Embed Size (px)
Citation preview
CRRT for AKI and non AKI patients in the ICU
Thomas RIMMELE – MD PhD
Anesthesiology and Intensive Care Medicine
Edouard Herriot Hospital
LYON, FRANCE
April, 12 2018 – Dalat, Viet-Nam
Conflicts of Interest
Scientific partnership with the following companies:
- Baxter
- Fresenius Medical Care
- Bbraun
- Nikkiso
- Bellco-Medtronic
- Biomérieux
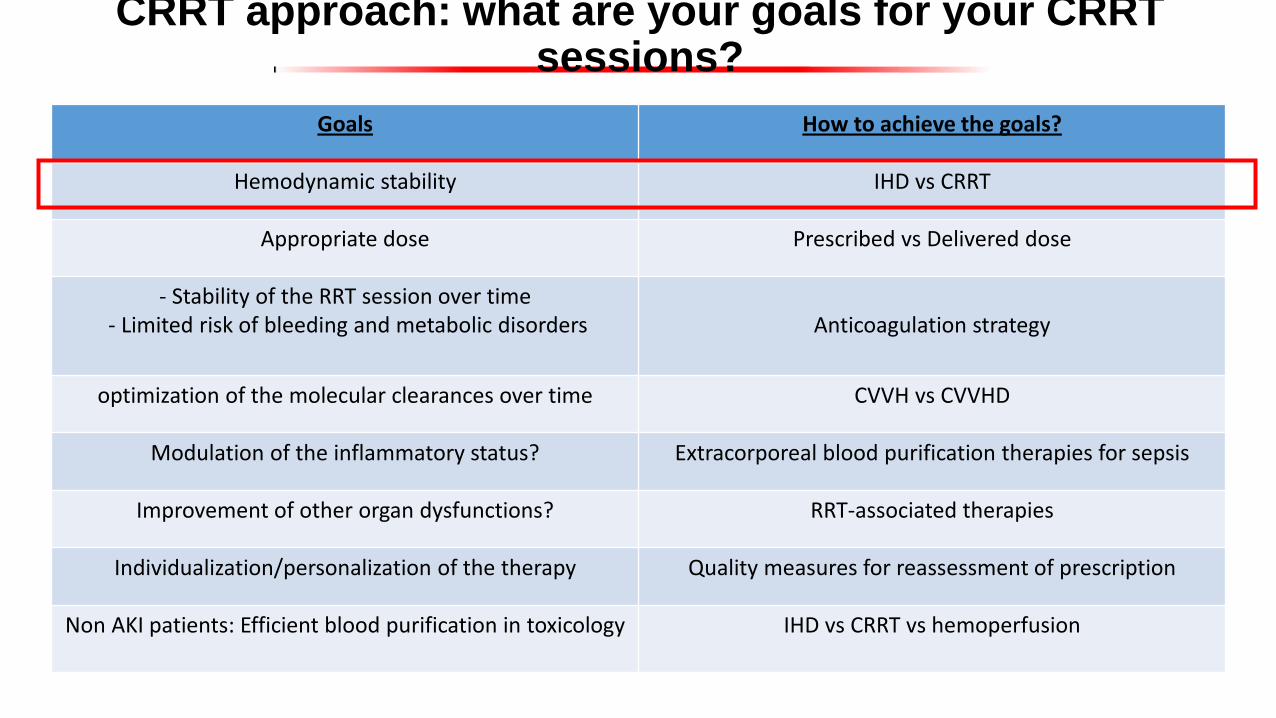
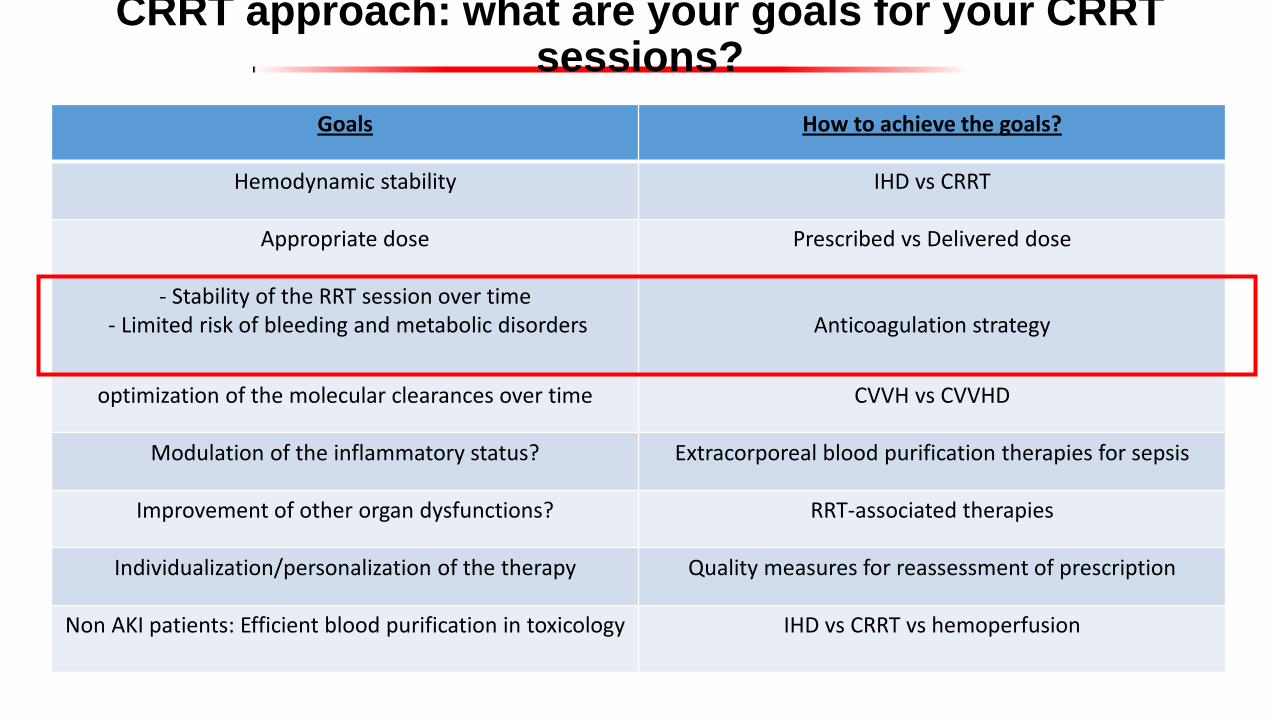
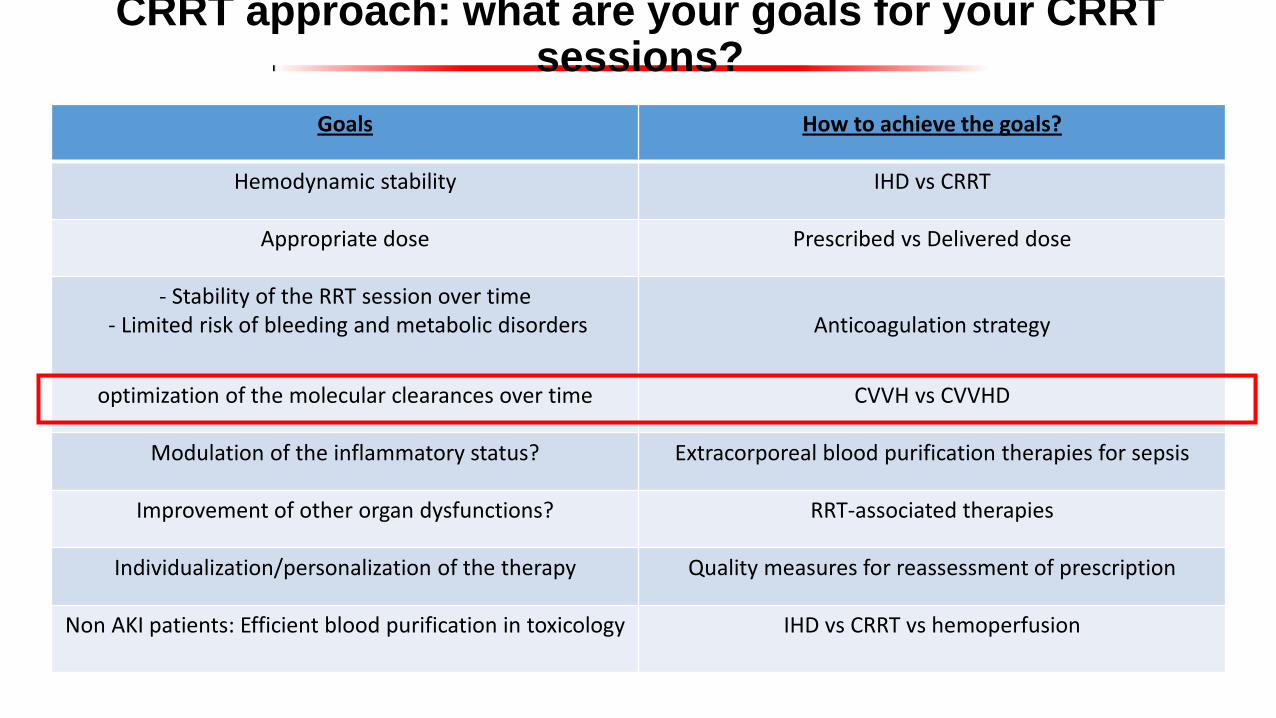
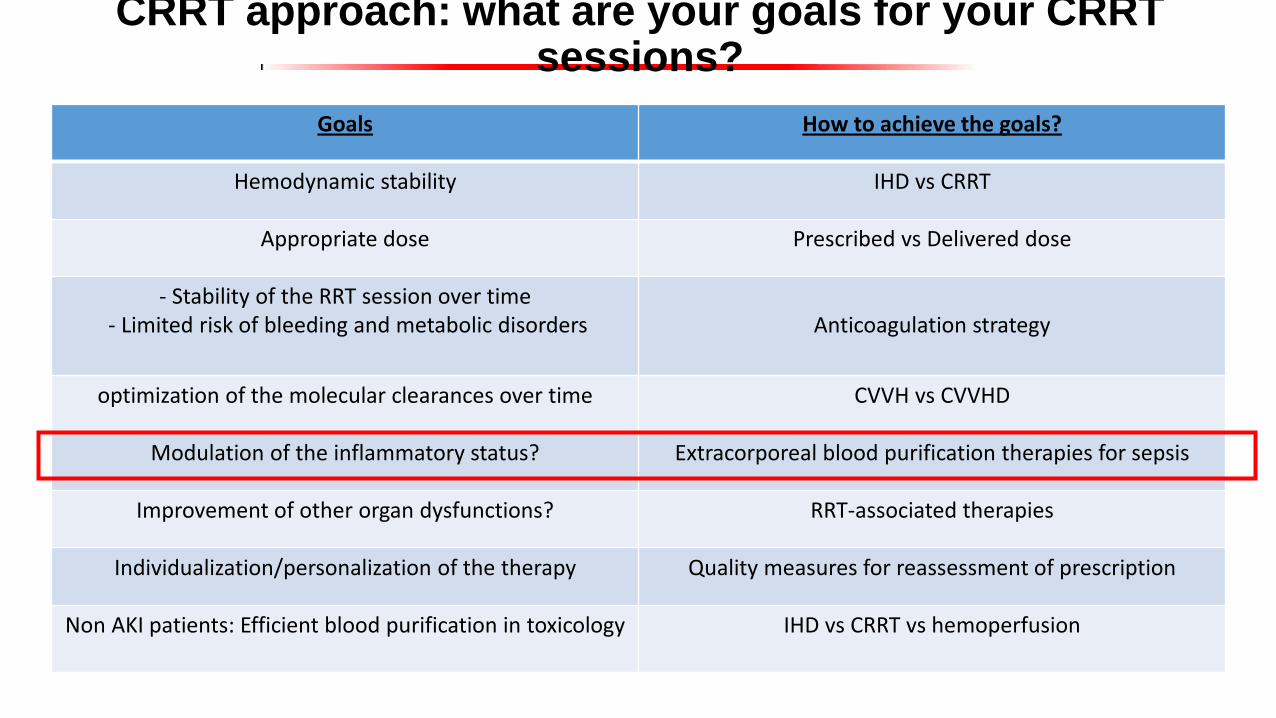
CRRT approach: what are your goals for your CRRT sessions?
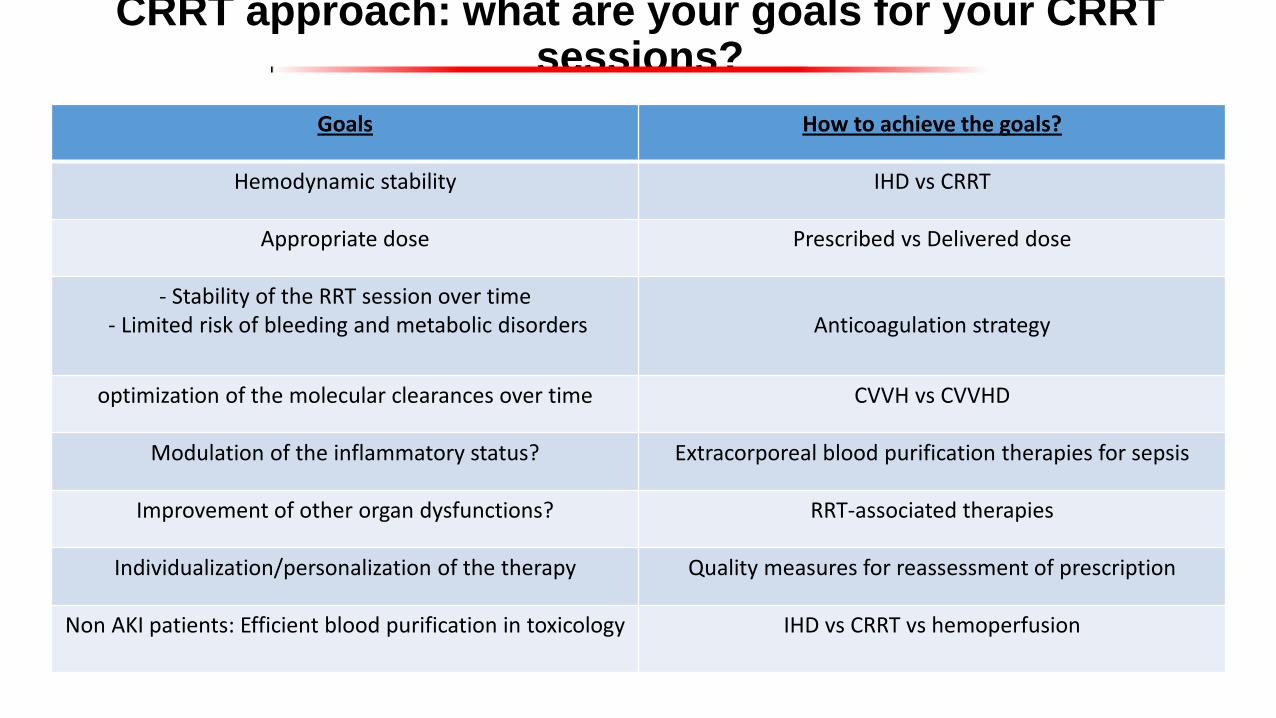
Goals How to achieve the goals?
Hemodynamic stability IHD vs CRRT
Appropriate dose Prescribed vs Delivered dose
- Stability of the RRT session over time - Limited risk of bleeding and metabolic disorders
Anticoagulation strategy
optimization of the molecular clearances over time CVVH vs CVVHD
Modulation of the inflammatory status? Extracorporeal blood purification therapies for sepsis
Improvement of other organ dysfunctions? RRT-associated therapies
Individualization/personalization of the therapy Quality measures for reassessment of prescription
Non AKI patients: Efficient blood purification in toxicology IHD vs CRRT vs hemoperfusion
CRRT approach: what are your goals for your CRRT sessions?
CRRT approach: what are your goals for your CRRT sessions?
Goals How to achieve the goals?
Hemodynamic stability IHD vs CRRT
Appropriate dose Prescribed vs Delivered dose
- Stability of the RRT session over time - Limited risk of bleeding and metabolic disorders
Anticoagulation strategy
optimization of the molecular clearances over time CVVH vs CVVHD
Modulation of the inflammatory status? Extracorporeal blood purification therapies for sepsis
Improvement of other organ dysfunctions? RRT-associated therapies
Individualization/personalization of the therapy Quality measures for reassessment of prescription
Non AKI patients: Efficient blood purification in toxicology IHD vs CRRT vs hemoperfusion

