Embed Size (px)
Citation preview

CRRT And AKI
Overview
Mostafa Abdel_Salam Mohamed MD
Consultant of Nephrology
bull Sudden interruption of kidney function resulting from obstruction reduced circulation or disease of the renal tissue
bull Results in retention of toxins fluids and end products of metabolism
bull Usually reversible with medical treatment
bull May progress to end stage renal disease uremic syndrome and death without treatment
definitions of AKI
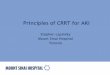
RIFLE criteria for diagnosis of AKI based on The ldquoAcute Dialysis Quality Initiativerdquo
Increase in SCr Urine output
Risk of renal injury
Injury to the kidney
Failure of kidney function
03 mgdl increase
2 X baseline
3 X baseline OR
gt 05 mgdl increase if SCr gt=4 mgdl
lt 05 mlkghr for gt 6 h
lt 05 mlkghr for gt12h
Anuria for gt12 h
Loss of kidney function
End-stage disease
Persistent renal failure for gt 4 weeks
Persistent renal failure for gt 3 months
Am J Kidney Dis 2005 Dec46(6)1038-48
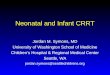
Stage Increase in Serum Creatinine
Urine Output
1 15-2 times baselineOR 03 mgdl increase from baseline
lt05 mlkgh for gt6 h
2 2-3 times baseline lt05 mlkgh for gt12 h
3 3 times baseline OR05 mgdl increase if baselinegt4mgdlORAny RRT given
lt03 mlkgh for gt24 hOR Anuria for gt12 h
Definition of Acute Kidney Injury (AKI) based on ldquoAcute Kidney Injury Networkrdquo
Epidemiology
AKI occurs in
bullasymp 7 of hospitalized patients
bull36ndash67 of critically ill patients(depending on the definition)
bull5-6 of intensive care unite (ICU)patients with AKI require renalreplacement therapy (RRP)
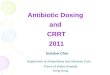
Mortality according to RIFLE
Mortality increases proportionately with increasing severity of AKI (using RIFLE)
Mortality in pts with AKI requiring RRT 50-70
Even small changes in serum creatinine are associated with increased mortality
CRITICALCARENURSE Vol 27 No 2 APRIL 2007
bull In 1977 Kramer in Goumlttingen (Germany)developed the continuousarteriovenous hemofiltration(CAVH) technique which used asystemic arteriovenous pressure difference inan extracorporeal circuit to continuouslyproduce an ultrafiltrate
bull In the 1980s a blood pump such as thoseused in intermittent hemodialysis and adouble-lumen catheter in a large vein wereused to provide a consistent
blood-flow rate without
the risks associated
with the arteriovenous approach
The Acute Disease Quality Initiative (ADQI)
Published online August 26 2016
When should acute RRT be initiated (includes AKI and non-AKI indications)
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
How should RRT be integrated into other extracorporeal therapies
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
How should patients be liberated from RRT
When should acute RRT be initiated
Consensus statement 11
bullAcute RRT should be consideredwhen metabolic and fluiddemands exceed total kidneycapacity
Individual
Renal function
Clinical context
562 We suggest using CRRT rather thanstandard intermittent RRT for hemodynamicallyunstable patients (2B)
563 We suggest using CRRT rather thanintermittent RRT for AKI patients with acute braininjury or other causes of increased intracranialpressure or generalized brain edema (2B)
Indications for CRRT
bullCRRT is an effective method toremove fluid and to achieve a targetfluid balance in patients with fluidoverload including those withcongestive cardiac failure (CCF) oracute lung injury
RRT is also effective at removingbiologically active substancesincluding cytokines butthere is still insufficientevidence to recommend the routineuse of CRRT for the treatment ofsepsis
When should acute RRT be initiated
Consensus statement 12
bullDemand for kidney function isdetermined by non-renalcomorbidities the severity ofthe acute disease and solute andfluid burden
When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

