Embed Size (px)
DESCRIPTION
Citation preview

Contact dermatitisBoonthorn
23 June 2010

Definition Classification Epidemiology Pathology & Pathophysiology Clinical presentation & Differential diagnosis Investigation Special exposure associated with CD management
Outline

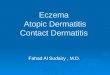
Common inflammatory skin disorder Most common recognized as eczematous
inflammation Allergic or irritant skin reaction caused by
an external agent
Definition
J Allergy Clin Immunol 2010;125:S138-49.Allergy 2009:64:1669-1714.

Allergic contact dermatitis (ACD) (20%)◦ inflammation caused by allergen-specific T
lymphocytes. rapid development of dermatitis occurs following re-exposure to low concentrations of allergen, not cause lesions in non-sensitized individuals
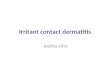
Irritant contact dermatitis (ICD) (80%)◦ develop following prolonged and repeated exposure to
irritants◦ inflammatory cells have role in development of
dermatitis◦ allergen-specific lymphocytes not involved in
pathogenesis ◦ prior sensitization is not necessary
Classification
www.worldallergy.org

In U.S. (2004)◦ overall prevalence rate 24,400 /100,000 people
Cohort population-based studies in Europe◦ prevalence rates 0.7% - 18.6% for ACD
Incidence of OCD in other countries 1.3 - 19 cases per 10,000
All age groups are affected with slight female preponderance
prevalence increases with age decreased prevalence in patients >70 years
Epidemiology
J Allergy Clin Immunol 2010;125:S138-49.

Pathology epidermal hyperplasia
with spongiosis and mounds of parakeratosis.
There is superficial, perivascular infiltrate of lymphocytes and eosinophils with exocytosis

inflammation in epidermis and superficial dermis
Acute◦ superficial perivascular infiltration with lymphocytes,
monocytes and small number of eosinophils◦ increased intercellular spaces between keratinocytes
(spongiosis): predominant histologic feature of CD Chronic
◦ thickening of epidermis, irregular elongation of the rete ridges and vertical thickening of collagen of papillary dermis
Pathology
WWW.worldallergy.org

ACD ◦ prototype of type IV cell-mediated hypersensitivity
reaction ICD
◦ nonimmunologic, multifactorial, direct tissue reaction
◦ T cells activated by nonimmune, irritant, or innate mechanisms release proinflammatory cytokines
◦ dose-dependent inflammation ACD and ICD frequently overlap because
many allergens at high enough oncentrations can also act as irritants
Pathophysiology
J Allergy Clin Immunol 2010;125:S138-49.

Pathophysiology (ACD)
Allergy 2009: 64: 1699–1714.

Pathophysiology (ACD)
Allergy 2009: 64: 1699–1714.

Keratinocytes play key role in development of both ACD and ICD
synthesize and release pro-inflammatory cytokines, in particular interleukins IL-1, 6 and 8, TNF-α and GM-CSF
These cytokines play important part in recruitment and homing of inflammatory cells and can be induced and released from keratinocytes by both irritants and allergens
role of keratinocyte

Langerhans cells are primary APCs of epidermis cell surface expression of CD1a and presence of
intracytoplasmic Birbeck granules process protein Ag by cleaving them into peptides
and present fragments in peptide-binding groove of their surface located MHC class II
Hapten-conjugated LC migrate to local LN where they present allergen to T lymphocytes
T lymphocytes must then home to inflamed skin
Antigen presentation: The role of Langerhans cell

Homing is process whereby circulating cells migrate to relevant sites
This process relies on linkage between adhesion molecules expressed on endothelial cells and their ligands expressed on lymphocytes
homing receptor on T lymphocytes probably "cutaneous lymphocyte antigen" (CLA), ligand for E-selectin
Additional adhesion molecule ◦ ICAM-1 interacts with LFA-1◦ VCAM-1 interacts with VLA-4
Homing of T lymphocytes

Classic presentation ◦ pruritic, eczematous plaque localized to site of allergen
exposure◦ redness, edema,papules, vesiculation, weeping,
crusting Geometric or linear patterns or involvement of
unusual focal skin areas, eg. earlobes, or weight-bearing areas of feet may suggest contact cause
Chronic ACD (i.e. nickel and fragrances) can be insidious and present as localized lichenification or with more generalized reactions
Clinical presentation
ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY, VOLUME 97, SEPTEMBER, 2006

Differentiation between ICD and ACD
J Allergy Clin Immunol 2010;125:S138-49.

