Embed Size (px)
Citation preview

Disorders of Gas ExchangeDisorders of Gas Exchange
Hypercapnia and HypoxiaHypercapnia and Hypoxia

OutlineOutline
Review of normal gas exchangeReview of normal gas exchange (Brief) review of normal oxygen transport(Brief) review of normal oxygen transport HypercapniaHypercapnia HypoxiaHypoxia Example CasesExample Cases

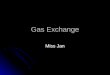
Overview of Gas Exchange in the LungsOverview of Gas Exchange in the Lungs
Adapted from: Costanzo, LS. Physiology, 1st ed. 1998.

Mathematical Description of Gas Mathematical Description of Gas ExchangeExchange
PPaaCOCO22 – Partial pressure of CO – Partial pressure of CO22 in the arterial blood. in the arterial blood.
PPAACOCO22 – Partial pressure of CO – Partial pressure of CO22 in the alveolar gas. in the alveolar gas.
PPaaOO22 – Partial pressure of O – Partial pressure of O22 in the arterial blood. in the arterial blood.
PPAAOO22 – Partial pressure of O – Partial pressure of O22 in the alveolar gas. in the alveolar gas.

Mathematical Description of Gas Mathematical Description of Gas Exchange (cont)Exchange (cont)
Alveolar Ventilation Equation – Primarily Alveolar Ventilation Equation – Primarily describes the relationship between Pdescribes the relationship between PaaCOCO22
and alveolar ventilation.and alveolar ventilation.
Alveolar Gas Equation – Primarily Alveolar Gas Equation – Primarily describes the relationship between Pdescribes the relationship between PAAOO22, ,
FFIIOO22, and P, and PaaCOCO22..

PPaaCOCO22 and the Alveolar Ventilation and the Alveolar Ventilation
EquationEquation
VVCOCO22 = V = VAA x F x FAACOCO22
Many steps…Many steps…
PPaaCOCO22 = (V = (VCOCO22 x P x PII) / V) / VAA
Rate of CORate of CO22 production by the body = production by the body =
Rate of CORate of CO22 removal by the lungs removal by the lungs

PPAAOO22 and the Alveolar Gas Equation and the Alveolar Gas Equation
Rate of ORate of O22 consumption by the body = consumption by the body =
Net rate of ONet rate of O22 entering the lungs entering the lungs
Many steps…Many steps…
PAO2 = [FIO2 (PI – PH2O)] – (PaCO2 / RQ)

The A-a GradientThe A-a Gradient
In general terms, the A-a gradient is a In general terms, the A-a gradient is a measure of how effectively oxygen that is measure of how effectively oxygen that is in your alveoli moves into your pulmonary in your alveoli moves into your pulmonary vasculature.vasculature.
The A-a gradient = PThe A-a gradient = PAAOO22 – P – PaaOO22
Normal A-a gradient Normal A-a gradient ≈ (age + 10) / 4≈ (age + 10) / 4

Oxygen TransportOxygen Transport
Oxygen is carried in the blood in 2 forms:Oxygen is carried in the blood in 2 forms:
Dissolved ODissolved O22 (~2% of total O (~2% of total O22 content) content)
OO22 bound to hemoglobin (~98% of total O bound to hemoglobin (~98% of total O22 content)content)

Oxygen Transport (cont)Oxygen Transport (cont)
Total O2 content of blood (CaO2) =
+
Dissolved O2
O2 bound to hemoglobin

Oxygen Transport (cont)Oxygen Transport (cont)
Total O2 content of blood (CaO2) =
PaO2 Solubility of OSolubility of O22 in blood in blood
+
OO22 binding binding
capacity of Hbcapacity of Hbx
x
x[Hb][Hb] O2 sat

Oxygen Transport (cont)Oxygen Transport (cont)
Total O2 content of blood (CaO2) =
PaO2 Solubility of OSolubility of O22 in blood in blood
+
OO22 binding binding
capacity of Hbcapacity of Hbx
x
x[Hb][Hb] O2 sat
(During Normal Gas Exchange)

Oxygen Transport (cont)Oxygen Transport (cont)
Total O2 content of blood (CaO2) =
100 mmHg 0.003mL O0.003mL O22___ ___
100mL blood 100mL blood ∙∙ mmHg mmHg+
1.34mL O1.34mL O22
1g 1g
HbHb
x
x
x15g Hb15g Hb
1dL 1dL bloodblood
0.98
(During Normal Gas Exchange)

