Embed Size (px)
DESCRIPTION
cerebellum tract.puduncle .connection ataxia
Citation preview


Ataxia is a syndrome of imbalance and incoordination involving gait, limbs, and speech
Disorder of the cerebellum and/or its connections
Derived from the Greek word taxis, meaning “order” Approach to ataxia involves differentiating ataxia from other sources of imbalance and incoordination
Ataxia

Ataxic gait and position: Ataxic gait and position: Left cerebellar tumorLeft cerebellar tumor
a. Sways to the right ina. Sways to the right in standing positionstanding position
b. Steady on the b. Steady on the right legright leg
c. Unsteady on the c. Unsteady on the left legleft leg
d. ataxic gaitd. ataxic gait



1. HEMISPHERES - Appendicular coordination
2. VERMIS - Gait & other axial functions
3. FLOCCULO- NODULAR/ VESTIBULO CEREBELLUM - Eye movements & gross balance & gross orientation like up and down



Inferior cerebellar peduncle contains fiber from spinal cord (dorsal spinocerebellar tracts and cuneocerebellar tract and lower brain stem (olivocerebellar fibers from inferior olivary nuclei,give rise to climbing fibers within cerebellar cortex
Inferior cerebellar peduncle also contains inputs from the vestibular nuclei and nerve and efferents to the vestibular nuclei

Middle cerebellar peduncle consists fibers from C/L pontine
nuclei. These nuclei receive input from areas of the cerebral
cortex
Superior cerebellar peduncle, composed mostly of efferent
fibers, contains axons that send impulses to both the thalamus
and spinal cord, with relays in the red nuclei. Afferent fibers from
the ventral spinocerebellar tract also enter the cerebellum via this
peduncle


ARCHICEREBELLUM/ FLOCCULO NODULAR/ VESTIBULO CERELLUM
- Eye movements, gross balance and orientation - Inferior cerebellar pudenclePALLEOCEREBELLUM/ SPINOCEREBELLUM/
VERMIS & PAR VERMIAN REGION - Posture, Muscle tone, Axial muscle control, Locomotion - Inferior/ middle/ superior pudencleNEOCEREBELLUM/ CELEBELLAR HEMISPHERES/
PONTO CEREBELLUM - Coordinating movements, Fine motor control - middle/ superior pudencle


Motor coordination required
1. sensory input from muscles and joints
2.motor output from the cortex and basal ganglia via the efferentmotor tracts, including the lower motor neuron
3. modulating control from the cerebellum
4. vestibular system


Afferent ataxia due to loss of proprioceptive sensory feedback during movement and stance, loss of function of muscle spindles
Pathology of afferent ataxia
Peripheral nerves, dorsal root ganglia, and spinal cord
Afferent ataxia distinguished from cerebellar ataxia
(1) heavy dependence on visual guidance (2) the minor degree of oculomotor deficits (3) the absence of dysarthria
Afferent ataxia mostely associated with impaired tendon reflexes and sensory deficits
Afferent Ataxia

Acquired Sensory Neuropathies Causing Afferent Ataxia
b Miller Fisher syndromeb Chronic inflammatory demyelinating polyneuropathyb Diabetic polyneuropathyb CANOMAD (chronic ataxic neuropathy, ophthalmoplegia, monoclonal IgM protein, cold agglutinins and disialosyl antibodies) syndromeb AntiYmyelin-associated glycoprotein (MAG) antibodiesb Vitamin E deficiencyb Chemotherapy-induced polyneuropathies (cisplatin, carboplatin, oxaliplatin, doxorubicin)

Psychogenic Ataxia
Psychogenic ataxia should be suspected
Presence of unusual, bizarre clinical features, which may correct when attention is manipulated
Onset is abrupt and spontaneous remissions

Clinical Approach
• Is ataxia the problem (in contrast to other causes forincoordination)?
• Is cerebellar dysfunction related to the medial structuresor a hemispheral lesion?
• Are we dealing with “pure” ataxia, or is there evidencefor other system involvement?
• What is the time course of symptoms?

