Embed Size (px)
Citation preview

BLEEDING AND CLOTTING ABNORMALITIES
SUPREET KUMAR

BLEEDING

WHAT IS BLEEDING ???
Bleeding, technically called as HAEMORRHAGING is the loss or escape of blood from the circulatory system… BLEEDING CAN EITHER BE :-

1) EXTERNAL
2) INTERNAL

TYPES OF BLEEDING
A) CLASS I HAEMORRHAGE : 10-15 % of blood volume
B) CLASS II HAEMORRHAGE : 15-30 % of blood volume
C) CLASS III HAEMORRHAGE : 30-40 % of blood volume
D) CLASS IV HAEMORRHAGE : > 40 % of blood volume

CAUSES OF BLEEDING
A)TRAUMA - Lacerations - Incisions - Contusions - Crush injuriesB)UNDERLYING MEDICAL CONDNS - Anatomical defects - Cancer & infections - Disorders of hemostasis - Drugs & Anticoagulation therapy


A DELICATE BALANCE

HEMOSTASIS
HEMOSTASIS is the co-ordinated sequence of events that eventually stops the bleeding..
EFFECTIVE HEMOSTASIS :-
A) Response should be rapid
B) Response should be localised to the region of damage
C) Response should be carefully controlled

MECHANISMS THAT REDUCE BLOOD LOSS
THERE ARE 3 IMP MECHANISMS :-
1) VASCULAR SPASM
2) PLATELET PLUG FORMATION > Platelet adhesion > Platelet release action > Platelet aggregation
3) BLOOD CLOTTING




BLOOD CLOTTING
DEFINITION :
The process of formation of jelly like substance over the ends and within the walls of the blood vessels, with the resultant stoppage of blood flow ..
> Clotting involves a series or a cascade of chemical reactions that culminates in formation of FIBRIN THREADS.
> Clotting involves specific substances known as the CLOTTING FACTORS.

CLOTTING FACTORSNUMBER NAME OF FACTOR SOURCE ACIVATION
I FIBRINOGEN LIVER COMMON
II PROTHROMBIN LIVER COMMON
III THROMBOPLASTIN PLATELET EXTRINSIC
IV CALCIUM IONS PLATELET & BONE
ALL PATHWAYS
V LABILE FACTOR LIVER & PLATELET
EXTRINSIC AND INTRINSIC
VII PROCONVERTIN LIVER EXTRINSIC
VIII ANTIHEMOPHILIAC FACTOR A
LIVER INTRINSIC

CLOTTING FACTORSNUMBER NAME OF THE FACTOR
SOURCE ACTIVATION
IX ANTIHEMOPLHILIAC FACTOR B
LIVER INTRINSIC
X STUART-PROWER FACTOR / THROMBOKINASE
LIVER INTRINSIC AND EXTRINSIC
XI PLASMA THROMBOPLASTIN ANTECEDENT
LIVER INTRINSIC
XII HAGEMAN FACTOR LIVER INTRINSIC
XIII FIBRIN STABILISING FACTOR
LIVER AND PLATELETS
COMMON PATHWAY

THE CLOTTING CASCADECLOTTING is a complex cascade of enzymatic reactions in which each clotting factor activates many molecules of the next one in a fixed sequence…
CLOTTING CAN BE DIVIDED INTO 3 STAGES
1) THE 2 pathways : EXTRINSIC & INTRINSIC Leading to formation of PROTHROMBINASE
2) PROTHROMBINASE converts PROTHROMBIN into enzyme THROMBIN
3) THROMBIN converts soluble FIBRINOGEN into insoluble FIBRIN


SOME FAQs
1) WHAT IS THE NEED FOR 2 PATHWAYS ??
2) WHAT ARE THESE EXTRINSIC AND INTRINSIC PATHWAYS ??
3) WHY ARE THEY CALLED SO ??
4) HOW DOES THE INSOLUABLE FIBRIN FORMED IN THE LAST STEP OF THE CASCADE LEAD TO CESSATION OF BLEEDING ??