CRRT IHD
IHD vs CRRT:a 20-yr controversy

• Avoids risks associated with continuous anticoagulation
• (Easily deployed at the bedside)
• Allows the patient to achieve greater mobility
• Cheaper “per se”
Advantages of IHD Advantages of CRRT
• Greater hemodynamic stability
• Continuous control of volume status
• Steady control of electrolyte and acid-base status
• Temperature control
• Avoidance of solute swings and cerebral edema
• Superior uremic control

RRT modality (CRRT vs IHD)
KDIGO guidelines. Kidney Int suppl 2012

Friedrich et al. Crit Care 2012
RRT modality and mortality
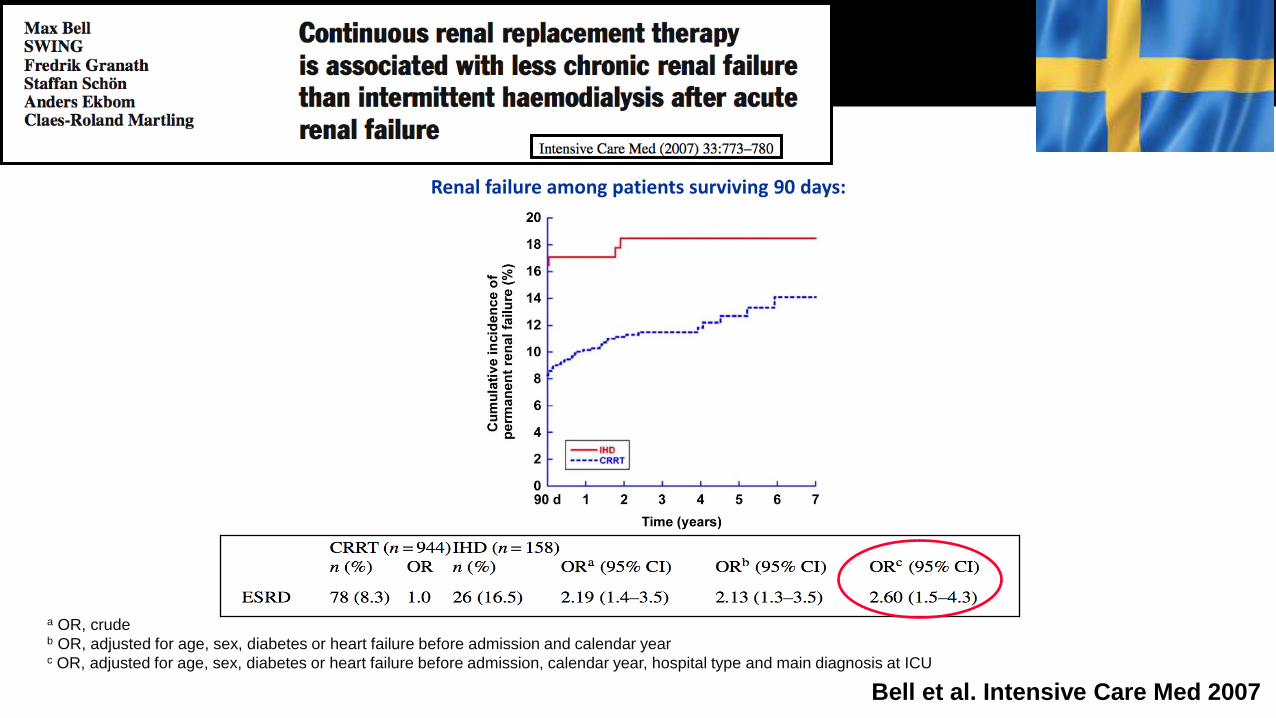
a OR, crude b OR, adjusted for age, sex, diabetes or heart failure before admission and calendar year c OR, adjusted for age, sex, diabetes or heart failure before admission, calendar year, hospital type and main diagnosis at ICU
Renal failure among patients surviving 90 days:
Bell et al. Intensive Care Med 2007
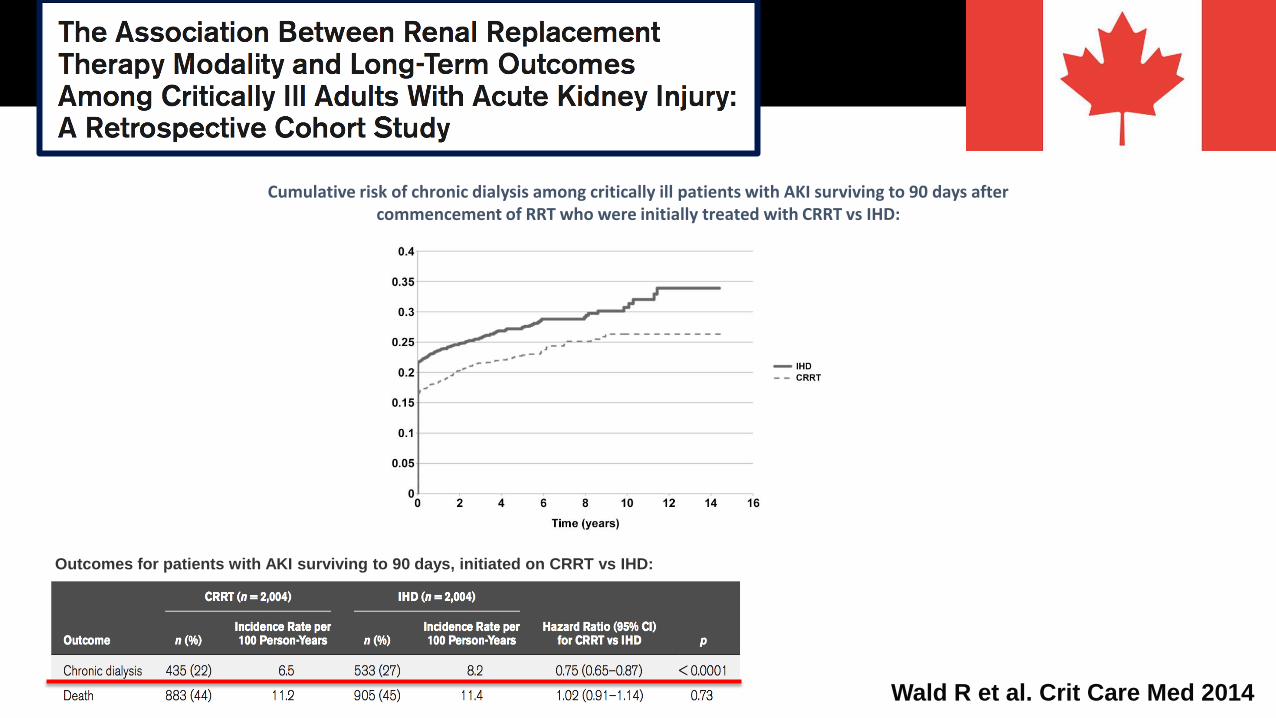
Wald R et al. Crit Care Med 2014
Cumulative risk of chronic dialysis among critically ill patients with AKI surviving to 90 days after commencement of RRT who were initially treated with CRRT vs IHD:
Outcomes for patients with AKI surviving to 90 days, initiated on CRRT vs IHD:

Variable Odds ratio (95% CI) p
Technique (IHD vs CRRT) 0.912 (0.835–0.996) 0.04
Shock (yes vs no) 1.188 (1.060–1.331) 0.003
Vasopressors (yes vs no) 1.192 (1.088–1.305) 0.0002
Ventilation (yes vs no) 1.541 (1.404–1.692) <0.0001
Cardiac arrest (yes vs no) 1.243 (1.009–1.531) 0.0413
Cardiac surgery 1.676 (1.281–2.192) 0.0002
Non terminal CKD (yes vs no) 0.635 (0.575–0.702) <0.0001
Center (<250 vs >450 beds) 0.547 (0.427–0.702) <0.0001
Multivariate analysis: 1 million ICU patients over 4 years
Bonnassieux et al. Crit Care Med 2017

CRRT approach: what are your goals for your CRRT sessions?
Goals How to achieve the goals?
Hemodynamic stability IHD vs CRRT
Appropriate dose Prescribed vs Delivered dose
- Stability of the RRT session over time - Limited risk of bleeding and metabolic disorders
Anticoagulation strategy
optimization of the molecular clearances over time CVVH vs CVVHD
Modulation of the inflammatory status? Extracorporeal blood purification therapies for sepsis
Improvement of other organ dysfunctions? RRT-associated therapies
Individualization/personalization of the therapy Quality measures for reassessment of prescription
Non AKI patients: Efficient blood purification in toxicology IHD vs CRRT vs hemoperfusion
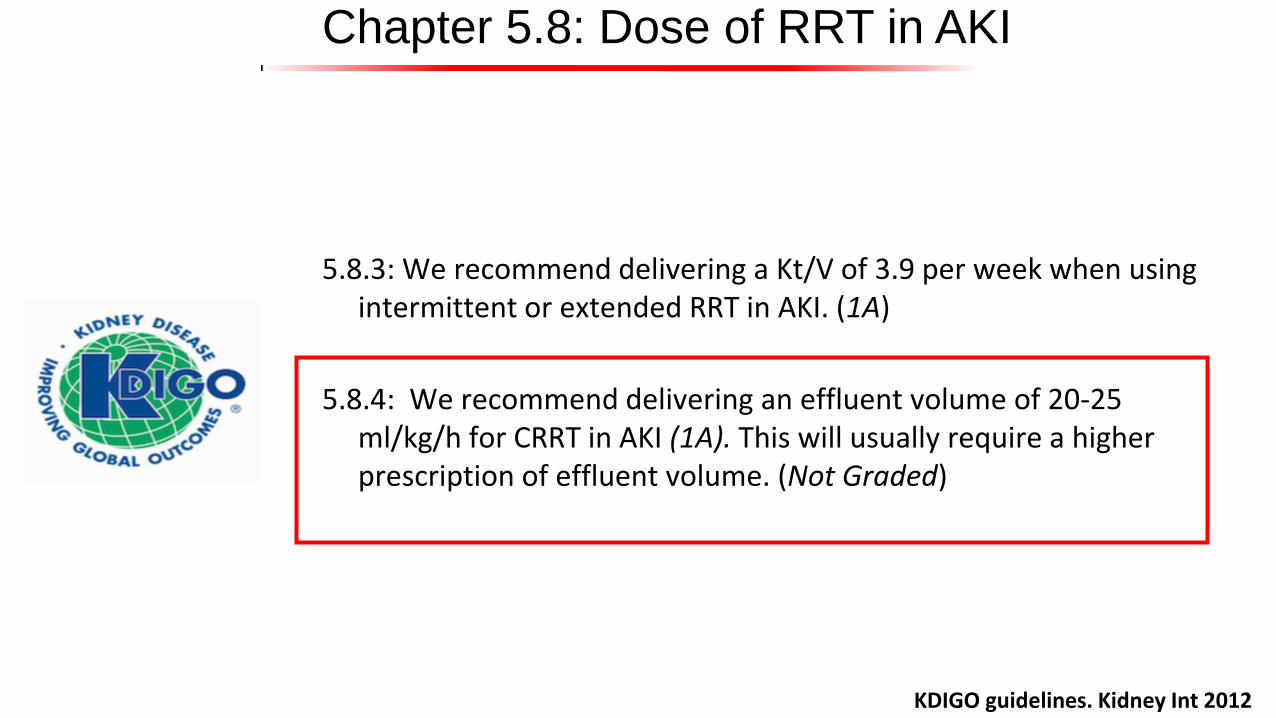
Chapter 5.8: Dose of RRT in AKI
5.8.3: We recommend delivering a Kt/V of 3.9 per week when using intermittent or extended RRT in AKI. (1A)
5.8.4: We recommend delivering an effluent volume of 20-25 ml/kg/h for CRRT in AKI (1A). This will usually require a higher prescription of effluent volume. (Not Graded)
KDIGO guidelines. Kidney Int 2012
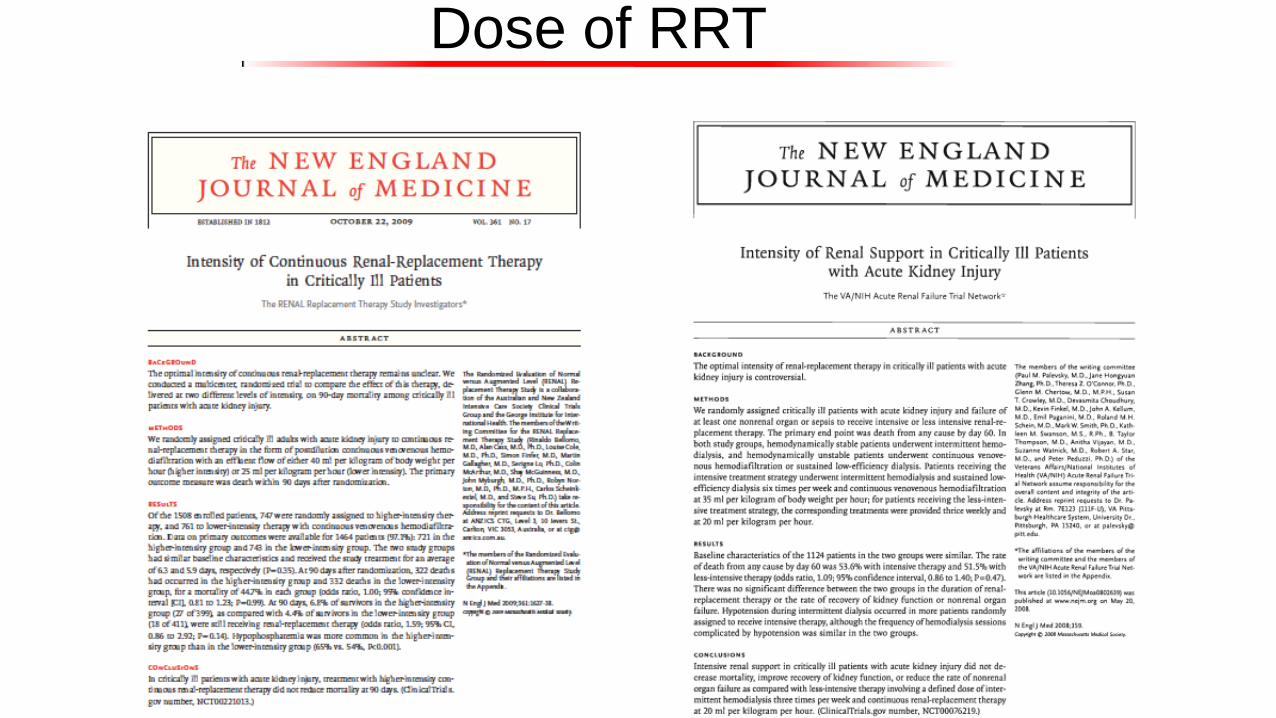
Dose of RRT

