Embed Size (px)
DESCRIPTION
Keynote presentation from the TSA Internatonal Conference 2012 sharing psychological and organizational research on health and social care partnerships
Citation preview

Health and Social Care Partnerships:Can they really work?
Jim McManus, CPsychol, CSci, AFBPsS, FFPH, MCIPDDirector of Public Health
Hertfordshire County Council/NHS Hertfordshire

Sometimes it feels like another planet

Five partnership meetings this week

What do you mean the partnership plan was due today?

Context – change and transformation Financial challenges Traditional barriers and approaches have
delivered some gains others have remained elusive and barriers
often seem embedded between agencies. The perennial problem - some partnerships
building a “third culture” which competes with the existing cultures.
Partnerships are a given because they seem to be a necessity

The cynics view of partnerships A loose confederation of warring tribes
A group of people all united, but against what nobody really knows
A group of people whose hands are so deeply in each others budgets they can’t get out again
A set of people who have come together to discuss governance while people die around them
Take minutes and waste hours

Content
learning from experience, filtered through research evidence on
culture and partnerships identify some critical success factors
where partnerships work or do not. Informed by behavioural sciences

The NHS structure from April 2013 – a very DH centrist view
ParliamentFundingAccountability Department
of Health
NHS Commissioning
BoardCQC
+ HealthWatch EnglandMonitor
Providers
Patients and PublicLocal Health Watch
Local Authorities + PHClinical
CommissioningGroups
Localpartnership Contract
Accountability for results
Licensing
“Health & Wellbeing Boards”
CommissioningSupport Services

Environmental Health& Regulatory Services NHS
Police, Fire, Community Safety Third Sector and
Community Bodies
Public Health England
Specialist Public Health Agencies with Major Public Health Roles
NHS Public Health (moving into HCC)
County CouncilDistrict Councils

The Literature Partnerships vague multi-meaning concept
(Glendinning,2002) Evaluation needs to take account of multiple outcomes
(Gillies, 1998) Some positives but depends on behavioural and
governance factors (Kodner, 2006) Co-ordination across systems is big on most country
agendas in West (Leichsenring ,2004) Wicked issues to be addressed (Ailsa Cook, Alison Petch,
Caroline Glendinning, Jon Glasby,2007) Evidence not always clear (Walid El Ansari, Ceri J. Phillips,
Marilyn Hammick,2001) So why not just redesign the system?

Research in the commercial sector Salience of Value Salience of strategic benefit (money, market
share, customer) Structures and governance fits strategic benefit (Rondinelli and London, 2003;Waddell & Brown,
1997) Private sector – Intellectual Property Issues Public Sector – Inter-professional issues

Public sector partnerships research Assets
Understanding key issues and drivers Focused action
Problems Far too process and governance obsessed Doesn’t learn lessons from commercial sector Takes on a life of its own

A small sample….

Summary A problem in many nations Understand what you want to
achieve They can work They often don’t Blunt instrument As many positives as negatives No one got any better ideas? And no, we won’t reorganise the
universe so get on with it – partnerships are a necessity in some areas of public life
Dr Thomson hadn’tQuite undertstood theTelemedicine project

So how do we make it happen?
A public health perspective population, outcome, salience, Intervention System capabilities
Lifecourse of the human person
Lifecourse of the partnership

Admit your limits of knowledge and competence – it’s liberating!

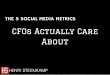
Contributors to overall health outcomes are in multiple agency control
Smoking 10%
Diet/Exercise 10%
Alcohol use 5%Poor sexual health
5%
Health Behaviours 30%
Education 10%
Employment 10%
Income 10%
Family/Social Support 5%Community Safety 5%
Socioeconomic Factors 40%
Access to care 10%
Quality of care 10%
Clinical Care 20%
Environmental Quality 5%
Built Environment
5%
Built Environment
10%
Source: Robert Wood Johnson Foundation and University of Wisconsin Population Health Institute. Used in US to rank counties by health status
While this is from a US context it does have significant resonance with UK Evidence, though I would want to increase the contribution of housing to health outcomes from a UK perspective.

Partnerships don’t think often enough about timeframes of yield
Years
0 1 5 10 15
Planning
Education
Vitamin Supplements
Air Pollution
Decent Homes
Jobs
Primary Care
20
CVD Events
Self Care
Vitamin D and TBRickets
CVD Events
Acute Bronchitis Admissions
RespiratoryMental Health overcrowding educational attainment
Life Expectancy
Healthier space use Changing culture of activity
Life ExpectancyMental Health

The Lifecourse impact of health, little evidence most partnerships think of this

Degrees of PartnershipCheminais, 2008 Coexistence – clarity as to who does what and with whom.
Co-operation – pooling the collective knowledge, skills and achievements available.
Co-ordination – partners planning together; sharing some roles and responsibilities, resources and risk-taking; avoiding overlap.
Collaboration – longer-term commitments with organizational changes bringing shared leadership, control, resources and risk-taking. Partners from different agencies agree to work together on strategies or projects, each contributing to achieving shared goals.
Co-ownership –different agencies commit themselves to achieving a common vision, making significant changes in what they do and how they do it.

Blast from the past 2003, republished 2011 Innovative partnerships Blend of private and public
sector insights Where this has been used http://thepartneringinitiati
ve.org/w/resources/toolbook-series/the-partnering-toolbook/

From thePartneringToolbook

Critical success factors

Critical Success Factors – the people Psychological Contract
Within and between agencies and individuals
Clarity of outcomes Clarity of processes Clear advantage to each
agency Control and governance fit
for purpose

Critical Success Factors 2 – the why! Understand need Identify the priorities to meet that need Understand timescale, yield and salience Identify effective candidate interventions Identify who is best placed to deliver what Implement well - fidelity to the evidence/theory Build from the person not the agency Psychological Contract

A helpful friend for improvement
Tools for service improvement
Available from internet
http://www.goalqpc.com/

Case Finding and targeting using locally designed guidelines and protocols
Intervention Components linking NHS with sports for inactive peopleHealth Psychology for intervention design, public health for programme design and leadership, primary care for case finding, screening and referral, sports sector for delivery and also for screening
Clinical Engagement and Support across programme
Public Health, Clinical and Sport Leadership across programme
Behavioural Change Training for Sport and Primary Care Staff
Evaluation including pre and post intervention measures
Call in and Screen using Health Checks (multiple settings)
Regular goal checks and positive feedback
One to one and group support with Sport prescribed. Individual “feeling good, feeling fit” plans made
Ongoing motivation from NHS and from Sports staff to stay on programme