Embed Size (px)
DESCRIPTION
Biological psychiatry is an interdisciplinary approach to psychiatry that aims to understand mental disorder in terms of the biological function of the nervous system. This book is strongly recommended for all researchers and professionals wishing for an authoritative, easy to digest and accessible review of the latest advances and conceptualizations in the field.
Citation preview



Biological PsychiatryThird Edition


Biological PsychiatryThird Edition
Michael R. Trimble, MD, FRCP, FRCPsychProfessor of Behavioural Neurology, Institute of Neurology,
Queen Square, London UK
Mark S. George, MDDistinguished Professor of Psychiatry, Radiology and Neurosciences,
Medical University of South CarolinaDirector, Brain Stimulation Laboratory
Director, Center for Advanced Imaging Research (CAIR)MUSC Director, SC Brain Imaging Center of Excellence
Ralph H. Johnson VA Medical Center, Charleston, SC, USA
A John Wiley & Sons, Ltd., Publication

This edition first published 2010, John Wiley & Sons Ltd.
Wiley-Blackwell is an imprint of John Wiley & Sons, formed by the merger of Wiley’s global Scientific, Technical andMedical business with Blackwell Publishing.
Registered office: John Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK
Other Editorial Offices:9600 Garsington Road, Oxford, OX4 2DQ, UK111 River Street, Hoboken, NJ 07 030–5774, USA
For details of our global editorial offices, for customer services and for information about how to apply for permission toreuse the copyright material in this book please see our website at www.wiley.com/wiley-blackwell
The right of the author to be identified as the author of this work has been asserted in accordance with the Copyright,Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in anyform or by any means, electronic, mechanical, photocopying, recording or otherwise, except as permitted by the UKCopyright, Designs and Patents Act 1988, without the prior permission of the publisher.
Wiley also publishes its books in a variety of electronic formats. Some content that appears in print may not be available inelectronic books.
Designations used by companies to distinguish their products are often claimed as trademarks. All brand names andproduct names used in this book are trade names, service marks, trademarks or registered trademarks of their respectiveowners. The publisher is not associated with any product or vendor mentioned in this book. This publication is designedto provide accurate and authoritative information in regard to the subject matter covered. It is sold on the understandingthat the publisher is not engaged in rendering professional services. If professional advice or other expert assistance isrequired, the services of a competent professional should be sought.
The contents of this work are intended to further general scientific research, understanding, and discussion only and arenot intended and should not be relied upon as recommending or promoting a specific method, diagnosis, or treatment byphysicians for any particular patient. The publisher and the author make no representations or warranties with respect tothe accuracy or completeness of the contents of this work and specifically disclaim all warranties, including withoutlimitation any implied warranties of fitness for a particular purpose. In view of ongoing research, equipmentmodifications, changes in governmental regulations, and the constant flow of information relating to the use of medicines,equipment, and devices, the reader is urged to review and evaluate the information provided in the package insert orinstructions for each medicine, equipment, or device for, among other things, any changes in the instructions or indicationof usage and for added warnings and precautions. Readers should consult with a specialist where appropriate. The factthat an organization or Website is referred to in this work as a citation and/or a potential source of further informationdoes not mean that the author or the publisher endorses the information the organization or Website may provide orrecommendations it may make. Further, readers should be aware that Internet Websites listed in this work may havechanged or disappeared between when this work was written and when it is read. No warranty may be created orextended by any promotional statements for this work. Neither the publisher nor the author shall be liable for anydamages arising herefrom.
Library of Congress Cataloguing-in-Publication Data
Trimble, Michael R.Biological psychiatry / Michael R. Trimble, Mark S. George. – 3rd ed.
p. ; cm.Includes bibliographical references and index.ISBN 978-0-470-68894-6
1. Biological psychiatry. I. George, Mark M. II. Title.[DNLM: 1. Biological Psychiatry – methods. 2. Brain – physiology. 3. Mental Disorders – physiopathology.
WM 102 T831b 2010]RC341.T73 2010616.89 – dc22
2009053116
ISBN: 978-0-470-68894-6
A catalogue record for this book is available from the British Library.
Typeset in 10/12 and Palatino-Roman by Laserwords Private Limited, Chennai, IndiaPrinted in Singapore by Markono Print Media Pte Ltd, Singapore
First Impression 2010
Cover design by Jim Wilkie. Portrait of Hippocrates inspired by his words, ‘Men ought to know that from the brain, andfrom the brain only, arise our pleasures . . . as well as our sorrows . . . and tears’ as quoted in ‘The Soul in the Brain’ byMichael Trimble, 2007.

