Embed Size (px)
Citation preview
Dementia Basics Workshop
Dr Yasir Hameed (Specialist Registrar, ST6)Dr Jonathan Hillam (Consultant Old Age Psychiatrist)
Norwich19 February 2016
Outline
Describe the various types and treatment for dementia
Role of investigations/imaging
Discuss issues related to driving and capacity
Case scenarios
Duration 90 minutes
Learning objectives
Elicit the clinical features of dementia (both cognitive and non-cognitive / BPSD)
Describe the common causes of dementia, potentially reversible causes and understand the differential diagnosis of cognitive changes or deterioration in the elderly.
Identify the common risks associated with dementia (to self, to others, from others) and risk management strategies
Explain the management of dementia using psychological, social and medical interventions
Explain the medico-legal issues associated with dementia, driving and dementia

What is common?

Statistics 1 in 20 people over 60 have a diagnosis of dementia
1 in 5 people over 80 have a diagnosis of dementia
There are about 800,000 people in the UK with dementia (Alzheimer's society, 2012)
Around 2/3 people with Dementia are cared for at home
However, it can affect younger people: there are over 17,000 people in the UK under the age of 65 who have dementia (Alzheimer's society, 2012)
What is Dementia?(1) Memory impairment (impaired ability to learn new information or to recall previously learned information)
(2) One or more cognitive disturbances:(a) aphasia (b) apraxia (c) agnosia (d) disturbance in executive functioning
ICD 10 Dementia (F00-F03) is a syndrome …..of a chronic or
progressive nature….disturbance … of memory, thinking, orientation, comprehension, calculation, learning capacity, language, and judgement.
Consciousness is not clouded.
The cognitive impairment is accompanied by deterioration in emotional control, social behaviour, or motivation.
Dementia is NOT
Learning disabilityStrokeDelirium (“acute confusional state”)Depression (“pseudodementia)“Just getting old”Just forgetfulness
Dementia?
Mild Cognitive Impairment?
Depression?
Superman in his later years
Dang! . . . Now where
was I going?

Causes of DementiaNeuro-degenerative (Alzheimer’s, Lewy body, Parkinson’s)
Vascular (infarction, bleeding, vasculitis, Binswanger’s)
Metabolic (thyroid, vitamin deficiency)Infectious (AIDS, neuro-syphilis)HypoxicToxic (heavy metal)Intracranial lesion (mass)Trauma (dementia pugilistica)
Types of DementiaAlzheimer’s disease (50-60%)Lewy body disease (15-20%)Vascular dementia (VD)(15-20%)Parkinson’s dementia (1-3%)Fronto-temporal dementia (1-2%)Other/Mixed: dementia in Huntington’s disease,
CJD (BSE), dementia in multiple sclerosis)
Alzheimer's disease Predominately early episodic memory difficulties
Difficulties with STM and recall / orientation
Word finding and ability to generate words (Salmon & Bondi 2009)
Some awareness of their symptoms, so the person may become anxious, depressed and may be in denial
Later stages characterised by more severe cognitive impairment, psychotic symptoms and speech problems.
Dementia with Lewy bodies
McKeith et al. Diagnosis and management of dementia: Third Report of the DLB consortium. Neurology 2005
Evidence of cognitive impairment (esp characteristic profile) of sufficient magnitude to interfere with normal social and occupational function
Core features Fluctuating cognitive impairment – 80% Recurrent complex visual hallucinations – 70% Spontaneous features of parkinsonism – 25-50% (75%
eventually)
Suggestive features REM sleep behaviour disorder Severe neuroleptic / antipsychotic sensitivity Low dopamine transporter uptake in basal ganglia
demonstrated by Nuclear Imagining
Males > females, mean onset 75y
Vascular Dementia
Refers to the pathology – many different types
Early symptoms are memory difficulties and executive difficulties
Often history of stroke / falls
Stepwise progression
Vascular risk factors usually present (High blood pressure, high cholesterol, diabetes) (Salmon & Bondi, 2009)
Frontotemporal dementia Umbrella term – may different variants including Picks,
semantic dementia, primary progressive aphasia (PPA)
Main cognitive deficits are in executive functioning and attention.
