Embed Size (px)
Citation preview

Breast pathologyDr.CSBR.Prasad, M.D.

Cases

Cases

Cases

Cases

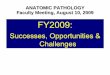
Left image – affected breast Right image – Normal breast
Cases

60yo male
Cases

Cases
1 2

Cases

Cases

Cases

Cases

Cases

Breast pathology

Mammary gland – Normal features
1. Covered by skin & subcutaneous tissue
2. Rests on pectoralis muscle
3. Pectoral fascia separates it from the pectoral muscles

Breast – Normal features
• Modified skin appendage.• Composed of specialized epithelium and stroma
that gives rise to both benign and malignant lesions.• 6-10 major ductal system originate at the nipple.• Keratinizing sq.epithelium of overlying skin
continues into the ducts and then abruptly changes to a double layered cuboidal epithelium.
• Surrounding areolar skin is pigmented & supported by smooth muscle.

• Normal duct system microSource: Ackerman’s Surgical Pathology 9th Ed, 1765p

• Morphofunctional unit of the organ is SINGLE GLAND composed of 2major parts:
1-TDLU (secretory unit of the gland) a-lobule b-terminal ductule 2-Large duct system
Breast – Normal features

• Importance of division of mammary gland unit into 2 major portions resides in its relation to disease of this organs.
• TDLU (FCD, Ductal hyperplasia, Carcinoma)
• Large duct system (Solitary papilloma, ductectasia, rare ductal carcinomas)
Breast – Normal features

Normal anatomy and possible pathological lesions

3910Source: Ackerman’s Surgical Pathology 9th Ed, 1765p

Histology

Histology
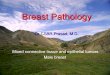
Epithelium & Stroma:• Ducts and lobules are lined by 2 cell types 1-Myoepithelial cell lying on the BM. 2-Epithelial cells lines the lumen.• Stroma 1-Interlobular stroma 2-Intralobular stroma (hormonally responsive)

The normal microscopic appearance of female breast tissue is shown here. There is a larger duct to the right and lobules to the left. A collagenous stroma extends between the structures (Interlobular – Red stars). Intralobular stroma is hormonally responsive (Blue Stars). A variable amount of adipose tissue can be admixed with these elements.
Normal histology
Source: webpath

Normal histology
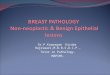
At high magnification, the appearance of a normal breast acinus is shown here. Note the epithelial cells lining the lumen demonstrate apocrine secretion with snouting, or cytoplasmic extrusions, into the lumen. A layer of myoepithelial cells, some of which are slightly vacuolated, is seen just around the outside of the acinus.
Source: webpath

Epithelial markers
• EMA• Milk Fat Globule Membrane antigen• alfa-Lactalbumin
Source: Ackerman’s Surgical Pathology 9th Ed, 1765p

Normal histology
An immunoperoxidase stain with antibody to actin demonstrates the myoepithelial cell layer around the breast acinus. The myoepithelial cells are contractile and are very sensitive to oxytocin.
Source: webpath

Markers for Myoepithelium
• S-100 protein• P-Cadherin• SMA• Calponin• Smooth muscle myosin-heavy chain• Maspin• Caldesmon• p63
Source: Ackerman’s Surgical Pathology 9th Ed, 1765p

Disorders of development
1. Milk line remnants.2. Accessory axillary breast tissue.3. Congenital nipple inversion.

Milk line remnants“POLYTHELIA”
Epidermal thickening along the milk line extending from axilla to perineum.

The classification established by Kajava in 1915 is still valid: (De Cholnoky, 1939)
1. Complete SN: Nipple + areola + glandular breast tissue 2. SN: Nipple + glandular tissue (no areola) 3. SN: Areola + glandular tissue (no nipple) 4. Aberrant glandular tissue only 5. SN: Nipple + areola + pseudomamma (fat tissue that replaces the
glandular tissue) 6. SN: Nipple only (the most common SN) 7. SN: Areola only (polythelia areolaris) 8. Patch of hair only (polythelia pilosa)
Milk line remnants

Disorders of development Milk line remnants

In some persons normal ductal system extends into subcutaneous tissue of the chest wall and into the axillay fossa.
Importance: Therapeutic mastectomy might remove the entire breast but not remove all breast epithelium.
Hence cannot compeltely eliminate the risk of developing breast cancer.
Disorders of development Accessory axillary breast tissue

Disorders of development Accessory axillary breast tissue

It may be bilateral or unilateral.
Importance: may be mistaken for carcinoma or inflammation.
Disorders of development Congenital nipple inversion

Disorders of development Congenital nipple inversion

Clinical presentations
• Symptomatic: 1. Pain2. Palpable mass3. Nipple discharge• Asymptomatic (mammography screening)1. Densities2. Calcifications

Clincal presentationsPAIN
• Mastalgia / mastodynia• Cyclical / non-cyclical1. Ruptured cyst2. Injury3. Infection4. Some times without any specific lesionNote: only about 10% of breast carcinoma patients present with pain.