Clinical Differences Between Basic Types of Ataxia

Symptoms of Ataxia
Gait Disturbances
The initial symptoms sense of insecurity while walking, especially when require more skill, such as turning or balancing on a narrow base
Even before gait becomes abnormal, patients may note problems with specialized skills such as skiing, bicycling, or climbing
Patients and family notice that the patient feels more secure with the feet progressively apart

Limb AtaxiaAtaxia cause symptoms in the upper limbs, resulting from incoordination and tremor
Patients have clumsiness with activities such as writing, picking up objects, and buttoning
Movements become slower
Truncal Ataxia
Midline cerebellar lesions cause truncal ataxia
Patients experience head tremor and truncal instability leading to oscillatory movements of the head and trunk while sitting or standing (titubation)

Dysarthria and Bulbar SymptomsCerebellar ataxia cause slurred speech and abnormalities of pitch and volume control (scanning speech)Dysphagia result from incoordination of swallowing muscles, and patients report strangling and choking Visual SymptomsPatients experience blurriness or a sense of environmental movements as a result of cerebellar ocular oscillations associated with cerebellar disease
Symptoms in Sensory AtaxiaPatients with sensory ataxia usually not experience dysarthria or visual symptomsThey may have paresthesias and numbness

Stance and Gait
Cerebellar disease initially had body sway when the feet are placed together; the trunk moves excessively in the sideways direction (lateropulsion)
Healthy persons have foot spread of <12 cm during normal stance
Cerebellar disease have a much larger foot spread during quiet stance
Romberg test positive in cerebellar ataxia, although this more prominent in patients with proprioceptive or vestibular lesions
The speed of movements is not severely impaired, though patients deliberately slow down to keep their balance

Diagnostic Approach to Ataxia
Acquired Causes of Ataxia
Genetic Causes of Ataxia
Ataxia Related to Age at Onset
Ataxia Based on Onset and Course
Ataxias That Are Primarily Cerebellar, Cerebellar and Sensory, Primarily Sensory, and Associated with Spasticity
Noncerebellar Neurological Signs or Symptoms

Acquired Cause of AtaxiaCongenital: “ataxic” cerebral palsy, other early insults
Vascular: ischemic stroke, hemorrhagic stroke, AVMs
Infectious: acute cerebellitis, postinfectious encephalomyelitis, cerebellar abscess, Whipple disease, HIV, CJD
Toxic: alcohol, anticonvulsants, mercury, 5FU, cytosine arabinoside, lithium
Neoplastic/compressive: gliomas, ependymomas, meningiomas, basal meningeal carcinomatosis, craniovertebral junction abnormalities
Immune: MS, paraneoplastic syndromes, anti-GAD, gluten ataxia
Deficiency: hypothyroidism, vitamin B1 and B12, vitamin E

Genetic Causes of Ataxia
Autosomal recessive: FA, AT, AVED, AOA 1, AOA 2, MIRAS, ARSACS
Autosomal dominant: SCA types 1 through 31, episodic ataxias (types 1, 2, others)
X-linked, including fragile X tremor-ataxia syndrome (FXTAS)
Mitochondrial: NARP, MELAS, MERRF, others including Kearns-Sayre syndrome

Causes of Ataxia Related to Age at OnsetAge at Onset Acquired Genetic
Infancy Ataxic cerebral palsy, other intrauterine insultsInherited congenital ataxias (Joubert, Gillespie)
Childhood
Acute cerebellitis; cerebellar abscess; posterior fossa tumors such as ependymomas, gliomas; AVM; congenital anomalies such as Arnold-Chiari malformation; toxic such as due to anticonvulsants; immune related to neoplasms (opsoclonus-myoclonus)
FA; other recessive ataxias; EA ; mitochondrial; SCAs such as SCA 2, SCA 7, SCA 13, DRPLA
Young adult
Abscesses; HIV; mass lesions such as meningiomas, gliomas, AVM; immune such as MS; Arnold-Chiari malformation; hypothyroidism; toxic such as alcohol and anticonvulsants
FA; SCAs, von Hippel-Lindau syndrome
Older adultSame as above plus “idiopathic” ataxia, immune related such as anti-GAD and gluten ataxia
More benign SCAs such as SCA 6