bull Sudden interruption of kidney function resulting from obstruction reduced circulation or disease of the renal tissue
bull Results in retention of toxins fluids and end products of metabolism
bull Usually reversible with medical treatment
bull May progress to end stage renal disease uremic syndrome and death without treatment
definitions of AKI
RIFLE criteria for diagnosis of AKI based on The ldquoAcute Dialysis Quality Initiativerdquo
Increase in SCr Urine output
Risk of renal injury
Injury to the kidney
Failure of kidney function
03 mgdl increase
2 X baseline
3 X baseline OR
gt 05 mgdl increase if SCr gt=4 mgdl
lt 05 mlkghr for gt 6 h
lt 05 mlkghr for gt12h
Anuria for gt12 h
Loss of kidney function
End-stage disease
Persistent renal failure for gt 4 weeks
Persistent renal failure for gt 3 months
Am J Kidney Dis 2005 Dec46(6)1038-48
Stage Increase in Serum Creatinine
Urine Output
1 15-2 times baselineOR 03 mgdl increase from baseline
lt05 mlkgh for gt6 h
2 2-3 times baseline lt05 mlkgh for gt12 h
3 3 times baseline OR05 mgdl increase if baselinegt4mgdlORAny RRT given
lt03 mlkgh for gt24 hOR Anuria for gt12 h
Definition of Acute Kidney Injury (AKI) based on ldquoAcute Kidney Injury Networkrdquo
Epidemiology
AKI occurs in
bullasymp 7 of hospitalized patients
bull36ndash67 of critically ill patients(depending on the definition)
bull5-6 of intensive care unite (ICU)patients with AKI require renalreplacement therapy (RRP)
Mortality according to RIFLE
Mortality increases proportionately with increasing severity of AKI (using RIFLE)
Mortality in pts with AKI requiring RRT 50-70
Even small changes in serum creatinine are associated with increased mortality
CRITICALCARENURSE Vol 27 No 2 APRIL 2007
bull In 1977 Kramer in Goumlttingen (Germany)developed the continuousarteriovenous hemofiltration(CAVH) technique which used asystemic arteriovenous pressure difference inan extracorporeal circuit to continuouslyproduce an ultrafiltrate
bull In the 1980s a blood pump such as thoseused in intermittent hemodialysis and adouble-lumen catheter in a large vein wereused to provide a consistent
blood-flow rate without
the risks associated
with the arteriovenous approach
The Acute Disease Quality Initiative (ADQI)
Published online August 26 2016
When should acute RRT be initiated (includes AKI and non-AKI indications)
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
How should RRT be integrated into other extracorporeal therapies
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
How should patients be liberated from RRT
When should acute RRT be initiated
Consensus statement 11
bullAcute RRT should be consideredwhen metabolic and fluiddemands exceed total kidneycapacity
Individual
Renal function
Clinical context
562 We suggest using CRRT rather thanstandard intermittent RRT for hemodynamicallyunstable patients (2B)
563 We suggest using CRRT rather thanintermittent RRT for AKI patients with acute braininjury or other causes of increased intracranialpressure or generalized brain edema (2B)
Indications for CRRT
bullCRRT is an effective method toremove fluid and to achieve a targetfluid balance in patients with fluidoverload including those withcongestive cardiac failure (CCF) oracute lung injury
RRT is also effective at removingbiologically active substancesincluding cytokines butthere is still insufficientevidence to recommend the routineuse of CRRT for the treatment ofsepsis
When should acute RRT be initiated
Consensus statement 12
bullDemand for kidney function isdetermined by non-renalcomorbidities the severity ofthe acute disease and solute andfluid burden
When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

