Embed Size (px)
Citation preview

Forensic medicine

Timing of rigor mortis
Firstly in small muscle groups
(around the eyes and mouth, the jaw and the fingers)
From Head to the legs
In the face 1-4 hs
In the limbs 3-6 hs after death
strength of rigor increasing to a maximum by approximately 18 hours after death
Will remain for up to approximately 50 hours after death

Hypostasis
Aka : livor mortis / postmortem lividity / suggillation
settling of the blood in the lower (dependent) portion
of the body, causing a purplish red discoloration of
the skin
Appear 20m-3h after death
Maximum lividity occurs within 6–12 hours

Hypostasis
The color of hypostasis is variable and may extend from:
pink to dark pink to deep purple
in some congestive hypoxic states, to blue.
in pressure areas such as the shoulder blades, buttock & calvesdiscoloration will be pale.
Some indicators : Cherry-pink: CO poisoning
Dark red: cyanide poisoning
Bronze: Clostridium perfringes infection.

Hypostasis
Hypostasis is not always seen
it may be absent in :
the young, the old
anemic
death from severe blood
loss.
It may be masked :
by dark skin colors
by jaundice
by some dermatological
conditions.

Sites of hypostasis
Depends on the position of the body before death: Supine:
shoulders, buttocks
heels pressing against surface give white color (pale).
Vertical (hanging): distally in legs & feet.
Drowning: غرق chest, upper chest, and upper limbs.
Face-down death: as in epilepsy, drunken victims
whitening around nose & lips.
Hypostasis may also occur in viscera: Heart: mistaken for MI
Lungs: mistaken for pneumonia
Intestine: mistaken for hemorrhagic infarction
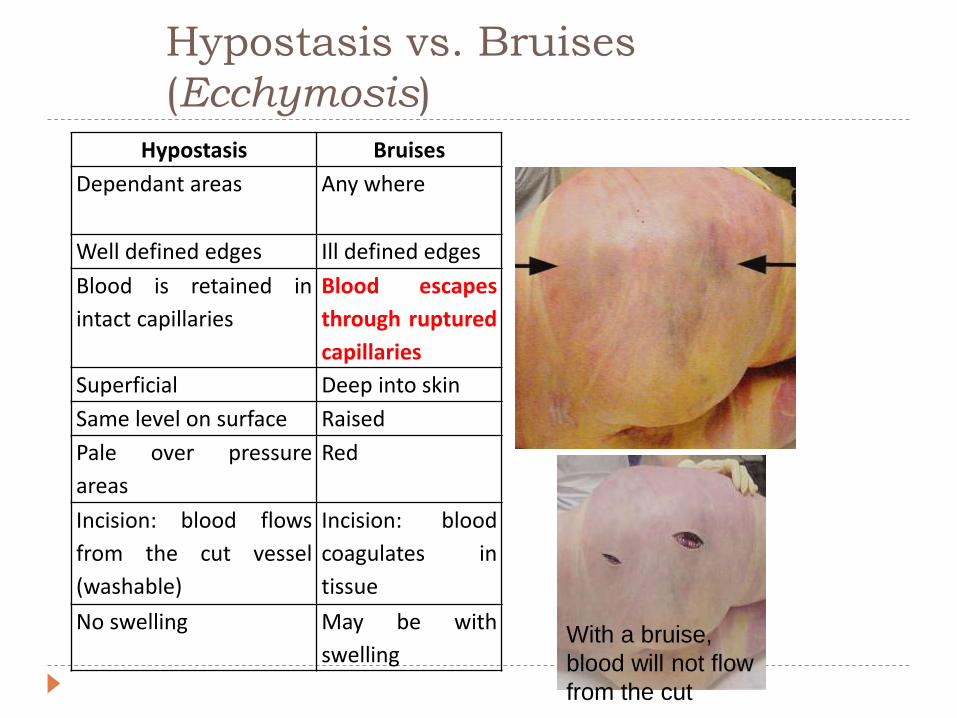
Hypostasis vs. Bruises
(Ecchymosis)
Hypostasis Bruises
Dependant areas Any where
Well defined edges Ill defined edges
Blood is retained in
intact capillaries
Blood escapes
through ruptured
capillaries
Superficial Deep into skin
Same level on surface Raised
Pale over pressure
areas
Red
Incision: blood flows
from the cut vessel
(washable)
Incision: blood
coagulates in
tissue
No swelling May be with
swellingWith a bruise,
blood will not flow
from the cut


