Embed Size (px)
DESCRIPTION
lecture by Dr. Ahmed Rehman
Citation preview

Dr Ahmed RehmanFCPS UrologyAssistant Professor Urology
30-march, 2010, tuesday 1

Learning Objectives
Enlist congenital abnormalities of kidney & ureter
Describe clinical significance of these abnormalities, ie What problems these can cause (symptoms) What are risks to health ( complications)
Enlist diagnostic investigation plan– history, examination, investigations
Suggest treatment plan in these conditions
30-march, 2010, tuesday 2

Congenital abnormalities of kidney Uncommon ( <1:1000) Commonly Symptomless – found
incidentally – US,IVU, CT. Why ????
sometimes detected only when have caused sufficient damage
Endanger kidneys to various complications
30-march, 2010, tuesday 3

Agenesis / aplasia of kidney Bilateral – fatal Unilateral –
compatable with normal life, contralateral kidney hypertrophed
Failure of mesonephric duct to bud
Ureteric orifice absent on cystoscopy
Rarely ureters & pelvis may be present but renal tissue is absent or so
30-march, 2010, tuesday 4

Hypoplasia-dysplasia
30-march, 2010, tuesday 5

Renal Ectopia / pelvic kidneys Doesn't ascend, formed
near pelvic brim No symptom Present with pain or mass
which one may tempt to remove as unexplained pelvic mass
pose diagnostic problems in case of disease or surgery
May be source of stone, infection
Liable to trauma30-march, 2010, tuesday 6

30-march, 2010, tuesday 7

Crossed Ectopia / Crossed Dystopia
Both kidneys lie in one loin
May be fused with each other or separate
Ureter of lower crosses midline to open into bladder on its normal side
30-march, 2010, tuesday 8

Crossed Ectopia contrasted with normal IVU
30-march, 2010, tuesday 9

Mal rotated kidneys
Calyces face anteriorly or antrolaterally
Have some element of obstruction causing inadequate drainage – leading to infection & stone formation
30-march, 2010, tuesday 10

Horse shoe kidney
low lying – ascent impeded by inferior mesenteric artery
Lower poles fused in mid line in front of 4th lumber vertebra.(isthemus).
Longitudinally lie medially and downwards,
instead of laterally and down wards,
Part or whole of pelvicaliceal system is malrotated ( facing medially),
Ureters curve over fused poles.
30-march, 2010, tuesday 11

Horse shoe kidney
Pain, hematuria, fever, mass
Exam : fixed mass below umbilicus Diagnosis: US & IVU Significance: Liable to disease
angulated ureters + PUJ obstruction urinary stasis stones, infection & obstruction CRF
30-march, 2010, tuesday 12

Horse shoe kidney
Treatment Asymptomatic = nothing doing Mild sypmtoms = treat accordingly PUJ or ureteric obstruction, recurrent
infections, Stones surgery (pyelolithotomy + /-reconstruction)
ISTHEMECTOMY with straightening of ureters – less commonly done.
30-march, 2010, tuesday 13

Polycystic kidneys
Hereditary – autosomal dominant Not manifested before 30 Kidneys enlarged, studded with cysts Unyeilding capsule compresses renal
parenchyma causing atrophy Liver,lungs and pancreas may be
affected Defact : not clear, many theories
30-march, 2010, tuesday 14

Polycystic kidneys
Loin pain- weight dragging upon peddicle or capsule stretch, hemorhage in cyst, stone
abdominal mass- confused with cystic tumor
hematuria- cyst rupture in pelvis,moderate, episodic.
hypertention, infection, & uremia/CRF.
Nonspecific symptoms: anorexia, headache, vague abdominal discomfort, vomiting, drowsiness, anemia.
ESRD: suddenly in middle age, survival without RRT ( dialysis/ transplant) unlikely
30-march, 2010, tuesday 15

30-march, 2010, tuesday 16

Polycystic kidneys
US and CT: cysts in kidneys,liver & others Simple (aquired) cysts: solitary, smooth
walled & homogeneous contants Blood & debris – cystic adenocarcinoma FNA- cytology – differentiates
IVU Enlarged renal shadow, Renal pelvis – compressed & elongated Calyces – narrow, stretched over cysts
( spider legs / bell shaped)
30-march, 2010, tuesday 17

