Embed Size (px)
DESCRIPTION
ROLE OF RADIOTHERAPY IN EWINGS SARCOMA
Citation preview

EWINGS SARCOMA: ROLE OF RADIOTHERAPY
DR.PAUL GEORGE
RCC


• Identified in 1921 by James Ewing
• 2nd most common bone tumor in children
• Ewing’s Sarcoma Family of tumors:
– Ewing’s sarcoma (Bone –87%)
– Extraosseous Ewing’s sarcoma (8%)
– Peripheral PNET(5%)
– Askin’s tumor
Occurs most commonly in 2nd decade◦ 80% occur between ages 5 and 25
3
Introduction

characteristics• Small blue round cell neoplasm• Consistent cytogenetic abnormality
t(11;22)(q24;q12) in 90-95%resultant fusion gene is EWS/FLI-1
• The c-myc protooncogene isfrequently expressed in Ewing’s.
• CD 99 ( MIC2)• PAS +ve
• more common in diaphysis or metadiaphysiscentral axis (47%): pelvis25%, chest wall, spine,H&Nextremities (53%)
• 25% present with metastatic disease– Lungs (38%)Bone (31%)Bone Marrow (11%)
• Nearly all pts. have micromets at diagnosis ,so all Need chemo.



Induction Chemotherapy
Local Control
• Surgery
• Radiotherapy
Maintenance
• Chemotherapy
GENERAL PRINCIPLES OF MANAGEMENT
12 TO 24WKSVAC/IE
AT 12WK/18WK
UP TO 1YEAR

LOCAL THERAPY
The need to attain complete tumor eradication must be weighed against the twin goals of
• maximizing function and
• minimizing long-term morbidity

RT versus surgery• No randomized trials which directly compare both
modalities, and their relative roles continue to be debated
• Contemporary treatment guidelines emphasize surgical resection as the local control modality of choice
• In many retrospective series, rates of local control and survival are superior after surgery compared to RT alone.However, larger cooperative group studies have failed to reflect this advantage, and selection bias likely accounts for at least some of these results.

• CESS-86, which included central quality assurance, the five-year RFS rates following chemotherapy plus either RT or surgery were 67 and 65 percent, respectively
• US Intergroup study 0091 (IESS III), a randomized comparison of VACA +/- IE,The rates of five-year, event-free survival (EFS) and local failure in the entire group were 49 and 21 percent, respectively which was present regardless of the local control modality.
The choice between surgery and RT is dictated by
• the age of the patient,
• the location and size of the primary, and
• functional as well as long-term consequences of therapy.

SURGERY
Surgery is preferred for potentially resectable lesions,and for those arising in dispensable bones (eg, fibula, rib,small lesions of the hands or feet) for the followingreasons:
• It avoids the risk of secondary radiation-induced sarcomas.
• An analysis of the degree of necrosis in the excised tumor can permit refinements in the estimate of prognosis
• In the skeletally immature child, resection may be associated with less morbidity than radiation, which can retard bone growth and cause deformity

• Tumors affecting the long bones of the leg, distal humerus, or ulna can usually be resected and reconstructed using intercalary techniques (allografts, autografts, or metallic prostheses) or joint replacement, depending on tumor location

RADIOTHERAPY & EWINGS
MELTING LIKE SNOW
1.Control of PRIMARY
2.ADJUANT/POSTOP RT
3.METASTATIC SETTING

RT FOR LOCAL CONTROL OF THE PRIMARY
Patients who
• lack a function-preserving surgical option because of tumor location or extent, and
• those who have clearly unresectable primary tumors following induction chemotherapy are appropriate candidates for RT.
Primary tumors involving the proximal humerus and upper
Scapula may be best treated with RT, since limb reconstruction is
difficult and shoulder morbidity may be substantial.
Patients with lesions of the skull, facial bones, or vertebrae are
often candidates for nonsurgical treatment because of the
difficulty in achieving negative margins without substantial
functional deficit

Adjuvant RT• Recommended if there is residual microscopic or gross
disease after surgery, or inadequate surgical margins
• For bulky tumors in difficult sites such as the pelvis, combined surgery and RT might allow for a more limited surgical procedure, better functional outcome, and enhanced local control as compared to single modality therapy.
• Prophylactic whole lung irradiation is not recommended (IESS1)
• adjuvant hemithorax irradiation improves outcomes in patients with high-risk chest wall primary tumors (close or involved margins, initial pleural effusion, pleural infiltration, and intraoperative contamination of the pleural space)

RT FOR METASTATIC DISEASE
1.Management of primary site
2.Pulmonary metastasis
3.Bone & soft tissue mets
4.Total Body Irradiation?

