Embed Size (px)
Citation preview
JITESH HARYANI
CLASS III
MALOCCLUSION
CONTENTS
Definition
Classification
Prevalence
Etiology
Growth pattern in class III
Components of class III malocclusion
Differential diagnosis
Treatment planning
Treatment modalities
Retention
DEFINITION
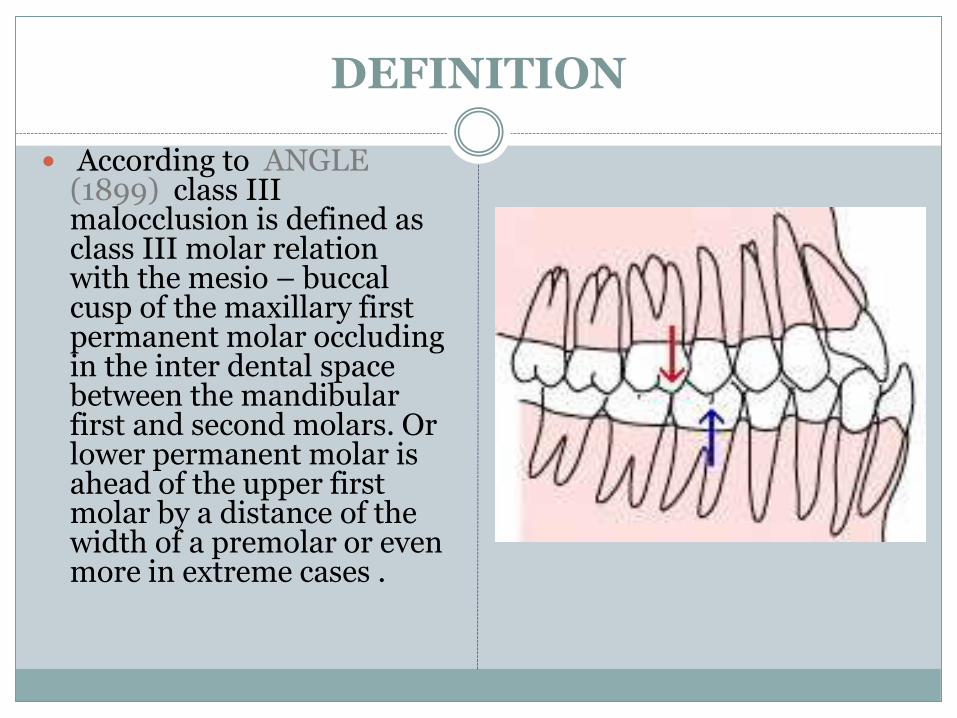
According to ANGLE (1899) class III malocclusion is defined as class III molar relation with the mesio – buccal cusp of the maxillary first permanent molar occluding in the inter dental space between the mandibular first and second molars. Or lower permanent molar is ahead of the upper first molar by a distance of the width of a premolar or even more in extreme cases .
CLASSIFICATION
1. Tweed (1966) divided Class III malocclusion into two categories –
Pseudo class III : normally shaped mandibles (L shaped) and under developed maxilla.
Skeletal class III : large mandibles.
2. Moyers (1997) :
Osseous
Muscular
dental
3. Park and Baik (2001) classified class III based on position of maxilla relative to the craniofacial skeleton. :
Type A : individuals have a normal maxilla and overgrown mandible. This is true mandibular prognathism
Type B : maxillary and mandibular excess, but mandible grows more than maxilla. They have a acute nasolabial angle
Type C : hypoplasia of maxilla; their facial profile is concave with large nasolabial angle, which is frequently camouflaged by dentoalveolar compensations.
PREVALENCE
The frequency of class III malocclusion varies among different ethnic groups.
Caucasians : 1%-4%
African Americans : 5%-8%
Hispanic : 4%- 14%
Indians : 3.4% (Kharbanda et al, 1995)
Only few studies have seperated pseudo and true class III for prevelance.
According to a study by Lin (1985), prevelance of class III malocclusion in chinese children between 9-15 years.
-pseudo class III : 2.3%
-true class III : 1.7%
ETIOLOGY
Class III skeletal growth has a multifactorial basis that is influenced by :
Genetics
Environment
Gene- Environment interaction
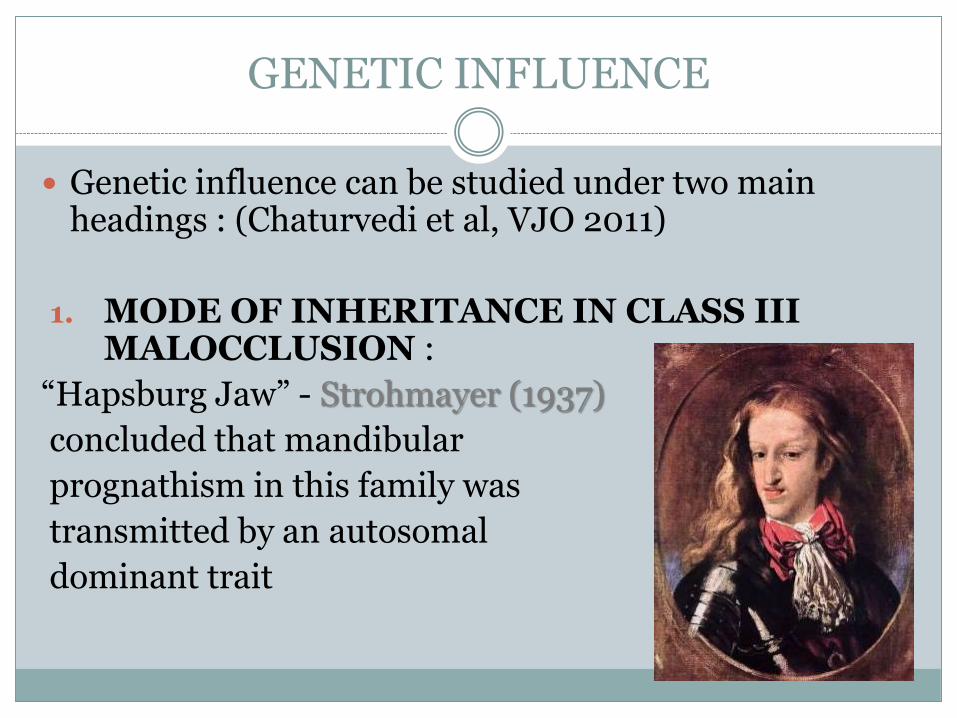
GENETIC INFLUENCE
Genetic influence can be studied under two main headings : (Chaturvedi et al, VJO 2011)
1. MODE OF INHERITANCE IN CLASS III MALOCCLUSION :
“Hapsburg Jaw” - Strohmayer (1937)
concluded that mandibular
prognathism in this family was
transmitted by an autosomal
dominant trait
Suzuki (1961) studied offspring of parents with mandibular prognathism from 243 Japanese families, and reported a frequency of 31% of this condition if the father was affected, 18% if the mother was affected and 40% if both parents were affected.
Polygenic hypothesis : Litton et al (1970)
Manfredi et al (1997) found strong genetic control in vertical parameters and in mandibular structure in twins.
2. ROLE OF GENES IN EXPRESSION OF CLASS III MALOCCLUSION
Condylar cartilage grows in response to functional stimuli or mechanical loading. This in turn leads to mandibular growth.
McNamara and Carlson hypothesized that class III malocclusion might be precipitated under these biomechanical conditions by the inheritance of genes that predispose to a class III phenotype.
Genes involved in mandibular prognathism :
VEGF
IGF – 1
HOX – 3
Ihh and Pthlh (Rabie et al)
COL2A1
Craniofacial anomalies
Cleft lip and palate
Crouzan syndrome
Apert syndrome
Downs syndrome
Binder’s syndrome
ENVIRONMENTAL FACTORS
Enlarged tonsils (Angle; 1907)
Hormonal disturbances (Downs; 1928)
Posture (Gold; 1949)
Nasal blockage (Davidov; 1961)
Congenital anatomic defects (Monteleone; 1963)
Large tongue as in the case of thyroid deficiency can
contribute to a mandibular prognathism by causing the
mandible to be positioned forward all times.
Rakosi and Schilli suggested mouth breathing in the
etiology of class III malocclusions.
Acute cranial base angle and anterior positioned glenoid fossa : Ellis and McNamara (1984) and Singh et al (1997)
GROWTH PATTERN IN CLASS III MALOCCLUSION
Sugawara and Mitani (1997) reported that a class III skeletal pattern is developed at a young age and does not change fundamentally.
However long term growth studies in untreated class III individuals have suggested that the class III pattern worsens with age. (Deguchi et al)
Battagel showed a sexual dimorphism in growth of class III subjects.
Baccetti et al (2007) conducted a longitudinal study in untreated class III subjects based on CVM staging. They concluded that there is persistence of typical Class III growth characteristics well beyond the adolescent growth spurt into early adulthood.
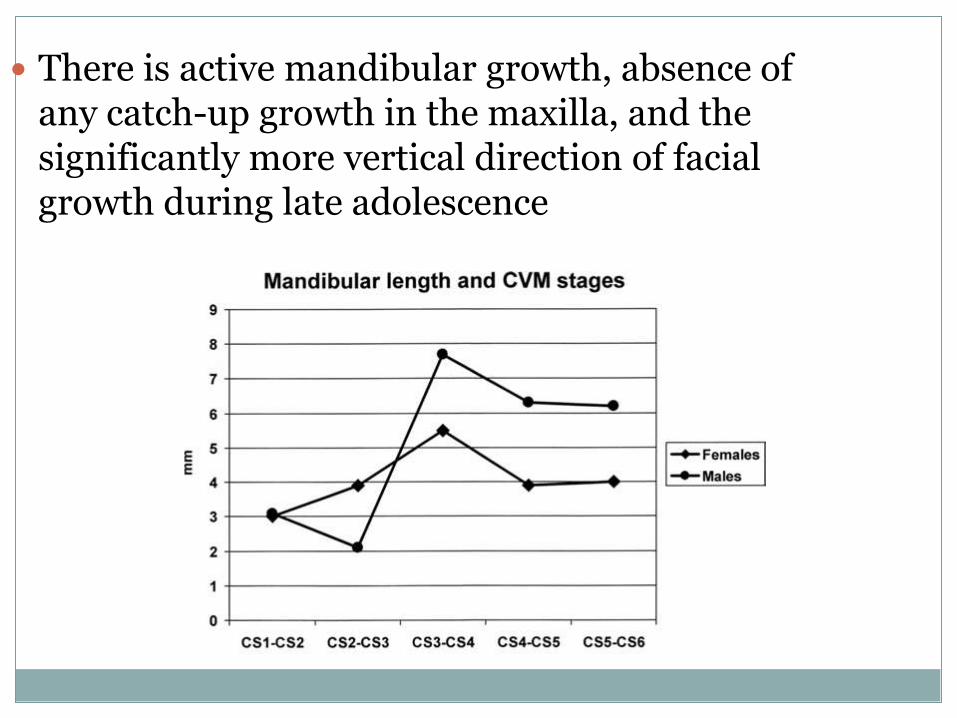
There is active mandibular growth, absence of any catch-up growth in the maxilla, and the significantly more vertical direction of facial growth during late adolescence
COMPONENTS OF CLASS III MALOCCLUSION
The components of class III malocclusion can be grouped into :
1. Mandibular prognathism
2. Maxillary retrognathism
3. Dental retrusion or protrusion
4. Combinations of above
5. Pseudo class III or functional class III
According to Guyer et al, mandibular prognathismand class III malocclusion are not synonymous.
Infact mandibular prognathism as a primary cause of class III was found in only 19 % cases.
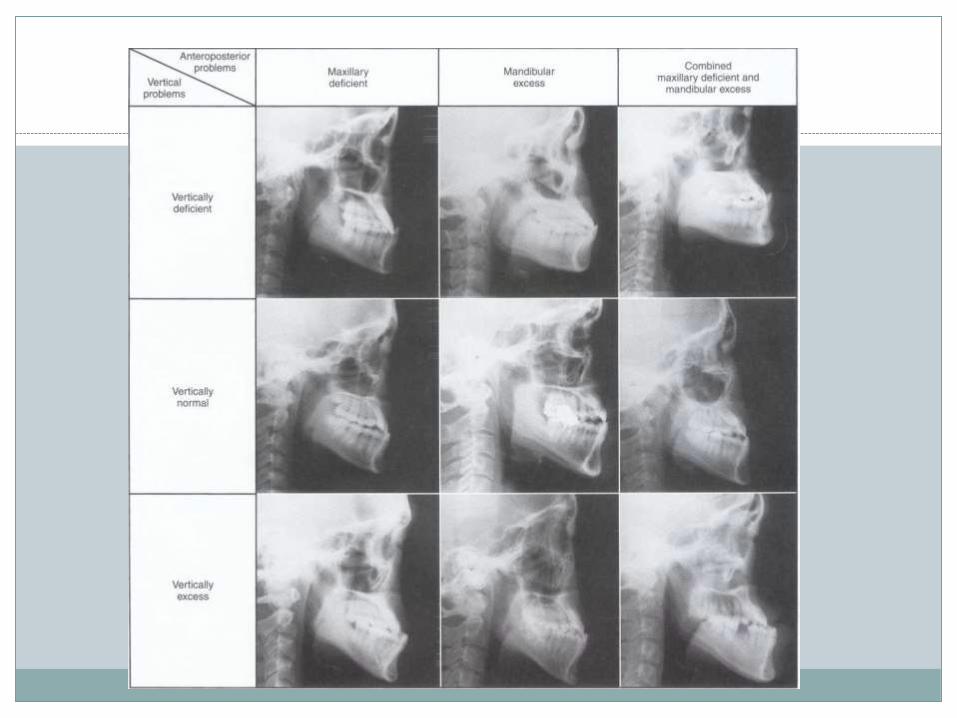
Ellis and McNamara calculated 243 possible combinations of class III malocclusion.