We dedicate this book to our late friend, mentor and scholar Paul MacLean.


Contents
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xi
Quotations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xiii
Preface to the First Edition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xv
Preface to the Second Edition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xix
Introduction and Preface to the Third Edition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xxi
1 Principles of Brain Function and Structure: 1 Genetics,Physiology and Chemistry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1Genetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1Brain chemistry and metabolism . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8The metabolism of glucose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Proteins and fatty acids . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Cell membranes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Synapses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Receptors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Neurones . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Neurotransmitters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Interrelationships among transmitters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Transmitter dispersal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29CNS inflammation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
2 Principles of Brain Function and Structure: 2 Anatomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31The neuroanatomy of emotion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32Individual anatomical structures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41Ascending and descending limbic-system connections . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53Macrosystems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55The basal ganglia and the re-entrant circuits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57The ventral striatum and ‘limbic striatum’ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58The ascending cholinergic systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60Cortical regions of interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60The cerebellum . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63

viii Contents
3 Important Brain–Behaviour Relationships . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65Important anatomical structures for understanding behaviour . . . . . . . . . . . . . . . . . . . . . . . 68Some specific behaviours . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74Limbic lobe disorders in a clinical context . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77Re-entrant circuits in a clinical context . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78The frontal lobes in a clinical context . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79Laterality . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
4 Classifications and Clinical Investigations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83Signs, symptoms, syndromes and disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84Classification in psychiatry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84Clinical investigation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 87
5 Personality Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113General introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113Introduction to the concept of personality . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113Genetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 118Somatic variables . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 121Metabolic and biochemical findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 121Neurophysiological and neurological data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 123Some outstanding issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 127
6 Anxiety Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 131Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 131Genetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 134Somatic variables . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 135Metabolic and biochemical findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 135Neurochemical investigations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 137Neurophysiological and neurological data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 140Imaging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 140Obsessive–compulsive disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 142Post-traumatic stress disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 143Some outstanding issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 144
7 The Schizophrenias . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 147Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 147Genetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 150Somatic variables . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153Metabolic and biochemical findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 154Neurochemical investigations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 159Neurophysiological and neurological data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 164Some outstanding issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 176
8 Affective Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 183Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 183Genetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 184

Contents ix
Metabolic and biochemical findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 186Neurochemical investigations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 198Neurophysiological and neurological data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 200Some outstanding issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 209
9 The Addictions and Disorders of Motivation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 215Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 215Disorders of motivation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 216Conditioning . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 217Genetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 219Metabolic and biochemical findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 221Neurophysiological and neurological data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 223Some outstanding issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 228
10 Epilepsy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 231Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 231Prevalence and clinical characteristics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 231Classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 231Genetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 235Symptomatic epilepsy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 235Biochemical findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 236Investigation and differential diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 237Psychiatric disorders in epilepsy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 237Cognitive deterioration and epilepsy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 254Some outstanding issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 255
11 The Dementias . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 257Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 257Definition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 257Prevalence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 258Diagnosis and classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 258Alzheimer’s disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 259Dementia of frontal-lobe type . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 267Focal cortical atrophies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 268Dementia with Lewy bodies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 268Vascular dementias . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 269Other forms of dementia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 271Further causes of dementia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 275Some outstanding issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 275
12 Biological Treatments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 281Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 281Pharmacology: pharmacokinetics and pharmacodynamics . . . . . . . . . . . . . . . . . . . . . . . . . . 281Antidepressants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 284Antipsychotic drugs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 296Anxiolytics and hypnotics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 304Beta-Adrenergic blockers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 308Lithium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 308

x Contents
Anticonvulsants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 310Drugs for the treatment of dementia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 316Medications for the addictions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 317Brain-stimulation therapies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 318Sleep-deprivation therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 329
13 Epilogue: Progress toward a Neuroanatomically, Biological-psychiatricallyInformed Classification Scheme in Psychiatry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 331
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 335
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 395

Acknowledgements
The editors wish to acknowledge the following people for their helpful comments on varioussections of the manuscript:
Andrea Cavanna, Tim Crow, Ray Dolan, Mark Edwards, Paul Johns, Eileen Joyce, Marco Mula,Karl Friston, Nick Wood.
Professor Trimble acknowledges his late friend and mentor Dr Lennart Heimer who has givenhim many of the images used in this text. He is also grateful for the contributions of Dr Scott Zahmand Gary van Hoesen. He thanks his wife Dame Jenifer for her continuing support to his writingactivities.
Dr George acknowledges his wife, Eloise, and children, Laura and Daniel, who have allowedhim to merge his hobby (brain and behavior) with his work (clinical neuroscience) and toleratedthe time away, Dr Edmund Higgins, for his help with several of the illustrations and figures inthis edition, Dr James Ballenger, for creating the combined residency program in neurology andpsychiatry, and encouraging him to pursue research and further training, and Professors MichaelTrimble and Robert Post, his research fellowship advisors who opened up so many doors and haveproved such good colleagues and mentors through the years.
Both editors are grateful for the hours of work that Jackie Ashmenall has put into preparationof the final manuscript and helping with the editorial process.


