Embed Size (px)
DESCRIPTION
neurocirugia
Citation preview



CONTENTS xi
Contributors iiiEvidence based medicine ivBooking the case vAbbreviations vi
1. Neuroanesthesia 11.1. General information 11.2. Drugs used in neuroanesthesia 11.3. Anesthetic requirements for intraoper-
ative evoked potential monitoring 41.4. Malignant hyperthermia 51.5. References 6
2. Neurocritical care 72.1. Fluids and Electrolytes 72.2. Blood pressure management 192.3. Sedatives & paralytics 232.4. Neurogenic pulmonary edema 282.5. References 28
3. General care 313.1. Endocrinology 313.2. Hematology 343.3. Pharmacology 443.4. References 53
4. Neurology 564.1. Dementia 564.2. Headache 574.3. Parkinsonism 594.4. Multiple sclerosis 614.5. Motor neuron diseases 654.6. Guillain-Barré syndrome 664.7. Myelitis 694.8. Neurosarcoidosis 714.9. Vascular dysautoregulatory
encephalopathy 734.10. Vasculitis and vasculopathy 744.11. References 80
5. Neuroanatomy and physiology 845.1. Surface anatomy 845.2. Cranial foramina & their contents 895.3. Cerebellopontine angle anatomy 905.4. Occiptoatlantoaxial-complex anatomy
915.5. Spinal cord anatomy 925.6. Cerebrovascular anatomy 965.7. Internal capsule 1075.8. Miscellaneous 1085.9. Neurophysiology 1095.10. References 119
6. Neuroradiology 1226.1. Contrast agents in neuroradiology 1226.2. Radiation safety for neurosurgeons
1266.3. CAT scan or CT scan 128
6.4. Magnetic resonance imaging (MRI) 129
6.5. Angiography (cerebral) 1346.6. Plain films 1356.7. Myelography 1406.8. Radionuclide scanning 1406.9. References 141
7. Operations and procedures 1447.1. Intraoperative dyes 1447.2. Operating room equipment 1447.3. Surgical hemostasis 1467.4. Craniotomies 1467.5. Cranioplasty 1737.6. Localizing levels in spine surgery 1737.7. Anterior approaches to the spine 1747.8. Surgical fusion of the cervical spine
1797.9. Surgical fusion of the thoracic spine
1907.10. Surgical fusion of the lumbar and lum-
bosacral spine 1917.11. Bone graft 1977.12. Percutaneous access to the CSF 2017.13. CSF diversionary procedures 2077.14. Sural nerve biopsy 2147.15. Nerve blocks 2157.16. References 217
8. Developmental anomalies 2228.1. Arachnoid cysts 2228.2. Intracranial lipomas 2258.3. Hypothalamic hamartomas 2268.4. Neurenteric cysts 2278.5. Craniofacial development 2288.6. Chiari malformation 2338.7. Dandy Walker malformation 2408.8. Aqueductal stenosis 2418.9. Neural tube defects 2438.10. Absence of the septum pellucidum
2478.11. Klippel-Feil syndrome 2538.12. Tethered cord syndrome 2548.13. Split cord malformation 2568.14. Lumbosacral nerve root anomalies
2568.15. References 257
9. Neuroendovascular intervention 2629.1. Neuroendovascular procedure basics
2639.2. References 264
10. Electrodiagnostics 26610.1. Electroencephalogram (EEG) 26610.2. Evoked potentials 26610.3. NCS/EMG 269
Contents

