Embed Size (px)
Citation preview


EssentialNeurosurgery
KAYPR 12/16/04 7:32 PM Page i

KAYPR 12/16/04 7:32 PM Page ii

THIRD EDITION
EssentialNeurosurgeryAndrew H. Kaye MBBS,MD,FRACSJames Stewart Professor of Surgery and Head of Department of Surgery,The University of MelbourneDirector of Neurosurgery and Director, The Melbourne Neuroscience Centre,The Royal Melbourne Hospital, Melbourne, Australia
KAYPR 12/16/04 7:32 PM Page iii

© 1991 Longman Group UK Limited© 1997 Pearson Professional Limited© 2005 Andrew KayePublished by Blackwell Publishing LtdBlackwell Publishing, Inc., 350 Main Street, Malden, Massachusetts 02148-5020, USABlackwell Publishing Ltd, 9600 Garsington Road, Oxford OX4 2DQ, UKBlackwell Publishing Asia Pty Ltd, 550 Swanston Street, Carlton, Victoria3053, Australia
The right of the Author to be identified as the Author of this Work has beenasserted in accordance with the Copyright, Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored ina retrieval system, or transmitted, in any form or by any means, electronic,mechanical, photocopying, recording or otherwise, except as permitted bythe UK Copyright, Designs and Patents Act 1988, without the prior permission of the publisher.
First published 1991Second edition 1997Third edition 2005
Library of Congress Cataloging-in-Publication Data
Kaye, Andrew H., 1950–Essential neurosurgery / Andrew H. Kaye. — 3rd ed.
p. ; cm.Includes bibliographical references and index.ISBN 1-4051-1641-21. Nervous system — Surgery.[DNLM: 1. Neurosurgical Procedures. 2. Central Nervous System —
surgery. 3. Central Nervous System Diseases — diagnosis. WL 368 K23e 2005] I. Title.
RD593.K28 2005617.4¢8 — dc22
2004021462
ISBN-13: 978-1-405-1641-1ISBN-10: 1-4051-1641-2
A catalogue record for this title is available from the British Library
Set in 9/12 Palatino by SNP Best-set Typesetter Ltd., Hong KongPrinted and bound in India by Replika Press Pvt., Ltd.
Commissioning Editor: Vicki NoyesDevelopment Editor: Lorna HindProduction Controller: Kate Charman
For further information on Blackwell Publishing, visit our website:http://www.blackwellpublishing.com
The publisher’s policy is to use permanent paper from mills that operate asustainable forestry policy, and which has been manufactured from pulpprocessed using acid-free and elementary chlorine-free practices. Further-more, the publisher ensures that the text paper and cover board used havemet acceptable environmental accreditation standards.
KAYPR 12/16/04 7:32 PM Page iv

Preface to the third edition, vii
Preface to the first edition, ix
1 Neurological assessment and examination, 1
2 Neurosurgical investigations, 14
3 Raised intracranial pressure and hydrocephalus, 27
4 Head injuries, 40
5 Traumatic intracranial haematomas, 56
6 Brain tumours, 64
7 Benign brain tumours, 93
8 Pituitary tumours, 109
9 Subarachnoid haemorrhage, 125
10 Stroke, 140Stephen M. Davis MD, FRACP
11 Developmental abnormalities, 158
12 Infections of the central nervous system, 170
13 Low back pain and leg pain, 185
14 Cervical disc disease and cervical spondylosis, 197
15 Spinal cord compression, 206
16 Spinal injuries, 225
17 Peripheral nerve entrapments, injuries and tumours, 234
18 Facial pain and hemifacial spasm, 248
19 Pain — neurosurgical management, 254
20 Movement disorders — neurosurgical aspects, 263
21 Epilepsy and its neurosurgical aspects, 269Christine Kilpatrick MD, FRACP
Index, 281
Contents
v
KAYPR 12/16/04 7:33 PM Page v

KAYPR 12/16/04 7:33 PM Page vi

Preface to the third edition
vii
Neurosurgery has continued to benefit consider-ably from a wide range of technological advancesthat have enabled better imaging of central ner-vous system disease, understanding of diseaseprocesses and the consequent development of rational treatments.
Magnetic resonance imaging has now becomethe standard radiological technique to investi-gate central nervous system disease, and this hasfurther demystified the diagnostic process inneurosurgery. However, it has entailed a newlearning process not only for students, but alsofor practising clinicians. Magnetic resonancespectroscopy has become a routine diagnostictool as has magnetic resonance angiography.
Improved understanding of the biology of thecentral nervous system and tumour biology, hasled to the introduction of more rational treatmentregimes, with improved outcomes. Molecular biology techniques, the introduction of biologicaltherapies including gene therapies, and the development of endovascular surgery have considerably broadened the horizon for the management of a wide range of neurological dis-eases. Technological advances in the operatingtheatre have increased the surgical possibilities,particularly combining stereotactic techniqueswith microneurosurgery. Our patients have ben-efited considerably from these advances, andover the next two decades biological and techni-cal advances will continue to provide consider-able benefit for even more of our patients.
This third edition of Essential Neurosurgeryhas essentially been based on the first and second
editions, but has incorporated many of the ad-vances described. Modern neurosurgical prac-tices still differ considerably in North Americaand Europe, and despite the ‘global village’ therecontinues to be substantive differences in thephilosophical approach to the management ofclinical problems. The author has described hisown practice, which hopefully continues to uti-lize the best of both systems, as well as incorpo-rating the unique advances and philosophies ofthe Asia–Pacific rim region.
It is not possible to list and acknowledge all themany people who have helped in the preparationof this third edition. However, I particularly ac-knowledge my neurological and neurosurgicalcolleagues at The Royal Melbourne Hospital.Stephen Davis and Christine Kilpatrick haveagain provided chapters on their own areas of ex-pertise. I am very grateful to Nicholas Maartensfor his considerable help with chapters on HeadInjury, Brain Tumours and Pituitary Tumours,John Laidlaw for his assistance with a chapter onSubarachnoid Haemorrhage and Bhadu Kavarfor his input into the rewriting of the Spinal Injuries chapter.
I would like to especially thank KateLagerewskij for the many hours she spentpreparing the manuscript and to Helen Harvey at Blackwell Publishing for making this editionpossible.
As always I am especially grateful to the en-couragement and patience of my wife Judy andson Ben.
Andrew H. Kaye, Melbourne, 2004
KAYPR 12/16/04 7:33 PM Page vii

KAYPR 12/16/04 7:33 PM Page viii

Clinical neurosurgery requires an understandingof the art of neurology and of the principles of theneurosciences, particularly neuropathology andneurophysiology. In the past the mystique ofneurosurgery has inadvertently prevented bothmedical trainees and physicians from a properappreciation of even basic neurosurgery and con-sequently has created a rather nihilistic view ofneurosurgical illnesses. The improvements inmedical technology have markedly improvedthe accuracy of the diagnosis, the efficacy of neu-rosurgical treatment and the range of diseasesthat can be diagnosed and treated. In particular,the exciting advances in neuroradiology havesimplified the diagnostic process and made neu-rosurgery more accessible.
This book is intended as an introduction toneurosurgery. It is hoped that it will be useful forphysicians in training, neurosurgical traineesand medical students. The book is not intendedto be an exhaustive coverage of neurosurgery butrather concentrates on the more common neuro-surgical problems and only briefly mentions rareentities.
The neurological principles, pathological basisand relevant investigations that form the basis ofthe diagnosis are emphasised. The neurosurgicalmanagement is outlined but the surgical tech-niques are only briefly mentioned, so that thereader will understand the postoperative prob-lems likely to be encountered in the managementof the patient. Modern neurosurgery has evolvedprincipally from North American and Europeanpractices and there are often significant differ-ences in the philosophical approach in the man-agement of clinical problems. The author has in
general described his own practice, which hope-fully utilises the best of both systems.
The references have been chosen for their gen-eral coverage of the topics, ease of access, histori-cal interest and, in some cases, because they willprovide thought provoking alternatives that givea different perspective to the subject.
It is not possible to list and acknowledge all themany people who have helped in the preparationof this book, both knowingly and as a result oftheir influence on my own neurosurgical prac-tices. However, the late John Bryant Curtis wasthe major initial influence not only on my ownneurosurgical education but on that of manyother Australian neurosurgeons. I particularlyacknowledge the help of my neurological andneurosurgical colleagues at the Royal MelbourneHospital in the preparation of this book. StephenDavis and Christine Kilpatrick have providedchapters on their own areas of expertise. Profes-sor Brian Tress, Director of Radiology at theRoyal Melbourne Hospital, has always been ac-cessible and helpful and I am indebted to him forhis expert teaching over many years and for as-sistance with the details on magnetic resonanceimaging. His department supplied most of the X-rays. Dr Meredith Weinstein, neuroradiologist atthe Cleveland Clinic, kindly provided magneticresonance scans (Figs 7.9, 12.7, 13.5). ProfessorColin Masters, Department of Pathology, Univer-sity of Melbourne and Dr Michael Gonzales, neu-ropathologist at the Royal Melbourne Hospital,gave assistance with the pathology details and illustrations. My residents and registrars at theRoyal Melbourne Hospital have always pro-vided stimulating advice and criticisms. I par-
Preface to the first edition
ix
KAYPR 12/16/04 7:33 PM Page ix

x PREFACE TO THE FIRST EDITION
ticularly acknowledge the assistance of Drs JohnLaidlaw and Michael Murphy, registrars in neurosurgery, who proof read the manuscriptand offered constructive criticism. I thank SueDammery for the many hours spent preparingthe manuscript and Richard Mahoney for the illustrations.
The book would not have been possible with-out the guidance and stimulus from PeterRichardson at Churchill Livingstone.
I am especially grateful to the encouragementand patience of my wife Judy and son Ben.
Andrew H. Kaye, Melbourne, 1990
KAYPR 12/16/04 7:33 PM Page x

An accurate neurological assessment is funda-mental for the correct management of the patient.The basic aim of the neurological examination isto solve the following four questions:1 Is there a neurological problem?2 What is the site of the lesion (or lesions) in thenervous system?3 What are the pathological conditions that cancause the lesions?4 Having ascertained the neuroanatomical siteand the pathological cause from the history, whatis the most likely diagnosis?
Answering these four questions in turn will in-dicate the type of investigation necessary to con-firm the diagnosis.
The neurological assessment involves:• the history of the illness• clinical examination:
(a) of the nervous system(b) general examination.
The neurological history
As in general medicine and surgery the neuro-logical history is the key to the diagnosis. The his-tory involves not only questioning the patientbut also careful observation. Many neurologicalillnesses can be diagnosed just by observing thepatient. The patient’s general manner, mood,posture, gait, facial expression and speech are allvital clues to the final diagnosis. In addition, pa-tients who do not have an organic disease maypresent in a characteristic manner, particularlywith an exaggeration of the complaint.
The history and examination commences withobservation, and this should begin when first
meeting the patient and while taking the history.The way in which the patient walks into the ex-amination room, sits on the chair, answers ques-tions and climbs on to the examination couch willprovide vital clues in the search for the diagnosis.Initially it is important to allow the patient ade-quate opportunity to explain their symptoms inan unstructured and unprompted manner. Directquestioning should then follow.
The questions concerning neurological symp-toms are in essence a verbal examination of theneurological system. It is not just the content ofthe answer that is important but the way in whichthe patient responds to the questions. The follow-ing is a general classification of neurologicalsymptoms.1 General neurological symptoms:
(a) headache(b) drowsiness (decreased conscious state)(c) vertigo(d) seizures, blackouts.
2 Symptoms of meningismus:(a) headache(b) photophobia(c) neck stiffness(d) vomiting.
3 Symptoms related to the special senses:(a) vision(b) hearing(c) taste(d) smell.
4 Symptoms related to speech and comprehen-sion.5 Motor symptoms:
(a) power(b) coordination.
CHAPTER 1
1 Neurological assessment and examination
1
KAY1 12/16/04 7:34 PM Page 1

2 CHAPTER 1
6 Sensory symptoms.7 Cognitive symptoms, e.g. memory.8 Symptoms of other systems which may relateto diseases of the nervous system.
Careful questioning will ascertain the impor-tant details concerning each symptom. These include:• The time, mode of onset, progression and duration of the symptom. The mode of onset is avaluable clue in discerning the pathologicalprocess. Sudden onset of a neurological distur-bance is usually due to a vascular or epileptiformcause; a sudden severe headache is characteristicof subarachnoid haemorrhage whereas a slowlyprogressive headache is more in keeping with acerebral tumour. Similarly, the abrupt onset of ahemiplegia may result from a vascular catastro-phe and slowly progressive weakness may bedue to a compressive or infiltrative cause.• What factors result in alleviation or exacerba-tion of the symptom? Headache from raised in-tracranial pressure is characteristically worse inthe morning and on coughing and straining. Patients find the hand pain associated withcarpal tunnel syndrome is often worse at nightand is alleviated by shaking the hand over theside of the bed.• Is there a past history of any similar event?
It is often helpful to obtain details of the histo-ry from the patient’s relatives or a witness; it isvital to do this if the patient is a child or if there isimpairment of conscious state or memory distur-bance. Details of the nature of epileptic seizuresshould always be obtained from a relative orfriend who has witnessed an event.
A thorough understanding of the nature of theillness and symptomatology should have beenobtained before the examination is commenced.
Neurological examination
The formal neurological examination should beundertaken in a systemic fashion in the followingorder.1 Mental state.2 Speech.3 Cranial nerves.4 Examination of limbs and trunk:
(a) posture(b) wasting(c) tone(d) power(e) reflexes(f) sensation(g) coordination and gait.
Mental state
Examination of the mental state involves an as-sessment of:• conscious state• orientation in time, place and person• memory• emotional state• presence of delusions or hallucinations.A correct assessment of the mental state is essen-tial prior to the evaluation of the other neurologi-cal signs. The remainder of the neurologicalexamination will be undertaken within the con-text of the patient’s mental state. The accurate assessment of conscious state is especially important in neurosurgical disorders and theevaluation of the level of consciousness using theGlasgow coma scale is described in the chapteron head injuries (Chapter 4). Imprecise termssuch as ‘stuporose’ should be avoided and the examiner should objectively assess and des-cribe the patient’s response to specific stimuli.‘Drowsiness’ — a depressed conscious state — isthe most important neurological sign and indi-cates major intracranial pathology. As with allneurological symptoms and signs it is essential toobtain an assessment of the progression of thedrowsiness by questioning the patient’s friendsor relatives. A deteriorating conscious state is aneurosurgical emergency.
Memory disturbances should be tested for-mally for both short-term and long-term preser-vation. Short-term memory should be tested bylisting a name, address and type of flower andasking the patient to recall it after 5 minutes. Lossof short-term memory with relative preservationof memory for long-past events is typical of de-mentia, e.g. Alzheimer’s disease. In Korsakoff’spsychosis the disturbance of recent memory anddisorientation may be so severe that the patient
KAY1 12/16/04 7:34 PM Page 2

will make up stories to provide a convincing answer to the questions. This is confabulationand is classically associated with alcoholism, although it may rarely be seen as a result of anterior hypothalamic lesions due to trauma or following subarachnoid haemorrhage and vasospasm.
Speech disorders
There are four main speech disorders:1 Mutism.2 Aphonia.3 Dysarthria.4 Dysphasia.
MutismMutism is characterized by the patient being alertbut making no attempt to speak. It may resultfrom lesions affecting the medial aspect of bothfrontal lobes, classically occurring as a result ofvasospasm following subarachnoid haemor-rhage from a ruptured anterior communicatingartery aneurysm.
AphoniaAphonia is said to occur when the patient is ableto speak but is unable to produce any volume ofsound. It is due to a disturbance of the vocal cordsor larynx. If the patient is able to cough normallythen it is usually hysterical.
DysarthriaDysarthria is due to impaired coordination of thelips, palate, tongue and larynx and may resultfrom extrapyramidal, brainstem or cerebellar le-sions. The volume and content of the speech willbe normal but the enunciation will be distorted.
Spastic dysarthria. This is due to bilateral uppermotor neurone disease due to pseudobulbarpalsy, motor neurone disease or brainstem tumours.
Ataxic dysarthria. This is due to incoordinationof the muscles of speech; the words are often stac-cato or scanning and the rhythm is jerky. Thistype of dysarthria is seen in cerebellopontineangle tumours, cerebellar lesions, multiple scle-rosis and phenytoin toxicity.
Dysarthria may result from lesions of the lowermotor neurones and the muscles, such as occur inpalatal palsies or paralysis of the tongue.
‘Rigid dysarthria’. This is characteristic ofParkinson’s disease. In severe cases the phenom-enon of palilalia is seen, in which there is a con-stant repetition of a particular syllable.
DysphasiaDysphasia may be either expressive or receptive.Patients with expressive dysphasia can under-stand speech but cannot formulate their ownspeech. Patients with receptive dysphasia cannotunderstand spoken or written speech. Althoughone type of dysphasia may predominate there isfrequently a mixture of the two patterns of dis-ability. Dysphasia results from lesions of thedominant hemisphere, which is the left hemi-sphere in right-handed people as well as in a highproportion of left-handed people.
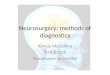
Expressive dysphasia. This is due to a lesion affecting either Broca’s area in the lower part ofthe precentral gyrus (Fig. 1.1) or the left posteriortemporoparietal region. If the latter region is af-fected the patient may have a nominal dysphasia,in which the ability to name objects is lost but theability to speak is retained.
Receptive dysphasia. This results from lesions inWernicke’s area, which is the posterior part of thesuperior temporal gyrus and the adjacent pari-etal lobe.
AlexiaAlexia is the inability to understand writtenspeech. Alexia with agraphia (inability to write)is due to a lesion in the left angular gyrus. The pa-tient is unable to read or write spontaneously andthe condition is often accompanied by nominaldysphasia, acalculia, hemianopia and visual agnosia. Gerstmann’s syndrome consists of fin-ger agnosia for both the patient’s own finger andthe examiner’s finger, acalculia, right/left disori-entation and agraphia without alexia. It is foundin lesions of the dominant hemisphere in the re-gion of the angular gyrus.
NEUROLOGICAL ASSESSMENT AND EXAMINATION 3
KAY1 12/16/04 7:34 PM Page 3

4 CHAPTER 1
Examination of the cranial nerves
Olfactory nerveThe sense of smell should be tested by the patientsniffing through each nostril as the other is com-pressed. The common causes of anosmia are ol-factory nerve lesions resulting from head injury,and tumours involving the floor of the anteriorcranial fossa, especially olfactory groove menin-giomas. It is important to use non-irritant sub-stances when testing olfaction, as irritatingcompounds (e.g. ammonia) will cause irritationof the nasal mucosa. The stimulus is then per-ceived by the general sensory fibres of the trigem-inal nerve.
Optic nerveThe optic nerve should be tested by:• measuring the visual acuity and colour vision• charting the visual fields• fundal examination with an ophthalmoscope• the pupillary light reflex.
Visual acuityThe visual acuity should be tested using the stan-dard Snellen type charts placed at 6 m. The acuityis recorded as a fraction, e.g. 6/6 or 6/12, inwhich the numerator indicates the distance inmetres from the chart and the denominator theline on the chart that can be read. 6/6 is normalvision. Refractive errors should be corrected bytesting with the patient’s glasses or by asking thepatient to view the chart through a pinhole.
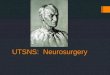
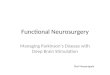
Visual fieldsThe visual fields can be charted by confrontation,with the patient facing the examiner and objectsof varying size being moved slowly into the visu-al field (Fig. 1.2). Formal testing using perimetryshould be undertaken in all cases of visual failure, pituitary tumour, parasellar tumour,other tumours possibly involving the visualpathways and demyelinating disease, or if thereare any doubts after confrontation that the fieldsmay be restricted.
Perimetry can be performed using either a tan-gent screen, such as a Bjerrum screen (Fig. 1.3), or
Central sulcus
Secondary visual area
Primary visual area
Larynx
Tongue
Lips
ShoulderElbow
WristFingers
Lips
Hand
Nose
Jaw
Toes
Leg
Knee
Cortex
Hip
NeckThumb
Brow
NoseEyelid
Motor activity Sensory activity
Primarymotor area
Primary somatosensory area
Precentral gyrus
Supplementary motor area
Toes
AnkleAnkle
Leg
Knee
HipShoulder
ElbowWrist
FingersThumb
NeckBrow
Eyelid
Broca's motor speech area
Trunk Trunk
Fig. 1.1 Major areas ofsomatotopic organization ofthe cerebrum.
KAY1 12/16/04 7:34 PM Page 4

a Goldmann perimeter. The Bjerrum screenrecords the central field of vision. By enlargingthe central area out to 30° it is easier to detect sco-tomas and to measure the blind spot and, provid-ed a small enough target is used, the tangentscreen provides an accurate representation of theperipheral fields. An automated perimetry ma-chine will enable an accurate and reproduciblefield test that is particularly useful in cooperativepatients.
The pattern of visual field loss will depend onthe anatomical site of the lesion in the visualpathways (Fig. 1.4):
• total visual loss — optic nerve lesion• altitudinous hemianopia — partial lesion of theoptic nerve due to trauma or vascular accident• homonymous hemianopia — lesions of theoptic tract, radiation or calcarine cortex• bitemporal hemianopia — optic chiasm lesionssuch as pituitary tumour, craniopharyngioma orsuprasellar meningioma.
Fundal examinationThe fundus should be examined using the oph-thalmoscope with particular attention to the:• optic disc• vessels• retina.A pale optic disc is due to optic atrophy whichmay be either primary, as a result of an opticnerve lesion caused by compression or demyeli-nation, or consecutive, which follows severeswelling of the disc. Papilloedema is due toraised intracranial pressure and is evident by:• blurring of the disc margins• filling in of the optic cup• swelling and engorgement of retinal veins,with loss of normal pulsation of the veins• haemorrhages around the disc margin (if severe).
Third, fourth and sixth cranial nervesAs these cranial nerves are all involved in inner-vation of the extraocular muscles they are usuallyexamined together. This examination involvesassessment of:• the position of the eyelids• the pupils• extraocular movements.
Position of the eyelidsPtosis is due to paralysis of the levator palpebraesuperioris as a result of a 3rd cranial nerve lesionor due to weakness of the tarsal muscle due to asympathetic lesion (Horner’s syndrome).
The pupilsAn assessment should be made of the pupil size,shape and equality. The pupils’ reaction to lightshould be tested by shining a beam into the eyeand noting the reaction in that eye, as well as the
NEUROLOGICAL ASSESSMENT AND EXAMINATION 5
Examiner
Test object
Patient
Fig. 1.2 Visual field testing by confrontation.
30∞
20∞
10∞
Fixationpoint
BJERRUM SCREEN
Record target colour anddiameter/distance of eyefrom fixation point, e.g. 10/2000
Fig. 1.3 The Bjerrum screen.
KAY1 12/16/04 7:34 PM Page 5

6 CHAPTER 1
consensual response in the opposite eye. The reac-tion to convergence and accommodation for nearvision should be tested by asking the patient to fixon a distant object and then placing a pen approx-imately 12 cm in front of the bridge of the nose.
A unilateral constricted pupil (miosis) oftenindicates a lesion in the sympathetic supply tothe pupillary dilator muscle.
Horner’s syndrome, in its complete state, con-sists of miosis, ptosis, enophthalmos and drynessand warmth of half of the face. It is due to a lesionof the sympathetic supply such as results from anintracavernous carotid artery aneurysm, or aPancoast’s tumour of the apex of the lung.
Adilated pupil (mydriasis) results from paral-ysis of the parasympathetic fibres originatingfrom the nucleus of Edinger–Westphal in themidbrain, and is therefore seen in a 3rd nervepalsy. The possible causes are an enlarging poste-rior communicating artery aneurysm causing
pressure on these fibres in the 3rd cranial nerve(Chapter 9) and tentorial herniation resultingfrom intracranial pressure with the herniateduncus of the temporal lobe compressing the 3rdnerve (Chapter 5).
The Argyll–Robertson pupil is a small, irregu-lar pupil not reacting to light, reacting to accom-modation but responding poorly to mydriatics; itis usually caused by syphilis.
The myotonic pupil (Holmes–Adie) usuallyoccurs in young women and presents as a unilat-eral dilatation of one pupil with failure to react tolight. The pupil shows a slow constriction occur-ring on maintaining convergence for a prolongedperiod. In the complete syndrome the knee andankle jerks are absent.
Ocular movementThe following are the general actions of the ex-traocular muscles.
Temporalfield
Nasal field
Lefteye
Righteye
Left Right
AB
C
D
Opticnerve
Opticchiasm
Optictract
Lateral geniculate body
Geniculocalcarine tractD
A
B
C
Occipital cortex
Fig. 1.4 Diagrammaticrepresentation of visualpathways, the common sitesof lesions and the resultingfield defects.
KAY1 12/16/04 7:34 PM Page 6

• Lateral rectus (6th nerve) moves the eye hori-zontally outwards.• Medial rectus (3rd nerve) moves the eye hori-zontally inwards.• Superior rectus (3rd nerve) elevates the eyewhen it is turned outwards.• Inferior oblique (3rd nerve) elevates the eyewhen it is turned inwards.• Inferior rectus (3rd nerve) depresses the eyewhen it is turned outwards.• Superior oblique (4th nerve) depresses the eyewhen it is turned inwards.
The patient should be tested for diplopia,which will indicate ocular muscle weakness be-fore it is evident on examination. The followingrules help determine which muscle and cranialnerve are involved.• The displacement of the false image may behorizontal, vertical or both.• The separation of images is greatest in the di-rection in which the weak muscle has its purestaction.• The false image is displaced furthest in the di-rection in which the weak muscle should movethe eye.
Disorders of eye movement may be due to im-paired conjugate ocular movement. The centrefor the control of conjugate lateral gaze is situatedin the posterior part of the frontal lobe, with inputfrom the occipital region. The final commonpathway for controlling conjugate movement isin the brainstem, particularly the median longi-tudinal bundle. A lesion of the frontal lobe causescontralateral paralysis of conjugate gaze (i.e. eyesdeviated towards the side of the lesion) and a le-sion of the brainstem causes ipsilateral paralysisof conjugate gaze (i.e. eyes deviated to side oppo-site to the lesion).
Nystagmus should be tested by asking the pa-tient to watch the tip of a pointer. This should beheld first in the midline and then moved slowlyto the right, to the left and then vertically up-wards and downwards.
Jerk nystagmus is the common type, consist-ing of slow drift in one direction and fast correct-ing movement in the other.
Horizontal jerk nystagmus is produced by le-sions in the vestibular system which may occur
peripherally in the labyrinth, centrally at the nu-clei, in the brainstem or in the cerebellum. In pe-ripheral lesions the quick phase is away from thelesion and the amplitude is greater in the direc-tion of the quick phase. In cerebellar lesions thequick phase is in the direction of gaze at that mo-ment but the amplitude is greater to the side ofthe lesion. By convention the quick phase is takento indicate the direction of the nystagmus, so thatif the slow phase is to the right and the quickphase to the left the patient is described as havingnystagmus to the left.
Vertical nystagmus is due to intrinsic brain-stem lesions such as multiple sclerosis, brainstemtumours or phenytoin toxicity. The so-called‘downbeat’ nystagmus, which is characterizedby a vertical nystagmus exaggerated by down-gaze, is particularly evident in low brainstem lesions as caused by Chiari syndrome, where the lower brainstem has been compressed by the descending cerebellar tonsils (Chapter 11).
Trigeminal nerveThe 5th cranial nerve (trigeminal nerve) is testedby assessing facial sensation over the three divi-sions of the cranial nerve; corneal sensationshould be tested using a fine piece of cotton wool.The motor function of the 5th nerve can be testedby palpating the muscles while the patientclenches their jaw, testing the power of jaw open-ing and lateral deviation of the jaw (Fig. 1.5).
Facial nerveThe facial nerve is tested by assessing facialmovement. In an upper motor neurone facialweakness the weakness of the lower part of the
NEUROLOGICAL ASSESSMENT AND EXAMINATION 7
Greater occipitalC. 2, 3
Lesser occipitalC. 2Greater auricularC. 2, 3Dorsal rami ofC. 3,4,5
Ophthalmic(V1)
Maxillary(V2)
Mandibular(V3)
Transverse cutaneousnerves of neck C. 2,3
SupraclavicularC. 3,4
Fig. 1.5 Cutaneous nerve supply of the face, scalp andneck.
KAY1 12/16/04 7:34 PM Page 7

8 CHAPTER 1
face is very much greater than the upper, with thestrength of the orbicularis oculis being relativelypreserved. This is due to a lesion between the cor-tex and the facial nucleus in the pons. Lowermotor neurone weakness is evident by equal in-volvement of the upper and lower parts of theface and is due to a lesion in, or distal to, the facialnerve nucleus in the pons.
The chorda tympani carries taste sensationfrom the anterior two-thirds of the tongue andthis should be examined using test flavoursplaced carefully on the anterior tongue.
Vestibulocochlear nerveThe 8th cranial nerve consists of:• the cochlear nerve — hearing• the vestibular nerve.
The cochlear nerveHearing can be examined at the bedside by mov-ing a finger in the meatus on one side, to producea masking noise, and repeating words at a stan-dard volume and from a set distance in the otherear. Differentiation between conduction and sen-sorineural deafness can be aided using tests witha tuning fork.
The Rinne’s test involves holding a vibratingtuning fork in front of the external meatus andthen on the mastoid process. In nerve deafnessboth air and bone conduction are reduced, but airconduction remains the better. In conductivedeafness bone conduction will be better than airconduction.
In Weber’s test the vibrating tuning fork isplaced on the centre of the forehead. In nervedeafness the sound appears to be heard better inthe normal ear, but in conductive deafness thesound is conducted to the abnormal ear.
Formal audiometry should be performed ifthere are symptoms of impaired hearing.
The vestibular nerveThe simplest test of vestibular function is thecaloric test, which is usually performed in pa-tients suspected of having a cerebellopontineangle tumour or as a test of brainstem function inpatients with severe brain injury. The test is de-scribed in Chapter 4, p. 44.
Glossopharyngeal and vagus nervesThe glossopharyngeal and vagus nerves can bemost easily assessed by testing palatal movementand sensation from the pharynx and soft palate.If necessary the vocal cords (vagus nerve) can beexamined and taste from the posterior one-thirdof the tongue (glossopharyngeal nerve) can betested.
Accessory nerveThe accessory nerve supplies the motor power tothe upper part of the trapezius and sternocleido-mastoid. The latter muscle can be tested by turn-ing the patient’s head against resistance andwatching and palpating the opposite sternomas-toid muscle. The trapezius muscle is best testedby asking the patient to shrug the shoulders andattempting to depress the shoulders forcibly.
Hypoglossal nerveThe hypoglossal nerve is responsible for move-ments of the tongue. The tongue should be in-spected to detect wasting and movements fromside to side should be observed to detect weak-ness. The tip of the protruded tongue will deviatetoward the side of weakness.
Examination of the periphery
Posture and general inspectionThe patient’s posture may indicate an underlyingneurological disability, or an abnormal posturemay result from pain. A patient with sciatica willoften lie on the opposite side with the affected legflexed at the hip and knee. The decerebrate pos-ture is discussed in Chapter 4.
The limbs should be inspected to compare size and shape and to detect deformity; long-standing neurological lesions may result in impaired growth or wasting. Lesions of lowermotor neurone in infancy, such as a brachialplexus palsy or poliomyelitis, will cause markedretardation in limb growth. Upper motor neu-rone lesions of long standing, such as acute infan-tile hemiplegia and cerebral birth trauma, willalso cause retardation in growth, but of a lesserdegree, with a hemiplegic posture and exaggera-ted reflexes.
KAY1 12/16/04 7:34 PM Page 8

WastingThe limbs and shoulder girdles should be in-spected to detect wasting and fasciculation. Aswell as palpating for specific muscle wasting ineach limb the circumference of the limbs shouldbe measured at clearly identifiable positions,such as 8 cm above or below the olecranon, 10 cmabove the patella and 8 cm below the tibialtuberosity.
The pattern of wasting will be an importantclue as to the underlying neurological disease.
Wasting of the forearm and small muscles of the hand.This results from lower motor neurone lesions af-fecting particularly the C7, C8 and T1 levels andmay be due to lesions of the:• spinal cord — motor neurone disease, syr-ingomyelia, cervical cord tumours• cervical nerve root — cervical disc prolapse• brachial plexus — trauma, cervical rib, axillarytumour• peripheral nerve — ulnar nerve compression atthe elbow, carpal tunnel syndrome (mediannerve).
Wasting of the muscles of the lower leg. This will re-sult from compression of the cauda equina orlumbosacral nerve roots caused by a lumbar discprolapse or tumour.
Muscular dystrophies. These are genetically deter-mined inherited degenerative myopathies andcause particular patterns of muscle wasting.• Facioscapulohumeral dystrophy involves theface and shoulder girdle.• Proximal limb girdle dystrophy involves bothshoulder and hip girdles.• Dystrophia myotonica involves the face, ster-nomastoids and quadriceps femoris. Myotonia(the failure of muscle to relax after contraction) ispresent, particularly in the peripheral musclesand tongue.• Peroneal muscular atrophy, with predominantinvolvement of the lower limbs, causes the ‘in-verted bottle appearance’ with similar but lessstriking changes in the upper limbs.• Duchenne’s muscular dystrophy occurs mainly in young boys and affects the arms and
legs; the muscles have a pseudohypertrophic appearance.
ToneThe tone in the upper limbs should be testedusing a flexion–extension movement of the wrist,by holding the patient’s terminal phalanges andby pronation–supination of the forearm. The tonein the lower limbs should be tested by flexion ofthe hip, knee and ankle.
Decreased toneThis is due to:• a lower motor neurone lesion involving thespinal roots or anterior horn cell of the spinalcord• lesions of the sensory roots of the reflex arc, e.g.tabes dorsalis• cerebellar lesions, which cause ipsilateral hypotonia• myopathies• spinal shock (the acute phase of a severe spinallesion usually due to trauma).
Increased toneThis will be produced by any upper motor neu-rone lesion involving the corticospinal tractsabove the level of the anterior horn cell in thespinal cord.
There are three major types of hypertonicity.1 ‘Clasp knife’ spasticity, in which the resistanceis most pronounced when the movement is firstmade. It is usually more marked in the flexormuscles of the upper limbs and extensor musclesof the lower limbs and is a sign of an upper motorneurone lesion.2 ‘Lead pipe’ rigidity, in which there is equal re-sistance to all movements. This is a characteristicfeature of a lesion of the extrapyramidal systembut is also seen in severe spasticity from an uppermotor neurone lesion.3 ‘Cog wheel’ rigidity, in which there is an alter-nating jerky resistance to movement and whichoccurs in degenerative lesions of the extrapyra-midal system, particularly Parkinson’s disease.
‘Clonus’ is best demonstrated by firm rapiddorsiflexion of the foot and is indicative ofmarked increased tone.
NEUROLOGICAL ASSESSMENT AND EXAMINATION 9
KAY1 12/16/04 7:34 PM Page 9

10 CHAPTER 1
PowerThe power should be tested in all limbs, compar-ing each side. Asystematic evaluation will enablethe recognition of a particular pattern of weak-ness that will be in keeping with either a cerebral,spinal cord, plexus or peripheral nerve weak-ness. The major nerve and main root supply ofthe muscles are shown in Table 1.1.
The Medical Research Council classifies the de-gree of weakness by recording power, rangingfrom 0 to 5 (Table 1.2). It is apparent that there is aconsiderable range of power between grades 4and 5 and some clinicians make their own furthersubclassification in this region.
Weakness due to a corticospinal tract lesion ismost marked in the abductors and extensors ofthe upper limbs and the flexors of the lowerlimbs. It is normally associated with increasedtone and exaggerated reflexes.
Weakness due to lower motor neurone lesionsis usually more severe than when the uppermotor neurone is involved and is seen in the dis-tribution of the nerve affected. It is associatedwith wasting, hypotonia and diminished reflexes.
Fasciculation is an irregular, non-rhythmicalcontraction of muscle fascicles which is most eas-ily seen in the deltoid or calf muscles. It occursclassically in motor neurone disease but may alsooccur in lower motor neurone lesions, e.g. in thelower limbs following long-standing lumbar rootcompression.
ReflexesThe deep tendon reflex requires the stimulus,sensory pathway, motor neurone, contractingmuscle and the synapses between the neuronesin order to elicit a response.
Reduced or absent tendon reflexThis may occur due to any breach in the reflex arc:• sensory nerve — polyneuritis• sensory root — tabes dorsalis• anterior horn cell — poliomyelitis• anterior root — compression• peripheral motor nerve — trauma• muscle — myopathy.
Increased deep tendon reflexesDue to lesions of the pyramidal system, increaseddeep tendon reflexes may be excessively pro-longed, with a larger amplitude in a cerebellar le-sion. In myxoedema the relaxation phase of thereflex is retarded.
Each deep tendon reflex is associated with aparticular segmental innervation and peripheralnerve as listed in Table 1.3.
The superficial abdominal reflex has a segmen-tal innervation extending from T9 in the upperabdominal region to T12 in the lower area. The re-flex may be absent in pyramidal lesions above thelevel of segmental innervation, particularly inspinal lesions. However, the reflex may also bedifficult to elicit when the abdominal muscleshave been stretched or damaged by surgical oper-ations, or in a large, pendulous, obese abdomen.
Plantar reflexThis should result in the great toe flexing themetatarsophalangeal joint. The Babinski re-sponse consists of extension of the great toe at themetatarsophalangeal joint, and usually at the in-terphalangeal joint, and indicates disturbance ofthe pyramidal tract.
SensationThe modalities of sensation which should be tested are:• light touch• pinprick (pain)• temperature• position (proprioception)• vibration.
Sensory testing involves an accurate under-standing of the anatomical pathways of sensa-tion. All modalities of sensation travel by theperipheral nerve and sensory root to the spinalcord, or via the cranial nerves to the brainstem.The fibres for pain and temperature sensationenter the posterolateral aspect of the spinal cord,travel cranially for a few segments and then crossto the opposite anterolateral spinothalamic tract.This tract ascends to the brainstem and is joinedby the quintothalamic (trigeminothalamic) tractin the pons. The fibres end mostly in the ventro-lateral nucleus of the thalamus and from here the
KAY1 12/16/04 7:34 PM Page 10

NEUROLOGICAL ASSESSMENT AND EXAMINATION 11
Table 1.1 Nerve and major root supply of muscles.
Spinal roots
Ulnar nerveFlexor carpi ulnaris C7, C8, T1Flexor digitorum profundus III C7, C8
and IVHypothenar muscles C8, T1Adductor pollicis C8, T1Flexis pollicis brevis C8, T1Palmar interossei C8, T1Dorsal interossei C8, T1Lumbricals III and IV C8, T1
Lower limb
Femoral nerveIliopsoas L1, L2, L3Rectus femorisVastus lateralis } Quadriceps L2, L3, L4Vastus intermedius femorisVastus medialis
Obturator nerveAdductor longus }Adductor magnus
L2, L3, L4
Superior gluteal nerveGluteus medius and minimus }Tensor fasciae latae
L4, L5, S1
Inferior gluteal nerveGluteus maximus L5, S1, S2
Sciatic and tibial nervesSemitendinosus L5, S1, S2Biceps L5, S1, S2Semimembranosus L5, S1, S2Gastrocnemius and soleus S1, S2Tibialis posterior L4, L5Flexor digitorum longus L5, S1, S2Flexor hallucis longus L5, S1, S2Small muscles of foot S1, S2
Sciatic and common peroneal nervesTibialis anterior L4, L5Extensor digitorum longus L5, S1Extensor hallucis longus L5, S1Extensor digitorum brevis L5, S1Peroneus longus L5, S1Peroneus brevis L5, S1
* Flexor pollicis brevis is often supplied wholly orpartially by the ulnar nerve.
Spinal roots
Upper limbSpinal accessory nerve
Trapezius C3, C4
Brachial plexusRhomboids C4, C5Serratus anterior C5, C6, C7Pectoralis major
Clavicular C5, C6Sternal C6, C7, C8
Supraspinatus C5, C6Infraspinatus C5, C6Latissimus dorsi C6, C7, C8Teres major C5, C6, C7
Axillary nerveDeltoid C5, C6
Musculocutaneous nerveBiceps C5, C6Brachialis C5, C6
Radial nerveTriceps
Long headLateral head C6, C7, C8Medial head
Brachioradialis C5, C6Extensor carpi radialis longus C5, C6
Posterior interosseous nerveSupinator C6, C7Extensor carpi ulnaris C7, C8Extensor digitorum C7, C8Abductor pollicis longus C7, C8Extensor pollicis longus C7, C8Extensor pollicis brevis C7, C8Extensor indicis C7, C8
Median nervePronator teres C6, C7Flexor carpi radialis C6, C7Flexor digitorum superficialis C7, C8, T1Abductor pollicis brevis C8, T1Flexor pollicis brevis* C8, T1Opponens pollicis C8, T1Lumbricals I and II C8, T1
Anterior interosseous nerveFlexor digitorum profundus I and II C7, C8Flexor pollicis longus C7, C8
KAY1 12/16/04 7:34 PM Page 11

12 CHAPTER 1
sensory impulses pass through the posterior limbof the internal capsule to the postcentral sensorycortex (see Chapter 19, Fig. 19.1). Fibres carryinglight touch, proprioception and vibration sensa-tion ascend mainly in the ipsilateral posteriorcolumns of the spinal cord on the same side to thenuclei gracilis and cuneatus. The fibres cross themidline to ascend through the brainstem in the medial lemniscus, to synapse in the thalamusand then on to the sensory cortex.
The sensory loss involving nocioceptive stim-uli (pain and temperature) should conform to aparticular pattern:• peripheral nerve• dermatome (nerve root)• spinal cord — resulting in a sensory level• ‘glove and stocking’ due to peripheral neu-ropathy• hemianalgesia — thalamic or upper brainstem
• loss of pain and temperature on one side of theface and the opposite side of the body — lesion ofthe medulla affecting the descending root of the5th nerve and the ascending spinothalamic tractfrom the remainder of the body.
CoordinationCoordination should be tested in the upper andlower limbs. In the upper limb it is best assessedusing the ‘finger–nose’ test and in the lower limbusing the ‘heel–knee’ test. It is important to deter-mine whether abnormalities of coordination aredue to defects in:• cerebellar function• proprioception• muscular weakness.
GaitAn essential part of the examination is to observethe patient’s gait. This is best done not only as aformal part of the examination but also when thepatient is not aware of observation. The type ofgait is characteristic of the underlying neurologi-cal disturbance.
Ahemiparesis will cause the patient to drag theleg and, if severe, the leg will be thrown out fromthe hip, producing the movement called circum-duction.
A high stepping gait occurs with a foot drop(e.g. L5 root lesion due to disc prolapse, lateralpopliteal nerve palsy, peroneal muscular atrophy). The patient raises the foot too high toovercome the foot drop and the toe hits theground first. In tabes dorsalis the high steppinggait is due to a profound loss of position sense but
Table 1.2 Medical Research Council classificationof power.
0 Total paralysis1 Flicker of contraction but no movement of limb2 Muscle only able to make normal movement
when limb is positioned so that gravity iseliminated
3 Normal movement against gravity but notagainst additional resistance
4 Full movement but overcome by resistance5 Normal power
Table 1.3 Deep tendon reflexes, peripheral nerve and segmental innervation.
Tendon reflex Major segmental innervation Peripheral nerve
Biceps jerk C5(6) MusculocutaneousSupinator jerk C5/C6 RadialTriceps jerk C7(8) RadialFlexor finger jerk C6–T1 Median and ulnarKnee jerk L3/L4 FemoralAnkle jerk S1(2) Medial popliteal and sciatic
KAY1 12/16/04 7:34 PM Page 12

a similar gait, of lesser severity, will result frominvolvement of the posterior column of the spinalcord or severe sensory neuropathy which inter-feres with position sense. The gait is worse in thedark and the heel usually strikes the ground first.
In Parkinson’s disease or other extrapyrami-dal diseases the patient walks with a stooped,shuffling gait. The patient may have difficulty instarting walking and stopping. A slight push for-ward will cause rapid forward movement (pro-topulsion).
In the ataxic gait, the patient is unstable due tocerebellar disturbance. A midline vermis tumourwill result in the patient reeling in any direction.If the cerebellar hemisphere is involved then thepatient will tend to fall to the ipsilateral side.
A waddling gait is associated with congenitaldislocation of the hips and muscular dystrophy.
The hysterical gait is often bizarre and is di-minished when the patient is unaware of any ob-servation.
Following the clinical assessment, a presump-tive diagnosis is made and further investigationscan be performed to confirm the diagnosis. Theselaboratory investigations and radiological proce-dures are described in the following chapter.
Brain death
The use of donor organs for transplantation andthe advent of improved intensive care facilitieshave resulted in the necessity of medically andlegally accepted criteria of brain death.
If there is irrecoverable brainstem damage andthe tests described below show no evidence ofbrainstem function, then the patient is medicallyand legally dead. If artificial ventilation is contin-ued the other organs may continue to function forsome time. However, continued prolonged venti-lation of the patient after the diagnosis of braindeath is not only undignified for the dead patientand distressing to the relatives, but is also waste-ful of expensive medical resources that are oftenin short supply.
The diagnosis of brain death relies on:• preconditions before testing can be performed• brain death tests.
The preconditions are that all reversible causes ofbrainstem depression have been excluded. Theseinclude:• depressant drugs• hypothermia (temperature must be greaterthan 35°C)• neuromuscular blocking drugs• metabolic or endocrine disturbance as a causeof the patient’s condition.Brain death testing must be delayed until thesepreconditions are absolutely satisfied.
The tests for brainstem function are:• lack of pupil response to light• lack of corneal reflex to stimulation• lack of oculocephalic reflex• failure of vestibulo-ocular reflex (caloric testing)• failure of a gag or cough reflex on bronchialstimulation• no motor response in the face or muscles sup-plied by the cranial nerves in response to painfulstimulus• failure of respiratory movements when the pa-tient is disconnected from a ventilator and thePaCO2 is allowed to rise to 50 mmHg.
The tests should be repeated after an interval of30 minutes and it is essential that they should becarried out by two doctors of adequate seniorityand with expertise in the field.
Further readingConference of Medical Royal Colleges and Their Facul-
ties in the UK (1979) Diagnosis of death. British Jour-nal of Medicine 1, 322.
Harrington D (1974) The Visual Fields, 4th edn. C VMosby, St Louis.
Jennett B (1981) Brain death. British Journal of Anaesthe-sia 53, 1111–1119.
Medical Research Council (1976) Aids to the examinationof the peripheral nervous system. Her Majesty’s Sta-tionery Office, London.
Plum F (1980) Brain death. Lancet ii, 379.Plum F, Posner JB (1980) Diagnosis of Stupor and Coma,
3rd edn. F A Davis, Philadelphia.Walton J, ed. (1977) Brain. In: Diseases of the Nervous Sys-
tem. Oxford University Press, Oxford.
NEUROLOGICAL ASSESSMENT AND EXAMINATION 13
KAY1 12/16/04 7:34 PM Page 13

Investigations to determine the exact diagnosisare nearly always necessary following the clinicalexamination. The following is a list of the morecommon investigations that may need to be undertaken:• cerebrospinal fluid (CSF) studies• radiological investigations• electroencephalography• nerve conduction studies• evoked potential studies• nuclear medicine investigations.
Some of these investigations will be describedin this chapter. The others will be dealt with in thechapters dealing with the relevant neurosurgicalproblems.
Cerebrospinal fluid investigation
The CSF is produced by the choroid plexus at a rate of approximately 0.4 ml per minute. The fluid circulates from the lateral ventriclesthrough the interventricular foramen (of Monro)into the 3rd ventricle, through the cerebral aque-duct of Sylvius into the 4th ventricle, and into thesubarachnoid space via the two laterally placedforamina of Luschka and a medial aperture in the roof of the 4th ventricle — the foramen of Magendie. The fluid circulates caudally into thespinal subarachnoid space, throughout the basalcisterns, up through the tentorial hiatus and thenover the cerebral hemispheres. It is absorbed bythe arachnoid villi of the dural sinuses, and espe-cially by the superior sagittal sinus. Approxi-mately 500 ml of CSF is produced each day. Thetotal CSF volume is 140 ml; the lateral ventriclescontain approximately 25 ml, the spinal cord
subarachnoid space 30 ml and the remainder ofthe fluid is found in the basal cisterns. Table 2.1shows the normal constituents of CSF.
The CSF glucose content is approximately 65%of the blood plasma level in the fasting state.There is a gradient for many of the constituents ofCSF along the cerebrospinal axis (Table 2.2).
The fluid is normally clear and colourless; itwill appear turbid if it contains more than 400white blood cells or 200 red blood cells per mm3.Yellow discolouration, xanthochromia, is due tothe breakdown products of red blood cells; thesefollow haemorrhage into the CSF.
CSF can be obtained by:• lumbar puncture• cisternal puncture• cannulation of the lateral ventricle.The fluid is usually obtained by lumbar punc-ture. Cisternal puncture is performed if the lumbar puncture has failed due to technical difficulties, if there is local skin sepsis or, in someradiology investigations, where it is the preferredroute of contrast administration for myelogra-phy. Ventricular puncture is usually only per-formed as an intraoperative procedure or fortemporary reduction of intracranial pressure inan emergency.
Lumbar puncture
The most common indications for CSF examina-tion by lumbar puncture are:• meningitis• subarachnoid haemorrhage• neurological diseases such as multiple sclerosis
CHAPTER 2
2 Neurosurgical investigations
14
KAY2 12/16/04 7:35 PM Page 14

• cytological examination for neoplastic disease• radiological imaging (e.g. myelography) orradio-isotope investigations• measurement of intracranial pressure.
The most important contraindication to lum-bar puncture is clinical evidence of raised in-tracranial pressure. Papilloedema is an absolutecontraindication and a lumbar puncture shouldnever be performed in a patient in whom an in-tracranial space-occupying lesion is suspected. Ifthere is any doubt a CT scan or MRI must be per-formed prior to lumbar puncture. A lumbarpuncture should not be performed if there is localinfection.
Technique of lumbar punctureThe patient should be positioned on the side, theback vertical on the edge of the bed and the kneesflexed up to the chest. The iliac crest is palpated;
this lies at the L3/4 level. The lumbar puncturecan be carried out at this space or at the spacesimmediately above or below. The area is pre-pared with antiseptic solution and draped. Theprocedure must be performed under completelysterile conditions. The interspinous area is pal-pated and the skin injected with 1–2 ml of 1% lig-nocaine local anaesthetic. The lumbar punctureneedle is inserted between the two spinousprocesses, pointing in a slightly cranial direction.If performed carefully it is usually possible to feelthe needle pass through the interspinous liga-ment and then through the dura. The stilette ofthe lumbar puncture needle is withdrawn and amanometer attached to measure the pressure.The fluid is drained into sterile containers andsent for examination.
Complications of lumbar punctureIf performed properly, with the appropriate indi-cations, lumbar puncture is well tolerated andcomplications should be minimal. However,there are several potential hazards and complica-tions; these include:• progression of brain herniation• progression of spinal cord compression• injury to the neural structures• headache• backache• infection — local and meningitis• implantation of epidermoid tumour (rare).
The potential risk of lumbar puncture worsen-ing brain herniation can be avoided if the proce-dure is not undertaken in patients with raisedintracranial pressure. Neurological deteriorationmay follow lumbar puncture and myelographyin patients with spinal tumours where there is se-vere cord compression. Although the proceduremay occasionally be necessary to make the diag-nosis, myelography should be avoided as mag-netic resonance imaging is the investigation ofchoice for spinal tumours. Neurological deterio-ration requires prompt surgery; this is discussedin Chapter 15. Infection should be avoided by theuse of scrupulous sterile techniques. If the proce-dure is performed at a level that is too high thereis a risk of neural damage, particularly to theconus medullaris. Rarely, a nerve root may be in-
NEUROSURGICAL INVESTIGATIONS 15
Table 2.1 CSF statistics (lumbar).
Volume 140 mlRate of production 0.4 ml/minPressure (recumbent) 10–15 cm of CSFCells Less than 3–4 white
cells/mm3
Protein 0.15–0.45 g/l (15–45 mg/100 ml)
Glucose 2.8–4.2 mmol/l (50–75 mg/100 ml)
IgG 10–12% of total proteinChloride 120–130 mmol/l
The values are expressed in SI (SystèmeInternationale) units and the correspondingtraditional units are in parentheses.
Table 2.2 CSF gradients along the cerebrospinalaxis.
Ventricle Cisternal Lumbar
Protein (g/l) 0.1 0.2 0.4Glucose (mmol/l) 4.5 4.0 3.4
KAY2 12/16/04 7:35 PM Page 15

16 CHAPTER 2
jured by the improper placement of the needle.Injury to a spinal radicular artery may occasion-ally give rise to a spinal subdural or epiduralhaematoma; this risk is increased if the patient istaking anticoagulation therapy.
The traumatic effects of the lumbar punctureare responsible for minor, transient low back dis-comfort. Very rarely, frank disc herniation hasbeen reported due to damage of the annulus fibrosus of the disc.
HeadacheThe most common complication of lumbar punc-ture is headache. In most cases this is due to lowCSF pressure that results from persistent leakageof the fluid through a hole in the arachnoid anddura. It is generally recommended that patientsshould remain flat for 12 hours following a lum-bar puncture to minimize the risk of this com-plication. The use of a narrow-gauge needle (20 gauge or less) and avoiding multiple punc-ture holes in the meninges also decreases thechance of troublesome postlumbar punctureheadache.
If the headache develops following mobiliza-tion the patient should be instructed to lie flat fora further 24 hours and encouraged to drink largevolumes of non-alcoholic fluids. Some cliniciansadvocate the use of ‘blood patch’ for the treat-ment of persistent postspinal headache. Thistechnique uses the epidural injection of autolo-gous blood at the site of dural puncture to form athrombotic tamponade which seals the duralopening, but this is usually unnecessary.
CSF examination
The CSF should be examined immediately. If thefluid is blood-stained it should be spun down in acentrifuge and examined for evidence of xan-thochromia, this being indicative of haemor-rhage into the CSF.
Three major pigments derived from red cellsmay be detected in CSF: oxyhaemoglobin, biliru-bin and methaemoglobin.
Oxyhaemoglobin is red, but after dilution itappears pink or orange. It is released by lysis ofred cells and may be detected in the CSF within 2
hours of the release of blood into the subarach-noid space. It reaches a maximum in the first 36hours and gradually disappears over the next7–10 days.
Bilirubin is yellow and is the iron-free deriva-tive of haemoglobin produced in vivo followingthe haemolysis of red cells. Bilirubin formation in the CSF probably depends on the ability of macrophages and other cells in the lep-tomeninges to degrade haemoglobin. It is firstdetected about 10 hours after the onset of subarachnoid bleeding and reaches a maximumat 48 hours. It may persist for 2–4 weeks after extensive haemorrhage.
Methaemoglobin is a reduction product ofhaemoglobin. It is a brown pigment that is darkyellow in dilution and it is characteristicallyfound in encapsulated subdural haematomas.Although it may be detected by spectrophotome-try of the spinal fluid in patients with large encapsulations of this sort, the pigment is notusually observed in other xanthochromic spinalfluids.
Xanthochromic spinal fluid may also occur injaundice, such as jaundice secondary to liver disease or in haemolytic disease of the newborn.
The fluid should be sent for microbiologicaland biochemical examination and, if clinically in-dicated, cytological examination for malignantcells.
The common abnormalities are shown in Table 2.3. Normal CSF contains no more thanfour lymphocytes or mononuclear cells per mm3.Polymorphonuclear cells are never found in nor-mal CSF but an isolated granulocyte, presumablyderived from blood at the time of lumbar punc-ture, may be seen if the CSF has been cytocen-trifuged. A granulocyte pleocytosis is thehallmark of bacterial infection; a granulocyticphase also occurs at the onset of a viral meningi-tis, prior to the development of a purely mononu-clear reaction.
Eosinophils are not seen in normal CSF. Themost common causes of prominent eosinophilicreaction are parasitic diseases, but eosinophiliamay also occur in inflammatory diseases and in arange of other diseases, as shown in Table 2.3.
Examination of the CSF using the polymerase
KAY2 12/16/04 7:35 PM Page 16

chain reaction (PCR) technique is useful in confirming the diagnosis of herpes simplex encephalitis (Chapter 12).
CSF electrophoresisElectrophoresis of the spinal fluid is useful in thediagnosis of patients suspected of having de-myelination. An IgG of over 15% of the total pro-tein is suggestive of disseminated sclerosis but itmay also be raised in autoimmune states, such asGuillain–Barré syndrome and carcinomatosis.Electrophoresis of the CSF may also demonstratemyeloma protein.
In addition to the absolute increase noted ingamma globulins in inflammatory diseases of thenervous system, qualitative changes in CSF
gamma globulins have been demonstrated in concentrated CSF with agarose gel elec-trophoresis and other gels. This techniquedemonstrates discrete bands in the gamma globulin pattern which have been called oligo-clonal bands. The term describes a population ofproteins, having identical electrophoretic charac-teristics derived from the same population of immunocompetent cells. A single antigen is presumed to give rise to a single band. Oligo-clonal bands are reported in about 90% of pa-tients with multiple sclerosis and are frequentlyobserved whenever CSF gamma globulin is increased due to a variety of inflammatory disorders of the nervous system. In patients withmultiple sclerosis the band pattern seems to be
NEUROSURGICAL INVESTIGATIONS 17
Table 2.3 CSF abnormalities.
CSF abnormality Disease suspected
Polymorphonuclear pleocytosis Bacterial meningitis
Mononuclear pleocytosis Viral meningitisTuberculous meningitisAcute demyelination
Eosinophils Parasitic infectionsTrichinella and AscarisToxoplasmaCysticercosis
Inflammatory diseasesTuberculosisSyphilisSubacute sclerosing panencephalitisFungal infections
Other diseasesLymphomaHodgkin’s diseaseMultiple sclerosis
Raised protein CNS infectionSpinal block (very high levels — Froin’s syndrome)Carcinomatosis of the meningesSpinal neurofibromasAcoustic neuromasGuillain–Barré syndrome
Low sugar Bacterial meningitis
Low chloride (<110 mmol/l) Tuberculous meningitis
KAY2 12/16/04 7:35 PM Page 17

18 CHAPTER 2
unique for each patient, and it remains stableover time.
Serological investigations for neurosyphilisshould be performed on the CSF if suspected.
Radiological investigations
The major radiological investigations are:• plain X-rays• CT scan• cerebral angiography• myelography• MRI.
Skull X-ray
The usefulness of the plain skull X-ray has beenlargely superseded by CT scanning. However, itis still a helpful preliminary investigation in patients with head injuries. The details of the useof this investigation in trauma are discussed inChapter 4.
The major abnormalities to look for on a skullX-ray are:• fractures• hyperostosis, e.g. meningioma• bone erosion due to skull vault tumours• midline shift of the pineal gland — from space-occupying lesion• abnormal calcification, e.g. tumours such asmeningioma, oligodendroglioma, craniopharyn-gioma or calcified wall of an aneurysm• signs of long-standing raised intracranial pres-sure — erosion of the dorsum sellae• ‘copper beating’ of the skull vault. Enhanceddigital markings are not uncommon under theage of 30 but may indicate long-standing raisedintracranial pressure if present over the wholevault.
Plain X-rays of the spine
These are useful preliminary investigations forpatients presenting with spinal pain. Particularnote should be taken of:• vertebral alignment• presence of degenerative disease with narrow-ing of the neural foramina and spinal canal
• evidence of metastatic tumour with erosion orsclerosis of the vertebral body, pedicles or lamina• enlargement of a neural foramen indicating aspinal schwannoma• congenital abnormalities such as spina bifida.
Computerized tomography scanning
Computerized tomography (CT) scanning wasintroduced in the 1970s and at that time revolu-tionized the radiological investigation of neuro-logical disease. Since then considerable technicaladvances have greatly improved the quality ofscanning which can now be performed in boththe axial (horizontal) and coronal planes. Sagittalreconstruction pictures can be obtained by com-puter manipulation of the data.
The CT scan is the initial investigation ofchoice in the investigation of nearly all intracra-nial diseases. Figure 2.1 shows the normal struc-tures seen in axial CT scans at various positionsthrough the cranium.
Intracranial calcification may be seen on theplain CT scan. Intracranial lesions that show cal-cification on the plain CT scan include:• meningioma — will also show hyperostosis ofcranial vault• most oligodendrogliomas• astrocytoma — 30% of low-grade tumours butinfrequently in high-grade tumours• ependymoma and subependymoma• craniopharyngioma• wall of giant aneurysm, arteriovenous malformations.
The pineal gland is usually calcified and calci-fication of the choroid plexus, basal ganglia andfalx may occur in normal scans.
Following a plain CT scan iodine-based con-trast medium is administered intravenously; thiswill enhance areas with increased vascularity orwith impairment of the blood–brain barrier. Thenon-ionic iodine agents have reduced the verysmall risk following intravenous administrationof contrast, the most serious side-effect being ananaphylactic reaction. Intracranial lesions thatenhance following contrast administration include:• high-grade cerebral gliomas
KAY2 12/16/04 7:35 PM Page 18

• meningiomas• acoustic neuromas• large pituitary tumours• metastatic tumours• arteriovenous malformations.
Cerebral abscesses usually enhance with a pe-ripheral ring. Low-grade gliomas often havescanty, if any, enhancement.
An intracranial mass will cause distortion ofthe lateral ventricles either as a result of the lesionitself or because of the associated cerebral oedema, which appears as an area of decreaseddensity around the lesion.
CT scanning of the spine is valuable in themanagement of:• lumbar disc prolapse• degenerative disease of the lumbar spine• lumbar canal stenosis• cervical disc prolapse• cervical canal stenosis
• spinal trauma• spinal dysraphism.
CT scanning, when combined with intrathecaliodine contrast, has been utilized as a usefulimaging technique for cervical disc prolapse buthas been superceded by MRI. This is discussed inChapter 14.
Cerebral angiography
Angiography of the intra- and extracranial ves-sels is now usually performed using com-puterized digital subtraction angiographictechniques. The procedure is usually done underlocal anaesthesia in the adult patient. Thecatheter is inserted into the femoral artery andthreaded up into the carotid or vertebral arteryorigin with the aid of an image intensifier.
Digital subtraction angiography has consi-derably reduced the complications of standard
NEUROSURGICAL INVESTIGATIONS 19
Sylvian fissure
3rd ventricle
Quadrigeminal cistern
Lateral ventricle
Parietal lobe
Occipital lobeFrontal hornof lateralventricle
Septumpellucidum
Pinealgland
Occipital hornof lateral ventricle
Corpuscallosum Sulci
Falx cerebri
Cerebellum4th ventricle
Mastoidair cells
Pons
Temporallobe
Frontalsinus
OrbitalroofChiasmatic
cistern
Midbrain
Quadrigeminal cistern
Frontal lobe
Temporal lobeFig. 2.1 Normal intracerebraland cranial structures on CTscan at various levels throughthe cranium.
KAY2 12/16/04 7:35 PM Page 19

20 CHAPTER 2
angiography, although there is still a very smallrisk of cerebral embolus from a clot or an athero-sclerotic plaque broken off by the catheter tip.
The major indications for angiography are:• investigation of cerebral ischaemia due tocarotid artery disease and intracranial atheroma• investigation of subarachnoid haemorrhage,e.g. cerebral aneurysm, arteriovenous malfor-mation• investigation of venous sinus thrombosis• preoperative embolization of meningioma.
Cerebral angiography is now only infrequen-tly used in the investigation of intracranial tumours. The major intracranial vessels areshown in Fig. 2.2.
Myelography
Myelography has been used in the past in the
investigation of spinal disease causing com-pression of the adjacent neural structures. Theuse of water-soluble contrast agents has made thetechnique safer and produces higher qualityimaging than was achieved with the previouslyused oil-based media. In particular, the dreadedcomplication of postmyelography arachnoiditisdoes not occur with water-based media. Compli-cations, which are now very uncommon, includeepileptic seizures, systemic reactions to the contrast medium and the risks of the lumbarpuncture itself. The major indications for myelography were:• cervical disc prolapse• lumbar disc prolapse• spinal tumour• cervical canal stenosis causing cervicalmyelopathy• lumbar canal stenosis.
Posterior cerebral
Anterior cerebral
Middle cerebral
Ophthalmic
Frontopolar
Anteriorcerebral
PericallosalCallosomarginal
Anterior choroidal
Posterior communicating
Middle cerebral arteryInternal carotid
(a)
Towne's view Lateral view
Posterior cerebralarteries
Basilar artery
Vertebral arteries
Superior cerebellar artery
Posterior inferior cerebellar artery
Posteriorcerebralartery
Anterior inferiorcerebellar artery
(b)
Fig. 2.2 The major intracranialvessels seen on cerebralangiography.
KAY2 12/16/04 7:35 PM Page 20

However, the advent of high-quality CT scan-ning and MRI have considerably reduced the in-dications for myelography. Myelography (oftencombined with CT) is now used occasionally forpatients with clinical features of cervical or lum-bar nerve root compression, such as due to discprolapse (often recurrent) or perineural fibrosis(that can follow previous surgery) and in whomthe MRI findings are equivocal and not diagnostic.
Magnetic resonance imaging
Magnetic resonance imaging (MRI) is a diagnos-tic radiological technique which utilizes the mag-netic properties of the body’s hydrogen nuclei toproduce cross-sectional images in any plane. Amoving charged particle creates a small magneticfield. At equilibrium the multiple tiny magneticfields created by the randomly spinning hydro-gen nuclei (protons) within the body cancel eachother out. If the body is placed within a strong ex-ternal magnetic field, the protons tend to alignthemselves within that field. If energy, in theform of pulses of electromagnetic waves of precisely the right frequency and band width(usually in the FM radio range), is introducedinto the body, the protons can be induced to spinin unison, or resonantly (Fig. 2.3). When the external energy source is removed, the energyfrom the excited protons is emitted in the form of
a radio signal, which progressively dies away. Although faint, the decaying signal can be detec-ted by sensitive antennae (receiver coils) placedstrategically in relation to the part of the bodybeing scanned. Initially, the strength of the signalis proportional to the distribution of the protonswithin the tissue. The rate of decay, or ‘relaxa-tion’, is dependent upon three factors.
The first is the efficiency with which energy istransferred from the protons to their imme-diately adjacent molecular lattice, or framework,which is described by an exponential curve withtime constant T1. Although this is commonlynamed ‘T1 relaxation time’, other eponyms usedinclude ‘longitudinal relaxation time’, ‘spin lat-tice relaxation time’ and ‘thermal relaxationtime’. The second factor contributing to signaldecay is the destructive interference of the pro-tons’ spins with each other. Because the protonsare exposed to minute differences in local mag-netic field, their spins become out of phase, re-sulting in loss of synchronization, or resonance.The rate of signal decay due to this factor is de-scribed by another exponential curve with timeconstant T2, which is commonly called ‘T2 relaxa-tion time’. It is also known as ‘horizontal relaxa-tion time’ and ‘spin–spin relaxation time’.
The third factor is ‘magnetic susceptibility’ of atissue. This refers to the ease with which tissuebecomes magnetized when placed in a strongmagnetic field. The induction of relatively stronglocal magnetic fields induces marked phase dispersal and signal loss. This phenomenon iscommonly exhibited by haematoma degrada-tion products such as deoxyhaemoglobin andhaemosiderin. Magnetic susceptibility is directlyproportional to the square of the magnetic field,so that a 1.5-tesla magnet is 25 times more sensi-tive to magnetic susceptibility than a 0.3-teslamagnet. The phenomenon is best exhibited at allfield strengths when gradient echo sequences areused.
Contrast between different tissues in MRI images is due to differences in proton concentra-tion, T1 and T2, magnetic susceptibility and flow.These differences can be maximized by varyingthe rate of the pulses of electromagnetic energy(TR, or pulse repetition time) and the time interval
NEUROSURGICAL INVESTIGATIONS 21
N N
SSFig. 2.3 The spinning protons are aligned in amagnetic field (left). An electromagnetic pulsedisplaces the protons (right).
KAY2 12/16/04 7:35 PM Page 21

22 CHAPTER 2
following the pulses at which the signal is record-ed (TE, or echo time).
In MRI studies of the CNS the T1-weightedscans show the anatomical structures in detail(Fig. 2.4) ; the CSF is black. The T2-weighted scansshow intracranial pathological processes, all ofwhich are associated with abnormal accumula-tions of water: the CSF is white, and fast-movingblood in arteries and venous sinuses is black. Asignificant exception to the rule that T2-weightedsequences depict the CSF as white is the sequenceknown as fluid-attenuated inversion recovery(FLAIR) which is a heavily T2-weighted se-quence, but has pulse timing such that normalCSF signal is dulled so that it appears black.Pathological accumulations of fluid still appearwhite against a predominantly grey background.The differential signal of moving blood is utilizedby subtracting out the static background to de-pict only blood vessels in a technique known asmagnetic resonance angiography (MRA). Theimages of the blood vessels are retained in thecomputer as a three-dimensional data stack,which allows viewing from any angle. The reso-lution of MRA is still inferior to that of digitalsubtraction angiography (DSA), but intravenouscontrast-enhanced MRA has partially bridgedthat gap.
Magnetic resonance spectroscopy (MRS) ex-ploits the empirical fact that the frequency withwhich protons spin (process) in space is directlyproportional to the magnetic field to which theyare exposed. Electrons have 800–1000 times themagnetic strength of protons. Thus protons indifferent molecules and even in different parts ofthe same molecule are exposed to very slightlydifferent net magnetic fields and therefore spin atvery slightly different frequencies. MRS mea-sures those differences in spin frequency and depicts them as a spectrum of peaks, with separation of the peaks measured in parts permillion. The resultant proton spectra show lac-tate peaks in areas of ischaemia or anaerobic metabolism, as seen in infarcts and malignant tumours. Decreased N-acetyl aspartate (NAA)levels indicate neuronal loss, and increasedcholine is seen in areas of increased membranetumour. The most sensitive results are obtained
by measuring a single voxel, but using spatiallyencoding gradients as is done with standardMRI, multiple voxels can be simultaneously examined. Individual peaks can be selected andtheir distribution shown as a coloured overlay onstandard MRI images. This technique is knownas chemical shift spectroscopy.
MRI, or nuclear magnetic resonance, has con-siderable potential advantages over CT scanningincluding:• no ionizing radiation• no bone artefact so that lesions around theskull base are clearly identified• high resolution.
Intravenous contrast medium using gadoli-nium compounds considerably enhances thevalue of MRI. These media are water-soluble andcross the abnormal blood–brain barrier in a man-ner similar to the iodine-based, water-solublecontrast media used in CT scanning. The para-magnetic compounds function by changing thelocal magnetic environment. The signal intensityof those hydrogen nuclei that are in direct contactwith the paramagnetic compounds is altered.The consequent shortening of the T1 relaxationtime results in an enhancement or brightening ofthe area.
Ultrafast image acquisition with echoplanarimaging (EPI) allows accurate measurement ofblood flow. The technique either utilizes a bolusof gadolinium contrast medium or detectschanges in the ratio of oxyhaemoglobin to deoxy-haemoglobin in stimulated portions of the brain(blood oxygen level-dependent imaging, orBOLD). BOLD allows accurate localization of arange of motor or sensory functions. Of particu-lar use in neurosurgery is the accurate de-lineation of the functional motor strip, which is
Fig. 2.4 Normal MRI. T1, T2 and magnetic resonancespectroscopy. (a) Axial T1 MRI through midponsshowing upper 4th ventricle. (b) Axial T1 MRI throughlower midbrain. (c) Axial T1 MRI showing cerebralpeduncles. (d) Axial T1 MRI showing symmetricalmidline lateral ventricles. (e) Axial T1 MRI showinghyperdense CSF in lateral ventricles and subarachnoidspace. (f) Midline sagittal T1 MRI. Arrow points to 4thventricle. Arrowhead shows genu of corpus callosum.
KAY2 12/16/04 7:35 PM Page 22

NEUROSURGICAL INVESTIGATIONS 23
(a) (b)
(c) (d)
(e)
(f)
KAY2 12/16/04 7:35 PM Page 23

24 CHAPTER 2
simply obtained by performing BOLD sequencesduring repetitive hand movements. This form ofimaging is sometimes named ‘functional MRI’(fMRI).
EPI obtains individual images in as little as 30milliseconds. Diffusion-weighted sequences are able to image actual water diffusion rate differences at the molecular level. Cytotoxic orcellular oedema results in restricted diffusion,which appears white in diffusion-weighted se-quences. Standard diffusion-weighted sequencesmeasure diffusion in all directions (isotropic diffusion). By applying gradients in at least sixdifferent directions, directionally restricted oranisotropic diffusion can be measured. Becausediffusion in axons is largely restricted to theirlongitudinal axes, white matter maps can be con-structed and superimposed on standard images.
The main disadvantage of MRI at present is itsrelative unavailability due to insufficient availa-bility of equipment. It is a valuable investigationin the following neurosurgical conditions.• Intracranial tumours — especially menin-gioma, acoustic neuromas, pituitary tumours,skull base tumours, metastases, lymphoma,meningeal infiltration (with gadolinium con-trast), glioma.• CNS infection — cerebral abscess, herpes sim-plex encephalitis.• Arteriovenous malformations.• Venous sinus thrombosis.• Craniospinal abnormalities such as the Chiarimalformation.• Syringomyelia.• Hippocampal or mesial sclerosis.• Spinal tumours.• Lumbar disc prolapse, lumbar canal stenosis.• Cervical cord compression — cervical myelo-pathy, cervical central disc prolapse.• Cervical disc prolapse.• Thoracic disc prolapse.
Radio-isotope studies
Isotope brain scanning for the initial diagnosis ofa cerebral tumour is now obsolete. However iso-tope scanning using the thallium isotope may behelpful in distinguishing a recurrent glioma from
radionecrosis, as the thallium will be taken upinto the tumour region. Radio-isotope cisternog-raphy is sometimes useful in the detection of thesite of CSF leakage following a fracture of theskull base. The technique is also sometimes usedto assess CSF flow in patients with communicat-ing hydrocephalus; reflux into the ventricularsystem, followed by slow clearance, suggestscommunicating or normal-pressure hydro-cephalus. However, the technique has been largely superseded by intracranial pressure monitoring.
Other highly sophisticated techniques usingradioisotopes, such as single photon emissioncomputerized tomography (SPECT) or positronemission tomography (PET), are used to mea-sure cerebral blood flow or cerebral metabolism.They are particularly useful in the evaluation ofpatients for epilepsy surgery (Chapter 21).SPECT utilizes single photon emitting radio-pharmaceuticals which distribute in the brain according to regional blood flow. Imaging is performed using a gamma camera and computeranalysis. PET utilizes positron-emitting isotopeswhich depend on a cyclotron for their productionand, in general, their short half-life dictates that acyclotron should be readily available. The scan-ning is of particular use in studying the relation-ship between cerebral blood flow, oxygenutilization and extraction in focal ischaemia or infarction. Both techniques have been used forthe investigation of epilepsy and to study the biological activity of brain tumours, especiallygliomas, in order to differentiate low-grade tumours from high-grade and post-radiationnecrosis from recurrent tumour.
Electroencephalography
Electroencephalography (EEG) records the spon-taneous electrical activity of the brain. The detailsare described in the chapter on epilepsy (Chapter21). The major indications for EEG recordings inneurological practice are:• suspicion of epilepsy in a new patient• assessment of epilepsy in a patient with recur-rent seizures• assessment of the risk of epilepsy in a patient
KAY2 12/16/04 7:35 PM Page 24

who has undergone intracranial surgery or fol-lowing a severe head injury• as an aid in the diagnosis of herpes simplex en-cephalitis and Creutzfeldt–Jakob disease.
Nerve conductionstudies/electromyography
The electrical activity within a particular muscle is recorded by needle electromyography.Nerve conduction studies measure the electricalactivity occurring within a particular nerve.
In electromyography a needle is inserted intomuscle and the electrical activity assessed; nor-mal muscle is electrically ‘silent’ at rest. As themuscle contracts motor unit potentials appear.This activity, which is seen on voluntary contrac-tion of the muscle, is known as the interferencepattern. Neuropathy or myopathy will producecharacteristic abnormalities.
Spontaneous activity at rest• Fibrillation potentials are due to single musclefibre contraction and indicate active denervation,e.g. neuropathy, motor neurone disease, somemyopathies.• Fasciculation — spontaneous contraction of abundle of muscle fibres.• Slow negative waves preceded by sharp posi-tive spikes — known as ‘positive sharp waves’ —in chronically denervated muscle.
Motor unit potentials• In neuropathy. Where there is significant dener-vation the surviving motor unit potentials arepolyphasic with large amplitude and long duration.• In myopathy the potentials are polyphasicwith small amplitude and short duration.
Interference pattern• Neuropathy — reduced interference due to diminished motor units.• Myopathy — interference pattern normal.Nerve conduction studies measure the latencyfrom the stimulus to the recording electrodes(distal latency), amplitude of the evoked re-sponse and conduction velocity. The studies areuseful in assessing:
• peripheral nerve injuries (Chapter 17)• peripheral nerve entrapment (Chapter 17)• brachial plexus injury (Chapter 17)• neuropathy• myopathy (studies are normal)• muscular dystrophy (studies are normal).
Evoked potentials
Visual, auditory and somatosensory evoked po-tential monitoring may be of value in the detec-tion of neurological and neurosurgical diseasesas well as providing useful intraoperative moni-toring. Stimulation of the sensory receptor willevoke a signal in the appropriate region of thecerebral cortex.
Visual evoked potentialThis involves retinal stimulation using either astroboscopic flash or an alternating checkerboardpattern. The evoked visual signal is recordedover the occipital cortex. It is particularly usefulin the diagnosis of multiple sclerosis. Intraopera-tive visual evoked potential monitoring has beenused by some neurosurgeons during pituitarysurgery to detect subtle interference with theoptic nerves and chiasm but the technique is notsufficiently developed for general use at thistime.
Brainstem auditory evoked potentialThis stimulates the auditory pathways in thevestibulocochlear cranial nerve and records theelectrical activity in the auditory cortex. The tech-nique has been used in the detection of smallacoustic neuromas but has been largely super-seded by high-quality MRI. Intraoperativerecording has been performed during acoustictumour surgery and microvascular decompres-sion operations but its use is limited.
Somatosensory evoked potentialThis involves sensory evoked potential recordingover the cortex in response to stimulation of a pe-ripheral nerve and has been used in the detectionof lesions within the sensory pathways, particu-larly the brachial plexus, spinal cord or brainstem. The technique is used in some
NEUROSURGICAL INVESTIGATIONS 25
KAY2 12/16/04 7:35 PM Page 25

26 CHAPTER 2
neurosurgical units during complicated spinaland vascular surgery as an additional intraopera-tive monitoring technique.
Further readingChien D, Edelman RR (1992) Basic principles and clini-
cal applications of magnetic resonance angiography(Review). Seminars in Roentgenology 27, 53–62.
DuBoulay GH (1965) Principles of X-Ray Diagnosis of theSkull. Butterworth, London.
Edelman RR, Warach S (1993) Magnetic resonanceimaging (Review I). New England Journal of Medicine328, 708–716.
Edelman RR, Warach S (1993) Magnetic resonanceimaging (Review II). New England Journal of Medicine328, 785–791.
Fishman RA (1980) Cerebrospinal Fluid in Diseases of theNervous System. W B Saunders, Philadelphia.
McComb JG (1983) Recent research into the nature ofcerebrospinal fluid formation and absorption. Journalof Neurosurgery 59, 369–383.
Stevens JM, Valentine AR (1987) Magnetic resonanceimaging in neurosurgery. British Journal of Neurosurgery 1, 405–426.
Taveras JM, Wood EH (1986) Diagnostic Neuroradiology,2nd edn. Williams & Wilkins, Baltimore.
KAY2 12/16/04 7:35 PM Page 26

Raised intracranial pressure
Raised intracranial pressure is a major clinicalfeature of many neurological illnesses. It is a mostimportant neurological condition, requiringprompt diagnosis and often needing urgent treatment.
Pathophysiology
The mechanisms of raised intracranial pressureare best understood by considering the normalphysiology of pressure within the intracranialcavity. The normal supine intracranial pressure is10–15 mmHg, measured at a position equal to thelevel of the foramen of Monro. The intracranialpressure is directly related to the volume of theintracranial contents within the skull. The basisof the Monro–Kellie doctrine is that the cranialcavity is a rigid sphere filled to capacity with non-compressible contents and that an increase in thevolume of one of the constituents will lead to arise in intracranial pressure. In 1783, AlexanderMonro (the third Monro to become Professor ofAnatomy in Edinburgh and the son of the manwho described the connection between the lateral and 3rd ventricles) published his observa-tions on the intracranial contents. Forty yearslater, Kellie made observations that appeared tosupport Monro’s hypothesis, although at thattime neither was aware of CSF. Subsequently, the Monro–Kellie doctrine has been generally accepted but with the qualification that the craniospinal intradural space is nearly constantin volume and its contents are nearly incompressible.
The intracranial contents are:• brain• CSF• blood.
The relative volumes of the contents are shownin Fig. 3.1. Raised intracranial pressure may bedue to:• increased volume of normal intracranial constituents• a space-occupying lesion.
The increase in volume of normal intracranialcontents may be due to:• brain
• cerebral oedema• benign intracranial hypertension
• CSF• hydrocephalus
• blood volume• vasodilatation due to hypercapnia.The increase in volume of intracranial contents
will determine the rise of intracranial pressure.Figure 3.2 shows the intracranial pressure–volume relationship. Initially, a small increase inthe volume of the intracranial contents causes norise in pressure; a small amount of CSF can moveinto the spinal subarachnoid space, which is veryslightly distensible. However, the skull being arelatively closed container, a critical volume issoon reached when a small rise in intracranialvolume will result in an exponential rise in pres-sure. The relationship of the volume to pressureis described in terms of compliance or elastanceof the intracranial space. Compliance is ex-pressed as dV/dP and is the amount of ‘give’available within the intracranial space. Elastanceis the inverse of compliance and is the resistance
CHAPTER 3
3 Raised intracranial pressureand hydrocephalus
27
KAY3 12/16/04 7:36 PM Page 27

28 CHAPTER 3
offered to expansion of a mass or of the brain it-self (Fig. 3.3). A brain that has a small degree ofcompliance, i.e. very little ‘give’ within the in-tracranial space, would be reflected by a smallchange in volume producing a large change in in-tracranial pressure. This is the situation on thevertical portion of the volume/pressure curve,where the compliance is said to be low and theelastance is high.
Experiments using Rhesus monkeys, and in-volving the gradual expansion of an extraduralballoon, showed that the vertical section of thecurve could be shifted to the left with either morerapid inflation of the balloon or pathologicalchanges, such as experimentally produced brainswelling, that reduced the amount of displace-able CSF before the balloon was expanded.
Cerebral blood flow
Between physiological ranges in blood pressure,the brain is able to maintain a constant cerebralblood flow. This is achieved by a process calledautoregulation whereby the brain adjusts the in-tracranial vascular resistance by altering vesseldiameter and tone. Following a severe cerebral
insult such as subarachnoid haemorrhage, thisability is compromised and the cerebral perfu-sion pressure (CPP) becomes virtually depen-dent on the mean arterial pressure. Normalcerebral blood flow is about 800 ml/min or 20%of the cardiac output. The cerebral blood flow is afunction of the CPP and the cerebral vascular re-sistance (CVR):
CBF = CPP/CVR
The cerebral perfusion pressure is a function ofthe systemic mean arterial pressure (MAP) andthe intracranial pressure (ICP):
CPP = MAP - ICP
Thus in order to maintain cerebral perfusion inthe presence of raised ICP, the systemic bloodpressure needs to be elevated.
ECF 100-150ml
Glia 700-900ml
Neurones 500-700ml
Blood 100-150ml
CSF 100-150ml
Fig. 3.1 The volume of the intracranial contents.
Volume
Intracranialpressure
Fig. 3.2 Intracranial pressure changes related to thevolume of the intracranial contents.
2
3
4
1
Fig. 3.3 Brain herniations. A lateral supratentorialmass will cause displacement of the lateral ventricleswith: (1) subfalcine herniation of the cingulate gyrusbelow the falx cerebri; (2) herniation of the uncus intothe tentorial hiatus; (3) caudal displacement of thebrainstem. Raised pressure within the posterior fossamay cause herniation of the cerebellar tonsils into theforamen magnum (4). (Adapted from Jennett &Teasdale (1981). Reproduced with permission.)
KAY3 12/16/04 7:36 PM Page 28

Cerebral herniation
Depending on the cause of the raised intracranialpressure or the position of the intracranial mass,brain herniae may occur as shown in Fig. 3.3. Thethree major herniations of the brain are describedas:1 Transtentorial.2 Foramen magnum.3 Subfalcine.
Transtentorial herniation involves displace-ment of the brain and herniation of the uncus ofthe temporal lobe through the tentorial hiatus,causing compression of the 3rd cranial nerve andmidbrain. The 3rd cranial nerve is affected, ini-tially on the ipsilateral side, and in most casescompression of the pyramidal tracts in the cruscerebri causes contralateral hemiparesis. How-ever, lateral displacement of the brainstem mayresult in the opposite crus cerebri being com-pressed against the sharp rigid tentorial edge, in-denting the crus (Kernohan’s notch), and causingan ipsilateral hemiparesis. Similarly, the posteri-or cerebral artery may be kinked, causing cerebral ischaemia resulting in a hemianopia.Compression of the brainstem and the reticularactivating system will result in a deterioration ofconscious state leading to coma, hypertensionand bradycardia (the Cushing response) and res-piratory failure, often being initially manifest byCheyne–Stokes periodic breathing (Table 3.1).
Increased pressure within the posterior fossa
will result in herniation of the cerebellar tonsilsinto the foramen magnum and compression ofthe medulla. If this is slowly progressive the pa-tient may develop an abnormal neck posture anda child with a posterior fossa tumour may have ahead tilt. Neck stiffness results from irritation ofthe dura around the foramen magnum. Com-pression of the medulla may cause rapid respira-tory failure, which is manifest as apnoea orabnormalities of respiratory rate and rhythm,such as Cheyne–Stokes breathing. These mayoccur without significant impairment of con-scious state. The pressure from the herniated ton-sils may cause abrupt limb paresis and sensorydisturbance.
Progressive raised intracranial pressure causesfurther downward herniation of the brainsteminto the foramen magnum or ‘coning’. This re-sults in shearing of the perforators supplying thebrainstem and haemorrhage within (Durethaemorrhages). The descent of the intracranialcontents with raised intracranial pressure causestraction damage to the pituitary stalk, resultingin diabetes insipidus. With progressive hernia-tion and destruction in the brainstem the pupilschange from dilated and fixed to midsize and un-reactive. These are invariably irreversible eventsleading to brainstem death.
Clinical symptoms and signs of raisedintracranial pressure
The common causes of raised intracranial pres-sure are:• space-occupying lesion — cerebral tumour(and oedema), abscess, intracranial haematoma• hydrocephalus• benign intracranial hypertension.The clinical features will be determined in largepart by the underlying cause of the raised pres-sure. However, some of the clinical symptomsand signs will be the same, no matter what thecause of the raised pressure. The major featuresare:• headache• nausea and vomiting• drowsiness• papilloedema.
RAISED INTRACRANIAL PRESSURE AND HYDROCEPHALUS 29
Table 3.1 Transtentorial herniation.
Compression of 3rd cranial nerve — causing initial dilatation of the ipsilateral pupil
Compression of the midbrainHemiparesis, usually contralateralOccasional compression of opposite crus
cerebri causes ipsilateral hemiparesisHypertension, bradycardia — Cushing responseRespiratory failure
Compression of posterior cerebral artery
KAY3 12/16/04 7:36 PM Page 29

30 CHAPTER 3
Headache. The headache associated with in-creased intracranial pressure is usually worse onwaking in the morning and is relieved by vomit-ing. Intracranial pressure increases during sleep,probably from vascular dilatation due to carbondioxide retention. The cause of the headache inraised intracranial pressure is probably tractionon the pain-sensitive blood vessels and compres-sion of the pain-sensitive dura at the base of thecranium.
Nausea and vomiting. The nausea and vomiting isusually worse in the morning.
Drowsiness. As is often repeated in this book,drowsiness is the most important clinical featureof raised intracranial pressure. It is the portent ofrapid neurological deterioration and must neverbe brushed aside as simply ‘sleepiness’, or disas-ter will almost certainly occur.
Papilloedema. The definitive sign of raised in-tracranial pressure, papilloedema is due to trans-mission of the raised pressure along thesubarachnoid sheath of the optic nerve. Theoedema of the nerve head, which may also be due to obstruction of axoplasmic flow, results initially in ‘filling in’ of the optic cup and dilata-tion of the retinal veins. The experienced obser-ver will be able to note that there is failure of thenormal pulsations of the retinal veins and venouscongestion. As the pressure rises the nerve headbecomes more swollen and the disc margins willbecome blurred on fundoscopic examination.Flame-shaped haemorrhages develop, particu-larly around the disc margins and alongside thevessels. In severe papilloedema ‘blob’ haemor-rhages and exudates appear. Long-standing pa-pilloedema from prolonged raised intracranialpressure will subsequently develop into secondary optic atrophy.
Cushing reflex. As intracranial pressure rises, inorder to maintain a constant CPP, there has to bea compensatory rise in the systemic blood pressure. A hypertensive response is thereforeelicited which is classically associated with abradycardia. This is termed the Cushing reflex in
honour of the eminent neurosurgeon HarveyCushing who first described it.
Sixth nerve palsy, causing diplopia, may occur inraised intracranial pressure due to stretching ofthe 6th nerve by caudal displacement of thebrainstem. This is a so called ‘false localizing’sign, as it need not occur on the side of the primary lesion.
In an infant, raised intracranial pressure willcause a tense, bulging fontanelle.
Other clinical manifestations of raised in-tracranial pressure may result from brain hernia-tion, as described above, and from the masslesion that has caused the rise in pressure.
Measurement of intracranial pressureMonitoring and recording the intracranial pres-sure was first described in the early 1960s byLundberg and Langfitt and within a decade wasbeing extensively used in clinical practice. The in-dications for monitoring the intracranial pres-sure vary considerably in neurosurgical practice.The most common indications are:• Head injury (Chapter 4).• Following major intracranial surgery, whenmeasurement of the intracranial pressure mayhelp in the management of patients. In particular,after posterior fossa surgery early detection of aprolonged rise in intracranial pressure will indi-cate evolving hydrocephalus and the possibleneed for a CSF shunt or ventricular drain.• In the assessment of dementia and benign in-tracranial hypertension, described later in thechapter.
The major abnormalities in the pressure are:• elevation of the baseline intracranial pressure• the development of pressure waves.
Normal intracranial pressure has a baseline be-tween 10 and 15 mmHg, with small pulsationsdue to respiration and the cardiac pulse. The nor-mal amplitude of the combined cardiac and res-piratory variation is approximately 3–5 mmHg.As the intracranial pressure increases the pulsepressure will increase. When the pressure israised abnormal pressure waves may occur.‘Plateau’ waves, described by Lundberg as ‘A’waves, are pressure waves above 50 mmHg and
KAY3 12/16/04 7:36 PM Page 30

last at least 5 minutes, but often up to 20 minutes.They are always pathological and are probablydue to increased cerebral blood flow and bloodvolume. ‘B’ waves are smaller in height and havea short duration (1–2 minutes) (Fig. 3.4). If theyare infrequent and of low amplitude they may bea normal finding.
The intracranial pressure may be recordedfrom the ventricle, brain substance, subdural orextradural space. The intracranial catheters areattached by a transducer to a continuousrecorder. There are now numerous monitoringdevices with various degrees of technical sophis-tication. Every method has its own particular advantages and complications and the type ofmonitoring performed will depend on the clini-cal situation (e.g. size of the ventricles) and theneurosurgeon’s preference. The major complica-tion from intracranial pressure monitoring is in-fection and the risk is directly proportional to theduration of the monitoring.
Management of raised intracranial pressureThe treatment of raised intracranial pressure willdepend on the underlying cause. The definitivetreatment involves removing the cause. This may
involve resection of a space-occupying lesion, orin the case of hydrocephalus, a CSF shunt.
In an emergency situation, when the patienthas become comatose and has failing respiration,it is essential that the patient’s ventilatory state isurgently maintained and this will necessitate thepassage of an endotracheal tube and ventilatorysupport. While the patient is being transferred fordefinitive treatment of the raised pressure it maybe possible to temporarily lower the intracranialpressure by hyperventilation which will reducearterial CO2 and diminish vasodilatation, and bythe administration of a diuretic such as mannitolor frusemide (furosemide) (Chapter 4).
Hydrocephalus
Hydrocephalus is an abnormal enlargement ofthe ventricles due to an excessive accumulationof CSF resulting from a disturbance of its flow,absorption or, uncommonly, secretion. The nor-mal volume of CSF is 140 ml. CSF is produced bythe choroid plexus in the ventricles at a rate of0.4 ml per minute (or about 500 ml in 24 hours).The CSF flows from the lateral ventricles throughthe foramen of Monro into the 3rd ventricle, viathe aqueduct of Sylvius into the 4th ventricle andthen through the foramina of Magendie andLuschka into the subarachnoid space and basalcisterns. The CSF circulates throughout thespinal subarachnoid space and the basal cisternsup through the tentorial hiatus. It flows over thecerebral hemispheres and is largely absorbed bythe arachnoid villi of the dural sinuses. There area number of ways of classifying hydrocephalusbut the most useful classification system is:• obstructive hydrocephalus — when there is anobstruction to the flow of CSF through the ven-tricular system• communicating hydrocephalus — when thereis no obstruction to the flow of CSF within theventricular system but the hydrocephalus is dueeither to obstruction to CSF flow outside the ven-tricular system or to failure of absorption of CSFby the arachnoid granulations.
The most common causes of hydrocephalusare:1 Obstructive hydrocephalus:
RAISED INTRACRANIAL PRESSURE AND HYDROCEPHALUS 31
Fig. 3.4 Intracranial pressure waves. (a) ‘A’ waves, orplateau waves, are elevations of intracranial pressureabove 50 mmHg lasting 5–20 minutes. (b) ‘B’ waveshave a smaller amplitude and short duration.
(a)
(b)
KAY3 12/16/04 7:36 PM Page 31

32 CHAPTER 3
(a) lateral ventricle obstruction by tumours,e.g. basal ganglia glioma, thalamic glioma(b) 3rd ventricular obstruction, due to colloid cystof the 3rd ventricle or glioma of the 3rd ventricle(c) occlusion of the aqueduct of Sylvius (eitherprimary stenosis or secondary to a tumour)(d) 4th ventricular obstruction due to posteriorfossa tumour, e.g. medulloblastoma, ependy-moma, acoustic neuroma.
2 Communicating hydrocephalus:(a) obstruction to flow of CSF through the basalcisterns(b) failure of absorption of CSF through thearachnoid granulations over the cerebral hemispheres.The most common causes of communicating
hydrocephalus are infection (especially bacterialand tuberculous) and subarachnoid haemor-rhage (either spontaneous, traumatic or postoperative). Other uncommon causes are car-cinomatous meningitis, increased CSF viscosityfrom a high protein content and excessive secre-tion of CSF due to a choroid plexus papilloma.
Presenting features
Hydrocephalus in infantsThe incidence of infantile hydrocephalus is ap-proximately 3–4 per 1000 births and most casesare due to congenital abnormalities. The inci-dence of hydrocephalus occurring as a singlecongenital disorder is 1–1.5 per 1000 births. Hy-drocephalus occurring with spina bifida andmyelomeningocele varies from 1.5 to 2.9 per 1000births, but with prenatal screening and folatesupplementation the incidence of spina bifida isdecreasing (Chapter 11).
The most common congenital cause is stenosisof the aqueduct of Sylvius. This is a major causeof hydrocephalus in children with spina bifidaand myelomeningocele who also have a Chiaritype II malformation (Chapter 11). Congenitalatresia of the foramen of Luschka and Magendie(Dandy–Walker cyst) is a rare cause. The ac-quired forms of hydrocephalus occur most fre-quently after intracranial bleeding, particularlyin premature infants, in meningitis and becauseof tumours. The marked improvements in the
survival of very low birth weight premature in-fants has resulted in an increase in infants withhydrocephalus resulting from perinatal intracra-nial haemorrhage.
Hydrocephalus can present as acute raised in-tracranial pressure but because of the relative dis-tensibility of the infant skull the presentation canbe more subtle.
The major clinical features in infants are:• failure to thrive• failure to achieve milestones• increased skull circumference (compared withnormal growth curves)• tense anterior fontanelle• ‘cracked pot’ sound on skull percussion• transillumination of cranial cavity with stronglight• when severe, impaired conscious level andvomiting• ‘setting sun’ appearance due to lid retractionand impaired upward gaze from 3rd ventricularpressure on the midbrain tectum• thin scalp with dilated veins.
Adult hydrocephalus (Fig. 3.5)Adult patients with hydrocephalus may presentwith either:
Fig. 3.5 Hydrocephalus of the lateral and 3rdventricles due to aqueduct stenosis.
KAY3 12/16/04 7:36 PM Page 32

• acute onset and deterioration or• gradual onset and slowly progressive deterioration.
Acute-onset adult hydrocephalusThis type of presentation occurs particularly inpatients with tumours causing obstructive hy-drocephalus, although it may occur with any of the causes of hydrocephalus and an acuterapid neurological deterioration may occur in pa-tients who have had long-standing chronic hydrocephalus.
The major presenting features are due to thesigns and symptoms of raised intracranial pres-sure as described earlier:• headache• vomiting• papilloedema• deterioration of conscious state.Upgaze will often be impaired due to pressure ofthe dilated 3rd ventricle on the superior collicu-lus of the tectum.
Gradual-onset adult hydrocephalusThis type of onset occurs less frequently than theprevious type in patients with obstructive hydro-cephalus due to a tumour. The symptoms ofraised intracranial pressure are only very gradu-ally progressive and late diagnosis is common.Early features in the adolescent involve deter-iorating school performance as a result ofheadaches, failing mental function, memory lossand behavioural disturbances. Endocrine abnor-malities such as infantilism and precocious puberty can occur in association with chronic hydrocephalus in older children and adolescentsdue to disturbance of the hypothalamus and pos-sible compression of the pituitary gland. If thecondition is unrecognized progressive visual failure will occur, secondary to papilloedema andoptic atrophy. As mentioned earlier, acute de-compensation may occur and the patient maysuddenly develop a rapid deterioration of con-scious state.
In elderly patients a chronic form of hydro-cephalus is called ‘normal-pressure hydro-cephalus’; this is described later in the chapter.
Radiological investigation
The most important investigation is either a CTscan (Fig. 3.5) or MRI of the brain (Fig. 3.6) whichwill show which ventricles are dilated. If the lateral ventricles and 3rd ventricle are all very di-lated, and the 4th ventricle is small, it is likely thatthe obstruction is at the level of the aqueduct ofSylvius. An enhanced CT scan or MRI will helpdetermine the cause, as it will better define thepresence of an obstructing tumour. In a communi-cating hydrocephalus all the ventricles are dilated.
Magnetic resonance imaging. In the sagittal planeMRI is particularly helpful in showing aqueductstenosis and lesions around the 3rd ventriclecausing obstructive hydrocephalus.
Ultrasonography. Ultrasonography through theopen anterior fontanelle is useful in assessingventricular size in infants and may obviate theneed for repeated CT scans.
Plain skull X-ray. May demonstrate splayed sutures, erosion of the bony buttresses aroundthe tuberculum sellae or a ‘copper beaten’ appearance to the inside of the calvarium.
Records of the head circumference and its com-parison with body weight and length centilecharts are an integral part of postnatal follow-upof any child.
Treatment
In general, the treatment of hydrocephalus is aCSF shunt or a 3rd ventriculostomy. If there hasbeen rapid neurological deterioration this willneed to be performed as an emergency.
If the hydrocephalus is due to an obstructingtumour that is surgically accessible, resection ofthe mass may lead to resolution of the hydro-cephalus and a shunt might not be necessary.
Arrested hydrocephalus. This is a state of chronichydrocephalus in which the CSF pressure has returned to normal and there is no pressure gradient between the cerebral ventricles andbrain parenchyma. It is uncommon and is mostlikely to occur in communicating hydrocephalus.The patients, often children and adolescents,should be followed carefully with neurologicalexaminations, IQ tests and careful assessment of
RAISED INTRACRANIAL PRESSURE AND HYDROCEPHALUS 33
KAY3 12/16/04 7:36 PM Page 33

