Embed Size (px)
Citation preview
Child PsychiatryChild Psychiatry
A. AvramovaA. Avramova

MAJOR DEVELOPMENTAL STAGESMAJOR DEVELOPMENTAL STAGES
Prenatal/BirthPrenatal/BirthInfancy (Birth –18 months) Infancy (Birth –18 months)
TrustTrust - form attachment/bond - form attachment/bond (development of motor functions and speech) (development of motor functions and speech)
Toddler (1.5 - 3 years) Toddler (1.5 - 3 years)
AutonomyAutonomy - walk/talk/ Toilet Training / - walk/talk/ Toilet Training / tolerate separationtolerate separation
Early childhood (3-5 years) Early childhood (3-5 years) InitiativeInitiative - build vocabulary, build superego - build vocabulary, build superego (Dresses Self; Draws a person - main (Dresses Self; Draws a person - main
parts)parts)Middle childhood (6-12 years) Middle childhood (6-12 years)
IndustryIndustry - build peer-relations and competencies - build peer-relations and competenciesAdolescence (12-adult) Adolescence (12-adult)
Identity Identity issues issues
(Normal variation is present)(Normal variation is present)
Bio-psycho-social approach Bio-psycho-social approach
REASONS TO LEARN ABOUT REASONS TO LEARN ABOUT NORMAL DEVELOPMENTNORMAL DEVELOPMENT
To identify and be supportive of age-appropriate To identify and be supportive of age-appropriate skills and emotional expressions (e.g. skills and emotional expressions (e.g. expressions of autonomy; stranger anxiety) - expressions of autonomy; stranger anxiety) - these are healthy. these are healthy. To better identify what is really abnormal - so To better identify what is really abnormal - so treatment is focused on psychopathology.treatment is focused on psychopathology.To better understand common patterns of To better understand common patterns of regression (a return to earlier developmental regression (a return to earlier developmental behaviors) that may occur with illness or stress.behaviors) that may occur with illness or stress. To better understand adult psychopathology.To better understand adult psychopathology.

DISORDERS OF CHILDHOOD AND DISORDERS OF CHILDHOOD AND ADOLESCENCEADOLESCENCE
Epidemiology: 1 in 5 children involved (20% of children Epidemiology: 1 in 5 children involved (20% of children need at least once in their life consultation with child need at least once in their life consultation with child mental health professional)mental health professional)Specific disorders with childhood onset are listed Specific disorders with childhood onset are listed separately in ICD X, DSM-IV (ADHD, Conduct Disorder, separately in ICD X, DSM-IV (ADHD, Conduct Disorder, Learning Disorders, Mental Retardation, etc). These may Learning Disorders, Mental Retardation, etc). These may persist into adulthood.persist into adulthood.
Basically all adult disorders can occur in children and Basically all adult disorders can occur in children and adolescents (Depression, Bipolar, Schizophrenia, Anxiety adolescents (Depression, Bipolar, Schizophrenia, Anxiety disorders, etc.) at particular level of development.disorders, etc.) at particular level of development.
Personality Disorders (Axis II, DSM-IV) are usually not Personality Disorders (Axis II, DSM-IV) are usually not diagnosed, although personality traits are often diagnosed, although personality traits are often identified. identified. Comorbidity is common.Comorbidity is common.

EVALUATION STRATEGIESEVALUATION STRATEGIES
Patient InterviewPatient Interview
Collateral InformationCollateral Information Testing Testing (Parents, School)(Parents, School) (IQ, Education, Projective, (IQ, Education, Projective,
Personality, Neuropsych,Personality, Neuropsych, labs, EEG, MRI)labs, EEG, MRI)
ObservationObservation
Infants and toddlersInfants and toddlers(birth to 3y):(birth to 3y):
impairment of gross and fine motor functionsimpairment of gross and fine motor functions sleep and appetite disturbancessleep and appetite disturbances language and communication deficits language and communication deficits bonding and social behavior abnormalitiesbonding and social behavior abnormalities
Usual Concerns: Usual Concerns: • delayed development (e.g., MR), delayed development (e.g., MR), • abnormal development (e.g., PDD),abnormal development (e.g., PDD),• poor bonding (e.g., attachment disorder - neglect, poor bonding (e.g., attachment disorder - neglect, abuse)abuse)