xii CONTENTS
10.4. References 27111. Neurotoxicology 273
11.1. Ethanol 27311.2. Opioids 27511.3. Cocaine 27611.4. Amphetamines 27711.5. Carbon monoxide 27711.6. References 278
12. Coma 27912.1. General information 27912.2. Approach to the comatose patient 28112.3. Herniation syndromes 28412.4. Hypoxic coma 28712.5. References 288
13. Brain death 28913.1. Brain death in adults 28913.2. Brain death in children 29213.3. Organ and tissue donation 29313.4. References 296
14. Cerebrospinal fluid 29714.1. General information 29714.2. CSF constituents 29714.3. Artificial CSF 30014.4. CSF fistula (cranial) 30014.5. Intracranial hypotension 30514.6. References 306
15. Hydrocephalus 30715.1. Treatment of hydrocephalus 31415.2. Shunt problems 32115.3. Normal pressure hydrocephalus 32915.4. Blindness from hydrocephalus 33515.5. Hydrocephalus and pregnancy 33615.6. References 337
16. Infections 34216.1. Prophylactic antibiotics 34216.2. Meningitis 34316.3. Shunt infection 34516.4. Wound infections 34816.5. Osteomyelitis of the skull 34916.6. Cerebral abscess 35016.7. Subdural empyema 35616.8. Viral encephalitis 35816.9. Creutzfeldt-Jakob disease 36116.10. Neurologic manifestations of AIDS
36416.11. Lyme disease - neurologic manifesta-
tions 36816.12. Parasitic infections of the CNS 36916.13. Fungal infections of the CNS 37416.14. Amebic infections of CNS 37516.15. Spine infections 37616.16. References 388
17. Seizures 39417.1. Seizure classification 39417.2. Special types of seizures 39617.3. Status epilepticus 40217.4. Antiepileptic drugs (AEDs) 40717.5. Seizure surgery 42017.6. References 425
18. Spine & spinal cord 42818.1. Low back pain and radiculopathy 42818.2. Sagittal balance 44118.3. Intervertebral disc herniation 44218.4. Degenerative disc/spine disease 47418.5. Craniocervical junction and upper cer-
vical spine abnormalities 49418.6. Rheumatoid arthritis 49418.7. Atlantoaxial subluxation (AAS) in
Down syndrome 49818.8. Paget’s disease 49818.9. Ankylosing spondylitis 50218.10. Ossification of the posterior longitudi-
nal ligament (OPLL) 50418.11. Ossification of the anterior longitudi-
nal ligament (OALL) 50618.12. Diffuse idiopathic skeletal hyperosto-
sis 50618.13. Scheuermann's kyphosis 50618.14. Spinal vascular malformations 50718.15. Spinal meningeal cysts 50918.16. Syringomyelia 51018.17. Spinal cord herniation (idiopathic)
51418.18. Spinal epidural hematoma 51518.19. Spinal subdural hematoma 51518.20. Spinal epidural lipomatosis (SEL) 51618.21. Coccydynia 51618.22. References 517
19. Functional neurosurgery 53219.1. Deep brain stimulation 53219.2. Surgical treatment of Parkinson’s dis-
ease 53219.3. Dystonia 53619.4. Spasticity 53619.5. Torticollis 54119.6. Neurovascular compression syn-
dromes 54219.7. Hyperhidrosis 54419.8. Tremor 54519.9. Sympathectomy 54519.10. References 546
20. Pain 54820.1. Neuropathic pain syndromes 54820.2. Craniofacial pain syndromes 54920.3. Postherpetic neuralgia 56420.4. Pain procedures 56720.5. Complex regional pain syndrome
(CRPS) 57620.6. References 577
21. Tumor 58221.1. General information 58221.2. Primary brain tumors 59021.3. Pediatric brain tumors 69721.4. Skull tumors 69821.5. Cerebral metastases 70221.6. Carcinomatous meningitis 71121.7. Foramen magnum tumors 71121.8. Idiopathic intracranial hypertension
(IIH) 713

CONTENTS xiii
21.9. Empty sella syndrome 71921.10. Tumor markers 72021.11. Neurocutaneous disorders 72221.12. Tumors of the spine and spinal cord
72821.13. Neuroblastomas 74821.14. References 749
22. Radiation therapy (XRT) 77022.1. Conventional external beam radiation
77022.2. Stereotactic radiosurgery & radiother-
apy 77322.3. Interstitial brachytherapy 77922.4. References 779
23. Stereotactic surgery 78223.1. References 783
24. Peripheral nerves 78624.1. Some basic points about peripheral
nerve injury/surgery 78924.2. Brachial plexus 79024.3. Peripheral neuropathies 79324.4. Thoracic outlet syndrome 82224.5. Miscellaneous peripheral nerve 82424.6. References 824
25. Neurophthalmology 82825.1. Nystagmus 82825.2. Papilledema 82825.3. Visual fields 82925.4. Pupillary diameter 82925.5. Extraocular muscle (EOM) system
83425.6. Miscellaneous neurophthalmologic
signs 83825.7. References 839
26. Neurotology 84026.1. Dizziness and vertigo 84026.2. Meniere’s disease 84226.3. Facial nerve palsy 84426.4. Hearing loss 84826.5. References 849
27. Head trauma 85027.1. Transfer of trauma patients 85427.2. Management in E/R 85527.3. Neuromonitoring 86627.4. Skull fractures 88527.5. Posttraumatic parenchymal injuries
89227.6. Epidural hematoma 89427.7. Subdural hematoma 89627.8. Traumatic posterior fossa mass lesions
90527.9. Posttraumatic hydrocephalus 90627.10. Aspects of general care in severe TBI
90727.11. Outcome from head trauma 90827.12. Gunshot wounds to the head 91227.13. Non-missile penetrating trauma 91627.14. High altitude cerebral edema 91627.15. Pediatric head injury 91727.16. References 919
28. Spine injuries 93028.1. Whiplash-associated disorders 93128.2. Pediatric spine injuries 93228.3. Initial management of spinal cord in-
jury 93328.4. Neurological assessment 94428.5. Spinal cord injuries 94828.6. Cervical spine fractures 95128.7. Blunt cerebrovascular injuries 98228.8. Thoracic & lumbar spine fractures 98628.9. Osteoporotic spine fractures 99228.10. Sacral fractures 99728.11. Gunshot wounds to the spine 99828.12. Penetrating trauma to the neck 99828.13. Delayed deterioration following spi-
nal cord injuries 100028.14. Chronic management issues with spi-
nal cord injuries 100028.15. References 1002
29. Stroke 101029.1. Cerebrovascular hemodynamics 101029.2. Strokes: general information 101129.3. Stroke in young adults 102429.4. Lacunar strokes 102629.5. Collateral circulation 102729.6. “Occlusion” syndromes 102729.7. Miscellaneous stroke 102929.8. References 1030
30. SAH and aneurysms 103430.1. Introduction to SAH 103430.2. Grading SAH 103930.3. Initial management of SAH 104030.4. Vasospasm 104530.5. Cerebral aneurysms 105530.6. Treatment options for aneurysms 105730.7. Timing of aneurysm surgery 106030.8. General technical considerations
of aneurysm surgery 106130.9. Aneurysm recurrence after treatment
106530.10. Aneurysm type by location 106630.11. Post-op orders for aneurysm clipping
107630.12. Unruptured aneurysms 107730.13. Multiple aneurysms 108030.14. Familial aneurysms 108030.15. Traumatic aneurysms 108130.16. Mycotic aneurysms 108230.17. Giant aneurysms 108230.18. SAH of unknown etiology 108330.19. Nonaneurysmal SAH 108430.20. Pregnancy & intracranial hemorrhage
108630.21. References 1087
31. Vascular malformations 109831.1. Arteriovenous malformation 109831.2. Venous angiomas 110431.3. Angiographically occult
vascular malformations 110531.4. Dural AVM 1109