34 CHAPTER 3
their development. If there is any deterioration ofthose parameters a shunt will be necessary.
It is interesting to briefly review the history ofsurgical treatment of hydrocephalus, as this com-mon neurosurgical problem has only relativelyrecently been solved. Until early this century nu-merous remedies had been employed, includingblood-letting, head-wrapping and repeated ven-tricular taps. In 1918 Walter Dandy introducedthe technique of excising the choroid plexus todecrease the formation of CSF in patients withprogressive hydrocephalus. In 1922 he describedan operation of 3rd ventriculostomy, in which ahole was made in the thinned floor of the 3rd ventricle creating a fistula into the chiasmatic cisterns. Subsequently, the procedure was performed through the lamina terminalis. In 1939Torkildsen introduced the ventriculocisternos-tomy to treat hydrocephalus caused by lesionsobstructing the outflow from the 3rd ventricle. Athin rubber tube was inserted into the lateral ven-tricle through an occipital burr hole and passedsubcutaneously into the cisterna magna.
All these procedures had significant limita-tions, risk of morbidity and substantial failurerates. The extracranial shunting procedures re-lied on the development of flow-directed valves,allowing CSF to flow in one direction without re-flux through the catheter. This type of valve wasinvented by an engineer, Holter, and was firstused in 1952. Subsequently, numerous improve-ments and modifications have been made and atpresent there are a large variety of reliable shuntdevices.
Operative procedureThe usual method of CSF diversion is a ventricu-loperitoneal shunt, in which a catheter is placedinto the lateral ventricle and is connected to asubcutaneous unidirectional pressure-regulated
Fig. 3.6 MRI demonstrating obstructivehydrocephalus. (a) Axial T1 MRI showing dilatedlateral ventricles. (b) Axial T2 MRI showinghyperdense CSF in lateral ventricles. (c) Coronal T1
MRI with arrow pointing to dilated 3rd ventricle.
(a)
(b)
(c)
KAY3 12/16/04 7:36 PM Page 34

valve which is attached to a catheter threadedsubcutaneously down to the abdomen and in-serted into the peritoneal cavity. Alternativedrainage sites such as the atrium, pleural cavityand ureter have now been largely abandoned, except in exceptional circumstances. Modernvalves can have their draining pressures adjustedpercutaneously and shunts are being developedallowing intracranial pressure to be monitoredpercutaneously.
Technique of ventriculoperitoneal shunt (Fig. 3.7).The operation is performed under general anaes-thesia and the shunt is usually inserted on theright side, so as to avoid interference with thedominant hemisphere. The head is turned to the left on the neurosurgical headrest. The head,neck, chest and abdomen are shaved, preparedwith antiseptic solution and draped. It is absolutely essential to maintain the most strictsterile techniques to avoid the serious complica-tion of infection of the shunt. A small curvilinearincision is made in the parieto-occipital area anda small skin flap elevated. The peritoneal cavity isopened, either through a transverse rectus split-ting incision in the right hypochondrium orthrough a midline incision. A burr hole is per-formed, the lateral ventricle cannulated and theventricular catheter inserted into the lateral ven-tricle so that its tip lies in the frontal horn of the
lateral ventricle, anterior to the choroid plexus.Insertion of the catheter in this way minimizesthe other major complication, shunt obstruction.As one of the major causes of obstruction of theventricular catheter is blockage by the choroidplexus it is wise to place the perforations of thecatheter into the frontal horn. The peritonealcatheter can be threaded subcutaneously be-tween the abdominal and cranial wounds usingone of many devices. Each catheter is joined tothe valve, which is then sutured in place. Afterchecking that the system is functioning properly,the peritoneal catheter is placed within the peri-toneal cavity.
There are numerous shunt systems and thetype of shunt used, the particular clinical situa-tion and the neurosurgeon’s own preference re-sult in many modifications of this basic system ofimplanting a ventriculoperitoneal shunt.
Postoperative careThe postoperative management is similar for anyintracranial procedure. Initially the patient isnursed flat, to avoid rapid decompression of theventricular system. Deterioration of neurologicalstate or failure to improve will require an urgentCT scan to confirm that the catheter has beenplaced accurately into the ventricular system andto exclude the possibility of intracranial compli-cations such as intracerebral haematoma.
Complications of ventriculoperitoneal shuntThe major possible complications are:• infection of the shunt• obstruction of the shunt• intracranial haemorrhage.
Shunt infection is a dreaded complication withpossible disastrous consequences, particularly inpatients who are shunt dependent. Avoidance ofthis complication is aided by:• meticulous sterile technique, including the useof a ‘no touch’ technique of the shunt and totalavoidance of skin contact with the shunt• intraoperative prophylactic antibiotic medication.
InfectionThe use of intraoperative prophylactic antibiotics
RAISED INTRACRANIAL PRESSURE AND HYDROCEPHALUS 35
Subcutaneouscatheter
Catheter in theperitoneal cavity
Valve locatedin burr hole
Ventricular catheterin lateral ventricle
Fig. 3.7 Diagram of ventriculoperitoneal shunt.
KAY3 12/16/04 7:36 PM Page 35

36 CHAPTER 3
during shunt placement is relatively well sub-stantiated. Although the continuation of the anti-biotics for 24–36 hours postoperatively has notbeen proven to be effective, it is a reasonable pre-caution. An infected shunt almost invariablyneeds to be removed and replaced by a newshunt, preferably in a different position andunder appropriate antibiotic cover.
ObstructionThe shunt may fail to perform satisfactorily dueto blockage of the ventricular catheter, malfunc-tion or blockage of the valve or obstruction of theperitoneal catheter. The patient will usually pre-sent with recurrent symptoms of raised intracra-nial pressure and in some cases there may be analarmingly rapid deterioration of neurologicalstate. Auseful clinical sign in the less acute case ofshunt malfunction is failure of upgaze due topressure of the distended 3rd ventricle on the su-perior colliculus. The diagnosis will usually beconfirmed by CT scan. Compression of the valveis often helpful in determining the position of theobstruction. If the ventricular catheter is blockedthe contents of the pump can be expressed but thevalve will refill slowly. If the block lies in thevalve or the peritoneal catheter the valve is usually not compressible.
The treatment of a malfunctioning shunt is ex-ploration and revision of the component that isnot functioning adequately.
Intracranial haemorrhageIntracranial haematomas may occur followingthe insertion of a ventriculoperitoneal shunt andmay be either:• intracerebral or• subdural.
The intracerebral haematoma will be due to thetrauma of the passage of the ventricular catheter.Subdural haematomas are particularly likely tooccur in patients with long-standing severe hy-drocephalus. If there is a sudden decompressionof the ventricular system the cortical mantle willfall away from the cranial vault; this may causerupture of a bridging vein and the developmentof a subdural haematoma. Consequently, pa-tients thought to be particularly at risk should
initially be nursed lying flat and should be ele-vated gradually. Some neurosurgeons use shuntsthat incorporate an antisiphon device to decreasethe possibility of a ‘siphoning’ effect causing fur-ther reduction of intracranial pressure.
Other CSF shuntsAlso used sometimes are:• ventriculoatrial shunts• ventriculopleural shunts• lumboperitoneal shunts.
The ventriculoatrial shunt, in which the distalend is placed through the internal jugular veininto the right atrium, is occasionally necessarywhen there has been marked intraperitoneal sep-sis or multiple abdominal operations. It will occa-sionally be necessary to place the shunt into thepleural cavity.
The lumboperitoneal shunt involves drainageof the CSF from the lumbar theca rather than the ventricle. This type of shunt can only be con-sidered in patients with communicating hydro-cephalus. A catheter is threaded percutaneouslyinto the lumbar theca and then tunnelled subcu-taneously to the anterior abdominal wall andplaced into the peritoneal cavity. The techniquehas the theoretical advantage that the brain is notmanipulated, but the disadvantage is that theshunts are not as reliable and are more difficult toassess if the patient develops symptoms resem-bling malfunction of the shunt.
Third ventriculostomyIn recent years this old technique, originally performed by Walter Dandy in 1922, has beenreintroduced for treatment of obstructive hydrocephalus using an endoscopic technique. Aventriculoscope is introduced into the lateralventricle via a frontal burr hole and advancedthrough the foramen of Monro. The floor of the3rd ventricle just anterior to the mamillary bodiesis then fenestrated, allowing CSF to bypass anyobstruction in the CSF pathway and be reab-sorbed by the arachnoid villi.
Normal-pressure hydrocephalus
Normal-pressure hydrocephalus was first de-
KAY3 12/16/04 7:36 PM Page 36

scribed as a clinical entity by Hakim and Adams in1965. They described a group of patients withsymptoms of dementia, ataxia and incontinence,where the radiological studies showed hydro-cephalus but the lumbar CSF pressure was normal.
Aetiology
The exact cause of the ventricular dilatation can-not be defined in every case. However, in a largepercentage the communicating hydrocephalusmay have resulted from obliteration of the subarachnoid pathways in the basal cisterns fol-lowing an episode of meningitis or subarachnoidhaemorrhage, from either rupture of ananeurysm, arteriovenous malformation or fol-lowing trauma.
Although lumbar puncture pressure is, by definition, within the normal range, continuousmonitoring of the intracranial pressure in thesepatients will frequently reveal abnormal waveformation, especially at night.
Clinical presentation
The classic clinical ‘triad’ consists of:1 Dementia.2 Ataxia.3 Incontinence.
The syndrome is progressive and the distur-bance of gait, which may be the first and mostprominent symptom, is more of an apraxia than atrue gait ataxia. Urinary incontinence is commonbut not universal. The dementia is similar to thatseen in Alzheimer’s disease, with profound lossof short-term memory. The patient does not usually complain of headaches.
Investigations
The CT scan or MRI will show dilated ventricleswithout significant cortical atrophy. The diffi-culty arises that normal-pressure hydrocephalusmay occur in patients with a scan appearance ofcortical atrophy, but in these patients the degreeof ventricular dilation should be more thanwould be expected just to compensate for the degree of atrophic change.
Other investigations, including isotope cis-ternography, neuropsychological assessmentand CSF infusion studies, have been used. Theseinvestigations have a high failure rate in predict-ing which patients will benefit from a CSF shunt.Abnormal isotope cisternography, with pro-longed ventricular retention of isotope and slightor delayed flow over the cerebral convexity, is as-sociated with improvement following shuntingin only a half to two-thirds of cases of normal-pressure hydrocephalus. Improvement in symp-toms after lumbar puncture and removal of CSFfluid may be a good prognostic sign but failure toimprove does not exclude the diagnosis.
Continuous intracranial pressure monitoringis a useful technique as it will exclude patientswith low intracranial pressure and make a defi-nite diagnosis in those patients with intermittentwaves of raised intracranial pressure, whichoccur particularly at night. However, some pa-tients with intracranial pressure in the high normal range will also benefit from a CSF shunt.
Treatment
The major difficulty in the treatment of normal-pressure hydrocephalus is in deciding which patient should be shunted. Dementia is a devastating disease with disastrous effects forthe patient and profound social consequences forthe patient’s family and the general community.It is not surprising that the neurosurgeon is fre-quently asked to consider patients for a shuntwhere the diagnosis is far from certain. The slimchance that an operative procedure might be ofsome benefit is often considered worthwhile bythe patient and their relatives. The following cri-teria can be used to assess those patients with thegreatest chance of improvement following ashunt.• A clinical presentation of the classic triad, par-ticularly if the features of gait disturbance predominate.• The CT scan or MRI showing marked hydro-cephalus with minimal cortical atrophy.• A clearly defined cause for the hydrocephalus,such as a past episode of subarachnoid hae-morrhage, trauma or meningitis.
RAISED INTRACRANIAL PRESSURE AND HYDROCEPHALUS 37
KAY3 12/16/04 7:36 PM Page 37

38 CHAPTER 3
• Abnormal pressure waves on continuous in-tracranial pressure monitoring.
Naturally, a patient who has all these positivecriteria deserves a shunt and should make a goodrecovery following the operation. However, theusual situation is a patient who presents withonly a few of these criteria and the neurosurgeonneeds to make a careful assessment of whether ashunt is truly appropriate.
Operative procedureThe usual operation is a ventriculoperitonealshunt preferably with a programmable valve.
If the diagnosis has been correct and the shuntworks satisfactorily, the patient can make a strik-ing recovery with almost complete resolution ofsymptoms.
Benign intracranial hypertension
Benign intracranial hypertension, also known aspseudotumour cerebri, is, as its name implies, a disease of raised intracranial pressure whichusually runs a self-limiting course. Althoughtermed ‘benign’, this condition can cause blind-ness due to severe papilloedema. The pathogene-sis is poorly understood. The condition usuallyoccurs in obese females.
Aetiology
The aetiology is generally poorly understood andthe exact mechanisms of the raised pressure arenot known. The condition is found typically in young, obese women, often with menstrual irregularities or taking an oral contraceptive pill,and an endocrine disturbance has been sugges-ted. However, careful endocrine studies havefailed to show significant endocrine abnormali-ties. In a minority of patients a definite precipitat-ing cause is found; these include:• hypoparathyroidism• vitamin A excess (used to treat acne)• pernicious anaemia• drug reaction — tetracycline, nalidixic acid,sulfamethoxazole, indomethacin, danazole, lithium carbonate, oral contraceptive steroids.
A similar condition results from venous sinus
thrombosis. Prior to antibiotic therapy chronicmastoiditis was a cause of pseudotumour cerebrias a consequence of spread of inflammation tothe sigmoid and lateral sinuses. This is now a relatively rare occurrence but recent studies haveshown that an ‘occult’ venous sinus thrombosismay play a role in the development of benign intracranial hypertension.
Presenting features
Most patients are obese females who present with:• headaches• visual disturbance.
The headaches have the features of raised in-tracranial pressure in that they are worse in themorning and exacerbated by straining, stoopingand coughing.
The visual problems result from:• papilloedema• secondary optic atrophy• diplopia due to 6th cranial nerve palsy.
The papilloedema may be severe and the visual fields will show enlargement of the blindspot. Obscurations of vision may occur, particu-larly on standing or stooping, and the swelling ofthe optic discs may be so severe as to lead to visu-al failure and associated secondary optic atrophy.
An unusual but well-recognized complicationof benign intracranial hypertension is sponta-neous CSF rhinorrhoea, usually associated withthe empty sella syndrome (Chapter 8).
Investigations
The CT and/or MRI scan will show no cause forthe papilloedema and the ventricles will often besmaller than usual.
Digital subtraction cerebral angiography ormagnetic resonance venography may be per-formed to exclude thrombosis of a venous sinusas the cause.
If the CT scan or MRI shows no mass or lesiona lumbar puncture is usually performed; thepressure will be raised. CSF examination is nor-mal in benign intracranial hypertension but bio-chemistry and cytological investigations shouldbe performed to exclude underlying pathology.
KAY3 12/16/04 7:36 PM Page 38

If there is doubt as to the diagnosis continuousintracranial pressure monitoring is occasionallyperformed in order to assess the level of intracra-nial pressure.
Treatment
Benign intracranial hypertension is usually aself-limiting disease and most cases respond tosimple conservative treatment. The usual mea-sures undertaken are:• weight loss (the patients are usually obese)• stopping any medication that may have led tothe disease, e.g. oral contraceptives, tetracycline• diuretic therapy• acetazolamide (reduces CSF production).
Visual acuity, visual field examination (espe-cially size of the blind spot) and fundal photogra-phy are essential to evaluate the progress of thedisease. If there is no improvement with theabove measures, treatment with glycerol orsteroids may be tried. However, both of thesemedications will tend to increase obesity. Someclinicians recommend serial lumbar puncturesbut this is of limited value as the formation of CSFquickly replaces any that is withdrawn.
The major indications for surgical treatmentare:• persistent severe papilloedema despite con-servative measures• failing vision• intractable headaches despite conservativemeasures.
The surgical procedures that can be performedare:• optic nerve sheath decompression• lumboperitoneal shunt.
If the symptoms are primarily visual andheadache is not a problem then optic nervesheath decompression may be useful. In this pro-cedure a small window of dura is excised fromthe optic nerve sheath to decompress the opticnerve head. If this procedure is not successful inimproving papilloedema or reversing the failingvision, or if headaches are a major component ofthe disease, then a lumboperitoneal shunt can beperformed. This operation is usually highly ef-fective in reversing the symptoms and in improv-
ing the papilloedema. Recently endovascularstenting of the narrow regions of the transversesinus has been suggested as a treatment, but itssafety and efficacy are as yet unproven in largeclinical trials.
Further readingAdams RD et al. (1965) Symptomatic occult hydro-
cephalus with normal cerebrospinal fluid pressure: atreatable syndrome. New England Journal of Medicine273, 117–126.
Beks JWF, Bosch DA, Brock M (1976) Intracranial Pressure III. Springer Verlag, Berlin.
Black P McL (1980) Idiopathic normal pressure hydro-cephalus. Journal of Neurosurgery 52, 371–377.
Corbett JJ et al. (1982) Visual loss in pseudotumour cerebri. Archives of Neurology 39, 461–474.
Greer M (1968) Management of benign intracranial hypertension (pseudotumour cerebri). Clinical Neurosurgery 15, 161–174.
Hakim S, Adams RD (1965) The special clinical problemof symptomatic hydrocephalus with normal cere-brospinal fluid pressure: Observations on cerebrospinal fluid hydrodynamics. Journal of Neurological Science 2, 307–372.
Jefferson A, Clark J (1976) Treatment of benign intracra-nial hypertension by dehydrating agents with partic-ular reference to measurement of the blind spot as ameans for recording improvement. Journal of Neurology, Neurosurgery and Psychiatry 39, 627–639.
Jennett B, Teasdale G (1981) Management of Head Injuries. Contemporary Neurology Series. F A Davis,Philadelphia.
Kaye AH, Black P McL (2000) Operative Neurosurgery.Churchill Livingstone, London, New York, Edinburgh.
Langfitt TW et al. (1964) Transmission of intracranialpressure. I. Within the cranio-spinal axis. Journal ofNeurosurgery 21, 989–997.
Langfitt TW et al. (1964) Transmission of intracranialpressure. II. Within the supratentorial space. Journalof Neurosurgery 21, 998–1005.
Nulsen FE, Spitz EB (1952) Treatment of hydrocephalusby direct shunt from ventricle to jugular vein. Surgical Forum 2, 339–343.
Shulman K et al. (1980) Intracranial Pressure. IV. SpringerVerlag, Berlin.
Torkildsen A (1939) A new palliative operation in casesof inoperable occlusion of the sylvian aqueduct. ActaChirurgica Scandinavica 82, 117–119.
RAISED INTRACRANIAL PRESSURE AND HYDROCEPHALUS 39
KAY3 12/16/04 7:36 PM Page 39

Head injuries are a major cause of morbidity andmortality in the community. Trauma is the thirdmost common cause of death in the UnitedStates, exceeded only by cardiocerebral vasculardisease and cancer. Trauma is the leading causeof death in youth and early middle age and thedeath is often associated with major head trau-ma. Head injury contributes significantly to theoutcome in over half of trauma-related deaths.There are approximately 2.5 deaths from head injury per 10 000 population in Australia andneurotrauma causes approximately 3.5% of alldeaths. Road traffic accidents are responsible forabout 65% of all fatal head injuries in Australia.
There is a wide spectrum of head injury frommild concussion to severe brain injury resultingin death. The management of the patient follow-ing a head injury requires the identification of thepathological processes that have occurred.
Pathophysiology of head injury
The management of head injury has been basedon the concept of primary and secondary braininjury. The primary brain injury was defined asthe irreversible pathology sustained at the timeof the trauma, whereas the secondary brain in-jury has been considered the subsequent or pro-gressive brain damage that occurs due to anevolving pathology following the injury. It hasbeen the general contention that the primary injury is irreversible, and management should be directed at preventing or treating secondarypathology (such as cerebral swelling, hydroceph-alus and intracerebral haematoma). However, it is now clear that some of the biochemical
events associated with what was considered irre-versible brain injury are potentially preventable,or even reversible if treatment is instituted earlyenough. The distinction between primary andsecondary injury has become blurred, and theterms, whilst useful concepts, are now becomingobsolete.
Most head injuries result from blunt trauma, asdistinct from a penetrating wound of the skulland brain caused by missiles or sharp objects.The pathological processes involved in a head injury are:• direct trauma• cerebral contusion• intracerebral shearing• cerebral swelling (oedema)• intracranial haemorrhage• hydrocephalus.
Direct trauma. Although penetrating injuries pro-duce most of their damage by direct trauma tothe brain this is not the case with blunt injuries, inwhich the energy from the impact has a morewidespread effect.
Cerebral contusion. This may occur locally underthe position of the impact although it usually oc-curs more severely at a distance from the area ofimpact as a result of a ‘contre-coup’ injury. As thebrain is mobile within the cranial cavity the sud-den acceleration/deceleration force will result inthe opposite ‘poles’ of the brain being jammedagainst the cranial vault. A sudden blow to theback of the head will cause the temporal lobes to slide across the floor of the middle cranial fossa and the frontal lobes across the floor of the
CHAPTER 4
4 Head injuries
40
KAY4 12/16/04 7:36 PM Page 40

anterior cranial fossa, causing contusion on theundersurface of those lobes and to the temporaland frontal poles of the brain as they strike thesphenoid ridge and frontal bones, respectively.Cerebral contusion consists of lacerated haemor-rhagic brain, and a ‘burst temporal lobe’ may re-sult when the temporal pole has been severelyinjured.
Shearing forces. Intracerebral shearing forcesoccur as a result of the differential brain move-ment following blunt trauma, frequently in con-junction with a contre-coup type of injury. Therotational acceleration following injury willcause shear forces that result in petechial haem-orrhages (particularly in the upper brainstem,cerebrum and corpus callosum), and tearing ofaxons and myelin sheaths. The early pathologicalchanges consist of retraction balls or microglialscars, and if the patient lives for a number ofmonths before death then widespread degenera-tion of myelin will be apparent at postmortem.
Cerebral swelling. This occurs following trauma,either in a focal pattern around an intracerebralhaematoma or diffusely throughout the cere-brum and/or cerebellum. The nature of thepathological processes are not clearly under-stood but involve a disturbance of vasomotortone causing vasodilatation and cerebral oedema. In addition, cerebral contusion and petechial haemorrhages will contribute to thebrain swelling.
Intracranial haemorrhage. Intracranial haemor-rhage following trauma is discussed in more detail in Chapter 5 and may be:• intracerebral• subdural• extradural.
The intracranial haematoma or cerebralswelling may cause the types of cerebral hernia-tion described in Chapter 3. The medial surface ofthe hemisphere may be pushed under the falx(subfalcine), the uncus and hippocampal gyrusof the temporal lobe may herniate through thetentorium causing pressure on the 3rd nerve andmidbrain (Fig. 4.1), or there may be a caudal dis-
placement of the brainstem and/or cerebellum,herniating into the foramen magnum.
Hydrocephalus. This occurs infrequently in theearly stages after a head injury. It may be due to obstruction of the 4th ventricle by blood,swelling in the posterior fossa, or the result of atraumatic subarachnoid haemorrhage causingobstruction to the absorption of CSF and result-ing in a communicating hydrocephalus. This lat-ter type of hydrocephalus is an uncommon, butimportant, cause of delayed neurological deterio-ration either in the weeks following the head injury or some years later (see ‘Normal-pressurehydrocephalus’, Chapter 3).
Concussion
Concussion involves an instantaneous loss ofconsciousness as a result of trauma. The term‘concussion’ was introduced by Pare and is de-rived from the Latin ‘concutere’ which means toshake. In 1941 Denny-Brown and Russell showedthat concussion was produced by a blow on thecranium when it was free to move and subse-quent studies showed that the acceleration/de-celeration of the head resulted in shear strains,contre-coup injury, petechial and punctate haem-orrhages throughout the brainstem, cerebralhemispheres and corpus callosum, and neuronalinjury, the extent depending on the force of the
HEAD INJURIES 41
Midbraindistorted
Posteriorcerebralartery
Transtentorialherniation of uncus oftemporal lobe
3rd nervedeformed
Frontal lobe
Temporal lobeHaematoma
Fig. 4.1 Herniation of the uncus and hippocampalgyrus of the temporal lobe into the tentorial notchcausing pressure on the 3rd nerve and midbrain.(Adapted from Jennett & Teasdale, 1981. Reproducedwith permission.)
KAY4 12/16/04 7:36 PM Page 41

42 CHAPTER 4
impact. The term concussion is not strictly de-fined with respect to the severity of the injury.However, a minimum criterion is that the patientwill have had a period of amnesia. The retro-grade amnesia of most cerebral concussion isusually short term, lasting less than 1 day. Theinitial retrograde amnesia may extend over amuch longer period but it gradually shrinksdown. A more reliable assessment of the severityof the head injury is the post-traumatic amnesia.If the amnesia following the head injury lastsmore than 1 day then the concussion is regardedas being severe.
Associated injuries
Cranial nervesThe cranial nerves may be injured as a result of either direct trauma by the skull fracture, movement of the brain, or cerebral swelling.
The olfactory nerves. These are the most commonlyaffected and this may be as a result of either a fracture through the anterior cranial fossa, directly affecting the tracts, or tearing of the delicatenerve rootlets passing through the cribriformplate caused by the sudden brain movement,particularly from a blow to the back of the head.
The 8th nerve. Damage to this nerve is often asso-ciated with a fracture of the petrous temporalbone. Deafness may be conductive, due to ahaemotympanum, or sensorineural as a result of injury to the inner ear or to the nerve itself. Vertigo and nystagmus are due to vestibularnerve or end-organ damage and usually resolvewithin a few months of the injury.
Facial paralysis. This is usually associated with afracture through the petrous temporal bone, although this may only be evident on a high-resolution CT scan using the bone ‘window’. Itmay be either immediate, as a result of directcompression of the nerve, or delayed, due tobleeding and/or swelling around the nerve.
The 6th cranial nerve. This has a long course fromthe brainstem to its entry into Dorello’s canal and
the nerve is easily damaged by torsion or hernia-tion of the brain.
The 3rd nerve. This may also be damaged by directtrauma or by brain herniation, the herniateduncus of the temporal lobe either impinging onthe midbrain or directly stretching the nerve.
The optic nerve. This is infrequently injured by direct trauma.
Skull fracturesTrauma may result in skull fractures which areclassified as:• simple — a linear fracture of the vault• depressed — when the bone fragments are depressed beneath the vault• compound — when there is a direct communi-cation with the external environment. This mayresult from either a laceration over the fracture ora fracture of the base of the skull which will becompound because there will be a direct connec-tion outside the vault, usually via the air sinuses.
Scalp lacerationsThe extent of the scalp laceration does not neces-sarily indicate the degree of trauma to the under-lying brain.
Other injuriesThe most common associated injuries are to thechest, skeletal and cardiovascular systems.
Initial management of head injury
The key aspects in the management of patientsfollowing head injury involve:• accurate clinical assessment of the neurologi-cal and other injuries• determination of the pathological process involved• the concept that a change in the neurologicalsigns indicates a progression or change in thepathological processes.
Immediate treatment at the site of the injury involves a rapid restoration and maintenance ofan adequate airway, ventilation, essential circu-latory resuscitation, first aid treatment of other
KAY4 12/16/04 7:36 PM Page 42

injuries and the urgent transfer of the patient to hospital. It is essential to avoid hypoxia andhypotension as these will cause further brain injury.
Clinical assessment
It is fundamental to the management of the patient to know of changes in the neurologicalcondition as soon as possible. It is essential to ascertain the type of accident that caused thehead injury and the time injury occurred. An accurate assessment of the patient’s initial neurological condition, albeit in non-medicalterms, can be obtained from bystanders at the siteof the accident or from the ambulance officers.
Neurological examinationAn accurate neurological examination will helpto determine the type and position of the patho-logical process and provide a baseline for comparison with subsequent examinations. Although a full neurological examination shouldbe undertaken, special emphasis should be givento the:• conscious state• pupillary size and reaction• focal neurological signs in the limbs.
The conscious stateIf the patient will respond verbally an assessmentshould be made of the retrograde amnesia andpost-traumatic amnesia.
There is a continuum of altered consciousnessbetween those patients who are alert and respond appropriately to verbal command andthose who are deeply unconscious. The first signof a depressed conscious state is drowsiness, atwhich time the patient may be easily arousableand orientated in time, place and person. As thelevel of consciousness deteriorates the patientwill become confused and more drowsy. Theterm ‘coma’ is generally restricted to patientswho show no response to external stimuli, do notobey commands, are unable to utter comprehen-sible words, and do not open their eyes. How-ever, the use of the words ‘coma’, ‘semicoma’ or‘stuporose’ should be avoided, as they convey
different meanings to different observers. The assessment is more accurate and reproducible if either the exact nature of the response is described or, more simply, the Glasgow comascale is used.
The Glasgow coma scale (Table 4.1) gives a nu-merical value to the three most important para-meters of the level of consciousness — opening ofthe eyes, best verbal response and best motor response. The exact response can be representedon a chart (Fig. 4.2) or the level of conscious-ness given as a numerical score — the sum of thethree parameters of the Glasgow coma scale. Ascore of 8 or less indicates a severe injury.
Pupillary size and reactionCareful evaluation of the pupil size and responseto light is essential at the initial clinical assess-ment and during further observation. Raised intracranial pressure causing temporal lobe her-niation will cause compression of the 3rd nerve,resulting in pupillary dilatation, which nearly always occurs initially on the side of the raisedpressure. The pupil will at first remain reactive tolight but subsequently will become sluggish andthen fail to respond to light at all. As the intra-cranial pressure increases this same process com-mences on the contralateral side. A traumaticmydriasis will also result from direct trauma to the eye, and the dilated pupil should not beconfused with that due to a 3rd cranial nervepalsy.
Disorders of ocular movement occur followinghead injury as a result of injury to an extraocularmuscle or its nerve supply, or due to disturbanceof the conjugate gaze centres and pathways. Adestructive lesion of either a frontal or pontinegaze centre results in tonic overaction of the opposite frontal–pontine pathway for horizontaleye movement, causing ipsilateral deviation ofthe eyes with a frontal lobe lesion and contralat-eral gaze deviation with pontine lesions. Theoculocephalic manoeuvre and caloric stimula-tion are important tests of functional activity ofthe brainstem reticular formation.
The oculocephalic response should only beperformed after a cervical spine fracture has beenexcluded. The head is raised 30° and rotated from
HEAD INJURIES 43
KAY4 12/16/04 7:36 PM Page 43

44 CHAPTER 4
side to side in the horizontal plane. In the normalresponse the eyes maintain their position in spaceby moving opposite to the rotation of the head.The afferent impulses are from the cervical nerveroots and the semicircular canals.
Caloric testing should also be performed withthe head elevated 30° so that the horizontalcanals are positioned in the vertical plane. Irriga-tion with ice-cold water causes ipsilateral tonicgaze deviation.
Skew deviation involves divergence of theeyes in the vertical plane and is a sign of a lesionwithin the brainstem.
Ocular bobbing occurs only after a very severehead injury resulting in pontine damage.
Focal neurological signs in the limbsNeurological examination of the limbs will as-sess the tone, power and sensation. A hemipare-sis will result from an injury of the corticospinaltract at any point from the motor cortex to thespinal cord. Following a severe brain injury thelimbs may adopt an abnormal ‘posturing’ atti-tude. The decerebrate posture consists of theupper limbs adducted and internally rotated
against the trunk, extended at the elbow andflexed at the wrist and fingers, with the lowerlimbs adducted, extended at the hip and kneewith the feet plantar flexed. There is a continuumof severity of brain injury with the decerebrateposturing response being partial and unilateraland occurring only as a result of a painful stimu-lus to severe continuing bilateral decerebraterigidity. The posture probably results from anupper brainstem injury. Less frequently, theupper limbs may be flexed, probably due to theinjury predominantly involving the cerebralwhite matter and basal ganglia — correspondingto a posture of decortication.
Particular attention must be given to the pa-tient’s ventilation, blood pressure and pulse. Atall times it is essential that care is taken to ensurethe patient’s ventilation is adequate. Respiratoryproblems may result either as a direct manifesta-tion of the severity of the head injury or due to anassociated chest injury. Cheyne–Stokes breathingis due to either intrinsic brainstem damage orraised intracranial pressure causing pressure anddistortion of the brainstem. Bradycardia and hypertension, the Cushing response, are also
Table 4.1 The Glasgow coma scale.
Parameter Response Numerical value
Eye opening Spontaneous 4To speech 3To pain 2None 1
Best verbal response Orientated 5Confused 4Inappropriate 3Incomprehensible sounds 2None 1
Best motor response to painful stimulus Obeys commands 6Localize to pain 5Flexion to pain — withdrawal 4Flexion — abnormal 3Extension to pain 2None 1
TOTAL 3–15
KAY4 12/16/04 7:36 PM Page 44

HEAD INJURIES 45
Fig. 4.2 The standard observation chart used at the Royal Melbourne Hospital and at many major traumacentres. The chart incorporates the Glasgow coma scale.
KAY4 12/16/04 7:37 PM Page 45

46 CHAPTER 4
both indicative of brainstem compression due to raised intracranial pressure (Chapter 3).
Pyrexia frequently occurs following a head injury. A temperature lasting for more than 2days is usually due to traumatic subarachnoidhaemorrhage or may occur in patients with a severe brainstem injury.
General examinationCareful assessment must be made of any other injuries. Chest, skeletal, cardiovascular or intra-abdominal injury must be diagnosed and the ap-propriate management instituted. Hypotensionor hypoxia may aggravate the brain injury, and, ifsevere, will themselves cause brain damage.
Radiological assessment
Following the clinical evaluation radiological assessment will be essential unless the injury has been minor. The CT scan will show themacroscopic intracranial injury and should beperformed where:• there is loss of consciousness (post-traumaticamnesia) of greater than 10 minutes• the patient is persistently drowsy or has amore seriously depressed conscious state• there is persisting nausea or vomiting• there are lateralizing neurological signs• there is neurological or focal deterioration• there is skull fracture• there is CSF rhinorrhoea• there are associated injuries which will entailprolonged ventilation so that ongoing neurologi-cal assessment is difficult.
The CT scan will clearly show the presence ofintracerebral or extracerebral haematoma, as wellas cerebral contusion, oedema and infarction.Small ‘slit’ ventricles and absence of the basal cisterns will indicate generalized brain swelling.
The indications for a skull X-ray have dimin-ished since the introduction of the CT scan, espe-cially as the bony vault can be assessed by the CTscan using the bone ‘windows’. If a CT scan hasnot been performed, a skull X-ray is obligatory ifthere has been any loss of consciousness or if themechanism of injury is suggestive of an underly-ing fracture.
Cerebral angiography is indicated if a carotico-cavernous fistula is suspected by the presence of a bruit over the orbit or by pulsating prop-tosis. Carotid or vertebral angiography will benecessary if arterial dissection is considered apossibility.
NB Full radiological assessment of the cervi-cal spine utilizing plain X-ray and CT scan is essential in patients who have sustained a significant head injury, particularly if there areassociated facial injuries.
Further management of head injury
Following the clinical and radiological assess-ment the subsequent management will dependon the intracranial pathology and the extent ofany neurological injury.
Minor head injury
The patient would be assessed as describedabove. Any patient who has suffered a head injury must be observed for at least 4 hours. Thefollowing are the minimal criteria for obligatoryCT scan and admission to hospital:• loss of consciousness (post-traumatic amne-sia) of greater than 10 minutes• persistent drowsiness• focal neurological deficits• skull fracture• persisting nausea or vomiting after 4 hours’observation• intracranial pathology noted on a CT scan• if the patient does not have adequate care athome.
The further management of these patients willbe careful observation; the neurological observa-tions should be recorded on a chart displayingthe features of the Glasgow coma scale. If therehas been a period of significant loss of conscious-ness, or if the patient is drowsy, then the follow-ing measures should be instituted to minimizethe development of cerebral swelling:• elevation of the head of the bed 20°• mild fluid restriction to 2–2.5 l/day in an adult.
Should the patient’s neurological state deterio-rate an immediate CT scan is essential to re-
KAY4 12/16/04 7:37 PM Page 46

evaluate the intracranial pathology; further treatment will depend on the outcome.
Severe head injury
The management of a patient following a severehead injury depends on the patient’s neurologi-cal state and the intracranial pathology resultingfrom the trauma. In general, the following apply.1 The patient has a clinical assessment and CTscan as described previously.2 If the CT scan shows an intracranialhaematoma causing shift of the underlying brain structures then this should be evacuatedimmediately.3 If there is no surgical lesion, or following theoperation, the management consists of:
(a) Careful observation using a chart with theGlasgow coma scale.(b) Measures to decrease brain swelling; theseinclude:
(i) careful management of the airway to en-sure adequate oxygenation and ventilation.Hypercapnia will cause cerebral vasodilata-tion and so exacerbate brain swelling(ii) elevation of the head of the bed 20°(iii) fluid and electrolyte balance.Maintenance of isotonic fluid requirements,
avoiding dextrose solutions and following resuscitation should be administered until thepatient is able to commence nasogastric feed-ing. Blood loss from other injuries should be replaced with colloid or blood and not withcrystalloid solutions. Care should be taken toavoid overhydration, as this will increase cere-bral oedema.
Following general injury there is retention ofsalt and water and excretion of potassium. Theretention of water is usually greater than theretention of sodium, resulting in mild hypo-natraemia. Following a severe head injuryfluid and electrolyte abnormalities may occurfor a variety of reasons. Severe hyponatraemia(sodium less than 130 mmol/l) may be due toexcessive fluid intake or, occasionally, becauseof inappropriate excessive secretion of antidi-uretic hormone (SIADH). The urine is usuallyhypertonic with a high sodium level, probably
as a result of suppression of aldosterone secretion occurring as a response to overhy-dration and expansion of the circulating vol-ume. The term ‘cerebral salt wasting’, whichhas been applied to this syndrome, is usuallyinappropriate.
Serum sodium of less than 125 mmol/l mayproduce neurological impairment with de-pression of conscious state. If due to SIADHthe usual treatment is to restrict fluid intake to800 ml per day or less.
Hypernatraemia is usually associated withhyperosmolality and often results from inade-quate fluid intake. Other causes are diabetesinsipidus, as a result of hypothalamic injuryand excessive use of osmotic agents for controlof intracranial pressure. Excessive administra-tion of some feeding mixtures may lead to electrolyte abnormalities, particularly whencomplicated by diarrhoea.(c) Temperature control — pyrexia may be dueto hypothalamic damage or traumatic sub-arachnoid haemorrhage. However, infection asa cause of the fever must be excluded. The mostcommon sites of infection after a head injuryare the respiratory and urinary tracts, particu-larly if a urinary catheter has been inserted. Ifthe injury is compound, and especially if therehas been a CSF leak, intracranial infectionshould be suspected. The temperature can usually be controlled using tepid sponges, and rectal paracetamol or aspirin. Chlorpromazine, to abolish the shivering response, should beadministered if a cooling blanket is required.Every attempt should be made to control thetemperature because hyperthermia can elevatethe intracranial pressure, will increase brainand body metabolism and will predispose toseizure activity. Although hypothermia hasbeen advocated in the management of a severehead injury no clear-cut benefit has beendemonstrated.(d) Nutrition — during the initial 2–3 days thefluid therapy will include 1.5–2 l of 4–5% dextrose, providing 250–400 calories per day.Proper nutritional support should be com-menced after 3–4 days. Feeding at this stage is best done by intragastric administration,
HEAD INJURIES 47
KAY4 12/16/04 7:37 PM Page 47

48 CHAPTER 4
usually by a nasogastric tube, unless this is precluded by other injuries. The nasogastricfeeding should supply 2500–3000 calories perday with a calorie : nitrogen ratio of 180 : 1. The feeding should commence slowly, with dilute mixtures, and the stomach should be aspirated regularly to prevent regurgitationand pulmonary aspiration.(e) Routine care of the unconscious patient including bowel, bladder and pressure care.More aggressive methods to control intra-
cranial pressure are advisable if:• the patient’s neurological state continues todeteriorate and the CT scan shows evidence ofcerebral swelling without an intracranialhaematoma• there is a posturing (decerebrate) response tostimuli• the Glasgow coma score is less than 8.
In these patients an intracranial pressure monitor should be inserted to assess the intracra-nial pressure as accurately as possible. A trans-ducer can be placed intraparenchymally via atwist drill craniostomy. A catheter placed into theventricle will give an accurate reading of the intracranial pressure and CSF can be drained tohelp in the control of the pressure. However, thedisadvantages of an intraventricular catheter in-clude difficulty of placement if the ventricles aresmall, possible injury to the brain during place-ment and infection resulting in ventriculitis following prolonged monitoring. A subduralcatheter will also give an adequate measurementof the intracranial pressure but may be difficultto insert satisfactorily if the brain is swollen, and will tend to block. Extradural monitors areless accurate, although satisfactory recordingsare obtainable with meticulous placement technique.
An intracranial pressure monitor will also beuseful in patients requiring prolonged sedationand ventilation as a result of other injuries. Measurement of the intracranial pressure willprovide another useful monitoring parameterand any sustained rise in the pressure will be anindication for careful reassessment and, if neces-sary, CT scan.
Following the insertion of the intracranial
pressure monitor the patient will be transferredto the intensive care department. The techniquesused to control intracranial pressure are as follows.• Controlled ventilation, maintaining PaCO2 at30–35 mmHg. Reduction of the PaCO2 will reducecerebral vasodilatation and consequently de-crease the intracranial pressure.• If the pressure remains elevated despite hyper-ventilation CSF can be drained from a ventricularcatheter if this has been inserted.• Diuretic therapy utilizing intermittent admin-istration of mannitol or frusemide (furosemide)can be used if the preceding techniques havefailed to control the intracranial pressure. Manni-tol is an osmotic diuretic and may also exert its effect by increasing serum osmolality and draw-ing water out of the brain. The usual dose is0.5–1.0 g/kg. The serum osmolality should notexceed 320 mosmol/kg.• Barbiturate therapy can be considered if the in-tracranial pressure is resistant to treatment withthe above techniques. Pentobarbitone (thiopen-tone) when given as a bolus dose (3–5 mg/kg) isfrequently effective in temporarily reducing theintracranial pressure. There is probably littlevalue in using barbiturate infusion at a dose tocontrol burst suppression on EEG, although ithas been postulated that this provides brain protection by reducing cerebral metabolism.• Steroids. Although steroids dramatically re-duce the oedema around cerebral tumours theyhave little effect in controlling the brain swellingfollowing a head injury. Steroid medication is nolonger considered advisable as there is no provenbenefit for the patient and possible complica-tions, such as gastrointestinal bleeding, poorwound healing and infection, may result fromtheir administration.• Hypothermia. In some centres hypothermia(to reduce cerebral metabolism and intracranialpressure) has been advocated, with cooling thepatient to 34°C. However there is no clear evi-dence it is beneficial.• Hyperbaric oxygen has been used in the past,but without proven benefit.
Decompressive craniotomy involving re-moval of a large area of cranial vault from the
KAY4 12/16/04 7:37 PM Page 48

frontal and temporal regions bilaterally has beenadvocated as a means of controlling raised intracranial pressure due to severe cerebralswelling following a head injury. The techniqueis controversial, but it needs to be performedearly following the injury if it is to have a chanceof being of benefit to the patient. At present thereare no clinical trials proving its efficacy in headinjury.
There is some controversy concerning the effectiveness of the more aggressive techniquesto treat patients with severe head injuries. If a patient has suffered a profound brain injury andthe neurological examination shows little or noremaining brainstem function then it is obviousthat the aggressive techniques will provide nobenefit and only delay the inevitable. Similarly,there are some patients who have suffered a se-vere head injury and whose intracranial pressurecontinues to rise despite all the above techniques.Other patients will have a fatal brain injury with-out any substantial rise in intracranial pressure,usually when the brainstem has been the primarysite of injury. However, about 30% of patientswho have suffered a severe brain injury will obtain substantial benefit from control of the intracranial pressure. Clinical studies have notyet conclusively proven the value of intracranialpressure control in reducing morbidity followinga brain injury as it is thought that the patients inthe studies that were performed were overventi-lated and the cerebral blood flow might havebeen compromised. There is now consensus thata reduction in raised intracranial pressure willnot only decrease the mortality but will improvethe quality of the patient’s outcome after a severehead injury.
Cerebral perfusion pressure is a vital physio-logical parameter in the management of severelyhead injured patients. The cerebral perfusionpressure — mean arterial BP minus mean in-tracranial pressure — should be maintainedabove 70 mmHg. Consequently head injury man-agement involves ensuring that the arterial bloodpressure is maintained whilst the intracranialpressure is reduced. This often involves close cooperation between the neurosurgeon and theintensive care physician.
Management of associated conditions
Scalp injuryScalp injuries may include:• abrasion• confusion• laceration• subgaleal haematoma.
A large scalp laceration may result in consider-able blood loss. When the patient arrives in the emergency department ‘spurting’ arteriesshould be controlled with haemostatic clips priorto the application of a sterile bandage to the head.The extent of the soft tissue scalp injury may notreflect the severity of the underlying brain injury.The principles of management are similar tothose of soft tissue injury at other sites of the bodyand the wound should be closed without delay.
The hair should be shaved widely around thewound, which should be meticulously cleanedand debrided. The closure should be performedin two layers if possible, with careful appositionof the galea prior to closing the skin. The skin sutures should approximate the cut edges of theskin and care should be taken to avoid excessivetension which would cause skin necrosis andwound breakdown.
Straightforward, clean scalp lacerations cannearly always be closed with local anaesthetic infiltration. However, if the scalp wound has resulted in loss of soft tissue the wound may need to be extended to provide an extra ‘flap’ of healthy tissue so that the skin edges can be approximated without tension.
Skull fracturesSimple linear fracture. There is no specific manage-ment for a simple skull fracture that is undisplaced without an overlying skin injury.However, the presence of a fracture is an indica-tion that the trauma was not trivial and it shouldprovide a warning that a haematoma may develop beneath the fracture. The patient should be admitted for observation and CT scanperformed.
Compound fracture. A skull fracture may be compound either because of an overlying scalp
HEAD INJURIES 49
KAY4 12/16/04 7:37 PM Page 49

50 CHAPTER 4
laceration or if it involves an air sinus. The scalp wound should be debrided and closed asdescribed above. A short course of prophylacticantibiotics should be administered to reduce therisk of infection.
Depressed skull fracture (Fig. 4.3). A skull vaultfracture is considered to be significantly de-pressed if the inner table fragments are depressedby at least the thickness of the skull. About halfthe injuries are due to road trauma and most ofthe remainder are due either to objects falling onthe head at work or to assault with a heavy, bluntinstrument. A depressed fracture caused by anon-missile injury usually causes only focal braindamage, so that many patients never lose con-sciousness. If the underlying injured brain is aneloquent area the patient will exhibit focal neuro-logical signs. Haemorrhage from the bony edges,the dura or underlying brain trauma may resultin an intracranial haematoma which will causeprogressive neurological deterioration. If the de-pressed fracture is compound and the dura hasbeen lacerated there is a significantly increasedrisk of intracranial infection.
If the depressed skull fracture is compound,prophylactic antibiotics and tetanus prophylaxisshould be administered and surgery, usually re-
quiring a general anaesthetic, should be per-formed as soon as possible. A preoperative CTscan will show not only the position of the de-pressed skull fragments but also the presence ofany underlying intracranial pathology (Figs 4.4and 4.5). At operation the scalp wound should becleaned and debrided, as described previously,and the bone fragments elevated. If the dura hasbeen penetrated, or if bone fragments and exter-nal foreign material have been driven down intothe brain, this must be meticulously debridedand haemostasis obtained. It is desirable that thedura should be closed and this may require theuse of a patch of pericranium or fascia lata fromthe thigh. If the wound and bone fragments areheavily contaminated, and particularly if therehas been some delay in surgery, the bone shouldnot be replaced and a reconstructive cranioplastymay be necessary later.
If the depressed fracture is closed there is no urgency in elevating the bone fragments, provided there is no underlying intracranialcomplication. There is controversy over whethera depressed fragment might lead to epilepsy dueto continued pressure on the brain. In general, thedepressed fragments should be elevated if:• careful studies using the bone ‘windows’ onthe CT scan show that the dura might have beenpenetrated
Fig. 4.3 Depressed skull fracture.
Fig. 4.4 Depressed skull fracture with underlyingbrain contusion.
KAY4 12/16/04 7:37 PM Page 50

• there is significant brain compression• the fracture is compound• there are cosmetic considerations such as afrontal fracture in a young child.
The risk of epilepsy following a depressed frac-ture is 15% for the whole group, but the riskranges from 3 to 70% depending upon other asso-ciated intracranial pathology resulting from theinjury. Prophylactic anticonvulsant medicationshould be continued for 1 year if the dura hasbeen penetrated.
Cerebrospinal fluid rhinorrhoeaA fracture involving the base of the anterior cranial fossa may cause tearing of the basal duraresulting in a fistula into the frontal, ethmoid orsphenoid sinuses (Fig. 4.6). This type of fistulousconnection should also be suspected if the patientsuffers from an episode of meningitis or if the ra-diological investigations show a fracture in theappropriate site. An intracranial aerocele (Fig.4.7) is proof of a fistulous connection. CSF rhinor-rhoea may also occur as a result of a fistulathrough the tegmen tympani into the cavity of themiddle ear, and may leak via the eustachian tube.
Base of skull fractures are relatively frequent asskull fractures are often directed into the skullbase by its bony buttresses. They are often occultradiologically but diagnosed clinically. Anteriorfossa fractures may open into the frontal, sphe-noid or ethmoid sinuses, often running across thecribriform plate. They present with:• subconjunctival haemorrhages extending tothe posterior limits of the sclera. Periorbitalhaematomas or ‘racoon eyes’ indicate subgalealhaemorrhage and not necessarily a base of skullfracture• anosmia• nasal tip paraesthesiae due to anterior eth-moidal nerve injury.
Middle fossa fractures involving the petroustemporal bone present with:
HEAD INJURIES 51
Fig. 4.5 (a,b) CT showing severe trauma resulting inmultiple fractures, disruption of the orbit, intracranialcontusions involving the right temporal lobe andintracranial air.
(a)
(b)
Sphenoid sinus Frontal sinusEthmoid sinus
Fig. 4.6 Relationship of base of skull to air sinuses.
KAY4 12/16/04 7:37 PM Page 51

52 CHAPTER 4
• CSF otorrhoea (or rhinorrhoea) via the eu-stachian tube• deafness due to 8th nerve injury or ossiculardisruption• haemotympanum• Battle’s sign — bruising over mastoid bone• 7th nerve palsy — often delayed.
The diagnosis of CSF rhinorrhoea may be diffi-cult. In the early stages following a head injuryinvolving fractures to the facial bones, CSF needsto be differentiated from a bloody nasal dis-charge. Allergic rhinitis is the major differentialdiagnosis in patients presenting weeks ormonths after a head injury. Testing for sugar orB2-transferrin in the nasal discharge may help toidentify the fluid as being CSF. CSF isotope scansusing technetium-99 injected through the lumbartheca are only likely to be positive if there is alarge leak. High-resolution CT scanning follow-ing the administration of intracisternal contrastmay help to identify the position of the hole.
The major concern of a dural fistula is the riskof intracranial infection, particularly bacterialmeningitis. A CSF leak may not become apparentfor a few days after the head injury, but as thebrain swelling decreases the dural tear becomes
unplugged. Alternatively, CSF leakage may ceasedue to a brain hernia ‘plugging’ the hole in thedura and bone. Although the brain hernia mightstop the CSF escaping it will not provide protec-tion against future intracranial infection, as thedural defect will remain.
There is controversy concerning the indica-tions for an anterior cranial fossa exploration anddural repair, but there is general agreement thatsurgery should be performed if:• CSF leakage continues for more than 5 days,indicating the fistula is not trivial• there is an intracranial aerocele• there has been an episode of meningitis in a pa-tient with a fracture of the anterior cranial fossa.
Patients with a possible dural fistula should beplaced on prophylactic antibiotic medication. Ingeneral, penicillin is recommended as Pneumo-coccus is the most common organism; amoxy-cillin is appropriate in children due to the risk ofHaemophilus infection. Broad-spectrum anti-biotics may lead to the development of resistantorganisms and should be avoided. Nasal swabsmay indicate the need for more individualizedantibiotic prophylaxis.
It is best to delay surgery for about 2 weeks,until the initial brain swelling has resolved. Earlysurgery, using a craniofacial type of exposure,has been advocated by some neurosurgeons ifthere are associated major facial and anteriorvault fractures. However, early surgery may re-sult in further damage to an already swollenfrontal lobe during the retraction necessary to ob-tain adequate exposure of the dural tear.
The operative procedure involves a frontalcraniotomy with repair of the dural defect usingeither pericranium or fascia lata taken from thethigh.
Cerebrospinal fluid otorrhoeaCSF otorrhoea may occur as a result of a base ofskull fracture involving the petrous temporalbone. Unlike fractures of the anterior cranialfossa the leakage nearly always settles and thefistula does not usually provide a route of infec-tion, unless there is evidence of chronic middleear infection. Occasionally, a persistent leak mayrequire surgical exploration and repair.
Fig. 4.7 CT scan showing intracranial air in asubarachnoid space and within the lateral ventricles.
KAY4 12/16/04 7:37 PM Page 52

Cranial nerve injuriesInjuries to the cranial nerves occurring directly asa result of the trauma are not helped by surgery.Steroid medication is appropriate for patientswith a delayed facial nerve palsy following frac-ture of the petrous temporal bone. Some otolo-gists recommend surgical decompression of thefacial nerve when the palsy is delayed but, as thefacial function nearly always recovers, operativeintervention is usually not justified.
Post-traumatic epilepsyThe indications for prophylactic medication following head injury are discussed in Chapter21.
Missile injuries
Although most literature on missile injuries is re-lated to warfare, these injuries are unfortunatelybecoming more common in civilian conflict, par-ticularly as a result of the increased availability offirearms. In general the cranial injury is directlyproportional to the velocity of the missile. The‘high-velocity’ injury is defined as resulting froma missile travelling faster than the speed of sound(1050 ft/s), and modern rifle bullets have a muzzle velocity greater than 3000 ft/s. There arethree categories of missile injury:• tangential — the missile does not enter the cranium but causes a depressed skull fracture,lacerating the scalp with an underlying corticalcontusion, laceration or haematomas• penetrating — the missile enters the craniumresulting in the deposition of metal, bone frag-ments and debris within the brain• through-and-through — the missile enters andexits the cranium, frequently creating more thanone tract due to fragmentation
The cranial injury is directly related to the ve-locity of the missile. The energy dissipated by themissile equals MV2 where M is the mass and V the velocity of the missile. Modern ballisticshas designed missiles to have maximal velocityand stability in flight with maximal dissipation ofenergy upon impact. The primary missile fre-quently fragments and can cause further sec-ondary missiles from fragments of bone or metal.
The missile causes cerebral damage via threemechanisms:• mechanical laceration of brain tissue duringtransit• the shock wave promulgated ahead of the missile• cavitation in the wake of the missile.
The pathological processes involve scalp injury, depressed skull fracture, intracranialhaemorrhage and the intracranial pathologicalsequelae resulting from a ‘closed’ head injury, including cerebral contusion, haemorrhage,swelling and raised intracranial pressure. Thepattern of injury will depend on the velocity ofthe weapon and the trajectory of the missilethrough the bone and brain. A high-velocitywound may result in a rapid increase of intracra-nial pressure of more than 3000 mmHg due to the temporary cavity about the missile, whichmight be 50 times as large as the missile itself. The high intracranial pressure resulting from the cavitation may result in death from failure of the respiratory and cardiac centres in the brainstem.
Management
Rapid transport of the patient to hospital and ur-gent treatment is of paramount importance. Theearly definitive treatment resulting from prompttransport and the introduction of antibiotics werethe major factors in lowering mortality from headwounds in the Korean and Vietnam wars.
The management of the patient after transfer tohospital is essentially the same as described forsevere head injuries previously. Antibioticsshould be administered immediately, in large in-travenous doses because of the risk of infection;penicillin and chloramphenicol were the mostcommonly used during the Vietnam conflict. Op-timal antibiotic administration should provide a broad cover of Gram-positive, Gram-negativeand anaerobic organisms. After neurological assessment, a CT scan should be performed to ascertain the position of the intracranialhaematomas, depressed bone fragments andmetal fragments.
Surgery is not appropriate if the patient is brain
HEAD INJURIES 53
KAY4 12/16/04 7:37 PM Page 53

54 CHAPTER 4
dead with no evidence of brainstem reflexes. Patients with less severe injuries should have urgent surgical intervention, particularly as early exploration reduces the risk of subsequentinfection.
The operation is performed under generalanaesthesia and intravenous diuretic therapy isadministered to reduce intracranial pressure. Alarge scalp flap is designed, with excision and de-bridement of the entry and exit wounds. Meticu-lous care is taken to remove any accessible boneor metallic fragments. Haematoma and necroticbrain debris are excised. A watertight dural clo-sure should be performed and the scalp shouldbe closed in two layers (galea and skin). Follow-ing surgery, a repeat CT scan will identify anyfurther retained bone or metallic fragments. Accessible fragments should be removed, butisolated deep or inaccessible bone or metallicfragments are probably best left as further neuro-logical damage may occur during an attempt atexcision of these particles. In civilian practice, infection is unlikely if exploration has taken place within 2 hours of the injury. In general it is thought that retained metallic fragments haveless potential for infection than other debris.
Postoperative management is similar to thatdescribed for severe head injury, with particularattention to controlling intracranial pressure.Prophylactic antibiotics and anticonvulsantmedication are administered.
Non-accidental head injury
The infantile chronic subdural haematoma or ef-fusion is a distinct clinical entity. Birth trauma is afrequent cause but in many cases a past history isinadequate to establish the nature of the injurywith certainty. Chronic subdural haematomasoccur in approximately 20% of battered children.The violent shaking of the immature brain mightbe sufficient to rupture bridging veins or causeshearing at the grey/white interface without evi-dence of external trauma. If an inadequate histo-ry is provided in such a setting, it is important toscreen for a coagulopathy, examine the fundi forretinal haemorrhages, arrange a skeletal surveyand when appropriate involve a paediatrician
and social services. MRI now plays an importantrole in determining the chronicity of cerebral injuries in infants. Collections of differentchronicity, or in unusual locations, should alertthe physician to the possibility of non-accidentalinjury.
Rehabilitation
Some form of rehabilitation is essential followingany significant head injury. If the injury has beenrelatively minor then the necessary rehabilitationmay involve only advice and reassurance to thepatient and family. However, rehabilitation following a severe head injury will usually involve a team of paramedical personnel, includ-ing physiotherapists, occupational therapists,speech therapists and social workers.
The major groups of disabilities resulting froma head injury are:• impairment of motor function — hemiparesis,quadriparesis, ataxia, poor coordination• speech disturbances — dysphasia, dysarthria• impairment of special senses — vision, hearing• cognitive disturbance — memory impairment,intellectual disability, personality change.
The general aims of the rehabilitation processare:• in the initial period, to prevent complicationssuch as contractures of the limbs and to providecounselling for the family• to maximize the neurological recovery byrestoring old skills and teaching new skills — thisis usually undertaken in a rehabilitation unit• retraining for future employment, if necessaryand if possible.
The rehabilitation process should commenceas soon as possible after the head injury andshould initially concentrate on preventing com-plications. Limb contractures and pressure soresare avoided by frequent patient turning, physio-therapy and the use of splints. As the neurologi-cal state improves the patient’s rehabilitation willnormally be undertaken in a rehabilitation unit.Orthotic devices will assist hemiplegic patientsto walk and, if they can follow simple instruc-tions, most are able to relearn the activities ofdaily living.
KAY4 12/16/04 7:37 PM Page 54

The speech therapist may provide valuable assistance for patients with dysarthria and swallowing difficulties. Formal speech therapyprobably does little to improve global aphasiabut it does offer important psychological supportfor the patient with a severe communication disorder.
Damage to the non-dominant hemisphere results in perceptual disturbances, particularlyrelating to visual spatial tasks. Although the perceptual problems may resolve with time andrehabilitation, the problems associated with cog-nitive disturbances and alteration of personalitymay persist. Family counselling and support isessential to help the relatives understand andcope with these long-term disabilities.
Further readingBecker DP, Miller JD, Ward JD, Greenberg RP, Young
HF, Sakalas R (1977) The outcome from severe headinjury with early diagnosis and intensive manage-ment. Journal of Neurosurgery 47, 491–502.
Blackwood W, Corsellis JAN, eds (1976) Greenfield’sNeuropathology. Edward Arnold, London.
Cushing H (1908) Surgery of the head. In: Kean WW, ed.Surgery — Principles and Practice. W B Saunders,Philadelphia, Vol 3, 217–276.
Cushing H (1918) Notes on penetrating wounds of thebrain. British Medical Journal 1, 22–26.
Gurdjian ES, Thomas RS (1964) Surgical managementof a patient with head injury. Clinical Neurosurgery 12,56–74.
Holbourn AHS (1943) Mechanisms of brain injuries.Lancet ii, 438–441.
Jamieson KG, Yelland JD (1975) Surgical repair of anterior fossa because of rhinorrhoea, aerocele ormeningitis. Journal of Neurosurgery 39, 328–331.
Jefferson A, Reilly G (1972) Fractures of the floor of the
anterior cranial fossa. The selection of patients fordural repair. British Journal of Surgery 59, 585–592.
Jennett B, Miller JD (1972) Infection after depressedfracture of the skull. Implications for management ofnon-missile injuries. Journal of Neurosurgery 36,333–339.
Jennett B, Miller J D, Braakman R (1974) Epilepsy afternon-missile depressed skull fracture. Journal of Neurosurgery 41, 208–216.
Jennett B, Teasdale G (1981) Management of Head In-juries. Contemporary Neurology Series. F A Davis,Philadelphia.
Johnston IH, Johnston JA, Jennett B (1970) Intracranialpressure changes following head injury. Lancet ii,433–436.
Kaye AH, Black P McL (2000) Operative Neurosurgery.Churchill Livingstone, London, New York, Edinburgh.
Langfitt TW (1978) Measuring the outcome from headinjuries. Journal of Neurosurgery 48, 673–678.
Levy ML, Masri LS, Lavine S, Apuzzo M (1994) Out-come prediction after penetrating craniocerebral injury. Neurosurgery 35, 77–85.
Plum F, Posner JB (1972) The Diagnosis of Stupor andComa, 2nd edn. F A Davis, Philadelphia.
Rosner MJ, Rosner SD, Johnson AH (1995) Cerebral per-fusion pressure: Management protocol and clinicalresults. Journal of Neurosurgery 83, 949–962.
Russell WR, Schiller F (1949) Crushing injuries of the skull: Clinical and experimental observations.Journal of Neurology, Neurosurgery and Psychiatry 12,52–60.
Stone JL, Lichtor T, Fitzgerald LF (1995) Gunshotwounds to the head in civilian neurosurgery. Neurosurgery 37, 1104–1112.
Teasdale G, Jennett B (1974) Assessment of coma impaired consciousness. Lancet ii, 81–84.
Walsh FB, Hoyt WF (1969) Clinical Neuro-ophthalmology,Vol 3. Williams & Wilkins, Baltimore.
HEAD INJURIES 55
KAY4 12/16/04 7:37 PM Page 55

Intracranial haematoma formation followinghead injury is the major cause of fatal injuries inwhich death may have been potentially avoid-able and in which many survivors are unneces-sarily disabled following head injury due to adelay in the evacuation of the haematoma. Theincidence of intracranial haematomas and thetype of haematoma varies widely depending onthe different admission policies. In general hospi-tals that receive an unselected series of patients,the incidence varies between 1 and 5% of all headinjuries, while the incidence will be much higherin specialist neurosurgical centres.
Classification of traumatic intracranial haematomas
The general classification depends on the rela-tionship of the haematoma to the dura and brain.Haematomas can be:• extradural• subdural• intracerebral.However, many haematomas occupy more thanone of the intracranial sites (Table 5.1).
Extradural haematoma
Extradural haematomas are more likely to occurin the younger age group as the dura is able to strip more readily off the underlying bone. In patients under 20 years of age, extraduralhaematomas account for about two-thirds of alltraumatic intracranial haematomas, but repre-sent less than 5% of haematomas in patients overthe age of 50. Although an extradural haematoma
may occur in the presence of a severe head injury and coexist with a severe primary brain injury, the important feature of an extraduralhaematoma is that it may occur when the injury to the underlying brain is either trivial ornegligible.
Distribution of extradural haematomas
The most common sites for extraduralhaematoma are the temporal region followed bythe frontal area. Posterior fossa and parasagittalextradural haematomas are relatively uncom-mon. The relative proportions in a consecutiveseries of 200 cases from The Royal MelbourneHospital are shown in Fig. 5.1. In most cases thehaemorrhage is from a torn middle meningealartery or its branches but haematomas may alsodevelop from haemorrhage from extraduralveins, the superior sagittal sinus, transversesinus or posterior meningeal artery, the last two being responsible for the posterior fossa extradural haematomas. A fracture overlies thehaematoma in nearly all (95%) adults and most(75%) children.
Clinical presentation
As previously mentioned, an extraduralhaematoma may occur as a result of a severe headinjury and the haematoma will then becomemanifest as a further deterioration of the neuro-logical state, particularly with lateralizing fea-tures involving a 3rd nerve palsy (dilatation ofthe pupil) and progressive hemiparesis.
More frequently the extradural haematoma
CHAPTER 5
5 Traumatic intracranialhaematomas
56
KAY5 12/16/04 7:37 PM Page 56

occurs following a head injury that has resultedin only a transient loss of consciousness and inapproximately one-quarter of cases there hasbeen no initial loss of consciousness. In these patients the most important symptoms are:• headache• deteriorating conscious state• focal neurological signs (dilating pupil, hemi-paresis)• change in vital signs (hypertension, brady-cardia).
Headache. This is the outstanding initial symptomin patients who have not lost consciousness orwho have regained consciousness. The headacheincreases in severity and is followed by vomiting.
Deteriorating conscious state. This is the most important neurological sign, particularly when itdevelops after a ‘lucid’ interval. It is essential thatthe drowsiness that occurs in a patient followinga head injury is not misinterpreted just as the patient wishing to sleep. It is well to rememberthe nursery rhyme:
It’s raining, it’s pouring,The old man is snoring,He bumped his head and went to bed,And couldn’t get up in the morning.
This is a classic description of an extraduralhaematoma leading to drowsiness and death.
Focal neurological signs. These will depend uponthe position of the haematoma. In general, a temporal haematoma will produce a progressivecontralateral spastic hemiparesis and an ipsilat-eral dilated pupil. Further progression will resultin bilateral spastic limbs, a decerebrate postureand bilaterally dilated pupils (see Chapter 4, Fig.4.1). Occasionally the hemiparesis may initiallybe ipsilateral, due to compression of the con-tralateral crus cerebri of the tentorial edge, but itis rare for the opposite pupil to be involved first.
Change in vital signs. The change in vital signsshows the classic Cushing response to a rise in intracranial pressure — bradycardia accompanied by an increase in blood pressure. Disturbances inrespiration will develop into a Cheyne–Stokespattern of breathing.
Extradural haematomas occurring at other than
TRAUMATIC INTRACRANIAL HAEMATOMAS 57
Table 5.1 Position of traumatic intracerebral haematomas.
Extradural Extradural and Subdural Subdural and Intracerebral Series only (%) intradural (%) only (%) intracerebral (%) only (%)
International Collaborative Study 16 7 22 34 20(Glasgow, Rotterdam, Groningen, Los Angeles)
Brisbane (Jamieson & Yelland) 13 11 34 36 6Melbourne (The Royal 13 9 29 31 18
Melbourne Hospital)
9
8
66
11
7
Fig. 5.1 Frequency of sites of extradural haematomasin The Royal Melbourne Hospital series of 200consecutive cases.
KAY5 12/16/04 7:37 PM Page 57

58 CHAPTER 5
the temporal position show modifications of thisclinical presentation. Frontal haematomas showevidence of lateralizing signs late in their evolu-tion, the predominant features being a deteriora-tion of consciousness and pupil abnormalities. Inthe posterior fossa the vital signs tend to be af-fected early, followed by a change in consciousstate. The pupils and limbs may not be affecteduntil the patient becomes deeply unconscious.Haematomas in the posterior fossa may causesudden respiratory failure.
Radiological investigationsThe CT scan is the radiological investigation ofchoice and must be performed urgently if an ex-tradural haematoma is considered a possibility.The CT scan will show the typical hyperdense(white) biconvex haematoma (Fig. 5.2) with com-pression of the underlying brain and distortion ofthe lateral ventricle.
Treatment
The treatment of extradural haematoma is urgentcraniotomy with evacuation of the clot.
The patient should have an urgent CT scan assoon as an extradural haematoma is suspectedclinically. In some cases the rate of neurological
deterioration may be so rapid that there is notsufficient time for a CT scan and the patientshould be transferred immediately to the operat-ing theatre. Infusion of mannitol (20% solution,1 g/kg) or frusemide (20 mg intravenously) maytemporarily reduce the intracranial pressure during the transfer to the operating theatre. If unconscious, the patient must be intubated andhyperventilated during the transfer. It is essen-tial that there should be no delay in evacuatingthe haematoma. An extradural haematoma is asurgical emergency which will result in death ifnot removed promptly.
Operation for extradural haematomaThe type of operation performed will depend onthe circumstances in which the patient is beingtreated.1 If a CT scan has been performed and the posi-tion of the haematoma is known, the skin flapwill be lifted directly over the haematoma.2 If the patient’s neurological state is stable oronly slowly progressive and if the surgeon istrained in neurosurgical operations, a formalcraniotomy can be performed over the site of thehaematoma.3 A craniectomy, rather than a craniotomy,should be performed:
(a) if the surgeon is inexperienced(b) if craniotomy instruments are not available(c) if the rate of neurological deterioration hasbeen so rapid that time has not permitted a CTscan to be performed.
Exploratory burr holes should be insertedfirst in the temporal region and then in thefrontal and parietal areas (Fig. 5.3). When thehaematoma is identified the burr hole incisionshould be extended and the bone over the region of the haematoma should be rapidly removed. If the haematoma is not found on thefirst side that is explored burr holes should beperformed in the same order on the other side.
The following are guidelines for the positionof the haematoma if a CT scan has not beenperformed:
(i) it underlies the fracture (that may havebeen seen on the skull X-ray)(ii) it underlies a boggy swelling on the skull
Fig. 5.2 Extradural haematoma with the typicalhyperdense biconvex appearance.
KAY5 12/16/04 7:37 PM Page 58

(iii) it is on the same side as the pupil that dilated first(iv) in 85% of cases it is on the contralateralside to the hemiparesis.
Following removal of the bone of the vault bycraniotomy or craniectomy it is easy to evacuatethe haematoma. The original source of thehaematoma, usually the bleeding middlemeningeal artery in the temporal haematoma, iscontrolled by diathermy or with a haemostaticclip. The haematoma will have stripped away thedura from the inner table of the vault, often resulting in considerable oozing from the duralsurface. The dura should be opened, if a CT scanhas not previously been performed, to excludethe coexistence of a subdural haematoma. Itshould then be closed in a watertight fashion. It isusually advisable to insert a closed-system, low-pressure extradural drain to evacuate any bloodthat may continue to ooze.
The postoperative care is similar to that for anyother intracranial procedure. If the neurologicalstate fails to improve following the evacuation ofthe haematoma, or if there is further deteriora-tion, another CT scan should be performed to exclude recurrence of the haematoma formation.
Prognosis. If the initial head injury has resulted inonly a transient loss of consciousness, the patientshould make a full recovery following removal of the extradural haematoma, provided thehaematoma has been evacuated early enough toprevent permanent neurological disability. Thedamage caused by an extradural haematoma is
potentially reversible, provided the haematomais evacuated before pressure from the blood clothas caused secondary intracranial pathologicaleffects.
Subdural haematoma
Subdural haematomas have been classified intoacute, subacute and chronic, depending on thetime they become clinically evident following injury:• acute subdural haematoma — less than 3 days• subacute subdural haematoma — 4–21 days• chronic subdural haematoma — more than 21days.
The CT scan enables a further classification de-pending on the density of the haematoma rela-tive to the adjacent brain. An acute subduralhaematoma is hyperdense (white) and a chronicsubdural haematoma is hypodense. Between the end of the 1st week and the 3rd week the subdural haematoma will be isodense with theadjacent brain.
Acute subdural haematoma
The acute subdural haematoma frequently results from severe trauma to the head and com-monly arises from cortical lacerations. However,an acute subdural haematoma can result from aless severe trauma caused by rupture of a bridg-ing vein or focal tear of a cortical artery, especiallyif the patient has been anticoagulated for othermedical reasons (e.g. for atrial fibrillation). Cases
TRAUMATIC INTRACRANIAL HAEMATOMAS 59
Fig. 5.3 Emergency surgery for suspected extradural haematoma. (a) Position of exploratory burr holes. (b) Ifhaematoma found in the temporal position the skin wound is extended. (c) Further bone removed to enablecomplete evacuation of haematoma and haemostasis.
(a) (b) (c)
KAY5 12/16/04 7:37 PM Page 59

60 CHAPTER 5
of spontaneous acute subdural haematoma havebeen reported and in these patients it is essentialto exclude a ruptured aneurysm or bleedingdiathesis as a cause. Acute subdural haematomasare bilateral in approximately one-third of cases,in comparison with less than 3% of extraduralhaematomas.
An acute subdural haematoma often presentsin the context of a patient with a severe head in-jury whose neurological state is either failing toimprove or deteriorating. The features of deterio-rating neurological state — decrease in consciousstate and/or increase in lateralizing signs —should raise the possibility of a subduralhaematoma.
The CT scan will show the characteristic hy-perdense haematoma, which is concave towardsthe brain, with compression of the underlyingbrain and distortion of the lateral ventricles (Fig.5.4). Over 80% of patients with acute subduralhaematomas have a fracture of either the cranialvault or the base of the skull, which may be evident on the bone ‘windows’ of the CT scan.
A craniotomy is nearly always necessary toevacuate an acute subdural haematoma. If thehaematoma is liquid the blood can sometimes be
washed out with gentle irrigation through burrholes. However if bleeding persists a craniotomywill be required for haemostasis.
Chronic subdural haematoma in the adult
In 1863, Virchow first proposed chronic inflam-mation of the meninges as being the cause of achronic subdural haematoma. In 1914, Trottersuggested trauma as the aetiological factor and in1932 Gardner, and later Zollinger and Gross, pro-posed that an osmotic gradient occurred from thebreakdown of haemoglobin. However, it wassubsequently shown that the osmolarity of thehaematoma did not change with time and so thistheory was abandoned.
Chronic subdural haematoma can be dividedinto two major groups. The first involves patientshaving suffered a significant, and often severehead injury. However, in approximately one-third of patients there is no definite history of preceding head trauma. The aetiology of the subdural haematoma in this non-traumaticgroup is probably related to rupture of a fragilebridging vein in a relatively atrophic ‘mobile’brain. In this group the majority of patients areover 50 years of age. Shrinkage of the brain re-sulting from atrophy allows the brain to becomemore mobile and increases the space traversed bythe veins bridging between the cortex and thevault. A relatively trivial injury may result inmovement of the brain, like a walnut inside itsshell, with tearing of the bridging vein. Patientswho are anticoagulated are especially prone todevelop a subdural haematoma following rela-tively minor trauma.
Clinical presentationThe presence of a chronic subdural haematomashould be considered if the neurological state of apatient being treated in hospital for a significanthead injury begins to deteriorate. Alternatively,the patient may present without the history of asignificant head injury in one of three characteris-tic ways.1 Raised intracranial pressure without signifi-cant localizing signs. The patient presents withheadache, vomiting and drowsiness and the
Fig. 5.4 Acute subdural haematoma causing markedshift of the lateral ventricle.
KAY5 12/16/04 7:37 PM Page 60

absence of focal neurological signs, raising thedifferential diagnosis of a cerebral neoplasm or chronic subdural haematoma.2 Fluctuating drowsiness. The predominantcharacteristic is a decline in the level of con-sciousness and the patient may abruptly becomedeeply unconscious.3 A progressive dementia, which may be misdi-agnosed as Alzheimer’s disease. However, thecourse of the dementia is usually more rapid and progressive. Focal neurological signs maydevelop, particularly a hemiparesis with an ex-tensor plantar response. In up to 20% of cases thehemiparesis may be ipsilateral to the side of thehaematoma due to shift of the brain causing the contralateral crus cerebri to be compressed bythe tentorial edge.
A chronic subdural haematoma will be diag-nosed on the CT scan as a hypodense, extra-cerebral collection causing compression of theunderlying, brain (Fig. 5.5). In 25% of cases thehaematoma is bilateral (Figs 5.6 and 5.7).
OperationThe chronic subdural haematoma can be drainedthrough burr holes or a craniotomy located overthe haematoma. No attempt should be made to
excise all the membrane of the haematoma. Asthese haematomas may be multiloculated it is advisable to insert more than one burr hole and to visualize the underlying brain at each site.
TRAUMATIC INTRACRANIAL HAEMATOMAS 61
Fig. 5.5 Chronic subdural haematoma. The fluid ishypodense compared with the adjacent brain.
Fig. 5.6 Bilateral chronic subdural haematoma. Thecollection on the left is not as hypodense, indicatingthat it is more recent than the haematoma fluid on theright. It also has a hyperdense area, indicating morerecent haemorrhage.
Fig. 5.7 T1 MRI showing bilateral chronic subduralhaematoma.
KAY5 12/16/04 7:37 PM Page 61

62 CHAPTER 5
The haematoma fluid should be washed out completely and after the operation it is usuallyadvisable to place a subdural catheter for furtherdrainage in a closed drainage system.
Following the operation the patient is nursedflat, or even with the head down initially, to en-courage the brain to expand into the haematomaspace. Careful attention should be given to thefluid intake and serum electrolytes. The normaldaily fluid requirements are given (3 l/day inadults) provided there is no clinical or radiologi-cal evidence of brain swelling. The patient shouldbe slightly more hydrated after this type of oper-ation than other intracranial procedures, in an attempt to encourage the brain to swell into theprevious haematoma space. However, hypona-traemia is a common occurrence, both prior toand following surgery, and if the serum sodiumdecreases to less than 130 mmol/l the fluid intakeshould be reduced.
Subdural haematomas in infancy
The infantile chronic subdural haematoma, or effusion, is a distinct clinical entity. Birth traumais a frequent cause but in many cases a past his-tory is inadequate to establish the nature of theinjury with certainty. Chronic subdural haema-tomas occur in 10% of ‘battered children’ and theviolent shaking of an infant may be sufficient tolacerate bridging cerebral veins without evi-dence of external trauma. Subdural bleeding ininfants occurs bilaterally in 85% of cases and isusually over the dorsolateral surfaces of thefrontal and parietal lobes.
The earliest finding in infants with chronicsubdural haematomas is excessive cranial enlargement as the sutures are unfused. Thesymptoms are non-specific and usually involvelistlessness, irritability and failure to thrive.
The diagnosis will be confirmed by CT scan.Treatment initially involves aspiration of thefluid but if, after 2 or 3 weeks, repeated taps havefailed to reduce the volume significantly, a shuntmay be inserted to drain the fluid from the sub-dural space to the peritoneal cavity.
Intracerebral haematoma
Traumatic intracerebral haematomas occur as aresult of a penetrating injury (such as a missile in-jury) or a depressed skull fracture, or following asevere head injury. Intracerebral haematoma isfrequently associated with subdural haematoma.
The size of the haematoma varies considerablyand multiple haematomas are frequently seen onthe CT scan following a severe head injury. Thecontre-coup injury described in Chapter 4 may beresponsible for a ‘burst’ temporal lobe which re-sults in a large temporal haematoma associatedwith subdural blood.
An intracerebral haematoma should be sus-pected in any patient with a severe head injury or in a patient whose neurological state is deteriorating.
The CT scan will show the size and position ofthe haematomas (Fig. 5.8). It should be noted thattraumatic intracerebral haematomas not infre-quently evolve more than 24 hours after the trauma. Consequently if is essential to repeat a CT scan if the initial scan performed after the injury was negative but the patient’s neurologi-cal state deteriorates.
Fig. 5.8 Traumatic frontal intracerebral haematomasresulting from contre-coup injury.
KAY5 12/16/04 7:37 PM Page 62

A large intracerebral haematoma should beevacuated, unless the patient’s neurological stateis improving. Small intracerebral haematomas,particularly if multiple, are not removed but theclinician must be aware that they may expandand require subsequent evacuation.
Further readingGardner WJ (1932) Traumatic subdural haematoma
with particular reference to the latent interval.Archives of Neurology and Psychiatry 27, 847–855.
Hooper RS (1959) Observations on extradural haemor-rhage. British Journal of Surgery 47, 71–87.
Jamieson KG, Yelland JD (1968) Extradural haema-toma. Report of 167 cases. Journal of Neurosurgery29, 13–23.
Jamieson KG, Yelland JD (1972) Traumatic intracerebralhaematoma. Report of 63 surgically treated cases.Journal of Neurosurgery 37, 528–532.
Jennett B, Murray A, Carlin J et al. (1979) Head injuriesin three neurosurgical units, Scottish Head Injury
Management Study. British Medical Journal 2,955–958.
Jennett B, Teasdale G (1981) Intracranial haematoma.In: Jennett B, Teasdale G, eds. Management of Head Injuries. Contemporary Neurology Series. F A Davis,Philadelphia.
Kaye AH, Black P McL (2000) Operative Neurosurgery.Churchill Livingstone, London, New York, Edinburgh.
Reilly PJ, Adams JH, Graham DI et al. (1975) Patientswith head injury who talk and die. Lancet ii, 375–381.
Teasdale G, Galbraith S (1981) Acute traumatic intra-cranial haematomas. In: Teasdale G, Galbraith S, eds.Progress in Neurological Surgery 10. Karger, Basel.
Trotter W (1914–1915) Chronic subdural haemorrhageof traumatic origin and its relation to pachymeningi-tis haemorrhagica interna. British Journal of Surgery 2,271–291.
Weir BKA (1971) The osmolarity of subduralhaematoma fluids. Journal of Neurosurgery 34,528–533.
TRAUMATIC INTRACRANIAL HAEMATOMAS 63
KAY5 12/16/04 7:37 PM Page 63

Brain tumours are responsible for approximately2% of all cancer deaths. Central nervous systemtumours comprise the most common group ofsolid tumours in young patients, accounting for20% of all paediatric neoplasms. The overall inci-dence of brain tumours is 8–10 per 100 000 popu-lation per year. A study by the United StatesDepartment of Health in 1966 showed the inci-dence to be 21 per 100 000 per year at 2 years oldand 1 per 100 000 during the teenage years. Theincidence increases after the 4th decade of life toreach a maximum of 16 per 100 000 per year in the7th decade. There has been an intense debate con-cerning the increased incidence of brain tumours,especially in the elderly, but this possible increasecould be explained due to the advent of CT andMRI leading to better detection of tumours.
Classification
The general brain tumour classification is relatedto the cell of origin, and is shown in Table 6.1.
Table 6.2 shows the approximate distributionof the more common brain tumours.
This chapter will discuss the tumours derivedfrom the neuroectoderm and metastatic tumours.The following chapters will describe the benignbrain tumours and pituitary tumours.
Aetiology
Epidemiology studies have not indicated anyparticular factor (viral, chemical or traumatic)that causes brain tumours in humans, although arange of cerebral tumours can be induced in ani-mals experimentally. There is no genetic predis-
position but chromosome abnormalities havebeen noted in many CNS tumours (Table 6.3).Neurofibromatosis type 1 (NF1), previouslyknown as von Recklinghausen’s disease, occurswith an approximate frequency of 1 in 4000 livebirths. It is inherited as an autosomal dominantpattern and there is a high spontaneous mutationrate. NF1 is associated with a variety of centraland peripheral nervous system tumours. Anoptic nerve glioma is the most common CNS tu-mour associated with NF1, occurring in about15% of those affected. Less commonly low-gradeglioma of the hypothalamus, cerebellum, brain-stem or spinal cord may occur. Peripheral neu-rofibromas are the hallmark of NF1 (Chapter 17).Neurofibromas of the spinal roots are a commonfeature of NF1 (Chapter 15). The gene causingNF1 is located on the long arm of chromosome 17(17q 11.2).
Neurofibromatosis type 2 (NF2), previouslyknown as central neurofibromatosis, is an auto-somal dominant disorder which, beyond a fewsuperficial similarities, is phenotypically and genetically distinct from NF1. It has an incidenceof approximately 1 in 100 000 live births. The hall-mark of NF2 is bilateral acoustic (vestibular)schwannomas, but patients with NF2 have an in-creased risk of other intracranial schwannomas,multiple meningiomas (both cranial and spinal)and gliomas. The NF2 gene locus is sited on the long arm of chromosome 22 (22q 11.2) (Table6.4).
There is no specific evidence linking CNS tu-mours to environmental carcinogens, althoughmany chemicals, especially ethyl and methyl nitrosourea and anthracene derivatives, show
CHAPTER 6
6 Brain tumours
64
KAY6 12/16/04 7:39 PM Page 64

of the brain, particularly in transplant recipients,there is not the corresponding increased inci-dence of gliomas.
At present there is considerable conjecture re-garding the role of other possible aetiologicalagents, including trauma, electromagnetic radia-tion and organic solvents but, as yet, there is no
BRAIN TUMOURS 65
Table 6.1 General classification of brain tumours.
Neuroepithelial tumoursGliomas
Astrocytoma (including glioblastoma)OligodendrocytomaEpendymomaChoroid plexus tumour
Pineal tumoursNeuronal tumours
GangliogliomaGangliocytomaNeuroblastoma
Medulloblastoma
Nerve sheath tumour — acoustic neuroma
Meningeal tumoursMeningioma
Pituitary tumours
Germ cell tumoursGerminomaTeratoma
Lymphomas
Tumour-like malformationsCraniopharyngiomaEpidermoid tumourDermoid tumourColloid cyst
Metastatic tumours
Local extensions from regional tumourse.g. glomus jugular (i.e. jugulare), carcinoma of
ethmoid
Table 6.2 Incidence of common cerebral tumours(%).
Neuroepithelial 52Astrocytoma (all grades including 44
glioblastoma)Ependymoma 3Oligodendroglioma 2Medulloblastoma 3
Metastatic 15
Meningioma 15
Pituitary 8
Acoustic neuroma 8
carcinogenic activity in animals and produceCNS tumours.
Viral induction of brain tumours has been usedin animal models but there is no firm evidence forviral aetiology in humans. A human polyoma JCvirus injected into primates produces tumourssimilar to human astrocytomas after an 18-monthincubation period. This type of ‘slow virus’ effectmay account for some of the problems of isolat-ing viruses from human tumours.
Although immunosuppression is known to in-crease markedly the risk of primary lymphoma
Table 6.3 Chromosomal deletions and loci of lossof heterozygosity (LOH) in CNS tumours.
Chromosomal Tumour deletions/loci of LOH
Astrocytoma #10, #13, 17p, 17q, 19q, #22
Glioblastoma multiforme 9, #10, 17p, 19q, 22qOligodendroglioma 1p, 4, 6, 11p, 19q, 22qMedulloblastoma 17p, 10, 11, 19Retinoblastoma 13q 1.4Meningioma 1p, 14, #22, 22q
12.3-qterHaemangioblastoma 3p
(von Hippel–Lindau)Pituitary adenoma 11q
(MEN1)Acoustic nerve tumours 22q
(NF2)Neurofibromas (NF1) 17q
KAY6 12/16/04 7:39 PM Page 65

66 CHAPTER 6
convincing evidence to implicate these as beinginvolved with the development of brain tumoursin humans.
The four hallmarks of the development of acancer cell are the ability to proliferate, with theintracellular growth pathways constituitively ac-tivated, the evasion of apoptosis, with the cancercells having escaped from cell death pathways,the attraction and induction of new blood vessels(angiogenesis) to supply increased metabolic ac-tivity of tumour cells, and tissue invasion. Eachof these are dependent on ligand–receptor inter-actions on the cell surface leading to a cascade ofcytoplasmic events that eventually result in dif-ferential gene expression.
Molecular biology techniques have enabled
the identification of a variety of alterations in thegenome of the tumour cell, including those ofbrain tumours. The present concept of oncogene-sis involves both the addition of oncogenes to thegenome and the loss of the normally occurringtumour suppressor genes. Transformation (spon-taneous or induced) is a multistep process requir-ing both initiation and promotion. Oncogenesencode proteins that participate in the signaltransduction and second messenger systems thatmodulate cell metabolism and proliferation.These proteins include both growth factors andgrowth factor receptors such as epidermalgrowth factor receptor, platelet-derived growthfactor, tryosine-specific protein kinases and guanine-binding proteins.
Tumour suppressor genes are normally pre-sent in the genome and act as a ‘brake’ on celltransformation. Mutations in the p53 tumoursuppressor gene on chromosome 17 are the mostcommon gene alteration found to date in tu-mours and have been shown to occur in both as-trocytomas and meningiomas. The Li–Fraumenisyndrome is due to a germ line mutation in thep53 gene with the development of numerous cancers including gliomas, ependymomas andmedulloblastomas.
Glioma
Neuroectodermal tumours arise from cells de-rived from neuroectodermal origin. Gliomascomprise the majority of cerebral tumours andarise from the neuroglial cells. There are four distinct types of glial cells: astrocytes, oligo-dendroglia, ependymal cells and neuroglial precursors. Each of these gives rise to tumourswith different biological and anatomical charac-teristics. The neuroepithelial origin of microgliais in question.
Astrocytoma
The most common gliomas arise from the astro-cyte cells which comprise the vast majority of intraparenchymal cells of the brain. Their mainfunction appears to be as a supporting tissue forthe neurones. The tumours arising from astro-
Table 6.4 Diagnostic criteria forneurofibromatosis.
NF1: Two or more of the following1 Six or more café au lait macules, each greaterthan 5 mm in diameter in prepubertal personsand over 15 mm in diameter in postpubertalpersons2 Two or more neurofibromas or any type of oneplexiform neurofibroma3 Freckling in the axillary or inguinal regions4 Optic glioma5 Two or more Lisch nodules (iris hamartomas)6 A distinctive osseous abnormality such assphenoid dysplasia or thinning of long bonecortex with or without pseudoarthrosis7 A first-degree relative (parent, sibling oroffspring) with NF1 by the above criteria
NF2: One of the following1 Bilateral 8th nerve tumours seen with magneticresonance imaging or computerized tomography2 A first-degree relative with NF2 and either aunilateral 8th nerve tumour or two of thefollowing:
• neurofibroma• meningioma• glioma• schwannoma• juvenile posterior subcapsular lenticularopacity
KAY6 12/16/04 7:39 PM Page 66

cytes range from the relatively benign to thehighly malignant. The term ‘malignant’ for braintumours differs from its usage for systemic tumours. Intrinsic brain tumours very rarelymetastasize (except for medulloblastoma andependymoma), and ‘malignant’ refers to aggres-sive biological characteristics and a poor prognosis.
Classification
There are many classification systems of brain tu-mours in general and gliomas in particular. Theperiod of systematic classification of tumoursbegan in 1846, when Virchow described the neu-roglia and related it to brain tumours. AlthoughVirchow created the term ‘glioma’, these tu-mours had already been described under othernames. In 1926, Bailey and Cushing described ahistogenetic classification system which com-pared the predominant cell in the tumours withthe embryonal development of the neuroglia.The comparison with stages of cytogenesis wasprobably more of a working hypothesis than anoncological theory for the origin of the tumours’cells. The theory that gliomas originate from pro-liferation of cells of varying degrees of maturitylying dormant in the brain is not generally ac-cepted except in the case of medulloblastoma,which may arise from a primitive layer in thecerebellar cortex.
A valuable prognostic system of subclassifica-tion of astrocytoma was described by Kernohanin 1949. Astrocytomas were graded from I to IV,with Grade IV being the most malignant andGrade I cytologically, but not necessarily biologi-cally, benign. Ringertz simplified the four-gradeclassification of Kernohan into a three-tiered sys-tem; the comparison between the two is shown inFig. 6.1. The glioblastoma multiforme, equivalentto the Kernohan Grade III and IV tumours, is themost common adult cerebral tumour, accountingfor approximately half of all gliomas. The low-grade gliomas — the astrocytoma, or Grade I or II Kernohan astrocytoma — account for only10–15% of astrocytomas.
The World Health Organization (WHO) classi-fication recognizes four grades of astrocytoma.Grade I is assigned to the pilocytic astrocytomawhich is biologically distinct from the diffuse as-trocytomas, which are classified as astrocytoma(WHO Grade II), anaplastic astrocytoma (WHOGrade III) and glioblastoma multiforme (WHOGrade IV).
A grading system proposed by Daumas-Duport and also known as the St Anne–Mayo System assessed the tumours according to thepresence or absence of four morphological fea-tures — nuclear atypia, mitosis, endothelial pro-liferation, and necrosis — and they are gradedaccording to the cumulative features score.Grade I tumours have none of the features, Grade
BRAIN TUMOURS 67
Ringertz Grade I(Well differentiated)
Grade II(Anaplastic astrocytoma)
Grade III(Glioblastoma multiforme)
Kernohan Grade IGrade II
Grades III and IV
Grade IIAstrocytoma variants
• Fibrillary• Protoplasmic• Gemistocytic
WHO Grade IJuvenile pilocytic
astrocytoma
Grade IIIAnaplastic
astrocytoma
Grade IVGlioblastoma variants
• Giant cell• Gliosarcoma
St Anne-Mayo Grade IScore: 0
Grade IIScore: 1
Grade IIIScore: 2
Grade IVScore: 3 or 4
Fig. 6.1 Relationship of the Kernohan system, the ‘three-tiered’ classification system, the WHO system and the StAnne/Mayo (Dumas-Deport) grading system for astrocytomas.
KAY6 12/16/04 7:39 PM Page 67

68 CHAPTER 6
II tumours have one feature, Grade III tumourshave two features and Grade IV tumours havethree or four features.
Pathology
Macroscopic changesAn astrocytoma may arise in any part of thebrain, although it usually occurs in the cerebrumin adults and the cerebellum in children.
A low-grade tumour in the cerebral hemi-spheres invades diffusely into the brain. The tu-mour does not have a capsule and there is nodistinct tumour margin. The low-grade gliomasare usually relatively avascular with a firm fi-brous or rubbery consistency. Fine deposits ofcalcium are present in 15% of astrocytomas. Oc-casionally, a low-grade astrocytoma may invadediffusely throughout the cerebral hemisphere. Incontrast, the macroscopic appearance of a high-grade tumour, the glioblastoma multiforme, ischaracterized by a highly vascular tumour mar-gin with necrosis in the centre of the tumour. Al-though in certain areas the margin of the tumourmay seem to be macroscopically well definedfrom the surrounding brain, there are micro-scopic nests of tumour cells extending well outinto the brain.
Microscopic changesThe histological appearance of the tumour varies
with the tumour’s grade. The low-grade astrocy-toma is characterized by an increased cellularity,composed entirely of astrocytes (Fig. 6.2). Intermediate-grade tumours show nuclear pleomorphism, mitotic figures are frequent, andthere is increased vascularity, as evidenced by en-dothelial and adventitial cell proliferation. In thehigh-grade astrocytoma very few astrocytes ap-pear normal. There is marked cellular pleomor-phism, extensive endothelial and adventitial cellproliferation and numerous mitotic figures withextensive necrosis (Fig. 6.3).
The major histological features of glioblastomamultiforme are endothelial proliferation andnecrosis. The anaplastic astrocytoma is char-acterized by nuclear pleomorphism and mitoses,which are absent in the astrocytoma.
Clinical presentation
The presenting features can be classified under:• raised intracranial pressure• focal neurological signs• epilepsy.
The duration of the symptoms and the pro-gression and evolution of the clinical presenta-tion will depend on the grade of thetumour — that is, its rate of growth. A patient pre-senting with a low-grade astrocytoma (Grade I or II) may have a history of seizures extendingover many years, antedating the development of
Fig. 6.2 Low-gradeastrocytoma. There is only aslight increase in thecellularity and mild nuclearatypia. There is a disturbedarchitecture with formation oftriplets and quadruplets ofastrocytes (haematoxylin andeosin, ¥40).
KAY6 12/16/04 7:39 PM Page 68

progressive neurological signs and raised in-tracranial pressure. The tumours may evolve his-tologically into the more malignant anaplasticastrocytoma or glioblastoma multiforme. Pa-tients with the higher-grade tumours presentwith a shorter history and glioblastoma multi-forme is characterized by a short illness of weeksor a few months.
Raised intracranial pressureRaised intracranial pressure is due to the tumourmass, surrounding cerebral oedema and hydro-cephalus due to blockage of the CSF pathways.The features of raised intracranial pressure aredescribed in detail in Chapter 3. The major symp-toms are headache, nausea and vomiting, anddrowsiness.
Headache is the most common symptom in patients with cerebral astrocytoma and occurs in nearly three-quarters of patients; vomiting occurs in about one-third. The headaches areusually gradually progressive and although frequently worse on the side of the tumours, theymay be bitemporal and diffuse. Characteristi-cally, the headache is worse on waking and im-proves during the day. Nausea and vomitingoccur as the intracranial pressure increases, andthe patient frequently indicates that vomitingmay temporarily relieve the severe headache.Drowsiness, that is, a deterioration of conscious
state, is the most important symptom and sign ofraised intracranial pressure. The extent of im-pairment of conscious state will be related to theseverity of raised intracranial pressure. An alertpatient with severely raised intracranial pressuremay rapidly deteriorate and become deeply un-conscious when there is only a very small furtherrise in the pressure within the cranial cavity.
Focal neurological deficitsFocal neurological deficits are common in patients presenting with cerebral gliomas; the nature of the deficit will depend on the positionof the tumour.
Patients presenting with tumours involvingthe frontal lobes frequently have pseudopsychi-atric problems, personality change and mooddisturbance. These changes are particularly char-acteristic of the ‘butterfly glioma’, so called be-cause it involves both frontal lobes by spreadingacross the corpus callosum, giving it a character-istic macroscopic (Fig. 6.4) and CT or MRI ap-pearance. This type of tumour may also occurposteriorly, with spread across the splenium ofthe corpus callosum into both parieto-occipitallobes.
Limb paresis results from interference withthe pyramidal tracts, at either a cortical or a sub-cortical level, and occurs in just under 50% of pa-tients. Field defects associated with tumours of
BRAIN TUMOURS 69
Fig. 6.3 Glioblastoma multiforme. (a) There is a marked increase in cellularity and variation in nuclear size,shape and staining density with frequent mitotic figures (haematoxylin and eosin, ¥40). (b) Low-power view ofthe same tumour showing pallisaded necrosis typical of glioblastoma multiforme.
(a) (b)
KAY6 12/16/04 7:39 PM Page 69

70 CHAPTER 6
the temporal, occipital and parietal lobes arecommon, but may be evident only on careful test-ing. Dysphasia, either expressive or receptive, isa particularly distressing symptom occurring inpatients with tumours involving the relevantareas of the dominant hemisphere.
The particular characteristics of posterior fossaand brainstem gliomas will be discussed in thefollowing section on paediatric tumours.
Epileptic seizuresSeizures are the most frequent initial symptom inpatients with cerebral astrocytoma and occur in50–75% of all patients. Tumours adjacent to thecortex are more likely to be associated withepilepsy than those deep to the cortex and tu-mours involving the occipital lobe are less likelyto cause epilepsy than those which are more anteriorly placed. Astrocytomas may produce either generalized or focal seizures; the focal characteristics will depend on the position withinthe brain and the cortical structures involved.
Investigations
Computerized tomographyCT scan or MRI of the brain are the essential radi-ological investigations (Figs 6.5 and 6.6); an accu-rate diagnosis can be made in nearly all tumours.Low-grade gliomas show decreased density onthe CT scan; this does not enhance with contrastand there is little or no surrounding oedema. Cal-cification may be present. High-grade gliomasare usually large and enhance vividly followingintravenous injection of contrast material (Fig.6.7). The enhancement is often patchy and non-uniform and frequently occurs in a broad, irregu-lar rim around a central area of lower density.Although tumour cysts may occur in the high-grade tumours, the central area of low densitysurrounded by the contrast enhancement is usu-ally due to tumour necrosis. High-grade tumoursare surrounded by marked cerebral oedema andthere is frequently considerable distortion of thelateral ventricles. Compression of the lateral ven-tricle in one hemisphere, with pressure extendingacross the midline, may result in an obstructivehydrocephalus involving the opposite lateralventricle.
Fig. 6.4 ‘Butterfly glioma’. Glioblastoma multiformeof corpus callosum spreading into both frontal lobes.
Fig. 6.5 Low-grade astrocytoma. CT scan shows non-enhancing low-density lesion with little or nomass effect.
KAY6 12/16/04 7:39 PM Page 70

