Embed Size (px)
Citation preview

Epilepsy and Anaesthesia
Presented by – Dr. Dhritiman Chakrabarti
Moderated by – Dr. Gopala Krishna K N

Basic Definitions
• Seizure (from the Latin sacire—to take possession of) is the clinical manifestation of an abnormal, excessive, hypersynchronousdischarge of a population of cortical neurons.
• Epilepsy is a disorder of the central nervous system characterized by recurrent seizures unprovoked by an acute systemic or neurologic insult.

Mechanisms of Neuronal Excitability
• Intrinsic Factors:
1. The type, number and distribution of voltage- and ligand-gated channels.
2. Biochemical modification of receptors
3. Activation of second-messenger systems
4. Modulating gene expression, as by RNA editing
• Extrinsic Factors:
1. Changes in extracellular ion concentration
2. Remodeling of synaptic contacts and neuronal network
3. Modulating transmitter metabolism by glial cells

Seizure InitiationSeizure initiation is characterized by two concurrent
events:
1) High-frequency bursts of action potentials (paroxysmal depolarization shift)
2) Hypersynchronization of a neuronal population (local spread).
3) Distal Seizure propagation (loss of surround inhibition)
Epileptogenesis
1) Neuronal network reorganization.
2) Kindling.
Antiepileptic Drug Interactions
• Induction and inhibition of the cytochromeP450 isoenzymes.
• Inducers – CBZ, Phenytoin, Phenobarbital, Topiramate
• Inhibitors – Valproate• No effect - Gabapentin, lamotrigine,
levetiracetam, tiagabine, and vigabatrin
Drugs to be careful about – Antibiotics, Amiodarone, β-Blockers, CCB, NMBA, Opioids.
Carbepenems induce Valproate metabolism.

Effect of Anaesthetic agents on Epilepsy
• Inhalational Agents:
1) N2O – Proconvulsant in animal models; Suppresses Ecog epileptiform potentials intraoperatively; Myoclonus observed in humans at hyperbaric doses and along with other inhaled agents.
2) Sevoflurane – Well known proconvulasant activity in children and when combined with hypocapnea. Widespread EEG activation.
3) Isoflurane & Desflurane – Well known anticonvulsant properties, even used in SE.
• Opioids (Proconvulsant):1) Pethidine – Association with myoclonus and tonic clonic
seizure activity.2) Alfentanyl and Remifent – Used to induce spike activity
and help in localization of epileptogenic zones intraoperatively.
3) GTCS in low to moderate doses – Fent, alfent, sufent and morphine.
• IV Anaesthetic agents:1) Propofol, thiopentone, methohexital, etomidate, ketamine
all have proconvulsant effects (myoclonus, ophistotonus, GTCS) in low doses and anticonvulsant at high doses.
2) Benzodiazepines – always anticonvulsant.3) LA – GTCS at high plasma levels. Lignocaine used to treat
SE in children in small case series.4) NMBA – Laudanosine.

