Embed Size (px)
DESCRIPTION
Rare Bleeding Disorders. Dr Joseph MAKDESSI TYR 31-07-2010. Clotting factor deficiencies (I, II, V, combined V & VIII, VII, X, XI, XIII) Platelet function disorders (e.g. Glanzmann Thrombasthenia , Bernard- Soulier Syndrome) - PowerPoint PPT Presentation
Citation preview


Rare Bleeding DisordersDr Joseph MAKDESSI
TYR 31-07-2010


• Clotting factor deficiencies (I, II, V, combined V & VIII, VII, X, XI, XIII)
• Platelet function disorders (e.g. Glanzmann Thrombasthenia, Bernard-Soulier Syndrome)
• Increase in identified number of people with rare clotting factor deficiencies or platelet function disorders (WFH)



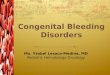
GPIb-IX-V Complex
• In 1948 Bernard & Soulier described a young man with a severe bleeding disorder, prolonged BT, thrombocytopenia and large platelets
• BSS platelets fail to aggregate with ristocetin or adhere to blood vessel subendothelium
• BSS platelets fail to express major membrane-associated glycoproteins: GPIbα, GPIbβ, IX and V
• GPIb-IX-V complex is the receptor for Von Willebrand factor plus other adhesive proteins , and receptors, and thrombin

Why the clinical effect
• Macrothrombocytopenia: Megakaryocyte defects in the formation of demarcation membranes and proplatelet formation
• Clinical bleeding: failure of platelets to adhere to VWF ligands in damaged vessel wall subendothelium

Syndromes associated with GPIb-IX-V
Bernard-Soulier syndrome:
– Autosomal recessive– Macrothrombocytopenia– Deficient aggregation with ristocetin– Normal vWF multimeric pattern in plasma– Loss-of-function mutations

Syndromes associated with GPIb-IX-V
Platelet- type vWD
– Autosomal dominant– Thrombocytopenia– Enhanced aggregation with ristocetin– Loss of HMW vWF multimers from plasma– Gain-of-function mutations


Dense Granule deficiency• Mild to moderate mucocutaneous bleeding• Non syndromic• Associated with pigment abnormalities: – Hermansky-Pudlak syndrome– Chediak-Higashi syndrome– Griscelli syndrome
• Associated with other inherited disorder– familial myeloid leukemia
• Combined α,δ-granule deficiency• Acquired deficiencies

Hermansky – Pudlak syndrome• Autosomal recessive • Presentation:
– δ-granule deficiency– Oculocutaneous albinism– Pulmonary fibrosis– Granulomatous colitis
• Defects in three cytoplasmic organelles:– Platelet dense granules– Melanosomes– lysosomes

MYH9-Related Disorders• Autosomal dominant disorders of
macothrombocytopenia, platelet dysfunction, and leuKocyte inclusions– May-Hegglin Anomaly– Sebastian syndrome– Fechtner syndrome– Epstein syndrome
• Clinical aspects:– Mild bleeding diathesis– Renal disease– Hearing loss– cataracts

Why The Clinical Effects
• Macrothrombocytopenia: disordered cytoskeleton affecting proplatelet formation
• Platelet dysfunction: abnormal cytoskeletal reorganization and shape change
• Other organ dysfunction may be related to defects in:– Epithelial cell organization– Cell-matrix adhesion– Cell migration and differentiation– Tissue morphogenesis

Inherited Platelet Disorders
• Study of these rare platelet disorders:– Has identified specific molecular defects– Reveals the physiology of the normal
• Understanding the basic mechanisms:– May explain unusual syndromic associations– Improves our understanding of more common
diseases– May help to identify new therapeutic targets

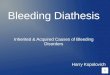
Glanzmann Thrombasthenia (GT)
• It was first described by Glanzmann in 1918 as hereditary hemorrhagic thrombasthenia
• It is an autosomal, recessive, bleeding syndrome affecting megakaryocyte lineage
• It is characterized by lack of platelet aggregation
• It is moderate to severe disorder with mainly mucocutaneous bleeding

Cell Biology
• In GT, platelets fail to aggregate in response to all natural agonists,although they undergo normal shape change
• Thrombasthenic platelets can also adhere to exposed subendothelial matrix and undergo exocytosis of storage granules
• The inability of the platelets to bind these adhesive proteins explains the platelet phenotype in GT

Epidemiology
• GT is a rare disease with an estimated prevalence of 1/million
• The disease is known to have a higher prevalence in communities where consanguinity is common
• Examples of these communities include: Indians, Iranians, Iraki Jews, Palestinian and Jordanian Arabs, French gypsies
• GT related bleeding is more common in females, probably due to menorrhagia

Inheritance
• GT is an autosomal recessive bleeding disorder
• Heterozygote individuals are usually asymptomatic carriers
• Heterozygote couples may have a homozygote offspring who will have moderate to severe disease

Hematological Work Up
• CBC, Blood group, Ferritin, aPTT, PT, vWF Ag, RiCof
• If abnormal : Specific Coagulation Assays
• If normal: suspect platelet dysfunction

Platelet Function Tests
• Prolonged BT or abnormal PFA 100 closure time• Defective aggregation with ADP, thrombin,
epinephrin or collagen alone or in combination• Defective clot retraction test• Deficiency of αIIbβ3 in new patients should
always be demonstrated by specific monoclonal antibodies using flow cytometry

Transfusion in GT
• Patients with GT may have frequent transfusions throughout their lives
• They may be more exposed to transfusion complications mainly: transmission of viral diseases and Bacteria.
• Immunological complications:– Allergy and anaphylaxis– Platelet isoantibody formation and refractoriness

• To avoid these complications the following requirements should be considered whenever possible:– Pathogen inactivated platelets– Leucoreduced cellular blood components– Reduction of plasma volume in RBCs and Platelets
concentrates by the use of additive solutions– Use of HLA, HPA matched platelets, or cross matched
platelets whenever platelet allo-immunization and refractoriness develop