observe milestonesobserve milestones
assess what child talks and thinks about (e.g. through play)assess what child talks and thinks about (e.g. through play)
parent-child relationparent-child relation
Preschoolers: Preschoolers:
Possible concerns: Possible concerns: as before, plus as before, plus speech-language delays, speech-language delays, hyperactivity,hyperactivity, difficult temperament, law frustration tolerance, self-regulation difficulties difficult temperament, law frustration tolerance, self-regulation difficulties excessive anxiety, shynessexcessive anxiety, shyness aggressive/defiant behaviors aggressive/defiant behaviors
how does child function in family?how does child function in family? how does child function in school? (behavior and academics)how does child function in school? (behavior and academics) what kind of peer relations?what kind of peer relations? formal psychological and academic testing formal psychological and academic testing
School-age childSchool-age child
Common concerns: Common concerns:
as before, plusas before, plus
learning problemslearning problems
externalizing conditions (hyperactivity disorders, behavioral and conduct disorders)externalizing conditions (hyperactivity disorders, behavioral and conduct disorders)
separation anxiety, obsessive compulsive disorder, tic disorders)separation anxiety, obsessive compulsive disorder, tic disorders)

AdolescentsAdolescents
early biological onsetearly biological onset later socio-economical independencylater socio-economical independency identity crisisidentity crisis authority crisisauthority crisis autonomyautonomy
unspecific problems:unspecific problems: school problems, school refusal, school failureschool problems, school refusal, school failure isolationisolation problematic peer relationships problematic peer relationships parent-adolescent relationship crisisparent-adolescent relationship crisis

Adolescents Adolescents
depressive disorders depressive disorders
risk behaviours (suicidal, self harming risk behaviours (suicidal, self harming behaviours)behaviours)
substance abusesubstance abuse
eating disorderseating disorders
personality disorderspersonality disorders
psychotic disorders (bipolar disorder, psychotic disorders (bipolar disorder, schizophrenia)schizophrenia)
MENTAL RETARDATIONMENTAL RETARDATIONIQ 70 or less on an individually administered IQ testIQ 70 or less on an individually administered IQ test
BORDRELINE intellectual functioning: IQ 71 to 85BORDRELINE intellectual functioning: IQ 71 to 85 MILD MR: IQ MILD MR: IQ 50/55 to 70; 50/55 to 70; mental age mental age 9 to under 129 to under 12 years years (~ 85%) (~ 85%)
May first be detected in school.May first be detected in school.
Social and Communication Skills: develop spontaneously.Social and Communication Skills: develop spontaneously.
May achieve autonomy.May achieve autonomy. MODERATE MR: IQ 35/40 to 50/MODERATE MR: IQ 35/40 to 50/55; 55; mental age mental age 6 to 96 to 9 years years (~ 10%) (~ 10%)
Social and Communication Skills: impaired.Social and Communication Skills: impaired.Early detection (i.e., before entering school).Early detection (i.e., before entering school).May work under close supervision (sheltered workshop)May work under close supervision (sheltered workshop)
SEVERE MR: IQ SEVERE MR: IQ 20/25 to 35/40; 20/25 to 35/40; mental age 3mental age 3 to 6 to 6 years years (~ 3%)(~ 3%)
Social/Communication Skills: little or no communicative speech, few Social/Communication Skills: little or no communicative speech, few words. words.
Often display poor motor development.Often display poor motor development.
May acquire elementary hygiene skills and perform simple tasksMay acquire elementary hygiene skills and perform simple tasks PROFOUND MR: IQ Below PROFOUND MR: IQ Below 20/25; 20/25; mental age below 3 yearsmental age below 3 years (~ 1-2%)(~ 1-2%)
Social and Communication Skills: rarely have communicative Social and Communication Skills: rarely have communicative speech efforts; minimal sensorimotor abilities.speech efforts; minimal sensorimotor abilities.Require constant aid and supervision; nursing care.Require constant aid and supervision; nursing care.