Dose of RRT

Dose of RRT
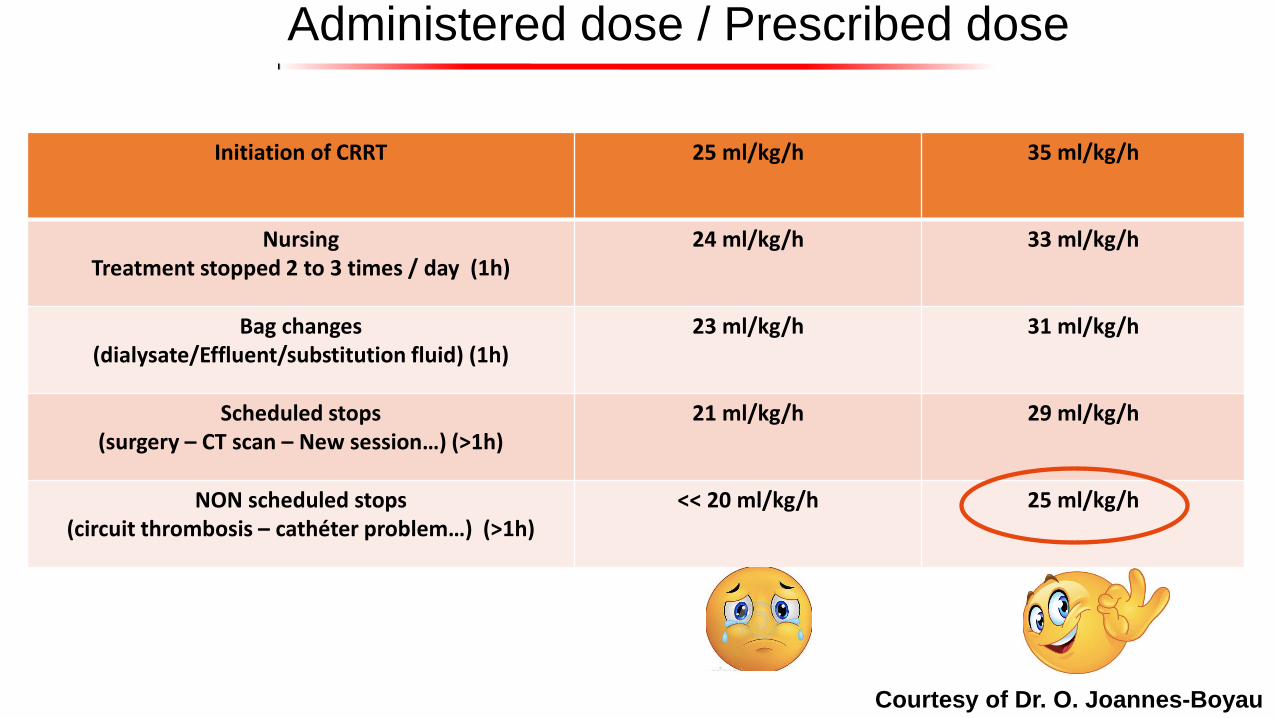
Administered dose / Prescribed dose
Initiation of CRRT 25 ml/kg/h 35 ml/kg/h
Nursing Treatment stopped 2 to 3 times / day (1h)
24 ml/kg/h 33 ml/kg/h
Bag changes (dialysate/Effluent/substitution fluid) (1h)
23 ml/kg/h 31 ml/kg/h
Scheduled stops (surgery – CT scan – New session…) (>1h)
21 ml/kg/h 29 ml/kg/h
NON scheduled stops (circuit thrombosis – cathéter problem…) (>1h)
<< 20 ml/kg/h 25 ml/kg/h
Courtesy of Dr. O. Joannes-Boyau
CRRT approach: what are your goals for your CRRT sessions?
Goals How to achieve the goals?
Hemodynamic stability IHD vs CRRT
Appropriate dose Prescribed vs Delivered dose
- Stability of the RRT session over time - Limited risk of bleeding and metabolic disorders
Anticoagulation strategy
optimization of the molecular clearances over time CVVH vs CVVHD
Modulation of the inflammatory status? Extracorporeal blood purification therapies for sepsis
Improvement of other organ dysfunctions? RRT-associated therapies
Individualization/personalization of the therapy Quality measures for reassessment of prescription
Non AKI patients: Efficient blood purification in toxicology IHD vs CRRT vs hemoperfusion
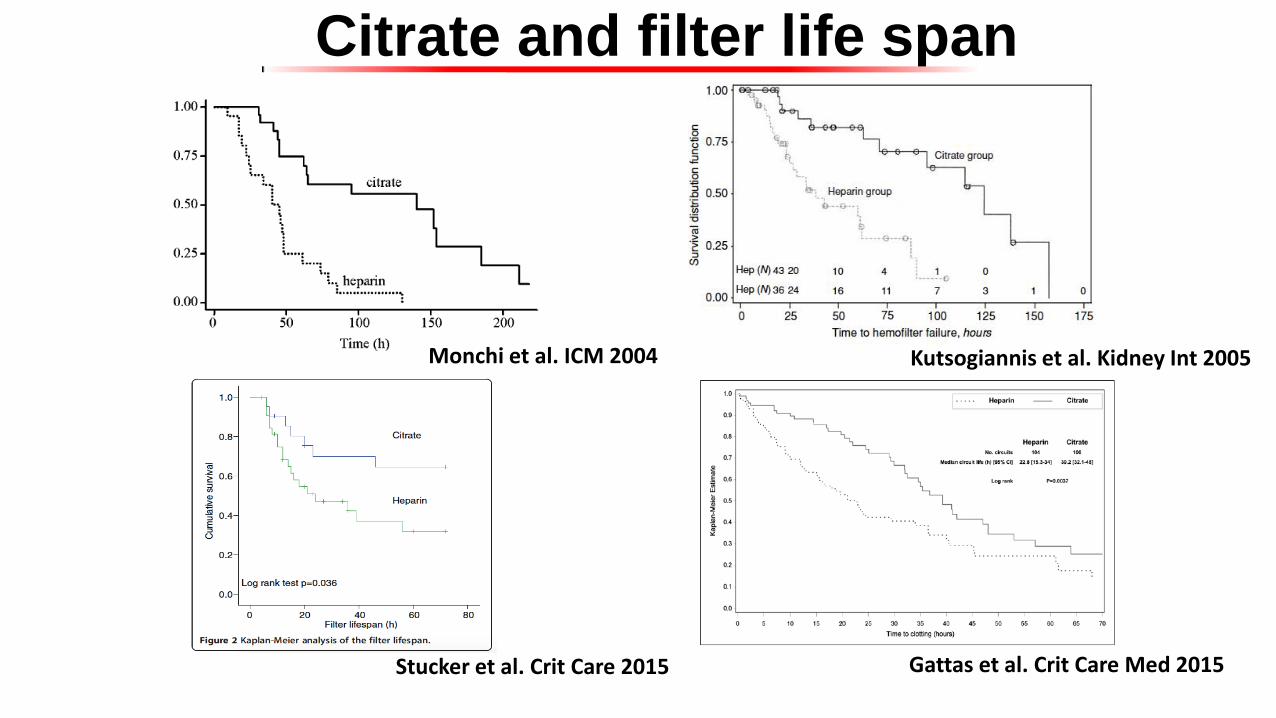
Monchi et al. ICM 2004 Kutsogiannis et al. Kidney Int 2005
Stucker et al. Crit Care 2015 Gattas et al. Crit Care Med 2015
Citrate and filter life span
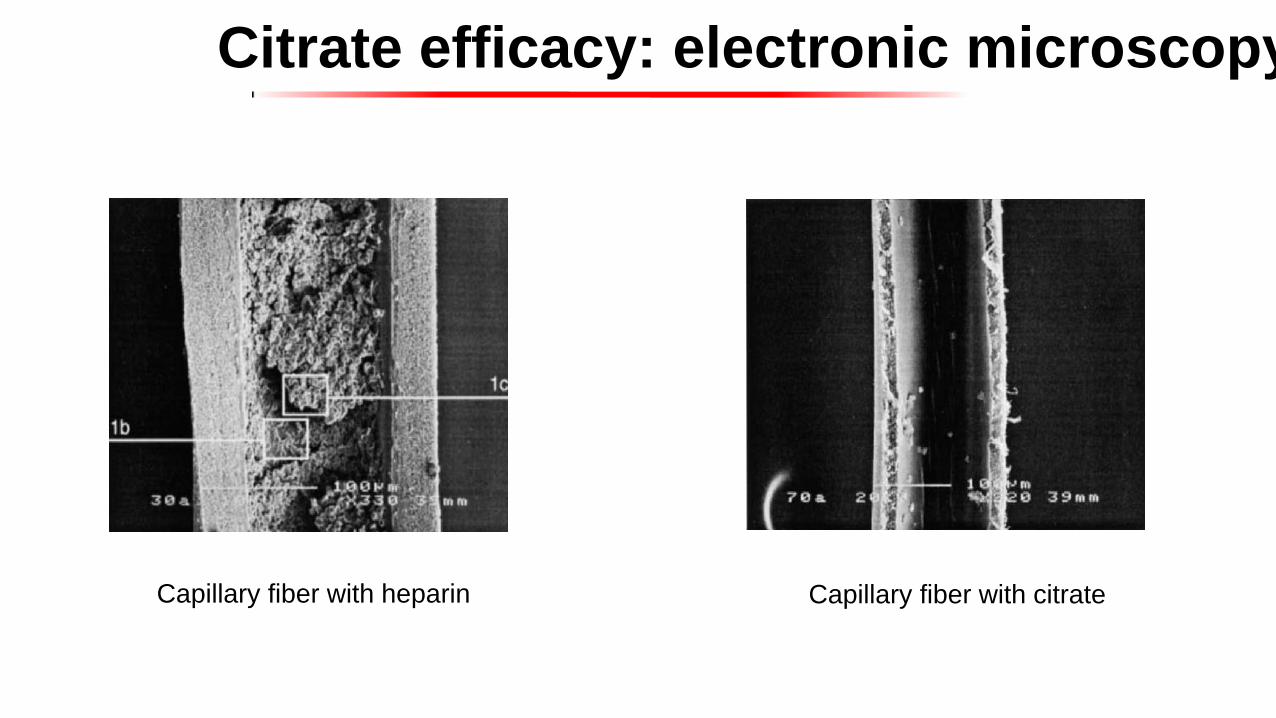
Citrate efficacy: electronic microscopy
Capillary fiber with heparin Capillary fiber with citrate
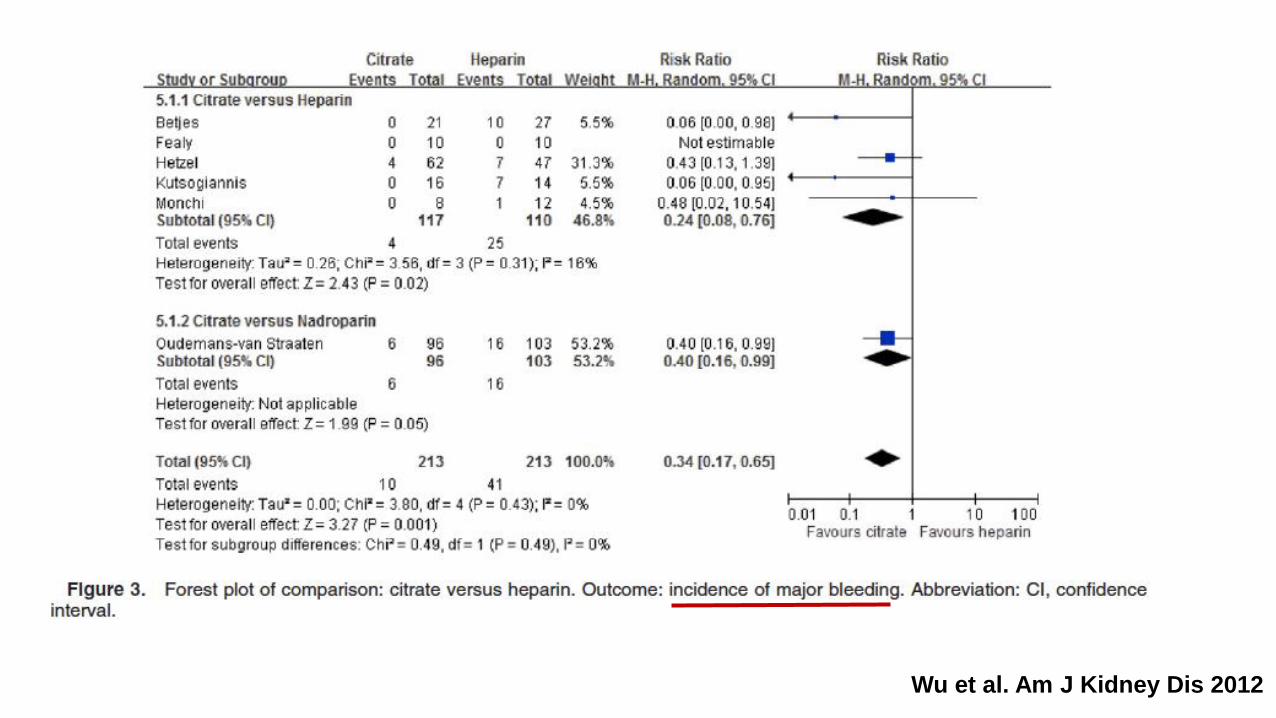
Wu et al. Am J Kidney Dis 2012