1.Putrefaction
Start immediately after death at the
cellular level
Become visible by naked eye at
about 3-4 days
Its onset depend on several factors
mainly: temperature and humidity
Two phenomena for putrefaction:
1.autolysis:by digestive enzymes
that released from the
cells
2.bacterial action: most of them
come from the bowel and
clostridium welchii predominates
Start as an area of green discoloration
of the Rt iliac fossa of the ant.
Abdominal wall
The gut bacteria find their way out the
bowel lumen to the abdominal cavity
and the blood vessels
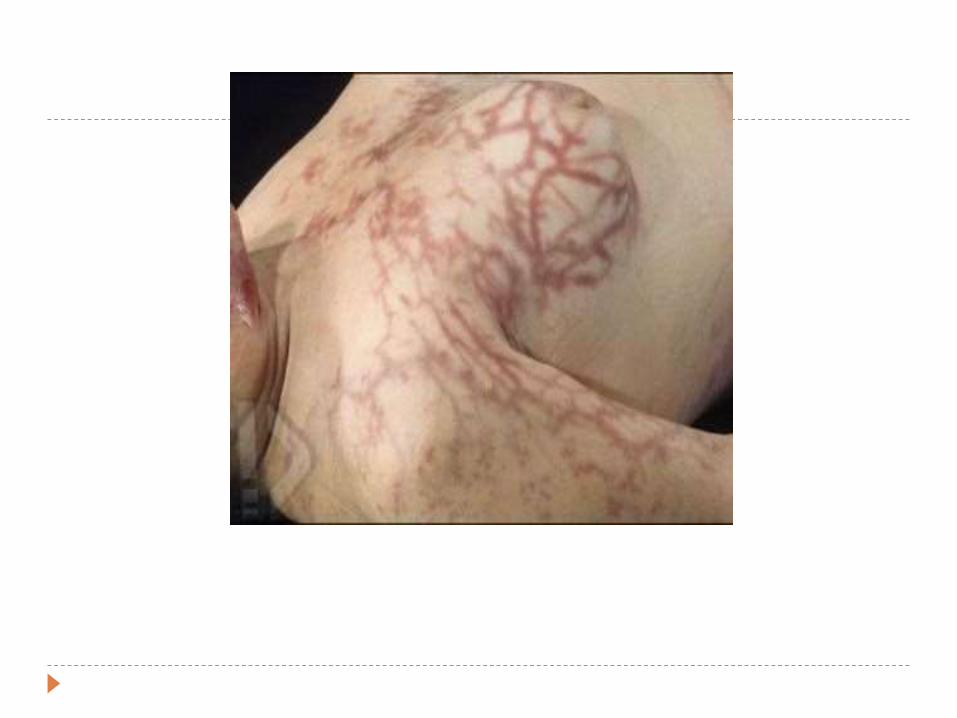
As the bacteria spread through the
blood vessels they decompose
hemoglobin
When present in the superficial vessels
results in linear branching patterns of
variable discoloration of the skin called
“marbling”.
Prostate and uterus are relatively
resistant to putrefaction

Estimating the time of death1.Body temperature :
the best and the most commonly
used
Rectally using long, low-reading
thermometer
2.Rigor mortis
3.Hypostasis:
complete after 6 hrs
4.Biochemical investigation of the CSF:
requires the determination of the
amino acid content & lactic
acid & non-protein nitrogen
content of the CSF.
5.Eye pressure:
eye balls become softer, and less
fluid pressure in the first 3 hrs
6.Gastric emptying:
depend on type of meal and
emotional status.
7.The entomology of dead:
Studying insects & their maggots
which infest the dead body for
estimating the probable time of death.
Different types of insects infest the
dead body at different stages after
death occurs.