• Notable points:1. Masses must be distingusihed from the normal
nodularity of the breast.2. Breast masses usually does not become palpable
until it’s about 2cms in diameter.3. Likelyhood of malignancy in a papable mass
increses with age ---- <40yrs (only 10% of masses are malignant) ---- >50yrs (about 60% of the masses are
malignant)
Clincal presentationsPALPABLE MASSES

• Gains importance only if it’s 1. Spontaneous & 2. Unilateral
Clincal presentationsNipple discharge

• Types of discharges:1. Milky (>prolactin, hypothyroidism, anovulatory
cycle, OCs, M-Dopa, phenothiazines) (Not associated with malignancy)
2. Serosanguinous (most commonly associated with benign lesion)
3. Bloody (most commonly associated with benign lesion – duct papillomas)
Clincal presentationsNipple discharge


Acute mastitis
• Pyogenic infections• Occurs during first few weeks of lactation• Pathogens: 1. Staphylococcus2. Streptococcus

1. Breast mass2. Fever3. Erythematous painful breasts4. If not Tx it may spread to entire breast Complictions:---fibrous scarring---may be mistaken for carcinoma
Acute mastitis

Acute mastitis
During lactation, or at other times with dermatologic conditions that allow cracks and fissures to form in the skin of the nipple, infectious organisms can invade into breast and result in acute inflammation, and this may progress to breast abscess formation (Circle). The most common organism is Staphylococcus aureus. Organization with fibrous scar formation around the abscess can mimic a carcinoma on physical examination, by mammography, and grossly.

Acute mastitis
While breast-feeding the baby, the skin of the breast may become irritated and inflamed. The skin may fissure, predisposing to infection. Acute mastitis typically involves just one breast and is most often caused by Staphylococcus aureus, though other bacterial organisms such as streptococci can produce this condition, with neutrophilic infiltrates microscopically. If untreated by antibiotic therapy, spread of infection and abscess formation can occur.

Granulomatous mastitis
• Chronic non-specific mastitisEtiology:1. Systemic granulomatous disease
(Sarcoidosis, Wegener’s)2. Inections (TB, Fungal)3. Silicone breast implants4. Idiopathic (hypersensitivity to luminal
secretions)

Periductal mastitisRecurrent sub areolar abscesses
“ZUSKA disease”
• Painful erythematous subareolar masses• >90% are smokers (vit-A deficiency)• Seen both in males and females• Not associated with lactation

Subareolar abscess with fistulous opening at the edge of areola
Periductal mastitisRecurrent sub areolar abscesses
“ZUSKA disease”

Pathlogy:1. Keratinization of epithelium extending to an
abnormal depth into the orifices of the nipple ducts.
2. Keratin plugs block the ductal system and causes dilatation & eventual rupture of the ducts.
3. Intense chronic granulomatous inflammatory response develops to ketain spilled into periductal tissue.
Periductal mastitisRecurrent sub areolar abscesses
“ZUSKA disease”

• 3945
Periductal mastitisRecurrent sub areolar abscesses
“ZUSKA disease”
Source: Robbins Pathologic basis of disease, 7th ed. 1125p

Mammary ductectasia• 4th to 7th decade of life.• Usually seen in multiparous women.• NOT assocated with cigarette smoking.Clinically:• Nipple discharge.• Retraction of nipple.• Palpable dilated ducts in the subareolar area.

• Gross: 1-Poorly defined indurated area. 2-Ropyness of the surface. 3-c/s shows dilation of one or more large
ducts containing cheesy inspissated secretions.
Mammary ductectasia

• Microscopically: 1-Dilated ducts with necrotic & atrophic
epithelium 2-Lumen filled with powdery debri and foam
cells 3-Periductal & insterstitial chronic inflammaotry
cell infiltration (Ly, Plas, Histio, Giant cells)
Note: Plasma cell mastitis (when numerous plasma cells are seen)
Obliteration mastitis (when inflammatory scarring obliterates the lumen of the ducts)
Mammary ductectasia

• 3955
Mammary ductectasia
Source: Ackerman’s Surgical Pathology 9th Ed.

FAT NECROSIS
• Usually seen in obese & pendulous breasts• Generally iniciated by trauma or prior
surgery• It presents as painless palpable mass

• 3914
FAT NECROSIS

Gross: 1. Central pale cystic area of necrosis2. Chalky white areas
FAT NECROSIS

FAT NECROSIS
• Lipid filled spaces surrounded by neutrophils, lymphocytes, plasma cells and histiocytes having foamy cytoplasm
• FB type giant cell reaction• Fibrosis & calcifiction

FAT NECROSIS
• Lipid filled spaces surrounded by neutrophils, lymphocytes, plasma cells and histiocytes having foamy cytoplasm
• FB type giant cell reaction• Fibrosis & calcifiction

Non-proliferative breast changes – FCD

Non-proliferative breast changes – FCD
• Form palpable masses• Calcifications• Spontaneous unilateral nipple discharge• They mey disappear after FNAC