Causes of Ataxia Based on Onset and CourseTempo Acquired Diseases Genetic Diseases
Episodic Many inborn errors of metabolism; EA syndromes
Acute (hours/days)
Strokes, ischemic and hemorrhagic; MS; infections; parainfectious syndromes; toxic disorders
Subacute (weeks/months)
Mass lesions in the posterior fossa; meningeal infiltrates; infections such as HIV, CJD; deficiency syndromes such B1 and B12; hypothyroidism; immune disorders such as paraneoplastic, gluten, and anti-GAD ataxia; alcohol
Chronic
Mass lesions such as meningiomas; craniovertebral junction anomalies; alcoholic; idiopathic cerebellar and olivopontocerebellar atrophy; MSA
Most genetic disorders such as FA, AT, and other AR ataxias; SCAs

Ataxias Primarily Cerebellar, Cerebellar and Sensory, Primarily Sensory, and Associated with Spasticity
Cerebellar AtaxiasMost of the acquired lesions in ; SCAs characterized by pure cerebellar ataxia (e.g., SCA 6, SCA 11, SCA 15)
Cerebellar-Sensory AtaxiasAT, AOAs, SCA 2, MJD, SCA 4, SCA 25
Sensory AtaxiasFA, AVED, acquired sensory ataxias related to “ataxic polyneuropathies” (e.g., paraneoplastic sensory neuropathy), Sjögren syndrome, diabetes, B6 toxicity
Spastic AtaxiasSCA 1, MJD, SCA 7, SCA 8, some cases of FA, ARSACS

Phenotypic Clues to Gene Mutations in the Dominant AtaxiasClue Related Dominant Ataxia
Age at onset Young adult: SCA1, 2, 3; childhood onset: DRPLA, SCA7, SCA13Older adult: SCA6
Degree of anticipation in age at onset
Often large in SCA7, DRPLAOften seen in all CAG repeat–related SCAs
Benign course SCA6
Upper motor neuron signs SCA1, 5, 7, 8, MJDRare in SCA2
Akinetic-rigid syndrome MJD, SCA2Chorea Prominent in DRPLA; may occur late in other SCAsAction tremor SCA12, SCA15/16Very slow saccades SCA2, 7; may occur late in SCA1, 3; uncommon in SCA6Downbeat nystagmus SCA6, EA2
Generalized areflexia SCA2, 4SCA3 with older-adult onset
Visual loss SCA7Seizures SCA10; early-onset cases of DRPLA and SCA7Dementia/psychiatric features
SCA12, 17, 27, DRPLA
Myoclonus DRPLA, SCA14Mental retardation SCA13Episodic symptoms EA1 and EA2

Episodic Ataxia Syndromes
Disease Phenotype Onset Mutation
EA1Very brief episodes of ataxia; interictal skeletal myokymia
Early childhood KCNA1
EA2Ataxic episodes lasting hours; interictal nystagmus
Childhood to young adult CACNA1A
EA3 Episodic vertigo and tinnitus
Linked to 1q
EA4Episodic vertigo; interictal nystagmus
Late onset
EA6Associated with hemiplegic migraine
EA7Attacks of vertigo, weakness, slurred speech
<20 years Linked to 19q

Noncerebellar Neurological Signs or Symptoms ,Help in D/D Ataxia
Non-neurological Signs or Symptoms Possible DiagnosisFocal and lateralized brainstem deficits such as facial palsy, hemiparesis
Posterior circulation strokes, tumors, MS
Visual loss from optic atrophy/retinopathyMS, FA, SCA 7, mitochondrial disease, Refsum disease, AVED
Papilledema, headachePosterior fossa tumors, ataxia as “false localizing” sign
Internuclear ophthalmoplegiaPosterior circulation strokes, MS, some SCAs
Gaze palsies Strokes, MS, NPC, MJD, SCAs 1, 2, 7Ptosis, ophthalmoplegia Strokes, MS, mitochondrial diseaseSlow saccades/ocular apraxia SCA 2, SCA 7, MJD, AT, AOA
Downbeat nystagmusArnold-Chiari malformation, basilar invagination, SCA 6, EA 2, lithium toxicity