Disease of the heart :
Δ Coronary artery disease1-Coronary atherosclerosis:
-The most common cause of sudden death .
-Mostly affects :
* Left Anterior Descending Artery (LADA)
*Right Coronary Artery (RCA)
*Left Common Carotid Artery (LCCA)

Complications of coronary Atherosclerosis :
1-rupture of ulcer atheromatous plaque .
2-sub-intimal hemorrhage .
3-Thrombosis most common
4-aneurysm
5-Ischemia
6-Infarction
7-Peripheral Vascular Diseases

Δ Coronary artery disease ,Cont:
2- Myocardial Infarction :
- Myocardial infarction occurs when there is severe stenosis - 75%
or more of the lumen of a major branch - or complete occlusion
of a coronary artery . but death can be attributed to coronary
artery disease (CAD) with less stenosis if other signs of chronic
myocardial ischemia are apparent (left ventricular
hypertrophy [LVH], fibrosis, previous infarct).

Complications of MI :
1-Rupture of myocardial infarct :
The area of the myocardial infarct is weakest between 3 days
and 1 week after the clinical onset of the infarct and it is
at this time that the weakened area of myocardium may
rupture, leading to sudden death from :
*haemopericardium
*cardiac tamponade

2-Cardiac Aneurysm :
- One week post MI .
- may form at sites of infarction; they may calcify
and they may rupture.

Δ Cardiomyopathies :
HCM (hypertrophic cardiomyopathy):
-inherited (AD)or sporadic
-leading cause of sudden cardiac death in young athletes
-decreased compliance and death due to diastolic dysfunction.
-sudden death may be the first manifistation. RCM (restrictive cardiomyopathy ):
-causes . -enlarged atria and small thin ventricles . –death also due to diastoloic dysfunction
Functional abnormalities
Pathologically, there are no ‘naked eye’ or microscopic
abnormalities in the heart as the defects are at a
molecular level.
Long QT syndrome (LQTS).
short QT syndrome (SQTS).
Brugada syndrome ( It is the major cause of
sudden unexplained syndrom (SUDS) in young men)

Dissecting aortic aneurysm
(90% occur in the ascending aorta either just distal to the aortic valve or the left subclavian artery) Dissecting aneurysms are principally found in individuals with hypertension, but may also be seen in younger individuals with connective tissue defects, such as Marfan syndrome

Rupture of berry aneurysm
Any rise in the blood pressure will cause rupture of the apex
of the aneurysm/ one of the most common causes of
death inyoung to middle-aged adults, if coronary
disease is excluded.

Asthmatic patients
Pulmonary embolism
massive hemopt
ysis
Pneumonia
Respiratory causes :
1-Asthmatic patients : may die suddenly and unexpectedly, without necessarily being in status asthmaticus or even in an acute asthmatic attack.
May be due to Hypoxia and respiratory acidosis. autopsy little or nothing is found, except confirmation of the chronic asthmatic state.2-Pulmonary embolism (most common cause of death in pregnancy) :
In almost every case, the source of the emboli is in the leg veins and pelvic veins. After any tissue trauma, or even surgical operation, especially where immobility or bed rest occurs, deep vein thrombosis develops.3-massive hemoptysis from cavitating pulmonary tuberculosis or from a malignant tumor4-pneumonia
Fatal abdominal
catastrophes
Esophageal varices
Perforation of a peptic
ulcer
GI
Causes
Mesenteric
thrombosis and
infarction ,
Strangulated
intestine
: It is often difficult to identify
the varices at autopsy, as they have
collapsed

Genitourinary system
If a woman in child-bearing age is found unexpectedly death,
complications of pregnancy must be considered like :
Induced abortions
Amniotic fluid emblosim
Ruptured Uterus
ruptured ectopic gestation.