J Allergy Clin Immunol 2010;125:S138-49.

Exogenous causes of ICD in Occupational Dermatology Clinic, Skin and Cancer Foundation, Australia (total 621 patients over the period 1993–2002)
Australasian Journal of Dermatology (2008) 49, 1–11

Differential diagnosis
ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY, VOLUME 97, SEPTEMBER, 2006

Condition Differentiating signs/symptoms Patch tests
Atopic dermatitis Lesions are generally symmetrically distributed over flexural areas, less likely to be vesicular, more chronic in nature with seasonal variation, and not sharply delineated.FH is often positive for atopy.
Negative
Nummular eczema Lesions coin-shaped plaques, with pinpoint vesiculation, symmetrically distributed, most commonly on extensor lower extremities
Negative
Dyshidrotic eczema
Dyshidrotic eczema almost exclusively involves palms and soles with little to no involvement of dorsal hands and feet
Negative
Differential diagnosis
Best practice

Physical examination
Current Opinion in Pediatrics 2009, 21:491–498

Patch tests◦ gold standard for identification of contact allergen◦ occlusive patch testing is most common technique
Patch testing a patient with active AD more likely to produce “angry back” reaction, resulting in a false-positive reading
affected by ◦ oral corticosteroids (>20 mg of prednisone per day or its
equivalent)◦ cancer chemotherapy, or immunosuppressive drugs◦ Topical corticosteroids should be discontinued for 5 to 7
days before patch testing not affected by antihistamines
Investigation
J Allergy Clin Immunol 2010;125:S138-49.

Sources of allergens◦ T.R.U.E. TEST :not US FDA approved◦ But recommended by CD experts
No. of allergens◦ ideal number remains controversial◦ T.R.U.E. Test contains 29 allergens
higher false-negative reactions to neomycin, thiuram mix, balsam of Peru, fragrance mix, cobalt, and lanolin
◦ NACDG series from 65 to 70 allergens◦ use of FDA-certified antigen panel available in US
can fully evaluate ~ 25- 30% of ACD
Investigation
J Allergy Clin Immunol 2010;125:S138-49.

Current Opinion in Pediatrics 2006, 18:385–390

applied to upper or middle back areas (2.5 cm lateral to midspinal reference point) free of dermatitis and hair
kept in place for 48 hours read 30 minutes after removal of patches second reading should be done 3 to 5 days after
initial application Metals , topical antibiotics , topical orticosteroids,
and PPD can elicit positive reactions after 7 days Nonstandardized patch tests tested at 1:10 to
1:100 dilutions
Patch test technique
J Allergy Clin Immunol 2010;125:S138-49.

ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY, VOLUME 97, SEPTEMBER, 2006

Repeat open application test (ROAT)◦ Improving reliability of interpreting tests for leave-on
products◦ suspected allergens are applied to antecubital fossa
twice daily for 7 days and observed for dermatitis◦ absence of reaction makes CD unlikely◦ If eyelid dermatitis is considered, ROAT can be
performed on back of ear dimethyl-glyoxime test for nickel
◦ identification of allergens Skin biopsy
◦ Distinguishing CD from morphologically similar diseases
Investigation
J Allergy Clin Immunol 2010;125:S138-49.

localized or generalized inflammatory skin disease in contact-sensitized individuals exposed to hapten orally, transcutaneously, intravenously, or by means of inhalation
Cause◦Metal (cobalt, copper, chromium, gold, mercury, nickel, and zinc)
◦ Medications corticosteroids, antihistamines (diphenhydramine, ethylenediamine, hydroxyzine, and doxepin), miconazole, terbinafine, neomycin,gentamicin, erythromycin, pseudoephedrine, benzocaine, tetracaine, oxycodone, IVIG, aminopenicillins, 5-aminosalicylic acid, naproxen, allopurinol, mitomycin C, 5-FU
◦ Herbal medicine
Systemic contact dermatitis
J Allergy Clin Immunol 2010;125:S138-49.

Symmetric drug-related intertriginous and flexural exanthema
Criteria for diagnosis :◦ exposure to systemic drug at first or repeated
dosing (contact allergens excluded)◦ erythema of gluteal/perianal area, V-shaped
erythema of inguinal/perianal area, or both◦ involvement of at least 1 other
intertriginous/flexural localization◦ symmetry of affected areas◦ absence of systemic signs and symptoms
Drug induced SCD
J Allergy Clin Immunol 2010;125:S138-49.