Schilder et al. Critical Care 2014
Stucker et al. Critical Care 2015
Gattas et al. Crit Care Med 2015
Citrate =
- Less bleeding complications
- Higher filter life time
- Less unwanted stops = optimized administered dialysis dose
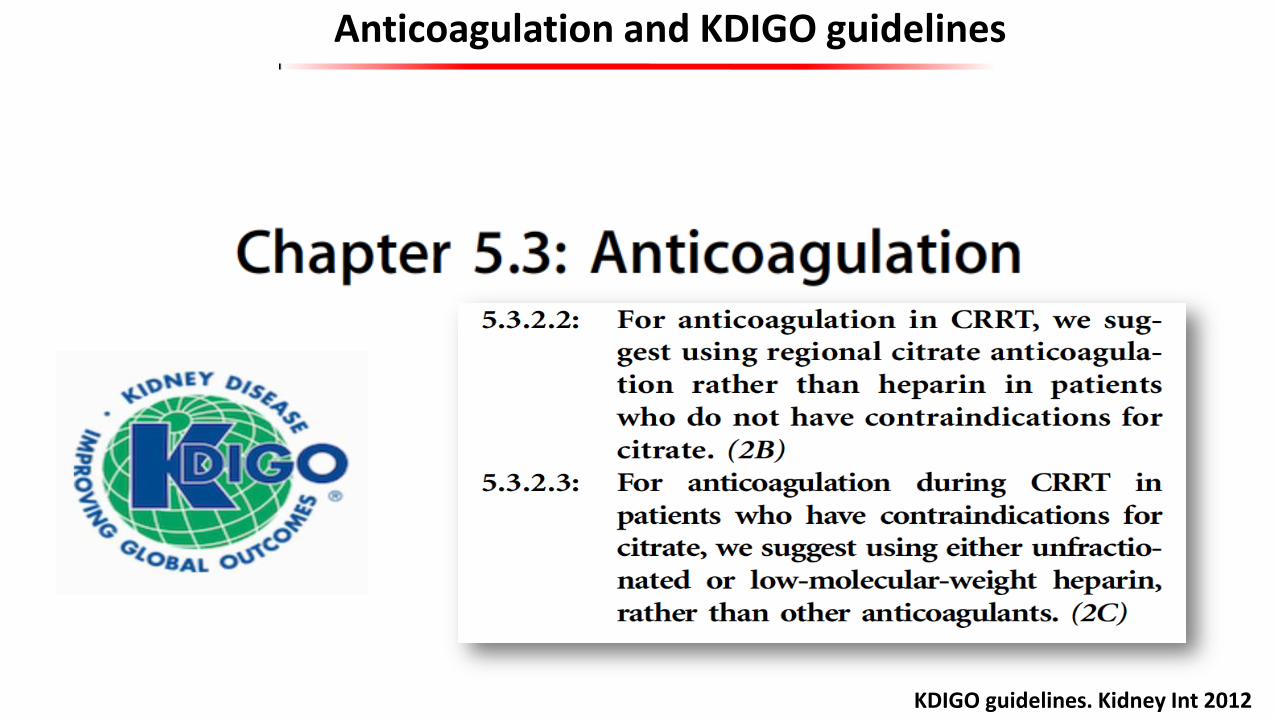
Anticoagulation and KDIGO guidelines
KDIGO guidelines. Kidney Int 2012
Any issue(s) with citrate?
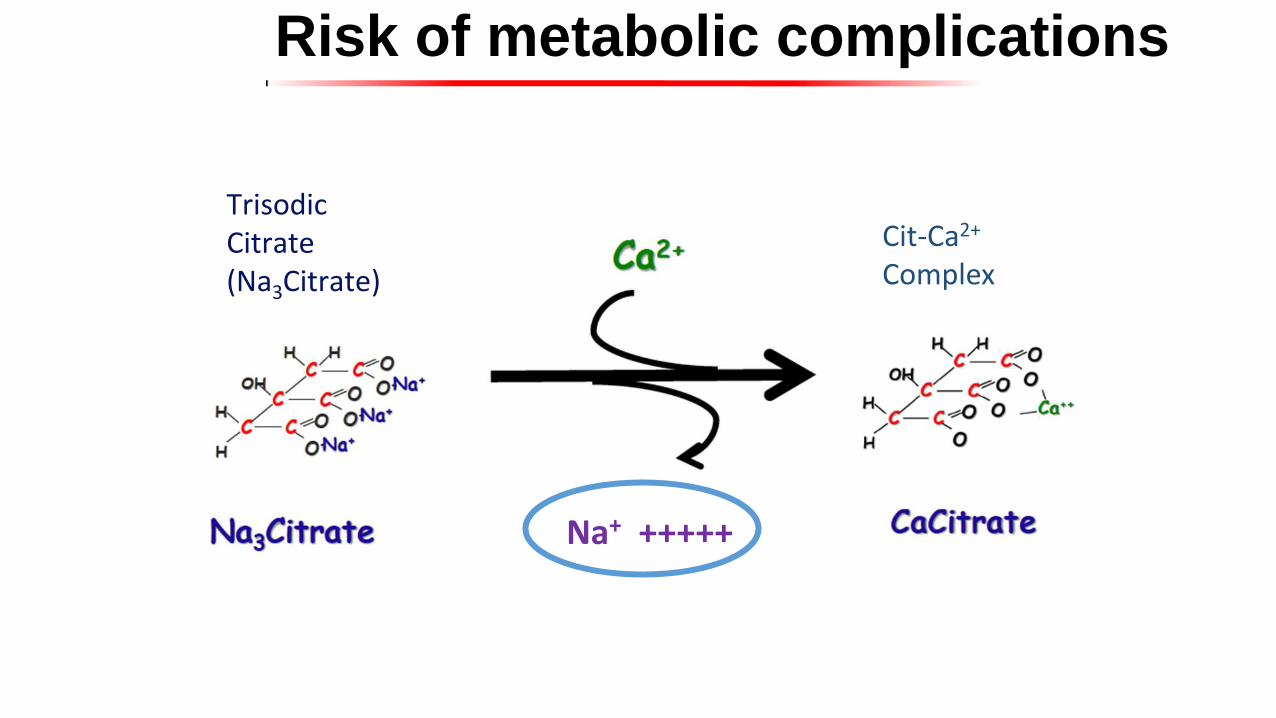
Risk of metabolic complications
Trisodic Citrate (Na3Citrate)
Cit-Ca2+
Complex
Na+ +++++

Strong Ion Difference
SID = (Na+ + K+ + Ca2+ + Mg2+ + UA+) – (Cl- + UA-)
- Metabolic alkalosis - Metabolic acidosis - Hypernatremia - Hypocalcemia - Hypercalcemia - Hypomagnesemia
Citrate overload or citrate
accumulation?
What is the best way to avoid these metabolic complications?

= How should I proceed to give to the patient as little citrate as
possible?
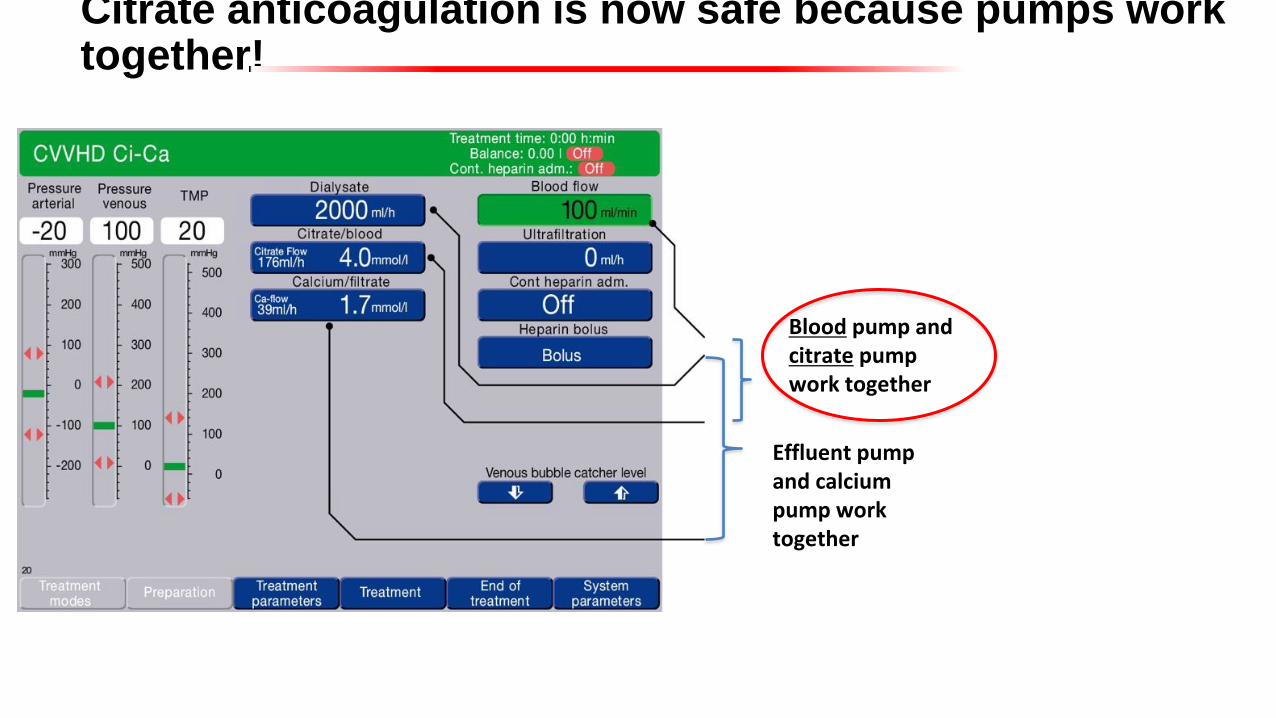
Citrate anticoagulation is now safe because pumps work together!
Blood pump and citrate pump work together
Effluent pump and calcium pump work together