Autopsy-negative causes of
death
Every cause of death we’ve mentioned so far will have
A positive finding manifested during autopsy , now what if
there were NO PSTIVE FINDINGS ?
Then we will probably be left with what we call
Endocrinopathies ( DKA , thyrotoxicosis ..).
Electrolyte abnormalities.
Other:malignant syndrome,Cardiac
dysrhythmia,anaphylaxis
Autopsy-negative causes of death

A-External examination
Signs of malnutrition or dehydration .
Supraclavicular congestion in sudden cardiac
death.
fingernail clubbing in chronic heart disease.
Splinter hemorrhage in infective endocarditis.
Signs of trauma, such as manual strangulation or
low-voltage electrocution.

B-General internal examination
Organs should be examined in situ before manipulation
fluid within any body cavity should be measured (volume) and described (serous, serosanguineous, purulent, chylous, frank blood)
The lungs should be examined for evidence of hyperinflation (asthma, emphysema aquosum)
Evisceration should be performed, or directly observed, by the pathologist
Evaluations for tension pneumothorax should be done before the thoracic cavity is entered
Internal examination of body systems most often implicated in sudden death ( CVS , RS ,CNS , GIS)

Sudden infant death syndrome(SIDS)
Crib death, syndrome in which healthy infants(1 month to a year) die from unknown causes (usually during sleep).
Most deaths due to SIDS occur between 2 and 4 months of age, and incidence increases during cold weather.
More boys than girls fall victim to SIDS..

What are the risk factors for SIDS ?
Smoking, drinking, or drug use during pregnancy.
Poor prenatal care.
Poor prenatal nutrition.
Prematurity or low birth-weight.
No breast feeding.
Mothers younger than 20.
Smoke exposure following birth.
Overheating from excessive sleepwear and bedding.
Stomach sleeping.

Lethal Dose ( LD50 ) : the dose at which 50% of which who
took the dose will die

SPECTRUM OF ALCOHOL USE / ABUSE
Social drinker - drinks occasionally (not frequent)
Heavy drinker - drinks regularly and heavily (Men >7
units/day, Women >5 units/day).
Binge drinker - drinks irregularly and heavily.

Alcohol Absorption
*completed 1-3 hrs
20 % Stomach
80% Upper Small
Intestine

Increase Absorption
• Empty Stomach
• Gasterectomy
• 10 – 20% concentration is the optimum
Decrease Absorption
• Food in Stomach
• Higher Concentration of Alcohol

Physical clues are blood-shot eyes, dilated pupils,
rapid bounding pulse, physical inco-ordination and
nystagmus (jerking eye movements) on lateral gaze

More about alcohol effect
Skin =vasodilation and hypothermia
Respiratory=aspiration pnemonia
Blood=anemia and leukopenia
GIT=liver cirrhosis, pancreatitis, gastritis, peptic Ulcer, portal varices
Reproductive:
=Irregular period ,breast & genital atrophy
=loss of libido ,decrease sperm count, testicular atrophy
Pregnancy=spontaneous abortion ,fetal alcoholic syndrome ,delayed mental and motor development in child lactating from alcoholic mom,

