Embed Size (px)
DESCRIPTION
Sending The Right Signals: How Can HTA Optimally Inform PLAs in the Context of pCPA
Citation preview

Sending the Right Signals: How Can HTA Optimally Inform PLAs in the context of pCPA
Mona Sabharwal, BScPhm, PharmD
Executive Director
pan-Canadian Oncology Drug Review
April 8, 2014

Building linkages to pCPA
• pCODR provides a more predictable, regularized entry point for
new drugs/new uses to be evaluated for public funding,
including non-commercially generated data
• pCODR’s commitment to transparency, need to be accountable
to patients and the public, allow for multiple perspectives on
value to be elicited and shared
• Adoption feasibility discussion systematically solicited and
incorporated into reviews
• By having singular evidence-base for recommendations,
provides clearer and more consistent direction on areas of
uncertainty which could be used for negotiation purposes
2 Copyright pan-Canadian Oncology Drug Review

National context for pCODR
• Cancer is increasingly viewed as a serious, life threatening but
chronic disease
• Number and pace of new treatments available rising fast
• National differences in structures and processes for review and
funding of cancer drugs
• Variation in use/acceptability of pharmacoeconomic information,
submission requirements, roles/expectation for manufacturers
• Variation in coverage across jurisdictions
• Frustration amongst patients and stakeholders
3 Copyright pan-Canadian Oncology Drug Review

Key lessons from national collaborative efforts
• Ownership, involvement and support of cancer agencies is critical
• Transparency of process for all stakeholders (ministry, agency,
patients, manufacturers) is essential
• Cancer control community ready for an evidence-based review
process:
• strong culture of evidence generation (NCIC and others)
• clinical guidelines and protocol-based care well established
• systems for data capture exist or are being created
• Economic evaluation a necessary part of any HTA process
• significant need for capacity enhancement across spectrum
of generators and users of this type of information in
cancer control system
4
Copyright pan-Canadian Oncology Drug Review

About pCODR
• pCODR was created in recognition of certain unique characteristics of how
cancer care is organized and delivered in Canada
• Implemented in 2010 to:
assess cancer drugs and makes recommendations to provinces and territories to
guide their drug funding decisions by ensuring that all provinces and cancer
agencies benefit from a single, clear approach to new cancer drug evaluation
leverage best practices and expertise from across Canada to provide provinces
and territories with the best possible information on which to base their funding
decisions
bring consistency and clarity to assessment of cancer drugs by looking at clinical
evidence, cost-effectiveness and patient perspectives
• Transitioned governance under CADTH as of April 1, 2014
5 Copyright pan-Canadian Oncology Drug Review

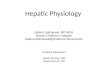
pCODR Review Process Updated March 31, 2011
1. Conduct
Pre-
Submission
Planning
activities
including
getting
input from
PAG and
notifying
Patient
Advocacy
Groups
2. Prepare
& submit
Request
for Drug
Review
4.2
Conduct
Economic
Review
5.
Summarize
& Review
with pERC
6. Prepare &
Publicly
Post Initial
Recomm,
Post
Reviews
8. Summarize
& Review with
pERC
3.1 Screen
Submission
and Initiate
Review
Process
End‡
Ind
us
try/
Tu
mo
ur
Gro
up
p
CO
DR
*
Variable 5 business days 70-90 business days 12 business days 10 business days 20 business days
7.1 Get
Feedback
from
Submitter
(and impacted
manufacturer)
7.3 Get
Feedback
from Patient
Advocacy
Group
7.2 Get
Feedback
from PAG
Pati
en
t A
dv
ocac
y
Gro
up
s
9. Prepare &
Publicly Post
Final
Recomm &
Post Input
12 business days
*Includes pCODR Secretariat, Clinical
Guidance Panel, Economic Guidance Panel,
pCODR Expert Review Committee (pERC)
and Provincial Advisory Group (PAG)
4.1.1/4.2.2
Clarify info
with
Submitter
during
review
4.1
Conduct
Clinical
Review
3.2 Collect
Patient
Advocacy
Group
Input
Estimated
99 – 149
business days
7.4
Eligible for
Early
Conversion?
No Yes
‡Next steps could include
Recommendation implementation,
Procedural Review or Resubmission
6 © 2013 pan-Canadian Oncology Drug Review