xiv CONTENTS
31.5. Vein of Galen malformation 111231.6. Carotid-cavernous fistula 111331.7. References 1114
32. Intracerebral hemorrhage 111832.1. Intracerebral hemorrhage in adults
111832.2. ICH in young adults 113132.3. Intracerebral hemorrhage in the new-
born 113132.4. References 1138
33. Occlusive cerebro-vascular disease 114433.1. Atherosclerotic cerebrovascular dis-
ease 114433.2. Cerebral arterial dissections 116033.3. Extracranial-intracranial (EC/IC) by-
pass 116533.4. Cerebrovascular venous thrombosis
116633.5. Moyamoya disease 117033.6. References 1174
34. Outcome assessment 118234.1. References 1184
35. Differential diagnosis 118535.1. Differential diagnosis (DDx)
by signs and symptoms 118535.2. Differential diagnosis (DDx) by loca-
tion 120935.3. References 1235
36. Index 1240Quick reference tables 1331

NEUROSURGERY 5.1. Surface anatomy 85
eye movements to the opposite direction
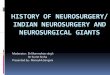
Medial surface(Figure 5-2)
The cingulate sul-cus terminates posteri-orly in the pars marginalis (pM) (plu-ral: partes marginales). On axial imaging, the pMs: are visible on 95% of CTs and 91% of MRIs4, are usually the most prominent of the paired grooves strad-dling the midline, and they extend a greater distance into the hemispheres4. On axial CT, the pM is located slightly posterior to the widest biparietal diameter4; on the typi-cally more horizontally oriented MRI slices the pM assumes a more posterior position. The pMs curve posteriorly in lower slices and anteriorly in higher slices (here, the paired pMs form the “pars bracket” - a characteristic “handlebar” configuration straddling the mid-line).
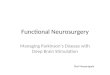
Central sulcus on axial imagingSee Figure 5-3. Identification is
important to localize the motor strip (contained in the PreCG). The central sulcus (CS) is visible on 93% of CTs and 100% of MRIs4. It curves posterior-ly as it approaches the interhemispher-ic fissure (IHF), and often terminates in the paracentral lobule, just anterior to the pars marginalis (pM) within the pars bracket (see above)4 (i.e. the CS of-ten does not reach the midline).
Pointers:• parieto-occipital sulcus (pos) (or
fissure): more prominent over the medial surface, and on axial imag-ing is longer, more complex, and more posterior than the pars marginalis5
• post-central sulcus (pocs): usually bifurcates and forms an arc or pa-renthesis (“lazy-Y”) cupping the pM. The anterior limb does not en-ter the pM-bracket and the posteri-or limb curves behind the pM to enter the IHF
Figure 5-2 Medial aspect of the right hemisphere “CT” & “MRI” bars depict typical axial slice orientation for CT & MRI scans.
See Table 5-1 and Table 5-2 for abbreviations
CinG
LG
SFG PL
PCu
Cu
corpus callosum
cins cins
prcs CENTRAL SULCUSCT
MRIpos
spspM
pons
Figure 5-3 CT scan (upper cut) showing gyri/sulci.See Table 5-1 and Table 5-2 for abbreviations
SFG
PL
PreCGcscs
pM
pocsPostCG