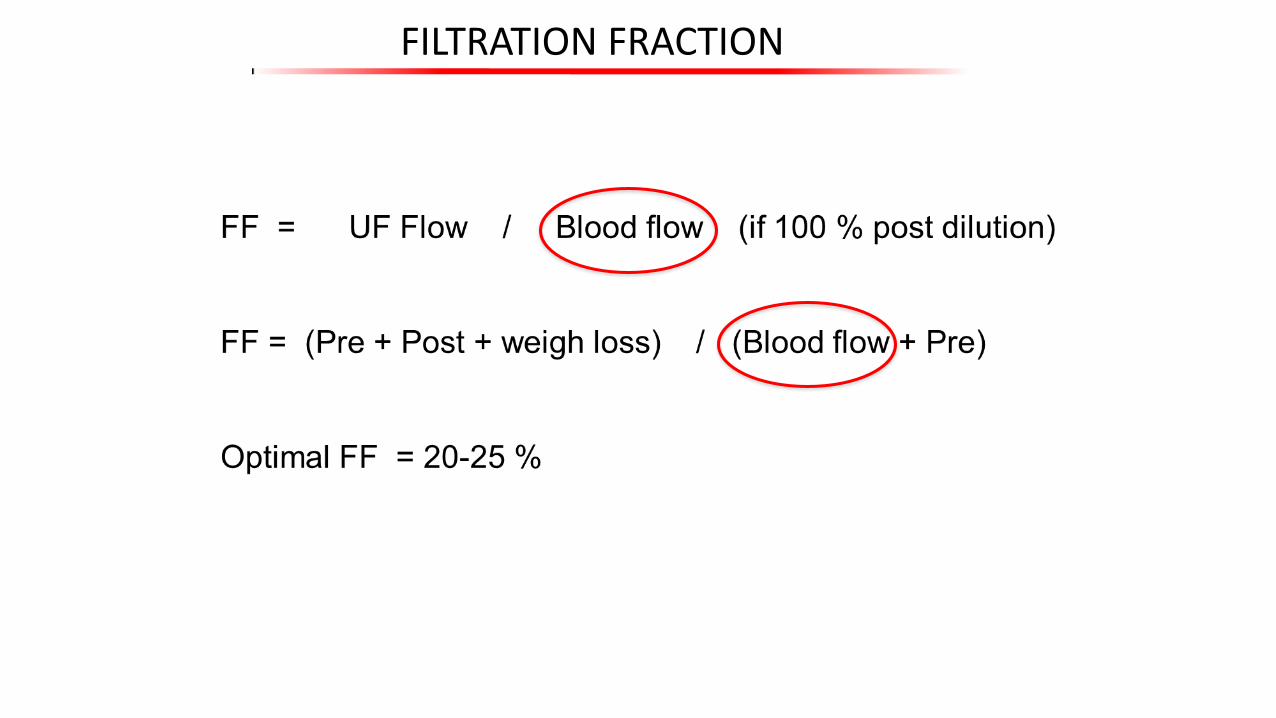
FILTRATION FRACTION
Courtesy of Pr. Didier Journois
FILTRATION FRACTION