Onset before age 18 yearsOnset before age 18 years
Deficits or impairments in adaptive functioning in Deficits or impairments in adaptive functioning in at least two of these areas:at least two of these areas: communication, self care, home living, social and communication, self care, home living, social and
interpersonal skills, use of community resources, self interpersonal skills, use of community resources, self direction, functional academic skills, work, leisure, direction, functional academic skills, work, leisure, health, or safety.health, or safety.
Epidemiology: 1-3% Epidemiology: 1-3%
Causes: Causes: Unknown (50% of mild MR)Unknown (50% of mild MR) Known (75% of severe MR) – Hereditary (Down’s, Known (75% of severe MR) – Hereditary (Down’s,
fragile X); Toxins; Birth Trauma; Infection.fragile X); Toxins; Birth Trauma; Infection.
Pervasive Developmental DisorderPervasive Developmental Disorder
Developmental disorders with severe and Developmental disorders with severe and pervasive impairment in essential developmental pervasive impairment in essential developmental areasareas
Reciprocal social skillsReciprocal social skillsLanguage developmentLanguage developmentLimited range of behavioral repertoire Limited range of behavioral repertoire
Following disorders are included:Following disorders are included: AutismAutism Rett’s DisorderRett’s Disorder Childhood Disintegrative DisorderChildhood Disintegrative Disorder Asperger’s DisorderAsperger’s Disorder PDD, not otherwise specifiedPDD, not otherwise specified
60/10 00060/10 000 ? (1/166 – 1/80) ? (1/166 – 1/80)
AutismAutismOnset within first two yearsOnset within first two years
Autistic aloneness – inability to make warm Autistic aloneness – inability to make warm emotional relationships with peopleemotional relationships with people
Gaze avoidance, absence of eye to eye contact.Gaze avoidance, absence of eye to eye contact.
Speech and language disorder. Speech and language disorder. Speech develops late or never appear or Speech develops late or never appear or develops normally until about age of two years and develops normally until about age of two years and
then disappears in part or completely. then disappears in part or completely. echolalia, misuse of pronouns. echolalia, misuse of pronouns.
Non-verbal communication is affected as well.Non-verbal communication is affected as well.
Interest can be provoked by sensor Interest can be provoked by sensor stimulus - spinning toys, specific stimulus - spinning toys, specific shapes, sounds, lights. colors etc. shapes, sounds, lights. colors etc. 50 to 70% have some degree of MR50 to 70% have some degree of MRObsessive desire for sameness –Obsessive desire for sameness –repetitive games, same food and repetitive games, same food and clothes and etc.clothes and etc.Bizarre behaviour and mannerism – Bizarre behaviour and mannerism – play with fingers, flapping hands. play with fingers, flapping hands. Sudden anger or fear, smile without Sudden anger or fear, smile without apparent reason apparent reason
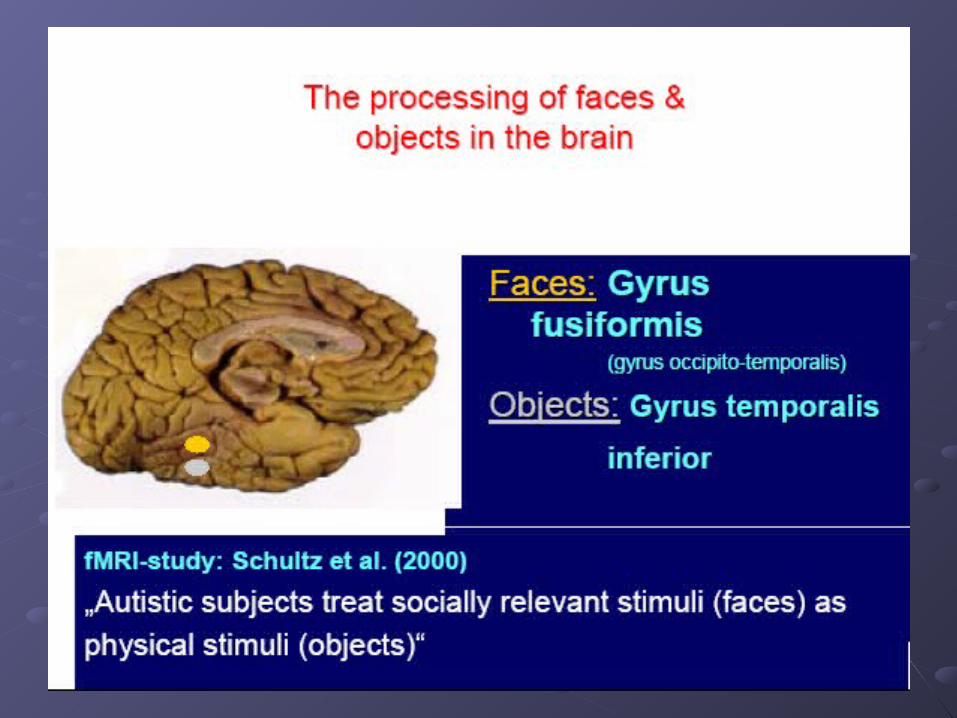

