Embed Size (px)
Citation preview

EWING’S SARCOMA
By : Dr. Utsav Agrawal

IntroductionEwing, in 1921 described it as a tumor occuring in
the diaphysis of long bone, in children, asso. With febrile attacks , anorexia and anaemia and which was radio-sensitive.
He believed it arose from endothelial elements of bone marrow and described it as diffuse endothelioma of bone
Willis found rosette formation and presence of primary lesion, usually in adrenals, in many cases
Ewings sarcoma is thought to be of either neuro-ectodermal or stem cell origin
All Ewings sarcoma’s are considered high grade malignancy and categorized under Enneking Stage II or III

Epidemiology9% of primary bone sarcomas4th most common primary malignancy of bone but
2nd most common below 30yrs.Age Group – 95% patients age between 5 to 30 yrs
- of these most range between 5 to 15 yrs• Sex - slight male predilection – 60%• More common in Whites (95%)• No known predisposing factor• Chromosomal translocation – t(11;22)(q24;q12) leading to fusion of EWS and FLI gene. also t(21;22) and t(7;22)

Clinical FeaturesPainSwellingFeverWeight lossAnemiaRaised ESR and CRPLeukocytosisAnd, symptoms depending on area of
involvement

LocationCan develop in any bonePrincipally affects the lower segment of the skeleton in
more than 2/3 casesIn long tubular bones – proximal segment more
frequently involved than distal fragment (5:1 to 3:1) Usually of diaphyseal origin. Sometimes dia-metaphyseal. Rarely, metaphyseal.In vertebrae, most commonly involved – Sacrum Body is mainly affected with subsequent involvement of intra and para-spinal tissues and posterior elements mostly metastatic.• Rarely may be localized to soft-tissue or peri-osteum.

10%
22 %
11%
F - 9%
8
126
1
3%

RadiologyOn Plain X-ray – In long bones- Diaphyseal/metadiaphyseal Cortical erosion Periostitis Soft-tissue mass Osteolysis Aggressive nature with permeative/moth-eaten type of bone
destruction Peri-osteal response – may be lamellated (‘onion-skin’) or
hair-0n-end Cortical changes – longitudinal cross striations, tunnelling
and saucerization. Occasionally, osteosclerosis and pathological fractures

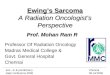
Hair-on-end periosteal reaction
Onion skin formation

Metatarsal involvement with moth-eaten appearance, periostitis Involvement of long bone with
lamellated appearance, saucerisation, cortical breach, periostitis

Ewings sarcoma with extensive soft tissue involvement

In Vertebrae – OsteolysisFracturesVertebra planaExtension to posterior segmentSoft tissue mass• In RibsOsteo-lytic/sclerotic/bothDirection of growth usually intrathoracicLarge extra-pleural mass
• Metastasis – Usually to Lungs(m.c.) and Bones.

• Bone Scan - uptake - rarely cold spots• Gallium scan• CT scan – to assess cortical destruction
- For extra-osseous and trans-articular spread - for chest metastasis - evaluation of response to therapy• MRI – for extra-osseous(T2) and intramedullary(T1) extent of
lesion - metastasis -relationship with neurovascular structures - pre-operative planning ( along with MR-angio) - response to therapy• PET scan• Biopsy – For definitive diagnosis with histopathology,immuno- histochemistry, cytogenetics, karyotyping, RT-PCR
– Open or Needle - should include incision within area of specimen to be resected - best to avoid making a cortical defect when planning RT for
local control of disease (increased risk of pathological fractures)

Histo-pathologyDiaphyseal/dia-metaphysealPredominantly medullary, then extends to
haversian system and cortexGreyish-white to pink in colorsoft, friableOften of semi-liquid consistencyAreas of hemorrhage, necrosis and cyst
formation presentOnion-skin periosteal reaction

MicroscopySmall round undifferentiated tumor cells with little
cytoplasm and indistinct bordersRound nuclei with stippled evenly distributed powder-
like chromatin and 1-2 nucleoliFrequent mitosisNecrosis and Ghost cellsMinimal inter-cellular substanceRosette and psuedo-rosette formationPeritheliomaNO GIANT CELLSPAS +ve presence of glycogenReactive for vimentin

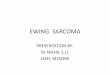
Ewings sarcoma under light microscopy H&E stain. Intensely stained cells with scant intercellular matrix, pseudo-rosette formation

Under high power - Small round cells with indistinct borders, powdery chromatin, 1-2 nucleoli, minimal inter-cellular substance, no giant cells.