RIFLE criteria for diagnosis of AKI based on The ldquoAcute Dialysis Quality Initiativerdquo
Increase in SCr Urine output
Risk of renal injury
Injury to the kidney
Failure of kidney function
03 mgdl increase
2 X baseline
3 X baseline OR
gt 05 mgdl increase if SCr gt=4 mgdl
lt 05 mlkghr for gt 6 h
lt 05 mlkghr for gt12h
Anuria for gt12 h
Loss of kidney function
End-stage disease
Persistent renal failure for gt 4 weeks
Persistent renal failure for gt 3 months
Am J Kidney Dis 2005 Dec46(6)1038-48
Stage Increase in Serum Creatinine
Urine Output
1 15-2 times baselineOR 03 mgdl increase from baseline
lt05 mlkgh for gt6 h
2 2-3 times baseline lt05 mlkgh for gt12 h
3 3 times baseline OR05 mgdl increase if baselinegt4mgdlORAny RRT given
lt03 mlkgh for gt24 hOR Anuria for gt12 h
Definition of Acute Kidney Injury (AKI) based on ldquoAcute Kidney Injury Networkrdquo
Epidemiology
AKI occurs in
bullasymp 7 of hospitalized patients
bull36ndash67 of critically ill patients(depending on the definition)
bull5-6 of intensive care unite (ICU)patients with AKI require renalreplacement therapy (RRP)
Mortality according to RIFLE
Mortality increases proportionately with increasing severity of AKI (using RIFLE)
Mortality in pts with AKI requiring RRT 50-70
Even small changes in serum creatinine are associated with increased mortality
CRITICALCARENURSE Vol 27 No 2 APRIL 2007
bull In 1977 Kramer in Goumlttingen (Germany)developed the continuousarteriovenous hemofiltration(CAVH) technique which used asystemic arteriovenous pressure difference inan extracorporeal circuit to continuouslyproduce an ultrafiltrate
bull In the 1980s a blood pump such as thoseused in intermittent hemodialysis and adouble-lumen catheter in a large vein wereused to provide a consistent
blood-flow rate without
the risks associated
with the arteriovenous approach
The Acute Disease Quality Initiative (ADQI)
Published online August 26 2016
When should acute RRT be initiated (includes AKI and non-AKI indications)
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
How should RRT be integrated into other extracorporeal therapies
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
How should patients be liberated from RRT
When should acute RRT be initiated
Consensus statement 11
bullAcute RRT should be consideredwhen metabolic and fluiddemands exceed total kidneycapacity
Individual
Renal function
Clinical context
562 We suggest using CRRT rather thanstandard intermittent RRT for hemodynamicallyunstable patients (2B)
563 We suggest using CRRT rather thanintermittent RRT for AKI patients with acute braininjury or other causes of increased intracranialpressure or generalized brain edema (2B)
Indications for CRRT
bullCRRT is an effective method toremove fluid and to achieve a targetfluid balance in patients with fluidoverload including those withcongestive cardiac failure (CCF) oracute lung injury
RRT is also effective at removingbiologically active substancesincluding cytokines butthere is still insufficientevidence to recommend the routineuse of CRRT for the treatment ofsepsis
When should acute RRT be initiated
Consensus statement 12
bullDemand for kidney function isdetermined by non-renalcomorbidities the severity ofthe acute disease and solute andfluid burden
When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

Stage Increase in Serum Creatinine
Urine Output
1 15-2 times baselineOR 03 mgdl increase from baseline
lt05 mlkgh for gt6 h
2 2-3 times baseline lt05 mlkgh for gt12 h
3 3 times baseline OR05 mgdl increase if baselinegt4mgdlORAny RRT given
lt03 mlkgh for gt24 hOR Anuria for gt12 h
Definition of Acute Kidney Injury (AKI) based on ldquoAcute Kidney Injury Networkrdquo
Epidemiology
AKI occurs in
bullasymp 7 of hospitalized patients
bull36ndash67 of critically ill patients(depending on the definition)
bull5-6 of intensive care unite (ICU)patients with AKI require renalreplacement therapy (RRP)
Mortality according to RIFLE
Mortality increases proportionately with increasing severity of AKI (using RIFLE)
Mortality in pts with AKI requiring RRT 50-70
Even small changes in serum creatinine are associated with increased mortality
CRITICALCARENURSE Vol 27 No 2 APRIL 2007
bull In 1977 Kramer in Goumlttingen (Germany)developed the continuousarteriovenous hemofiltration(CAVH) technique which used asystemic arteriovenous pressure difference inan extracorporeal circuit to continuouslyproduce an ultrafiltrate
bull In the 1980s a blood pump such as thoseused in intermittent hemodialysis and adouble-lumen catheter in a large vein wereused to provide a consistent
blood-flow rate without
the risks associated
with the arteriovenous approach
The Acute Disease Quality Initiative (ADQI)
Published online August 26 2016
When should acute RRT be initiated (includes AKI and non-AKI indications)
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
How should RRT be integrated into other extracorporeal therapies
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
How should patients be liberated from RRT
When should acute RRT be initiated
Consensus statement 11
bullAcute RRT should be consideredwhen metabolic and fluiddemands exceed total kidneycapacity
Individual
Renal function
Clinical context
562 We suggest using CRRT rather thanstandard intermittent RRT for hemodynamicallyunstable patients (2B)
563 We suggest using CRRT rather thanintermittent RRT for AKI patients with acute braininjury or other causes of increased intracranialpressure or generalized brain edema (2B)
Indications for CRRT
bullCRRT is an effective method toremove fluid and to achieve a targetfluid balance in patients with fluidoverload including those withcongestive cardiac failure (CCF) oracute lung injury
RRT is also effective at removingbiologically active substancesincluding cytokines butthere is still insufficientevidence to recommend the routineuse of CRRT for the treatment ofsepsis
When should acute RRT be initiated
Consensus statement 12
bullDemand for kidney function isdetermined by non-renalcomorbidities the severity ofthe acute disease and solute andfluid burden
When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