86 5. Neuroanatomy and physiology NEUROSURGERY
5.1.2. Surface anatomy of the cranium
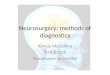
CRANIOMETRIC POINTSSee Figure 5-4.
Pterion: region where the following bones are approximat-ed: frontal, parietal, temporal and sphenoid (greater wing). Esti-mated as 2 finger-breadths above the zy-gomatic arch, and a thumb’s breadth be-hind the frontal pro-cess of the zygomatic bone (blue circle in Fig-ure 5-4).
Asterion: junc-tion of lambdoid, occip-itomastoid and parietomastoid su-tures. Usually lies within a few millime-ters of the posterior-in-ferior edge of the junction of the trans-verse and sigmoid si-nuses (not always reliable6 - may overlie either sinus).
Vertex: the top-most point of the skull.
Lambda: junc-tion of the lambdoid and sagittal sutures.
Stephanion: junction of coronal suture and superior temporal line.
Table 5-2 Cerebral gyri and lobules(abbreviations)
AG angular gyrusCinG cingulate gyrusCu cuneusLG lingual gyrusMFG, SFG middle & superior frontal gyrusOG orbital gyrusPCu precuneousPreCG, PostCG pre- and post-central gyrusPL paracentral lobule (upper SFG and PreCG
and PostCG) IFG
POpPTPOr
inferior frontal gyruspars opercularispars triangularis pars orbitalis
STG, MTG, ITG superior, middle & inferior temporal gyrusSPL, IPL superior & inferior parietal lobuleSMG supramarginal gyrus
Table 5-1 Cerebral sulci (abbreviations)
cins cingulate sulcuscs central sulcusips-ios intraparietal-intraoccip-
ital sulcuslos lateral occipital sulcuspM pars marginalispocn pre-occipital notchpocs post-central sulcuspof parieto-occipital fissurepos parieto-occipital sulcusprcs pre-central sulcussfs, ifs superior, inferior frontal
sulcussps superior parietal sulcussts, its superior, inferior tem-
poral sulcustos trans occipital sulcus
Figure 5-4 Craniometric points & cranial sutures.Named bones appear in all upper case letters. Abbreviations: GWS = greater wing of sphenoid bone, NAS = nasal bone, stl = superior temporal line, ZYG = zygomatic. Sutures: cs = coronal, ls = lambdoid, oms = occipitomastoid, pms = parietomas-toid, sms = squamomastoid, sqs = squamosal
opisthionasterion
nasionrhinion
prosthion
inferioralveolar point
glabella
gnathionor menton
gonion
inion
bregmavertex
lambdastl
sqs
pmssms
pterion
ls
oms
cs
stephanion
ophyron
MANDIBLE
MAXILLA
ZYGNASAL
TEMPORAL
PARIETAL
MASTOID
FRON
TAL
OCCIP
ITAL
GW
S

NEUROSURGERY 5.1. Surface anatomy 87
Glabella: the most forward projecting point of the forehead at the level of the su-praorbital ridge in the midline.
Opisthion: the posterior margin of the foramen magnum in the midline.Bregma: the junction of the coronal and sagittal sutures.Sagittal suture: midline suture from coronal suture to lambdoid suture. Although
often assumed to overlie the superior sagittal sinus (SSS), the SSS lies to the right of the sagittal suture in the majority of specimens7 (but never by > 11 mm).
The most anterior mastoid point lies just in front of the sigmoid sinus8.
RELATION OF SKULL MARKINGS TO CEREBRAL ANATOMY
Taylor-Haughton linesTaylor-Haughton (T-H)
lines can be constructed on an angiogram, CT scout film, or skull x-ray, and can then be re-constructed on the patient in the O.R. based on visible external landmarks9. T-H lines are shown as dashed lines in Figure 5-5.
1. Frankfurt plane, AKA baseline: line from inferi-or margin of orbit through the upper mar-gin of the external audi-tory meatus (EAM) (as distinguished from Re-id’s base line: from infe-rior orbital margin through the center of the EAM)10 (p 313)
2. the distance from the na-sion to the inion is mea-sured across the top of the calvaria and is divid-ed into quarters (can be done simply with a piece of tape which is then folded in half twice)
3. posterior ear line: perpendicular to the baseline through the mastoid process4. condylar line: perpendicular to the baseline through the mandibular condyle5. T-H lines can then be used to approximate the sylvian fissure (see below) and the
motor cortex (also see below)
Sylvian fissure AKA lateral fissureApproximated by a line connecting the lateral canthus to the point 3/4 of the way
posterior along the arc running over convexity from nasion to inion (T-H lines).
Angular gyrusLocated just above the pinna, important on the dominant hemisphere as part of
Wernicke’s area. Note: there is significant individual variability in the location2.
Angular arteryLocated 6 cm above the EAM.
Motor cortexNumerous methods utilize external landmarks to locate the motor strip (pre-central
gyrus) or the central sulcus (Rolandic fissure) which separates motor strip anteriorly from primary sensory cortex posteriorly. These are just approximations since individual variability causes the motor strip to lie anywhere from 4 to 5.4 cm behind the coronal suture11. The central sulcus cannot even be reliably identified visually at surgery12.
• method 1: the superior aspect of the motor cortex is almost straight up from the EAM near the midline
• method 213: the central sulcus is approximated by connecting:
Figure 5-5 Taylor-Haughton linesand other localizing methods
©2001 Mark S Greenberg, M.D.All rights reserved.Unauthorized use is prohibited.
3/4
1/2
posterior ear line
Frankfurtplane
condylar line
syan ssure
cent
ral s
ulcu
s
2 cm
lvifi
EAMEAMEAM