CAUSES OF DEATH IN CHRONIC ALCOHOLICS
1. Trauma. The largest group (26%).
Fire deaths were the most common. Drunken falls were frequently followed by fatal head injury. Murder, Road traffic accidents (pedestrians),Drowning, Accidental poisonings.
2. Incidental Natural Disease (25%). Ischemic heart disease, cerebral hemorrhage, chronic obstructive airways disease and malignancy.
3. Alcohol Related Disease (22%). Bronchopneumonia and lobar pneumonia are the commonest. Cirrhosis of the liver due to ruptured varices or hepatic failure. Many of these deaths occur in hospital and are excluded from forensic practice. Alcoholic cardiomyopathy and pancreatitis are other rarely reported causes of death.
4. Acute Intoxication (24%).
Possible mechanisms of death from simple intoxication:
1. Simple depression of the respiratory centre in lower brain stem by alcohol itself.
2. Inhalation of vomit due to coma.
3. Postural asphyxia (obstruction of the upper airway by the swallowed tongue during coma.
5.'Obscure' cause of Death is noted in a variable proportion of cases, up to 10%.
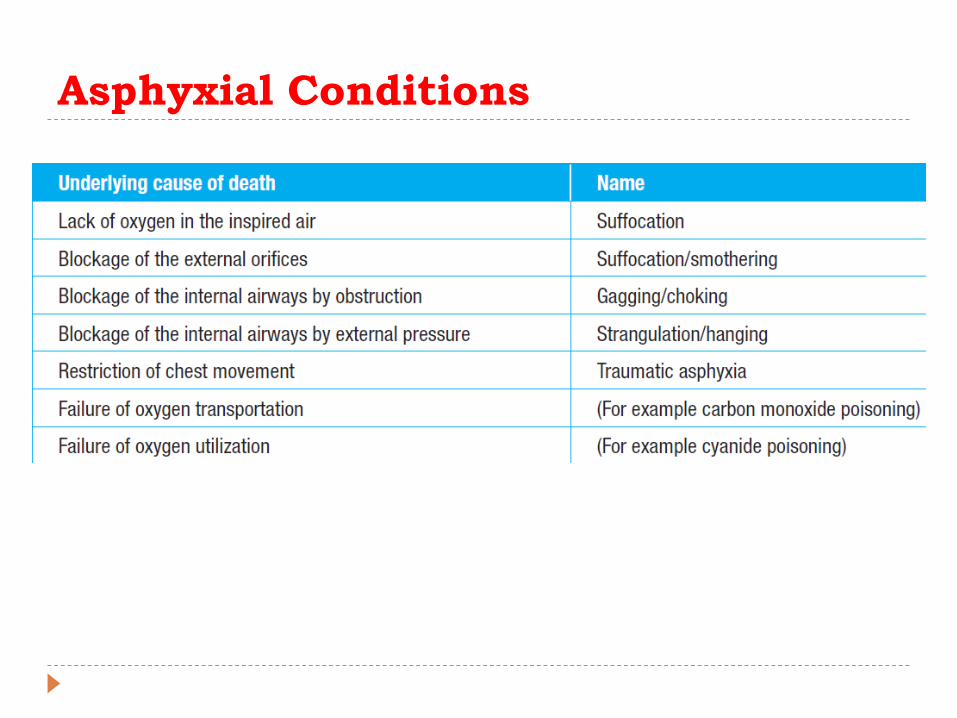
Asphyxial Conditions

Phases of Asphyxia
1- Forced respiration: Due to Stimulation of respiratory center
Clinical Picture: Dyspnea.
2- Stage of convulsions:
It is due to cerebral irritation
Clinical Picture: Convulsions, cyanosis, Hypertension, loss of consciousness, constricted pupil.
• 3- Paralysis: Clinical Picture:loss of consciousness, flaccid muscles & lost reflexes, deep cyanosis, dilated pupils, irregular breathing.
Death occur after 5 minutes

Classical Signs of Asphyxia
Petechial hemorrhages in the skin of the face and in
the lining of the eyelids.
In the viscera, they are called Tardieu spots.
Congestion & edema of the face.
Cyanosis (blue discoloration) of the skin of the face.
Right heart congestion and abnormal fluidity of the blood.


Petechial Hemorrhages

Tardieu Spots

Survivors of Asphyxial Episodes suffer
from:
Pain and tenderness around the neck.
Damage to the larynx and hyoid bone.
Dried saliva around the mouth.
Cyanosis, congestion, edema and petechiae of the
structures above the level of compression.
Hemorrhage from the mouth, nose and ears.
Incontinence of feces and urine.