Magnetic resonance imagingWhen used with gadolinium contrast enhance-ment, MRI improves the visualization andanatomical localization of the tumours (Figs 6.8and 6.9). MRI has the advantage of being more
sensitive than CT scan, enabling the detection of small tumours and particularly low-gradegliomas that might be missed by CT scan. MRIprovides better anatomical detail and is moreuseful in visualizing skull base, posterior fossaand brainstem tumours.
BRAIN TUMOURS 71
Fig. 6.6 MRI showing low-grade glioma in posterior frontal region. (a) T1 scan, (b) T2 scan.
(a) (b)
Fig. 6.7 Glioblastoma multiforme. CT shows a largetumour with contrast enhancement particularly at the margins surrounding a necrotic centre. There ismarked surrounding oedema with compression of the ventricles.
Fig. 6.8 Glioblastoma multiforme. MRI shows largeenhancing tumour invading into corpus callosum andventricle.
KAY6 12/16/04 7:39 PM Page 71

72 CHAPTER 6
Low-grade astrocytomas may show up on MRIas abnormal areas of increased T2 signal and de-creased T1 signal, even if the CT scan was normal.High-grade astrocytomas characteristically havelow signal intensity on T1-weighted images andhigh signal intensity on T2-weighted images.Gadolinium enhancement is more likely to occurin the higher-grade tumour.
Perfusion-weighted MRI is used to determinethe regional cerebral blood volume, which is increased in high-grade glioma and may be ofvalue in differentiating recurrent tumour fromradiation necrosis. Magnetic resonance spec-troscopy (MRS) is a non-invasive technique thatprovides information on the composition andspatial distribution of cellular metabolites. Onproton MRS, tumours have an increased lactateproduction, loss of N-acetyl aspartate (due to lossof neurones in the tumour area) and increasedcholine levels (due to active membrane biosynthesis).
Cerebral angiographyThis was the standard study in most patientswith astrocytomas prior to the introduction ofCT. It provides helpful information on the vascular supply of the tumours but is now onlyrarely indicated.
Plain X-raysPlain X-rays of the skull do not need to be
performed as a routine. The most common abnormality is erosion of the sella turcica due to long-standing raised intracranial pressure. Radiologically visible calcification is present inabout 8% of patients with astrocyte-derivedgliomas.
Management
Following the presumptive diagnosis of a gliomathe management involves:• surgery• radiotherapy• other adjuvant treatments.
SurgerySurgery is performed with three principal aims.• To make a definite diagnosis.• Tumour reduction to alleviate the symptomsof raised intracranial pressure.• Reduction of tumour mass as a precursor toadjuvant treatments.
The patient is started on glucocorticoid steroidtherapy (e.g. dexamethasone) when presentingwith clinical features of raised intracranial pressure with the aim of decreasing the cerebraloedema prior to surgery.
The type of operation performed will largelybe determined by the position of the tumour andby the patient’s clinical presentation. In general,the tumour is excised as radically as possible,
Fig. 6.9 Cystic anaplastic astrocytoma.
(a) (b)
KAY6 12/16/04 7:39 PM Page 72

provided the surgery will not result in any dis-abling neurological deficit. Craniotomy is per-formed in the position that provides the bestaccess to the tumour and usually with the aid of aframeless stereotactic system to aid accuracy oflocalization. If the tumour has not grown to in-volve the cortical surface, a small incision is madein a non-eloquent gyrus or sulcus and the subcor-tical brain is divided down to the tumour mass.The tumour is excised, often with the aid of an ultrasonic aspirator. Occasionally, the tumourmay involve one of the ‘poles’ of the hemisphereand the excision may entail a partial lobectomy.Although a craniotomy with radical tumour excision will alleviate the symptoms of raised intracranial pressure, there has been controversyas to whether a radical resection improves sur-vival. Most high-grade gliomas weigh approxi-mately 100 g at the time of diagnosis and consistof 1011 cells. A radical tumour excision is able toexcise the macroscopic tumour but cannot re-move the tumour cells that are infiltrating deepinto the adjacent, often vital, areas of normal oroedematous brain. Consequently, a radical exci-sion is unlikely to achieve more than a 90–95% reduction in tumour cell numbers, resulting in1010 cells remaining. Whether the 1–2 logs of tumour cell reduction are a significant reductionin tumour burden prior to adjuvant therapy and whether it improves the effectiveness of subsequent treatment is still not completely resolved, although recent clinical studies doseem to show a survival benefit following tu-mour resection and this is favoured by most neurosurgeons provided the tumour excision can be performed without causing significantneurological mortality.
Alternatively, a biopsy, which can be per-formed most accurately using stereotactic meth-ods, may be undertaken to obtain the definitehistological diagnosis, without macroscopic tu-mour excision, if:• the tumour is small and deep seated• the tumour is diffuse, without major featuresof raised intracranial pressure, and macroscopicresection is not feasible• the tumour involves highly eloquent areas(e.g. speech centre) without pronounced featuresof raised intracranial pressure.
Stereotactic biopsy involves localization of thetumour with a stereotactic frame applied to thehead of the patient using the CT scan or MRI. The three-dimensional coordinates of the tumourare ascertained. The surgeon chooses the point ofentry and the desired path through the brain anda computer program determines the necessaryangles for the biopsy probe and the depth to thetumour (Fig. 6.10).
Postoperative careThe postoperative management of astrocytomainvolves the routine care of a patient following acraniotomy. Careful neurological observationsare performed, as prompt intervention is essen-tial if the patient’s neurological state deterioratesas a result of either increasing cerebral oedema orpostoperative haemorrhage. A postoperativehaematoma may occur in the region of the tu-mour excision or it may be extracerebral, eithersubdural or extradural. A CT scan should be performed urgently if there is neurological deterioration, to determine the exact pathology.Occasionally, postoperative deterioration may be so rapid as to require urgent re-exploration
BRAIN TUMOURS 73
Fig. 6.10 Schematic diagram of stereotactic biopsy ofcerebral tumour using the Cosman–Roberts–Wells(CRW) system.
KAY6 12/16/04 7:39 PM Page 73

74 CHAPTER 6
of the craniotomy without prior radiological assessment.
In the initial postoperative period it is essentialto avoid overhydration of the patient so as not toprecipitate cerebral oedema. The patient isnursed with the head of the bed elevated 20°, soas to promote venous return and reduce intra-cranial venous pressure. Steroid medication isusually required in the initial postoperative period and is gradually decreased over the following days. The steroids may need to be re-instituted during the course of radiotherapy.
The patient is usually mobilized as soon aspossible, if necessary with the help of a physiotherapist.
Radiation therapyPostoperative radiation therapy is generally aneffective adjunct to surgery in the treatment ofhigher-grade gliomas. It has been shown to double the median survival for high-gradegliomas to 37 weeks.
Radiation treatment is planned to optimize thehomogeneity of the radiation dose throughoutthe tumour volume selected and to minimizehigh dose regions in normal brain transited bythe radiation beam. The size of the daily radiationfraction is related to the incidence of complica-tions and a maximal daily dose is usually be-tween 1.8 and 2.0 gray. The total radiation dosevaries depending on the tumour type, locationand size of field, but for gliomas it is usually be-tween 45 and 60 gray. Opinion varies regardingthe tissue volume that should be treated for ma-lignant glioma but radiation to the tumour areaand a ‘generous volume’ of surrounding brain isnow advocated, rather than radiation to thewhole brain. The selection of the proper radiationdose for gliomas is as controversial. Although in-creasing the radiation dosage from 50 to 65 graydoes slightly improve survival, the higher doseof radiation therapy, especially over 65 gray, sig-nificantly increases the risk of brain necrosis.
PrognosisAt present there is no satisfactory treatment forthe malignant cerebral glioma — the anaplasticastrocytoma and glioblastoma multiforme. The
median survival following surgery is approxi-mately 17 weeks and when radiation therapy isused as an adjuvant the median survival is ap-proximately 37 weeks. Chemotherapy for high-grade gliomas has been disappointing and thebest results with surgery, radiation therapy andchemotherapy consistently show a median sur-vival time of less than 1 year. The median normalfor the low-grade glioma (fibrillary astrocytoma;WHO Grade II, Daumus–Duport Grades I and II)is approximately 8 years, with most tumours pro-gressing to a higher grade.
The role of surgery, radiation therapy andother adjuvant therapies in low-grade gliomas iseven less certain than for the high-grade glioma.The low-grade tumour may remain relativelyquiescent for some years before it either con-tinues to grow slowly or changes to a moreanaplastic tumour with resulting debilitatingneurological deterioration. In general, the sameprinciples for surgical excision apply for low-grade gliomas as for high-grade gliomas. How-ever, a number of clinical studies have shownthat patients having a radical excision of a tu-mour have a longer 5-year survival than thosewith a subtotal excision. Radiation therapy hasnot been shown to improve the survival in pa-tients with low-grade tumours. In general, otheradjuvant therapies are not used for the treatmentof low-grade astrocytoma, but may be of benefitfor oligodendrogliomas.
Other adjuvant therapiesMany different adjuvant therapies have been in-vestigated for the treatment of glioma. These in-clude the use of new chemotherapeutic agents,new methods of administering cytotoxic chemi-cals, immunotherapy, hyperthermia, new tech-niques of radiotherapy, photodynamic therapy,and gene therapy.
The lack of effectiveness of the present treat-ment of gliomas is related to the biology of the tu-mour. The most common position for tumourrecurrence following conventional treatment islocally, in the tumour bed, indicating that treat-ment has failed in local control. Although lightmicroscopy shows high-grade gliomas to have arelatively well-defined border with the adjacent
KAY6 12/16/04 7:39 PM Page 74

brain, special staining techniques, includingmonoclonal antibodies, show malignant cells ex-tending well out into the surrounding brain. It isthe failure to control the growth of these cells thatis largely responsible for the local tumour recur-rence. As indicated previously, a good surgicalresection with 90% of the tumour excised wouldstill result in 1010 cells being present. Effective ra-diotherapy will result in 1 log (90%) or at the most2 logs (99%) of cell kill and it is unlikely that sub-sequent chemotherapy would reduce remainingtumour cells by more than 90%. Consequently,the effect of cytoreductive surgery, radiotherapyand chemotherapy would result in approxi-mately 108 cells remaining; the immune system is unlikely to be able to cope with a tumour burden of more than 105 cells. It follows that, forany extra treatment to be effective, whethersurgery or adjuvant therapy, it must provide atleast 1 log of cell kill.
ChemotherapyConventional chemotherapy has been disap-pointing. Many of the chemotherapy agents thatare active in vitro, or in other systemic tumours,have reduced activity in malignant brain tu-mours, either by exerting an inherently limitedcytotoxic potential on brain tumour cells or bythe inability of the chemotherapeutic agent toreach the cells that are responsible for the tumourrecurrence. A study of brain tumour cell kineticsof high-grade gliomas shows only a small pro-portion of the cells (5–10%) in an active growthphase; this has serious consequences for any cellcycle-specific cytotoxic agent. Until recently themost commonly used single agent cytotoxicregime involves administration of nitrosoureacompounds. The high lipid solubility and lowionization of these agents ensures a relatively ef-fective penetration of the cytotoxic compoundinto the tumour. Combination therapy, utilizingmany different cytotoxic compounds, has beenused in various trials but none of the combina-tions has been shown to be more beneficial thanthe use of the single nitrosourea.
Temozolomide is an alkylating agent that canbe taken orally, penetrates the CNS and is welltolerated with predictable myelotoxicity. Clinical
studies have shown it to be effective in about 40%of patients. It is now the initial chemotherapyagent of choice, but it is usually used at the timeof tumour recurrence, rather than as an adjuvantto surgery.
It has been postulated that a reason for the lackof effectiveness of chemotherapy is the inabilityof the cytotoxic compound to reach the tumourcells which are invading the normal adjacentbrain. This has resulted in new techniques of delivering the cytotoxic agent. High-dosechemotherapy with bone marrow rescue haslargely been abandoned because of its high morbidity and lack of effectiveness. Techniquesof disrupting the blood–brain barrier have beenused before chemotherapy infusion to improvethe delivery of chemotherapeutic agents to tu-mour cells within the environment of a normalblood–brain barrier. This has resulted in substan-tially increased neurotoxicity to the normal brainwithout significantly improving survival. Intra-carotid chemotherapy suffers from serious limi-tations — the perfusion of the tumour mass is lessthan expected because most tumours are not supplied entirely by one carotid artery and‘streaming’ of the cytotoxic agent results in very high doses of chemotherapy to small areas,with relative hypoperfusion in other regions.Complications such as serious retinal damageand neurotoxicity have further reduced the attractiveness of this technique.
RadiotherapyAttempts to enhance the effect of radiotherapyhave included the use of radiosensitizers, such asmetronidazole and misonidazole, which increasethe radiosensitivity of hypoxic tumour cells with-out a corresponding increase in the sensitivity ofeuoxic cells. However, the clinical trials haveshown only a marginal advantage. The use of in-terstitial brachytherapy, involving stereotacti-cally implanted radioactive sources into thetumour, has the advantage of applying a highdose of radiotherapy to the tumour while sparingthe surrounding brain. However, the clinical trials performed so far have resulted in a high in-cidence of radionecrosis to the surrounding brainand improvements in the technique will need to
BRAIN TUMOURS 75
KAY6 12/16/04 7:39 PM Page 75

76 CHAPTER 6
be devised before this method would become acceptable. Similarly, stereotactic radiosurgery,that involves radiation to a very highly focusedarea, is of limited use as it does not target the infiltrative tumour cells that are responsible fortumour recurrence.
HyperthermiaThis has inherent basic limitations as, althoughcell death occurs at approximately 42°C, damageto the surrounding brain occurs at 45°C, so there isa very narrow therapeutic index. In addition, thereis a marked tolerance of tumour cells to hyperther-mia and the treatment has not been effective.
ImmunotherapyThe possibilities for immunotherapy as an adjuvant treatment have been investigated formany years. Investigations have included the use of active immunotherapy techniques and, more recently, the application of adoptive immunotherapy. This technique involves stimu-lating peripheral blood lymphocytes in vitro withhuman recombinant interleukin-2 to producelymphokine activated killer cells (LAK cells)which can be administered in conjunction withinterleukin-2. However, the LAK cells do notcross the blood–brain barrier and so need to beinjected in close proximity to the tumour cells.Recent studies using this technique have beendisappointing.
Photodynamic therapyThis is a technique that offers special advantagesas an adjuvant therapy of malignant brain tu-mours since it has been shown to be an effectivemethod of controlling local tumours. The tech-nique involves the selective uptake of sensitizerinto the brain tumour, followed by open or intra-operative irradiation of the sensitized tumourcells with light of an appropriate wavelength toactivate the sensitizer and selectively destroy thetumour cells. Clinical studies using this methodhave shown a favourable trend, although formalphase III studies have not been undertaken.
Gene therapyExperimental therapies of glioma at present
being investigated involve the use of retrovirus,adenoviruses or adeno-associated viruses tocarry a variety of gene therapies to the cancer cell.It is hoped that as these treatments are refinedover the next decade they will be useful in thetreatment of cerebral glioma.
Oligodendroglioma
Oligodendrogliomas are responsible for approximately 5% of all gliomas and occurthroughout the adult age group with a maximalincidence in the 5th decade. The tumour is rare inchildren.
Pathology
Nearly all oligodendrogliomas occur above thetentorium; most are located in the cerebral hemispheres and about half of these are in thefrontal lobes. Oligodendrogliomas may projectinto either the 3rd or lateral ventricles.
Oligodendrogliomas have the same spectrumof histological appearance as astrocytomas, rang-ing from very slow growing, benign tumours to amore rapidly growing, malignant variety withabundant mitotic figures, endothelial prolifera-tion and foci of necrosis. Calcium deposits arefound by histological examination in up to 90% ofoligodendrogliomas. Unlike the astrocyte group,most oligodendrogliomas are well differentiated.Not infrequently tumours have mixed histology,with both oligodendroglial and astroglial features.
Clinical presentation
The presenting features are essentially the sameas for the astrocyte group but, as these tumoursare more likely to be slow growing, epilepsy iscommon, occurring in 80% of patients and seenas an initial symptom in 50%. The features ofraised intracranial pressure and focal neurologi-cal deficits are each present in approximatelyone-third of patients.
As for astrocyte tumours, MRI with contrastmay be beneficial but other investigations areusually unnecessary.
KAY6 12/16/04 7:39 PM Page 76

Radiological investigation
CT scanning and MRI are the fundamental inves-tigations. They will confirm the diagnosis of anintracranial tumour and in many cases the diag-nosis of oligodendroglioma will be highly proba-ble. Calcification will be present in 90% of casesand over half show contrast enhancement (Fig.6.11).
Treatment and results
Treatment involves:• surgical resection• radiotherapy• other adjuvant treatments.
The standard treatment for oligodendrogliomahas been an aggressive resection of the tumourfollowed by radiation therapy, although radio-therapy would now not be given to low-grade tu-mours, and utilized only for the intermediate- orhigh-grade oligodendroglial tumours. Oligoden-drogliomas have been shown to be more sensi-tive to chemotherapy than the astrocytomatumours, especially if the oligodendrogliomasbelong to the group with loss of heterozygosityOF chromosome 1p or 19q.
The survival of patients depends on the degree
of histological malignancy. Five-year survivalrates are between 30 and 50% with a small num-ber of patients living for many years (up to 5% for20 years). However, many tumours with histo-logical features of oligodendroglioma also have acomponent of astrocyte-derived cells, usuallyanaplastic astrocytoma, and the tumour behavesbiologically and clinically as an anaplastic astro-cytoma rather than an oligodendroglioma.
Recurrent cerebral glioma
As discussed earlier, most high-grade cerebralgliomas will recur within 1 year of the initialtreatment with surgery and radiotherapy. Low-grade tumours may either recur as a continuingprogression of the slow growth or, alternatively,the histological characteristics may alter and the tumour may become more anaplastic andrapidly growing.
The clinical presentation of a recurrent tumourwill be evidenced by either a progression of thefocal neurological signs or the signs of an increasein the intracranial pressure. The diagnosis will beconfirmed by CT scan or MRI in most cases. Themajor differential diagnosis is postradiotherapyradiation necrosis, which may develop as early as4 months or as late as 9 years after radiotherapy.
BRAIN TUMOURS 77
Fig. 6.11 Oligodendrogliomas. (a) Non-enhancing low-grade calcified tumour. (b) Contrast-enhancing high-grade oligodendroglioma.
(a) (b)
KAY6 12/16/04 7:39 PM Page 77

78 CHAPTER 6
The radiological features of necrosis are an avas-cular mass, and the diagnosis may be suspectedfrom the dose of radiotherapy that has been administered. However, there may be consider-able difficulty in differentiating necrosis from recurrent glioma, and sometimes an operation is required both for definitive diagnosis and to remove the mass.
The initial deterioration following a diagnosisof recurrent glioma can usually be temporarilyhalted by the use of steroid medication. Themajor decision is whether further surgery andother adjuvant therapy should be undertaken. Ingeneral, a further operation involving debulkingof the tumour would be considered if:• the patient is less than 65 years old• there has been a symptom-free interval of 1 year or more since the first operation• debilitating irreversible neurological signs areabsent• the tumour is in an accessible position and repeat surgery would not result in additionalmorbidity.
Adjuvant therapies
Adjuvant therapies have limited benefit for pa-tients with recurrent tumour and, consideringthe morbidity involved, may not be indicated.Chemotherapy, utilizing temozolomide adminis-tered orally, has shown to have a temporary ben-efit in up to 40% of patients. Other chemotherapyagents, especially the nitrosourea compounds,have much greater toxicity.
Ependymoma
Ependymomas are glial neoplasms arising fromthe ependyma and constitute approximately 5% of all gliomas. Approximately two-thirds ofependymomas occur in the infratentorial com-partment and most of these present in children,adolescents and young adults. The supraten-torial ependymomas occur mostly in adults.
Pathology
The tumour arises from the ependyma of the ven-
tricle and, although predominantly intraventric-ular, the tumour often invades into the adjacentcerebellum, brainstem or cerebral hemisphere.Fourth ventricular tumours usually arise fromthe floor or lateral recess of the 4th ventricle andthey may extend into the subarachnoid space toencase the medulla or upper cervical spinal cord.Alternatively, the tumour may grow laterallythrough the foramen of Luschka and into thecerebellopontine angle.
The tumours are well demarcated, nodular,soft and pale. Calcification is common, especiallyin supratentorial ependymomas.
There are numerous histological classificationsystems of ependymomas, and the World HealthOrganization classification divides these tu-mours into cellular, papillary and clear cell typesof non-anaplastic ependymoma and anaplasticependymoma.
The myxopapillary variety is a slow-growingdistinct variant of ependymoma that occurs inthe cauda equina and is discussed in the chapteron spinal cord tumours (Chapter 15).
In an adult the subependymoma variant maybe encountered as an incidental autopsyfinding — a discrete nodular mass based in thebrain’s ventricular surface, particularly the flooror lateral recess of the 4th ventricle or the septumpellucidum — or it may be large enough to pre-sent clinically. It is usually heavily calcified and iscomposed of cells with astrocytic as well asependymal features.
The papillary and anaplastic varieties ofependymoma are responsible for the majority ofclinically symptomatic ependymomas. The cellu-larity and architecture of the ependymomas varybut a diagnostic feature is the presence of rosettes,and most ependymomas contain areas in whichperivascular pseudorosettes are conspicuouslydeveloped. In these formations the blood vessel issurrounded by an eosinophilic halo composed ofthe radiating tapering processes of the cells. Ble-pharoplasts frequently occur in ependymomasbut may be difficult to visualize. These are tiny intracytoplasmic spherical or rod-shaped struc-tures which represent the basal bodies of cilia,and are most frequently encountered in the apicalportion of cells that form ependymal rosettes.
KAY6 12/16/04 7:39 PM Page 78

Clinical presentation
Posterior fossa ependymomasDetails will be discussed in the section on paedi-atric tumours (p. 91). Patients present with fea-tures of raised intracranial pressure due tohydrocephalus as a result of obstruction of the4th ventricle, ataxia due to cerebellar involve-ment, and occasionally features of brainstempressure or infiltration.
Supratentorial tumoursVirtually all patients with supratentorial ependy-momas present with features of raised intracra-nial pressure, often due to hydrocephalus as aresult of obstruction of the CSF pathways. Ataxiais common and focal neurological deficits mayoccur due to involvement of the underlying cere-bral hemisphere.
Radiological investigation
The CT scan and MRI will show a tumour thatarises in the ventricle and enhances after admin-istration of intravenous contrast. Calcification iscommon in tumours arising from the lateral ven-tricles (Fig. 6.12). There is frequently associatedhydrocephalus. In the posterior fossa differentia-tion from a medulloblastoma may be difficult.
Treatment
The treatment of ependymomas is initially surgi-cal, with an attempt to perform a radical macro-scopic resection of the tumour. Supratentorialtumours are often very large and may extendthroughout the lateral and 3rd ventricles, but theassociated hydrocephalus makes the excision ofthe intraventricular portion feasible. However,the tumour may arise from the ventricular wall inthe region of the basal ganglia and blend imper-ceptibly with the underlying cerebral structuresso that a complete excision is not possible. Fourthventricular tumours can be excised from the ven-tricle but microscopic infiltration into the under-lying brainstem cannot be removed surgically.Postoperative radiation therapy is advisable and,as these tumours may spread through the CSF
pathways, sometimes whole neuraxis radiationis recommended.
The prognosis is related to the degree ofanaplasia of the tumour and for intratentorial tu-mours varies from 20% to 50% 5-year survival.The prognosis for the supratentorial tumours isbetter, particularly in adults.
Pineal tumours
Tumours arising in the region of the pineal glandare mostly not of pineal origin, but are generallycalled ‘pineal’, as they have a similar clinical presentation.
The tumours are relatively uncommon, ac-counting for 0.5% of all intracranial tumours.However, they occur more frequently in Japanand China, where the incidence is up to 5%. Mosttumours make their clinical appearance between10 and 30 years of age.
Classification
Pineal region tumours are classified in decreas-ing frequency as:
BRAIN TUMOURS 79
Fig. 6.12 Calcified contrast-enhancing ependymomainvolving lateral ventricles.
KAY6 12/16/04 7:39 PM Page 79

80 CHAPTER 6
• germinoma• teratoma• pineocytoma• pineoblastoma• miscellaneous:
• glioma• cyst.Germinoma is the most common pineal region
tumour and is similar in histological appearanceto germinoma of the gonads and mediastinum; itoccurs predominantly in males. These tumoursmay also arise in the suprasellar region, and synchronous tumours in both the pineal andsuprasellar region occur occasionally. Teratomais like germinoma; it also arises from displacedembryonic tissue. The other tumour types occurless commonly.
Clinical presentation
Patients with pineal tumours present with:• raised intracranial pressure• neurological signs due to focal compression• endocrine disturbance.
Raised intracranial pressure. The features of raised intracranial pressure, such as headaches,drowsiness and papilloedema, are due to hydrocephalus, which is a result of the tumouroccluding the aqueduct of Sylvius.
Focal compression. Compression of the efferentcerebellar pathways in the superior cerebellar peduncle results in limb ataxia and distortion ofthe quadrigeminal plate, produces limitation ofupgaze, convergence paresis with impairment of reaction of pupils to light and accommodation(Parinaud’s syndrome), and may result in convergence-retraction nystagmus on upgaze(Koerber–Salius–Elschnig syndrome).
Endocrine disturbance. Endocrine disturbances areuncommon but include precocious puberty in10% of patients, almost invariably male, and diabetes insipidus in 10%. The endocrine effectscan either be due to direct tumour involvement ofthe hypothalamus or result from the secondaryeffects of hydrocephalus.
Radiological investigationsCT scan and MRI will show a pineal region tumour and will often suggest the correct pathol-ogical diagnosis (Fig. 6.13). On CT scan, beforecontrast, a germinoma will be a hyperdense le-sion in the region of the pineal gland infiltratinginto the surrounding tissue and there will be uni-form vivid enhancement following intravenouscontrast. Calcification is uncommon. On MRIgerminomas are relatively isointense to normalwhite matter on T1-weighted images and slightlyhyperintense on T2-weighted scans. Gadoliniumcontrast defines the tumour well as germinomasenhance markedly and homogeneously.
Management
This consists of surgery and radiotherapy.A ventriculoperitoneal shunt or drainage of
CSF by a 3rd ventriculostomy may be required ifthe hydrocephalus is severe.
There is controversy over whether the defini-tive treatment should be an attempt at surgicalexcision or radiotherapy. As most of the tumoursare germinomas, and these tumours are very radiosensitive, a course of radiotherapy can begiven as the initial treatment if the radiologicalappearance is typical for germinoma. If serial CTscans show the tumour has failed to respond toradiotherapy then surgery may be necessary. Alternatively, if the features on the initial CT and MRI scans are atypical, and the lesion doesnot resemble a germinoma, exploration of the tu-mour and surgical excision may be appropriateas the initial procedure.
The preferred surgical approach is usually by aposterior fossa craniotomy, above the cerebellumand below the tentorium cerebelli. Alternativesupratentorial surgical exposures include ap-proaching the tumour through the corpus callo-sum or by retracting the occipital lobe.
Metastatic tumours
Metastatic tumours are responsible for approxi-mately 15% of brain tumours in clinical series butup to 30% of brain tumours reported by patholo-gists. Approximately 30% of deaths are due to
KAY6 12/16/04 7:39 PM Page 80

cancer and 1 in 5 of these have intracranialmetastatic deposits at autopsy. The metastatic tumours most commonly originate from:• carcinoma of the lung• carcinoma of the breast• metastatic melanoma• carcinoma of the kidney• gastrointestinal carcinoma.
In 15% a primary origin is never found.Most metastatic tumours are multiple and one-
third are solitary. In about half of these systemicspread is not apparent. The incidence of tumoursin the cerebrum relative to the cerebellum is 8 : 1,and most occur in the distribution of the middlecerebral artery. The size of the tumours may vary considerably if the deposits are multiple.Metastatic tumours are often surrounded by intense cerebral oedema.
Clinical presentation
The interval between diagnosis of the primarycancer and cerebral metastases varies consider-ably. In general, secondary tumours from carci-noma of the lung present relatively soon after the initial diagnosis, with a median interval of 5months. Although cerebral metastases may pre-sent within a few months of the initial diagnosisof malignant melanoma or carcinoma of thebreast, some patients may live many years (up to15 years) before an intracranial tumour appears.
The presenting features are similar to those described for other intracranial tumours:• raised intracranial pressure• focal neurological signs• epileptic seizures.
Headache and vomiting, indicative of raisedintracranial pressure, occur in most patients andthe presenting history is usually short, often onlya few weeks or months. The increased intracra-nial pressure will be caused by either the tumourmass and surrounding oedema or, in posteriorfossa tumours, obstructive hydrocephalus.
The pattern of focal neurological signs will de-pend on the position of the tumour deposits andthe patient may present with a progressive hemi-paresis or speech disturbance with supratentorialtumours or gait ataxia with cerebellar tumours.
BRAIN TUMOURS 81
Fig. 6.13 MRI in coronal (a), sagittal (b) and axial (c)plane showing pineal region germinoma causingobstructive hydrocephalus.
(a)
(b)
(c)
KAY6 12/16/04 7:39 PM Page 81

82 CHAPTER 6
Epileptic seizures occur in approximately 25% of patients and may be either focal or generalized.
Occasionally, metastases, especially melanomaor choriocarcinoma, present following an intra-cerebral haemorrhage.
Radiological investigations
CT scan or MRI will diagnose the metastatic tu-mour and will show whether the deposits aresolitary or multiple (Fig. 6.14). Most metastatictumours are relatively isodense on the unen-hanced CT scan and they enhance vividly afterintravenous contrast injection. Tumours that maybe hyperdense prior to contrast are melanoma,choriocarcinoma, mucoid adenocarcinoma (e.g.from the gastrointestinal tract) and 50% of lymphomas. There is usually considerable sur-rounding cerebral oedema with distortion of the ventricular system.
MRI following gadolinium contrast willdemonstrate small metastatic tumours often notvisible on the CT scan (Fig. 6.15).
Fig. 6.14 Multiple contrast-enhancing tumours typicalof metastatic melanoma.
Treatment
Steroid medication (e.g. dexamethasone) willcontrol cerebral oedema and should be com-menced immediately if there is raised intracra-nial pressure.
Surgery to remove the metastasis is indicated if:• there is a solitary metastasis in a surgically accessible position• there is no systemic spread.
Removal of a solitary secondary is preferableonly if the primary site of origin has been, or willbe, controlled. However, excision of a singlemetastasis will provide excellent symptomaticrelief and consequently may be indicated even ifthe primary site cannot be treated satisfactorily.Surgery is, of course, mandatory if the diagnosisis uncertain.
Radiotherapy, together with steroid medica-tion to control cerebral oedema, is used to treatpatients with multiple cerebral metastases andmay be advisable following the excision of a single metastasis. The treatment, up to 45 gray, is usually given in a 2-week course.
Over the past decade stereotactic radiosurgeryutilizing a highly focused beam of radiation hasbeen used to treat single and multiple cerebralmetastases. The therapy does seem to be effectivein some cases and its role relative to surgery isbeing evaluated.
Anticonvulsant medication is given both to patients who have suffered epileptic seizures and as a prophylactic measure.
PrognosisAbout 30% of patients with solitary metastaticdeposits from carcinoma of the lung ormelanoma and 50% of patients with carcinoma ofthe breast survive 1 year following surgical exci-sion. In those patients where the source of themetastatic tumours is undetermined, about 50%survive 1 year.
Leptomeningeal metastases
Meningeal carcinomatosis is widespread, multi-focal seeding of the leptomeninges by systemiccancer. The clinical presentation includes:
KAY6 12/16/04 7:39 PM Page 82

• hydrocephalus, causing headaches and vomiting• cranial nerve abnormalities due to direct invasion by the tumours• spinal root involvement due to local infiltration.
The CT scan or MRI findings may be subtle butfrequently show excessive enhancement of themeninges. Lumbar puncture can be performed if there is no evidence of raised intracranial pressure. Malignant cells may be seen in the CSF, the protein concentration is increased andthe glucose reduced.
Cerebral lymphoma
The term cerebral lymphoma encompasses anumber of distinct pathological and clinical entities. Current nomenclature divides cerebrallymphoma into: non-Hodgkin’s lymphoma orHodgkin’s disease; primary or secondary dis-ease; and patients who are immunocompetent orimmunosuppressed.
Historically, lymphoma involving the CNSwas considered to be rare, being less than 3% ofall CNS tumours, with about half of these lym-phomas being primary cerebral lymphoma, thatis, the tumour being confined entirely to the CNS.Over the past decade there has been an unprece-dented increase in the incidence of cerebral lym-phoma, which can be attributed to at least twoknown factors: the acquired immune deficiencysyndrome (AIDS) epidemic and the use of im-munosuppressive therapy. However, there hasalso been an unexplained increase in the inci-dence of primary cerebral lymphoma in non-immunosuppressed patients.
Cerebral lymphoma may be secondary to sys-temic lymphoma and in large studies of patientswith systemic lymphoma, up to 30% of patientsdevelop clinical or pathological evidence of cere-bral involvement. However, almost all cases areassociated with either relapsed or progressivesystemic disease and an isolated CNS relapse isvery rare.
BRAIN TUMOURS 83
Fig. 6.15 MRI following gadolinium shows multiplesmall metastatic tumours.
(a)
(b)
(c)
KAY6 12/16/04 7:39 PM Page 83

84 CHAPTER 6
Intracerebral Hodgkin’s disease is a very rareentity.
Clinical presentation
The most common site for primary cerebral lymphoma is in the frontal lobe, followed by thetemporal lobe, parietal lobe and deep nuclei. Tumours may also occur in the cerebellum andbrainstem. The tumours may be either solitary ormultiple and primary leptomeningeal diseasehas been reported in up to 10% of primary cere-bral lymphoma.
There are no pathognomonic presenting symp-toms or signs in primary cerebral lymphoma andthe presenting features are similar to those de-scribed for other intracranial tumours: raised in-tracranial pressure, focal neurological signs andepileptic seizures. The high frequency of frontallobe involvement results in a common mode ofpresentation as memory loss, forgetfulness andaltered affect. Up to 10% of patients with primarycerebral lymphoma present with a seizure. Inview of the incidence of multiple lesions, it is not surprising that many patients present with aconstellation of symptoms and signs. The pre-senting features in primary cerebral lymphomaarising in immunodeficient patients (includingAIDS-related primary cerebral lymphoma) do not appear to be different from those in im-munocompetent patients with primary cerebrallymphoma.
Radiological investigations (Figs 6.16 and 6.17)
The CT scan characteristically shows a hypo-dense or isodense or sometimes hyperdense tumour, which enhances following contrast injection with associated mild to moderate oedema. Multifocal disease is observed in about40% of CT scans. Most primary cerebral lym-phomas arise in the periventricular region. MRIis now the investigation of choice for primarycerebral lymphoma. The lesions are usually hy-pointense to isointense on T1-weighted imagesand isointense to hyperintense on T2-weightedimages. The tumours enhance following intra-venous injection of gadolinium.
Although CSF examination may show a popu-lation of abnormal lymphocytes, concern regard-ing raised intracranial pressure usually preventsa lumbar puncture being performed in the major-ity of patients.
Management
The principles concerning the management ofprimary cerebral lymphoma involve:• histological diagnosis• ensuring that the disease is confined to the brain• excluding an underlying, predisposing illness• instituting appropriate therapy.
The usual sequence of events is a CT and MRIscan followed by a biopsy proving intracerebrallymphoma. In general, it is thought appropriate
Fig. 6.16 (a) MRI and (b) CT of cerebral lymphoma.(a) (b)
KAY6 12/16/04 7:39 PM Page 84

to exclude systemic disease, although concurrentcerebral and systemic lymphoma is uncommon.Patients usually undergo bone marrow aspirateand trephine, chest X-ray, CT scan of the chestand abdomen and testing for evidence of HIV infection.
Surgical treatmentThere is no clear evidence that craniotomy withexcision of the lymphoma is superior to obtain-ing an accurate tissue diagnosis using a stereotac-tic biopsy. It must be noted that the early use ofcorticosteroids, to treat cerebral oedema, maymake histological assessment difficult due to theexquisite sensitivity of primary cerebral lym-phoma to steroids. The tumour may disappearon the CT scan or MRI after the commencementof corticosteroids and this has significant impli-cations for obtaining a stereotactic biopsy.
RadiotherapyPrimary cerebral lymphoma is usually radiosen-sitive with a clinical response rate of up to 80%.However, cranial radiotherapy alone as a treat-ment for primary cerebral lymphoma rarely produces long-term survivors, despite the highresponse rate and an improvement in mediansurvival time to 15 months.
ChemotherapyNumerous chemotherapy regimes have been re-ported, including the use of both intrathecal andintravenous therapies which can be given priorto, synchronous with, or following radiotherapy.The most commonly used drugs are those used in
the therapy of systemic non-Hodgkin’s lym-phoma and include methotrexate, cortico-steroids, anthracyclines, vinca alkaloids,cytosine, arabinoside and alkylating agents. Me-dian survival times of up to 44 months have been reported. However, methotrexate given after radiotherapy increases the risk of leukoen-cephalopathy with consequent serious neuro-psychological impairment. The need forpostchemotherapy radiation has been ques-tioned, in view of the effectiveness of chemother-apy, especially in the elderly.
Paranasal sinus tumours
Tumours of the paranasal sinuses may spread di-rectly to involve the brain. These uncommon tu-mours most frequently arise from the ethmoid ormaxillary sinuses, less frequently from the sphe-noid sinus and rarely from the frontal sinus. Thetumours invade through the floor of the anteriorcranial fossa in the region of the cribriform plateand may extend through the dura into the frontallobe (Fig. 6.18). The tumours are usually squa-mous cell carcinoma and less frequently adeno-carcinoma or adenoid cystic adenocarcinoma.The aesthesioneuroblastoma is a rare nasal
BRAIN TUMOURS 85
Fig. 6.17 Autopsy specimen of cerebral lymphoma.
Fig. 6.18 Carcinoma of the ethmoid extendingthrough the cribriform plate into the anterior cranialfossa.
KAY6 12/16/04 7:39 PM Page 85

86 CHAPTER 6
tumour arising from the olfactory epitheliumthat may invade through the cribriform plate.
The patients usually present with a blood-stained or purulent nasal discharge and pain inthe involved region. CSF rhinorrhoea may occurif the dura has been breached.
Surgical excision using a craniofacial resectionmay be the only method of controlling these tu-mours and, if the tumour has spread into theorbit, an adequate resection may involve orbitalexenteration.
Chordomas
Chordomas are rare tumours arising from noto-chord cell nests. They may arise throughout thecraniospinal axis but occur predominantly at theends of the axial skeleton in:• the basioccipital region• the sacrococcygeal region.
The intracranial chordoma presents as a skullbase tumour. It infiltrates and erodes the sphe-noid and basiocciput and may spread into thepetrous bones, the paranasal sinuses, the sellaturcica and the cavernous sinuses. The tumourwill compress and distort the adjacent brain andengulf the cranial nerves and arteries.
These tumours do not have histological fea-tures of malignancy and only rarely metastasize.However, it is not usually possible to excise thecranial tumours completely; most patients diewithin 10 years of initial presentation.
Spinal chordomas occur predominantly in thesacrococcygeal region, although they may alsoarise in the cervical area. Like the cranial tu-mours, spinal chordomas invade and destroybone and compress adjacent neural structures.Remote metastases occasionally occur. Patientswith spinal chordomas present with back pain,radicular pain and slowly progressive lum-bosacral nerve root involvement resulting insphincter difficulties and sensory and motor dis-turbances in the legs.
Histological appearance
The tumours consist of notochord cells and mu-coid stroma. Many of the cells may be coarsely
vacuolated and some will contain a single large vacuole giving a ‘signet ring’ appearance.The characteristic histological appearance isphysaliphorous (bubble-bearing) cells contain-ing multiple vacuoles.
Clinical presentation
The majority of intracranial chordomas arise be-tween 20 and 60 years of age. The clinical featuresresult from the widespread tumour extensionand include:• raised intracranial pressure, causingheadaches and vomiting• multiple cranial nerve palsies, often unilateral• nasopharyngeal obstruction.
The radiological appearances are of a destruc-tive lesion at the base of the skull or in the verte-bral bodies (Fig. 6.19).
Treatment
It is rarely possible to excise all the tumour. Post-operative radiotherapy is usually administeredbut is of doubtful value.
Paediatric tumours
Intracranial tumours are the most common formof solid tumours in childhood, with 40% of the
Fig. 6.19 Sacral chordoma. A destructive tumourextending into the vertebral canal.
KAY6 12/16/04 7:39 PM Page 86

tumours occurring above the tentorium cerebelli.The most common supratentorial tumours areastrocytomas, followed by anaplastic astrocy-tomas and glioblastoma multiforme. Cranio-pharyngioma occurs more commonly in childrenthan in adults and is situated in the suprasellarregion; this tumour is described in Chapter 8.Other, less common, supratentorial tumours include primitive neuroectodermal tumours(PNETs), ependymomas, ganglioglioma andpineal region tumours.
Posterior fossa tumours
Sixty per cent of paediatric brain tumours occurin the posterior fossa. The relative incidence ofthe tumours is:1 cerebellar astrocytoma 30%2 medulloblastoma (infratentorial primitiveneuroectodermal tumour) 30%3 ependymoma 20%4 brainstem glioma 10%5 miscellaneous 10%:
(a) choroid plexus papilloma(b) haemangioblastoma(c) epidermoid, dermoid(d) chordoma.
Clinical presentationThe presenting clinical features of posterior fossaneoplasms in children are related to:• raised intracranial pressure• focal neurological signs.
Raised intracranial pressureThis is the most common presenting feature. It isdue to hydrocephalus caused by obstruction ofthe 4th ventricle and is manifest by headaches,vomiting, diplopia and papilloedema.
The headaches begin insidiously, gradually be-coming more severe and frequent; they are worstin the early morning. There is usually no specificheadache localization. Vomiting is frequently associated with the headaches and may tem-porarily relieve the headache. Raised intracranialpressure may result in a strabismus causingdiplopia due to stretching of one or both of the6th (abducens) cranial nerves. This is a so-called
‘false localizing sign’. Papilloedema is usuallypresent at the time of diagnosis. In infants, an ex-panding head size is an additional sign of raisedintracranial pressure.
Focal neurological signsThese are due to the tumour invading or com-pressing the cerebellum (nuclei and tracts), thebrainstem and cranial nerves. Truncal and gaitataxia result particularly from midline cerebellarinvolvement. Horizontal gaze paretic nystagmusoften occurs with tumours around the 4th ventri-cle. Upbeat vertical nystagmus is indicative ofbrainstem involvement.
Disturbances of bulbar function, such as diffi-culty in swallowing with nasal regurgitation offluid, dysarthria and impaired palatal and pharyngeal reflexes, result from brainstem in-volvement. In addition, compression or tumourinvasion of the pyramidal tracts may result inhemiparesis and, if the ascending sensory path-ways are involved, sensory disturbance willoccur in the trunk and limbs.
The tumour may directly envelop the lowercranial nerves — glossopharyngeal, vagal, spinalaccessory and hypoglossal — as well as the 7thcranial nerve.
Neck stiffness and head tilt may occur in chil-dren with posterior fossa neoplasms, and may bedue to herniation of a cerebellar tonsil or tumourtissue resulting in dural irritation.
InvestigationsCT scan and MRI have replaced the need for the previous radiological investigations that included radio-isotope brain scanning, air ven-triculography and posterior fossa angiography.The CT scan and/or MRI will show the presenceof a posterior fossa tumour, its position andwhether it arises primarily in the brainstem, 4thventricle or the cerebellum (Figs 6.20–6.24).
ManagementThe treatment of posterior fossa tumours involves:• surgery• radiotherapy• chemotherapy.
BRAIN TUMOURS 87
KAY6 12/16/04 7:39 PM Page 87

88 CHAPTER 6
Fig. 6.20 (a) CT scan. Contrast-enhancingmedulloblastoma arising from the vermis causingobstructive hydrocephalus. (b) MRI scan.Medulloblastoma.
Fig. 6.21 Cystic cerebellar astrocytoma causingobstructive hydrocephalus. There is a contrast-enhancing nodule in a large cyst.
(a)
(b)
A preliminary CSF shunt may need to be per-formed in a child with severely raised intracra-nial pressure due to hydrocephalus. The CSFdiversion can be achieved by either an externaldrain or a ventriculoperitoneal shunt. An exter-nal drain is a temporary measure only, because ofthe risk of infection. Aventriculoperitoneal shuntprovides immediate and controlled relief of intracranial hypertension and the subsequentposterior fossa operation can be performed as a planned elective procedure, rather than anurgent operation in suboptimal conditions. Acriticism of a preoperative ventriculoperitonealshunt is that it might promote the metastaticspread of tumour. A filtering chamber in theshunt system may lessen this risk but this predis-poses to shunt malfunction.
KAY6 12/16/04 7:39 PM Page 88

Steroid medication to control local oedema iscommenced preoperatively. The operation is per-formed in either the sitting or prone positionthrough a vertical midline incision. A posteriorfossa craniotomy is performed, usually with exci-sion of the bone down to and around the foramenmagnum. Tumour excision is aided by the use ofmagnifying loupes and illumination with a fibre-optic headlight, or by the use of an operating microscope.
Postoperative care involves careful monitoringof the neurological signs. Postoperative haemor-rhage or oedema may result in rapid deteriora-tion of the neurological state, and in respiratoryarrest. An urgent CT scan may indicate the causeand site of the problem but the deterioration maybe so rapid that the wound may need to be re-opened without the benefit of prior scanning.
If a ventriculoperitoneal shunt has not been in-serted prior to tumour removal an exacerbationof the obstructive hydrocephalus may occur if the tumour excision has failed to relieve the CSFobstruction. Disturbances of bulbar and lowercranial nerve function may cause difficulty in
BRAIN TUMOURS 89
Fig. 6.22 Contrast-enhancing ependymoma in the 4thventricle causing obstructive hydrocephalus.
(a)
(b)
Fig. 6.23 MRI scan showing (a) pontine glioma, (b) cystic brainstem glioma.
KAY6 12/16/04 7:39 PM Page 89

90 CHAPTER 6
swallowing. Nasogastric feeding may be neces-sary until the protective mechanisms return, andgreat care should be taken to avoid aspiration.
Medulloblastoma
Medulloblastoma, also referred to as an infraten-torial PNET, is a malignant tumour usually aris-ing in the midline from the cerebellar vermis,although it may occur more laterally in a cerebel-lar hemisphere in older patients. The tumour ex-pands to invade the adjacent cerebellum andlarge tumours completely fill the 4th ventricle(see Fig. 6.19).
The tumours arise from the external granularlayer of the fetal cerebellum (Obersteiner’slayer). Histologically the medulloblastoma ishighly cellular, with numerous mitoses. Truerosettes do not occur but the cells are seen in con-centric patterns around homogeneous materialor blood vessels (pseudorosettes).
Presenting features. The presenting features arerelated to hydrocephalus and cerebellar dysfunc-tion. Truncal ataxia is typically present in chil-dren with medulloblastoma but cranial nervedeficits, except for a 6th nerve palsy, are uncom-mon in the early stages.
Surgery. At surgery the cerebellar vermis issplit in the midline and it is usually possible to ob-tain a gross macroscopic excision of the tumourwith complete removal from the 4th ventricle.
Radiation therapy. Medulloblastoma is rela-tively radiosensitive and radiation therapy is recommended to the entire neuraxis because ofthe tendency of the tumours to seed along theCSF pathways.
Chemotherapy. Adjuvant chemotherapy is usually recommended and numerous protocolsusing a variety of chemotherapeutic agents havebeen investigated. There is no uniformity of opinion as to which drugs or routes of adminis-tration are the most effective and whetherchemotherapy should be administered as part ofthe initial treatment plan or only used at the timeof recurrence of the tumour.
Young children are exquisitely sensitive to theneurotoxicity due to radiation therapy, such thatthe possibility of utilizing chemotherapy alone
Fig. 6.24 MRI scan showing glioblastoma invadingthrough the brainstem of a 25-year-old man. Beforeintravenous gadolinium contrast: (a) sagittal T1. Afterintravenous gadolinium contrast: (b) axial and (c)coronal.
(a)
(b)
(c)
KAY6 12/16/04 7:39 PM Page 90

and postponing the use of radiotherapy has beentrialled.
Prognosis. Although the combination of radicalsurgery and irradiation has improved the prog-nosis, the 5-year survival rate is approximately40%.
Cerebellar astrocytoma
The cerebellar astrocytoma is frequently a be-nign, slowly growing cystic tumour which is themost favourable of all the intracranial paediatricneoplasms. The tumours may arise in either thehemisphere or vermis and frequently consist of alarge tumour cyst with a relatively small solidcomponent in the wall of the cyst (see Fig. 6.20).Less frequently the tumour may be entirely solidwith little or no cystic component. Histologically,the solid portion of the tumour is usually a Grade1 or 2 astrocytoma.
Presenting features. The clinical presenting fea-tures are similar to those of a medulloblastoma,but as the tumour may be located more laterallythe presenting features are accompanied by ipsilateral cerebellar disturbance. The duration of symptoms is variable but tends to be longer thanwith medulloblastoma, averaging 6–12 months.
Surgery. Acomplete surgical excision is usuallypossible and it is only necessary to excise thesolid component from the cystic tumour.
Radiation therapy. Postoperative radiation therapy is not usually indicated if an excision has been possible. The prognosis is the mostfavourable of all intracranial childhood tumourswith a cure rate in excess of 75%.
Ependymoma
The ependymoma of the 4th ventricle arises fromthe floor of the 4th ventricle and is attached to,and may infiltrate, the underlying brainstem (seeFig. 6.21).
Pathological features. The pathological featuresand histology are described earlier in the chapter(see p. 78).
Presenting features. The presenting features aresimilar to those described for a medulloblastoma,although the initial symptoms and signs are usu-
ally due to hydrocephalus. Involvement of thedorsal brainstem results in unilateral or bilateralfacial weakness.
Surgery. The surgical excision of the ependy-moma involves splitting the inferior vermis toobtain access to the 4th ventricle. It is usually pos-sible to perform a gross macroscopic excision ofthe tumour from the ventricle and adjacent cere-bellum but, as the tumour often originates fromthe floor of the 4th ventricle, total excision israrely possible.
Radiation therapy. Postoperative radiation ther-apy is usually administered to the posterior fossaand, as the tumour seeds along the CSF path-ways, entire neural axis irradiation is often recommended, particularly in the higher-gradeependymoma.
There is no definite advantage from adjuvantchemotherapy, although it may be used at thetime of tumour recurrence.
Brainstem glioma
The brainstem glioma arises predominantly inthe pons, less frequently in the medulla but mayinfiltrate extensively throughout the brainstem.The tumour infiltrates between the normal structures with a histological appearance vary-ing from the relatively benign astrocytoma toanaplastic astrocytoma and glioblastoma multi-forme. Over 50% of brainstem gliomas examinedat autopsy will have microscopic features ofglioblastoma multiforme.
Clinical presentation. The clinical presentationcharacteristically includes progressive multiplebilateral cranial nerve palsies with involvementof pyramidal tracts and ataxia. Facial weaknessand 6th cranial nerve palsy are common and aninternuclear ophthalmoplegia is indicative of anintrinsic brainstem lesion. The child’s personalityoften changes — they become apathetic. Raisedintracranial pressure is less common than withother paediatric posterior fossa neoplasms, as obstruction of the 4th ventricle or aqueduct ofSylvius occurs late in the illness.
The CT and MRI appearance is of an expandedbrainstem. MRI has considerably improved theaccuracy of the diagnosis (Fig. 6.22).
BRAIN TUMOURS 91
KAY6 12/16/04 7:39 PM Page 91

92 CHAPTER 6
Surgery. Surgical treatment is not usually indi-cated, although either an open or a stereotacticbiopsy may be performed to confirm the diagnosis.
Radiation therapy. Palliative radiation therapyis the only treatment. The tumour usually causesdeath within 24 months of diagnosis, althoughsome patients with low-grade tumours will livelonger.
Chemotherapy has limited benefit.
Further readingApuzzo MJ et al. (1984) Ionising and non-ionising
radiation treatment of cerebral malignant gliomas:specialised approaches. Clinical Neurosurgery 31,470–496.
Bailey P, Cushing H (1971) A Classification of Tumours of the Glioma Group on a Histogenetic Basis with a Cor-related Study of Prognosis. J B Lippincott, Philadelphia,1926. Reprinted Argosy Antiquarian, New York.
Burger PC, Vogel FS (1982) Surgical Pathology of the Nervous System and its Coverings, 2nd edn. John Wiley, New York.
Cairncross JG, Ueki K, Zlatescu MC et al. (1998) Specificgenetic predictors of chemotherapeutic response and survival in patients with anaplastic oligoden-drogliomas. Journal of the National Cancer Institute 90(19), 1473–1479.
Dohrmann GJ, Farwell JR, Flannery JI (1976) Ependy-momas and ependymoblastomas in children. Journalof Neurosurgery 45, 273–283.
Higginbotham NL, Phillips RJ, Farr HW (1979) Chordoma: thirty five year study at the MemorialHospital. Cancer 29, 1841–1850.
Kaye AH, Black P McL (2000) Operative Neurosurgery.Churchill Livingstone, London, New York, Edinburgh.
Kaye AH, Laws EL (1995) Brain Tumours. Churchill Livingstone, London.
Kaye AH, Morstyn G, Apuzzo MJ (1988) Photoradia-tion therapy and its potential in the management ofneurological tumours. Journal of Neurosurgery 69,1–14.
Kernohan JW, Maybon RF, Svein HJ, Adson AW (1949)A simplified classification of gliomas. Mayo ClinicProceedings 24, 71–75.
Kornblith PL, Walker M (1988) Chemotherapy ofgliomas. Journal of Neurosurgery 68, 1–17.
Liebel SA, Sheline GE (1987) Radiation therapy for neoplasms of the brain. Review article. Journal of Neurosurgery 66, 1–22.
Rich TA et al. (1985) Clinical and pathologic review of 48cases of chordoma. Cancer 56, 182–187.
Ringertz N (1950) Grading of gliomas. Acta PathologicaMicrobiologica Scandinavica 27, 51–64.
Wold LF, Laws ER Jr (1983) Cranial chordomas in children and young adults. Journal of Neurosurgery59, 1043–1047.
Yung WK (2000 June) Temozolomide in malignantgliomas. Seminars in Oncology 27 (3 Suppl. 6), 27–34.
Zulch KJ (1986) Brain Tumours, Their Biology and Pathology, 3rd edn. Springer Verlag, Berlin.
KAY6 12/16/04 7:39 PM Page 92

The benign brain tumours may be intimately as-sociated with, and surrounded by, the adjacentbrain, but the tumour cells do not invade the un-derlying brain. This is in contradistinction to thegliomas, which are intrinsic brain tumours ac-tively invading the adjacent brain. This chapterwill discuss the more common benign brain tu-mours — meningioma and acoustic neuroma —and give a brief description of the less commontumours: haemangioblastoma, epidermoid anddermoid cysts and colloid cysts.
Meningioma
Meningiomas are the most common of the benignbrain tumours and constitute about 15% of all in-tracranial tumours, being about one-third of thenumber of gliomas. Although they may occur atany age, they reach their peak incidence in mid-dle age, are very uncommon in children andoccur more frequently in women than men.
The term meningioma was introduced by Harvey Cushing in 1922, although the tumourhad been described in the late eighteenth century.The tumour arises from the arachnoid layer of themeninges, principally the arachnoid villi andgranulations.
Aetiology
As for other brain tumours, no definite aetiologi-cal factor has been identified. However, the possibility that head trauma predisposes to thedevelopment of meningioma has been the subjectof controversy for many years. Although epi-demiological studies do not support trauma as
an aetiological factor, there have been cases reporting the development of meningiomas atthe site of substantial meningeal trauma.
Meningiomas are known to occur followinglow levels of irradiation as was given in the pastfor tinea capitis, and an analysis of the Nagasakiatomic bomb survivors found a high correlationbetween the incidence of meningiomas and thedistance from the epicentre of the explosion.
Meningiomas occur with a high frequency inpatients with neurofibromatosis type 2 (NF2)(often multiple). This association has promptedcytogenetic studies, which have shown thatmonosomy of chromosome 22 is the most common chromosomal abnormality noted inmeningiomas, occurring in 50–80% of sporadictumours. In addition, alterations of many otherchromosomes (including chromosomes 1, 6, 9, 10,11, 13, 14, 18 and 19) have been noted to be involved in the formation and progression ofmeningioma.
The importance of sex hormones and their re-ceptors in meningioma is suggested by the 2–4times incidence in females. Oestrogen binds inless than 30% of meningiomas, with the majorityof those receptors being type II subtype, thathave a lower affinity and specificity for oestrogenthan the classic type I receptor usually found inbreast cancer. Progesterone receptors are muchmore commonly associated with meningiomas,occurring in 50–100% of tumours tested.
Position of meningiomas (Fig. 7.1)
Meningiomas arise from the arachnoid layer ofthe meninges, especially the arachnoid cap cells.
CHAPTER 7
7 Benign brain tumours
93
KAY7 12/16/04 7:40 PM Page 93

94 CHAPTER 7
The most common location is in the parasagittalregion arising either from the wall of the superiorsagittal sinus (parasagittal) or from the falx (falcine). Less frequently the tumours may arisefrom the convexity of the cranial vault, wherethey are particularly concentrated in the region ofthe coronal suture. Sphenoidal ridge menin-giomas are divided into those that arise from theinner part of the lesser wing of the sphenoid andthe adjacent anterior clinoid process, and thosearising from the outer sphenoidal ridge, compris-ing the greater wing of the sphenoid and the adjacent pterion (the junction of the temporal,parietal and frontal bones). Less frequently, thetumours may arise from the olfactory groove, tu-berculum sella (suprasellar), floor of the middlecranial fossa, cavernous sinus or posterior fossa(Table 7.1).
Meningiomas usually occur as a single in-tracranial tumour but multiple intracranialmeningiomas may present in NF2 (see p. 64).
Pathology
Unlike gliomas, where the classification system is
based on the histological appearance of the tu-mour, meningiomas are usually classified accord-ing to their position of origin rather than theirhistology. The reason for this is that the biologicalactivity of the tumour, the presenting features,the treatment and prognosis are all related moreto the site of the tumour than to the histology.
The major histological types are listed below.• Syncytial or meningotheliomatous — sheets ofcells with varying amounts of stroma.• The transitional type is characterized by
Tuberculum sellae
Olfactory groove
Parasagittal section
Foramen magnum
Posterior fossa(convexity)
Clivus
Parasagittal/falcine
Olfactory groove
Tuberculum sellae
Clivus
Foramen magnum
Basal
Sphenoidal wing
Posterior fossa- cerebellopontineangle
Fig. 7.1 Typical positions ofintracranial meningiomas.
Table 7.1 Position of intracranial meningiomas(%).
Parasagittal and falx 25Convexity 20Sphenoidal wing 20Olfactory groove 12Suprasellar 12Posterior fossa 9Ventricle 1.5Optic sheath 0.5
KAY7 12/16/04 7:40 PM Page 94

whorls of cells which may undergo hyalin degen-eration with subsequent deposition of calciumsalts. These calcified concentric psammomabodies form the characteristic feature of manytransitional meningiomas but they may also bepresent in the syncytial or fibroblastic types.• The fibroblastic type contains abundant reticulin and collagen fibres.• Angiomatous meningiomas are much lesscommon and their characteristic feature is thepredominance of vascular channels separated by sheets of cells. Histologically, these tumoursresemble cerebellar haemangioblastomas.• Malignant meningiomas occur infrequently.The indications of malignancy include cellularpleomorphism, necrosis, increased numbers ofmitotic figures and local invasion of brain. Atypi-cal meningiomas are tumours that lack the histological features of malignancy, but have a biological behaviour intermediate between thetypical and malignant meningioma. These tu-mours are most likely to recur.
Clinical presentation
Meningiomas present with features of:• raised intracranial pressure• focal neurological signs• epilepsy.
The position of the tumour will determine thefeatures of the clinical presentation. The tumoursgrow slowly and there is frequently a long his-tory, often of many years, of symptoms prior tothe diagnosis.
Parasagittal tumours (Fig. 7.2)These tumours most often arise in the middlethird of the vault and the patient may presentwith focal epilepsy and paresis, usually affectingthe opposite leg and foot as the motor cortex onthe medial aspect of the posterior frontal lobe isaffected. Tumours arising anteriorly are often bilateral and patients present with features ofraised intracranial pressure. As these tumours involve the frontal lobes, pseudopsychiatricsymptoms, as well as impairment of memory, intelligence and personality, may occur. Urinaryincontinence is occasionally a symptom of a large
frontal tumour, especially if it is bilateral. Tumours arising from the posterior falx may affect the parieto-occipital region and produce ahomonymous hemianopia. If the tumour liesabove the calcarine fissure the inferior quadrantis more affected; when the tumour is below thefissure the upper quadrant is predominantly affected.
Convexity tumours (Fig. 7.3)Convexity tumours may grow to a large size if
BENIGN BRAIN TUMOURS 95
Fig. 7.2 Parasagittal meningioma. (a) CT scan. (b) MRI.
(a)
(b)
KAY7 12/16/04 7:40 PM Page 95

96 CHAPTER 7
situated in front of the coronal suture. They present with raised intracranial pressure. Moreposterior tumours will cause focal neurologicalsymptoms and focal epilepsy.
Sphenoidal ridge tumours (Fig. 7.4)Tumours arising from the inner sphenoidalridge cause compression of the adjacent opticnerve and patients may present with a history ofuniocular visual failure. If the tumour is largeenough to cause raised intracranial pressure pa-pilloedema will develop in the contralateral eye.
The presenting features of primary optic atrophyin one eye and papilloedema in the other isknown as the Foster Kennedy syndrome, andwas described in 1911. Inner sphenoidal ridge tumours may also cause compression of the olfactory tract, resulting in anosmia.
Patients with tumours involving the outersphenoidal ridge present with features of raisedintracranial pressure, often severe papilloedemawith relatively inconspicuous localizing symp-toms or signs. Tumours in this region occur as a
Fig. 7.3 Convexity meningioma. (a) CT scan. (b) MRI.
Fig. 7.4 (a) CT scan. Hyperostosis of the leftsphenoidal ring causing unilateral proptosis due to a sphenoidal ring meningioma. (b) MRI. Innersphenoidal wing meningioma.
(a)
(b)
(a)
(b)
KAY7 12/16/04 7:40 PM Page 96

BENIGN BRAIN TUMOURS 97
thin sheet, and are known as ‘en plaque’. Theymay cause an excessive bony reaction (hyperos-tosis) resulting in proptosis (Fig. 7.4).
Olfactory groove tumours (Fig. 7.5)Olfactory groove meningiomas cause anosmia,initially unilateral and later bilateral. The pre-senting features may include symptoms of raisedintracranial pressure, and failing vision eitherfrom chronic papilloedema or from direct com-pression of the optic nerve or chiasm causing visual field defects. These tumours may also present with the Foster Kennedy syndrome andthe intellectual and psychiatric problems causedby frontal lobe compression described for innerspheroidal ridge meningiomas.
Suprasellar tumours (Fig. 7.6)Suprasellar meningiomas arising from the tuber-culum sellae will cause visual failure and abitemporal hemianopia, but the lack of endocrinedisturbance will distinguish the clinical presenta-tion of this tumour from that of a pituitary tumour.
Ventricular tumours (Fig. 7.7)Tumours arising in the lateral ventricle presentwith symptoms of raised intracranial pressureextending over several years and associated with a mild global disturbance of function of one hemisphere and frequently a homonymoushemianopia.
Posterior fossa tumours (Fig. 7.8)Posterior fossa tumours may arise from the cere-bellar convexity or from the cerebellopontineangle or clivus. The cerebellopontine angle tu-mours simulate an acoustic neuroma with symp-toms involving the acoustic nerve, trigeminalnerve and facial nerve, ataxia due to cerebellar in-volvement and raised intracranial pressure, oftendue to hydrocephalus caused by obstruction ofthe 4th ventricle. Meningiomas arising from the
Fig. 7.5 (a) CT scan. Olfactory groove meningioma. (b) MRI. Olfactory groove meningioma extending onto tuberculum sella and over pituitary fossa.
(a)
(b)
KAY7 12/16/04 7:40 PM Page 97

98 CHAPTER 7
clivus or the foramen magnum region may com-press the brainstem directly.
Radiological investigations
The CT scan appearance shows a tumour ofslightly increased density prior to contrast; it enhances vividly and uniformly following intravenous contrast. Hyperostosis of the cranial vault may be a focal process at the site of
the tumour attachment or, as seen with en plaquemeningioma, a more diffuse sclerosis. Thesebone changes may also be seen on plain skull X-ray.
Magnetic resonance imaging will demonstratemeningiomas following the intravenous injec-tion of gadolinium contrast (Figs 7.9–7.11).Meningiomas are usually isointense on T1-weighted images, but enhance intensely and usu-ally homogeneously following administration ofgadolinium. Cerebral angiography is no longernecessary as a diagnostic investigation but maybe useful preoperatively to ascertain the positionof the cerebral vessels. It will demonstrate exter-nal carotid artery supply to the tumour with acharacteristic tumour blush, differentiating itfrom a glioma or metastatic tumour (Fig. 7.12).Angiography also allows preoperative emboliza-tion of the tumour, if necessary.
Preoperative management
Meningiomas are frequently surrounded by se-vere cerebral oedema and patients should betreated with high-dose steroids (dexamethasone)prior to surgery if possible. Preoperative embolization of the tumour vasculature may beconsidered advisable in some anterior basal and sphenoidal wing tumours where the major
Fig. 7.6 Tuberculum sellae meningioma. (a) CT scan.(b) MRI.
Fig. 7.7 Intraventricular meningioma.(a)
(b)
KAY7 12/16/04 7:40 PM Page 98

vascular supply is not readily accessible in theearly stages of the operation.
Treatment
The treatment of meningiomas is total surgicalexcision, including obliteration of the dural at-tachment. Although this objective is usually pos-sible there are some situations where completeexcision is not possible because of the position ofthe tumour. Tumours arising from the clivus, infront of the brainstem or those situated within the cavernous sinus, are notoriously difficult toexcise without causing serious morbidity.
Radiation therapy may be used to treat residual tumours following subtotal resection, in order to reduce the risk of recurrent growth.
BENIGN BRAIN TUMOURS 99
Fig. 7.8 (a) CT scan. Meningioma arising in thecerebellopontine angle and from the tentorial edge. (b) MRI. Clivus meningioma. (c) MRI. Foramenmagnum meningioma.
(a)
(b)
(c)
Fig. 7.9 MRI of parasagittal meningioma. Themeningioma may be isodense on the plain T1 and T2
scans (a) but will enhance vividly after intravenousgadolinium (b).
(a)
(b)
KAY7 12/16/04 7:40 PM Page 99

100 CHAPTER 7
(a)
(b)
Fig. 7.10 MRI. Falcine meningioma. (a) Before contrasttumour is iso- or hypodense. (b) Tumour enhanceswith intravenous contrast.
(a)
(b)
Fig. 7.11 MRI. Extensive parasagittal meningioma. (a) Sagittal view. (b) Coronal view.
Fig. 7.12 Cerebral angiogram of olfactory groove meningioma showing displacement of anterior cerebral arteries(a,b) and the characteristic tumour blush, usually due to the external carotid artery supply (c).
(a) (b) (c)
KAY7 12/16/04 7:40 PM Page 100

Stereotactic radiotherapy has been used totreat small meningiomas (less than 3 cm in diam-eter), particularly if the tumours are located inportions not easily amenable to surgery, or in theelderly or medically infirm patient.
Clinical studies have shown short-term controlrates of over 90%, but long-term studies will be necessary to prove the efficacy and safety offocused radiation treatment.
Postoperative managementThe postoperative care of patients following exci-sion of a meningioma involves the routine man-agement of patients following a craniotomy butwith particular attention to the minimization ofcerebral oedema. Steroid therapy is continuedinitially and gradually tapered. Care is taken toavoid excessive hydration and the patient isnursed with the head of the bed elevated to pro-mote venous return. Neurological deteriorationrequires urgent assessment and a CT scan willdetermine the pathological cause, either post-operative haemorrhage or cerebral oedema.
Tumour recurrence
The risk of tumour recurrence depends on the extent of tumour excision. When the tumour and its dural origins are completely excised, therisk of recurrence is remote. The most commonsource of recurrence is from a tumour that has invaded a venous sinus and which was not re-sected (e.g. superior sagittal sinus or cavernoussinus). Recurrence is more common if the tumourhas histological features of malignancy.
Meningeal haemangiopericytoma
Meningeal haemangiopericytoma is a malignantneoplasm with sarcoma-like behaviour. It wasoriginally classified by Cushing and Eisenhardtin 1938 as an angioblastic variant of meningioma.The tumour’s radiological and macroscopic ap-pearance resembles a vascular meningioma, butit arises from the meningeal capillary pericyteand typically contains a subpopulation of cellsthat express factor VIIIa.
The tumour incidence is 2–4% of meningioma
and it is slightly more common in males than infemales.
The presenting features are dependent on thetumour location, with symptoms usually beingpresent for less than 1 year.
Acoustic neuroma
Acoustic schwannomas arise from the 8th cranialnerve and account for 8% of intracranial tu-mours. Schwannomas occur less frequently onthe 5th cranial nerve and rarely involve other cranial nerves. The acoustic schwannoma takesorigin from the vestibular component of the 8thcranial nerve near the internal auditory meatus,at the transition zone where the Schwann cells replace the oligodendroglia. As such it shouldmore correctly be called a vestibular schwan-noma, although the term acoustic neuroma orschwannoma is more commonly used.
Macroscopically, the acoustic schwannoma islobulated with a capsule that separates it fromthe surrounding neural structures. Small tu-mours usually arise from within the internal auditory canal and occupy the porus of the inter-nal auditory canal and, as the tumour grows, the8th nerve is destroyed and the adjacent cranialnerves become stretched around the tumour. The7th nerve is typically displaced on the ventraland anterior surface of the tumour and thetrigeminal nerve is carried upwards and for-wards by the upper pole. The 6th nerve lies ven-tral and usually medial to the major mass and thelower cranial nerves are displaced around the in-ferior pole of the tumour. As the tumour growsmedially it compresses and displaces the cerebel-lum and distorts the brainstem. Large tumourswill result in obstruction of the 4th ventricle andhydrocephalus.
Bilateral acoustic neuromas are the hallmark ofneurofibromatosis type 2 (NF2), inherited as anautosomal dominant condition (see Chapter 6).
Clinical presentation
The presenting features will depend on the sizeof the tumour at the time of diagnosis. The earliersymptoms are associated with 8th nerve involve-
BENIGN BRAIN TUMOURS 101
KAY7 12/16/04 7:40 PM Page 101

102 CHAPTER 7
ment. Tinnitus and unilateral partial or completesensorineural hearing loss are the earliest fea-tures. Episodes of vertigo may occur but thesemay be difficult to distinguish from Menière’sdisease. Although the tumour causes compres-sion of the facial nerve, the growth of the tumouris so slow that facial paresis is not evident untilthe tumour is large. At that stage 5th nerve com-pression may be evident, with diminished facialsensation and a depressed corneal reflex. Cere-bellar involvement will result in ataxia, and compression of the pyramidal tracts from a verylarge tumour causing brainstem compressionwill cause a contralateral hemiparesis. If a largetumour has caused obstructive hydrocephalusthe patient will also present with features ofraised intracranial pressure.
Radiological investigations
The CT scan or MRI will show an enhancing tu-mour extending from the internal auditory canalinto the cerebellopontine angle (Fig. 7.13). The in-ternal auditory meatus will be widened indicat-ing that the tumour has arisen from the 8thcranial nerve (Fig. 7.14). While there is no diffi-culty in diagnosing a tumour large enough to beevident on the CT scan, very small acoustic neuromas, which are predominantly within theinternal auditory canal, may be more difficult todiagnose. These tumours may be seen on high-quality CT scan but are particularly evidentusing MRI, especially following gadolinium con-trast (Fig. 7.15), which is now the investigation ofchoice.
Other investigations
Pure tone audiometry, by both air and bone con-duction, is an essential part of the investigation ofa patient with an acoustic neuroma, the mostcommon finding being high-frequency hearingloss. Other special auditory tests include the useof brainstem auditory evoked responses whichare particularly sensitive for changes in the retro-cochlear auditory system; these are helpful in diagnosing a small intracanalicular tumour.
Vestibular function is impaired early in
patients with acoustic neuroma. The Hallpikecaloric test is carried out with the patient supineon a couch and the head raised to 30°C above horizontal, bringing the horizontal canals intothe vertical plane with the position of maximumsensitivity to thermal stimuli. Warm and coolwater is irrigated and the nystagmus reaction observed. The caloric response on the side of theacoustic nerve tumour is depressed or absent.
Differential diagnosis
The major differential diagnoses for a cerebello-
Fig. 7.13 Acoustic neuroma. A contrast-enhancingtumour in the cerebellopontine angle arising from the8th cranial nerve in the internal auditory canal.
Fig. 7.14 Widened internal auditory meatus,indicative of an acoustic neuroma.
KAY7 12/16/04 7:40 PM Page 102

pontine angle tumour, in decreasing frequency,are:• meningioma• metastatic tumour• exophytic brainstem glioma• epidermoid tumour.
Treatment
The total excision of a large acoustic neuroma remains one of the major operative challenges in what Cushing has described as ‘the gloomycorner of neurologic surgery’.
The aim of the operation is complete resectionof the tumour while sparing the adjacent neuralstructures. If the patient presents with a large tu-mour causing severe hydrocephalus and raisedintracranial pressure, a preliminary ventricu-loperitoneal shunt or ventricular drain may beconsidered. Steroid administration prior tosurgery may be advisable if the tumour is large.
There are three basic approaches to the cerebel-lopontine angle: by excision of the labyrinth(translabyrinthine); through a posterior fossacraniectomy (suboccipital/retrosigmoid); or viathe middle cranial fossa.
No clear consensus has emerged from the liter-ature as to which is the procedure of choice.There are definite advantages and disadvantagesassociated with each surgical approach. Theroute chosen is governed by tumour size, the degree of hearing loss, the hearing level in the contralateral ear, and the surgical preferenceand expertise of the operator.
The major advantage of the translabyrinthineoperation is that the facial nerve can be identifiedlateral to the tumour at an early stage in the dis-section, and access to the fundus of the internalauditory meatus is excellent. Furthermore, re-traction of the cerebellum is minimal and the riskof postoperative oedema is consequently less.The major disadvantage of this route is that residual hearing is irrevocably destroyed. Theapproach is unfamiliar to neurosurgeons, and requires the close cooperation of a neurotologistexperienced in dissection of the temporal bone.Access is confined, but even the largest of tu-mours can be removed safely via this approach.
BENIGN BRAIN TUMOURS 103
Fig. 7.15 (a) MRI showing small intracanalicularmeningioma. (b) MRI showing large acoustic neuromainvading into temporal bone and extending intocerebellopontine angle with severe compression of thebrainstem.
(a)
(b)
KAY7 12/16/04 7:40 PM Page 103

104 CHAPTER 7
As a consequence of progressive improve-ments in operative results, particularly in mortal-ity and facial nerve outcome, attention hasturned more recently to the ability to preserveuseful hearing. The suboccipital operation pro-vides good access to the cerebellopontine anglebut, if hearing is to be conserved, tumour at thefundus of the internal auditory meatus may bedifficult to expose under direct vision. This is trueparticularly when the posterior semicircularcanal is medially placed. Theoretically, this mayincrease the risk of subtotal tumour excisionwhen compared with the translabyrinthine oper-ation. Recently there has been renewed interest in the middle fossa approach for removal of intracanalicular tumours or those with a smallcerebellopontine angle component, particularlywhere the tumour in the internal auditory canalextends to the fundus. Higher rates of hearingpreservation have been reported without anycompromise of facial nerve function, but thisroute provides more limited access to the cerebel-lopontine angle, and is therefore restricted to thetreatment of small lesions.
The question of hearing conservation deservescareful consideration when selecting the surgicalapproach. Anatomical preservation of the innerear and cochlear nerve does not guarantee func-tion, and it is exceptional for hearing to be im-proved beyond its preoperative level. Whethersuch hearing is useful depends upon the level ofhearing in the contralateral ear. Hearing lossneed not be profound before it is socially uselesswhen the other ear is normal. For hearing to beuseful socially there must be both good speechdiscrimination, and a pure tone audiogram with-in 20–40 dB of the contralateral ear. It is also essential that the attempt to preserve hearingshould not compromise the likelihood of com-plete tumour removal.
At The Royal Melbourne Hospital thetranslabyrinthine operation is favoured for largetumours, regardless of hearing level, and formedium-sized lesions with poor hearing. It pro-vides a more direct approach to the cerebellopon-tine angle, and retraction of the cerebellum isnegligible. For hearing preservation the retrosig-moid approach for tumours with up to 2 cm cere-
bellopontine angle extension is preferred. Themiddle fossa approach is preferred for intra-canalicular tumours and for those with up to1 cm cerebellopontine angle extension where tu-mour completely fills the internal auditory canal.
Stereotactic radiosurgery using either a 60COGamma Knife or a highly focused linear accelera-tor has been advocated for the treatment of smaller tumours, less than 3 cm in diameter. Thecontrol rates are greater than 90% over a 5-yearperiod, but post-radiation neurological compli-cations have been reported including delayed facial numbness and dysaesthesia, facial weak-ness and hearing loss. To minimize the complica-tions of single-dose stereotactic radiosurgerymany centres advocate fractionated stereotacticradiotherapy.
There is continuing debate as to the relative advantages of surgery and stereotactic radiationtreatment. Whilst some clinicians advocate radia-tion treatment for smaller tumours, others wouldonly recommend it for elderly or medically infirm patients or if there is residual tumour or regrowth after subtotal resection.
The management plan for patients with bilat-eral acoustic neuromas (NF2) is complex, andmust be tailored for each patient, with the aim ofpreserving useful hearing for as long as possible,whilst minimizing the possible serious neuro-logical complications from enlarging tumourscausing cranial nerve, cerebellar and brain-stem compression. Therapeutic options includesurgery, radiosurgery and hearing preserva-tions/restoration utilizing brainstem electrodeimplants at the time of tumour resection.
Postoperative careThe postoperative management is similar to thatindicated for the posterior fossa tumours in theprevious chapter. Any neurological deteriorationmust be investigated urgently. A postoperativehaemorrhage in this region may be rapidly fatal.
Postoperative swallowing difficulties mayoccur if there has been injury to the lower cranialnerves or brainstem. Great care should be takento avoid aspiration and nasogastric feeding maybe necessary. Facial paralysis will occur if the 7thnerve is not intact at the end of the operation and
KAY7 12/16/04 7:40 PM Page 104

may result even if the nerve is in continuity dueto neuropraxia of the nerve. A tarsorrhaphy maybe necessary to prevent corneal ulceration andwill be essential if there is a facial palsy andcorneal sensation is diminished due to 5th nervedamage. Alternatively temporary closure of theeye can be obtained by using botulinum toxin.
The cosmetic appearance of a permanent facial paralysis can be improved by a number ofprocedures including:• nerve anastomoses, such as a hypoglossal–facial anastomosis• cross-facial nerve grafts• facial slings.
Haemangioblastoma
Haemangioblastomas are uncommon intracra-nial tumours accounting for 1–2% of all brain tumours and approximately 10% of posteriorfossa tumours.
The haemangioblastoma arises from prolifera-tion of endothelial cells. The tumour usually oc-curs in young adults, although it may occur atany age. It usually occurs in the posterior fossaand often produces a large cyst. Although hae-mangioblastoma may occur as a component ofvon Hippel–Lindau’s disease, which includesmultiple haemangioblastomas, haemangioblas-tomas of the retina (von Hippel tumour), renaltumour, renal cyst, pancreatic cyst and tubularadenomata of the epididymis, the majority of patients with the cerebellar tumour do not havevon Hippel–Lindau’s disease. Incomplete formsof the syndrome may occur and cerebellar hae-mangioblastomas occur in about 20% of patientswith retinal haemangioblastoma.
Clinical presentation
The tumour presents as a slowly growing posterior fossa mass with features of raised intracranial pressure and cerebellar involvement.Occasionally the patient may be polycythaemicdue to increased circulating erythropoietin.
Radiological investigations
CT scan or MRI show a cerebellar tumour whichmay involve the vermis and hemispheres andwhich shows vivid enhancement following intra-venous contrast (Fig. 7.16). There is usually alow-density cyst surrounding the tumour nodule(Fig. 7.17), although haemangioblastomas maysometimes be solid. If considered necessary, vertebral angiography will confirm the highlyvascular mass.
Total surgical excision through a posteriorfossa craniotomy is nearly always possible. Greatcare must be taken not to enter the highly vascu-lar tumour during the dissection and excision.
BENIGN BRAIN TUMOURS 105
Fig. 7.16 Haemangioblastoma in the vermis of thecerebellum. (a) A vividly enhancing tumour nodule in the wall of a cyst. (b) Vertebral angiogram showssmall tumour nidus (arrowhead).
(a)
(b)
KAY7 12/16/04 7:40 PM Page 105

106 CHAPTER 7
Colloid cyst of the 3rd ventricle
The colloid cyst of the 3rd ventricle is situated inthe anterior part of the ventricle and is attachedto the roof just behind the foramen of Monro.
Several possibilities as to the origin of the tumour have been proposed, including the para-physis, choroid plexus epithelium, ependyma or a diverticulum of the diencephalon.
The cyst consists of a thin, outer fibrous cap-sule lined by a layer of epithelium; the contentsconsist of mucoid material, epithelial debris andmucin. The cyst may be very small and asympto-matic, as was the case with Harvey Cushing,where a 1-cm colloid cyst was found at post-mortem. As the tumour grows it will cause bilateral obstruction to the foramina of Monro,leading to raised intracranial pressure from hy-drocephalus. The headaches may fluctuate,being aggravated by stooping and relieved bystanding upright. Episodes of abrupt, suddenleg weakness causing the patient to fall mayoccur without a change in conscious state.Alternatively, an abrupt loss of consciousnessmay occur and this, although usually transient,might be fatal.
Radiological investigations
The usual CT scan picture is a high-density,rounded tumour in the anterior 3rd ventriclewhich enhances following intravenous contrast(Fig. 7.18), although isodense, hypodense andnon-enhancing tumours have been reported.MRI helps to define the position of these tumours(Fig. 7.18) and will be able to differentiate between a colloid cyst and an aneurysm of the basilar tip, which may occasionally be indistinguishable on CT scan.
Treatment
Surgical excision is performed through a cran-iotomy with a small incision in the anterior corpus callosum giving access to the lateral ventricle. The tumour is seen expanding the fora-men of Monro and, using the operating micro-scope, a complete excision is usually possible.Great care must be taken during the operation topreserve the venous structures, including theseptal veins, thalamostriate vein and internalcerebral veins. Damage to the columns of thefornix will result in severe postoperative memory disturbance.
Epidermoid and dermoid cysts
Epidermoid and dermoid cysts arise from epithelial cells embryologically misplaced in-tracranially, particularly into the meninges andventricles and, less frequently, into the paren-chyma of the brain. Rarely, the cells can be im-planted as a result of trauma such as a lumbarpuncture, which can implant skin into the spinalcanal causing an epidermoid cyst.
Epidermoid cysts make up about 1% of braintumours, although their incidence is higher inJapan, where the incidence of dermoid cysts ismuch less.
Epidermoid tumours are found principally inthe arachnoid spaces, the cisterns or the diploe of the bone. The most frequent localizations arethe cerebellopontine angle, the suprasellar andparasellar regions, the lateral or 4th ventricles,and the quadrigeminal cistern.
Fig. 7.17 MRI. Cystic haemangioblastoma.
KAY7 12/16/04 7:40 PM Page 106

BENIGN BRAIN TUMOURS 107
Fig. 7.18 Colloid cyst of the 3rd ventricle. (a) CT scanshows hyperdense tumour before contrast. (b) MRI.Colloid cyst. (c) MRI. Colloid cyst sagittal view.
(a)
(b)
(c)
(a)
(b)
Fig. 7.19 (a) Dermoid cyst. A very low density lesionon CT scan that does not enhance. (b) MRI.Epidermoid cyst adjacent to brainstem.
KAY7 12/16/04 7:40 PM Page 107

108 CHAPTER 7
Treatment
The treatment is operative, with resection of thecyst. Complete excision may be prevented if thecyst wall is densely adherent to major vessels andimportant neural structures.
Further readingCushing H (1917) Tumours of the Nervus Acusticus and
the Syndrome of the Cerebellopontine Angle. W B Saunders, Philadelphia.
Cushing H, Eisenhardt L (1938) Meningiomas: their Classification, Regional Behaviour, Life History and Surgical End Results. Charles C Thomas, Springfield.
Di Tullio MV, Rand RW (1978) The Rand–Kurze Suboccipital Transmeatal Operation. In: Rand RW,eds. Microneurosurgery. C V Mosby, St Louis, 206–232.
Kaye AH, Laws ER (2001) Brain Tumours. Churchill Livingstone, London.
Kaye AH, Black P McL (2000) Operative Neurosurgery.Churchill Livingstone, London, New York, Edinburgh.
Kennedy F (1911) Retrobulbar neuritis as an exact diagnostic sign of certain tumours and abscesses inthe frontal lobes. American Journal of Medical Science142, 355–368.
King TT (1982) The translabyrinthine operation for removal of acoustic nerve tumours. In: SchmidekHH, Sweet WH, eds. Operative Surgical Techniques: Indications, Methods and Results. Grune & Stratton,New York, 609–636.
Little JR, McCarty CS (1974) Colloid cysts of the thirdventricle. Journal of Neurosurgery 39, 230–235.
Rand RW, Kurze T (1965) Facial nerve preservation byposterior fossa transmeatal microdissection in totalremoval of acoustic neuromas. Journal of Neurology,Neurosurgery and Psychiatry 28, 311–316.
Russell DS, Rubenstein LJ (1977) Pathology of Tumours of the Nervous System, 4th edn. Williams & Wilkins,Baltimore.
Zulch KJ (1986) Brain Tumours, Their Biology and Pathology, 3rd edn. Springer Verlag, Berlin.
Dermoid tumours occur mostly in the posterior fossa as a midline lesion and a fistulamay connect the dermoid with the skin.
Histology
The epidermoid cyst contains desquamated epithelium surrounded by keratin-producingsquamous epithelium. The dermoid cyst in-cludes dermal elements such as hair follicles, sebaceous glands and sometimes sweat glands.
Clinical presentation
The cysts usually present following a long his-tory of symptoms related to their position. Cranial nerve abnormalities such as trigeminalneuralgia and hemifacial spasm may occur withcerebellopontine angle epidermoid tumours andthe suprasellar cyst will produce visual impair-ment with optic atrophy and often a bitemporalhemianopia. Leakage of epidermoid cyst con-tents may result in a chemical meningitis, and inpatients with posterior fossa dermoid cysts, bacterial meningitis may occur through the dermal sinus connecting the cyst with the skin.
Radiological investigations
The CT scan of an epidermoid cyst is char-acterized by a low-density lesion that does notenhance. The dermoid cyst will also have areaswhich are even less dense than CSF, indicatingthe presence of fat (Fig. 7.19). MRI has sup-erceded CT for accurate preoperative evaluationand planning. Epidermoid lesions are usuallymanifest as low signal on T1 and high signal on T2
images, although depending on lipid content,variable signal intensities may be seen within thesame lesion.
KAY7 12/16/04 7:40 PM Page 108

Pituitary adenomas account for 8–10% of all in-tracranial tumours.
In 1886 Pierre Marie first made the connectionbetween acromegaly and pituitary adenomas.Patients may present either with signs of en-docrine disturbance or with compression of theadjacent neural structures, especially the opticpathways.
Classification
Historically, three main types of pituitary adeno-mas were defined by their cytoplasmic stainingcharacteristics: chromophobic, acidophilic andbasophilic — the implication being that these tu-mours were either hormonally inactive, secretedgrowth hormone, or produced adrenocorti-cotrophic hormone (ACTH), respectively.
The development of immunoperoxidase tech-niques and electron microscopy has provided amore refined classification of pituitary adenomasbased on the specific hormone that is produced.This classification is shown in Table 8.1.
Pathology
Pituitary adenomas arise from the anterior lobe(adenohypophysis) of the pituitary gland whichdevelops from Rathke’s pouch, an ectodermal diverticulum arising from the roof of the stomodeum, immediately in front of the buccopharyngeal membrane. The posterior lobe(neurohypophysis/pars nervosa) arises from theinfundibulum developing from the floor of thediencephalon (Fig. 8.1).
The tumour arises within the pituitary fossa. If
it is less than 10 mm in diameter it is known as a‘microadenoma’. The tumour may grow locallywithin the sella and cause erosion and remodel-ling of the floor of the sella and posterior clinoidprocesses (macroadenoma). The tumour usuallyspreads superiorly into the suprasellar cisterns,where it may cause compression of the opticpathways, particularly the optic chiasm. Furthergrowth superiorly causes compression of the hy-pothalamus and, if large enough, obstruction ofthe 3rd ventricle, resulting in hydrocephalus(Figs 8.2 and 8.3).
The tumour may also grow laterally out of thesella into the cavernous sinus. Occasionally thelateral extension may be sufficient to cause dis-turbance of the cranial nerves in the cavernoussinus. Uncommonly the tumour penetrates fur-ther laterally, into the temporal lobe.
The tumour may infrequently extend inferior-ly through the floor of the pituitary fossa into thesphenoid sinus, resulting in CSF rhinorrhoea.
The localization of microadenomas within thepituitary fossa corresponds somewhat with theregional distribution of the normal adenohy-pophyseal cells. Prolactin- and growth hormone-secreting microadenomas tend to occur laterally,whereas most adenomas secreting ACTH occurin the central zone.
The pituitary hormones are synthesized in therough endoplasmic reticulum and are packagedin the Golgi apparatus. After packaging they canbe visualized by either electron microscopy orimmunoperoxidase staining as secretory gran-ules within the cytoplasm. The hormone is re-leased from the cell by exocytosis, followingfusion of the granule with the cell membrane
CHAPTER 8
8 Pituitary tumours
109
KAY8 12/16/04 7:41 PM Page 109

110 CHAPTER 8
which usually occurs at the vascular pole of thecell. Adenomas may either be densely or sparselygranulated and this will determine their stainingproperties (Fig. 8.4).
Multiple endocrine neoplasia type 1 (Werner’ssyndrome) is an autosomal dominant disorderrepresenting the inherited occurrence of both be-nign and malignant neoplasms involving the pi-tuitary gland, parathyroid gland and pancreas.
Functional types of pituitary adenoma
Prolactin cell adenoma
Prolactin is a 23 500-Da polypeptide hormoneproduced by the prolactin-secreting cells (lac-totrophs) situated predominantly in the postero-
Table 8.1 Classification of pituitary adenomas.
Percentage Hormone secreted of tumours
Prolactin 40Growth hormone 20Null cell (no hormone) 20ACTH 15Prolactin and growth hormone 5FSH/LH 1–2TSH 1Acidophil stem cell (no hormone) 1–2
ACTH, adrenocorticotrophic hormone; FSH,follicle-stimulating hormone; LH, luteinizinghormone; TSH, thyroid-stimulating hormone.
ArachnoidDura
Sphenoid
Pituitary fossa
Posterior lobe
Clivus
Basal cisterns(CSF)
Infundibulum
Anterior lobe
Fig. 8.1 Pituitary gland.
3rd ventricle
Abducent nerveSphenoidsinus
Internal carotidartery
Optic chiasm
Cavernous sinus
Oculomotor nerveTrochlear nerve
Ophthalamic nerve(V1)Maxillary nerve (V2)
Pituitary gland
Basal cisterns (CSF)
Fig. 8.2 Anatomical relations of the pituitary gland.
Fig. 8.3 Large pituitarytumour compressing thehypothalamus and 3rdventricle.
KAY8 12/16/04 7:41 PM Page 110

lateral hypophysis and constituting 15–20% ofadenohypophyseal cells. The best known physio-logical functions of prolactin are stimulation ofbreast growth and promotion of lactation. Its rolein the male is poorly understood but it is impor-tant in spermatogenesis.
Unlike the secretion of other pituitary hor-mones which is controlled primarily by a hypo-thalamic releasing hormone, prolactin secretion
is primarily under the influence of an inhibitoryagent, ‘prolactin-inhibiting factor’, believed to bedopamine.
Prolactinomas are the most frequently occur-ring pituitary adenomas. The majority present as microadenomas in young females with symptoms of hypersecretion causing amenor-rhoea and galactorrhoea; impotence may be theonly symptom in males. This explains the muchgreater surgical frequency of prolactinomas inwomen, and why these tumours may grow to alarge size in males and elderly females.
Three-quarters of prolactin-secreting tumoursare chromophobe by light microscopy, the restbeing either weakly acidophilic or composed of amixture of cells. The serum levels of prolactinwill be elevated and levels exceeding 2000 ng/mlare suggestive of an invasive prolactinoma. Aminor elevation of serum prolactin, up to a levelof twice normal, is not necessarily diagnostic of aprolactin-secreting adenoma, as any lesion of thehypothalamus, pituitary or pituitary stalk whichinterferes with the production or release of prolactin-inhibiting factor may cause some increase in the serum prolactin.
Growth hormone cell adenoma
Growth hormone is a single chain 21 000-Dapolypeptide produced by cells situated princi-pally in the lateral part of the gland. Growth hormone adenomas represent approximately15–20% of pituitary adenomas. Under light mi-croscopy the features are either acidophil or chromophobe, depending on the extent of the cytoplasmic granules. The adenomas may becomposed of either densely or sparsely granu-lated cells, occurring with approximately equalfrequency; about 10% of tumours show a mixtureof both cell types (Fig. 8.4).
Hyperprolactinaemia occurs quite frequentlyin growth hormone-producing adenomas andmay result either from an adenoma producingboth hormones or from a growth hormone-producing adenoma being of sufficient size to interfere with the release of prolactin-inhibitingfactor, thereby elevating the serum prolactin secondarily.
PITUITARY TUMOURS 111
Fig. 8.4 Electron microscopy. (a) Membrane-boundelectron-dense granules of growth hormonesynthesized in the endoplasmic reticulum andpackaged by the Golgi apparatus (¥ 20000). (b) Immunogold labelling of granules with antiserumagainst growth hormone (¥ 75000).
(a)
(b)
KAY8 12/16/04 7:41 PM Page 111

112 CHAPTER 8
ACTH (corticotrophic) adenomas
ACTH is a single chain polypeptide which stimu-lates the adrenal cortex and promotes secretion ofcortisol and related steroids. Adenomas produc-ing ACTH are the cause of Cushing’s disease. The adenomas are densely granulated with ba-sophilic cytoplasm.
ACTH-producing tumours constitute approxi-mately 15% of adenomas, over 80% of which aremicroadenomas. About 15–20% of adenohy-pophyseal cells are corticotrophs, located in thecentral component of the anterior lobe of the pi-tuitary gland, and it is not surprising that mostmicroadenomas are located centrally rather thanlaterally, as occurs with the other hormone-producing microadenomas.
Gonadotroph cell adenoma
Follicle-stimulating hormone (FSH) and luteiniz-ing (LH) cells represent approximately 10% of thenormal pituitary cells and are scattered through-out the adenohypophysis. Adenomas resultingfrom these cells are very uncommon and most arefunctionally silent.
Thyrotroph cell adenoma
Thyroid-stimulating hormone (TSH)-producingtumours are rare.
Null cell adenomas
Twenty to thirty per cent of pituitary adenomashave no clinical or biological evidence of hyper-function. Mild hyperprolactinaemia may occursecondary to distortion of the pituitary stalk.Most (75% of) null cell adenomas are chromo-phobic, with few or no cytoplasmic granules. Approximately 20% of null cell tumours showmarked accumulation of mitochondria and arecalled ‘oncocytomas’.
Clinically, null cell adenomas are aggressiveand, as they are hormonally silent, they maygrow to a large size, so that patients present withvisual disturbance.
About 10% of pituitary adenomas are invasive,
with extensive penetration of the pituitary cap-sule, dural sinuses and surrounding bone. Mostinvasive pituitary adenomas are sparsely granu-lated or chromophobic and are either hormonallyinactive or prolactin producing.
Metastasizing pituitary carcinoma, either ex-tracranially or throughout the CSF pathway, isextremely rare.
Clinical presentation (Table 8.2)
The presenting features are due to:• the size of the tumour• endocrine disturbance.
Headache occurs principally in patients withacromegaly and is uncommon in other types ofpituitary tumour.
Visual failure
Careful assessment of the visual fields, the visualacuity and the optic fundi is essential.
Suprasellar extension of the pituitary tumourcauses compression of the optic chiasm resultingin a bitemporal hemianopia. The bitemporalhemianopia initially involves the upper quad-rants, before extending to the lower quadrants ofthe visual field. If the chiasm is prefixed, that is,placed more anteriorly than usual, a homony-mous hemianopia may occur due to compressionof the optic tract. Bilateral central scotomas resultfrom the tumour pressing on the posterior part ofthe chiasm where the macular fibres decussate.Primary optic atrophy will be evident in patientswith long-standing compression of the chiasm.
Ocular palsies occur in about 10% of patientsand are due to invasion of the cavernous sinus.The 3rd nerve is the most frequently affected, fol-lowed by the 6th and 4th cranial nerves. Facialpain results from compression of the trigeminalnerve, usually the ophthalmic division, as a re-sult of cavernous sinus invasion.
Endocrine abnormalities
Endocrine disturbance is due to either hypopi-tuitarism or excess secretion of a particular pituitary hormone.
KAY8 12/16/04 7:41 PM Page 112

HypopituitarismHypopituitarism results from failure of the hor-mones secreted by the adenohypophysis and itgives rise to the clinical features first described bySimmonds in 1914. Pituitary gland failure doesnot occur if the tumour is a microadenoma, but
may be clinically evident in the larger tumours.The endocrine secretions are not equally de-pressed but there is a selective failure and theorder of susceptibility is as follows: growth hor-mone, gonadotrophin, corticotrophin, thyroid-stimulating hormone.
Gonadotrophic deficiency prior to puberty re-tards the development of secondary sex charac-teristics; adult men have poor beard growth,women suffer from amenorrhoea and both sexeshave loss of libido and deficient pubic and axil-lary hair. The biochemical abnormality is mani-fest by a low oestrogen and androgen productionwith reduced urinary 17-ketosteroids.
Hypopituitarism initially results in vaguesymptoms, including lack of energy, undue fa-tiguability, muscle weakness and anorexia and,when prolonged and severe, it will cause lowblood pressure. Clinical hypothyroidism is manifest by physical and mental sluggishnessand a preference for warmth. When the hypopi-tuitarism is severe, episodic confusion occursand the patient will become drowsy. It is essentialto recognize the features of severe pituitary insuf-ficiency as an endocrine crisis can be precipitatedby minor stressful events occurring during hos-pital investigation or as a result of an intercurrentinfection.
Pituitary apoplexy results from spontaneoushaemorrhage into a pituitary tumour. It is charac-terized by sudden, severe headache followed bytransient or more prolonged loss of conscious-ness with features of neck stiffness, vomiting andphotophobia. The condition is similar to sub-arachnoid haemorrhage resulting from a rup-tured aneurysm, but is often associated withparalysis of one or more of the ocular muscles(usually bilateral) and acute visual deterioration.An acute endocrine crisis may be precipitated bythe apoplexy (Fig. 8.5).
ProlactinomaThe prolactin-secreting tumour may be a mi-croadenoma or macroadenoma within the pitu-itary fossa. The patients are usually women whopresent with infertility associated with amenor-rhoea and galactorrhoea, although the tumourmay occasionally cause infertility in men. Large
PITUITARY TUMOURS 113
Table 8.2 Clinical manifestations of pituitarytumours.
‘Mass’ effectsHeadaches (especially acromegaly)Superior extension
Chiasmal syndrome (impaired visual acuity and fields)
Hypothalamic syndrome (disturbance in thirst, appetite, satiety, sleep and temperature regulation; diabetes insipidus — uncommon; inappropriate ADH syndrome — uncommon)
Obstructive hydrocephalusLateral extension
Cranial 3rd, 4th, 6th, diplopiaCranial 5th, facial painTemporal lobe dysfunction
Inferior extensionNasopharyngeal massCSF rhinorrhoea
‘Endocrine’ effectsHyperpituitarism
GH — gigantism/acromegalyPRL — hyperprolactinaemic syndromeACTH — Cushing’s diseaseTSH — thyrotoxicosis
HypopituitarismGH — child: shortness of stature,
hypoglycaemiaPRL — adult female: failure of postpartum
lactationACTH — hypocortisolism (Addison’s)TSH — hypothyroidismLH/FSH — hypogonadism
Acute deteriorationPituitary apoplexy
GH, growth hormone; PRL, prolactin; TSH,thyroid-stimulating hormone; LH, luteinizinghormone; FSH, follicle-stimulating hormone;ACTH, adrenocorticotrophic hormone.
KAY8 12/16/04 7:41 PM Page 113