• Perioperative AEDs: -
1. IV is better than oral (doses are equal)
2. Continue AEDs perioperatively, without missing out a single dose.
3. ICU stay with changes in pH and S. Albumin levels and other drug interactions warrant serum drug level measurements (esp. Phenytoin).
STATUS EPILEPTICUS
• Status epilepticus is defined as 5 min or more of(i) continuous clinical and/or electrographic seizure activity or(ii) recurrent seizure activity without recovery (returning to
baseline) between seizures.
• Refractory status epilepticus (RSE) is defined as SE that fails to respond to first- and any two drugs in the second-line therapy and it is observed in 9% to 31% of patients with SE .
• Most convulsive seizures abate within 2–3 min and a seizure that continues for more than 5 min has a low chance of terminating spontaneously, so should be treated with emergency antiepileptic medications.
• The traditional definition of 30 min for SE definition has been revised to 5 min because permanent neuronal injury and pharmacoresistance may occur before deadline of 30 min (Brophy 2012).
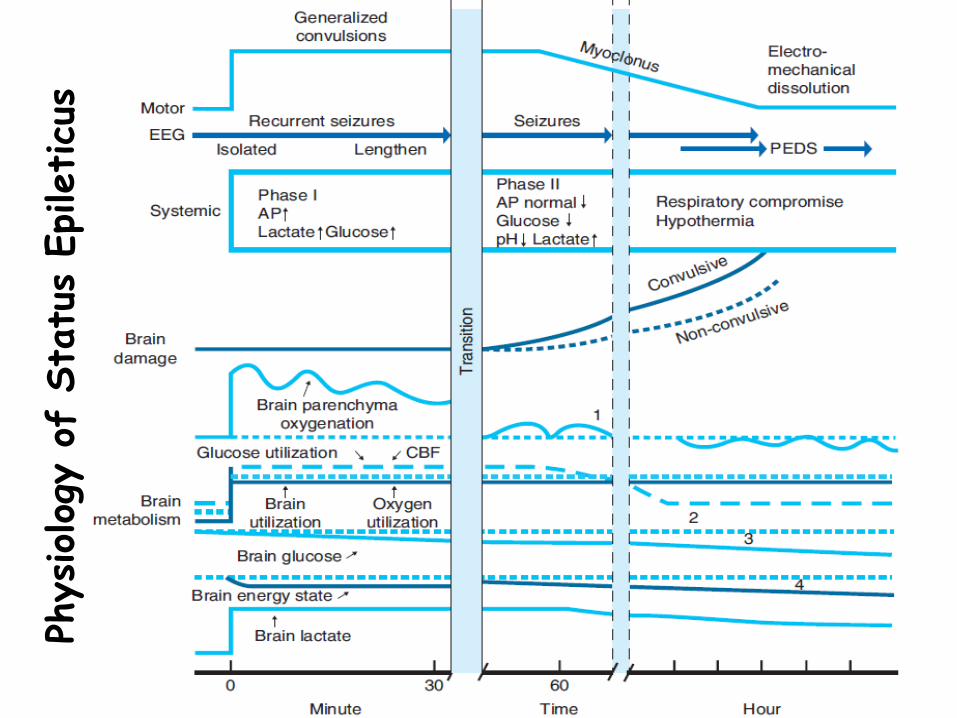
Physiolog
y o
f Sta
tus
Epileticu
s
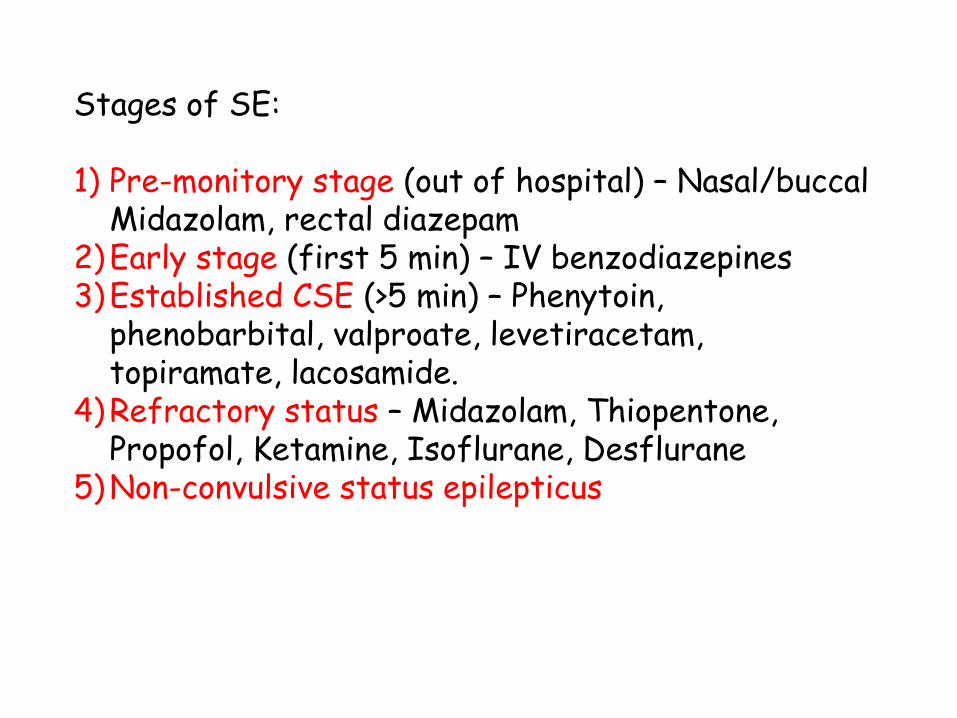
Stages of SE:
1) Pre-monitory stage (out of hospital) – Nasal/buccalMidazolam, rectal diazepam
2)Early stage (first 5 min) – IV benzodiazepines3)Established CSE (>5 min) – Phenytoin,
phenobarbital, valproate, levetiracetam, topiramate, lacosamide.
4)Refractory status – Midazolam, Thiopentone, Propofol, Ketamine, Isoflurane, Desflurane
5)Non-convulsive status epilepticus
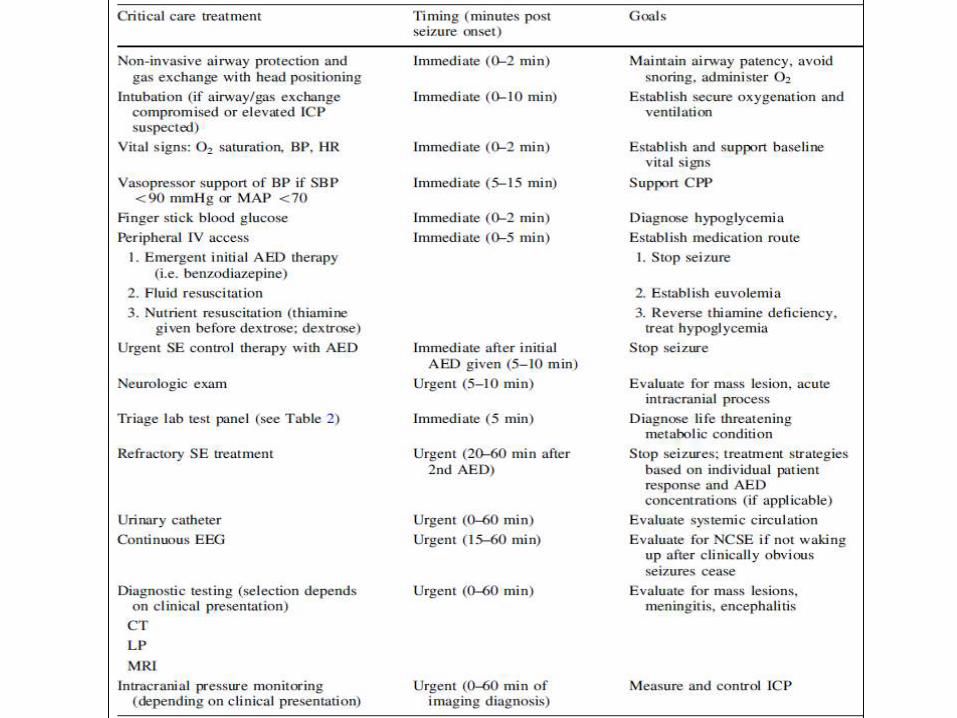

Status Epilepticus Treatment
Refractory SE Treatment

Alternative therapies for RSE

Epilepsy Surgery -Identifying Surgical Candidates
1) Medical intractability:
–Two appropriately chosen, well-tolerated first line antiepileptic drug regimens have failed due to lack of efficacy.
2) Sufficient Disability
3) Minimum duration from diagnosis – 2 yrs (Adults)
4) Difference between Adults and Paediatric population.
• Plasticity phenomenon: Early surgical intervention can maximize efficacy, recovery, and cognitive potential.
• No defining concept of disability.

