Embed Size (px)
DESCRIPTION
Citation preview

Research Report
Comparison of the Effects of Exercise in Water and on Land on the Rehabilitation of Patients With Intra-articular Anterior Cruciate Ligament Reconstructions
Key Words: Knee; Ligaments; Lower extremity, knee; Muscle pe$omance, lower extremity; Rehabilitation.
Background and Purpose. Exercises in water have been shown to be effective for improving strength and passive range of motion (PROM). Traditional rehabili- tation following intra-articular anterior cruciate ligament (ACL) reconstruction has taken place o n land. This study was designed to compare the effects of exer-
Rehabilitation following anterior cru- ciate ligament (ACL) reconstruction has evolved over the past few decades and is considered important in guar- anteeing a beneficial outcome follow- ing surgety.1 Advances in surgical approaches, such as graft placement and graft fixation, and the use of ar- throscopically assisted procedures
Brlan J Tovln Steven L Wolf Bruce H Greenfield Jerl Crouse
have influenced rehabilitation, as have knowledge of stress-strain patterns in the ACL during various exercises.2 Twelve-month protocols requiring immobilization and non-weight bear- ing3 have given way to accelerated protocols permitting immediate weight bearing, no immobilization, and return to activity within 6
cises in water o n strengh and girth of the thgb musculature, knee PROM, joint Blane A Woodfin laxity, emion , and functional outcome with the effects of similar mercises on land in subjects following intra-articular reconstruction of the ACL. Subjects. Twenty subjects were randomly asstgned to either a group that exercised o n land or a group that exercised in water. Metbods. Thigh girth, joint effm'on, and knee PROM measurements were recorded at 2-week intervals for the first 8 weeks post- operatively. Isokinetic and isometric peak torque measurements for the thigh mus- culature, knee joint laxity assessments, and Lysholm scores were obtained at the end of 8 weeks. Results. Higher outcome scores were recorded in the water group than in the landgroup, as measured by Lysholm scales. No dtferences were noted between groups for knee PROM, thigh girth, or quadriceps femoris muscle per fomwe . In the water group, less joint e f m o n was noted aJer the 8 weeks. In the land group, greater peak torque for isokinetic knee flexion was recorded. Concluston and Discussion. Although exercise in water may not be as effec- tive as exercise on land for regaining maximum muscle perfomnce, rehabilita- tion in water may minimize the amount of joint ef f i ion and lead to greater self-reports of functional improvement in subjects with intra-articular ACL recon- structions. [Tovin BJ, Wolf SL, Greenfield BH, et al. Comparison of the effects of exercise in water and on land o n the rehabilitation of patients with intra- articular anterior cruciate ligament reconstmctions. Phys Ther. 199g 74: 710-719.1
months.2 Primary goals continue to be the recovery of joint range of motion (ROM), quadriceps femoris muscle force-generating capability, and ambu- latory skills.2 Attaining these goals, however, may be delayed by postop- erative joint effusion and the persis- tence of pain. Early phases of rehabili- tation must minimize the deleterious
22/710 Physical Therapy/Volume 74, Number B/August 1994

effects of surgery through ROM and muscle strengthening exercises while ensuring that each activity is per- formed without overstressing the ACL grafts.435
Electromyographic biofeedback5j6 and neuromuscular electrical stimulation7.8 are two modalities used in the early phases of rehabilitation following ACL reconstruction to reduce muscle atro- phy and to facilitate strengthening. The effectiveness of these modalities in imprc~ving quadriceps femoris muscle force in subjects with ACL reconstruction has been measured by isokinetic dynomometry.6~7 These studies, however, applied feedback or neuroml~scular electrical stimulation during isometric quadriceps femoris exercises, and this approach may not simulate functional activities.
We believe knee extension exercises should be designed to simulate func- tional activities. "Closed-chain" knee extension has been advocated as a safe exercise for patients after ACL reconstruction.9 These exercises in- volve applying resistance through the terminal joint of a limb segment, which restrains the joint's free move- ment (eg, rising from a chair), whereas "openchain" exercises in- volve applying resistance to an ex- tremity in a way that the distal joint is free to move (eg, kicking into the air).IO Although both of these forms of exercise can address the physical
impairments of patients following ACL reconstruction, research suggests that closed-chain exercises are safer than open-chain exercises because there is less stress on the graft.11-13 Despite this fact, some subjects experience increased pain and knee effusion following closed-chain exercises.14 Therefore, performing closed-chain exercises in an environment in which the forces around the knee joint are reduced may aid in reducing knee pain and joint effusion.
Fkercises in water could expedite rehabilitation because of the de- creased stress on the joints, improved circulation, and facilitated movement that occur in water.15.16 Researchers have analyzed limb movement in water17-'9 and have compared differ- ent aquatic exercise devices,2&22 but few studies have quantified gains in muscular force that occur following an aquatic exercise program. Bartow and Diamond23 have concluded that exercises performed using water as resistance can increase the torque- generating capabilities of the thigh musculature in healthy subjects. Gehlsen et a124 have made similar conclusions in patients with multiple sclerosis, but no control group was used for comparison.