Oxygen Transport (cont)Oxygen Transport (cont)
Total O2 content of blood (CaO2) =
0.3mL O0.3mL O22_ _
100mL 100mL blood blood
+
19.7mL O19.7mL O22_ _
100mL 100mL
bloodblood
(During Normal Gas Exchange)
(Dissolved O2)
(Hb-bound O2)

Hypercapnia (Hypercapnia (↑ P↑ PaaCOCO22))
Respiratory failure manifesting as Respiratory failure manifesting as hypercapnia is known as ventilatory failure.hypercapnia is known as ventilatory failure.
Signs of ventilatory failure:Signs of ventilatory failure:
TachypneaTachypnea
AcidemiaAcidemia
Increased pulsus paradoxusIncreased pulsus paradoxus
HyperinflationHyperinflation
Somnolence / Decreased mental statusSomnolence / Decreased mental status

Hypercapnia - EtiologiesHypercapnia - Etiologies
PPaaCOCO22 = (V = (VCOCO22 x P x PII) / V) / VAA
Alveolar Ventilation Equation
VA = RR (VT – VD)
VA – Alveolar Ventilation
RR – Respiratory Rate
VT – Tidal Volume
VD – Dead Space

Hypercapnia - EtiologiesHypercapnia - Etiologies VVCOCO22 x P x PII
RR (VRR (VTT – V – VDD))PaCO2 =
↑VCO2 (Hypermetabolism)
Fever
Seizures
Sepsis
Hyperalimentation
↓RR (Central hypoventilation)
Drugs
Brainstem lesions
Obesity-hypoventilation syndrome
↓VT
Skeletal muscle weakness
Impaired neuromuscular transmission
↓ Lung / chest wall compliance
Airway obstruction
COPD
Asthma
Obstructive sleep apnea
↑VD
Excessive PEEP

Hypercapnia - TreatmentHypercapnia - Treatment
Treat the underlying processTreat the underlying process
Non-invasive positive pressure ventilationNon-invasive positive pressure ventilation
Intubation and mechanical ventilationIntubation and mechanical ventilation

Hypoxia (Hypoxia (↓ P↓ PaaOO22))
Respiratory failure manifesting as hypoxia is Respiratory failure manifesting as hypoxia is known as oxygentation failure.known as oxygentation failure.
Signs of oxygenation failure:Signs of oxygenation failure: TachypneaTachypnea Alkalemia (acidemia if concurrent Alkalemia (acidemia if concurrent ventilatory failure)ventilatory failure) Increased pulsus paradoxusIncreased pulsus paradoxus CyanosisCyanosis Agitation Agitation Somnolence Somnolence

Hypoxia - EtiologiesHypoxia - Etiologies
A-a Gradient = PAO2 – PaO2
Rearrangement: PaO2 = PAO2 – A-a gradient
Alveolar Gas Equation
PAO2 = [FIO2 (PI – PH2O)] – (PaCO2 / RQ)
Substitution:
PaO2 = [FIO2 (PI – PH2O)] – (PaCO2 / RQ) – (A-a gradient)

Hypoxia - EtiologiesHypoxia - EtiologiesPaO2 = [FIO2 (PI – PH2O)] – (PaCO2 / RQ) – (A-a gradient)
↑ A-a gradient
V/Q mismatch
COPD
Pulmonary embolus
Pneumonia
Pulmonary edema
Anatomic shunt
Right to left intracardiac shunts
Pulmonary AVMs
Impaired diffusion
Emphysema
Pulmonary fibrosis
↓ FIO2
Suffocation
↓ PI
High altitude
↑ PaCO2
As above

Hypoxia – TreatmentHypoxia – Treatment
Treat the underlying processTreat the underlying processIncrease FIncrease FIIOO22 with supplemental oxygen with supplemental oxygen
Reposition the body Reposition the body Secretion managementSecretion managementBronchodilationBronchodilationDiuresisDiuresisIncrease mean lung volumeIncrease mean lung volumeReduce OReduce O22 requirement requirement
Consider transfusion if [Hb] < 7.0 g/dLConsider transfusion if [Hb] < 7.0 g/dL