Surgical candidacy to be determined on a case by case basis using data from an extensive multimodality assessment.
• Timing of Surgery - People suffering from epileptic syndromes with a high probability of medical intractability and a favourable surgical prognosis should be considered for surgery early.
• Presurgical Evaluation:-1) Medical History with ictal and interictal symptoms.2) High resolution Neuroimaging.3) Identifying Epileptogenic Zone – EEG, Neurophysiological
evaluation, Video EEG..4) Invasive intracranial recordings.5) Other ancillary neurophysiologic techniques - evoked
potential studies, cerebral functional mapping, MEG and magnetic stimulation.
6) Identifying Functional deficit zone and lateralization of eloquent cortex - interictal SPECT and/or PET, and the intracarotid sodium amytal (Wada) test, fMRI
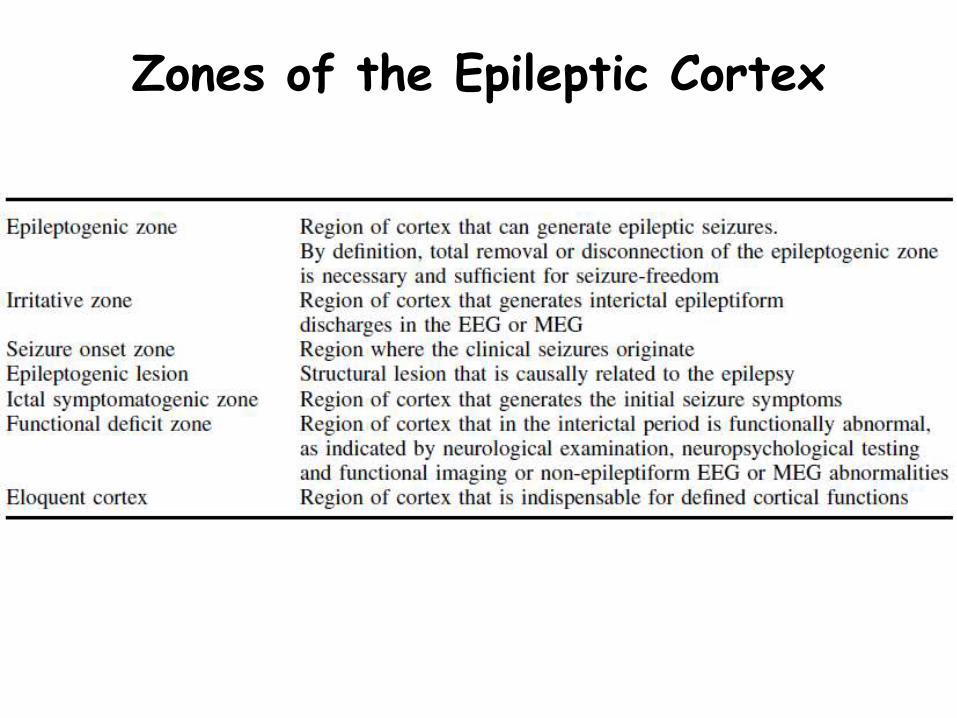
Zones of the Epileptic Cortex
EEG for Diagnosis and Localization
• Interictal sharp or spike wave is cornerstone for epilepsy diagnosis.
• Represents cortical hyperexcitability and hypersynchrony, which may persists in the “normal” interictal state.
• Montage specificity of EEG abnormality helps localize epileptogenic zone.
• Chowdhary et al (2013) found overall sensitivity of EEG in yielding abnormal interictal epileptiformdischarges was 62.7% in epilepsy patients.
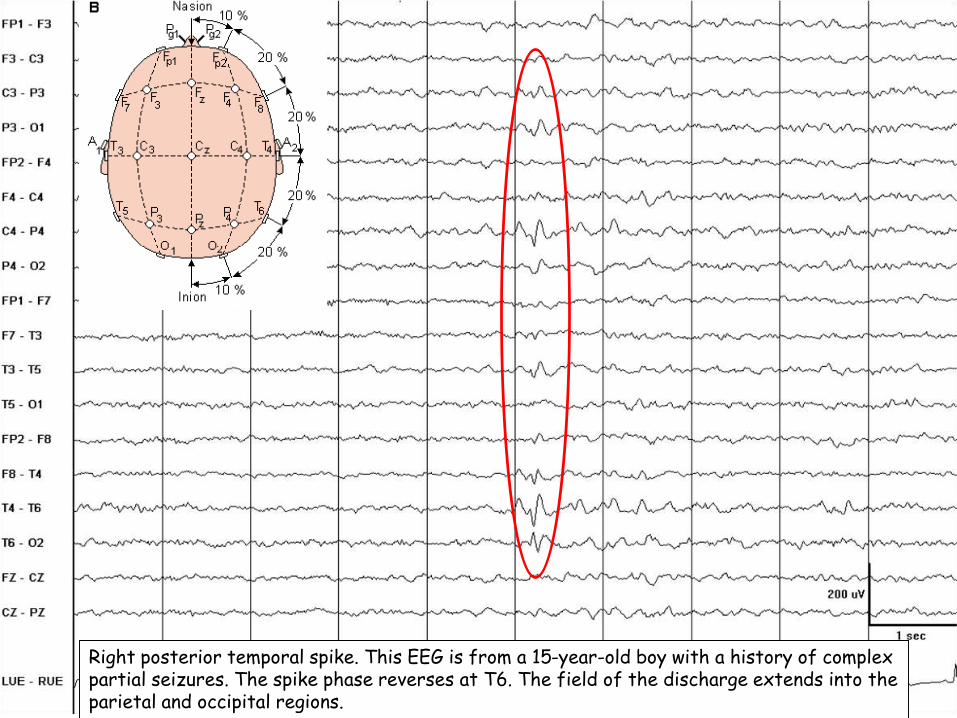
Right posterior temporal spike. This EEG is from a 15-year-old boy with a history of complex partial seizures. The spike phase reverses at T6. The field of the discharge extends into the parietal and occipital regions.