Theory of mind
Prevalence estimates: variable and Prevalence estimates: variable and increasing (increasing (2,5 2,5 -- 30,8/10 000, 10/10 000 30,8/10 000, 10/10 000 children)children)
Boys are effected 3 to 5 times more than Boys are effected 3 to 5 times more than girlsgirls
Associated with Tuberous Sclerosis, Associated with Tuberous Sclerosis, Fragile X SyndromeFragile X Syndrome
20 to 25% have grand-mal seizures and 20 to 25% have grand-mal seizures and about 50% have non-specific EEG about 50% have non-specific EEG abnormalitiesabnormalities
MRI, EEG, KaryotypingMRI, EEG, Karyotyping
INTERVENTIONS IN AUTISMINTERVENTIONS IN AUTISM
Presently no curative treatment available; Presently no curative treatment available; symptomatic interventions focus.symptomatic interventions focus.MainstayMainstay: Early intervention; speech and : Early intervention; speech and language services; structured behavioral language services; structured behavioral and educational programs.and educational programs.Family is coping with loss of “ideal” childFamily is coping with loss of “ideal” child
- Grief and loss issues.- Grief and loss issues.MedicationsMedications: To control seizures, severe : To control seizures, severe aggression, hyperactivity.aggression, hyperactivity.

Retts DisorderRetts DisorderNormal growth for the first few Normal growth for the first few months of lifemonths of lifeDeceleration of head growth Deceleration of head growth between 5-18 monthsbetween 5-18 monthsRegression – to the level of 8-Regression – to the level of 8-10m., profound impairment of 10m., profound impairment of socio-communicative and cognitive socio-communicative and cognitive abilitiesabilitiesImpairment of motor skills, Impairment of motor skills, coordination; impairment of jointscoordination; impairment of joints
Lack of purposeful hand Lack of purposeful hand movements; stereotypic movements; stereotypic movementsmovements
Disorder of femalesDisorder of femalesSimilar criteria as PDDSimilar criteria as PDDOver 80 percent of patients Over 80 percent of patients diagnosed with Rett's have a diagnosed with Rett's have a specific mutation in the MeCP2 specific mutation in the MeCP2 gene on the X chromosome. This gene on the X chromosome. This mutation is not inherited, but mutation is not inherited, but occurs after conception.occurs after conception.