NapoletanZ5 found that in subjects with ACL reconstructions, underwater treadmill ambulation in conjunction with traditional rehabilitation was
BJ Tovin, IT, ATC, is StafT Physical Therapist, Physiotherapy Associates, 2770 Lenox Rd NE, Ste 102, Atlanta, GA 30324 (USA), and Director of Rehabilitation, Georgia Tech Athletic Association, Atlanta, GA 30332. Mr Tovin was a student at Emory University, Atlanta, GA, at the time this study was com- pleted in partial fulfillment of the requirements for his Master of Medical Science degree. Address all correspondence to Mr Tovin.
SL Wolf, PhD, FT, FAlTA, is Professor and Director of Research, Department of Rehauilitation Medi- cine, Professor, Division of Geriatrics, Department of Internal Medicine, and Associate Professor, Department of Anatomy and Cell Biology, Emory University School of Medicine, 1441 Clifton Rd NE, Atlanta, GA 30322.
BH Greenfield, FT, OCS, is Clinical Coordinator of Education and Clinic Director, Physiotherapy Associ- ates, Jonestmro, GA 30236, and Clinical Instructor, Division of Physical Therapy, Emory University.
J Crouse, IT, is Clinical Coordinator of Physical Therapy, HealthSouth, Atlanta, GA 30342.
BA Woodfin, MD, is Orthopaedic Surgeon, Resurgeons Orthopaedics, and Team Physician, Georgia Tech Athletic Association.
This study was approved by the Human Investigation Committee of Emory University and Pied- mont Hospital.
This article was submitted April 13, 1993, and was accepted Januaty 6, 194.
more effective in retarding thigh atro- phy than traditional rehabilitation alone. Thigh atrophy, however, is only one measure of recovery. Whether rehabilitation in water will be differ- ent from traditional rehabilitation in reducing knee joint laxity, enhancing muscle force, and improving func- tional outcomes in subjects with intra- articular ACL reconstructions is uncertain.
The purpose of this study was to determine whether exercises in a pool will lead to less joint effusion, less thigh atrophy, increased ROM and thigh musculature strength, and less difficulty with activities of daily living in patients after intra-articular ACL reconstruction compared with exercises on land. An effort was made to match specific exercises in both groups so that each program was identical and only the rehabilitation environment was manipulated.
Method
Subjects
Twenty subjects (14 male, 6 female) ranging in age from 16 to 44 years @=29.0, SD=7.8) participated in this study. All subjects had undergone arthroscopically assisted intra-articular ACL reconstruction using a bone- patellar tendon-bone autograft, per- formed by the same orthopedic sur- geon. Subjects who had prior ACL surgery to either knee or who had a meniscus repair at the time of surgery were excluded from the study.
Procedure
During the preoperative visit, subjects were familiarized with the study and postoperative rehabilitation protocols were explained. Each subject signed an informed consent statement, writ- ten to conform with the guidelines of Emory University and Piedmont Hos- pital (Atlanta, Ga), and a questionnaire was administered. Subjects were as- signed to either a traditional rehabili- tation (TR) group or a pool rehabilita- tion (PR) group using the following method of group assignment. The first 2 subjects were randomly assigned to
Physical Therapy /Volume 74, Number 8/August 1994

- Table 1 . Rehabilitation Pmgrams
--
Week 1 and Home Program Exercises (Both Groups)
1. Wall slides: 25 repetitions
2. Active-assistive range of motion: 25 repetitions
3. Passive knee extension: 10 minutes
4. Hamstring muscle and calf stretching: 10 minutes each
5. Quadriceps femoris muscle sets
6. Straight leg raisesa: 3 sets x 10 repetitions for hip flexion, abduction, adduction, and extension
7. Active knee flexiona: 3 sets x 10 repetitions
8. Toe raises: 3 sets x 10 repetitions
9. Partial wall squats (usually added to the home program after first week): 3 sets x 10 repetitions
Week 2-8 Exercise Programs
Traditional Rehabilitation Group Pool Rehabilitation Group
1. Stationary cycling: 10 minutes
2. Gait training without brace, alternating forward and backward ambulation: 10 min
3. Side step-ups, front step-ups, step-downs: beginning with 3 sets of 10 repetitions, progressing to 3 sets of 15 repetitions
4. Hip flexion, extension, abduction, adduction in standing using a wall pulley with 4.54-kg (10-lb) plates: beginning with 3 sets of 10 repetitions, progressing to 3 sets of 15 repetitions
5. Knee flexion in sitting: 3 sets of 10 repetitions; boot: beginning with 3 sets of 10 repetitions, progressing to 3 sets of 15 repetitions
1. Stationary cycling: 10 minutesb
2. Gait training without brace, alternating forward and backward ambulation: 10 min
3. Side step-ups, front step-ups, step-downs: beginning with 3 sets of 10 repetitions, progressing to 3 sets of 15 repetitionsC
4. Hip flexion, extension, abduction, adduction in standing using the Hydrotone resistance boot: beginning with 3 sets of 10 repetitions and progressing to 3 sets of 15 repetitions
5. Knee flexicn in standing using the Hydrotone resistance boot: beginning with 3 sets of 10 repetitions and progressing to 3 sets of 15 repetitions
"Cuff weights were added to straight leg raises and knee flexion in increments of 0.91 kg (2 lb).
