms : pathognomic of NSAID injury
• Scarring reaction to ulcerative injury. • Thin, multiple, concentric, diaphragm-like
septa with pinhole-sized lumen • Mid-intestine, ileum and colon
Colorectal Dis 2012; 14:804

Intraoperative enteroscopy of a patient with capsule retention showed multiple ring-like NSAID-induced strictures (diaphragm disease).

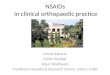
A small-bowel resection specimen from a patient with CE retention from NSAID-induced diaphragm-like strictures. Four diaphragms are present. Indicated by the asterisks

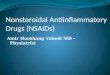
CE of a retained capsule shows NSAID enteropathy (diaphragm disease)–associated ulcer and stricture.

• MANAGEMENT — Discontinuation of the NSAID.
• Nonstrictured ileocecal lesions: prompt improvement.
• Repeat colonoscopy six to eight weeks later should confirm partial or complete resolution of ulcerations and/or colitis

• Endoscopically accessible strictures or diaphragms :through-the-scope (TTS) balloon dilatation
• Diaphragm-like strictures : resection of the involved segment strictureplasty

• Surgery : significant bleeding perforation carcinoma is suspected

HEPATIC INJURY
• Elevations of serum aminotransferases (transaminases) are common.
• The net hepatic risk was seen in 625,000 patients who received more than 2 million prescriptions for NSAIDs and who were evaluated for newly diagnosed acute liver injury

• The study revealed The incidence of acute liver injury was 3.7 per 100,000 NSAID users or 1.1 per 100,000 NSAID prescriptions; None of the cases had a fatal outcome
Arch Intern Med 1994; 154:311

Sulindac : greatest risk • Incidence 27 per 100,000 prescriptions• Mild and reversible• women >> men • more prevalent over the age of 50.• Idiosyncratic hypersensitivity reactions.• Increased by use of another hepatotoxic drug
simultaneously

• Diclofenac :clinical hepatitis, including ANA positivity
histologic evidence of chronic active hepatitis.• Liver function abnormalities due to NSAIDs
may be disease-specific like SLE

The principal determinants of AST concentrations were • baseline AST value, • duration of therapy• daily dose

• Laboratory testing — serum transaminase levels should be monitored
transaminases >> three times normal ↓in serum albumin ↑(INR), • NSAID toxicity should be suspected offending
agent should be discontinued.

Conclusions

• Use NSAIDs judiciously• Minimum days possible• PPIs to be given alongside whenever long term
NSAIDs have to be given• Early intervention decreases the mortality• COX 2 inhibitors don’t provide any extra
benefit

Thanks..!!!



















![[Sent] NSAIDs for UPN](https://img.pdfslide.us/doc/110x75/5695d1ba1a28ab9b0297b3cd/sent-nsaids-for-upn.jpg)