Interictal generalized spike-wave complexes - Idiopathic eneralized epilepsy
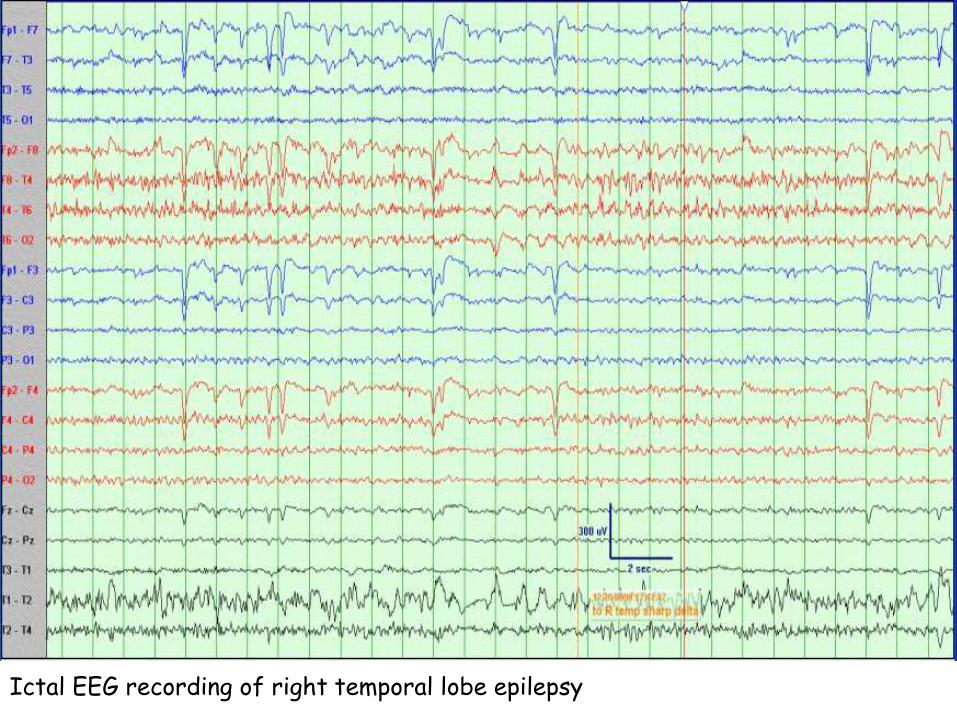
Ictal EEG recording of right temporal lobe epilepsy