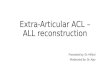
*stationary cycling in the pool rehabilitation group used a peddling device (see Fig. 1) rather than a stationary bicycle.
'Step-ups in the water were done with 20.32-cm (8-in) and 40.64-cm (16-in) steps.
one of the two groups using a coin toss. The next 2 subjects recruited were placed in opposite groups of the first 2 subjects. This procedure was continued for every 4 subjects until 20 subjects were recruited. As a result, 6 men and 4 women were placed in the PR group and 8 men and 2 women were placed in the TR group. This method of group assignment was used to evenly distribute subjects between the two groups over time, while also incorporating random assignment to groups.
Week 1 Exercises for Both Oroups
During the first postoperative session, patients in both groups were in- structed in an identical program (Tab. I), which they performed at home twice per day. The first week of post- operative rehabilitation consisted of three or four treatment sessions in
which one of the authors reviewed the home program to ensure that the exercises were done safely and inde- pendently. To facilitate passive knee extension, each subject was posi- tioned prone and the involved leg (from the superior third of the tibia to the foot) was placed off the side of a treatment table or bed, letting grav- ity pull the knee into extension. Resis- tance for the straight leg raises and leg curls was added using variable- resistance cuff weights. Subjects initi- ated each exercise, performing three sets of 10 repetitions without weight and progressing until they could per- form three sets of 15 repetitions with- out difficulty. Subjects then added 0.9 kg (2 lb) to the cuff weight and re- peated the progression starting with three sets of 10 repetitions. This pro- cedure was continued, and resistance was added in 0.9-kg increments (most patients progressed their weight every 2-3 days). Subjects were instructed
how to keep a log of their home exercise p r o g m , which was checked by one of the authors to help assess compliance.
Weight Bearing
Gait training was also initiated on the first postoperative session with axil- lary crutches and a hinged knee brace. The braces were locked in full extension for the first 4 to 7 days, and subjects were instructed to bear as much weight as they could tolerate. Subjects were progressed from two crutches to one crutch between the 4th and 7th postoperative days and were usually off the crutch by the 10th postoperative day. The hinged knee brace was unlocked at the be- ginning of the 2nd week, permitting 90 degrees of knee flexion. The ROM of the braces were increased to 120 degrees by the beginning of the 3rd postoperative week, and subjects were
24/712 Physical Therapy /Volume 74, Number 8/August 1994

achieved a maximum height of 30.48 cm (12 in).
Figure I. Pedalling device used by subjects in the water group.
Rehabliltation Programs
out of the brace by the 6th postopera- tive week.
During the second through the eighth postope~ztive weeks, the TR group performed a land rehabilitation pro- gram and the PR group performed a similar program in the water (Tab. 1). Both programs were performed three times per week in the same sequence.
Subjects in the TR group warmed up with 10 minutes of stationary cycling, followed by 10 minutes of gait train- ing (alternating forward and backward walking) and 5 minutes of passive stretching. The PR group warmed up
with the same exercises, but used a pedalling device underwater (Fig. 1) instead of a stationary bicycle.
Subjects in the TR group initiated closed-chain exercises on a 5.08-cm (2-in) step. Three sets of 10 repeti- tions were performed, progressing to three sets of 15 repetitions. When subjects could perform three sets of 15 repetitions comfortably at a given height, the height was increased by 5.08 cm and they started with three sets of 10 repetitions again. Subjects usually advanced every two or three sessions and continued the same exercise progression while the height of the step was increased in incre- ments of 5.08 cm. Subjects usually
'Hydrotone International Inc, 3535 NW 58th St, Ste 1000, Oklahoma City, OK 73112.
Subjects in the PR group initiated closed-chain exercises on a 20.32-cm (8-in) step. Subjects began with three sets of 10 repetitions and progressed until they could do three sets of 15 repetitions without difficulty. This progression usually occurred within 1 week of rehabilitation in the water. Between the second and third weeks, subjects were advanced to a 40.64-cm (16-in) step in chest-deep water and the progression format was repeated. Between the fourth and eighth weeks, subjects used the 40.64-cm step in waist-deep water to reduce the force of buoyancy on body weight, thereby increasing resistance. Exercises in waist-deep water progressed in the same manner. If subjects were able to perform three sets of 15 repetitions on the 40.64-cm step in waist-deep water without difficulty, they were positioned on a 40.64-cm step in thigh-deep water for maximal resis- tance and the sequencing format was repeated.
The next group of exercises consisted of standing hip flexion, extension, abduction, adduction, and knee flex- ion strengthening. The TR group performed these exercises using pul- leys that contained a stack of 4.5-kg (10-lb) plates. Subjects initiated each exercise with a weight they could lift comfortably for three sets of 10 repe- titions and progressed until they could perform three sets of 15 repeti- tions without difficulty. Another 4.5-kg plate was then added, and the exer- cise was repeated with three sets of 10 repetitions.
Hip strengthening and knee flexion exercises were done using a Hydro- tone exercise boot* (Fig. 2). Exercises consisted of three sets of 10 repeti- tions for hip flexion-extension, abduction-adduction, and knee flex- ion. Because this study did not intend to quantify the amount of resistance in the water or to increase the surface area of the Hydrotone boot, subjects were instructed to move their in- volved legs through the water as fast as they could. As symptoms decreased
Physical Therapy /Volume 74, Number 8/August 1994

ware (version 5.1)* were used to calculate and record peak torque (in
Flgure 2. Hydrotone resistance boot used by subjects in the water group.
and muscle performance improved, subjects increased the speed and created more resistance.