88 5. Neuroanatomy and physiology NEUROSURGERY
A. the point 2 cm posterior to the midposition of the arc extending from nasion to inion (illustrated in Figure 5-5), to
B. the point 5 cm straight up from the EAM• method 3: using T-H lines, the central sulcus is approximated by connecting:
A. the point where the “posterior ear line” intersects the circumference of the skull (see Figure 5-5) (usually about 1 cm behind the vertex, and 3-4 cm be-hind the coronal suture), to
B. the point where the “condylar line” in-tersects the line representing the sylvian fissure
• method 4: a line drawn 45° to Reid’s base line starting at the pterion points in the direction of the motor strip14 (p 584-5)
RELATIONSHIP OF VENTRICLES TO SKULL
Figure 5-6 shows the rela-tionship of non-hydrocephalic ventricles to the skull in the lat-eral view. Some dimensions of in-terest are shown in Table 5-315.
In the non-hydrocephalic adult, the lateral ventricles lie 4-5 cm below the outer skull sur-face. The center of the body of the lateral ventricle sits in the midp-upillary line, and the frontal horn is intersected by a line pass-ing perpendicular to the calvaria along this line16. The anterior horns extend 1-2 cm anterior to the coronal suture.
Average length of third ventricle ≈ 2.8 cm.
Table 5-3 Dimensions from Figure 5-6
Dimension(see Figure 5-6)
Description Lower limit(mm)
Average(mm)
Upper limit(mm)
D1 length of frontal horn anterior to FM 25D2 distance from clivus to floor of 4th ventricle at
level of fastigium*
* the fastigium is the apex of the 4th ventricle within the cerebellum
33.3 36.1 40.0
D3 length of 4th ventricle at level of fastigium* 10.0 14.6 19.0D4 distance from fastigium* to opisthion 30.0 32.6 40.0
Figure 5-6 Relationship of ventricles to skull landmarks*
* Abbreviations: (F = frontal horn, B = body, A = atrium, O = oc-cipital horn, T = temporal horn) of lateral ventricle. FM = fora-men of Monro. Aq = sylvian aqueduct. V3 = third ventricle. V4 = fourth ventricle. cs = coronal suture. Dimensions D1-4 → see Table 5-3
baseline
sella turcica
V3
V4
Aq
FM
D2 D3
opisthion
Twining
D4
D1
T
F
B
O
T
A
sigmoid sinus
cs

NEUROSURGERY 5.2. Cranial foramina & their contents 89
5.1.3. Surface landmarks of spine levels
Estimates of cervical levels for anterior cervical spine surgery may be made using the landmarks shown in Table 5-4. Intra-operative C-spine x-rays are essential to verify these estimates.
The scapular spine is located at about T2-3.The inferior scapular pole is ≈ T6 posteriorly.Intercristal line: a line drawn between the high-
est point of the iliac crests across the back will cross the midline either at the interspace between the L4 and L5 spinous processes, or at the L4 spinous process itself.
5.2. Cranial foramina & their contents
Porus acusticusAKA internal auditory canal (see Figure 5-7)The filaments of the acoustic portion of VIII penetrate tiny openings of the lamina
cribrosa of the cochlear area18. Transverse crest: separates superior vestibular area and facial canal (above) from
the inferior vestibular area and cochlear area (below)18.Vertical crest (AKA Bill’s bar): separates the meatus to facial canal anteriorly (con-
Table 5-5 Cranial foramina and their contents*
* Abbreviations: a. = artery, aa. = arteries, v. = vein, vv. = veins, n. = nerve, nn. = nerves, br. = branch, Cr. N. = cranial nerve, fmn. = foramen, div. = division
Foramen Contentsnasal slits anterior ethmoidal nn., a. & vsuperior orbital fissure Cr. Nn. III, IV, VI, all 3 branches of V1 (ophthalmic division divides into nasociliary, fron-
tal, and lacrimal nerves); superior ophthalmic vv.; recurrent meningeal br. from lacrimal a.; orbital branch of middle meningeal a.; sympathetic filaments from ICA plexus
inferior orbital fissure Cr. N. V-2 (maxillary div.), zygomatic n.; filaments from pterygopalatine branch of max-illary n.; infraorbital a. & v.; v. between inferior ophthalmic v. & pterygoid venous plexus
foramen lacerum usually nothing (ICA traverses the upper portion but doesn’t enter, 30% have vidian a.)carotid canal internal carotid a., ascending sympathetic nervesincisive foramen descending septal a.; nasopalatine nn.greater palatine foramen greater palatine n., a., & v.lesser palatine foramen lesser palatine nn.internal acoustic meatus Cr. N. VII (facial); Cr. N. VIII (stato-acoustic) - (see text & Figure 5-7 below)hypoglossal canal Cr. N. XII (hypoglossal); a meningeal branch of the ascending pharyngeal a.foramen magnum spinal cord (medulla oblongata); Cr. N. XI (spinal accessory nn.) entering the skull; ver-
tebral aa.; anterior & posterior spinal arteriesforamen cecum occasional small veincribriform plate olfactory nn.optic canal Cr. N. II (optic); ophthalmic a.foramen rotundum Cr. N. V2 (maxillary div.), a. of foramen rotundumforamen ovale Cr. N. V3 (mandibular div.) + portio minor (motor for CrN V)foramen spinosum middle meningeal a. & v.jugular foramen internal jugular v. (beginning); Cr. Nn. IX, X, XIstylomastoid foramen Cr. N. VII (facial); stylomastoid a.condyloid foramen v. from transverse sinusmastoid foramen v. to mastoid sinus; branch of occipital a. to dura mater
Table 5-4 Cervical levels17
Level LandmarkC1-2 angle of mandibleC3-4 1 cm above thyroid carti-
lage (≈ hyoid bone)C4-5 level of thyroid cartilageC5-6 crico-thyroid membraneC6 carotid tubercleC6-7 cricoid cartilage

