Embed Size (px)
Citation preview

Moderator :Director & HOD
PROF.DR.K.PRAKASAM M.S.Ortho,D.Ortho,DSC (HON)
PRESENTOR:DR.THOUSEEF.A.MAJEED
M S Ortho PG
VMKVMCH Salem
CHONDROsARCOMA

• It is a malignant bone tumour of cartilageneous origin

• 9% of all primary malignancies of bone
• Primary chondrosarcoma - Between 40 and 60 years
• Secondary chondrosarcoma-Between 25 and 45
years

Classification
• PRIMARY CHONDROSARCOMA
• SECONDARY CHONDROSARCOMA

PRIMARY CHONDROSARCOMA
• Central (medullary)
• Intra cortical
• Clear cell
• Mesenchymal
• Dedifferentiated

SECONDARY CHONDROSARCOMA (from pre existing lesions)
• Multiple enchondromas & Exostosis
• Chondroblastoma
• Irradiation induced
• Fibrous dysplasia

Location
Types according to the site
• CENTRAL
• PERIPHERAL (surface type)

COMMON SITES
• Pelvis
• Proximal femur
• Proximal humerus.
• Ribs
• Rarely occur in the hand
• Incidence is higher among males

CLINICAL FEATURES
• A palpable mass with
increasing pain
• Hard in consistency with
lobulated surface
• Continuous with the bone
• slow growing .
• Mechanical restriction of joint
movements.
Secondary chondrosarcomas
• Arise at the site of a pre-existing benign cartilage
lesion.
• Most frequently in the enchondromas and
multiple hereditary exostoses.
INCIDENCE –
• 5% for patients with multiple hereditary exostoses
• Approximately 1% for patients with solitary
osteochondromas

RADIOLOGY
• It is arising in the medullary
cavity with irregular matrix
calcification.
• Calcification is a specific sign
• Gives a “punctate,”
“popcorn,” or “comma-
shaped.” calcification


• The size of the cartilaginous cap of an osteochondroma,
is to be evaluated with Computerised Tomography (CT-
Scan) or Magnetic resonance imaging (MRI).
• It is important in evaluating the possibility of a
secondary chondrosarcoma.

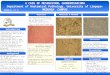
HISTOLOGY

CONVENTIONAL CHONDROSARCOMA
• Composed of malignant cells
with abundant cartilaginous
matrix.
• If malignant osteoid is present
the diagnosis should be
chondroblastic osteosarcoma

Diagnosing Factors that favor the malignant transformation
• Hypercellularity
• Plump nuclei
• More than occasional binucleate cells
• Entrapment of bony trabeculae.

Histological subtypes
• Clear cell chondrosarcoma
• Mesenchymal chondrosarcoma
• Dedifferentiated chondrosarcoma

Clear cell chondrosarcoma
• Low-grade malignancy.
• Round cells with abundant
clear cytoplasm
• Distinct cytoplasmic
borders with a background
of cartilaginous matrix.
• Multinucleated giant cells
are usually apparent.

• Clear cell Chondrosarcoma has a strong tendency to
arise in an epiphysis
• Benign radiographic features and can be confused with
chondroblastoma or giant cell tumor.

Mesenchymal chondrosarcoma
• High-grade tumor
• Small round blue cells
• Islands of benign-appearing
cartilage.
• The cellular portions have a
“Hemangiopericytomatous” pattern
of growth with “staghorn-like”
vessels.

Dedifferentiated chondrosarcoma
High-grade sarcoma
• ( Commonly osteosarcoma followed
in frequency by fibrosarcoma and
malignant fibrous histiocytoma)
• The radiography shows aggressive
radiolucent area

Teatment
Low-grade chondrosarcoma
• Extended curettage with the use of intraoperative
adjuvant treatments.

High-grade chondrosarcoma
• Wide or radical resection
• Amputation.

• The local recurrence rate after intraoperative
tumor contamination is high.
• For lesions in an expendable locations, Primary
wide resection without a biopsy may be
indicated
• It is to decrease the chance of tumor
contamination.

• After wide resection local recurrence is
less than 10%
• Pulmonary metastases Treated with
surgical resection if possible.

• Chemotherapy has no role in the treatment of
conventional chondrosarcoma
• Radiotherapy is used only as a palliative measure
for surgically inaccessible lesions.
Inaccessible areas include
• Tumour arising from floor of pelvis
Vertebrae &spinous process

PROGNOSIS
The prognosis depends on
• Size
• Grade
• Location of the lesion.
Low-grade lesions • Greater than 90% 10-year survival rate
High-grade conventional chondrosarcoma
• 20% to 40% 10-year survival rate

THANK YOU



![Chondrosarcoma of the Foot: A Rare Occurrence in the ... · chondrosarcoma, and mesenchymal chondrosarcoma [2]. Chondrosarcomas are most frequently found in men between the ages of](https://img.pdfslide.us/doc/110x75/5f3b1db0e636c85ef24c91bb/chondrosarcoma-of-the-foot-a-rare-occurrence-in-the-chondrosarcoma-and-mesenchymal.jpg)