Data Collection
Arthrometric measurements. Joint laxity was measured preoperatively and at 8 weeks following surgery. Measurements were made by one of two physical therapists (BJT and JC) using a KT-1000 knee arthrometer.' This device has the highest diagnostic accuracy of five different arthrometric de~ices.~6 Anterior drawer testing was performed with the knee flexed 30 degrees. Anterior displacement of the
tibia on the femur was measured (in millimeters) during 6.8-kg (15-lb) and 9.1-kg (20-lb) Lachman tests. Greater forces were not used in fear of over- stressing the graft during this critical period of graft healing. The testers maintained 100% agreement, within 0.5 mm, both with a prior reliability study and throughout this study.
Muscle performance measurements. Isometric and isoki- netic peak knee torques were mea- sured at the end of the eighth week of rehabilitation and compared be- tween groups. An electromechanical dynamometer$ and LIDO@ AC+ soft-
+Medrnetric, San Diego. CA.
$Loredan Biomedical Inc, 2121-B 2nd St, Ste 107, Davis, CA 95616.
"elcro USA Inc, 406 Brown Ave, Manchester, NH 03108.
foot-pounds), and gravity-corrected measurements were obtained. Accord- ing to the manufacturer, the dyna- mometer's accuracy is self-calibrated through the computer software pack- age. One tester, who was blind to group assignment, performed all the testing.
During the testing session, subjects were positioned with their hips in 80 to 90 degrees of flexion. The hips and tested limb were stabilized with Vel- cro@ straps across the pelvis and over the thigh. Subjects were in- structed to grasp the handrails during the test. The axis of rotation of the dynamometer was aligned with that of the knee, and the lever arm pad was placed 7.62 cm (3 in) below the tibial tubercle. Subjects were allowed a short period of familiarization at each speed.
Isometric testing consisted of three maximal 5-second repetitions with the knee flexed 85 degrees to measure knee extension torque and three maximal 5-second repetitions with the knee flexed 60 degrees to measure knee flexion torque. Subjects were given a 30-second rest period be- tween repetitions. The highest torque value was recorded.
Isokinetic testing consisted of three separate contractions at 90°/s with a 30-second rest period between repeti- tions. Isokinetic extension was tested from 80 to 40 degrees of knee flex- ion, and isokinetic flexion was tested from 0 to 70 degrees of knee flexion. Isohnetic extension was done sepa- rately from isokinetic flexion to pre- vent possible shearing during changes in direction. The maximum peak torque for the three repetitions was recorded for each of the four tests. AU subjects were tested in the same order.
Passlve range of motion measurements. Passive range of motion (PROM) measurements for knee flexion and extension were taken by one of the two physical ther- apists using a standard plastic goni-
26/714 Physical Therapy/Volume 74, Number 8/August 1994

- Table 2. Results of Analysis of Variance of Dzferences in Joint Laxity Measurements During a 6.8-kg (15-lb) Lachmun Test
Source df SS MS F P
Between subjects Groups (A) 1 21 .OO 21 .OO 3.43 ,082
Error 17 104.08 6.12
Within subjects Weeks (B) 1 50.84 50.84 8.39 .01
A x B 1 0.003 0.003 0.00 ,984
Error 17 103.05 6.06
ometer (17.78 cm [7 in] long with a 360" scale and 1" increments). The testers maintained 100% agreement, within 5 degrees, both with a prior reliability study and throughout this study.
Passive range of motion was mea- sured at the beginning of each treat- ment session at 2, 4, 6, and 8 weeks postoperatively. Subjects were al- lowed a 3-minute warm-up, which consistell of self-stretching within their available ROM. Both measure- ments were taken with subjects posi- tioned supine. Knee extension mea- surements were taken with a towel roll under the heel of the involved extremity. Knee flexion measurements were taken with the hip maintained at 90 degrees of flexion, while the heel was moved toward the buttocks. End- range was determined by applying overpressure until firm resistance was met. The maximum value of three measurements was recorded.
Girth measurements. Girth mea- surements were taken by one of the two physical therapists during the preoperative visit and at 2, 4, 6, and 8 weeks following surgery. Measure- ments were taken at the mid-patella level and 15.24 cm (6 in) above the mid-patella using a standard tape measure (increments of 0.3175 cm [?h in]) with subjects positioned su- pine with their thigh musculature relaxed. 'These measurement locations were used to document changes in knee joint ehs ion and thigh muscu- lar atrophy. The testers maintained
100% agreement, within 0.636 cm (Y4 in), both with a prior reliability study and throughout this study.
Functional questlonnalre. A func- tional questionnaire was administered at the end of the eighth postoperative week. The questionnaire consisted of a Lysholm scale,27 which quantifies the functional use of the knee joint using a scale of 0 to 100. This rating system is a self-report of the subject's perceived ability of activities such as walking, stair climbing, and squatting and is an accepted method of evaluat- ing functional impairment.27,28 Higher scores indicated better functional use with fewer symptoms.