Second most common type of occupational disease
In 1999, incidence rate of occupational skin disorders was 49 cases per 100,000
most common occupations associated with OCD are health professionals (especially nurses), food processors, beauticians and hairdressers, machinists,and construction workers
Occupational contact dermatitis
ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY, VOLUME 97, SEPTEMBER, 2006

4 of 7 criteria must be positive to conclude OCD◦ clinical appearance is consistent with CD◦ cutaneous irritants or allergens are present in workplace◦ anatomic distribution of dermatitis is consistent with skin
exposure to chemicals in course of various job tasks◦ temporal relationship between exposure and onset of
symptoms is consistent with CD◦ nonoccupational exposures are excluded as probable
causes of dermatitis◦ dermatitis improves away from work exposure and
reexposure causes exacerbation◦ there are positive-reaction and relevant patch tests
performed according to established guidelines
Occupational contact dermatitis
ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY, VOLUME 97, SEPTEMBER, 2006

Toxicodendron dermatitis (poison ivy) is most common form of ACD and can be readily identified by its streak-like or linear papulovesicular presentation
caused by urushiol, which is found in saps of this plant family
Urushiol contained in mango skin,cashew nut oil, ginkgo (female) leaves, Japanese lacquer, and Indian marking ink
Plant dermatitis
ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY, VOLUME 97, SEPTEMBER, 2006

Allergic contact dermatitis to poison ivy (toxicodendron radicans). Note the linear lesions induced by contact with branches
www.worldallergy.org

Current Opinion in Pediatrics 2006, 18:385–390

Current Opinion in Pediatrics 2009, 21:491–498

Metals Nickel
◦ NACDG reported 18.7% of patients evaluated for ACD had positive patch test reaction to nickel
◦ Female sensitization to nickel higher because of increased ear piercing
◦ 1% of nickel allergy have systemic reactions to nickel content of normal diet
◦ Foods with higher nickel content include soybean, fig, cocoa, lentil, cashew, nuts, and raspberry
SELECTED CONTACT ALLERGENS
J Allergy Clin Immunol 2010;125:S138-49.

Allergic contact dermatitis to nickel in watchband

Allergic contact dermatitis to nickel in earring

Allergic contact dermatitis to nickel in belt buckle
Current Opinion in Pediatrics 2006, 18:385–390

Gold NACDG reported that 389/4101(9.5%) had
positive patch test reactions to gold hands (29.6%); face, with seborrheic
distribution (19.3%); and eyelids (7.5%) mostly used for fashion appeal, anti-
inflammatory medication, used in electroplating industry, part of dental appliances (present with oral symptoms)
J Allergy Clin Immunol 2010;125:S138-49.

Common allergens in these products include fragrances, preservatives, excipients, glues, and sun blocks
Fragrance most common cause of ACD from cosmetics results in positive patch test reactions in 10.4% of patients ‘‘unscented’’ and ‘‘Fragrance-free’’ Fragrance mix I contains allergens found in 15% to 100% of
cosmetic products and might detect ~85% of subjects with fragrance allergy
positive patch test reaction to fragrance must correlate with distribution of dermatitis and evaluation of clinical relevance, eg. positive ROAT reaction
Cosmetics
J Allergy Clin Immunol 2010;125:S138-49.

Preservatives and excipients Lanolin : common component of consumer products It is weak sensitizer on normal skin but a stronger
sensitizer on damaged skin stasis dermatitis, are at higher risk of lanolin sensitivity Cosmetic preservatives
◦ Formaldehyde releasers ◦ non–formaldehyde releasers : Paraben most commonly used
preservative in cosmetics, as well as in pharmaceutical and industrial products
Type I immediate hypersensitivity reactions (contact urticaria) and SCD from ingestion of paraben-containing medications or foods have been reported
J Allergy Clin Immunol 2010;125:S138-49.

Hair products Second most common cause of cosmetic allergy PPD (Paraphenylenediamine) is most common
cause of CD in hairdressers In hair dye users the dermatitis often spares the
scalp and usually involves the face near the hairline, eyelids, and neck
PPD cross-reacts with COX-2 inhibitor (celecoxib), sunscreens, and antioxidants used in manufacture of rubber products
New hair dyes that contain FD&C and D&C dyes have very low levels of cross-reactivity with PPD
J Allergy Clin Immunol 2010;125:S138-49.