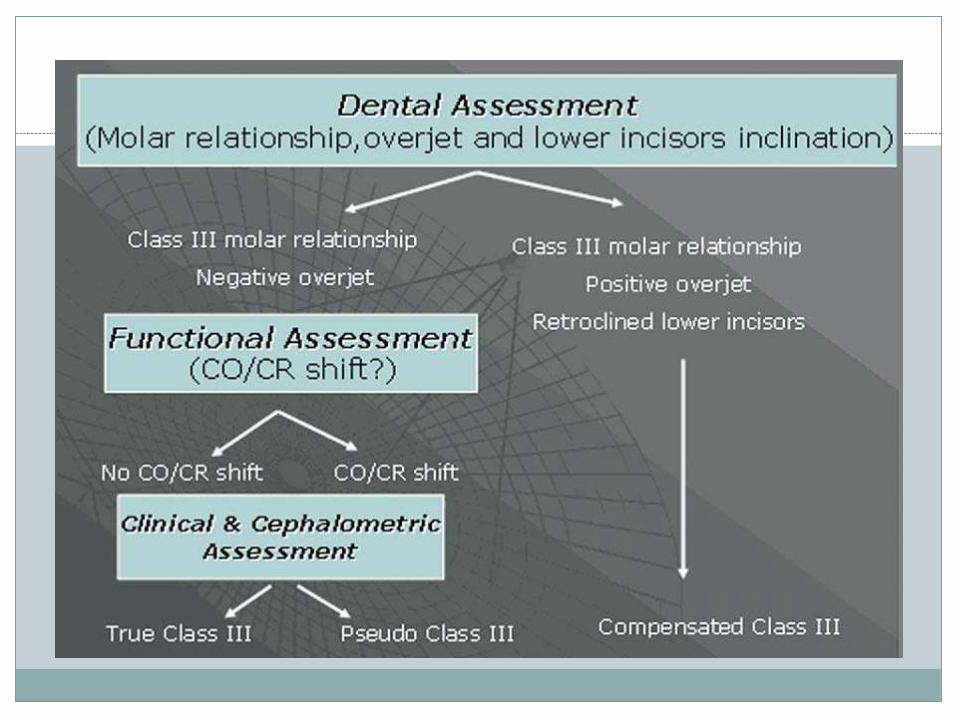
DIAGNOSIS OF CLASS III MALOCCLUSION
In evaluating the Class III relationship during the primary or mixed dentition period, it is important to consider whether the problem is dentoalveolar or skeletal in origin.
Dental assessment
Functional assessment
Profile assessment
Cephalometric assessment
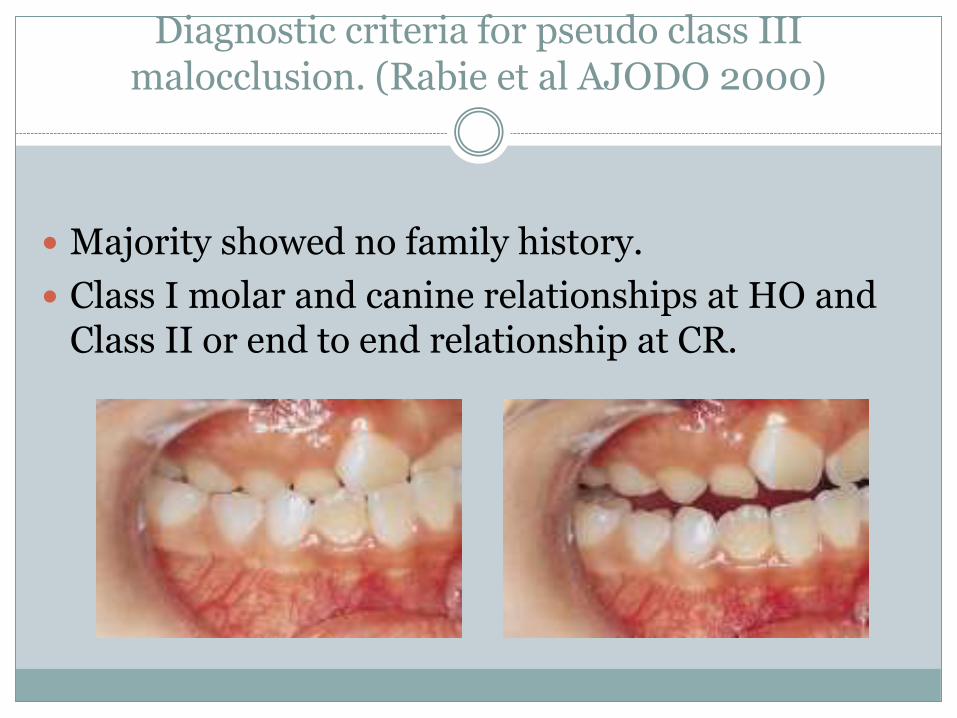
Diagnostic criteria for pseudo class III malocclusion. (Rabie et al AJODO 2000)
Majority showed no family history.
Class I molar and canine relationships at HO and Class II or end to end relationship at CR.
Decreased midface length.
Forward position of the mandible with normal mandibular length.
Retroclined upper incisors and normal lower incisors.
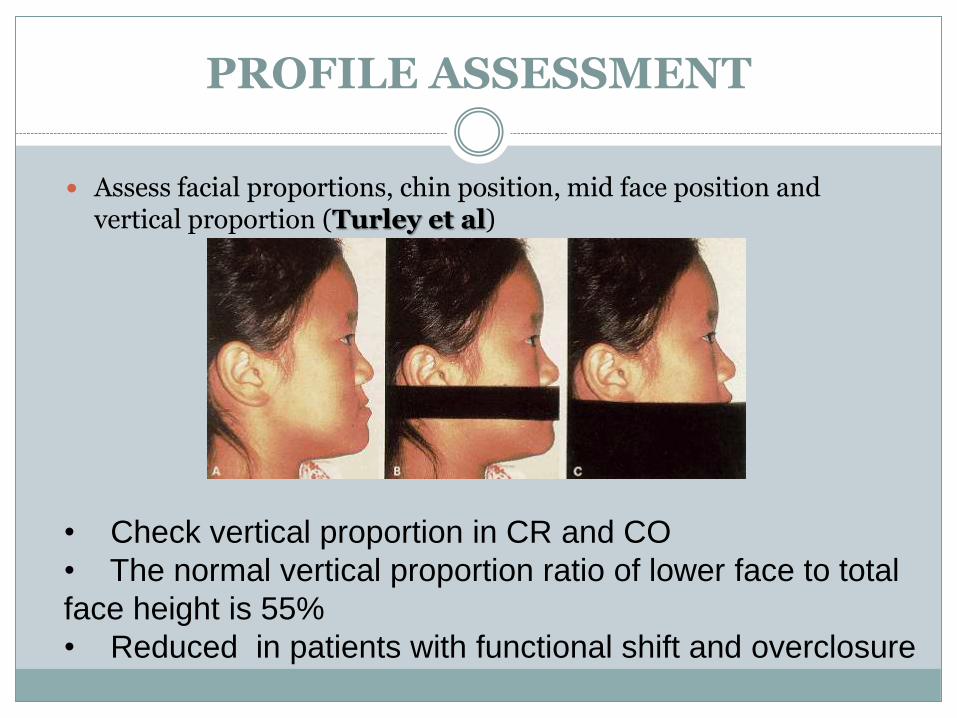
PROFILE ASSESSMENT
Assess facial proportions, chin position, mid face position and vertical proportion (Turley et al)
• Check vertical proportion in CR and CO
• The normal vertical proportion ratio of lower face to total
face height is 55%
• Reduced in patients with functional shift and overclosure
CEPHALOMETRIC ASESSMENT
The following distinctions can be made in categorizing the class III sagittal relationship:
Class III malocclusion with dentoalveolarmalrelationship.
Class III malocclusion with a long mandibularbase.
Class III malocclusion with an underdeveloped maxilla.
Class III malocclusion with combination of underdeveloped maxilla and prominent mandible; horizontal or vertical growth pattern.
Class III malocclusion with tooth guidance or pseudo-forced bite.
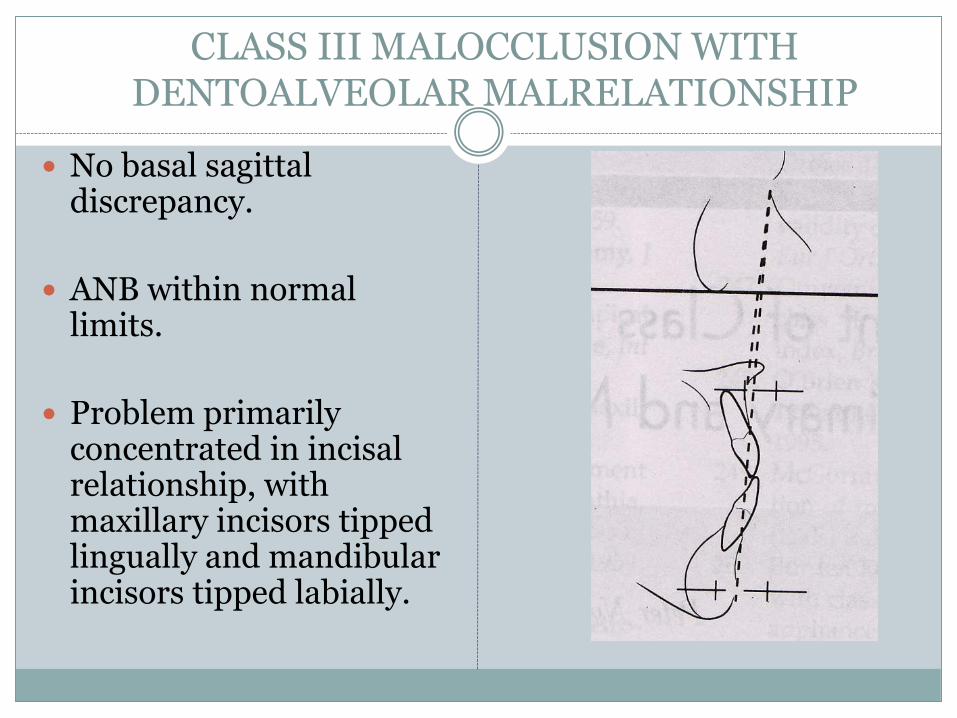
CLASS III MALOCCLUSION WITH DENTOALVEOLAR MALRELATIONSHIP
No basal sagittaldiscrepancy.
ANB within normal limits.
Problem primarily concentrated in incisal relationship, with maxillary incisors tipped lingually and mandibular incisors tipped labially.
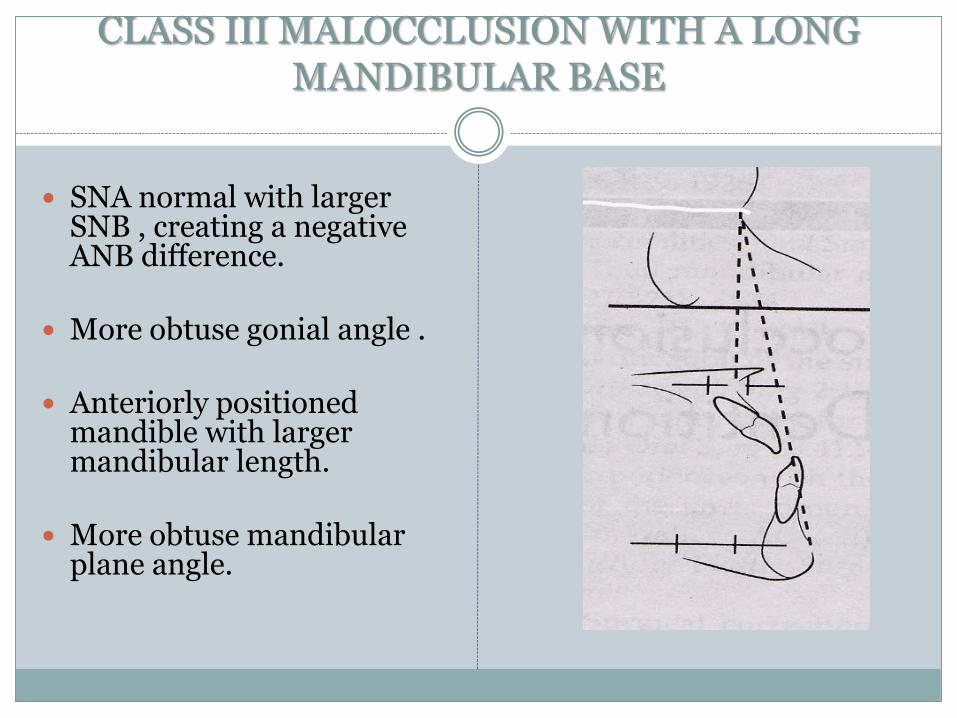
CLASS III MALOCCLUSION WITH A LONG MANDIBULAR BASE
SNA normal with larger SNB , creating a negative ANB difference.
More obtuse gonial angle .
Anteriorly positioned mandible with larger mandibular length.
More obtuse mandibular plane angle.
Tongue morphology is flattened ; whereas tongue is postured forward and lies lower in the mouth.
