Embed Size (px)
Citation preview
Foot and Mouth Disease: An Indian Perspective
म ुँह-पका ख र-पका रोगFMD, Aftosa, Hoof & Mouth
Disease
Dr. Bhoj R SinghPrincipal Scientist & Head Division of Epidemiology
Indian Veterinary Research Institute, Izatnagar-243122, Bareilly, UP, India.Email; [email protected]
FMD in India
FMD is an economically important disease of cloven-footed animals. It causes an estimated loss of Rs. 20-22thousand crores per year to livestock owners in India.To control the disease, DAHDF of India launched aNational FMD Control Program (FMD-CP) in 2003 withan outlay of about Rs. 500 crores a year by CentralGovernment and each state government also investedan equally good amount of money. The program isongoing all over India. However, results are humiliatingand harassing. We are almost at the same spot fromwhere we started 15 years back in 2003.
Etiology
• FMD is caused by a virus: Aphthovirus: foot-and-mouth disease virus of the family Picornaviridae.
• Signs of illness can appear after an incubation period of 1 to 8 days, but often develop within 3 days.
• The virus survives in lymph nodes and bone marrow at neutral pH, but is destroyed in muscle when pH is less than 6.0, i.e., after rigor mortis.
• The virus can persist in contaminated fodder and the environment for up to 1 month, depending on the temperature and pH conditions.
• There are seven known serotypes: A, O, C, Asia 1, and SAT (Southern African Territories) 1, 2, and 3.
• More than 60 subtypes of the FMD virus. Immunity to one type does not protect an animal against other types.
• Six of the 7 serotypes have occurred in Africa (O, A, C, SAT-1, SAT-2, SAT-3), 4 in Asia (O, A, C, Asia-1), and 3 in South America (O, A, C). North and Central America, Australia, New Zealand, Greenland, Iceland, and Western Europe are free of FMD. In 2001, FMD was introduced into the UK, where it spread to Ireland, the Netherlands, and France. The highly virulent pan-Asiatic serotype O causing the outbreak was the same found throughout Asia.
Transmission• Foot-and-mouth disease (FMD) is a highly communicable
contaagious viral disease.• FMD viruses can be spread by animals, people, or materials that
bring the virus into physical contact with susceptible animals. An outbreak can occur when: – Animals carrying the virus are introduced into susceptible herds. – Contaminated facilities are used to hold susceptible animals. – Contaminated vehicles are used to move susceptible animals. – Raw or improperly cooked garbage containing infected meat or animal
products is fed to susceptible animals.– People wearing contaminated clothes or footwear, or using
contaminated equipment, pass the virus to susceptible animals. – Susceptible animals are exposed to materials such as hay, feedstuffs,
hides, or biologics contaminated with the virus. – Susceptible animals drink common source contaminated water. – A susceptible animal is inseminated by semen from an infected
animal.– Direct contact or aerosolized virus via respiratory secretions, milk,
semen, and ingestion of feed from infected animals (meat, offal, milk).
Host Range
• It primarily affects cloven-hooved animals of the order Artiodactyla.
• Livestock hosts include cattle, pigs, sheep, goats, and experimental infections in alpacas and llamas.
• FMD virus has also been reported in >70 species of wild artiodactyls, including bison, giraffes, Indian elephants, and several species of deer and antelope.
Signs• Vesicles (blisters) followed by erosions in the mouth or on the feet and the
resulting excessive salivation or lameness are the best known signs of the disease. Often blisters may not be observed because they easily rupture, leading to erosions.
• These signs may appear in affected animals during an FMD outbreak: – Marked rise in body temperature for 2 to 3 days. – Vesicles that rupture and discharge clear or cloudy fluid, leaving raw, eroded
areas surrounded by ragged fragments of loose tissue. – Production of sticky, foamy, stringy saliva. – Reduced consumption of feed due to painful tongue and mouth lesions. – Lameness with reluctance to move. – Abortions. – Low milk production (dairy cows). – Myocarditis (inflammation of the muscular walls of the heart) and death,
especially in newborn animals. – Animals do not normally regain lost weight for many months. – Recovered cows seldom produce milk at their former rates, and conception
rates may be low.– In a susceptible population, morbidity reaches 100% with rare fatalities except
in young animals. Fatalities in young calves may be very high sometimes seen up to 50%.
– After FMD, in draught animals and buffaloes excessive panting.
Diagnosis
• In cattle and pigs, the clinical signs of FMD are indistinguishable from those of vesicularstomatitis, and in pigs from those of swine vesicular disease and swine vesicularexanthema.
• Laboratory diagnosis is usually performed via antigen capture–ELISA or serotypingELISA. This is the preferred method for endemic FMD for viral antigen detection andserotyping.
• Detecting nucleic acids via RT-PCR combined with real-time PCR is more sensitive andrapid than conventional methods and may be more useful when samples contain lowconcentrations of virus.
• ELISA is preferred over complement fixation tests because of its increased sensitivityand specificity.