Deafness Mitochondrial disease; superficial hemosiderosis
EpilepsyAtaxia associated with anticonvulsants; DRPLA, SCA 7, SCA 10
MyoclonusMitochondrial disease, Unverricht-Lundborg disease, SCA 7 of early onset, SCA 14, sialidosis, ceroid lipofuscinosis, idiopathic (Ramsay-Hunt syndrome)
Palatal myoclonus Alexander disease, SCA 20
Polyneuropathy FA, AOA, AVED, SCA 2, MJD, SCA 1,4,25
Cognitive declineAlcohol, MS, CJD, HIV, DRPLA, SCA 12, SCA 13, end-stage SCAs, superficial siderosis
Psychiatric features SCA 12, SCA 17, SCA 27
Noncerebellar Neurological Signs or Symptoms ,Help D/D Ataxia
Spasticity, upper motor neuron signs
Strokes, MS, tumors compressing brainstem, SCA 1, SCA 3, SCA 7, SCA 8; rarely FA
Basal ganglia deficitsMany SCAs like SCA 2, MJD, SCA 1, SCA 12, SCA 17; DRPLA, FXTAS, MSA, Wilson disease, Fahr disease
Tremor SCA 12, SCA 15/16, FXTASAutonomic failure Ataxic form of MSA, FXTAS

Systemic Feature Possible DiagnosisShort stature Mitochondrial disease, early CNS insults, ATConjunctival telangiectasia ATCataracts Marinesco-Sjögren syndrome, CTXCataplexy NPCKF rings Wilson diseaseCervical lipoma Mitochondrial diseaseAbnormal ECG, Echocardiogram FA, mitochondrial disease
Organomegaly Niemann-Pick disease, LOTS, Gaucher disease, alcohol
Hypogonadism Ataxia with hypogonadism (Holmes ataxia)Myopathy mtDNA mutations, CoQ10 deficiencyDiabetes ATSpine/foot deformity FA, AT, AVEDIncreased skin pigmentation AdrenoleukodystrophyHematologic malignancy ATSinopulmonary infections ATTendon xanthomas CTXHigh CK Mitochondrial disease, AOAHigh α-fetoprotein AT, AOA 2
Systemic Feature, Help D/D Ataxia

Imaging Abnormalities to D/D in Ataxias
MRI Abnormality Possible Diagnosis
Mass in the cerebellum/posterior fossa
Gliomas, meningiomas, abscess
Abnormal craniovertebral junction Arnold-Chiari malformation, basilar invagination
Infarcts, vascular malformations Ischemic lesions, AVM
Signal density change in the cerebellum
MS, acute cerebellitis
Signal density change in the MCP FXTAS
Pure cerebellar atrophySCAs with pure cerebellar signs (e.g., SCA 5, SCA 6); idiopathic cortical cerebellar atrophy; toxic, deficiency, and autoimmune ataxias
Pontocerebellar atrophyMany SCAs such as SCA 1, 2, and MJD; sporadic olivopontocerebellar atrophy; ataxic form of MSA
Cervical cord atrophy FA, AVED
Cerebral white matter changes Leukodystrophies presenting with ataxia, MS

Ataxias With Specific Abnormalities Confirm to Diagnosis
Disorder Diagnosis
Abetalipoproteinemia Low vitamin E levels, abnormal lipoprotein electrophoresis
Aceruloplasminemia Serum copper, ceruloplasmin, MRI brain
Adrenomyeloneuropathy MRI, serum long-chain fatty acidsAtaxia with coenzyme Q10 (CoQ10) deficiency
Low CoQ10 in muscle biopsy
AOA1 High serum cholesterol, low albumin
AOA2 High α-fetoprotein
AT High α-fetoprotein, low immunoglobulin (Ig)
Congenital disorders of glycosylation (CDG) Transferrin isoelectric focusing
Cerebrotendinous xanthomatosis Tendon xanthoma, serum cholestanol
Late-onset Tay-Sachs (LOTS) Hexosaminidase levels, hex-A mutation analysis
Maple syrup urine disease Urine amino acids
Niemann-Pick type C (NPC) disease Vertical gaze palsy, fibroblast and NPC mutation tests
Organic acidurias Urine organic acids, ketone bodies

Pyruvate dehydrogenase complex (PDHC) deficiency
Plasma and CSF lactate; PDHC in fibroblasts
Refsum disease Plasma phytanic acid
Sialidosis Neuraminidase
Urea cycle defects Plasma ammonia
Vanishing white matter disease MRI and MRS
Wilson disease Serum copper, ceruloplasmin
Ataxias With Specific Abnormalities Confirm to Diagnosis

