Embed Size (px)
Citation preview

Seizure &
EpilepsyProf. Nabil Khalil

Definitions

Seizure A sudden wave of synchronous
electrical activity in brain that usually affects how a person feels or acts for a short time.
Some seizures can hardly be noticed, while others are totally disabling.

Epilepsy A condition that affects central
nervous system (CNS) had at least 2 seizures not caused by some known
medical condition like alcohol withdrawal or extremely low blood sugar.
not indicate anything about the cause of the seizures, what type they are, or how severe they are.

Momentary loss of consciousness
Fit Faint Fake(False)

Transient loss of consciousness
Déjà vuJamais vuAphasiaOlfactory auraEpigastric sensationTongue bitingPost event deliriumFocal neurodeficit
Light-headednessSweatingProlonged standingPrecipitants eg.micturitionChest painPalpitationSlow heart rateLow blood pressure
History and Physical Witness account
AphasiaDeliriumHead turnAutomatismPosturingConvulsionPostictal delirium
Myoclonus or convulsionafter pallor,sweating and collapse
PallorSweatingSlow pulseLow BP
Syncope Seizure
Convulsive syncopeSyncope Seizure

Character Syncope Epileptic seizure
Position
usually upright any
Time daytime day or nighttime
Color pallor normal or cyanotic
Aura dizziness, visual blurring
possible specificaura
Autonomic common uncommon
Duration brief brief or prolonged
Incontinence rare more common

Character Syncope Epileptic seizure
Motor activity occasionally brief tonic seizure or
clonic jerks
variable
Automatism none absence,CPS
Disorientation, posictal
rare can occur withGTC,CPS

Nonepileptic causes for spells
Physiologic Tremor Vasovagal syncope Cardiac arrhythmias Migraine Medication adverse effects Transient ischemic attacks Autonomic dysfunction

Nonepileptic causes for spells
Psychologic Anxiety Panic attacks Mood disorder Personality disorder Psychosis Somatiform illness Psychogenic seizures

Phase of seizures
Preictal phase or aura or warning Ictal phase : simple or complex partial or
generalized tonic-clonic seizure Postictal phase or recovery period : last
from seconds to minutes to hours

Precipitants of seizure
Sleep and lack of sleep
Drugs and alcohol
Intercurrent illness : infection, fever
electrolyte imbalance
Menstruation
Stress and worry
Other precipitants-reflex epilepsy

Classification of seizure
Partial (focal, localized) seizures
Generalized seizures (convulsive or non-convulsive)
Unclassified epileptic seizures

Partial (focal, localized)seizures
1. Simple partial seizures (preserved consciousness)
2. Complex partial seizures (impaired
consciousness)
3. Partial seizures evolving to secondarily
generalized seizures

1. Simple partial seizures
(preserved consciousness)
With - motor signs
- somatosensory or special
sensory systems
- autonomic symptoms or signs
- psychic symptoms

2. Complex partial seizures (impaired
consciousness)
- Simple partial onset followed by
impairment of conscious
- With impairment of consciousness at
onset

3. Partial seizures evolving to
secondarily generalized seizures
- Simple partial seizures evolving to
generalized seizures
- Complex partial seizures evolving to
generalized seizures
- Simple partial seizures evolving to complex
partial seizures evolving to generalized
seizures

Generalized seizures (convulsive
or nonconvulsive)
- Absence seizures
Typical absences
Atypical absences
- Myoclonic seizures
- Clonic seizures
- Tonic seizures
- Tonic-clonic seizures
- Atonic seizures (astatic seizures)

Unclassified epileptic seizures - Neonatal seizures
- Recurrent status epilepticus
- Rare or ‘isolated’ seizures

Epileptic seizure
Seizuretype (s)
Etiology
All clinical andlaboratory dataneuroimaging
Seizuredescription and EEG

Seizure
Idiopathic Generalized
epilepsy likely
Features of focal epilepsy
Epilepsy or PNES
Provoked seizures
EEGEEG
MRI/CT brain
Video EEG
Treat cause +/- AED
PNES=psychogenic non-epileptic seizures
AED=antiepileptic drug

Laboratory investigation
CBC
FBS, BUN, Creatinine
Electrolyte , Liver function test , Ca+2 Mg+2
Electro-encephalography (EEG)
Video EEG
Neuroimaging : CT Scan, MRI, MR Spect, PET
Special investigation : ammonia, lactate , pyruvate etc.

Electroencephalogram

What value is the EEG?
Add weight to the clinical diagnosis
Aid classification of epilepsy
Detection of the structural brain lesion.