• Commercially available lateral flow devices have not yet been validated by the OIE.• Serologic tests for FMD are used to certify animals for import/export (i.e., trade), to
confirm suspected cases of FMD, to test efficacy of vaccination, and to provide evidencefor absence of infection.
• Serologic tests for antibodies to the viral structural (capsid) proteins cannot be used invaccinated animals, because FMD vaccines induce antibodies to these proteins.Detection of antibodies to non-structural proteins (with NSP ELISA) which areexpressed only during virus replication, can be used to determine past or presentinfection with any of the 7 serotypes. However, NSP-ELISA are less sensitive and mayresult in false-negatives in cases with limited virus replication such as in vaccinatedanimals that become infected, because the vaccine suppresses viral replication.
Hand-Foot-Mouth syndrome & FMD
• Hand-Foot-Mouth syndrome is an infectious disease that inmost cases is caused by the Coxsackie virus A16.The disease most often occurs in young children and ischaracterized by a rash of small blister-like sores (lesions).The rash usually occurs on the palms of the hands, soles ofthe feet, and in the mouth.
• Zoonotic infections with FMD virus have been reportedmostly in livestock handlers. The virus type O, C and rarelyA has been isolated from more than 40 human cases. Thediseases in man showing vesicles in the mouth or on thehands and feet were called FMD. The first suggestion of ahuman infection with FMD was reported in 1695 byValentini in Germany. (Arch Virol Suppl. 1997;13:95-7, Foot- and-mouth disease as zoonosis).