Data Management and Analysis
Side-to-side differences in joint laxity measurements were calculated and used to compare the values between groups prior to surgery and 8 weeks following surgery. Mean differences were compared using an analysis of variance (ANOVA). A Tukey's pair-wise comparison was used for within- group comparisons, and a Bonferroni pair-wise comparison was used for between-group comparisons.
Measurements of isometric and isoki- netic peak torque for the quadriceps femoris and hamstring muscles were normalized to the values of the unin- volved contralateral musculature and expressed as a percentage. The mean peak torque percentage and the mean Lysholm score were compared be- tween groups using a Student's t test.
The ROM measurements for weeks 2, 4, 6, and 8 were analyzed using a two-way ANOVA (groups X weeks) for repeated measures. A Tukey's pair- wise comparison post hoc test for significance was used for within- group comparisons, and a Bonferroni pair-wise comparison was used for between-group comparisons.
Girth measurements were calculated from measurements of girth at mid- patella and 15.24 cm above mid- patella. Mean differences were com- pared at 2, 4, 6, and 8 weeks using tests identical to those undertaken for ROM. The alpha level of significance was set at .05.
Results
Results of the ANOVAs for joint laxity measurements, presented in Tables 2 and 3, showed no significant differ- ence between groups (F=3.43, 4.04; df=l,l; P=.08, .06), indicating that neither program induced more laxity than the other. A significant effect for time did exist at both the 6.8-kg (F=8.39, df=l, P=.01) and 9.1-kg forces (F=24.0, df= 1, P=.0001), indi- cating that both groups had sign&- cantly less joint laxity at 8 weeks after surgery compared with before surgery.
Comparison of quadriceps femoris and hamstring muscle isometric and isokinetic peak torque percentages (Tab. 4) between groups revealed no significant differences for isometric knee flexion, isometric knee exten- sion, and isokinetic knee extension peak torque percentages. The isoki- netic knee flexion peak torque per- centage, however, was significantly higher for the TR group @=96.4, SD=13.5) than for the PR group @= 81.7, SD=11.1) (P=.01).
Passive range of motion measure- ments were recorded at weeks 2,4, 6, and 8. Table 5 shows that there were no significant differences between groups at each measurement period (F=0.38, df=l, P=.546). As expected, there was a significant effect for time (F= 116.49, df=3, P=.0001), implying that knee joint PROM for both groups
Physical 'rherapy/Volume 74, Number

- between the baseline measurement and the second postoperative week,
Table 3. Results of Analysis of Variance of Differences in Joint Laxity Measurements During a 9.1-kg (20-lb) Lachrnan Test but no difference existed between
groups. Mean Lysholrn scores were significantly higher in the PR group
Source df SS MS F P @=92.2, SD=4.31) than in the TR group @=82.4, SD=12.36) (P=.03)
Between subjects
Groups (A)
Error 17 156.20
Within subjects
Weeks (B) 1 123.73
A x B 1 0.25
Error 17 87.64
improved over the 8 weeks. At 2 weeks following surgery, the first PROM measurement showed that both groups had an average of 117 degrees of knee PROM. Both groups showed progressive increments over time, averaging 20 degrees between weeks 2 and 4, 8 degrees between weeks 4 and 6, and 4 more degrees between weeks 6 and 8. Mean knee PROM for both groups at the end of the 8-week program was 150 degrees. Post hoc analysis revealed that gains in PROM were significant for both groups only during the first 6 weeks. No significant differences were noted between groups. There was no signifi- cant groupx time interaction, indicat- ing that change in PROM over time was not dependent on assignment.
Girth measurements taken at mid- patella and 15.24 cm above mid- patella were compared between knees to determine mean differences (Tab. 6). Between-group analysis showed that the PR group had less girth than the TR group for each mid- patella measurement, but the differ- ence was significant only at 8 weeks. No significant difference between groups was noted (F=2.09, df= 1, P=.l66). A time effect was shown (F=23.45, df=4, P=.0001), as both groups had a significant increase in girth at mid-patella between the base- line measurement and the second postoperative week. Additionally, both groups showed a significant decrease in girth at mid-patella after the second week, but only until week 4. At 15.54 cm above mid-patella, both groups had significant decreases in girth
Lysholm scale measurements showed that the PR group scored significantly higher than the TR group at 8 weeks, indicating that this group had fewer problems with activities of daily living. Increased pain, based on the subjects' self-report, and knee swelling during activities of daily living were primarily responsible for lower scores in the TR group. The results of the laxity and girth measurements may offer possible reasons why the PR group had higher Lysholm scores.
At 8 weeks following surgery, both groups had less than 3 mm of differ- ence in joint laxity between the in- volved and uninvolved knees for both the 6.8- and 9.1-kg Lachman tests. Neither program induced knee joint laxity, as a laxity difference of 5 3 mm is considered normal.29 Although between-group comparisons revealed no significant difference, the within- group means at the end of 8 weeks indicated that the TR group had greater than 1.5 mm more laxity for both tests than the PR group. The inability to detect a significant differ- ence between groups may have been due to insufficient sample size. This - result may be due to the increased stresses on the knee joint during
Table 4. Means and Standard Deviations for Group Peak Torque Recovery at the rehabilitation on land with Eighth Postoperative Week (Percentage of Nonoperative Limb's Peak Torque) in water.l5 Increased knee joint laxity
in the surgical knee at 8 weeks could lsometrlc Peak lsoklnetlc Peak have resulted in increased knee joint Torque Percentage Torque Percentage effusion, which may have led to the (07s) (90°1s) lower Lysholm scores.