Personality change.
Memory and visuospatial abilities mostly spared (Lezak, 2004)
Robin Williams’ silent suffering
NICE Guidelines CG42 (2006, 2012)
Non-discriminationValid consentInvolvement of CarersMemory servicesStructural imaging for diagnosisChallenging behaviour TrainingMental health needs in acute hospitals

“Structural imaging should be used in the assessment of people with suspected dementia to exclude other cerebral pathologies and to help establish the subtype diagnosis.
Magnetic resonance imaging (MRI) is the preferred modality to assist with early diagnosis and detect subcortical vascular changes, although computed tomography (CT) scanning could be used. Specialist advice should be taken when interpreting scans in people with learning disabilities.”
What is the purpose of imaging?
Establishing the subtype diagnosis
• Diagnosis is based on clinical criteria
Imaging supportive but not required• Alzheimer’s disease• Dementia with Lewy bodies• Frontotemporal dementia
Imaging needed for vascular dementia• Extent• Topography• Severity
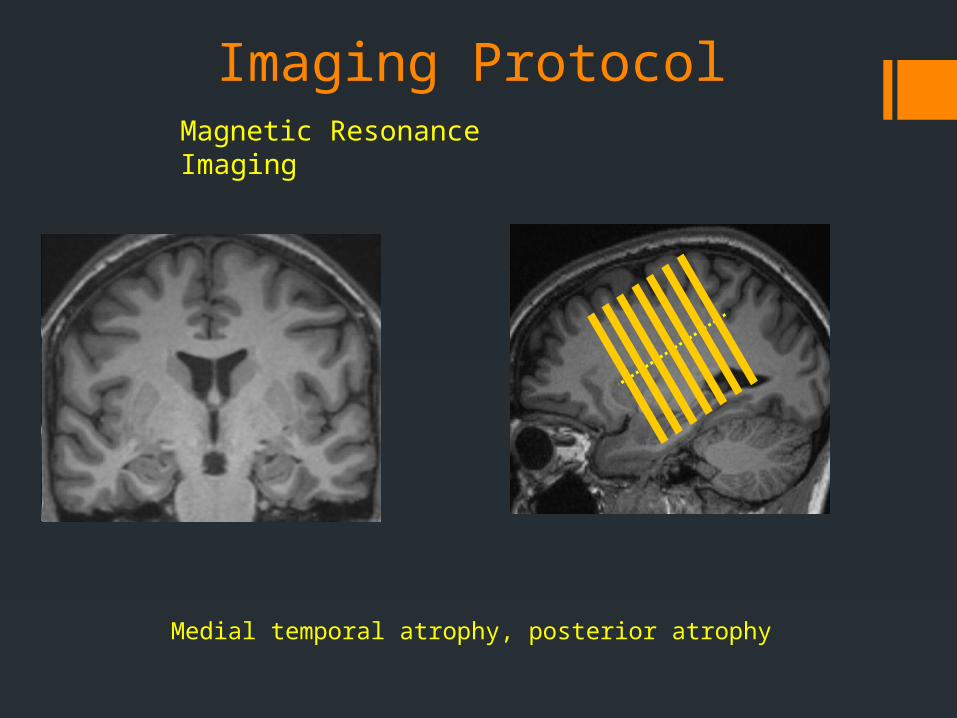
Imaging ProtocolMagnetic Resonance Imaging
Medial temporal atrophy, posterior atrophy
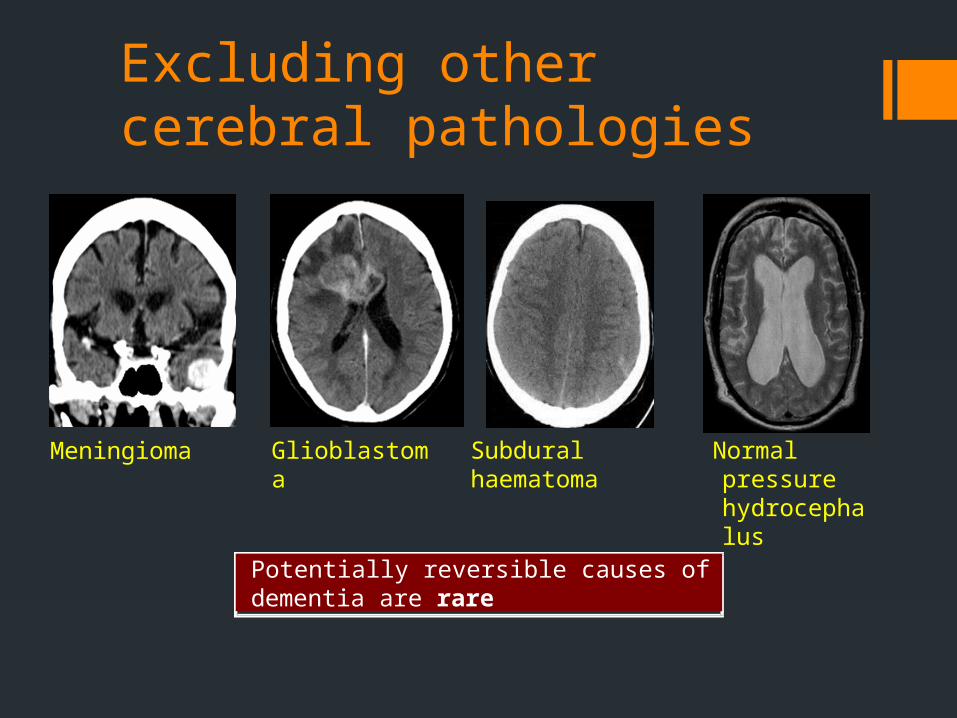
Excluding other cerebral pathologies
Meningioma Glioblastoma
Potentially reversible causes of dementia are rare
Subdural haematoma
Normal pressure hydrocephalus
Initial AssessmentMake a diagnosis of dementia only after a comprehensive Assessment
If dementia is mild or questionable, conduct formal neuropsychological testing.
Assess medical and psychiatric comorbidities, including depression and psychosis.