The upper incisors are labially tipped, and the lower incisors are inclined lingually.
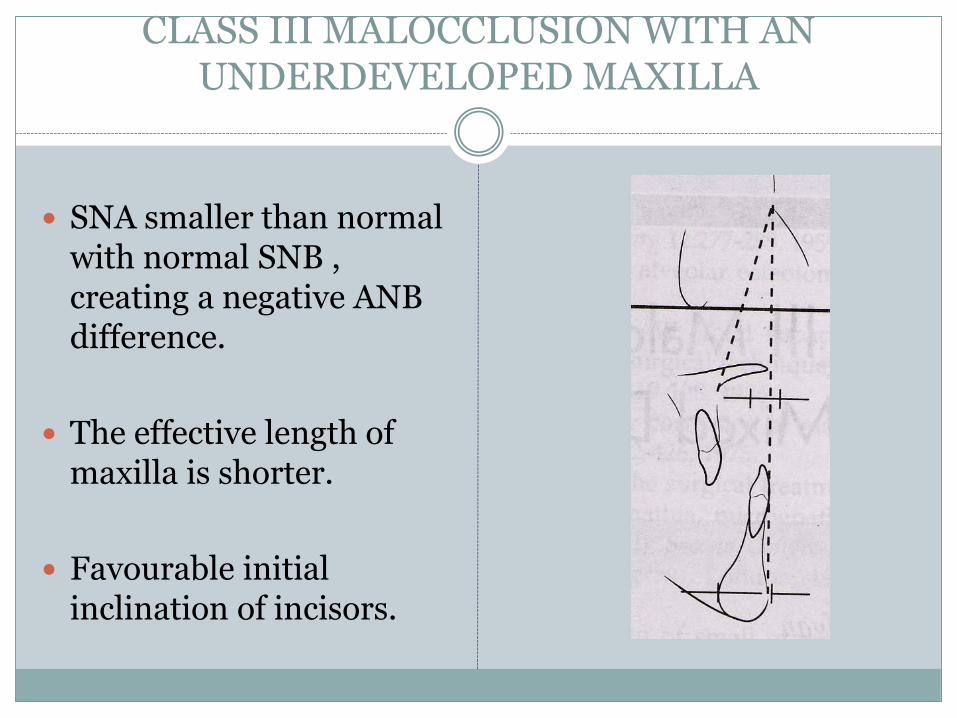
CLASS III MALOCCLUSION WITH AN UNDERDEVELOPED MAXILLA
SNA smaller than normal with normal SNB , creating a negative ANB difference.
The effective length of maxilla is shorter.
Favourable initial inclination of incisors.
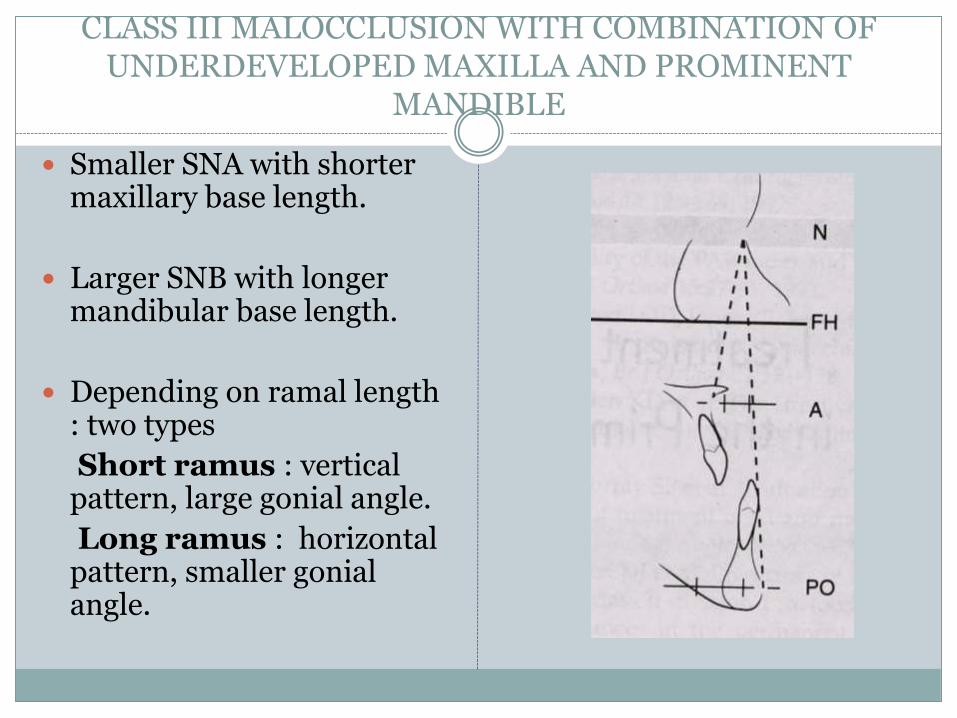
CLASS III MALOCCLUSION WITH COMBINATION OF UNDERDEVELOPED MAXILLA AND PROMINENT
MANDIBLE
Smaller SNA with shorter maxillary base length.
Larger SNB with longer mandibular base length.
Depending on ramal length : two types
Short ramus : vertical pattern, large gonial angle.
Long ramus : horizontal pattern, smaller gonialangle.
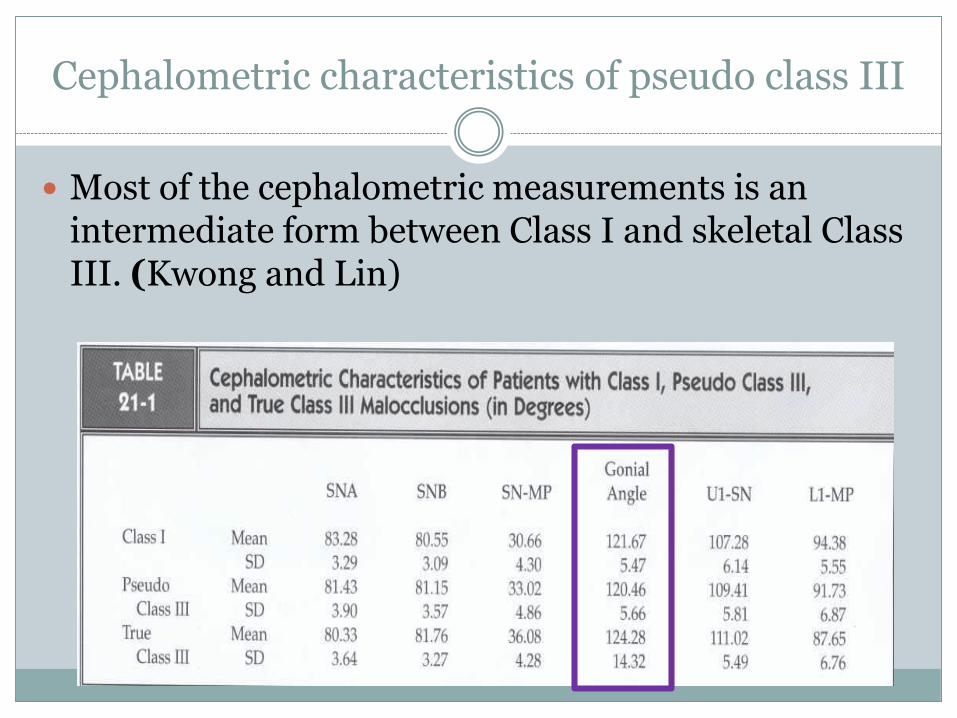
Cephalometric characteristics of pseudo class III
Most of the cephalometric measurements is an intermediate form between Class I and skeletal Class III. (Kwong and Lin)
Measurement of the gonial angle in the pseudo Class III sample is found to be rather similar to the Class I sample, making this measurement a key diagnostic feature in the differential diagnosis between pseudo and skeletal Class III malocclusions.
DIAGNOSTIC CHARACTERISTICS OF AN
UNFAVOURABLE CLASS III GROWTH
38
1. An increased gonial angle
2. Antegonial notching
3. Backward direction of condylar growth
4. Thin mandibular symphysis
5. Compensation in position of upper and lower incisors in response to disproportionate jaw growth.
Mandibular incisors are retroclined as child becomes older there roots tend to press against the labial plate producing a WASH BOARD EFFECT.
Maxillary incisors are usually flared anteriorly.
TREATMENT PLANNING FOR CLASS III MALOCCLUSION
The therapeutic possibilities of class III malocclusion depends upon :
The developmental age of the patient
The nature of malocclusion.
There are three main treatment options for skeletal class III malocclusion:
Growth modification,
Dentoalveolar compensation (orthodontic camouflage), and
Orthognathic surgery.
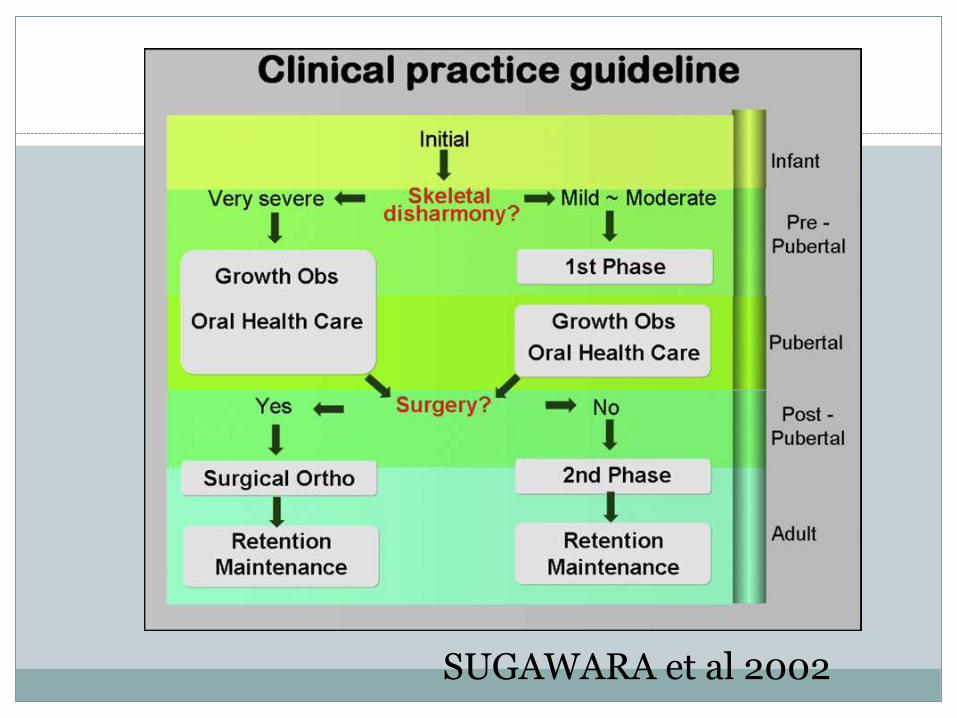
SUGAWARA et al 2002
TWO MAIN DILEMMAS
ONE PHASE V/S TWO PHASE THERAPY
CAMOUFLAGE V/S SURGERY
EARLY TREATMENT OF SKELETAL
CLASS III MALOCCLUSION:43
The “Doctrine of limitations” was in full swing in the 40”s and 50”s. Early treatment was condemned except for serial extractions.
But evidence based researches have led to many favorable conclusions for early treatment. Class III malocclusion, in particular gets the nod from many authors in favor of early treatment .Starting with Tweed, treatment timings can be as early as 4 years of age.
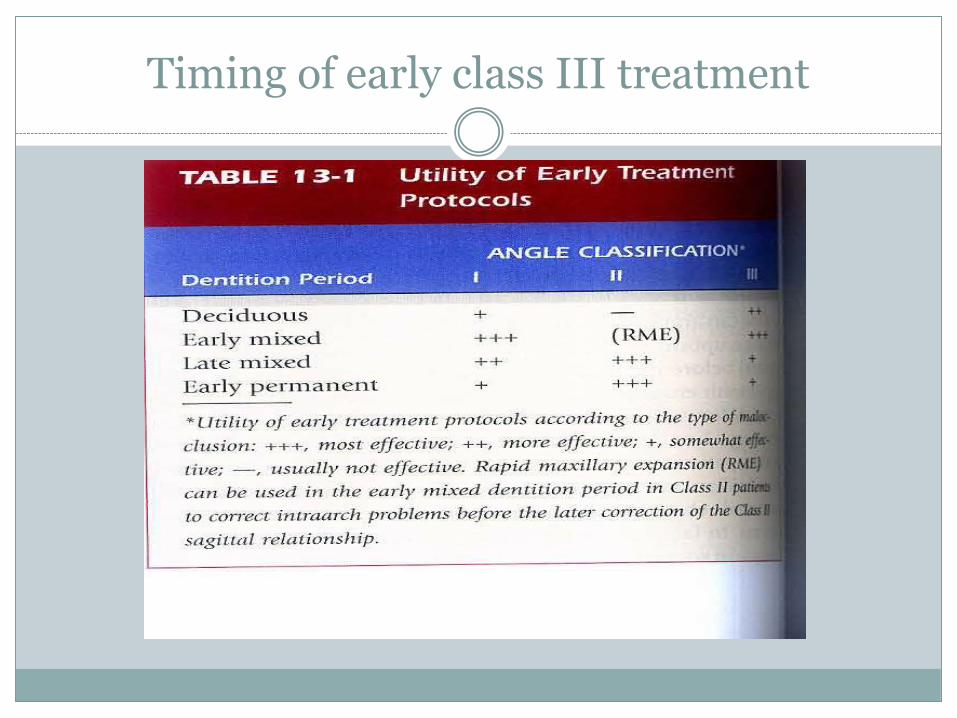
Timing of early class III treatment
45
Turpin has developed a list of positive and negative factors to aid in deciding when to interrupt a developing class III malocclusion
POSITIVE FACTORS:
1. Good facial esthetics
2. Mild skeletal disharmony
3. No familial prognathism
4. Antero posterior functional shift
5. Convergent facial type
6. Symmetric condylar growth
7. Growing patients with expected good cooperation.
8. If the above factors are not present in the patient , they are listed as negative and treatment can be delayed until growth is completed.