Group % SD % SD Girth measurements taken at 15.24 kg -
above mid-patella showed no signs- Traditional rehabilitation (n=9)
cant difference between groups for Flexion 85.1 9.1 96.4 13.5 atrophy of the thigh musculature. Extension 43.1 11.6 56.1 9.2 Within-group comparison, however,
Pool rehabilitation (n=10) revealed that both groups followed Flexion 83.7 10.6 81.7 1 l . l the same significant changes from the Extension 42.8 12.7 50.6 18.1 presurgical measurement until the
eighth postoperative week. Both
Physical Therapy /Volume 74, Number 8/August 1994

in greater circumferential measurements. Table 5. Results of Analysis of Variance of Dgerences Between Groups in Recovey
of Range of Motion
Source df SS MS F P
Between subjects
Groups (A) 1 132.61 132.61 0.38 ,546
Error 18 6287.63 349.31
Within subjects
Weeks (B) 3 13277.84 4425.95 1 16.49 .0001
A X B 3 48.24 16.08 0.42 ,737
Error 54 2051.66 37.99
groups experienced the greatest change between the presurgical mea- surement and the second postopera- tive week, with the greatest decrease in girth occurring at the fourth post- operative week. Thigh musculature atrophy is commonly observed during the acutt: postsurgical period due to muscle inhibition that takes place from the increased joint effusion and increased pain. DeAndrade et a13O have shc~wn that with increased knee joint effusion, there is less muscle output as measured by electromyo- graphic activity.
Thigh girth began to increase after the fourth postoperative week, and the involved extremity was within 1.90 cm (0.75 in) of the contralateral extremity by the eighth postoperative week for both groups. Increases in thigh girth at this time may be attrib- uted to several factors. As postopera- tive joint effusion and pain decrease while ROM increases, the thigh mus- culature can be exercised through a greater ROM. As exercises are per- formed more vigorously, muscle tissue begins to hypertrophy, resulting -
Table 6. Results of Analysis of Variance of Dzffwences Between Groups for Girth Measurenzents at Mid-patella and 40.62 cm (6 in) Above Mid-patella
Source df SS MS F P
Mid-patella
Between subjects
Groups (A)
Error
Within sl~bjects
Weeks (B)
A x Bm
40.64 cm above mid-patella
Betweeri subjects
Groups (A) 1 0.006 0.006 0.01 ,933
Error 17 15.53 0.80
Within S L J ~ ~ ~ C ~ S
Weeks (B)
A X B
Error
Girth measurements taken at mid- patella showed that the girth for the PR group was consistently less at each time period, but these differences were significant only at 8 weeks. As discussed earlier, the increased ginh in the TR group may have been caused by the joint effusion resulting from greater stress on the joint dur- ing land exercises compared with water exercises. This increased joint effusion may have led to lower Ly- sholm scores.
Within-group comparison reveals that mid-patella ginh measurements changed similarly for both groups; that is, measurements at this location were inversely related to the mea- surements taken at 15.24 kg above mid-patella. The greatest increase in girth was noted between the presurgi- cal measurement and the second postoperative week, suggesting the increased joint effusion that typically occurs following surgery. These re- sults indicate that as joint effusion decreases, muscle girth increases, with the transition occurring around 4 to 6 weeks following surgery.
Between-group comparison for peak torque percentages (PTPs) showed that the TR group had a significantly higher PTP for the hamstring muscles at 90°/s, indicating that the traditional rehabilitation approach was more effective than the pool rehabilitation approach for strengthening the ham- string muscles. This result may have occurred for two reasons. First, resis- tance in the water was partially deter- mined by the speed of limb move- ment, which was controlled by each subject.16 Subject effort can be affected by pain and motivation. Therefore, subjects may not have generated enough resistance to facilitate maxi- mal strengthening. Hamstring muscle exercises in the TR group were done using weights, so resistance was not self-paced. Second, there is a differ- ence in the type of muscle contrac- tion that occurs on land. Empirical evidence suggests that an eccentric muscle contraction is important for
Physical Therapy /Volume 74, Number 8/August 1994

restoring muscle perf0rmance.3~ This type of contraction is more likely to occur on land than in water due to increased gravitational forces.
In both groups, there was equal effec- tiveness in restoring quadriceps femo- ris muscle strength. These results also showed that greater joint effusion in the TR group did not significantly affect peak torque muscle perfor- mance. A possible reason for this finding is that all subjects were tested in the range of 85 to 40 degrees of knee flexion, rather than at the end- range where joint effusion has been shown to s e c t muscle perfonnance.30
The mean PTPs for both groups are similar to those reported for other subjects with ACL reconstructions.5 Other studies,7,8 however, have dem- onstrated higher peak torque values. Two possible explanations for lower PTPs in this study are the type of quadriceps femoris muscle strength- ening and methodological factors.