Childhood Disintegrative Childhood Disintegrative DisorderDisorder
Normal Development for at least two years of life.Normal Development for at least two years of life.Clinically significant loss of previously acquired skills Clinically significant loss of previously acquired skills prior to age 10 years in two or more of the following prior to age 10 years in two or more of the following areas:areas:
LanguageLanguage Social skills or adoptive behaviorSocial skills or adoptive behavior Bowel or bladder controlBowel or bladder control PlayPlay Motor skillsMotor skills
Abnormal functioning in at least two areas:Abnormal functioning in at least two areas: Social interaction; communication; patterns of Social interaction; communication; patterns of
behaviors/interestsbehaviors/interests
0,1-0,6/10 0000,1-0,6/10 000
Asperger’s DisorderAsperger’s Disorder
““High functioning autism” – No delays in High functioning autism” – No delays in language and cognitive developmentlanguage and cognitive developmentLack of warmth and empathy, impaired Lack of warmth and empathy, impaired interpersonal relationsinterpersonal relationsImpaired use of non-verbal communication Impaired use of non-verbal communication (gaze, posture, gestures regulating social (gaze, posture, gestures regulating social interaction)interaction)Lack of interactive playLack of interactive playStereotypic, repetitive mannerismsStereotypic, repetitive mannerisms
2,5/10 0002,5/10 000
PDD NOSPDD NOS
Diagnosis assigned when there is Diagnosis assigned when there is a severe and pervasive impairment in a severe and pervasive impairment in
the development of reciprocal social the development of reciprocal social interaction, or communication skills, interaction, or communication skills,
or when stereotyped behaviors and or when stereotyped behaviors and activities are present activities are present
but the criteria are not met for a specific but the criteria are not met for a specific pervasive developmental disorder.pervasive developmental disorder.

New research:New research:Test, which uses magnetic resonance imaging (MRI) Test, which uses magnetic resonance imaging (MRI) to measure deviations in brain circuitryto measure deviations in brain circuitry Diffusion tensor imaging - measures white matter Diffusion tensor imaging - measures white matter microstructure by mapping directions of water diffusion microstructure by mapping directions of water diffusion in a local brain tissue in a local brain tissue Study of white matter microstructure in regions of the Study of white matter microstructure in regions of the brain responsible for language, emotion, and social brain responsible for language, emotion, and social cognition – focus on the superior temporal gyrus and cognition – focus on the superior temporal gyrus and temporal stem in 30 high-functioning males aged 7 to temporal stem in 30 high-functioning males aged 7 to 28 years who were diagnosed as having autism by the 28 years who were diagnosed as having autism by the standard subjective scoring system and in 30 matched standard subjective scoring system and in 30 matched controlscontrols 94% accuracy94% accuracy
Harvard University and University of UtahHarvard University and University of Utah Autism Autism Res. Res. November 29, 2010November 29, 2010
SPECIFIC LEARNING, MOTOR SKILLS AND SPECIFIC LEARNING, MOTOR SKILLS AND LANGUAGE DISORDERSLANGUAGE DISORDERS
Measured achievement in a specific (academic, motor, Measured achievement in a specific (academic, motor, speech) area is substantially below that expected based speech) area is substantially below that expected based on the age/IQ of the individual. This differs from MR on the age/IQ of the individual. This differs from MR where the deficits are global in nature.where the deficits are global in nature.Types:Types:
Receptive Language DisorderReceptive Language Disorder Expressive Language DisorderExpressive Language Disorder Mixed Receptive-Expressive Language DisorderMixed Receptive-Expressive Language Disorder Developmental Coordination DisorderDevelopmental Coordination Disorder
Reading Disorder (Dyslexia)Reading Disorder (Dyslexia) Mathematics Disorder (Dyscalculia)Mathematics Disorder (Dyscalculia) Disorder of Written Expression (Dysgraphia)Disorder of Written Expression (Dysgraphia)
ADHDADHD
Persistent pattern of inattention and/or hyperactivity more Persistent pattern of inattention and/or hyperactivity more frequent and severe than is typical of children at a similar frequent and severe than is typical of children at a similar level of development.level of development.Onset before age 7Onset before age 7Impairment in at least two settings: at home, at school, with Impairment in at least two settings: at home, at school, with friendsfriendsDuration at least six monthsDuration at least six monthsInattention, Hyperactivity, ImpulsivityInattention, Hyperactivity, Impulsivity
Types (DSMIV)Types (DSMIV)Predominantly Inattentive typePredominantly Inattentive typePredominantly Hyperactive typePredominantly Hyperactive typeCombined typeCombined type
Incidence: 2 to 20% of grade-school children Incidence: 2 to 20% of grade-school children Boys > Girls Ratio 3-5:1Boys > Girls Ratio 3-5:1
EtiologyEtiology
Specific Specific etiologyetiology unknown; unknown;
Contributory factors:Contributory factors: GeneticsGenetics Pre and perinatal complicationsPre and perinatal complications Neurological Neurological Environmental toxinsEnvironmental toxins
Psychosocial correlates include: poverty, Psychosocial correlates include: poverty, dysfunctional familydysfunctional family,, parental psychiatric parental psychiatric disorder, living in the city environment. disorder, living in the city environment.
Interventions – Interventions – Multimodality treatment programsMultimodality treatment programs
Environmental structuring; parental education Environmental structuring; parental education and trainingand training
Behavioral modifications; social skills trainingBehavioral modifications; social skills training
Pharmacotherapy Pharmacotherapy Stimulants: Methylphenidate, Dextroamphetamine, Stimulants: Methylphenidate, Dextroamphetamine,
(Pemoline)(Pemoline) Non-Stimulants: Clonidine and Bupropion; Non-Stimulants: Clonidine and Bupropion; atypical antipsychotics for treatment unresponsive atypical antipsychotics for treatment unresponsive
casescases
Disinhibited attachment disorderDisinhibited attachment disorder
AArises during the first five years of life rises during the first five years of life TTends to persist despite marked changes in ends to persist despite marked changes in environmental circumstancesenvironmental circumstancesDDiffuse, nonselectively focused attachment iffuse, nonselectively focused attachment behaviour, attention-seeking and indiscriminately behaviour, attention-seeking and indiscriminately friendly behaviour, poorly modulated peer friendly behaviour, poorly modulated peer interactions; depending on circumstances there interactions; depending on circumstances there may also be associated emotional or may also be associated emotional or behavioural disturbance.behavioural disturbance. IInstitutional syndromenstitutional syndrome. Adoptive children.. Adoptive children.