46
Joondeph, after Turpin’s thesis, also pointed out
the goals of early intervention:
1. Reduce the skeletal discrepancy and provide a
more favorable environment for normal growth.
2. Achieve as much relative maxillary advancement
as possible.
3. Improve occlusal relationships.
4. Improve facial esthetics for more psychosocial
development.
5. Reduce or simplify, phase II or surgical treatment.
Studies showing greater maxillary protraction in early treatment of class III
Irie and Nakamura – 1975
Profitt – 1986
Nakada et al – 1993
Kapust et al – 1998
Baccetti et al – 1998
Franchi , Baccetti and McNamara - 2004
Studies which concluded no difference in early or late treatment of classIII
Baik – 1995
Baik and Sung 1998
Yuksel et al 2001
But none of these studies evaluated the long term effect of early class III treatment
Long term effect of early class III treatment
Despite the known influence of early treatment on the facial appearance of growing patients with skeletal Class III malocclusion, few comparative reports on the long-term effects of different treatment regimens (1-phase vs 2-phase treatment) have been published.
In a case report presented by Sugawara and Nanda (AJODO 2012), they compared the effects of early orthodontic intervention as the first phase of a 2-phase treatment vs 1-phase fixed appliance treatment in identical twins over a period of 11 years.
They reported that inspite of the different treatment approaches, both their patients showed identical dentofacial characteristics in the retention phase.
They concluded that :
Early treatment had no impact on jaw growth in the pubertal growth period.
The criteria for the selection of 1-phase or 2-phase treatment depend entirely on the patient’s requirements. Because the biologic outcome is the same
Prediction of class III growth pattern
One of the reasons clinicians are reluctant to render early orthopedic treatment in Class III patients is the inability to predict mandibular growth.
Discriminant analysis of long-term results of early treatment identified several variables that had predictive values.
Franchi et al found the inclination of the condylarhead, the maxillomandibular vertical relationship together with the width of the mandibular arch could predict success or failure of early Class III treatment
Ghiz et al found that the position of the mandible, the ramal length, the corpus length, and the gonialangle can predict successful outcomes with 95% accuracy.
GTRV analysis(Growth Treatment Response Vector)
3/8/2015 3:04 PM
54
This analysis helps in determination of the individual growth rate and direction. Lateral cephalometric radiographs are taken after facemask treatment and during the 3 to 4-year follow-up visit.
55
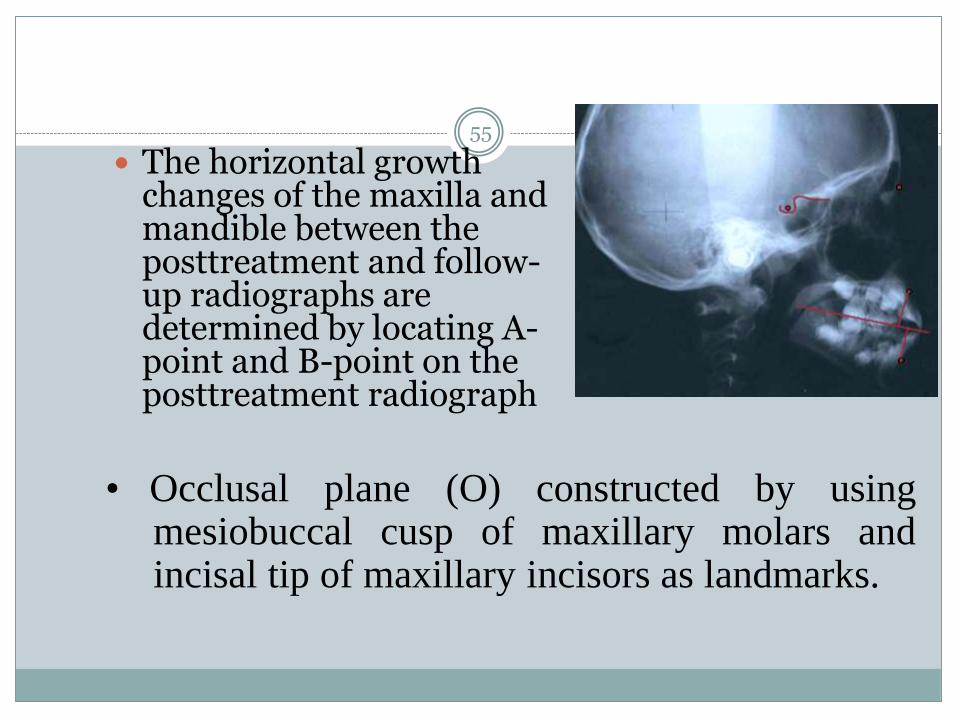
The horizontal growth changes of the maxilla and mandible between the posttreatment and follow-up radiographs are determined by locating A-point and B-point on the posttreatment radiograph
• Occlusal plane (O) constructed by usingmesiobuccal cusp of maxillary molars andincisal tip of maxillary incisors as landmarks.
3/8/2015 3:04 PM
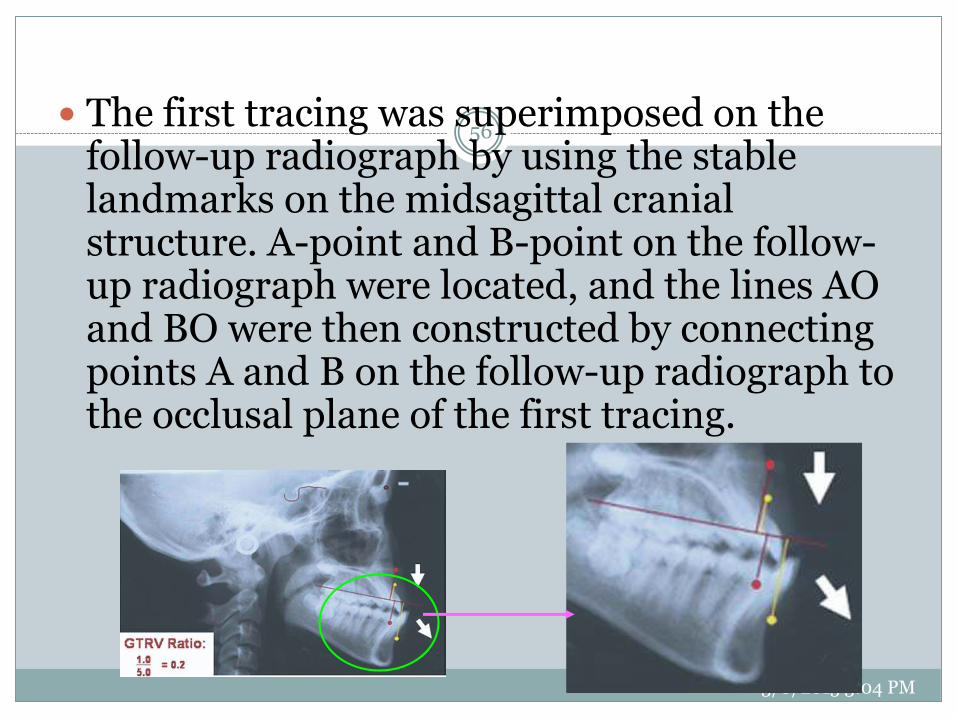
56 The first tracing was superimposed on the
follow-up radiograph by using the stable landmarks on the midsagittal cranial structure. A-point and B-point on the follow-up radiograph were located, and the lines AO and BO were then constructed by connecting points A and B on the follow-up radiograph to the occlusal plane of the first tracing.
3/8/2015 3:04 PM
57
The distance between the A-point on the 2 tracings along the occlusal plane represents the growth changes of the maxilla, and the distance on the occlusal plane of B-point represents the growth changes of the mandible
3/8/2015 3:04 PM
58
The GTRV ratio was calculated by using the following formula:
This ratio and vector analysis provides information
on growth rate and direction and helps clinicians
to decide whether the Class III malocclusion can
be camouflaged by orthodontic treatment or
whether a surgical treatment is warranted.
3/8/2015 3:04 PM
59
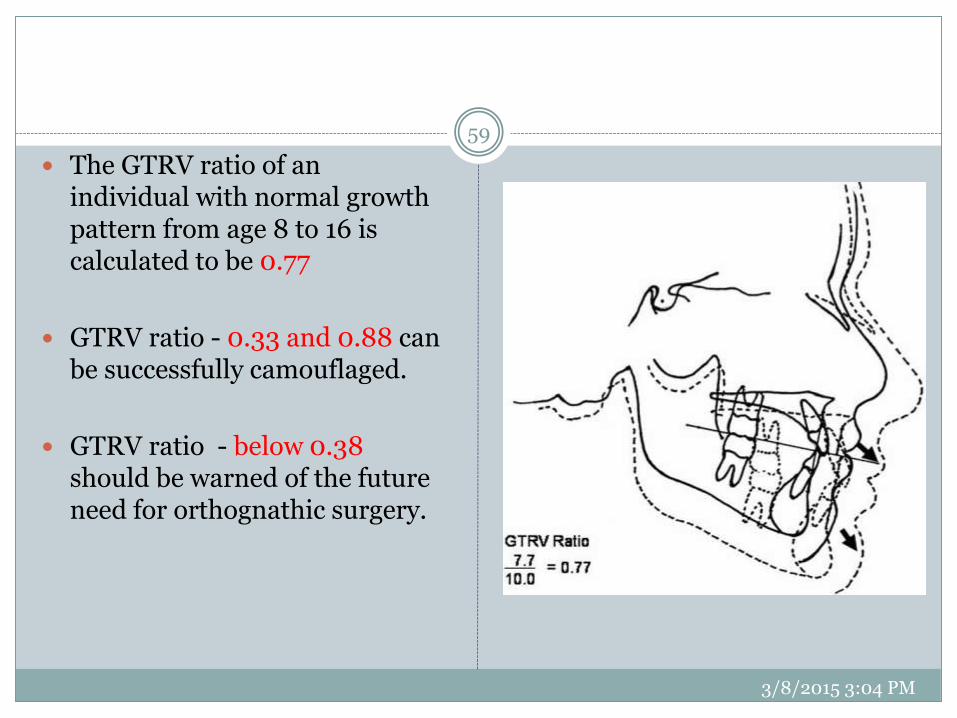
The GTRV ratio of an individual with normal growth pattern from age 8 to 16 is calculated to be 0.77
GTRV ratio - 0.33 and 0.88 can be successfully camouflaged.
GTRV ratio - below 0.38 should be warned of the future need for orthognathic surgery.
Camouflage v/s surgery – The borderline case
Cassidy (AJODO 1993) defined “borderline cases” as those patients who were similar with respect to the characteristics on which the orthodontic/surgical decision appeared to have been based.
Kerr et al(BJO 1992) established some cephalometricyardsticks in adult patients with class III malocclusion to find objective criteria for treatment options. These researchers suggested that surgery should be performed for patients with
an ANB angle of less than -4°, a
maxillary/mandibular (M/M) ratio of 0.84,
an inclination of the lower incisors to the mandible of 83°
and a Holdaway angle of 3.5°.
Discriminate analysis has shown that Wits appraisal is most decisive in distinguishing camouflage treatment from surgical.
Average Wits for camouflage = -4.6±1.7mm
For surgical treatment it was = -12.1±4.3mm
(Eisenhauer AJODO 2002)
Musich (2007) : 3 categories
Green - Wits < 4mm (camouflage)
Yellow – Wits 4-8mm (borderline)
Red – Wits >12mm (definite surgical)
Rabie et al (2008) suggested that Holdaway angle can be a reliable guide.
The threshold value was 12°., a Holdaway angle of >12° can successfully be treated by camouflage.
