Embed Size (px)
Citation preview

Breast PathologyBreast Pathology
Dr.CSBR.Prasad, M.D.Dr.CSBR.Prasad, M.D.
Mixed connective tissue and epithelial tumors
Male breast

Source: Sabiston – Text book of Surgery, 15th Ed, Vol-1

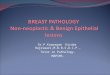
The normal microscopic appearance of female breast tissue is shown here. There is a larger duct to the right and lobules to the left. A collagenous stroma extends between the structures (Interlobular – Red stars). Intralobular stroma is hormonally responsive (Blue Stars). A variable amount of adipose tissue can be admixed with these elements.
Normal histologyS
ourc
e: w
ebpa
th

Mixed connective tissue & Epithelial tumors
There are two types of stroma in the breast:
1. Intralobular stroma (Fibroadenoma, Phyllodes tumor)
2. Interlobular stroma (tumors similar to other sites of the body – Lipoma, angiosarcoma, PASH, Fibrous tumors et.c.)

Fibroadenoma (FA)
• Most common benign tumor of female breast
• Wide age range but, common <30yrs
• They may be multiple & bilateral
• Mammography – densities, pop-corn calcifications
• Epithelium in FA is hormonally responsive
• Tumors may regress after menopause

• Sharply circumscribed• Freely movable in the surrounding breast tissue
(Mouse in the breast)
• Size may vary from 1cm to very large tumors• Encapulated• Rubbery in consistency• c/s bulges above the surrounding tissue• Contain slit like spaces – cut cabbage
appearence
Fibroadenoma (FA)

Fibroadenoma (FA)

Here is a surgical excision of a small mass from the breast. The mass is well-circumscribed. Grossly it felt firm and rubbery. This is a fibroadenoma. The blue dye around the fibroadenoma was used to mark the lesion during needle localization in radiology so that the surgeon could find this small mass.

Microscopy:
1. Stroma is spindly, cellular with myxoid areas
2. Glands dispersed in the stroma and there may be slit like spaces lined by the epithelium
3. Stroma may become densely hyalinized in older women
Fibroadenoma (FA)

Here is the microscopic appearance of a fibroadenoma. To the right is compressed breast connective tissue forming a "capsule" to this mass. The neoplasm itself is composed of a fibroblastic stroma in which are located elongated compressed ducts lined by benign appearing epithelium.
Capsule
Stroma
Ducts

At low power, this fibroadenoma has compressed ducts surrounded by a fibrous stroma. These lesions are most likely to be found as a "breast lump" on examination of young women. They are discrete, firm, rubbery masses that are freely movable.

At medium power, the benign appearance of the ductular epithelium and collagenous stroma is apparent. Fibroadenomas may enlarge slowly over time, and they may enlarge and cause some discomfort during the menstrual cycle. After menopause, they regress and form a firm mass that must be distinguished from breast carcinoma.

• Pathogenesis: polyclonal in origin due to focal hyperplasia of lobular stroma.
• There is no increased risk of developing Carcinoma
• FAs associated with cysts >0.3cm, sclerosing adenosis, epithelial calcifications and papillary apocrine change (complex FA) may show slightly increased malignant potential
Fibroadenoma (FA)

Phyllodes tumor
• Originates from the intralobular stroma
• Terminology – cystosarcoma phyllodes / Phyllodes tumor
• Size: a few cms to massive lesions
• Cut surface is usually fleshy

Phyllodes tumor in a 52 yo woman

Source: Sabiston – Text book of Surgery, 15th Ed, Vol-1

-Phyllode’s tumor in a women of 28years.
-Weight 18kgs.-Ulceration (arrow)
due to pressure.

This mammogram demonstrates a large 10 cm mass lesion consistent with a phyllodes tumor.
Source: webpath

Microscopy:• Proliferating stroma covered by epithelium• They exhibit bulbous protrusions (leaf like)• Sometimes protrusions extend into cystic spaces• Foci of mesenchymal differentiation (Rhabdo,
Liposarcoma)DD: ----it can be differentiated from FA by
cellularity and mitotic activity ----if the lesion is high grade, it may be
impossible to distinguish from other soft tissue sarcomas
Phyllodes tumor

A phyllodes tumor of the breast is shown here. They arise from interlobular stroma, but unlike fibroadenomas are not common and are much larger. They are low-grade neoplasms that rarely metastasize. They are more cellular than fibroadenomas. Projections of stroma into the ducts create the leaf-like pattern for which these tumors are named
(from the Greek word phyllodes meaning leaf-like).

Cystosarcoma phyllodes. H&E
http://www.hopkinsbreastcenter.org/pathology/malignant/

Treatment:
• Must be excised with wide margin or by mastectomy
• They recur with high grade• Axillary dissection is not indicated• One third will recur and spread hemtogenously• Only stromal component metastasizes.
Phyllodes tumor

Duct papilloma




A small benign intraductal papilloma appears here in a breast duct, typically in one of the main lactiferous ducts beneath the areola. Note that the epithelial cells show no atypia and that there is a fine pink collagenous stroma within the papilloma. An intraductal papilloma may be associated with a serous or bloody nipple discharge, or it may cause some nipple retraction.

Gynecomastia
• Enlargement of male breast
• It can be unilateral / bilateral
• Usually presents as button like subareolar enlargement
• It’s an indication of hyperestrinism

Causes:
1. Cirrhosis of the liver2. Functioning testicular tumor (leydig cell tumor,
sertoli cell tumor)3. Anabolic steroids4. Alcoholism5. Antipsychotic agents6. Antiretroviral drugs7. Marijuana / heroin
Gynecomastia
33

Microscopy:
1. Proliferation of dense collagenous tissue
2. Micropapillary hyperplasia of ductal epithelium
3. Edema of the stroma around the ducts
Gynecomastia


Gynecomastia in a 25yo male. Secondary to Leyding cell tumor of testis.


An increased amount of breast tissue in a male is known as gynecomastia. This condition is not common. In pubertal males it may be idiopathic and resolve, or persist and require surgical removal, as in this case seen here. In older males it may be the result of cirrhosis of the liver (from decreased hepatic clearance of estrogenic substances), from pharmacologic agents, or from neoplasms such as Leydig cell tumor of the testis.

The normally small amount of male breast tissue consists of just a few ducts, without lobules, in a fibrous stroma. With gynecomastia, this tissue is increased, and there can be ductal epithelial hyperplasia, or prominent periductular edema as seen here. Gynecomastia can be unilateral or bilateral.

Carcinoma of male breast
• Rare (<1:100 when compared to female breast carcinomas)
• Risk factors – similar to female breast ca• Gynecomastia is not a risk factor• BRCA 2 mutation• Histology is similar to female breast ca• Papillary carcinomas are more common• ER positivity is more common (81%)• Prognostic factors are similar to male & female
breast cancers when age and stage are matched

• Presents usually as subaereolar mass• Nipple discharge is a common symptom• As there is very little fat the tumor invades
the skin and muscle rapidly• Axillary LN mets are seen in 50% of cases
at the time of presentation• Distant mets also common• prognosis is similar to female breast ca
when matched for age and stage
Carcinoma of male breast

Prognostic & predictive factors
MAJOR PF MINOR PFInvasive Vs in situ Small tumor w or w/o node
positivity
Distant mets ER/PR status
LN mets Her-2/Neu
Tumor size Tumor grade
Locally advanced disease Histological type
Inflammatory carcinoma Proliferation rate
DNA content
LVI

Carcinoma of the male breast.

Carcinoma of the male breast – advanced.


E N D