Allergic dermatitis from black leather watch band. Possible allergens include chromates used to tan leather and paraphenylenediamine dye
www.worldallergy.org

CAPB ( Cocoamidopropyl betaine )◦ amphoteric surfactant often found in shampoos,
bath products, and eye and facial cleaners◦ CAPB allergy typically presents as eyelid, facial,
scalp, and/or neck dermatitis Glycerol thioglycolate
◦ active ingredient in permanent wave solution◦ Unlike PPD, thioglycolates might remain allergenic
in hair long after it has been rinsed out◦ skin eruptions can continue for weeks after
application of permanent wave solution
J Allergy Clin Immunol 2010;125:S138-49.

Antibiotics and antiseptics Neomycin and nitrofurazone are potent
sensitizers Neomycin sulfate can cross-sensitize with
gentamicin, kanamycin, streptomycin, spectinomycin, tobramycin,and paromomycin
Medications
J Allergy Clin Immunol 2010;125:S138-49.

corticosteroid◦ 0.2-6%◦ Patients with worsening of previous dermatitis or
initial improvement followed by deterioration of dermatitis after application of corticosteroids should be evaluated
◦ Cross-reactivity between groups A and D2 and groups B and D2 also has been reported
◦ optimal patch test concentration not worked out for most corticosteroids
◦ 30% of ACD to corticosteroids be missed if delayed 7-day reading not done
Medications
J Allergy Clin Immunol 2010;125:S138-49.

Current Opinion in Pediatrics 2009, 21:491–498

Allergic contact dermatitis to topical steroid preparation applied to hands. Note massive edema, erythema, and sparing of skin under watch band
www.worldallergy.org

use of nickel in biomedical devices,led to increasing concern about safety in suspected nickel-sensitized patients
Presently,high variability of care no large, evidence-based guidelines 10 patients with positive patch test reaction
to metal had in-stent restenosis associated with clinical symptoms
allergy to metals,plays relevant role in inflammatory fibroproliferative restenosis
CD Due to Surgical Implant Devices
J Allergy Clin Immunol 2010;125:S138-49.

criteria for diagnosis of cutaneous implant–induced reaction◦ dermatitis (localized or generalized) appearing
after implant surgery◦ persistent dermatitis that is resistant to
appropriate therapies◦ positive patch test result proven history to
metallic component of implant or to commonly used acrylic glues
◦ resolution of dermatitis after removal of implant
CD Due to Surgical Implant Devices
ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY, VOLUME 97, SEPTEMBER, 2006

Allergen identification to improve contact avoidance
Alternatives and substitutes to cosmetics should be offered to patient to increase compliance
supportive care and relief of pruritus, cold compresses with water or saline, Burrow solution , calamine, and colloidal oatmeal baths might help acute oozing lesions
Excessive handwashing should be discouraged in hand dermatitis, and nonirritating or sensitizing moisturizers must be used after washing
Treatment
J Allergy Clin Immunol 2010;125:S138-49.

TC is first-line treatment for ACD For extensive(>20% BSA) and severe CD,
systemic corticosteroids might offer faster relief (12-24hr)
recommended dose is 0.5 to 1 mg/kg daily for 5 to 7 days, and only if patient is comfortable at that time is dose reduced by 50% for next 5 to 7 days
Treatment
J Allergy Clin Immunol 2010;125:S138-49.

topical T-cell selective inhibitors ◦ efficacy in ACD or ICD not been established
antibiotics should be used for secondary infections of ACD or ICD
antihistamines have been used for relief of pruritus associated with ACD, generally ineffective ◦ diphenhydramine not be used in patients with ACD to
Caladryl and hydroxyzine hydrochloride in ethylenediamine-sensitive patient
Other modes of therapy : UV light treatment and immunomodulating agents, eg.MTX,AZA, and MMF
Treatment
ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY, VOLUME 97, SEPTEMBER, 2006

Primary prevention◦ In high-risk industries and professions, preventive
surveillance programs are possible, especially for apprentices or newly hired workers
Secondary prevention◦ Once diagnosis of ACD or ICD is established,
emollients, moisturizers, and/or barrier creams may be instituted
Prevention
ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY, VOLUME 97, SEPTEMBER, 2006

ICD is caused by direct toxicity without prior sensitisation and ACD is delayed hypersensitivity reaction
Results in localised burning, stinging, itching, blistering, redness and swelling at area of contact with allergen or irritant.
Patch testing may aid identification of offending agent Skin biopsy may also be helpful Treatment involves removal of offending agent, future
avoidance of offending agent, topical corticosteroids and/or short course of oral corticosteroids.
Conclusion