Quotations
Mental disorders are neither more nor less than nervous diseases in which mental symptomspredominate, and their entire separation from other nervous diseases has been a sad hindranceto progress.
Henry Maudsley (1870, p.41)
Le Gros Clark has also drawn attention to the difficulty of judging what constitutes normalityin some of these old rhinencephalic regions. It is not inconceivable that a pathological changein one or the other region has been overlooked in schizophrenic brains. In the text booksof neurology and psychiatry of my student days chorea, parkinsonism and related motordisorders were treated as neuroses. When the first discoveries of their organic nature weremade, there was surprise bordering on disbelief that circumscribed lesions, for instance inthe substantia nigra and periaqueductal grey matter, should give rise to massive neurologicaland psychopathological syndromes. Such experiences should make us cautious before wegive a final verdict that there is no pathological change in schizophrenic brains.
Professor A. Meyer, writing in the early 1950s


Preface to the First Edition
In the last thirty years there has been a remarkable explosion of knowledge in medicine, andpsychiatry is no exception. Much of the progress is related to the exploration of the biologicalfoundations of the discipline, and this may be referred to as biological psychiatry. It is often said,quite mistakenly, that psychiatrists are unscientific and that psychiatry has made little progressover the years, and in any case lacks an adequate foundation of knowledge. In reality, psychiatryas a discipline is one of the more critical of all in medicine, continually questioning not only its database, but also its fundamental methodological principles. Further, it has a long and distinguishedhistory of progress, a point of departure for this book.
Thus, Chapter 1 outlines the development of psychiatry from its early origins, noting that itis one of the oldest medical specialties. The emphasis of most practitioners has been to elucidateany underlying pathology that is related to psychopathology, an endeavour that has been highlysuccessful. Although much of this may be more appropriately referred to as neuropsychiatry, itshould be recognized that, for example, in the last century, psychopathologists were in the mainneuropathologists and vice versa. The reduction in morbidity and mortality of psychiatric patientsthat followed discovery of the cause and treatment of general paralysis of the insane (GPI) wassubstantial, and the progress that was made in the first half of this century in relation to treatmentssuch as electroconvulsive therapy had a dramatic impact on the lives of thousands of patientsotherwise condemned to long-term institutionalization.
Such progress is often ignored when discussing psychiatry, and emphasis is often given to analternative stream of thought, one of psychological theorizing, which arose on the neo-romantictide of the turn of the century. This culminated in the psychoanalytic movement, which for aconsiderable time became synonymous with psychiatry. The point is made, however, that this erahas provided psychiatry with a legacy that it does not deserve, the main trend of the tradition forover 2000 years being medical and neuropathologically based.
The position today is that these psychological theories of pathogenesis have been overtaken by awealth of neurochemical and neuropathological hypotheses and findings, especially with regardsto the major psychoses. Further, in addition to using knowledge accumulated in cooperationwith other disciplines, biological psychiatry now seeks an understanding of psychopathologyusing theories and findings often based on clinical observations of patients and their effectivetreatment with biological remedies. Hence, the importance of the neurochemical era, ushered inby the psychopharmacological discoveries of the 1950s. These have given us not only a completelynew image of the brain to work with, but also have allowed a more complete understandingof underlying functional and structural changes of the brain that accompany psychiatric illness.Functional, a misused word in the clinical neurosciences, once again may be used in its originalsense, to designate a physiological disturbance, rather than as an epithet for ‘psychological’.