Ask people who are assessed for possible dementia whether they wish to know the diagnosis and with whom it should be shared.
Cognitive TestingNICE:6-Item Cognitive Impairment Test (6-CIT)General Practitioner Assessment of Cognition (GPCOG)7-Minute Screen
We use:Addenbrook's Cognitive Examination (Ace III)Mini ACE
Others:MoCA
MedicationThe three acetylcholinesterase (AChE) inhibitors donepezil, galantamine and rivastigmine for managing mild to moderate Alzheimer’s disease.
Memantine is recommended for people with Moderate Alzheimer’s disease (if AChE inhibitors are not tolerated) and for people with Severe Alzheimer’s disease
Cholinesterase inhibitors
These drugs stop the breakdown of acetylcholine which is an important neurotransmitter in memory and cognition
All show modest improvement in cognition and function, and behavioural symptoms
Response: 1/3 improve, 1/3 stabilise, 1/3 have no response
Do not prevent progression of underlying disease
Cholinesterase inhibitors
Donepezil (Aricept) given once daily, dosage of 5mg to 10mg
Rivastigmine (Exelon) given twice daily, dosages of 3mg to 12mg
Galantamine (Reminyl) given once daily, dosages of 8mg to 24mg (can also be given
twice daily)
Use of cholinesterase inhibitorsNeed specialist diagnosis of Alzheimer's Disease, and
a MMSE score of 10 to 24.
Side effects - nausea, vomiting, diarrhoea, dizziness, headache, muscle cramps
Use carefully if gastric ulcer, heart disease, chronic lung disease present
Use of cholinesterase inhibitorsWarn against unrealistic expectations
Stopping of medication:unacceptable side effects lack of response to medication (controversial) late stages of the disease
Always consider patients’ and carers’ views.