114 CHAPTER 8
Fig. 8.5 MRI showing pituitary tumour extendingfrom expanded pituitary fossa into the suprasellarcisterns with compression of optic chiasm.
OphthalmologicalRelated to tumour mass effectsRelated to GH hypersecretion
GlaucomaExophthalmos
LaryngealVoice changesCord fixation
Sleep disorders
SkeletalAcral changesArthropathy
CardiovascularHypertensionCardiomegalyCongestive heart failureConduction defects and arrhythmias
DermatologicalAcral changesHyperhydrosisAcneHypertrichosisHyperpigmentationAcanthosis nigricans
Table 8.3 Clinical manifestations of growth hormone-producing pituitary tumours.
prolactinomas occur in the elderly and in males,and these can cause endocrine disturbance asso-ciated with hypopituitarism and visual failure.
AcromegalyAcromegaly results from a growth hormone-secreting pituitary adenoma which, as describedpreviously, consists of cells that stain either asacidophils, chromophobes or both. The onset ofacromegaly is slow and insidious, usually duringthe 3rd and 4th decades of life, with both sexesbeing affected equally. The clinical features(Table 8.3) include bone and soft tissue changesthat are evident as an enlarged supraciliary ridge,enlarged frontal sinuses and increased mandibu-lar size, which will cause the chin to project(prognathism) (Fig. 8.6). The hands and feet en-large, and the skin becomes coarse and greasy
EndocrineEffect of excess GH on tissue growth and
intermediary metabolismSkin and subcutaneous tissue overgrowthSkeletal overgrowthVisceromegalyIncreased BMR, heat intolerance, hyperhydrosisCarbohydrate intoleranceDiabetes mellitus
Associated pituitary dysfunctionOwing to pituitary compression or destructionHypopituitarism
Associated thyroid dysfunctionGoitreThyrotoxicosis — toxic nodular goitre, Graves’
diseaseAssociated multiple endocrine neoplasia type 1
Primary hyperparathyroidismTumours of the endocrine pancreas syndromes
NeurologicalRelated to tumour mass effectsRelated to GH hypersecretion
AcroparaesthesiasEntrapment neuropathiesPeripheral neuropathyMyopathy
KAY8 12/16/04 7:41 PM Page 114

and sweats profusely. The voice becomes hoarseand gruff and thoracic kyphosis occurs as a resultof osteoporosis.
Other problems associated with acromegalyinclude hypertension, cardiac hypertrophy anddiabetes. Headache is often severe in patientswith pituitary tumours causing acromegaly and
patients complain of lack of energy, physicalweakness and lassitude.
Suprasellar extension of the tumour occurs inabout 15% of cases and may result in compres-sion of the optic pathways.
A pituitary adenoma with excessive growthhormone secretion occasionally presents in child-hood and results in gigantism.
Cushing’s diseaseCushing’s disease is due to ACTH-producing pituitary adenomas. Over 80% of the tumours are microadenomas and the remainder aremacroadenomas involving the whole of the sellaor with extrasellar extension.
The onset is insidious and the disease may af-fect children or adults. Severe obesity occurs, theskin is tense and painful, and purple striae ap-pear around the trunk. Fat is deposited, particu-larly on the face (moon face), neck, cervicodorsaljunction (buffalo hump) and trunk. The skin be-comes a purple colour due to vasodilatation and stasis. Spontaneous bruising is common. Theskin is greasy, acne is common and facial hair ex-cessive. Patients complain of excessive fatigueand weakness. There is wasting and flaccidity ofthe muscles. Osteoporosis predisposes to sponta-neous fractures.
Glucose tolerance is impaired, the serumpotassium is low and vascular hypertension oc-curs. If untreated, 50% of cases are fatal in 5 years.
Cushing’s syndromeThere is excessive cortisol production, due to anACTH-producing pituitary adenoma (Cushing’sdisease) in 90% of cases. Other causes of Cush-ing’s syndrome are an adrenal adenoma or carci-noma, or an ectopic source of ACTH productionsuch as from an oat cell carcinoma of the lung oraberrant adrenocortical tissue occurring outsidethe adrenal gland.
Nelson–Salassa syndromeThis consists of an ACTH-producing pituitaryadenoma in a patient who has undergone bilater-al or subtotal adrenalectomy. Before the develop-ment of CT scanning and trans-sphenoidalmicrosurgery, patients with Cushing’s disease
PITUITARY TUMOURS 115
Fig. 8.6 A 58-year-old female with acromegaly. Aboveis a photograph taken when she was 25 years old.
KAY8 12/16/04 7:41 PM Page 115

116 CHAPTER 8
often underwent total adrenalectomy whenpneumoencephalography had failed to reveal apituitary tumour. However, accelerated growthof an existing adenoma is induced by the loss of normal corticosteroid feedback. Unlike theadenomas of Cushing’s disease, about half of patients with Nelson–Salassa syndrome havemacroadenomas. Patients have marked cuta-neous hyperpigmentation due to secretion of either beta melanocyte-stimulating hormoneand/or beta lipotrophin.
Laboratory investigations
Radioimmunoassay will help to identify the hor-mone being secreted.
Serum prolactin level in patients with pro-lactinomas will vary from just above the upperlimit of normal to values greater than20 000 mIU/l (normal 70–550 mIU/l). The levelsmay show considerable variation in a particularpatient and prolactin levels greater than2000 mIU/l are almost always indicative of a pituitary tumour. As mentioned previously, hy-perprolactinaemia may be associated with otherpituitary tumours and has been noted in somepatients with acromegaly. Null cell tumours maybe associated with mild hyperprolactinaemiadue to distortion of the pituitary stalk or im-pingement on the hypothalamus.
Serum growth hormone is measured by ra-dioimmunoassay, the normal values being lessthan 5 mIU/l in males and less than 10 mIU/l infemales. Growth hormone exerts its effects on pe-ripheral tissues indirectly via somatomedins —polypeptides produced primarily by the liverand fibroblasts. Serum somatomedin C (insulin-like growth factor I, IGF-I) is a more accurate in-dicator of growth hormone bioactivity than theserum growth hormone levels. Provocative tests of growth hormone secretion are useful in confirming acromegaly. Most patients withacromegaly do not show the normal suppressionof growth hormone following glucose load.Other provocative tests utilize thyrotrophin-releasing hormone and growth hormone-releasing hormone.
In contrast to other pituitary tumours that rely
on imaging studies as the foremost diagnostic in-vestigation, a careful endocrinological assess-ment is critical in the diagnosis of Cushing’sdisease, especially as in nearly 50% a tumour isnot evident on MRI.
There are three essential steps in the diagnosisof Cushing’s disease due to pituitary pathology.1 Confirm excess secretion of cortisol (normal120–650 nmol/l).2 Distinguish ACTH-dependent from ACTH-in-dependent causes of hypercortisolaemia.3 Distinguish pituitary-based Cushing’s diseasefrom ectopic states of ACTH production.
A24-hour urine specimen is the simplest initialmeans of establishing hypercortisolaemia.
The investigation of Cushing’s disease in-volves the measurement of ACTH by radioim-munoassay of samples of both peripheral bloodand blood from the petrosal sinus. A differentiallevel of ACTH in petrosal vein blood and periph-eral blood will help confirm the presence of a pi-tuitary basis for the ACTH production, especiallyafter administration of corticotrophin-releasinghormone (CRH). A dexamethasone suppressiontest will help diagnose Cushing’s syndrome andits cause. The urine- and plasma-free cortisol ismeasured and is normally suppressed followingadministration of low-dose dexamethasone(0.5 mg 6-hourly). The levels will be suppressedfollowing high-dose dexamethasone (2 mg 6-hourly) in pituitary-dependent Cushing’s dis-ease. There will be a failure of suppression of thelevels with high-dose dexamethasone if theCushing’s syndrome is due to other than pitu-itary causes.
Radiological investigations
High-resolution CT scanning and magnetic reso-nance imaging using thin slices and intravenouscontrast are the appropriate investigation. Pitu-itary microadenomas are usually hypodense andmay cause upward bulging and convexity of theupper border of the gland in adults, deviation ofthe pituitary stalk and thinning of the sellar flooron the side of the tumour (Fig. 8.7). High-qualityCT scanning is able to demonstrate tumours assmall as 4 mm in diameter. Macroadenomas en-
KAY8 12/16/04 7:41 PM Page 116

hance after intravenous contrast and the exactnature of the extrasellar extension can be best ap-preciated with direct coronal scans (Fig. 8.8).
MRI has improved the identification of mi-croadenomas, which appear as low-density focallesions on T1-weighted scans and high intensityon T2-weighted scans (Fig. 8.9). Macroadenomasusually appear as isointense on the T1-weightedimages and moderately hyperintense on the T2-images (Fig. 8.10). Haemorrhage into a tumour,such as occurs following pituitary apoplexy,shows as high-intensity areas because ofmethaemoglobin on the T1- and T2-weightedscans intermingled with low-density regions due
to haemosiderin (see Figs 8.5 and 8.9). Dynamicscans taken at 30-second intervals following in-travenous gadolinium may help demonstratesmall microadenomas.
Plain skull X-rays may show enlargement ofthe sella with thinning erosion or bulging of itscontours (Fig. 8.11).
In the past angiography has been performed toexclude incidental aneurysms and to determinethe position of the internal carotid arteries in thecavernous sinuses, but this information can nowbe obtained satisfactorily from good-quality MRI and, if necessary, magnetic resonance angiography.
PITUITARY TUMOURS 117
Fig. 8.7 (a) CT showing hypodense microadenoma in pituitary gland. (b) MRI showing microadenoma.
Fig. 8.8 Axial and coronal CT scans showing large pituitary tumours.
(a)
(b)
KAY8 12/16/04 7:41 PM Page 117

118 CHAPTER 8
Fig. 8.11 Plain lateral skull X-ray showingthinning of the dorsum sellae anddestruction of the pituitary fossa in a patientwith a large pituitary tumour.
Fig. 8.9 MRI scan (T1) showing large pituitary tumourwith area of recent haemorrhage. Fig. 8.10 Enhanced MRI showing large pituitary
tumour extending up to the 3rd ventricle.
(a)
(b)
(a)
(b)
KAY8 12/16/04 7:41 PM Page 118

Differential diagnosis
The major differential diagnoses are:• craniopharyngioma• suprasellar meningioma (arising from the tu-berculum sellae).
Uncommon masses around the suprasellar re-gion also include optic nerve and hypothalamicglioma (Fig. 8.12), giant aneurysm arising fromthe carotid artery, Rathke’s cleft cysts, suprasellargerminomas and chordomas.
Treatment
The objectives of treatment of patients with pitu-itary tumours depend on whether the patient haspresented with features of endocrine disturbanceor problems related to compression of adjacentneural structures. The methods of treatment usedare:1 Operative procedures:
(a) trans-sphenoidal excision(b) transcranial excision.
2 Radiotherapy.3 Medical treatment with antisecretory drugs.
Surgical excision
This will be used as the primary method of treat-ment for:• large tumours causing compression of adja-
cent neural structures, particularly the visualpathways• GH-secreting tumours causing acromegaly• ACTH-secreting tumours causing Cushing’sdisease• the occasional treatment of a prolactin-secretingadenoma, either microadenoma or macroade-noma confined within the sella, when medicaltreatment using bromocriptine is not tolerated.
Most tumours can be excised via the trans-sphenoidal approach to the pituitary fossa (Fig.8.13). The development of the surgical micro-scope and fluoroscopic radiography has madethis a safe procedure. The sphenoid sinus is usu-ally entered using a unilateral trans-septal ap-proach, with the incision either in the nasalmucosa or sublabially. The mucosa is reflectedfrom the nasal septum and floor and the sphe-noid is opened. The anterior wall of the sella is removed and the pituitary fossa entered. Microadenomas (tumours less than 10 mm in diameter) may be evident on the surface of the gland or may become evident only once thegland is incised. These tumours can be comple-tely excised, preserving pituitary function. Thesuprasellar extension of the tumour can be gentlycoaxed down into the pituitary fossa by slightlyraising the intracranial pressure using a Valsalvamanoeuvre or by the anaesthetist injecting smallincrements of nitrous oxide and oxygen mixtureinto the lumbar theca until the intracranial pres-sure forces the suprasellar tumour into the oper-ative field. This will also have the additionalbenefit that the intracranial gas will provide apneumoencephalogram, outlining the remainingsuprasellar extension of tumour.
A transcranial operation is occasionally neces-sary, particularly where there is a subfrontal orretroclival extension of the tumour.
Postoperative management requires careful at-tention to the fluid balance and hormonal status.Endocrine deficiency in the immediate post-operative period will require replacement withparenteral hydrocortisone and possibly the useof vasopressin for the treatment of diabetes insipidus, which often occurs at least transientlyafter the excision of a large pituitary tumour. Inthe early postoperative period aqueous vaso-
PITUITARY TUMOURS 119
Fig. 8.12 Hypothalamic glioma.
KAY8 12/16/04 7:41 PM Page 119

120 CHAPTER 8
pressin (Pitressin ®) should be given by intra-muscular or subcutaneous injection and, if the di-abetes insipidus persists, by the intranasal route.Other long-term hormonal replacements may in-clude cortisone acetate (12.5–25 mg twice daily),thyroxine and testosterone.
Radiotherapy
Postoperative radiotherapy may be used if therehas been a subtotal excision of the tumour or if
the postoperative endocrine studies demonstrateresidual excessive hormone secretion.
Medical treatment
Treatment of pituitary adenomas is undertakento restore the endocrine status of the patient byreplacement of either the pituitary hormone itself or the hormone of the pituitary-dependentglands. This will be a necessary preoperative pro-cedure in patients with evidence of hypopitu-itarism and will frequently be necessary after thesurgical excision of a macroadenoma.
Prolactin-secreting pituitary tumours are treat-ed with bromocriptine, a dopamine agonist. Thisis the preferred treatment for a symptomatic pro-lactin-secreting microadenoma and may be usedeither as the definitive treatment of larger pro-lactin-secreting tumours or in conjunction withsurgery. Some patients show poor tolerance tobromocriptine, as it may cause intractable nausea, vomiting and postural hypotension, andthese patients will require surgical treatment ofthe tumour.
Craniopharyngioma
This tumour may occur at any age, althoughnearly half occur in the first 20 years of life. Theyare thought to arise from the epithelial remnantsof Rathke’s pouch.
The tumours occur in the region of the pitu-itary fossa and extend through the suprasellarcisterns to the hypothalamus. The majority arecystic, and the fluid is often yellow and sparklingwith cholesterol crystals. The cyst may be largerthan the solid component, which is often paleand crumbly, consisting of epithelial debris.
There are two histological types of tumours.The adamantinous type resembles adamantino-ma of the jaw and is encountered in virtually allchildren. The papillary type, so-called adult cran-iopharyngioma, occurs in about one-third ofadults and is rare in children.
Clinical presentation
Clinical features include:
Nasal speculum
Tumour
Sphenoid sinus
Endotracheal tube
Fig. 8.13 (a) Diagram of operative exposure in trans-sphenoidal resection of pituitary tumour. A self-retaining retractor is inserted and the anterior wall ofthe sphenoid sinus is removed. (b) Intraoperative X-ray showing the retractor in position and the forceps inthe pituitary fossa.
(a)
(b)
KAY8 12/16/04 7:41 PM Page 120

• raised intracranial pressure• visual impairment• endocrine dysfunction.
Raised intracranial pressureThis is common, particularly in children, who pre-sent with headache, vomiting and papilloedema.
Visual impairmentThis is due to papilloedema, chiasmal compres-sion or a combination of both. Papilloedema isdue to hydrocephalus as a result of 3rd ventricu-lar obstruction by the tumour. The visual field defect is frequently similar to that produced by apituitary tumour, a bitemporal hemianopia, buthomonymous defects are more common than inpituitary adenoma.
Endocrine abnormalitiesThese are frequent in children and consist of:• hypogonadism• stunting of growth• diabetes insipidus.
Endocrine failure due to craniopharyngiomaarising in adults is essentially similar to thatcaused by a pituitary tumour, except that dia-betes insipidus occurs more commonly in pa-tients presenting with craniopharyngioma.
Investigations
The CT scan usually shows a cystic tumour in thesuprasellar region with calcification (Fig. 8.14).Tumours in adults may be solid and are less calci-fied than those seen in younger patients. MRI isuseful in showing the full extent of the tumour(Fig. 8.15).
Changes in the sella turcica are seen in approx-imately 50% of patients. Suprasellar tumours andthe associated hydrocephalus press downwardson the dorsum sellae and anterior clinoids andmay enlarge the sella. Nearly 90% of tumours inchildren have radiographically identifiable calci-fication in the tumour, whereas only 40% ofadults have radiologically demonstrable calcifi-cation. The calcification consists of aggregates ofsmall flecks of calcium and may be curvilinear,outlining a portion of the cyst wall.
On occasions craniopharyngioma and pitu-itary tumours need to be distinguished from aRathke’s cleft cyst (Fig. 8.16). Both craniopharyn-giomas and Rathke’s cleft cysts are thought toarise from embryonic remnants of Rathke’spouch. By the 6th week of embryonic life theresidual lumen of Rathke’s pouch is reduced to anarrow cleft that generally regresses. Persistentenlargement of this cleft is said to be the cause ofRathke’s cleft cyst. These cysts are epithelium-lined cysts containing mucoid material. They areusually confined to the sella, but on occasions can
PITUITARY TUMOURS 121
Fig. 8.14 CT scan. Craniopharyngioma.
(a)
(b)
KAY8 12/16/04 7:41 PM Page 121

122 CHAPTER 8
form large cystic tumours extending into thesuprasellar cisterns (Fig. 8.16).
Treatment
Preoperative visual and endocrine assessment is essential. The standard treatment for cranio-pharyngioma is operative, with an attempt atmaximal resection of the tumour. However, com-plete resection may not be possible due to the extent of the tumour and the intimate attachmentto hypothalamic vital structures.
The usual surgical approach is through a pteri-
onal craniotomy or a bifrontal craniotomy withseparation of the frontal lobes and division of thelamina terminalis. Tumours extending into the3rd ventricle may also need to be approachedthrough the corpus callosum. An extended trans-sphenoidal approach is sometimes advised forthose tumours extending down to the floor of thepituitary fossa.
Postoperative management will include care-ful attention to fluid and electrolyte balance asmany patients have at least a transient diabetesinsipidus following surgery. Other hormonesmay need replacement depending on endocrino-logical assessment.
The role of postoperative radiotherapy in pa-tients with a subtotal resection is controversialbut radiotherapy may be beneficial in decreasingthe production of cyst fluid and delaying recur-rence of the tumour.
Empty sella syndrome
The empty sella refers to a communicating exten-sion of the subarachnoid space into the pituitaryfossa (Fig. 8.17). This may occur as a result of anincomplete anatomical formation of the di-aphragma sellae which allows the arachnoid toherniate directly into the pituitary fossa or as asecondary phenomenon following either pitu-itary surgery or radiotherapy.Fig. 8.15 MRI. Craniopharyngioma.
Fig. 8.16 MRI showing largeRathke’s cleft cyst.
KAY8 12/16/04 7:41 PM Page 122

There is good reason to regard the empty sellaas an anatomical variant rather than a syndrome.Bergland showed the presence of subarachnoidspace within the sella in 20%, and anatomical de-fects of the diaphragma sellae of 5 mm or more innearly 40%, of an autopsy series without pitu-itary disease. However, defects in the diaph-ragma are not the only requirement for formationof an empty sella. Increased intracranial pressureassociated with benign intracranial hypertensionor long-standing hydrocephalus will cause her-niation of the subarachnoid space into the sellaand will result in the remodelling of the pituitaryfossa to produce the classic globular appearanceon plain X-ray and CT scan (Fig. 8.18). It is possi-ble that the normal variations in CSF pressuremay be transmitted into the fossa through an in-competent diaphragma and so result in the bonychanges.
Clinical presentation
Most patients with the radiological features of anempty sella are asymptomatic. The majority ofpatients presenting with symptoms are obese,middle-aged, hypertensive women. Headache isthe most common symptom associated with theempty sella but the features are so varied thattheir relevance to the intrasellar subarachnoidspace is dubious without an underlying cause forpossible raised intracranial pressure.
Visual field defects and endocrine abnormali-ties are subtle and uncommon in patients with
PITUITARY TUMOURS 123
Dura
Basal cisterns(CSF)
Anterior lobe pituitary Anterior lobe pituitary
Arachnoid
CSF
Diaphragma sellae
Normal Empty sella
Fig. 8.17 Empty sella. Thesubarachnoid space is able toenter the sella through anincomplete diaphragma sellae.
Fig. 8.18 Empty sella. (a) The classic globular enlargedsella. (b) CSF within the sella.
(a)
(b)
KAY8 12/16/04 7:41 PM Page 123

124 CHAPTER 8
primary empty sella syndrome. In patients with asecondary empty sella, e.g. following surgery orradiotherapy, field defects may be more pro-nounced but are rarely severe.
The most serious consequence of an emptysella is spontaneous CSF rhinorrhoea. This usual-ly occurs only if there has been an underlyingcause of raised intracranial pressure, such as benign intracranial hypertension. It is managedby repairing the leak in the floor of the sella withcrushed muscle and fascia lata and performing aCSF shunt.
Further readingAbboud CF, Laws ER (1988) Diagnosis of pituitary tu-
mours. In: Young WF, Klee GG, eds. Endocrinologyand Metabolism Clinics of North America. W B Saun-ders, Philadelphia, Vol. 17, 241–277.
Bergland RM, Ray BS, Torak RM (1968) Anatomicalvariations in the pituitary gland and adjacent struc-tures in 225 human autopsy cases. Journal of Neurosurgery 28, 93–99.
Black P McL, Zervas NT, Candia G (1987) Incidence andmanagement of complications of transsphenoidaloperation for pituitary adenomas. Neurosurgery 20,920–924.
Cushing H (1912) The Pituitary Body and its Disorders.Clinical States Produced by Disorders of the HypophysisCerebri. JB Lippincott, Philadelphia.
Ebersold MJ et al. (1983) Pituitary apoplexy treated bytranssphenoidal surgery. A clinicopathological andimmunocytochemical study. Journal of Neurosurgery58, 315–320.
Hardy J (1968) Transphenoidal microsurgery of the nor-mal and pathological pituitary. Clinical Neurosurgery16, 185–217.
Kaufman B (1968) The ‘empty’ sella turcica: a mani-festation of the intrasellar subarachnoid space. Radiology 90, 931–941.
Kaye AH, Black P McL (2000) Operative Neurosur-gery. Churchill Livingstone, London, New York, Edinburgh.
Kaye AH, Galbraith JEK, King J (1981) Intracranialpressure in patients with empty sella syndrome with-out benign intracranial hypertension. Journal of Neurosurgery 55, 453–456.
Kovacs K, Horvath E (1985) Morphology of adenohy-pophyseal cells and pituitary adenomas. In: Imura H,ed. The Pituitary Gland. Raven Press, New York.
Laws ER, Randle RV, Abboud CF (1982) Surgical treat-ment of acromegaly: results in 140 patients. In:Givens JR, ed. Hormone Secreting Pituitary Tumours.Year Book. Medical Publishers, Chicago.
Molitch ME, Fahlbusch R (1995) Medical versus surgi-cal treatment of giant pituitary prolactinomas. In: Al-Mefty O, Origitano TC, Harkey HL, eds. Controversiesin Neurosurgery. Thieme, New York.
Ross D, Wilson CB (1988) Results of transsphenoidalmicrosurgery for growth hormone secreting pitu-itary adenoma in series of 214 patients. Journal of Neurosurgery 68, 854–867.
Scheithauer BW (1984) Surgical pathology of the pitu-itary. The adenomas Part I. In: Sommers SC, RosenPP, eds. Pathology Annual Part I. Appleton-Century-Crofts, Connecticut, 317–374.
Scheithauer BW (1984) Surgical pathology of the pitu-itary. The adenomas Part II. In: Sommers SC, RosenPP, eds. Pathology Annual Part I. Appleton-Century-Crofts, Connecticut, 269–329.
Thapar K, Laws ER (1995) Pituitary tumours. In: KayeAH, Laws ER, eds. Brain Tumours. Churchill Living-stone, Edinburgh.
Trumble HC (1951) Pituitary tumours: observations ontumours which have spread widely beyond the con-fines of the sella. British Journal of Surgery 39, 7–24.
Wilson CB (1984) A decade of pituitary microsurgery.Journal of Neurosurgery 61, 814–833.
Editorial (1982) The intrasella subarachnoid space.Lancet July 31, 249–250.
KAY8 12/16/04 7:41 PM Page 124

The sudden onset of a severe headache in a pa-tient should be regarded as subarachnoid haem-orrhage until proven otherwise.
Subarachnoid haemorrhage occurs whenbleeding is primarily within the subarachnoidspace rather than into the brain itself. It repre-sents about 5–10% of all non-traumatic intra-cranial haemorrhage with an incidence ofapproximately 15 per 100 000 population.Apoplectic death has been mentioned in the ear-liest medical writings but its relationship to in-tracranial haemorrhage and cerebral aneurysmwas not established until the latter part of the sev-enteenth century. The introduction of cerebralangiography by Moniz and Lima in Lisbon in1927 allowed the diagnosis of cerebral aneurysmto be made in living patients who had sustainedsubarachnoid haemorrhage. Pioneering surgeryin the 1930s and 1940s, by Krayenbuhl in Switzer-land and Dandy in North America, showed that aneurysms could be treated operatively, al-though at that time with considerable morbidityand mortality. Consequent improvements in mi-crosurgical techniques and neuroanaesthesiahave considerably improved the safety ofsurgery.
Causes of subarachnoid haemorrhage
The most common cause of subarachnoid haem-orrhage in adults is rupture of a berry aneurysm.Subarachnoid haemorrhage in children is muchless common than in the adult population andthe most common paediatric cause is rupture of an arteriovenous malformation. Cerebralaneurysm as a cause of subarachnoid haemor-
rhage becomes more frequent than arteriovenousmalformations over the age of 20 years. Rarecauses of subarachnoid haemorrhage includebleeding from a tumour, bleeding disorders,blood dyscrasias and rupture of a spinal arteri-ovenous malformation (Table 9.1). The aetiologyof subarachnoid haemorrhage remains undis-covered in approximately 15% of cases after thor-ough clinical and radiographic study. Thesepatients often have associated intracranial vascu-lar atherosclerosis and hypertension.
Subarachnoid haemorrhage —presenting features (Table 9.2)
Headache
The sudden onset of a severe headache of a typenot previously experienced by the patient is thehallmark of subarachnoid haemorrhage. A rela-tively small leak from an aneurysm may result ina minor headache, sometimes referred to as the‘sentinel headache’, as this may be the warningepisode of a subsequent major haemorrhagefrom the aneurysm. Naturally, recognition of apossible minor ‘warning’ haemorrhage is essen-tial to avert a possible later catastrophic bleed, al-though many are only recognized in retrospect.
Diminished conscious state
Most patients have some deterioration of theirconscious state following subarachnoid haemor-rhage. This varies from only a slight changewhen the haemorrhage has been minor toapoplectic death resulting from massive haem-
CHAPTER 9
9 Subarachnoid haemorrhage
125
KAY9 12/16/04 7:42 PM Page 125

126 CHAPTER 9
orrhage. It is a common cause of sudden death inyoung adults.
Meningism
Blood in the subarachnoid cerebrospinal fluidwill cause the features of meningism — headache,neck stiffness, photophobia, fever and vomiting.Irritation of the nerve roots of the cauda equina,which occurs when the blood extends down tothe lumbar theca, may result in sciatica-type painand low back discomfort.
Focal neurological signs
Focal neurological signs may occur in subarach-
noid haemorrhage due to concomitant intracere-bral haemorrhage, the local pressure effects of theaneurysm itself, or cerebral vasospasm.
A cerebral aneurysm usually lies within thesubarachnoid cisterns but the aneurysm may be-come adherent to the adjacent brain parenchymadue to adhesions, frequently resulting from pre-vious leakage of blood. A haemorrhage from ananeurysm in these circumstances may also ex-tend into the brain and the position of the intra-cerebral haematoma will determine the type ofneurological deficit. A middle cerebral arteryaneurysm frequently ruptures into the temporallobe, resulting in hemiparesis and aphasia if thedominant hemisphere is involved (Fig. 9.1). An-terior communicating artery aneurysms mayhaemorrhage into the frontal lobes with subse-quent akinetic mutism (Fig. 9.2). Defective conjugate ocular movement may result fromhaemorrhage into a frontal lobe, persistent devia-tion usually being towards the side of the lesionand purposeful gaze defective away from thatside.
Occasionally, an aneurysm may also ruptureinto the subdural space, resulting in a subduralhaematoma and brain compression causing lat-eralizing neurological signs. An arteriovenousmalformation usually lies at least partially within
Table 9.1 Causes of subarachnoid haemorrhage(%).
Cerebral aneurysm 70Arteriovenous malformation 10Undiscovered 15Other rare causes 5
Spinal arteriovenous malformationTumourBlood dyscrasia
Table 9.2 Subarachnoid haemorrhage —presenting features.
Headache
Diminished conscious state
MeningismNeck stiffness, vomiting, photophobia, fever
Focal neurological signsIntracerebral haemorrhageFocal pressure by aneurysmVasospasm
Fundal changesSubhyaloid haemorrhageRetinal haemorrhagePapilloedema
Fig. 9.1 Intracerebral haematoma in temporal lobedue to rupture of a middle cerebral artery aneurysm.
KAY9 12/16/04 7:42 PM Page 126

the brain parenchyma, so that when it rupturesintracerebral bleeding is frequently associatedwith the subarachnoid haemorrhage.
Focal neurological signs may result from theposition of the aneurysm itself. An aneurysmarising from the internal carotid artery at the origin of the posterior communicating artery(known as a posterior communicating arteryaneurysm) may cause pressure on the 3rd cranialnerve. Patients with an enlarging aneurysm inthis position may present with features of a 3rdcranial nerve palsy (ptosis, pupil dilatation, ex-traocular muscle palsy) prior to a subarachnoidhaemorrhage. It is vital that the correct diagnosisof an enlarging cerebral aneurysm is made in thissituation, so as to avoid the possible catastrophiceffects of subarachnoid haemorrhage. The majordifferential diagnosis of the aetiology of an ap-parently isolated 3rd cranial nerve palsy is an is-chaemic lesion such as those resulting fromdiabetes mellitus or atherosclerosis. Pupil size isa useful guide in differentiating between thesecauses. The pupil is usually dilated, with an expanding aneurysm which compresses the superior aspect of the nerve that contains the
parasympathetic pupillary fibres arising fromthe nucleus of Edinger–Westphal in the mid-brain. An expanding aneurysm usually results inmore pain than the ischaemia associated with di-abetes mellitus, although this is an unreliableguide. If there is any doubt about the cause of the3rd nerve palsy then angiography must be per-formed expeditiously. In a patient with impairedconscious state, or in one with other abnormalneurological signs suggesting a massive haemor-rhage, 3rd cranial nerve palsy may be secondaryto temporal lobe herniation.
A giant aneurysm (defined as larger than2.5 cm in diameter) may cause compression ofadjacent neural structures resulting in focal signs(Fig. 9.3). Alarge aneurysm of the internal carotidartery or anterior communicating artery willcause compression of the optic nerve or chiasm,respectively, resulting in visual failure. Large vertebrobasilar aneurysms may cause brainstemcompression.
Cerebral vasospasm following subarachnoidhaemorrhage does not usually result in clinicalmanifestations for 2 or 3 days after the initialbleed so that, although it may be the cause of subsequent focal signs resulting from brain is-chaemia, it is not the cause of focal signs imme-diately after the haemorrhage.
Optic fundiMild papilloedema is common within the firstfew days of haemorrhage because of the sudden
SUBARACHNOID HAEMORRHAGE 127
Fig. 9.2 Frontal intracerebral haematoma with bloodin the Sylvian fissure and ventricles from a rupturedanterior communicating artery aneurysm.
Fig. 9.3 Giant internal carotid artery aneurysm.
KAY9 12/16/04 7:42 PM Page 127

128 CHAPTER 9
elevation of intracranial pressure resulting fromhydrocephalus or cerebral oedema. A transientcommunicating hydrocephalus often occurs aftersubarachnoid haemorrhage due to blood block-ing the arachnoid villi. In about 10% of cases thehydrocephalus persists and is severe enough torequire a CSF shunt.
Ophthalmoscopy may reveal fundal haemor-rhages, particularly in severe subarachnoidhaemorrhage. Small, scattered retinal haemor-rhages usually resolve satisfactorily, although the large subhyaloid haemorrhages may breakinto the vitreous, resulting in permanent visualdefect.
Clinical assessment
The diagnosis is usually obvious when the histo-ry is obtained from the patient, relative or friend.The classic sudden onset of severe headache withfeatures of meningism and decreased consciousstate is characteristic of a subarachnoid haemor-rhage. However, difficulty may occur when thehaemorrhage has been minor and, tragically, a
subarachnoid haemorrhage may be misdiag-nosed as either migraine or tension headache. Afull neurological examination should be per-formed with particular attention given to thepresence of neck stiffness, altered conscious state,pupillary status and fundal haemorrhage. Clini-cal grading systems have been based on theseverity of the headache and neck stiffness andon the level of conscious state. The two major systems are the Hunt and Hess classification andthe World Federation of Neurological Surgeons(WFNS) system (Table 9.3).
Investigations
The major differential diagnosis is meningitis, al-though a minor haemorrhage is often misdiag-nosed as migraine. Confirmation of the clinicaldiagnosis of subarachnoid haemorrhage shouldbe undertaken as soon as possible. Computer-ized tomography (CT) scanning (Fig. 9.4) is thebest initial investigation as it will confirm the di-agnosis in over 85% of cases. It will also provideadditional information on associated pathology
Table 9.3 Subarachnoid haemorrhage grading systems.
Hunt and Hess grading system*Grade Description
1 Asymptomatic, or minimal headache and slight nuchal rigidity2 Moderate to severe headache, nuchal rigidity, no neurological deficit (except cranial nerve palsy)3 Drowsiness, confusion or mild focal deficit4 Stupor, moderate to severe hemiparesis, possible early decerebrate rigidity and vegetative
disturbances5 Deep coma, decerebrate rigidity, moribund
WFNS grading systemGrade Glasgow Coma Score (GCS) Motor deficit
1 15 No deficit except a cranial nerve palsy2 14–13 No deficit3 14–13 Any deficit4 12–7 With or without focal neurodeficit5 6–3 Coma with or without abnormal posturing
* Serious systemic disease such as hypertension, diabetes, severe arteriosclerosis, chronic pulmonarydisease, and vasospasm on angiography result in placement in next less favourable category.
KAY9 12/16/04 7:42 PM Page 128

such as intracerebral haemorrhage and hydro-cephalus, and on the position of the haemor-rhage, which is helpful if there is more than oneaneurysm. Arteriovenous malformation causingsubarachnoid haemorrhage can frequently be di-agnosed on the CT scan. If there is any doubt thatsubarachnoid blood is present on the CT scan, asmay occur following more minor haemorrhages,a lumbar puncture is essential. The presence ofxanthochromia (yellow staining) in the CSF will confirm subarachnoid haemorrhage. Xan-thochromia resulting from breakdown of haemo-globin in the red blood cells occurs within 6–8hours after the initial haemorrhage and it willconfirm that the blood in the CSF is not due totrauma from the lumbar puncture needle. A fur-ther method frequently suggested to excludetrauma from the passage of the lumbar punctureneedle as a cause of bloody CSF is to allow theCSF to drip into three consecutive tubes; if theblood fails to ‘clear’ in the last tube subarach-noid haemorrhage is confirmed. However, thismethod will result in many false positive diag-noses. The CSF should also be immediately ex-amined for the presence of white blood cells andorganisms.
Cerebral angiography will confirm the cause of
the subarachnoid haemorrhage and will deter-mine the subsequent treatment. Intra-arterialdigital subtraction angiography has consider-ably reduced the risks of conventional angio-graphy and should be undertaken as soon as thediagnosis has been confirmed and it is clear thatthe patient will survive the initial haemorrhage.
Cerebral aneurysm
Cerebral aneurysms are the most common causeof subarachnoid haemorrhage in the adult popu-lation, with a maximal incidence in the 4th and5th decades of life, although they can occur at anyage.
Surgical anatomy
The great majority of aneurysms arise at thebranch points of two vessels, usually at an acuteangle, and are situated mainly on the circle ofWillis and the trunks of the large arteries whichsupply it. A few arise from its immediate branch-es but aneurysms on peripheral vessels are rare(Fig. 9.5). The majority of aneurysms occur inconstant positions on the circle of Willis andabout 85% occur on the anterior half of the circle(Table 9.4). Aneurysms arise at approximatelyequal frequency from the internal carotid artery,anterior communicating artery and middle cere-bral artery. Those associated with the internalcarotid artery most frequently arise at the origin
SUBARACHNOID HAEMORRHAGE 129
Fig. 9.4 Blood in the Sylvian fissure and basal cisternsindicative of subarachnoid haemorrhage.
Anterior cerebral
Anterior communicating
Middle cerebral
Posteriorcommunicating
Superior cerebellarBasilar Anterior inferior
cerebellar
Posterior inferiorcerebellarVertebral
Posterior cerebral
Internalcarotid
Fig. 9.5 Usual sites of cerebral aneurysms.
KAY9 12/16/04 7:42 PM Page 129

130 CHAPTER 9
Table 9.4 Position of cerebral aneurysm.
Anterior circle of WillisAnterior communicating arteryMiddle cerebral artery — bifurcation ortrifurcationInternal carotid artery
Posterior communicating arteryTerminal bifurcationAnterior choroidal arteryOphthalmic arteryIntracavernous
Pericallosal artery
Posterior circulation (15%)Terminal basilar artery — most commonVertebrobasilar junctionPosterior inferior cerebellar arteryAnterior inferior cerebellar arterySuperior inferior cerebellar arteryPosterior cerebral artery
Pathogenesis of cerebral aneurysms
The common type of cerebral aneurysm resultingin a subarachnoid haemorrhage is a saccularaneurysm, which is also known as a berry or con-genital aneurysm. Fusiform aneurysms occur inthe intracranial circulation, particularly the ver-tebrobasilar arteries or internal carotid arteries,and are due to diffuse atheromatous degenera-tion of the arterial wall, frequently associatedwith hypertension. Mycotic aneurysms resultfrom septic emboli. They may be situated on pe-ripheral vessels, are frequently multiple andhave a high risk of haemorrhage.
The saccular or berry aneurysm arises at thejunction of vessels where there is a congenital de-ficiency in the muscle coat. The elastic layer incerebral arteries, in contrast with arteries else-where, is limited to the internal lamina, makingthese vessels more susceptible to weakening ef-fects of degeneration. Fragmentation and disso-lution of the internal elastic membrane occurs atthe site of aneurysm development. The combina-tion of the muscle defect and the discontinuity ofthe underlying internal elastic membrane isprobably necessary for the formation of a saccu-lar aneurysm. Other factors that increase the riskof aneurysm formation include atheroma and hypertension. There is an increased incidence of atheroma in the vessels of the circle of Willisand hypertension in patients with rupturedaneurysms. It is probable that these factors play arole in the growth of the aneurysm and its subse-quent rupture in some patients.
Related diseasesThere is no definite hereditary basis to the devel-opment of intracranial aneurysms, although anepidemiology study has shown an increased inci-dence of approximately seven-fold in first-degreerelatives of patients who have had an aneurys-mal subarachnoid haemorrhage, with a lifetimerisk of 2–5% of developing an aneurysmal sub-arachnoid haemorrhage. Aneurysms do occur inassociation with hereditary syndromes such asEhlers–Danlos syndrome, coarctation of the aortaand polycystic kidney disease.
of the posterior communicating artery (the so-called posterior communicating arteryaneurysm), less frequently at the terminal bifur-cation, and occasionally at the origin of the oph-thalmic artery, the anterior choroidal artery or inthe cavernous sinus. Middle cerebral arteryaneurysms arise from the middle cerebral arteryat its bifurcation or trifurcation in the Sylvian fis-sure (Fig. 9.6). Less commonly an aneurysm mayarise from the pericallosal artery at the genu ofthe corpus callosum.
Approximately 15% of aneurysms arise fromthe posterior half of the circle of Willis, the mostcommon position being the basilar artery, mostfrequently at the terminal bifurcation into theposterior cerebral arteries. However, ananeurysm may arise from any of the mainbranches of the vertebral or basilar arteries, inparticular the posterior inferior cerebellar artery,anterior inferior cerebellar artery or superiorcerebellar artery (Fig. 9.7).
Multiple aneurysmsAneurysms occur in more than one position inapproximately 15% of cases.
KAY9 12/16/04 7:42 PM Page 130

Management of ruptured cerebral aneurysm
The management of patients following ruptureof a cerebral aneurysm is determined by threemajor factors.1 Severity of the initial haemorrhage.
2 Rebleeding of the aneurysm.3 Cerebral vasospasm.
Severity of the initial haemorrhageAbout 30% of all patients suffering a subarach-noid haemorrhage from a ruptured aneurysm
SUBARACHNOID HAEMORRHAGE 131
Fig. 9.6 (a) Anterior cerebral artery aneurysm. (b) Middle cerebral artery aneurysm. (c) Posterior communicatingartery aneurysm. (d) Terminal internal carotid artery aneurysm.
(a) (b)
(c) (d)
Fig. 9.7 (a) Terminal basilar artery aneurysm. (b) Aneurysm arising from junction of basilar artery and superiorcerebellar artery. (c) Posterior inferior cerebellar artery aneurysm.
(a) (b) (c)
KAY9 12/16/04 7:42 PM Page 131

132 CHAPTER 9
either have an apoplectic death or are deeply co-matose as a result of the initial haemorrhage.
RebleedingThis occurs in about 50% of patients within 6weeks and 25% of patients within 2 weeks of theinitial haemorrhage. About half the patients thathave a subsequent haemorrhage will die as a re-sult of the rebleed. After the first year the risk of afurther haemorrhage from the aneurysm is about2–3% per year.
The only certain way to prevent an aneurysmrebleeding is to exclude it from the circulation.Antifibrinolytic agents (such as epsilon aminocaproic acid or tranexamic acid) decrease therisks of rebleeding but, as they are associatedwith increased incidence of thrombosis (such asdeep vein thrombosis and pulmonary embolus)and an increased risk of cerebral thrombosis as-sociated with vasospasm, these agents are nowrarely used.
Cerebral vasospasmAngiographic vasospasm (Fig. 9.8) occurs inabout 50% of patients following subarachnoidhaemorrhage and in 25% it results in serious neu-rological complications. There is a direct correla-tion between the amount of blood noted in thebasal cisterns on the CT scan, the risk of develop-ing vasospasm and its severity. Although thespasm may principally affect the vessels most ad-
jacent to the ruptured aneurysm, generalized vasospasm occurs frequently. The clinical mani-festations resulting from vasospasm will be determined by the vessels which are most severe-ly affected. Spasm of the internal carotid arteryand middle cerebral arteries produces hemipare-sis and aphasia in the dominant hemisphere. Va-sospasm of the anterior cerebral vessels causesparalysis of the lower limbs and akinetic mutism.Severe vasospasm may cause widespread cere-bral ischaemia so that the patient may becomeobtunded; if the vasospasm is sufficiently severeit will result in death. Vasospasm does not usual-ly occur until 2 or 3 days after the initial haemor-rhage and its onset is rarely delayed beyond 14days. The cause of delayed cerebral vasospasmremains obscure but it is certainly related to vaso-constrictor substances in the CSF as a result of thehaemorrhage. Vasoactive substances isolatedfrom both the blood clot surrounding the spasticvessels and the adjacent CSF include oxy-haemoglobulin released from the erythrocytes,serotonin, thromboxane A2, prostaglandins (F2-alpha and E2), angiotensin and histamine. In ad-dition, unidentified vasoconstrictor substanceshave been isolated from incubates of fibrinogen,platelets, erythrocytes and blood/CSF mixtures.The contractile process ultimately depends onthe availability of cytosolic activator calciumions.
Until recently there has been no satisfactorytreatment for established cerebral vasospasm. Ifthe aneurysm has been surgically occluded fromthe circulation then hypertensive therapy com-bined with hypervolaemia may overcome the hy-poperfusion due to narrowing of the cerebralblood vessels and reverse the ischaemic effects.Calcium channel blocking agents such as nimod-opine and nifedipine are frequently used in sub-arachnoid haemorrhage to prevent and treatvasospasm, although there is still some doubt asto their effectiveness. Nimodopine, a substituted1,4-dihydropyridine, is a calcium ‘antagonist’that blocks the influx of extracellular calcium, theprimary source of calcium for contraction of largecerebral arteries. Trials in North America, Britainand Scandinavia have shown promising resultswhen the calcium channel blocking agents are
Fig. 9.8 Spasm of the anterior cerebral arteriesfollowing subarachnoid haemorrhage from an anteriorcommunicating artery aneurysm.
KAY9 12/16/04 7:42 PM Page 132

used prophylactically, although there is debate asto whether their effect is due to their action on the cerebral vessels or due to a ‘brain protection’effect.
Following the angiogram that confirms a cere-bral aneurysm, a decision is then made as to thedefinitive treatment of the aneurysm. This willinvolve either:• surgery with clipping of the aneurysm or• endovascular obliteration of the aneurysm.
Surgery for ruptured aneurysmThe timing of the operation is critical in obtain-ing optimal results following subarachnoidhaemorrhage. Although better operative resultsmay be achieved when the surgery is delayed,the longer the operation is deferred the greaterthe risk that the aneurysm will rebleed. In gener-al, the operation is performed as soon as possibleafter the cerebral angiogram. In the past surgerywas avoided when the patient had clinical or an-giographically severe vasospasm, but it is nowrecognized that it is best to clip the aneurysmeven in the presence of clinical or radiological va-sospasm as with the aneurysm excluded from thecirculation the spasm can be treated using hyper-tensive hypervolaemic therapy and endovascu-lar techniques.
Surgery is usually not performed on patientswho are comatosed or have features of decere-brate posturing response, unless the CT scanshows a large intracerebral haematoma resultingfrom the ruptured aneurysm which needs to beevacuated, or hydrocephalus as a cause of thepoor neurological state.
Preoperative managementIn those patients in whom it has been elected forsome reason to delay surgery, the managementshould include careful attention to the following.• Posture. The patient should lie flat in a quietroom with subdued lighting. Every attemptshould be made to avoid environmental situa-tions which could cause sudden elevation of thepatient’s blood pressure and thus increase therisk of rupture of the aneurysm. Sedation usingbarbiturates or diazepam may be necessary if thepatient is agitated.
• Blood pressure control. The blood pressure is fre-quently elevated immediately after the haemor-rhage and should be carefully controlled. Initiallythis should be done using intravenous medica-tion and utilizing vasodilating agents (such ashydralazine or glyceryl trinitrate) and beta-blockers. Although it is essential to control highblood pressure, as this may lead to rupture of the aneurysm, hypotension may result in cere-bral ischaemia, particularly when vasospasm ispresent. The appropriate desirable blood pres-sure will depend upon the premorbid level.• Fluids and electrolytes. Correct hydration is es-sential to avoid electrolyte disturbance; in addi-tion, overhydration may precipitate cerebraloedema and insufficient fluids may increase the risk of cerebral thrombosis associated withvasospasm. Electrolyte disturbances may alsooccur following subarachnoid haemorrhage dueto inappropriate antidiuretic hormone (ADH) se-cretion, which results in hyponatraemia.• Pain relief. Simple analgesic medication orcodeine phosphate is best used for controlling the headaches resulting from subarachnoidhaemorrhage.
Surgical proceduresThe surgical procedures available are:• occlusion of the neck of the aneurysm• reinforcement of the sac of the aneurysm• proximal ligation of a feeding vessel.
Haemorrhage from an aneurysm is due to rup-ture of the fundus of the aneurysmal sac. There-fore, the best surgical procedure is to occlude the neck of the aneurysm, thereby isolating theaneurysm from the circulation. In brief, the oper-ation involves a craniotomy which is usuallybased on the pterion (pterional craniotomy) foraneurysms of the anterior circulation. This typeof craniotomy may also be used for aneurysmsarising from the terminal basilar artery, althoughsome surgeons prefer an approach under thetemporal lobe via a temporal craniotomy. Micro-surgical techniques, utilizing the operating mi-croscope and microneurosurgical instruments,are employed. Access to the basal cisterns may beaided by withdrawing CSF either using a ventric-ular drain or from the lumbar theca. The arach-
SUBARACHNOID HAEMORRHAGE 133
KAY9 12/16/04 7:42 PM Page 133

134 CHAPTER 9
noid around the basal cisterns is opened, the neckof the aneurysm identified and dissected and aclip placed across the neck to exclude theaneurysm from the circulation. During the dis-section of the aneurysm it is essential that vitaladjacent vessels, including the perforating arter-ies, are not injured, as damage to these vesselsmay result in severe neurological disability.
Occasionally it is not possible to safely place aclip across the neck of the aneurysm, usually as aresult of branches of the parent vessel either aris-ing from the aneurysm or being inseparable fromthe fundus. In this case the wall of the aneurysmmay be reinforced by a number of techniques, in-cluding wrapping the wall with crushed muscle,gauze or cotton wool or a combination of these.Rapidly solidifying polymer (aneurysm cement)may be poured around the aneurysm to provideit with a solid covering.
Although ligation of the common or internalcarotid artery in the neck was commonly used fortreatment of aneurysms of the internal carotidartery, improved microneurosurgical techniqueshave made this operation almost obsolete. Theprocedure has also been used for intracavernousaneurysms but these are now best treated by en-dovascular techniques usually performed by aradiologist. Ligation of the internal carotid arterymay be performed for a giant internal carotidartery aneurysm which is not amenable to directsurgery, but an extracranial–intracranial bypassprocedure may need to be performed prior to theocclusion to prevent cerebral ischaemia.
Postoperative managementThe usual postcraniotomy operative manage-ment applies, with special attention to be given tothe neurological state, hydration, posture, oxy-genation and blood pressure. Anticonvulsantmedication is recommended for 3 months to 1year. Steroid medication is sometimes used in theinitial postoperative course to control cerebraloedema, although its effectiveness is not proven.
The major specific postoperative problem re-sults from delayed cerebral vasospasm. As indi-cated previously, prophylactic calcium channelblocking agents may be of use in preventing thiscomplication. The transcranial Doppler, utilizing
non-invasive ultrasound, may give useful infor-mation on the degree of intracranial vasospasm.Symptomatic vasospasm can be treated using hypervolaemic hypertensive therapy. This treat-ment entails careful monitoring and requires thetransfer of the patient to an intensive care unit.Recently, endovascular techniques to dilate thevessels in spasm or administer intra-arterial pa-paverine into the intracranial vessels have beenused to treat cerebral vasospasm postoperativelywith some success.
Endovascular procedures for ruptured aneurysms
Over the past 10 years endovascular techniques(using detachable coils) have been used to oblit-erate cerebral aneurysms. These have been inves-tigated in international trials, and have proven tobe effective in excluding the aneurysm from thecirculation.
The technique is usually performed by a spe-cialist interventional radiologist, and almost al-ways under general anaesthesia. As with surgery,it is recommended that the aneurysm is ‘coiled’as soon as possible after the angiogram has been performed to confirm the presence of ananeurysm (Fig. 9.9).
The recent ISAT trial showed the possible superiority of endovascular coiling over surgery,although there has been some debate as to these findings. The main concern remains as towhether the obliteration of the aneurysm is per-manent, as the aneurysm can recur, particularlywith ‘impaction’ of the coils into the fundus of theaneurysm, some months after the initial treat-ment. In most centres a check angiogram is per-formed at 6, 12 and 24 months after the treatment.
The decision as to whether an aneurysmshould be ‘clipped’ by a surgeon or ‘coiled’ by aninterventional neuroradiologist is best madejointly by the treating specialist, cerebrovascularneurosurgeon and neuroradiologist. The inter-ventional neuroradiologist will base his decisionon• the access to the aneurysm and• the configuration of the aneurysm.
Access to the aneurysm may be impaired by
KAY9 12/16/04 7:42 PM Page 134

stenosis or tortuosity within the carotid artery(for anterior circulation aneurysms) and verte-brobasilar artery (for posterior circulationaneurysms). The ‘dome to neck’ ratio is an im-portant consideration in deciding whether theconfiguration of the aneurysm is appropriate forcoiling. In general, most neuroradiologists preferthe ratio to be 2 : 1 or greater. New techniques ininterventional radiology including the use ofstents and three-dimensional coils have in-creased the number of aneurysms that can betreated by endovascular techniques. At present,over 80% of terminal basilar aneurysms can betreated by endovascular techniques, but onlyabout half of the anterior circulation aneurysmsare amenable to ‘coiling’. Most interventional ra-diologists do not coil middle cerebral arteryaneurysms, as there is difficulty in obliterating
the aneurysm whilst maintaining patency of thevessels. At The Royal Melbourne Hospital ap-proximately 50% of aneurysms since the year2000 have been treated by coiling.
Management of an unruptured aneurysm
Multiple aneurysms occur in 15% of patients whopresent following subarachnoid haemorrhage. Ingeneral, an unruptured aneurysm will be clippedat the same time as the surgery for the rupturedaneurysm, provided it can be performed throughthe same craniotomy. The indications for surgeryare controversial for an unruptured aneurysmoccurring in a patient who has suffered a sub-arachnoid haemorrhage from another aneurysm,or for an unruptured aneurysm found incidental-ly. The debate regarding the optimal manage-ment of patients with an unruptured aneurysmrevolves around the relative risk of rupture of theaneurysm vs. the risk of treatment, by eithersurgery or an endovascular approach. In the pastthe risk of haemorrhage from an unrupturedaneurysm was usually quoted at 2–3% per year.However, in 1998 the New England Journal of Medicine published a large study of the naturalhistory of unruptured intracranial aneurysmswhich indicated that the risk of haemorrhage wasvery much lower, particularly for aneurysms lessthan 10 mm in diameter and those arising fromthe middle cerebral artery. There has been con-siderable debate in the neurosurgical literatureregarding the veracity of the so-called ISUIA(International Study of Unruptured IntracranialAneurysms) study, with some experts question-ing the methodology. In general, the risk of rup-ture will depend on the size of the aneurysm, onthe configuration of the aneurysm, in particular ifthere is a ‘daughter sac’ attached to the fundus,on a positive family history for aneurysmal sub-arachnoid haemorrhage and on the age of the pa-tient. Symptomatic aneurysms of all sizes shouldbe considered for treatment.
Arteriovenous malformation
Arteriovenous malformations are the most common cause of subarachnoid haemorrhage in
SUBARACHNOID HAEMORRHAGE 135
Fig. 9.9 (a) Endovascular treatment of internal carotidartery aneurysm. Figure (b) shows the aneurysmexcluded from the circulation following theendovascular insertion of coils.
(a)
(b)
KAY9 12/16/04 7:42 PM Page 135

136 CHAPTER 9
children. Other types of vascular malformationsof the brain include the following.• Capillary telangiectasia — bleed infrequentlybut may result in fatal haemorrhage, particularlyin the pons.• Cavernous haemangioma (see Fig. 9.12) —often cause minor local extravasations of bloodbut major haemorrhage is uncommon. Patientsfrequently present following an epileptic seizureif the haemangioma is in the cerebral hemi-spheres. Posterior fossa haemangiomas may pre-sent with a brainstem stroke.• Venous malformations.
The arteriovenous malformation is the mostcommon vascular malformation. Although it ac-counts for approximately 60% of all subarach-noid haemorrhage in children, by the 3rd decadeit is responsible for 20% and by the 5th decade forless than 5%.
Clinical presentation
Haemorrhage. This is the most frequent first symp-tom of an arteriovenous malformation and, al-though the bleeding may be subarachnoid, thereis commonly an intracerebral component. The ar-teriovenous fistulous communication results inthe development of aneurysms within the lesion,enlargement of the arteries which feed the malformation and, consequently, the possiblesecondary development of saccular aneurysmson the major feeding vessels. The haemorrhageassociated with an arteriovenous malformationmay quite often be due to rupture of a saccularaneurysm on the feeding vessel.
Epilepsy. This is the second most common pre-senting manifestation of an arteriovenous mal-formation.
Headache. Migraine characteristics are particu-larly associated with headache due to arterio-venous malformation.
Progressive neurological deficit. For example, aslowly progressive hemiparesis may occur in alarge malformation due either to local ischaemiainduced by the shunt or to increasing size of thelesion.
Surgical anatomy
Most arteriovenous malformations are situatedin the cerebral hemispheres, although they mayoccur in the posterior fossa involving either thecerebellum or brainstem and they show consid-erable variation in size. The malformations in-volving the cerebral hemispheres frequentlyform a pyramidal mass, the base of which mayreach the cortical surface with the apex pointingtowards the lateral ventricle. There are frequent-ly multiple, enlarged arteries feeding the malfor-mation and arterialized draining veins extendsuperficially to the superior sagittal sinus ortransverse sinus or deeply into the deep cerebralvenous system.
Radiological investigations for arteriovenousmalformations (Figs 9.10–9.12)
An arteriovenous malformation is often apparenton the CT scan because of the vivid enhancementof the enlarged feeding vessel and arterializeddraining veins after intravenous contrast. Cere-bral angiography is best performed using digitalsubtraction angiographic techniques and is es-sential for adequate evaluation of the malforma-tion. Precise determination of the position of themajor feeding and draining vessels is vital priorto surgery. Magnetic resonance imaging is a valu-able aid in determining the exact position of thearteriovenous malformation and the vessels.
Preoperative occlusion of accessible majorfeeding vessels close to the malformation by aninterventional radiologist may be useful if theprocedure is technically feasible. A flow-directedcatheter is positioned in the artery, which is oc-cluded using cyanoacrylate glue or a polymeriz-ing collagen mixture.
Management
As with cerebral aneurysms the aim of treatmentis to avoid either an initial haemorrhage or re-bleed from the malformation. There has beencontroversy over the risk of haemorrhage and themorbidity and mortality associated with ruptureof an arteriovenous malformation. Recent stud-
KAY9 12/16/04 7:42 PM Page 136

ies have shown that the chance of haemorrhagefor both ruptured and unruptured arteriovenousmalformations is about 3% each year and that thecombined morbidity and mortality of each haem-orrhage is at least 40%. However, unlike cerebralaneurysms, haemorrhage from an arterioven-ous malformation rarely causes symptomatic vasospasm.
Surgical excision, provided it is technically fea-sible and would not result in a disabling neuro-logical deficit, should be performed if themalformation has haemorrhaged.
Unruptured arteriovenous malformationsshould be considered for excision if surgery is un-likely to produce significant neurological deficit.
Surgery for arteriovenous malformationsThe principles of the operation involve isolationand occlusion of the principal feeding arteriesfollowed by meticulous dissection of the malfor-mation, with occlusion and division of the nu-merous small feeding vessels. The draining veinsshould be ligated only after all the feeding vesselshave been occluded, since premature obstructionto the arterialized venous outflow will result in aprecipitous swelling and rupture of the vascularmass.
The surgical management of giant arterio-venous malformations is fraught with consid-erable risk. The lesions may be surrounded by chronically ischaemic brain ‘steal’ by the
SUBARACHNOID HAEMORRHAGE 137
Fig. 9.10 (a) The arteriovenous malformation enhances vividly on the CT scan after intravenous contrast and themajor dilated feeding vessels can be seen. (b) The MRI shows the position of the malformation in coronal andaxial planes and further information about the feeding vessels and draining veins (c).
(a) (b) (c)
Fig. 9.11 Cerebral angiography (digital subtraction angiogram) demonstrates the vascular anatomy of thearteriovenous malformation. (a) The major feeding vessels are shown on the arterial phase. (b) The drainingveins are demonstrated on the venous phase.
(a) (b)
KAY9 12/16/04 7:42 PM Page 137

138 CHAPTER 9
malformation and abrupt occlusion of the shuntthrough the malformation has led in some casesto oedema and haemorrhage in the adjacentbrain, a phenomenon first described by Spetzlerand which was called the ‘normal perfusionpressure breakthrough’ theory. Methods thathave been employed to avoid this complica-tion include preoperative and intraoperativeembolization and staged excision of the malformation.
The use of radiosurgical techniques, involvingeither the gamma knife (a highly focused cobaltsource of irradiation) or stereotactic radiosurgeryusing a linear accelerator, has been advocated forthe treatment of small (less than 3 cm diameter),unruptured and surgically inaccessible arterio-venous malformations with complete angio-graphic obliteration in greater than 80% oflesions with a diameter of 3 cm or less at 3 yearsafter radiation. However, as the radiotherapy ef-fect is slow, the patient remains at risk fromhaemorrhage for some years.
Vein of Galen malformation
This unusual malformation results when arteriesfeed directly into the vein of Galen and producesdistinct clinical syndromes depending on the ageat which the disease presents.
• Neonates present shortly after birth withcyanosis and heart failure due to the shuntthrough the malformation.• Infants and young children present withseizures and hydrocephalus due to obstruction ofthe cerebral aqueduct.• Adults may present with multiple subarach-noid haemorrhage.
Subarachnoid haemorrhage of unknown aetiology
In about 15% of patients the cause of subarach-noid haemorrhage remains unclear, despite clini-cal and radiological investigation. Many of thesepatients are hypertensive and have evidence ofintracranial arterial atherosclerosis, although thisis not inevitable. Most patients make a good re-covery following the subarachnoid haemorrhageand rebleeding is uncommon.
Management
It is essential to exclude a cause for the subarach-noid haemorrhage and this may entail repeatingthe cerebral angiography, particularly if the ini-tial angiography has been in some way imperfectand especially if not all the major vessel brancheshave been shown adequately. Systemic causes forthe subarachnoid haemorrhage must be exclud-ed, as well as rare causes such as pituitaryapoplexy.
The patient is managed symptomatically withbed rest until the headache has settled.
Further readingChyatte D, Fode N, Sundt T (1988) Early versus late in-
tracranial aneurysm surgery in subarachnoid haem-orrhage. Journal of Neurosurgery 69, 326–331.
Dorsch NWC, King MT (1994) A review of cerebral va-sospasm in aneurysmal subarachnoid haemorrhage.Journal of Clinical Neuroscience 1, 19–26.
Dorsch NWC, King MT (1994) A review of cerebral va-sospasm in aneurysmal subarachnoid haemorrhage.Journal of Clinical Neuroscience 1, 78–92.
Dorsch NWC, King MT (1994) A review of cerebral va-sospasm in aneurysmal subarachnoid haemorrhage.Journal of Clinical Neuroscience 1, 151–160.
Fig. 9.12 Cavernous haemangioma.
KAY9 12/16/04 7:42 PM Page 138

Drake CJ (1984) Early times in aneurysm surgery. Clini-cal Neurosurgery 32, 41–50.
Freedman WA (1995) Linear accelerator radiosurgeryfor arteriovenous malformations, the relationship ofsize to outcome. Journal of Neurosurgery 82, 180–189.
Heros RC, Tu YK (1987) Is surgical therapy needed forunruptured arteriovenous malformations? Neurology37, 279–286.
Heros RC, Zervas NT, Varsos V (1983) Cerebral va-sospasm after subarachnoid haemorrhage: an up-date. Annals of Neurology 14, 599–603.
Jane JA et al. (1985) The natural history of aneurysmsand arteriovenous malformations. Journal of Neuro-surgery 62, 321–323.
Kaye AH, Black P McL. (2000) Operative Neurosur-gery. Churchill Livingstone, London, New York, Edinburgh.
International subarachnoid aneurysm trial (ISAT) of
neurosurgical clipping versus endovascular coilingin 2143 patients with ruptured intracranialaneurysms: a randomised trial. Lancet 360,1267–1273.
Ljunggren B, Brandt L (1985) Timing of aneurysmsurgery. Clinical Neurosurgery 33, 147–176.
Maraire JN, Awad IA (1995) Intracranial cavernousmalformations: lesion behaviour and managementstrategies (Review). Neurosurgery 37, 591–605.
The International Study of Unruptured Aneurysm Investigators (1998) Unruptured intracranialaneurysms — risk of rupture and risks of surgical in-tervention. New England Journal of Medicine 339 (24),1725–1733.
Weir B (2002) Unruptured intracranial aneurysms; a re-view. Journal of Neurosurgery 96, 3–42.
Weir B, MacDonald MD (1992) Cerebral vasospasm.Clinical Neurosurgery 40, 40–56.
SUBARACHNOID HAEMORRHAGE 139
KAY9 12/16/04 7:42 PM Page 139

Introduction and terminology
Stroke is the third most common cause of death inmost Western countries and the commonestcause of chronic adult disability. In many West-ern countries, there has been an impressive fall inpopulation-based stroke mortality over the pastfew decades, averaging 4–5% each year. This hasbeen chiefly attributed to the more effectiverecognition and treatment of hypertension andother risk factors. Despite this progress, with theincreasing life expectancy of the population, amarked increase in stroke prevalence has beenpredicted. Stroke is generally a disease of ageing,but young adults are also affected, with a some-what different pathogenetic spectrum. The over-all approach to stroke has undergone a dramaticchange in recent years, with important recent ad-vances in prevention strategies, the widespreadintroduction of acute stroke units, the applicationof new imaging technologies and the introduc-tion of thrombolysis for selected patients withacute ischaemic stroke.
The term ‘stroke’ is used to describe a suddenneurological deficit of vascular aetiology last-ing more than 24 hours. A transient ischaemicattack (TIA) indicates a transient neurologicaldeficit of vascular origin lasting less than 24hours, although many patients with TIAs last-ing more than minutes have in fact sufferedsome neuronal damage and this time definitionhas been recently challenged. Stroke is classi-fied as cerebral infarction or ischaemic stroke,signifying ischaemic brain damage, or cerebralhaemorrhage, where the primary pathology in-volves vascular rupture and extravasation of
blood into the surrounding tissues. The term‘haemorrhagic infarction’ is used to describean infarct into which there has been a secondaryextravasation of blood. Although subarach-noid haemorrhage (SAH) may not be associat-ed with a focal neurological deficit, it is usuallycategorized as a stroke subtype. Old and mis-leading terms such as ‘CVA’ (cerebrovascularaccident) and ‘RIND’ (reversible ischaemicneurological deficit) have generally been aban-doned.
Stroke prevention
Stroke prevention involves primary and sec-ondary strategies. Primary prevention includeslifestyle modification and treatment of risk fac-tors in individuals who have not experiencedcerebrovascular symptoms. Risk factor manage-ment can be categorized into the high risk ap-proach (detecting and treating patients at highrisk of stroke, such as those with atrial fibrillationor hypertension) and the mass or population ap-proach (such as reducing salt intake and henceattempting to lower blood pressure in the entirepopulation). These two approaches are comple-mentary, although the population approach hasthe potential of much greater impact on strokerates in society as a whole.
Secondary prevention involves the use ofstrategies in a symptomatic individual after astroke or TIA, generally tailored to the specifictype of cerebrovascular pathology. Most strokeprevention studies have focused on a reductionin the incidence of stroke, neurological disabil-ity and other vascular endpoints. Recently,
CHAPTER 10
10 StrokeStephen M. Davis
140
KAY10 12/16/04 7:42 PM Page 140

prevention of vascular dementia has also beenrecognized as an important additional goal.
Primary prevention
Primary prevention strategies target the modifi-able risk factors for stroke (Table 10.1). In the con-sideration of risk factors and stroke, thepopulation attributable risk is a useful conceptin evaluating the overall importance of a risk fac-tor, combining the relative risk of the individualfactor and its prevalence.
Age and genderIn general, the frequency of stroke increases withadvancing age. Overall, male gender is associat-ed with increased stroke risk. Among older pa-tients there is a slightly higher rate of stroke infemales, but this may simply reflect the greaterlongevity of women.
HypertensionHypertension is the most important risk factorfor both cerebral infarction and haemorrhage.The population attributable risk from hyperten-sion has been estimated as 26%. Many popula-tion studies have demonstrated an increasedfrequency of stroke with both systolic and dias-tolic hypertension. Hypertension is correlatedwith common pathogenetic stroke mechanisms.These include cardiac disease (risk of cerebralembolism), intracerebral small vessel disease(lacunar infarction, intracerebral haemorrhage),extracranial atherosclerosis (thromboem-bolism), development of cerebral aneurysms(subarachnoid haemorrhage) and rupture of
deep perforating vessels (intracerebral haemor-rhage).
A meta-analysis in 1990 showed that modestreduction of systolic blood pressure (BP) re-duces stroke risk by about 40%. This benefit alsoextends to those with mild hypertension. Mostof these earlier trials of antihypertensive agentsinvolved beta-blockers and diuretics, ratherthan the newer agents such as the angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers and calcium channel antagonists. Blockade of the angiotensin recep-tor has theoretical appeal, with potential bene-fits beyond blood pressure reduction. However,there is still uncertainty about the relative bene-fits of different classes of antihypertensiveagents. Some still advocate diuretics as first-lineantihypertensive agents. One study suggestedclass-specific benefits for angiotensin receptorblockade over beta-blockers, but recent meta-analysis shows that the degree of benefit is notrelated to drug class, but rather the extent ofblood pressure reduction.
Atrial fibrillationValvular heart disease has long been recognizedas a cause of cerebral embolism. The decline inthe incidence of rheumatic heart disease, associ-ated with a 17-fold increase in stroke risk in thosewith atrial fibrillation, may have contributed tothe reduction in population-based stroke mortal-ity. Non-valvular atrial fibrillation (NVAF) isnow the most common cause of cardiogenic cere-bral infarction in Western countries, associatedwith a 6–8 times increase in stroke risk. NVAF isage-related, affecting approximately 1.7% of the
STROKE 141
Table 10.1 Modifiable risk factors for ischaemic stroke.
Risk factor Relative risk of stroke Benefits proven
Smoking 1.0–4.0 YesHypertension 2.0–4.0 YesDiabetes 2.0–8.0 YesHeart disease (particularly atrial fibrillation) 6.0–8.0 YesHypercholesterolaemia 1.0–2.0 Yes
KAY10 12/16/04 7:42 PM Page 141

142 CHAPTER 10
population aged 60 years and rising to 11% inthose older than 75 years.
Clinical trials have demonstrated a relativerisk reduction of about 70% in the stroke rate inpatients with NVAF without prior cerebrovascu-lar symptoms, treated with warfarin. In compli-ant patients, there are low risks of majorhaemorrhagic complications with careful moni-toring, with approximately a 1% major haemor-rhage rate per year, aiming at an internationalnormalized ratio (INR) in the 2–3 range. There isa modest benefit with aspirin, but it is only abouthalf as effective as warfarin. Aspirin is generallyused when patients are not candidates for antico-agulation, and in those under the age of 60 yearswith atrial fibrillation, but without risk factors orechocardiographic features of structural heartdisease (termed ‘lone atrial fibrillation’). War-farin is often combined with aspirin to conveyadditional benefit in patients with prostheticheart valves and atrial fibrillation or prior throm-bo-embolism.
DiabetesDiabetes mellitus is associated with a two- tofivefold increase in the rate of stroke. This is dueto both accelerated atherogenesis in the extracra-nial and intracranial arteries (macrovascular dis-ease) and the development of small vessel,lacunar infarcts (microvascular disease). Theprognosis of acute stroke in diabetic and otherhyperglycaemic patients is worse than in thosewith normal blood sugar levels, probably due tothe production of excessive lactate and increasedtissue damage. Optimal control of blood glucoseis likely to reduce the vascular complications ofdiabetes.
SmokingSmoking is an important risk factor for stroke,particularly ischaemic stroke and subarachnoidhaemorrhage. It at least doubles stroke risk inboth men and women. Like diabetes, smokingaccelerates atherogenesis and has intravasculareffects on platelet adhesion and viscosity. The in-travascular effects appear to be particularly im-portant, evidenced by a substantial reduction ofstroke risk within 2–4 years of smoking cessa-
tion. Chronic smoking also lowers cerebral bloodflow.
HypercholesterolaemiaHyperlipidaemia, and in particular hypercholes-terolaemia, is a much weaker risk factor forstroke than ischaemic heart disease in epidemio-logical studies. However, trials of the HMG-CoAreductase inhibitors (statins), which produce po-tent cholesterol reduction, have been shown inhigh-risk patients (generally with ischaemicheart disease) and cholesterol ranging from nor-mal to high levels, to markedly reduce the risk ofstroke. The efficacy of these drugs may also re-flect other pharmacological actions, including ef-fects on the endothelium and atheroscleroticplaque.
Heavy alcohol useHeavy alcohol usage is associated with an in-creased risk of both ischaemic and haemorrhagicstroke, particularly subarachnoid haemorrhage.In contrast, some studies have suggested that lowto moderate alcohol intake is stroke-protective.
Miscellaneous factorsPolycythaemia is an important and treatable riskfactor for cerebral infarction. Leisure-time physi-cal activity has been linked with reduced risk ofischaemic stroke. There has been interest in thetherapeutic role of vitamins such as folic acid andB6, given epidemiological links between homo-cystinaemia and stroke, but further trial resultsare awaited.
Asymptomatic carotid diseaseCarotid bruits occur in at least 4% of asympto-matic adults over the age of 40 years, of whichonly a proportion are due to severe internalcarotid stenosis. There have been a number ofrandomized controlled trials to determinewhether carotid endarterectomy (CEA) is indi-cated in patients with severe but asymptomaticcarotid stenosis (Fig. 10.1). The most definitive ofthese indicated that there was an 11% stroke ratein the hemisphere ipsilateral to a 60% or greatercarotid stenosis, reduced significantly to 5% byCEA in good surgical hands. However, this study
KAY10 12/16/04 7:42 PM Page 142

indications for carotid endarterectomy and theintroduction of cerebral angioplasty/stenting.
Antiplatelet strategiesThe benefits of aspirin were established by pivotal studies more than 25 years ago, with a relative risk reduction of about 22% for the com-posite outcomes of stroke, death or myocardialinfarction. Meta-analysis of the 10 secondary pre-vention trials where aspirin was tested againstplacebo in secondary stroke prevention showedno discernible difference between high, mediumand low doses of aspirin. The consensus amongststroke clinicians today is that doses in the ‘low’50–325 mg range are preferred, given that bleed-ing risk is lower than the high-dose regimens.
The effectiveness of aspirin depends on the in-hibition of platelet cyclo-oxygenase, but other an-tiplatelet strategies with differing actions havealso been proven in stroke prevention. Unlike as-pirin, clopidogrel inhibits platelet ADP. It wasshown in the CAPRIE trial to be more effectivethan aspirin in overall vascular protection inhigh-risk patients, with a relative risk reductionof 8.7% for clopidogrel over aspirin. If one as-sumes about a one-quarter reduction of all vascu-lar events in high-risk patients with aspirin, thiscan be improved to approximately one-thirdwith clopidogrel. However, because of the smallabsolute risk reduction (approximately 0.5% peryear) and the cost of the drug, clopidogrel tendsto be used as second-line therapy in patients whoare either intolerant of aspirin or are aspirin fail-ures. Clopidogrel and aspirin have an additive or synergistic effect because of their different actions. This combination approach has beenproven in acute coronary syndromes and is cur-rently being tested in patients with prior TIA orstroke.
Dipyridamole reduces platelet aggregation byraising the antiaggregating effects of cyclic AMPand cyclic GMP. A synergistic effect between as-pirin and dipyridamole was demonstrated in theESPS 2 trial. The relative stroke risk was reduced by 18% with aspirin, 16% with dipyri-damole, and an apparently additive 37% with thecombination of the two therapies. This combina-tion antiplatelet approach is also widely used.
STROKE 143
Fig. 10.1 Arterial digital subtraction angiogramdemonstrating severe, proximal internal carotid arterystenosis (arrow).
also confirmed that the natural history of asymp-tomatic carotid stenosis was relatively benign. Alarge number of operations are required in strokeprevention, about 83 to prevent one stroke peryear. The place of CEA for asymptomatic carotidstenosis therefore remains controversial, andshould only be considered in highly selected patients.
Secondary prevention
Secondary prevention strategies after stroke orTIA, unlike the primary prevention techniques,are tailored to the underlying stroke pathology.The range of secondary prevention strategiescontinues to expand (Table 10.2). These includethe introduction of a number of new antiplateletstrategies, proof of the efficacy of warfarin innon-valvular atrial fibrillation, clarification of the
KAY10 12/16/04 7:42 PM Page 143

144 CHAPTER 10
The platelet glycoprotein IIb/IIIa receptor is thefinal common pathway of platelet aggregation.Oral platelet GPIIb/IIIa antagonists prevent the binding of fibrinogen to platelets but haveproved hazardous in patients with coronary orcerebrovascular disease and have now beenabandoned.
WarfarinThe European Atrial Fibrillation trial comparedwarfarin, aspirin and placebo in secondarystroke prevention. Warfarin was substantiallymore effective than aspirin and is the recom-mended strategy in anticoagulation candidates.However, warfarin is not superior to aspirin in patients with symptomatic cerebral atherosclerosis.
Carotid endarterectomyTwo large trials (the North American Sympto-matic Carotid Endarterectomy Trial — NASCETand the European Carotid Surgery Trial — ECST)showed major benefits for carotid endarterecto-my over optimal medical therapy in patientswith greater than 70% carotid stenosis and ei-ther TIA or non-disabling stroke. In theNASCET study, an absolute risk reduction of17% over 18 months was achieved, indicatingthat one stroke could be prevented for every sixpatients.
Cerebrovascular angioplasty/stentingPercutaneous transluminal angioplasty is in-creasingly used for symptomatic and asympto-matic carotid stenosis, usually combined with
Table 10.2 Therapeutic opportunities in secondary prevention.
Strategy Indication Level of evidence
Antiplatelet and anticoagulant strategiesAspirin IClopidogrel IIDipyrimadole IICombination antiplatelet strategies II (combined aspirin/
dipyrimadole)Glycoprotein IIb/IIIa inhibitors Discarded IWarfarin Non-valvular atrial fibrillation, valvular I
heart disease
Surgical and interventional strategiesCarotid endarterectomy Symptomatic carotid stenosis (< 70%) I
Asymptomatic carotid stenosis IIAngioplasty/stenting Not yet proven; possible role in patients with III
extracranial, intracranial symptomatic atherosclerotic stenosis
No randomized, controlled trials to date confirming benefits
Quality of evidence ratingsLevel I: Evidence is obtained from a systematic review of all relevant randomized controlled trials.Level II: Evidence is obtained from at least one properly designed randomized controlled trial.Level III: Evidence is obtained from well-designed controlled trials without randomization; from well-designed cohort or case–control analytical studies.Level IV: Opinions of respected authorities, based on clinical experience, descriptive studies or reports ofexpert committees.
KAY10 12/16/04 7:42 PM Page 144

endovascular stenting. However, there is limitedproof of efficacy and safety compared with en-darterectomy. One trial showed that the benefitsand risks of surgery and angioplasty/stentingwere approximately equivalent. Large trials arenow being conducted in patients with sympto-matic carotid stenosis, comparing stenting withendarterectomy. Distal protection devices, whichtrap embolic debris at the time of the procedure,represent an important advance. Stenting hasalso been used in small series of patients withsymptomatic intracranial stenoses, in whom optimal medical therapy has failed.
Acute stroke
It is estimated that approximately 20 millionstrokes occur around the world each year, with 5million deaths. Many stroke patients are left with significant neurological disability that canthreaten their independence, ability to work and quality of life. Better acute stroke treatmentsare improving this dismal picture.
The spectrum of transient ischaemic attacks and stroke
Transient ischaemic attacks (TIAs) and com-pleted cerebral infarcts are caused by similarpathological mechanisms, most commonly largevessel atherosclerotic disease, cardioembolismand small vessel lacunar disease. Patients withTIAs and completed infarcts, whether large orsmall, have a similar prognosis, with a 5–10-foldannual increase in stroke risk. Both conditionsshould be regarded as medical emergencies.
While TIAs by convention last less than24 hours, most last only minutes. The majority ofTIAs lasting more than 1–2 hours produce tissuedamage on sensitive brain imaging techniques,such as magnetic resonance imaging. The old 24-hour definition is therefore increasingly criti-cized and is not clinically useful. The recognitionof patients with minor ischaemic deficits presentsa vital opportunity for prevention of majorstroke. Patients with TIAs should be urgentlyevaluated within 24 hours of the episode. Investi-gations would typically include a CT or MR scan
to detect infarction or non-vascular pathology,carotid duplex Doppler to diagnose majorcarotid disease, and ECG, sometimes followed byechocardiography, to diagnose atrial fibrillationor another cardioembolic source.
Carotid-territory TIAs
These are due to transient ischaemia in the retinaor cerebral hemisphere. Transient monocularblindness (‘amaurosis fugax’) is due to a tran-sient reduction in retinal perfusion produced byembolism or haemodynamic failure. The patientoften describes a shade pulled down over oneeye. In clinical practice it is vital to determinewhether a visual disturbance is truly monocular,indicating retinal ischaemia, or binocular, oftenimplicating the vertebrobasilar circulation.Hemispheric symptoms most commonly consistof transient dysphasia and varying degrees ofhemiparesis or hemisensory disturbance, eithersingly or in combination.
Vertebrobasilar TIAs
These are often more complex than carotid terri-tory events and usually include two or more ofthe following symptoms:• binocular visual disturbance• vertigo• diplopia• ataxia• bilateral weakness or paraesthesiae• deafness• tinnitus• amnesia.
These symptoms are produced by transient is-chaemia of the brainstem, occipital and medicaltemporal lobes and upper spinal cord.
Classification and pathogenesis of stroke
Cerebral infarction (ischaemic stroke)
Cerebral infarction accounts for approximately80% of stroke patients and may be classified ac-cording to anatomical location or pathogenesis. It
STROKE 145
KAY10 12/16/04 7:42 PM Page 145

146 CHAPTER 10
is useful to incorporate both classifications whenconsidering stroke in a particular patient.
Anatomical classification (Table 10.3)The anatomical location refers to the specific arterial territory (e.g. internal carotid vs. verte-brobasilar, anterior cerebral vs. middle cerebral)or specific location within the brain (e.g. lateralmedullary syndrome, ventral pontine infarctionor internal capsular infarction). Infarction mostcommonly occurs in the middle cerebral arterialterritory and can be classified as cortical or deep(subcortical). The cortical middle cerebral syn-dromes depend on whether a small branch hasbeen occluded, or whether one or both of themain two divisions of the middle cerebral arteryis involved, the superior or inferior division.
Subcortical infarcts occur in the territory of thedeep perforating vessels supplying the internalcapsule, thalamus, basal ganglia and brainstem.
The occlusion of a single perforating vesselproduces a small deep infarct, less than 1.5 cm indiameter, called a lacunar infarct, particularly ifassociated with one of the five classical clinical
syndromes (see below). The obstruction of theorigins of several of the deep perforating branches can produce a larger subcortical infarcttermed a striatocapsular infarct.
Pathogenetic classificationGreater emphasis is now placed on the pathogen-esis of cerebral infarction, as this is useful for theselection of secondary prevention therapies. Thisclassification is often referred to as the TOASTsystem, after the TOAST trial.1 Large artery atherosclerosis.2 Cardiogenic embolism.3 Lacunar infarction.4 Rare causes (e.g. dissection, vasculitis, pro-thrombotic states).5 Unclassified:
• despite adequate investigation• due to inadequate investigation.
Large artery atherosclerosis (Figs 10.1–10.3)The development of extracranial atheroscleroticplaque produces a progressive arterial stenosis.Subsequent plaque complications include ulcera-
Table 10.3 Anatomical stroke syndromes.
Arterial territory Stroke syndrome
Internal carotid artery May be asymptomatic. Mixture of middle and anterior cerebral artery syndromes
Middle cerebral artery occlusion Contralateral hemiplegia (arm often more affected than leg), hemianaesthesia, homonymous hemianopia, aphasia, inattention, cortical sensory loss
Anterior cerebral artery occlusion Hemiparesis, chiefly in the leg
Posterior cerebral occlusion Homonymous hemianopia, disconnection syndromes, hemianaesthesia, amnesia, midbrain and thalamic syndromes
Vertebrobasilar thrombosis (basilar Quadriparesis, bulbar paralysis, impaired gaze, cortical blindness, occlusion) coma
Ventral pontine infarction Quadriparesis, bulbar paralysis, absent horizontal but retained vertical gaze. Normal conscious state; able to blink to command (‘locked in’ syndrome)
Lateral medullary syndrome Ipsilateral ataxia, Horner’s syndrome, nystagmus, facial numbness, 9th and 10th nerve palsies, contralateral spinothalamic loss
KAY10 12/16/04 7:42 PM Page 146

stenosis and the absence of a cardiac source. An-terior circulation infarcts typically involve thecerebral cortex. Prodromal TIAs in the same arte-rial territory are another pointer.
Cardiogenic embolism (Fig. 10.6)A variety of cardiac diseases affecting the cardiacwalls, valves or chambers can lead to cerebralembolism. These include:• non-valvular atrial fibrillation (the most common)• valvular heart disease• myocardial infarction with ventricular throm-bus formation• post-cardiac surgery (valvular surgery or coro-nary artery bypass grafts)• prosthetic cardiac valves• infective endocarditis• atrial myxoma• cardiomyopathy• septal defect with paradoxical embolism.
Clinical features include delineation of a car-diac source and lack of evidence of large arterydisease. Similarly, the cerebral cortex is usuallyinvolved.
Lacunar infarction (Fig. 10.7)The occlusion of single deep perforating arteriessupplying the internal capsule, basal ganglia orbrainstem can lead to the development of smalllacunar infarcts. These are most commonly theresult of hypertensive disease, which produceslocalized arterial wall pathology, termed lipo-hyalinosis, in these small penetrating arteries, orlocalized microatheroma. Lacunar infarcts are
STROKE 147
Fig. 10.2 Carotid ultrasound of the carotid bifurcation,demonstrating an ulcerated stenotic plaque (arrows) atthe common carotid bifurcation.
Fig. 10.3 Diffusion-weightedimaging scan (left image)showing large acute middlecerebral artery (MCA) corticalinfarct. Magnetic resonanceangiography (right image)shows lack of flow in the leftMCA.
tion, intraplaque haemorrhage and superim-posed platelet–fibrin thrombus formation. Stroke is most often due to the development ofthrombus (Fig. 10.4) followed by propagationand distal thromboembolism into the intracra-nial vessels, sometimes embolism composed ofatheromatous debris, or haemodynamic failuredue to the reduction of cerebral perfusion in thearterial border zones (borderzone or watershedinfarction). Primary intracranial atherosclerosisand atherothrombosis is rare in Caucasian popu-lations, but more common in African, African-American and Asian stroke patients (Fig. 10.5).
Clinical features include demonstration of rel-evant arterial pathology with 50% or greater
KAY10 12/16/04 7:42 PM Page 147

148 CHAPTER 10
less often due to embolism from a proximalsource such as extracranial atherosclerosis or in-tracardiac thrombus.
Classical lacunar syndromes include puremotor hemiparesis, pure sensory stroke, sensori-motor stroke, ataxic hemiparesis and thedysarthria/clumsy hand syndrome. Clinicalpointers include clinical diagnosis of one of theclassical syndromes, usually exclusion of a largeartery or cardiac source and ideally neuroimag-ing confirmation of a small, deep infarct.
Oxfordshire classificationAnother commonly used stroke classification,termed the Oxfordshire classification, dividesischaemic stroke into TACI (total anterior circula-tion infarction) (Fig. 10.8), PACI (partial anteriorcirculation infarction), POCI (posterior circula-tion infarction) and LACI (lacunar infarction).
Fig. 10.4 Internal carotid atherothrombosis fromautopsy specimen.
Fig. 10.5 Magnetic resonance angiographydemonstrating severe distal vertebral/proximalbasilar artery stenosis (arrow).
Fig. 10.6 Echocardiogram demonstrating clot (CL) inleft ventricle (LV).
Fig. 10.7 Diffusion-weighted imaging scan showingacute left thalamic lacunar infarct (hyperintenselesion).
KAY10 12/16/04 7:42 PM Page 148

This classification is also useful and the subtypescorrelate with prognosis.
Cerebral haemorrhage (haemorrhagic stroke)
Cerebral haemorrhage is generally classified intointracerebral and subarachnoid haemorrhage.
Intracerebral haemorrhage (Figs 10.9–10.11)Non-traumatic (primary) intracerebral haemor-rhage is most commonly due to hypertension,which leads to rupture of deep perforating arter-ies in the putamen, thalamus, central white matter, brainstem and cerebellum. The precisemechanism of this vascular rupture is uncertain,but may be related to the development of smallCharcot–Bouchard microaneurysms on the ves-sel walls of these end-arteries, or direct rupture ofvessels affected by lipohyalinosis.
‘Lobar’ haemorrhage refers to superficial vascu-lar rupture within the cerebral lobes, outside thesedeep arterial territories. It is sometimes due to anunderlying structural lesion, such as an arteriove-nous malformation, cerebral aneurysm, tumour,vasculopathies or coagulation disorders. Amyloid
STROKE 149
Fig. 10.8 CT scan showing severe left middle cerebralcortical infarction. Note sparing of anterior andposterior cerebral arterial territories.
Fig. 10.9 CT scan showing hypertensive putaminalhaemorrhage.
Fig. 10.10 CT scan showing frontal and occipital lobarhaemorrhages in a patient with amyloid angiopathy.
KAY10 12/16/04 7:42 PM Page 149

150 CHAPTER 10
angiopathy is an important cause of lobar cerebralhaemorrhage in elderly patients and is due toamyloid deposition in the walls of the cerebral ar-teries. These haemorrhages may be multiple andtypically occur in patients who are normotensiveand may show features of Alzheimer’s disease.
Clinical clues to ICH include the features of asudden rise in intracranial pressure with de-pressed conscious state, headache and vomiting.The mortality is much higher than in ischaemicstroke. However, patients with ICH may be sur-prisingly alert and well looking. Conversely, pa-tients with ischaemic stroke may have earlydepression of conscious state. Hence, neuroimag-ing, usually with CT, is mandatory in all cases torapidly diagnose ICH.
Subarachnoid haemorrhage (see Chapter 9)Subarachnoid haemorrhage is classified accord-ing to pathological cause and site. The two mostimportant identifiable causes include rupture ofa berry aneurysm and arteriovenous malforma-tion, but in up to 15% of cases no bleeding can be
identified at angiography. Some of these idio-pathic bleeds are due to perimesencephalichaemorrhage.
Modern principles of acute stroke management
In Australia, the USA and Europe, guidelines foracute stroke management have been developed,based on the evidence from large controlled clin-ical trials. Key principles of acute stroke manage-ment include:1 Urgent recognition of stroke symptoms by thepatient or their carer.2 Urgent ambulance transport to a hospital withadequate diagnostic facilities and organizedstroke care.3 Urgent triage and investigation in the emer-gency department including CT brain scanning.4 Assessment for acute stroke therapy, particu-larly thrombolysis.5 Admission to a specialized stroke unit.
Hospital arrival times: ‘Time is Brain’
Delayed hospital arrival times are a worldwideproblem. New therapies such as tPA (see below)are time-dependent. In many centres, only aquarter of stroke patients arrive within 3 hours.Much of this delay is due to public ignorance andconfusion about the nature of stroke and the needfor urgent evaluation and treatment. However,professional nihilism is another barrier.
Clinical assessment of stroke
The following questions should be considered inthe management of any patient with a presumedstroke.• Is it a stroke?• Is it an infarct or haemorrhage?• Is the patient eligible for thrombolytic therapyor other urgent intervention?• What is the arterial or anatomical localizationand pathogenesis?
Stroke and pseudostrokeNon-vascular pathologies (‘pseudostroke’) such
Fig. 10.11 CT scan showing right cerebellarhaemorrhage. The brainstem and 4th ventricle arecompressed.
KAY10 12/16/04 7:42 PM Page 150

as cerebral tumour, subdural haematoma, ab-scess, migraine, metabolic disturbances andepilepsy can mimic the stroke process. All pa-tients with suspected stroke require an urgent CTor MR scan to exclude non-cerebrovascular dis-orders, as well as to differentiate between infarctand haemorrhage (Figs 10.8 and 10.9). Lumbarpuncture is reserved for those cases wheremeningitis is considered (usually after a CT scan)or where the diagnosis of subarachnoid haemor-rhage is still contemplated after a normal CTscan.
The distinction between infarct andhaemorrhageThe distinction between cerebral haemorrhageand infarction is vital, as some haemorrhages areconsidered for surgical evacuation, while pa-tients with ischaemic stroke may be consideredfor thrombolysis or anticoagulation. While thereare clinical pointers (see above) this differentia-tion is usually based on CT scan findings. Al-though CT scanning remains the workhorse foracute stroke assessment, recent studies indicatethat MRI is at least as sensitive for intracerebralhaemorrhage as CT and far more sensitive foracute ischaemia. Patients with ischaemic strokeoften have early infarct changes on CT, althoughthese may be subtle. MRI with diffusion-weighted imaging (DWI) is increasingly used asthis technique allows a sensitive diagnosis ofcerebral ischaemia (Figs 10.3 and 10.7).
Is the patient eligible for thrombolysis?The thrombolytic agent tissue plasminogen acti-vator (tPA) has now been licensed in most partsof the world as the first proven stroke drug thera-py, given intravenously within 3 hours of strokeonset in selected patients with ischaemic stroke.The approval of this acute therapy followed thepositive results of a two-part pivotal trial, con-ducted in the USA. Other European trials testingtPA up to 6 hours have shown a marked trend tobenefit over risk, and meta-analysis confirms the3-hour window for tPA. Use of tPA increases therisk of symptomatic haemorrhagic complicationsby three- to fourfold. Major early infarct changeson CT, for example greater than one-third of the
area of the middle cerebral artery, are associatedwith a higher risk of haemorrhagic transforma-tion. Up to 10% of ischaemic stroke patients canbe treated in well-organized centres. In contrastto the tPA trials, three trials evaluating the role ofintravenous streptokinase produced negative re-sults, chiefly linked to the substantial risk of intracerebral haemorrhage associated with thedrug.
Direct infusion of thrombolytics via intra-arte-rial catheters has been shown to be effective inone trial up to 6 hours after middle cerebralartery occlusion. There is interest in experimentalmechanical devices which can break up thrombi,with a much lower risk of cerebral haemorrhage.
Location and pathogenesis of infarctionCortical infarcts (Fig. 10.3). Based on the clinicalexamination, a distinction should be made between an infarction in the carotid or in the vertebrobasilar territory. With regard to carotidterritory infarction, the presence or absence ofcortical signs — dysphasia, apraxia, anosognosia(unawareness or denial of the stroke), sensory,motor or visual agnosia (inattention), acalculia,right/left confusion, dysgraphia or cortical sen-sory loss (loss of two-point discrimination, astereognosis, dysgraphaesthesia) — suggests anembolic source from either the extracranial ves-sels or the heart, rather than lacunar infarction.
Subcortical infarcts (Fig. 10.7). As indicated ear-lier, lacunar infarcts (less than 1.5 cm in diameter)rely on diagnosis of one of the classical lacunarsyndromes. Cortical signs are not present. Lacu-nar syndromes reflect small vessel occlusions inthe internal capsule, thalamus and brainstem.
HaemorrhageIntracerebral haemorrhage (Fig. 10.9). As previous-ly discussed, the rapid onset of a stroke withearly depression of conscious state favours thediagnosis of a primary intracerebral haemor-rhage. Primary intracerebral haemorrhage andaneurysmal subarachnoid haemorrhage canoverlap in their clinical presentations. For exam-ple, a berry aneurysm can rupture primarily intothe brain parenchyma, presenting as an intra-cerebral haemorrhage, whereas a primary brain
STROKE 151
KAY10 12/16/04 7:42 PM Page 151

152 CHAPTER 10
haemorrhage can rupture directly into the ven-tricular system and present with markedmeningeal features due to subarachnoid blood.
For subarachnoid haemorrhage see Chapter 9.
Urgent assessment in the emergencydepartment
Rapid triage of suspected stroke patients shouldbe performed in an emergency department, withskilled medical evaluation and urgent investiga-tions. These involve blood tests, including ablood glucose measurement to exclude hypogly-caemia (which can mimic acute stroke), and anECG to diagnose atrial fibrillation or acute my-ocardial infarction, which can reveal the cause ofcerebral embolism. Most importantly, a CT brainscan must be performed urgently in all patientsto differentiate between cerebral infarction andcerebral haemorrhage. In addition, CT scanningis essential to exclude the other brain pathologiesthat can simulate stroke. As noted above, manycentres are now using acute MRI with DWI andmagnetic resonance angiography (MRA). Com-puted tomographic angiography (CTA) is another useful tool. Duplex Doppler scanning isof value in the diagnosis of large vessel athero-sclerosis, while echocardiography (usually lessurgent) can aid in the diagnosis of intracardiacthrombi and valvular or cardiac wall kinetic ab-normalities. Transoesophageal echocardiographyis superior to transthoracic echocardiography.
Acute stroke units
One of the most important developments inacute stroke management in recent years hasbeen the proven value of stroke units, based onthe results of clinical trials which have comparedorganized expert care in a special unit to the man-agement of patients in general medical wards.The usual stroke unit model involves a geo-graphical area in the hospital, incorporating askilled multidisciplinary stroke team, led by aneurologist or other physician with expertise instroke management. Vascular surgeons and neu-rosurgeons should be readily available for con-sultation and intervention in selected cases. In a
systematic overview of the benefits of strokeunits, it was shown that mortality could be re-duced by about 25%, also with evidence of re-duced disability. In addition, stroke units havebeen found to reduce bed stay and hence hospitalcosts.
The components of team management in thestroke unit include:1 Acute medical, surgical and nursing care.2 Diagnosis of the pathological mechanism ofthe stroke and the institution of tailored sec-ondary prevention strategies.3 Prevention, early detection and treatment ofcomplications such as aspiration pneumonia,pressure sores, hyperglycaemia, seizures andsepsis.4 Use of measurement instruments and strokeregisters.5 Early integrated neurorehabilitation with eval-uation of premorbid status and therapy goals.6 Involvement, education, and support for pa-tient and family.7 Early, coordinated discharge planning.
Acute medical care
Three key, evidence-based advances include theuse of tPA, aspirin (see below) and stroke unitcare. In the acute phase, close monitoring of vitaland neurological signs is paramount, given thatabout a third of stroke patients deteriorate afteradmission to hospital. Cardiac monitoring isuseful for many acute stroke patients. Initial clin-ical evaluation should involve assessment of thepatient’s function and clinical state before thestroke, the stroke type and pathogenesis, docu-mentation of the nature and severity of neuro-logical deficits, and comorbid diseases. Earlymobilization, range of motion exercises forhemiplegic limbs, frequent turning, fluid andnutritional maintenance, dysphasia manage-ment, avoidance of aspiration, prevention ofdeep venous thrombosis (DVT) and pneumonia,management of incontinence, treatment of uri-nary tract infections and other causes of fever,and maintenance of skin integrity are all keyplanks in the team treatment of the acute strokepatient.
KAY10 12/16/04 7:42 PM Page 152