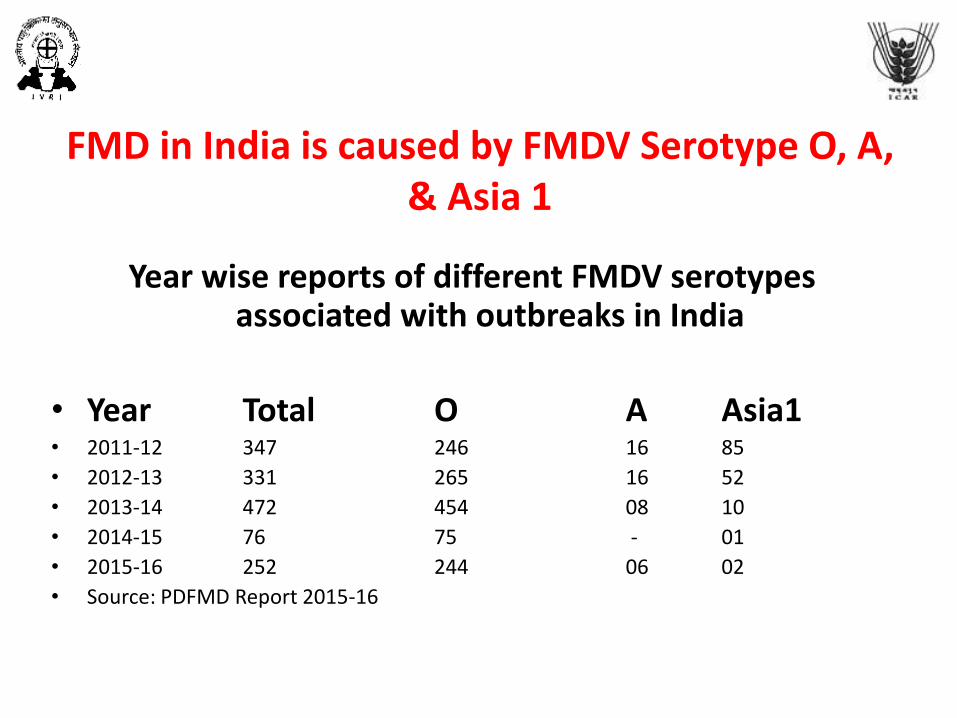
FMD in India is caused by FMDV Serotype O, A, & Asia 1
Year wise reports of different FMDV serotypes associated with outbreaks in India
• Year Total O A Asia1• 2011-12 347 246 16 85
• 2012-13 331 265 16 52
• 2013-14 472 454 08 10
• 2014-15 76 75 - 01
• 2015-16 252 244 06 02
• Source: PDFMD Report 2015-16
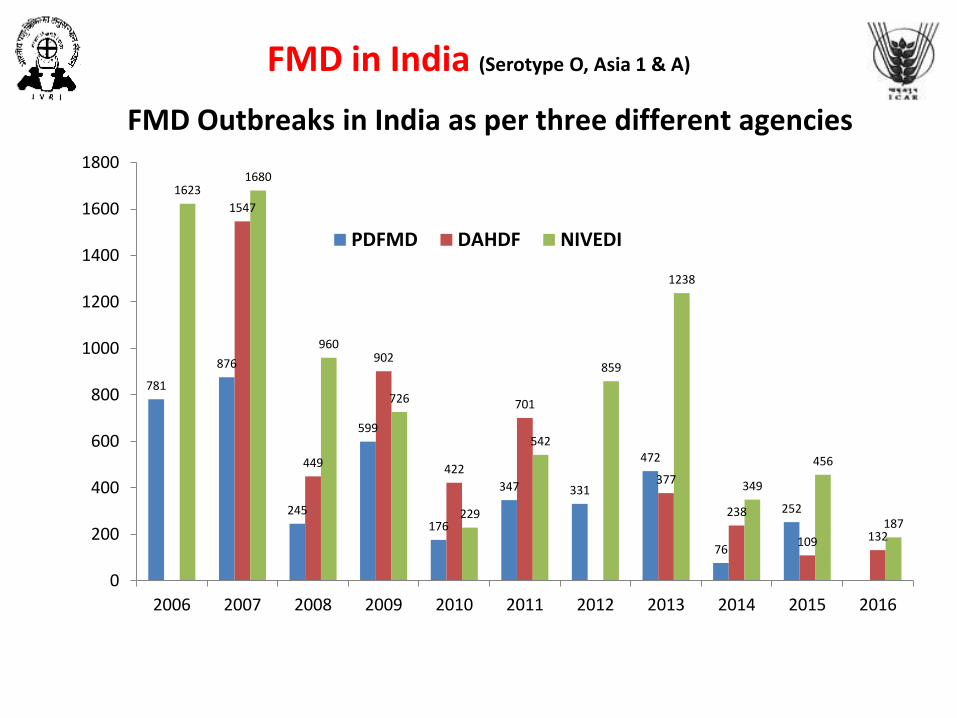
FMD in India (Serotype O, Asia 1 & A)
781
876
245
599
176
347 331
472
76
252
1547
449
902
422
701
377
238
109 132
16231680
960
726
229
542
859
1238
349
456
187
0
200
400
600
800
1000
1200
1400
1600
1800
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
PDFMD DAHDF NIVEDI
FMD Outbreaks in India as per three different agencies
2.622.18
1.78 1.81
1.00
10.15
6.95
3.21
4.70
3.13
2.442.67 2.56
2.34
3.95
3.26
1.96
2.63
4.71
4.114.42 4.30 4.34
4.94
4.42
3.46
3.95
3.19
2.652.96
2.632.85
2.582.38
2.04 2.12
0.00
2.00
4.00
6.00
8.00
10.00
12.00
2007 2008 2009 2010 2011 2013 2014 2015 2016
Percent Case fatality in FMD in India
Deaths due to FMD in India Log10
Animals affected Log10
Outbreaks Log10
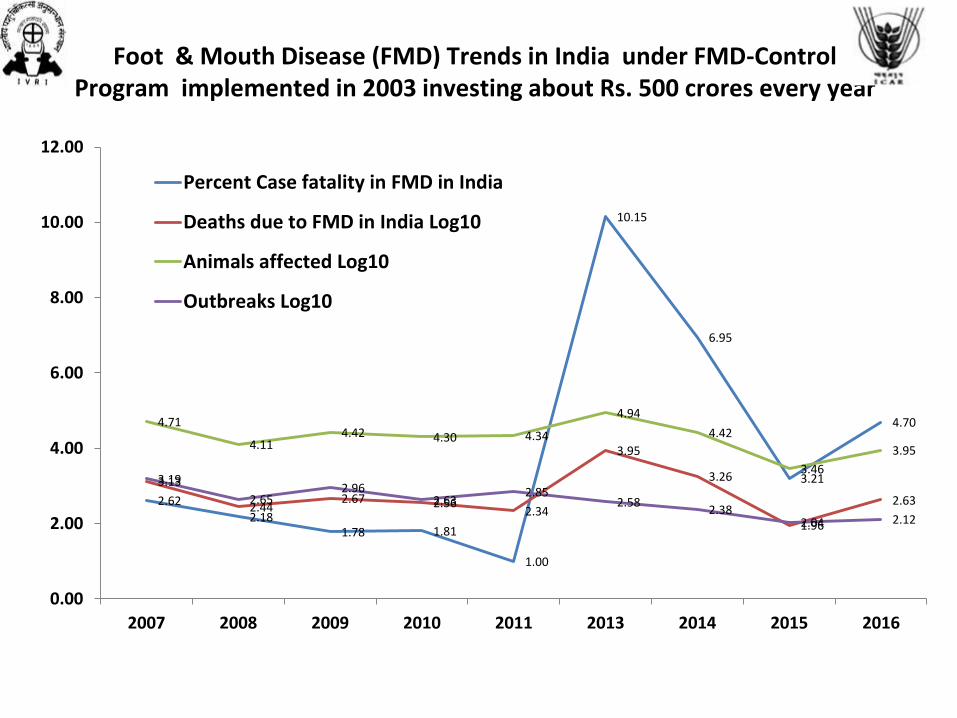
Foot & Mouth Disease (FMD) Trends in India under FMD-Control Program implemented in 2003 investing about Rs. 500 crores every year
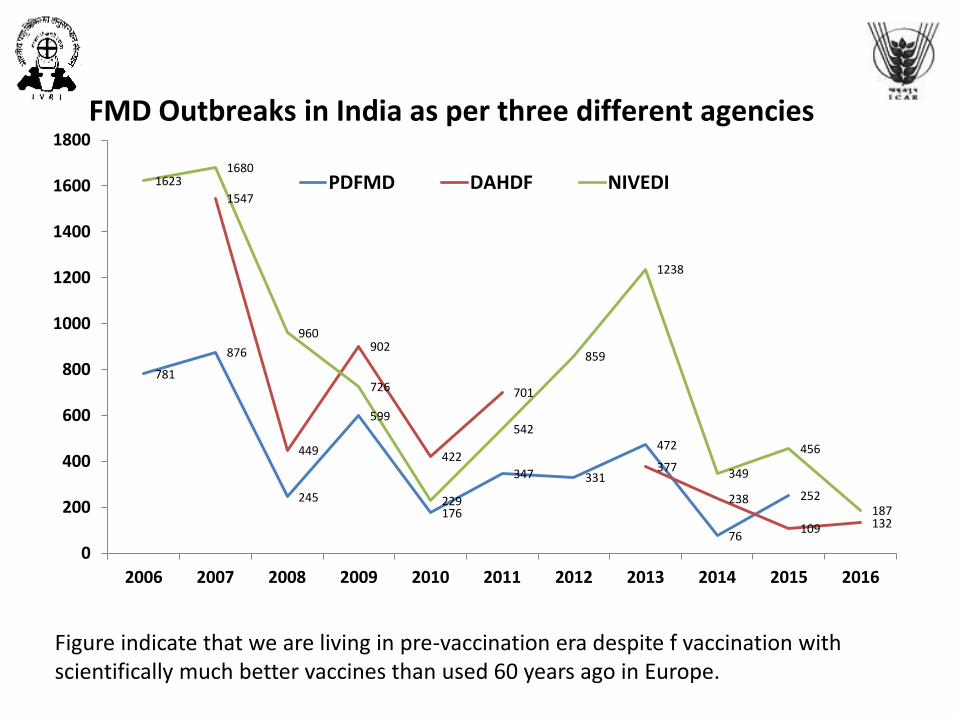
Figure indicate that we are living in pre-vaccination era despite f vaccination with scientifically much better vaccines than used 60 years ago in Europe.