xvi Preface to the First Edition
Indeed, with our present knowledge the distinction between ‘organic’ and ‘functional’ melts away,stripped of its Cartesian dualism.
In spite of such progress, the very concept of biological psychiatry still meets with scepticism inthe eyes of many. As we approach the turn of the next century, there may well be a revival of a finde siecle phenomenon, in which the recent gains will become submerged and lost in a quagmire ofnew, old or revived psychological theorizing. The reasons for this are not difficult to understand.Thus, biological psychiatry is a complicated subject, requiring in particular an intimate knowledgeof the central nervous system. Many find such knowledge hard to grasp, and the very pace ofdiscoveries is often bewildering. The principles rely to some extent on diagnosis and measurementof biological variables, yet in the clinical area these are often ignored, thought unnecessary orcounterproductive. This is in spite of them being fundamental to medicine, and psychiatry being amost important branch of medicine. The latter fact is often trivialized, many, especially of the laypublic, but also sadly some practitioners, preferring to deny the medical roots of psychiatry, but indoing so confusing it with psychology.
Biological treatments, in spite of their obvious and proven efficiency, are criticized. However,the psychopharmacological revolution has given psychiatrists, not for the first time, powerfulremedies. The days when multitudes of patients suffered intensely because of lack of adequatetreatment are forgotten, and false arguments that compare and contrast psychotherapy to biologicaltreatments are constructed. It is assumed that the use of such treatments implies a lack of interestin patients, and that somehow the doctor is less than adequate for prescribing them. However,in medicine it is obvious that often several approaches to patient care are appropriate and canbe applied simultaneously if required. The neurologist or the chest physician know the value ofphysiotherapy and when it is applicable, and likewise the psychiatrist may recognize the valueof other treatments for his patients, in addition to the biological ones. However, the neurologistwould not hesitate to prescribe medication to his patient with Parkinson’s disease, or the chestphysician antituberculous remedies to a consumptive. Indeed, with tuberculosis, the remediesof 50 years ago, which relied mainly on changes in environment and the passage of time, havebeen superseded by more effective modern treatment regime, as is the case with many psychiatricillnesses.
One challenge for biological psychiatry is to unite information we now have regarding functionalchanges in the brain in psychopathology with that which we know about brain – behaviourrelationships and brain structure. The latter was of great interest to the neuropsychiatrists of thelast century, and has recently been an area of much research, but often referred to as behaviouralneurology. This discipline has developed rapidly in the United States of America, and may cometo be seen as a neurological discipline if its relevance for psychiatry is not acknowledged, and theessential value of examining patients with known structural disease for helping to understand thecourse and development of psychopathology is not appreciated.
In this text I have reviewed a number of key areas of importance for biological psychiatry. Astrong emphasis has been placed on the work of Jaspers, and the fundamental distinction betweenillness, which is related to a process, and development. The whole area of personality disordersis one of continuing disagreement, although as emphasized in Chapter 7 neurochemical andneuropathological substrates of at least some personality traits are being uncovered. However,it is arguable to what extent psychiatrists are an appropriate professional group to deal withpersonality disorders generally, and their ready acceptance of this task in the past has led to agreat deal of criticism, not the least being the failure to influence behaviour patterns in wayswhich the then-accepted theories, predominantly psychoanalytic, predicted they should changewith treatment. An alternative argument would be that psychiatrists should deal with illness, notpersonality problems, for which latter group other agencies in society are readily available as asource of help.