Patients should have oximetry, but there is noevidence of the value of routine supplementaloxygen by mask or nasal prongs. Patients shouldbe well hydrated using normal saline rather thanglucose-containing solutions, because of the haz-ards of even mild degrees of hyperglycaemia. Ingeneral, blood pressure should not be acutelylowered, because this can compromise cerebralperfusion in acute stroke. Hypertension is usualin acute stroke and this usually settles sponta-neously over 2–3 days. We routinely use com-pression stockings and usually low-doseheparin, or low molecular weight heparin or he-parinoid, in DVT prophylaxis. Airway assess-ment should be an urgent priority to avoidaspiration pneumonia. We generally use naso-gastric feeding after 24–48 hours if the patient’sbulbar function is compromised.
Adverse prognostic factors include advancingage, depression of conscious state, severity ofneurological deficit, conjugate gaze palsy andearly urinary incontinence. Causes of mortalityin stroke patients are predominantly neurologi-cal (transtentorial herniation) in the 1st week,and due to secondary systemic factors in the 2ndand 3rd weeks such as pneumonia, pulmonaryembolism and cardiac causes.
Progressing stroke
A deteriorating neurological deficit is seen inabout one-third of stroke patients. Cerebral oede-ma, with progressive elevation of intracranialpressure, is an important cause of death. Howev-er, this oedema is generally cytotoxic and clinicaltrials have demonstrated that corticosteroids areof no value in either cerebral infarction or haem-orrhage. Intravenous mannitol and glycerol aresometimes empirically used, but their value hasnot been proven. In highly selected young pa-tients with severe, early brain oedema, surgicaldecompression with hemicraniectomy should beconsidered.
Heparin
Heparin has been the most widely used un-proven therapy in most countries. The Interna-
tional Stroke Trial (IST) evaluated unmoni-tored, subcutaneous heparin up to 48 hoursafter stroke onset and showed that a slight re-duction in recurrent stroke was offset by an in-creased risk of haemorrhagic transformation.The rate of early, recurrent embolism in patientswith atrial fibrillation was much lower in recenttrials than in a number of earlier clinical studies.
Systematic overview of the available evidenceleads to the conclusion that heparin is not generally indicated for most patients with acuteischaemic stroke, but heparin should be considered for selected patients with non-disabling ischaemic stroke and a very high risk of recurrent embolism.
Acute aspirin
Two large trials (the International Stroke Trialand the Chinese Acute Stroke Trial) both showedthat, as for acute myocardial infarction, aspirinadministered within 48 hours of stroke onset pro-duced a modest improvement in outcomes at 6months. Hence, aspirin should be used routinelyin acute ischaemic stroke, unless thrombolysis isbeing used.
Neuroprotective therapies
A complex cascade of biochemical changes oc-curs in stroke, secondary to the initial ischaemia.Ischaemic brain injury is associated with ele-vated levels of the excitatory neurotransmittersglutamate and aspartate. These lead to exces-sive stimulation of the N-methyl D-aspartate(NMDA) receptor on the cell surface. This activa-tion is followed initially by an influx of sodiumand water into the cells and secondly by a suddenrise in intracellular calcium. A range of neuropro-tective compounds has been designed to inhibitvarious points in the excitotoxic cascade. Theseinclude calcium channel and NMDAantagonists,glutamate release inhibitors, glycine antagonists,free radical scavengers, inhibitors of the neu-trophil influx into the ischaemic region and vari-ous growth factors. To date, none of thesecompounds have proven effective in adequately
STROKE 153
KAY10 12/16/04 7:42 PM Page 153

154 CHAPTER 10
powered, Phase III clinical trials, but there areseveral ongoing studies. Other approaches in-clude the combination of thrombolysis with neu-roprotective drugs.
Cerebral hemorrhage
While routine surgical evacuation of haematomais unproven, we consider evacuation in selectedpatients with cerebral haemorrhage, particularlyin the cerebellum, as well as younger patientswith lobar haemorrhage. The general principlesof acute stroke management apply equally to in-tracerebral haemorrhage as to infarction.
Prevention of recurrent stroke —secondarystroke prevention
Patients with symptomatic high-grade carotidstenosis should be considered for subacutecarotid endarterectomy. While surgery is awaited, or if endarterectomy is inappropriate,antiplatelet therapy should be instituted. In cardioembolic stroke, there is uncertainty as tothe optimal timing of anticoagulation, particu-larly in patients with atrial fibrillation. Our ap-proach is to employ heparin acutely if the patienthas a mild deficit and there is a high risk of recur-rent embolism. Many patients with atrial fibrilla-tion are commenced on warfarin 7–10 days afteronset, without prior heparin, because of the riskof haemorrhagic transformation. Lacunar in-farcts are less commonly embolic and generallyhave a good prognosis.
Post-stroke rehabilitation
While beyond the scope of this review, rehabilita-tion after stroke is of immense importance. Manymodels of care have been developed, includinghome-based care as well as the more common in-patient and outpatient models. Increasingly,comparative trials of different therapeutic proto-cols are being conducted to provide a more ratio-nal evidence-based approach to post-strokerehabilitation. In optimal stroke care, the rehabil-itation team should be integrated into the acutestroke unit.
Young adult and rarer causes of stroke
Stroke in young adults is due to a wide spectrumof causes. Those presenting with cerebral haem-orrhage usually have an underlying lesion suchas an aneurysm or vascular malformation. Pa-tients presenting with cerebral infarction have arange of pathologies somewhat different to thosein older age groups, including:• migraine• oral contraceptive pill• mitral valve prolapse• cerebral vasculitis• extracranial arterial dissection• fibromuscular dysplasia• moya-moya disease• hypercoagulability states.
Consequently, these patients require more in-tensive investigation than many older stroke pa-tients. Some form of cerebral angiography andtransoesophageal echocardiography are virtual-ly mandatory in all cases. Many patients will alsorequire a lumbar puncture, to look for evidenceof an underlying inflammatory condition, anddetailed haematological investigations directedat diagnosis of a hypercoagulability state.
Migraine
Migraine is a well-recognized cause of stroke inyoung adults, but the precise mechanism of in-farction is unclear. Although vasospasm is usually postulated, it has only rarely beendemonstrated on cerebral angiography in pa-tients with migraine and stroke. The diagnosis ofmigraine as the cause of infarction should only bemade in a migraineur who has a persisting neu-rological deficit, in the wake of a classical attack,and where other causes have been excluded bydetailed investigations, including angiographyand echocardiography.
Oral contraceptive pill
Oral contraceptive agents, particularly the high-er-dosage oestrogen-containing forms whichcan increase blood coagulability, have beenlinked with stroke. However, the relative risk of
KAY10 12/16/04 7:42 PM Page 154

the oral contraceptive pill is probably very small,and should not be assumed to be the cause of ayoung adult stroke without exclusion of othercauses.
Cardiac causes
Mitral valve prolapse is a common echocardio-graphic finding in young women, but also fig-ures prominently in clinical series of young adultstroke patients. Another cardiac embolic sourcein young adults is patent foramen ovale (PFO)with paradoxical embolism from the venous cir-culation. The investigation of young adult strokepatients with transoesophageal echocardio-graphy (TOE) not infrequently shows PFO at ahigher rate than those seen in a control popula-tion, but their precise significance and therapeu-tic implications are often uncertain. There is anincreased risk when PFO is associated with atri-al septal aneurysm. There are current trials eval-uating endovascular devices to close these lesions.
Cerebral vasculitis
Cerebral vasculitis used to be commonly seen inpatients with an underlying basal meningitis dueto tuberculosis or syphilis but it is now seenmainly with aseptic, inflammatory conditions.These include multisystem disorders such as polyarteritis nodosa. Isolated central angiitis(granulomatous angiitis) is an aseptic vasculitisassociated with multifocal cerebral infarcts and ahigh mortality. The cause is unknown. As withthe other types of intracranial arteritis, some pa-tients have ‘beading’ of arteries on angiography,an excess of cerebrospinal fluid lymphocytes andan elevated erythrocyte sedimentation rate. De-finitive diagnosis often depends on brain biopsy,but a negative biopsy does not exclude the condi-tion. High-dose steroids are used, sometimes incombination with other immunosuppressiveagents, particularly cyclophosphamide.
Cerebral arteritis can also be caused by illicitdrug use with heroin, oral or intravenous am-phetamines, cocaine and other agents. Giant cellarteritis (temporal arteritis) is seen in older pa-
tients with extracranial artery inflammation,headache, systemic symptoms and an elevatederythrocyte sedimentation rate. The chief compli-cation is ischaemic optic neuropathy due to in-farction of the optic nerve, but cerebral infarctionoccasionally occurs due to involvement of thevertebral arteries. Ophthalmic herpes zoster canbe followed by middle cerebral arteritis and infarction.
Dissection of the extracranial and intracranial arteries
Dissections are often due to trauma, although thepreceding injury may be extremely mild. Recog-nized causes include motor car accidents withtorsional neck or seat belt injuries, and cervicalmanipulation. Spontaneous dissections alsooccur, some of these cases having an underlyingarteriopathy such as fibromuscular dysplasia.Carotid artery dissection may be associated withocular pain and Horner’s syndrome. Neurologi-cal deficits may follow due to intimal thrombussuperimposed on the ruptured lining of theartery and distal thromboembolism. The lateralmedullary syndrome is a common clinical pre-sentation of vertebral artery dissection. Diagno-sis is made by angiography or MRA, whichshows a narrowed or tapered artery, the ‘stringsign’, sometimes with the formation of an arterialaneurysm. MRA may show intramural throm-bus. Anticoagulation is often used to preventsubsequent thromboembolic events. Intracranialarterial dissections are much rarer, and can pre-sent with brain ischaemia or subarachnoid haemorrhage.
Fibromuscular dysplasia
This arteriopathy chiefly affects females andmost commonly involves the distal portions ofthe extracranial carotid artery. It may be associat-ed with renal fibromuscular dysplasia. It is usual-ly asymptomatic, but is associated with anincreased risk of both TIAs and cerebral infarc-tion. There is also an increased risk of subarach-noid haemorrhage due to associated berryaneurysms. The ischaemic events are probably
STROKE 155
KAY10 12/16/04 7:42 PM Page 155

156 CHAPTER 10
due to thromboembolism and occasionally arter-ial dissection. Angiography demonstrates a clas-sic saw tooth appearance. Treatment is usuallyconservative with aspirin.
Moya-moya disease (Fig. 10.12)
Moya-moya disease is a rare obliterative arterialcondition where the terminal internal carotid ar-teries are occluded and there is a fine, telang-iectatic web of anastomotic, intracranial vesselswhich produces the classic angiographic ‘puff ofsmoke’ appearance (Fig. 10.12). The posterior cir-culation is usually spared. It is associated with anincreased risk of either cerebral infarction due tobrain ischaemia or haemorrhage due to ruptureof the abnormal telangiectatic vessels. The causeof the condition is unknown and medical therapyis ineffective. Surgical revascularization proce-dures constitute the mainstay of therapy.
Hypercoagulability states
Disorders of blood haemostasis and coagulationare sometimes recognized as the cause of strokein young adults. Various rare abnormalities of thecoagulation process have been identified in somestroke patients. These include the presence of thelupus anticoagulant, which is an antiphospho-lipid antibody, activated protein C resistance,and deficiencies of protein S and C.
Cerebral venous thrombosis
Cerebral venous thrombosis is a rare type ofstroke with variable clinical manifestations, butincreasingly recognized with the widespread useof MRI. Septic and aseptic syndromes are recog-nized. Septic thrombosis is now very rare. It mostcommonly involves the cavernous sinus but canalso affect the superior sagittal and lateral sinuses. Sources of infection include the face,paranasal sinuses, middle ear infection and bac-terial meningitis. Aseptic cerebral venous throm-bosis is most commonly seen in conditionsassociated with hypercoagulability states such asthe postpartum period, presence of the lupus an-ticoagulant or the oral contraceptive pill. Clinicalfeatures range from the insidious development ofheadache and papilloedema, to more fulminantfocal syndromes in the cavernous sinus region,hemiplegia, depressed conscious state, fever,seizures, sinus tachycardia and meningismus.(Fig. 10.13). Therapy in septic cases is directedagainst the causative infection. Treatment inaseptic cases involves the use of early anticoagu-lation, which has been shown to improve the outcome. Transdural thrombolysis is also used inselected cases, particularly when the patient’scondition worsens, despite heparin.
Fig. 10.12 Cerebral angiography demonstratingmoya-moya disease. Fig. 10.13 Sagittal MRI scan showing features of
cerebral venous thrombosis, with high signal (arrows)due to blood clot in the superior sagittal sinus.
KAY10 12/16/04 7:42 PM Page 156

Further readingAlbers GW, Caplan LR, Easton JD, Fayad PB, Mohr JP,
Saver JL, Sherman DG; TIA Working Group (2002)Transient ischemic attack — proposal for a new defin-ition. New England Journal of Medicine 347, 1713–1716.
Antiplatelet Trialists Collaboration (1994) Collabora-tive overview of randomised trials of antiplatelettreatment, Part 1. Prevention of death, myocardial in-farction, and stroke by prolonged antiplatelet thera-py in various categories of patients. British MedicalJournal 343, 139–142.
Atrial Fibrillation Investigators (1994) Risk factors forstroke and efficacy of antithrombotic therapy in atri-al fibrillation. Analysis of pooled data from five ran-domized controlled trials. Archives of InternalMedicine 154, 1449–1457.
Blood Pressure Lowering Treatment Trialists’ Collabo-ration (2003) Effects of different blood-pressure-low-ering regimens on major cardiovascular events:results of prospectively designed overviews of ran-domised trials. Lancet 362, 1527–1535.
Bucher HC, Griffith LE, Guyatt GH (1998) Effect ofHMG-CoA reductase inhibitors on stroke. A meta-analysis of randomized controlled trials. Annals of Internal Medicine 128, 89–95.
CAPRIE Steering Committee (1996) A randomised,blinded, trial of clopidogrel vs. aspirin in patients atrisk of ischemic events (CAPRIE). Lancet 348,1329–1339.
CAVATAS Investigators (2001) Endovascular vs. surgi-cal treatment in patients with carotid stenosis in theCarotid and Vertebral Artery Transluminal Angio-plasty Study (CAVATAS): a randomised trial. Lancet357, 1729–1737.
Diener H, Cunha L, Forbes C, Sivenius J et al. (1996) Eu-ropean Stroke Prevention Study 2. Dipyridamole andacetylsalicylic acid in the secondary prevention ofstroke. Journal of Neurological Science 143, 1–13.
European Carotid Surgery Trialists’ Collaborative(ECST) Group (1991) MRC European CarotidSurgery Trial: interim results for symptomatic pa-tients with severe (70–99%) or with mild (0–20%)carotid stenosis. Lancet 337, 1235–1243.
Executive Committee for the Asymptomatic CarotidAtherosclerosis Study (1995) Endarterectomy forasymptomatic carotid artery stenosis. Journal of theAmerican Medical Association 273, 1421–1428.
Furlan A, Higashida R, Wechsler L, Gent M, Rowley H,Kase C, Pessin M, Ahuja A, Callahan F, Clark WM,Silver F, Rivera F (1999) Intra-arterial prourokinasefor acute ischemic stroke. The PROACT II study: arandomized controlled trial. Prolyse in Acute Cere-bral Thromboembolism. Journal of the American Medical Association 282, 2003–2011.
Heart Protection Study Collaborative Group (2002)MRC/BHF heart protection study of cholesterol low-ering with simvastatin in 20536 high risk individuals:a randomized placebo-controlled trial. Lancet 360,7–22.
International Stroke Trial Collaborative Group (1997)The International Stroke Trial (IST): a randomisedtrial of aspirin, subcutaneous heparin, both, or nei-ther among 19 435 patients with acute ischemicstroke. Lancet 349, 1569–1581.
Madden KP, Karanjia PN, Adams HP Jr, Clarke WR(1995) Accuracy of initial stroke subtype diagnosis inthe TOAST study. Trial of ORG 10172 in acute stroketreatment. Neurology 45, 1975–1979.
Mohr JP, Thompson JL, Lazar RM, Levin B, Sacco RL,Furie KL, Kistler JP, Albers GW, Pettigrew LC,Adams HP Jr, Jackson CM, Pullicino P (2001) War-farin-Aspirin Recurrent Stroke Study Group. A com-parison of warfarin and aspirin for the prevention ofrecurrent ischemic stroke. New England Journal ofMedicine 345, 1444–1451.
The National Institute of Neurological Disorders andStroke rt-PA Stroke Study Group (1995) Tissue plas-minogen activator for acute ischemic stroke. NewEngland Journal of Medicine 333, 1581–1587.
North American Symptomatic Carotid EndarterectomyTrial Collaborators (1991) Beneficial effect of carotidendarterectomy in symptomatic patients with highgrade carotid stenosis. New England Journal of Medicine 325, 445–453.
Stroke Unit Trialists’ Collaboration (1997) Collabora-tive systematic review of the randomised trials of or-ganized inpatient (stroke unit) care after stroke.British Medical Journal 314, 1151–1159.
Whisnant JP (1997) Modelling of risk factors for is-chemic stroke: The Wills Lecture. Stroke 28,1840–1844.
Zimmet PZ, Alberti KGMM (1997) The changing face ofmacrovascular disease in non-insulin-dependent di-abetes mellitus: an epidemic in progress. Lancet 350,1–4.
STROKE 157
KAY10 12/16/04 7:42 PM Page 157

There are a number of neurosurgical conditionsthat are developmental in origin and that involvethe cranium, intracranial contents and spinal column. The more important of these will be described in this chapter.
Arachnoid cyst
Arachnoid cysts are benign developmental cyststhat occur along the craniospinal axis.
Bright (after whom Bright’s disease was named)was the first to accurately describe the condition in1831. In 1964 Robinson described a large series ofmiddle cranial fossa arachnoid cysts and errone-ously postulated that the primary defect was agen-esis of the temporal lobe; he later revised his opinionand recognized that the cysts were arachnoid mal-formations. In 1958 Starkman recognized that thecysts were developmental, were ‘intra-arachnoid’in location, and that they resulted from splitting andduplication of the arachnoid membrane.
The cysts contain clear, colourless fluid whichresembles normal cerebrospinal fluid; they occurin characteristic locations.• Sylvian fissure 50%• Cerebellopontine angle 10%• Quadrigeminal 10%• Suprasellar 10%• Vermian 8%• Cerebral convexity 5%• Other 7%
Clinical features
The presenting features depend on the positionof the arachnoid cyst.
Sylvian fissureThe Sylvian fissure is the most common site forarachnoid cysts and symptoms may becomemanifest at any age. There is a marked male predominance. The most common presentingfeatures are:1 Raised intracranial pressure:
(a) headaches(b) nausea(c) vomiting.
2 Seizures.Haemorrhage into the cyst following minor
head injury, although uncommon, will cause a sudden onset of neurological symptoms andsigns due to raised intracranial pressure andcompression of the underlying brain.
However, as with arachnoid cysts in any otherlocation, the cyst may remain asymptomaticthroughout life.
Cerebellopontine angleThe clinical features are similar to those of anacoustic neuroma, with sensorineural hearingloss as the most common initial symptom. Alargecyst may cause minor impairment of 5th nervefunction, with depression of the corneal reflexand, rarely, ataxia due to cerebellar compression.
Suprasellar arachnoid cystsThe majority of cysts in this position present inchildren and adolescents and the clinical mani-festations are due to:• hydrocephalus• visual impairment• endocrine dysfunction.
The hydrocephalus results from protrusion of
CHAPTER 11
11 Developmental abnormalities
158
KAY11 12/16/04 7:43 PM Page 158

the cyst into the 3rd ventricle and occlusion of the foramen of Monro. Visual failure results fromcompression of the optic pathways, as well aslong-standing raised intracranial pressure caus-ing optic atrophy. Endocrine dysfunction may bedue to intrasellar extension of the cyst and com-pression of the pituitary gland, or long-standingpressure on the hypothalamus, and is manifest ashypopituitarism, growth retardation or isosexualprecocious puberty.
Cerebral convexityIn adults arachnoid cysts over the convexity present with seizures, headaches or a progressivehemiparesis. The presenting feature in infantsmay be asymmetrical enlargement of the head.
Convexity and Sylvian fissure cysts slightlypredispose the patient to subdural haematomaformation.
Quadrigeminal cisternThe cysts arising in the supracollicular regionmimic pineal masses and the most common pre-senting symptom is obstructive hydrocephaluswith raised intracranial pressure.
Radiological investigations
The computerized tomography scan or magneticresonance imaging will show the cyst in the characteristic position and the fluid will have the same density as CSF (Figs 11.1 and 11.2). Thebone windows on CT scan or plain skull X-raysmay show remodelling and erosion of adjacentbone. The Sylvian fissure arachnoid cyst is char-acteristically associated with expansion of themiddle cranial fossa, elevation of the lesser wingof the sphenoid, and outward expansion andthinning of the squamous portion of the temporalbone.
The suprasellar arachnoid cyst extending intothe 3rd ventricle and causing hydrocephalus maybe difficult to differentiate from a dilated 3rd ven-tricle due to aqueduct stenosis. MRI, particularlysagittal views, will help to differentiate the conditions.
Treatment
Arachnoid cysts are frequently diagnosed as anincidental finding on CT scan. Surgery is not nec-essary if they are completely asymptomatic, withno distortion or enlargement of the ventricularsystem; the patient should be carefully reviewedat regular intervals.
There are two major surgical procedures forarachnoid cysts.1 Craniotomy, excision of the cyst wall andopening of the membranes to allow drainage intothe basal cisterns.
DEVELOPMENTAL ABNORMALITIES 159
Fig. 11.1 (a) Arachnoid cyst arising in the Sylvianfissure. (b) Suprasellar arachnoid cyst causingobstructive hydrocephalus.
(a)
(b)
KAY11 12/16/04 7:43 PM Page 159

160 CHAPTER 11
2 Shunting of the cyst into the peritoneal cavity.
The type of surgical procedure will depend onthe position of the cyst, the presenting featuresand the surgeon’s preference.
Chiari malformations andsyringomyelia
Chiari malformations and syringomyelia arecomplex developmental malformations with awide spectrum of severity; they may present atany stage of life. The conditions are linked
closely through both their underlying patho-physiology and their clinical presentation.
The Chiari malformation results from abnor-malities at the craniocervical junction involvingthe caudal cerebellum, medulla and upper cervi-cal region. In 1881 and 1885 Chiari reported theanomaly of the cerebellum and medulla oblon-gata and described three types of malformation.The type I malformation consists of caudal dis-placement of the cerebellar tonsils below theforamen magnum into the upper cervical canal.The type II malformation comprises caudal dis-placement of the cerebellar vermis, 4th ventricleand medulla oblongata below the foramen mag-num. This is similar to the case reported byArnold in 1894 and consequently is also knownas the ‘Arnold–Chiari malformation’ (Fig. 11.3).The type III malformation involves caudal dis-placement of the cerebellum and brainstem into ahigh cervical meningocele. Chiari also describeda type IV abnormality, comprising two cases ofhypoplastic cerebellum.
It is usual for Chiari type I malformations topresent clinically in adults and many of the presenting features are related to the common as-sociation of syringomyelia. The Chiari type IImalformation has an even higher incidence of association with syringomyelia and it is almost invariably present in patients withmyelomeningocele. Other frequent associationsare hydrocephalus due to aqueduct stenosis, atre-sia or forking of the aqueduct, fusion of the supe-rior and inferior colliculi on both sides into aFig. 11.2 MRI. Posterior fossa arachnoid cyst.
Medulla(normal position)
Cerebellartonsils
Fourth ventricle (normal position)
Herniatedcerebellarvermis
Medulladisplacedcaudally
Fourth ventricle (displaced caudally)
Type I Chiari Type II Chiari
Fig. 11.3 Major features ofChiari types I and IImalformation.
KAY11 12/16/04 7:43 PM Page 160

single ‘beaked’ structure, and a small and ‘crowd-ed’ posterior fossa. Supratentorial anomalies include enlargement of the massa intermedia, microgyria and heterotopias, which may involveboth the cerebral hemispheres and cerebellum.Cranial lacunae or mesodermal defects of theskull (luckenschadel) are common and the radi-ographic appearance is of multiple ‘punched-out’areas which usually resolve in the first 6 monthsof life. The Chiari type II malformation may alsobe associated with anomalies of the cardiovascu-lar system, gastrointestinal system (imperforateanus) and genitourinary system.
Syringomyelia is cavitation within the spinalcord. However, the cavitation occurring in asso-ciation with the Chiari malformation is usuallycalled hydromyelia, as it is a dilatation of the cen-tral canal which is lined by ependyma. The termsyringomyelia is reserved for cavitation lyingoutside the central canal area lined by glial tissue.
Aetiology
Gardner popularized the hydrodynamic theoryof the origin of syringomyelia (hydromyelia) as-sociated with Chiari malformation. In brief, thetheory proposes that the CSF is unable to passfreely out of the 4th ventricle as the normal path-ways have either failed to open or are obliterateddue to ‘crowding’ in the posterior fossa. The nor-mal pulsations of CSF are consequently transmit-ted down the central canal of the spinal cord. Theclose association of the Chiari type II malforma-tion and meningomyelocele led to a theory thatspinal cord tethering resulted in the caudal dis-placement of the cranial structures as a result ofgrowth. Alternatively, the malformation may result from hindbrain maldevelopment duringearly fetal life.
Williams has proposed a differential pressurebetween the intracranial and intraspinal fluidcompartments as another mechanism for the de-velopment of the malformation. With a Valsalvamanoeuvre, the engorgement of the spinalepidural veins causes a rise in the intraspinalpressure. The spinal subarachnoid space is com-pressed and a pressure wave moves into the intracranial cavity. When the spinal pressure
returns to normal the reverse should occur, withflow from the intracranial cavity into the spinalcavity. If this equalization of pressures is im-paired and delayed by adhesions and tissue inthe foramen magnum, a pressure differential iscreated between the intracranial and intraspinalfluid compartments and alternative pathwaysdevelop, such as through a patent obex into thespinal central canal. In addition, the pressure dif-ferential promotes progressive caudal displace-ment of cerebellar tissue through the foramenmagnum.
Clinical presentation
The clinical features of the Chiari type II malfor-mation present in infancy, childhood or adoles-cence. A Chiari type I malformation causessymptoms presenting in adolescence and adult-hood and the neurological features are almost al-ways due to the development of a syrinx withinthe spinal cord or lower brainstem.
In infancy the abnormality will be apparentwith its association with myelomeningocele. Progressive hydrocephalus may develop. Severebrainstem dysfunction may result in episodic apnoea, depressed gag reflex, nystagmus andspastic paresis of the upper limbs.
In childhood the type II malformation may bemanifest by nystagmus, spastic paralysis andbulbar dysfunction.
In adolescence the symptoms may be due to either a type I or type II Chiari malformation. The features will involve a progressive spasticparalysis of the upper and/or lower limbs andmay also include the features of syringomyelia,including suspended thermoanaesthesia sensoryloss, atrophic changes in the hands and upper extremities and bulbar problems due either to extension of the syrinx into the lower brainstemor to the direct pressure from the Chiari type IImalformation itself.
Adult symptoms are primarily due to a com-bination of the Chiari type I malformation and syringomyelia. The characteristic symptomsinclude occipital headache, exacerbated bycoughing, and neck and arm pain. Nystagmus iscommon and may be either horizontal or vertical.
DEVELOPMENTAL ABNORMALITIES 161
KAY11 12/16/04 7:43 PM Page 161

162 CHAPTER 11
Downbeat nystagmus, exacerbated by the pa-tient looking down and out, is characteristic of acraniocervical junction abnormality.
The characteristic clinical features resultingfrom syringomyelia include:• dissociated sensory loss (loss of pain and temperature sensation with preservation of joint position sense) occurring in a ‘cape-like’ distribution (Fig. 11.4). The sensory loss willoften result in painless injury of the fingers orhands and Charcot joints may develop• weakness and wasting of the small muscles ofthe hand• progressive long tract signs resulting in spasticparesis of the lower limbs and paralysis of theupper limbs• bulbar features, if the syrinx extends into thelower brainstem.
Radiological investigations
MRI has revolutionized the radiological investi-
gations of craniocervical junction abnormalities.Sagittal and coronal scans will show displace-ment of the cerebellum into the upper cervicalcanal, with caudal displacement of the 4th ventri-cle and brainstem in the type II malformation.MRI will also show the other associated intra-cranial abnormalities (Fig. 11.5). However, it may not adequately demonstrate the underlyinganatomy of the bony structures.
MRI has virtually replaced CT scanning with intrathecal contrast, and myelography is nolonger necessary.
Syringomyelia (hydromyelia)As discussed earlier, intraspinal cavitation can beeither hydromyelia, where the syrinx is a dilata-tion of the central canal and there is usually com-
Fig. 11.4 ‘Cape-like’ distribution of pain andtemperature loss typically resulting from syrinx orother intramedullary lesion in the cervical and upperthoracic regions. Fig. 11.5 (a) Chiari type II malformation with
dysplastic cerebellum extending through foramenmagnum to C2 level and caudal displacement of 4thventricle and medulla. There is a syrinx (hydromyelia)in the cervical and upper thoracic spinal cord. (b)Chiari type I malformation with cervical syrinx(hydromyelia).
(a)
(b)
KAY11 12/16/04 7:43 PM Page 162

munication with the CSF pathways, or the non-communicating syringomyelia, where the syrinxis separate from the central canal.
Hydromyelia (communicating syringomyelia)usually results from Chiari type I and type II malformations and occasionally from basilar arachnoiditis. Non-communicating syringomyelia may be due to previous trauma or neoplasms, orassociated with spinal arachnoiditis. Occasion-ally, no underlying abnormality can be found as acause of the syrinx.
The most valuable radiological investigation isMRI, which will show the extent of the syrinx andassociated abnormalities. This investigation hasalmost completely replaced the use of CT scanwith water-based contrast injected into the sub-arachnoid space. Delayed post-contrast CT scan-ning shows intramedullary opacification as wellas the enlarged cord.
Treatment
There are two major surgical procedures.1 Posterior fossa and upper cervical decom-pression.2 Shunting of the syrinx.
The posterior fossa operation involves decom-pression by removing the posterior rim of theforamen magnum, posterior arch of the atlas andlaminae of the upper cervical spine, extendingdown to below the level of the descent of the cerebellar tonsil. The dura is opened widely, as it often acts as a constricting band, particularly at the level of the foramen magnum. A variety ofother procedures may be performed at that time,including dissection of the subarachnoid adhe-sions, opening of the foramen of Magendie intothe 4th ventricle, plugging the enlarged openingof the central canal at the obex with tissue, andplacing a stent through the foramen of Magendie.These procedures must be done with meticulousmicrosurgery techniques to avoid further dam-age to this extremely sensitive area. The dura isclosed using a graft of cervical fascia.
The syringomyelia (hydromyelia) may beshunted into either the subarachnoid space or theperitoneal or pleural cavity. Some surgeons pre-fer to carry out this procedure at the same time as
the posterior fossa decompression but others pre-fer to perform the operation only if there is con-tinuing progression of neurological disability.
Craniovertebral junction abnormalities
The craniovertebral junction region involves theforamen magnum, the adjacent occipital boneand the atlas and axis vertebrae. Numerous con-genital or acquired abnormalities occur in this region which may result in compression of theunderlying neural structures. Some abnormali-ties, including spina bifida of the anterior or pos-terior arch of the atlas, remain asymptomatic.
Basilar invagination (impression)
Basilar invagination is a deformation of the basi-occiput in which there is an upward indentationor invagination of the base of the skull, includ-ing the rim of the foramen magnum, occipitalcondyles and neighbouring bone, into the poste-rior fossa. The clivus is often shortened and theinvagination reduces the diameter of the foramenmagnum. The odontoid process frequently pro-jects into the anterior part of the foramen mag-num so that its diameter is reduced still further.There is a frequent association with congenitalfusion of the cervical vertebrae to each other or tothe occiput.
Acquired basilar impression may be due tosoftening of the bone by disease. The most common cause is Paget’s disease but it may alsooccur in osteomalacia, hyperparathyroidism andosteogenesis imperfecta.
The clinical features resulting from basilar impression are due to compression of the neuralstructures at the cervicomedullary junction — themedulla oblongata, the cranial nerves, the cervi-cal roots and the spinal cord.
The clinical features may include a progressivequadriparesis, dysphagia, respiratory difficul-ties, nystagmus (sometimes downbeat) and sub-occipital headache due to irritation of the 2ndcervical nerve.
Useful radiological investigations include CTscan (with sagittal reconstruction and intrathecalcontrast) (Fig. 11.6), MRI and plain X-rays.
DEVELOPMENTAL ABNORMALITIES 163
KAY11 12/16/04 7:43 PM Page 163

164 CHAPTER 11
Various measurements at the base of the skull canbe used to diagnose the anomaly. Chamberlain’sline joins the tip of the dorsal lip of the foramenmagnum to the dorsal margin of the hard palateand, on a lateral skull X-ray or sagittal MRI,should normally lie above the tip of the odontoidprocess of the axis and pass through the ventrallip of the foramen magnum. McGregor’s linejoins the hard palate to the most caudal portion ofthe occipital curve. In basilar invagination the tipof the odontoid lies more than 4.5 mm above thisline (Fig. 11.7).
Platybasia
Platybasia is sometimes erroneously used syn-onymously with basilar impression. Platybasiarefers to an obtuse basal angle joining the plane ofthe clivus with the plane of the anterior fossa of the skull; it is said to be present if the angle exceeds 145°.
Although platybasia is often present with basi-lar impression it causes no symptoms by itself.
Atlantoaxial dislocation
Dislocations at the atlantoaxial joint can resultfrom congenital malformations, involving in par-ticular the congenital fusion of the occiput to theatlas and fusions of C2 and C3. Multiple congen-ital cervical fusions occur in the Klippel–Feil syn-drome. These types of fusions will increase thestrain on the ligaments of adjacent vertebrae, resulting in instability. Atlantoaxial dislocationmay also result from inflammatory conditionssuch as rheumatoid arthritis or following trauma(Fig. 11.8).
Dandy–Walker cyst
The Dandy–Walker cyst is a cystic enlargement of the 4th ventricle, usually associated with hy-poplasia or partial agenesis of the cerebellum andhydrocephalus of the 3rd and lateral ventricles.
It is probable that the primary cause is an em-bryological failure of the foraminal outlets of the4th ventricle to open, resulting in cystic enlarge-ment of the 4th ventricle and hydrocephalus.However, the Dandy–Walker cyst is sometimesassociated with other congenital abnormalities,such as agenesis of the corpus callosum andaqueduct stenosis, and it has been suggested thatit may represent a cerebellar dysraphism.
The clinical features are usually apparent in in-fancy and result primarily from hydrocephalus.
Fig. 11.6 Sagittal reconstruction of CT scan (withintrathecal contrast) demonstrating the odontoidprocess extending through the foramen magnum.
Hard palate
Chamberlain's line
McGregor's line
Fig. 11.7 Plain X-ray measurement for basilarinvagination.
Fig. 11.8 Atlantoaxial subluxation in rheumatoidarthritis.
KAY11 12/16/04 7:43 PM Page 164

The cyst may be diagnosed in childhood, par-ticularly if it does not produce significant hydro-cephalus, and the major presenting features areataxia and delayed motor development.
The diagnosis is made by CT scan (Fig. 11.9) orMRI. The standard treatment is now shunting ofthe cyst but, if aqueduct stenosis is present, a ven-tricular shunt may also need to be inserted.
Spinal dysraphism
Spinal dysraphism results from incomplete orfaulty closure of the dorsal midline embryol-ogical structures. The major forms of spinal dys-raphism are:1 Myelomeningocele.2 Meningocele.3 Lipomyelomeningocele.4 Occult spinal dysraphism:
(a) dermoid tumours(b) diastematomyelia(c) intraspinal lipoma(d) hypertrophic filum terminale.Spina bifida occulta is a bony deficit usually
found in the laminae of the lumbosacral spineand due to a midline fusion defect. It is an inci-dental radiological finding and is present in up to20% of adults. In the vast majority there is no neu-
rological involvement and the lesion is asympto-matic throughout life.
Myelomeningocele
Myelomeningocele is the most common and im-portant form of spinal dysraphism presentingduring the neonatal period (Fig. 11.10). It is char-acterized by protrusion of the neural elementsthrough a vertebral defect into a meningeal-linedsac. Typically, the cord at this level is not fusedbut is in its flattened embryological state, withthe nerve roots arising from the ventral surfaceand the open central canal lying dorsally. Themajor disability from this condition results fromthe irreversible neurological deficit caused bythis spinal cord abnormality. Depending on thelevel of the defect the spinal cord or conus and cauda equina may be involved. Althoughmyelomeningocele may occur at any level, it ismost common in the lumbar and lumbosacralsegments.
This disorder occurs in approximately 1 in1000 live births. There is a greater frequencyamong whites than blacks, with a slight femalepredominance. There is a familial incidence: ifone member of a family is affected the risk of thedisorder occurring in subsequent offspring isabout 5%. Seasonal outbreaks of myelomeningo-cele have been reported and there are ethnic
DEVELOPMENTAL ABNORMALITIES 165
Fig. 11.9 Dandy–Walker cyst in posterior fossa withhydrocephalus of lateral and 3rd ventricles.
Dysplasticnerve roots
Sac
Myelomeningocele Meningocele
a b
Fig. 11.10 Myelomeningocele and meningocele.
KAY11 12/16/04 7:43 PM Page 165

166 CHAPTER 11
differences, with a higher incidence of the condi-tion in the western United Kingdom, northernIndia and Egypt.
Prenatal diagnosis of myelomeningocele andother open neural tube disorders is possible bymeasuring alpha-fetoprotein in the amnioticfluid at 14–16 weeks and by prenatal ultrasoundexamination. The widespread use of increasinglyaccurate ultrasound examination in the firsttrimester of pregnancy has led to detection ofmyelomeningocele, and in many centres detec-tion is followed by parental decision to terminatethe pregnancy. Consequently there has been adramatic decrease in the incidence of childrenborn with this type of anomaly. The ultrasoundfindings can be confirmed by MRI.
Myelomeningocele is frequently associatedwith other congenital abnormalities, most commonly the Chiari type II malformation, aqueduct stenosis (forking) and hydromyelia(syringomyelia).
The management of myelomeningocele involves:1 Assessment of the sac and its coverings.2 Neurological evaluation.3 Examination for other associated conditions:
(a) within the CNS, e.g. hydrocephalus(b) extracranial anomalies, e.g. gastrointesti-nal, urinary.
4 Counselling and careful discussions with theparents.5 Surgical procedures.
Decisions concerning whether a patient shouldundergo a surgical procedure with closure of thesac are among the most difficult in neurosurgicalpractice. On the one hand, the child has a right tolife but there is also a right to a life of sufficientquality to be worth living. The immediate deci-sion is whether to close the myelomeningocelesac. In 1959 physicians in Sheffield undertook aprogramme of immediate closure in all neonates,with aggressive treatment of the hydrocephalusand other malformations. However, when the series was examined, only 7% ‘had less thangrossly crippling disability and may be consid-ered to have a quality of life not inconsistent withself respect, earning capacity, happiness andeven marriage’. Consequently, selective criteria
were developed and the children excluded fromtreatment were those with:• paralysis at L2 to L3 or above• marked hydrocephalus• kyphosis• other major congenital abnormalities or birthinjuries.
However, although when these criteria areused, a large number of untreated infants do notlive long, a significant minority do, and there isgreat concern about their quality of life.
The initial operation aims to:• preserve all the neural tissue and reduce it intothe intervertebral canal; untether the spinal cord• obtain a watertight closure of dura lining thesac• cover the defect with muscle, fascia and skin.
It will subsequently be necessary to make deci-sions concerning the treatment of hydrocephalusand other associated malformations.
The continued care of these children requires amultidisciplinary approach including urologists,orthopaedic surgeons, physicians, physiothera-pists and social workers. The children frequentlyhave severe urological problems, which may re-sult in renal failure as adolescents. The muscu-loskeletal disorders, including talipes and hipdislocation, require careful orthopaedic man-agement to maximize any residual lower limbfunction.
Lipomyelomeningocele
This is a much less common disorder thanmyelomeningocele. The mass is covered by skinand the lipomatous tissue extends intradurallyand is intimately interwoven with the rootlets of the cauda equina and the conus medullaris,which is not usually fused. Neurological exami-nation is usually normal at birth and progres-sive neurological deficits occur, resulting fromgrowth and tethering of the spinal cord. The mostcommon symptoms include bladder and boweldisturbance, back pain and progressive paralysisin the legs with foot deformities and loss of sensation.
Surgery is delayed until about 4 months. Thelipoma is removed as completely as possible
KAY11 12/16/04 7:43 PM Page 166

without endangering the neural tissue; the primary surgical aim is to untether the spinalcord.
Meningocele
This is much less common than myelomeningo-cele and is characterized by a cystic lesion containing only meninges and CSF; it does notcontain any neural tissue.
Occult spinal dysraphism
Occult spinal dysraphism includes a number ofspinal disorders, the vast majority of which aresituated in the lumbar region and produce progressive neurological dysfunction, often as aresult of tethering of the spinal cord. The morecommon lesions include:• intraspinal lipomas (and lipomyelomenin-gocele)• dermoid tumours• diastematomyelia.
The underlying intraspinal lesion can often besuspected from an overlying skin lesion such as adimple, sinus tract, fatty mass, haemangioma orabnormal tuft of hair. The neurological symp-toms are usually first noted in childhood or ado-lescence. There is usually a slowly progressiveneurological dysfunction involving:• bowel and bladder disturbance• progressive weakness of the legs and foot deformities• back pain• sensory disability in the lower limbs• progressive scoliosis.
Depending on the level of the abnormality, theneurological examination will show evidence of either lower and/or upper motor neuronedamage.
Lipomas are the most frequent form of occultspinal dysraphism. The lumbosacral lipoma pre-sents at birth as a soft subcutaneous mass, usu-ally in the midline and covered by skin. In itsmost severe form — lipomyelomeningocele — thelipoma will involve neural tissue and will extendthrough a spina bifida. Less severe abnormalitieswill be associated with a low-lying conus and
with tethering of the cord by an enlarged filumterminale or fatty tissue.
Diastematomyelia is a condition in which thespinal cord is bifid and the two hemicords areseparated by a bony spur or dural band. Progres-sive neurological dysfunction will occur due totraction on the cord that is transfixed duringgrowth periods (Fig. 11.11).
The cord is occasionally tethered by a short-ened, thickened filum terminale — hypertrophicfilum terminale — and the only associated abnor-malities are spina bifida occulta and an occa-sional hairy patch over the lower spine.
Radiological assessment will utilize plain X-ray, CT scan (with intrathecal contrast) and MRI.Plain X-rays will show a range of vertebral ab-normalities including spina bifida, hemiverte-brae, abnormal spinal curves, diastematomyelicspurs and widened interpedicular distances.
The surgical treatment is aimed at:• removing the underlying pathological causewhile preserving neural tissue• untethering the cord.
Craniosynostosis
Craniosynostosis is premature closure of cranialsutures and occurs in 1 in 3000 births. It mayoccur as a condition involving a single cranial su-ture or as part of a complex syndrome involvingmultiple fusion abnormalities.
The posterior fontanelle has usually closed by2–3 months of age and the anterior fontanelle byabout 16–18 months. The brain ceases to grow at10–12 years of age, at which time the cranial sutures are obliterated by firm fibrous tissue.Complete ossification of the sutures does notoccur until after the 3rd decade of life.
The clinical features of craniosynostosis are related to:• the cranial deformity• raised intracranial pressure• the presence of associated congenital abnor-malities.
Sagittal synostosisThis is by far the most common type of primarycraniosynostosis; the incidence is greater than
DEVELOPMENTAL ABNORMALITIES 167
KAY11 12/16/04 7:43 PM Page 167

168 CHAPTER 11
that of all other types of craniosynostosis com-bined. Males are most commonly affected andthe condition is usually not associated with othercongenital abnormalities.
Premature fusion of the sagittal suture resultsin the head expanding in the occipitofrontal diameter and produces a long narrow head(scaphocephaly). Compensatory growth alongthe metopic and coronal sutures causes the fore-head to expand laterally (frontal bossing).
Coronal synostosisCoronal synostosis occurs more commonly in females. The head expands superiorly and later-ally (brachycephaly). This produces a short ante-rior cranial fossa, shallow orbits, hypertelorismand elevation of the forehead. Choanal atresia iscommon.
Bilateral coronal synostosis commonly occursas one of several congenital defects in Crouzon’sand Apert’s syndromes.
If only one coronal suture fuses prematurelythere will be an asymmetrical cranial deformity.
Metopic synostosisMetopic synostosis produces a narrow, triangu-lar forehead (trigonocephaly) associated with hypotelorism.
Lambdoid synostosisLamboid synostosis is uncommon. There is sym-metrical flattening of the posterior cranium.
Operative treatment
Surgery is performed to:• correct the cranial deformity• relieve the effects of raised intracranial pressure.
If only one suture is fused, compensatorygrowth along the open suture lines will reducethe risk of raised intracranial pressure, althoughthere have been studies showing raised intracra-nial pressure, usually only moderate, in childrenwith single suture fusion. However, if two ormore cranial sutures fuse prematurely there is arisk of increased intracranial pressure as growthproceeds. This may lead to mental and motor retardation and to optic atrophy.
Fig. 11.11 Lumbar diastematomyelia with bone spurand dural band (arrow) passing through the caudaequina.
(a)
(b)
(c)
KAY11 12/16/04 7:43 PM Page 168

The operative procedure has usually involveda strip craniectomy of the fused suture. However,as the long-term results have been somewhat dis-appointing, the trend is now to undertake a moremajor vault reconstruction to obtain a permanenteffect.
Surgery is usually best delayed until the childis 3–6 months old, but if two or more cranial su-tures are fused then it may be undertaken earlierto minimize the effects of brain compression.
The operation involves resection of the affected sutures. It should be carefully plannedand meticulously performed to minimize bloodloss, which is the greatest risk of the procedure.
Further readingDelashaw JB et al. (1989) Cranial vault growth in cran-
iosynostosis. Journal of Neurosurgery 70, 159–166.Dyste GN, Menezes AH, Vanglider JC (1989) Sympto-
matic Chiari malformations. An analysis of presenta-tion, management and long term outcome. Journal ofNeurosurgery 71, 159–168.
Gardner WJ (1965) Hydrodynamic mechanism of syringomyelia: its relationship to myelocoele. Journalof Neurology, Neurosurgery and Psychiatry 28, 247–259.
Hockley AD, Wake MJ, Goldin H (1988) Surgical management of craniosynostosis. British Journal ofNeurosurgery 2, 307–314.
Hoffman HJ et al. (1982) Investigation and managementof suprasellar arachnoid cysts. Journal of Neurosurgery57, 597–602.
Hoffman HJ, Hendrick EB, Humphreys RP (1975) Man-ifestations and management of Arnold Chiari malformation in patients with myelomeningocoele.Child’s Brain 1, 255–259.
Hoffman HJ, Hendrick EB, Humphreys RP (1976) Thetethered spinal cord: its protean manifestations,
diagnosis and surgical correction. Child’s Brain 2,145–151.
Humphreys RP (1985) Spinal dysraphism. In: WilkinsRH, Rengochary SS, eds. Neurosurgery. McGraw-Hill,New York, 2041–2052.
Kaye AH, Black P McL (2000) Operative Neurosur-gery. Churchill Livingstone, London, New York, Edinburgh.
Levy WJ, Mason L, Hahn JF (1983) Chiari malformationpresenting in adults: a surgical experience in 127cases. Neurosurgery 12, 377–390.
Little JR, Gomez MR, McCarty CS (1973) Infratentorialarachnoid cysts. Journal of Neurosurgery 39, 380–386.
Lorber J (1971) Results of treatment of myelomeningo-coele: an analysis of 524 unselected cases, with special reference to possible selection for treatment.Developmental Medicine and Child Neurology 18,279–303.
Mapstone T (1994) Management of tethered cord syndrome. Neurosurgery Quarterly 4, 82–91.
Matson DD (1969) Neurosurgery in Infancy and Child-hood. Charles C Thomas, Springfield.
Milhorat TH (1978) Paediatric Neurosurgery. Contempo-rary Neurology Series. F A Davis, Philadelphia.
Milhorat TH, Miller JI, Johnson WD (1993) Anatomicalbasis of syringomyelia. Neurosurgery 32, 748–754.
Robinson RG (1964) The temporal lobe agenesis syn-drome. Brain 87, 87–106.
Robinson RG (1971) Congenital cysts of the brain:arachnoid malformations. Progress in NeurologicalSurgery 4, 133–174.
Shillito J, Matson DD (1968) Craniosynostosis: a reviewof 519 surgical patients. Paediatrics 41, 829–853.
Starkman SP, Brown TC, Linell EA (1958) Cerebralarachnoid cysts. Journal of Neuropathology and Experi-mental Neurology 17, 480–500.
Williams B (1980) On the pathogenesis of syringo-myelia: a review. Journal of the Royal Society of Medicine 73, 298–806.
DEVELOPMENTAL ABNORMALITIES 169
KAY11 12/16/04 7:43 PM Page 169

Infections involving the nervous system presentin a variety of ways, many of which result indeath or severe morbidity if not diagnosed andtreated promptly. The infections usually occur asthe result of haematogenous spread or direct ex-tension from adjacent bone, soft tissue or sinuses.A large variety of pathogens are involved, in-cluding viruses, fungal agents and bacteria. Themost common infections involving the neurosur-geon are:• acute bacterial meningitis• cerebral abscess.
Neurosurgeons are involved in the manage-ment of nervous system infections because patients frequently present with manifestationsof a rapidly progressive neurological illness, aswell as the systemic manifestations of sepsis.
Infection may involve any part of the nervoussystem or its coverings and can be classified inthe following way.1 Cranial vault infections.2 Extradural abscess/empyema.3 Subdural abscess/empyema.4 Meningitis.5 Brain:
(a) brain abscess(b) encephalitis.
Meningitis
Bacterial meningitis is a serious, life-threateninginfection of the meninges. Viral meningitis is the more common infection but is usually self-limiting, and the neurosurgeon is rarely involved.
Most of the common organisms that cause bac-
terial meningitis are related to the patient’s ageand to the presence and nature of any underlyingpredisposing disease. Although a few types ofbacterial organisms account for most cases ofacute pyogenic meningitis there is a wide rangeof organisms that may be responsible. Table 12.1shows the most common causes of bacterialmeningitis related to age.
The bacteria reach the meninges and cere-brospinal fluid by three main routes.1 Haematogenous spread from extracranial fociof infection.2 Retrograde spread via infected thrombi withinemissary veins from infections adjacent to thecentral nervous system, such as sinusitis, otitis ormastoiditis.3 Direct spread into the subarachnoid space,such as from osteomyelitis of the skull and infec-tions of the paranasal sinuses.
The CSF is a good culture medium which willsupport the growth of many microorganisms.Normal CSF contains very low concentrations ofimmunoglobulins and complement componentsand is devoid of polymorphonuclear phagocytes.Furthermore, phagocytosis is impaired by thelow opsonic activity of CSF and organisms such as Streptococcus pneumoniae, Haemophilus in-fluenzae type B, Group B streptococci, Escherichiacoli and Klebsiella pneumoniae have a polysaccha-ride capsule that hinders phagocytosis.
Clinical presentation
Bacterial meningitis is usually an acute illnesswith rapid progression of clinical signs. Manycases are preceded by symptoms of an upper
CHAPTER 12
12 Infections of the central nervous system
170
KAY12 12/16/04 7:44 PM Page 170

respiratory tract infection. The major presentingfeatures are:• high fever• meningismus, including headaches, neck stiffness, photophobia, vomiting and an alteredmental state in terms of clinical presentation.
Although patients are usually alert at the com-mencement of the illness they will frequently be-come drowsy and confused. If treatment is notcommenced promptly there may be further dete-rioration of the conscious state as a result of a di-rect septic effect on the underlying brain, septicthrombosis of the cerebral arteries and veins, orthe development of hydrocephalus. Focal neuro-logical signs may develop as a result of corticalinfarction secondary to thrombosis.
In infants, neonates, the elderly and the im-munocompromised, the presentation of bacterialmeningitis may be different. Neck stiffness andfever are often absent and the presentation in-cludes listlessness and irritability in the youngand confusion or obtundation in the elderly/immunocompromised.
A careful search should be made for a skinrash. Meningococcal infection frequently has acoexisting petechial rash, which occurs less fre-quently in other bacterial (e.g. staphylococcalbacteraemia, Haemophilus influenzae infection) orviral infections. The original source of infection,e.g. sinusitis, bacterial endocarditis, otitis mediaor mastoiditis, may be evident and many patientshave evidence of pharyngitis — bacterial menin-gitis sometimes follows an upper respiratorytract infection.
Diagnosis
The diagnosis is made by CSF examination ob-tained by lumbar puncture which should be per-formed immediately the diagnosis is suspected.If the patient is drowsy, has other signs of raisedintracranial pressure or there are focal neurologi-cal signs, an urgent computerized tomographyscan must be performed prior to the lumbarpuncture to exclude an intracranial space-occupying lesion.
The CSF features on lumbar puncture are:• Macroscopically cloudy CSF.• Raised white cell count. This is usually in excess of 500 cells/mm3 and is predominantly apolymorphonuclear leukocytosis.• The protein level is greater than 0.8 g/l; it isoften substantially higher.• The glucose level is less than 2 mmol/l, frequently much lower. A useful index is theCSF : serum ratio which is less than 0.4 in a bacte-rial infection.• The Gram stain will be positive in over 70% ofpatients if common pathogens are involved, andin approximately 50% of patients for Gram-negative bacilli.Other tests which should be performed on theCSF include:• examination for Cryptococcus neoformans usingan India ink preparation and an agglutinationtest for cryptococcal antigen• investigation for Mycobacterium tuberculosis(Ziehl–Neelsen stain for acid-fast bacilli) andamoebae.
INFECTIONS OF THE CENTRAL NERVOUS SYSTEM 171
Table 12.1 Common organisms causing primary bacterial meningitis related to age.
Age Organism
Neonate (0–4 weeks) Group B streptococcus, Escherichia coli4–12 weeks Group B streptococcus, Streptococcus pneumoniae, Salmonella, *Haemophilus
influenzae, Listeria monocytogenes3 months–5 years Haemophilus influenzae*, Streptococcus pneumoniae, Neisseria meningitidisOver 5 years and adults Streptococcus pneumoniae, Neisseria meningitides
*In countries with routine Haemophilus influenzae immunization this organism is a rare cause of meningitis.
KAY12 12/16/04 7:44 PM Page 171

172 CHAPTER 12
Difficulties arise in diagnosis of partially treat-ed bacterial meningitis because the CSF culture isoften negative. Other investigations include:• blood cultures• radiological investigations to detect the sourceof infection — chest X-ray, CT scan or skull X-rayfor sinusitis.
The differential diagnosis includes:1 Other types of meningitis:
(a) viral(b) fungal (Cryptococcus neoformans)(c) amoebic(d) tuberculous(e) carcinomatous (Chapter 6).
2 Subdural empyema.3 Subarachnoid haemorrhage (Chapter 9).4 Viral encephalitis (especially herpes simplexencephalitis).
Treatment
High-dose intravenous antibiotic therapy shouldbe commenced immediately, and the selection ofthe antibiotic depends on:• the initial expectation of the most likely organ-ism involved, taking into account the age of thepatient and the source of infection• CSF microbiology studies• the antibiotic that has the best penetration intothe CSF.
There are many antibiotic regimes but if thereis no obvious site of infection initial therapyshould commence immediately as follows.• Neonates (under 3 months) — cefotaxime or ceftriaxone plus benzyl penicillin or amoxy-/ampicillin.• Three months to 15 years — cefotaxime or ceftriaxone.• 15 years to adult — benzyl penicillin plus cefotaxime/ceftriaxone.• Add vancomycin if Gram-positive strepto-cocci are seen and there is any suspicion of intermediate and/or resistant Streptococcus pneumoniae.
When the organism has been identified themost appropriate antibiotic should be used, de-pending on sensitivities and the ability of the antibiotic to penetrate into the CSF. Table 12.2shows the CSF penetration of antibiotics.
The usual specific antimicrobial therapy fol-lowing identification of the organism is:• Pneumococcus or meningococcus — benzylpenicillin (child: 60 mg/kg up to 1.8–2.4 g intra-venously 4-hourly). If patient is sensitive to peni-cillin use cefotaxime (child: 15 mg/kg 6-hourly orceftriaxone 100 mg/kg daily). About half the patients with meningococcal meningitis have petechiae or purpura. Subclinical or clinical disseminated intravascular coagulation often ac-companies meningococcaemia and may progress
Table 12.2 Antibiotic penetration into cerebrospinal fluid.
Good penetration with or without Good penetration only with meningeal inflammation meningeal inflammation Fair to poor penetration
Chloramphenicol* Penicillins First-generation cephalosporinsMetronidazole Penicillin Aminoglycosides‘Third-generation’ cephalosporins Amoxycillin Gentamicin
Ceftriaxone/Cefotaxime Flucloxacillin TobramycinRifampicinTrimethoprim/sulphamethoxazoleVancomycinCarbapenems
Meropenem
*Limited availability in most countries. Rarely used.
KAY12 12/16/04 7:44 PM Page 172

to haemorrhagic infarction of the adrenal glands,renal cortical necrosis, pulmonary vascularthrombosis, shock and death. The antibiotic ther-apy must be accompanied by intensive medicalsupportive therapy.• H. influenzae — amoxy-/ampicillin if organismis susceptible. If the patient is allergic or organ-ism-resistant use cefotaxime or ceftriaxone.• Listeria — benzyl penicillin or amoxy-/ampi-cillin plus trimethoprim and sulfamethoxazole.• Hospital-acquired meningitis — vancomycinplus cefotaxime, ceftriaxone or meropenem.
Complications of bacterial meningitis
Complications are more likely to occur if treat-ment is not commenced immediately. The majorcomplications are as follows.• Cerebral oedema.• Seizures.• Hydrocephalus — communicating hydroceph-alus. This may occur early in the disease or as alate manifestation.• Subdural effusion, particularly in children.Most resolve spontaneously but some may require drainage.• Subdural empyema. A rare complication thatusually requires drainage.• Brain abscess, which occurs as a rare complica-tion of meningitis.
Bacterial meningitis following neurosurgical procedures
Bacterial meningitis may complicate any in-tradural neurosurgical procedure, often withdevastating consequences. It is a much fearedcomplication following insertion of a CSF shunt(Chapter 3).
The majority of shunt infections are caused byStaphylococcus epidermidis and diphtheroids,species that are present in the normal skin flora.However, other pathogens such as Staph. aureus,pneumococcus and Haemophilus species may also be involved. Unlike primary bacterialmeningitis, the clinical presentation is frequentlysubacute or chronic and patients present with a low-grade fever before developing the more
overt signs of meningitis. There is frequently acoexisting ventriculitis.
The diagnosis is confirmed by examination ofthe CSF via a lumbar puncture or occasionally bywithdrawal of CSF from the reservoir mecha-nism of the shunt. The treatment consists of ad-ministration of antibiotics and removal of theshunt.
The most frequently isolated organisms inmeningitis following neurosurgical operationsare Staph. aureus, Staph. epidermidis and Gram-negative aerobic bacilli. The clinical features ofbacterial meningitis may be masked, or confusedwith the underlying neurosurgical illness andoperation. Although the meningitis may presentas a rapidly fulminating infection, it is also possi-ble for the clinical features to evolve slowly. Thediagnosis must be suspected if there is unex-plained fever, impaired conscious state, seizuresor neck stiffness following surgery.
CSF must be obtained and treatment with theappropriate antibiotics commenced. However, itmay be difficult to identify the causative organ-ism, as perioperative prophylactic antibioticsmay make isolation of the organism difficult.
Brain abscess
Cerebral abscess may occur at any age, may besingle or multiple and, although most are supra-tentorial, can also occur in the cerebellum orbrainstem.
Pathogenesis
Pyogenic inflammation of the brain leading tocerebral abscess may result from:• haematogenous spread from a known septicsite or occult focus• direct spread from an adjacent infectedparanasal or mastoid sinus• trauma causing a penetrating wound.
The metastatic brain abscesses arising byhaematogenous dissemination of infection arefrequently multiple and develop at the junctionof white and grey matter. The incidence in eachpart of the brain is proportional to its regionalblood flow, so that most abscesses occur in the
INFECTIONS OF THE CENTRAL NERVOUS SYSTEM 173
KAY12 12/16/04 7:44 PM Page 173

174 CHAPTER 12
distribution of the middle cerebral artery, princi-pally the parietal lobe, although they can also befound in the cerebellum and brainstem.
The most common sources of infection includeskin pustules, chronic pulmonary infection (e.g.bronchiectasis), diverticulitis, osteomyelitis andbacterial endocarditis. Patients with congenitalheart disease and who have a right-to-left shuntare particularly prone to brain abscesses becausetheir blood does not filter through the capillarybeds within the lungs. The site of origin of thehaematogenous spread is unknown in approxi-mately 25% of patients.
Direct spread from paranasal sinuses, mastoidair cells or the middle ear are the most commonpathogenic mechanisms in most series. Infectionfrom the paranasal sinuses spreads, by retro-grade thrombophlebitis, through the diploicveins into either the frontal or temporal lobe. Theabscesses are usually single and are located superficially. Frontal sinusitis may cause a brainabscess in the frontal lobe, sphenoid sinusitis anabscess in either the frontal or temporal lobe,maxillary sinusitis an abscess in the temporallobe and ethmoid sinusitis an abscess in thefrontal lobe. Middle ear infection may spreadinto the temporal lobe and, uncommonly, a cere-bellar abscess may result from infection spread-ing from the mastoid air cells. The mechanism ofabscess formation is either by erosion of the adja-cent bone and spread through the dura or due toretrograde septic thrombophlebitis in an emis-sary vein.
A cerebral abscess may result from craniocere-bral trauma which has caused a penetrating braininjury, particularly if foreign bodies such as boneor hair have been implanted in the brain. A lesscommon but well-documented cause of brain abscess results from infection spreading fromskull tongs used in skeletal traction for cervicaldislocation.
Histopathology
The abscess begins as a small area of focal in-flammation — cerebritis — consisting of polymor-phonuclear leukocytes, lymphocytes and plasmacells, which migrate from the peripheral blood
circulation and which surround the area of devel-oping infective necrosis. The necrotic centre enlarges and pus is formed by the release of enzymes from the inflammatory cells. At the periphery of this necrotic centre fibroblasts laydown a reticulin network and, as the abscess enlarges, a collagen capsule develops. The wall ofthe abscess develops more slowly on the ventric-ular side because of the poorer vascularity of thedeep white matter compared with the corticalgrey matter. Consequently, the abscess tends toenlarge into the deep white matter, and it mayrupture into the lateral ventricle.
Bacteriology
In the preantibiotic era brain abscess was causedpredominantly by Staph. aureus and streptococci.After the introduction of antibiotics the inci-dence of staphylococcal abscesses declined andmost abscesses were thought to be due to strep-tococci, although up to 50% of culture results in some series were ‘sterile’. When improvedanaerobic culture techniques became availablethe incidence of positive cultures increased, andmany of the abscesses previously thought to besterile were found to have been caused by an-aerobic organisms, particularly streptococci and Bacteroides species. Meticulous culture tech-niques have resulted in considerable improve-ment in the definition of the bacterial spectrum inbrain abscesses and have confirmed that strepto-cocci are the most common organisms isolated inbrain abscesses of all origins, but the exact bacte-rial flora depends on the cause of the abscess(Table 12.3).
Streptococci are isolated from approximately80% of brain abscesses. The most common singlespecies is the beta-haemolytic carboxyphilic Strep.milleri, a microaerophilic streptococcus whichgrows in anaerobic culture and also 10% carbondioxide. The major habitat of Strep. milleri is the alimentary tract, including the mouth and dentalplaque. The association between frontal lobe ab-scesses, Strep. milleri and sinusitis indicates thatthe source of infection in many brain abscesses isthe upper respiratory tract, the organism passinginto the brain from the paranasal sinuses.
KAY12 12/16/04 7:44 PM Page 174

Otogenic abscesses usually yield a mixed flora,including bacteroides (Bacteroides fragiles), various streptococci and members of the Entero-bacteriaceae (Escherichia coli, Proteus andPseudomonas species).
Metastatic haematogenous infection may bedue to various aerobic and anaerobic strepto-cocci, enterobacteria and other Gram-negativebacilli.
Staph. aureus is often the pathogen in abscessesresulting from trauma and can also be seen inpostoperative abscesses.
Presenting features
Patients present with features of:1 An intracranial mass:
(a) raised intracranial pressure(b) focal neurological signs, e.g. hemiparesis,dysphasia(c) epileptic seizures.
2 Systemic toxicity — fever and malaise.3 Clinical features of the underlying source ofthe infection — sinusitis, bacterial endocarditis,diverticulitis.
The clinical features develop over 2–4 weeks,although a slower progression is not unusual. If
the abscess involves an eloquent intracerebral location it may present when quite small. Alter-natively, an abscess in the frontal lobe may reacha large size before producing any major neuro-logical deficit. About half the patients with brainabscess have systemic symptoms, includingfever, at the time of the diagnosis. Marked toxicsymptoms may be attributable to the abscess rup-turing into the ventricle or associated meningitis.
Diagnosis
CT scanning has been responsible for a dramaticreduction in the mortality from cerebral abscessbecause of its ability to diagnose single and multiple abscesses and to localize the lesion accurately.
The CT scan or magnetic resonance imagingappearance is typically a ring-enhancing massoften surrounded by considerable oedema (Figs12.1–12.4). The enhancing capsule is usually thin-ner adjacent to the ventricle compared with themore superficial capsule. The lesions may bemultiple (Fig. 12.2b) or multiloculated (Fig. 12.3).In the early stages of development of the abscess,when the infection is localized as ‘cerebritis’, theCT scan or MRI appearance will be an area of low
INFECTIONS OF THE CENTRAL NERVOUS SYSTEM 175
Table 12.3 Cerebral abscess — pathogenesis and principal organisms.
History Site of abscess Predominant organisms
Sinusitis — frontal Frontal lobe Aerobic and anaerobic streptococciStreptococcus milleri
Haemophilus species
Mastoiditis, otitis Temporal lobe Mixed floraAerobic and anaerobic streptococciEnteric bacteria or EnterobacteriaBacteroides fragilisHaemophilus species
Haematogenous, cryptogenic Brain Aerobic streptococciAnaerobic streptococciEnterobacteriaStaphylococcus aureus
Trauma Brain Staphylococcus aureus
KAY12 12/16/04 7:44 PM Page 175

176 CHAPTER 12
Peripheral blood examination may show aleukocytosis. Raised erythrocyte sedimentationrate and positive blood cultures may be obtainedif there is a coexisting septicaemia.
Management
The principles of treatment are to:• identify the bacterial organisms• institute antibiotic therapy• drain or excise the abscess.
A specimen of the pus is essential for accurateidentification of the organism so that the appro-priate antibiotic therapy can be commenced. Oc-casionally, the organism can be identified from apositive blood culture or other obvious source ofinfection. A lumbar puncture is absolutelycontraindicated (and of no diagnostic benefit) inthe presence of a cerebral abscess.
Surgical treatmentSurgical treatment of the abscess involves either:• aspiration of the abscess through a burr hole,with repeated aspirations as required or• excision of the abscess.
Drainage of the abscess through a burr hole, ifnecessary using CT-guided stereotaxis, is a safe,effective way of obtaining the pus and emptyingthe abscess. It is frequently necessary to repeat
Fig. 12.1 Cerebral abscess early in its development. Asmall contrast-enhancing lesion surrounded by low-density cerebral oedema.
Fig. 12.2 (a) Typical ring-enhancing cerebral abscess in the frontal lobe with surrounding cerebral oedema. (b) Multiple cerebral abscesses.
(a) (b)
density which enhances after intravenous con-trast but without the typical ‘ring’ appearanceand usually with marked adjacent oedema. MRIis a more sensitive investigative tool and can helpdifferentiate between an abscess and tumour. Ifthe abscess is due to haematogenous spread it isusually located at the grey/white matter junction(Fig. 12.1).
KAY12 12/16/04 7:44 PM Page 176

the aspirations and this is best evaluated by follow-up CT scans.
Surgical excision of the abscess should be con-sidered if:• there is persistent reaccumulation of pus de-spite repeated aspirations• the abscess is in an accessible site• there is a well-formed fibrous capsule whichfails to collapse despite repeated aspirations• there is a cerebellar abscess.
Antibiotic therapyAs soon as pus has been obtained, antibiotic ther-apy should commence. The initial choice of an-tibiotic, before culture results are available, willdepend on the probable cause of the brain ab-scess and the Gram stain. The usual initial treatment is high-dose penicillin, ceftriaxone andmetronidazole. Strep. milleri is the organism mostfrequently found in abscesses of sinusitic origininvolving the frontal lobe; it is highly sensitive topenicillin. Abscesses of otitic origin, usually occurring in the temporal lobe, are caused by awide range of aerobic and anaerobic bacteria. Acombination of penicillin with cefotaxime, ceftri-axone or metronidazole should be used. Abs-cesses of metastatic or cryptogenic origin may becaused by streptococci or by a mixture of bacte-ria, and broad-spectrum therapy, including peni-cillin, should be used until bacteriological resultsare available. As many of the organisms are resis-tant to penicillin, it has been suggested that apenicillinase-stable penicillin (e.g. flucloxacillin)should be substituted. For postsurgical brain ab-scess it is recommended that vancomycin be used with cefotaxime or ceftriaxone.
As soon as the culture results are available the appropriate antibiotic should be used intra-venously in high doses and selection should bemade bearing in mind the antibiotic’s penetra-tion into the brain and CSF.
Corticosteroid therapy (dexamethasone) maybe necessary to reduce cerebral oedema andshould be considered in patients who are drowsyor have a deteriorating neurological state despitesurgery and antibiotic treatment.
Anticonvulsant medication should be com-menced as there is an incidence of seizures in between 30 and 50% of cases.
Prognosis
The improvements in antibiotic therapy and CTscanning have dramatically reduced the mortalityof bacterial abscesses from 50% to less than 10%.
Epidural abscess
Cranial epidural abscess results following:
INFECTIONS OF THE CENTRAL NERVOUS SYSTEM 177
Fig. 12.3 Multiloculated cerebral abscess.
Fig. 12.4 CT scan. Large cerebral abscess.
KAY12 12/16/04 7:44 PM Page 177

178 CHAPTER 12
• trauma• surgery — craniotomy or insertion of skull trac-tion tongs• paranasal sinusitis or mastoiditis.
The condition is frequently associated with osteomyelitis of the cranial vault.
Clinical features
The clinical features of an epidural abscess areprimarily those of osteomyelitis, with acute local-ized pain and tenderness and localized pittingoedema of the scalp over the affected area, de-scribed by Percival Pott and known as ‘Pott’spuffy tumour’. There are usually systemic symp-toms of infection. When the epidural collectionenlarges the patient will start to have symptomsof raised intracranial pressure and, if the mass islarge enough, associated symptoms of a neuro-logical deficit.
The most common organisms are aerobic andanaerobic streptococci and Staph. aureus.
Treatment
Treatment involves evacuation of the pus, exci-sion of any infected bone and surgical eradica-tion of the underlying cause (e.g. sinus infection).High-dose antibiotic therapy should be com-menced with di-/flucloxacillin plus gentamycin.This must be utilized until the organism is identi-fied and sensitivity determined.
The diagnosis is made on CT scan or MRI,which will show the extradural collection of pusas well as osteomyelitis and the infected sinuses.
Subdural abscess
A subdural abscess is an uncommon but poten-tially life-threatening infection with possible serious neurological sequelae in the patients who survive. The abscess follows infection in theparanasal sinuses, particularly frontal sinusitisand, less commonly, infection in the mastoid aircells. The infection in the subdural space is an ex-tension of the sinusitis through emissary veinsand retrograde thrombophlebitis.
Subdural empyema may also result from
penetrating wounds, or may follow surgery. Ininfants subdural empyema may occur as an infection of the subdural space followingmeningitis.
Microbiology
The most common organism responsible for subdural empyema following frontal sinusitis isStrep. milleri. However, other aerobic and anaero-bic streptococci, other anaerobes and Staph. au-reus may also be responsible, with a patternsimilar to that indicated for intracerebral abscesses.
Clinical presentation
In contrast to patients with extradural abscesses,patients presenting with subdural empyemas areusually seriously ill, being toxic and febrile, withfeatures of meningeal irritation. They frequentlyhave rapidly progressive neurological signs, in-cluding depressed conscious state, hemiparesisand dysphasia. Epileptic seizures occur in mostpatients.
The classic presentation is a patient with a his-tory of acute frontal sinusitis who develops severe headaches and high fever and has a rapidneurological deterioration with seizures.
Diagnosis
The differential diagnosis includes:• viral encephalitis• bacterial meningitis• brain abscess• septic cavernous sinus thrombosis.
Investigations
Evidence of underlying sinusitis will be presenton plain skull X-ray and CT scan. The CT scan orMRI findings may be subtle, as the abscess is usu-ally iso- or hypodense. The interhemispheric col-lection can easily be overlooked and thus must beconsidered in patients with this sort of clinicalpresentation. There may be contrast enhance-ment of the underlying inflamed membranes and
KAY12 12/16/04 7:44 PM Page 178

evidence of underlying cerebral oedema, al-though these features are not universal.
Lumbar puncture should not be performed ifthe diagnosis is suspected clinically, as it is haz-ardous and frequently not diagnostic. There isusually a pleocytosis in the CSF with elevatedprotein, but the sugar may be normal and organ-isms cannot usually be cultured.
Treatment
Subdural empyema is a surgical emergency. Theprinciples of treatment, as for any abscess, are:• treat the source of sepsis — sinus surgery (if indicated)• drain the abscess• identify the organism• treat with appropriate high-dose antibiotics.
The surgical techniques used to drain the ab-scess are either multiple burr holes, craniotomyor craniectomy. The advantage of the multipleburr hole technique is that the pus may be wide-spread and bilateral and the patient is frequentlyseriously ill. However, it may be difficult to drainthe pus adequately through burr holes, as the underlying oedematous brain may swell up toocclude the hole. In addition, it is difficult to provide adequate drainage for the parafalcinepus, which frequently lies between the falx andthe medial aspect of the hemispheres, throughburr holes.
The subdural space should be irrigated withantibiotic solution at the time of surgery and sub-dural catheters should be left in place for furtherdrainage of pus and postoperative antibiotic irri-gation. It is arguable whether the antibiotic irri-gation is useful but it is probably worthwhile, inview of the seriousness of the situation.
High-dose systemic antibiotic therapy shouldbe commenced as soon as pus is obtained for cul-ture. The initial therapy will depend on the un-derlying cause, as for cerebral abscess, bearing inmind that the most common infecting organismis penicillin-sensitive Strep. milleri from frontal sinusitis. Further antibiotic therapy will dependon the results of the culture.
Anticonvulsant therapy is important as the pa-tients have a high incidence of seizures.
Tuberculosis
Tuberculosis involving the brain is unusual inWestern countries but is not uncommon in India,Africa, Asia, the Middle East, South America andeastern Europe. In developed countries tubercu-losis is more likely to present in patients who are immunocompromised — HIV-positive andimmunosuppressed patients.
The infection may occur as:• tuberculous meningitis• intracranial tuberculomas.
Tuberculous meningitis
Tuberculous meningitis is usually a subacute ill-ness; patients present with headaches, confusionand features of meningitis. It occurs more fre-quently in children and will result in secondarypathological changes and neurological deficit, including:• basal arachnoiditis causing hydrocephalus• visual failure due to arachnoiditis around theoptic pathways• multiple cranial nerve palsies due to the basalarachnoiditis• arteritis causing cerebral infarction.
CSF examination will show:• lymphocytic pleocytosis (100–500 cells/mm3)• elevated protein (greater than 0.8 g/l)• low glucose (less than 2 mmol/l)• low chloride (less than 110 mmol/l)• acid-fast bacilli in 20% of patients using aZiehl–Neelsen stain.
The definitive diagnosis is often only made onculture of M. tuberculosis, which may take up to 6 weeks.
Antituberculous therapy should be com-menced if tuberculous meningitis is suspected, asit is invariably fatal within 6 weeks and is oftenmore rapidly fatal. The antituberculous medica-tion includes isoniazid, rifampicin, ethambutoland pyrazinamide.
Hydrocephalus should be treated with a ven-triculoperitoneal shunt. Steroid therapy has beenused to diminish the risk of arachnoid adhesionsand arteritis but is probably of little benefit. Abrief course may be indicated in patients with
INFECTIONS OF THE CENTRAL NERVOUS SYSTEM 179
KAY12 12/16/04 7:44 PM Page 179

180 CHAPTER 12
raised intracranial pressure. The serum sodiumin older patients may drop, probably due to inap-propriate antidiuretic hormone secretion, andshould be treated by fluid restriction.
Intracranial tuberculoma
An intracranial tuberculoma or abscess origi-nates by haematogenous spread from tubercu-lous lesions in other parts of the body, especiallythe lung. They are frequently multiple and arepredominantly located in the posterior fossa inchildren and young adults, but may occurthroughout the cerebral hemispheres.
The clinical presentation is similar to an in-tracranial tumour, with features of raised in-tracranial pressure, focal neurological signs andepileptic seizures. Systemic symptoms of tuber-culosis, such as fever, excessive perspiration andlethargy, occur in less than 50% of cases.
The CT scan or MRI appearance of a tubercu-lous granuloma will show an area of low attenu-ation with surrounding vasogenic oedema. Theenhancement on this occasion tends to be periph-eral. Once again there may be multiple lesions.There is usually surrounding oedema and the lesions may be multiple. The tuberculoma is occasionally calcified.
The preoperative diagnosis is usually appreci-ated only after recognition of tuberculous focielsewhere in the body.
The optimal treatment is surgical excision ofthe tuberculoma, if it is in a surgically accessibleregion, and antituberculous chemotherapy.
Cerebral cryptococcosis
Cryptococcosis (torula) is a fungal infection thatmay involve the CNS.
Cryptococcus neoformans is commonly found inavian habitats, and particularly among pigeons.The usual portal of entry is by inhalation of theairborne cryptococcus.
Up to half of patients with CNS involvementhave an underlying predisposing condition suchas AIDS, intravenous drug use, sarcoidosis, lym-phoma or prolonged steroid therapy, and somepatients also have cryptococcal lesions in the lung.
Cerebral cryptococcosis presents as:• meningitis• meningoencephalitis• cerebral granuloma.
MeningitisThe most common presentation is meningitis,which is usually subacute, and the patients pre-sent with increasing headaches followed by vomiting, seizures and impaired conscious state.Papilloedema occurs in up to half of patients andcranial nerve palsies may develop.
MeningoencephalitisThis will develop if the meningeal infection ex-tends along the Virchow–Robin spaces into thebrain.
Intracerebral granulomasThese are uncommon in cryptococcal infectionbut may develop in conjunction with meningitisor in isolation (Fig. 12.5).
Patients present with symptoms of raised in-tracranial pressure, convulsions and neurologi-cal deficit including lower cranial nerve palsies.
The CSF studies will show:
Fig. 12.5 Cryptococcal granuloma. A contrast-enhancing mass with surrounding oedema.
KAY12 12/16/04 7:44 PM Page 180

• elevated pressure• pleocytosis — usually lymphocytes• elevated protein• decreased glucose (in 50%)• Cryptococcus neoformans on wet preparationstained with India ink• positive latex cryptococcal agglutination testwhich detects cryptococcal capsular antigen in CSF.
Treatment
Treatment consists of anticryptococcal therapyusing amphotericin B, 5-flucytosine or flucona-zole. Intracerebral granulomas may need to beexcised and a thoracotomy may be necessary fora lung lesion.
Hydrocephalus is a common complication ofcryptococcal infection of the CNS system andshould be treated with a shunt.
Hydatid
Hydatid disease is endemic in rural areas, par-ticularly those involved with sheep and cattleraising such as the western region of Victoria in Australia, South America and South Africa.Echinococcus granulosus is a small tapeworm,about 6 mm long and with approximately foursegments, which lives in the small bowel of ca-nines. The ova are shed in the faeces of dogs andthe intermediate hosts are cattle and sheep, al-though humans may also serve in this capacity.Following ingestion the egg capsule is digestedand the hexocanth oncosphere penetrates theintestinal mucosa and passes into the portal cir-culation. Most are trapped in the liver (65%) orlungs (20%) and less than 5% pass to the bone orCNS. The embryos lodge within the capillariesand will develop into cysts, which progres-sively increase in size. The cyst is filled with the clear hydatid fluid, around which is an inner nucleated germinative layer and an outeropaque non-nucleated layer with delicate lami-nations. Daughter cysts develop from the ger-minative layer (Fig. 12.6). The inflammatoryreaction occurring in the tissue which sur-rounds the laminated layer does not usuallyoccur in the brain.
The neurosurgeon is involved when the hyda-tid cyst lodges in the brain, vertebrae or orbit.
Intracerebral hydatid cyst
Intracerebral hydatid cyst presents as a mass lesion with slowly developing neurological in-volvement. Hydatid cysts in the brain are usuallysingle and large and are often primary. In rare in-stances they are embolic and multiple and canarise from cysts in the left ventricle of the heart.Cysts can also arise from rupture of a cerebralcyst and secondary seedings. The MRI or CT scan(Fig. 12.7) shows a hypodense cyst with minimalor low enhancement around the margins.
The surgical treatment is excision and greatcare should be taken to remove the cyst intact. Ifthe contents are spilled the hydatid disease maybe disseminated through the CNS and anaphy-lactic shock has occasionally been reported.
Orbital involvement is usually manifest byunilateral proptosis. If the vertebral column is in-volved there will be destruction of cancellousbone with vertebral collapse and possible cordcompression.
If cerebral hydatid disease is suspected, clinicalexamination and radiological investigation mayshow involvement of the liver and lung. Serolog-ical investigations help in the diagnosis.
INFECTIONS OF THE CENTRAL NERVOUS SYSTEM 181
Fig. 12.6 Hydatid daughter cyst or ‘brood capsule’.
KAY12 12/16/04 7:44 PM Page 181

182 CHAPTER 12
Medical therapy is with prolonged use of albendazole.
AIDS
Acquired immune deficiency syndrome (AIDS)is due to the T-cell lymphotrophic virus type III,also known as the human immunodeficiencyvirus (HIV) type I.
The virus attacks the patient’s immune system,rendering the patient prone to opportunistic infection or malignancy. The virus is also neu-rotrophic and can involve the CNS directly. Approximately 10% of patients are diagnoseddue to CNS symptoms at presentation and up to70% of patients have central nervous symptomsat death.
CNS manifestations have several causes.• Secondary infection. The most common infec-tion is Toxoplasma gondii, which is a mass lesionand may present with features indistinguishablefrom a tumour. The lesions may be solitary ormultiple and are usually ring-enhancing on CT
scan and MRI (Fig. 12.8). Cerebral toxoplasma infections are treated with sulfadiazine andpyrimethamine. Cryptococcus neoformans is thesecond most common cause of CNS infection andother infections include tuberculosis, Candida al-bicans, herpes simplex encephalitis (Fig. 12.9) andprogressive multifocal leukoencephalopathy.• Malignant disease of the brain may be eitherprimary CNS lymphoma, secondary lymphomafrom systemic disease or secondary Kaposi’s sarcoma.• The AIDS virus may infect the nervous systemdirectly, causing the AIDS dementia complex in
Fig. 12.7 Hydatid cyst in frontal lobe extending intothe lateral ventricle.
Fig. 12.8 MRI following gadolinium showingintracerebral toxoplasmosis.
Fig. 12.9 MRI of herpes simplex encephalitis withmajor involvement of the right temporal lobe and lesssevere changes in the left temporal lobe.
KAY12 12/16/04 7:44 PM Page 182

over 90% of patients. This may present as a be-havioural change similar to presenile dementia.Transverse myelitis and peripheral neuropathymay also occur.
The advisability of biopsy of intracerebral le-sions in AIDS patients and the possible benefitsare not clear at this stage, as there is no satisfac-tory treatment of the underlying disease process.A reasonable approach is to treat HIV-positivepatients with cerebral lesions that have the radio-logical appearance typical of toxoplasmosis withtherapy for Toxoplasma infection, and to reservebiopsy for patients who do not respond to therapy, or if the radiological appearance is atypical for toxoplasmosis.
Neurocysticercosis
This is the most common parasitic disease of thecentral nervous system. It is caused by the larvalstage of a tapeworm Taenia solium. Human beingsare the only definitive host for this parasite,whilst both humans and pigs are the intermedi-ate hosts for the embryonic form. Infestation oc-curs by eating poorly cooked infested food orthrough contamination of food by fertilizer con-taining the eggs. The larva penetrates the intesti-nal wall and gains access to brain, muscle or eyevia the bloodstream.
There are multiple forms of neurocysticercosis,the commonest form being parenchymal disease.However, the cyst can also be concentrated in thesubarachnoid space, intraventricular space, in-trasellar region or spinal canal.
Neurocysticercosis commonly has multiplecysts at various stages of the disease process fromcalcified lesions to cysts of varying sizes in vary-ing locations and often variations in terms of en-hancement (when present).
The lesions can present with hydrocephalus,coma, convulsions and neurological deficits.
A lumbar puncture examination of the CSF canbe diagnostic provided it is not contraindicated.This cyst can occasionally be found in the CSF; however, the presence of a lymphocytosis,eosinophilia and a positive complement fixationtest will contribute to the diagnosis.
Surgical intervention is indicated for mass
lesions or hydrocephalus. Medical treatment iswith albendazole or praziquantel. Steroids areused in the early stage of treatment to attenuatethe acute inflammatory response.
Herpes simplex encephalitis
This viral infection can present with rapid onsetof fever, headaches, vomiting and progressiveneurological deterioration. The type 1 virus is thecausative organism in most of the adult cases. Itpresents as an acute necrotizing encephalitis andhas a high morbidity and mortality in the absenceof early antiviral therapy.
Patients present with symptoms of meningitis,a progressive deteriorating neurological stateand seizures. Diagnosis can be reached with elec-troencephalography that reveals focal slowing,periodic spikes or sharp and wave patterns. CT scanning can be normal initially or revealoedema-like changes in the temporal or frontallobes. This can be associated with areas of haem-orrhage. MRI is the investigation of choice, re-vealing the signal changes within the temporallobe with oedema and haemorrhage (Fig. 12.9).The diagnosis is confirmed by the presence ofmononuclear cells in the CSF and the detection ofviral DNA. Early treatment with aciclovir is thetreatment of choice and can be life-saving. Veryrarely does the patient develop raised pressure to the extent of requiring intracranial pressuremonitoring, ventricular drain or a decompres-sive craniotomy.
Further readingBecker GL et al. (1980) Amoebic abscesses of the brain.
Neurosurgery 6, 192–194.Bell WE (1981) Treatment of bacterial infections of
the central nervous system. Annals of Neurology 9,313–327.
Brown E (1987) Antimicrobial prophylaxis in neuro-surgery. British Journal of Neurosurgery 1, 159–162.
Chan KH, Mann KS, Yue DP (1989) Neurosurgical aspects of cerebral cryptococcosis. Neurosurgery 25,44–48.
Everett ED, Stausbaugh LJ (1980) Antimicrobial agentsand the central nervous system. Neurosurgery 6,691–714.
INFECTIONS OF THE CENTRAL NERVOUS SYSTEM 183
KAY12 12/16/04 7:44 PM Page 183

184 CHAPTER 12
Garvey G (1983) Current concepts of bacterial infec-tions of the central nervous system. Journal of Neuro-surgery 59, 735–744.
Gotvai P, De Louvis J, Hurley R (1987) The bacteriologyand chemotherapy of acute pyogenic brain abscess.British Journal of Neurosurgery 1, 189–204.
Haines SJ (1989) Efficacy of antibiotic prophylaxis inclean neurosurgical operations. Neurosurgery 24,401–405.
Hlavin ML, Kaminski HJ, Fenstermaker RA, White RJ(1994) Intracranial suppuration: a modern decade ofpostoperative subdural empyema and epidural ab-scess. Neurosurgery 34, 974–981.
Mampalam TJ, Rosenblum ML (1988) Trends in the
management of bacterial brain abscesses: a review of102 cases over 17 years. Neurosurgery 23, 451–458.
Mandel GL, Douglas RG, Bennett JE (1985) Principlesand Practice of Infectious Diseases, 2nd edn. John Wiley,New York.
Richards P (1987) AIDS and the neurosurgeon. BritishJournal of Neurosurgery 1, 163–172.
Rosenblum ML, Levy RM, Bredesen DE (1986) Neuro-logical implications of the acquired immunodefi-ciency syndrome (AIDS). Clinical Neurosurgery 34,419–445.
Stephanov S (1988) Surgical treatment of brain ab-scesses. Neurosurgery 22, 724–730.
KAY12 12/16/04 7:44 PM Page 184

About 90% of the population suffer from low back pain at some time and 30% of these will develop leg pain due to lumbar spine pathology.
The critical factor in assessing patients withlow back pain is whether there are also features oflumbosacral nerve root compression, such as legpain or focal signs of neural compression in thelower limbs. In general, neurosurgeons are prin-cipally concerned with lumbar spine pathologythat causes nerve root compression.
Sciatica is the clinical description of pain in theleg due to lumbosacral nerve root compressionwhich is usually in the distribution of the sciaticnerve. Sciatica was first mentioned in an Egypt-ian manuscript dated 2500–3000 BC. In 1934 Mixter and Barr established that a prolapsedlumbar intervertebral disc was commonly thecause of sciatica.
Lumbar canal stenosis, a narrowing of the lum-bar spinal canal, is the other major spinal cause ofleg pain. In 1949 Verbiest specifically defined theclinical significance of the narrow spinal canaland the syndrome of intermittent neurogenicclaudication of the legs.
A lumbar disc prolapse can occur at any age inadults but is uncommon in teenagers. The symp-toms of lumbar canal stenosis usually commenceafter the 5th decade. Although lumbar canalstenosis and lumbar disc prolapse may be pre-sent in the same patient, they each produce a distinct clinical entity which will be describedseparately.
Sciatica
Aetiology (Table 13.1)
The most common cause of sciatica is a lumbardisc prolapse causing nerve root compression.Sciatica-type pain may also occur as a result ofbony compression of the nerve root, usually byan osteophyte, and is often associated with lum-bar canal stenosis or spondylolisthesis. Narrow-ing of the ‘lateral recess’ of the spinal canal may also occur in conjunction with lumbar canalstenosis, and may cause compression of a nerveroot. Sciatica may occasionally be caused by tu-mours of the cauda equina or by pelvic tumours,such as spread from carcinoma of the rectum.
Anatomy and pathology
Nearly 75% of the lumbar flexion–extension andof total spinal movement occurs at the lumbo-sacral junction, 20% of lumbar flexion–extensionoccurs at the L4/5 level and the remaining 5% isat the upper lumbar levels. Consequently, it is notsurprising that 90% of lumbar disc prolapsesoccur at the lower two lumbar levels; the mostfrequently affected disc is at the L5/S1 level.
The lumbar disc consists of an internal nucleuspulposus surrounded by an external laminar fibrous container, the annulus fibrosus. A disc prolapse may consist of the nucleus pulposusbulging, with the annulus being stretched but intact. Alternatively, the nucleus may rupturethrough the annulus and sequestrate as a freefragment under the posterior longitudinal liga-ment or lie in the extradural space. Prolapse of
CHAPTER 13
13 Low back pain and leg pain
185
KAY13 12/16/04 7:44 PM Page 185

186 CHAPTER 13
the disc is usually in a posterolateral direction, asthe posterior longitudinal ligament prevents direct posterior herniation. Less frequently thedisc may herniate laterally to trap the nerve in the neural foramen.
A prolapsed intervertebral disc causes com-pression of the nerve which runs along the posterior aspect of the disc and down under the pedicle of the vertebra below (Fig. 13.1). Con-sequently, an L4/5 posterolateral intervertebraldisc prolapse will usually compress the L5 nerveroot, which runs caudally across the disc to enterthe neural foramen below the L5 pedicle. Simi-larly, a lumbosacral (L5/S1) disc prolapse willusually affect the S1 nerve root. The less commonlateral disc prolapse will cause compression ofthe nerve root at one level higher than expected(e.g. L4 nerve root compression due to L4/5 lateral disc prolapse). In the case of a large discprolapse, there may be evidence of more than one nerve root compression.
Cauda equina compression may result if thedisc herniation is sufficient to rupture the pos-terior longitudinal ligament and produce a pos-terior central disc prolapse.
Patient assessment
The patient suffering from sciatica will be in ob-vious discomfort, which will be reflected bymovements and posture when lying supine. Thepatient lies tilted, usually to the side opposite tothe sciatica, with the affected hip and knee slightly flexed taking pressure off the stretchednerve. The pain is worse on movement, cough-ing, sneezing or straining. Although back pain
may be present, the important feature is the painwhich radiates down the leg in the distribution ofthe affected nerve. The pain usually radiates intothe buttock, along the posterolateral aspect of thethigh and calf into the foot (S1 nerve root); it mayextend into the dorsum of the foot and great toe(L5 nerve root). An L3/4 disc herniation may pro-duce pain in the posterior thigh but, as with anL2/3 disc prolapse, the pain is frequently alongthe anterior aspect of the thigh. L4 root pain fre-quently radiates into the anterior aspect of thelower leg. Depending on the degree of nerve rootcompression, the patient may complain of senso-ry disturbance such as numbness or tingling inthe leg or foot, and weakness may be present. Thehistory must include an assessment of sphincterfunction, as a large disc prolapse may causecauda equina compression.
Examination features
Lumbar back movements may be restricted and ascoliosis may be seen, usually concave to the sideof the affected leg. Straight leg raising (Lasegue’stest) will be restricted on the affected side and, insevere cases, pain in the affected leg will be re-produced when the opposite leg is raised.
Table 13.1 Causes of sciatica.
Prolapsed lumbar discLumbar spondylosis (osteophyte)Lumbar canal stenosis (lateral recess)Lumbar spondylolisthesisCauda equina tumours (e.g. ependymoma)Pelvic tumours (e.g. rectal carcinoma)Spinal arteriovenous malformation (rare)
(a) (b)
Fig. 13.1 The diagram shows (a) a posterolaterallumbar disc proplapse causing compression of lumbarnerve root passing across the disc to enter the neuralcanal below the pedicle and (b) a lateral disc prolapsecausing compression of the nerve root passing beneaththe pedicle above the disc prolapse.
KAY13 12/16/04 7:44 PM Page 186

Examination of the neurological disabilityshould proceed in an ordered fashion. Initially asearch is made for ‘wasting’ in specific musclegroups, particularly the quadriceps, calf muscles,extensor digitorum brevis muscle and the smallmuscles of the foot. The patient is then examinedfor weakness in each of the muscle groups (Tables13.2 and 13.3). Weakness of dorsiflexion of thefoot and extension of the great toe (extensor hallucis longus) is most commonly caused by a prolapsed L4/5 intervertebral disc with in-volvement of the L5 nerve root; severe cases mayresult in a complete foot drop.
Plantar flexion weakness is caused by com-pression of the S1 nerve root, usually due to aprolapsed lumbosacral disc. However, plantarflexion is a very strong movement and any weak-ness may be difficult to elicit unless tested by ask-ing the patient to stand on the toes of the affectedside. A large prolapsed disc at the L4/5 level mayresult in some plantar flexion weakness becauseof compression of the S1 nerve root, and simi-larly a large lumbosacral disc prolapse may be associated with dorsiflexion weakness due to L5nerve root compression.
The deep tendon reflexes should be carefullytested as they provide objective evidence ofnerve root compression. The ankle jerk is de-pressed or absent when the S1 nerve root is com-pressed, usually by a lumbosacral disc prolapse.
Sensation should be tested in the foot and leg(Fig. 13.2).
At the end of the examination the patientshould be turned prone so that the buttocks canbe inspected for atrophy of the gluteal muscles,sensation can be tested along the back of the legsand in the perianal region, and anal tone can beassessed. A rectal examination should be per-formed if there are clinical features suggestive ofa pelvic tumour.
LOW BACK PAIN AND LEG PAIN 187
Table 13.2 Segmental innervation of lower limb musculature.
L1 Psoas major; psoas minorL2 Psoas major; iliacus; sartorius; gracilis; pectineus; adductor longus; adductor brevisL3 Quadriceps; adductors (magnus, longus, brevis)L4 Quadriceps; tensor fasciae latae; adductor magnus; obturator externus; tibialis anterior; tibialis
posteriorL5 Gluteus medius; gluteus minimus; obturator internus; semimembranosus; semitendinosus; extensor
hallucis longus; extensor digitorum longus and peroneus tertius; popliteusS1 Gluteus maximus; obturator internus; piriformis; biceps femoris; semitendinosus; popliteus;
gastrocnemius; soleus; peronei (longus and brevis); extensor digitorum brevisS2 Piriformis; biceps femoris; gastrocnemius; soleus; flexor digitorum longus; flexor hallucis longus;
some intrinsic foot musclesS3 Some intrinsic foot muscles (except abductor hallucis; flexor hallucis; brevis; flexor digitorum brevis;
extensor digitorum brevis)
Table 13.3 Segmental innervation of lower limbjoint movements.
Hip Flexors, adductors, medial L1, 2, 3rotators
Extensors, abductors, lateral L5, S1rotators
Knee Extensors L3, 4Flexors L5, S1
Ankle Dorsiflexors L4, 5Plantar flexors S1, 2
Foot Invertors L4, 5Evertors L5, S1Intrinsic muscles S2, 3
KAY13 12/16/04 7:44 PM Page 187

188 CHAPTER 13
Summary of clinical features
Clinical localization of the disc prolapse shouldbe possible in the majority of patients with scia-tica. The following features are typical (but notinvariable) of disc herniation.
L5/S1 prolapsed intervertebral disc• Pain along the posterior thigh with radiation tothe heel• Weakness of plantar flexion (on occasion)• Sensory loss in the lateral foot• Absent ankle jerk.
L4/5 prolapsed intervertebral disc• Pain along the posterior or posterolateral thighwith radiation to the dorsum of the foot and greattoe• Weakness of dorsiflexion of the toe or foot• Paraesthesia and numbness of the dorsum ofthe foot and great toe• Reflex changes unlikely.
L3/4 prolapsed intervertebral disc• Pain in the anterior thigh• Wasting of the quadriceps muscle• Weakness of the quadriceps function and dor-siflexion of foot• Diminished sensation over anterior thigh,knee and medial aspect of lower leg• Reduced knee jerk.
Management
Most patients with sciatica achieve good pain relief with simple conservative treatment andless than 20% will require surgery. The likelihoodof symptomatic relief without surgery is relatedto the pathology of the disc prolapse. A ‘bulging’disc is likely to settle with simple conservativemeasures, but sciatica due to a nucleus pulposusthat has herniated out of the disc space and ‘se-questrated’ outside the annulus will probablyneed surgery for satisfactory relief of symptoms.
Conservative treatmentMost patients achieve good pain relief followingbed rest, usually for a period of about 7–10 days,and the use of simple analgesic agents and non-steroidal anti-inflammatory medication. Al-though traction is sometimes recommended itprobably has only limited benefit and may resultin lower leg complications. Resolution of thepain is probably due to a combination of some resorption of the prolapsed disc material, theoedema of the nerve decreasing and possibleadaptation of the pain fibres to pressure. Spinalmanipulation is not recommended and the con-cept that a disc prolapse can be ‘reduced’ by ma-nipulation is a myth. Initially, the only necessaryinvestigations are a plain lumbar spine X-ray andan erythrocyte sedimentation rate (ESR). Thelumbar spine X-ray will diagnose an associatedspondylolisthesis which may contribute to thesciatica, and it also helps to exclude sinisterpathology, such as metastatic tumour involvingthe spinal vertebrae. The ESR will also excludesystemic disease.
Some clinicians advocate the use of high-dosecorticosteroids in the conservative managementof sciatica due to lumbar disc prolapse. Whilst
L1
L2
L3
L4
L5
L5
S3
S2
S1
S4
S1
Dorsalaxialline
Ventralaxialline
Extensionforwardsfrom dorsalaxial line
L5
L2
L5
L3
L4
Fig. 13.2 Segmental distribution of nerves of thelumbar and sacral plexuses to the skin of the anteriorand posterior aspect of the lower limb.
KAY13 12/16/04 7:44 PM Page 188

steroid therapy may help to give transient painrelief, the limited benefit is probably outweighedby the possible complications of corticosteroidtreatment.
Chemonucleolysis has, in the past, been advo-cated as a treatment for lumbar disc prolapse. Itinvolves the intradiscal injection of a proteolyticenzyme, such as chymopapain, which dissolvesdisc material. Chymopapain was first isolated in1941 and has been used intermittently since 1963in clinical studies. There is a small risk of seriousanaphylactic reaction following intradiscal injec-tion. Although chymopapain dissolves the nor-mal nucleus pulposus it has a high failure rate inthe treatment of prolapsed disc, as it fails to affectthe extruded disc material, and further nervecompression may occur following chemonucle-olysis from the disc dissolving and collapsing, re-sulting in narrowing of the intervertebral neuralforamen. The procedure is not recommended foruse at this time.
Indications for surgeryPain. The most common indication for surgery inpatients with disc prolapse is pain in the follow-ing situations.• Incapacitating pain despite 7–10 days of bedrest.• Continuing episodes of recurrent pain when
mobilizing despite adequate relief with bed rest.In this group of patients physiotherapy and alimited trial of a spinal brace might be tried, butthey usually have only limited success.
Neurological deficit. A significant weakness or in-creasing amount of weakness is an indication forearly investigation and surgery.
Central disc prolapse. Patients with bilateral sciati-ca or other features indicating a central disc prolapse, such as sphincter disturbance and di-minished perineal sensation, should be investi-gated promptly. An acute central disc prolapsemay lead to acute, severe, irreversible caudaequina compression and should be investigatedand treated as an emergency.
Tumour. Surgery is indicated if the clinical fea-tures suggest that a tumour could be the cause ofsciatica.
Investigations
Lumbar myelography (Fig. 13.3) was the time-honoured investigation for lumbar disc prolapse.The use of water-soluble non-ionic contrast material avoids the risk of the postmyelogramarachnoiditis previously seen with the oil-based
LOW BACK PAIN AND LEG PAIN 189
Fig. 13.3 Lumbar myelogram using water-soluble contrast medium showing (a) posterolateral L4/5 discprolapse and (b) complete block due to a large central L5/S1 disc protrusion.
(a) (b)
KAY13 12/16/04 7:44 PM Page 189

