Embed Size (px)
DESCRIPTION
Are you Struggling to Control of your Diabetes and Weight? People who are overweight or obese are more prone to developing Type 2 diabetes. Those who have Type 1 and Type 2 diabetes with weight problems struggle to control their blood sugar levels. Research shows that people with diabetes find it more difficult to lose weight than those without diabetes. Weight loss significantly improves blood sugar control and also reduces the risk of getting complications from diabetes. However, whilst attempting to lose weight, people with diabetes find it hard to restrict their intake of food since eating less may trigger hypoglycaemia (low blood sugar). All these facts explain the need for specialist input in management of weight in people with diabetes. This Slideshow gives you insight to Diabesity For more information please visit http://www.simplyweight.co.uk Articles http://www.simplyweight.co.uk/articles/ Videos http://www.simplyweight.co.uk/video/ Blogs http://simplyweight.co.uk/blogs/ Forum http://www.simplyweight.co.uk/forum/forum.php Contact Us http://www.simplyweight.co.uk/how-to-contact-us/
Citation preview

Diabesity - 21st century pandemic
Diabesity is now the single greatest contributor to chronic disease
Obesity will soon become the leading cause of death

Aims of this forum
Open forum to discuss management of Diabesity
Forum will be interactive
New studies in this field will be presented
Emerging treatments in Diabesity will be discussed

Aims of this forum
External speaker
Discussion of case studies
Website to be launched
Expand to regional forum and National

Meeting Three monthly
Clinical leads in Primary care (Two doctors and two nurses)
Members will be contacted via email

Obesity can alter the natural history of T2DM
by virtue of the role of visceral fat with its
Proinflammatory
Prothrombotic
Proinsulin resistant environments.







Ramlo-Halsted BA, et al. Prim Care 1999;26:771–789.
Impaired insulin production & secretion
The underlying defects: insulin resistance and -cell dysfunction
Insulin resistance (IR)
- Hyperinsulinaemia - Normal glucose tolerance
IR + declining insulin levels + impaired glucose tolerance
- Failure of β-cell to adapt to IR
Impaired responsivenessto insulin
↑FFA levels
Sedentary lifestyle
Diet Obesity
Type 2 diabetes
Glucotoxicity
-cell dysfunction
Genetic predispositions

Physiological functions
• Incretins are hormones secreted by intestinal endocrine cells in response to nutrient intake
• Glucose-dependent insulin secretion, postprandial glucagon suppression and slowing of gastric emptying

Incretins were identified when it was observed that orally ingested glucose provoked a higher insulin response than comparable glucose administered intravenously
This well-described phenomenon is called the ‘incretin effect’
The incretin effect accounts for ~60% of total insulin release following a meal

The two primary incretin hormones are GLP-1 and GIP
• Circulating GIP and GLP-1 levels are regulated by multiple factors2
– Low in the basal fasting state, rise rapidly following a meal due to neuronal, neuroendocrine, and direct nutrient stimulation of intestinal cells
1Wei Y, et al. FEBS Lett 1995;358:219–224; 2Drucker DJ. Diabetes Care 2003;26:2929–2940.
GLP-1 GIP30 amino acid peptide1 42 amino acid peptide2
Synthesised and released by L cells of ileum and colon2
Synthesised and released from K cells of jejunum and duodenum2
Sites of action1:
Pancreatic β-cells and α-cells
GI tract
CNS
Lungs
Heart
Sites of action2:
Pancreatic β-cells
Adipocytes

The incretin effect is reduced in patients
with Type 2 diabetes
0
20
40
60
80
0 30 60 90 120 150 180
Time (min)
** *
** **
0
20
40
60
80
0 30 60 90 120 150 180
Time (min)
Oral Glucose

GLP-1 is a more potent insulin secretagogue than GIP in patients with type 2 diabetes
Mean (SE); N = 18.Nauck MA, et al. J Clin Invest 1993;91:301–307.
Low-dose GIP or GLP-1 (7–36 amide)High-dose GIP or GLP-1 (7–36 amide)
GLP-1 (7–36 amide)GIPHyperglycaemic clamp
Ins
uli
n (
pm
ol/
L)
0 30 60 90 120 150 180 2100
250
500
750
1000
1250
1500
17502000
Time (min)0 30 60 90 120 150 180 210
0
250
500
750
1000
1250
1500
17502000
Time (min)
Patients with type 2 diabetesNormal subjects