781
876
245
599
176
347 331
472
76
252
1547
449
902
422
701
377
238
109 132
16231680
960
726
229
542
859
1238
349
456
187
0
200
400
600
800
1000
1200
1400
1600
1800
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
PDFMD DAHDF NIVEDI
FMD Outbreaks in India as per three different agencies

33 28 2947
31
231
110
26
68
0
50
100
150
200
250
2007 2008 2009 2010 2011 2013 2014 2015 2016
Cases per Outbreak of FMD in India
2.6 2.2 1.8 1.81.0
10.2
6.9
3.2
4.7
0.0
2.0
4.0
6.0
8.0
10.0
12.0
2007 2008 2009 2010 2011 2013 2014 2015 2016
Percent Case fatality in FMD in India
51101
12753
2652719982 21847
87109
26216
28688984
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
100000
2007 2008 2009 2010 2011 2013 2014 2015 2016
Animals affected with FMD in India
1338
278 473 361 218
8843
1822
92422
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
10000
2007 2008 2009 2010 2011 2013 2014 2015 2016
Deaths due to FMD in India
FMD CP in IndiaStarted in 2003
With Faulty selection of vaccine strains: Selection of the Vaccine strains should be based on epidemiological
distribution the causal agent and it must be updated as soon as possible.
• Vaccine strains: serotype O, the vaccine strain,INDR2/1975 covered 88% of the field isolates.
• In case of serotype A, none of the isolates showedperfect match with the vaccine strain, IND40/2000.
• Asia1 vaccine strain, IND63/1972, was last recorded inthe year 2000.
• The vaccine strain C IND/51/79. Since 1996, type Coutbreaks have not been recorded in India.