Epidemiology
AKI occurs in
bullasymp 7 of hospitalized patients
bull36ndash67 of critically ill patients(depending on the definition)
bull5-6 of intensive care unite (ICU)patients with AKI require renalreplacement therapy (RRP)
Mortality according to RIFLE
Mortality increases proportionately with increasing severity of AKI (using RIFLE)
Mortality in pts with AKI requiring RRT 50-70
Even small changes in serum creatinine are associated with increased mortality
CRITICALCARENURSE Vol 27 No 2 APRIL 2007
bull In 1977 Kramer in Goumlttingen (Germany)developed the continuousarteriovenous hemofiltration(CAVH) technique which used asystemic arteriovenous pressure difference inan extracorporeal circuit to continuouslyproduce an ultrafiltrate
bull In the 1980s a blood pump such as thoseused in intermittent hemodialysis and adouble-lumen catheter in a large vein wereused to provide a consistent
blood-flow rate without
the risks associated
with the arteriovenous approach
The Acute Disease Quality Initiative (ADQI)
Published online August 26 2016
When should acute RRT be initiated (includes AKI and non-AKI indications)
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
How should RRT be integrated into other extracorporeal therapies
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
How should patients be liberated from RRT
When should acute RRT be initiated
Consensus statement 11
bullAcute RRT should be consideredwhen metabolic and fluiddemands exceed total kidneycapacity
Individual
Renal function
Clinical context
562 We suggest using CRRT rather thanstandard intermittent RRT for hemodynamicallyunstable patients (2B)
563 We suggest using CRRT rather thanintermittent RRT for AKI patients with acute braininjury or other causes of increased intracranialpressure or generalized brain edema (2B)
Indications for CRRT
bullCRRT is an effective method toremove fluid and to achieve a targetfluid balance in patients with fluidoverload including those withcongestive cardiac failure (CCF) oracute lung injury
RRT is also effective at removingbiologically active substancesincluding cytokines butthere is still insufficientevidence to recommend the routineuse of CRRT for the treatment ofsepsis
When should acute RRT be initiated
Consensus statement 12
bullDemand for kidney function isdetermined by non-renalcomorbidities the severity ofthe acute disease and solute andfluid burden
When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

Mortality according to RIFLE
Mortality increases proportionately with increasing severity of AKI (using RIFLE)
Mortality in pts with AKI requiring RRT 50-70
Even small changes in serum creatinine are associated with increased mortality
CRITICALCARENURSE Vol 27 No 2 APRIL 2007
bull In 1977 Kramer in Goumlttingen (Germany)developed the continuousarteriovenous hemofiltration(CAVH) technique which used asystemic arteriovenous pressure difference inan extracorporeal circuit to continuouslyproduce an ultrafiltrate
bull In the 1980s a blood pump such as thoseused in intermittent hemodialysis and adouble-lumen catheter in a large vein wereused to provide a consistent
blood-flow rate without
the risks associated
with the arteriovenous approach
The Acute Disease Quality Initiative (ADQI)
Published online August 26 2016
When should acute RRT be initiated (includes AKI and non-AKI indications)
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
How should RRT be integrated into other extracorporeal therapies
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
How should patients be liberated from RRT
When should acute RRT be initiated
Consensus statement 11
bullAcute RRT should be consideredwhen metabolic and fluiddemands exceed total kidneycapacity
Individual
Renal function
Clinical context
562 We suggest using CRRT rather thanstandard intermittent RRT for hemodynamicallyunstable patients (2B)
563 We suggest using CRRT rather thanintermittent RRT for AKI patients with acute braininjury or other causes of increased intracranialpressure or generalized brain edema (2B)
Indications for CRRT
bullCRRT is an effective method toremove fluid and to achieve a targetfluid balance in patients with fluidoverload including those withcongestive cardiac failure (CCF) oracute lung injury
RRT is also effective at removingbiologically active substancesincluding cytokines butthere is still insufficientevidence to recommend the routineuse of CRRT for the treatment ofsepsis
When should acute RRT be initiated
Consensus statement 12
bullDemand for kidney function isdetermined by non-renalcomorbidities the severity ofthe acute disease and solute andfluid burden
When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