Preface to the First Edition xvii
The main diagnostic system used in this book is that of the American Psychiatric Association’sDSM III. However, as noted in Chapter 2, classification is in a constant process of change, and isnot immutable. However, the DSM III is likely to dominate psychiatric research for many years tocome – hence the emphasis. The reader will quickly note the profusion of different terms used inthe book for similar states, many of which do not even conform to the alternative ICD system. Thisis because in quoting papers, the original patient designation used by the authors is selected. Manyof the investigations were carried out prior to the introduction of the DSM III, but reclassificationof patients would be an inappropriate exercise. It is hoped that the introduction of such systemsas the DSM III, and soon the DSM IIIR and DSM IV, will lead to more uniformity of patientsincluded in research populations, making a reviewer’s task easier and increasing the validity ofany findings.
It is hoped that the two chapters on neurochemistry and neuroanatomy will be of interest,and give an up-to-date account of the state of knowledge. These fields are moving so rapidlythat information has a danger of soon being out of date. Nonetheless, it is hoped that areas ofimportance for biological psychiatry are adequately outlined, and that their inclusion, essential forthe text, will increase the reader’s interest in exploring some of these areas further.
The main clinical chapters cover the major psychopathologies, notably affective disorders(Chapter 9) and schizophrenia (Chapter 8). Structural disorders of the limbic system are discussedseparately (Chapter 6), and individual chapters are devoted to dementia (11) and epilepsy (10). Thisfollows some other psychiatric texts, including in the contents mainly information on the majorpsychoses, although the neuroses are discussed where relevant (Chapters 7 and 9). These areas ofpsychopathology have been chosen to reflect subjects of relevance to biological psychiatry, but alsorelate to the author’s interests. Dementia and epilepsy are of growing importance. Patients withdementia, from those with dementia praecox to those with the disorders identified by Alzheimerand Pick, are often assessed and managed by psychiatrists. The recent neurochemical findings,especially in Alzheimer’s disease and the possibility of replacement therapy to hold the conditionfor a few years at least have encouraged renewed interest in this area. Epilepsy is included, in partreflecting the author’s own area of special interest, but mainly because of the very close relationshipbetween epilepsy and psychiatry that has existed for many years. Epilepsy has a great deal to teachus about the CNS, about psychopathology and about patient management.
There are many topics missing from this book, which no doubt will lead to comment. Forexample, not discussed are conditions such as alcoholism and the addictions, and eating disorders,the biological bases for which are becoming clarified, and relevant neurochemical and neuropatho-logical findings have been reported. Inevitably, the final size of the volume, as well as the author’spersonal interests, are responsible for the exclusions. In addition, this volume is a companion tomy earlier book Neuropsychiatry (Trimble, 1981a). Although there is some overlap, here the data ondementia, epilepsy and biological treatments have been rewritten and updated, and some subjectsthat may interest the reader, but not included here, may be found there.
Biological psychiatry is such a rapidly advancing field, and the number of papers of relevance sovast, that much selectivity has gone into the choice quoted in this book. Undoubtedly there will bethose disappointed that their paper is not quoted, and others who will point to a missing referenceof some negative finding not substantiating a claim made in the text. To a large extent I havequoted work that has either been independently replicated or seems to be of interest to the themeof the topic at hand. In several areas, for example the neuropathology of schizophrenia, all thefindings consistently show some changes, but there is not exact replication as to the precise changesin all studies. Nevertheless, the combined findings add up to an extremely important conclusionwith regards to schizophrenia, namely the obvious, but until recently ignored, relationship of thecondition to structural brain lesions.

xviii Preface to the First Edition
It is hoped that the text will provide an informative data base for those psychiatrists interestedin exploring the biological foundations of their discipline further. It may help to stimulate theinterests of students wanting to explore one of the most exciting areas of current research inpsychiatry, and may provide those active in the field with ideas for future investigations that willincrease our knowledge even further.
Michael R. TrimbleLondon, 1987

Preface to the Second Edition
It is nearly a decade since I started to write the first edition of this book, and the progress inbiological psychiatry since that time has been truly remarkable. Of course many of the piecesfor this progress were in place at that time, but the speed of progress, and the studies thathave been completed have been, in some areas, awesome. I refer in particular to advances inneuroanatomy and neurochemistry, to progress in genetics, and to the development of highresolution neuroimaging techniques. The elegance of some of the methods, their complexity, andyet their ability to answer for us questions of principal relevance for the discipline would have leftour forefathers breathless.
Attempting to harness such progress, and to interpret the findings from an ever expandingdatabase has not been a simple task. Students over the past few years have asked me if, andwhen, I would be writing a second edition of this book, and I had carefully avoided any decisionsor deadlines. However, it was rapidly becoming clear around 1993 that revision was essential,especially for those faithful readers who were still buying copies of the first text. The newclassifications of psychiatric illness (ICD 10: DSM IV) perhaps became the final goad to action,although the wish to provide a helpful guide to the technological advances was also important.
As with the first edition, one major problem has been what to leave out. I can only apologise,once again if some researcher is aggrieved because I have not quoted him or her, and if another isupset because I have selectively quoted, and not cited all references available on a particular topic.However, for a single authored book, to achieve its aim, some selectivity is essential, and withoutit, the text would become quite unwieldy.
However, equally difficult has been the problem of what to remove from my first edition.Marrying new text, with something written several years ago is difficult enough, sacrificing textwith scissors can be positively painful. Particularly since much of what went into the first editionstill forms part of the corpus of the subject, and has become the foundation of later investigationsand data.
I hope that, these faults notwithstanding, the final product is readable and informative. Itwill succeed for me if it stimulates even one student to find the richness and excitement ofneurobiological research which has so stimulated me over the years. For others, it may providea spur to further research in a particular area, to enhance or refute a conclusion of mine orsome investigator I have quoted. Once again I am grateful to colleagues and patients alike whohave helped me understand some of the complexities of human behaviour, and the relevance ofbiological psychiatry for contemporary medicine.
M.R.T.London, 1995