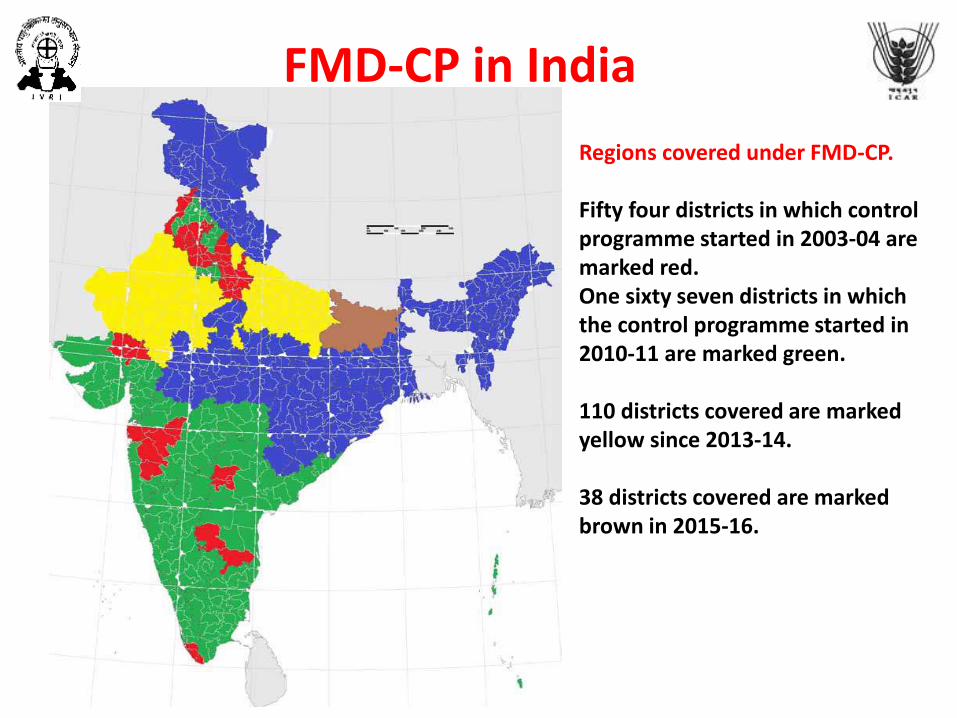
Regions covered under FMD-CP.
Fifty four districts in which control programme started in 2003-04 are marked red. One sixty seven districts in which the control programme started in 2010-11 are marked green.
110 districts covered are marked yellow since 2013-14.
38 districts covered are marked brown in 2015-16.
FMD-CP in India
FMD Treatment & Control
Treatment: Permitted only in enzootic regions. Only supportive type.Control: 1. Combined use of trade and movement restrictions of animals and animal
products has not completely prevented introductions of FMD into FMD-free areas.
2. These viral incursions into countries or regions where FMD is not enzootic are usually controlled by slaughter of all infected and susceptible animals, strict restriction of animal and vehicle movement around infected premises, proper carcass disposal, and environmental disinfection, without the use of vaccines.
3. Inactivated virus vaccines are limited in their use, because: 1. They protect for only 4–6 mo against the specific serotype(s)2. Protect animals from clinical illness but not viral persistence in the pharyngeal
region; therefore, they can induce a carrier state. 3. It is difficult to distinguish infected animals from vaccinated animals unless
purified killed vaccines are used.
4. Thus, vaccination is used more in enzootic countries to protect producing animals, particularly high-yielding dairy cattle, from clinical illness because slaughter of all at-risk individuals may be legally/ economically unfeasible.
What we need for control of FMD?
• Rapid disease reporting is essential to control an FMD outbreak. • Veterinarians who encounter any vesicular disease should immediately inform their state
and regional veterinary authorities. • After an outbreak, tracing must be done through epidemiologic inquiries to help identify
the source of disease introduction. • Where mass slaughter is not possible, strict quarantining and movement restriction
should be enforced. • However, quarantine may not be long enough to prevent carrier animal movement after
an outbreak. • The dead infected carcasses must be disposed of via incineration, burial, or rendering on
or close to the infected premises. • Scavengers and rodents should be prevented or killed to prevent mechanical
dissemination of virus. • Buildings should be cleaned with a mild acid or alkali disinfectant and fumigation, and
people that have come into contact with virus may be asked to decontaminate their clothing and avoid contact with susceptible animals for a period of time.
• FMD persistence in wildlife populations can make FMD eradication unrealistic. • Control measures, such as fencing of wildlife reserves to prevent contact with domestic
livestock may help to limit the spread of virus in certain areas. • A twice-yearly vaccination buffer zone in livestock proximal to endemic wildlife reserves
may additionally help decrease outbreak occurrence.
FMD Control
• The FMD Control component of the strategy therefore not onlyaims to reduce the burden of FMD on animal production indeveloping countries, but also in FMD-free countries. Whenincursions do occur, the cost of outbreak control may be enormousand the FMD control methods used are increasingly criticized.Reducing FMD at source in FMD-endemic countries is therefore ashared interest and should be considered a Global Public Good.
• The Global FMD Control Strategy is not a ‘stand-alone activity’ Onthe contrary: FMD control implies to simultaneously progress in thestrengthening of veterinary systems and vice versa StrengtheningVS creates better possibilities to control other priority diseases andFMD control creates opportunities through cost-effectivecombinations of activities.
• The Strategy includes three Components: 1- Improving global FMDcontrol 2- Strengthening Veterinary Services 3- Improving theprevention and control of other major diseases of livestock.