TREATMENT
Acquired ataxias treated according to their specific etiology
Include treatment of strokes, tumors, multiple sclerosis, avoidance of toxic agents, and vitamin supplementation
Immunomodulatory treatments, like IV immunoglobulin, may be effective for some immune-mediated ataxias

AVED responds to high-dose vitamin E supplementation (800 mg/d to 1500 mg/d)
Recessive ataxias with coenzyme Q deficiency coenzyme Q10 150 mg/d to 300 mg/d
Cerebrotendinous xanthomatosis chenodeoxycholic acid, 750 mg/d
Refsum disease avoidance of phytanic acid and a high-calorie diet
Niemann-Pick type C disease- miglustat that inhibits glycolipid synthesis, at the dose of 200 mg 3 times a day
The ataxia telangiectasia patients treated with steroids (originallyfor lymphoma) showed improvement of ataxic symptoms

Approach to Ataxia

A Summary

SCA patterns in India


•Dysfunction of midline cerebellum causes truncal ataxia
• Truncal ataxia tested—with increasing difficulties—patient’s ability maintain posture while standing, walking, tandem walking, or standing on one leg
• Dysfunction of lateral (hemispheral) cerebellum results in ipsilateral limb ataxia
• To limb incoordination, tests coordination while the patient is building a tower, writing and drawing
• Motor incoordination from disturbance of afferent sensory input is exacerbated by eye closure
• Cerebellar ataxia does not worsen, or worsens only slightly, if visual guidance is eliminated

MLFMLF
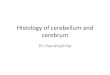
Main Connections of the VestibulocerebellumMain Connections of the VestibulocerebellumMain Connections of the VestibulocerebellumMain Connections of the Vestibulocerebellum
lower motor neuronlower motor neuron
LMNLMN
vestibulospinal tractvestibulospinal tract
FASTIGIALFASTIGIAL NUCLEUSNUCLEUS
VestibularVestibular OrganOrgan FloculonodularFloculonodular
LobeLobe
VermisVermis
ARCHICEREBELLUMARCHICEREBELLUM
VESTIBULAR NUCLEUSVESTIBULAR NUCLEUS

Main Connections of the PaleocerebellumMain Connections of the PaleocerebellumMain Connections of the PaleocerebellumMain Connections of the Paleocerebellum
lower motor neuronlower motor neuron
SPINAL CORDSPINAL CORD
rubrospinal rubrospinal tracttract
NUCLEUSNUCLEUSINTERPOSITUSINTERPOSITUS
InferiorInferior OlivryOlivryNucleusNucleus
ANTERIOR ANTERIOR LOBELOBEPARAVERMAL PARAVERMAL ZONEZONE
PALEOCEREBELLUMPALEOCEREBELLUM
RED RED NUCLEUSNUCLEUS
spinocerebellar tractspinocerebellar tract

CEREBRALCEREBRAL CORTEXCORTEX
CEREBRALCEREBRAL CORTEXCORTEX
DENTATEDENTATENUCLEUSNUCLEUS
DENTATEDENTATENUCLEUSNUCLEUS
Main Connections of the NeocerebellumMain Connections of the NeocerebellumMain Connections of the NeocerebellumMain Connections of the Neocerebellum
lower motor neuronlower motor neuron
LMNLMN
pyramidal pyramidal tracttract POSTERIOR POSTERIOR
LOBELOBECEREBELLARCEREBELLAR HEMISPHEREHEMISPHERE
POSTERIOR POSTERIOR LOBELOBE
CEREBELLARCEREBELLAR HEMISPHEREHEMISPHERE
THALAMUSTHALAMUSTHALAMUSTHALAMUS
NEOCEREBELLUMNEOCEREBELLUM
PontinePontineNucleusNucleusPontinePontineNucleusNucleus

upper motor neuronupper motor neuron
UMNUMN
upper motor neuronupper motor neuron
UMNUMN
BASALBASALGANGLIAGANGLIABASALBASAL
GANGLIAGANGLIA
Pyramidal Tract and Associated CircuitsPyramidal Tract and Associated CircuitsPyramidal Tract and Associated CircuitsPyramidal Tract and Associated Circuits
lower motor neuronlower motor neuron
UMNUMN
lower motor neuronlower motor neuron
UMNUMN
pyramidal tractpyramidal tract
CerebellumCerebellumCerebellumCerebellum