Polycystic kidneys
Nephrologist : BP control, infection,anemia, disturbances
of Ca metabolism, low protein diet to delay need for DIALYSIS
Urologist: Surgical / laproscopic deroofing of cysts
( Rovsing’s operation) Relieves pain & pressure saving kidneys Rarely performed / not preserve function
Renal transplant/ pretransplant bilateral native kidneys nephrectomy
30-march, 2010, tuesday 18

solitary / Simple (acquired) renal cysts Common, may be multiple ( not
always 1 ) Incidentally found– no treatment
needed Rarely symptomatic; pain- stretch,
bleed in cyst, infection,mass papa-pelvic cyst at hilum presses
PUJ obs IVU: filling defect. US, CT :smooth, homogeneous
contant DD: hydatid, cystic
adenocarcinoma Percuteneous FNA Cytology Treat only in case obstructing
30-march, 2010, tuesday 19

Infantile polycystic kidneys Rare Inheritance- autosomal recessive Enlarged kidneys – may obstruct
labour, Many stillborn Die of renal failure in in early
childhood
30-march, 2010, tuesday 20

Unilateral Multicystic kidney More common Presents as nonfunctioning mass Exploration & removal is treatment
of chioce DD: wilm’s, neuroblastoma,
congenital hydronephrosis
30-march, 2010, tuesday 21

Aberrant vessels
Variation in no of vessels – common Arteries – END arteries, damage
ischemia Veis – extensive colaterals = can be
ligated are not cause of hydronephrosis-
though the bulging renal pelvis in between them makes them noticeable
30-march, 2010, tuesday 22

Abnormalities of renal pelvis and ureter Most common, harmless,
asymptomatic
DUPLICATION OF RENAL PELVIS
Common,4%, usually unilateral – left
Upper pelvis – small, drains upper calyx
Asymptomatic no treatnment
If one moity severly damaged – partial nephrectomy
30-march, 2010, tuesday 23

Duplex kidney, double moiety
30-march, 2010, tuesday 24

DUPLICATION OF URETER. 3%
Often join before reaching bladder, suffer obstruction ( esp from stones) & YOYO reflux
May open independently, ureter from upper moity opens distal and medial to its fellow.
Uppermoity ureter suffers ureterocele.
Lower moity ureter suffers VUR
Infection, calculus formation, PUJ obst and VUR, ectopic opening
30-march, 2010, tuesday 25

Abnormalities of ureter Ectopic uretric opening
Female – into urethra below sphincter on vagina = incotinance since childhood with desire and passage of urine normally as well. IVU and cystoscopy ( indigocarmine)
Male.continent as opening is above sphincter Opening in trigone apex, post. Urethra, seminal vesical
or ejaculatory duct – functionally abnormal, infection common
Treatment: Frequently ectopic ureter drains hydronephrotic,
chronically infected moity --- best excised - nephrectomy Incontinence can be cured and renal function preserved
by implanting ureter into bladder ( tunneling) or joining its fellow. (URETERO-NEOCYSTOSTOMY, URETERO-URETEROSTOMY)
30-march, 2010, tuesday 26

30-march, 2010, tuesday 27

Abnormalities of ureter CONGENITAL MEGA URETER
Uncommon, bilateral FUNCTIONAL
obstruction at lower end dilatation & infection
Ureteric orifices normal, ureteric cath passes easily
Reflux not feature till opened endoscopically
Treatment: refashioning and tunneled reimplant
30-march, 2010, tuesday 28

Abnormalities of ureterPOST (retro) CAVAL URETER
Right ureter passes behind IVC instead of lying to the right of it (laterally)
If causing obstruction, can be devided and joined in front of cava – long oblique ETE anastomosis
30-march, 2010, tuesday 29

Abnormalities of ureter URETEROCELE
Cystic enlargement of intramural portion of ureter
Thought to result from congenital atresia of ureteric orifice
Though present since childhood, unrecognised till adulthood
More common in female, cause BOO by obstructing / prolapsing into internal urinary meatus. May even prolapse out of urethra
30-march, 2010, tuesday 30

Adder head on IVU Cyst wall composed of
urothelium only confirmed on cystoscopy
Translucent cyst, enlerging and collapsing as urine flows
Treatment avoided unless symptoms of infection / stone
Endoscxopic diahermy incision / deroofing Postoperatove MCUG to
see VUR Ureteral reimplant Sever hydronephrosis,
pyonephrosis nephrectomy
30-march, 2010, tuesday 31

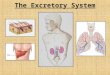
Hydronephrosis
Aseptic dilatation of pelvicaliceal system due to complete or partial obstruction.
Unilateral hydronephrosis Epsilateral
ureteric obstruction
( unilateral supravesical obstruction)
30-march, 2010, tuesday 32

Hydronephrosis:Bilateral
Bilateral ureteric obstruction ( bilateral supravesical obstruction) Urethral obstruction
( bladder outlet obstruction, infravesical obstruction )
Detrusor hypertrophy intramural ureteric obstruction
VUR Pregnancy –physiologic
dilatation - progesterone, early pregnancy – 20 weeks marked reverts 12 week of delivery
Infection, diagnostic difficulty in acute abdominal pain in pregnancy
30-march, 2010, tuesday 33