Type of Quadriceps Femoris Muscle Strengthenlng
The method of quadriceps femoris muscle strengthening in both groups focused on closed-chain exercises, which may not have provided enough isolated stimulus to the quadriceps femoris muscle to facilitate maximum strength gains. Previous studies,7.8 which demonstrated higher strength gains, applied neuromuscular electri- cal stimulation during open-chain knee extension exercises. Both groups in this study may have bene- fited from isolated knee extension exercises through a limited ROM (90" to 40" of knee flexion to ensure graft protection), as recent research find- ings indicate that closed-chain exer- cises alone may not be enough to facilitate maximum muscle perfor- mance as measured by isokinetic dynamometry.32
Methodological Factors
Changing the methodology may have resulted in higher mean PTPs. Per- forming three 5-second isometric quadriceps femoris muscle contrac-
tions resulted in donor site pain (the anatomical site at which the central third of the patellar tendon was surgi- cally removed for use as an au- tograft) in some subjects in both groups, which may have altered the remaining tests. Anterior knee pain is common in the early phases of ACL rehabilitation if a patellar tendon autograft is used. Testing isometrically and at slow speeds increases the joint reaction forces around the patella, but usually is a better indicator of strength. Although strength testing in this study provided adequate graft protection, testing at faster speeds first and slower speeds at the end of the testing session might have resulted in better PTP scores. The testing proce- dure in this study did not take these factors into account because at the time the study was proposed, no published research had incorporated isokinetic testing at 8 weeks, using only subjects with patellar tendon autografts.
Clinical lmpllcatlons
Although a primary goal in the reha- bilitation of patients with ACL recon- structions is the restoration of quadri- ceps femoris muscle performance, the means of achieving this goal must avoid overstressing the graft and in- creasing joint ehsion. Addttionally, to expedite recovery, patients must toler- ate the rehabilitation program. Some patients find postoperative exercises too uncomfortable because of age, low presurgical activity level, o r low pain tolerance, and progression dur- ing the early phases of rehabilitation is limited.
Exercises in water may make the total rehabilitation program more tolera- ble. Although a complete aquatic exercise program may be unneces- sary, augmenting a land program with pool exercises may permit loading the joint to a greater degree. For patients who are unable to tolerate traditional exercises on land, water can be used to facilitate progression to more aggressive exercises. In this study, a water environment was most beneficial for facilitating closed-chain exercises, such as gait training and
step-ups, and the land pulleys ap- peared to be most beneficial for ham- string muscle and hip strengthening. Isolated quadriceps femoris muscle contractions in a safe range using open-chain exercises may have bene- fited both groups.
Patients using a pool for rehabilitation are likely to tolerate an even more aggressive rehabilitation program than that presented in this study. In this study, however, exercises in both groups had to be carefully matched to ensure that the main effect between rehabilitation programs was due to the environment. The PR group could have performed more advanced exer- cises, but varying the exercises would have made interpretation of results unclear because differences between groups could have then been attrib- uted to the environment, exercises, or interaction between the two.
Although traditional exercises have been the treatment choice of most clinicians, the results of this study suggest that a rehabilitation program for patients with intra-articular ACL reconstructions performed in a pool is more effective in reducing joint effusion and facilitating recovery of lower-extremity function as indicated by Lysholm scores. The results also suggest that rehabilitation in water is equally effective as on land for restor- ing knee ROM and quadriceps femo- ris muscle strength, but not as effec- tive in restoring hamstring muscle strength. Clinicians who wish to allow maximal weight bearing may find the adjunct of aquatic exercises useful. Future studies should analyze the effectiveness of a program that com- bines traditional and water exercises, using larger sample sizes and a longer follow-up period.
Acknowledgments
We thank Lynn Snyder-Mackler, ScD, PT, for assisting with preparation of this manuscript; Roberto Infante, PT, and the staff at Resurgeons Ortho- paedics for their assistance with data
Physical Therapy/Volume 74, Number 8/August 1994

collection; and Piedmont Hospital for use of their facilities.