ReticularFormation
ReticularFormation
CEREBELLUMCEREBELLUM
Cerebellum and Automatic Motor ControlCerebellum and Automatic Motor ControlCerebellum and Automatic Motor ControlCerebellum and Automatic Motor Control
Lower Motor Neuron (LMN)Lower Motor Neuron (LMN)Lower Motor Neuron (LMN)Lower Motor Neuron (LMN)
Motor CortexMotor Cortex
Red NucleusRed Nucleus
Vestibular Nucleus
Vestibular Nucleus
ProprioceptorsProprioceptorsProprioceptorsProprioceptors

Machado-Joseph Disease/Sca3MJD was first described among the Portuguese and their descendants in New
England and California. Subsequently, MJD has been found in families from Portugal, Australia, Brazil, Canada, China, England, France, India, Israel, Italy, Japan, Spain, Taiwan, and the United States. In most populations, it is the most common autosomal dominant ataxia.
Symptoms and SignsMJD has been classified into three clinical types. In type I MJD (amyotrophic lateral sclerosis–parkinsonism–dystonia type), - neurologic-deficits appear in the first two decades and - involve weakness and spasticity of extremities, especially the legs, often with
dystonia of the face, neck, trunk, and extremities. - Patellar and ankle clonus are common, as are extensor plantar responses. The
gait is slow and stiff, with a slightly broadened base and lurching from side to side; this gait results from spasticity, not true ataxia.
- There is no truncal titubation. Pharyngeal weakness and spasticity cause difficulty with speech and swallowing.
- Of note is the prominence of horizontal and vertical nystagmus, loss of fast saccadic eye movements, hypermetric and hypometric saccades, and impairment of upward vertical gaze.
- Facial fasciculations, facial myokymia, lingual fasciculations without atrophy, ophthalmoparesis, and ocular prominence are common early manifestations.

In type II MJD (ataxic type)
- true cerebellar deficits of dysarthria and gait and extremity ataxia begin in the second to fourth decades along with corticospinal and extrapyramidal deficits of spasticity, rigidity, and dystonia.
- Type II is the most common form of MJD. Ophthalmoparesis, upward vertical gaze deficits, and facial and lingual fasciculations are also present.
- Type II MJD can be distinguished from the clinically similar disorders SCA1 and SCA2.
Type III MJD (ataxic-amyotrophic type) - presents in the fifth to the seventh decades with a pancerebellar
disorder that includes dysarthria and gait and extremity ataxia. - Distal sensory loss involving pain, touch, vibration, and position
senses and distal atrophy are prominent, indicating the presence of peripheral neuropathy.
- The deep tendon reflexes are depressed to absent, and there are no corticospinal or extrapyramidal findings.

The mean age of onset of symptoms in MJD is 25 years.
Neurologic deficits invariably progress and lead to death from debilitation within 15 years of onset, especially in patients with types I and II disease.
Usually, patients retain full intellectual function.
The major pathologic findings are variable loss of neurons and glial replacement in the corpus striatum and severe loss of neurons in the pars compacta of the substantia nigra.
A moderate loss of neurons occurs in the dentate nucleus of the cerebellum and in the red nucleus.
Purkinje cell loss and granule cell loss occur in the cerebellar cortex. Cell loss also occurs in the dentate nucleus and in the cranial nerve motor nuclei.
Sparing of the inferior olives distinguishes MJD from other dominantly inherited ataxias.



Friedreich’s ataxia….

FA:Inheritance and onset
Most frequent of autosomal recessive ataxia’sOnset in late childhood or adolescence

Tracts affected in Friedreich’s

FA: Clinical features

Atypical features of FAReflexes may be preserved or hyperactiveCalled FA with retained reflexes[FARR]Kyphoscoliosis and heart disease less common and
prognosis is betterLate onset FA [LOFA]. Onset beyond 25 years.

……does it differ in clinical features?

FA in India: 30 patients followed up for 2-10 yearsSimilar neurologic features
Only 20% had ECG abnormalities
Cardiac enlargement and heart failure seen in only one patient
Cardiac involvement less frequent in Indian patients
FA is less common than dominant ataxia’s in India [ ataxia registry 1997-2002]