190 CHAPTER 13
mediums. Although myelography is now muchsafer, there is a very small risk of reaction to thecontrast medium, particularly epileptic seizures.Some patients suffer headaches following themyelogram. These are due to the lumbar punc-ture (Chapter 2) and/or the effects of the contrastmaterial.
High-quality computerized tomography scan-ning (Figs 13.4 and 13.5) and magnetic resonanceimaging (Fig. 13.6) have largely supersededmyelography for the diagnosis of lumbar discprolapse. The MRI is especially helpful in show-ing the size, configuration and position of the discprolapse, as well as any associated nerve root orthecal compression. In addition the MRI will alsodemonstrate pathology at other discs, such as de-generative changes as evidenced by decreasedsignal in the disc on the T2-weighted scans.
Operative procedure for lumbar disc prolapse
The operation involves excision of the disc pro-lapse with decompression of the affected nerveroot.
In the past the operation usually entailed acomplete or partial laminectomy, identificationof the compressed nerve root, its mobilization offthe disc prolapse and excision of the herniateddisc. However, with improvements in instru-mentation and magnification, e.g. the operatingmicroscope, most disc prolapses can be excisedwith minimal disturbance to the normal bonyanatomy and with the removal of only a smallamount of bone, usually from the adjacent lami-nae on the side of the prolapse.
A full laminectomy may occasionally be neces-sary prior to the disc excision of a large centraldisc prolapse causing cauda equina compression.
A percutaneous lumbar discectomy to removethe nucleus pulposus is sometimes advocated forthe ‘bulging’ lumbar disc. However, if the disc is‘bulging’ the sciatica will nearly always settlewith conservative treatment and surgery is notnecessary. A percutaneous discectomy of the in-tradiscal contents will fail to relieve the sciatica ifthe disc has ruptured through the annulus, be-cause it will not remove the herniated disc mate-rial causing the nerve root compression.
Fig. 13.4 (a) CT scans of lumbar spine showingposterolateral disc prolapses. (b) CT scan of leftposterolateral disc prolapse after intrathecal contrast.
(a)
(b)
Postoperative mobilization
Most patients commence walking the day aftersurgery and are discharged from hospital on day2 or 3 following the operation. A gently graduat-ed mobilizing programme should be carefully
KAY13 12/16/04 7:45 PM Page 190

and straining for the first 4 weeks. A graduatedactive exercise programme can commence afterthe first month.
Prognosis following surgery
The results following lumbar disc surgery are directly related to the accuracy of the preopera-tive clinical evaluation. Excellent results can beachieved if:• there is a good history of sciatica• there are good signs of nerve root irritation• the investigations show evidence of a herniated disc• at surgery the nerve root is stretched by a discprolapse• the patient is well motivated.
If any of the above criteria are absent the resultsfollowing surgery are disappointing.
Recurrent sciatica following surgery occurs inabout 10% of cases and is usually due to furtherdisc prolapse, either at the same level or at another level. The principles of management aresimilar to those described for the initial treatmentof sciatica. Recurrent sciatica is sometimes due toadhesions developing around the nerve rootcausing perineural fibrosis. The treatment is con-servative, with judicious use of bed rest followedby gentle mobilizing exercises, simple analgesicmedication and non-steroidal anti-inflammatoryagents. Surgery to excise the adhesions is suc-cessful in relieving the pain in less than 60% ofpatients.
Rarely, recurrent sciatica is due to intraduralarachnoiditis. Treatment is conservative andsurgery to divide the intradural adhesion israrely successful.
Lumbar canal stenosis
The patient with lumbar canal stenosis usuallycomplains of pain radiating diffusely into thelegs, particularly when standing or walking. Thepain may be a diffuse ache, or is sometimes de-scribed as having a ‘burning’ quality; it is usuallyrelieved with sitting and patients often adopt aposture of bending the body forward when walk-ing to help relieve the discomfort. The pain may
LOW BACK PAIN AND LEG PAIN 191
Fig. 13.5 CT scan of left lateral disc prolapse.
Fig. 13.6 MRI of lumbar disc prolapse.
explained to the patient, often with the help of aphysiotherapist. Gentle back strengthening exer-cises commence after 10 days, and the patientshould avoid prolonged periods of sitting, lifting
KAY13 12/16/04 7:45 PM Page 191

192 CHAPTER 13
be similar to that described by patients with vas-cular occlusive disease, although a key feature isthe presence of pain when standing only.
On occasions there may be features of sciatica-like pain in association with the diffuse pain oflumbar canal stenosis due to entrapment of anerve root by an osteophyte or within the ‘lateralrecess’ of the canal.
The patient often complains of a subjectivefeeling of weakness and of a diffuse ‘numbness’and ‘tingling’ radiating down the legs. Sphincterdifficulties may occur if the stenosis is particul-arly severe.
Examination findings
The examination of the lower limbs and backoften reveals little or no abnormality. Focal wast-ing may occur in the lower limbs if the compres-sion is severe, and the ankle jerks may bedepressed or absent. Definite sensory disturbanceor weakness occur only in the most severe cases.
The peripheral pulses should be checked as thesymptoms may mimic those due to peripheralvascular disease.
Pathology and anatomy
The stenosis of the lumbar canal may involve re-duction of the sagittal diameter of the canal, nar-rowing of the ‘lateral recess’ and stenosis of theneural foramen. The pathology is frequently dueto a combination of congenital canal stenosis anddegenerative pathology, such as lumbar spondy-losis with hypertrophy of the facet joints and ligamentum flavum, osteophyte formation andthickening of the laminae causing further nar-rowing of the canal and bulging of the discs suchthat the space for the neural elements becomescompromised.
The most frequently affected levels are L4/5and L3/4. The lumbosacral level may be in-volved, but this is less common. The stenosis mayalso be related to a degenerative spondylolisthe-sis, particularly at the L4/5 level.
Management
The clinical diagnosis of lumbar canal stenosis is
usually straightforward, but it should be con-firmed by radiological investigations. High-quality CT scanning (Fig. 13.7) and MRI (Fig.13.8) have replaced the need for myelography(Fig. 13.9). All these radiological studies demon-strate the canal stenosis. The myelogram willshow marked indentation of the contrast columnand, if the stenosis is severe, there may be a com-plete block to the flow of contrast. The MRI willshow the extent and severity of the stenosis aswell as other pathology related to the lumbardiscs such as degenerative disease and prolapse.
The clinical features of lumbar canal stenosisdo not respond favourably to conservative treat-ment, and surgery is almost invariably successfulin relieving the symptoms. The operation con-sists of a decompressive lumbar laminectomy extending over the whole region of the stenosiswith decompression of the lumbar theca andnerve roots.
The patient can be mobilized promptly afterthe operation and a course of gently graduatedactive exercises prescribed, usually with the helpof a physiotherapist.
Back pain
Low back pain without leg pain or signs of nerveroot compression is a common problem. Theusual presentations are:
Fig. 13.7 CT scan of lumbar spine showing severelumbar canal stenosis.
KAY13 12/16/04 7:45 PM Page 192

• acute low back pain, often following minortrauma• chronic or recurrent low back pain.
Acute sudden-onset back pain, following a rec-ognized episode of trauma, is usually due to softtissue strain. If the injury was severe it may havecaused a fracture or disc herniation. The manage-ment of patients with an acute onset of back painfollowing trauma involves:• history and examination to exclude symptomsand signs of nerve root compression
LOW BACK PAIN AND LEG PAIN 193
Fig. 13.8 MRI showing severe canal stenosis.
Fig. 13.9 Lumbar myelogram showing lumbar canalstenosis.
KAY13 12/16/04 7:45 PM Page 193

194 CHAPTER 13
• radiological evaluation to exclude fracture ordisc herniation (if severe trauma)• conservative management with initial bed restfollowed by gentle mobilization and simple anal-gesic medication.
Most of the pain and stiffness should settleafter a few days, although mild discomfort maylinger for some weeks.
The more difficult problem is chronic or recur-rent back pain, where the patient gives a historyof less severe or even trivial trauma. In somecases no pathological cause will be found. Themost common aetiology is degenerative diseasewhich includes:• lumbar spondylosis• spondylolisthesis• degenerative disc disease.
Other uncommon but important causes of lowback pain which, in the early stages, may presentwithout pain radiating into the legs or radicularsigns, include:• spinal tumours (Chapter 15)• thoracic disc prolapse (Chapter 15)• spinal abscess (Chapter 15)• arteriovenous malformation (Chapter 15).
These serious but unusual causes may presentwith acute or chronic back pain but nearly alwayshave other features, e.g. symptoms or signs ofnerve root involvement, which would alert the
clinician to the possibility of a more sinister basisfor the back pain.
Intra-abdominal pathology should also be con-sidered in patients presenting with back pain, especially:• pancreatic disease — pancreatitis or tumours• aortic aneurysm• renal disease — calculus, infection or tumour.
Lumbar spondylosis, a degenerative diseaseinvolving the vertebral column, is the mostcommon demonstrable cause of low back pain.The arthritic process may involve any of thespinal joints and be associated with degenera-tive disc disease. Low back pain, without fea-tures of sciatica, is only rarely caused by discprolapse, and then only if the prolapse is largeand central.
Spondylolisthesis
Spondylolisthesis is a subluxation of one verte-bral body on another, usually involving the L4 orL5 levels, and may be due to congenital defectsinvolving the neural arch or to degenerativechanges. Spondylolysis describes a defect in thepars interarticularis, often the precondition forspondylolisthesis (Fig. 13.10).
Various classifications have been used to categorize spondylolisthesis; most subdivide the
Fig. 13.10 Lumbar spondylolysis with bilateral defects in thepars interarticularis.
(a)
(b)
KAY13 12/16/04 7:45 PM Page 194

forms into those of congenital and those of de-generative origin (Table 13.4).
The congenital dysplastic variety results fromcongenital deficiencies of the superior facets ofthe sacrum or the inferior facets of the 5th lumbarvertebra. The lumbosacral junction is incapableof withstanding the truncal forces imposed bythe erect stance and there is gradual forward slip-page of the 5th vertebral body. This is frequentlyassociated with spina bifida occulta of L5 or S1.The congenital isthmic category involves a defectof the pars interarticularis, either a lytic fatiguefracture or, rarely, when the interarticularis frac-ture occurs following severe trauma.
Afurther subtype is when the pars is elongatedbut intact.
Degenerative spondylolisthesis, also known aspseudospondylolisthesis, results from severe localized arthritis of the facets (apophysealjoints) of the slipped vertebrae.
Radiological investigations, including plain X-rays, CT scan and MRI, will show the type ofspondylolisthesis, the amount of slippage andthe associated narrowing of the neural canals(Fig. 13.11). The degree of subluxation is com-monly described by the percentage of slip (Tail-lard method) or assigned a grade (I–IV) based onthe number of quarters of the adjacent bodyspanned by the slip.
Clinical presentationThe presenting features involve back pain andleg pain. The initial symptom is usually back
pain, which may radiate into the buttocks, butpatients often complain of a ‘tight’ feeling in theupper thighs. Symptomatic children and adoles-cents often have a gait disturbance, the so-called‘tight hamstring’ syndrome.
The vertebral slippage may produce compres-sion of the lumbar nerve roots in the neural fora-men. This causes sciatica, the symptoms of whichmay be indistinguishable from those due to discprolapse. Narrowing of the bony canal may result in clinical symptoms of ‘lumbar canalstenosis’.
TreatmentChildren and adolescentsIn the majority of children and adolescents
LOW BACK PAIN AND LEG PAIN 195
Table 13.4 Classification of spondylolisthesis.
CongenitalDysplastic Congenital deficiency of superior facet of sacrum or inferior facet of 5th lumbar vertebraIsthmic Lesion in pars interarticularis
Lytic fatigue fractureElongated but intact parsAcute fracture
Degenerative In adults, usually at L4/5; a cause of lumbar canal stenosis
Traumatic
Pathological Paget’s disease, neoplastic, osteogenesis imperfecta and achondroplasia
Fig. 13.11 CT scan showing lumbar spondylolisthesis
KAY13 12/16/04 7:45 PM Page 195

196 CHAPTER 13
symptomatic spondylolisthesis responds to con-servative treatment. The following indicationsare guidelines for lumbar fusion.• Pain unrelieved by conservative measures.• Progression of subluxation on serial radiologi-cal studies.• Subluxation of greater than 30%.• Tight hamstring gait.
The usual surgical procedure is a spinal fusion.Only rarely is a laminectomy necessary, and itshould never be performed unless the spine isfused as there will be a progressive slip.
AdultsIn most patients conservative therapy involvingshort periods of bed rest during exacerbations ofdiscomfort, gentle mobilizing exercises, simpleanalgesic medication and non-steroidal anti-in-flammatory medication will be sufficient. If somepain persists following bed rest a period with aproperly fitted lumbar brace may be of value.Surgery involves either a laminectomy to decom-press the neural structures and/or a spinal fusion to prevent instability. The indications forlaminectomy include:• symptomatic spinal canal stenosis (that is,symptoms of lumbar canal stenosis)• clinical features of nerve root compression(e.g. sciatica) unrelieved by conservative therapy.
A laminectomy decompresses the lumbartheca and nerve roots, usually with satisfactoryrelief of lower limb symptoms. However, alaminectomy may increase the instability andsome surgeons prefer to combine a decompres-sive laminectomy with a spinal fusion. An intertransverse fusion between the transverseprocesses has been the traditional method of fusion, but more recently internal pedicle screwfixation and/or interbody ‘cages’ placed in theemptied disc space between the vertebral bodieshave become the preferred method.
Spinal fusion, without laminectomy, is occa-sionally indicated and should be considered inpatients with the following conditions.• Incapacitating low back pain unrelieved by
conservative treatment, where the radiologicalfindings show a relative absence of degenerativedisease as a cause for the pain. This is an uncom-mon situation since, in most cases, it is not possi-ble to identify that the spondylolisthesis is thesole cause of the back pain.• Documented progressive subluxation. This isuncommon in adults but is a definite indicationfor spinal fusion.
In general, the treatment of symptomatic gradeI spondylolisthesis by fusion and fixation re-mains controversial and should be considered onan individual basis. Symptomatic patients with agrade II slip usually benefit from surgery, andsymptomatic patients with grade III or IV benefitgreatly.
Further readingBogduk N (2004) Management of chronic low back
pain. Medical Journal of Australia 180 (2), 79–84.Branch CL, Handley EN, Ducker T (1995) Treatment of
lumbosacral spondylolisthesis. In: Al-Mefty O, Orig-itano TC, Harkey HL, eds. Controversies in Neuro-surgery. Thieme, New York.
Hardy RW (1982) Lumbar disc disease. Seminars in Neuro-logical Surgery. Raven Press, New York.
Kaye AH, Black P McL (2000) Operative Neurosurgery.Churchill Livingstone, London, New York, Edinburgh.
Maroon JC, Young P, Tarlov E, Haines SJ (1995) Treat-ment of lumbar disc protusion, percutaneous discec-tomy, microdiscectomy, conservative treatment. In:Al-Mefty O, Origitano TC, Harkey HL, eds. Contro-versies in Neurosurgery. Thieme, New York.
Mixter W, Barr J (1934) Rupture of the intervertebraldisc with involvement of the spinal canal. New Eng-land Journal of Medicine 211, 210–214.
Sherman FC, Rosenthal RK, Hall JE (1979) Spine fusionfor spondylolysis and spondylolisthesis in children.Spine 4, 59–67.
Vierbiest H (1954) A radicular syndrome from develop-mental narrowing of the lumbar vertebral canal.Journal of Bone and Joint Surgery 36B, 230–237.
Wiltse LL, Newman PH, MacNab I (1976) Classificationof spondylolysis and spondylolisthesis. Clinical Or-thopaedics 177, 23–29.
KAY13 12/16/04 7:45 PM Page 196

Cervical spine disorders predominantly causeneck pain and/or arm symptoms. Cervical discprolapse and cervical spondylosis are the twocommon cervical spine disorders. Degenerativechanges in the vertebral column are the basic un-derlying pathological processes in both theseconditions. Although the two conditions may bedistinct clinical entities, the shared commonpathogenetic mechanism results in a spectrum ofclinical presentation depending upon whetherthe degenerative disease has resulted primarilyin disc rupture or cervical spondylosis. As in thelumbar region the critical clinical feature de-pends on whether there is nerve root entrapmentcausing arm pain and/or focal signs of neuralcompression in the upper limb. Cervical cordcompression due to disc prolapse or cervicalspondylosis is discussed in Chapter 15.
Cervical disc prolapse
In the 1934 report of their experiences with rup-tured intervertebral discs, Mixter and Barr described four cases with cervical disc disease.Prolapse of an intervertebral disc is less commonin the cervical region than in the lumbar area. The disc herniation occurs most frequently at the C6/7 level and slightly less commonly at theC5/6 level. Disc herniation above these levelsand at the C7/T1 level is much less common. Thepredominant frequency of disc prolapse at C6/7and C5/6 is due to the force exerted at these levels which act as a fulcrum for the mobile spine and head.
Anatomy and pathology
The structure of the cervical disc is essentially thesame as in the lumbar region and consists of aninternal nucleus pulposus surrounded by the ex-ternal fibrous lamina, the annulus fibrosus. Therole of trauma in the degenerative process anddisc herniation is not clear. It is probable thatrepetitive excessive stresses do exacerbate thenormal ageing process and cause disc degenera-tion. Although it is frequently possible to identifysome minor episode of trauma prior to the onsetof an acute disc prolapse, a readily identifiableepisode of more major trauma as the precipitat-ing event is much less frequent.
The cervical disc prolapse is usually in theposterolateral direction, because the strong posterior longitudinal ligament prevents directposterior herniation. The posterolateral discherniation will cause compression of the adja-cent nerve root as it enters and passes throughthe intervertebral neural foramen. Unlike thelumbar region, the nerves pass directly laterallyfrom the cervical cord to their neural foramen,so that the herniation compresses the nerve atthat level (Fig. 14.1). The arrangement of thecervical nerve roots and the relationship to the vertebral bodies differ from the lumbar region — the C1 nerve root leaves the spinalcanal between the skull (the foramen magnum)and the atlas, and the C8 root, for which there isno corresponding numbered vertebra, passesthrough the C7/T1 foramen. Consequently, aC5/6 disc prolapse will cause compression ofthe C6 nerve root, a C6/7 prolapse causes com-pression of the C7 nerve root and the C7/T1 disc
CHAPTER 14
14 Cervical disc disease andcervical spondylosis
197
KAY14 12/16/04 7:45 PM Page 197

198 CHAPTER 14
prolapse causes compression of the C8 nerveroot.
Occasionally a cervical disc may herniate directly posteriorly, causing compression of theadjacent cervical spinal cord (Chapter 15) whichis a neurosurgical emergency.
Clinical presentation
The characteristic presenting features of a patientwith an acute cervical disc herniation consist ofneck and arm pain and the neurological manifes-tations of cervical nerve root compression.
Although the pain usually begins in the cervi-cal region it characteristically radiates into theperiscapular area and shoulder and down thearm (brachial neuralgia). The neck pain com-monly regresses while the radiating arm pain be-comes more severe. It is usually described as a‘deep’, ‘boring’ or ‘aching’ pain and the patient isusually severely distressed and debilitated by thediscomfort. The distribution of the pain is wide-spread and conforms to sclerotomes (segmentaldistribution to muscle and bone) rather than todermatomes. The patient frequently complainsof sensory disturbance, particularly numbness ortingling in the distribution of the dermatome af-fected. The location of the sensory disturbance ismore useful than the pain as an indication of rootlevel: thumb (and sometimes index finger) in C6
lesions, middle finger (and sometimes index fin-ger) in C7 lesions, and little and ring fingers in C8lesions. The patient may notice weakness of thearm, particularly if the C7 root is affected, as thiscauses weakness of elbow extension and themovement has only very little supply by othernerve roots (C8). A severe C5 root lesion maycause weakness of shoulder abduction and thepatient may complain of difficulty in elevatingthe arm.
Examination features
Cervical spine movements will be restricted andthe head is often held rigidly to one side, usuallymoderately flexed, and tilted towards the side ofthe pain in some patients but occasionally awayfrom it in others. Lateral tilt relaxes the roots onthe side of the concavity but diminishes the inter-vertebral foraminae, and flexion slightly sepa-rates the posterior part of the intervertebral spaceand lessens the tension in the prolapse. If the discherniation is long standing there may be wastingin the appropriate muscle group, particularly thetriceps in a C7 root lesion. The patient is then ex-amined for weakness in each of the musclegroups (Tables 14.1 and 14.2). Weakness of elbowextension and finger extension is most common-ly caused by a C6/7 prolapse with compressionof the C7 nerve root. Less commonly, disc hernia-tion with compression of the C5 root will causeweakness of shoulder abduction, compression ofthe C6 root will cause mild weakness of elbowflexion, and compression of C8 may cause weak-ness of the long flexor muscles, triceps, finger ex-tensors and intrinsic muscles.
The deep tendon reflexes provide objective ev-idence of nerve root compression in the followingdistribution.• Biceps reflex C5• Brachioradialis (supinator) reflex C6• Triceps reflex C7
Sensation should be tested in the arm and handand the sensory loss will be characteristic for thenerve root involved (Fig. 14.2) although theremay be some overlap.
A full neurological examination must be per-formed and particular care taken to assess the
Fig. 14.1 Posterolateral cervical disc prolapse causingcompression of the adjacent nerve root.
KAY14 12/16/04 7:45 PM Page 198

presence in the lower limbs of long tract signs,such as increased tone, a pyramidal pattern ofweakness, hyperreflexia or an upgoing plantarresponse. If there is a cervical disc herniationthese features will indicate that it is compressingthe spinal cord.
Summary of clinical features
Clinical localization of disc prolapse is possible in
CERVICAL DISC DISEASE AND CERVICAL SPONDYLOSIS 199
Table 14.1 Segmental innervation of upper limb musculature.
C3, 4 Trapezius; levator scapulae
C5 Rhomboids; deltoids; supraspinatus; infraspinatus; teres minor; biceps
C6 Serratus anterior; latissimus dorsi; subscapularis; teres major; pectoralis major (clavicular head);biceps; coracobrachialis; brachialis; brachioradialis; supinator; extensor carpi radialis longus
C7 Serratus anterior; latissimus dorsi; pectoralis major (sternal head); pectoralis minor; triceps;pronator teres; flexor carpi radialis; flexor digitorum superficialis; extensor carpi radialis longus;extensor carpi radialis brevis; extensor digitorum; extensor digiti minimi
C8 Pectoralis major (sternal head); pectoralis minor; triceps; flexor digitorum superficialis; flexordigitorum profundus; flexor pollicis longus; pronator quadratus; flexor carpi ulnaris; extensor carpiulnaris; abductor pollicis longus; extensor pollicis longus; extensor pollicis brevis; extensor indicis;abductor pollicis brevis; flexor pollicis brevis; opponens pollicis
T1 Flexor digitorum profundus; intrinsic muscles of the hand (except abductor pollicis brevis; flexorpollicis brevis; opponens pollicis); hypothenar muscles
Table 14.2 Segmental innervation of upper limbjoint movements.
Shoulder Abductors and lateral C5rotators
Adductors and medial C6, 7, 8rotators
Elbow Flexors C5, 6Extensors C7, 8
Forearm Supinators C6Pronators C7, 8
Wrist Flexors and extensors C6, 7
Digits Long flexors and extensors C7, 8
Hand Intrinsic muscles C8, T1
C6
T2
T1
C7
T1
C5
C4
C6
T2
C7
C4
C5
C8C8 C6
C3
Fig. 14.2 Upper limb dermatome distribution.
KAY14 12/16/04 7:45 PM Page 199

200 CHAPTER 14
most patients with brachial neuralgia due to cer-vical disc prolapse. The following features aretypical (but not invariable) for disc herniation:
C6/C7 prolapsed intervertebral disc (C7 nerve root)• Weakness of elbow extension• Absent triceps jerk• Numbness or tingling in the middle or indexfinger.
C5/6 prolapsed intervertebral disc (C6 nerve root)• Depressed supinator reflex• Numbness or tingling in the thumb or indexfinger• Occasionally mild weakness of elbow flexion.
C7/T1 prolapsed intervertebral disc (C8 nerve root)• Weakness may involve long flexor muscles,triceps, finger extensors and intrinsic muscles• Diminished sensation in ring and little fingerand on the medial border of the hand and forearm• Triceps jerk may be depressed.
Differential diagnosis
The clinical features of an acute cervical disc pro-lapse, with severe neck and arm pain and com-monly diminished sensation in the dermatome ofthe affected cervical root, are so characteristicthat in the vast majority of cases the diagnosis isself-evident. The most common cause of radiat-ing arm pain, other than acute prolapse, isspondylosis but, as has been indicated, disc pro-lapse and spondylosis are aspects of one continu-ing degenerative process and, in the cervicalregion, the distinction between them becomesblurred. Other unlikely but possible differentialdiagnoses include:• cervical nerve root compression by a spinal tumour (e.g. meningioma, neurofibroma) (Chapter 15)• thoracic outlet syndrome (Chapter 17)• Pancoast’s tumour infiltrating the roots of thebrachial plexus• peripheral nerve entrapments, such as carpaltunnel syndrome, median nerve entrapment inthe cubital fossa and tardy ulnar palsy (Chapter17).
Management
Most patients with arm pain due to an acute softcervical disc herniation achieve good pain reliefwith conservative treatment. This should includebed rest, a cervical collar, simple analgesic medication, non-steroidal anti-inflammatorymedication and muscle relaxants. Manipulationof the neck is potentially hazardous and is contraindicated.
The following are indications for further inves-tigation and surgery.1 Pain:
(a) continuing severe arm pain for more than10 days without benefit from conservativetherapy(b) chronic or relapsing arm pain.
2 Significant weakness in the upper limb thatdoes not resolve with conservative therapy.3 Evidence of a central disc prolapse causingcord compression — this should be investigatedurgently.
Radiological investigations
High-quality MRI is now the investigation ofchoice and has almost completely replaced bothmyelography and CT (Fig. 14.3). The cervicalmyelogram using water-based non-ionic iodinecontrast material was a most useful investigationfor determining the presence and site of the discherniation (Fig. 14.4). CT scanning by itself is fre-quently not helpful, but if performed followingintrathecal iodine contrast it will demonstrate adisc herniation, and smaller volumes of intra-thecal contrast are necessary than with myelo-graphy (Fig. 14.5).
Operative procedure
The two most commonly performed operationsfor cervical disc prolapse are:1 Cervical foraminotomy with excision of thedisc prolapse.2 Anterior cervical discectomy, with subsequentfusion.
Cervical foraminotomy. This involves fenestration
KAY14 12/16/04 7:45 PM Page 200

recurrent disc herniation, but this is very uncom-mon. In general, the results of the procedure arevery satisfactory, with excellent relief of arm painand, provided the nerve has not been irreparablydamaged by long-standing disc herniation, re-turn of full strength to the arm.
Anterior cervical discectomy. This involves an ante-rior approach to remove the cervical disc and theprolapse. Some surgeons perform formal fusionat the level using bone taken from the iliac crest,bovine bone, artificial bone, or an intervertebralcage, usually filled with bone chips. The fusion
CERVICAL DISC DISEASE AND CERVICAL SPONDYLOSIS 201
(a)
(c)
(b)
Fig. 14.3 MRI of cervical disc prolapse. (a) Cervicalaxial T1-weighted image (arrow shows disc prolapse).(b,c) Sagittal MRI showing disc prolapse compressingthe spinal theca and distorting the cervical cord.
of the bone posteriorly, to provide direct access tothe cervical nerve root and disc prolapse. A smallamount of bone from the lateral margins of theadjacent lamina and articular facets is removed toidentify the nerve root in the foramen. Furtherbone can then be removed from around the nerveroot to enlarge the neural canal. The nerve root isgently retracted and the disc herniation excised.The major advantages of the technique are thatthe nerve is directly decompressed both by re-moval of the disc herniation and by enlargementof the foramen, and cervical fusion is not neces-sary. The major disadvantage is the possibility of
KAY14 12/16/04 7:46 PM Page 201

202 CHAPTER 14
may be supplemented by a metal (usually titani-um) plate screwed onto the anterior vertebralsurface, bridging the disc space. Some surgeonsdo not perform a formal fusion, as spontaneousfibrous or bony fusion will occur across the discspace provided all the disc has been excised. Themajor disadvantage is that the fusion will resultin additional stress at the adjacent cervical levels,thereby rendering them more prone to degenera-tive disease.
An anterior approach with disc excision ismandatory for a central disc protrusion.
Postoperative careWhatever approach is used, the patient is encour-aged to mobilize the day after surgery. A soft cer-vical collar may be useful in the first week after aforaminotomy to minimize the neck pain. A firmcollar is usually worn for the first 4–6 weeks afteranterior discectomy, or until there is evidence offusion.
The prognosis for pain relief following the op-eration is excellent provided the diagnosis hasbeen accurate and the nerve decompressed.
Cervical spondylosis
Cervical spondylosis is a degenerative arthriticprocess involving the cervical spine and affectingthe intervertebral disc and zygapophyseal joints.Radiological findings of cervical spondylosis arepresent in 75% of people over 50 years of age whohave no significant symptoms referable to thecervical spine.
Pathological changes
The degenerative process resulting in cervicalspondylosis and its progression occur in mostcases largely as a result of the inevitable stressesand traumas that occur to the cervical spine as aresult of the normal activities of daily living. It isprobable that the process is aggravated by repet-itive or chronic trauma, as may occur in some oc-cupations, and as a result of an episode of severetrauma.
The process principally involves the interver-tebral discs and zygapophyseal joints. Reducedwater content and fragmentation of the nuclearportion of the cervical discs are natural ageingprocesses. As the disc degenerates there isgreater stress on the articular cartilages of thevertebral end-plates and osteophytic spurs de-velop around the margins of the disintegratingend-plates, projecting posteriorly into the spinalcanal and anteriorly into the prevertebral space.
Fig. 14.4 Cervical myelogram showing a postero-lateral cervical disc protrusion with compression of the cervical nerve root.
Fig. 14.5 CT myelogram showing a posterolateralcervical disc protrusion.
KAY14 12/16/04 7:46 PM Page 202

The degenerative process involving the zy-gapophyseal joints will also lead to osteophyteformation. The intervertebral foramen may benarrowed by these osteophytes, so causing com-pression of the nerve root. The osteophyte forma-tion that causes compression of the nerve in theneural foramen, and which is seen around abulging annulus, is sometimes called a ‘hard discprotrusion’, as distinct from the acute ‘soft’ cervi-cal disc herniation.
The spondylitic process may cause narrowingof the spinal canal as a result of osteophyte for-mation, particularly the formation of hyper-trophic bony ridges at the anterior intervertebralspaces of the spinal canal and hypertrophy ofthe ligamenta flavum. This may result in com-pression of the underlying cord. Such compres-sion is maximal during hyperextension of the neck and may cause cervical myelopathy(Chapter 15).
Presenting features
There are three major manifestations of cervicalspondylosis, depending on whether there is com-pression of a cervical nerve root or the spinalcord.1 Neck pain.2 Radiating arm pain.3 Cervical myelopathy (Chapter 15).
Neck pain. This is the most common clinical man-ifestation of cervical spondylosis and its onsetmay be precipitated by minor trauma. The painusually settles over a period of a few days orweeks but frequently recurs and is associatedwith increasing stiffness of the neck.
Radiating arm pain. Brachial neuralgia (radiatingarm pain) results from a nerve root being com-pressed in the neural foramen by osteophyte for-mation, with subsequent narrowing of the bonycanal. The patient frequently has a history of intermittent neck pain as a result of cervicalspondylosis for some months or years, and theonset of the arm pain may be precipitated by anepisode of minor trauma. The clinical features aresimilar to the neuralgia caused by an acute soft
disc prolapse, in that the pain radiates diffuselyinto the periscapular area and shoulder, and intothe upper limb in a scleratomal distribution.There may be other features of nerve root com-pression, including numbness and tingling in theappropriate dermatome distribution, and weak-ness of the arm. Although the clinical featuresmay be almost indistinguishable from those dueto an acute soft disc prolapse, the process is usu-ally not as acute and the patient often has a histo-ry of intermittent or chronic pain. Wasting of amuscle group in the appropriate nerve root dis-tribution is more common because of the longerhistory, but the examination findings will other-wise be similar to those seen with an acute softdisc protrusion.
Cervical myelopathy. This may result from cervicalspondylosis causing narrowing of the spinalcanal with compression of the underlying spinalcord. The features of progressive weakness andsensory disability are described in Chapter 15.
Radiological findings
Plain cervical spine X-rays (Fig. 14.6) show:• narrowing of the disc space (the C5/C6 andC6/C7 levels are the most commonly affected)• osteophyte formation with encroachment intoeither the spinal canal or neural foramen• reduced mobility at positions of fusion and in-creased mobility at adjacent levels.
The indications for further radiological investi-gations depend on the clinical presentation. Although CT scan will clearly show the bonychanges seen on the plain cervical spine X-rays, itis not indicated for the investigation of cervicalspondylosis which is causing only neck pain.Nerve root entrapment, causing arm pain, is bestvisualized by high-quality MRI. A CT scan fol-lowing intrathecal contrast or a cervical myelo-gram with water-based non-ionic iodine contrastwill also show the nerve root compression, butare now only rarely necessary as MRI providessuch excellent visualization of the pathology andnerve root compression. The radiological assess-ment of cervical myelopathy is discussed inChapter 15.
CERVICAL DISC DISEASE AND CERVICAL SPONDYLOSIS 203
KAY14 12/16/04 7:46 PM Page 203

204 CHAPTER 14
Differential diagnosis
Neck painThere are numerous possible causes of neck pain,depending on the mode of clinical presentationand the presence of neurological signs in thelimbs. The most common cause of neck pain is aminor muscular or ligamentous strain whichusually follows minor trauma. If there has been amajor injury then a fracture dislocation or acutedisc herniation should be considered and exclud-ed. Other rare causes of neck pain are spinal tu-mours or spinal abscess.
The other possible diagnoses in a patient presenting with arm pain have been describedearlier in the chapter.
Management
Neck pain due to cervical spondylosisThe pain usually resolves with simple conserva-tive measures, including the use of non-steroidalanti-inflammatory medication and simple anal-
gesics. During an acute episode the patient maybe more comfortable in a soft cervical collar. Asthe pain subsides the patient should be encour-aged to perform simple mobilizing exerciseswhich may be best undertaken with the supervi-sion of a physiotherapist. If the episodes becomefrequent and severe the patient may need to con-sider a change of lifestyle, particularly workpractices and recreational behaviour, whichmight be aggravating the cervical spondylosis.
Arm painThe symptoms frequently settle with the man-agement described above. The following are in-dications for surgery.• Severe pain that does not settle with conserva-tive treatment over 2–3 weeks.• Chronic or recurrent pain.• Progressive weakness in the arm which causesfunctional disability. The most frequently in-volved nerve root producing significant func-tional weakness is the C7 root, but the C8 or C5roots may also result in functional disability as aresult of long-standing root compression.
The choice of surgical procedure is similar tothat for an acute soft disc prolapse. Cervical fora-menotomy, with decompression of the nerveroot, excision of the osteophytes and enlarge-ment of the neural foramen, is an effective surgi-cal technique. As the spondylitic process is oftenat multiple levels, two roots often need to be de-compressed. Some surgeons favour an anteriorapproach and cervical discectomy with excisionof the osteophyte extending into the neural fora-men. The decompression is followed by a fusionas described in the previous section on cervicaldisc prolapse.
Cervical myelopathy(See Chapter 15.)
Further readingAdams CBT, Logue V (1971) Studies in cervical
spondylitic myelopathy: 1. Movement of the cervicalroots, dura and cord and their relationship to thecourse of the extrathecal roots. Brain 94, 557–568.
Hoff J (1980) Cervical spondylosis. In: Wilson CB, Hoff
Fig. 14.6 Cervical spondylosis. There is narrowing ofthe C5/6 and C6/7 disc spaces, osteophyte formationand a subluxation at the C4/5 level.
KAY14 12/16/04 7:46 PM Page 204

JT, eds. Current Surgical Management of NeurologicalDisease. Churchill Livingstone, New York.
Kaye AH, Black P McL (2000) Operative Neurosurgery.Churchill Livingstone, London, New York, Edinburgh.
Lees F, Aldren-Turner JW (1963) Natural history andprognosis of cervical spondylosis. British MedicalJournal 2, 1607–1610.
Lunsford LD et al. (1980) Anterior surgery for cervicaldisc disease. Part 1. Treatment of lateral cervical discherniation: 253 cases. Journal of Neurosurgery 53, 1–11.
Martins AN (1976) Anterior cervical discectomy withand without interbody bone graft. Journal of Neuro-surgery 44, 290–295.
Simeone FA, Vise WM, Grob D, Henderson F (1995)Treatment of soft cervical disc herniation. In: Al-Mefty O, Origitano TC, Harkey HL, eds. Controversiesin Neurosurgery. Thieme, New York.
Zeidman SM, Ducker TB (1992) Cervical disc diseases(Review). Neurosurgery Quarterly 2, 116–159.
CERVICAL DISC DISEASE AND CERVICAL SPONDYLOSIS 205
KAY14 12/16/04 7:46 PM Page 205

Compression of the spinal cord is a common neu-rosurgical problem. Although the initial clinicalmanifestations vary considerably, if the condi-tion is unrecognized and untreated the eventualoutcome will inevitably be disabling paralysisand sphincter disturbance. Spinal cord compres-sion requires early diagnosis and urgent treat-ment if these disastrous consequences are to beavoided.
The compression may occur at any positionfrom the cervicomedullary junction to the conusmedullaris. Although compression of the caudaequina is not strictly spinal cord compression, thepathophysiology and treatment is so similar thatit is considered with cord compression.
Spinal trauma may also cause cord compres-sion but will be discussed separately in the nextchapter (Chapter 16).
Pathology
The spinal cord may be compressed by lesionsthat are:• extradural (80%)• intradural, extramedullary (15%)• intramedullary (5%).
The major groups of pathological causes are:1 Tumour:
(a) metastatic(b) primary.
2 Degenerative:(a) disc prolapse(b) osteoporosis/spondylosis.
3 Infection:(a) vertebral body(b) disc space
(c) extradural(d) intradural.
4 Haematoma:(a) spontaneous (trauma)(b) arteriovenous malformation.
5 Developmental:(a) syrinx(b) arteriovenous malformation(c) arachnoid cyst.Although there is a large range of possible
causes of cord compression, in clinical practicethe large majority are due to the following.1 Extradural:
(a) metastatic tumour(b) extradural abscess.
2 Intradural, extramedullary:(a) meningioma(b) schwannoma.
3 Intramedullary:(a) glioma (astrocytoma and ependymoma)(b) syrinx.Table 15.1 shows a list of the possible causes
of spinal cord compression and their primary positions.
Presenting features
There are two major presenting features that arethe hallmarks of spinal cord compression.1 Pain.2 Neurological deficit.
There is considerable variation in the mannerin which these two major features present, de-pending on:• the site of the compression and the involve-ment of adjacent nerve roots
CHAPTER 15
15 Spinal cord compression
206
KAY15 12/16/04 7:47 PM Page 206

• the speed of the compression• the pathological cause and the nature of thecompressive lesion• the involvement of the blood supply of thespinal cord.
PainPain is a common early feature of cord compres-sion and often precedes the onset of any neuro-logical disturbance, sometimes by many months.• Pain is due to involvement of local, pain-sensitive structures, such as the bone of the verte-bral column. Pain in the back may also be causedby spasm of the erector spinae muscles.• Pain of spinal root origin is due to involvementof the nerve root at the level of the compression.In cervical compression nerve root involvementwill cause pain radiating into the upper limb inthe distribution of the nerve root. Thoracic cord
compression, with involvement of the thoracicnerve roots, will often be associated with pain radiating around the chest wall. This ‘girdle’ painis an important feature associated with a lesionwhich may cause cord compression. Whereasback pain in general is a non-specific commonsymptom, usually associated with degenerativedisease, ‘girdle’ pain should arouse the suspicionof an underlying sinister cause. The pain is oftenaggravated by coughing and straining.• ‘Central’ pain due to spinal cord compressionitself is an unpleasant diffuse dull ache, oftenwith a ‘burning’ quality, and is frequently de-scribed with difficulty. It may involve a limb orside of the trunk, depending on the segment involved.
Flexion or extension of the neck may cause‘electric shock’ or tingling radiating downthrough the body to the extremities of the limbs.This is called Lhermitte’s sign, and is typically as-sociated with cervical cord involvement, eitherby a compressive lesion or due to an inflammat-ory process.
Neurological deficitThe neurological features of spinal cord compres-sion consist of:• progressive weakness• sensory disturbance• sphincter disturbance.
Motor impairmentThe level of paralysis will depend on the positionof the cord compression. Thoracic cord compres-sion will result in a progressive paraparesis of thelower limbs and if the cervical cord is involvedthe upper limbs will also be affected. The com-pression of the corticospinal pathways will resultin an upper motor neurone weakness with littleor no wasting, increased tone, increased deeptendon reflexes and positive Babinski response.As the cord becomes more severely compressed acomplete paraplegia will result. The weaknesshas an initial ‘pyramidal’ pattern, with the flexormovements being most severely affected, whilstthe extensor movements, e.g. hip extension, kneeextension and plantar flexion, are relatively preserved.
SPINAL CORD COMPRESSION 207
Table 15.1 Spinal cord compression.
ExtraduralMetastatic tumourLymphomaMyelomaLeukaemiaPrimary vertebral body tumourChordomaDisc prolapseOsteoporosis/spondylosisExtradural abscessExtradural haematoma
Intradural, extramedullaryMeningiomaSchwannomaArteriovenous malformationSpinal seeding from intracranial tumour
(medulloblastoma, ependymoma)
IntramedullaryGlioma — ependymoma, astrocytomaArteriovenous malformation, haematomaAbscessMetastatic tumourSyrinxHaemangioma
KAY15 12/16/04 7:47 PM Page 207

208 CHAPTER 15
As described in Chapter 1, the pattern of weak-ness may also be influenced by the position of the compressing lesion. The descending corti-cospinal pathways decussate at the level of thecervicomedullary junction so that lateral com-pression in the spinal cord will initially causeweakness, predominantly on the side of the com-pressing lesion.
The compressing mass will cause weakness ofthe nerve root segment at the involved level. Inthe cervical region this will result in a lowermotor neurone weakness of the involved nerveroots in the upper limb, with the other associatedfeatures of focal wasting and depressed reflexesat that level. A mass below T1 in the thoracic areawill cause no clinically demonstrable nerve rootweakness. In the lumbar region, involvement ofthe conus medullaris may produce a mixture oflower motor neurone features and upper motorneurone signs in the lower limbs.
Cauda equina compression produces a lowermotor neurone pattern of weakness.
Sensory disturbanceA sensory level is the hallmark of spinal cordcompression. In the thoracic region the sensorylevel will be to all modalities of sensation overthe body or trunk, although there may be spar-ing of some modalities in the early stages of com-pression. A useful guide to remember is the T4dermatome lies at the level of the nipple, the T7at the xiphisternum and the T10 at the umbilicus.Careful examination will often reveal a band ofminor hyperaesthesia at the level of the com-pression. If the compression is in the cervicalarea there will be sensory loss in the upper limbin the appropriate dermatomal pattern (Fig.15.1).
Specific patterns of sensory loss will occur de-pending on the tracts within the cord that are initially involved. A laterally placed mass willinitially cause a ‘Brown-Séquard’ syndrome.There will be contralateral impairment of painand temperature sensation, with ipsilateral pyra-midal weakness and impairment of joint positionsense, vibration and fine touch. This is becausethe fibres of pain and temperature cross to the op-posite side of the spinal cord to ascend in the lat-
eral spinothalamic tracts, whereas the fibres ofproprioception ascend in the dorsal columns ofthe spinal cord and do not cross until they reachthe low medullary region. Intrinsic lesions affect-ing the central cord in the cervicothoracic regionand damaging the sensory neurones crossing tothe lateral spinothalamic tract will initially causea ‘cape-like’ distribution of thermoanalgesia,such as occurs in syringomyelia (Chapter 11, Fig.11.3). The sacral fibres lie peripherally in the lat-eral spinothalamic tracts and so some degree ofsacral sparing can occur, even with large intrinsiclesions. Analgesia affecting primarily the saddlearea (buttocks and upper posterior thigh) occursparticularly in cauda equina or conus medullarislesions.
C8
L2
L1
T3
5
7
9
11
T2
4
6
8
10
12
T2
C3
T1
C4
Fig. 15.1 Dermatomes of the trunk (thoracic) andadjacent cervical and lumbar areas. The sensory levelwill be a useful guide to the level of cord compression.(See also Figs 13.2 and 14.2.)
KAY15 12/16/04 7:47 PM Page 208

Sphincter involvementSphincter disturbance occurs following compres-sion of the spinal cord, conus medullaris or caudaequina. The first symptom is difficulty in initiat-ing micturition and this is followed by urinary retention, which is often relatively painless. Constipation and faecal incontinence will subse-quently occur. The clinical signs include an en-larged, palpable bladder, diminished perianalsensation and decreased anal tone.
In summary the clinical features of spinal cordcompression are:• pain — local and radicular• progressive weakness of the limbs• sensory disturbance — often a sensory level• sphincter disturbance.
Management
The general principles of management are simi-lar whatever the cause of the cord compression.It is again emphasized that the investigationsand treatment must be undertaken as a matter ofurgency once the diagnosis is suspected, so as toreduce the possibility that the neurologicaldeficit will progress or become permanent.Spinal cord compression is a neurosurgicalemergency.
Radiological investigationsThe radiological studies undertaken to confirmthe diagnosis of spinal cord compression include:• plain spinal X-rays• MRI• myelography• CT scan (with intrathecal contrast).
Magnetic resonance imaging is of considerablevalue in diagnosing the cause and position ofspinal cord compression, and has replaced myel-ography as the definitive investigation. It is by farthe best investigation for spinal cord compres-sion as it is a non-invasive investigation and willclearly show the pathological changes in the ver-tebral body, spinal canal, spinal cord and par-avertebral region, thereby helping considerablywith treatment planning in general, and in partic-
ular planning the most appropriate surgical approach.
Spinal myelography, using water-soluble, iodine-based contrast agents injected intrathecally, wasthe benchmark investigation for confirming thediagnosis and the level of spinal cord compres-sion prior to MRI. The contrast is injected in-trathecally in the lumbar region and the level ofthe compression can be identified. If there is acomplete block to the flow of contrast it is oftenhelpful to inject further contrast using a Cl/2puncture, so as to ascertain the upper level of theblock. The pattern of ‘block’ on the myelogramwill usually demonstrate whether the cord hasbeen compressed by an extradural mass or an ex-tramedullary intradural tumour, or whether thecord is swollen by an intramedullary lesion (Fig.15.2).
Computerized tomography scanning at the level ofthe compression and just above and below thearea will often help to further demonstrate thenature and cause of the compression and givemore detail about the adjacent bony structures.
Plain spinal X-rays are essential in patients withspinal cord compression. The important radio-logical features are:• focal bony destruction indicating a metastaticlesion, e.g. erosion of a pedicle, vertebral collapse• evidence of multiple destructive or sclerotic lesions, indicating multiple metastatic tumours• thinning of a pedicle and widening of the interpedicular distance, suggestive of long-standing intradural compression• scalloping of the posterior surface of the verte-bral body, indicating a long-standing intradurallesion• expansion of an intervertebral foramen onoblique X-rays, indicative of a neurofibroma• destruction of a disc space, suggestive of infection.
Other investigations• Further investigations to evaluate the extent ofthe disease and site of origin may be useful in pa-tients with metastatic disease prior to surgery.
SPINAL CORD COMPRESSION 209
KAY15 12/16/04 7:47 PM Page 209

210 CHAPTER 15
However, these investigations should not delaythe definitive treatment.• Many patients with malignant disease have apoor general medical condition and require car-diorespiratory and biochemical assessment priorto surgery.
Treatment
The standard treatment for spinal cord compres-sion is urgent surgery, except in some cases ofcompression due to malignant tumour, in whichtreatment with high-dose glucocorticosteroidsand radiotherapy is indicated. This will be dis-cussed further in the next section.
Malignant spinal cord compression
By far the most common cause of spinal cordcompression results from extradural compres-sion by malignant tumours. The most commontumours are:• carcinoma of the lung• carcinoma of the breast• carcinoma of the prostate• carcinoma of the kidney• lymphoma• myeloma.
Less common tumours include leukaemias,melanoma, carcinoma of the thyroid and primarysarcomas.
The thoracic region is by far the most com-
monly affected but metastases may occur at anysite and are often multiple. The compression isdue to the tumour itself or to vertebral collapse,or a combination of these.
The clinical features are basically as describedin the previous section. The patient invariablycomplains of pain local to the involved regionand a radicular girdle pain is frequently present.Although, in retrospect, minor symptoms of cordcompression may have been present for a fewweeks or even months, there is often a rapid neu-rological deterioration resulting in paralysis, sen-sory disturbance and sphincter difficulties.
Urgent investigation and treatment is essentialif permanent severe disability (Figs 15.3–15.5) isto be avoided.
Surgical treatment for malignant spinal cordcompression utilizes either:• decompressive laminectomy (posterior ap-proach) or• vertebrectomy and fusion (anterior approach).
The decision regarding the type of surgery willdepend on the position of the compressive lesion(whether anterior or posterior to the spinal cord)and the extent of the compression.
The standard treatment has been a decompres-sive laminectomy over the affected levels. The exposed tumour is resected as much as possibleto relieve the cord compression. Glucocortico-steroids (e.g. dexamethasone) are often used toreduce local oedema of the spinal cord, and thesurgery is usually followed by radiotherapy.
Uneven edge to contrast material
Completeblock
Extramedullaryblock
Intramedullaryblock
Cord displaced to one sideRounded edge of contrast material
Contrast material is splayed around the swollen cord
Extradural Intradural
Fig. 15.2 Diagram ofmyelographic appearance dueto extradural, intradural andextramedullary, orintramedullary lesions.
KAY15 12/16/04 7:47 PM Page 210

SPINAL CORD COMPRESSION 211
Fig. 15.3 Extensive destruction of vertebral body andadjacent neural arch with invasion into spinal canal bymetastatic carcinoma.
Fig. 15.4 Extradural block onmyelogram due to metastatic carcinoma. (b)(a)
If the metastatic tumour is localized to one ortwo vertebral bodies only, and is causing com-pression anterior to the spinal cord, a posteriordecompressive laminectomy may not relieve thecompression and may result in vertebral instabil-ity. Vertebral body resection, excision of the
anterior tumour and reconstruction with fixationmay be appropriate. However, this entails a moremajor operative procedure and may not be toler-ated or indicated in debilitated patients withwidespread metastatic tumour.
The initial results following surgical decom-pression depend largely on the severity andlength of time of the preoperative compression.Patients with a complete paraplegia of more than36 hours have a poor prognosis for neurologicalrecovery.
Some studies have shown that urgent radio-therapy, with high-dose glucocorticosteroids,may be effective in controlling the tumour caus-ing spinal cord compression. The treatment mustbe commenced immediately following diagnosisand should be considered:• if the patient has a known primary tumourthat is radiosensitive (e.g. carcinoma of theprostate, lymphoma)• if there is a partial incomplete neurological lesion that is only slowly progressive• if sphincter function is retained.
This form of treatment is also particularlyadvantageous if the tumour is mostly anterior
KAY15 12/16/04 7:47 PM Page 211

212 CHAPTER 15
to the spinal cord over a number of vertebrallevels because the compression from this typeof lesion may not be satisfactorily relieved following a posterior decompressive lamin-ectomy.
Conversely, radiotherapy as the primary formof treatment is not appropriate if:• the tumour is known to be radioresistant• the compression is primarily due to bone col-lapse rather than tumour mass• the origin of the tumour is not known• there is a rapidly progressive neurologicaldeficit and/or sphincter disturbance.
Schwannoma (neurofibroma)
Schwannomas are the most common of the in-trathecal tumours and may occur at any position.They arise invariably from the posterior nerveroots and grow slowly to compress the adjacentneural structures. Occasionally the intrathecal tu-mour extends through the intervertebral fora-men to form a ‘dumb-bell’ tumour, and thetumour may rarely present as a mass in the tho-rax, neck or posterior abdominal wall.
The presenting features are those of a slowlygrowing tumour causing cord compression. Painin a radicular distribution is the most commonfirst symptom and is often present for severalyears. In the cervical region there may be evi-dence of long-standing neurological involve-ment of the cervical nerve root prior to thefeatures of cord compression becoming apparent.There is frequently some degree of a Brown-Séquard syndrome due to the lateral position ofthe tumour.
The plain X-rays show radiological evidence ofbone erosion, and enlargement of the interverte-bral foramen is typical (Fig. 15.6). A large tumour
Fig. 15.5 (a,b) MRI of metastatic tumour in cervicalvertebral bodies and compression of spinal cord.
(a)
(b)
Fig. 15.6 Enlarged neural foramen due toschwannoma.
KAY15 12/16/04 7:47 PM Page 212

SPINAL CORD COMPRESSION 213
Fig. 15.7 (a) ‘Dumb-bell’ schwannoma extending through intervertebral neural foramen. The intrathecal contrastmedium outlines the tumour in the spinal canal causing spinal cord compression. (b) MRI of schwannoma. (c) MRI of cervical schwannoma.
(a)
(c)
(b)
will erode the adjacent part of the vertebral bodyand there is frequently an increase in the inter-pedicular distance.
The myelogram and CT scan (following in-trathecal contrast) will show an intradural tu-mour with cord compression (Fig. 15.7) and theCT scan will also show the extraspinal extension.MRI with intravenous gadolinium contrast hasreplaced myelography for the diagnosis of theselesions (Fig. 15.7b).
The treatment is surgical excision of the tumour. Access to the tumour is obtained by a laminectomy. If there is a large extraspi-nal extension it may be necessary to obtain additional exposure through the neck, chest orabdomen.
Spinal meningioma (Fig. 15.8)
Spinal meningiomas occur particularly in mid-
KAY15 12/16/04 7:47 PM Page 213

214 CHAPTER 15
dle-aged or elderly patients and show a markedfemale predominance. The thoracic region of thespinal cord is the most common site and they areinvariably situated intradurally, causing markedcompression of the adjacent cord.
The tumours grow extremely slowly and there
is usually a long history of ill-defined back pain,often nocturnal, and a very slowly progressiveparalysis prior to diagnosis.
Plain X-rays may show erosion of the pediclesdue to long-standing intradural compression.Hyperostosis, which is frequently present in
Fig. 15.8 (a) Intradural extramedullary block onmyelogram due to meningioma. (b) Meningioma withsevere compression of adjacent spinal cord. (c) MRI ofspinal meningioma.
(a)
(c)
(b)
KAY15 12/16/04 7:47 PM Page 214

cranial meningiomas, does not occur in spinalmeningiomas.
The diagnosis will be made using the radio-logical investigations mentioned earlier in thechapter. MRI with intravenous gadolinium con-trast will give an accurate diagnosis of these tumours and has replaced myelography (Fig.15.8c).
The treatment of spinal meningioma is resec-tion of the tumour and the involved dura. The tu-mour often lies lateral to the cord and, followingthe excision, there is an excellent chance of neuro-logical improvement, even when there is sub-stantial neurological disability at the time ofdiagnosis. Occasionally the tumour lies directlyanterior to the spinal cord and resection withoutfurther injury to the cord in these circumstancesis difficult.
Intramedullary tumours
Intrinsic intramedullary tumours are uncommonand much less frequent than the extradural or in-tradural extramedullary tumours mentionedpreviously. The tumours usually present in the3rd and 4th decades, although they may occur atany age. The two most common tumours of thespinal cord are:1 Ependymoma.2 Astrocytoma.
Ependymomas comprise about 60% of intrin-sic spinal tumours. They can occur at any level inthe spine, but the majority arise from the filumterminale where they usually have a myxopapil-lary histological appearance and cause compres-sion of the cauda equina.
Astrocytomas of the spinal cord may occur atany level and frequently initially have a low-grade histological appearance.
Presenting features
The presenting features of the tumours dependon the level of cord involved. Ependymomasarising in the filum terminale will cause featuresof cauda equina compression. There is often a his-tory of low back and leg pain, progressive weak-ness in the legs (often with radicular features),
sensory loss over the saddle area and eventuallysphincter disturbance.
Spinal rigidity and pain are common featuresin patients with intrinsic spinal cord tumours,particularly in children, and there is a progres-sive paralysis and sensory loss. A ‘cuirasse’(cape-like) pattern of sensory loss may be seeninitially but there is invariably progression to in-volve all lower segments below the level of thetumour. Tumour expansion and involvement ofthe anterior horn cells may produce a lowermotor neurone weakness and wasting of the cor-responding muscle groups, but long tract in-volvement causes upper motor neuroneweakness below the level of the lesion.
The progression of the spinal cord involve-ment will depend on the histological nature ofthe tumour. Although the tumours are initiallylow grade, they may evolve into a more aggres-sive morphology.
Radiology
MRI is the investigation of choice. It will showexpansion of the cord which may enhance fol-lowing intravenous injection of gadolinium. Asyrinx is frequently associated with an in-tramedullary tumour (Fig. 15.9b,c). Plain X-raysor CT will show expansion of the spinal canalwith increase of the interpedicular distancethrough several segments, scalloping of the ver-tebral bodies and sometimes thinning of theneural arches.
Treatment
It is often possible to obtain a complete macro-scopic excision of an ependymoma arising fromthe filum terminale which is causing compres-sion of the cauda equina (Fig. 15.10). Meticulousmicrosurgical techniques are necessary to dissectthe tumour from the nerve roots. In someependymomas of the spinal cord it is possible toobtain a plane of cleavage and perform a partialor even complete resection. However, it is notpossible to resect astrocytomas of the cord, andsurgery is usually restricted to obtaining a diag-nosis by biopsy, aspiration of cyst cavities and
SPINAL CORD COMPRESSION 215
KAY15 12/16/04 7:47 PM Page 215

216 CHAPTER 15
exclusion of other possible rare resectable le-sions. Radiotherapy is usually administered.
The prognosis is good if an ependymoma canbe resected. However, although patients with as-trocytomas may have prolonged survival, thereis frequently progressive tumour growth result-ing in permanent, severe neurological disability.Death will result if the tumour extends into thehigh cervical level or brainstem.
Intervertebral disc prolapse
Intervertebral disc herniation is a common cause
of cervical nerve root compression causing armpain (Chapter 14) and lumbar nerve root com-pression causing sciatica (Chapter 13). The nerveroot compression results from posterolateral discherniation. Occasionally, the disc may prolapsedirectly posteriorly (centrally) causing compres-sion of the spinal cord in the cervical or thoracicregion and cauda equina in the lumbar region(Chapter 13).
Cervical disc prolapse
Central posterior cervical disc herniation causesa rapidly progressive paralysis with upper motorneurone features below the level of the compres-sion and lower motor neurone features at thelevel of the compression. There is frequently apreceding history of some neck discomfort andoccasionally brachial neuralgia. However, thepatient often presents following the suddenonset of severe neck pain with rapidly progres-sive paralysis.
(a)
(b)
(c)
Fig. 15.9 Cervical cord intramedullary ependymomain a 24-year-old female. (a) Myelogram shows typicalfeatures of intramedullary tumour with ‘splaying’ ofcontrast around the expanded cervical cord. (b,c) MRIshows the tumour and the associated syrinx cavityextending up into the medulla.
Fig. 15.10 MRI showing myxopapillary ependymomaof the filum terminale.
KAY15 12/16/04 7:47 PM Page 216

Urgent MRI is the best investigation and willshow the disc prolapse and anterior cord com-pression, which is usually at the C5/6 or C6/7level (Fig. 15.11). If MRI is not readily availablemyelography followed by a CT scan will alsodemonstrate the disc prolapse. Plain X-rays willshow narrowing of the disc space.
Urgent surgery is necessary to relieve the com-pression. The disc is excised by an anterior ap-proach which involves removing the disc at thatlevel and, using microsurgical techniques, excis-ing the disc fragments which have usually prolapsed through the posterior longitudinal ligament. It is sometimes necessary to drill awaythe adjacent margins of the vertebral body to obtain adequate exposure and a formal vertebralfusion is usually necessary.
Thoracic disc prolapse
A central posterior thoracic disc prolapse is lesscommon. It usually occurs in males, predomi-nantly between the ages of 30 and 55, and usually occurs below the T8 level.
The thoracic disc protrusion is usually a conse-
quence of disc degeneration. The thoracic spinalcanal is small and there is very little space be-tween the disc and the thoracic cord. In addition,the circulation to the low thoracic region is a‘water shed’ and the region is often largely sup-plied by a single unilateral radicular vessel — theartery of Adamkiewicz — which usually arisesbetween T8 and L2, particularly on the left side.
The most common presenting symptom ispoorly localized back pain related to the degener-ative disc disease and stretching of the pain-sensitive posterior longitudinal ligament. Thereare often features of radicular involvement withgirdle pain. The neurological features of thoraciccord compression may progress rapidly or pro-ceed only slowly.
There are numerous possible differential diag-noses for thoracic disc prolapse. It is extremelydifficult to exclude spinal degenerative disease asthe cause when back pain is the only symptomand there are no neurological signs. The clinicalpicture associated with the neurological deficitcould be due to any other cause of spinal cordcompression, as well as to multiple sclerosis.
The plain X-rays show disc space narrowingand there is often evidence of calcified disc mate-rial either in the intervertebral space or withinthe canal. Disc space calcification is highly sug-gestive of thoracic disc herniation and is presentin up to 70% of cases, as opposed to an incidenceof less than 4% in the normal population. As withother causes of spinal cord compression the di-agnosis is best made with MRI (Fig. 15.12). IfMRI is not available myelography or CT scan-ning following intrathecal contrast will show an anterior compression at the level of the disc space and is also helpful in confirming thediagnosis.
It is essential that an accurate preoperative diagnosis is made because treatment involves excision of the disc protrusion by an anterior or anterolateral approach. The disc herniationshould not be resected using a laminectomy foraccess because the protrusion lies in front of thespinal cord and any manipulation of the thoraciccord will inevitably result in devastating neurological consequences. The usual surgicalapproach is via either a thoracotomy or a costotransversectomy at the involved level, with
SPINAL CORD COMPRESSION 217
Fig. 15.11 MRI of cervical disc prolapse causing spinalcord compression.
KAY15 12/16/04 7:47 PM Page 217

218 CHAPTER 15
excision of the disc and disc prolapse from infront of the dura without any manipulation of thecord.
Spinal abscess
Spinal epidural abscess is an uncommon condi-tion requiring urgent treatment. The abscess usu-ally occurs in the low thoracic or thoracolumbarregion but may occur in the cervical or upper tho-racic levels. It is due either to haematogenousspread from obvious distant or occult infection orto direct spread from the adjacent intervertebraldisc or vertebral column, particularly the pedicleor neural arch. Osteomyelitis of the body of thevertebra is less likely to infect the extraduralspace because there is no loose, anterior, fatty areolar tissue and the posterior longitudinal ligament helps to restrain the intraspinal spreadof infection (Table 15.2).
The most common organism is Staphylococcusaureus but other causative organisms includestreptococci, pneumococci and Pseudomonasspecies (Table 15.3).
Fig. 15.12 MRI of thoracic disc prolapse causing spinalcord compression.
Table 15.2 Reported sources of infection of epidural spinal abscess vary with the patient populationstudied. Sources of infection are changing over time as spinal surgery, other invasive procedure andimmunosuppression become more common and diagnosis and treatment of distant infection improve.
Source Incidence (%) Site of primary infection
Unknown 20–50 Skin/soft tissuePharynx/respiratory tractSinus/middle earDentalGenitourinary tractInfected vascular accessInfected prosthesisEndocarditis/phlebitisIntravenous drug useInfected surgical/traumatic wound
Contiguous focus 15–75 Osteomyelitis/discitisPostoperative infectionLumbar puncture/epidural catheterParaspinal abscessDecubitus ulcer
KAY15 12/16/04 7:47 PM Page 218

Spinal cord compression is due to inflammat-ory swelling and pus. Involvement of the ex-tradural spinal veins causes thrombophlebitiswhich can spread into the veins of the spinalcord, and the radicular arteries may develop anarteritis and thrombosis. Consequently, the cordis not only compressed by the abscess itself, but itis also at risk from infarction due to venous andarterial thrombosis.
The presenting features consist of:• severe local spinal pain• neurological signs of a rapidly progressivespinal cord compression• constitutional features of infection such ashigh fever, sweating and tachycardia.
MRI is the preferred investigation; it will bestshow the level, extent and position of the abscess.MRI has replaced the need for a lumbar punctureand myelography, which should only be per-formed if MRI is not available. Lumbar puncturefor myelography should be performed carefullyif a spinal extradural abscess is suspected and as-piration of the extradural space should be under-taken before the subarachnoid space is entered. If
pus is obtained from the needle it should be ad-vanced no further, to avoid the risk of meningitis.If there is no pus in the extradural space at thelevel of lumbar puncture the needle can be ad-vanced into the subarachnoid space and themyelogram can proceed. Not infrequently thecerebrospinal fluid contains increased proteinand sometimes a mild polymorphonuclear pleocytosis.
Treatment consists of urgent laminectomy (oranterior approach if necessary) and completeevacuation of the extradural abscess. The patientshould be started on high-dose antibiotics.
Subdural spinal abscesses (Fig. 15.13). These are rare. Some are associated with congenital dermal sinuses and others are a consequence ofhaematogenous spread from sepsis at a differentsite.
The clinical presenting features are similar tothose of extradural spinal abscess and meningitisis more likely to occur.
Intramedullary abscesses. These result from
SPINAL CORD COMPRESSION 219
Table 15.3 The incidence of microorganisms causing epidural spinal abscess varies with the populationstudied. In particular, infections due to Mycobacterium tuberculosis are more common in developing nationsand among the underprivileged. The incidence of unusual infections, such as fungi and parasites, isincreasing as a result of the rising numbers of immunosuppressed patients.
Type of infection Microorganism Incidence (%)
Unknown Unknown 3–13
Bacterial Staphylococcus speciesStaph. aureus 45–70Others 3–14
Streptococcus species: pyogenes, pneumoniae, viridans; anaerobic species 5–17
Gram-negative bacteria: Escherichia coli, Pseudomonas, Klebsiella, 3–18Proteus, Enterobacter species
Anaerobes: Bacteroides, Proprionibacterium species 3–10
Multiple microorganisms 5–10
Mycobacterial Mycobacterium tuberculosis 3–10
Fungal Aspergillus, Actinomyces, Nocardia, Cryptococcus, Sporotrichium 3–4
Other Parasites, syphilis Rare
KAY15 12/16/04 7:47 PM Page 219

220 CHAPTER 15
haematogenous spread, from a penetrating in-jury or in association with a congenital dermalsinus. They are rare, and patients present withfeatures of rapidly progressive spinal cord involvement.
Spinal tuberculosis (Pott’s disease)
Although spinal tuberculosis is uncommon inWestern countries it is still relatively prevalent insome Asian regions and in South America. Theosteomyelitis affects two or more adjacent verte-bral bodies and destroys the intervening discspace.
Spinal cord compression occurs as an early fea-ture due to tuberculous granulation tissue andpus, extruded sequestrae and fragments of intervertebral disc and vertebral collapse. Alternatively, the compression may be a latemanifestation resulting from the cord being dis-torted over the apex of an angular kyphus.
Treatment involves the use of antituberculouschemotherapy. If there is progressive cord com-pression the abscess, granulation tissue and dis-eased bone may be excised by an anterolateral
approach with access by a costotransversectomyor a more extensive vertebral resection.
Spinal arteriovenous malformation
Although spinal vascular malformations only oc-casionally cause actual compression of the spinalcord, the presenting features are those of primaryspinal cord involvement and may mimic a com-pressive lesion.
There are numerous morphological and patho-logical classifications of spinal vascular malfor-mations. Arteriovenous malformations (AVMs)constitute the most common type of vascularanomaly and occur with a frequency of approxi-mately 4% of all primary spinal tumours. Theyare much more frequent in males, occurring four times more frequently than in females.Other uncommon morphological types includetelangiectasia (capillary angiomas), cavernousmalformations and venous malformations com-posed entirely of veins.
The gross appearance of the spinal AVM ishighly variable. The malformation may be a sim-ple arteriovenous fistula involving a single coiledvessel and resulting in a fistulous communica-tion or, at the other extreme, it may be the so-called ‘juvenile’ type, in which there are multiple,large feeding arteries supplying an extensive di-lated vascular mass that may fill the spinal canaland permeate throughout the cord. This is thetype most frequently seen in children. The so-called ‘glomus’ type consists of single or mul-tiple vessels converging on a highly localizedvascular plexus which is drained by one or morearterialized veins.
The malformations may occur at any level andnot only involve the surface of the cord but fre-quently have an intramedullary component.
The most common type of spinal AVM in-volves the ‘nidus’ of the malformation being em-bedded in the dura covering the nerve root, andthe intradural malformation being the dilated ar-terialized veins of the dural nidus. This type ofmalformation was first recognized in the 1970s. Itis confined to the thoracolumbar and sacral re-gions and in nearly all cases there is a solitaryfeeding vessel supplying the nidus of malforma-
Fig. 15.13 MRI of subdural spinal abscess.
KAY15 12/16/04 7:47 PM Page 220

tion in the dura. Most cases occur in middle-agedor elderly men.
Presenting features
The clinical manifestations of AVM involving thespinal cord may be due to a number of mecha-nisms.• A steal phenomenon. It is possible that themalformation steals blood from the normal neur-al tissue and that this shunt causes local spinalcord hypoxia.• Thrombosis, which may cause catastrophicsymptoms.• Compression or, more appropriately, a pul-satile compression, which probably plays only asmall role.• Chronic increase of venous pressure, whichcould explain the progressive myelomalacia.• Haemorrhage.
The presenting features include the following.1 Back pain and root pain.2 Progressive neurological disability involving:
(a) paresis(b) sensory disturbance(c) sphincter dysfunction(d) impotence.
3 A sudden catastrophic neurological event due to either haemorrhage within the cord orthrombosis.4 Subarachnoid haemorrhage.
Pain is a common feature. Most patients pre-sent with a progressive neurological loss which,in half of the cases, is intermittent and recurrent.
About 15% of patients present with subarach-noid haemorrhage. The diagnosis is obviouswhen the haemorrhage is accompanied by para-plegia or quadriplegia. However, there may notbe any obvious associated cord manifestationsand the diagnosis of spinal subarachnoid haem-orrhage may be difficult. The onset of subarach-noid haemorrhage associated with suddensevere back pain is strongly indicative of an AVMof the spinal cord.
Investigations
MRI facilitates the diagnosis of these lesions.
Myelography is now rarely necessary but mayshow the tortuous vessels which will also beseen on CT scan following intrathecal iodinecontrast. The exact nature of the malformationcan only be determined by highly selectivespinal angiography (Fig. 15.14). The technique,requiring considerable expertise, has been facilitated by the use of digital subtraction angiography.
Treatment
The previous surgical technique of stripping themalformation from the surface of the cord hasnow been largely replaced by the recognition thatthe majority of these angiographic intraduralmalformations are merely the arterialized dilatedveins of the dural AVM. All that is necessary is toexcise the dural nidus or obliterate the arterial-ized draining vein from the nidus. It is not neces-sary to ‘strip away’ the intradural componentcovering the cord.
The surgical treatment of the true intraduralAVM, which often has a major intramedullary
SPINAL CORD COMPRESSION 221
Fig. 15.14 Spinal angiogram of arteriovenousmalformation and major feeding vessel.
KAY15 12/16/04 7:47 PM Page 221

222 CHAPTER 15
component, is fraught with hazard. The surgicaltechnique involves accurate identification of thedraining vessels at the level of the malformationand meticulous microsurgical dissection to pre-serve the normal cord tissue. The large, in-tramedullary, juvenile-type malformations arefrequently inoperable because an attempted surgical excision would inevitably result in devastating consequences. It may be possible tocombine angiographic embolization of thesemalformations with surgical excision.
Cervical myelopathy
Cervical myelopathy results from cervical cordcompression due to a narrow cervical vertebralcanal. The constriction of the canal enclosing thecervical cord is due to:• congenital narrowing• cervical spondylosis involving hypertrophy ofthe facet joints and osteophyte formation• hypertrophy of the ligamenta flava• bulging (or prolapse) of a cervical disc• excessive mobility, usually associated withcervical spondylosis.
The myelopathy results from:• direct pressure on the spinal cord• ischaemia of the cord due to compression andobstruction of small vessels within the cord, or tocompression of the feeding radicular arterieswithin the intervertebral foramen.
The morphological changes within the cord in-clude:• degeneration and loss of nerve cells, cavitationand proliferation of glia within the grey matter• demyelination of the lateral and posteriorcolumns• Wallerian degeneration in ascending tractsabove and descending tracts below the compression• proliferation of small blood vessels with thick-ening of the vessel walls• rare involvement of the anterior columns.
Clinical features
There is frequently a long history of slowly pro-gressive disability, although it is not unusual for
the neurological disability to increase rapidly,particularly following an injury.
The presenting features are pain and neurolog-ical disturbance attributable to cervical cord involvement.
Neck pain. This is not due to the cervical myelo-pathy itself but may occur as part of the degen-erative disease of the cervical spine. Narrowingof a neural foramen may result in entrapment of acervical nerve root causing brachial neuralgia.This is discussed in Chapter 14.
Muscular weakness. This is the most common ini-tial symptom and usually occurs earlier in thelower limbs. The patient initially notices clumsi-ness involving the hands and fingers, particular-ly in fine skilled movements, and dragging orshuffling of the feet. According to the level andextent of the cord lesion the signs in the upperlimbs will be predominantly of a lower or uppermotor neurone type and there will be a spasticparaparesis of the lower limbs.
Depending on the level of the compressionthere may be wasting of the suboccipital spinalmuscles, shoulder girdle muscles and biceps andtriceps. Fasciculation may be present but is usu-ally not severe. The deep tendon reflexes in theupper limbs will be depressed at, or exaggeratedbelow, the level of compression correspondingwith the presence of lower motor neurone andupper motor neurone damage, respectively. Thesupinator (brachioradialis) reflex may be of valuein localizing the level. If it is absent, but the reflexevokes flexion of the digits and sometimes the bi-ceps or triceps, this is regarded as evidence of alesion restricted to the C6 segment (the invertedsupinator reflex).
The lower limbs will show upper motor neu-rone changes due to corticospinal tract involve-ment with increased tone, a pyramidal pattern ofweakness, exaggerated reflexes and upgoingplantar responses.
Sensory symptoms. These frequently occur as dif-fuse numbness and paraesthesiae in the handsand fingers. Severe sensory loss is unusual inspondylolytic myelopathy, but an entirely nor-
KAY15 12/16/04 7:47 PM Page 222

mal sensory examination is also rare. The sensorychanges may be limited to the upper limbs andmay involve a dermatomal pattern if a particularnerve root is being compressed. Posterior columninvolvement will be reflected by a loss of joint po-sition and vibration sense.
The major differential diagnoses are:• spinal tumour• multiple sclerosis• motor neurone disease (particularly if onlyminor sensory changes)• syringomyelia (Chapter 11)• subacute combined degeneration of the cord.
Radiological investigations
Plain X-rays of the cervical spine may show a nar-row vertebral canal which could be either con-genital and/or due to spondylolytic degenerativedisease and osteophyte formation. Flexion–extension views testing the mobility of the cer-vical spine may show excessive movement of the vertebrae.
Although a CT scan without intrathecal con-trast may confirm a narrow canal, it is necessaryto perform MRI to confirm the nature and extentof the cord compression. An MRI will show theexact pathological basis for the compression and,in particular, whether it is primarily an anteriorcompression due to disc bulging or osteophyteformation or whether the compression is mostly from a posterior bulging hypertrophiedligamentum flava.
These are critical issues to be considered in theplanning of surgery (Fig. 15.15). An additionalbenefit of MRI is that it may show myelomalacia(high signal within the cord) indicating the sever-ity of the compression and a poorer prognosis fol-lowing surgery.
Treatment
Surgery is definitely indicated for clinically pro-gressive or moderate or severe myelopathy.There is some controversy over the indicationsfor the surgery in patients with a mild, non-pro-gressive myelopathy because these patients willoften improve with conservative treatment, in-
cluding rest in a cervical collar. However, surgeryis usually advisable, and is definitely indicated ifthere is marked compression of the cervical cordbecause these patients may suffer a severe cord
SPINAL CORD COMPRESSION 223
Fig. 15.15 Cervical canal stenosis. (a) Severe cervicalcanal stenosis with incomplete block on myelogramwhich has now been superceded by MRI. (b) MRI ofcervical canal stenosis.
(a)
(b)
KAY15 12/16/04 7:47 PM Page 223

224 CHAPTER 15
injury resulting in quadriparesis or quadriplegiafollowing even a minor injury to the cervical re-gion, such as a jolt or ‘whiplash’ type of injury. Afurther reason for advising early surgery is thatany existing neurological deficit may not im-prove following an operation, due to irreversiblechanges within the cervical cord, so that it ispreferable that the condition be arrested in itsearly stage.
The type of surgical procedure performed willdepend upon:• the extent of the compression• the number of vertebral levels involved• whether the compression is predominantly infront of or behind the cord• the presence of cervical instability.
A decompressive cervical laminectomy is thepreferred operation if there is a narrow canal overa number of levels and if there is significant pos-terior compression, usually from hypertrophiedligamenta flava.
If the compression is predominantly anteriorto the cord at one or two levels, usually due to anosteophyte or disc bulge, an anterior approachwith excision of the compressive lesion and ante-rior cervical fusion is preferred.
Whatever surgical procedure is used, extremecare must be taken in removing the compressionto avoid further injury to the highly sensitive cer-vical cord.
As indicated previously, surgery should arrestthe progress of the cervical myelopathy and onlyin a minority of patients will there be marked im-provement of neurological function followingthe operation. Asmall percentage of patients whohave severe neurological impairment and evi-dence of myelomalacia on MRI may have furtherneurological deterioration following surgery.
Further readingHulme A (1960) A surgical approach to thoracic inter-
vertebral disc protrusion. Journal of Neurology, Neuro-surgery and Psychiatry 23, 133–137.
Kaye AH, Black P McL (2000) Operative Neurosurgery.Churchill Livingstone, London, New York, Edinburgh.
Logue V (1979) Angiomas of the spinal cord: Review ofthe pathogenesis, clinical features and results ofsurgery. Journal of Neurology, Neurosurgery and Psychi-atry 42, 1–11.
Mack P (1979) Spinal metastases: Current status andrecommended guidelines for management. Neuro-surgery 5, 726–746.
Malis LI (1978) Intramedullary spinal cord tumours.Clinical Neurosurgery 254, 512–540.
Perin N, O’Laoire S, Benzel E, Connolly ES (1995) Treat-ment of thoracic disc herniation. In: Al-Mefty O,Origitano TC, Harkey HL, eds. Controversies in Neu-rosurgery. Thieme, New York.
Rosenblum B et al. (1987) Spinal arteriovenous malfor-mations: a comparison of dural arteriovenous fistu-las and intradural arteriovenous malformations in 81patients. Journal of Neurosurgery 67, 795–802.
Simeone FA, Rashbaum R (1977) Transthoracic disc ex-cision. In: Schymidek HH, Sweet WH, eds. CurrentTechniques in Operative Neurosurgery. Grune andStratton, New York, 324–333.
Solero CL et al. (1989) Spinal meningiomas: review of174 operated cases. Neurosurgery 25, 240–252.
Stein BM (1979) Surgery of intramedullary spinal cordtumours. Clinical Neurosurgery 26, 529–542.
Stein BM (1985) Spinal intradural tumours. In: WilkinsRH, Rengachery SS, eds. Neurosurgery. McGraw Hill,New York, 1048–1061.
Sundaresan N et al. (1979) Spinal chordomas. Journal ofNeurosurgery 50, 312–319.
Symon L, Kuyama H, Kendall B (1984) Dural arterio-venous malformations of the spine. Journal of Neuro-surgery 60, 238–247.
KAY15 12/16/04 7:47 PM Page 224

Trauma to the spinal column occurs at an inci-dence of approximately 2–5 per 100 000 popula-tion. Although the majority of spinal injuries donot affect the cord or spinal roots, about 10% willresult in quadriplegia or paraplegia.
Adolescent and young adult males are themost commonly affected group. Most of the seri-ous spinal cord injuries are a consequence of roadtraffic accidents (involving cars, motor bikes andbicycles) although there are other major causes ofspinal cord injury, for example water sports, es-pecially diving into shallow water, and injuriesfollowing skiing and horse riding accidents anddrunken falls.
Mechanisms of injury
Although severe disruption of the vertebral column usually causes serious neurologicaldamage, it is not always possible to correlate thedegree of bone damage with spinal cord injury.Minor vertebral column disruption does notusually cause neurological deficit, but occasion-ally may be associated with severe neurologicalinjury. The mechanism of injury will determinethe type of vertebral injury and neurologicaldamage.
Trauma may damage the spinal cord by direct compression by bone, ligament or disc,haematoma, interruption of the vascular supplyand/or traction.
The X-rays taken following a potential spinalcord injury show the vertebral alignment at thattime but do not necessarily indicate the amountof disruption that may have occurred at the moment of injury, or the degree of ligamentous
damage. In general the injuries can be classifiedby mechanism of the trauma.
Cervical spine
Flexion and flexion–rotation injuriesThis is the most frequent type of injury to the cervical spine; C5/6 is the most common site.Usually, one or both of the posterior facets aresubluxed or dislocated and may be locked in thisposition. There is extensive posterior ligamen-tous damage and these injuries are usually unsta-ble. The spinal cord may be compressed anddistracted, sustaining both direct damage andvascular impairment from involvement of theanastomotic segmental vessels or feeders andsecondary compression from subluxation with orwithout instability (Fig. 16.1).
Compression injuriesThe vertebral body is decreased in height andthere may be a wedge compression fracture or acomminuted fracture with the posterior aspect ofthe body (retropulsed fragment) encroachingupon the spinal canal. C5/6 is the most commonlevel for this fracture. The wedge fracture injuries are usually stable because the posterior bony elements and longitudinal ligaments are intact.However those with a significant retropulsedfragment are likely to have disruption of the as-sociated ligaments and thus have to be consid-ered unstable. When combined with a rotationforce in flexion, a ‘tear drop’ fracture may occur,with separation of a small anteroinferior frag-ment from the vertebral body, and these shouldalso be considered unstable. Of the patients who
CHAPTER 16
16 Spinal injuries
225
KAY16 12/17/04 10:06 AM Page 225

226 CHAPTER 16
do have spinal cord injuries about half have com-plete neurological deficit below the level of the lesion, the remainder having incomplete deficitwith the most damage being to the anterior aspect of the cord.
Hyperextension injuriesThese injuries are most common in the older agegroups and in patients with degenerative spinalcanal stenosis. Bony injury is often not demon-strated and the major damage is to the anteriorlongitudinal ligament secondary to hyperexten-sion. Most of the injuries result in incompletecord damage resulting from compression of thecord between the degenerative body and disc anteriorly, and the hypertrophic ligamentumflavum protruding posteriorly. The injuries arenearly always stable and a central cervical cordsyndrome (p. 228) is the most common neurolo-gical impairment.
Thoracolumbar spine
Flexion–rotation injuriesThese injuries occur most frequently at theT12/L1 level and result in anterior dislocation ofthe T12 on the L1 vertebral body. There is usuallydisruption of the posterior longitudinal ligamentand posterior bony elements. The inferior verte-bral body often sustains an anterior superiorwedge compression fracture. These are unstableinjuries which usually result in complete neuro-logical deficit of either the spinal cord, conus orcauda equina.
Compression injuriesThese injuries are common and the vertebralbody is decreased in height. They are usually stable injuries and neurological damage is uncommon.
Hyperextension injuryThis is a very uncommon mechanism of injury at
Fig. 16.1 (a) Cervical spine X-ray with C5/6 fracturedislocation. (b) Cervical spine CT reconstruction withC5/6 fracture dislocation. (c) Cervical spine CTreconstruction showing a perched facet with a fracture.
(a)
(b)
(c)
KAY16 12/17/04 10:06 AM Page 226

the thoracolumbar spine. It involves rupture ofthe anterior longitudinal ligament, rupture of theintervertebral disc and fracture through the in-volved vertebral body anteriorly. The injuries areunstable and usually cause severe cord injury.
Chance fracturesThis injury needs to be considered in patientswho are involved in a high-speed accident wear-ing lap belts without a shoulder harness. Theysustain a hyperflexion distraction injury to thethoracolumbar spine. The forward flexion andbending result in two potential types of injuries,and they can cause a fracture through the spinousprocess pedicle and vertebral body (Fig. 16.2a) ora fracture through the end-plate with disruptionof the facet joint and ligamentous structures (Fig. 16.2b). These injuries can easily be missedbecause of the unusual radiological findings.They could well be associated with internal injuries, especially abdominal injuries.
Open injuries
These may result from stab injuries or gunshotwounds resulting in cord damage due to the blastinjury, vascular damage and/or cord penetrationby the missile or bony fragments.
Types of neurological impairment
Immediately after a severe cord injury there is astate of diminished excitability of the isolatedspinal cord. This is referred to as ‘spinal shock’ or‘altered reflex activity’. The transient depressionin the segments caudal to the cord lesion is due tosudden withdrawal of a predominantly facilitat-ing or excitatory influence from supraspinal cen-tres. There is an areflexic flaccid paralysis. Theduration of spinal shock varies: minimal reflexactivity may appear within a period of 3–4 daysor may be delayed up to 6–8 weeks, the averageduration being 3–4 weeks.
The spinal cord injury is caused by:• the direct force applied to the cord• ischaemia due to vascular injury• secondary haemorrhage in and around thecord.
The degree of neurological injury will be determined by the extent and severity of thesemechanisms.
Complete lesions
The most severe consequence of spinal trauma iscomplete transverse myelopathy, in which allneurological function is absent below the level of
SPINAL INJURIES 227
(a) (b)
Fig. 16.2 Chance fracture: (a)through vertebral body andpedicle; (b) through end-plate, facet and ligament.
KAY16 12/17/04 10:06 AM Page 227

228 CHAPTER 16
the lesion, causing either a paraplegia or quadri-plegia, depending on the level. There will also be impairment of autonomic function includingbladder and bowel function.
Motor deficitInjuries to the spinal cord will result in an uppermotor neurone paralysis characterized by loss ofvoluntary function, increased muscle tone andhyperreflexia. Injuries to the lumbar spine caus-ing cauda equina injuries result in lower motorneurone paralysis characterized by reducedmuscle tone, wasting and loss of reflexes. A com-bination of upper and lower motor neurone lesions results from a thoracolumbar injury involving the conus medullaris and caudaequina.
Sensory deficitIn complete lesions the afferent long tracts carry-ing the various sensory modalities are inter-rupted at the level of the lesion, abolishingsensory appreciation of pain, temperature, touchand position and tactile discrimination below thelesion. Visceral sensation is also lost. Sensationmay decrease over a few spinal segments beforebeing lost altogether. Occasionally there is a levelof abnormally increased sensation, hyperaesthe-sia and hyperalgesia at or just below the lesion.
Autonomic deficitVasomotor control. Cervical and high thoracic le-sions above the sympathetic outflow at T5 maycause hypotension. Interruption of the sympa-thetic splanchnic vasomotor control will initiallycause a severe postural hypotension as a result ofimpaired venous return.
Temperature control. The patient with a completespinal lesion will not have satisfactory thermalregulation as there will be impairment of the au-tonomic mechanisms for vasoconstriction andvasodilatation.
Sphincter disturbanceThere is impairment of bowel and bladder control; this is discussed later.
Incomplete lesions
Anterior cervical spinal cordAcute anterior cervical spinal cord syndrome isdue to compression of the anterior aspect of thecord. This causes damage to the corticospinal andspinothalamic tracts, with motor paralysis belowthe level of the lesion and loss of pain, tempera-ture and touch sensation but relative preserva-tion of light touch, proprioception and positionsense, which are carried in the posterior columns.The exact pathophysiological process causingthis syndrome has not been precisely defined andit may be due either to stretch applied by the at-tachment of the dentate ligaments at the equator-ial plane of the cord or to ischaemic injury fromcompromise of the anterior spinal artery whichsupplies the anterior two-thirds of the cord (Fig. 16.3c).
Central spinal cordAcute central spinal cord syndrome is usuallydue to a hyperextension of the cervical spine withcompression of the spinal cord between the
Dorsalcolumns
Lateralspinothalamictract
Anteriorspinothalamictract
Lower limb
Chest & abdomen
upper limb
Corticospinal tract
Fig. 16.3 (a) Normal cord cross-section. (b) Centralcord syndrome. (c) Anterior spinal artery syndrome.(d) Brown-Séquard syndrome. (e) Posterior columnsyndrome.
(a)
(b)
(c)
(d) (e)
KAY16 12/17/04 10:06 AM Page 228

degenerative intervertebral disc and osteophyteanteriorly and the thickened ligamentum flavumposteriorly. The cord damage is located centrally,with the most severe injury to the more centrallylying cervical tracts which supply the upperlimbs. There is disproportionately greater weak-ness in the upper limbs in comparison to thelower extremities below the level of the injury.Sensory loss is usually minimal, although this is variable and frequently occurs in no specificpattern (Fig. 16.3b).
Brown-Séquard syndromeThe Brown-Séquard syndrome results fromhemisection of the spinal cord (Chapter 1) asfrom a stab wound, although it infrequently fol-lows a blunt injury. There is ipsilateral paralysisof the limbs below the level of the lesion with lossof pain, temperature and touch on the oppositeside of the body. The posterior columns will be in-terrupted ipsilaterally, but as some fibres crossthere is not a great deficit (Fig. 16.3d).
Spinal cord concussion
There may be a transient loss of function fromconcussion of the spinal cord. The exact patho-logical processes involved in spinal cord concus-sion are not clear but they are probably similar tothose occurring in cerebral concussion, resultingin temporary impairment of neuronal function.Recovery usually begins within 6 hours andshould be detected within 48 hours.
Management of spinal injuries
As with head injuries, there is little that can bedone to repair the damage caused by the initialinjury and therefore the major efforts are directedtowards prevention of further spinal cord injuryand the complications resulting from the neuro-logical damage. The general principles of man-agement are:• prevention of further injury to the spinal cord• reduction and stabilization of bony injuries• prevention of complications resulting fromspinal cord injury• rehabilitation.
Initial treatment
The first aid management of patients with injuries to the spinal column and spinal cord requires the utmost caution in turning and liftingthe patient. The spine must be handled with greatcare to avoid inflicting additional damage. Beforemoving the patient sufficient help should beavailable to provide horizontal stability and longitudinal traction. Spinal flexion must beavoided. A temporary collar should be applied ifthe injury is to the cervical spine. An assessmentshould be made for other injuries to the chest, abdomen or limbs.
Hypotension and hypoventilation imme-diately following an acute traumatic spinal cordinjury may not only be life-threatening but mayalso increase the extent of neurological impair-ment. Resuscitation techniques may need to bemodified to ensure that the spine remains stable.Respiratory insufficiency may require oxygentherapy and ventilatory assistance. Loss of sym-pathetic tone may result in peripheral vaso-dilatation with peripheral vascular pooling and hypotension. Treatment will include the use of intravascular volume expanders, alpha-adrenergic stimulators, intravenous atropine andoccasionally the use of a transvenous pacemaker.There must be careful attention to the body tem-perature — the spinal patient is poikilothermicand will tend to assume the temperature of theenvironment. Body temperature must be pre-served in cold weather and the patient must notbe overheated in warm weather. A nasogastrictube should be passed to avoid problems associ-ated with vomiting due to gastric stasis and par-alytic ileus. A urinary catheter should be passedto prevent the complications of bladder overdis-tension, although intermittent catheterizationmay become preferable later. Prophylaxis fordeep vein thrombosis and subsequent pul-monary embolus should be commenced as soonas possible using low-dose heparin (5000 unitssubcutaneously twice daily) or low molecularweight heparins. Some centres also favour usingvarious types of compression stockings on thelower limbs.
SPINAL INJURIES 229
KAY16 12/17/04 10:06 AM Page 229

230 CHAPTER 16
Radiological investigationsPlain cervical spine X-rays and computerized to-mography scan will show the bony injuries, andmagnetic resonance imaging is very helpful inshowing the associated cord, soft tissue and liga-mentous pathology (Fig. 16.4). If a cervical spineinjury is suspected (in the absence of neurologi-cal signs or symptoms) but the plain X-ray andCT scan show no abnormality, the X-rays shouldbe carefully repeated in flexion and extension toexclude instability due to ligamentous damage.
Spinal reduction and stabilizationAs soon as the systemic parameters have beenstabilized, attention should be directed to align-ment and stabilization of the spine. The use ofskeletal traction for the restoration and/or main-tenance of the normal alignment of the spinal col-umn is a time-honoured and effective treatment.There are various types of cervical traction de-vices. The spring-loaded tongs have becomepopular because of their ease of application andmaintenance. The usual practice is to applyweight to the traction device to a maximum of5 lb or 2.25 kg for each level below the occiput(e.g. C6 = 30 lb or 13.5 kg). It is usual to commencewith half the maximum weight and, under X-rayor fluoroscopic control, gradually add weightsup to the maximum if necessary (Fig. 16.5). These
patients will require analgesia. Their bodyweight is utilized for counter traction by tiltingthe entire bed in a head-up position. It is impor-tant to maintain a neutral spine. Extreme careshould be taken to avoid distraction at the frac-ture site as the traction on the underlying cordmay worsen the neurological injury. Reduction of
Fig. 16.4 MRI of spinal injury showing the bonedamage and cord injury with localized syrinx.
Fig. 16.5 The reduction of fractures following tractionin patients illustrated in Fig. 16.1. (a) The plain X-rayshows the distracted disc spaces. (b,c) The CTreconstruction shows normal alignment andcorrection of perched facet.
(a)
(b)
(c)
KAY16 12/17/04 10:06 AM Page 230

facet dislocations may be more difficult and re-quire more weight for the traction. Some advo-cate manipulation of the neck under fluoroscopiccontrol while weight is being applied to accom-plish reduction of locked facets. In Australia andEurope cervical traction under general anaesthe-sia has been used for closed reduction of somefracture dislocations but this has not been popu-lar in the United States. Open surgery may benecessary to reduce the fracture — subluxationwith overriding and locked facet joints.
Following reduction the position may be maintained with skeletal traction or halo immobilization.
Injuries of the thoracolumbar spine can usually be managed conservatively by posturalreduction in bed. The correct posture must bemaintained during positioning on the side, aswell as on the back; this is achieved by the appro-priate placement of bolsters and pillows by aturning team.
Indications for surgical interventionThere has been considerable controversy oversurgical intervention in patients with spinal cordinjuries. The damage to the spinal cord occursprincipally at the time of the injury and it is notsurprising that there has been no evidence toshow improved neurological function from acuteoperative decompression of the spine. The fol-lowing are the general indications for surgical intervention.1 Progression of neurological deficit is an ab-solute indication. It requires emergency interven-tion if a compressive lesion is demonstrated byeither MRI or CT scan.2 Patients who have a partial neurological injury,with preservation of some distal neurologicalfunction, and who fail to improve should havefurther radiological assessment. Surgery shouldbe considered if this shows persisting extrinsiccompression of the spinal cord within the canal(particularly from a herniated cervical disc), a de-pressed fractured lamina or an osteophytic bar,although removal of the compression may not result in any neurological improvement.3 An open injury from a gunshot or stab woundshould be explored to remove foreign particles,
elevate bone spicules and, if possible, repair thedura.4 The most common indication for operative in-tervention is to stabilize the spine. This is usuallyundertaken:
(a) if there is gross instability, particularly inthe presence of an incomplete neurological lesion(b) if it has not been possible to reduce lockedfacets by closed reduction — posterior reduc-tion and fusion is appropriate(c) if operative procedures are needed to stabi-lize the unstable cervical spine and so avoidprolonged bed rest; these are favoured bymany spinal injury units (Fig. 16.6).
Other treatments for spinal cord injuryNumerous pharmacological agents have been investigated in experimental laboratory modelsbut as yet there has been no controlled clinicalstudy to show the usefulness of these agents inspinal cord injury. The treatments include gluco-corticoids, diuretics, local hypothermia, barbitu-rates and endogenous opiate agonists. Althoughthere is no proven benefit, some spinal units useglucocorticoids and osmotic diuretics for thetreatment of oedema. The early use of high-dosedexamethasone may be beneficial, but there is noconclusive proof.
Further management
Following reduction and immobilization of the
SPINAL INJURIES 231
Fig. 16.6 Postoperative X-ray — anterior cervicaldiscectomy and bone and plate fusion.
KAY16 12/17/04 10:06 AM Page 231