Reactive attachment disorderReactive attachment disorder
Starts in the first five years of life Starts in the first five years of life PPersistent abnormalities in the child's pattern of ersistent abnormalities in the child's pattern of social relationships that are associated with social relationships that are associated with emotional disturbance and are reactive to emotional disturbance and are reactive to changes in environmental circumstances changes in environmental circumstances FFearfulness and hypervigilance, poor social earfulness and hypervigilance, poor social interaction with peers, aggression towards self interaction with peers, aggression towards self and others, misery, and growth failure in some and others, misery, and growth failure in some cases. cases. The syndrome probably occurs as a direct result The syndrome probably occurs as a direct result of severe parental neglect, abuse, or serious of severe parental neglect, abuse, or serious mishandling.mishandling.

Conduct DisorderConduct Disorder
Characterized by severe and persistent Characterized by severe and persistent antisocial behaviour. antisocial behaviour. Largest group of psychiatric disorders in older Largest group of psychiatric disorders in older children and adolescents. children and adolescents. Prevalence 3 – 6%, more common in boys.Prevalence 3 – 6%, more common in boys.Characteristics:Characteristics: Serious violation of rules Serious violation of rules Destruction of propertyDestruction of property Deceitfulness or theftDeceitfulness or theft Aggression to people and animalsAggression to people and animals
Oppositional Defiant DisorderOppositional Defiant Disorder
Young childrenYoung childrenRecurrent pattern of negativistic, defiant, disobedient & Recurrent pattern of negativistic, defiant, disobedient & hostile behavior towards authority figureshostile behavior towards authority figuresDDoes not include delinquent acts or the more extreme oes not include delinquent acts or the more extreme forms of aggressive or dissocial behaviourforms of aggressive or dissocial behaviour Duration > 6 MonthsDuration > 6 MonthsImpairment in social, academic and work settingsImpairment in social, academic and work settingsSymptoms not part of the mood or thought disorderSymptoms not part of the mood or thought disorder
Multimodality treatment programs: Multimodality treatment programs: Environmental structuring; Family Therapy; Group Environmental structuring; Family Therapy; Group Therapy; Ind. Therapy – problem solving skills; Therapy; Ind. Therapy – problem solving skills; Medications as adjunctsMedications as adjuncts