CLOT RETRACTION
ONCE the clot is formed
IT plugs the ruptured area of blood vessel & thus stops further bleeding
CLOT RETRACTION is the consolidation of the fibrin clot
AS the clot retracts , it pulls the edges of the damaged vessels close to each other and bridges the gap caused due to the trauma or injury and hence leads to arrest of bleeding

HEMOSTATIC CONTROL MECHANISMS
REGULATION of hemostasis is of optimum importance
The body has an in built mechanism to CONTROL AND REGULATE the process of hemostasis.
1) THE FIBRINOLYTIC SYSTEM
2) PROSTACYCLIN
3) NATURAL ANTI COAGULANTS IN BLOOD

WHY DOESN’T THE BLOOD CLOT WHILE FLOWING THROUGH THE VESSELS ??
1) THE ENDOTHELIAL LINING OF THE VESSEL
2) AXIAL FLOW OF THE BLOOD
3) VELOCITY OF THE BLOOD FLOW
4) NATURAL ANTICOAGULANTS

DYSREGULATION OF THE HEMOSTATIC MECHANISM …
> CLOTTING is a dynamic process that involves AMPLIFICATION and POSITIVE FEED BACK CYCLE.
> DYSREGULATION in the control mechanism can lead to uninhibited clotting and hence a large clot called THROMBUS is formed.
> THROMBUS has the potential to clog the vessels and impair the blood flow that has hazardous consequences.

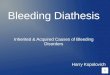
THROMBUS FORMATION
VIRCHOW’S TRIAD
ENDOTHELIAL INJURY
STASIS OF BLOOD
HYPER COAGULABI
LITY

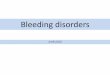
VENOUS THROMBI : INITIAL PHASE

MASSIVE THROMBUS IMPAIRING BLOOD FLOW

VESSEL OCCLUDED BY THE THROMBUS

AN APPROACH TO BLEEDING DISORDERS 1) HISTORY
* Site of bleeding * Duration of bleeding * Precipitating factors of the bleeding * History of previous operative procedures * Family history * History of drug intake
2) EXAMINATION
* Look for BRUISES,PURPURA,TELANGIECTASIA * Examination of joints ( HAEMOPHILIA ) * stigmata of liver diseases * SPLEENOMEGALY ( indicates thrombocytopenia )

MANAGEMENT OF BLEEDING DISORDERS
INVESTIGATIONS TREATMENT

INVESTIGATIONS IN CASE OF A BLEEDING DISORDER
* PLATELET COUNT* BLEEDING TIME* CLOTTING TIME* PROTHROMBIN TIME* ACTIVATED PARTIAL THROMBOPLASTIN TIME* FIBRINOGEN LEVEL* CLOT RETRACTION TIME* ACTIVATED CLOTTING TIME* PLASMA THROMBIN TIME

TREATMENT MODALITIES
* TREATMENT IS DEPENDENT ON THE TYPE OF BLEEDING DISORDER
* THE MAIN AIM OF THE TREATMENT IS TO REPLACE THE COMPONENT OR THE FACTOR WHOSE DEFICIENCY LEADS TO BLEEDING

AN APPROACH TO CLOTTING DISORDERS
1) HISTORY
* Careful history taking is important for evaluation * Family history should be enquired about
2) EXAMINATION
Careful evaluation of the signs and symptoms
* Pain * swelling * Redness at the site and other relevant symptoms

INVESTIGATIONS FOR ABNORMAL CLOTTING OR THROMBOTIC DISORDERS
1) BLOOD EXAMINATION
* D- DIMER* CBC* COAGULATION STUDIES BT,CT,APTT,FIBRINOGEN* LIVER ENZYMES
2) IMAGING STUDIES
* DOPPLER* ULTRASOUND* DUPLEX AND THERMOGRAPHY

TREATMENT MODALITIES FOR ABNORMAL COAGULABILITY
ANTI-THROMBOTIC DRUGS ARE THE DRUGS USED FOR TRAETMENT OF HYPER COAGULABILITY
ANTI THROMBOTIC DRUGS
ANTI PLATELET DRUGS
ANTI COAGULANTS
FIBRINOLYTIC AGENTS

ANTI PLATELET DRUGS
1) ASPIRIN
2) THIENOPYRIDINES
* CLOPIDOGREL * TICLOPIDINE
3) DIPYRIDAMOLE
4) GP II b / III a RECEPTOR ANTAGONIST * ABCIXIMAB * TIROFIBAN

ANTI COAGULANTS
1) HEPARIN
2) LMW HEPARIN
3) FONDAPARINUX
4) DIRECT THROMBIN INHIBITOR * LEPIRUDIN * BIVALIRUDIN * ARGATROBAN

FIBRINOLYTIC DRUGS
1) STREPTOKINASE
2) UROKINASE
3) ALTEPLASE
4) TENECTEPLASE
5) RETEPLASE
6) ANISTREPLASE