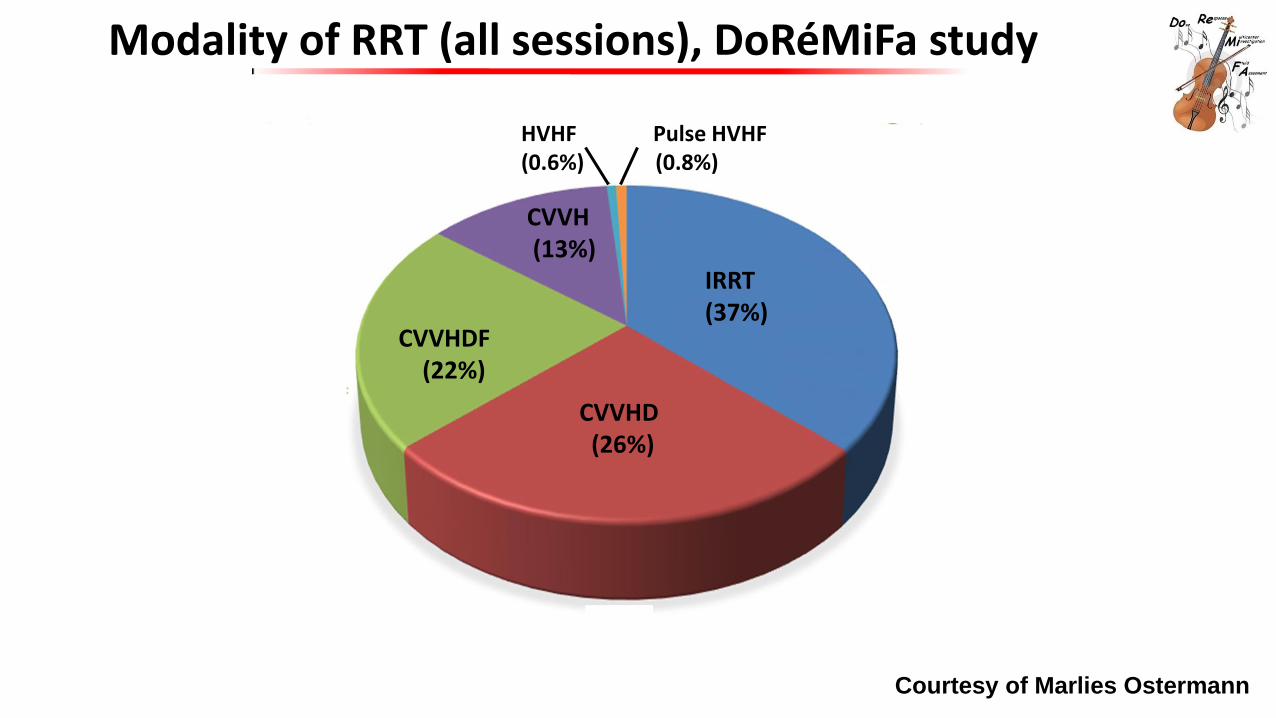
Modality of RRT (all sessions), DoRéMiFa study
CVVHDF (22%)
CVVH (13%)
IRRT (37%)
CVVHD (26%)
HVHF Pulse HVHF (0.6%) (0.8%)
Courtesy of Marlies Ostermann
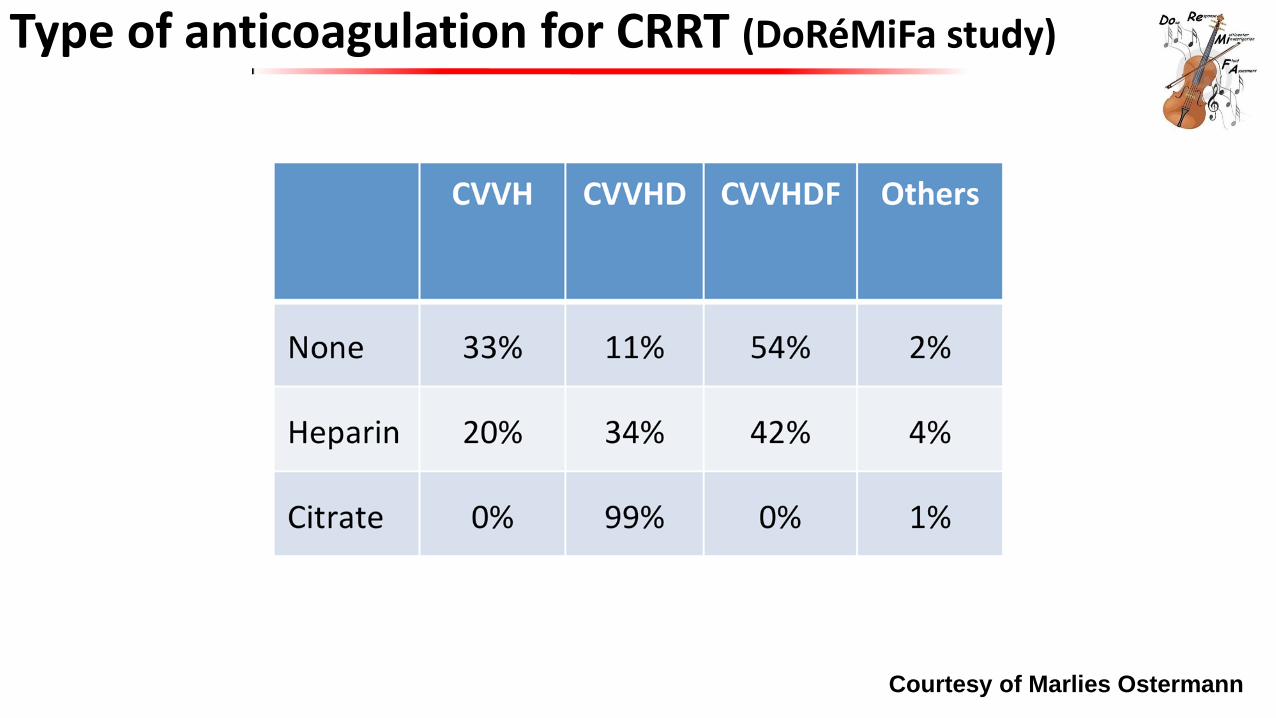
Type of anticoagulation for CRRT (DoRéMiFa study)
Courtesy of Marlies Ostermann
CRRT approach: what are your goals for your CRRT sessions?
Goals How to achieve the goals?
Hemodynamic stability IHD vs CRRT
Appropriate dose Prescribed vs Delivered dose
- Stability of the RRT session over time - Limited risk of bleeding and metabolic disorders
Anticoagulation strategy
optimization of the molecular clearances over time CVVH vs CVVHD
Modulation of the inflammatory status? Extracorporeal blood purification therapies for sepsis
Improvement of other organ dysfunctions? RRT-associated therapies
Individualization/personalization of the therapy Quality measures for reassessment of prescription
Non AKI patients: Efficient blood purification in toxicology IHD vs CRRT vs hemoperfusion
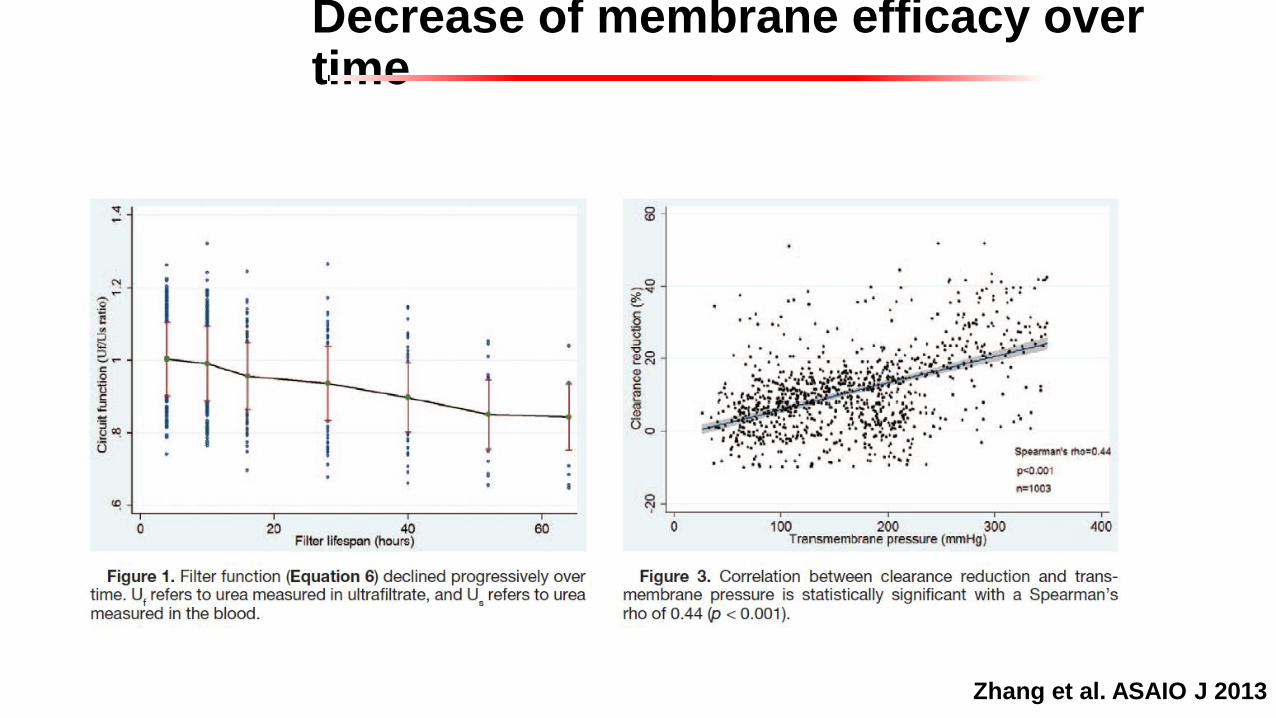
Decrease of membrane efficacy over time
Zhang et al. ASAIO J 2013
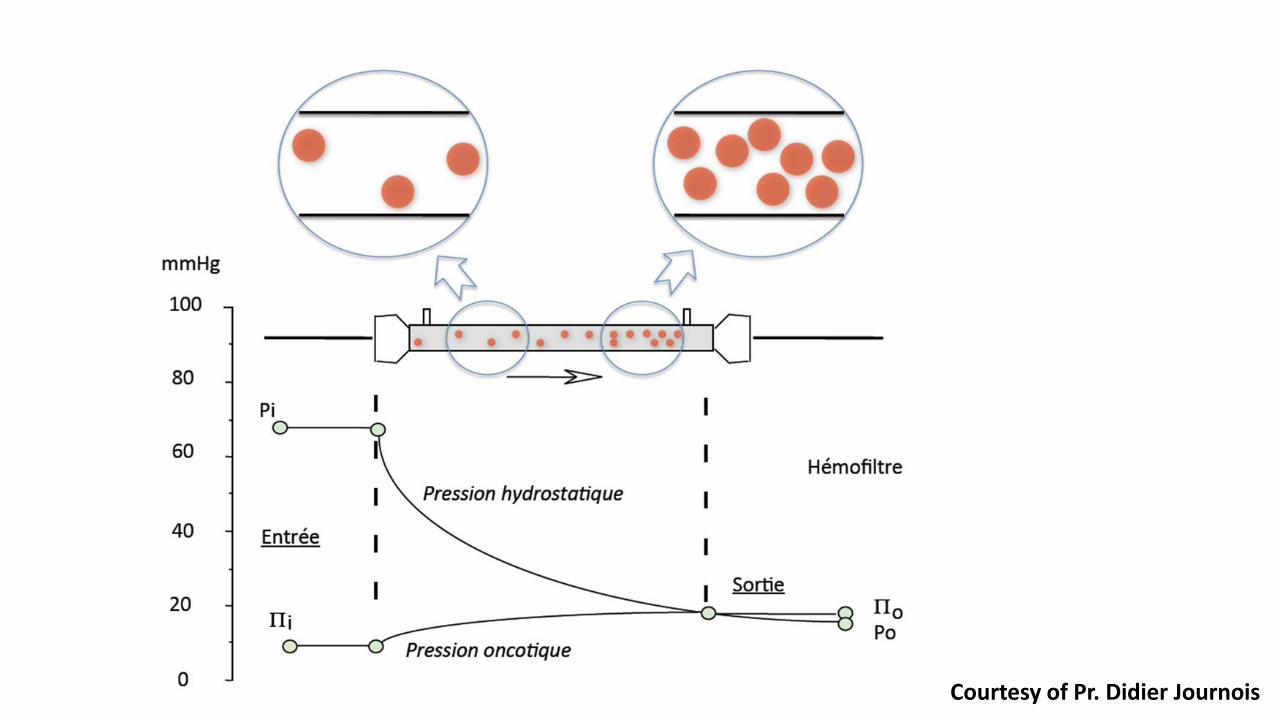
Courtesy of Pr. Didier Journois
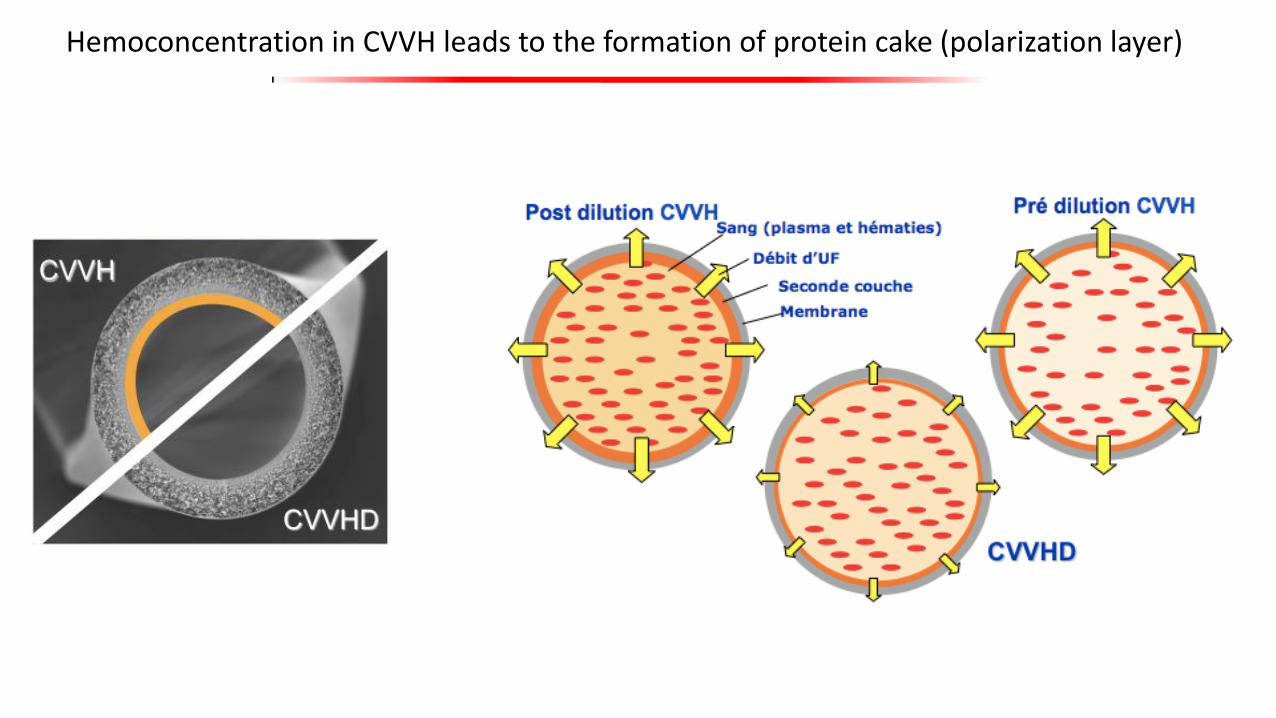
Hemoconcentration in CVVH leads to the formation of protein cake (polarization layer)
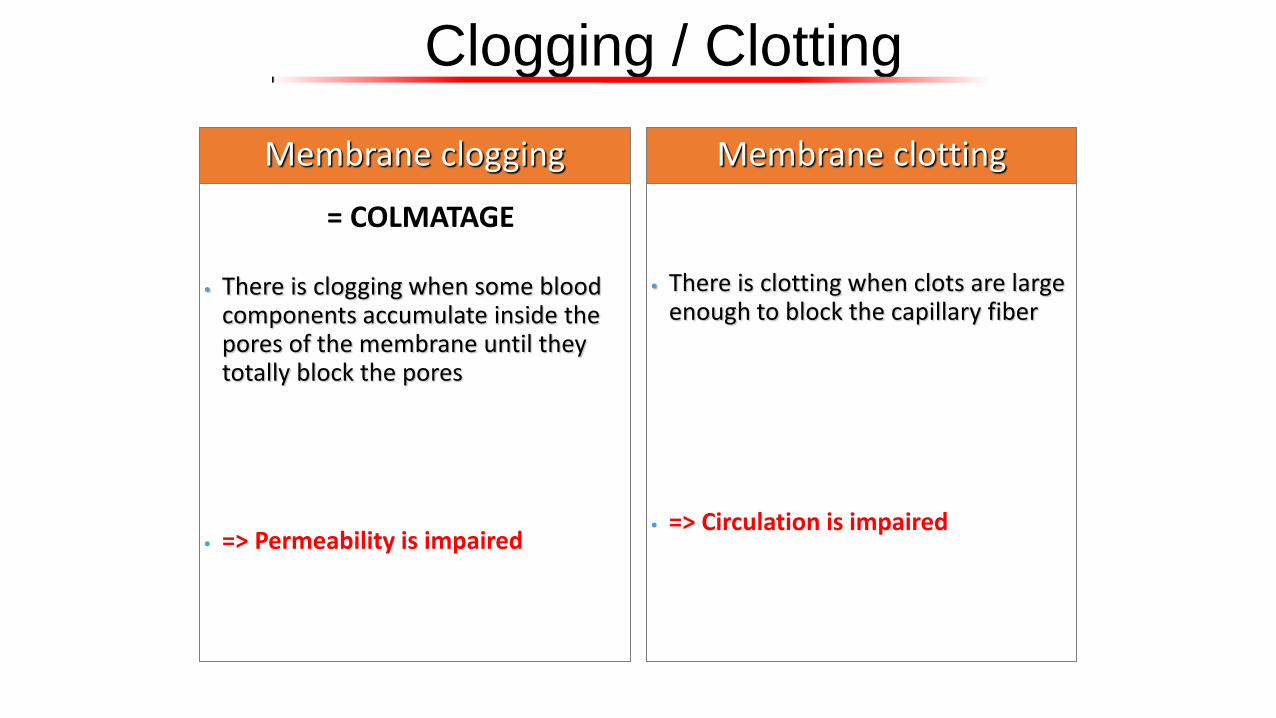
Clogging / Clotting
• There is clogging when some blood components accumulate inside the pores of the membrane until they totally block the pores
• => Permeability is impaired
Membrane clogging
• There is clotting when clots are large enough to block the capillary fiber
• => Circulation is impaired
Membrane clotting
= COLMATAGE
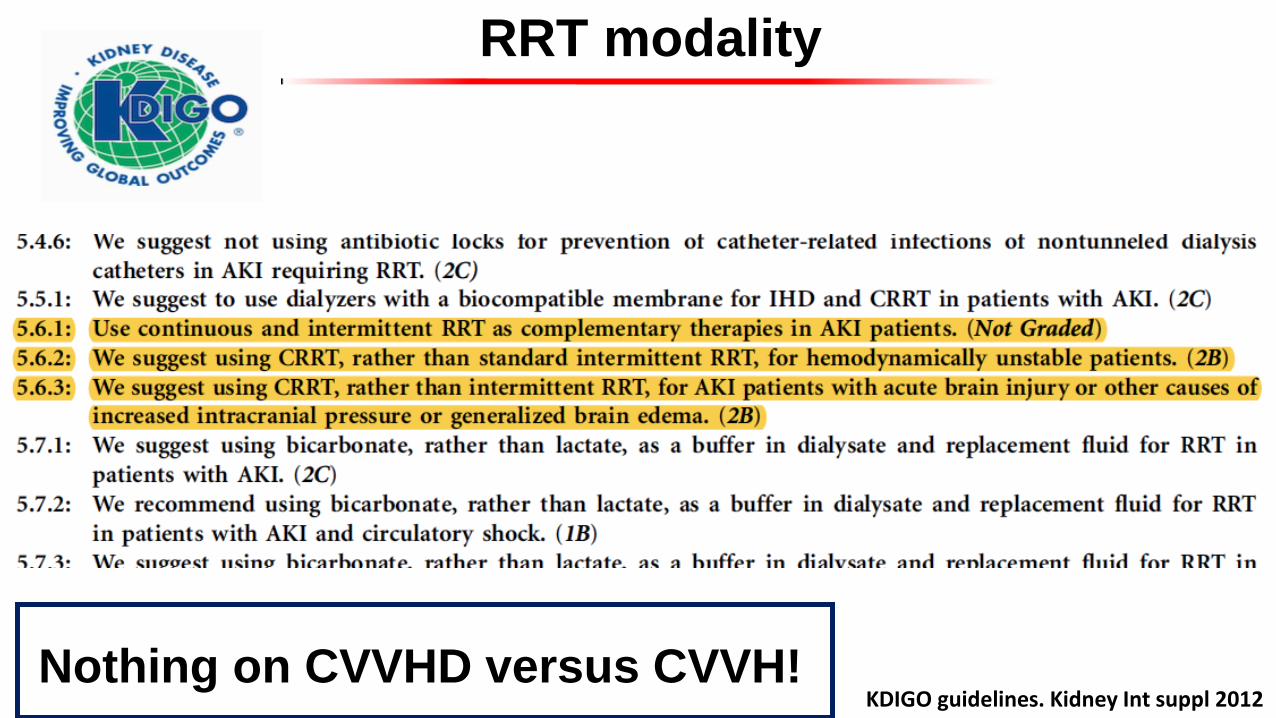
RRT modality
KDIGO guidelines. Kidney Int suppl 2012 Nothing on CVVHD versus CVVH!
CRRT approach: what are your goals for your CRRT sessions?
Goals How to achieve the goals?
Hemodynamic stability IHD vs CRRT
Appropriate dose Prescribed vs Delivered dose
- Stability of the RRT session over time - Limited risk of bleeding and metabolic disorders
Anticoagulation strategy
optimization of the molecular clearances over time CVVH vs CVVHD
Modulation of the inflammatory status? Extracorporeal blood purification therapies for sepsis
Improvement of other organ dysfunctions? RRT-associated therapies
Individualization/personalization of the therapy Quality measures for reassessment of prescription
Non AKI patients: Efficient blood purification in toxicology IHD vs CRRT vs hemoperfusion
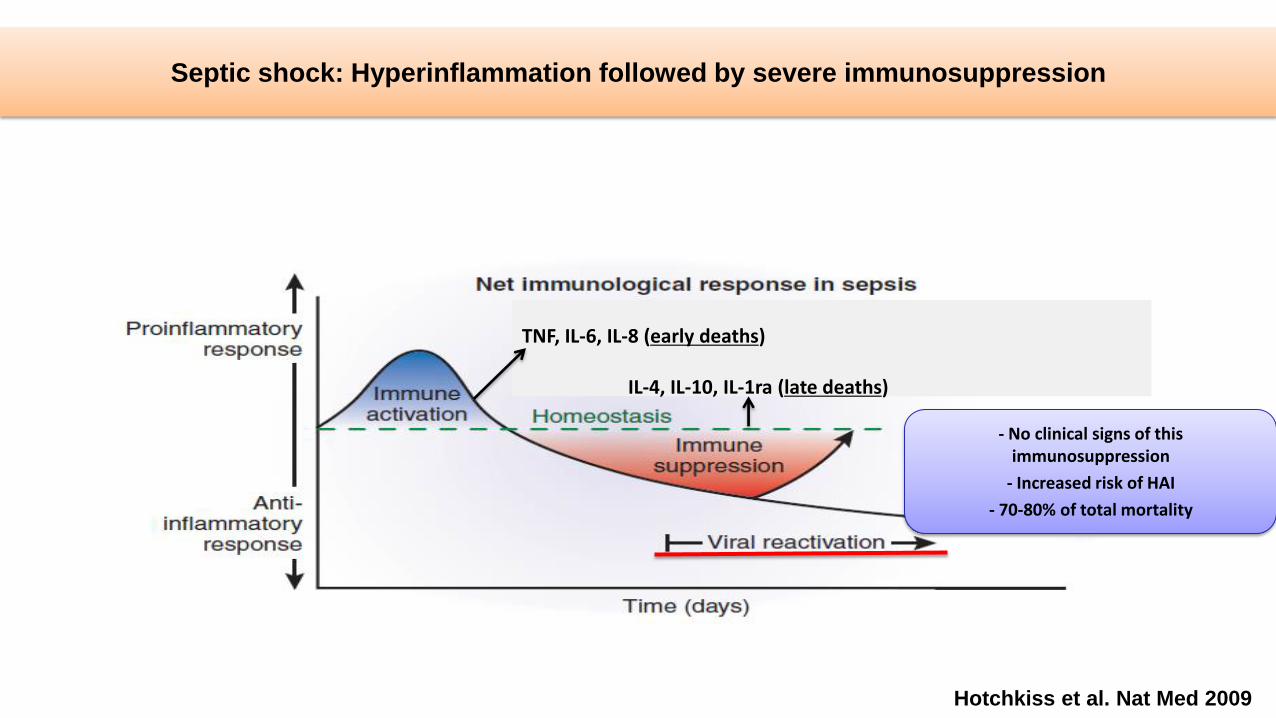
Hotchkiss et al. Nat Med 2009
Septic shock: Hyperinflammation followed by severe immunosuppression
TNF, IL-6, IL-8 (early deaths) IL-4, IL-10, IL-1ra (late deaths)
- No clinical signs of this immunosuppression
- Increased risk of HAI
- 70-80% of total mortality
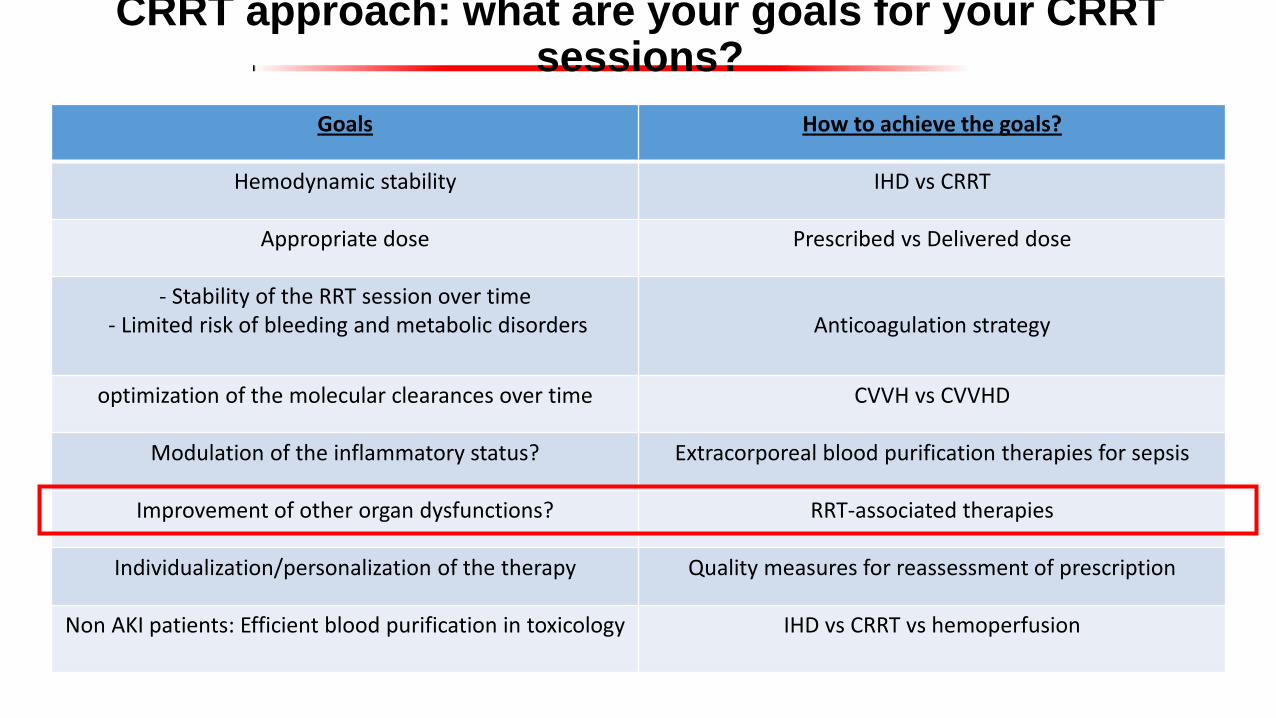
CRRT approach: what are your goals for your CRRT sessions?
Goals How to achieve the goals?
Hemodynamic stability IHD vs CRRT
Appropriate dose Prescribed vs Delivered dose
- Stability of the RRT session over time - Limited risk of bleeding and metabolic disorders
Anticoagulation strategy
optimization of the molecular clearances over time CVVH vs CVVHD
Modulation of the inflammatory status? Extracorporeal blood purification therapies for sepsis
Improvement of other organ dysfunctions? RRT-associated therapies
Individualization/personalization of the therapy Quality measures for reassessment of prescription
Non AKI patients: Efficient blood purification in toxicology IHD vs CRRT vs hemoperfusion
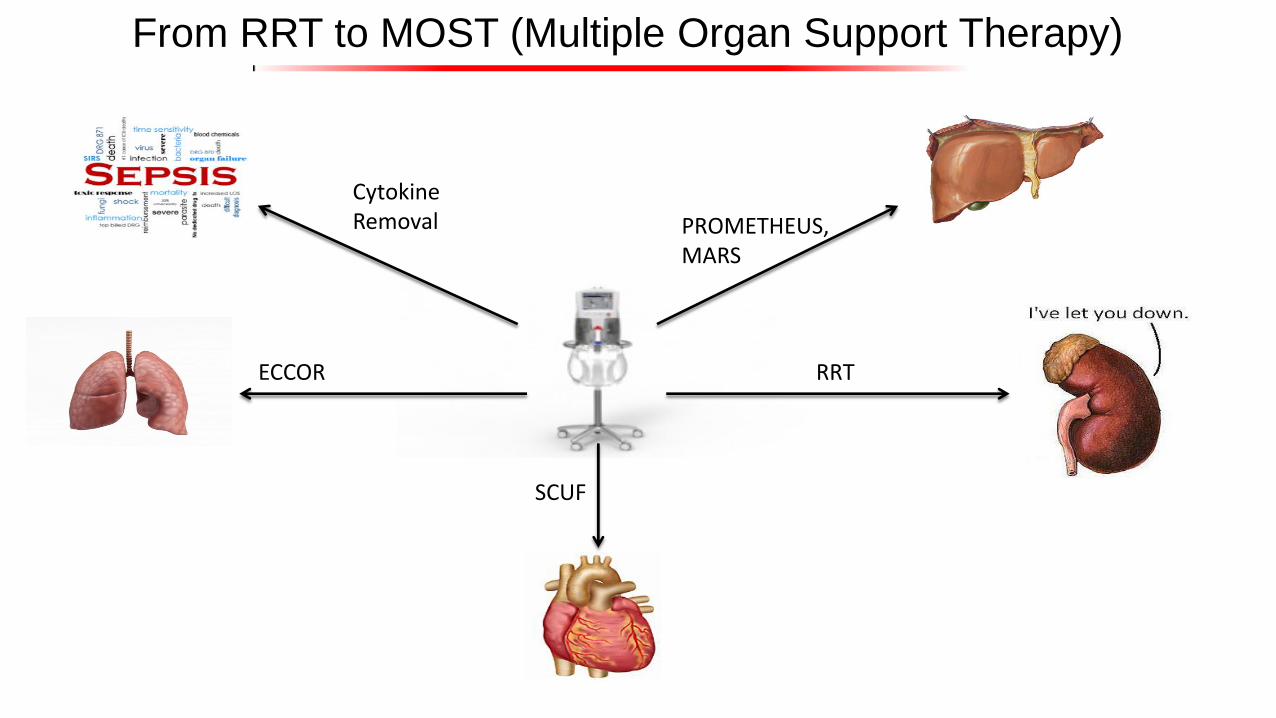
PROMETHEUS,MARS
ECCOR
SCUF
RRT
Cytokine Removal
From RRT to MOST (Multiple Organ Support Therapy)

