Embed Size (px)
Citation preview

Template provided by: “posters4research.com”
METASTATIC CONVENTIONAL PRIMARY
CHONDROSARCOMA OF THE HYOID
Mary Ondinee U. Manalo, MD, Fellow-in-Training, Section of Medical Oncology, UP-Philippine General Hospital
Gracieux Y. Fernando, MD, Consultant, Section of Medical Oncology, UP-Philippine General Hospital
FIGURES
THE CASE
DISCUSSION
THE CASE INTRODUCTION
In conclusion, according to
the published clinical series,
head and neck CHS is usually a
low grade neoplasia with a high
propensity for local recurrences
that is commonly treated by
surgery alone. The case
reported in the present article
reveal a high grade tumor that
metastasized early in its clinical
course. Surgery was not an
option so palliative
chemotherapy was attempted
but was not successful.
Outcomes of CHS are
unpredictable, so strict follow-
up is required. //
CONCLUSION
Chondrosarcoma (CHS) is classified by the World
Health Organization as a malignant tumour
characterized by the formation of cartilage, but not of
bone, by tumour cells. Chondrosarcoma is the third
most common primary malignancy of bone after
myeloma and osteosarcoma. They are rare in the head
and neck region which accounts for less than 1 per
cent. Most chondrosarcomas of the head and neck
region occur in the maxilla; others are found in
descending order of frequency in the ramus, the body
of the mandible, the nasal septum, and the paranasal
sinuses.
The etiology of these tumours is unknown.
However, they are formed from cartilage in tissues not
normally harbouring cartilage or, secondly, from the
cartilage cap of exostosis or enchondromas. Vestigial
rests of multipotential differentiation of mesenchymal
cells may be the forerunner.
Chondrosarcomas of the head and neck have been
reported in patients ranging in age from 17 months to
75 years. The peak age of incidence is the third to the
sixth decade. There does not seem to be a sex
predilection. The tumours show a less aggressive
course when found in the long bones rather than when
found in the head and neck as the latter have a greater
rate of growth, recurrence, and metastasis. They
usually present as painless swellings.
Conventional radiographic findings are usually
not pathognomonic. Single or multiple lucencies with
poorly defined borders or bone destruction with
associated calcifications or ground-glass or sun-burst
appearance, and uniform widening of the periodontal
ligament (PDL) space, may occasionally be present.
However, contemporary imaging techniques like
computed tomography (CT) scan, magnetic resonance
imaging (MRI), and fluorine-18 fluorodeoxyglucose
positron emission tomography (FDG PET) are useful to
diagnose chondrosarcoma and to differentiate this
malignancy from its benign counterpart.
A 22-year old male from the Philippines had a
seven-month history of a fast-growing anterior neck
mass (Fig 1). Thinking that it was just goiter, he did not
seek consult until a few weeks prior to admission when
he developed difficulty in breathing and swallowing.
This progressed in severity and he was subsequently
rushed to the emergency room of the Philippine
General Hospital where he underwent emergency
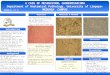
tracheostomy. On imaging, a heterogenous mass with
complex echoes measuring 24 x 13 x 12 cm on its
greatest diameter was seen on his neck with primary
destruction of the hyoid bone, encasing both the
internal carotids and the subclavian veins. Pulmonary
masses and nodules were seen bilaterally (Fig 2), the
largest of which measured 3.4 x 2.3 x 2.1 cm. Biopsy of
both the neck mass and the pulmonary mass revealed
grade III conventional chondrosarcoma (Fig 3).
Surgical resection was not attempted because the
mass encased major vessels and the defect will lead to
significant morbidity. Palliative chemotherapy using
single agent doxorubicin was given. The patient
received two cycles with no decrease in the size of his
neck mass. Prior to his third cycle, the neck mass
ulcerated and became infected. Due to meager
finances, he was not brought immediately for medical
consult until he developed high grade fevers and chills.
He was managed in a local hospital but he later
succumbed to septic shock. Wound and blood culture
isolated Burkholderia cepacia.
CHS is a slow growing malignant tumour with
hyaline cartilaginous differentiation, accounting for
approximately 20% of all malignant bone tumors. CHS
arising in the head and neck region is rare, accounting
only 0.1% of head and neck malignant tumours,
consequently, very few clinical series concerning the
clinicopathological features of head and neck CHS have
been published in the literature and most of them
comprise a small number of patients. In this paper, the
authors updated the review of Pontes. We reviewed all
the clinical series dealing with head and neck CHS,
summarizing the most important aspects found by each
author using PubMed and Medline.
In the review, these tumors present with a wide
range of clinical alterations, but a painless swelling is
the most common complaint. This is similar to the case
presently being reported. Microscopically, conventional
CHS constitutes the most common subtype, accounting
for approximately 90% of the cases, again was
consistent with the case being presented. The other
variants account for the remaining 10% and include
secondary, dedifferentiated, clear cell, and
mesenchymal chondrosarcomas.
The most common cause of death is related to
direct extension of the tumor to involve nearby
structures, since node and distant metastases are rarely
observed in head and neck CHS. Our patient died from
septic shock from the superimposed bacterial infection
on his necrotic tumor. We hypothesized that his tumor
probably developed necrosis that led to tumor rupture.
According to the observations in the clinical series,
when distant metastases develop, they are most likely
to be seen first in the lung. Computed incidence of
metastases is at 5.9%. In the case of the patient, when
he came to our Institution, he already had bilateral
pulmonary metastases.
Taking into account the overall biological behaviour
of head and neck CHS, the most effective treatment
modality for this neoplasia is aggressive surgery with
wide en-bloc resection. Irradiation and chemotherapy,
although variably used in cases of CHS, do not appear
to have a significant effect on survival and it is generally
accepted that these treatment modalities should be
used for palliative purpose.
According to the clinical series reviewed, the 5-year
survival rate for head and neck CSH varies between 32%
and 87.5%.
Fig 1. The patient with his rapidly enlarging
neck mass. He developed respiratory distress
and subsequently had a tracheostomy.
Fig 2. On metastatic workup, bilateral
pulmonary metastases were noted. This was
taken a week before tracheostomy.
Fig 3. Conventional chondrosarcoma on light
field microscopy.