Treatment of class III malocclusion
Treatment strategies for developing skeletal class III patients
Treatment modalities include:
Chin cup therapy
Functional appliance therapy
Maxillary protraction by conventional face mask therapy
Maxillary protraction by SAS
Treatment approach non growing class III patients
Camouflage with conventional fixed appliances
Camouflage with SAS
Orthognathic surgery
Chin Cup Therapy
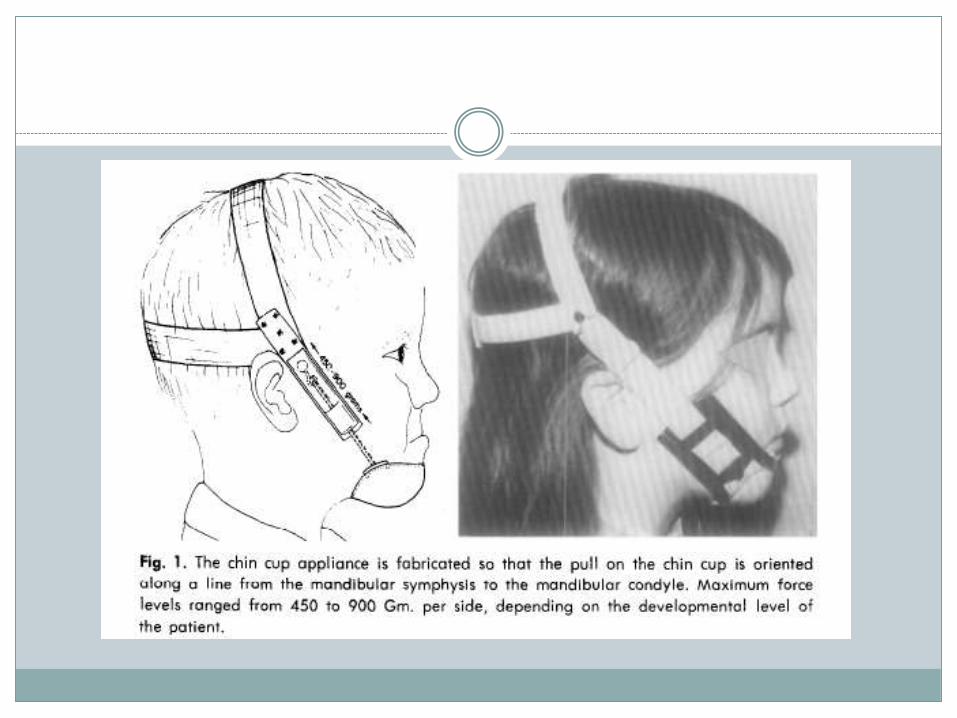
In the late 1940’s and early 1950’s after observation of the gross effects of Milwaukee brace treatment on the growth and form of the mandible, it was proposed that strong “orthopedic” forces in the range of 400 to 800 gm.
A chin cup or mental anchorage serves to redirect mandibular growth
Force Magnitude and Direction
Chin cups are divided into two types:
Occipital-pull chin cup that is used for patients with mandibular protrusion and
Vertical-pull chin cup that is used in patients presenting with a steep mandibular plane angle and excessive anterior facial height.
Most of the reported studies recommended an orthopedic force of 300 to 500 g per side.
Patients are instructed to wear the appliance 14 hr/day.
The orthopedic force is usually directed either through the condyle or below the condyle.
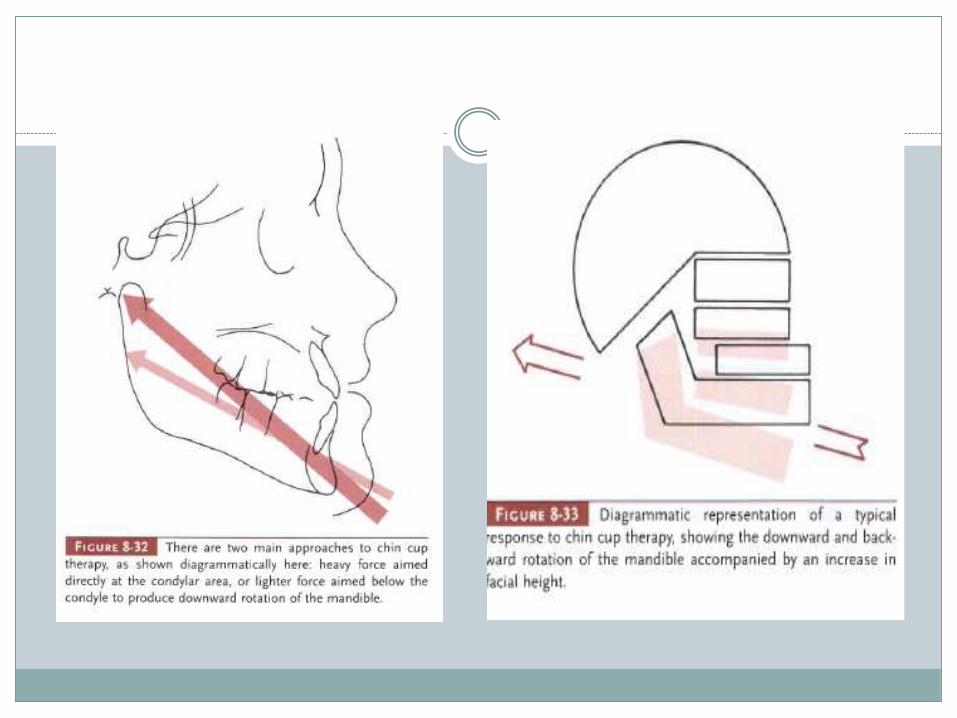
Effects of Chin Cup Therapy
Redirection of mandibular growth at the chin.
Backward repositioning of the mandible.
Retardation of mandibular growth at the condyle.
Remodeling of mandibular morphology at the gonialangle and symphysis.
Evidence exists that treatment to reduce mandibular protrusion is more successful when it is started in the primary or early mixed dentition.
The treatment time varies from 1 year to as long as 4 years depending on the severity of the original malocclusion.
Stability of Treatment The stability of chin cup treatment remains unclear. Several
investigators reported stability in horizontal maxillary and mandibular changes associated with chin cup treatment.
However, a few studies reported a tendency to return to the original growth pattern after the chin cup is discontinued.
Sugawara et al published a report on the long-term effects of chin cup therapy on three groups of Japanese girls who started chin cup treatment at 7, 9, and 11 years with serial lateral head films
The authors found that the skeletal profile was greatly improved during the initial stages of chin cup therapy, but these changes were often not maintained, due to catch-up mandibular displacement.
They concluded that chin cup therapy did not necessarily guarantee a positive correction of the skeletal profile after completion of growth, which suggests the need for the extended use of the chin cup over the growth period.
Chincap therapy is applicable when a growing patient has a true skeletal Class III malocclusion and a large mandible; lacks maxillary recession, an acute cranial base angle, a long-face syndrome, and symptoms of temporomandibular disorders; and orthognathic surgery is not an option.
Treatment must continue until growth has ceased to prevent redevelopment of the prognathic face after chincap therapy, and some overcorrection might be warranted
Hideo Mittani AJODO JUNE 2002
Functional appliances
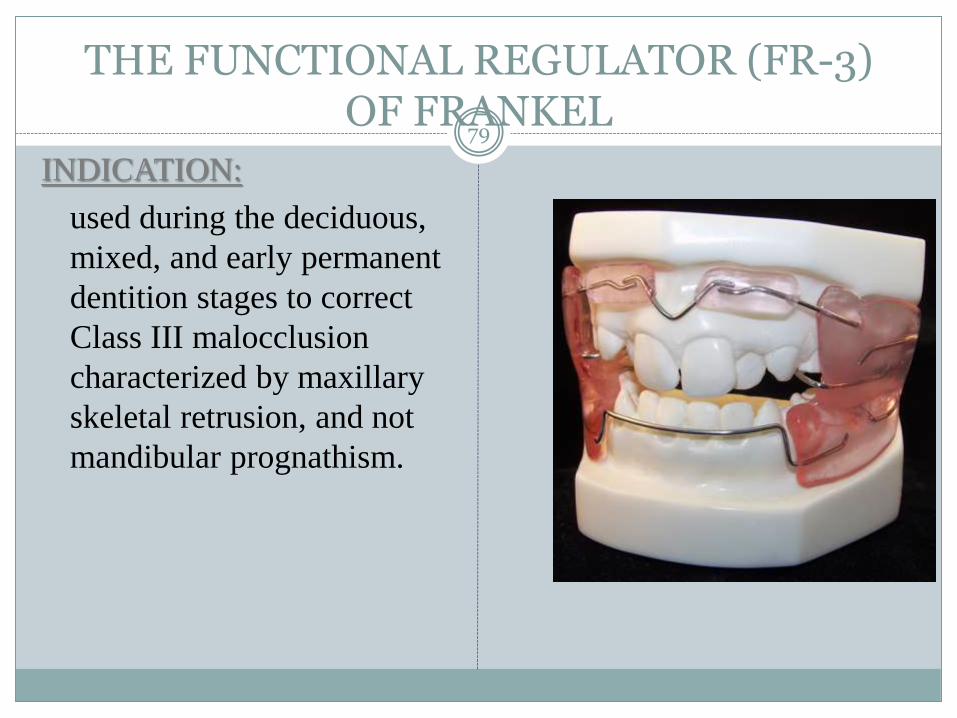
THE FUNCTIONAL REGULATOR (FR-3) OF FRANKEL
79
INDICATION:
used during the deciduous,
mixed, and early permanent
dentition stages to correct
Class III malocclusion
characterized by maxillary
skeletal retrusion, and not
mandibular prognathism.
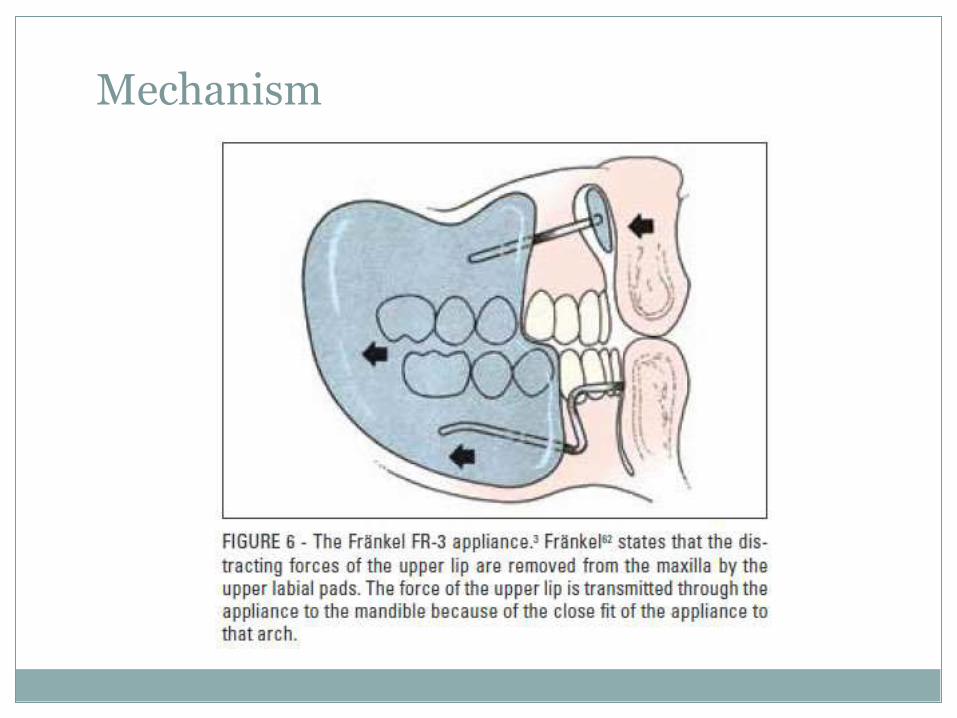
Mechanism
FR – 3 can also be used as a retainer after class III correction by protraction face mask (Petit) or orthognathic surgery (Eirew)
Bionator III appliance
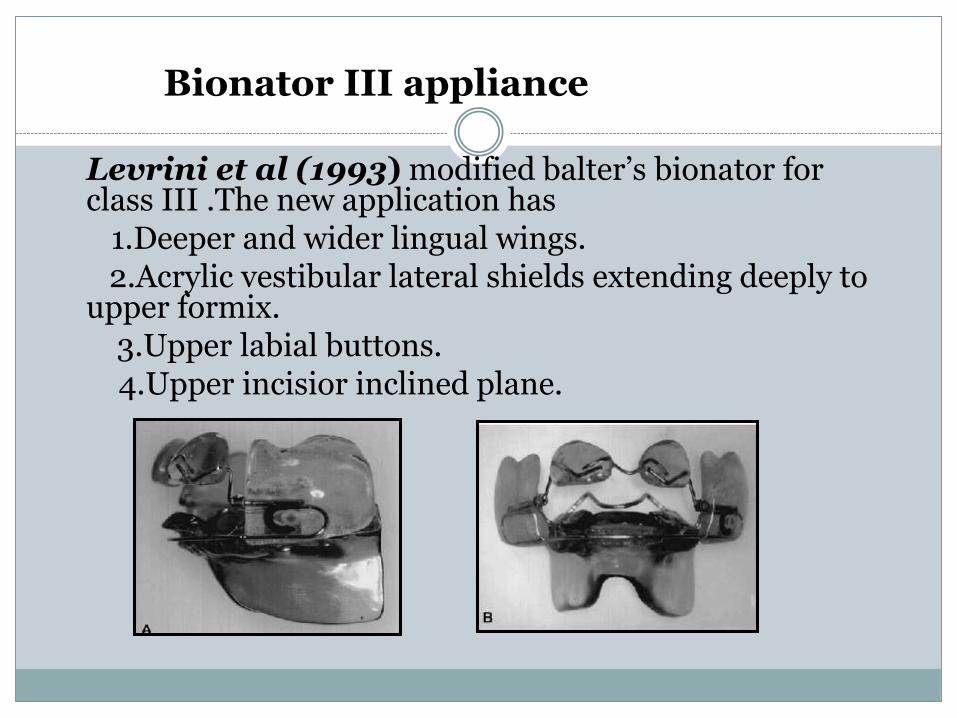
Levrini et al (1993) modified balter’s bionator for class III .The new application has
1.Deeper and wider lingual wings.2.Acrylic vestibular lateral shields extending deeply to
upper formix.3.Upper labial buttons.4.Upper incisior inclined plane.
According to Garrattini et al (AJO 1998)
bionator is an effective appliance in mid facial
deficiency especially with hypo divergent
growth pattern.
The control of mandibular growth is
unpredictable with this appliance. The
dentoalveolar chances exceeded the skeletal
effects of bionator III.