Management of the primary site:
• difficult to justify a large resection of the primary site because of the poor long-term prognosis.On the other hand, RT can provide adequate local control with acceptable morbidity

Pulmonary metastases: In highly selected patients, between 20 and 40 percent five-year OS can be achieved
In the CESS and EICESS trials, the rate of pulmonary relapse was reduced by 50 percent over that for patients who did not undergo lung RT, and this was accompanied by improvements in event free survival (from 19 to 40)
Despite the lack of controlled trials, low-dose bilateral lung irradiation (15 to 18 Gy, in daily 1.5 to 2.0 Gy fractions) with a focal boost dose to a total of 40 to 50 Gy to large deposits is commonly recommended for patients with pulmonary metastases who have had a good response to chemotherapy

Bone and soft tissue metastases limited data
For patients with solitary or limited bone metastases, RT is delivered to metastatic lesions (doses of 40 to 50 Gy) in addition to irradiation of the primary tumor for patients who are good responders of chemotherapy.

TOTAL BODY IRRADIATION
TBI has not contributed significantly to the control of metastatic disease. This approach should not be considered at present
TBI: The use of TBI as a conditioning regimen prior to high-dose chemotherapy and hematopoietic stem cell transplantation for patients with poor-risk disease

RADIATION TREATMENT PLANNING —
• Treatment volume — Historically, Ewing sarcoma was thought to be a tumor of the bone marrow. Consequently, RT was administered to the entire marrow cavity of the involved bone.
• However, an analysis of the RT fields for the Intergroup Ewing's Sarcoma Study Group (IESS) trial I suggested that most relapses were at the site of initially bulky tumor. Subsequent efforts were geared toward reducing the irradiated field and targeting higher doses to the site of the initial primary tumor.

In 1983, the Pediatric Oncology Group attempted a randomized trial of whole bone versus tailored-field RT after 12 weeks of induction chemotherapy .
IESS III: first cooperative group trial to include tailored RT ports, and the first to be carried out with modern MRI imaging of the primary site and CT-based treatment planning. The addition of IE significantly improved five-year survival (72 versus 61 percent) and event-free survival rates (69 versus 54 percent), which was present regardless of the local control
modality.


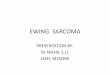
FIG. Changes in treatment volume. (A) Field encompassing the entire length of the medullary cavity for a tumor involving the proximal left humerus. (B) Tailored field encompassing only the proximal aspect of the leg for a limited tumor of the left tibia.

PLANNING CONT…
DEFINITIVE RT:
Phase 1:
• Gross tumor in bone and soft
tissue (pre chemo ) + 2cm
longitudinal margins + 2 cm lateral
margins
• Dose:45 Gy/180-225cGy/#
Boost phase :
• Reduced 1-2 cm margins
(bone and residual tissue)
Up to total dose of 55.8Gy(10.8Gy/6#)

• For rib primary ,with pleural effusion, RT to hemithorax
• Lesion of vertebral body treated with 45Gy.
Adjuant RT
• Pretreatment gross tumor volume +surgical scar+2cm margin(45 Gy) boost to post op residual +2cm margin.
Dose:
• MICROSCOPIC DISEASE- 45 Gy
• MACROSCOPIC RESIDUAL – 55.8Gy
Pre op RT
• 45 Gy to original bone and soft tissue

METASTATIC LESIONS
• For isolated pulmonary metastasis: low-dose bilateral lung irradiation (15 to 18 Gy, in daily 1.5 to 2.0 Gy fractions)
• Pain palliation– advanced disease.
• Isolated bone secondaries

Attention to potential RT effects on normal tissue is critical in radiation planning
• Even partial treatment of uninvolved epiphyseal growth plates is avoided
• Circumferential irradiation of a limb is avoided
• Gonadal avoidance or additional shielding (for the testes)
• Irradiation of the Achilles tendon is usually avoided
• For pelvic tumors, distention of the bladder prior to each day's treatment can reduce the amount of small bowel in the radiated field

Proton beam therapy
• One way to reduce the volume of normal tissue irradiated is with charged particle irradiation using protons.
• Compared to photon beam irradiation, proton beam therapy permits the delivery of high doses of RT to the target volume while reducing the radiation dose received by normal tissues distal to the target.