EEG
30 minute interictal EEG –useful when clinical suspicion of epilepsy
Timing is important Within 24 hr of generalized convulsion: 50%
have abnormal EEG First 48 hr: 21-34% have epileptiform activity
Sleep EEG or sleep-deprived EEG might increase diagnostic yield

Normal EEG

Primary generalized epilepsy—ictal EEG

Primary generalized epilepsy- interictal EEG

Burst of generalized spike and wave discharges—typical absence seizure

EEG monitoring

Video Monitoring
Helpful in determining nature of seizure disorder (epilepsy, convulsive syncope, or psychogenic seizures)

Indication for neuroimaging in patients with seizures
Partial seizure
Late onset unprovoked seizure (age > 25)
Unexplained neurological signs
Focal slow waves EEG
poor control or new symptoms / signs

Neuroimaging
In the absence of trauma: CT and MRI brain for patients presenting with suspected first unprovoked seizure or with a focal neurological deficit.
MRI is preferable for looking for neuronal migrational disorders, major malformations, vascular anomalies, tumors

The causes of epilepsy Genetic factor Congenital abnormalities Trauma and the effect of craniotomy CNS infection Cerebrovascular disease Cerebral tumors Alzheimer’s disease and other degenerative
disease Others

Neurocysticercosis

Cerebral infarction

Intracerebral hemorrhage

Brain tumor or metastasis

Lt mesial temporal sclerosis

Cortical dysplasia

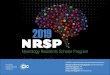
52 year old woman with intractable seizure
PET scan

PET using F-18 FDG-- Decreased FDG uptake in both temporal lobes, right worse then left but otherwise relatively symmetric

What to do?Generalized seizure
Loosening the patient’s clothing Lower the patient gently to the floor, turn them
onto their side and cushion head Nothing is put into the mouth Remove any items that could cause injury

What to do? ---Generalized seizure
When the seizure is over, allow the patient to rest or sleep
If they are able to return to their feet, help them home
Obtain medical help if they continue to experience breathing problems once the seizure is over, or if the seizure lasts a long time(over 10 mins), or when another attack quickly follows the first

What to do?
Partial seizures Stay with the patients throughout the seizure Protect them from any dangerous object Taking care not to restrain them in anyway

First aids

Treatment

------------------------------
Treatment

Choose a drug : considering the following factors The seizure type and prognosis Age The possibility of pregnancy Toxicity Drug interaction Price

The recurrence risk follow a first unprovoked seizure
50% recurrence occur within 3 months
Over 10% within 2 years of initial seizures
twice as likely to have another seizure if you have a
known brain injury or brain abnormality.
RISK OF RECURRENT SEIZURE

RISK OF RECURRENT SEIZURE (cont)
If you do have two seizures, there's about 80% chance that you'll have more.

Factors predictive of a high rate of seizure recurrence after the first
unprovoked seizure
Abnormal neurologic status by NE or imaging
EEG abnormalities (especially epileptiform)
Partial seizures

Counseling before treatment
1. Aims of treatment
2. Prognosis and duration of the
expected treatment
3. Importance of compliance
4. Side effects

Starting antiepileptic treatment Prospective risks Usual clinical
Factors that may modify of epilepsy practice usual practice Single seizure No treatment Progressive cerebral disorder
Clearly epileptic EEG
2 or more seizure Monotherapy Seizures widely separated in time (> 1 year)
Identified precipitating, factors (eg, drugs,
alcohol,reflex stimuli)
Probability of poor compliance (eg, personality disorder) Attitude of patients/parents

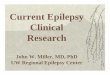
Antiepileptic Drug Development
1840 1860 1880 1900 1920 1940 1960 1980 20000
5
10
15
20
BromidePhenobarbital
Phenytoin Primidone
Ethosuximide
Sodium Valproate
BenzodiazepinesCarbamazepine
VigabatrinZonisamide
LamotrigineFelbamate
GabapentinTopiramate Fosphenytoin
OxcarbazepineTiagabine
Levetiracetam
More
Calendar year
Antiepileptic drugs
Pregabalin

First-line choice of AEDs according to seizure type
Seizure type First line
Absence (typical and atypical)
VPA, LTG
Myoclonic VPA
Tonic-clonic VPA, CBZ, PHT, PB
Atonic VPA
Simple and complex partial, with or without secondary generalization
CBZ, PHT, PB,OXC,LTG,TPM, GBP
Unclassifiable VPA

Advantages of Monotherapy
Better seizure controlReduced side effectsAbsence of drug interactionsReduced teratogenic effectsBetter complianceReduced cost of medication Improved quality of life

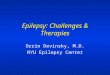
Expected outcomes of AED therapy
Well controlled
65%
Unsatisfactorilycontrolled
35%
Well controlled
10%
Unsatisfactorilycontrolled
25%
Well controlled
5%
Unsatisfactorilycontrolled
20%
Monotherapy
Add-on therapy
Multiple drug therapy

Managing newly diagnosed epilepsy
Newly diagnosed epilepsy
Seizure freeFirst drug
Second drug
Refractory
Surgical assessmentRational duotherapy
Seizure free
47%
13%

Adverse effect of AED
Dose related Idiosyncratic / allergic Chronic toxicity Teratogenicity

Older AEDs
Drugs Side effects
CBZ Tegretol
Diplopia, headache, dizziness, N/V, rash, mild leukopenia, mild hyponatremia
PHT Ataxia,nystagmus, dysarthria, somnolence,gingival hyperplasia, hirsutism, acne, facial coarsening, folate, deficiency, osteopenia, peripheral neuropathy, cerebellar atropy
VPA Dose-related tremor, weight gain,loss of hair, menstrual irregularities, PCOS, stupor and encephalopathy(rare), hepatotoxicity
PB Somnilleta
Sedation and behavioral problem(depression, agitation, hyperactivity)
CZP clonezipzm revotril
Sedation, ataxia, behavioral changes(depression)