CRITICALCARENURSE Vol 27 No 2 APRIL 2007
bull In 1977 Kramer in Goumlttingen (Germany)developed the continuousarteriovenous hemofiltration(CAVH) technique which used asystemic arteriovenous pressure difference inan extracorporeal circuit to continuouslyproduce an ultrafiltrate
bull In the 1980s a blood pump such as thoseused in intermittent hemodialysis and adouble-lumen catheter in a large vein wereused to provide a consistent
blood-flow rate without
the risks associated
with the arteriovenous approach
The Acute Disease Quality Initiative (ADQI)
Published online August 26 2016
When should acute RRT be initiated (includes AKI and non-AKI indications)
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
How should RRT be integrated into other extracorporeal therapies
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
How should patients be liberated from RRT
When should acute RRT be initiated
Consensus statement 11
bullAcute RRT should be consideredwhen metabolic and fluiddemands exceed total kidneycapacity
Individual
Renal function
Clinical context
562 We suggest using CRRT rather thanstandard intermittent RRT for hemodynamicallyunstable patients (2B)
563 We suggest using CRRT rather thanintermittent RRT for AKI patients with acute braininjury or other causes of increased intracranialpressure or generalized brain edema (2B)
Indications for CRRT
bullCRRT is an effective method toremove fluid and to achieve a targetfluid balance in patients with fluidoverload including those withcongestive cardiac failure (CCF) oracute lung injury
RRT is also effective at removingbiologically active substancesincluding cytokines butthere is still insufficientevidence to recommend the routineuse of CRRT for the treatment ofsepsis
When should acute RRT be initiated
Consensus statement 12
bullDemand for kidney function isdetermined by non-renalcomorbidities the severity ofthe acute disease and solute andfluid burden
When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

bull In 1977 Kramer in Goumlttingen (Germany)developed the continuousarteriovenous hemofiltration(CAVH) technique which used asystemic arteriovenous pressure difference inan extracorporeal circuit to continuouslyproduce an ultrafiltrate
bull In the 1980s a blood pump such as thoseused in intermittent hemodialysis and adouble-lumen catheter in a large vein wereused to provide a consistent
blood-flow rate without
the risks associated
with the arteriovenous approach
The Acute Disease Quality Initiative (ADQI)
Published online August 26 2016
When should acute RRT be initiated (includes AKI and non-AKI indications)
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
How should RRT be integrated into other extracorporeal therapies
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
How should patients be liberated from RRT
When should acute RRT be initiated
Consensus statement 11
bullAcute RRT should be consideredwhen metabolic and fluiddemands exceed total kidneycapacity
Individual
Renal function
Clinical context
562 We suggest using CRRT rather thanstandard intermittent RRT for hemodynamicallyunstable patients (2B)
563 We suggest using CRRT rather thanintermittent RRT for AKI patients with acute braininjury or other causes of increased intracranialpressure or generalized brain edema (2B)
Indications for CRRT
bullCRRT is an effective method toremove fluid and to achieve a targetfluid balance in patients with fluidoverload including those withcongestive cardiac failure (CCF) oracute lung injury
RRT is also effective at removingbiologically active substancesincluding cytokines butthere is still insufficientevidence to recommend the routineuse of CRRT for the treatment ofsepsis
When should acute RRT be initiated
Consensus statement 12
bullDemand for kidney function isdetermined by non-renalcomorbidities the severity ofthe acute disease and solute andfluid burden
When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

