Embed Size (px)
Citation preview

Dr.Rohan P Reddy2nd year resident
Dept. of Internal Medicine
A 21 yr old male patient,anand , student by occupation resident of vedira , karimnagardistrict came with the chief complaints of :
Distension of abdomen since 10 days
Shortness of breath since 3 days

Pt was apparently asymptomatic 10 days ago when he developed distension of abdomen which had a gradual onset and was progressive in nature ,
Associated with yellowish discoloration of eyes and urine
Associated with bloody vomitings
Associated with blackish discoloration of stool
Associated with loss of appetite
Associated with shortness of breath , grade 4

No h/o orthopnoea , PND episodes
No h/o cough
No h/o decreased urine output
No h/o pedal edema
No h/o facial puffiness
No h/o fever
No h/o abdominal pain
No h/o itching

Past h/o :
Pt had a history of similar complaints twice in the past for which he was admitted to the hospital for about 30 days and was later discharged when the symptoms subsided .
He underwent blood transfusions during the admission
He was not put on any long term medical therapy for his condition
He did not undergo any surgical procedures during the stay

Family h/o : Insignificant
Personal h/o : pt was non alcoholic , non smoker . He consumed non vegetarian diet had normal sleep and normal bowel habits

21 year old patient who is thin built , malnourished
Pallor present
Clubbing – grade 2
Icterus present
Leukonychia – present
Abdominal distension – present
No cyanosis , koilonychia , lymphadenopathy , edema



Vitals :
BP : 120/70 mm hg
PR : 80/min
RR : 20/min
Afebrile
SPO2 : 100 % without o2

S/O liver cell failure :
Absence of secondary sexual characterstics
Testicular atrophy
No gynaecomastia
No palmar erythema
No asterixis
No dupuytren’s contractures
No spider naevi
No parotid gland enlargement
No fetor hepaticus
GIT :Inspection :
shape of the abdomen : distended symetricallyShape of the umblicus : horizontal slit Moving with respiration
Engorged veins : engorged veins present on the epigastrium
No visible pulsations and peristalisisFlanks full
Hernial orifices – normal No scars and sinuses Genitals – normal


Palpation :
No local rise of temperature and tenderness
Flow of the blood through the veins : below upwards (away from the umblicus )
Liver : palpable 3cms below the coastal margin
Spleen : moderate splenomegaly , palpable 4cms below the coastal margin b/w the umblicus and the coastal margin
Fluid thrill +

Percussion : shifting dullness absent
Auscultation :
no bruit heard
Bowel sounds present
No venous hum heard
Gross ascites with portal hypertension
Etiology : cirrhosis of liver ( hepatitis B,C ,schistosomiasis, wilson’sdisease,hemochromatosis, drugs )
Vascular disorders

Complete blood picture
Liver function tests
Blood sugar
Serum creatinine
Blood urea
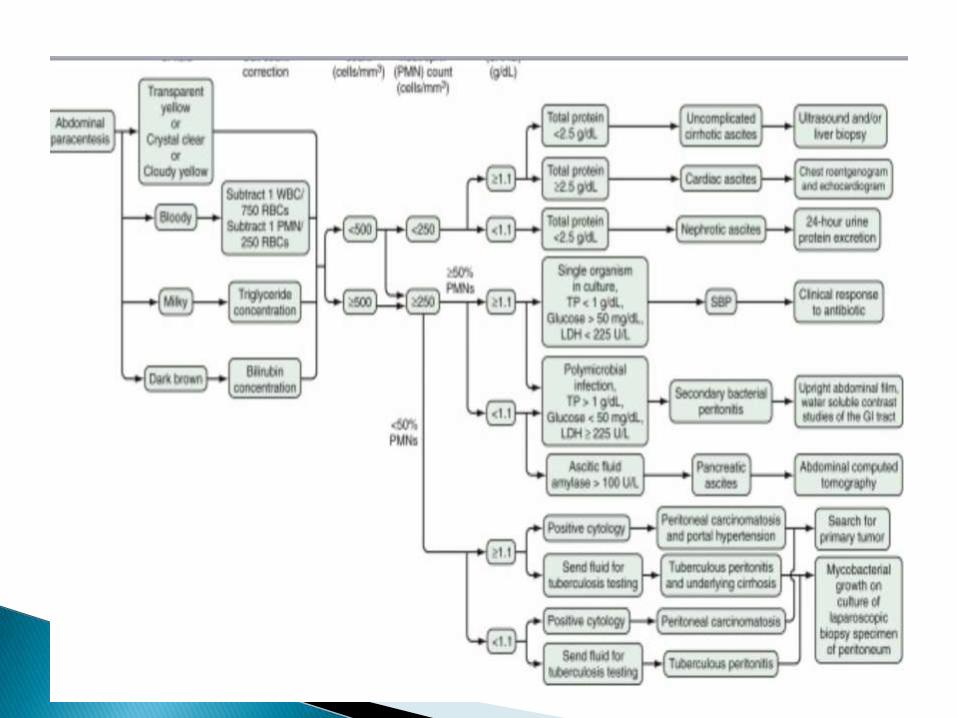
Ascitic fluid analysis
ECG
Ultrasound abdomen

Complete blood picture :
HB: 6.5g/dl
TLC : 3500 /cumm
Platelets : 1lakh/cumm
Reticulocyte count : 1%