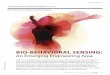
pERC Final Recommendation
7
pERC has issued 29 final recommendations as of
December 31, 2013
5 (17%) positive recommendation without
conditions
18 (62%) conditional recommendation*
(*subject to improve cost-effectiveness)
6 (21%) negative recommendation
17%
62% 21%
Column1 PositiveRecommendation
ConditionalRecommendation
NegativeRecommendation
Drug Name & Indication pCODR Recommendation
Pazopanib hydrochloride (Votrient) Metastatic Renal Cell Carcinoma
Recommend
Sunitinib malate (Sutent) Pancreatic Neuroendocrine Tumours
Recommend with conditions
Ipilimumab (Yervoy) Advanced Melanoma
Recommend with conditions
Vemurafenib (Zelboraf) Advanced Melanoma
Recommend with conditions
Eribulin mesylate (Halaven) Metastatic Breast Cancer
Recommend with conditions
Everolimus (Afinitor) Pancreatic Neuroendocrine Tumours
Recommend with conditions
Crizotenib (Xalkori) Advanced Non-Small Cell Lung Cancer
Do Not Recommend
Bendamustine hydrochloride (Treanda) Chronic Lymphocytic Leukemia (relapsed/refractory)
Do Not Recommend
Bendamustine hydrochloride (Treanda) Non-Hodgkin Lymphoma and Mantle Cell Lymphoma
Recommend
Pazopanib hydrochloride (Votrient) Soft Tissue Sarcoma (STS)
Do Not Recommend
Ruxolitinib (Jakavi) Myelofibrosis
Recommend with conditions
Bendamustine hydrochloride (Treanda) Chronic Lymphocytic Leukemia (first-line)
Recommend with conditions
Axitinib (Inlyta) Metastatic Renal Cell Carcinoma
Recommend
Everolimus (Afinitor) Advanced Breast Cancer
Recommend with conditions
Bortezomib (Velcade) Multiple myeloma pre ASCT
Recommend
Bortezomib (Velcade) Multiple myeloma post ASCT as monotherapy
Do Not Recommend
Crizotinib (Xalkori) - Resub Advanced Non-Small Cell Lung Cancer
Recommend with conditions
Lapatinib (Tykerb) in combo with letrozole Do Not Recommend
Enzalutamide (Xtandi) Recommend with conditions
Pertuzumab (Perjeta Herceptin) Recommend with conditions
Pazopanib (Votrient) Resubmission Recommend
Brentuximab (Adcetris) - HL Recommend with conditions
Regorafenib (Stivarga) - mCRC Do Not Recommend
Abiraterone (Zytiga) - mCRP Recommend with conditions
Lenalidomide (Revlimid) – Multiple Myeloma Recommend with conditions
Trametinib (Mekinist) – Metastatic Melanoma Recommend with conditions
Dabrafenib (Tafinlar) – Metastatic Melanoma Recommend with conditions
Pemetrexed disodium (Alimta) – Advanced or Metastatic Non-Squamous Non-Small Cell Lung Cancer Recommend with conditions
Brentuximab (Adcetris) - SALCL Recommend with conditions
Copyright pan-Canadian Oncology Drug Review

pERC Recommendations
• pERC recommendations help guide funding decisions; final
funding decisions remain responsibility of each participating
jurisdiction
• Funding recommendations are not static - they are context
specific, such as:
• evidence available at that point in time
• existing programs and policies – who is covered, what is/is
not covered
• basket of currently available and/or funded treatment
options
• current pricing arrangements
8 Copyright pan-Canadian Oncology Drug Review

pERC Recommendations
Recommend
• A drug with a clear clinical benefit and economic benefit
Consider with Conditions
• Provides context and describes conditions under which a specific
jurisdiction may or may not want to fund the drug
• These conditions would relate to issues that directly change the
efficacy or cost-effectiveness of the drug
• Factors or conditions to consider could include utilization
patterns, funding of comparators, availability/accessibility of
other options
Do Not Recommend
• No reason to recommend identified during pERC deliberations
9 Copyright pan-Canadian Oncology Drug Review

Building linkages to pCPA
• pCODR provides a more predictable, regularized entry point for
new drugs/new uses to be evaluated for public funding,
including non-commercially generated data
• pCODR’s commitment to transparency, need to be accountable
to patients and the public, allow for multiple perspectives on
value to be elicited and shared
• Adoption feasibility discussion systematically solicited and
incorporated into reviews
• By having singular evidence-base for recommendations,
provides clearer and more consistent direction on areas of
uncertainty which could be used for negotiation purposes
10 Copyright pan-Canadian Oncology Drug Review

Common Sources of Uncertainty in pCODR reviews
• Clinical uncertainty
need, burden of illness, practice patterns, magnitude of benefit
• Statistical uncertainty
cross over, non-inferiority
• Uncertainty in patient values
QoL, preferences and priorities
• Economic uncertainty
assumptions due to lack of clinical, epidemiological and
utilization data
• Structural/systems uncertainty
ability to deliver and integrate into systems, affordability
11 © 2014 pan-Canadian Oncology Drug Review

Time of launch evaluation (current HTA focus)
• Characterize uncertainty
which parameters are most uncertain e.g., surrogate marker,
magnitude of benefit
what are the drivers for that uncertainty e.g., clinical use
assumptions
what could help reduce uncertainty e.g., companion testing
for managing eligibility, marker for response
what will mitigate some risks e.g., controlled distribution
and delivery
• Challenge – what to actually do about uncertainty and
when
12 © 2014 pan-Canadian Oncology Drug Review

Post-launch evaluation (future HTA focus?)
• Coverage with evidence development
help define questions of relevance for specific drug and
disease instance
• Performance / Real world effectiveness
advice on what to measure and when
• Disinvestment opportunities
identify potentially obsolete therapies in favour of newer
option
• Challenges: simplicity, transferability, measurability
13 © 2014 pan-Canadian Oncology Drug Review





![Optimizing Fish Passage Barrier Removal Using Mixed Integer Linear Programming [Preliminary Report] Carla P. Gomes, Ashish Sabharwal Cornell University](https://img.pdfslide.us/doc/110x75/56649eef5503460f94bff825/optimizing-fish-passage-barrier-removal-using-mixed-integer-linear-programming.jpg)