bull In the 1980s a blood pump such as thoseused in intermittent hemodialysis and adouble-lumen catheter in a large vein wereused to provide a consistent
blood-flow rate without
the risks associated
with the arteriovenous approach
The Acute Disease Quality Initiative (ADQI)
Published online August 26 2016
When should acute RRT be initiated (includes AKI and non-AKI indications)
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
How should RRT be integrated into other extracorporeal therapies
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
How should patients be liberated from RRT
When should acute RRT be initiated
Consensus statement 11
bullAcute RRT should be consideredwhen metabolic and fluiddemands exceed total kidneycapacity
Individual
Renal function
Clinical context
562 We suggest using CRRT rather thanstandard intermittent RRT for hemodynamicallyunstable patients (2B)
563 We suggest using CRRT rather thanintermittent RRT for AKI patients with acute braininjury or other causes of increased intracranialpressure or generalized brain edema (2B)
Indications for CRRT
bullCRRT is an effective method toremove fluid and to achieve a targetfluid balance in patients with fluidoverload including those withcongestive cardiac failure (CCF) oracute lung injury
RRT is also effective at removingbiologically active substancesincluding cytokines butthere is still insufficientevidence to recommend the routineuse of CRRT for the treatment ofsepsis
When should acute RRT be initiated
Consensus statement 12
bullDemand for kidney function isdetermined by non-renalcomorbidities the severity ofthe acute disease and solute andfluid burden
When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

The Acute Disease Quality Initiative (ADQI)
Published online August 26 2016
When should acute RRT be initiated (includes AKI and non-AKI indications)
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
How should RRT be integrated into other extracorporeal therapies
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
How should patients be liberated from RRT
When should acute RRT be initiated
Consensus statement 11
bullAcute RRT should be consideredwhen metabolic and fluiddemands exceed total kidneycapacity
Individual
Renal function
Clinical context
562 We suggest using CRRT rather thanstandard intermittent RRT for hemodynamicallyunstable patients (2B)
563 We suggest using CRRT rather thanintermittent RRT for AKI patients with acute braininjury or other causes of increased intracranialpressure or generalized brain edema (2B)
Indications for CRRT
bullCRRT is an effective method toremove fluid and to achieve a targetfluid balance in patients with fluidoverload including those withcongestive cardiac failure (CCF) oracute lung injury
RRT is also effective at removingbiologically active substancesincluding cytokines butthere is still insufficientevidence to recommend the routineuse of CRRT for the treatment ofsepsis
When should acute RRT be initiated
Consensus statement 12
bullDemand for kidney function isdetermined by non-renalcomorbidities the severity ofthe acute disease and solute andfluid burden
When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

When should acute RRT be initiated (includes AKI and non-AKI indications)
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
How should RRT be integrated into other extracorporeal therapies
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
How should patients be liberated from RRT
When should acute RRT be initiated
Consensus statement 11
bullAcute RRT should be consideredwhen metabolic and fluiddemands exceed total kidneycapacity
Individual
Renal function
Clinical context
562 We suggest using CRRT rather thanstandard intermittent RRT for hemodynamicallyunstable patients (2B)
563 We suggest using CRRT rather thanintermittent RRT for AKI patients with acute braininjury or other causes of increased intracranialpressure or generalized brain edema (2B)
Indications for CRRT
bullCRRT is an effective method toremove fluid and to achieve a targetfluid balance in patients with fluidoverload including those withcongestive cardiac failure (CCF) oracute lung injury
RRT is also effective at removingbiologically active substancesincluding cytokines butthere is still insufficientevidence to recommend the routineuse of CRRT for the treatment ofsepsis
When should acute RRT be initiated
Consensus statement 12
bullDemand for kidney function isdetermined by non-renalcomorbidities the severity ofthe acute disease and solute andfluid burden
When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

When should acute RRT be initiated
Consensus statement 11
bullAcute RRT should be consideredwhen metabolic and fluiddemands exceed total kidneycapacity
Individual
Renal function
Clinical context
562 We suggest using CRRT rather thanstandard intermittent RRT for hemodynamicallyunstable patients (2B)
563 We suggest using CRRT rather thanintermittent RRT for AKI patients with acute braininjury or other causes of increased intracranialpressure or generalized brain edema (2B)
Indications for CRRT
bullCRRT is an effective method toremove fluid and to achieve a targetfluid balance in patients with fluidoverload including those withcongestive cardiac failure (CCF) oracute lung injury
RRT is also effective at removingbiologically active substancesincluding cytokines butthere is still insufficientevidence to recommend the routineuse of CRRT for the treatment ofsepsis
When should acute RRT be initiated
Consensus statement 12
bullDemand for kidney function isdetermined by non-renalcomorbidities the severity ofthe acute disease and solute andfluid burden
When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