232 CHAPTER 16
fractures the principles of the continuing care in-volve the avoidance of potential complications inpatients who are paraplegic or quadriplegic, andearly rehabilitation, which commences as soon asthe injury is stabilized.
General care
Careful attention to the general condition andmetabolic state is essential following the injury;patients frequently develop a negative nitrogenbalance and may become anaemic. Urinary tractor other infections will aggravate the metabolicdisorders. The patients and their relatives will re-quire skilled counselling and emotional supportduring the treatment and rehabilitation period.
Skin care
Meticulous attention to pressure areas will avoidthe development of pressure sores which wouldseriously complicate the recovery and rehabilita-tion of the patient.
Gastrointestinal complications
Paralytic ileus occurs in acute spinal cord paraly-sis and if this is unrecognized, the patient is atrisk from vomiting and aspirations. Anasogastrictube should be passed in the initial managementof the patient. Acute gastric dilatation may alsodevelop and is also treated by nasogastric suc-tion. In 3–5% of patients with acute spinal cordinjuries acute peptic ulceration occurs.
Bladder care
Urinary tract problems are a major cause of potential morbidity and mortality. During the pe-riod of spinal shock the areflexic, flaccid paralysisbelow the level of the lesion includes bladderfunction. The patient will develop acute retentionwith overflow incontinence and a catheter is required. Reflex activity returns in upper motorneurone lesions as the phase of spinal shock pass-es. The spinal micturitional reflex arc is intact in alesion above the conus and an autonomic type ofbladder results. The bladder will empty involun-
tarily as it fills with urine. The capacity may beless than normal, but there is good voiding pres-sure capacity. There is no sensation of bladderfullness. In a lower motor neurone lesion thespinal micturitional reflex is interrupted and anautonomous bladder results. Bladder function isgoverned by a myogenic stretch reflex inherent inthe detrusor fibres themselves. This type of dys-function is characterized by a linear increase inintravesical pressure, with filling until capacity isreached. Urine may then flow past the sphincterby overflow incontinence. In a mixed upper andlower motor neurone lesion, such as with a conusmedullaris and cauda equina injury, it is possibleto have a flaccid lower motor neurone detrusorand a spastic sphincter, as well as the reverse.
The principles of management of the bladderconsist of maintaining proper bladder drainageto prevent dilatation of the upper urinary tractand renal impairment, and the treatment of uri-nary tract infections. A catheter is passed initiallyand bladder training is commenced after the period of spinal shock. The details of bladdertraining and management depend on whetherthe neurogenic bladder has resulted from anupper or a lower motor neurone lesion and on theresults of a cystometrogram showing the intra-vesical volume pressure relationship.
Limb care
It is essential that the paralysed limbs should beput through their full range of movements regu-larly. Physiotherapy, in particular, is essential to prevent contractures as the tone returns andspasticity develops.
Special cervical spine injuries
Jefferson’s fracture
Jefferson described bilateral fractures of the pos-terior arch of the atlas from a direct vertical blowto the head in four patients. The mechanism ofthe fracture is due to the head pressing down onthe spinal column and the atlas being squeezedbetween the occipital condyles above and theaxis below. The grooves for the vertebral artery
KAY16 12/17/04 10:06 AM Page 232

are the sites where the arches of the atlas areweakest, and when fractures occur at this sitebursting fragments are displaced outwards.
Fractures of the odontoid process
A fracture of the odontoid process may occur atthe tip (type I) through the base of the dens (typeII) or at the base and extend into the adjacent C2vertebral body (type III). The fractures that occurat the base of the dens are the most common andmay cause disruption of the blood supply to the dens, resulting in non-union of the fracture(Fig. 16.7).
Many of the odontoid fractures can be treated
by immobilization in a firm brace or halo for 4months. If there is non-union and instability aposterior C1/2 fusion will be necessary. Anteriorscrew internal fixation of the odontoid fracturehas been advocated but is indicated in certain situations.
Hangman’s fracture (Fig. 16.8)
This fracture is the avulsion of the laminar archesof C2 with dislocation of the C2 vertebral body onC3. It is the characteristic lesion resulting from judicial hanging.
Further readingDickman C, Kalfas I, Traynel V, Cooper DR (1995) Treat-
ment of transmutic instability of the cervical spine.In: Al-Mefty O, Origitano TC, Harkey HL, eds. Controversies in Neurosurgery. Thieme, New York.
Harris P et al. (1980) The prognosis of patients sustain-ing severe cervical spine injury (C2–C7 inclusive).Paraplegia 18, 324–330.
Heiden JS et al. (1975) Management of cervical spinalcord trauma in Southern California. Journal of Neuro-surgery 43, 732–736.
Norrell H (1978) The treatment of unstable fracturesand dislocations. Clinical Neurosurgery 25, 193–208.
Norrell H (1980) The early management of spinal in-juries. Clinical Neurosurgery 27, 385–400.
Sherk HH (1978) Fractures of the atlas and odontoidprocess. Orthopaedic Clinics of North America 9,973–984.
Wood-Jones F (1913) The ideal lesion produced by judi-cial hanging. Lancet i, 533.
SPINAL INJURIES 233
OdontoidType I
OdontoidType III
OdontoidType II
Fig. 16.7 Fractures of theodontoid process.
Fig. 16.8 Hangman’s fracture.
KAY16 12/17/04 10:06 AM Page 233

Peripheral nerves may be trapped, compressedor injured at any position along their course, al-though there are certain regions where they areespecially vulnerable. Nerve entrapments occurparticularly where the peripheral nerve passesthrough a tunnel formed by ligaments, boneand/or muscle. Traumatic injury to the nerve occurs when it is either relatively superficial andexposed, or lying adjacent to bone, where it maybe directly injured by the jagged, fractured endsof the bone.
Peripheral nerve entrapment
Entrapment neuropathies occur when nervespass near joints. In this position they are particu-larly vulnerable to compression:• due to bone and joint disorders in the region• because they frequently pass under a tendi-nous arch• which may be exacerbated by movement ofthe adjacent joint.
Less common forms of entrapment neuropa-thy may lie at a distance from a joint. Table 17.1shows a list of the common and less frequent en-trapment neuropathies. Although thoracic outletsyndrome does not cause compression of a peripheral nerve, it will be considered in thischapter because the clinical features may mimicperipheral nerve entrapment and because thepathophysiology is similar to compression of aperipheral nerve.
Carpal tunnel syndrome
This is by far the most common nerve entrap-
ment; women are affected four times more oftenthan men.
The carpal tunnel is a fibro-osseous tunnel onthe palmar surface of the wrist (Fig. 17.1). Thedorsal and lateral walls consist of the carpalbones, which form a crescentic trough. Atunnel ismade by the fibrous flexor retinaculum (trans-verse carpal ligament) which is attached medially to the pisiform and hook of the hamateand laterally to the tuberosity of the scaphoid andcrest of the trapezium. The contents of the tunnelare the median nerve and the flexor tendons ofthe flexor digitorum superficialis, flexor digito-rum profundis and flexor pollicis longus.
Although the features of carpal tunnel syn-drome may present at any stage throughout theadult years, the initial symptoms often occur inwomen during pregnancy and in both sexeswhen they are performing unusually strenuouswork with their hands. There are a number ofsystemic conditions which are associated with,and may predispose to, carpal tunnel syndrome;these include:• pregnancy and lactation• contraceptive pill use• rheumatoid arthritis• myxoedema• acromegaly.
Any local condition that will decrease the sizeof the carpal tunnel will also predispose to carpaltunnel syndrome. Such conditions include a ganglion, tenosynovitis, unreduced fractures ordislocations of the wrist or carpal bones, and any local arthritis.
The principal clinical features of carpal tunnelsyndrome are:
CHAPTER 17
17 Peripheral nerve entrapments,injuries and tumours
234
KAY17 12/16/04 7:57 PM Page 234

• pain• numbness• tingling.
The pain, which may be described as burningor aching, is frequently felt throughout the wholehand and not just in the lateral three digits. Thereis often a diffuse radiation of pain up the forearmto the elbow and occasionally into the upper arm.The symptoms are worse at night, and on waking
the patient has to shake the hand to obtain any re-lief. The pain is also aggravated by activity of thehand.
Although the numbness and tingling is princi-pally in the lateral three and a half fingers, in thedistribution of the median nerve, the patient frequently complains of more diffuse sensoryloss throughout the fingers. This symptom is alsoworse at night and with activity.
The patient frequently complains that the handfeels ‘clumsy’, but with no specific weakness.
There are often only minimal signs of mediannerve entrapment at the wrist. The Tinel’s signmay be elicited by tapping over the median nervebut its presence or absence has little diagnosticvalue.
If the compression has been prolonged and severe there may be signs of median nerve dysfunction, including:• wasting of the thenar muscle• weakness of muscles innervated by the distalmedian nerve, especially abductor pollicis brevis• diminished sensation over the distribution ofthe median nerve in the hand.
Some patients, particularly the elderly or diabetic, may present with only minor discom-fort but rapid wasting, weakness and numbnessin the hand.
The clinical diagnosis can be confirmed byelectromyographic examination (EMG). The
PERIPHERAL NERVE ENTRAPMENTS, INJURIES AND TUMOURS 235
Table 17.1 Entrapment neuropathies.
Median nerveCarpal tunnel syndrome*Supracondylar entrapmentCubital fossa entrapmentAnterior interosseus nerve entrapment
Ulnar nerveTardy ulnar palsy*Deep branch of ulnar nerve
Radial nerve — posterior interosseus nerveSuprascapular nerveMeralgia paraesthetica — lateral femoral
cutaneous nerve of thighSciatic nerveTarsal tunnel syndromeThoracic outlet syndrome*
*The more common entrapment neuropathies.
Capitate Lunate Scaphoid
Trapezium
Pisiform Scaphoid
Trapezium
Hamate
Extensor pollicis brevis
Flexor pollicis longus
Median nerveFlexor retinaculum
Ulnar nerve and artery
Pisiform
Triquetrum
Tendons of flexor digitorum superficialis and profundus
Fig. 17.1 The carpal tunnel,just distal to the wrist.
KAY17 12/16/04 7:57 PM Page 235

236 CHAPTER 17
earliest feature of carpal syndrome is prolongedsensory latency, and the sensory action potentialsmay show a diminished amplitude and are oftenabsent. The distal motor latency may also be prolonged. Needle examination may show lossof motor units and presence of denervation potentials in the thenar muscles.
TreatmentSurgery is a simple and effective method of relieving the compression and curing the symptoms. However, conservative treatment isappropriate if:• the symptoms are mild or intermittent• there is a reversible underlying precipitatingcondition such as pregnancy or oral contracep-tive pill use.
Conservative treatment includes the use of awrist splint, particularly at night, and non-steroidal anti-inflammatory medication. Corti-costeroid injection into the carpal tunnel issometimes advocated but, at best, this offers onlytemporary relief and may damage the mediannerve.
The operation involves the division of the flexor retinaculum through a curvilinear incisionmade in the palm of the hand extending from thedistal wrist crease and exposing the whole of theflexor retinaculum in the hand. The operation canbe performed under general, regional or localanaesthesia, with or without a tourniquet. It is essential to divide the whole of the retinaculumand to avoid damage to the recurrent branch ofthe median nerve that innervates the thenar mus-cles. Although this important nerve usually arises distally, from the median nerve on the radial side in the carpal tunnel, it is common for itto have an anomalous origin and course beforeentering the thenar muscles. Recently an endo-scopic approach to decompress the nerve hasbeen advocated as a means of reducing postoper-ative wound discomfort. However, endoscopicdecompression does have a higher risk of injuryto the median nerve and most surgeons prefer anopen decompression.
Although some surgeons advocate postopera-tive immobilization of the hand it is preferable toencourage movement of the upper limb, includ-
ing the fingers and wrist, to avoid stiffness of thejoints.
Other median nerve entrapments
The median nerve may occasionally be com-pressed at other sites, particularly:• in the cubital fossa• under a supracondylar process of the humerusand Struther’s ligament.
Cubital fossaThe median nerve may occasionally be com-pressed in the region of the cubital fossa:• under the bicipital aponeurosis• as it passes between the two heads of thepronator teres muscle• as it passes under the fibrotendinous arch ofthe origin of the flexor digitorum superficialismuscle.
It is not usually possible to differentiate theexact cause of the compression prior to explo-ration. The symptoms are similar and have an in-sidious onset. There is usually a vague pain in theforearm, with increasing weakness of the handand numbness in the thumb and index finger.The clinical findings are of weakness of the medi-an nerve-innervated muscles, especially the flex-or pollicis longus, the radial half of the flexordigitorum profundus and the thenar muscles,and of numbness in the distribution of the median nerve.
Although the symptoms may resolve with con-servative treatment, which should include rest ofthe limb and avoidance of heavy work, it is usu-ally necessary to explore the nerve and relieve thecompression.
The anterior interosseous nerve arises fromthe lateral aspect of the median nerve as it passesbetween the two heads of the pronator teres mus-cle. The anterior interosseous nerve syndrome isusually due to compression of the nerve by thetendinous origin of the deep head of pronatorteres and is characterized by selective paralysis ofthe flexor digitorum profundus of the second andthird fingers, the pronator quadratus and theflexor pollicus longus. There are no sensorychanges and the patient is classically unable to
KAY17 12/16/04 7:57 PM Page 236

push the distal phalanges of the thumb and indexfinger together. Surgery to decompress the nerveis often necessary.
Compression of the median nerve under asupracondylar process of the humerus is rare. Afibrous ligament (Struther’s ligament) extendsfrom the anomalous bony process arising fromthe anteromedial surface of the humerus — thesupracondylar process — to the region of the medial epicondyle, and forms a fibro-osseousforamen through which the median nerve andbrachial artery pass. The clinical features are of aprogressive median nerve palsy, particularlywith pronator weakness, which distinguishesthis syndrome from more distal median nerve entrapment. Surgery consists of excision ofStruther’s ligament and removal of the bonyspur.
Ulnar nerve entrapment at the elbow
The ulnar nerve runs behind the medial epi-condyle of the humerus. It enters the forearmthrough a fibro-osseous tunnel formed by theaponeurotic attachment of the two heads of flex-or carpi ulnaris, which span from the medial epi-condyle of the humerus to the olecranon processof the ulnar, forming the cubital tunnel (Fig. 17.2).The ligament tightens during flexion of the elbowand the volume of the cubital tunnel decreaseswith increasing pressure over the underlyingnerve. Injuries in the region producing deformityof the elbow predispose to compression, al-
though the features of ulnar nerve entrapment donot usually appear for some years. This delay inthe appearance of symptoms led to the term‘tardy ulnar palsy’.
In most cases there is no particular predispos-ing cause. In a minority there are underlying factors which predispose to nerve entrapment,including lengthy periods of bed rest from comaor major illness and poor positioning of theupper limbs during long operations, causing prolonged pressure on the nerve, arthritis of the elbow, ganglion cysts of the elbow joint anddirect trauma.
The clinical features consist of:• paraesthesia and numbness in the ring and little fingers of the hand and the adjacent medialborder of the hand• wasting of the ulnar innervated muscles of thehand (particularly the hypothenar eminence andinterossei muscles)• weakness.
The most common initial presenting feature isparaesthesia in the ring and little fingers and theadjacent ulnar border of the hand. The patientmay complain of a painful ‘burning’ or ‘aching’in the forearm and/or the hand, but pain is usu-ally not a prominent symptom. There will be pro-gressive clumsiness of the hand with impairmentof fine movements.
In advanced cases there will be wasting of theulnar-innervated muscles, particularly notice-able in the hypothenar eminence and dorsal in-terossei. Entrapment of the ulnar nerve will leadto weakness of the muscles of the hypothenareminence, the interossei, the two medial lumbri-cals, the adductor pollicis, the flexor digitorumprofundus (ring and little fingers) and the flexorcarpi ulnaris. Paralysis of the small muscles of thehand causes ‘claw hand’, this posture being produced by the unopposed action of the antagonists of the paralysed muscles. Since the interossei cause flexion of the fingers at themetacarpophalangeal joints and extension at theinterphalangeal joints, when these muscles areparalysed the opposite posture is maintained bythe long flexors and extensors, which cause flex-ion at the interphalangeal joints and hyperexten-sion at the metacarpophalangeal joints. This is
PERIPHERAL NERVE ENTRAPMENTS, INJURIES AND TUMOURS 237
Medialepicondyle
Fascial roofof cubital tunnel
Olecranon
RadiusFlexorcarpiulnarisUlna
Ulnar nerve
Fig. 17.2 The ulnar nerve passing behind the medialepicondyle of the humerus and through the cubitaltunnel.
KAY17 12/16/04 7:57 PM Page 237

238 CHAPTER 17
most pronounced in the ring and little fingers asthe two radial lumbricals, innervated by the me-dian nerve, compensate to some degree for theimpaired action of the interossei on the index andmiddle fingers. Froment’s sign is demonstratedby asking the patient to grasp a piece of card-board between the index finger and thumbagainst resistance. There will be flexion of the interphalangeal joint of the thumb because themedian-innervated flexor pollicis longus is used,rather than the weakened adductor pollicis. Thesensory disturbance will be in the little finger andmedial half of the ring finger and medial borderof the hand.
The diagnosis will be confirmed by nerve conduction studies. The conduction velocity inthe ulnar nerve across the elbow is slowed, theamplitude of the motor response in the abductordigiti minimi is decreased, and the sensory latency is prolonged. Needle examination of theulnar-innervated muscles will show reduction in the voluntary motor unit action potentials.
TreatmentConservative treatment may be tried if the clinical features are minor and not progressive. It should include the advice to avoid pressure on the nerve at the elbow during reading, sittingor lying and to cease heavy work with the arms. Non-steroidal anti-inflammatory medica-tion may be helpful.
Surgery is indicated if there are progressivesymptoms or signs and if there is any wasting orweakness. The surgical procedure must releasethe nerve from compression and prevent furtherdamage to the nerve from flexion and extensionmovement of the elbow. The surgical techniqueshave included:• neurolysis• medial epicondylectomy• transposition of the nerve.
The nerve is explored through a curvilinear in-cision centred just behind the medial epicondyle.The dense fascia over the nerve, forming the roofof the cubital tunnel, is divided, extending fromthe medial intermuscular septum above distallyto where the nerve runs between the two heads of the flexor carpi ulnaris at which position the
nerve is often noted to be compressed. If theelbow is then flexed the nerve may be found to bealso trapped behind the medial epicondyle, sothat it is further traumatized during movementof the elbow, despite the bridge of fibrous tissuebeing divided. Excision of the medial epicondylethrough a subperiosteal resection of the condyleallows the nerve to move freely during a fullrange of movement of the elbow. Transposition ofthe nerve is not usually necessary although it isrecommended by some surgeons.
Ulnar nerve compression at the wrist
The ulnar nerve may occasionally be trapped andcompressed at the wrist, and the clinical featuresof this compression depend on the exact positionof the entrapment.
The deep branch of the ulnar nerve may becompressed at the pisohamate hiatus. The condi-tion can sometimes arise spontaneously, butthere is usually a history of injury, often of aheavy and repetitive type. Most of the patientsare men and it classically occurs in those usingheavy jack hammers or wire-cutting shears, andin motor cyclists, where there is repetitive traumaover the ulnar aspect of the hand. There ismarked wasting and weakness of the hand mus-cles innervated by the ulnar nerve. Flexor carpiulnaris and the medial half of the flexor digito-rum profundis are not impaired. Although thereis often spontaneous improvement after the trauma is ceased, surgery may be necessary to relieve the compression.
Less commonly the ulnar nerve is compressedat the wrist a little more proximally in ‘Guyon’scanal’ which is an oblique fibro-osseous tunnelthat lies within the proximal part of the hy-pothenar eminence. The roof of the tunnel isformed by the palmar fascia and palmaris brevismuscle. The floor is formed by the flexor retinac-ulum and the pisohamate ligament. The terminalpart of the tendon of flexor carpi ulnaris and thepisiform bone form the medial wall. The distalpart of the lateral wall is formed by the curvedulnar surface of the hook of the hamate. The canalcontains the ulnar nerve and ulnar artery. In themiddle of the canal the ulnar nerve divides into
KAY17 12/16/04 7:57 PM Page 238

the superficial and deep branches. The superfi-cial branch continues distally and supplies asmall branch to the palmaris brevis muscle andsensation to the medial half of the ring finger andlittle finger. The deep motor branch passes later-ally around the hook of the hamate and under thepisohamate hiatus, a fibrotendinous arch.
Compression in Guyon’s canal, often by a gan-glion (Fig. 17.3), leads to features similar to themore distal compression of the deep branch ofthe ulnar nerve, as well as to sensory loss and in-volvement of the palmaris brevis muscle. Sensa-tion is retained on the dorsal aspect of the hand,as the distal branch of the ulnar nerve arises prox-imal to the wrist. The symptoms may resolvewith conservative therapy but surgical decom-pression is often required.
Suprascapular nerve entrapment
The suprascapular nerve is occasionally com-pressed in the suprascapular notch under thesuprascapular ligament.
There is an occasional acute, precipitating trau-matic event, although there is usually no readilyidentifiable prior injury. The earliest presentingfeature is deep pain around the suprascapular re-gion and shoulder. The frequent clinical findingis marked atrophy of the supra- and infraspina-tus muscles. There is often weakness of externalrotation of the arm.
The important differential diagnoses are a rotator cuff injury of the shoulder, or a C5 nerveroot compression which will cause weakness ofshoulder abduction. Nerve conduction studieswill aid in the diagnosis. Section of the supras-capular ligament usually satisfactorily relievesthe compression and provides good sympto-matic relief.
Posterior interosseous nerve entrapment
The radial nerve divides into two terminalbranches — the superficial radial nerve, and theposterior interosseous nerve which supplies ex-tensor carpi radialis brevis and the supinatormuscles before it passes under a tough fibro-tendinous ring at the origin of the supinator mus-
cle. The nerve traverses the supinator muscle,winds around the lateral side of the radius andemerges on the dorsal aspect of the forearm,where it supplies the extensor muscles of thewrist and fingers. The usual site of entrapment is at the origin of the supinator muscle under thefibrotendinous ring (arcade of Frohse), althoughother adjacent skeletal abnormalities may alsocause a traumatic neuritis in the region.
The clinical presentation involves an inabilityto extend the fingers at the metacarpophalangealjoints (finger drop). There is not usually any wristdrop because the extensor carpi radialis longus issupplied by the radial nerve proximal to its terminal branching.
If symptoms do not improve spontaneouslywith conservative therapy, exploration and divi-sion of the compressing band is necessary.
PERIPHERAL NERVE ENTRAPMENTS, INJURIES AND TUMOURS 239
Fig. 17.3 MRI showing ganglion compressing ulnarnerve in Guyon’s canal.
(a)
(b)
KAY17 12/16/04 7:57 PM Page 239

240 CHAPTER 17
Thoracic outlet syndrome
Thoracic outlet syndrome is an entrapment neuropathy of the brachial plexus at the root ofthe neck. Numerous upper limb pain problemsare frequently and erroneously attributed tocompression at the thoracic outlet. Although thebrachial plexus may be trapped at the cervico-brachial junction, it is a relatively uncommoncause of upper limb symptoms.
The neurovascular bundle, consisting of theroots and trunks of the brachial plexus and thesubclavian artery (Fig. 17.4), emerges from the neck into the axilla through a slit or trianglewith a narrow base bounded anteriorly by thescalenus anterior, posteriorly by the scalenusmedius and inferiorly by the first rib.
Historically, a cervical rib was thought to bethe cause of compression of the neurovascularbundle. However, in the majority of patients thesymptoms are due to a compressive fibrous band,continuous with the medial edge of scalenusmedius, which extends from an elongated trans-verse process of C7 (a ‘forme fruste’ of a cervicalrib) to the first rib and produces its symptoms bycompression of the brachial plexus, particularlythe lower trunk.
The presenting features may be due to eitherneural or vascular compression and the features
of either one of these will usually predominate. Ifthere is a cervical rib the patient may present withvascular features of increasing pallor and cold-ness of the hand which, if variable in intensity,may simulate Raynaud’s syndrome. The clinicalfeatures of neural compression are usually grad-ual and are more likely to occur with a fibrousband than a full cervical rib. The major present-ing features are:• arm pain• motor weakness and sensory loss caused bycompression of the lower trunk of the brachialplexus.
The syndrome occurs typically in young tomiddle-aged females and the pain may be diffuseor in the distribution of the lower trunk of thebrachial plexus. Atrophy may be present in thethenar and hypothenar eminence and other in-trinsic hand muscles, and weakness may involvenot only the small muscles of the hand but some-times the long flexors, particularly on the ulnarside of the forearm. There may be diminishedsensation in the distribution of the C8 and T1 der-matomes.
Plain X-rays may show the characteristic elon-gated transverse process of C7. Nerve conduc-tion studies and electromyography may helpwith the diagnosis. Preoperative MRI is helpfulin excluding other cervical pathology as a basisfor the presentation.
Surgery should only be performed if there isunequivocal clinical evidence of neural entrap-ment. As indicated earlier the condition has oftenbeen erroneously diagnosed as the cause of non-specific arm pain. If there are objective neurologi-cal signs of entrapment the surgical procedure isdivision of the fibrous band or, in the case of a cer-vical rib, excision of the bone to relieve com-pression. These procedures are best performedthrough a supraclavicular approach using mag-nification to identify and protect the neural struc-tures. A transaxillary approach may also be usedto remove a cervical rib.
Lower limb entrapment neuropathies
Entrapment neuropathies of the lower limb areuncommon.
Scalenus medius
Scalenus anterior
C5, C6
C7
C8, T1
Brachialplexus
Subclavian artery1
2
Fig. 17.4 The brachial plexus passing through thecervicobrachial junction.
KAY17 12/16/04 7:57 PM Page 240

Meralgia paraestheticaMeralgia paraesthetica results from entrapmentof the lateral cutaneous nerve of the thigh beneath the inguinal ligament, just medial to theanterior superior iliac spine. At this position thenerve passes between two roots of attachment ofthe inguinal ligament to the iliac bone and thereis a sharp angulation of the nerve as it passesfrom the iliac fossa into the thigh.
Prolonged standing or walking and an obesependulous anterior abdominal wall accentuatesthe downward pull on the inguinal ligament andmay predispose to entrapment of the nerve. Thesyndrome is most frequently seen in middle-aged, overweight men, and also in young armyrecruits during strenuous training.
The principal symptom is a painful dysaesthe-sia in the anterolateral aspect of the thigh. The patient often describes the sensation as ‘burning’,‘pins and needles’ or ‘prickling’ which may be accentuated by standing up straight and relievedby flexion of the hip.
The only neurological sign is diminished sen-sation over the anterolateral aspect of the thigh inthe distribution of the lateral cutaneous nerve ofthe thigh.
The symptoms may only be minor and the patient may be satisfied with reassurance. Theunpleasant features may resolve with conserva-tive treatment, which should include weight reduction in an obese patient. Surgery may benecessary if the symptoms are debilitating. Thisinvolves decompression of the nerve or, if thatfails, division of the nerve.
Tarsal tunnel syndromeThe tarsal tunnel is the counterpart of the carpaltunnel of the wrist and is located posterior andinferior to the medial malleolus. The flexor retinaculum extends from the medial malleolusabove to the medial tubercle of the os calcisbelow. The posterior tibial nerve, a terminalbranch of the sciatic nerve, enters the footthrough the tarsal tunnel with the posterior tibialvessels and the tendons of the tibialis posterior,flexor digitorum longus and flexor hallucislongus muscles.
Men and women are equally affected. The
principal symptoms are pain, numbness and tingling along the plantar aspect of the foot andtoes.
Electrodiagnostic studies will help confirm thediagnosis. Operation involves division of theretinaculum and decompression of the nerve,usually with excellent results.
Sciatic nerve palsyA sciatic nerve pressure palsy typically occurs inpatients following a prolonged period of uncon-sciousness and is most frequently seen after drugoverdose. It is not a true entrapment neuropathybut rather a direct pressure palsy.
Common peroneal (lateral popliteal) nerve palsyEntrapment of the common peroneal nerve mayoccur rarely as it winds around the neck of thefibula deep to the peroneus longus muscle, re-sulting in a foot drop. More commonly, paralysisof the nerve will occur as a result of direct traumain this superficial vulnerable position.
Acute nerve injuries
Peripheral nerve anatomy
The axon projects from the cell body (theperikaryon) and is surrounded by a basementmembrane and myelin sheath. The axon is cov-ered by the endoneurium, the innermost layer ofconnective tissue, and a number of axons aregrouped together in a bundle called a fascicle,which is invested by a further connective tissuesheath called the perineurium. A peripheralnerve consists of a group of fascicles covered byan outermost layer of connective tissue, theepineurium. The nerve fibres can be classified ac-cording to their diameter and function. The nerveconduction velocity is proportional to the squareroot of the fibre diameter. The largest myelinatedaxons which produce the most rapidly conduct-ing potential are known as A fibres, which can befurther subdivided into alpha, beta, gamma anddelta, based on their size and conduction velo-city. The smaller, slower conducting B fibres aremostly responsible for autonomic conduction
PERIPHERAL NERVE ENTRAPMENTS, INJURIES AND TUMOURS 241
KAY17 12/16/04 7:57 PM Page 241

242 CHAPTER 17
and the unmyelinated C fibres have the slowestconduction.
Classification of nerve injuries
There is no single classification system that candescribe all the many variations of nerve injury.Most systems attempt to correlate the degree ofinjury with symptoms, pathology and prognosis.In 1943, during the Second World War, Seddonintroduced a classification of nerve injuries basedon three main types of nerve fibre injury andwhether there is continuity of the nerve (Table17.2).
Neurotmesis. This is the most severe injury, inwhich the nerve has been completely dividedand complete distal Wallerian degeneration oc-curs. There is complete loss of motor, sensory and
autonomic function. Electrical studies will showabsence of voluntary muscle potentials and evidence of denervation after 2–3 weeks.
Although the term neurotmesis implies a cut-ting of the nerve, the term is also used when theepineurium of the nerve is still in continuity butthe axons have been so destroyed and replacedby scar tissue that spontaneous regeneration isimpossible. The most common injuries to causeneurotmesis are laceration and a missile injury,but it can also result from other types of traumaincluding a crush or traction injury.
If the nerve has been completely divided, ax-onal regeneration causes a neuroma to form inthe proximal stump.
Axonotmesis. This is characterized by completeinterruption of the axons and their myelinsheaths, although the encapsulating tissue, the
Table 17.2 Classification of nerve injuries (Seddon).
Neurotmesis Axonotmesis Neurapraxia
PathologicalAnatomical continuity May be lost Preserved PreservedEssential damage Complete disorganization. Nerve fibres interrupted Selective
Schwann sheaths by larger fibres, no demyelinationpreserved degeneration of axons
ClinicalMotor paralysis Complete Complete CompleteMuscle atrophy Progressive Progressive Very littleSensory paralysis Complete Complete Usually much sparingAutonomic paralysis Complete Complete Usually much sparing
Electrical phenomenaReaction of degeneration Present Present PresentNerve conduction distal Absent Absent Preserved to the lesionMotor unit action Absent Absent Absent potentialsFibrillation Present Present Occasionally detectable
RecoverySurgical repair Essential Not necessary Not necessaryRate of recovery 1–2 mm/day after repair 1–2 mm/day Rapid; days or weeksMarch of recovery According to order of According to order No order
innervation of innervationQuality Always imperfect Perfect Perfect
Adapted from Seddon (1975). Reproduced with permission.
KAY17 12/16/04 7:57 PM Page 242

epineurium and perineurium, are preserved.Spontaneous regeneration will occur because theintact endoneurial sheaths guide the regenerat-ing fibres to their distal connections. There iscomplete and immediate loss of motor, sensoryand autonomic function distal to the lesion withan EMG picture similar to that of neurotmesis.Regeneration occurs at a rate of 1–2 mm per day,so that the time of recovery will depend on thedistance between a lesion and the end-organ andon the age of the patient.
The major types of injuries causing an ax-onotmesis include compression, traction, missileand ischaemic.
Neurapraxia. The mildest form of injury, neu-rapraxia, is akin to a transient ‘concussion’ of thenerve. Neurapraxia is a physiological block inconduction along one segment of the nerve withstructural changes confined primarily to de-myelination, if present at all. There is a tempo-rary loss of function, which is reversible withinhours to months of the injury (the average is 6–8weeks). If there is a complete, initial loss of func-tion, neurapraxia cannot be distinguished fromthe more serious type of injury but will be recog-nized only in retrospect when recovery of func-tion has occurred sooner than would be possiblefollowing Wallerian degeneration. There is fre-quently greater involvement of motor than sen-sory function with autonomic function beingretained.
Causes of peripheral nerve injury
The type of trauma will determine the nature ofthe injury to the nerve. In practice there are nu-merous possibilities, but these can be groupedinto the major types.• Lacerations cause neurotmesis with completeor partial division of the nerve. The usual injuryresults from a knife wound, laceration by glass orextensive contusion of the area with a chainsaw.• Missile injuries may cause the spectrum ofnerve injury from complete disruption of thenerve to a mild neurapraxia. If the brachialplexus is injured a variety of these injury typesmay occur to various parts of the plexus.
• Traction and stretch trauma may also result ineither complete disruption of the nerve or, ifminor, a neurapraxia. This type of mechanism isparticularly responsible for brachial plexus in-juries following motor bike accidents, or radial orperoneal nerve injuries. It is a common mecha-nism of nerve injuries associated with skeletalfractures.• Fractures or fracture dislocation may causenerve injuries when the adjacent nerve is eithercompressed by the displaced bone fragments,causing injury by stretch or ischaemia, or lesscommonly, severed by the jagged edge of thebone. Axonotmesis is the most common type ofinjury.• Compression ischaemia may produce a neu-rapraxia in mild cases or, if prolonged and severe,axonotmesis or neurotmesis. It is the cause of thepressure palsies following improper applicationof a tourniquet, or the ‘Saturday night palsy’ inwhich the radial nerve has been compressedagainst the humerus. Increased pressure in aclosed fascial compartment, as can occur follow-ing a musculoskeletal injury, may cause is-chaemic damage to a peripheral nerve and delayin treatment will result in severe ischaemic damage to the nerves and muscles resulting inparalysis and contraction deformities, such as inVolkmann’s ischaemic contracture.• Injection injury results from either direct trauma by the needle or the toxic effect of theagent injected. As would be expected, the sciatic and radial nerves are the most commonly affected.• Electrical and burn injuries are uncommoncauses of serious peripheral nerve damage.
Management of nerve injuries
The basis of the management depends on a pre-cise assessment of the damage that has been doneto the nerve. The types of injuries vary consider-ably from an isolated single nerve lesion to acomplex nerve injury in a patient with multipletrauma. The following are the general guidelinesfor management.1 Determination of the exact nerve involved by:
(a) the clinical deficit(b) the position of the injury.
PERIPHERAL NERVE ENTRAPMENTS, INJURIES AND TUMOURS 243
KAY17 12/16/04 7:57 PM Page 243

244 CHAPTER 17
2 Assessment of the type of nerve damaged bythe mechanism of the injury.3 If a neurapraxia or axonotmesis is suspectedon clinical grounds there is no specific surgicaltreatment for the nerve but physiotherapyshould commence as soon as possible to preventstiffness of the joints and contractures. However,a neurotmesis will not recover without surgery.4 Immediate or early exploration of the nerveshould be undertaken in the following situations:
(a) if it is highly probable that the type of injury(e.g. laceration) will have caused the nerve tobe severed(b) if the nerve injury has been caused by a dis-placed fracture that needs reduction by opensurgery, when exploration of the nerve can becarried out at the same time.
The operative procedure involves identificationof the nerve and relieving any compression. If thenerve has been severed the nerve ends should beisolated and continuity restored by either directsuture or inserting a nerve graft. Some surgeonsadvocate performing a graft as a secondary pro-cedure only, and delaying this until the woundhas healed and the risk of infection has subsided.5 Delayed exploration of the nerve will be indi-cated if the clinical and EMG findings indicatefailure of regeneration of the nerve beyond thetime expected, that is, if the injury has resulted ina neurotmesis rather than an axonotmesis or neurapraxia.
Brachial plexus injury
The mechanisms of injury are the same as for anyperipheral nerve. Birth injuries usually have oneof three patterns.1 Erb’s palsy due to damage to the upper trunkof the brachial plexus.2 Klumpke’s paralysis due to damage to thelower trunk of the brachial plexus (C8 and T1), re-sulting from the arm being held up while tractionwas applied to the body during a breech delivery.3 Paralysis of the whole arm as a result of severebirth trauma.
In adolescents and adults the most commoncause is severe traction on the brachial plexus re-sulting from violent trauma, frequently a motor
bike or motor vehicle accident. The trauma mayresult in damage to any part of the plexus, but severe axial traction may result in tearing of thearachnoid and dura with nerve root avulsion.
The management involves determination ofthe exact neurological injury, and particularly thepart of the brachial plexus involved. A Horner’ssyndrome is useful evidence for avulsion of thenerve roots from the spinal cord.
Magnetic resonance imaging or a myelogram(or CT scan/myelogram) may show the pseudo-meningocele, which is characteristic of nerve root avulsion.
Electrical studies rarely add any new diagnos-tic information concerning the neurological dam-age but they do provide useful baseline studiesfor future comparison. It is reasonable to obtainthese studies 8 weeks after the injury.
There is controversy concerning the exact indications for surgical intervention for closedbrachial plexus injuries in adults. Obviously, ifthe injury is partial and improving there is no indication for surgery, and supportive manage-ment, including intensive physiotherapy andmobilization of the joints, should be commencedas soon as possible. Similarly, there is no place forsurgery if there is clinical or radiological evi-dence of nerve root avulsion from the cord. Ingeneral there is little benefit from exploration ofthe plexus in closed injuries, although some sur-geons do advocate exploration approximately 4months after the injury if clinical and electricalevidence show the lesion to be complete.
Pain following nerve injuries
A number of pain problems occur specificallyafter nerve injuries. These include:• causalgia (Chapter 20)• phantom limb pains (Chapter 20)• irritative nerve lesions — neuroma• brachial plexus trauma pain.
Phantom limb pain and causalgia are de-scribed in more detail in Chapter 20. Causalgiaoccurs rarely; it is a burning pain that follows apartial or minor nerve injury and is relieved bysympathectomy. Phantom limb pain may occurfollowing traumatic amputation of a limb or after
KAY17 12/16/04 7:57 PM Page 244

surgical amputation for tumours or peripheralvascular disease.
There is a diffuse range of pain problems fol-lowing peripheral nerve injuries that is broadlytermed ‘irritative nerve lesions’. The pathologicalcause of the pain is often not evident, although insome cases a neuroma may be demonstrable andthe pain is relieved following excision.
A particularly severe form of pain followingnerve injury occurs after brachial plexus trauma.The onset of the pain is frequently delayed bysome weeks or months and the pain is describedas having both deep and superficial components.The deep pain is continuous and is described asan ‘ache’ throughout the affected limb. The superficial ‘burning’ pain is particularly severedistally in the limb and is associated with a hyperpathia. The skin is usually dry and cool andhyperthermia and sweating are uncommon.
The management of these pain problems involves an assessment of the particular pain pattern and the underlying pathological cause. Ingeneral, treatment consists of simple conserva-tive measures, including supportive care andsimple analgesic medication. If a neuroma isthought to be the cause of the pain it should be excised. The pain from brachial plexus injuries isnotoriously difficult to treat and is often unre-sponsive to conservative therapies. The dorsalroot entry zone (DREZ) operation has been mod-erately successful in controlling the pain in a significant percentage of these patients. The operation involves ablation of the DREZ over theinvolved segments by thermocoagulation. Thereis a small risk of further damage to the cord by theprocedure but most patients are willing to acceptthis because of the severity of the pain.
Peripheral nerve tumours
The classification and nomenclature of peripher-al nerve tumours has been confusing, mainly dueto disagreements as to the embryological originof the various tumours. Peripheral nerve tu-mours may arise from the nerve sheath or be ofneuronal origin. The nerve sheath tumours maybe neuroectodermal or mesodermal in origin; theneuronal tumours arise from the neuroectoderm.
The nerve sheath tumours originating from theneuroectoderm may arise from the Schwanncells, which form the axonal myelin, or from theperineurial cells. Those of mesodermal originarise from the fibrocytes that lie in the endoneuri-um and throughout the nerve sheath. The neu-ronal or nerve cell tumours nearly always arise inthe ganglia of the autonomic nervous system.
The more common peripheral nerve tumoursare shown in Table 17.3.
Benign tumours
SchwannomaSchwannomas may arise from intracranialnerves (Chapter 7) or intraspinal nerves (Chapter15). The extraspinal schwannomas derived fromthe Schwann cell may arise from motor, sensoryor autonomic nerves and are usually encoun-tered as solitary lesions in adults. They may beassociated with von Recklinghausen’s neurofi-bromatosis (neurofibromatosis type 1, NF1).They are sometimes classed together with neu-rofibromas as ‘benign nerve sheath tumours’.They are discrete, smooth and sometimes lobu-lated; they originate focally in a fascicle. As theygrow the discrete mass deflects the other fasciclesover its surface. Malignant transformation israre.
As in other schwannomas there are two dis-tinct architectural patterns, Antoni A and B. The
PERIPHERAL NERVE ENTRAPMENTS, INJURIES AND TUMOURS 245
Table 17.3 Peripheral nerve tumours.
Benign tumoursSchwannomaNeurofibroma
Cutaneous neurofibromaIntraneural (plexiform) neurofibroma
Malignant tumoursMalignant schwannomaNerve sheath fibrosarcoma (neurofibrosarcoma)
Non-neoplasticMorton’s neuromaTraumatic neuroma
KAY17 12/16/04 7:57 PM Page 245

246 CHAPTER 17
histological features of Antoni A typically consistof strands and whorls of closely packed spindlecells with elongated, darkly staining nuclei. Thenuclei show a tendency to aggregate and oftenshow striking pallisading. The type B patternconsists of loosely arranged stellate cells and aspongy meshwork of vacuolated cells.
Benign schwannomas are usually asympto-matic and most patients present with a painfullump or local tenderness if the tumours are su-perficial. Occasionally, the benign tumours maypresent with pain or neurological disturbance,particularly if they arise in an enclosed spacesuch as the carpal or tarsal tunnel. Most of the tu-mours arise in the head, neck and extremities.
The treatment, if indicated, involves tumourresection and, using microsurgical techniques,preservation of nerve function. The nerve fasci-cles passing by the tumour are reflected over thetumour surface, thereby making it possible to re-sect the tumour and preserve neural function.
NeurofibromaNeurofibromas arise spontaneously or in thecontext of NF1 (see also Chapter 6) (Fig. 17.5).Dermal neurofibromatosis may be isolated or nu-merous as part of NF1. The deeper solitary neu-rofibromas that are associated with NF1 in about50% of cases have a clinical presentation similarto that of a schwannoma.
As with schwannomas the management ofneurofibroma depends upon the clinical symp-toms. NF1 patients may have hundreds of dermal and visceral neurofibromas that requireno treatment and if they are asymptomatic theycan be followed clinically. Potential indicationsfor surgery are pain, progressive neurologicaldeficit, cosmetic reasons and rapid growth thatmight be suspicious for malignant transforma-tion. The operation involves neurosurgical techniques aided by intraoperative electro-physiological testing in order to preserve func-tional nerve fascicles. If functional fasciclescannot be preserved it might be necessary to perform a subtotal resection or, if clinically indi-cated, to proceed with a complete resection fol-lowed by an interposition nerve graft for neuralrestoration.
Intraneural neurofibromas. Less common than thecutaneous variety, intraneural neurofibromasusually arise from larger nerves, have a frequentassociation with von Recklinghausen’s diseaseand have a potential for malignant transforma-tion. They commonly occur in the cervical,brachial or lumbosacral plexus. The tumour is formed by an intraneural proliferation ofSchwann cells and is usually a diffuse transfor-mation of long segments of nerves and theirbranches. This plexiform neurofibroma ispathognomonic for von Recklinghausen’s disease (NF1).
The nerve containing the plexiform neurofi-broma has a macroscopic appearance similar torope, with the enlarged fascicles forming thebraids of the rope.
The surgical treatment provides a dilemma.Approximately 10% may undergo malignant
Fig. 17.5 Numerous cutaneous neurofibromatoma in a patient with von Recklinghausen’s disease (NF1).Other cutaneous features include café au lait spots and fibromas.
KAY17 12/16/04 7:57 PM Page 246

transformation, but radical resection will usuallyresult in serious neurological impairment. Ingeneral, an initial partial resection, with preser-vation of neurological function, should be at-tempted. The patient should be observed closelyand if there is evidence of malignant transforma-tion a radical resection should be performed.
Malignant tumours
Malignant tumours of peripheral nerves canarise spontaneously in a normal nerve fromSchwann cells of neuroectodermal origin or fi-brocytes of mesodermal origin, or in a plexiformneurofibroma of von Recklinghausen’s disease(NF1). The tumours are classified as either malig-nant schwannoma or a nerve sheath fibro-sarcoma. Sometimes, more overt mesenchymalcharacteristics such as osteoid, chondroid andrhabdomyoblasts are contained in malignant peripheral nerve neoplasms.
The patient usually presents with an enlargingpainful mass with a progressive neurological disturbance in the distribution of the nerve involved.
The tumour presents macroscopically as a lobulated, fusiform enlargement of the nerve thatmay extend over a long length, both proximaland distal to the major mass. The surroundingtissues are compressed and histological examina-tion may show microscopic invasion.
Surgery will entail a radical resection providedthere is no evidence of widespread metastases.
Non-neoplastic tumours
Morton’s neuroma is a reactive fibrosis asso-ciated with degeneration of a nerve. It occurs pre-dominantly in women in the plantar digital nervebetween the heads of the 3rd and 4th metatarsals.The patient presents with pain and, macroscopi-cally, the lesion is a discrete enlargement of the
neurovascular bundle. The ‘neuroma’ can be excised simply and the problem cured.
Traumatic neuromas appear macroscopicallyas a fusiform enlargement of the nerve or, if therehas been transection of the nerve, as a bulbous expansion of the proximal stump.
A painful neuroma can be excised. This is par-ticularly appropriate if a nerve block proximal tothe neuroma gives total pain relief.
The treatment of a neuroma of a nerve in conti-nuity is more difficult when there is retainednerve function. Neurolysis, with division of theepineurium, may relieve the pain. Occasionallyexcision of the neuroma in continuity and re-suture of the nerve may be necessary.
Further readingBrain WR, Wright AD, Wilkinson M (1947) Sponta-
neous compression of both median nerves in a carpaltunnel. Six cases treated surgically. Lancet i, 277–282.
Burger PC, Vogel FS (1982) Surgical Pathology of the Ner-vous System and its Coverings, 2nd edn. John Wiley,New York.
Ebeling P, Gilliat TRW, Thomas PK (1960) A clinical andelectrical study of ulnar nerve lesions in the hand.Journal of Neurology, Neurosurgery and Psychiatry 23,1–8.
Kaye AH, Black P McL (2000) Operative Neurosurgery.Churchill Livingstone, London, New York, Edinburgh.
Kline DG, Judice DJ (1983) Operative management ofselected brachial plexus lesions. Journal of Neuro-surgery 58, 631–649.
Pang D, Wessel HB (1988) Thoracic outlet syndrome.Neurosurgery 22, 105–121.
Seddon H (1975) Surgical Disorders of the PeripheralNerves, 2nd edn. Churchill Livingstone, London.
Sunderland S (1978) Nerves and Nerve Injuries. ChurchillLivingstone, Edinburgh.
Tindall SC, McGillicuddy JE, Kline DG (1995) Treat-ment of ulnar entrapment. In: Al-Mefty O, OrigitanoTC, Harkey HL, eds. Controversies in Neurosurgery.Thieme, New York.
PERIPHERAL NERVE ENTRAPMENTS, INJURIES AND TUMOURS 247
KAY17 12/16/04 7:57 PM Page 247

Facial pain may result from local pathology in-volving the face, mouth, jaw, temporomandibu-lar joint, paranasal sinuses or salivary glands, orit may be due to distinct pain disorders such astrigeminal neuralgia, glossopharyngeal neural-gia and postherpetic neuralgia. These specificpain entities are relatively uncommon but theclinical manifestations are stereotyped so that adiagnosis should be apparent.
Trigeminal neuralgia
Trigeminal neuralgia consists of excruciatingparoxysmal pain, which lasts for seconds to min-utes, in the distribution of the 5th cranial nerve. Itwas described by Avicenna 900 years ago and theterm ‘tic douloureux’ was applied by André in1756. Charles Bell demonstrated the anatomicalbasis for sensation in the face in the 1820s and dis-tinguished the sensory component of the trigem-inal nerve from the motor function of the facialnerve, consequently defining an anatomical basisfor trigeminal neuralgia. It is estimated that it occurs in about 1 in every 70 000 people.
Aetiology
There is some controversy concerning the preciseaetiology of trigeminal neuralgia. The microvas-cular compression theory is popular and postu-lates that the 5th cranial nerve is compressed atthe brainstem junction by a vascular loop. In 1934Dandy first proposed that trigeminal neuralgiawas caused by the nerve being compressed anddistorted by the superior cerebellar artery, andthis theory of microvascular compression was
extended by Gardner, at the Cleveland Clinic, toform the basis of hemifacial spasm due to pres-sure on the 7th cranial nerve. The concept hasbeen popularized by Jannetta, who proposedthat trigeminal neuralgia is the result of compres-sion of the root entry zone, which is a junctionalarea between the central and peripheral myelinon the nerve adjacent to the brainstem. However,others suggest that the pain is due to central dys-function in the brainstem in structures related tothe nucleus of the 5th nerve, or pathology withinthe gasserian ganglion.
Trigeminal neuralgia may occasionally presentas a symptom of multiple sclerosis, which shouldtherefore be considered as a cause in patientsunder 40 years of age.
In approximately 3% of cases there may be amass, such as a meningioma, epidermoid or arte-riovenous malformation, in the posterior fossa.This mass distorts the nerve and produces painsimilar to trigeminal neuralgia.
Clinical features
The main clinical feature is the sudden, severepain that lasts for a moment and then goes, leav-ing nothing behind — except the fear of its return.Shaving, talking, eating, washing or even a coldwind may disturb the skin and trigger a parox-ysm of pain which is so severe that the patient isimmobilized in agony.
The particular characteristics of trigeminalneuralgia are as follows.• The pain is strictly limited to one or morebranches of the trigeminal nerve. It most com-monly affects the 2nd and/or 3rd division.
CHAPTER 18
18 Facial pain and hemifacial spasm
248
KAY18 12/16/04 7:58 PM Page 248

• The pain is sudden and short lived, usuallylasting seconds, or at the most, minutes.• The pain is frequently provoked by light mechanical stimuli within the trigeminal area. Inparticular, it is often ‘triggered’ by touching theside of the face, or is brought on by facial move-ment, such as chewing. These patients are oftenunable to shave and they shield their faces whenoutside in the wind.• There is no detectable abnormality of trigemi-nal nerve function.
The incidence of trigeminal neuralgia reachesits maximum between the ages of 50 and 70 years,is very rare below the age of 25 and is uncommonunder the age of 35. The pain affects the territoryof the 2nd and 3rd divisions of the trigeminalnerve with equal frequency, and may involveboth territories simultaneously. The area of the1st division of the trigeminal nerve is involvedless frequently. In about 5% of cases the neuralgiaaffects both sides of the face, but not usually si-multaneously, so that each bout of pain remainsstrictly unilateral. Bilateral trigeminal neuralgiaoccurs more commonly in patients with multiplesclerosis.
Remissions of the pain are frequent and maylast for months or even years; occasionally com-plete freedom from the pain occurs.
There are no physical signs. The patient maypresent with a scarf shielding the head and willtalk from the corner of the mouth so as not to pre-cipitate a spasm of pain. If the pain has been verysevere the patient may be emaciated and dehy-drated from being unable to eat or drink and theface may be dirty and unshaven from fear of precipitating an attack of pain.
Investigations
MRI of the brain should be performed to excludea mass in the cerebellopontine angle in the poste-rior fossa or intrinsic brainstem lesion such as demyelination, especially in younger patients.
Differential diagnosisThe pain of trigeminal neuralgia is characteristicbut must be differentiated from:• atypical facial pain
• pain of dental origin, such as malocclusion ordental abscess• pain from the temporomandibular joint• postherpetic neuralgia• migrainous neuralgia (cluster headache).
Treatment
Management of a patient with trigeminal neural-gia may involve the use of a number of treatmentmodalities including:• drugs• local procedures on peripheral branches of thetrigeminal nerve• percutaneous procedures involving thetrigeminal ganglion or the retrogasserian rootlets• posterior fossa craniotomy procedures.
DrugsCarbamazepine initially relieves the pain in thegreat majority of patients although doses of 200-mg tablets up to 4–5 times a day are often neces-sary for adequate pain control. However, thepatients frequently have a relapse of pain andneed further treatment. In addition, many pa-tients are unable to tolerate the side-effects of carbamazepine which occur at the doses neces-sary to control the discomfort. The most frequentadverse reactions are dizziness, drowsiness, un-steadiness, nausea and vomiting. Haemopoieticcomplications due to bone marrow depressionoccur rarely. Other drugs that can be tried includephenytoin, baclofen and clonazepam, althoughthey are not as effective.
Procedures involving peripheral branches of the trigeminal nerveInfraorbital or supraorbital nerve section may beperformed in the uncommon situation of the painbeing localized to the area in the distribution ofthese nerves. However, the pain frequently re-curs and these procedures should probably belimited to the elderly frail patient.
Percutaneous thermocoagulationPercutaneous thermocoagulation of the retro-gasserian rootlets or ganglion of the trigeminalnerve can result in analgesia in selected areas of
FACIAL PAIN AND HEMIFACIAL SPASM 249
KAY18 12/16/04 7:58 PM Page 249

250 CHAPTER 18
the trigeminal distribution. In this procedure aneedle is passed percutaneously, under X-raycontrol, through the foramen ovale into the gan-glion and nerve roots just behind the ganglion inMeckel’s cave. The nerve rootlets and ganglionare heated with a radiofrequency current, whichresults in a differential loss of pain sensation butretention of light touch sensation. Alternatively,glycerol may be injected into Meckel’s cave so asto bathe the retrogasserian nerve rootlets. Al-though these procedures have a high initial suc-cess in relieving pain, they may produce facialnumbness and the trigeminal neuralgia fre-quently recurs. The procedures may be repeatedwhen the pain recurs or alternative treatmentsmay be considered.
Posterior fossa craniotomy proceduresTotal or partial trigeminal nerve section. Trigeminalroot section, by either a posterior fossa cranio-tomy or a middle cranial fossa approach (Frazier’s operation), used to be a common pro-cedure for trigeminal neuralgia but is now almostobsolete. Section of the nerve results in facialnumbness and the morbidity may be quite dis-abling, particularly if the ophthalmic divisionsupplying the cornea is affected. However, a par-tial section of the posterior half of the nerve causes only relatively minor disturbance of facialsensation and may result in lasting pain relief fortrigeminal neuralgia involving the 2nd and/or3rd divisions. An uncommon, but feared, dis-abling complication of nerve section is a painfuldysaesthesia of the face, ‘anaesthesia dolorosa’,for which there is no treatment. Anaesthesia dolorosa only rarely results from percutaneousradiofrequency rhizotomy.
Microvascular decompression. This is now the pro-cedure of choice. The operation is performed viaa small retrosigmoid posterior fossa craniotomyusing the operating microscope. The compres-sive vessel, most commonly the superior cerebel-lar artery, is dissected away from the 5th cranialnerve at the brainstem entry junction and thenerve is then shielded from the vessel by a smallpatch of sponge. Over 90% of patients have aninitial complete relief of pain, although about
10–15% have some relapse of trigeminal neural-gia over the next 5 years.
Summary of treatmentThere are a number of methods of treatingtrigeminal neuralgia and the treatment chosenwill frequently depend on the patient’s prefer-ence when the various options are explained. Ingeneral, carbamazepine is used first. If the med-ication is not tolerated, or when the pain relapses,the main choice is between a radiofrequency percutaneous rhizotomy or a posterior fossacraniotomy and microvascular decompression.Unless the patient is elderly and very frail, mi-crovascular decompression is the preferred op-tion, as it has the greatest chance of producingpermanent relief of pain with no facial numbness.
Glossopharyngeal neuralgia
Glossopharyngeal neuralgia is much less com-mon than trigeminal neuralgia, there being ap-proximately one case for every 50 of trigeminalneuralgia. It was first defined as a clinical entityby Harris in 1921. It is characterized by intense at-tacks of pain in the distribution of the glossopha-ryngeal nerve and the auricular and pharyngealbranches of the vagus nerve.
Aetiology
The precise cause of glossopharyngeal neuralgiais unclear, although Janetta proposed the theoryof microvascular compression of the 9th nerve, asfor trigeminal neuralgia and the 5th cranialnerve.
Presenting features
The patient presents with attacks of severe paininvolving the throat, tongue or ear. The pain maystart anywhere in the territory of the glosso-pharyngeal nerve or auricular and pharyngealbranches of the vagus nerve. The tonsil, root ofthe tongue and ear are common sites and the painoften extends into the base of the jaw and theneck. At times the pain may be confined to the
KAY18 12/16/04 7:58 PM Page 250

throat and occasionally only the ear is involved.In some patients the pain involves the area of the mandibular division of the trigeminal nerve,which may lead to a wrong diagnosis.
The attacks are frequently induced by talking,swallowing or chewing, and consequently, in se-vere cases, the patient may become cachectic. Oc-casionally, an episode of throat pain precipitatedby swallowing may be associated with bradycar-dia, hypotension and syncope.
Differential diagnosis
The distribution of the pain will distinguish glos-sopharyngeal neuralgia from trigeminal neural-gia. Geniculate neuralgia, described by Hunt, israre and involves the sensory component of the facial nerve (nervus intermedius). Geniculateneuralgia has two major forms, one affecting theear, with secondary radiation into the deep struc-tures of the face, the other involving primarilythe deep facial structures.
Treatment
Patients with glossopharyngeal neuralgia mayderive benefit from treatment with carba-mazepine, although with less effect than fortrigeminal neuralgia. However, surgery for glos-sopharyngeal neuralgia is straightforward andeffective. The operation involves a small posteri-or fossa craniotomy with section of the 9th nerveand the upper 10% of the fibres of the vagusnerve. The sensory loss resulting from thesenerve sections results in no disability. Some sur-geons advocate microvascular decompression asfor trigeminal neuralgia, but the nerve sectionoperation is effective and the microvascular decompression may require manipulation of thelower cranial nerves resulting in morbidity.
Postherpetic neuralgia
Herpes zoster may involve the distribution of thetrigeminal nerve, particularly the ophthalmic di-vision. In a manner similar to shingles involvingthe trunk or limbs, postherpetic neuralgia occursmore frequently in elderly patients. The pain,
usually in the distribution of the ophthalmic divi-sion, is severe, constant and unremitting, and isdescribed as ‘burning’ or a ‘crawling’ sensationunder the skin.
The diagnosis is usually obvious by the herpetic rash. Occasionally, however, the rashmay be minor and barely noticeable.
There is no surgical treatment for postherpeticneuralgia of the trigeminal nerve and sensoryroot section is of no benefit. Carbamazepine mayalleviate some of the discomfort, although unfor-tunately its benefit is usually limited.
There is some evidence that the early use ofsteroids and acyclovir in patients presenting withherpes zoster may reduce the risk of postherpeticneuralgia.
Atypical facial pain
Facial pain which has no pathological basis is relatively common and most frequently affectsmiddle-aged females. The pain presents a diag-nostic problem which can often only be solvedafter underlying pathology has been excluded byclinical and radiological investigations.
The pain is usually situated in the central portions of the face or cheek and is described asboring, dull or aching. The lancinating parox-ysms of pain characteristic of trigeminal neural-gia and glossopharyngeal neuralgia are absent.Dental malocclusion and pain from the temporo-mandibular joint, Costen’s syndrome, should beexcluded.
Hemifacial spasm
Hemifacial spasm is a facial disorder that is notpainful, but its proposed aetiology is so similar totrigeminal neuralgia that it is best described inthis chapter. The condition is characterized byunilateral spasms of the facial muscles suppliedby the facial nerve.
Aetiology
The aetiology is similar to that proposed fortrigeminal neuralgia and the microvascular com-pression theory postulates that the 7th cranial
FACIAL PAIN AND HEMIFACIAL SPASM 251
KAY18 12/16/04 7:58 PM Page 251

252 CHAPTER 18
nerve is compressed at the brainstem junction bya vascular loop, usually an artery. Gardner advo-cated this theory in the 1960s and it has been popularized by Jannetta who proposed that, asfor trigeminal neuralgia and the 5th cranialnerve, hemifacial spasm is due to pulsatile com-pression at the root exit zone of the 7th cranialnerve, which is a junctional area between the cen-tral and peripheral myelin where the 7th nerveleaves the brainstem. Very uncommonly, hemifa-cial spasm is associated with a compressive masssuch as an epidermoid, aneurysm or menin-gioma. Occasionally, hemifacial spasm andtrigeminal neuralgia may coexist in the same patient (known as ‘tic convulsif’).
Clinical features
The onset of hemifacial spasm usually com-mences in middle or old age and there is a slightfemale predominance. The spasms usually com-mence around the orbicularis oculi muscles andsubsequently spread down the face to involve theother facial muscles innervated by the facialnerve. The spasms are episodic and are fre-quently precipitated by emotional distress,chewing, talking or laughing. The conditioncauses the patient considerable social embarrass-ment and the spasms of the orbicularis oculi re-sult in eye closure, making driving difficult.
In contrast to trigeminal neuralgia, wherethere is no clinical evidence of 5th cranial nervedysfunction, there is frequently minor facialweakness between the episodes of spasm. Other-wise, there are no neurological findings.
Management
The diagnosis is self-evident, with the spasmsbeing located on one side of the face. In the veryearly stages hemifacial spasm needs to be differ-entiated from simple blepharospasm, but this isconfined to the muscles around the eye and isusually bilateral.
An MRI should be performed to exclude theunlikely possibility of a posterior fossa mass lesion causing the condition.
There is currently no lasting effective medical
treatment. Injections of botulinum toxin into theaffected muscles have limited, transient success,but need to be repeated every few months.
At present the only long-term effective treat-ment is surgical and the operation is a microvas-cular decompression of the 7th cranial nerve.However, as the condition is benign and painlessthe principal indication for operation is socialembarrassment. In many patients the hemifacialspasm is so annoying and socially distressingthat they are keen to proceed with an operation,bearing in mind its possible risks. Surgery is def-initely inappropriate if the patient is not troubledby the spasm.
The microvascular decompression is per-formed through a small posterior fossa cranio-tomy and, using the operating microscope, thevessel, often the anterior inferior cerebellarartery, compressing the 7th nerve at the brain-stem junction is carefully mobilized away fromthe nerve. The nerve is then protected from thevessel by a small patch of sponge. The operationis usually highly effective in relieving the spasm.There is a small risk of unilateral hearing loss dueto the proximity of the 8th nerve and its bloodsupply. As the operation involves a craniotomy,often in elderly patients, there is a small risk of serious complication, mostly as a result of cerebrovascular complications. This possibilityshould temper an obvious enthusiasm for an effective operation.
Further readingAdams CBT (1989) Microvascular compression, an
alternative view and hypothesis. Journal of Neurosurgery 57, 1–12.
Apfelbaum RI (1983) Surgery for tic douloureux. Clinical Neurosurgery 31, 351–368.
Burchiel KJ et al. (1981) Comparison of percutaneous radiofrequency gangliolysis and microvascular decompression for the surgical management of ticdouloureux. Neurosurgery 9, 111–119.
Dandy WE (1929) An operation for the cure of ticdouloureux: partial section of the sensory root at thepons. Archives of Surgery 18, 687–734.
Dandy WE (1934) Concerning the cause of trigeminalneuralgia. American Journal of Surgery 24, 447–455.
Gardner WJ (1962) Concerning the mechanism of
KAY18 12/16/04 7:58 PM Page 252

trigeminal neuralgia and hemifacial spasm. Journal ofNeurosurgery 19, 947–948.
Jannetta PJ (1980) Neurovascular compression in cra-nial nerve and systemic disease. Annals of Surgery192, 518–525.
Jannetta PJ et al. (1977) Aetiology and definitive micro-surgical treatment of hemifacial spasm: operativetechniques and results in 47 patients. Journal of Neuro-surgery 47, 321–328.
Kaye AH, Black P McL (2000) Operative Neurosurgery.Churchill Livingstone, London, New York, Edinburgh.
Lunsford LD, Apfelbaum RI (1985) Choice of surgicaltherapeutic modalities for treatment of trigeminalneuralgia. Clinical Neurosurgery 32, 319–333.
Nugent GR, Brown JA, Hakanson S, Matsushima T,Wilkins RH (1995) Treatment of patient with trigemi-nal neuralgia. In: Al-Mefty O, Origitano TC, HarkeyHL, eds. Controversies in Neurosurgery. Thieme, NewYork.
Resnick DK, Jannetta PJ, Bissonett D (1995) Microvas-cular decompression for glossopharyngeal neural-gia. Neurosurgery 36, 64–69.
Stookey B, Ransohoff J (1959) Trigeminal Neuralgia: itsHistory and Treatment. Charles C Thomas, Springfield.
Taha J, Tew S (1996) Comparison of surgical treatmentfor trigeminal neuralgia. Neurosurgery 38, 865–871.
FACIAL PAIN AND HEMIFACIAL SPASM 253
KAY18 12/16/04 7:58 PM Page 253

Pain is the most common symptom in patientspresenting to a neurosurgeon; in fact it is oftenthe only symptom that the patient will complainof. The features of the pain are often characteris-tic of the particular underlying disease; these fea-tures include:• mode of onset• pattern of the pain —continuous or intermittent• duration• position of the pain• quality of the pain• features that alleviate or exacerbate the pain.
There are three major clinical groups of painproblems.1 Benign specific pain syndromes.2 Benign non-specific pain syndromes.3 Cancer pain.
Mechanisms of pain
There is no ‘pain centre’ in the brain — such a con-cept would be quite inadequate to account for the complexity of pain. There are three major psychological–anatomical–physiological com-ponents to pain which aid in the understandingof the mechanisms of pain and in treating patients. These are:1 sensory–discriminative2 motivational–affective3 cognitive–evaluative.
Melzack and Casey proposed that each of thesecomponents are subserved by physiologicallyspecialized systems in the brain.
Sensory–discriminative dimensionThe sensory–discriminative dimension involves
the spatial, temporal and magnitude propertiesof pain and is subserved mostly by neo-spinothalamic projections to the ventrobasalthalamus and then to the somatosensory cortex(Fig. 19.1). The pain pathways are described inChapter 1. The receptors for pain consist of unencapsulated endings of peripheral nerves.The neural responses are mediated through themyelinated A-delta and unmyelinated C fibres.Pain may be felt as two waves, separated by avery short interval. The first is sharp and local-ized, with conduction along group A fibres. Thesecond wave, which is rather diffuse and moredisagreeable, depends on the slower conductionof group C fibres. The cell bodies are in the dor-sal root ganglia. Their axons traverse the dorsalroots and enter the dorsolateral fasciculus (tractof Lissauer) of the spinal cord, in which ascend-ing and descending branches travel for one ortwo segments. These fibres, which give off manycollateral branches in their short course, termi-nate in the substantia gelatinosa of the dorsalgrey horn. The substantia gelatinosa consists ofGolgi type II neurones whose axons are eitherconfined to the nucleus or run for short distancesin the tract of Lissauer, connecting adjacent re-gions of the substantia gelatinosa. Axons of thetract cells in the chief nucleus of the dorsal horncross the midline in the ventral commissure andthen course rostrally in the lateral spinothalamictract. Fibres are continually being added to theventromedial aspect of the lateral spinothalamictract. At the upper cervical levels fibres from thesacral segments are dorsolateral, followed by fibres from lumbar and thoracic segments, whilefibres from the cervical segments are in the
CHAPTER 19
19 Pain —neurosurgicalmanagement
254
KAY19 12/16/04 7:58 PM Page 254

ventromedial position. The fibres ascendthrough the brainstem, supplying inputs to thereticular formation and the superior colliculus,before terminating in the nuclei of the thalamus,particularly the intralaminar, ventral posterolat-eral (VPL) and posterior nuclear complex. Thereis a somatotopic representation of the oppositeside of the body in the lateral portion of the thal-amic nucleus. Tertiary neurones then project tothe primary and secondary sensory area in thecerebral cortex.
Pain fibres from the head enter the ponsthrough the sensory root of the trigeminal nerveand turn caudally in the trigeminal spinal tract,the spinal tract of V, which extends to the uppercervical levels. Terminals of the spinal tract of Vform synapses in the adjacent nucleus, the spinalnucleus of V. Axons of the spinal nucleus of Vcross to the opposite side and ascend as the ventral trigeminothalamic tract to the ventralposteromedial (VPM) nucleus of the thalamus, as
well as to the intralaminar nuclei. The fibres thenpass to the somatosensory cortex. There is a spa-tial arrangement of fibres in the sensory root andspinal tract corresponding to the divisions of thetrigeminal nerve. Ophthalmic fibres in the senso-ry root are dorsal, mandibular fibres are ventraland the maxillary fibres are between these. Be-cause of rotation of fibres as they enter the pons,the mandibular fibres are dorsal and the oph-thalmic fibres ventral in the trigeminal spinaltract. The dorsal part of the spinal trigeminaltract includes pain and temperature fibres fromthe facial, glossopharyngeal and vagus nerves,which may supply areas of the external ear, liningof the auditory canal, tympanic membrane, posterior tongue, pharynx and larynx.
Motivational–affective dimensionThe motivational–affective dimension compo-nent of pain is involved with the aversive qualityof pain, which provides the unique, distinctly
PAIN — NEUROSURGICAL MANAGEMENT 255
Parietal lobe
Sensory cortex
Secondarysomato-sensorycortex
VPLThalamus
Medulla
Spinothalamictract Reticular
formation
Lateralspinothalamictract
Spinal cord
Ventral whitecommisure
Spinal cord
Lateralspinothalamictract
VPM thalamus
Intralaminarnuclei
Ventraltrigemino-thalamic tract
Neurone intrigeminalganglion (V)at level of pons
Spinal tract of VSpinal nucleus of V
Neurone in dorsalroot ganglion
Ascending anddecending fibres inLissauer's tract
Lissauer's tract
Receptor endingsfor painful andthermal stimuli
Substantiagelatinosa
Fig. 19.1 Pathways thatmediate pain and temperature.(Adapted from Gilman andNewman 1987. Published withpermission.)
KAY19 12/16/04 7:58 PM Page 255

256 CHAPTER 19
unpleasant component to the sensory experi-ence. The brainstem reticular formation and the limbic system, which receive projectionsfrom the spinoreticular and palaeospinothalamiccomponents of the somatosensory pathways,play an important role in the motivational–affective dimension.
Cognitive–evaluative dimensionThe cognitive–evaluative dimension relates tothe person’s understanding of pain as regardstheir intellectual, social and cultural background.Cognitive activities such as cultural values, anxi-ety, attention and suggestion all have a profoundeffect on the pain experience. Cognitive functionsare able to act selectively on sensory processingor motivational mechanisms and there is evi-dence that the sensory input is evaluated andmodified before it activates the discriminative ormotivational systems. Men wounded in battlemay feel little pain from the wound but may com-plain bitterly about a seemingly trivial medicalprocedure such as intramuscular injection orvenepuncture. The neural mechanisms that perform these complex functions must conductrapidly to the cortex so that the somatosensoryinformation has the opportunity to undergo fur-ther analysis, interact with other sensory inputsand activate previous memory stores. Melzackand Wall proposed that dorsal column and dorsolateral projection pathways act as a ‘feedforward’ limb of this loop. The frontal cortex may play a particularly significant role.
Theories of pain mechanisms
There have been numerous theories of painmechanisms over the past few centuries. In 1644Descartes described a ‘specificity’ theory, inwhich he conceived that the pain system was adirect channel from the skin to the brain. Thereare numerous other theories which have concen-trated on one or more of the various dimensionsof pain and tried to explain these in a singleprocess. The ‘gate control theory’, proposed byMelzack and Wall in 1965, is a useful concept ofthe mechanism of pain. Although some of the details have been disproved, the proposal that
afferent stimulation can influence pain percep-tion is accepted. The theory proposes that neuralmechanisms in the dorsal column of the spinalcord act like a ‘gate’, which can either increase ordecrease the flow of nerve impulses from the periphery to the central nervous system. Theinput from the sensory nerve fibres can be modu-lated by the gate before evoking the perception ofpain and the person’s response. The relative ac-tivity of the large diameter A-beta fibres and thesmaller diameter of the A-delta and C fibres in-fluence the gate to either increase or decrease thesensory transmission (Fig. 19.2).
To this proposed mechanism of pain can beadded the central pathways that relate to thethree major dimensions of pain. In addition, themidline raphe nuclei of the brainstem have con-nections with the periventricular and periaque-ductal areas and their axons descend to the spinalcord through the dorsolateral fasciculus. Theseaxons terminate in the dorsal horn, where theymodify the responses to painful stimuli. Opioidpeptides (endorphins) are the neurotransmittersinvolved in these mechanisms.
T
Largefibres
Smallfibres
Gate control system
SGActionsystem
Cognitivecontrol
Descendinginhibitory
control
Fig. 19.2 The gate control theory of pain as proposedby Melzack and Wall. Excitatory (white circle) andinhibitory (black circle) links extend from thesubstantia gelatinosa (SG) to the transmission cells (T)as well as descending inhibitory control from thebrainstem systems. All connections are excitatoryexcept the inhibitory link from SG to T. The roundknob at the end of the inhibitory link implies that itsaction may be presynaptic, postsynaptic or both.(From Melzack and Wall 1985. Reproduced withpermission.)
KAY19 12/16/04 7:58 PM Page 256

Benign specific pain syndromes
There are numerous benign pain syndromes thathave a specific, well-recognized pathologicalbasis. The more common syndromes presentingin neurological and neurosurgical practice are:• Head pain. Headache due to raised intracra-nial pressure, dural irritation, migraine or occipi-tal neuralgia.• Facial pain due to trigeminal neuralgia, disor-ders of the temporomandibular joint or sinusitis.• Upper limb pain, most commonly due to cervi-cal nerve root compression from a cervical discprolapse, carpal tunnel syndrome or thoracicoutlet syndrome.• Pain involving the trunk in a dermatome dis-tribution due to thoracic nerve root inflammationor compression, due to shingles (herpes zoster)or tumour.• Lower limb pain due to sciatica or lumbarcanal stenosis.
These clinical problems are discussed in therelevant chapters. The treatment is specific and,in general, effective. The success of the treatmentdepends on an accurate diagnosis and appropri-ate management.
There are two specific benign pain syndromesthat present to neurosurgeons: causalgia (reflexsympathetic dystrophy) and phantom limb pain.These problems have perplexed neuroscientistsand neurosurgeons as to the aetiology of the painand its treatment. Both are types of deafferentia-tion pain, in which the pain occurs as a result ofinjury to an afferent nerve.
Reflex sympathetic dystrophy syndrome
Reflex sympathetic dystrophy (RSD) is alsoknown as complex regional pain syndrome(CRPS), and is a multisymptom pain syndromethat usually affects one or more extremities. Thepain syndrome follows injury to a nerve whichmay be so slight that the patient may not even re-call having received an injury. For reasons poorlyunderstood, the pain develops due to aberrentfunctioning of the sympathetic nervous system.
Although the syndrome may follow a veryminor nerve injury, first symptoms may also de-
velop following major nerve damage, as docu-mented clinically, the condition has been knownas causalgia. The terms complex regional painsyndrome (CRPS) type 1 and type 2 have been inuse since 1995, when the International Associa-tion for the Study of Pain (IASP) considered that the names ‘reflex sympathetic dystrophy’ and‘causalgia’ were not sufficient to represent thefull spectrum of the symptoms and signs of the syndrome.
The diagnosis of RSD/CRPS is made in thecontext of a history of trauma to the affected area,associated with pain that is disproportionate towhat would be expected from the trauma plusone or more of the following:• abnormal function of the sympathetic nervoussystem• swelling• movement disorder• changes in tissue growth (dystrophy and atrophy).
The clinical features of RSD/CRPS include thefollowing.• Pain, which is described as severe and persis-tent, often with a burning and pleasant quality,and which spreads beyond the territory of the in-jured nerve or nerves. It is aggravated by physi-cal and emotional stimuli. Pain usually involvesthe hand or foot, but may spread through the affected limb.• Changes to the skin, which appears shiny, dry orscaly. The patient may have a sensation ofwarmth or coolness in the affected limb (vasomo-tor changes) and the skin may show increasedsweating (pseudomotor changes).• Swelling with pitting or hard oedema, that is usually diffuse and localized to the painful region.• Movement disorder, due to the patient havingdifficulty moving the limb because of the pain; inaddition there appears to be a direct inhibitory effect of RSD/CRPS on muscle contraction.
Initially the RSD/CRPS symptoms are generally localized to the site of injury, but astime progresses the features become more diffuse. X-rays may show wasting of the bone(patchy osteoporosis).
The mechanism by which an injury triggers
PAIN — NEUROSURGICAL MANAGEMENT 257
KAY19 12/16/04 7:58 PM Page 257

258 CHAPTER 19
abnormal function of the sympathetic nervoussystem is unclear. There is no laboratory test con-stituting definitive proof of the syndrome, butsympathetic block can be helpful both in con-firming the diagnosis and as a therapeutic option.
TreatmentTreatment involves the following.• Education and encouraging normal use of thelimb using physical therapies, including the useof a TENS (transcutaneous electrical nerve stimu-lation) machine.• Minimizing pain with medications that in-clude non-steroidal anti-inflammatory agents,antidepressants, anticonvulsants (e.g. carba-mazepine, gabapentin, sodium valproate) andsimple analgesic agents. Oral opioids have beenadvocated, but are not recommended due to potential hazards including addiction.• A sympathetic nerve block may be therapeu-tic, providing either a permanent cure or partialremission and will also help in confirming the di-agnosis. If there is a significant decrease in painfollowing the sympathetic block a definitivesympathetic ablation can be undertaken.
Other therapeutic measures are controversialbut include the use of spinal cord stimulation.
Phantom limb pain
Phantom limb pain is the perception of a painful sensation in an extremity that has beenamputated.
Virtually all amputees have phantom sensa-tions but only a small percentage have disablingpain in the phantom limb. Pain in the stump ofthe limb due to local factors is common and mustbe differentiated from true phantom limb pain,although they may be related.
The cause of phantom limb pain is unknown. Itmay develop immediately after the injury or atany stage up to some years later. The pain may result from deafferentation of the dorsal hornneurones and more rostral structures, althoughenvironmental and affective factors do play a rolein the patient’s pain behaviour and influence thedisability.
The management of this problem is particu-larly difficult. It involves a careful assessment ofthe environmental and psychological factors thatmay affect the patient. Numerous treatmentshave been tried, including various types of physical therapies, analgesic medication, anti-depressants, minor tranquillizers, anticonvulsants (carbamazepine) and psychological treatmentsincluding hypnotherapy and psychotherapy.
Many neurosurgical ablative procedures, suchas cordotomy, dorsal rhizotomy, neurectomy and sympathectomy, have been tried without success.
The dorsal root entry zone (DREZ) operationhas been used with some initial success in thetreatment of phantom pain. The operation in-volves destruction of the zone where the dorsalroot fibres enter into the spinal cord, usually bythermocoagulation.
Benign non-specific pain syndromes
Patients with chronic pain that does not have anunderlying specific pathological cause are fre-quently referred to a neurosurgeon for assess-ment and management. The pain problems mayinvolve any region of the body but there are anumber of particularly common types of clinicalpresentation.• Head — headache.• Face — atypical facial pain.• Upper limb — non-specific arm pain.• Spine — non-specific neck, thoracic or low backpain.• Lower limb — diffuse leg pain.
Many of the patients who present may have astructural, organic basis for a component of thepain problem, but the clinical manifestations arefar more extensive than can be explained by anypathological changes that can be demonstratedby either clinical or radiological findings. In somecases the presenting pain problem may just be amarked exaggeration of a true organic problem.In others, the presenting features will bear no re-lationship at all to any recognized clinical abnor-mality. Detailed questioning may reveal that thepatient ‘gains’ from the pain and that this gainmay be either psychological or involving definite
KAY19 12/16/04 7:58 PM Page 258

material benefit for the patient. Unfortunately,pending litigation is a real and often powerfulconscious or subconscious motive for the con-tinuation or exaggeration of symptoms.
Management
The management of these patients generally involves the following.• Exclude an organic basis for the complaint.This will involve detailed history and examina-tion and radiological investigations. It is ab-solutely vital that the clinician should objectivelyassess the patient thoroughly. Patients with neu-rological disorders will often present with atypi-cal clinical manifestations early in the diseaseprocess. It is wise, and very helpful, to reassessthe patient at a subsequent examination to be cer-tain there is not an organic basis for the present-ing complaint. It is important not just to dismiss apatient as being disagreeable, eccentric or havingan odd personality, as they may also have an or-ganic problem which may or may not bear rela-tionship to their underlying personality trait.• The clinician should assess the possibility ofany psychological origins for the pain and the social background of the patient. Reassurance isoften all that is necessary. For example, frequent-ly a patient may present with chronic headachesand, if it becomes apparent that a friend or rela-tive died recently from a brain tumour, all the pa-tient requires is reassurance that they do not havea tumour. Unfortunately many of the problemsare not this simple and more detailed counsellingor psychiatric advice may be necessary.• Maintain a positive mental attitude. Chronic,non-specific benign pain problems are debilitat-ing for the patient and the various doctors in-volved. It is all too easy just to dismiss the patientand hope the problem will fade away as the pa-tient disappears from sight. The patient has oftensought numerous opinions and usually has anegative attitude about themself, their pain andthe medical profession. It is helpful if the doctorcan give positive advice, reassure the patientthere is no serious underlying disease, encouragea positive mental attitude and be optimistic thatthe pain will resolve.
• Never use addictive medications. In particu-lar, it is essential never to resort to the use of narcotic analgesia, as this will inevitably make adifficult problem disastrous.
Cancer pain
The successful relief of pain in a patient sufferingfrom cancer is one of the major challenges of neu-rosurgery. For many patients not only is the diag-nosis of cancer associated with an enormoussense of grief and anxiety, but their greatest fear isthat they will suffer severe pain during the ill-ness. The two common misconceptions are thatall cancer is painful and that cancer pain cannotbe relieved. It is essential that the patients are reassured early in their illness that any pain theydevelop will be relieved.
The basic principles of the management of cancer pain are:• Explanation, reassurance and counselling.• Modification of the pathological process. Bonemetastases are the main cause of pain in the ma-jority of patients with carcinoma of the kidneyand thyroid and in multiple myeloma. Modifica-tion of the pathology by surgery (e.g. oöphorec-tomy for carcinoma of the breast, orchidectomyfor carcinoma of the prostate), radiotherapy,chemotherapy or hormonal treatment should beconsidered in consultation with an oncologist.• Elevation of the pain threshold. Reduction ofanxiety and improvement of a depressed moodwill help to elevate the pain threshold. Consider-able benefit may result from admission to hospi-tal or a specialized unit (palliative care unit orhospice unit), even for a short time. Adequate as-sessment and control of pain may permit patientsto return home. A feeling of security leads to reduced anxiety which can lessen pain and improve other symptoms.• Appropriate analgesic medication.• Neurosurgical techniques.
Pharmacological agents in cancer painmanagement
There is a concept of an ‘analgesic ladder’, whichinvolves moving from weak to strong analgesic
PAIN — NEUROSURGICAL MANAGEMENT 259
KAY19 12/16/04 7:58 PM Page 259

260 CHAPTER 19
drugs, with appropriate adjuvant therapy whennecessary, until pain is controlled. These adjuvants, or coanalgesics, which may includeantiemetics, antidepressants and corticosteroids,can be of great value in potentiating the primaryanalgesics. However, they may at the same timecompound the side-effects, either by interferingwith the pharmacology of the primary analgesicsor by exacerbating a primary side-effect, such assedation, of these analgesics.
The first choice is aspirin or an aspirin-likedrug. These drugs provide excellent analgesic,anti-inflammatory and antipyretic effects. An al-ternative to aspirin is paracetamol, which has asimilar antipyretic and analgesic activity but onlya weak anti-inflammatory effect. The major ad-vantage of both these drugs is the absence of unwanted side-effects, such as those exerted bythe opiates on the CNS. They are particularly active in the treatment of bone pain but they alsohave powerful analgesic activity on other organs.Aspirin’s well known side-effect on the gastroin-testinal tract may diminish its use in some situations but enteric-coated aspirin may be ofassistance in patients who have gastric intoler-ance to soluble aspirin. It is important to appreci-ate that soluble aspirin has a maximum durationof analgesic action of only 3–4 hours and conse-quently it must be given strictly every 4 hours inappropriate dosage. The usual method of admin-istration is to administer the aspirin every4 hours in a dose below that which will producetoxicity, which is usually heralded by ringing inthe ears. Paracetamol is usually commenced at adose of 500 mg–1 g every 4 hours and is increasedas necessary. However, at doses of more than 12 gin 24 hours the incidence of hepatic toxicity increases precipitously.
Codeine phosphate is a popular, short-acting,mild narcotic which may be useful in pain not adequately controlled by simple analgesics.
The aim of the use of narcotic analgesics is tocontrol the pain with a minimum of side-effects,preferably by the oral route. The narcotic shouldbe ‘titrated’ to a dose that will alleviate the pain.Morphine is the most common narcotic drug.Oral morphine is very satisfactory, provided thedose is carefully adjusted to suit the individual
patient. Its oral bioavailability is approximatelyone-third that of the parenteral use and this mustbe taken into consideration when changing patients from one route to the other. Oral medication should be a regular 4-hourly dose.Longer-acting forms of slow-release oral mor-phine that can be administered twice daily areoften the preferred narcotic for patients with debilitating cancer pain.
There are numerous other narcotic prepara-tions that may be administered either orally, par-enterally or via a suppository or skin patch andwhich may be useful in the individual patient tocontrol pain. The major disadvantage of oral orparenteral narcotic medication is the side-effects,particularly drowsiness and nausea. Oxycodonehydrochloride can be administered in a short- or long-acting form and is especially useful forbone pain, and in those patients not toleratingmorphine. Antiepileptic drugs such as sodiumvalproate and gabapentin are effective in thetreatment of neuropathic pain.
Neurosurgical techniques for paincontrol
Neurosurgical procedures will interfere with one or more of the psychological–anatomical–physiological pathways described previously(Table 19.1). Although, in general, neurosurgicalprocedures are only performed when the patienthas continuing unrelieved pain despite the bestmedical treatment, some techniques are simpleand are worth undertaking so that the dose ofanalgesia can be diminished.
The major neurosurgical techniques are:• Nerve section. This is the time-honoured neuro-surgical tool, although it has only a limited placein the control of cancer pain. Occasionally it maybe of use when the tumour infiltrates a peri-pheral nerve. Section of the cranial nerves in theposterior fossa may relieve the pain of an infiltrating head and neck tumour, althoughthese patients are often severely debilitated andthe necessary multiple nerve section may furtherincrease the morbidity.• Spinal cordotomy. Cordotomy involves sectionof the lateral spinothalamic tract and can be
KAY19 12/16/04 7:58 PM Page 260

performed either by open operation or percuta-neously at the C1/2 level. Although a high cervi-cal cordotomy may initially control pain in theupper limb the effect is often transient. Unfortu-nately it has only a limited place in the control ofcancer pain, as it will control pain satisfactorilyon only one side of the body, usually in the lowerlimb. Unfortunately, it is rare for cancer pain to bethis well localized. Bilateral cordotomy has ahigh morbidity and will not control pain if it isdiffuse.• Spinal cord stimulation. Epidural spinal cordstimulation has been used for the treatment ofnon-malignant chronic pain syndromes for nearly 30 years. The effectiveness of the tech-nique is controversial, but has been especiallyused for management of chronic back and ex-tremity pain. The exact mechanism by whichspinal cord stimulation works is unclear but ithas been postulated that the large fibres (tactilepositions and vibratory sensation) have a lowerthreshold of activation and can be recruited selec-tively by electrical stimulation, thereby closingthe ‘gate’ for pain signals originating from the peripheral nervous system (as proposed byMelzack and Wall). An electrode array is im-
planted extradurally and attached to an implant-ed pulse generator. The potential effectiveness ofthe technique can be trialled for each particularpatient by implanting a temporary electrodeprior to insertion of the definitive system.• Sympathectomy. A percutaneous chemical orsurgical sympathectomy is a potent method of re-lieving pancreatic pain due to carcinoma but it isdisappointing for benign pancreatic pain.• Intracerebral procedures. Cerebral procedures,such as deep brain stimulation, thalamotomyand leukotomy, are now only rarely indicated inthe control of pain.• Deep brain stimulation (DBS) is a treatment oflast resort for a highly selected population of pa-tients with chronic pain but has been used withsome success in the treatment of central and de-afferentation pain including phantom pain, thalamic pain and anaesthesia dolorosa. It hasalso been used for peripheral neuropathic painand nociceptive pain. DBS does not work well forrecurring acute pain and is not generally effectivefor cancer pain, but may have a small role forcancer pain in sites which are difficult to treat bydestructive procedures.
The preferred targets for deafferentation painare sensory thalamus (ventroposteromedial(VPM) and ventroposterolateral (VPL), or the in-ternal capsule (IC)); and for peripheral nocicep-tive or neuropathic pain the periaqueductal greymatter (PAG) or periventricular grey (PVG).However, there is cross-over of effect betweenthese two sites. Two electrodes can be placedthrough the same burr hole, contralateral to themain pain, or on the non-dominant side for bilat-eral pain. Unilateral PVG or PAG stimulationmay control bilateral pain, but if thalamic (or in-ternal capsule) stimulation is required for bilater-al pain then bilateral electrodes may be required.
A high response rate for pain of peripheral ori-gin and for deafferentation pain of up to 60% hasbeen reported but a long-term overall successrate of only around 30%.
Chronic electrical stimulation of the septalarea, the Kölliker–Fuse nucleus and the motorcortex has also been used to treat centralsupraspinal pain and trigeminal neuropathicpain with promising results, although these tech-
PAIN — NEUROSURGICAL MANAGEMENT 261
Table 19.1 Neurosurgical procedures for cancerpain.
Nerve sectionCranial nervesPeripheral nerves
CordotomyOpenClosed
Sympathectomy
Cerebral proceduresDeep brain stimulationThalamotomyLeukotomy
Opiate administrationEpiduralIntrathecal (lumbar, subarachnoid)Intraventricular
KAY19 12/16/04 7:58 PM Page 261

262 CHAPTER 19
niques remain experimental. Chronic electricalstimulation of the trigeminal nerve root has beentried for intractable facial pain, including anaes-thesia dolorosa, with about 50% of patients re-porting at least a 50% reduction in pain. The useof DBS for pain may decrease in the future, as agreater understanding of the neuropharma-cology of pain has resulted in improved pharma-cotherapy for chronic pain.• Subarachnoid opiate administration. Most cancerpain can be effectively controlled with oral, sup-pository or subcutaneous infusion administra-tion of opiates. Lumbar intradural subarachnoidadministration of morphine is particularly usefulin patients with terminal cancer pain whose painis unrelieved by oral, subcutaneous or suppo-sitory administration, or who do not tolerate theside-effects of the high doses of narcotics neces-sary to control the pain. The technique allowsvery small doses of narcotic to be given directlyinto the subarachnoid space and avoids many ofthe unpleasant side-effects of high-dose narcoticadministration. Opiate receptors have been iden-tified in the brain and spinal cord. The receptordensity is high in the periventricular structuressuch as the amygdala, caudate, putamen, medialthalamus and habenular, in the periaqueductgrey matter, and in the floor of the 4th ventricle.The greatest concentration of receptors in thespinal cord is in the substantia gelatinosa. Thesereceptors are the likely synaptic site of action forlocal terminals, which release endogenous com-pounds with actions similar to opioid alkaloids(endorphins), and also for the injected subarach-noid morphine.
The basic technique of lumbar intradural opiate administration involves the insertion of acatheter into the subarachnoid space of the lum-bar theca. The catheter is threaded subcutaneous-ly to the anterior abdominal or chest wall, whereit is connected to a subcutaneous reservoir. Themorphine can be injected directly into the reser-voir, using meticulous sterile technique becauseof the risk of infection. Alternatively, infusionpumps can be implanted subcutaneously, filledwith morphine and joined to the spinal catheter.Their major disadvantage is the expense of thepump.
Injection of morphine through the lumbarcatheter will result in pain relief in most sites ofthe body, although it is less successful for pain in-volving the head, neck and upper limbs. In thesesituations an intraventricular catheter, with asubcutaneous reservoir, can be inserted for mor-phine administration.
There is a small risk of respiratory depressionand the patient should be observed closely fol-lowing the initial doses. If a subcutaneous reser-voir is implanted the treatment regime usuallycommences with 0.5 mg morphine twice daily.The patient should fill in a pain chart which willdocument the level of pain throughout the day;the intrathecal morphine can be increased as necessary. The pain is usually satisfactorily con-trolled with a dose of morphine of between 1 and10 mg/day. Supplementary oral narcotic or non-narcotic medication can also be used.
The major complications are infection of thecatheter, which may lead to meningitis, andblockage of the catheter.
Further readingGilman S, Newman SW (1987) Manter and Gatz’s Essen-
tials of Clinical Neuroanatomy and Neuropathology, 7thedn. F A Davis, Philadelphia.
Kaye AH, Black P McL (2000) Operative Neurosurgery.Churchill Livingstone, London, New York, Edinburgh.
Melzack R (1973) The Puzzle of Pain. Basic Books, NewYork.
Melzack R, Wall PD (1965) Pain mechanisms: a new series. Science 150, 971–979.
Melzack R, Wall PD (1985) In: Wilkins RH, RengacharySS, eds. Gate Control Theory in Neurosurgery. McGraw-Hill, New York, 2317–2319.
Nashold BS, Ostdahrl H (1979) Dorsal root entry zonelesions for pain relief. Journal of Neurosurgery 51,59–69.
Wall PD, Melzak R (1989) Textbook of Pain, 2nd edn.Churchill Livingstone, Edinburgh.
White JC, Sweet WH (1969) Pain and the Neurosurgeon.Charles C Thomas, Illinois.
Yaksh TL (1987) Opioid receptor systems and the endorphins. A review of their spinal organisation.Journal of Neurosurgery 67, 157–176.
KAY19 12/16/04 7:58 PM Page 262

Involuntary movement disorders are related todiseases of the extrapyramidal system, in parti-cular the basal ganglia and their connections. Thelesions are usually diffuse, affecting both the nu-clear connections and communicating pathways,and involve disorders of the delicate balance ofneurotransmitters. The pharmacological basis ofmovement disorders is generally a result of achemical imbalance between two or more oppos-ing neurotransmitter systems. The major basalganglia neurotransmitters identified includedopamine, norepinephrine, gamma-aminobu-tyric acid, serotonin, acetylcholine and glutamicacid.
Anatomical overview
The basal ganglia, and their connections, formthe anatomical substrate for most of the move-ment disorders, although the exact abnormalitymay not be clearly defined.
The corpus striatum is the major centre in thecomplex extrapyramidal motor system and iscomposed of:• the globus pallidus (palaeostriatum)• the caudate nucleus and putamen (the neostriatum).
The putamen and globus pallidus togetherform the lentiform nucleus.
The complex interconnections between thebasal ganglia, the red nucleus, the cerebellar out-flow tracts, the brainstem reticular formation andthe motor cortex are shown in Figs 20.1 and 20.2.There are two interconnecting pathways of par-ticular importance to the neurosurgical manage-ment of movement disorders.
1 The corpus striatum neurones project to theglobus pallidus and subsequently to the ventralanterior nucleus of the thalamus by:
(a) the lenticular fasciculus which passes ros-tral to the subthalamic nucleus(b) the ansa lenticularis passing below the sub-thalamic nucleus.
The majority of the fibres of the lenticular fascicu-lus and the ansa lenticularis merge in Forel’s fieldH, enter the thalamic fasciculus (Forel’s field H1)and project rostrally and dorsally into the ventralanterior and ventral lateral thalamic nuclei. Fibres from the thalamus pass to the supplemen-tary motor cortex. The circuit is completed bycortical neurones projecting to the caudate nucleus, then to the putamen and on to theglobus pallidus (Fig. 20.1).2 A circuit links the cerebellum to the thalamusvia the dentate nucleus and red nucleus, andthese fibres then pass to the primary and secondary motor cortex. Neurones descend fromthe cortex to the nuclei in the pontine reticularformation which project to the cortex of the cere-bellum (Fig. 20.2).
Neurosurgical lesions to control movementdisorders have been made:• in the ventrolateral nucleus of the thalamus(thalamotomy)• in the globus pallidus (pallidotomy)• in Forel’s field• in the dentate nucleus (dentatotomy) —historical only• in the ansa lenticularis (ansotomy).
CHAPTER 20
20 Movement disorders —neurosurgical aspects
263
KAY20 12/16/04 7:59 PM Page 263

264 CHAPTER 20
Involuntary movement disorders
Parkinson’s disease
Parkinson’s syndrome was described by JamesParkinson in 1817 in An Essay on the Shaking Palsyand was recognized as an extrapyramidal disor-der by Kinnier Wilson in 1912. The principalpathological disorder is a depletion of dopaminestores in the cells of the substantia nigra andneostriatum.
Parkinson’s syndrome has a number of possi-ble causes, of which idiopathic Parkinson’s disease is the most common (Table 20.1). Parkinson’s disease following encephalitislethargica is now rare, although it may occur dur-ing the course of degenerative disorders such asAlzheimer’s disease.
Essential clinical features• A coarse tremor (4–8 Hz) which usually beginsunilaterally in the upper limbs but eventuallyspreads to all limbs. Movement of the fingers oc-curs at the metacarpophalangeal joints and maybe combined with movements of the thumb, the‘pill rolling’ movement.• Rigidity. When tested by passive movementthe muscles may yield to tension in a series ofjerks — cog wheel rigidity — although the in-creased muscle rigidity is sometimes smooth andis called ‘plastic’ or ‘lead pipe’ rigidity.• Bradykinesia. The impairment of movement,consisting of difficulty in initiating movement
Supplementarymotor cortex
Putamen
Globuspallidus
Subthalamicnucleus
Forel's field
Thalamus
Caudatenucleus
Fig. 20.1 Extrapyramidal pathway for movementshowing Forel’s field and relationship to basal gangliaand thalamus described in text.
Motorcortex
Cerebellarcortex
Pons
Thalamus
Red nucleus
Dentate nucleus
Fig. 20.2 Dentatorubrothalamic extrapyramidalpathway which is adjacent to that shown in Fig. 20.1.
Table 20.1 Differential diagnosis of Parkinson’ssyndrome.
DegenerativeIdiopathic parkinsonism, adult and juvenile
formsStriatonigral degenerationShy–Drager syndromeOlivopontocerebellar degenerationSupranuclear palsyParkinson–ALS–dementia complex
InfectiousPostencephalitic parkinsonismCreutzfeldt–Jakob disease
ToxicHeavy metals (manganese)
DrugsPhenothiazinesButyrophenonesRauwolfia alkaloidsAlpha-methyldopa
VascularStrokeCarbon monoxide
Neoplasm
MetabolicHypoparathyroidismWilson’s disease
Taken from Olanow (1981). Reproduced withpermission.
KAY20 12/16/04 7:59 PM Page 264

(akinesia) and slowness with which it is per-formed (bradykinesia), is the most disabling feature of Parkinson’s disease. In general, themovements that are carried out by the small mus-cles are the most affected. Consequently, early inthe disease the patient shows weakness of ocularmovements and facial movements, resulting inthe ‘mask-like’ facies, and there is impairment ofmastication and articulation. Swinging the armswhen walking is diminished early and as the disease progresses the gait becomes severely im-paired. The slowness is most severe on initiatingmovements and the patient may ‘freeze’.• Other abnormalities include dementia, whichoccurs in a third of parkinsonian patients, seborrhoea, sialorrhoea and gastrointestinalproblems.
ManagementL-Dopa therapy revolutionized the treatment ofParkinson’s disease and dramatically decreasedthe need for stereotactic surgery. Most patientsare managed with medical therapy and are notreferred to the neurosurgeon. However, stereo-tactic surgery does have a limited place in thetreatment of Parkinson’s disease.
Many patients develop troubling side-effectsfrom the L-dopa medication with wide fluctua-tions in the severity of their movement disorderfrom total inactivity (‘off’ time) to hyperactivedyskinetic states (‘on’ time) which can be refrac-tory to any medical therapy. This group may re-spond to pallidotomy as it has a beneficial effecton the bradykinesia and the dyskinesia but littleeffect on tremor. Pallidotomy is usually per-formed bilaterally as these patients are affectedon both sides of the body.
Tremor responds best to thalamotomy whichhas little effect on the bradykinesia or rigidity.Tremor does not respond well to medication.Thalamotomy is particularly suitable for the patients with unilateral tremor. Bilateral thalam-otomy carries a significant risk to the patient ofcausing limb weakness, dysarthria or dysphonia.Deep brain stimulation is a new procedure inwhich an electrode is usually placed in the thala-mus and connected to a battery-operated pulsegenerator, which is implanted beneath the skin of
the chest wall. This produces a high-frequency,low-voltage current from the tip of the electrodewhich blocks the tremor. It has been highly effec-tive and carries a lower morbidity than thala-motomy because it is non-destructive and ispotentially reversible. It can be placed bilaterallyand is now being used to stimulate other parts ofthe brain, such as globus pallidus and subthala-mic nuclei, in patients with Parkinson’s disease.
Neural transplantation of fetal mesencephalonto the neostriatum of humans is a controversialexperimental technique which has had variableand questionable success. The ethical problemsof obtaining fetal tissue are a strong barrier toperforming this operation and there is the possi-bility of rejection of the immunologically foreigntissue.
Essential tremor
Benign, or ‘essential’, familial tremor often has afamilial basis, frequently commences before theage of 30, and may be fine and rapid or slowerand coarse. It is characteristically an ‘actiontremor’, as it tends to be increased by voluntarymovement and emotion. The patient frequentlynotes that it may be improved following drink-ing alcohol. The usual medication includespropanolol and/or diazepam.
Stereotactic surgery (thalamotomy or deepbrain stimulation) may be considered if thetremor is not improved with medication and ifthe patient is disabled by the symptoms; signifi-cant improvement has been reported in 70–80%of cases.
Tremor secondary to neurological degenera-tive diseases such as multiple sclerosis, cere-brovascular disease, encephalitis or traumaresponds less favourably to surgery.
Cerebral palsy
The two components of cerebral palsy that maybe helped by neurosurgical intervention are:• the choreoathetoid movements• spasticity.
Chorea is characterized by rapid, jerky, irrele-vant, asymmetrical movements of the limbs and
MOVEMENT DISORDERS — NEUROSURGICAL ASPECTS 265
KAY20 12/16/04 7:59 PM Page 265