CRRT approach: what are your goals for your CRRT sessions?
Goals How to achieve the goals?
Hemodynamic stability IHD vs CRRT
Appropriate dose Prescribed vs Delivered dose
- Stability of the RRT session over time - Limited risk of bleeding and metabolic disorders
Anticoagulation strategy
optimization of the molecular clearances over time CVVH vs CVVHD
Modulation of the inflammatory status? Extracorporeal blood purification therapies for sepsis
Improvement of other organ dysfunctions? RRT-associated therapies
Individualization/personalization of the therapy Quality measures for reassessment of prescription
Non AKI patients: Efficient blood purification in toxicology IHD vs CRRT vs hemoperfusion

Kellum JA, Ronco C. Blood purif 2016
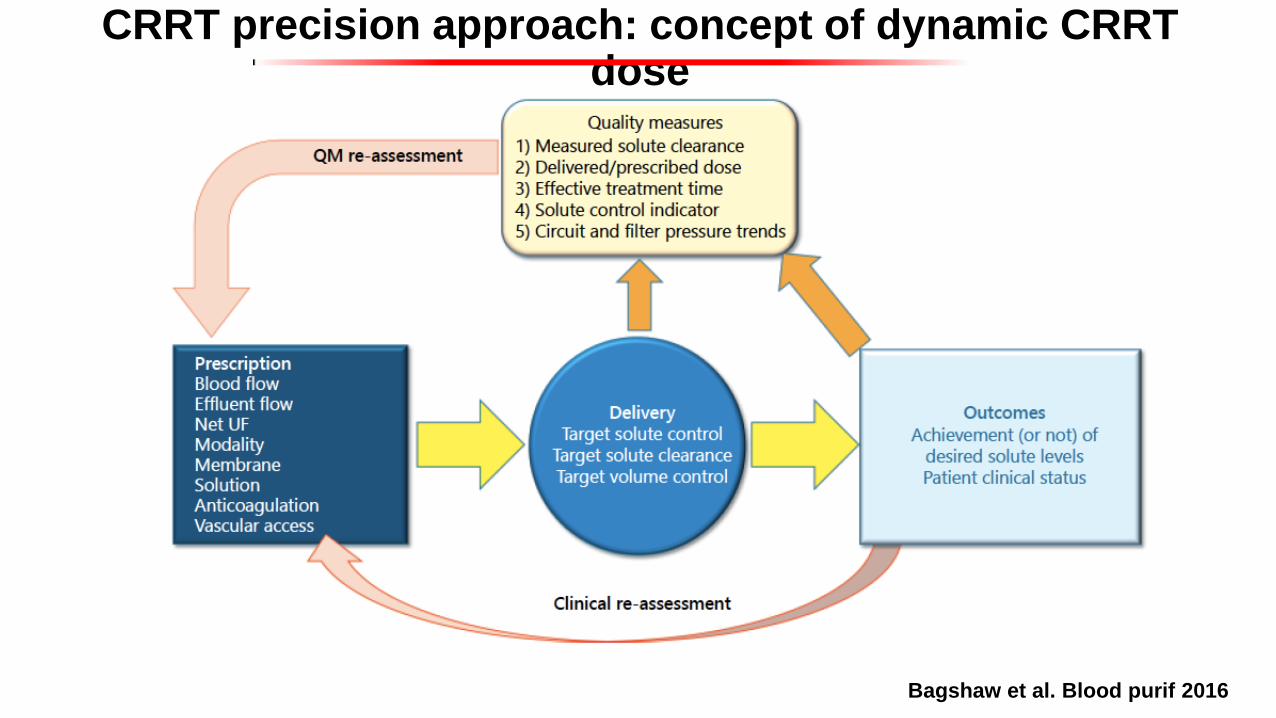
Bagshaw et al. Blood purif 2016
CRRT precision approach: concept of dynamic CRRT dose