Introduction and Prefaceto the Third Edition
‘Biological psychiatry’ may have a modern ring to it, but the idea of seeking naturalistic origins forpsychiatric disorders is part of a long-standing intellectual tradition. Hippocrates, in his writingson ‘The Sacred Disease’, the name given by the Greeks to epilepsy, pointed out that it was nomore sacred than any other disease, and ‘has a natural cause from which it originates like otheraffections’ (Adams, 1939, p. 355). He continues with one of the more quoted historical remarksthat ‘men ought to know that from nothing else but thence [from the brain] comes joys, delights,laughter and sports, and sorrows, griefs, despondency and lamentations . . . And by the sameorgan we become mad and delirious, and fears and terrors assail us . . . ’ (p. 366).
It is generally accepted that with a few notable exceptions such as Galen, and the contributionsof the Arab world, for the next 1300 years medicine abandoned any semblance of a scientificapproach, and retreated under the combined influences of theology and demonology.
The 17th century saw a revival of the idea that the brain was the seat of many mental diseases, andthe rudiments of present-day localization theories can be found in the writings of several authors,such as Thomas Willis (1671–1675), the founder of neurology and one of the first physicians of thenew enlightenment to clearly equate mental disorders with brain diseases.
Rene Descartes (1596–1650), the 17th-century philosopher, skillfully, with deductive reasoning,was able to philosophically separate the unextended mind from the extended body. While thisallowed examination and speculation about the brain and its relationship to sensation andmovement to progress relatively unfettered from the religious domination over anything that hadto do with the human mind, and hence the soul, it set the trend for three centuries in whichpsychological theories of mental illness vied with the biological.
The 19th century saw a rapid expansion of knowledge in medicine, and a continued growth ofthe anatomico-clinical method. Such an approach was seen especially with the attempts to localizemental functions in the brain. However, localization theories such as we are familiar with todaydid not emerge until the rise of the phrenological movement, the greatest exponents of which wereFranz Joseph Gall (1758–1828) and his collaborator Johann Caspar Spurzheim (1776–1832). Thebrain was conceived of as being composed of many different organs, which could be palpatedthrough the scalp. This last contention was the downfall of phrenology, since it quickly becametaken up by all sorts of charlatans and fell into disrepute. Nonetheless, Gall was the originator ofmodern localization theories and, for example, suggested the presence of a speech centre, a conceptrevived later by Paul Broca (1824–1880). The unfortunate overdue attention to the importanceof the cerebral cortex for mentation, with neglect of subcortical structures, represents a state ofaffairs that persisted until recently (see below). The studies of Broca also initiated a literaturewhich emphasized lateralization. Broca in fact was unable to explain the coincidence of aphasiaand right-sided hemiplegia, although, after consideration of the facts, the English neurologist JohnHughlings Jackson (1835–1911) referred to the left side of the brain as the ‘leading hemisphere’