REVERSE TWIN BLOCK
84
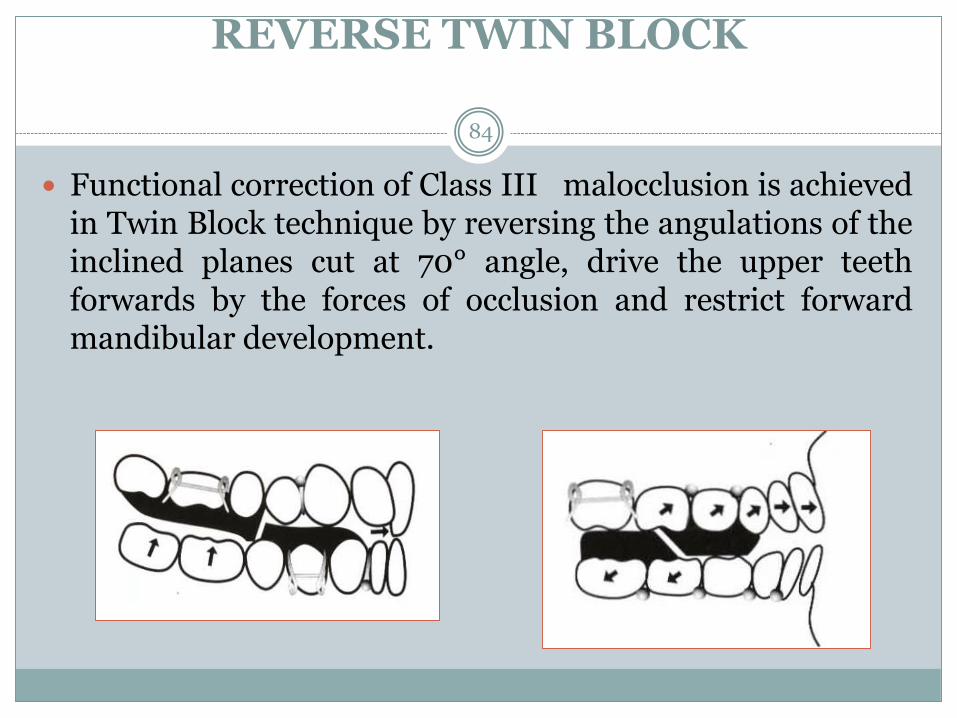
Functional correction of Class III malocclusion is achievedin Twin Block technique by reversing the angulations of theinclined planes cut at 70° angle, drive the upper teethforwards by the forces of occlusion and restrict forwardmandibular development.
85
Effects of RTB: (Kinder etal. JO.2003;30:197 201)
Mainly dentoalveolar.
Proclination of the maxillary incisors (mean: 5.1°)
Retroclination of the mandibular incisors (mean: 4.5°)
Downward and backward mandibular rotation.
Increase in lower facial height (mean: 1.75mm)
Reduction in mandibular prognathism (mean: −1.3°).
86
The average reported treatment time for these patients was 6.6 months—significantly shorter than the 3.1 years reported by Loh and Kerr with the use of a Function Regulator III appliance.
Treatment duration is usually 6-9 months.
RTB v/s Protraction facemask therapy87
A comparison of two different techniques for early correction of Class III malocclusion
(Seehraa etal. AO. 2012;82:96–101 )
Both appliances are capable of correction of Class III dental relationships; however, the relative skeletal and dental contributions differ. Skeletal effects, chiefly anterior maxillary translation, predominated with PFM therapy. The RTB appliance induced Class III correction, primarily as a result of dentoalveolareffects.
Protraction face mask
Initially in 1944 Oppenhim suggested moving the maxilla in an attempt to counterbalance mandibular protrusion.
Later Delaire in 1960’s revived the interest in use of protraction facemask which was further modified by Petit in 1983
Indications
Mild to moderate skeletal class III with retrusivemaxilla.
Hypodivergent growth pattern
Appliance design
The orthopedic face mask system has three basic components the facemask, maxillary splint, and elastic.
The Facemask: The protraction facemask is a one-piece construction consisting of a forehead pad , a chin pad connected with a heavy steel support rod and a adjustable anterior wire and hooks to accommodate a downward and forward pull of the maxilla with elastics
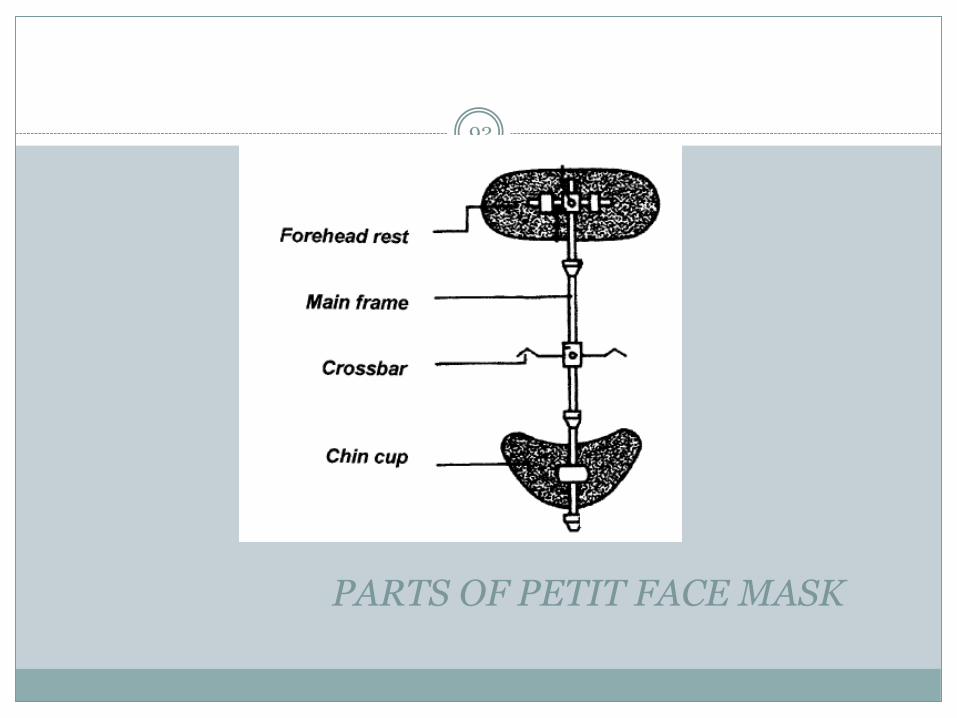
PARTS OF PETIT FACE MASK
92
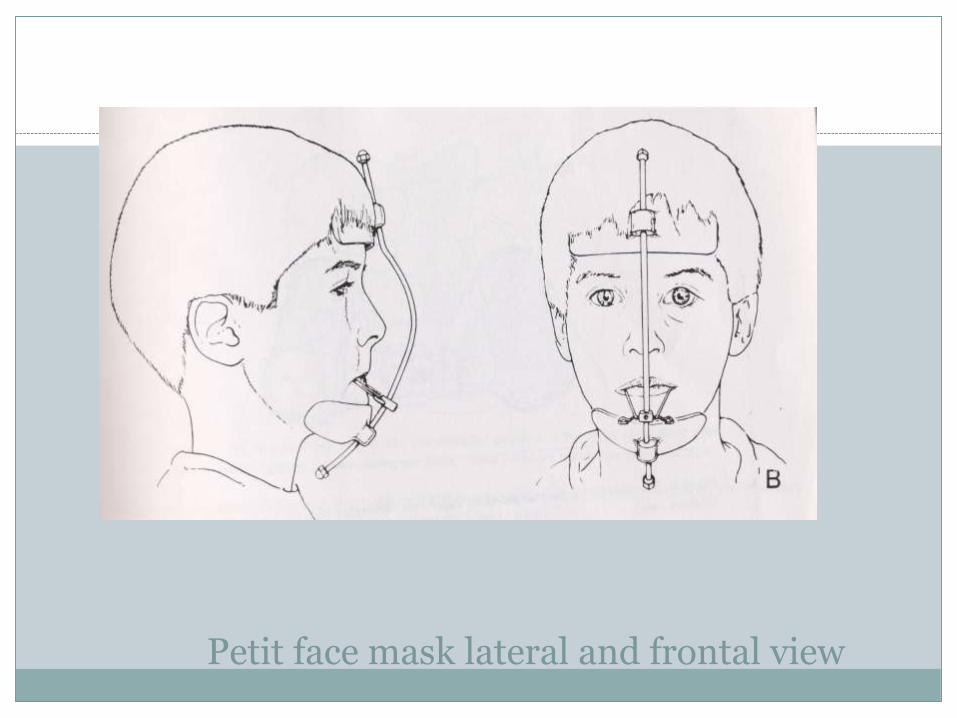
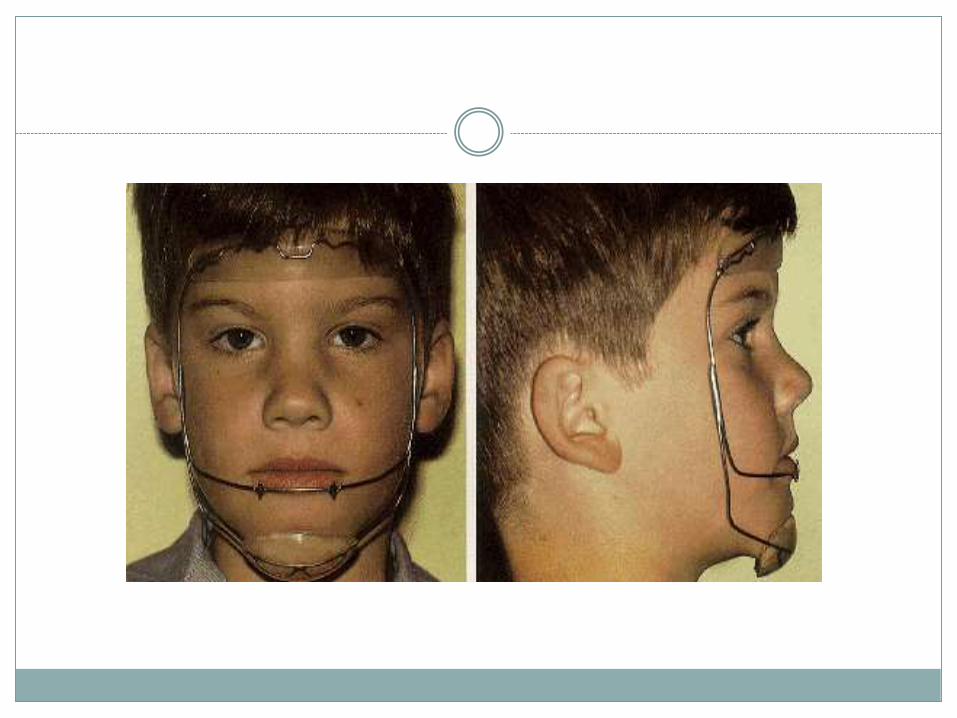
Petit face mask lateral and frontal view
93
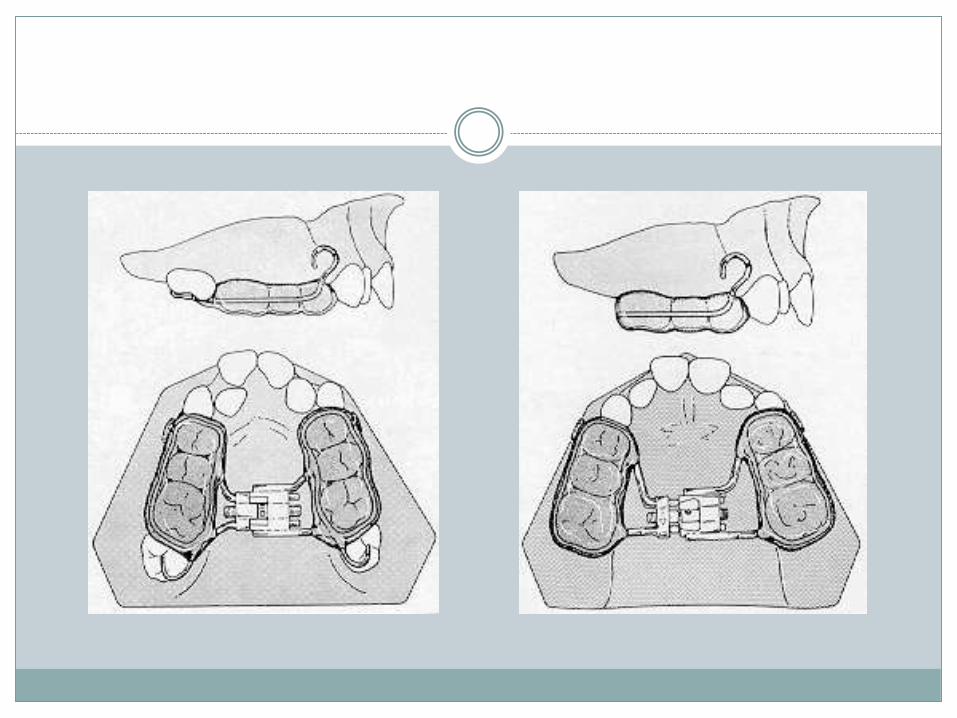
Maxillary splint:
The maxillary splint stabilizes the maxilla as a single unit.
In primary dentition it is advisable to use acrylic bonded palatal expansion appliance with 0.040’’ wire framework extending around the buccal and lingual surface of the dentition with hooks extending buccally at the level of the first deciduous molars for attachment of elastics
In mixed or early permanent dentition banded palatal expansion appliance is constructed with 0.045 inch wire extending bilaterally and hooks extending bucally in the canine region.