ANXIETY DISORDERSANXIETY DISORDERS
Common in childhood: 15%Common in childhood: 15%
Comorbidity is commonComorbidity is common
All adult anxiety disorders may be seen in All adult anxiety disorders may be seen in children.children.
PTSD - may be a result of abusePTSD - may be a result of abuse
Separation Anxiety DisorderSeparation Anxiety Disorder
Separation anxiety disorderSeparation anxiety disorder
developmentally inappropriate and excessive anxiety developmentally inappropriate and excessive anxiety about separation from caretakers or home, of at least 4 about separation from caretakers or home, of at least 4 weeks weeks first first difficulties occurdifficulties occur during the early years of childhood during the early years of childhood (with onset before 18 years)(with onset before 18 years). . iit is differentiated from normal separation anxiety when it t is differentiated from normal separation anxiety when it is of ais of ann unusual degree (severity) unusual degree (severity) andand persistence persistence beyond the usual age period, and when it is associated beyond the usual age period, and when it is associated with significant problems in social functioning.with significant problems in social functioning.associated with physical complaints, fear of sleeping associated with physical complaints, fear of sleeping alone, worries about parent’s safetyalone, worries about parent’s safetycan lead to school refusal (school phobia)can lead to school refusal (school phobia)
Phobic anxiety disorderPhobic anxiety disorder
Fears in childhood that show a marked Fears in childhood that show a marked developmental phase specificity and arise developmental phase specificity and arise (to some extent) in a majority of children, (to some extent) in a majority of children, but that are abnormal in degree. but that are abnormal in degree. Other fears that arise in childhood but that Other fears that arise in childhood but that are not a normal part of psychosocial are not a normal part of psychosocial development (for example agoraphobia) development (for example agoraphobia) should be coded under the appropriate should be coded under the appropriate category in section F40-F48.category in section F40-F48.

Social anxiety disorderSocial anxiety disorder
In this disorder there is a wariness of In this disorder there is a wariness of strangers and social apprehension or strangers and social apprehension or anxiety when encountering new, strange, anxiety when encountering new, strange, or socially threatening situations. or socially threatening situations. This category should be used only where This category should be used only where such fears arise during the early years, such fears arise during the early years, and are both unusual in degree and and are both unusual in degree and accompanied by problems in social accompanied by problems in social functioning.functioning.

Sibling rivalry disorderSibling rivalry disorder
Some degree of emotional disturbance Some degree of emotional disturbance usually following the birth of an usually following the birth of an immediately younger sibling is shown by a immediately younger sibling is shown by a majority of young children. majority of young children. A sibling rivalry disorder should be A sibling rivalry disorder should be diagnosed only if the degree or diagnosed only if the degree or persistence of the disturbance is both persistence of the disturbance is both statistically unusual and associated with statistically unusual and associated with abnormalities of social interaction.abnormalities of social interaction.
Mood DisordersMood Disorders
Childhood DepressionChildhood Depression irritabilityirritability sleep cycle disturbancesleep cycle disturbance oppositional behavioroppositional behavior social isolationsocial isolation crying spellscrying spells
Dysthymia – symptoms last at least 1 yearDysthymia – symptoms last at least 1 year

PROTECTIVE FACTORSPROTECTIVE FACTORS
Good parent-child relationshipGood parent-child relationship Easy, outgoing temperamentEasy, outgoing temperament Positive peer influencePositive peer influence Successful school experiencesSuccessful school experiences Caring adult role modelsCaring adult role models Participation in pro-social groupsParticipation in pro-social groups Access to needed services, e.g. healthcare, Access to needed services, e.g. healthcare,
mental health, crisis interventionmental health, crisis intervention


![CSCU Psychology Transfer Pathway - ct Pathway Documents.2017.… · 41 PSY 205, 206, 207 (Adolesc Dev) PSY 363 (Adol Psy) [PSY Elective #2] 42 PSY 208 (Adult Dev) PSY 364 (Adult Dev)](https://img.pdfslide.us/doc/110x75/5fd698b16564d4287628efd2/cscu-psychology-transfer-pathway-ct-pathway-documents2017-41-psy-205-206.jpg)