Causes of Ureteric Obstruction
Extramural Tumors of cervix, ovary, uterous, vagina, urinary bladder,
prostate, rectum, colon, caecum & lymphomas Idiopathic retroperitoneal fibrosis Retrocaval ureter Pararenal cysts Aberent vessels
Intraluminal Calculus, sloughed papilla, clot, ureteric malignancy
Intramural Congenital PUJ obstruction or stenosis Ureterocele and congenital small ureteric orifice Strictures ( stone, repair, tuberculosis, schistosomiasis) Ureteric / vecsical malignanncy Kenks & adhesions ( sec to VUR)
30-march, 2010, tuesday 34

Bladder outlet obstruction Phemosis / fused synichae, Ext. meatal
stenosis Urethral Stone / foreign body impaction, Enlarged prostate--------- benign /
malignant / inflammatory/abscess bladder neck stenosis, Post urethral,valve
Urethral stricture neoplasm of bladder, urethra, prostate and
penis vesical calculus, foreign body Neurogenic
Detrusor sphincter dys-synergia ,neurogenic bladder ,spine trauma,
multiple seclerosis. DM Stones , vesical , urethral,
30-march, 2010, tuesday 35

Congenital (idiopathic)pelvi-ureteric obstruction Right side effected more Female :male = 2:1 Clinical features
Insidious onset mild loin pain / dull ache / Sensation of dragging heaviness made worse by fluid intake
Little to call attention to renal damage
Kidney may / may not be palpable – renal failure intervenes before kidneys dilate
Intermittent hydronephrosis / Dietl’s crisis
Pain, swelling passage of large volume urine pain & swelling disappears
Trauma Mass – obstructed kidney hypertention
30-march, 2010, tuesday 36

30-march, 2010, tuesday 37

Congenital(idiopathic) pelvi-ureteric obstruction Pathogenesis
Adynamic segment of ureter Polyps, valves, kiks, angulation High origin, abnormal relation to vessels
Narrowing, strecture, Pathology
Pelvicaliceal system dilates at the expense of parenchyma which is compressed & destroyed by surrounding unyielding capsule. ( pressure atrophy)
Resultant nonfunctioning Kidney consists of thined out cortex making lobulated sac containing pale low specific gravity uriniferous fluid
Extrarenal pelvis Renal damage delayed and prolonged % lesser
Intrarenal pelvis Renal damage rapid and severe
Stasis leads to infection and stone formation – pain, fever , hematuria
30-march, 2010, tuesday 38

Workup
Urine RE Urea criatinine USG---------- hydronephrosis /cortical thickness, in utero
diagnosis IVU------------ provided RFTs normal
Shows degree of obtrusion / level of, (delayed films) Normal calyceal cupping lost, -- clubbed Pelvis dilated, if intrarenal parenchymal damage severe, as
compared to extrarenal In advance stage a faint nephrogram obtained around dilated
calyces == soap bubble appearances Renal isotope scans (DTPA, MAG 3)= obstruction
Diuretic ( frusimide) increases degree of obstruction Whitaker test : fluid innfused thru percuteneoous puncture
annd intra renal pressuures monitered Retrograde pyelogrphhy – level of obstruction
Deranged RFTs / contrast sensitivity MCUG
30-march, 2010, tuesday 39

Treatment
Indications Recurrent pain Increasinng hydronephrosis / renal damage Infection, stones
Aims Relieving obstruction Preserving renal tissue Preventing infection, stones
30-march, 2010, tuesday 40

Treatment - Options
Mild cases – follow up with USG, operate only if hydronephrosis increasing
Corrective / reconstructive surgery – pyelo-reteroplasty – Anderson-Hynes, VY plasty, Clup’s
Anastomosis protected by stent / nephrostomy
Nonfunctioning kidney – nephrectomy Avoid if DMSA SCAN SHOWS >20% FUNCTION
Endoscopic ballon dilatation under image intensifier ( pyelolysis)
Percuteneous / retrograde Endopyelotomy Laproscopic pyeloplasty
30-march, 2010, tuesday 41

30-march, 2010, tuesday 42

30-march, 2010, tuesday 43

30-march, 2010, tuesday 44

30-march, 2010, tuesday 45

Assignment
Define IVU Give indications (5 atleast) Precautions? (3) Detail procedure with preparation Adverse reactions –
? To prevent, ? To treat Contra-indications What does it tell how to read how to interpret
30-march, 2010, tuesday 46