There are 3 principle patterns of morphologic changes
1. Cyst formation with apocrine metaplasia2. Fibrosis3. Adenosis
Non-proliferative breast changes – FCD

CYSTS:• Cysts form by dilation and unfolding of
lobule.• Cystic lobules coalesce to form larger cysts.• Cysts lined by flattened atrophic or apocrine
epithelium• Papillary projections• Calcification is common (‘Milk of calcium’)
Non-proliferative breast changes – FCD

Fibrocystic Change (FCC)
This is the gross appearance of fibrocystic changes in the breast. A 1.5 cm cyst is noted here. This can lead to palpation of an ill-defined "lump" in the breast. Sometimes, fibrocystic changes produce a more diffusely lumpy breast.
Source: webpath

This is the histologic appearance of fibrocystic changes in breast. There are cystically dilated ducts, areas of lobules that are laced with abundant fibrous connective tissue (sclerosing adenosis), and stromal fibrosis. There is even a small area of microcalcification seen just to the upper right of center. No atypical changes are seen here.
Fibrocystic Change (FCC)
Source: webpath

Another example of microscopic fibrocystic changes of the breast are shown here. Fibrocystic changes account for the majority of "breast lumps" that are found in women of reproductive years, particularly between age 30 and menopause.
Fibrocystic Change (FCC)
Source: webpath

There is prominent apocrine change of the cells lining the cysts in this example of fibrocystic changes of breast. Note the tall, pink, columnar nature of the epithelial cells. This appearance is benign.
Fibrocystic Change (FCC)
Source: webpath

FIBROSIS: Rupture & release of secretory material into
the adjacent stroma elicit inflammation and fibrosis.
ADENOSIS: Increase in number of acini per lobule ‘Blunt duct adenosis’
Non-proliferative breast changes – FCD

Prominent sclerosing adenosis, one of the features of fibrocystic changes, is demonstrated by the appearance of a proliferation of small ducts in a fibrous stroma. Although it is benign, the gross and mammographic appearance may mimic carcinoma, and it can be difficult to distinguish from carcinoma on frozen section.
Fibrocystic Change (FCC)
Source: webpath

FCC
This mammogram demonstrates a suspicious lesion that could be a carcinoma or just an area of pronounced sclerosis with fibrocystic changes. On biopsy, this was benign.
Source: webpath

PROLIFERATIVE LESIONS

1-without atypia2-with atypia
PROLIFERATIVE LESIONS

Proliferative breast disease without atypia
• Rarely form palpable masses• They are often detected ---radiographically (densities, calcifications) ---in biopsies• Proliferation of ductal epithelium & or stroma
without cellular abnormalities suggestive of malignancy

Entities include:1. Florid epithelial hyperplasia2. Sclerosing adenosis3. Complex sclerosing lesion4. Papillomas5. Fibroadenomas with complex features
Proliferative breast disease without atypia

EPITHELIAL HYPERPLASIA:• Def: presence of >2 cell layers of epithelium• >4 cell layers designates it as moderate to florid
hyperplasia• When they fill the lumen it can be differentiated
from CIS by finding fenestrations are the periphery of the cellular masses.
Proliferative breast disease without atypia

SCLEROSING ADENOSIS:• Increase in # of acini per terminal duct at least
twice the normal.• Normal lobular arrangement is maintained.• Acini are characteristically dilated at the
periphery.• Myoepithelial cells are usually prominent.• Sclerosis• Calcifications are frequently present with in the
lumen of acini.
Proliferative breast disease without atypia

COMPLEX SCLEROSING LESION:• Stellate scar• Centrally entrapped glands in hyalinized stromaComplex sclerosing lesion include:1. Radial scar2. Radial scar related lesion with sclerosing
adenosis, papilloma formation3. Epithelial hyperplasia
Proliferative breast disease without atypia

PAPILLOMAS:• Multiple branching fibrovascular cores• Lined by luminal & myoepithelial cells• Growth occurs within a dilated duct• Epithelial hyperplasia and apocrine metaplasia are
frequently seen• Large duct papillomas are single and situated nearer to
the nipple• Small duct papillomas are multiple and located deeper
within ductal system (more prone for Ca.)
Proliferative breast disease without atypia

These breast ducts demonstrate epithelial hyperplasia. The epithelial cells are multilayered. There is no atypia. Thus, just as with fibrocystic changes such as fibrosis, cysts, and sclerosing adenosis, there is no increased risk for carcinoma. Source: webpath

More florid ductal epithelial hyperplasia of the breast is shown here. There is a slightly increased risk (1.5 to 2 times normal) for breast carcinoma when such changes are present. Source: webpath

• This includes: 1-ADH 2-ALH
Proliferative breast disease with atypia

Proliferative breast disease with atypia - ADH

This is atypical ductal epithelial hyperplasia of the breast. A significantly increased risk (5 times normal) for breast carcinoma occurs with cytologically atypical epithelial hyperplasia.

Proliferative breast disease with atypia - ALH

Source: Robbin’s test book of pathology17th Ed.


END