90 5. Neuroanatomy and physiology NEUROSURGERY
taining VII and nervus intermedius) from the vestibular area posteriorly (containing the superior division of vestibular nerve).
The “5 nerves” of the IAC: 1. facial nerve (VII)
(mnemonic: “7-up” as VII is in superi-or portion)
2. nervus intermedi-us: the somatic sensory branch of the facial nerve primarily inner-vating mechanore-ceptors of the hair follicles on the in-ner surface of the pinna and deep mechanoreceptors of nasal and buccal cavities and chemoreceptors in the taste buds on the anterior 2/3 of the tongue
3. acoustic portion of the VIII nerve (mnemonic: “Coke down” for cochlear portion)4. superior branch of vestibular nerve: passes through the superior vestibular area
to terminate in the utricle and in the ampullæ of the superior and lateral semi-circular canals
5. inferior branch of vestibular nerve: passes through inferior vestibular area to ter-minate in the saccule
5.3. Cerebellopontine angle anatomy
* NI = nervus intermediusFigure 5-7 Right internal auditory canal (porus acusticus) & nerves
facial canal (Cr. N. VII with NI*)
superior vestibular area (superior vestibular nerve) (to utricle &superior & lateral semicircular canals)
transverse crest (crista falciformis)
vertical crest (”Bill’s bar”)
inferior vestibular area (to saccule)foramen singulare (toposterior semicircular canal)
tractus spiralis foraminosus (cochleararea) (acoustic portion of Cr. N. VIII)
(inferiorvestibular nerve)
Figure 5-8 Normal anatomy of right cerebellopontine angle viewed from behind (as in a suboccipital approach)18
V
VIIIAC
VIIIIX
XXI
XII
medullaolive
ponsflocculuschoroidplexus
jugularforamen
Meckel'scave
cerebellartonsil
foramen ofMagendie
foramen ofLuschka
retractoron cerebellarhemisphere
PICA

NEUROSURGERY 5.4. Occiptoatlantoaxial-complex anatomy 91
5.4. Occiptoatlantoaxial-complex anatomy
≈ 50% of head rotation occurs at the C1-2 (atlantoaxial) joint.
Ligaments of the occipito-atlanto-axial complex
Stability of this joint complex is primarily due to ligaments, with little contribution from bony articulations and joint capsules (see Figure 5-9 through Figure 5-11):
1. ligaments that connect the atlas to the occiput: A. anterior at-
lanto-occipi-tal mem-brane: cephal-ad extension of the anteri-or longitudi-nal ligament. Extends from anterior mar-gin of fora-men magnum (FM) to ante-rior arch of C1
B. posterior at-lanto-occipi-tal mem-brane: con-nects the pos-terior margin of the FM to posterior arch of C1
C. the ascending band of the cruciate ligament2. ligaments that connect the axis (viz. the odontoid) to the occiput:
A. tectorial membrane: some authors distinguish 2 components1. superficial component: cephalad continuation of the posterior longitu-
Figure 5-9 Sagittal view of the ligaments of the craniovertebral junctionModified with permission from “In Vitro Cervical Spine Biomechanical Testing” BNI Quarterly,
Vol.9, No. 4, 1993
anterioratlantooccipital
membrane
apicalodontoidligament
cruciate ligament,ascending band
cruciate ligament,descending band
tectorialmembrane
transverseligamentanterior
longitudinalligament
posteriorlongitudinal
ligament
posterioratlantooccipitalmembrane
ligamentumflavum
C3
C2spinalcord
C1
Figure 5-10 Dorsal view of the cruciate and alar ligamentsViewed with tectorial membrane removed.
Modified with permission from “In Vitro Cervical Spine Biomechanical Testing” BNI Quarterly, Vol.9, No. 4, 1993
transverse bandCRUCIATE
LIGAMENT
right alarligament
accessory(deep) portionof tectorialmembrane
descendingband
C1
clivus
C2
ascending band