Video EEGUseful to diagnose distinguish Psychogenic seizures, Syncope, Parasomnias,Hemifacial spasms from actual epilepsy.
Interictal EEG findings – Sharp waves, Spike & wave complexes, Polyspikes, TIRDA, Continuous Polymorphic Delta etc.Ictal EEG findings – Generalized, Lateralized or Focal spikes accompanied with clinical seizure in patients. There may be post-ictal slowing of EEG.
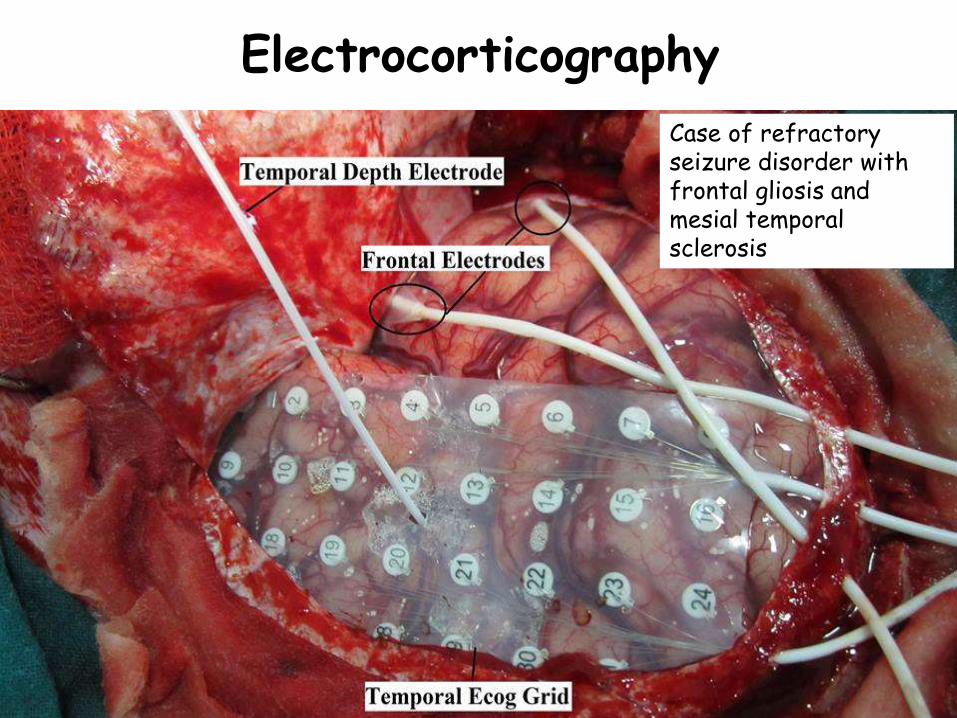
Electrocorticography
Case of refractory seizure disorder with frontal gliosis and mesial temporal sclerosis
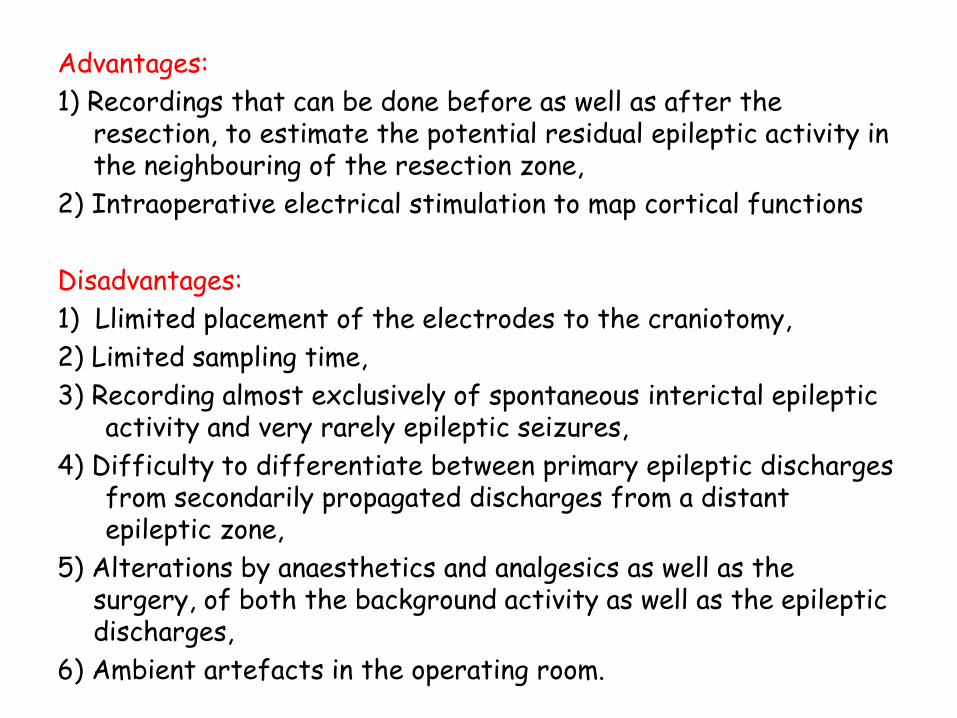
Advantages:
1) Recordings that can be done before as well as after the resection, to estimate the potential residual epileptic activity in the neighbouring of the resection zone,
2) Intraoperative electrical stimulation to map cortical functions
Disadvantages:
1) Llimited placement of the electrodes to the craniotomy,
2) Limited sampling time,
3) Recording almost exclusively of spontaneous interictal epileptic activity and very rarely epileptic seizures,
4) Difficulty to differentiate between primary epileptic discharges from secondarily propagated discharges from a distant epileptic zone,
5) Alterations by anaesthetics and analgesics as well as the surgery, of both the background activity as well as the epileptic discharges,
6) Ambient artefacts in the operating room.

fMRI
• Functional MRI (fMRI) methods use currently standard MRI scanning hardware to detect changes in regional blood flow and metabolism that accompany regional brain activation.
• Major applications of fMRI in epilepsy include the localization of task-correlated language and memory function, and the localization of ictal and paroxysmal phenomena.
• Language lateralization by fMRI provides comparable results to intracarotid amobarbital testing.