References
1 Paulos LE, Payne FC, Rosenberg TD. Rehabil- itation after anterior cruciate ligament surgery. In: Jackson DW, Drez D Jr, eds. The Anterior Cmciate LkJcient Knee. St Louis, Mo: CV Mosby Co; 1987:291-314. 2 Shelbourne KD, Nitz P. Accelerated rehabili- tation after anterior cruciate ligament recon- struction. Am ] Sports Med. 1990;18:292-299. 3 Paulos IE, Noyes FR, Grood ES, Butler DL. Knee rehabilitation after anterior cruciate liga- ment reconstruction and repair. Am] Sports Med. 1981 9140-149. 4 Shelbourne KD, Wilckens JH. Current con- cepts in ar~terior cruciate ligament rehabilita- tion. Orthcp Rev. 1990;11:957-964. 5 Draper V, Ballard L. Electrical stimulation versus electromyographic biofeedback in the recovery of quadriceps femoris muscle func- tion following anterior cruciate ligament sur- gery. Phys Thet. 1991;71:455-464. 6 Draper 'V. Electromyographic biofeedback and rec0vt:r-y of quadriceps femoris muscle function following anterior cruciate ligament reconstruction. Phys Thm 1990;70:11-17. 7 Snyder-Mackler L, Ladin 2, Schepsis Aq Young LC. Electrical stimulation of the thigh musculature after reconstruction of the ante- rior cruciate ligament.] Bone Joint Surg [Am]. 1991;73:1025-1036. 8 Delitto A, Rose SJ, McKowen JM, et al. Elec- trical stimulation versus voluntary exercise in strengthening thigh musculature after anterior cruciate ligament surgery. Phys Ther. 1988;68: 661-663. 9 Ohkoshi Y, Yasada K. Biomechanical analysis of shear force exerted to anterior cruciate liga- ment durirrg half squat exercise. Orrhop Trans. 1989;13:310. 10 Steindler A. Kinesiology of the Human Body Under Nonnal and Pathological Condi-
tions Springfield, Ill: Charles C Thomas, Pub- lisher; 1955. 11 Pope MH, Stankewich CJ, Beynnon BD, Fleming BC. Effect of knee musculature on anterior cruciate ligament strain in vivo. Jour- nal of Electromyography and Kinesiology. 1991;1:191-198. 12 Whieldon T, Yack J, Collins C. Anterior tib- ial translation during weight-bearing and non- weight-bearing rehabilitation exercises in the anterior cruciate deficient knee. Phys Ther. 1989;69:151. Abstract. 13 Henning CE, Lynch MA, Glick KR. An in vivo strain gauge study of elongation of the anterior cruciate ligament. Am] Sports Med. 1985;13:22-26. 14 Reynolds NL, Worrell TW, Perrin DH. Effect of a lateral step-up exercise protocol on quad- riceps isokinetic peak torque values and thigh ginh. ] Orthop Sports Phys Ther. 1992;15: 151- 155. 15 Golland A. Basic hydrotherapy. Physiother- apy. 1981;67:25%262. 16 Edlich RF, Towler MA, Goitz RJ, et al. Bioengineering principles of hydrotherapy. J Bum Care Rehabil. 1987;8:580-584. 17 Hillman MR, Matthews L, Pope J. The resis- tance to motion through water of hydrother- apy table-tennis bats. Physiotherapy. 1987;73: 570-572. 18 Harrison RA, Allard LL. An attempt to quan- tify the resistances produced using the bad ragaz ring method. Physiotherapy. 1982;68:23@- 231. 19 Harrison Rk A quantitative approach to strengthening exercises in the hydrotherapy pool. Physiotherapy. 1980;66:60. 20 Abidin MR, Lobardi SA, Devlin PM, et al. A new hydrofitness device for strengthening muscles of the upper extremity.] Bum Care Rehabil. 1988;9:402-406. 21 Abidin MR, Thacker JG, Becker DG, et al. Hydrofitness devices for strengthening upper extremity muscles.] Bum Care Rehabil. 1988; 9: 199-202. 22 Goitz RJ, Towler TA, Buschbacher LP, et al. A new hydrofitness device for leg muscu-
loskeletal conditioning.] Bum Care Rehabil. 1988;9:203-206. 23 Bartow L, Diamond L. Resistance Training in the Water: An Analysis Comparing the Hydro-tone System to Water Resistance Without a Training Tool in Resistance of the Knee Fler- ors and Extensors. Boston, Mass: Boston Uni- versity; 1989. Master's thesis. 24 Gehlsen GM, Grigsby SA, Winant DM. Ef- fects of an aquatic fitness program on the strength and endurance of patients with multi- ple sclerosis. Phys Ther. 1984;64:653457. 25 Napoletan JC. The Efect of Undenvatet Treadmill Exercise in the Rehabilitation of Sur- gical Anterior Cmciate Ligament Repair. Or- ange, Calif: Chapman College; 1990. Master's thesis. 26 Anderson AF, Snyder RB, Federspiel CF, Lipscomb B. Instrumented evaluation of knee laxity: a comparison of five arthrometers. Am] Sports Med. 1992;20:135-140. 27 Lysholm J, Gillquist J. Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am] Sports Med. 1982;10:150-154. 28 Tegner Y, Lysholm J. Rating systems in the evaluation of knee ligament injuries. Clin Or- thop. 1985;198:43-49. 29 Daniel DM, Malcom LL, Losse G, et al. In- strumented measurement of anterior laxity of the knee.] Bone Joint Surg [Am] 1985;67.720- 726. 30 deAndrade JR, Grant C, Dixon AJ. Joint dis- tension and reflex inhibition in the knee. ]Bone Joint Surg [Am]. 1965;47:3542. 31 Albert M. Physiologic and clinical princi- ples of eccentrics. In: Albert M, ed. Eccenmc Muscle Training in Sports and Orthopaedics. New York, NY: Churchill Livingstone Inc; 1991: 11-23. 32 Reynolds NL, Worrell TW, Perrin DH. Effect of a lateral step-up protocol on quadriceps isokinetic peak torque values and thigh ginh. J Orthop Sports Phys Ther. 1992;15:151-155.
Physical 'Therapy /Volume 74, Number B/August 1994


![Case Report Extra-Articular Lateral Tenodesis for Anterior ... · Extra-articular tenodesis were designed to limit internal tibial rotation in ACL de cient knees [ , , ]. Although](https://img.pdfslide.us/doc/110x75/60b4a6581cb93d1ac82218b2/case-report-extra-articular-lateral-tenodesis-for-anterior-extra-articular-tenodesis.jpg)