92 5. Neuroanatomy and physiology NEUROSURGERY
dinal ligament. A strong band connecting the dorsal surface of the dens to the ventral surface of the FM above, and dorsal surface of C2 & C3 bodies below
2. accessory (deep) portion: located laterally, connects C2 to occipital condyles
B. alar (“check”) ligaments19
1. occipito-alar portion: connects side of the dens to occipital condyle2. atlanto-alar portion: connects side of the dens to the lateral mass of C1
C. apical odontoid liga-ment: connects tip of dens to the FM. Little mechanical strength
3. ligaments that connect the axis to the atlas:
A. transverse (atlanto-axial) ligament: the horizontal component of the cruciate liga-ment. Traps the dens against the anterior at-las via a strap-like mechanism (see Figure 5-11). Provides the ma-jority of the strength (“the strongest liga-ment of the spine”20)
B. atlanto-alar portion of the alar ligaments (see above)
C. descending band of the cruciate ligament
The most important structures in maintaining atlanto-occipital stability are the tec-torial membrane and the alar ligaments. Without these, the remaining cruciate liga-ment and apical dentate ligament are insufficient.
5.5. Spinal cord anatomy
5.5.1. Spinal cord tracts
Figure 5-12 depicts a cross-section of a typical spinal cord segment, combining some elements from different levels (e.g. the intermediolateral grey nucleus is only present from T1 to ≈ L1 or L2 where there are sympathetic (thoracolumbar outflow) nuclei). It is schematically divided into ascending and descending halves, however, in actuality, as-cending and descending paths coexist on both sides.
Table 5-6 Descending (motor) tracts (↓) in Figure 5-12
Number (see Figure 5-12)
Path Function Side of body
1 anterior corticospinal tract skilled movement opposite2 medial longitudinal fasciculus ? same3 vestibulospinal tract facilitates extensor muscle tone same4 medullary (ventrolateral) reticulospinal tract automatic respirations? same5 rubrospinal tract flexor muscle tone same6 lateral corticospinal (pyramidal) tract skilled movement same
Figure 5-11 C1 viewed from above, showing the trans-verse and alar ligaments
Modified with permission from “In Vitro Cervical Spine Bio-mechanical Testing” BNI Quarterly, Vol.9, No. 4, 1993
tectorialmembrane
posterior arch C1
transverseligament
tubercle
right alarligament
odontoidprocess

NEUROSURGERY 5.5. Spinal cord anatomy 93
Figure 5-12 also depicts some of the laminae according to the scheme of Rexed. Lam-ina II is equivalent to the substantia gelatinosa. Laminae III and IV are the nucleus pro-prius. Lamina VI is located in the base of the posterior horn.
SENSATION
PAIN & TEMPERATURE: BODYReceptors: free nerve endings (probable).1st order neuron: small, finely myelinated afferents; soma in dorsal root ganglion
(no synapse). Enter cord at dorsolateral tract (zone of Lissauer). Synapse: substantia ge-
Table 5-7 Bi-directional tracts in Figure 5-12
Number (see Figure 5-12)
Path Function
7 dorsolateral fasciculus (of Lissauer)8 fasciculus proprius short spinospinal connections
Table 5-8 Ascending (sensory) tracts (↑) in Figure 5-12
Number (see Figure 5-12)
Path Function Side of body
9 fasciculus gracilis joint position, fine touch, vibration
same10 fasciculus cuneatus11 posterior spinocerebellar tract stretch receptors same12 lateral spinothalamic tract pain & temperature opposite13 anterior spinocerebellar tract whole limb position opposite14 spinotectal tract unknown, ? nociceptive opposite15 anterior spinothalamic tract light touch opposite
Figure 5-12 Schematic cross-section of cervical spinal cord
2
34
5
6
7 8 910
1112
13
14
15
MOTOR(descending
paths)
bi-directionalpaths
SENSORY(ascending
paths)
S TCTC
STCSTC
S TC
STC
CTSCTSCTS
{
1
S = sacralT = thoracicC = cervical
anterior spinalartery
dentateligament
{{
anterior motornerve root
2.5-4 cm
intermediolateralgrey nucleus
(sympathetic)IIIIII
IV
V
VI
IX
IX
VII
VIIIX

94 5. Neuroanatomy and physiology NEUROSURGERY
latinosa (Rexed II).2nd order neuron axon cross obliquely in the anterior white commissure ascending
≈ 1-3 segments while crossing to enter the lateral spinothalamic tract.Synapse: VPL thalamus. 3rd order neurons pass through IC to postcentral gyrus
(Brodmann’s areas 3, 1, 2).
FINE TOUCH, DEEP PRESSURE & PROPRIOCEPTION: BODYFine touch AKA discriminative touch. Receptors: Meissner’s & pacinian corpuscles,
Merkel’s disks, free nerve endings.1st order neuron: heavily myelinated afferents; soma in dorsal root ganglion (no
synapse). Short branches synapse in nucleus proprius (Rexed III & IV) of posterior gray; long fibers enter the ipsilateral posterior columns without synapsing (below T6: fascicu-lus gracilis; above T6: fasciculus cuneatus).
Synapse: nucleus gracilis/cuneatus (respectively), just above pyramidal decussa-tion. 2nd order neuron axons form internal arcuate fibers, decussate in lower medulla as medial lemniscus.
Synapse: VPL thalamus. 3rd order neurons pass through IC primarily to postcen-tral gyrus.
LIGHT (CRUDE) TOUCH: BODYReceptors: as fine touch (see above), also peritrichial arborizations.
Figure 5-13 Dermatomal and sensory nerve distribution(Redrawn from “Introduction to Basic Neurology”, by Harry D. Patton, John W. Sundsten, Wayne E. Crill and
Phillip D. Swanson, © 1976, pp 173, W. B. Saunders Co., Philadelphia, PA, with permission)
©2001 Mark S Greenberg, M.D.All rights reserved.Unauthorized use is prohibited.
DERMATOMESC U T A N E O U S
N E R V E S
P O S T E R I O RA N T E R I O R
trigeminalnerve {V1
V2
V3 superior clavicular
axillary
post. cutaneousdorsal cutan.
RADIAL
musculocutan.medial cutan.
radial
median
ulnar
INTERCOSTALSposterior
lateral
clunials
posteriorcutaneous
saphenous
sural
plantars {lat.med.
medial
occipitals
FEMORALanteriorcutaneous
SCIATIC
deep peroneal
DERMATOMES
(an te r io r ) (pos te r io r )
lateral cutan.nerve of thigh
ilio-inguinal
COMMON PERONEALlat. cutan.
sup. peroneal
TIBIAL
S3
S5
T12
C6
L3 L4
S1
C3
C4T2
T4
T6
T8
T10
C4T3T4
T6
T8
T10T12
L1
L2
S4
C3
C2
C5 C5
C8
T1
T2
L3
L4
L5
S1
C6
C7
C8
T1
T2
C2
S1
L5L4
C7