Liver function tests :
Se.bilirubin : 3mg/dl ( d: 1, id: 2)
Total proteins : 6g/dl
Se.albumin : 3mg/dl
Enzymes : normal
PT , APTT : normal

FBS : 120mg/dl
PLBS : 178mg/dl
Se.creatinine : 1 mg/dl
Bl.urea : 35
ECG : normal sinus rhythm

Color : straw colored
Quantity : 10ml
TLC : 110 cells
DC : 50% neutrophils , 50% lymphocytes
Total protein : 2g/dl
Ascitic fluid albumin : 0.5g/dl
SAAG : 2.5g/dl

Ultra sound abdomen :
Macronodular cirrhosis of the liver
Portal vein dilated ( 13 mm )
Massive splenomegaly
Doppler hepatobiliary system :
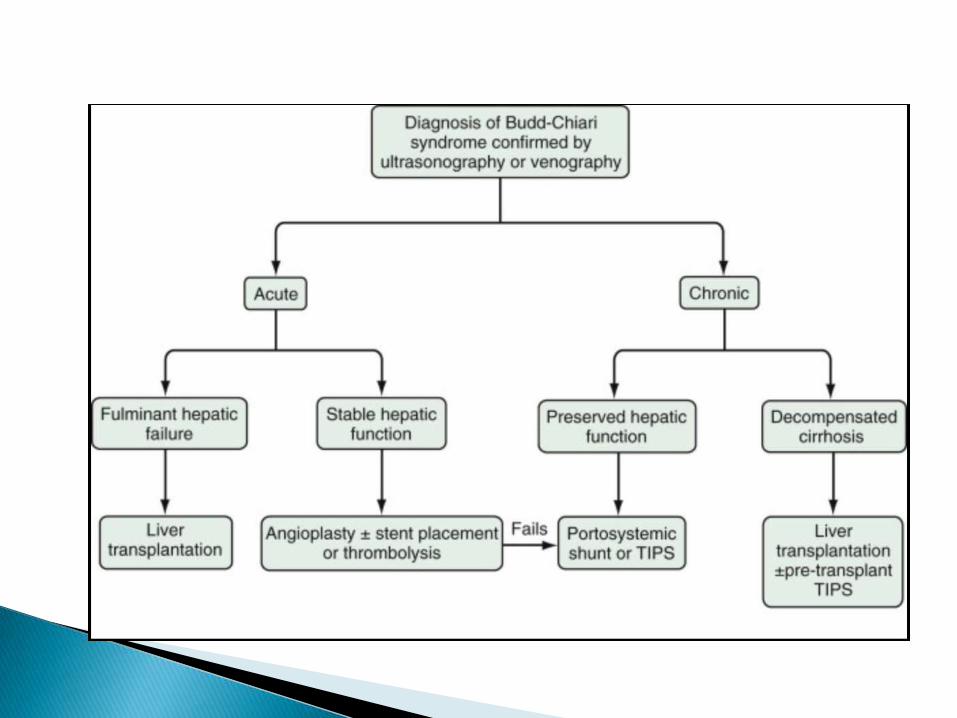
Non visualization of the hepatic veins









Antiphospholipid antibody syndrome with venous thrombosis ( budd chiari syndrome ) with inherited thrombophilia.

A clinicopathologic diagnosis…

International Consensus Statement on Classification Criteria for APS (2006).◦ Clinical criteria.
Vascular thrombosis.
Pregnancy morbidity.
◦ Laboratory criteria.
Lupus anticoagulant.
Anticardiolipin IgG or IgM antibody.
Anti- 2glycoprotein I IgG or IgM antibody.
-- Miyakis, et al., J.Thromb.Haemost., 2006; 4: 295

Thrombocytopenia and/or hemolytic anemia.
Transverse myelopathy or myelitis.
Livido reticularis.
Cardiac valve disease.
Nephropathy.
Non-thrombotic neurologic manifestations, including multiple sclerosis-like syndrome, chorea, or migraine headaches.
-- Miyakis, et al., J.Thromb.Haemost., 2006; 4: 295

Major criteria:◦ venous thrombosis .
◦ Anticardiolipin IgG antibody positive
Non-criteria APS-associated parameters:◦ Thrombocytopenia.
Yes.

Treatment of venous thromboembolism in patients with antiphospholipid antibodies.◦ We recommend … a target INR of 2.5 (INR range,
2.0 and 3.0) (Grade 1A). We recommend against high-intensity VKA therapy (Grade 1A).
◦ We recommend treatment for 12 months (Grade 1C+).
◦ We suggest indefinite anticoagulant therapy for these patients (Grade 2C).
-- Buller, et al., Chest, 2004; 126 (Supplement): 401S.

For patients with APS and venous thrombosis, treatment for 6 months with a target INR of 2.5 is reasonable.
Recurrent venous thrombosis should be treated by “long-term” oral anticoagulation.
Recurrence while the INR is between 2.0 and 3.0 should lead to more intensive warfarin therapy, target INR 3.5, but this is “uncommon”.
-- Greaves, et al., Br.J.Haematol., 2000; 109: 704













![Rx161 Arnold-Chiari Malformationfinalcopy0048502.netsolhost.com/.../pdfs/RXforms/Arnold_Chiari_Malformation.pdfArnold-Chiari malformation [Chiari malformation (CM)] is a congenital](https://img.pdfslide.us/doc/110x75/5ab9a8f17f8b9ac60e8e5491/rx161-arnold-chiari-malforma-malformation-chiari-malformation-cm-is-a-congenital.jpg)