Case 1Case 1
A 35 year old woman is brought to the ER by A 35 year old woman is brought to the ER by ambulance after a friend called 911 and reported ambulance after a friend called 911 and reported an attempted suicide. When paramedics found the an attempted suicide. When paramedics found the patient in her apartment, she was unresponsive, patient in her apartment, she was unresponsive, with several empty pill bottles nearby, including with several empty pill bottles nearby, including vicodin and some antidepressants. Her past vicodin and some antidepressants. Her past medical history is significant only for depression. medical history is significant only for depression. Upon arrival, her vitals are as follows: T=37.2, Upon arrival, her vitals are as follows: T=37.2, HR=62, BP=112/60, RR=5, OHR=62, BP=112/60, RR=5, O22 sat=72% on RA. sat=72% on RA. She has minimal response to painful stimuli, and is She has minimal response to painful stimuli, and is otherwise unresponsive. An ABG shows the otherwise unresponsive. An ABG shows the following: pH=7.15, Pfollowing: pH=7.15, PCOCO22=85, P=85, POO22=36.=36.

Case 2Case 2
A 48 year old man drives himself to the ER A 48 year old man drives himself to the ER because of shortness of breath that started acutely because of shortness of breath that started acutely 60 minutes ago. He has also noticed mild sharp 60 minutes ago. He has also noticed mild sharp chest discomfort when he takes deep breaths. His chest discomfort when he takes deep breaths. His past history is significant for GERD, for which he past history is significant for GERD, for which he takes ranitidine. His vitals on arrival: T=37.6, takes ranitidine. His vitals on arrival: T=37.6, HR=115, BP=144/84, RR=24, OHR=115, BP=144/84, RR=24, O22 sat=97% on RA. sat=97% on RA.
Although he appears anxious, the remainder of his Although he appears anxious, the remainder of his exam is completely normal. A room air ABG exam is completely normal. A room air ABG shows the following: pH=7.51, Pshows the following: pH=7.51, PCOCO22=28, P=28, POO22=82.=82.

Case 3Case 3While on-call, you admit a 72 year old man with a mild While on-call, you admit a 72 year old man with a mild upper GI bleed, possibly from gastritis, which he has upper GI bleed, possibly from gastritis, which he has known to have had in the past. He has never been to known to have had in the past. He has never been to this hospital before, but he reports his past medical this hospital before, but he reports his past medical problems are limited to diabetes and an MI 6 years problems are limited to diabetes and an MI 6 years ago. He is admitted to a monitored bed and transfused ago. He is admitted to a monitored bed and transfused 2 units pRBCs for a Hct=23%. 6 hours later, a post-2 units pRBCs for a Hct=23%. 6 hours later, a post-transfusion Hct=26%, so 2 more units are ordered. transfusion Hct=26%, so 2 more units are ordered. Midway through the 4th unit, you are called by nursing Midway through the 4th unit, you are called by nursing because the patient has developed some shortness of because the patient has developed some shortness of breath over the past 30 minutes. Although his vitals breath over the past 30 minutes. Although his vitals were initially normal on admission, currently they are: were initially normal on admission, currently they are: T=36.8, HR=102, BP=132/85, RR=28, OT=36.8, HR=102, BP=132/85, RR=28, O22 sat=88% on sat=88% on 2L. On exam, he has bilateral crackles and his heart 2L. On exam, he has bilateral crackles and his heart sounds are normal.sounds are normal.

Case 4Case 4
A 67 year old man with a 100 pack year smoking A 67 year old man with a 100 pack year smoking history is brought to the ER by ambulance due to history is brought to the ER by ambulance due to the development of severe shortness of breath and the development of severe shortness of breath and increased productive cough over the past 24-36 increased productive cough over the past 24-36 hours. He reports 2 previous hospital admissions hours. He reports 2 previous hospital admissions for “lung problems”. His vitals on exam: T=38.2, for “lung problems”. His vitals on exam: T=38.2, HR=110, BP=165/94, RR=32, OHR=110, BP=165/94, RR=32, O22 sat=75% on RA. sat=75% on RA. He has moderate rhonchi and wheezing He has moderate rhonchi and wheezing throughout both lung fields. A room air ABG is throughout both lung fields. A room air ABG is performed: pH=7.29, Pperformed: pH=7.29, PCOCO22= 57mmHg, P= 57mmHg, POO22=46. A =46. A CXR shows increased lung volumes, flattening of CXR shows increased lung volumes, flattening of the diaphragms, and a hazy opacity in the right the diaphragms, and a hazy opacity in the right lung base.lung base.