FMD Control• FMD control is applied in achievable steps • Disease control is a complex process requiring a considerable period of
time and many resources to implement. • The pathway begins with gaining an understanding of the disease’s
circulation in a country and its impacts. • At the next step, this knowledge is used to plan the initial strategic control
based on identified risks for FMD. • Critically, the control plan is monitored and evaluated.• PCP-FMD uses risk analysis principles to identify and prioritise risk
“hotspots” A risk “hotspot” might be a production sector, activity or geographical area where there is a high likelihood of spread of disease, or where disease leads to high impacts and losses. Once these risk “hotspots” are identified, these are used to define the objectives, tactics and activities of a risk-based strategic plan. Using risk analysis principles helps to make best use of limited resources, and direct FMD control measures where they will have most benefit.
• The PCP requires countries to progressively monitor the level of implementation of planned activities and evaluate the impact of these on occurrence of FMD. This provides evidence that the approach is working as planned and gives room to adapt or change the activities if necessary.
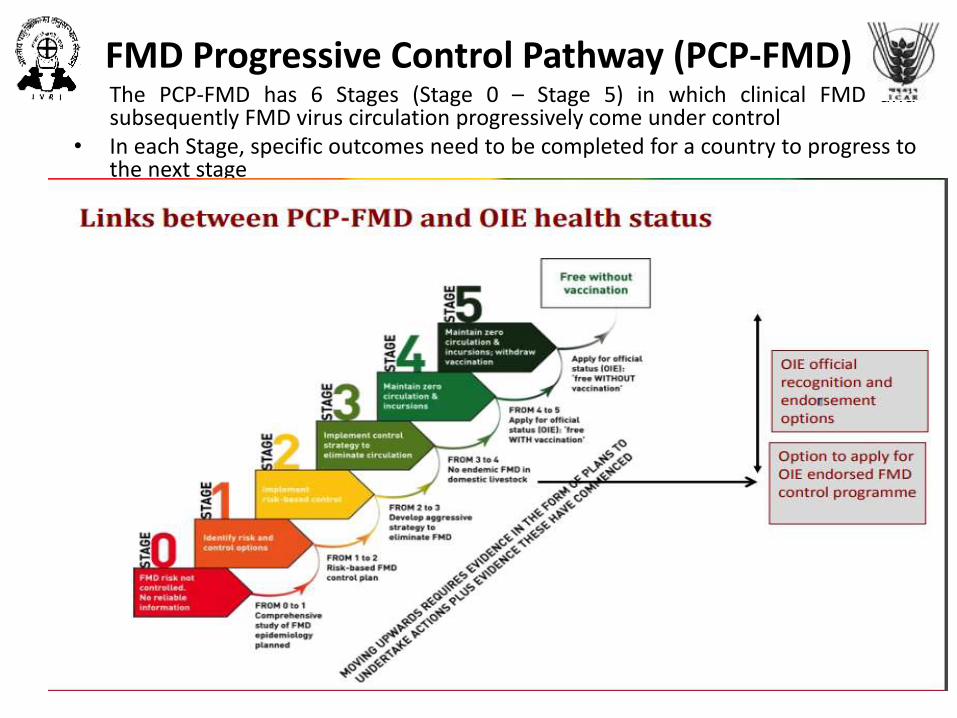
FMD Progressive Control Pathway (PCP-FMD)• The PCP-FMD has 6 Stages (Stage 0 – Stage 5) in which clinical FMD and
subsequently FMD virus circulation progressively come under control• In each Stage, specific outcomes need to be completed for a country to progress to
the next stage

PCP-FMDPCP-FMD and Misconceptions
• The PCP-FMD requires Huge investment just to get started. Countrieswithout these resources should not even consider starting to control foot-and-mouth disease. No, the PCP-FMD recognises that many countries withendemic FMD have limited resources. The PCP-FMD focuses on makingbest use of these limited resources to reduce the impacts of FMD as muchas possible.
• Countries which start on the PCPFMD pathway should eradicate FMD fromtheir entire country within 15 years. No, countries can choose how far andhow fast to progress along the pathway. It is not necessary for countries toaim for complete eradication, if this is not beneficial or viable. Somecountries may apply the pathway to only one geographical region orproduction sector.
• With FMD Control no other disease control program is feasible. No,identification of priority diseases that may be combined with FMD control(Anthrax, CBPP, Brucellosis, HS, BQ etc) may drastically reduce the cost.
• FMD can not be controlled without cull and slaughter policy. Ni, FMD canvery well be controlled, yes eradication may not be possible but a countrycan be free of FMD with and without vaccination even without culling andslaughter, it requires scientific planning and honest implementation.