AED interactions
CBZ : autoinduction, VPA, PHT, -PB PHT : CBZ, VPA, PB PB : CBZ, VPA, PHT VPA : CBZ, PB, PHT

AEDs Drug interaction with AED and other drugs: via
effect on hepatic CYP450 enzyme system PB, primidone, PHT, CBZ induce CYP enz. : Accelerate breakdown of many prescribed
lipid-soluble drugs metabolized by the same system: OCP, cytotoxic, antiarrythmic, warfarin
VPA is a weak CYP enz. Inhibitor: Slow clearance of other AEDs such as PHT,
LTG. Newer AEDs : less likely to interfere with
hepatic metabolism. GBP, LEV,PGB,VGB do not undergo hepatic
metabolism

Newer AEDs
Adjunctive treatment of refractory epilepsy
Some of these AEDs: LTG, GBP, OXC, TPM have also demonstrated efficacy as monotherapy

Effects of phenytoin levels
Level (mg/ml) Effect
0-10 Subtherapeutic
10-20 Therapeutic
20-30 Mild toxicity; nystagmus, mild ataxia
30-40 Moderate toxicity ; ataxia prominent
> 40 Severe toxicity; ataxia, conscious -
ness, encephalopathy

Potential Causes of Treatment Resistant Epilepsy
Diagnostic errors: Non-epileptic events Wrong diagnosis of seizure types/ epileptic
syndrome Missing of underlying causes/lesions
Patient’s errors: Non-compliance Inappropriate life style, inappropriate metabolism

Potential Causes of Treatment Resistant Epilepsy
Treatment errors: Wrong choice of drugs Less optimal doses of drugs Inadequate dosing schedules Antiepileptic drug toxicity
Disease itself: Treatment resistant epilepsy metabolic disorder

Absolute
requirement 2-3 years free of all
seizures
Patient’s informed
agreement
Stopping antiepileptic treatment

Factors in favour Childhood epilepsy Primary generalized epilepsy
Absence of cerebral disorder
Short duration of epilepsy
Normal EEG Non-driver

Adverse prognostic factors
Symptomatic etiology, identifiable brain pathology Partial-onset seizures or Atonic seizures Late-onset or first-year epilepsy Specific epilepsy syndrome (particularly JME) Abnormal EEGs Multiple seizure types in the same patient Additional mental or motor handicap Long duration or severe epilepsy prior to treatment Poor initial response to treatment

Features common to the surgically privileged seizure disorders
Presence of a well-circumscribed structural lesion on the MRI (lesional epilepsy)
Presence of well-localized interictal epileptiform discharged on the EEG
Clinical features of habitual seizures indicating focal onset
Absence of discordance between above feature
Focus localized by above features is surgically accessible and involves little or no eloquent cortex
Absence of other potentially epileptogenic abnormalities

Status epilepticus
A condition in which epileptic activity
persists for 30 minutes or more

Common etiologies for status epilepticus in children and adolescents
Idiopathic Acute symptomatic
Electrolyte disturbance Encephalitis Head trauma
Remote symptomatic Past stroke CNS infection Cerebral palsy
Progressive encephalopathy Tuberous sclerosis Other neurodegeneration
Febrile

Status epilepticus management



Epilepsy and pregnancy
Seizure control Obstetric complication
Neonatal outcome

Neonatal outcome Risk of seizure
(3 times > normal population)
developmental outcome
congenital anomalies 4-8%
(2-3 times > normal population)

The most common malformation
Congenital heart disease
orofacial cleft
neural tube defect
intestinal atresia
urogenital defects
Neural tube defect

Fetal antiepileptic drug syndrome (minor anomalies)
Facial dysmorphism
Distal digital hypoplasia
Developmental delay
Mental deficiency

Factors affecting neonatal outcome
AED
genetics
folic acid
socioeconomic
maternal health

Recommendations for managing Women With Epilepsy
Before Conception
Educate the family regarding risks
Review classification of epilepsy
Determine most appropriate medicine for
seizure control

Determine need for continued medication
- may discontinue if seizure-free for 2 or more
years
- do not discontinue medication if epilepsy
syndrome
suggests continued need for treatment
Reduce medicines to monotherapy, lowest dose
possible
Start folic acid 1 mg/day
Eliminate other risk factors – smoking, drugs,
alcohol

After conception
Do not change antiepileptic medication Refer for prenatal care Prescribe vitamins, including folic acid Check ‘free’ drug levels every trimester and change
doses as needed Evaluate for neural tube defects at 12 to 16 weeks
(ultrasound, alpha-fetoprotein, amniocentesis)

Consider vitamin K predelivery Check antiepileptic drug levels prior to
delivery and increase doses if needed

After Delivery
Check levels
Examine infant

Thank you