The splint is activated twice per day for 2 weeks or more depending on discrepancy
In patients whom no increase in transverse dimension is desired appliance is still activated for 8-10 days .
97
SEQUENCE OF ELASTICS:
Initially 3/8” 8 oz
After 2 weeks 1/2” 14 oz
Increased to a max of 5/16” 14 oz
Young patients (4-9) years should wear the mask on a full
time basis except during meals. Duration is 4-6 months.
They can be retained with only night time wear or with a
maintenance plate, chin cup or FR III. In older patients, it is
worn at all times except during school.
When is the best time to start protraction facemask treatment?
3/8/2015 3:04 PM
98
The optimal time to intervene a Class III malocclusion is at the time of the initial eruption of the maxillary incisors. (MacNamara)
A positive overjet and overbite at the end of the facemask treatment appears to maintain the anterior occlusion.
Biologically, the circummaxillary sutures are smooth and broad before age 8 and become more heavily interdigitated around puberty
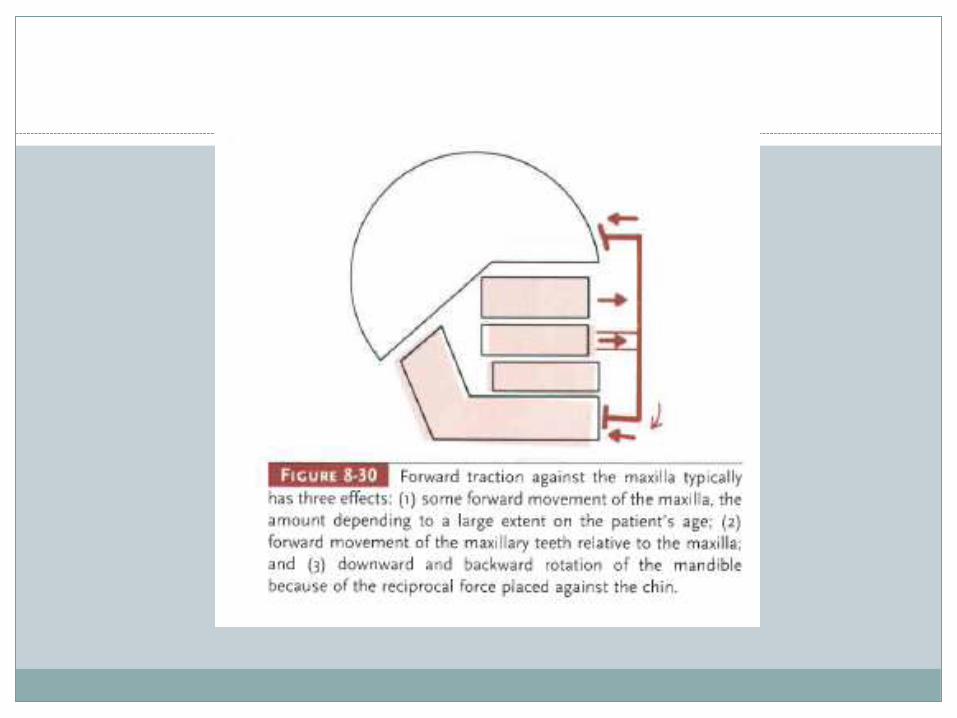
Treatment effect of protraction facemask
Maxillary forward displacement : increase in SNA angle.
Mandibular downward and backward rotation: decrease in SNB angle, increase in SN-MP angle .
Increase in anterior facial height .
Labial inclination of upper incisors .
Lingual inclination of lower incisors.
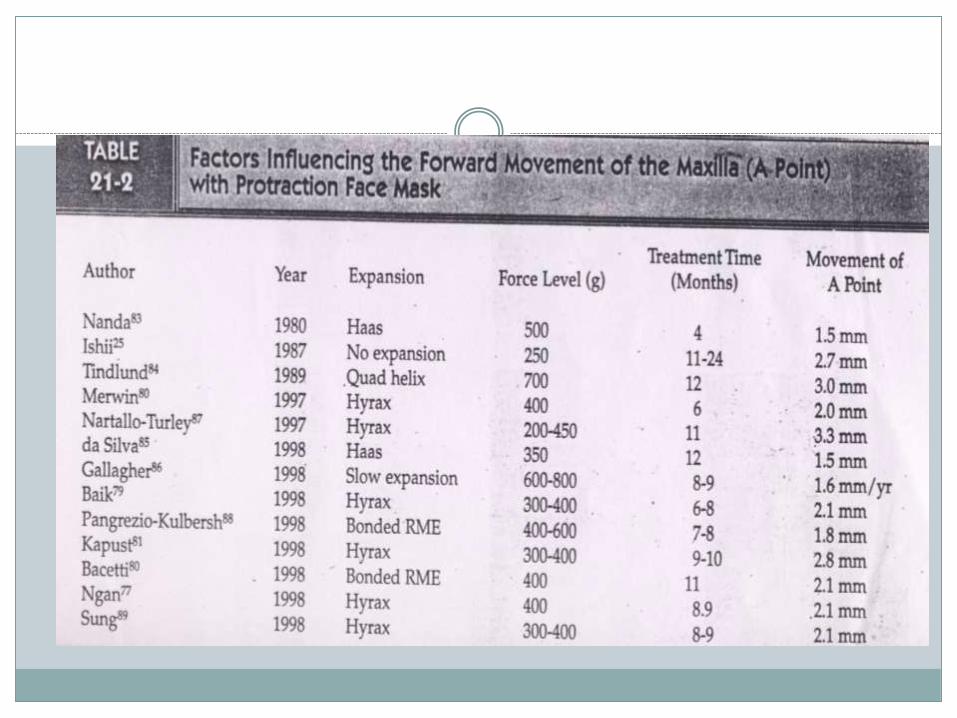
The following four components of force system are important for the protraction headgear:
The magnitude of force:
The force value used for maxillary protraction ranges from 200-800 gm.per side.
The sutural anatomy and the age of the patient play a major role in determining the amount of force needed to bring the maxilla forward with protraction force.
Preadolescent patient ( 4-8 years): 200-250 gm per side.
Early adolescent patient ( 8-11 years): 300-450 gm per side.
Late adolescent patient (>11 years ): 450-600 gm per side.
Direction and point of force application:
Nanda and Hickory speculated that the center of resistance of the mid face is 5-10 mm below the orbitaleon the zygomatic bone
Miki supported it with adding the vertical direction that it was between orbitale and distal root apex of maxillary first molar.
Hata et al and Lee et al reported that line of force 5mm above the palatal plane and 15 mm above occlusal plane did not result in counter clockwise rotation of maxilla
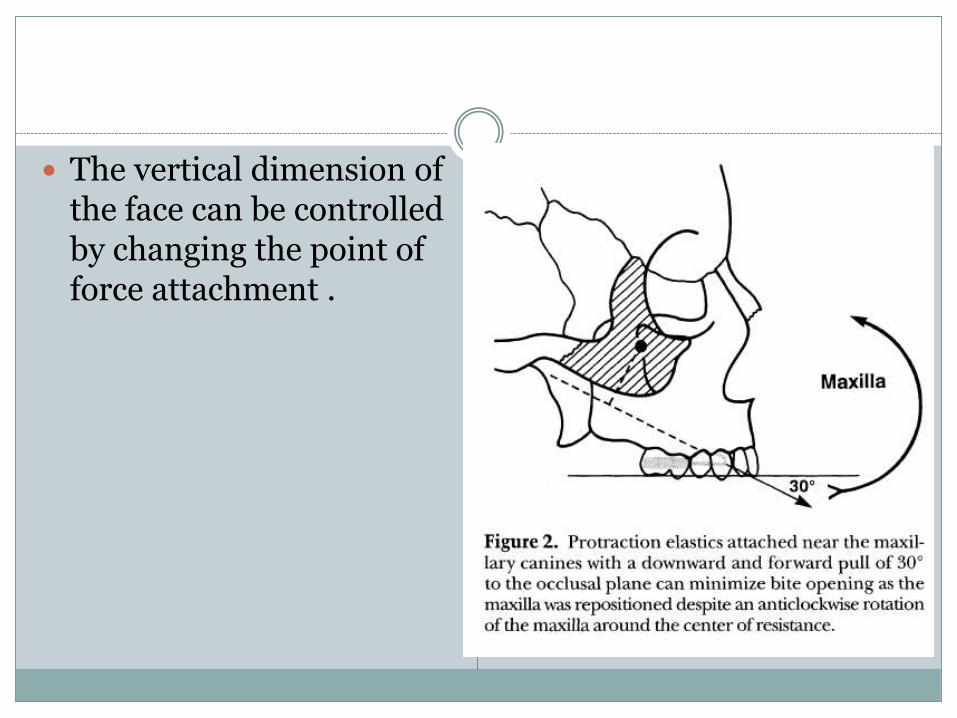
The vertical dimension of the face can be controlled by changing the point of force attachment .
Clinical response to maxillary protraction :
Total 3-16 month.
Anterior crossbite is corrected in 3-4 months while molar relation and overbite correction in additional 4-8 months
107
PROTRACTION WITH AND WITHOUT RME:
In patients whom no increase in transverse dimension is desired , the appliance should be still activated for 8 - 10 days to disrupt the maxillary sutural system and to promote maxillary protraction ( Hass ,1965)
Numerous authors have reported on the anterior constriction of the maxilla when it is protracted and emphasize the necessity of physically expanding the maxilla before protraction.
Palatal expansion alone has also been shown to facilitate correction of a Class III malocclusion by causing a downward and forward displacement of the maxilla.
Palatal expansion has been noted not only to affect the intermaxillary suture, but also all of the circum-maxillary articulations. It has also been suggested that palatal expansion ‘disarticulates’ the maxilla, initiating a cellular response which then allows a more positive reaction to protraction forces .
Baik et al (1997) found that forward movement of point A was more in exapansion group (2mm) than in labiolingual group (0.9mm)
Kim et al (1999) evaluated facemask therapy in a meta-analysis study and reported that the results of protraction with or without expansion were similar, but the average duration of treatment was longer in the nonexpansion group.
Vaughn et al (AJODO 2005) in a RCT study concluded that palatal expansion makes NO difference in the amount of anteroposterior skeletal change.
Turtop et al (SIO 2007) showed that skeletal change in both groups were same, but there was increased molar eruption in non expansion group.
Valiathan et al (AJODO 2009) in a finite element study showed that high stresses generated in various craniofacial sutures after maxillary protraction with expansion are responsible for disrupting the circummaxillary sutural system and presumably facilitating the orthopedic effect of the facemask.
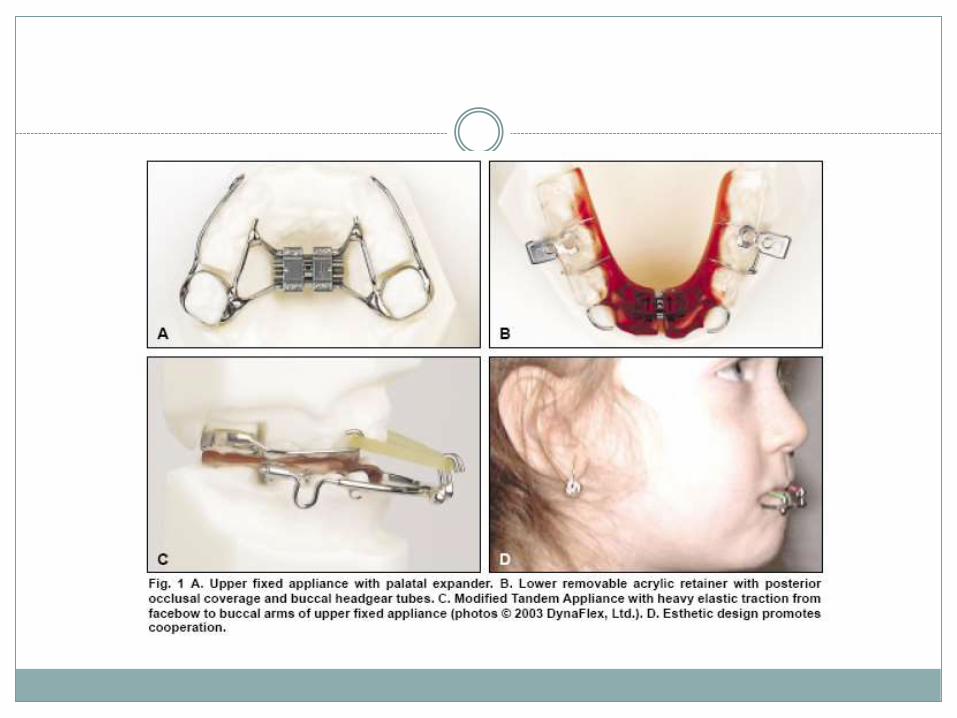
The Modified Tandem Appliance
Klempner [JCO2003]
Designed for Class III patients with skeletal midfacial deficiencies. The MTA has three components, one fixed and two removable.
The upper fixed appliance can be a traditional maxillary expander, with or without palatal acrylic. Soldered buccal arms are used for elastic traction.
Upper brackets can be added, depending on the patient’s age and clinical situation.
The lower appliance comprises a remov-able acrylic retainer with posterior occlusal coverage and buccal headgear tubes embedded in the area of the lower first molars
. An .045" headgear facebow with the outer bows bent out for elastic attachment is inserted into the lower tubes.
Advantages :
Promotes patient compliance, because it is more esthetic and comfortable than extraoral appliances.