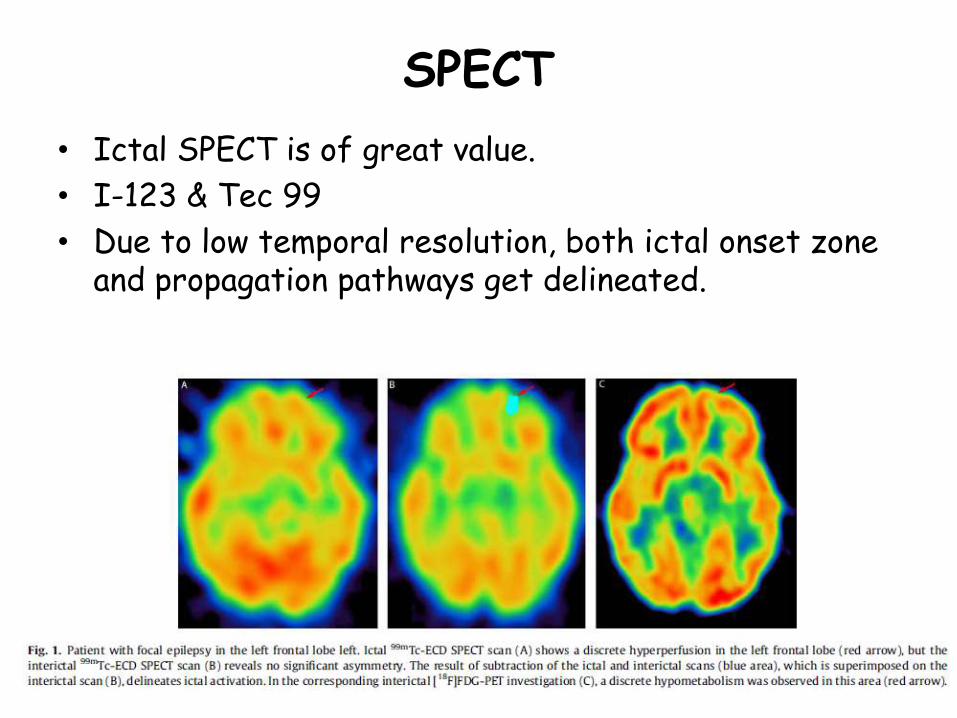
SPECT
• Ictal SPECT is of great value.
• I-123 & Tec 99
• Due to low temporal resolution, both ictal onset zone and propagation pathways get delineated.
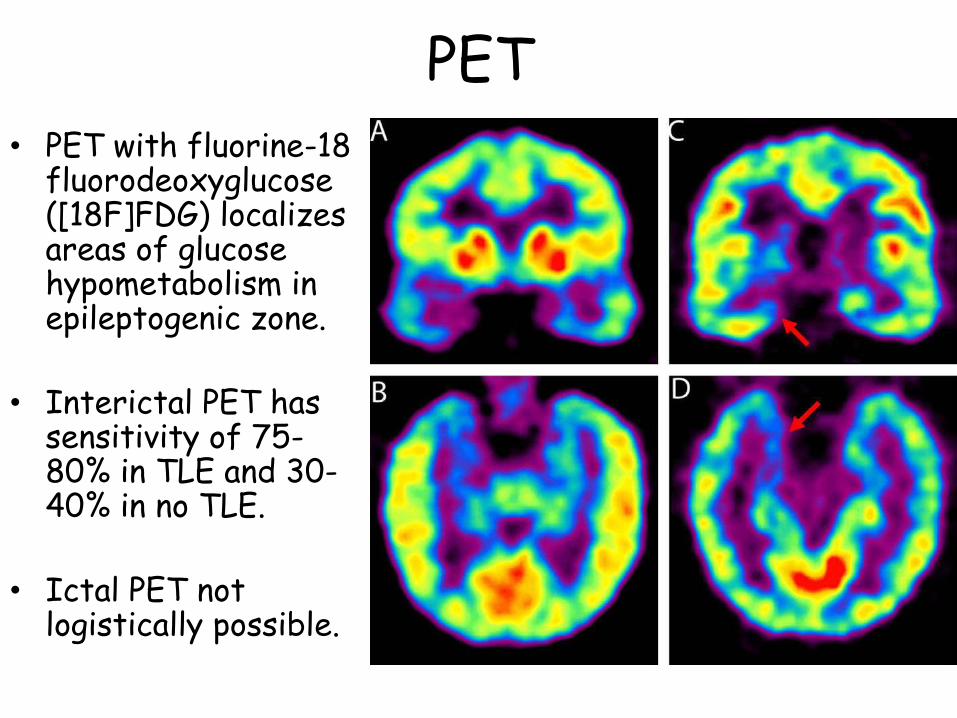
PET• PET with fluorine-18
fluorodeoxyglucose([18F]FDG) localizes areas of glucose hypometabolism in epileptogenic zone.
• Interictal PET has sensitivity of 75-80% in TLE and 30-40% in no TLE.
• Ictal PET not logistically possible.
Neuropsychologic evaluation & WADA Test
• For improvement of QoL:
1. Optimum resection of Seizure focus.
2. Minimal post operative neurological deficits.
Factors predicting good seizure outcome - presence of MRI abnormalities, extent of resection and the Wada Memory Asymmetry (WMA) score
Factors predicting post op cognitive decline - age at onset of seizures, side of surgery, preoperative neuropsychological test performance, presence or absence of MRI abnormalities, and the WMA.

Aims of Neuropsychological Testing:
1) Identify any pre-existing cognitive deficits.
2) Whether the deficits are concordant with the suspected epileptogenic focus.
3) If the suspected epileptogenic focus subservesimportant skill with no apparent deficits.
WADA Test:- Developed by Juhn Wada to establish speech dominance prior to temporal lobe resection .
Test extended to evaluate memory function also.
Modification – Usage of other agents Lignocaine, Etomidate instead of or along with amobarbital.
WMA – WADA Memory Assymetry.
Key Considerations for Surgery
1. Is a structural lesion identified? (MRI)
2. Is an epileptogenic zone identified? (EEG, functional imaging)
3. Are the lesion and epileptogenic zone concordant?
4. Location? Relationship to eloquent cortex? (MR landmarks, functional imaging, Neuropsychologic evaluation, WADA)
5. Focal or extensive? Single or multiple? Unilateral or bilateral?
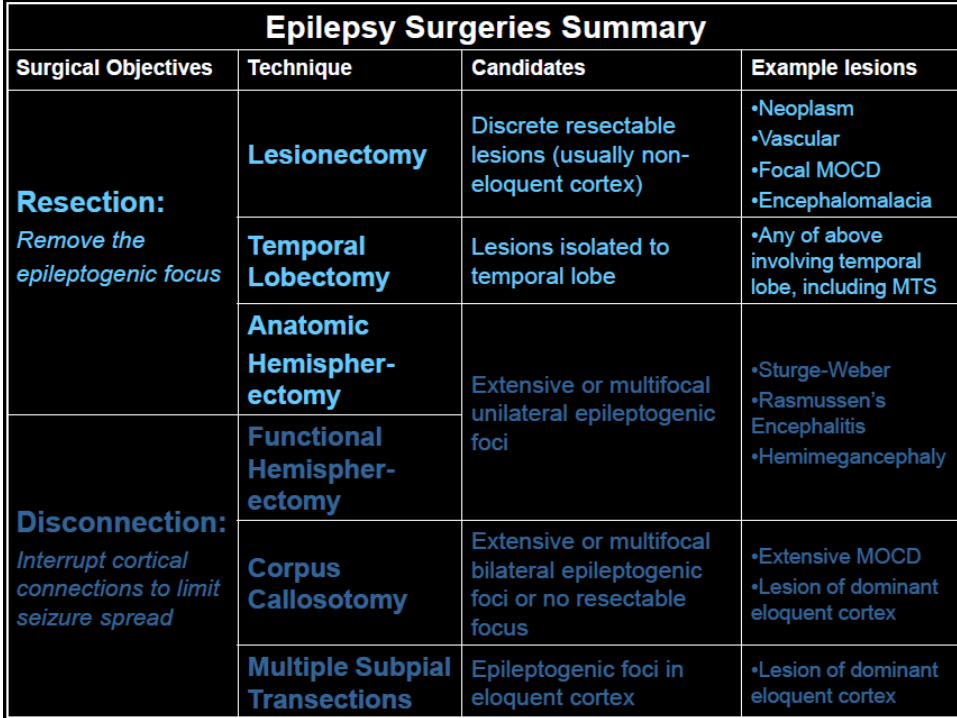
Common Types of Epilepsy Surgery
Goals of surgery: • To resect the epileptogenic zone, OR • To disconnect avenues of seizure spread
Types of surgery • Lesionectomy• Temporal Lobectomy• Hemispherectomy • Corpus Callosotomy• Multiple Subpial Transections• Radiosurgery• Vagal nerve stimulators