Memantine (Ebixa)Glutamate is a transmitter in the brain that is affected
by Alzheimer's Disease
Memantine blocks the pathological effects of abnormal glutamate release, and allows better function of the impaired brain
Indicated for moderate to severe AD
Trials show slowing in cognitive and functional decline and decrease in agitation in treated group compared to placebo
MemantineCan use with other AD medications
Side effects - headaches, dizziness
Do not use in kidney disease or seizure disorders
Dosage: start with 5mg daily and increase to10mg twice daily
Behavioural & Psychiatric Symptoms (BPSD)
Psychological: psychosis, depression, apathy and persecutory/paranoid.
Behavioural: aggression, agitation, wandering, repetitive behaviour or speech, disinhibited behaviour or speech, hiding or hoarding, accusing and “Sundowning” and changes to sleep pattern.
Top tips in assessment
Consider physical healthInspect medication or drug chartLook at care notesInvolve familySpend time with patient
Treatment
Antipsychotic controversyEstablished risks
Accelerated cognitive declineCerebrovascular eventsMortality
Non pharmacological management first
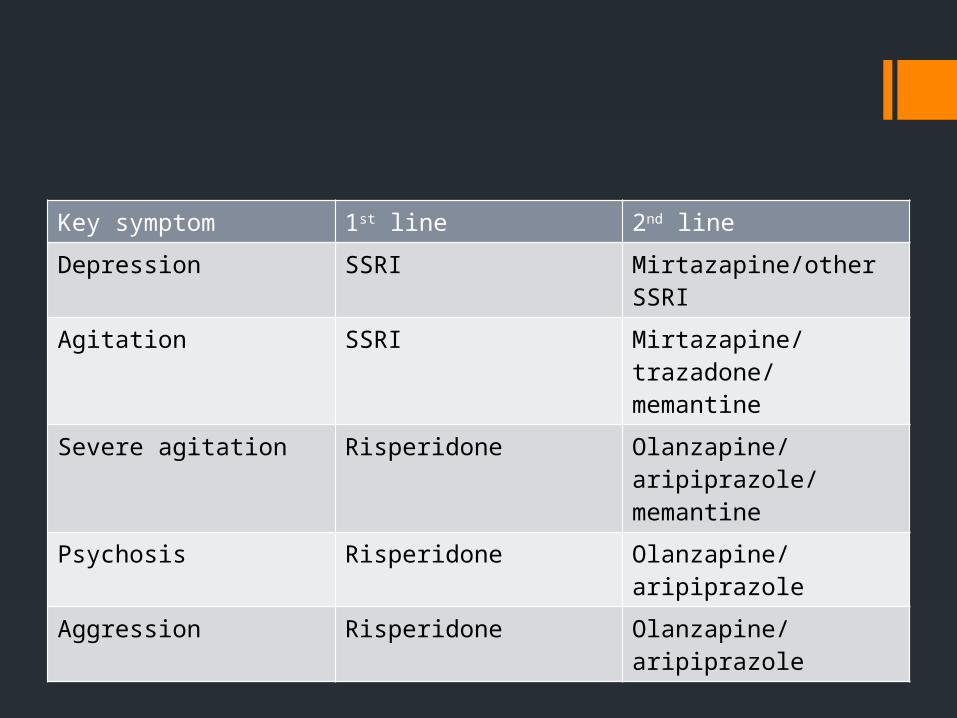
Prescribing guidelinesKey symptom 1st line 2nd line
Depression SSRI Mirtazapine/other SSRI
Agitation SSRI Mirtazapine/trazadone/memantine
Severe agitation Risperidone Olanzapine/aripiprazole/memantine
Psychosis Risperidone Olanzapine/aripiprazole
Aggression Risperidone Olanzapine/aripiprazole
Loss of fine motor control
Impaired balance and mobility
Urinary incontinence
Faecal incontinence
Eating and swallowing problems
Weight loss
Increased risk of infection
Seizures
Physical symptoms in dementia
Psychological interventions Cognitive stimulation therapy (www.cstdementia.com)