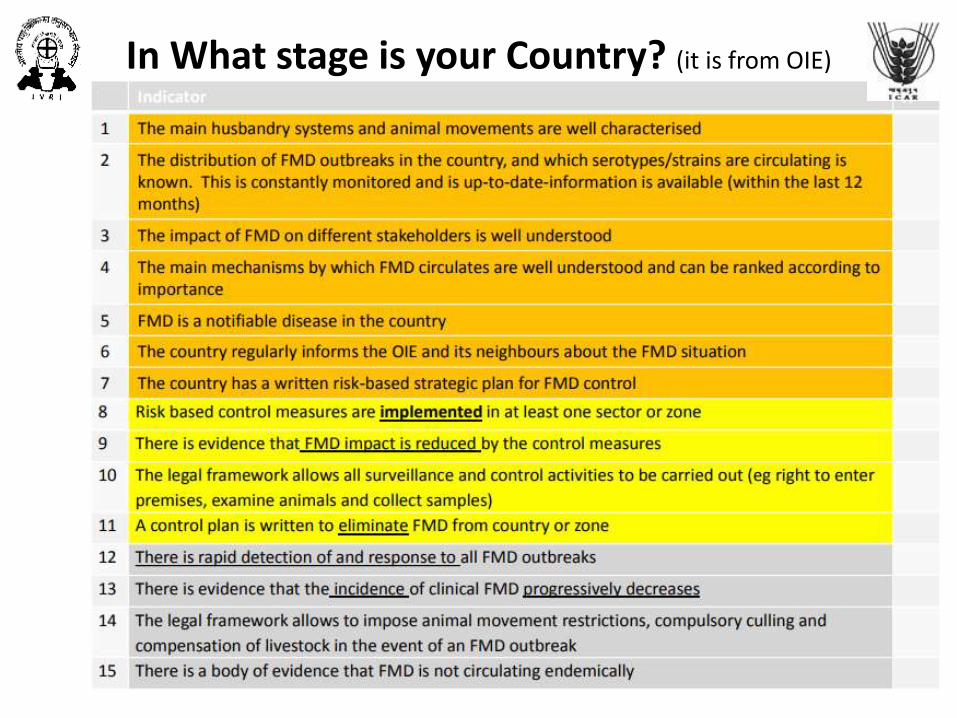
In What stage is your Country? (it is from OIE)
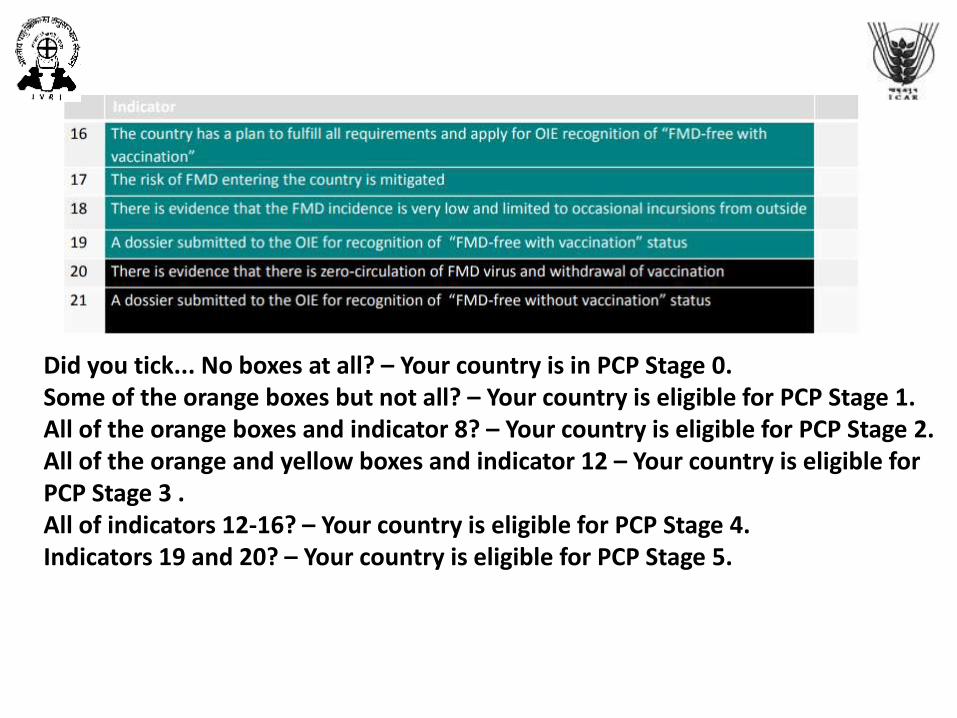
Did you tick... No boxes at all? – Your country is in PCP Stage 0.Some of the orange boxes but not all? – Your country is eligible for PCP Stage 1. All of the orange boxes and indicator 8? – Your country is eligible for PCP Stage 2. All of the orange and yellow boxes and indicator 12 – Your country is eligible for PCP Stage 3 .All of indicators 12-16? – Your country is eligible for PCP Stage 4. Indicators 19 and 20? – Your country is eligible for PCP Stage 5.
Major basic elements of FMD-PCP
https://www.oie.int/doc/ged/D12144.PDF
• Effective surveillance and alert systems • Quality controlled vaccines (OIE standards) Vaccine matching Vaccine banks
Vaccine quality control centres Vaccination strategies: massive, targeted… • Updated legislations • Use of OIE standards • Communication strategies
Major activities- Stage 1: focus on understanding FMD epidemiology and risk assessment - Stage 2: focus on implementing a control strategy targeted to part of the
country, a sector or subsector. Will usually involve vaccination - Stage 3: prompt response mechanisms become crucial - Stage 4: activities to be continued with a strong focus on prevention - Stage 5: the country may apply for OIE recognition as being FMD-free with
vaccination.