Promotes good oral hygiene, because it is removable. Allows early treatment of any Class III malocclusion,due to
optimal retention in the decidu-ous,mixed, or early permanent dentition.
Distributes the force of protraction to all maxillary teeth. Permits free mandibular movement, with its polished
occlusal surface, so that a functional shift is easily corrected.
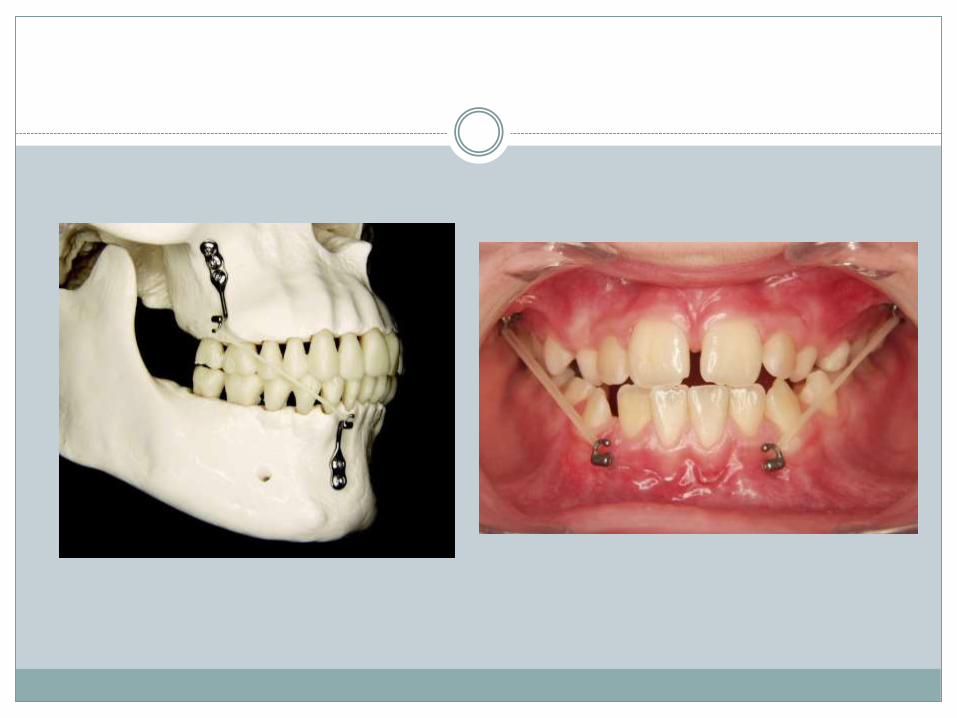
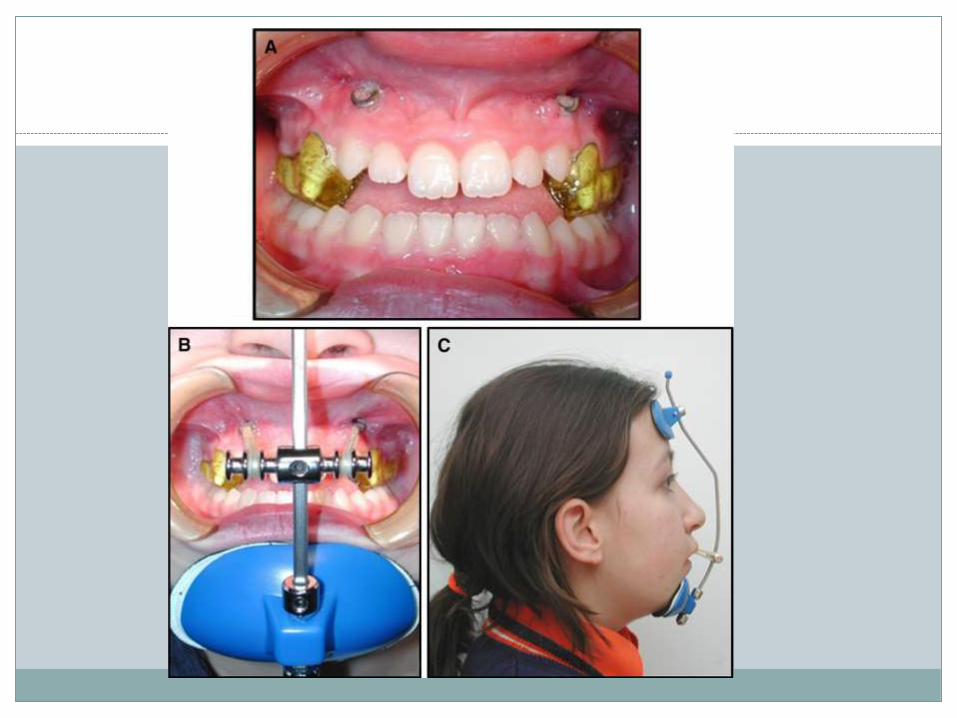
Protraction by skeletal anchored system
Two methods :
1. bone anchored intra oral class III elastics. (De Clerk et al 2009)
2. bone anchored face mask therapy (Cevidanes et al 2010)

ORTHODONTIC CAMOUFLAGE
Essentially two main approaches are used once the case is selected for camouflage.
1. Nonextraction approach
a) The MEAW technique
b) Lower arch Distalisation using TADs
2. Extraction approach
It is commonly believed that successful camouflage treatment for class III malocclusion can be achieved by :
proclination of maxillary incisors,
retrusion of mandibular incisors,
downward and backward rotation of mandible.
Distalisation of mandibular dentition
The multiloop edgewise archwire (MEAW, 0.016 ×0.022 Inch), multiple L-loops and tip-back bends, incorporated in the MEAW together with intermaxillary elastics can allow individual tooth movements and make it possible to upright posterior teeth, to change the inclination of the occlusal planes, to correct the occlusal sagittalrelationship, and to obtain the correct intercuspation
The use of MEAW requires completion of all alignment and levelling and constant use of vertical anterior elastics.
Studies suggest that improvement in molar relationship and overjet was achieved with upright and distal movement of the lower posterior teeth.
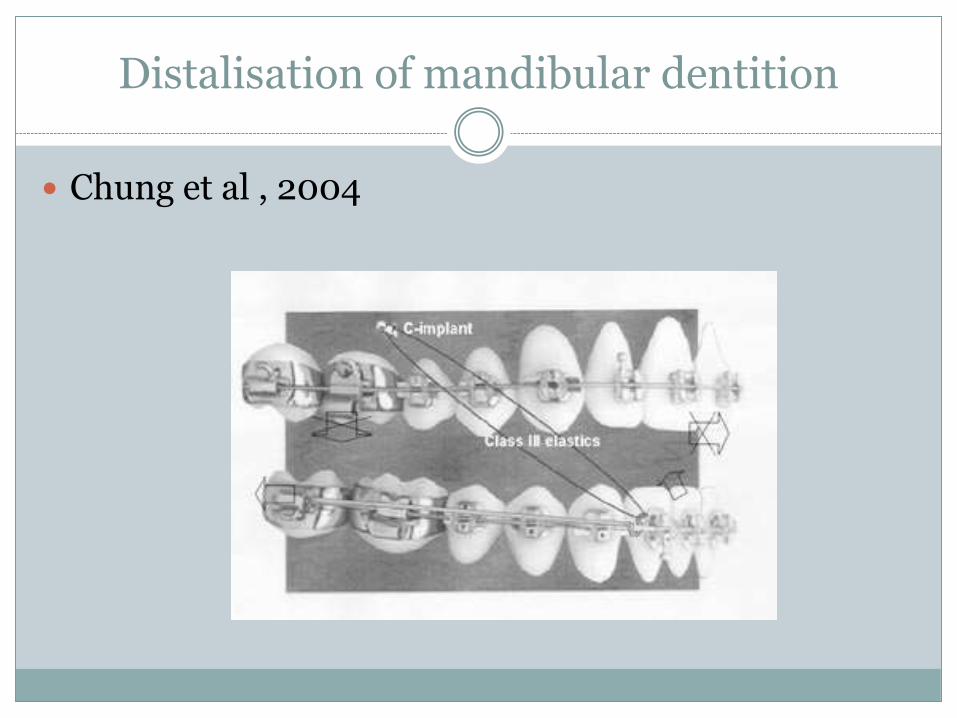
Distalisation of mandibular dentition
Chung et al , 2004
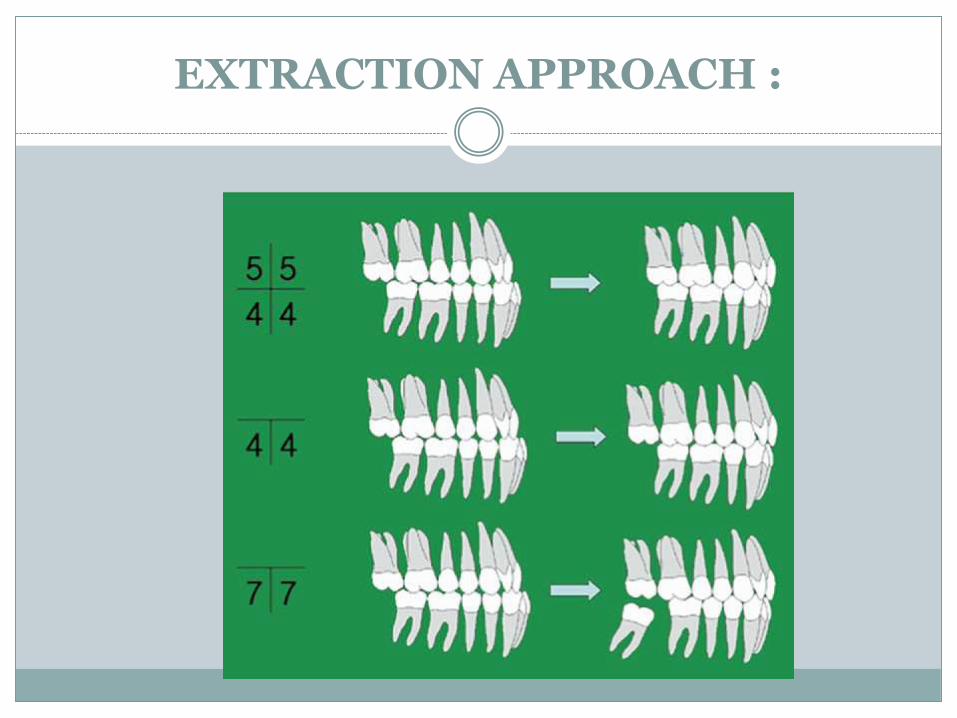
EXTRACTION APPROACH :
LIMITATIONS FOR INCISOR MOVEMENT BY CAMOUFLAGE : (Burns et al, 2010)
Upper incisor to SN – 120°
Lower incisor to MP - 80°
Orthognathic surgery
Ricketts described eight major characteristics of surgical class III case :
1. Open basion – nasion to FH plane angle (average 27°)
2. Closed Xi axis (average 15°)
3. Obtuse corpus condyle axis
4. Long condyle neck
5. Long corpus
6. Short porion distance from pterygoid vertical
7. Short anterior cranial length on basion – nasion
8. Concave profile
Retention of class III130
Class III malocclusion worsens with the continuing mandibular growth.
Relapse from continuing mandibular growth is likely to occur and such growth is extremely difficult to control.
Applying a restraining force to a mandible as from chin cap is not effective in controlling growth in a class III patient
In mild class III problems a functional appliance or a positioner may be enough to maintain the occlusal relationship during post treatment growth.
Bonded retainers in case of lower incisor extraction are generally required.
REFERENCES
Bishara SE. Textbook of orthodontics. Philadelphia: W.B. Saunders; 2001.
Peter Ngan ; Early “Timely” Orthodontic Treatment, SIO SEPTEMBER 2005 :VOL 11, NO 3
Guyer EC, Ellis EE, McNamara JA, et al. Components of Class III malocclusions in juveniles and adolescents. Angle Orthodontist 1986; 56: 7-30.
Tortop T, Keykubat A, Yuksel S. Facemask therapy with and without expansion. American Journal Orthodontics and DentofacialOrthopedics 2007,132: 467–474
Sugawara, J.; Asano, T.; Endo, N.; and Mitani, H.: Long-term effects of chincap therapy on skeletal profile in mandibular prognathism, Am. J. Orthod. 98:127-133, 1990.
Joondeph DR: Early orthodontic treatment. Am J Orthod Dentofacial Orthop 104:199-200, 1993
Rabie ABM, Wong RWK, Min GU. Treatment in borderline Class III malocclusion: orthodontic camouflage (extraction) versus orthognathic surgery. Open Dent J 2008;2:38-48.
Burns R et al. Class III camouflage treatment: What are the limits? Am J Orthod Dentofacial Orthop 2010;137:9.e1-9.e13
Ghiz M, Ngan P, Gunel E. Cephalometric variables to predict future success of early orthopedic Class III treatment. Am J Orthod Dentofacial Orthop 2005;127:301-6.
McNamara JA Jr, Brudon WL. Orthodontic and orthopedic treatment in the mixed dentition. Ann Arbor, Mich: Needham Press; 1993.
Litton SF, Ackermann LV, Isaacson RJ, et al: A genetic study of Class III malocclusion. Am J Orthod 58:565-577, 1970
Ngan P: Biomechanics of maxillary expansion and protraction in Class III patients. Am J Orthod Dentofacial Orthop 121:582-583, 2002
THANK YOU





