Music therapy Drama therapy/storytelling Movement/dance therapy Aromatherapy (mainly Melissa balm and lavender) Animal-assisted therapy Doll therapy Reminiscence therapy Validation therapy
Patel B et al. Psychosocial interventions for dementia: from evidence to practice. Advances in Psychiatric Treatment Sep 2014, 20 (5) 340-349
RiskSelf
Others
Neglect
Vulnerability

Capacity, Driving & Dementia
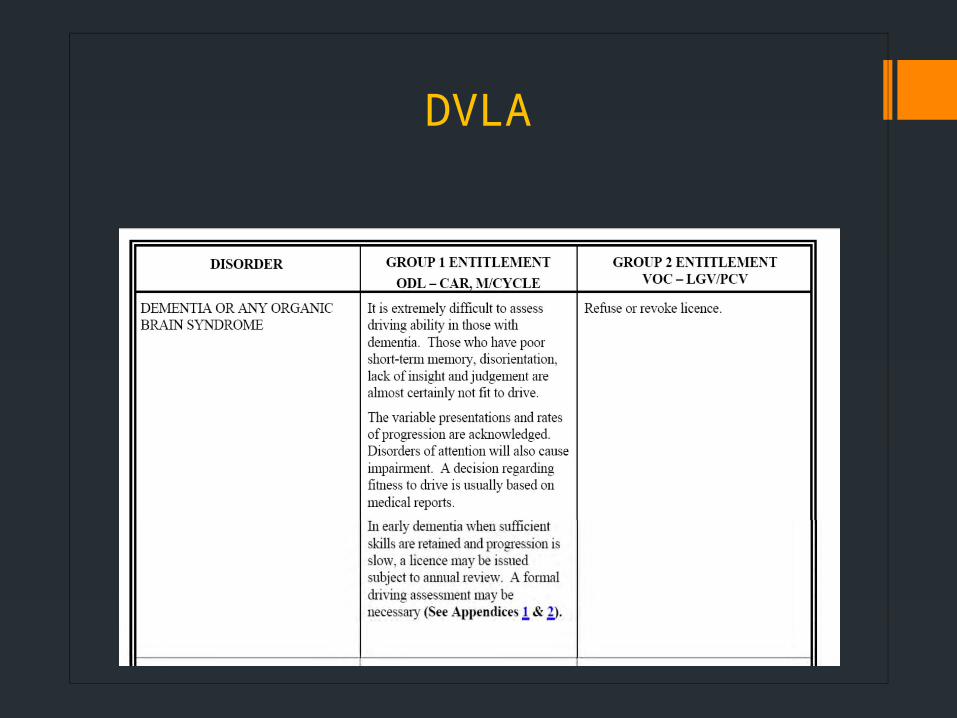
DVLA
Capacity
Mental Capacity
Mental Capacity Act 2005
Deprivation of Liberty safeguards (DoLS)
Five Key Principles
A presumption of capacity
A right for individuals to be supported to make their own decisions
A right to make apparently eccentric or unwise decisions
For those who lack capacity, acting in their best interests.. and in the least restrictive way
Capacity: definitionA person lacks capacity in relation to a matter ifat the material time he is unable to make adecision for himself in relation to the matterbecause of an impairment of, or a disturbance inthe functioning of, the mind or brain.
i.e.
the ability to make a particular decision at thetime it needs to be made.
Not just a doctor’s (or psychiatrist’s) job
Always consider mental state and cognitive function
Can patient understand information? and
Can patient retain information? and
Can patient weigh up the information? and
Can patient communicate his/her decision?
Assessment of capacity
In what situations may a capacity assessment be required in someone with dementia?
Managing financial affairs
Decisions about where to live
Hospital admission
Accepting or refusing medical treatment
Dementia and capacity
Mental Capacity Act (2005)
Best interests
Power of Attorney (property & affairs vs health & welfare)
Court of Protection
Deprivation of Liberty Safeguards (DoLS)
Advance decisions
Appeal to the High Court
If a patient lacks capacity