Lesionectomy
Lesions:1) FCD2)Tumors3)Vascular malformations

Temporal Lobectomy
Selective Amygdalohippocampectomy Anterior Temporal Lobectomy
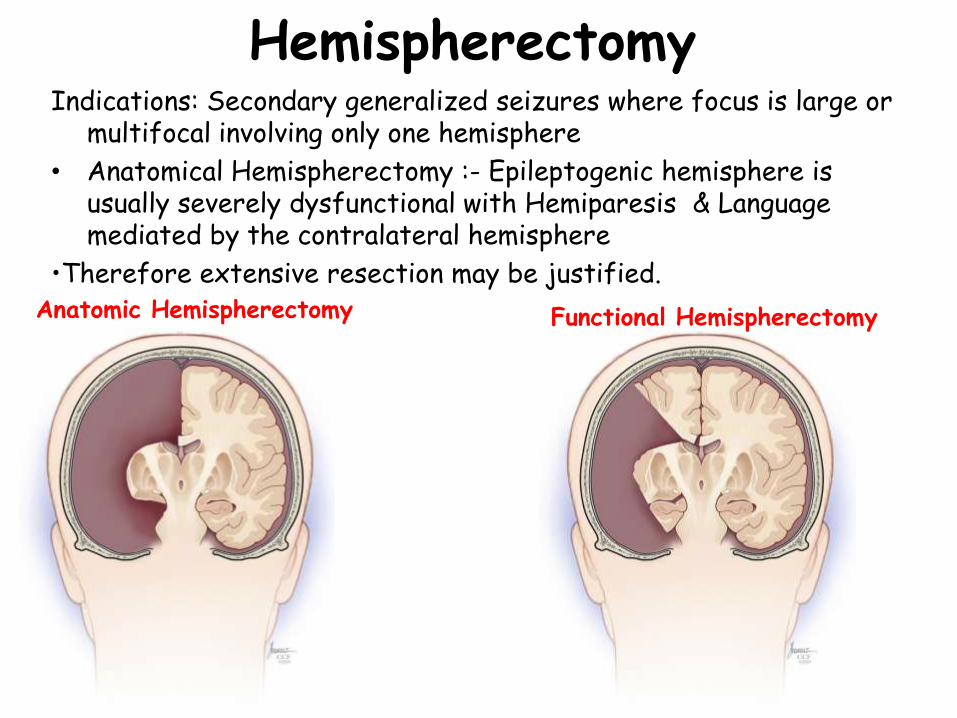
HemispherectomyIndications: Secondary generalized seizures where focus is large or
multifocal involving only one hemisphere
• Anatomical Hemispherectomy :- Epileptogenic hemisphere is usually severely dysfunctional with Hemiparesis & Language mediated by the contralateral hemisphere
•Therefore extensive resection may be justified. Anatomic Hemispherectomy Functional Hemispherectomy
• Functional Hemispherectomy:- A “window” of cortex may be removed to then make the appropriate white matter transections.
White matter tracts that are disconnected
–Corpus Callosum
–Coronal radiata/internal capsule
–Fornix
–Anterior Commisure
–Outflow tracts of the amygdala
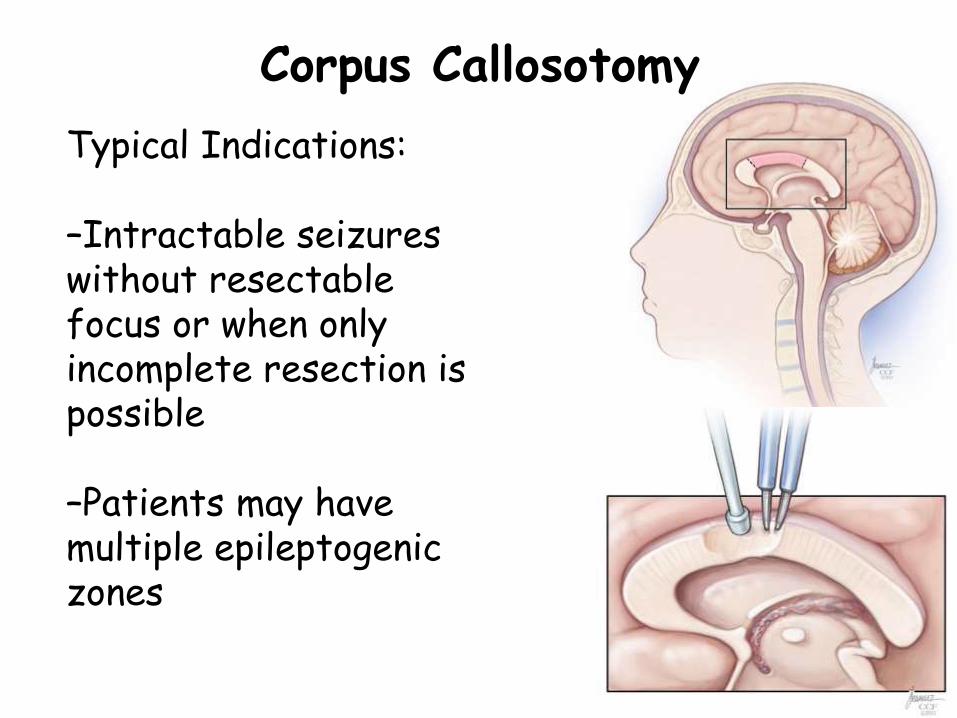
Corpus Callosotomy
Typical Indications:
–Intractable seizures without resectablefocus or when only incomplete resection is possible
–Patients may have multiple epileptogenic zones
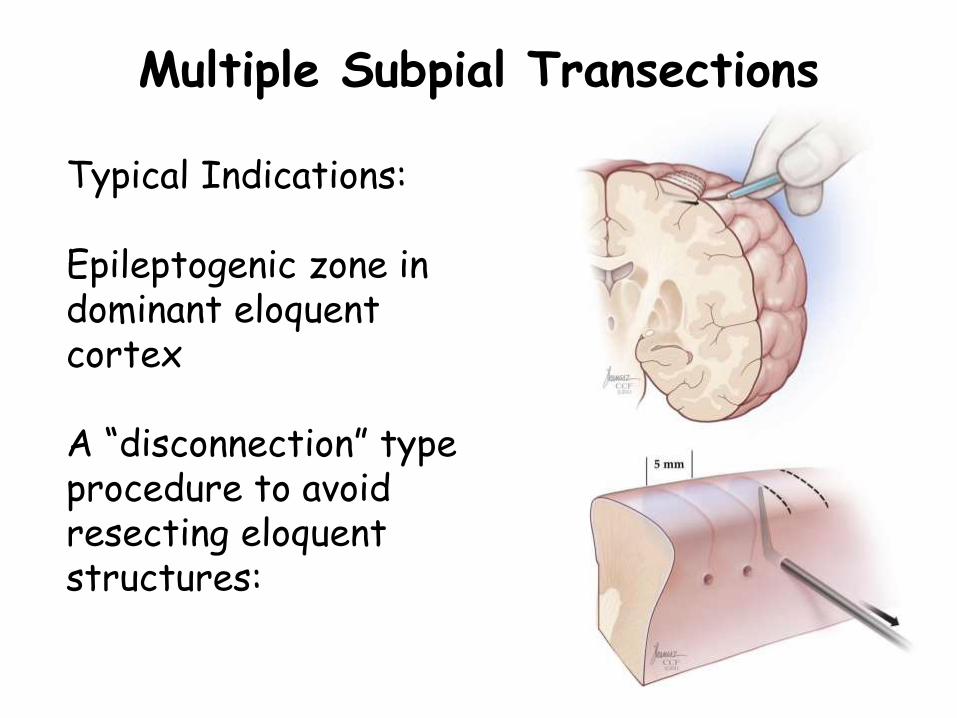
Multiple Subpial Transections
Typical Indications:
Epileptogenic zone in dominant eloquentcortex
A “disconnection” type procedure to avoid resecting eloquent structures:

Vagal Nerve Stimulation
• Simple device with two electrodes anchored and looped around the mid-cervical portion of left vagusnerve.
• Causes on demand summation to abort or deintensifyoncoming seizures.
• Indications: Medically intractable seizures in >12 yrs old patient who is not suitable or willing for surgical management.
• Adverse effects: Laryngeal irritation; Hoarseness; Cough; SOB in COPD; Change in voice quality; Bradycardia; Periodic apnoea; Cardiac arrest
• To be careful in MRI, Monopolar diathermy.

Anaesthetic Considerations
• Anaesthesia for ECog Monitoring:1) Effect of Anaesthetic agents on Ecog output.2) Usage of agents and techniques to increase
epileptiform activity (Opioids, Hyperventilation, low dose Methohexital)
3) Awake craniotomy is the best option.
• Anaesthesia for Surgeries near eloquent cortex:1. Anaesthetic technique – Awake craniotomy with
conscious sedation or asleep-awake-asleeptechnique with intraop neuropsychological monitoring of the patient.
2. General Anaesthesia with traditional anaesthesiapractice.

• Common Anaesthetic regimens for Awake craniotomy:-
1) Scalp block and Incision area field block + Propofol/ Opioid/ Dexmedetomidine infusion for sedation.
2) Scalp block + Asleep –awake-asleep technique using LMA as airway control.

Awake Craniotomy vs. GA
• Gupta et al (2007) studied 53 patients with intrinsic eloquent cortex lesions and compared Awake craniotomy vs GA for excision of such lesions (with electrophysiologic guidance).
• They found:
1) More than 90% tumor excision was observed in 57% patients in awake group versus 73.7% in GA group
2) Mean operative time, blood loss was found to be was found to be less in GA group patients than in awake group.
3) Better tumor cytoreduction, neurological improvement was seen in GA group (motor improvement in 35.7%, speech improvement in 62.5%) than in awake group patients (motor improvement in 18.7%, speech improvement in 14.3%) – in immediate postop, with no difference at 3 mths.
However only significant difference was for duration of surgery parameter.

Thank You





