Ewings Family of Tumors1. Ewings2. PNET3. AskinsSimilarity between Ewings and PNET• C/f, radiology, light microscopy• Chromosomal translocation t(11:22)(q24:q12)• Reactivity towards p30/32 MIC-2 in 90%Differences : In PNET• More frequent epiphyseal involvement, Pathological fractures,
metastasis• Rosette formation• Electron microscopy – features of neural differentiation like dendritic
processes, abundance of cytoplasmic granules, intermediate filaments, neurosecretory granules and microtubule formation.
• Immunohistochemistry - +ve for neural markers – S-100, synaptophysin, NSE, neuro-filament protein.

Differential diagnosisOsteosarcomaLymphomaLeukemiaOsteomyelitisPNET

Prognostic factorsGood prognosis in – involvement of distal segment of extremities No metastasis Infants and young children FemalesPoor prognosis – Proximal segment involvement Sacral involvement Patients above 18 yrs LDH and ESR Size greater than 8cm

Enneking system for malignant tumors
Stage Grade Site Metastasis
IA Low G-1 Intracompartmental T1
-
IB Low G-1 Extracompartmental T2
-
IIA High G-2 Intracompartmental T1
-
IIB High G-2 Extracompartmental T2
-
III Any G Any T Regional/ distant metastasis

TreatmentGoal – To eliminate tumor mass, prevent recurrence
and preserve functionDepends on Stage at presentation and Location of
lesionModalities of treatment – Chemotherapy, Surgery and
radiotherapyChemotherapy alone, as adjuvant or neo-adjuvant to
surgical excision or debulkingDrugs used – Vincristine, Actinomycin-D,
Cyclophosphamide ( VAC regimen)Also used - Doxorubicin, etoposide, ifosphamideRadiotherapy - Generally, a dose of 45-50 Gy is
administered over a 5 week course to treat local disease.

ChemotherapyInduction CT for 3-6 cycles followed by 6-10 cycles of maintenanceFirst Line therapy: VAC/IE
Given in cycles of 3 weeks Vincristine 2.0 mg/m2 on D1-2 Adriamycin 75 mg/m2 on D1-2 Cyclophosphamide 1.2 gm/m2 on D1-2 Ifosphamide 1.8 gm/m2 on D3-7 Etoposide 100 mg/m2 on D3-7
Second line therapy (relapse and refractory disease Cyclophosphamide (250 mg/m2)and topotecan(0.75 mg/m2) D1-D5 Temozolomide and irinotecan Ifosfamide and etoposide Ifosfamide ,etoposide and carboplatin Docetaxel and gemcitabine

RadiotherapyFor,Tumors where Resection is Impossible For skull, face, vertebra, or pelvic primarywhere only an intra-lesional resection is achievablePatient with poor Surgical riskPatient refusing surgeryPre-op - Indicated when narrow resection margins are expected To sterilize the tumor compartment before surgery & to potentially reduce the risk of dissemination during surgeryLocal recurrence with pre-op RT <5% Post-op - For gross or microscopic positive margin For marginal Resection For wide-resection with Poor Histological response to Neo-adjuvant Chemotherapy

Newer TherapiesNutlin – 3a MDM-2 antagonistFigitumumab – antibodies against IGF-R1mTOR inhibitors – everolimus, rapamycinRetinoids – FenretinideBiphosphonatesTRAIL receptor agonistsGene therapy

THANK YOU