Individual
Renal function
Clinical context
562 We suggest using CRRT rather thanstandard intermittent RRT for hemodynamicallyunstable patients (2B)
563 We suggest using CRRT rather thanintermittent RRT for AKI patients with acute braininjury or other causes of increased intracranialpressure or generalized brain edema (2B)
Indications for CRRT
bullCRRT is an effective method toremove fluid and to achieve a targetfluid balance in patients with fluidoverload including those withcongestive cardiac failure (CCF) oracute lung injury
RRT is also effective at removingbiologically active substancesincluding cytokines butthere is still insufficientevidence to recommend the routineuse of CRRT for the treatment ofsepsis
When should acute RRT be initiated
Consensus statement 12
bullDemand for kidney function isdetermined by non-renalcomorbidities the severity ofthe acute disease and solute andfluid burden
When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

562 We suggest using CRRT rather thanstandard intermittent RRT for hemodynamicallyunstable patients (2B)
563 We suggest using CRRT rather thanintermittent RRT for AKI patients with acute braininjury or other causes of increased intracranialpressure or generalized brain edema (2B)
Indications for CRRT
bullCRRT is an effective method toremove fluid and to achieve a targetfluid balance in patients with fluidoverload including those withcongestive cardiac failure (CCF) oracute lung injury
RRT is also effective at removingbiologically active substancesincluding cytokines butthere is still insufficientevidence to recommend the routineuse of CRRT for the treatment ofsepsis
When should acute RRT be initiated
Consensus statement 12
bullDemand for kidney function isdetermined by non-renalcomorbidities the severity ofthe acute disease and solute andfluid burden
When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

Indications for CRRT
bullCRRT is an effective method toremove fluid and to achieve a targetfluid balance in patients with fluidoverload including those withcongestive cardiac failure (CCF) oracute lung injury
RRT is also effective at removingbiologically active substancesincluding cytokines butthere is still insufficientevidence to recommend the routineuse of CRRT for the treatment ofsepsis
When should acute RRT be initiated
Consensus statement 12
bullDemand for kidney function isdetermined by non-renalcomorbidities the severity ofthe acute disease and solute andfluid burden
When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

RRT is also effective at removingbiologically active substancesincluding cytokines butthere is still insufficientevidence to recommend the routineuse of CRRT for the treatment ofsepsis
When should acute RRT be initiated
Consensus statement 12
bullDemand for kidney function isdetermined by non-renalcomorbidities the severity ofthe acute disease and solute andfluid burden
When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

When should acute RRT be initiated
Consensus statement 12
bullDemand for kidney function isdetermined by non-renalcomorbidities the severity ofthe acute disease and solute andfluid burden
When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

When should acute RRT be initiated
Consensus statement 13
bullTotal kidney function is measuredusing a variety of different methodsChanges in kidney function andduration of kidney dysfunction canbe anticipated by markers of kidneydamage
When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

When should acute RRT be initiated
Consensus statement 14
bullThe demandndashcapacityimbalance is dynamicand should be evaluatedregularly
When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

When should acute RRT be initiated
Consensus statement 15
bullFor patients requiring multipletypes of organ support decisionsabout initiating or withholdingRRT should be consideredtogether with other therapies
When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

When should acute RRT be initiated
Consensus statement 16
bullOnce the decision to initiateRRT has been made thetherapy should be started assoon as possible typicallywithin less than 3 h
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 21
bull Selection of RRT modality depends on thecapabilityavailability of the technology
bull Different RRT modalities provide differentcapabilities
bull different machines may provide some butnot all modalities
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 22
bull CRRT recommended in situations whereshifts in fluid balance and metabolicfluctuations are poorly tolerated
bull Intermittent and prolonged intermittenttypes of RRT have a role when fluid andmetabolic fluctuations can be tolerated
Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

Both CRRT and IHD achieve adequate
metabolic control and neither modality has
been shown to be superior in terms of
survival
What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

What is the most appropriate therapy to meet a demandndashcapacity imbalance for a specific patient
Consensus statement 23
bullAvailability of technologies isdetermined by local regulationslocal resources including stafftheir trainingexperience andlaboratory support and financialconstraints
bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

bullSCUF (slow continuous ultrafiltration)
bullCVVH (continuous veno-venous haemofiltration
bullCVVHD (continuous veno-venous haemodialysis)
bullCVVHDF (continuous veno-venous haemodiafiltration
How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