Goals How to achieve the goals?
Hemodynamic stability IHD vs CRRT
Appropriate dose Prescribed vs Delivered dose
- Stability of the RRT session over time - Limited risk of bleeding and metabolic disorders
Anticoagulation strategy
optimization of the molecular clearances over time CVVH vs CVVHD
Modulation of the inflammatory status? Extracorporeal blood purification therapies for sepsis
Improvement of other organ dysfunctions? RRT-associated therapies
Individualization/personalization of the therapy Quality measures for reassessment of prescription
Non AKI patients: Efficient blood purification in toxicology IHD vs CRRT vs hemoperfusion
CRRT approach: what are your goals for your CRRT sessions?
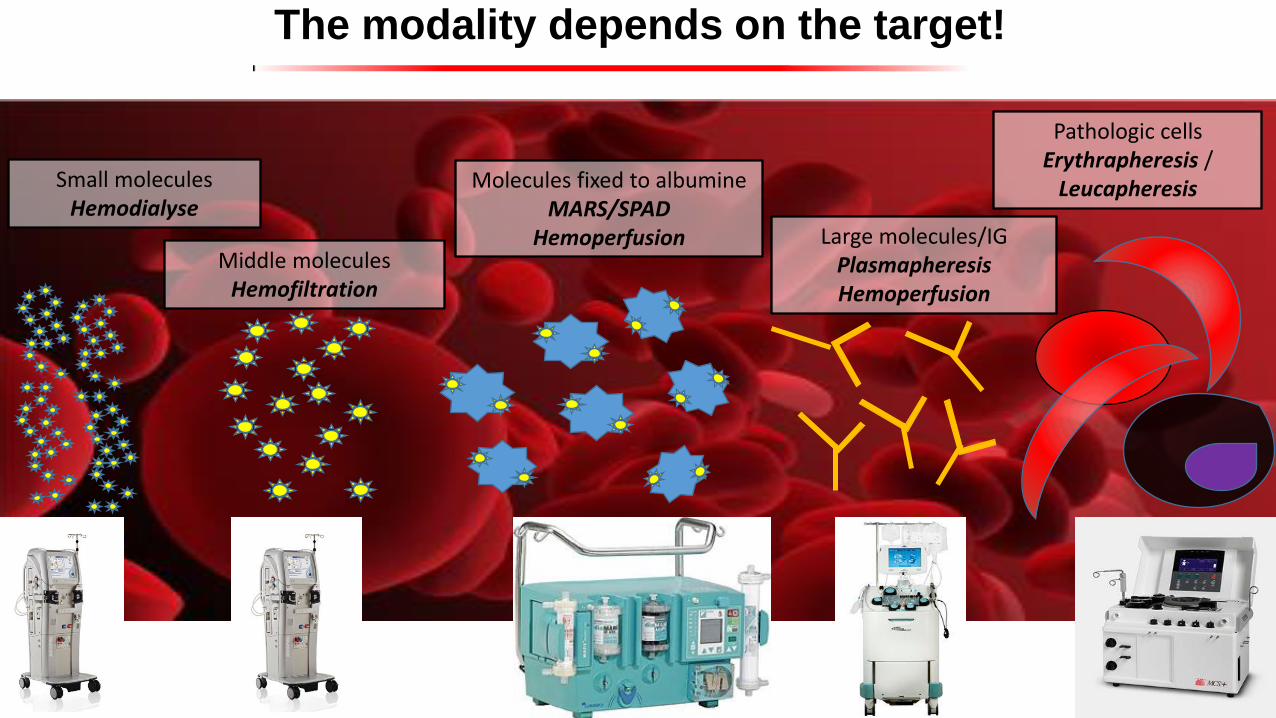
Small molecules Hemodialyse
Middle molecules Hemofiltration
Molecules fixed to albumine MARS/SPAD
Hemoperfusion Large molecules/IG Plasmapheresis Hemoperfusion
Pathologic cells Erythrapheresis /
Leucapheresis
The modality depends on the target!
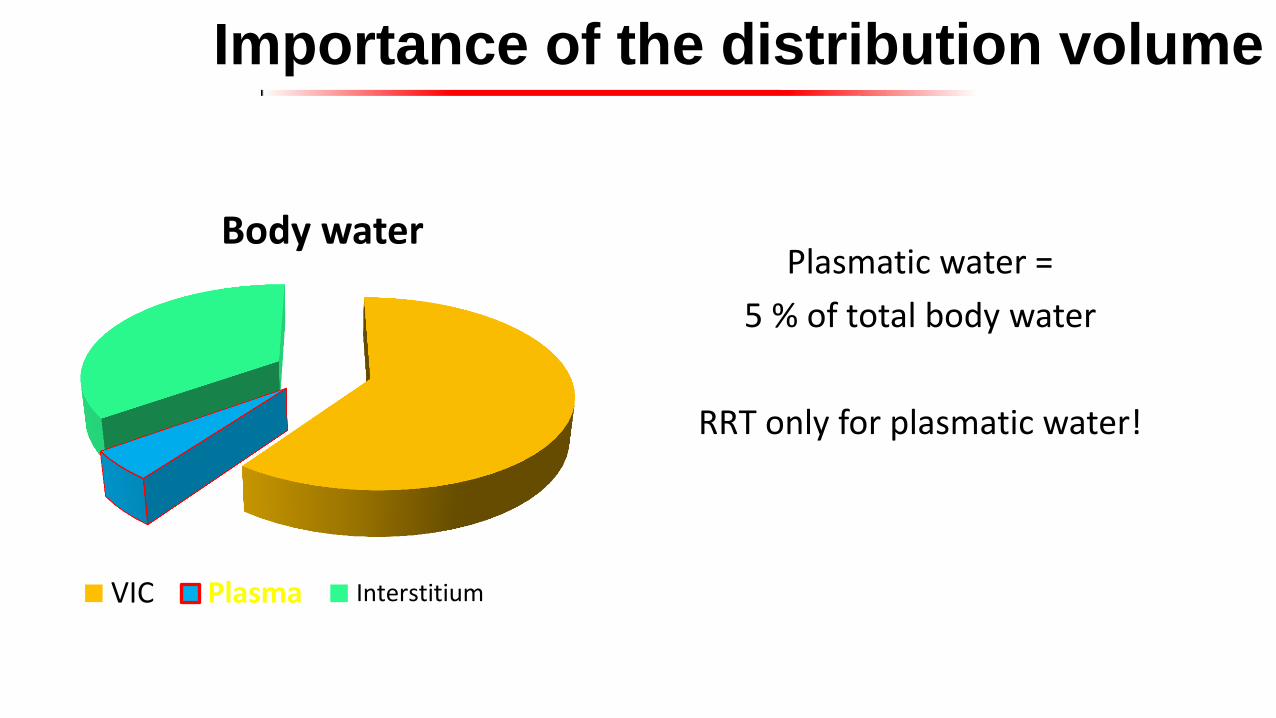
Body water
VIC Plasma Interstitium
Importance of the distribution volume
Plasmatic water =
5 % of total body water
RRT only for plasmatic water!
RRT for toxicology: Limits
• RRT such as hemodialysis / hemofiltration poorly efficient if:
• Large distribution volume
• Molecules very lipophilic
• Molecules bound to proteins
• Very large molecules
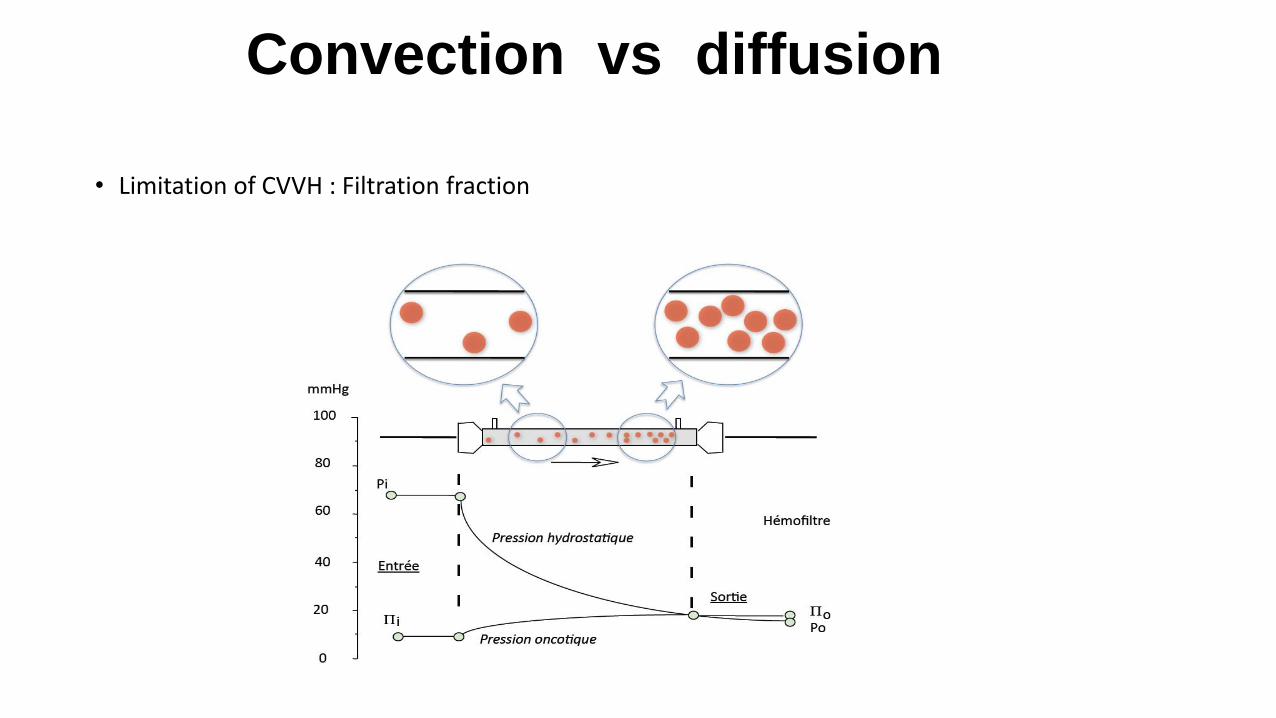
Convection vs diffusion
• Limitation of CVVH : Filtration fraction

Convection vs diffusion
• Limitation of CVVH: Filtration fraction
• FF = UF flow rate / Blood flow (if 100 % post dilution)
• FF = (Pre + Post + weight loss) / (Blood flow + Pré)
• Ideal FF = 20-25 % of blood volume (30-40 % of plasmatic volume)
• In the best scenario, we can remove only 40% of the toxin when it passes through the filter

Hemoperfusion Holubek et al. Kidney Intern 2008

In clinical practice?
• Group EXTRIP
• Literature reviews and recommendations
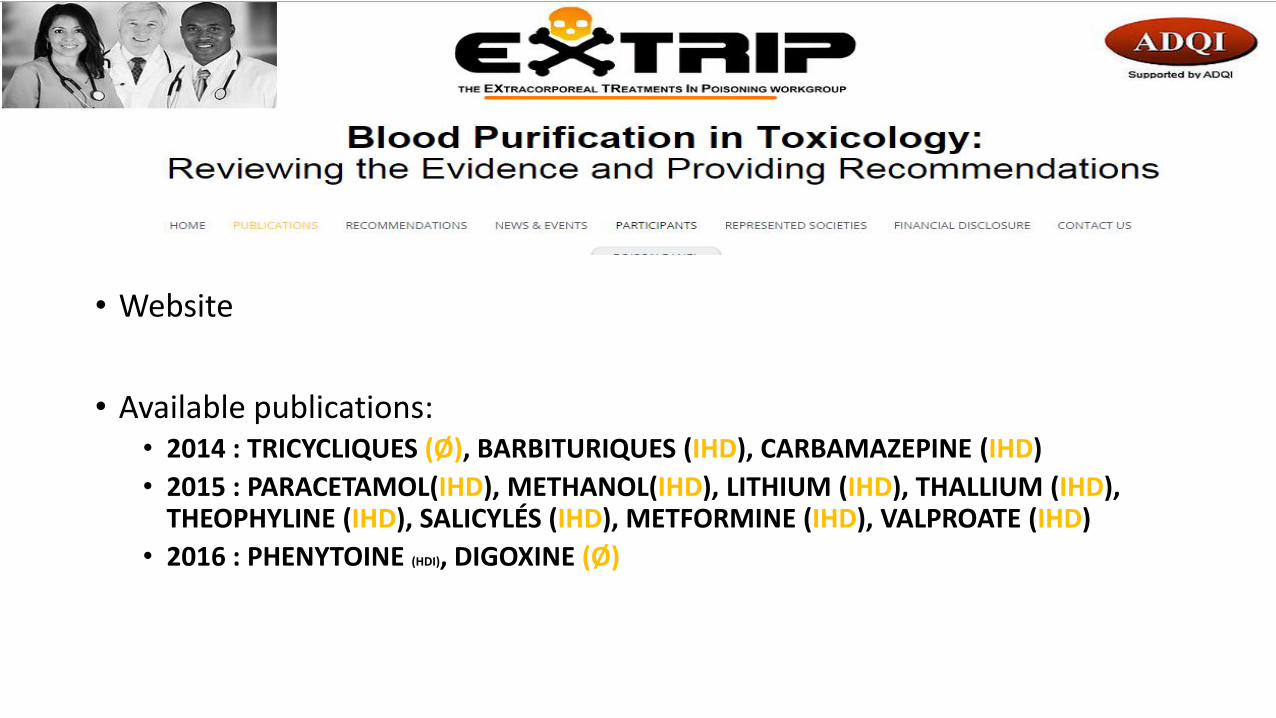
Groupe EXTRIP
• Website
• Available publications: • 2014 : TRICYCLIQUES (Ø), BARBITURIQUES (IHD), CARBAMAZEPINE (IHD)
• 2015 : PARACETAMOL(IHD), METHANOL(IHD), LITHIUM (IHD), THALLIUM (IHD), THEOPHYLINE (IHD), SALICYLÉS (IHD), METFORMINE (IHD), VALPROATE (IHD)
• 2016 : PHENYTOINE (HDI), DIGOXINE (Ø)
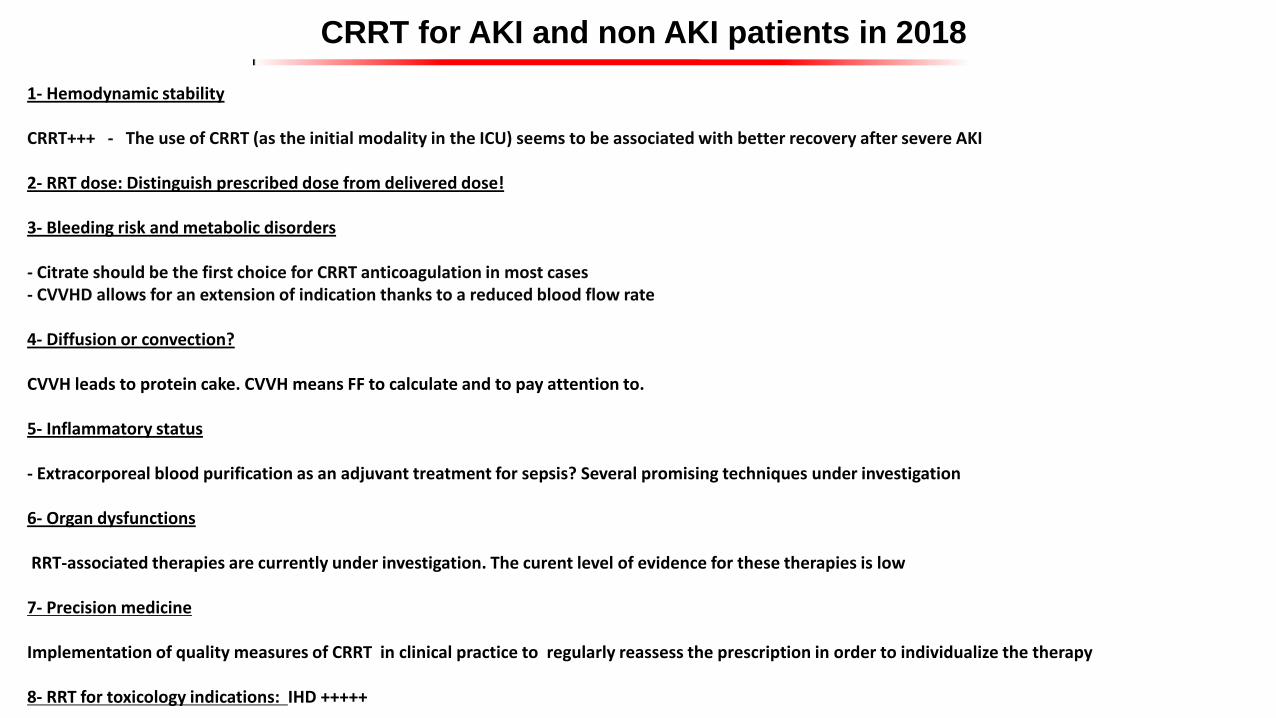
CRRT for AKI and non AKI patients in 2018
1- Hemodynamic stability CRRT+++ - The use of CRRT (as the initial modality in the ICU) seems to be associated with better recovery after severe AKI 2- RRT dose: Distinguish prescribed dose from delivered dose! 3- Bleeding risk and metabolic disorders - Citrate should be the first choice for CRRT anticoagulation in most cases - CVVHD allows for an extension of indication thanks to a reduced blood flow rate 4- Diffusion or convection? CVVH leads to protein cake. CVVH means FF to calculate and to pay attention to. 5- Inflammatory status - Extracorporeal blood purification as an adjuvant treatment for sepsis? Several promising techniques under investigation 6- Organ dysfunctions RRT-associated therapies are currently under investigation. The curent level of evidence for these therapies is low 7- Precision medicine Implementation of quality measures of CRRT in clinical practice to regularly reassess the prescription in order to individualize the therapy 8- RRT for toxicology indications: IHD +++++