• Because of the proximity of the spinal cord, the dose to vertebral body primaries using conventional photon irradiation has been often limited to 45 Gy. Proton beam therapy permits the delivery of higher doses while respecting spinal cord constraints.
• When used for pelvic lesions, proton beam therapy is associated with better sparing of the intestine, rectum, bladder, pelvic bone marrow, and femoral head as compared to photon irradiation Proton beam irradiation.

RT schedule
Data from the University of Florida suggest that
hyperfractionated RT (1.2 Gy twice daily with a six hour
interfraction interval) may be associated with less long-term
toxicity .
Limited field sizes with hyperfractionated high-energy RT could
minimize long-term complications and provide superior
functional outcomes.

IORT — A benefit for intraoperative RT (IORT) has been suggested in retrospective series involving a small number of patients .
• However, peripheral nerves are dose-limiting tissue structures for IORT, so the risk of severe neuropathy and soft tissue necrosis must be considered if this approach is used.

SEQUELAE OF TREATMENT• Acute effects — Acute reactions are those that occur during
or shortly after the completion of RT. The most prominent affect tissues within the radiated field that contain rapidly dividing cells, and include
• desquamation of the skin,
• myelosuppression,
• mucositis, diarrhea, nausea, and cystitis.
• Patients receiving whole lung irradiation are at risk for radiation pneumonitis.
Acute reactions are usually self-limited and subside within
10 to 14 days of RT completion

Late effects :
• Younger, prepubertal children are at greatest risk for radiation-induced arrest of bone growth. Sparing of uninvolved epiphyseal plates minimizes limb shortening after RT of extremity lesions.
• RT doses above 60 Gy are associated with markedly increased rates of soft tissue induration and fibrosis
• High-dose circumferential irradiation of an extremity is associated with edema, fibrosis, and compromised limb function . This can be avoided by sparing of an adequate strip of tissue.
• Weight-bearing bones are at risk for pathologic fractures. The highest risk is within the first 18 months of RT completion

Second malignancy after RT
• OSTEOSARCOMA
With protocols utilizing lower doses of RT and tailored RT fields suggest that the magnitude of the risk is somewhat lower.
• Cumulative risk at 15yrs = 6 – 6.7%
( CESS-81 & CESS-86; IJROBP:1997; 39)
• No secondary sarcomas seen at doses <48 Gy
( Kutterch et al; JCO:1996, 14 )

SUMMARY of RT in EWINGSLocalized disease — For patients with localized EFT, local and systemic
therapy are both necessary to achieve cure.
• For patients who lack a function-preserving surgical option because of tumor location or extent, and those who have clearly unresectable primary tumors following induction chemotherapy, recommend RT
• Bulky tumors in difficult sites (eg, the pelvis); in this setting, RT can be given either preoperatively or postoperatively, based upon institutional protocols
• If there is residual microscopic or gross disease after surgery, or inadequate surgical margins.
• Adjuvant hemithorax irradiation is indicated in patients with high-risk chest wall primary tumors (close or involved margins, initial pleural effusion, pleural infiltration, and intraoperativecontamination of the pleural space)

Advanced disease: For patients with metastatic EFT, RT rather than surgery for treatment of the primary site in most patients
• because of the potential for reduced pulmonary relapse and improved event-free survival, and the low rate of pulmonary toxicity, bilateral low-dose lung irradiation (15 to 18 Gy) is recommended

NCCN GUIDELINES V1.2014

NCCN CONT..

NCCN CONT…….
Patients who lack a function-preserving surgical option because of tumor location or extent, and those who have clearly unresectable primary tumors following induction chemotherapy are appropriate candidates for RT.

SURVIVAL



• Second most common childhood bone tumor.
• Multimodal treatment approach
• Overall survival with localized disease (55%) and metastatic disease 22%
• Radiation responsive tumor
• LOCAL THERAPY includes SURGERY/RT. Surgery when feasible first choice of local therapy
• There are no randomized trials that have directely compared Radiotherapy to surgery for local control of Ewing’s sarcoma.
• Refinements in diagnostic imaging, RT planning, and newer techniques (tailored field size, hyperfractionated treatment schedules, IMRT, proton beam irradiation) have resulted in better limb function among long-term survivors, and excellent functional results in the majority of patients following RT for EFT.
Conclusion

THANK YOU…….