xxii Introduction and Preface to the Third Edition
for speech, and concluded that there were important differences in the functions of the two brainhemispheres. Laterality differences in relationship to psychopathology, an area of study nowactively pursued, underwent a revival in the 1960s with the work of Pierre Flor-Henry on psychoticpatients with epilepsy.
Hughlings Jackson thoughtfully put forward four key ideas of brain function, which were theevolution of nervous functions, the hierarchy of functions, the negative and positive symptomsof dissolution and the distinction between local and uniform dissolution. For him, the nervoussystem was seen as developing both in space and time, and was not the static organ of thepathologist’s specimen. Further, it was hierarchically organized, not merely a collection of reflexes.With any lesion there are two effects, one due to the destruction of tissue, resulting in the negativesymptoms, and the other due to release of subjacent activity of healthy areas of the brain, causingpositive symptoms. He discussed mental disorders and noted that in all cases of insanity theprinciple of dissolution, the level of evolution that remains and the positive and negative elementsneed to be considered. In a paper called ‘The Factors of the Insanities’ he stated, ‘In everyinsanity there is morbid affection of more or less the highest cerebral centres . . . [they] are outof function, temporally or permanently from some pathological process’ (Taylor, 1958, vol. 2, p.411), a statement relevant for biological psychiatry. His use of the terms ‘positive’ and ‘negative’symptoms, as a reflection of a mechanism of nervous-system function equally applicable to awhole range of neuropsychiatric conditions, stands in contrast to the more recent reintroductionof these expressions into psychiatry, with a more-or-less descriptive use, and largely restricted toschizophrenia. The reintroduction of Hughlings Jackson’s terminology into psychiatry, and thecontinued awareness that strict localization hypotheses have not uncovered the essential linksbetween the brain and behaviour, has seen a renewed interest in Jacksonian ideas.
On the continent, Wilhelm Griesinger’s (1817–1868) book, Mental Pathology and Therapeutics,was published in Berlin in 1845, and translated into English in 1867. Griesinger’s thesis was thatmental illness (insanity) is only a symptom of a disordered brain, and the brain is the organ thatmust be diseased in mental illness. He stated: ‘ . . . we therefore primarily, and in every case ofmental disease, recognize a morbid action of that organ’ (Griesinger, 1867, p. 1). An importanttenet, reflecting the essential nature of biological psychiatry, is: ‘Insanity being a disease, and thatdisease being an affection of the brain, it can only be studied in a proper manner from the medicalpoint of view’ (p. 9).
Other substantial contributions of German psychiatry in this era come from Theodore Meynert(1833–1892), Carl Wernicke (1848–1905), Karl Kahlbaum (1828–1899) and Emil Kraepelin(1856–1926). Meynert’s work stimulated a whole generation of successors, including SigmundFreud (1856–1939). Meynert contrasted the functions of the cortex with those of the brainstem,postulating a neurophysiological foundation of the ego based on the principles of associationistpsychology and the presence of different cortical ‘centres’. Wernicke is well known for hisaphasiology, and his contributions to the study of chronic alcoholism are recognized in theeponym Wernicke–Korsakoff syndrome. Kahlbaum insisted on the clinical method, and hisattempts to clarify disease classification led to the delineation of catatonia. Later, Kraepelindeveloped his nosological scheme, which has had such a profound influence on modern psychiatry.
Although German psychiatry, especially the contributions to biological psychiatry (in that era,more properly referred to as ‘neuropsychiatry’), was especially dominant in the second half of the19th century, developments in France were somewhat earlier. Phillipe Pinel’s (1745–1826) influencewas profound, and like many others he had misgivings about philosophy and metaphysics.
Another very important figure in French psychiatry was A.L.J. Bayle (1799–1858). The late effectsof syphilis, dementia paralytica, were frequent causes of mental illness in patients admitted topsychiatric hospitals. Bayle, in his doctoral thesis of 1822, related chronic arachnoiditis to dementiaparalytica. This ascription of a defined pathology for general paralysis of the insane (GPI) had

Introduction and Preface to the Third Edition xxiii
profound consequences for psychiatry. It reinforced somatic theories of mental illness. Further,in later writings, Bayle emphasized the stages of the disease, with a specific form and pattern ofdevelopment, culminating in dementia. It was not until 1905 that Fritz Schaudinn (1871–1906)identified the spirochaete in genital lesions. In 1906, August von Wassermann (1866–1925)developed his diagnostic blood test, and in 1913 Hideyo Noguchi (1876–1928) identified thespirochaetes in the brains of patients with general paralysis of the insane. Julius von Wagner-Jauregg (1857–1940) introduced the first treatment by inducing pyrexia in patients with GPIusing malaria. Although no panacea, some were helped by this, their disease process apparentlyarresting. For this discovery Wagner-Jauregg was awarded a Nobel Prize in 1927. He was the onlypsychiatrist to be so honoured until 2000, when Eric Kandel, Arvid Carlsson and Paul Greengardwere also awarded the prize.
Much of the endeavour of the 19th-century neuropsychiatrists related to uncovering the causesof the more severe psychiatric disorders, especially the psychoses. However, disorders that werethen referred to as ‘the neuroses’ also became a focus of attention, especially in France.
It was the great French neurologist Jean Martin Charcot (1825–1892) who explored the neurosesin detail, and he was particularly interested in hysteria. It is interesting that at this time, the latterhalf of the 19th century, neuroses were considered the province of the neurologist. This in partreflected the fact that most severe pathology was seen in hospitals, and the neuroses presumably,as today, were largely found in out-patients, and tended to be seen by a different group ofphysicians, usually privately. An example of this was the development in the USA of the conceptof neuraesthenia by George Miller Beard (1839–1883), and the interest of Silas Wier Mitchell(1829–1914), one of the earliest and most influential of the American neurologists, in conditions ofnervous debility. His ‘rest cure’ became widely known and used as a treatment for these disorders.Neuraesthenia evolved from ideas such as those of Marshall Hall (1790–1857), who in 1850 definedthe reflex actions of the spinal cord, applying his definition to various disease states. The conceptof spinal weakness found a counterpart in brain weakness, and hence cerebral neuraesthenia.
Charcot was appointed Medecin de l’Hospice de la Salpetriere at the age of 37. It washis belief that the neuroses should be examined and investigated as any other disorders. Charcotexperimented with hypnosis, which he felt induced a specific pathological state, and his influence onFreud and the development of psychoanalysis is well known. Zilboorg summed up this era, stating:
The fundamental contribution of the School of the Salpetriere and its essential historical value lie in thefact that it was the first to capture for psychiatry the very last part of demonological territory, whichup to the middle of the 18th century had belonged to the clerical and judicial marshals of theology andfrom the middle of the 18th century to the last quarter of the 19th had remained for the most part a noman’s land (Zilboorg, 1941, p. 365).
Sadly, the first half of the 20th century saw an apparent eclipse of progress in biologicalpsychiatry, and psychological theorizing dominated psychiatry. This had the disastrous effect ofaccelerating the divisions between neurology and psychiatry, and held up the development ofeffective treatments, especially for the more severe psychiatric disorders. It was not until the secondhalf of the 20th century that biological approaches to psychiatry flowered again. This has provideda new generation of psychiatrists with a wide range of fascinating and important findings, whichplace psychiatry once again securely as a medical discipline. This has resulted in part from avastly increased knowledge of the anatomy and chemistry of the central nervous system, thedevelopment of brain imaging and a renewed interest in genetics.
The role that encephalitis played in the development of biological psychiatry has yet to befully appreciated. The most significant contribution initially came from Constantin von Economo(1876–1931). He studied with Wagner-Jauregg in Vienna, and towards the end of 1916 he reported