PCP-FMD assessment procedure
• The review process should be:
– Transparent
– Evidence-based
– Advisory (through networking)
– Consistent/Standard: regionally and globally
– Not too arduous
Limiting factors in FMD-CP
• Political commitment• Vet. Services• Economical capacity • Perception of no clear benefits except export• Movement controls • Wildlife reservoirs • Epidemiology knowledge • National surveillance systems, • International surveillance • Laboratory capacities and regional networking • Vaccine quality control • Education, training • Private Public Partnerships

Why FMD CP is a failure in India?No doubt FMD control is a very difficult task but international efforts made in different parts of the world have shown the path in
lucidity. The OIE has framed a Progressive Control Program for FMD (PCP-FMD) where the essentials are mentioned as under:See how the tenets of FMD control has been flawed in India
Strengthening Veterinary services: Either effort is not made or made half hearted or made to destroy the services. Without strong veterinary services, no disease control program can be implemented towards success.
Effective surveillance and alert systems: It is in primitive stage and in hands of those who have no or little experience.Quality controlled vaccines (OIE standards) Vaccine matching Vaccine banks Vaccine quality control centers Vaccination strategies:
massive, targeted: There is only one Centre to monitor the quality of vaccine to ensure the monopoly. There in India is a foolproof system to harass honest officials if they report about the poor quality of the vaccine.
Updated Legislation: All over the world culling of diseased animals is practiced to protect the healthy ones but legislations in India are humanitarian and you can not get rid of the diseased cattle in India.
Use of OIE standards: We believe on Made in India and Make in India standards.Communication strategies: Communication of truth is the essence of knowledge and knowledge is dangerous for the propagation of
corruption, thus only biased communication is permitted.Rapid disease reporting is essential to control an FMD outbreak. In India, administrators ensure through all the measures to hide the
reports.After an outbreak, tracing must be done through epidemiologic inquiries to help identify the source of disease introduction. In India,
administrators ensure through all the measures to prevent entry of the Epidemiologist in the scene.Where mass slaughter is not possible, strict quarantining and movement restriction should be enforced. In India, administrators
ensure through all the measures to get rid of sick animals as soon as possible through auction.However, quarantine may not be long enough to prevent carrier animal movement after an outbreak. In India, administrators
ensure through all the measures to move the diseased animals out of their administrative regions.The dead infected carcasses must be disposed of via incineration, burial, or rendering on or close to the infected premises. In India, you
may not see any such practice.Scavengers and rodents should be prevented or killed to prevent mechanical dissemination of the virus. In India, you may not see any
such practice.Buildings should be cleaned with a mild acid or alkali disinfectant and fumigation, and people that have come into contact
with virus may be asked to decontaminate their clothing and avoid contact with susceptible animals for a period of time. In India, you may not see any such practice.
FMD persistence in wildlife populations can make FMD eradication unrealistic. Control measures, such as fencing of wildlife reserves to prevent contact with domestic livestock may help to limit the spread of the virus in certain areas. In India, you may not see any such practice because when it is not possible to protect humans from wild-life invading in urban areas and getting killed the question of protecting livestock is a far fetched dream.
Investigation of all FMD outbreaks: Instead of investigation efforts are made to hide the outbreaks.
A solution to the Problem1. Redrafting of the program with the experts in Epidemiology specifically those who
are practicing epidemiology and certainly not by the so called experts sitting in the big chairs.
2. Ensuring the quality vaccine by creating multiple centers for quality control and abolishing the prevailing monopoly system.
3. Ensuring the punishment for those supplying and clearing the substandard vaccines.
4. Punishing those hiding the FMD or FMD like diseases in the livestock and other animals.
5. Rewarding the Veterinarians for reporting the FMD and FMD like diseases in animals and being proactive in the truthful investigation of the disease incidences and outbreaks.
6. Ensuring the implementation of available legislation towards disease control.
7. Bringing some suitable legislation targeted for disease control in animals leaving the political and religious taboos aside. We can permit sacrifice of animals for religious causes but prohibit scientific culling for disease control and healthy society.
8. To educate the society about disease control methods using scientific animal husbandry.
9. Strengthening of Veterinary services which are still in infancy in most parts of India.
10. Education for cleanliness and hygiene. Though Swachchhata Abhiyan is on, it needs to holistic and in the syllabus of primary education.
Quiz
1. Give reasons of occurrence of FMD outbreaks in Indiadespite FMD-CP.
2. Give reasons for increasing trends of case fatality rates dueto FMD.
3. Give reasons why sheep and goats are not included undercover of FMD-CP.
4. Write a note on Reservoirs of FMD in India.
5. Why India has been kept in PCP-Stage-3.