Embed Size (px)
Citation preview

The Next Era in GI The Next Era in GI Surgery Surgery BioDynamixTM
AnastomosisThe Colon Ring
Clinical Training Team
BENIGN PATHOLOGYBENIGN PATHOLOGYRectal ProlapseRectal Prolapse

2
Etiology and Symptoms
• Rectal prolapse (procidentia) involves weakness of the pelvic floor and the concept of herniation.
• It is basically a full-thickness rectal intussusception starting approximately three inches above the dentate line and extending beyond the anal verge.
• Women aged 50 and older are six times as likely as men to present with rectal prolapse.
• Contrary to the common assumption that rectal prolapse is a consequence of multiparity, 35% of patients with rectal prolapse are nulliparous.

3
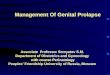
Rectal Prolapse
LEAD POINT
ANUS
LEAD POINT

4
Anatomy and Pathophysiology
• Diastasis of the levator ani, a redundant sigmoid colon, a patulous anal sphincter, and loss of the rectal sacral attachments are commonly described.
• Chronic constipation, defined as infrequent stools or severe straining, is present in over 30-67% of patients; and an additional 15% of patients experience diarrhea.
• Once a prolapse is apparent, fecal incontinence becomes a predominant symptomatic feature occurring in 50-75% of cases.
• Chronically prolapsed rectal mucosa may become thickened, ulcerated, and cause significant bleeding.

5
Differential Diagnosis and Investigation
• A common pitfall in the diagnosis of rectal prolapse is the potential for confusion with prolapsed, incarcerated internal hemorrhoids.
• Prolapsed, incarcerated hemorrhoids produce extreme pain and can be accompanied by fever and urinary retention.
• Prior to operative intervention, a careful history, physical examination, and colonoscopy should be performed.
• A patulous anus with diminished sphincter tone is usually identified.
• Proctoscopy reveals a solitary rectal ulcer on the anterior surface of the rectum in 10-15% of cases.
• Occasionally, the presentation of rectal prolapse can be quite dramatic when the prolapsed segment becomes incarcerated below the level of the anal sphincter. If the prolapse cannot be reduced, emergent operative therapy is indicated.

6
Operative Repair
• Two predominant general approaches, abdominal and perineal, are considered in the operative repair of rectal prolapse, each with multiple variations.
• The surgical approach is dictated by the co-morbidities of the patient, the surgeon’s preference and experience, and the patient’s age.
• Some surgeons will use prosthetic support for the prolapse without bowel resection.
• Some surgeons will fixate the rectum (rectopexy or proctopexy) without bowel resection.
• Various perineal approaches are also proposed.
• The most common procedure for rectal prolapse with which we will be involved is the anterior resection with rectopexy.

7
Abdominal Repairs
• Anterior Resection with Rectopexy—
– The sigmoid colon and rectum are mobilized to the level of the levators.
– The lateral ligaments are divided, elevated from the deep pelvis and often sutured to the presacral fascia (rectopexy).
– Alternatively, the extensive pelvic dissection is deemed adequate to result in an adhesive rectopexy (without sutures).
– The mesentery of the sigmoid colon is then divided with preservation of the inferior mesenteric artery.
– A tension-free anastomosis is created.