How should RRT be integrated into other extracorporeal therapies
bull Consensus statement 31
In situations where other extracorporealtherapies are required continuous RRT isrecommended and integrated systems arepreferred over parallel systems
extracorporeal liver assist devices (ELADs)
ECLS in Cardiac Failure
When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

When should transition of modalities be considered (CRRT IRRT hybrid therapy)
Consensus statement 41
bullTransition of modalities should beconsidered if the demandndashcapacityimbalance or treatment prioritieshave changed and can be metbetter by an alternative technique
How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

How should patients be liberated from RRT
RRT should bediscontinued ifkidney functionhas recovered
Consensus statement
51
How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

How should patients be liberated from RRT
Consensus statement 52
bullTo determine sustainedrecovery of kidney functionwe recommend monitoring ofurine output and SCr duringRRT
How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

How should patients be liberated from RRT
C onsensus statement 53
bullFor patients requiring multipletypes of organ supportdecisions about withdrawingRRT should be consideredtogether with other therapies
Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

Before
Before CRRT is started patients should have
a complete nursing assessment
bull Fluid status
bull Fluid input
bull Blood pressure
bull Dosages of any vasopressors
bull Weightbull Presence of edemabull CVPbull NaK and ABGs
Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

Nursing Management
During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

During
Once CRRT is started
bull Blood pressure central venous pressure andweight monitoring
bull The bedside nurse should discuss the possibilityof reducing intake to minimal volumes of fluidsif at all possible and concentrating medicationsand infusions to minimize fluid intake if thetarget not acheived
bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

bull Mechanical failures can occur if alarms are ignored or bypassed without determining the cause of the alarms
bull If scales are not properly calibrated the volumes of fluid administered and removed may not be the programmed volumes
541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

541 We suggest initiating RRT in patients with AKI via an uncuffed non tunneled dialysis catheter rather than a tunneled catheter (2D)
542 When choosing a vein for insertion of a dialysis catheter in patients with AKI consider these preferences (Not Graded)
bull First choice right jugular vein
bull Second choice femoral vein
bull Third choice left jugular vein
bull Last choice subclavian vein with preference for the dominant side
Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

Anticoagulation
CRRT can be performed with or without anticoagulation
The choice of anticoagulant depends on
bull The physicianrsquos preference
bull The patientrsquos condition
bull The familiarity of the nursing staff with anticoagulation regimens
The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

The bedside nurse is responsiblefor monitoring any adverse effectsof anticoagulation includinghemorrhage formation ofhematomas thrombocytopeniaand allergic reactions
Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

Heparin
bull The least expensive anticoagulant
bull Either systemically or regionally
When heparin is used
bull The hemofilter may be flushed with a dilute heparin solution continuously or intermittently
Systemic heparinization includes
bull Infusing heparin into a separate intravenous access or into the arterial side of the CRRT circuit
bull Mixing of the heparin with the blood from the patient before the blood reaches the filter
bull Anticoagulation of the circuit as well as for the patient
Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

Argatroban and lepirudin
bullDirect thrombin inhibitors
bullHIT
Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

Lepirudin is cleared by the kidneys and therefore may not be the drug of choice
for patients in ARF
Argatroban is eliminated by the liver and is therefore more suitable for use in
patients with renal failure
Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

Citrate
excellent anticoagulant ability and potential to prolong circuit life
bull Calcium is an essential component of the clotting cascade
bull Citrate binds to the calcium in the patientrsquos blood within the CRRT system and prevents clotting
Citrate is infused prefilter into the CRRT system and calcium is typically infused via another intravenous line outside the circuit
Ionized calcium levels are routinely monitored
1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

1048708Heparin
bull 250500 Uhr
1048708HIT Argatroban
bull 1048708051 mghr
1048708Bleeding risk
bull 1048708Citrate
bull 1048708No anticoagulation
Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

Dialysate
Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT

Conculsions
Critically ill patients AKI occurs in up to 30 of all ICU admissions
CRRT is almost exclusively applied to patients in (ICU)
Restrict monitoring and follow up of the patients during CRRT is mandatory
Well trained nurse is the corner stone of adequate CRRT