Therapeutic potential
GIP secretion is normal, but its action is diminished
GLP-1 secretion is diminished, but its action is preserved
Glucagon, secreted from pancreatic α-cells, is also elevated in type 2 diabetes
GLP-1 suppresses glucagon secretion from pancreatic α-cells in a glucose-dependent manner, suppressing hepatic glucose outputt

GLP-1 effects in humansUnderstanding the natural role of incretins
Adapted from 1Nauck MA, et al. Diabetologia 1993;36:741–744; 2Larsson H, et al. Acta Physiol Scand 1997;160:413–422; 3Nauck MA, et al. Diabetologia 1996;39:1546–1553; 4Flint A, et al. J Clin Invest 1998;101:515–520; 5Zander et al. Lancet 2002;359:824–830.
GLP-1 secreted upon the ingestion of food
1.-cell:enhances glucose-dependent
insulin secretion in the pancreas1
3.Liver: reduces hepatic glucose
output2
2.α-cell:suppresses postprandial
glucagon secretion1
4.Stomach: slows the rate of gastric emptying3
5.Brain:promotes satiety and
reduces appetite4,5

Change in body weight over time, Exenatide with metformin
ITT population, N = 336 (Placebo, N = 113; exenatide 5 µg, N = 110; exenatide 10 µg, N = 113)*P ≤ 0.05 ** P ≤ 0.001 compared to placeboDeFronzo RA, et al. Diabetes Care 2005;28:1092–1100.
*
***
-0.3 ± 0.3 kg
-2.8 ± 0.5 kg
-1.6 ± 0.4 kg
Time (weeks)
5 10 15 20 25 300-4
-3
-2
-1
0
1
**
**** **
*
Mea
n (
± S
E)
chan
ge
in b
od
y w
eig
ht
fro
m b
asel
ine
(kg
)
Placebo BD Exenatide 5 µg BD Exenatide 10 µg BD

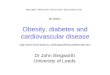
Change in body weight over time, Exenatide with sulphonylurea
ITT population, N = 377 (Placebo, N = 123; exenatide 5 µg, N = 125; exenatide 10 µg, N = 129); *P ≤ 0.05 vs placeboBuse J, et al. Diabetes Care 2004;27:2628–2635.
-0.6 kg
-0.9 kg
-1.6 kgMea
n (
± S
E)
chan
ge
in b
od
y w
eig
ht
fro
m b
asel
ine
(kg
)
Time (weeks)
0 10 20 30-2.00
-1.50
-1.00
-0.50
0
*-1.75
-1.25
-0.75
-0.25
5 15 25
Placebo BD Exenatide 5 µg BD Exenatide 10 µg BD









Case studies

DR age 48 years
T2DM 14 years
Metformin, Gliclazide, Lantus 56 units
Weight 142Kg BMI 52 Kg/m2
HbA1C 7.6%

Fasting blood glucose 5.6mmol/l
Post prandial 8.8 mmol/l
Recurrent hypoglycaemia at night
Daily supper
Lantus switched to morning
Solution??

Reduce Lantus
Correct Post prandial Glucose
Stop Supper
Weight loss after 6 months 23KG
HbA1C 6.8%
Lantus reduced to 22units

Case Study 2
EB 56 years House wife
Type 1 diabetes sine age 22years
Weight 112Kg BMI 48 Kg/m2
Also is hypertensive and has angina
On Lantus 66 units
Novarapid 12 units TDS

HbA1C 8.6%
Add Metformin
Weight 106 Kg after three months
Lantus down to 50 units
HbA1C 8.0%Metformin full dose
After three months Orlistat added with guidance
Lantus 36 units
HbA1C 7.4%
Weight 98 Kg

MA 62 years
T2DM 8 years
Weight 102 Kg BMI 56 Kg/m2
HbA1C 10.3 %
On Metformin, Lantus 64 units BD
Increasingly tired
And
Day time sleepiness

OSA ruled out
? Hypogonad
Testosterone 6.6 nmol/l
Testosterone replacement
After 4 months reduced Lantus to 32 units BD due to hypoglycaemia
Weight 90KG
HbA1C 8.1%
No day time sleepiness !!!!!!!

Next Forum
Presentation of GAME and LOOKAHEAD
Case discussion
External Speaker (TBC)

Thank you!Visit http://www.simplyweight.co.uk for more information