266 CHAPTER 20
trunk. Athetosis is a relatively slow movementwith a sinuous or writhing character. These twomovements frequently coexist in cerebral palsy,together with other features which may includecombinations of spasticity, rigidity, dystonia,ataxia and tremor.
Cerebral palsy patients with choreoathetosisand/or spasticity, who are not severely disabledby the other features of cerebral palsy and whodo not have severe mental retardation, have beenconsidered for stereotactic surgery, although thisis now rarely used. Lesions have been made inthe ventrolateral thalamus or in Forel’s field forchoreoathetosis, and in the dentate nucleus forspasticity. The lesions frequently need to be bilateral. Although initial significant improvement is reported in over 70% of cases in some series, theeffect diminishes with time. Chronic stimulationof the cerebellum using implanted electrodes hasbeen advocated for the treatment of spasticity incerebral palsy but there is no convincing evi-dence of significant benefit at this stage.
In patients with spastic diplegia which in-volves spasticity and incoordination of the lowerlimbs, selective dorsal rhizotomy, in which abnormally hyperactive dorsal rootlets on intraoperative stimulation are severed from L1 toS1 on each side, has been successful at reducingspasticity and improving the gait pattern. Orthopaedic surgery with tendon-lengtheningprocedures on the hips, knees and ankles is still amainstay of treatment for children with cerebralpalsy and is used in conjunction with a rhizo-tomy operation.
Hemiballismus
This movement disorder is characterized by vio-lent, irregular, jerky movements of one side of thebody; these arise primarily from the shoulder.The anatomical basis is a lesion of the sub-thalamic nucleus contralateral to the abnormalmovement. It usually results from vascular dis-ease but occasionally occurs in multiple sclerosis.It is an uncommon complication of stereotacticsurgery, resulting from the inadvertent involve-ment of the subthalamic nucleus during the pro-duction of a lesion in the thalamus.
The condition often settles spontaneously anddrug treatment is ineffective. Stereotactic surgeryis of benefit in over half of patients and the usualtarget is the ventrolateral nucleus of the thalamusor Forel’s field.
Dystonia
Dystonia is an abnormal posture produced byspasms of muscles and/or exaggerated muscletone. Dystonia may be generalized, as in dystoniamusculorum deformans, or restricted to specificmuscle groups. Spasmodic torticollis is some-times regarded as a partial form of torsion dysto-nia and is discussed in the next section.
Symptomatic dystonia may occur in manyneurological disorders including cerebral palsy,infantile hemiplegia, Wilson’s disease and in-toxication with phenothiazines. Idiopathic torsion dystonia is inherited as an autosomal recessivetrait in Ashkenazi Jews and as an autosomaldominant disorder in non-Jewish populations,but many cases are sporadic. The onset usuallyoccurs in childhood or adolescence and is ofteninitially manifest as a spasmodic plantar flexionof the feet. The involuntary movements in theupper limbs consist of rotation or torsion and areassociated with torsion movements of the verte-bral column, particularly in the lumbar region.Medical treatment, including L-dopa, haloperi-dol, carbamazepine and anticholinergic therapy,is usually of little benefit. Stereotactic surgeryproduces some benefit in over half the patients.The procedure involves bilateral stereotactic lesions in the ventrolateral nucleus or Forel’sfield.
Spasmodic torticollis
Spasmodic torticollis is characterized by a clonicor tonic contraction of the cervical muscles whichproduces rotation of the head and neck; this maybe sustained or spasmodic. Retrocollis is a similardisorder in which the neck is extended.
The aetiology of this unusual condition has notbeen clearly defined. Although in some cases thecondition may be hysterical, it is evident that tor-ticollis may be due to organic disease of the ner-
KAY20 12/16/04 7:59 PM Page 266

vous system and some regard it as a limited formof torsion dystonia. It has been noted as a sequelof encephalitis lethargica or as part of other extrapyramidal syndromes. The microvascularcompression theory, similar to that for trigeminalneuralgia and hemifacial spasm but with com-pression of the spinal accessory nerve or nerves,has been proposed, but as yet there is no evidenceto substantiate this possibility.
The clinical manifestations include a rotationof the head and neck by contraction of the cervi-cal muscles. The contraction of the sternocleido-mastoid, trapezius and splenius muscles isevident on examination, although the deep mus-cles of the neck are also involved. Rotation mayoccur with or without lateral flexion. The con-traction may be chronic, with repeated jerks, orpredominantly tonic with a sustained posture.Retrocollis is due to bilateral contraction of thesplenius and trapezius.
ManagementThe distinction between hysterical torticollis andtorticollis of an organic origin may be difficult.Treatment should include psychotherapy andminor tranquillizers if it is thought that the torti-collis has a hysterical basis.
Electromyographic studies may help to eva-luate the exact muscles involved in producing thetorticollis. Tetrabenazine is occasionally success-ful if there is an organic basis, but it may producedrug-induced parkinsonism. Botulinum toxin in-jected into the affected muscles may improve thetorticollis, but its effect is usually transitory andrepeated injections at regular intervals may benecessary.
There are a number of surgical operations,which include:• division of the accessory nerves and the anterior roots of C1–3• myotomy, particularly section of the dominantsternocleidomastoid muscle• various stereotactic procedures• microvascular decompression of the spinal accessory nerve or nerves.
Intradural section of one or both accessorynerves and of the anterior upper cervical rootshas been the most commonly performed proce-
dure. The anterior roots of C1–3 are usually di-vided on the passive side and C1–4 on the domi-nant side. The operation has been reported asproducing satisfactory results in up to 80% of pa-tients, although the general experience of mostsurgeons indicates a lower success rate. It is amajor operative procedure with a significant riskof morbidity, particularly dysphagia, but a lowrisk of mortality. This procedure has now beenlargely superseded by a selective peripheral denervation of the cervical rami, described in1991 by Claude Bertrand as a peripheral ramisec-tomy. This procedure can be undertaken withouta laminectomy and involves sectioning of theposterior primary rami after they emerge fromthe spinal canal. A sternocleidomastoid myoto-my or spinal accessory neurectomy is usuallyperformed with the procedure.
Further readingBenabid A et al. (1991) Long-term suppression of tremor
by chronic stimulation of the ventral intermediatethalamic nucleus. Lancet 337, 403–405.
Bucy C (1951) The surgical treatment of extrapyramidaldiseases. Journal of Neurology, Neurosurgery and Psychiatry 14, 108–115.
Burke RE, Fahn S (1981) Movement disorders. In: AppelSH, ed. Current Neurology. John Wiley, New York,92–137.
Cooper IS (1969) Involuntary Movement Disorders. Hoeber, New York.
Dandy WE (1930) An operation for treatment of spas-modic torticollis. Archives of Neurology 20, 1021–1032.
Gildenberg PL, Tasker RR (1982) Spasmodic torticollis.Contemporary Neurosurgery 4 (6), 1–7.
Hamby WB, Schiffer S (1969) Spasmodic torticollis: results after cervical rhizotomy in 50 cases. Journal of Neurosurgery 31, 323–326.
Hoehn MM, Yahr MD (1967) Parkinsonism: onset, pro-gression and mortality. Neurology 17, 427–442.
Iacono RP, Lonser RR, Ulloth JF, Shima F (1995) Pallidotomy in Parkinson’s disease. Neurosurgery 36(6), 1118–1125.
Kaye AH, Black P McL (2000) Operative Neurosurgery. Churchill Livingstone, London, New York, Edinburgh.
Kelly PJ, Gillingham FJ (1980) The long-term results ofstereotactic surgery and L-dopa therapy in patientswith Parkinson’s disease: A 10-year follow-up study.Journal of Neurosurgery 53, 332–337.
MOVEMENT DISORDERS — NEUROSURGICAL ASPECTS 267
KAY20 12/16/04 7:59 PM Page 267

268 CHAPTER 20
Laetinen LV, Bergenheim AT, Hariz MI (1992) Leksell’sposteroventral pallidotomy in the treatment ofParkinson’s disease. Journal of Neurosurgery 76, 53–61.
Lundsford LD (1988) Modern Stereotactic Neurosurgery.Martinus Nijhoff, Boston.
Marsden CD, Harrison MJG (1974) Idiopathic torsiondystonia (dystonia muscularum deformans): Areview of 42 patients. Brain 97, 793–810.
Olanow CW (1981) Current concepts in the manage-ment of movement disorders. Clinical Neurosurgery28, 137–170.
Parkinson J (1817) An Essay on the Shaking Palsy. Sherwood Neely and Jones, London.
Rasmussen T, Marino R (1979) Functional Neurosurgery.Raven Press, New York.
Rosenfeld JV (1994) Human neural transplantation:Current progress and future prospects. Journal ofClinical Neuroscience 1, 231–242.
Tasker RR (1987) Tremor of parkinsonism and stereo-tactic thalamotomy (editorial). Mayo Clinic Proceedings 62, 736–739.
KAY20 12/16/04 7:59 PM Page 268

Epilepsy is a common neurological disorder oc-curring in approximately 1% of the populationwith about 1 in 50 having a single seizure atsome stage in their lives. Epilepsy is defined as atendency to have recurrent seizures, and a single seizure does not therefore compriseepilepsy.
An epileptic seizure may be described as atransient derangement of the nervous systemdue to a sudden, excessive and disorderly dis-charge of cerebral neurones. This was the postu-lation of Hughlings Jackson, the eminent Britishneurologist, and to the present time remains theaccepted mechanism. The electrical dischargesresult in a diversity of clinical manifestationsranging from a tonic–clonic, or grand malseizure, to a brief episode of loss of awarenesswith minimal motor involvement, characteristicof an absence, or petit mal seizure.
In general, neurosurgical practice involves themanagement of epilepsy:• when an epileptic seizure is the presentingsymptom of an underlying intracranial lesionsuch as a brain tumour• as a complication of head injury or intracranialsurgery• in the surgical management of patients withintractable epilepsy; in particular, temporal lobeepilepsy.
Classification of seizures and epilepsies
It is important to distinguish between types ofseizures and types of epilepsies, the former beingthe symptom and the latter being the syndrome
or disease. The task of finding a satisfactory clas-sification of epileptic phenomena is one whichhas exercised the minds of experts over manydecades and continues.
Classification of seizures
Table 21.1 summarizes the classification ofepileptic seizures, based on the InternationalLeague Against Epilepsy classification. The clas-sification includes three major seizure types.1 Generalized.2 Partial.3 Unclassifiable.
Generalized seizuresIn generalized seizures the electrical dischargesare bilateral, synchronous and symmetrical, in-volving both cerebral hemispheres from theonset. Despite this common electrophysiolo-gical basis, the clinical manifestations of the generalized seizures vary markedly.
A typical tonic–clonic (grand mal) seizure isunmistakable. The seizure begins with a tonicphase lasting 10–15 seconds, during which thepatient may fall to the ground with loss of con-sciousness. The body stiffens and there may be apiercing cry as the body is seized in a tonicspasm. The patient clenches the teeth, may bitethe tongue and becomes apnoeic. Urinary incon-tinence may follow. The tonic phase is followedby a clonic phase lasting 1–2 minutes, charac-terized by rhythmical muscular contraction involving the entire body. A postictal phase, consisting of confusion and drowsiness, follows.Tonic–clonic seizures do not always conform to
CHAPTER 21
21 Epilepsy and its neurosurgical aspectsChristine Kilpatrick
269
KAY21 12/16/04 8:00 PM Page 269

270 CHAPTER 21
this classic description, but always involve loss ofconsciousness.
Petit mal, or absence seizures, are charac-terized by brief loss of consciousness often last-ing only 5–10 seconds. During this time, thepatient, usually a child, is witnessed to stare andthere may be minor motor involvement such asblinking of the eyes, but the patient does not fall.Abruptly, consciousness is regained with amne-sia for the event. During the seizure, the elec-troencephalogram shows bilateral synchronous3-Hz spike and wave activity. This EEG abnor-mality and the seizure may be provoked by hyperventilation.
Myoclonic seizures are less common and arecharacterized clinically by brief, often single,jerking of the trunk and/or limbs. These may berelatively minor, involving only one limb, or maybe profound, causing the patient to fall to theground. The EEG during a myoclonic seizureshows bilateral synchronized spike and wave activity.
Partial seizuresIn contrast to generalized seizures, in partialseizures the electrical activity begins in a definedfocus. Partial seizures are subdivided into:• simple• complex• secondarily generalized.
In simple partial seizures there is no alterationin the conscious state, whereas with complexpartial seizures the conscious state is impaired. Ifthe focus is in the motor cortex, as may occur witha parasagittal meningioma, the patient may ex-perience a rhythmical jerking of the contralaterallimb without impairment of conscious state — asimple partial seizure of motor type. When thefocus is in the temporal lobe, as with mesial tem-poral sclerosis (MTS) or a temporal lobe glioma,the conscious state is often impaired — the patienthas a complex partial seizure.
Most complex partial seizures arise from thetemporal lobe, but may arise from the frontal,parietal or occipital lobes. Complex partialseizures of temporal lobe origin often begin withan aura, such as a feeling of intense fear, an epi-gastric rising sensation, an unusual taste or smell,or a feeling of déjà vu. This aura or simple partialseizure may occur in isolation. The aura is oftenfollowed by arrest of motor activity with loss ofawareness. Oral automatisms such as lip smack-ing, chewing movements and repetitive swal-lowing are frequently seen, as are automatisms ofthe upper limbs. In some patients, lateralizingfeatures such as immobility or dystonic postur-ing of the contralateral upper limb are observed.If the seizure comprises impairment of consciousstate alone, then the seizure may be confusedwith an absence seizure. With both simple andcomplex partial seizures the focal electrical dis-charge may generalize and the patient has a secondarily generalized tonic–clonic seizure.
Classification of epilepsies
The types of epilepsy are defined on the basis of:• types of seizures• associated clinical features.
The approach to a patient with epilepsy shouldinclude analysis of the seizure type or types andan assessment of associated clinical features suchas age of onset, allowing in many patients the di-agnosis of an epilepsy syndrome or disease to be made. This is particularly relevant when considering the generalized forms of epilepsy.The epilepsies as proposed by the InternationalLeague Against Epilepsy are divided into partial
Table 21.1 Classification of seizures.
GeneralizedTonic–clonic (grand mal)Absence (petit mal)MyoclonicTonicAtonic
Partial (focal)Simple partial seizure — without impairment of
conscious stateComplex partial seizure — impairment of
conscious statePartial seizure — secondarily generalized
Unclassifiable
KAY21 12/16/04 8:00 PM Page 270

epilepsies and generalized epilepsies (Table21.2). Patients seen by neurosurgeons usuallyhave partial epilepsy. Partial epilepsies are thosein which the seizures have either a focal struc-tural basis (e.g. glioma) and/or a focal electricalorigin. A patient presenting with a tonic–clonicseizure and whose computerized tomography(CT) scan reveals a glioma has almost certainlyhad a secondarily generalized tonic–clonicseizure and hence has a symptomatic partialepilepsy. Even though the seizure, based on theavailable history, may have no obvious focal fea-tures, the electrical activity has almost certainlybegun at the site of the tumour. A patient withtemporal lobe epilepsy due to MTS with bothcomplex partial seizures and occasional secon-darily generalized tonic–clonic seizures also hasa symptomatic partial epilepsy.
Benign childhood epilepsy with centrotempo-ral spikes is an example of idiopathic partialepilepsy — there is no underlying structural basisfor the focal electrical and clinical features. Thiscondition occurs in otherwise normal childrenand remits spontaneously during adolescence.The seizures are focal or partial, frequently sleeprelated, and often characterized by orofacial or
oropharyngeal involvement. The interictal EEGdemonstrates a spike focus in the centrotemporalregion.
In the generalized epilepsies there is no underlying focal structural pathology and theseconditions are usually managed by neurologists.The generalized epilepsies are subdivided intoprimary generalized epilepsy and secondarygeneralized epilepsy. Primary generalizedepilepsy in its pure form constitutes a conditionwhere there is no underlying pathological abnor-mality and the major aetiological factor is the inherited trait for the gene that is expressed electrographically as generalized spike wave dis-charges. Secondary generalized epilepsy usuallybegins in childhood. In its pure form it consists ofa diffuse grey matter disease, usually due to ac-quired factors. The most common subgroup isthe Lennox–Gastaut syndrome. The former has agood prognosis, but the latter is associated with apoorer prognosis. Primary generalized epilepsyis subdivided into a number of recognized clini-cal syndromes; the more common syndromes areshown in Table 21.2.
Post-traumatic epilepsy
The occurrence of an epileptic seizure following ahead injury is well recognized.
Post-traumatic epilepsy may be classified intothree types.1 Immediate epilepsy.2 Early epilepsy.3 Late epilepsy.
Immediate epilepsy. Immediate epilepsy refers to aseizure which occurs at the time of, or withinminutes of, the head injury. It does not usuallyrecur, carries a good prognosis and its occurrencedoes not predispose patients to late post-trau-matic epilepsy.
Early epilepsy. Early epilepsy is defined asseizures occurring within the first week of a headinjury. In adults they tend to complicate quite severe head injuries, often with intracranial haemorrhage, prolonged post-traumatic amnesia or depressed fractures. In children early seizures
EPILEPSY AND ITS NEUROSURGICAL ASPECTS 271
Table 21.2 Classification of the epilepsies.
Partial epilepsiesSymptomatic (e.g. mesial temporal sclerosis,
tumour)Idiopathic (benign childhood epilepsy with
centrotemporal spikes)
Generalized epilepsiesPrimary generalized epilepsies
Benign neonatal convulsionsChildhood absence epilepsyJuvenile absence epilepsyJuvenile myoclonic epilepsy of JanzEpilepsy with tonic–clonic seizures on
awakeningSecondary generalized epilepsies
Lennox–Gastaut syndromeWest’s syndromeEpilepsy with myoclonic absences
KAY21 12/16/04 8:00 PM Page 271

272 CHAPTER 21
are relatively common and may complicate rela-tively minor injuries. In children, early seizuresare often limited to focal twitching. Early seizurespredispose to late seizures, with 25% of adult patients with early seizures having recurrent lateseizures. In children early seizures also predis-pose the patient to late epilepsy, but the risk isless than in the adult population. The incidenceof late epilepsy appears to be unaffected by thetype, time and number of early seizures.
Late epilepsy. Late epilepsy is defined as seizuresoccurring after the first week of trauma and mayappear for the first time some years after the headinjury. Over 50% of those destined to develop lateepilepsy will do so within the first year; the inci-dence then falls rapidly over the following 3years so that after 4 years there is only a small ongoing risk.
Fifty per cent of patients with late epilepsyhave seizures with focal features, although manyare subject to tonic–clonic seizures without obvious focal manifestation. Absence seizures are never the direct result of head trauma. Most pa-tients with late post-traumatic seizures continueto have recurring seizures, albeit infrequently.
Factors predisposing patients to late post-traumatic epilepsy include:• post-traumatic amnesia of more than 24 hours• intracranial haemorrhage• occurrence of early seizures• depressed skull fracture.
Table 21.3 tabulates these clinical features andassociated risks of late post-traumatic epilepsy.
Post-traumatic epilepsy is usually treated withphenytoin or carbamazepine. Head injuries withclinical features associated with a high risk ofpost-traumatic epilepsy are treated prophylacti-cally with phenytoin or carbamazepine. If noseizures occur, treatment is usually ceased after12 months.
Postoperative epilepsy
The occurrence of seizures for the first time following craniotomy is well recognized. The incidence varies depending on the type of
neurosurgical procedure, but the overall inci-dence is estimated to be about 18%. Almost halfoccur within the first week of surgery and two-thirds occur within the first postoperative month.Conditions such as cerebral abscess and tumourare frequently associated with seizures and howmuch of the risk relates to the surgery and howmuch to the underlying pathology is difficult toassess. The incidence of postoperative seizuresfollowing aneurysm surgery is about 20%, withseizures being most common with middle cere-bral artery aneurysms. A similar incidence is re-ported for convexity meningiomas. Burr holebiopsy has a lower incidence of seizures of 9%.Seizures do not complicate posterior fossasurgery.
Postoperative prophylaxis
Most studies assessing the value of seizure pro-
Table 21.3 Influence of various factors on theincidence of late post-traumatic epilepsy.
Risk of late post-traumatic
Associated clinical feature epilepsy (%)
Post-traumatic amnesia > 24 hours 3Early seizures 25
Post-traumatic amnesia > 24 hoursEarly seizures 25
Compound depressed fractureDura intact 7Dura torn 25Extradural haemorrhage 20Subdural haemorrhage (acute) 40Intracerebral haemorrhage 50
Post-traumatic amnesia > 24 hoursEarly seizures and intracranial 35
haemorrhage
Post-traumatic amnesia > 24 hoursDural tearEarly seizuresCompound depressed fracture 70
KAY21 12/16/04 8:00 PM Page 272

phylaxis with antiepileptic therapy have shown areduction in the incidence of postoperativeseizures. Phenytoin is the drug of choice for postoperative seizure prophylaxis.
As the incidence of seizures is high during thefirst postoperative week, patients should receivea preoperative loading dose of phenytoin andthen continue on maintenance therapy. Ifseizures do not occur and the intracranial lesionhas been excised, prophylactic treatment withphenytoin is usually discontinued after 6months.
If seizures occur despite adequate phenytoinplasma levels, carbamazepine should be introduced.
Tumours and seizures
Although the major concern when a patient pre-sents with a seizure is the possibility of a cerebraltumour, tumours are responsible for late-onsetepilepsy (as defined by seizures occurring afterthe age of 25 years) in only about 10% of cases; theincidence is higher in patients presenting withpartial seizures. Tumours are an uncommoncause of childhood epilepsy. Seizures are a com-mon presentation in patients presenting with abrain tumour: approximately 50% of patientspresent with a seizure. There is an inverse rela-tionship between the grade of malignancy of aglioma and the risk of seizure. The incidence ofseizures with meningiomas is approximately50%, 40% with glioblastoma multiforme and 80%with anaplastic astrocytoma.
Investigation of seizures and epilepsy
Investigation of seizures includes:• history of seizures• general and neurological examination• routine (interictal) EEG• CT scan• MRI• video EEG monitoring.
The initial step in investigating a patient pre-senting following an epileptic seizure is to obtaina full history from the patient and a witness ac-count of the event. A history of febrile convul-
sions of infancy in a patient presenting with com-plex partial seizures of temporal lobe origin suggests the diagnosis of MTS. A history of a significant head injury may suggest post-traumatic epilepsy and a strong family history of epilepsy suggests a primary generalizedepilepsy.
The EEG is non-invasive and relatively inex-pensive and is performed as an outpatient. Thetechnique involves the recording of electrical ac-tivity from the surface of the brain by the use ofscalp electrodes. The electrodes are placed atmultiple sites over the scalp, allowing recordingsto be made from multiple anatomical sites at onetime. These patterns of recording sites are knownas montages. The normal adult EEG has a back-ground rhythm of frequency of 8–13 Hz, knownas alpha rhythm. Fast activity of greater than13 Hz is known as beta rhythm and may be seenbifrontally or with drugs such as barbituratesand benzodiazepines. Slow activity is catego-rized as theta rhythm of 4–8 Hz and delta rhythmof less than 4 Hz (Fig. 21.1). The normal adultresting EEG contains only a minimal amount oftheta rhythm and no delta activity. Excess slowwave activity during the resting tracing is abnor-mal and may be generalized, such as in an en-cephalopathy, or focal, as with a structural lesionsuch as a glioma or abscess. The routine EEGcomprises a resting tracing and two provocativetests, hyperventilation and photic stimulation.These provocative tests may induce epileptic ac-tivity and hyperventilation may accentuate afocal abnormality.
The EEG is of particular value in showing:• focal abnormalities suggesting an underlyingfocal structural lesion and suggesting the seizureis partial in type
EPILEPSY AND ITS NEUROSURGICAL ASPECTS 273
Alpha rhythm (8-13 Hz - cycles/sec)
Beta rhythm (>13 Hz)
Theta rhythm (4 - 8 Hz)
Delta rhythm (<4 Hz)
1 sec50 uV
Fig. 21.1 EEG rhythms.
KAY21 12/16/04 8:00 PM Page 273

274 CHAPTER 21
• characteristic 3-Hz spike and wave (Fig. 21.2)of absence seizures and differentiating absenceseizures from complex partial seizures in whichthe EEG may show a focal, usually temporal lobe,abnormality (Fig. 21.3)• interictal bilateral synchronous spike, andwave, spike or polyspike activity in a patient pre-senting with a tonic–clonic seizure, indicating ageneralized epilepsy (Fig. 21.4).
When interpreting EEG findings, it must be re-membered that:
• a normal EEG does not exclude epilepsy• an abnormal EEG does not indicate epilepsy —epilepsy is a clinical diagnosis.
A contrast-enhanced CT scan is indicated in alladult patients presenting with a first seizure. TheCT scan is useful in identifying an acute underly-ing structural abnormality, such as a cerebral in-farct or haemorrhage, tumour or arteriovenousmalformation, and in identifying long-standingbenign, static and focal abnormalities, such ashemiatrophy or encephalomalacia.
Fig. 21.2 Patient presents withabsence seizures. EEG duringhyperventilation shows 3-Hzspike and wave activitybilaterally.
Fig. 21.3 Patient presents withcomplex partial seizures. EEGshows focal temporal lobeabnormality with excess slowwave activity and episodicsharp waves and sharp andslow wave complexes in theleft temporal leads.
KAY21 12/16/04 8:00 PM Page 274

MRI is a sensitive technique for demonstratingtumours and cerebral infarcts, relatively com-mon identifiable structural causes of late-onsetepilepsy. It is able to demonstrate MTS, a com-mon cause of temporal lobe epilepsy, a findingwhich is not seen on CT scanning. In additionMRI may identify a cavernoma, cortical dyspla-sia or low-grade glioma, lesions often not evidenton a CT scan. Although MRI is the investigationof choice, in most centres it is not readily avail-able in the acute setting and hence CT is recom-mended in this context. All patients with chronicepilepsy, in particular late-onset epilepsy andpartial epilepsy, should have an MRI scan
Video EEG monitoring, which involves simul-taneous recording of electroencephalographicdata and clinical events, is of particular value:• in investigating patients in whom the epilepsyis not well controlled and the type of seizure isuncertain• in differentiating non-epileptic attacks, themost common being psychogenic seizures, fromepileptic seizures• as part of the presurgical assessment of pa-tients with complex partial seizures of temporallobe origin prior to temporal lobectomy• as part of the presurgical assessment of pa-tients with extratemporal lobe epilepsy.
Management of epilepsy
Management of the first seizure
A patient presenting with a first seizure shouldbe fully investigated with an EEG and a CT scanor MRI. The role of MRI in first seizure presenta-tion is uncertain but should be performed in pa-tients with partial or focal seizures and/or focalfeatures on EEG. Following a first seizure a deci-sion as to whether or not the patient should betreated with an antiepileptic drug must bemade. Studies of the estimated risk of seizure re-currence in a patient presenting with a singlefirst seizure vary, but approximately 40% of pa-tients who have a first seizure and have a normalCT scan and EEG and no family history ofepilepsy will have a further seizure within a 3-year follow up period. Controversy as towhether or not one should treat a single firstseizure when investigations are normal remains,but most would defer treatment until a furtherseizure occurs. In patients where neuroimagingreveals an epileptogenic lesion and/or EEGepileptic activity, the risk of further seizures ishigh and the patient should be treated withantiepileptic medication.
EPILEPSY AND ITS NEUROSURGICAL ASPECTS 275
Fig. 21.4 Patient presents withtonic–clonic seizures. EEGshows bilateral synchronousspike and wave and polyspikeactivity.
KAY21 12/16/04 8:00 PM Page 275

276 CHAPTER 21
Antiepileptic drugs
Antiepileptic drug therapy is the most importantfacet of treatment of epilepsy. Certain drugs aremore effective in the treatment of one type ofseizure than another and some may aggravate cer-tain seizure types, hence the need for accurate diagnosis of the seizure type. Table 21.4 indicatesmost of the currently available antiepileptic drugsand their relative specificity of action for differenttypes of seizures. Vigabatrin is rarely initiated,due to the side-effect of visual failure. Table 21.5lists the common antiepileptic drugs as well assome of the newer drugs, their daily doses, dosageregimen, common and important side-effects,pharmacokinetics and relative value of plasmaconcentrations. Table 21.6 lists the commonseizure types and antiepileptic drug of choice.
Carbamazepine is the drug of choice in pa-tients with secondarily generalized seizures, asmay occur with a tumour or vascular malforma-tion. Complex partial seizures and simple partialseizures should be treated with carbamazepine.Sodium valproate is the drug of choice in an adultpatient with primary generalized epilepsy pre-senting with a tonic–clonic seizure. In some pa-tients it is not possible to determine whether thetonic–clonic seizure was generalized or partial in
onset. If there are no features to suggest primarygeneralized epilepsy such as generalized spikewave activity on EEG or associated absence ormyoclonic seizures, carbamazepine or valproateis appropriate.
Phenytoin is preferred in patients with post-traumatic epilepsy and postoperative seizures.Ethosuximide is the drug of choice in the treat-ment of absence seizures alone, but patients withboth absence seizures and tonic–clonic seizuresshould be treated with sodium valproate.
If, despite optimal tolerated dosage and an adequate trial of therapy, satisfactory results arenot achieved with one drug, then another shouldbe tried. Although one aims for monotherapy, insome patients better results are achieved with a combination of two drugs. Medication shouldalways be withdrawn gradually, as the suddenwithdrawal of a drug may lead to increasedseizure frequency; this is particularly true for thebarbiturates. In patients in whom multipleseizures have occurred, once an antiepileptic orcombination of antiepileptic drugs is found to beeffective, the medication should be continued forat least 3 years and possibly longer.
Teratogenicity of antiepileptic drugsThere is a well-recognized increased incidence of
Table 21.4 Relative efficacy of antiepileptic drugs for different seizure types.
Generalized epileptic seizures Partial epileptic seizures
Drug Absence Myoclonic Tonic–clonic Simple Complex Secondarily generalized
Carbamazepine + + + +Phenytoin + + + +Valproate + + + ± ± ±Phenobarbitone + + + +Ethosuximide +Clonazepam + + + +Lamotrigine + + + + + +Gabapentin + + + +Topiramate ± + + + + +Tiagabine + + +Levetiracetam + + +Oxcarbazepine + + + +
KAY21 12/16/04 8:00 PM Page 276

fetal malformations in infants born to womenwith epilepsy taking antiepileptic drugs duringpregnancy. How much of this increased inci-dence relates to epilepsy itself, and how much tothe drugs, is uncertain, but the risk is higher inwomen treated with antiepiletic drugs. All theantiepileptic drugs are thought to be teratogenic,but some appear to have a more specific risk thanothers. Phenytoin has been associated with an in-creased risk of congenital heart disease, cleft lipand palate, and valproate and carbamazepinehave been associated with an increased risk of
spina bifida. There is evidence that folate supple-mentation prior to conception and during thefirst 3 months of pregnancy reduces the risk ofspina bifida and should be recommended in allwomen with epilepsy during a pregnancy. Thesafety of the newer antiepileptic drugs is uncertain.
Although patients are always very concernedabout taking antiepileptic drugs during preg-nancy, the patient should be informed that thereis at least a 90% chance they will have a healthychild and they should be advised that the control
EPILEPSY AND ITS NEUROSURGICAL ASPECTS 277
Table 21.5 Antiepileptic drugs, side-effects and relative value of plasma levels.
Drug Average daily dose Regimen Side-effects Plasma levels
Carbamazepine 600 mg 12-hourly Initial drowsiness, rash, Usefulleukopenia, teratogenic
Phenytoin 300 mg Once daily or Gum hypertrophy, Very useful. Note 8–12-hourly hirsutism, acne, change from first
teratogenic order to zero order kinetics, hence small dose increase will result in therapeutic plasma levels
Valproate 1500 mg 8 or 12-hourly Gastrointestinal, weight Little valuegain, tremor, reduce platelet aggregation, hepatotoxicity (rare), teratogenic
Primidone 750 mg 12-hourly Drowsiness, teratogenic Some valuePhenobarbitone 120 mg 12-hourly Drowsiness, teratogenic Some valueLamotrigine* 100–400 mg 12-hourly Drowsiness, rash Probably no valueGabapentin* 1800 mg 6-hourly Minimal Probably no valueTopiramate* 200–400 mg 12-hourly Weight loss, speech Probably no value
disturbance, renal stones, drowsiness
Tiagabine* 30–50 mg 12-hourly Drowsiness Probably no valueLevetiracetam* 1000–2000 mg 12-hourly Drowsiness Probably no valueOxcarbazepine* 600 mg 12-hourly Drowsiness, rash, Probably no value
hyponatraemiaVigabatrin* 2–3 g 12-hourly Visual failure, sedation, No value
depression, rarely psychosis
* Teratogenicity of new antiepileptic drugs is uncertain.
KAY21 12/16/04 8:00 PM Page 277

278 CHAPTER 21
of the epilepsy is of the utmost importance. Therisk of malformations needs to be balancedagainst the risk of seizures to both the patientand the fetus.
Plasma concentrations of antiepileptic drugsPlasma concentrations of all the commonly usedantiepileptic drugs can be measured routinely.The plasma concentrations of an antiepilepticdrug aid the physician in choosing an appro-priate dosage to achieve maximal therapeutic re-sponse and avoid toxicity. Phenytoin plasmaconcentrations are particularly useful, as there isa good correlation between plasma phenytoinconcentrations and therapeutic and toxic effects.Plasma concentrations of carbamazepine andbarbiturates are of some value, but the correla-tion between plasma concentration of valproateand therapeutic benefit is poor (Table 21.5). Plasma concentrations of vigabatrin are not use-ful due to the mechanism of action of the drugand, although plasma concentrations of lamot-rigine and gabapentin can be measured, moststudies have not shown these to be useful.
Management of status epilepticus
Convulsive status epilepticus is defined as recur-rent seizures without recovery of consciousness
between attacks. It occurs in a minority of pa-tients with epilepsy and is more common in pa-tients with an underlying structural cause than inpatients with primary generalized epilepsy. Itmay be the first presentation of epilepsy. Statusepilepticus may be precipitated by withdrawal ofantiepileptic drugs or by intercurrent infection ormay be spontaneous. Non-convulsive statusepilepticus may be generalized (absence status)or focal/partial (complex partial or simple partial status). Convulsive status is a medicalemergency and requires urgent and intensivetreatment. Seizures which are multiple and fre-quent, but not continuous, may herald status andshould be controlled rapidly.
The principles of management of convulsivestatus epilepticus are:• simultaneous protection of airway and termi-nation of seizure activity• prevention of further seizures• identification of cause of seizures.
To stop the seizures use intravenous diazepamand, if this fails, intravenous clonazepam or in-tramuscular midazolam. All patients require ur-gent neuroimaging. In postoperative patients anurgent CT scan must be performed to exclude apostoperative collection, such as an intracerebralhaemorrhage. Maintenance antiepileptic drugtherapy should be introduced or optimized toprevent further seizures.
Surgical treatment of epilepsy
Surgical treatment of epilepsy is indicated if the epilepsy is inadequately controlled byantiepileptic medication and if it can be shownthat there is a focal origin for the seizures in anarea of the brain that can be removed withoutproducing a neurological deficit. Temporal lobec-tomy is the most common surgical procedure inthe management of patients with intractable par-tial epilepsy.
Temporal lobectomy
Assessment of patients prior to temporal lobectomy includes:• history of seizures and seizure semiology
Table 21.6 Type of seizure and antiepileptic drugof choice.
Type of seizure Drug of choice
Tonic-clonic seizure Valproate(primary generalized)
Absence seizure Ethosuximide, valproate
Myoclonic seizures ValproateTonic–clonic seizure Valproate,
(underdetermined if carbamazepinegeneralized or partial)
Complex partial seizure CarbamazepineSimple partial seizure CarbamazepineTonic–clonic seizure Carbamazepine
(secondarily generalized)
KAY21 12/16/04 8:00 PM Page 278

• high-resolution MRI including volumetricanalysis• video EEG recording with surface electrodesand, if necessary, intracranial monitoring• positron emission tomography (PET)• ictal single photon emission computerized tomography (SPECT)• neuropsychology assessment.
Successful surgical treatment depends on ac-curate localization of the seizure focus. Initial as-sessment involves a detailed clinical history fromboth the patient and a witness. Video EEGrecording of seizures is essential to confirm theseizure type and lateralization, which is based onboth the seizure semiology and the site of onset ofthe electrical discharge. Seizures may have fea-tures typical of temporal lobe origin, such as oralautomatisms and psychoparesis. Seizures pre-ceded by an aura of déjà vu, a feeling of fear or arising epigastric sensation are also very sugges-tive of temporal origin. Contralateral limb dysto-nia or limb paresis are reliable lateralizingfeatures. Typically the ictal EEG shows rhythmi-cal sharp activity of approximately 5 Hz in the ipsilateral temporal leads, and postictal focalslowing is also a reliable lateralizing feature.Monitoring initially involves use of surface elec-trodes with or without sphenoidal electrodeswith the aim of recording at least three typicalseizures. If there is doubt as to the site of theseizure onset, intracranial monitoring with depthelectrodes may be used.
In recent years there has been increased em-phasis on the role of neuroimaging, both struc-tural and functional, in identifying the seizurefocus in patients being assessed for epilepsysurgery. Although ictal EEG recordings remainimportant in the localization of the seizure focus,the best results from surgery are achieved in pa-tients in whom a lesion is seen on MRI and inwhom pathology is found in resected tissue. Themost common cause of temporal lobe epilepsy isMTS and in most surgical series this accounts forapproximately 60% of cases. This condition canbe diagnosed on MRI as atrophy of the hip-pocampus seen best on T1-weighted images andas increased signal on T2-weighted images (Fig.21.5). The technique of MRI volumetric analysis
has provided an objective measure of the volumeof the hippocampus, and allows detection of asmall but clinically significant reduction in hippocampal size, and therefore increases ourability to diagnose MTS. Ictal SPECT using 99mTc-bicisate (neurolite) can be extremely useful inidentifying the seizure focus, particularly in pa-tients with normal MRI or extratemporal lobeepilepsy. In temporal lobe epilepsy PET oftenshows hypometabolism of the ipsilateral tempo-ral lobe. This finding is particularly useful in pa-tients in whom MRI is normal. These imagingtechniques have circumvented the need fordepth electrodes in many patients being assessedfor surgery.
EPILEPSY AND ITS NEUROSURGICAL ASPECTS 279
Fig. 21.5 MRI showing atrophy of the hippocampus(a) and increased signal on T2-weighted images (b).
(a)
(b)
KAY21 12/16/04 8:00 PM Page 279

280 CHAPTER 21
All patients being assessed for epilepsysurgery undergo detailed neuropsychologicalevaluation. This provides an assessment of intel-lectual function and allows detection of abnor-malities suggestive of temporal or frontal lobedysfunction. Left hemisphere dominant patientswith a left temporal focus often show verbalmemory deficits, whereas patients with righthippocampal atrophy may demonstrate non-verbal deficits. Hence, these tests may providelateralization of temporal lobe abnormalities. Inaddition, in a patient in whom a temporal lobec-tomy is being contemplated, one needs to be reassured that the contralateral temporal lobefunction is adequate, otherwise an amnestic syn-drome may result. The intracarotid sodium amy-lobarbital test establishes whether or not thecontralateral temporal lobe can sustain memoryand identifies cerebral dominance for language.Functional MRI has circumvented the need forthis test in many patients.
If the clinical history and seizure semiology,electrographic data, imaging and neuropsycho-logical testing are all concordant for localizationand lateralization of the seizure focus, then tem-poral lobectomy has a high chance of success.Most series report an excellent outcome in70–80% of patients.
Callosotomy
The place of callosotomy in the management ofpatients with epilepsy remains unclear. The ratio-nale of the procedure is to prevent rapid spreadof epileptic activity from one hemisphere to theother and in so doing patients may experienceless severe seizures and less injury. The indica-tions for callosotomy are medically intractable
epilepsy with severe and frequent atonic andtonic seizures and the absence of localized resectable pathology.
Hemispherectomy
This procedure is considered in children or ado-lescents with medically intractable epilepsy withhemiparesis and severe unilateral hemispheredamage.
Driving and epilepsy
The management of a patient with a first seizureor epilepsy includes advice regarding the safetyto drive. Each country and state has different regulations and guidelines. Local guidelines should be reviewed and appropriate advice given.
Further readingCommission on Classification and Terminology of
the International League Against Epilepsy (1989)Proposal for revised classification of epilepsies andepileptic syndromes. Epilepsia 30, 389–399.
Engel J Jr (1993) Surgical Treatment of the Epilepsies, 2ndedn. Raven Press, New York.
Jennet B (1975) Epilepsy After Non-Missile Head Injuries,2nd edn. Heinemann, London.
LaRoche SM, Helmers SL (2004) The new antiepilepticdrugs: scientific review. Journal of the American Medical Association 4, 291 (5), 605–614.
North J (1989) Anticonvulsant prophylaxis in neuro-surgery (editorial). British Journal of Neurosurgery 3,425–428.
Shaw MDM, Foy PM (1991) Epilepsy after craniotomyand the place of prophylactic anticonvulsant drugs:discussion paper. Journal of the Royal Society of Medicine 84, 221–223.
KAY21 12/16/04 8:00 PM Page 280

Page numbers in italics refer tofigures and those in bold to tables;but note that figures and tables areonly indicated when they areseparated from relevant textreferences. Index entries are filed inletter-by-letter alphabetical order
acalculia 3accessory nerve 8, 11acoustic neuromas (schwannomas)
101–5aetiology 64, 65bilateral 101, 104clinical presentation 101–2differential diagnosis 102–3investigations 25, 102treatment 103–5
acquired immune deficiencysyndrome see AIDS
acromegaly 114–15, 119ACTH
ectopic production 115, 116secreting pituitary adenomas
112, 115–16, 119serum levels 116
acute stroke see stroke, acuteA-delta fibres 254aerocele, intracranial 51, 52age
meningitis aetiology and 171stroke risk and 141
agnosia, finger 3agraphia 3AIDS 182–3
cerebral lymphoma 83dementia complex 182–3
akinesia 265alcohol consumption, stroke risk 142
alexia 3alpha-fetoprotein 166amaurosis fugax 145amnesia, post-traumatic 42amputees 258amylobarbital test, intracarotid
sodium 280amyloid angiopathy 149–50anaesthesia dolorosa 250, 262analgesic ladder 259–60analgesics
in cancer 259–60in lumbar disc prolapse 188in reflex sympathetic dystrophy
258in subarachnoid haemorrhage
133aneurysms, cerebral see cerebral
aneurysmsangiography
cerebral see cerebralangiography
spinal arteriovenousmalformations 221
angioplasty, percutaneoustransluminal 144–5
ankle jerk 12anosmia 4
in meningioma 96, 97ansa lenticularis 263ansotomy 263anterior cerebral artery
aneurysm 131occlusion, stroke syndrome
146anterior cervical discectomy
201–2, 204anterior cervical spinal cord
syndrome 228
anterior communicating arteryaneurysms 126, 127
anterior interosseous nerve 11syndrome 236–7
anterior spinal artery syndrome228
antibioticsin brain abscess 177CSF penetration 172in epidural abscess 178in head injuries 52, 53in meningitis 172–3in subdural abscess 179
anticoagulationin acute stroke 153in stroke prevention 142, 144,
154anticonvulsant drugs see
antiepileptic drugsantidiuretic hormone, syndrome of
inappropriate secretion(SIADH) 47
antiepileptic drugs 276–8in brain abscess 177in neuropathic pain 260plasma concentrations 277, 278postoperative prophylaxis 273post-traumatic epilepsy 272in status epilepticus 278in subdural empyema 179teratogenicity 276–8
antifibrinolytic agents 132antihypertensive therapy
after subarachnoid haemorrhage133
stroke prevention 141antiplatelet therapy, stroke
prevention 143–4Apert’s syndrome 168
Index
281
KAYIndex 12/16/04 8:00 PM Page 281

282 INDEX
aphonia 3aqueduct stenosis 32arachnoid cysts 158–60
clinical features 158–9radiological investigations 159treatment 159–60
arachnoiditis, intradural 191Argyll–Robertson pupil 6arm pain (brachial neuralgia) 257
in cervical disc prolapse 198in cervical spondylosis 203differential diagnosis 200in thoracic outlet syndrome 240
Arnold–Chiari malformation 160arterial dissection, extracranial and
intracranial 155arteriovenous malformations
(AVMs) 135–8clinical presentation 136haemorrhage 125, 126–7, 136investigations 136, 137management 136–8spinal 220–2see also subarachnoid
haemorrhagearteritis, cerebral 155aspirin
in acute stroke 153in cancer pain 260in stroke prevention 142, 143,
144astrocytomas 66–76
adjuvant therapies 74–6aetiology 65anaplastic 67, 68clinical presentation 68–70grading systems 67–8paediatric cerebellar 87, 88, 91pathology 68pilocytic 67postoperative care 73–4prognosis 74radiation therapy 74radiology 18, 70–2spinal cord 215–16surgery 72–4
ataxia 13brain tumours 79, 80normal-pressure hydrocephalus
37atherosclerosis (atheroma
formation)
cerebral aneurysm risk 130large artery, ischaemic stroke
146–7stroke prevention 142
athetosis 266atlantoaxial dislocation 164atrial fibrillation, stroke prevention
141–2, 154atypical facial pain 251audiometry 8, 102aura 270autonomic deficits, spinal injuries
228autoregulation 28axillary nerve 11axonotmesis 242–3
Babinski response 10back pain
low 185–96in spinal cord compression 207in thoracic disc prolapse 217
Bacteroides 174, 175barbiturates, in head injury 48basal ganglia 263, 264basilar artery aneurysms 130, 131basilar invagination (impression)
163–4Battle’s sign 52benign childhood epilepsy with
centrotemporal spikes 271benign intracranial hypertension
38–9benzyl penicillin 172Bertrand’s procedure 267biceps jerk 12bilirubin, in CSF 16biopsy, stereotactic 73, 84–5birth injuries, brachial plexus 244Bjerrum screen 4–5bladder care, in spinal cord injuries
232blood oxygen level-dependent
imaging (BOLD) 24blood pressure
in acute stroke 153after subarachnoid haemorrhage
133bone metastases 259botulinum toxin injections 252,
267brachial neuralgia see arm pain
brachial plexus 11entrapment neuropathy 240injury 244, 245
brachycephaly 168brachytherapy, interstitial 75–6bradycardia
in head injury 44–6, 57in raised intracranial pressure
29, 30bradykinesia 264–5brain abscess 173–7
bacteriology 174–5diagnosis 175–6histopathology 174management 176–7metastatic 173–4pathogenesis 173–4, 175presenting features 175
brain death 13brain herniation 28, 29
in head injury 41lumbar puncture risks 15
brain injuryin missile injuries 53pathophysiology 40–1primary and secondary 40
brainstemfunction, testing 13gliomas, paediatric 87, 89, 91–2herniation 29
brainstem auditory evokedpotentials 25, 102
brain tumours 64–92aetiology 64–6benign 93–108chromosomal abnormalities 64,
65classification 64, 65incidence 65malignant 67metastatic 80–3neuroepithelial 65, 66–80paediatric 86–92postoperative care 73–4radiology 18, 19, 22, 24, 70–2seizures and 68–9, 70, 76, 271,
273surgery 72–4see also specific types of tumour
breast carcinoma 81Broca’s area 3, 4bromocriptine 120
KAYIndex 12/16/04 8:00 PM Page 282

INDEX 283
Brown-Séquard syndrome 208,212, 228, 229
burn injuries 243burr holes
brain abscess drainage 176–7in extradural haematoma 58, 59subdural abscess drainage 179
calcification, intracranial 18craniopharyngiomas 121gliomas 72, 77, 79
calcium channel blocking agents132–3, 134
callosotomy 280caloric testing 8
in acoustic neuroma 102in head injury 44
cancer pain 259–62neurosurgical procedures 260–2pharmacological agents 259–60
cape-like pattern of sensory loss162, 208, 215
capillary telangiectasia 136CAPRIE trial 143carbamazepine 277
in epilepsy 276in facial pain disorders 249, 251teratogenicity 277
carcinogens, chemical 64–5cardiogenic embolism 147, 155carotid artery
angioplasty/stenting 144–5asymptomatic disease, stroke
risk 142–3dissection 155
carotid endarterectomy (CEA)primary stroke prevention 142–3secondary stroke prevention
144, 154carotid territory
cerebral infarction 146, 151TIAs 145
carpal tunnel 234, 235carpal tunnel syndrome 2, 234–6cauda equina compression
clinical features 208, 209intervertebral disc prolapse 186,
190intramedullary spinal tumours
215cauda equina injuries 228caudate nucleus 263, 264
causalgia 244, 257–8cavernous haemangioma 136, 138cavernous sinus
pituitary tumour invasion 109,112
thrombosis 156cefotaxime 172central angiitis, isolated 155central nervous system infections
22, 170–84classification 170spinal 218–20see also specific syndromes
central pain, in spinal cordcompression 207
central spinal cord syndrome 228–9cerebellar astrocytomas, paediatric
87, 88, 91cerebellar disorders 13cerebellar tonsils, herniation 28, 29cerebellopontine angle
arachnoid cysts 158surgical approaches 103, 104tumours 97, 102–3, 108
cerebellum 263, 264electrical stimulation 266
cerebral abscess see brain abscesscerebral aneurysms 129–35
berry (saccular; congenital) 130fusiform 130giant 127management of unruptured 135multiple 130, 135mycotic 130pathogenesis 130pressure-related signs 127ruptured 125
endovascular procedures134–5
focal neurological signs 126management 130–5rebleeding 132surgical procedures 133–4see also subarachnoid
haemorrhagesurgical anatomy 129–30
cerebral angiography 19–20arteriovenous malformations
136, 137brain tumours 72in head injury 46in meningioma 98, 100
pituitary tumours 117in subarachnoid haemorrhage
129, 138cerebral blood flow (CBF) 28cerebral contusion 40–1cerebral convexity
arachnoid cysts 159meningiomas 94, 95–6
cerebral haemorrhage(haemorrhagic stroke) 140,149–50
acute management 154clinical assessment 151–2differential diagnosis 151lobar 149–50in young adults 154–6see also intracerebral
haematoma/haemorrhage;subarachnoid haemorrhage
cerebral herniation see brainherniation
cerebral infarction (ischaemicstroke) 140, 145–9
anatomical classification 146borderzone or watershed 147cardiogenic embolism 147clinical assessment 151cortical 146, 147, 151differential diagnosis 151haemorrhagic 140lacunar see lacunar infarctionlarge artery atherosclerosis
146–7Oxfordshire classification 148–9pathogenic classification
(TOAST) 146–8subcortical (deep) 146, 148, 151thrombolytic therapy 151in young adults 154–6
cerebral lymphoma 83–5cerebral metastases 80–3
clinical presentation 81–2prognosis 82radiology 82, 83treatment 82
cerebral oedema (swelling)acute stroke 153after tumour excision 73, 74brain abscess 175, 176brain tumours 70, 82, 98head injury 41
management 46, 47, 48–9
KAYIndex 12/16/04 8:00 PM Page 283

284 INDEX
cerebral palsy 265–6cerebral perfusion pressure (CPP)
28, 49cerebral salt wasting 47cerebral vasculitis 155cerebral venous thrombosis 156cerebritis 174, 175–6cerebrospinal fluid (CSF) 14–18
abnormalities 17cells 14, 15, 16, 17circulation 14, 31drainage, to reduce intracranial
pressure 48electrophoresis 17–18examination 16–17gradients along axis 15in meningitis 171–2microorganism growth/survival
170normal constituents 15pressure 15production rate 15, 31sampling methods 14–16shunts see shunts, CSFvolume 14, 15, 31
cerebrospinal fluid (CSF)otorrhoea, traumatic 52
cerebrospinal fluid (CSF)rhinorrhoea
diagnosis 52spontaneous 38, 124traumatic 51–2
cerebrovascular accident (CVA) seestroke
cerebrum, somatotopicorganization 4
cervical disc prolapse 197–202anatomy and pathology 197–8clinical features 198–200differential diagnosis 200investigations 200, 201, 202management 200spinal cord compression 216–17surgical treatment 200–2
cervical foraminotomy 200–1, 204cervical myelopathy 222–4
in cervical spondylosis 203, 222clinical features 222–3radiological investigations 223treatment 223–4
cervical rami, selective peripheraldenervation 267
cervical rib 240cervical roots, intradural section of
anterior upper 267cervical spine
assessment, in head injury 46disorders 197–205X-rays see under spinal X-rays
cervical spine injuries 225–6compression 225–6flexion and flexion–rotation 225,
226hyperextension 226, 228–9management 229–32neurological impairments 227–9special types 232–3
cervical spondylosis 197, 200,202–4
cervical myelopathy 203, 222clinical features 203differential diagnosis 204management 204pathology 202–3radiology 203, 204
cervical traction 230–1C fibres 254Chamberlain’s line 164Chance fractures 227chemical shift spectroscopy 22chemonucleolysis, prolapsed
lumbar disc 189chemotherapy
cerebral lymphoma 85gliomas 75, 78paediatric brain tumours 90–1,
92Cheyne–Stokes breathing, in head
injury 44, 57Chiari malformations 160–3
aetiology 161clinical presentation 161–2radiological investigations 162type I 160type II (Arnold–Chiari) 160type III 160
children see paediatric patientschloride, CSF 15, 17chlorpromazine 47cholesterol, serum 142chorda tympani 8chordomas 86chorea 265–6choriocarcinoma 82
chromosomal abnormalities, braintumours 64, 65, 93
chronic pain syndromes 258–9chymopapain 189circumduction 12cisternal puncture 14cisternography, radio-isotope 24,
37clasp knife spasticity 9claw hand 237–8clonazepam 276clonus 9clopidogrel 143, 144cochlear nerve 8codeine phosphate 260cog wheel rigidity 9, 264colloid cysts, 3rd ventricle 106, 107coma, in head injury 43common peroneal nerve 11
palsy 241complex regional pain syndrome
(CPRS; causalgia) 244,257–8
compliance (dV/dP), intracranial27–8
compression ischaemia, peripheralnerves 243
computed tomography (CT)18–19
acoustic neuroma 102acute stroke 149, 150, 151, 152arachnoid cysts 159arteriovenous malformations
136, 137brain abscess 175–6, 177brain tumours 18, 70, 71, 80cerebral lymphoma 84cervical disc prolapse 200, 202craniopharyngioma 121epidermoid/dermoid cysts 107,
108head injury 46, 47, 52hydrocephalus 32, 33, 37intracranial haematomas 58, 59,
60, 61intrathecal contrast
(myelography) 19intravenous contrast medium
18–19lumbar canal stenosis 192meningioma 97, 98, 99metastatic brain tumours 82
KAYIndex 12/16/04 8:00 PM Page 284

INDEX 285
paediatric brain tumours 87, 88,91
pituitary tumours 116–17sciatica 190, 191seizures 274spinal cord compression 209spinal tumours 213, 215subarachnoid haemorrhage
128–9vs MRI 22
concussion 41–2spinal cord 229
confabulation 3confrontation testing, visual fields
4, 5coning 29conjugate ocular movements 7conscious state
assessment 2, 43, 44brain tumours 69extradural haematoma 57, 58head injury 43, 46meningitis 171observation chart 45seizures 269–70subarachnoid haemorrhage
125–6see also drowsiness
contre-coup injury 40–1conus medullaris lesions 208, 209convexity see cerebral convexitycoordination, assessment 12cordotomy, spinal 260–1coronal synostosis 168corpus striatum 263corticospinal tract lesions 9, 10corticosteroids
(glucocorticosteroids)in brain abscess 177brain tumours 72, 82in carpal tunnel syndrome 236in cerebral lymphoma 85in head injury 48in lumbar disc prolapse 188–9in malignant cord compression
210, 211–12in meningioma 98paediatric brain tumours 89postoperative 74in spinal cord injuries 231in tuberculous meningitis
179–80
corticotrophin see ACTHcortisol excess 115, 116cortisone acetate 120Costen’s syndrome 251cranial nerves
examination 4–8injuries, in head injury 42, 53section, for cancer pain 267
craniectomy, in extraduralhaematoma 58–9
craniopharyngioma 87, 120–2craniosynostosis 167–9craniotomy
brain tumour surgery 72–3decompressive, in head injury
48–9in extradural haematoma 58
craniovertebral junctionabnormalities 163–4
Crouzon’s syndrome 168cryptococcosis (Cryptococcus
neoformans) 180–1AIDS-related 182intracerebral granulomas
180–1meningitis 171, 180meningoencephalitis 180
CSF see cerebrospinal fluidCT see computed tomographycubital fossa, median nerve
entrapment 236cubital tunnel, ulnar nerve
entrapment 237–8Cushing reflex (response) 29, 30
in head injury 44–6, 57Cushing’s disease 112, 115–16Cushing’s syndrome 115
Dandy–Walker cyst 32, 164–5deafferentation pain 261deafness see hearing lossdecerebrate posture 44decorticate posture 44deep brain stimulation (DBS)
261–2, 265dementia 2
AIDS-related 182–3in chronic subdural haematoma
61in normal-pressure
hydrocephalus 37dentate nucleus 263, 264
dentatotomy 263, 266dermatomes
lower limb 188trunk 208upper limb 199
dermoid cysts 106–8Descartes, René 256developmental abnormalities
158–69dexamethasone suppression test
116diabetes insipidus 29
after pituitary tumour resection119–20
in craniopharyngioma 121in head injury 47pineal tumours 80
diabetes mellitus, strokeprevention 142
diastematomyelia 167, 168digital subtraction angiography
19–20diplopia 7
paediatric brain tumours 87raised intracranial pressure 30
dipyramidole 143, 144disability, after head injury 54,
55disc, intervertebral see
intervertebral discdiscectomy
anterior cervical 201–2, 204lumbar 190
diuretic therapy, in raisedintracranial pressure 48
dorsal rhizotomy, selective 266dorsal root entry zone (DREZ)
procedure 245, 258driving, and epilepsy 280drowsiness 2
brain tumours 69in chronic subdural haematoma
61in head injury 43, 46, 57in raised intracranial pressure
30drug use, illicit 155Duchenne’s muscular dystrophy 9dura
repair, in head injuries 50, 52tears, in head injuries 51, 52
Duret haemorrhages 29
KAYIndex 12/16/04 8:00 PM Page 285

286 INDEX
dysarthria 3ataxic 3rigid 3spastic 3
dysphasia 3brain tumours 70expressive 3nominal 3receptive 3
dysphonia 3dystonia 266dystrophia myotonica 9
ear infection, middle 174, 175Echinococcus granulosus 181echocardiography, in acute stroke
148, 152echoplanar imaging (EPI) 24echo time (TE) 22Edinger–Westphal nucleus 6eighth nerve see vestibulocochlear
nerveelastance, intracranial 27–8electrical injuries 243electroencephalography (EEG)
24–5, 273–4, 275video monitoring 275, 279
electrolyte balanceafter subarachnoid haemorrhage
133in head injury 47
electromyography (EMG) 25,235–6
electrophoresis, CSF 17–18embolism
cardiogenic 147, 155paradoxical 155
emergency department, urgentstroke assessment 152
empty sella syndrome 122–4endocrine disturbances
arachnoid cysts 159craniopharyngioma 121pineal tumours 80pituitary tumours 112–16,
119endoneurium 241endovascular procedures
arteriovenous malformations136
benign intracranial hypertension39
ruptured cerebral aneurysms134–5
secondary stroke prevention144–5
enteral feeding, in head injury 47–8entrapment neuropathies 234–41eosinophils, in CSF 16, 17ependymomas 78–9
classification 78paediatric 87, 89, 91posterior fossa 79spinal cord 215, 216supratentorial 79
epidermoid cysts 106–8epidural abscess 177–8
spinal 218–19epidural blood patch 16epilepsy 269–80
arteriovenous malformations136
brain tumours and see underbrain tumours
classification 270–1driving and 280generalized 271investigations 24–5, 273–5management 275–8in meningioma 95partial 270–1postoperative 272–3post-traumatic 50, 51, 53, 271–2surgical treatment 278–80see also seizures
epineurium 241Erb’s palsy 244erythrocyte sedimentation rate
(ESR) 188essential tremor 265esthesioneuroblastoma 85–6ethmoid sinusitis 174ethosuximide 276European Carotid Surgery Trial
(ECST) 144evoked potentials 25–6extradural haematoma 56–9
clinical presentation 56–8distribution 56, 57radiological investigations 58treatment 58–9
extraocular muscles 6–7extrapyramidal system 263, 264
lesions 9, 13, 263
eyelids, position 5eye movements see ocular
movementseyes, skew deviation 44
facelower motor neurone weakness
8sensation 7upper motor neurone weakness
7–8facet joint arthritis 195facial nerve (7th nerve)
in acoustic neuroma 101, 102,103, 104–5
examination 7–8palsy, traumatic 42, 53
facial pain 248–53, 257atypical 251
facioscapulohumeral dystrophy 9falcine meningiomas 94, 95, 100false localizing signs 30, 87fasciculation 10, 25femoral nerve 11fetal tissue transplants 265fibrillation potentials 25fibromuscular dysplasia 155–6fifth nerve see trigeminal nervefilum terminale
ependymomas 215, 216hypertrophic 167
finger agnosia 3finger drop 239finger–nose test 12flexor finger jerk 12fluid-attenuated inversion
recovery (FLAIR) 22fluid management
in acute stroke 153after subarachnoid haemorrhage
133in chronic subdural haematoma
62in head injury 47
focal neurological signscerebral metastases 81chronic subdural haematoma 61extradural haematoma 57gliomas/astrocytomas 69–70head injury 44meningiomas 95paediatric brain tumours 87
KAYIndex 12/16/04 8:00 PM Page 286

INDEX 287
pineal tumours 80subarachnoid haemorrhage
126–7folate supplementation 277fontanelles
closure times 167in raised intracranial pressure
30foot drop 12, 187, 241foramen magnum, brain
herniation into 28, 29foramen ovale, patent (PFO) 155forearm, wasting 9Forel’s field 263, 264
neurosurgical lesions 263, 266Foster Kennedy syndrome 96, 97fourth cranial nerve, examination
5–7fractures
peripheral nerve injuries 243see also skull fractures; spinal
injuriesFrazier’s operation 250Froment’s sign 238frontal bossing 168frontal lobe
aneurysm rupture into 126symptoms, meningioma 95, 97tumours 69, 70, 84
frontal sinusitis 174, 175, 178frusemide (furosemide) 48, 58functional magnetic resonance
imaging (fMRI) 24fundal examination 5, 127–8
gabapentin 276, 277gadolinium contrast medium 22gait 12–13
ataxic 13high stepping 12–13hysterical 13in normal-pressure
hydrocephalus 37tight hamstring 195, 196waddling 13
gamma globulins (IgG), CSF 15,17–18
gastrointestinal complications,spinal cord injuries 232
gate control theory 256gender differences, stroke risk 141gene therapy, brain tumours 76
geniculate neuralgia 251germinoma, pineal 80, 81Gerstmann’s syndrome 3giant cell arteritis 155giant cerebral aneurysms 127gigantism 115girdle pain 207, 217Glasgow coma scale 43, 44, 45glioblastoma multiforme 67
aetiology 65clinical presentation 69pathology 68, 69prognosis 74radiology 70, 71
gliomas 66–79adjuvant therapies 74–6butterfly 69, 70chemotherapy 75classification 67–8clinical presentation 68–70hypothalamic 119management 72–6in NF1–64paediatric brainstem 87, 89, 91–2pathology 68, 69prognosis 74radiation therapy 74, 75–6radiology 70–2recurrent cerebral 77–8seizures 68–9, 70, 271surgery 72–4see also astrocytomas;
ependymomas;oligodendrogliomas
globus pallidus 263, 264glossopharyngeal nerve 8glossopharyngeal neuralgia 250–1glucocorticosteroids see
corticosteroidsglucose, CSF 14, 15, 17
in meningitis 171glycoprotein IIb/IIIa receptor
inhibitors 144gonadotroph cell adenoma 112Gram stain, CSF 171granulocytes, in CSF 16granulomas, cryptococcal
intracerebral 180–1growth hormone 111
secreting pituitary adenomas111, 114–15, 119
serum 116
Guyon’s canal, ulnar nervecompression 238–9
haemangioblastomas 105aetiology 65, 105radiology 105, 106
haemangioma, cavernous 136, 138
haemangiopericytoma, meningeal101
Haemophilus influenzae meningitis173
haemorrhagic infarction 140hand, wasting of small muscles 9hangman’s fracture 233headache 257
arteriovenous malformations136
benign intracranial hypertension38
brain tumours 69chronic 258, 259extradural haematoma 57history taking 2paediatric brain tumours 87pituitary tumours 112, 115post lumbar puncture 16raised intracranial pressure 30sentinel 125subarachnoid haemorrhage 125,
128head injuries 40–55
associated injuries 42, 49–53brain abscess complicating 174,
175clinical assessment 43–6epilepsy after see epilepsy, post-
traumaticfurther management 46–53initial management 42–6intracranial haematomas see
under intracranialhaematoma/haemorrhage
in meningioma aetiology 93minor 46–7missile injuries 53–4non-accidental 54, 62pathophysiology 40–2radiological investigations 18,
46rehabilitation 54–5severe 47–9
KAYIndex 12/16/04 8:00 PM Page 287

288 INDEX
head tilt, paediatric brain tumours87
hearingassessment 8conservation, acoustic neuroma
104hearing loss (deafness)
in acoustic neuroma 102, 103,104
assessment 8post-traumatic 42
heart disease, congenital 174heel–knee test 12hemianopia
altitudinous 5bitemporal 5, 6, 112homonymous 5, 6
hemiballismus 266hemifacial spasm 251–2hemiparesis
in arteriovenous malformations136
in cerebral herniation 29in chronic subdural haematoma
61in extradural haematoma 57in head injury 44
hemiplegia 2hemispherectomy 280heparin 153, 229herpes simplex encephalitis 182,
183herpes zoster, ophthalmic 155, 251history, neurological 1–2HMG-CoA reductase inhibitors
142Hodgkin’s disease, intracerebral
83, 84Holmes–Adie pupil 6Horner’s syndrome 5, 6, 244hospital arrival times, acute stroke
150human immunodeficiency virus
(HIV) 182–3Hunt and Hess subarachnoid
haemorrhage gradingsystem 128
hydatid disease (cysts) 181–2hydrocephalus 31–8
acute-onset adult 33arachnoid cysts 158–9arrested 33–4
causes 31–2communicating 31, 32ependymomas 79gradual-onset adult 33infantile 32meningitis 173normal pressure 36–8obstructive 31–2paediatric brain tumours 87,
88pineal tumours 80pituitary tumours 109post-traumatic 41presenting features 32–3radio-isotope cisternography
24, 37radiological investigation 33,
34subarachnoid haemorrhage 128treatment 33–6
hydrocortisone 119hydromyelia 161, 162–3hyperbaric oxygen 48hypercholesterolaemia 142hypercoagulability states 156hypernatraemia 47hyperostosis, in meningioma 96,
97, 98hyperprolactinaemia 111, 112, 116hypertension
in acute stroke 153cerebral aneurysms and 130in head injury 44–6in raised intracranial pressure
30stroke risk 141, 149
hyperthermia, for brain tumours76
hypervolaemic hypertensivetherapy, cerebral vasospasm132–3, 134
hypoglossal nerve, assessment 8hyponatraemia 47, 62hypopituitarism 113, 120hypotension, in spinal injuries
228, 229hypothalamus
compression by pituitarytumours 109, 110, 113
gliomas 119hypothermia, in head injury 48hypothyroidism 113
IgG (gamma globulin), CSF 15,17–18
immunosuppressive therapy,cerebral lymphoma and 83
immunotherapy, brain tumours 76infants
bacterial meningitis 171, 172chronic subdural haematoma
54, 62hydrocephalus 32non-accidental head injury 54, 62raised intracranial pressure 30see also paediatric patients
infarction, cerebral see cerebralinfarction
infectionspost lumbar puncture 15post-traumatic 47, 52shunt 35–6, 173see also central nervous system
infectionsinferior gluteal nerve 11infertility 113–14injection injuries, peripheral nerves
243inspection, general 8insulin-like growth factor I (IGF-I)
116interference pattern,
electromyography 25interleukin-2-stimulated
lymphocytes 76internal capsule (IC) 12, 261internal carotid artery
aneurysms 129–30, 131giant 127
asymptomatic stenosis 142–3ligation 134occlusion, stroke syndrome 146
International Stroke Trial (IST) 153International Study of Unruptured
Intracranial Aneurysms(ISUIA) 135
interventional radiology seeendovascular procedures
intervertebral discdegeneration 202prolapse
cervical see cervical discprolapse
lumbar see lumbar discprolapse
KAYIndex 12/16/04 8:00 PM Page 288

INDEX 289
spinal cord compression216–18
thoracic 217intracarotid sodium amylobarbital
test 280intracerebral
haematoma/haemorrhage(ICH)
after shunt insertion 36clinical assessment 151–2primary (non-traumatic) 149–50in subarachnoid haemorrhage
126, 127traumatic 62–3
intracranial contents 27causes of increased volume 27volume 28
intracranial haematoma/haemorrhage
after shunt insertion 36after tumour excision 73metastatic brain tumours 82perinatal 32traumatic 41, 56–63
classification 56management 47, 50
see also specific typesintracranial hypertension, benign
38–9intracranial pressure
measurement 30–1in head injury 48in normal-pressure
hydrocephalus 37normal 27raised see raised intracranial
pressurevolume relationship 27–8waves 30–1
intracranial tuberculoma 180intracranial tumours see brain
tumoursinvestigations 14–26
jaundice 16JC virus 65Jefferson’s fracture 232–3
Kernohan grading system forastrocytomas 67
Klippel–Feil syndrome 164Klumpke’s paralysis 244
knee jerk 12Koerber–Salius–Elschnig
syndrome 80Korsakoff’s psychosis 2–3
lacerationsperipheral nerves 243scalp 42, 49
lacunar infarction 146, 147–8, 151
lambdoid synostosis 168laminectomy
cervical 224lumbar 190, 192, 196in malignant cord compression
210lamotrigine 276, 277large artery atherosclerosis,
ischaemic stroke 146–7Lasegue’s test 186lateral cutaneous nerve of thigh
entrapment 241lateral medullary syndrome 146,
155lateral popliteal nerve palsy 241lateral recess stenosis 185, 192l-dopa 265lead pipe rigidity 9, 264leg see lower limbLennox–Gastaut syndrome 271lenticular fasciculus 263lentiform nucleus 263leptomeningeal metastases 82–3leukotomy 261levator palpebrae superioris
paralysis 5levetiracetam 276, 277Lhermitte’s sign 207limbic system 256limbs
care, in spinal cord injuries232
examination 8–13in head injury 44paresis, brain tumours 69see also lower limb; upper limb
lipomas, intraspinal 167lipomyelomeningocele 166–7Lissauer’s tract 254, 255Listeria meningitis 173loss of heterozygosity (LOH), brain
tumours 65
low back pain 185–92acute sudden-onset 193–4chronic or recurrent 194without leg pain 192–4
lower limb (leg)entrapment neuropathies 240–1muscle wasting 9, 187nerve and major spinal root
supply 11pain 185–96, 257segmental innervation 187,
188lower motor neurone lesions
signs 8, 9, 10in spinal cord compression 208in spinal injuries 228, 232
lumbar canal stenosis 185, 191–2,193
lumbar disc prolapse 185–6central 189clinical features 186–8conservative treatment 188–9indications for surgery 189investigations 189–90operative procedures 190postoperative mobilization
190–1prognosis after surgery 191
lumbar puncture 14–16complications 15–16indications 14–15in meningitis 171–2in spinal epidural abscess 219in subarachnoid haemorrhage
16, 129technique 15
lumbar spine injuries seethoracolumbar spineinjuries
lumbar spondylosis 194lumboperitoneal shunt 36, 39lumbosacral nerve root
compression 185, 186–8lung carcinoma 81lupus anticoagulant 156lymphokine activated killer (LAK)
cells 76lymphoma, cerebral 83–5
magnetic resonance angiography(MRA) 22
in acute stroke 148, 152
KAYIndex 12/16/04 8:00 PM Page 289

290 INDEX
magnetic resonance imaging (MRI)21–4
acoustic neuromas 102acute stroke 147, 148, 151, 152brain abscess 175–6brain tumours 22, 71–2cerebral lymphoma 84cervical disc prolapse 200, 201,
217cervical myelopathy 223Chiari
malformation/syringomyelia 162, 163
craniopharyngioma 121, 122epidermoid/dermoid cysts 107,
108epilepsy 275, 279functional (fMRI) 24herpes simplex encephalitis 182,
183hydrocephalus 33, 34, 37indications 22–4lumbar canal stenosis 192, 193meningioma 97, 98, 99, 100metastatic brain tumours 82,
83paediatric brain tumours 87, 88,
89, 90, 91pineal tumours 80, 81pituitary tumours 117, 118sciatica 190, 191spinal cord compression 209,
212spinal epidural abscess 219spinal tumours 213, 214, 215thoracic disc prolapse 217, 218
magnetic resonance spectroscopy(MRS) 22, 72
magnetic susceptibility, tissue 21malignant tumours
brain 67pain management 259–60peripheral nerves 247spinal cord compression 210–12see also cerebral metastases
manipulation, spinal 188, 200mannitol 48, 58mastoiditis 174, 175, 178maxillary sinusitis 174McGregor’s line 164medial epicondylectomy 238median nerve 11
median nerve entrapmentscarpal tunnel 234–6cubital fossa 236supracondylar process 237
Medical Research Councilclassification of power 10,12
medulloblastoma 88, 90–1chromosomal abnormalities 65presenting features 87, 90
melanoma, malignant 81, 82memory, assessment 2–3MEN1 (multiple endocrine
neoplasia type 1) 65, 120meningeal carcinomatosis 82–3meningeal haemangiopericytoma
101meningiomas 93–101
aetiology 93clinical presentation 95–8, 273convexity 94, 95–6intracranial positions 93–4olfactory groove 94, 97parasagittal 94, 95, 99, 100pathology 94–5posterior fossa 94, 97–8, 99postoperative care 101preoperative management 98–9radiology 18, 98, 99, 100recurrence 101sphenoidal ridge 94, 96–7spinal 213–15suprasellar 94, 97, 98, 119treatment 99–101ventricular 94, 97, 98
meningismin bacterial meningitis 171in subarachnoid haemorrhage
126meningitis 170–3
bacterial 170–3clinical presentation 170–1complications 173diagnosis 171–2postsurgical 173treatment 172–3
Cryptococcus neoformans 171, 180differential diagnosis 172hospital-acquired 173post-traumatic 52tuberculous 179–80viral 170
meningocele 165, 167meningococcal meningitis 171,
172–3meningoencephalitis, cryptococcal
180mental state examination 2–3meralgia paraesthetica 241mesial temporal sclerosis (MTS)
271, 273, 275, 279metastases
brain see cerebral metastasesleptomeningeal 82–3spinal 210–12
methaemoglobin, in CSF 16methotrexate 85metopic synostosis 168metronidazole 75microvascular compression theory
248, 251–2, 267microvascular decompression
procedures 250, 251, 252middle cerebral artery
aneurysms 126, 130, 131, 135occlusion, stroke syndromes 146
migraine, causing stroke 154miosis 6misonidazole 75missile injuries
head 53–4peripheral nerves 243
mitral valve prolapse 155Monro–Kellie doctrine 27morphine 260
subarachnoid administration262
Morton’s neuroma 247motor cortex 4motor impairment
in spinal cord compression207–8
in spinal injuries 228motor unit potentials 25movement disorders 263–8
anatomical substrate 263, 264involuntary 264–7in reflex sympathetic dystrophy
257moya-moya disease 156MRI see magnetic resonance
imagingmultiple endocrine neoplasia type
1 (MEN1) 65, 120
KAYIndex 12/16/04 8:00 PM Page 290

INDEX 291
multiple sclerosisCSF gamma globulins 17–18evoked potentials 25trigeminal neuralgia 248, 249
muscleelectromyography studies 25nerve and root supply 11power 10, 12tone 9wasting 9weakness see weakness
muscular dystrophies 9musculocutaneous nerve 11mutism 3Mycobacterium tuberculosis 171,
179, 219mydriasis (pupillary dilatation) 6,
43myelography 20–1
lumbar 189–90, 192, 193spinal cord compression 209,
210, 211spinal tumours 214
myelomalacia, cervical 223, 224myelomeningocele 165–6
Chiari II malformation 160, 161hydrocephalus 32
myelopathycervical see cervical myelopathycomplete transverse 227–8
myopathy 25myotomy, in spasmodic torticollis
267myotonia 9myxoedema 10
narcotic analgesics see opiateanalgesics
NASCET (North AmericanSymptomatic CarotidEndarterectomy Trial) 144
nasogastric aspiration, in spinalcord injuries 232
nausea and vomitingbrain tumours 69paediatric brain tumours 87raised intracranial pressure 30
neck painin cervical disc prolapse 198in cervical myelopathy 222in cervical spondylosis 203, 204differential diagnosis 204
neck stiffnesspaediatric brain tumours 87in subarachnoid haemorrhage
128Nelson–Salassa syndrome 115–16neonates, bacterial meningitis 171,
172nerve conduction studies 25, 238nerve injuries see peripheral nerve
injuriesnerve section, for pain control
260nerve sheath fibrosarcoma 247nerve sheath tumours 245neural tube disorders 166
see also spinal dysraphismneurapraxia 242, 243neurocysticercosis 183neurofibromas 246–7
intraneural 246–7peripheral 64plexiform 246–7spinal 212–13
neurofibromatosis type 1 (NF1)245
aetiology 64, 65diagnostic criteria 66peripheral neurofibromas 246–7
neurofibromatosis type 2 (NF2) 93,101
aetiology 64, 65diagnostic criteria 66
neurological assessment 1–13neurological examination 2–13
in head injury 43–6neurological history 1–2neurological observations, in head
injury 45, 46neuromas
in continuity 247Morton’s 247traumatic 242, 245, 247
neuronal tumours 245neuropathic pain, deep brain
stimulation 261neuropathy, nerve conduction
studies/electromyography25
neuroprotective therapy, in acutestroke 153–4
neuropsychological evaluation, inepilepsy 280
neurotmesis 242NF see neurofibromatosisnimodipine 132–3nitrosourea 75, 78N-methyl d-aspartate (NMDA)
receptors 153nociceptive pain, deep brain
stimulation 261non-accidental head injury 54,
62normal-pressure hydrocephalus
36–8nucleus pulposus herniation
185–6, 188null cell pituitary adenomas 112,
116nutrition, in head injury 47–8nystagmus 7
Chiari malformation 161–2downbeat 7, 162jerk 7paediatric brain tumours 87post-traumatic 42
obesitybenign intracranial hypertension
38, 39Cushing’s disease 115meralgia paraesthetica 241
obturator nerve 11ocular bobbing 44ocular movements 6–7
conjugate, impaired 7disorders 7in head injury 43–4in pituitary tumours 112
oculocephalic response 43–4odontoid process fractures 233oestrogen receptors, meningiomas
93olfactory groove meningiomas 94,
97olfactory nerve
examination 4traumatic injuries 42
oligoclonal bands 17–18oligodendrogliomas 76–7
aetiology 65radiology 18, 77
oncocytomas 112oncogenes 66ophthalmoscopy 5
KAYIndex 12/16/04 8:00 PM Page 291

292 INDEX
opiate (narcotic) analgesics 259,260
subarachnoid administration262
optic atrophy 5optic chiasm
compression by pituitarytumours 109, 112, 114
lesions 5, 6optic nerve
examination 4–5glioma, in NF1–64lesions 5, 6sheath decompression 39traumatic injury 42
optic tract, lesions 5, 6oral contraceptive pill, stroke risk
154–5osteomyelitis
cranial vault 178vertebral body 218
osteophytesin cervical spondylosis 202, 203,
204in lumbar canal stenosis 192
otitis media 174, 175oxcarbazepine 276, 277oxycodone hydrochloride 260oxygen, hyperbaric 48oxyhaemoglobin, in CSF 16
paediatric patientsbacterial meningitis 171, 172brain tumours 86–92craniopharyngioma 120developmental abnormalities
158–69spondylolisthesis 195–6subarachnoid haemorrhage 125,
135–6vein of Galen malformation 138see also infants
pain 254–62after nerve injuries 244–5benign non-specific (chronic)
syndromes 258–9benign specific syndromes
257–8cancer 259–62carpal tunnel syndrome 235cognitive–evaluative dimension
256mechanisms 254–6
motivational–affectivedimension 255–6
neurosurgical techniques 260–2pathways 10–12, 254–5reflex sympathetic dystrophy
257sensation testing 10–12sensory–discriminative
dimension 254–5spinal cord compression 207theories 256see also specific sites of pain
palilalia 3pallidotomy 263, 265Pancoast’s tumour 200papilloedema 5
in benign intracranialhypertension 38, 39
in craniopharyngioma 121in meningioma 96in paediatric brain tumours 87in raised intracranial pressure
30in subarachnoid haemorrhage
127–8paracetamol 260paralysis, in spinal injuries 228paranasal sinuses
traumatic fistulae 51tumours 85–6
paranasal sinusitisbrain abscess complicating 174,
175subdural abscess complicating
178paraplegia
management 232in spinal cord compression 207in spinal injuries 228
parasagittal meningiomas 94, 95,99, 100
Parinaud’s syndrome 80Parkinson’s disease 264–5
clinical features 13, 264–5management 265
pars interarticularis, defects 194,195
patent foramen ovale (PFO) 155penetrating injuries
head 40, 53–4spinal cord 231
penicillin 172, 177pentobarbitone 48
percutaneous thermocoagulation,in trigeminal neuralgia249–50
periaqueductal grey (PAG) 255perimetry 4–5perineurium 241periorbital haematomas 51peripheral nerve injuries 241–5
causes 243classification 242–3management 243–4pain problems after 244–5
peripheral nervesanatomy 241–2entrapments 234–41
peripheral nerve tumours 245–7benign 245–7malignant 247non-neoplastic 247
peripheries, examination 8–13periventricular grey (PVG) 255peroneal muscular atrophy 9phantom limb pain 244–5, 258phenobarbitone 276, 277phenytoin 273, 276, 277
plasma concentrations 278teratogenicity 277
photodynamic therapy 76physical activity, stroke prevention
142physiotherapy, after head injury
54pineal tumours 79–80, 81pinprick testing 10–12pisohamate hiatus, ulnar nerve
compression 238pituitary apoplexy 113, 117pituitary carcinoma 112pituitary gland, anatomy 119, 120pituitary tumours (adenomas)
109–24aetiology 65classification 109, 120clinical presentation 112–16differential diagnosis 119functional types 110–12laboratory investigations 116macroadenomas 119, 120microadenomas 119null cell adenomas 112, 116pathology 109–10radiological investigations
116–17, 118
KAYIndex 12/16/04 8:00 PM Page 292

INDEX 293
transsphenoidal resection 119,120
treatment 119–20plantar reflex 10platybasia 164pneumococcal meningitis 172polycythaemia, stroke risk 142polymorphonuclear cells, CSF 16,
17pons
infarction, ventral 146pain pathways 255
population attributable risk 141position sensation 10–12positron emission tomography
(PET) 24, 279posterior cerebral artery occlusion,
stroke syndrome 146posterior column syndrome 228posterior communicating artery
aneurysms 127, 130, 131posterior fossa
craniotomy, in trigeminalneuralgia 250
decompression, Chiarimalformation 163
posterior fossa tumoursdermoid cysts 108ependymomas 79meningiomas 94, 97–8, 99paediatric 87–90
posterior inferior cerebellar artery aneurysms 130, 131
posterior interosseous nerve 11entrapment 239
posterior tibial nerve, entrapmentin tarsal tunnel 241
postherpetic neuralgia 251posture 8
after subarachnoid haemorrhage133
decerebrate 44decorticate 44in thoracolumbar spine injuries
231Pott’s disease 220Pott’s puffy tumour 178power, muscle 10, 12precentral gyrus 4pregnancy, antiepileptic drugs in
276–8premature infants 32
primidone 277primitive neuroectodermal
tumours (PNETs) 87infratentorial see
medulloblastomaprogesterone receptors,
meningiomas 93prolactin 110–11, 116prolactin-inhibiting factor 111prolactinoma (prolactin cell
adenoma) 110–11, 119clinical features 113–14laboratory investigations 116treatment 119, 120
proprioception, testing 10–12proptosis, in meningioma 96, 97protein, CSF 15, 17
in meningitis 171proximal limb girdle dystrophy 9psammoma bodies 95pseudostroke 150–1pseudotumour cerebri (benign
intracranial hypertension)38–9
ptosis 5puberty, precocious 80pulse repetition time (TR) 21–2pupils
constricted 6dilated (mydriatic) 6, 43examination 5–6in head injury 43myotonic 6in posterior communicating
artery aneurysm 127reaction to light 5–6, 43
putamen 263, 264pyrexia, in head injury 46, 47
quadrigeminal cistern, arachnoidcysts 159
quadriplegiamanagement 232in spinal injuries 228
quality of life, inmyelomeningocele 166
racoon eyes 51radial nerve 11
compression 243radiation
in meningioma aetiology 93necrosis 77–8
radio-isotope cisternography 24,37
radio-isotope studies 24in CSF rhinorrhoea 52
radiological investigations 18–24see also specific modalities
radiosensitizers 75radiosurgery (stereotactic)
acoustic neuromas 104arteriovenous malformations
138brain tumours 76, 82, 101
radiotherapycerebral lymphoma 85craniopharyngioma 122gliomas 74, 75–6in malignant cord compression
212meningiomas 99–101metastatic brain tumours 82necrosis complicating 77–8paediatric brain tumours 90–1,
92pineal tumours 80pituitary tumours 120
raised intracranial pressure 27–31causes 29cerebral metastases 81chronic subdural haematoma
60–1craniopharyngioma 121craniosynostosis 168empty sella syndrome 123ependymomas 79fundal examination 5gliomas/astrocytomas 69head injury 43, 48–9, 53, 58hydrocephalus 32, 33lumbar puncture risks 15management 31, 48–9meningioma 95, 96paediatric brain tumours 87pathophysiology 27–9pineal tumours 80symptoms and signs 29–30
Rathke’s cleft cyst 121–2red nucleus 263, 264reflexes 10, 12
in cervical disc prolapse 198in cervical myelopathy 222increased 10reduced or absent 10in sciatica 187
KAYIndex 12/16/04 8:00 PM Page 293

294 INDEX
reflex sympathetic dystrophy(RSD; causalgia) 244, 257–8
rehabilitationin head injury 54–5post-stroke 154
relatives, history taking from 2relaxation times, MRI 21respiratory problems
in head injury 44in spinal injuries 229
respiratory tract infections, upper171
reticular formation, brainstem 255,256
retinal haemorrhages 128retinoblastoma 65retrocollis 266, 267rib, cervical 240rigidity 9, 264Ringertz grading system for
astrocytomas 67Rinne’s test 8
saddle area analgesia 208sagittal synostosis 167–8Saturday night palsy 243scalp injuries 42, 49scaphocephaly 168schwannomas 101
acoustic see acoustic neuromasmalignant 247peripheral 245–6spinal 212–13
sciatica 185–91aetiology 185, 186, 195anatomy and pathology 185–6clinical features 186–8investigations 189–90management 188–91patient assessment 186recurrent 191
sciatic nerve 11palsy 241
seizures 269–80absence (petit mal) 270in brain abscess 177brain tumours and see under
brain tumoursclassification 269–70generalized 269–70
secondarily 270history taking 2, 273
investigation 273–5management of first 275myoclonic 270partial 270
complex 270simple 270
postoperative prophylaxis272–3
tonic–clonic (grand mal) 269–70see also epilepsy
sella turcicachanges, craniopharyngioma
121empty sella syndrome 122–4
sensation, testing 10–12sensory disturbances (including
sensory loss)cape-like pattern 162, 208, 215in cervical disc prolapse 198in cervical myelopathy 222–3intramedullary spinal tumours
215patterns 12in spinal cord compression 208in spinal injuries 228in syringomyelia 162
sensory level 208seventh nerve see facial nerveshearing forces, in traumatic brain
injury 41shunts, CSF 33, 34–6
in benign intracranialhypertension 39
infections 35–6, 173in normal-pressure
hydrocephalus 36–7obstruction 36paediatric brain tumours 88in syringomyelia 163see also ventriculoperitoneal
shuntsingle photon emission computed
tomography (SPECT) 24,279
sinuses, paranasal see paranasalsinuses
sixth cranial nerveexamination 5–7palsy 30traumatic injuries 42
skincare, spinal cord injuries 232
changes, in reflex sympatheticdystrophy 257
skull fractures 42, 49–51base of skull 51–2compound 49–50depressed 50–1simple linear 49
skull X-rays 18brain tumours 18, 72in head injury 46in hydrocephalus 33pituitary tumours 117, 118
smell, sense of 4smoking, stroke risk 142Snellen type charts 4sodium balance 47, 62sodium valproate see valproate,
sodiumsomatomedins 116somatosensory cortex 4, 255somatosensory evoked potentials
25–6somatotopic organization,
cerebrum 4space-occupying lesions 29spasmodic torticollis 266–7spasticity
in cerebral palsy 266clasp knife 9
speech disorders 3speech therapy 55sphenoidal ridge meningiomas 94,
96–7sphenoid sinusitis 174sphincter disturbances
in spinal cord compression 209in spinal injuries 228
spina bifida see spinal dysraphismspinal abscess 218–20
epidural 218–19intramedullary 219–20subdural 219, 220
spinal accessory nerve 11spinal accessory neurectomy 267spinal arteriovenous
malformations 220–2spinal cord
concussion 229pain pathways 254–5tethering 166, 167
spinal cord compression 206–24cervical 222–4
KAYIndex 12/16/04 8:00 PM Page 294

INDEX 295
intervertebral disc prolapse216–18
investigations 15, 209–10malignant 210–12management 209–10pathological causes 206, 207presenting features 206–9treatment 210see also cauda equina
compressionspinal cord injuries 225
complete 227–8incomplete 228–9see also spinal injuries
spinal cordotomy 260–1spinal cord stimulation 261spinal dysraphism (spina bifida)
165–7antiepileptic drugs and 277hydrocephalus 32occult 165, 167
spinal fusioncervical 201–2lumbar 196
spinal injuries 225–33management 229–32mechanisms of injury 225–7neurological impairments 227–9open 227
spinal nerve root compressioncervical 197–8, 203lumbosacral 185, 186–8in spinal cord compression
207spinal shock 227spinal stenosis
cervical 223lumbar 185, 191–2, 193
spinal tuberculosis 219, 220spinal tumours
intramedullary 215–+216meningiomas 213–15metastatic 210–12schwannomas (neurofibromas)
212–13spinal X-rays 18
cervical myelopathy 223cervical spondylosis 203, 204spinal cord compression 209spinal injuries 230spinal tumours 212–13, 214–15thoracic disc prolapse 217
spinechordomas 86CT scanning 19reduction and stabilization
230–1spinothalamic tract 10, 254–5
surgical section 260–1spondylolisthesis 185, 194–6
classification 195congenital 195degenerative 192, 195
St Anne Mayo grading system forastrocytomas 67–8
Staphylococcus aureusintracranial infections 173, 174,
175, 178spinal epidural abscess 218, 219
Staphylococcus epidermidis 173statins 142status epilepticus 278stenting, secondary stroke
prevention 144–5stereotactic biopsy 73, 84–5stereotactic radiosurgery see
radiosurgerystereotactic surgery
brain tumours 73movement disorders 263, 265,
266sternocleidomastoid muscle 8steroids see corticosteroidsstraight leg raising test 186streptococci 174, 178Streptococcus milleri 174, 177, 178stretch trauma, peripheral nerves
243striatocapsular infarct 146stroke 140–57
acute 145, 150–4clinical assessment 150–2differential diagnosis 150–1emergency department triage
152hospital arrival times 150management principles 150medical care 152–4units 152
classification and pathogenesis145–50
haemorrhagic see cerebralhaemorrhage
ischaemic see cerebral infarction
prevention 140–5primary 140, 141–3secondary 140, 143–5, 154
progressing 153rehabilitation after 154risk factors 141terminology 140young adult/rarer causes
154–6Struther’s ligament 237subarachnoid haemorrhage (SAH)
125–39, 140, 150aneurysmal see cerebral
aneurysms, rupturedarteriovenous malformations
126–7, 136causes 125, 126cerebral vasospasm after 127,
132–3clinical assessment 128investigations 16, 128–9presenting features 125–8rebleeding after 132spinal arteriovenous
malformations 221of unknown aetiology 138see also stroke
subarachnoid opiateadministration 262
subconjunctival haemorrhages 51subdural abscess (empyema) 173,
178–9spinal 219, 220
subdural effusion 173subdural haematoma 59–62
acute 59–60after shunt insertion 36chronic adult 60–2
clinical presentation 60–1operative procedure 61–2
chronic infantile 54, 62subarachnoid haemorrhage with
126–7subfalcine herniation 28, 29substantia gelatinosa 254, 255, 256subthalamic nucleus 263, 264, 266superficial abdominal reflex 10superior gluteal nerve 11supinator jerk 12, 222supracondylar process of humerus,
median nerve entrapment237
KAYIndex 12/16/04 8:00 PM Page 295

296 INDEX
suprascapular nerve entrapment239
suprasellar arachnoid cysts 158–9suprasellar meningiomas 94, 97, 98swallowing problems 87, 104swelling, in reflex sympathetic
dystrophy 257Sylvian fissure, arachnoid cysts
158, 159sympathectomy 261sympathetic nerve blocks 258symptoms, neurological 1–2
classification 1–2history 2
syndrome of inappropriatesecretion of antidiuretichormone (SIADH) 47
syringomyelia 160–3aetiology 161clinical presentation 161–2radiological investigations
162–3terminology 161treatment 163
T1 relaxation time 21T1-weighted MRI scans 22, 23T2 relaxation time 21T2-weighted MRI scans 22tabes dorsalis 12–13Taenia solium 183tardy ulnar palsy 237tarsal tunnel syndrome 241taste sensation 8tear drop fractures 225telangiectasia, capillary 136temozolomide 75, 78temperature control
in head injury 47in spinal injuries 228, 229
temperature sensation 10–12temporal arteritis 155temporal lobe
‘burst’ 41, 62epilepsy 270, 275, 279
temporal lobectomy 278–80tendon reflexes, deep see reflexesteratogenicity, antiepileptic drugs
276–8teratoma, pineal 80tetrabenazine 267thalamotomy 261, 263, 266
thalamuselectrical stimulation 261, 265movement pathways 263, 264pain pathways 10–12, 255ventral posterolateral (VPL)
nucleus 255, 261ventral posteromedial (VPM)
nucleus 255, 261third cranial nerve 5–7third cranial nerve palsy 5, 6
brain herniation 29posterior communicating artery
aneurysm 127traumatic 42
third ventricle, colloid cysts 106,107
third ventriculostomy 33, 34, 36thoracic disc prolapse 217–18thoracic outlet syndrome 234, 240thoracolumbar spine injuries
Chance fractures 227compression 226flexion–rotation 226hyperextension 226–7management 229–32neurological impairments 227–9
thrombolysis, in ischaemic stroke151
thyrotroph cell adenoma 112TIA see transient ischaemic attacktiagabine 276, 277tibial nerves 11tic convulsif 252tic douloureux see trigeminal
neuralgiaTinel’s sign 235tinnitus, in acoustic neuroma 102tissue plasminogen activator (tPA)
151tone 9tongue, examination 8topiramate 276, 277torticollis, spasmodic 266–7torula see cryptococcosistouch, light 10–12tourniquets 243toxoplasmosis, intracerebral 182,
183traction
in spinal injuries 230–1trauma, peripheral nerves 243,
244
transient ischaemic attack (TIA)140
spectrum 145stroke prevention 143–5
transsphenoidal resection,pituitary tumours 119, 120
transtentorial herniation 28, 29transverse sinus, endovascular
stenting 39trapezius muscle 8trauma 40
peripheral nerve injuries 243spinal 225–33see also head injuries
tremoressential 265Parkinson’s disease 264
triceps jerk 12trigeminal nerve (5th nerve)
examination 7microvascular decompression
250root, electrical stimulation 262section of peripheral branches
249thermocoagulation of
rootlets/ganglion 249–50total or partial section 250
trigeminal neuralgia 248–50aetiology 248clinical features 248–9hemifacial spasm with 252management 249–50
trigeminothalamic tract 255trigonocephaly 168tuberculoma, intracranial 180tuberculosis 179–80
spinal 219, 220tuberculous meningitis 179–80tumour suppressor genes 66
ulnar nerve 11ulnar nerve entrapments
at elbow (cubital tunnel) 237–8at wrist 238–9
ulnar palsy, tardy 237ultrasonography
in hydrocephalus 33in stroke 148, 152
upper limbentrapment neuropathies
234–40
KAYIndex 12/16/04 8:00 PM Page 296

INDEX 297
nerve and major spinal rootsupply 11
pain 257see also arm pain
segmental innervation 199, 199weakness 198
upper motor neurone lesionssigns 7–8, 9in spinal cord compression 207in spinal injuries 228, 232
urinary incontinence 37, 95
vagus nerve, examination 8valproate, sodium 276, 277
plasma concentrations 278teratogenicity 277
vasculitis, cerebral 155vasomotor control, spinal injuries
228vasopressin 119–20vasospasm, cerebral
after aneurysm surgery 134after subarachnoid haemorrhage
127, 132–3vein of Galen malformation 138venous malformations 136venous thromboembolism
prophylaxis 153, 229ventilation, in head injury 44, 48ventral pontine infarction 146ventricular meningiomas 94, 97,
98ventricular puncture 14ventriculoatrial shunt 36ventriculocisternostomy 34ventriculoperitoneal shunt 34–6
complications 35–6normal-pressure hydrocephalus
38paediatric brain tumours 88postoperative care 35technique 35
vertebral artery dissection 155vertebrectomy, in malignant cord
compression 211vertebrobasilar territory
aneurysms 130ischaemic stroke 146, 151TIAs 145
vertigoin acoustic neuroma 102post-traumatic 42
vestibular nerve 8vestibular schwannomas see
acoustic neuromasvestibulocochlear nerve (8th nerve)
acoustic neuromas 101–2examination 8traumatic injuries 42
vibration sensation 10–12video EEG monitoring 275, 279vigabatrin 276, 277, 278Virchow, Rudolf 60, 67viruses, causing brain tumours 65visual acuity, testing 4visual cortex 4visual disturbances
arachnoid cysts 159benign intracranial hypertension
38, 39craniopharyngioma 121meningioma 96, 97pituitary tumours 112subarachnoid haemorrhage
127–8TIAs 145
visual evoked potentials 25visual fields
defectsbrain tumours 69–70, 95, 97craniopharyngioma 121pituitary tumours 112
examination 4–5patterns of loss 5, 6
visual pathways 6vitamins, stroke prevention 142Volkmann’s ischaemic contracture
243vomiting see nausea and vomitingvon Hippel–Lindau syndrome 65,
105von Recklinghausen’s disease see
neurofibromatosis type 1
warfarin, stroke prevention 142,144, 154
wasting 9weakness 10
in cervical spine disorders 198,204, 222
in sciatica 187in spinal cord compression
207–8Weber’s test 8Werner’s syndrome (MEN1) 65,
120Wernicke’s area 3white cell count, CSF 14, 15
abnormalities 16, 17in meningitis 171
World Federation of NeurologicalSurgeons (WFNS)subarachnoid haemorrhagegrading system 128
World Health Organization(WHO)
astrocytoma grading system 67ependymoma classification 78
xanthochromia 14, 16, 129X-rays, plain 18
see also skull X-rays; spinal X-rays
zygapophyseal joints,degeneration 203
KAYIndex 12/16/04 8:00 PM Page 297

KAYIndex 12/16/04 8:00 PM Page 298