Strangulation
Manual Strangulation
Throttling.
The application of
pressure to the neck
using the hands.
Seen usually in
Homicides.
Bruises and abrasions
in the front of the neck
and lower jaw.
Ligature strangulation
May be homicidal, suicidal or accidental.
Involves the application of pressure to the neck by an item capable of constricting the neck, such as a scarf, neck-tie, stocking or telephone cable…etc.
Ligature mark.

Hanging
Suspension of the body by the neck.
Ligature mark (V shaped) with discontinuity at
suspension point.
discontinuity at suspension point

Compressional and Positional
Asphyxia
Pressure on the trunk (chest and/or abdomen) can result in an inability to breathe effectively and result in death.
Traumatic, and crush asphyxia.
Persons with impaired neurological function are more susceptible.

Smothering
The physical occlusion of the nose and mouth resulting inasphyxia.
May leave no ‘asphyxial signs’ in survivors or thedeceased.
If the individuals are unable to struggle, owing to extremesof age or intoxication, for example, they may have noevidence of injury, including around the mouth or nose.
Occasionally, examination will reveal intraoral injury(including bruising or laceration of the insides of the lips orbruising of the gums in an edentulous individual) and softtissue dissection of the face may reveal subcutaneousbruising around the mouth and nose.
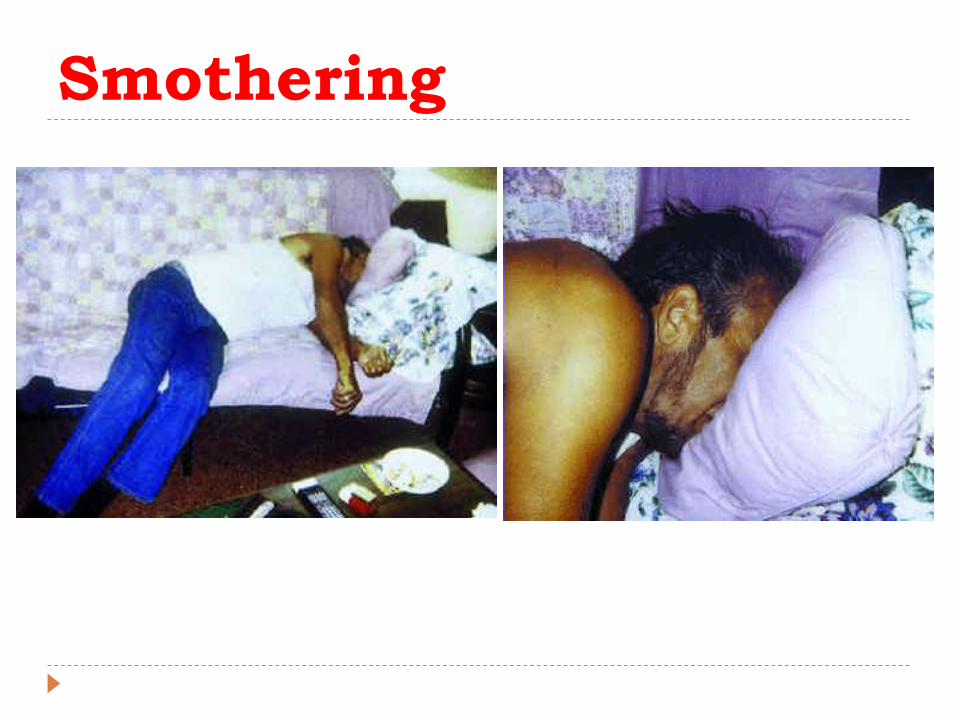
Smothering

Autoerotic Asphyxia Autoerotic asphyxia is the term used to describe
those fatalities occurring during some form of
solitary sexual activity.
Sexual asphyxia, sex hanging, asphyxiophilia,
Kotzwarrism, autoasphyxiophilia and
hypoxyphilia.
The recurrent feature tends to be the use of a
device, appliance or restraint that causes neck
compression, leading to cerebral hypoxia, with the aim of heightening the sexual response.





