NEUROSURGERY 5.5. Spinal cord anatomy 95
1st order neuron: large, heavily myelinated afferents (Type II); soma in dorsal root ganglion (no synapse). Some ascend uncrossed in post. columns (with fine touch); most synapse in Rexed VI & VII.
2nd order neuron axons cross in anterior white commissure (a few don’t cross); enter anterior spinothalamic tract.
Synapse: VPL thalamus. 3rd order neurons pass through IC primarily to postcen-tral gyrus.
5.5.2. Dermatomes and sensory nerves
Figure 5-13 shows anterior and posterior view, each schematically separated into sensory dermatomes (segmental) and peripheral sensory nerve distribution.
5.5.3. Spinal cord vasculature
Although a radicular artery from the aorta accompanies the nerve root at many lev-els, most of these contribute little flow to the spinal cord itself. The anterior spinal artery is formed from the junction of two branches, each from one of the vertebral arteries. Ma-jor contributors of blood supply to the anterior spinal cord is from 6-8 radicular arteries
Figure 5-14 Schematic diagram of spinal cord arterial supplyModified from Diagnostic Neuroradiology, 2nd ed., Volume II, pp. 1181, Taveras J M, Woods EH, editors, ©
1976, the Williams and Wilkins Co., Baltimore, with permission)
aorta
brachiocephalic trunk
rightsubclavian
right commoncarotid
right vertebralartery
left vertebralartery
left subclavian
costocervical trunk
anterior spinal artery
left commoncarotid
radicular artery at C3
radicular artery at C6
radicular artery at C8
deep cervical artery
radicular artery at T5
arteria radicularismagna(posterior branch)
artery ofAdamkiewicz(arteria radicularisanterior magna)
left posterior spinal artery
spinal cord
intercostal arteries}
basilar artery
posterior inter-costal artery(dorsal branch)
posteriorintercostalartery
aorta
radicularartery
Axial view
anteriorspinalartery
posteriorspinal arteries

96 5. Neuroanatomy and physiology NEUROSURGERY
at the following levels (“radiculomedullary arteries”, the levels listed are fairly consis-tent, but the side varies21 (p 1180-1)):
• C3 - arises from vertebral artery
• T4 or T5• artery of Adamkiewicz AKA arteria radicularis anterior magna
A. the main arterial supply for the spinal cord from ≈ T8 to the conusB. located on the left in 80%23
C. situated between T9 & L2 in 85% (between T9 & T12 in 75%); in remaining 15% between T5 & T8 (in these latter cases, there may be a supplemental radicular artery further down)
D. usually fairly large, gives off cephalic and caudal branch (latter is usually larger) giving a characteristic hair-pin appearance on angiography
The paired posterior spinal arteries are less well defined than the anterior spinal artery, and are fed by 10-23 radicular branches.
The midthoracic region has a tenuous vascular supply (“watershed zone”), possess-ing only the above noted artery at T4 or T5. It is thus more susceptible to vascular in-sults.
ANATOMIC VARIANTSArcade of Lazorthes: normal variant where the anterior spinal artery joins with
the paired posterior spinal arteries at the conus medullaris.
5.6. Cerebrovascular anatomy
5.6.1. Cerebral vascular territories
Figure 5-15 depicts approximate vascular distributions of the major cerebral arter-ies. There is considerable variability of the major arteries24 as well as the central distri-
• C6 - usually arises from deep cervical artery• C8 - usually from costocervical trunk } ≈ 10% of population lack an an-
terior radicular artery in lower cervical spine22
RAH = recurrent artery of HeubnerFigure 5-15 Vascular territories of the cerebral hemispheres
RAH
internal carotid
basilar artery
posterior cerebralartery
middle cerebralartery
anterior choroidalartery
anterior cerebralartery
AChA
MCA
PCommA
AXIAL VIEWCORONAL VIEW