xxiv Introduction and Preface to the Third Edition
on a number of patients who presented with an unusual variety of symptoms which followedan influenza-like prodrome. Some had marked lethargy and disturbance of their eye movements,and on post-mortem examination they invariably had inflammation almost exclusively confinedto the grey matter of the midbrain. Von Economo defined this as a new entity, and referredto it as encephalitis lethargica. It was attributed to influenza pandemics which occurred in thefirst years of the 20th century. A wide range of psychopathology was noted in the survivors,especially obsessive–compulsive and psychotic disorders. The importance of this was emphasizedby von Economo:
The dialectic combinations and psychological constructions of many ideologists will collapse like ahouse of cards if they do not in future take into account these new basic facts . . . Every psychologistwho in the future attempts to deal with psychological phenomena such as will, temperament, andfundamentals of character, such as self-consciousness, the ego, etc., and is not well acquainted with theappropriate observations on encephalitic patients, and does not read the descriptions of the psychologicalcauses in the many original papers recording the severe mental symptoms, will build on sand (vonEconomo, 1931, p. 167).
The last sentence of his book is ‘Encephalitis lethargica can scarcely again be forgotten’ (p. 167),but this prophesy was quickly to be proved wrong. This elegant work was ignored by at least twogenerations of psychiatric theorists, although the viral hypothesis of psychiatric illness has recentlybeen revived (see Chapter 7).
Epilepsy has always had close links with psychiatry (see Chapter 10). Hughlings Jacksonestablished significant clinical associations and Kraepelin, in his Lectures on Clinical Psychiatry(Kraepelin, 1904), included epileptic insanity as a variety of mental illness. The Hungarian Ladislasvon Meduna (1896–1964), impressed by his own pathological studies, which suggested differentpathological changes in the brains of patients dying with epilepsy versus schizophrenia, reasonedthat there was an antagonism between the two disorders. He postulated that the artificial inductionof a seizure may have a beneficial effect on the psychosis. He initially used camphor injections, butlater Ugo Cerletti (1877–1963) and Lucio Bini (1908–1964) introduced electric stimulation, and theefficacy of this form of treatment in a variety of conditions was soon reported (see Chapter 12).
Another bridge between epilepsy and psychiatry was the introduction into clinical practiceof the electroencephalogram (EEG). The psychiatrist Hans Berger (1873–1941), in a series ofpublications from 1928 to 1935, made regular observations of the electrical patterns he recordedfrom human brains. The identification of different forms of epilepsy followed; the significance ofthis disorder for biological psychiatry cannot be overemphasized. The identification that patientswith temporal-lobe epilepsy were more likely to have psychiatric disorders than those with otherseizure disorders, and the realization that psychic symptoms typified the onset of temporal-lobe seizures, coincided with the rediscovery of the limbic lobe of the brain by Paul MacLean(1913–2007). He recognized the importance of the temporal–limbic anatomy as a neurologicalframework for emotional feelings, and while he initially referred to this as the ‘visceral brain’, helater, in 1952, introduced the term ‘limbic system’.
Before MacLean there were others who had discussed how it is that we experience emotions. Thehypothesis independently developed by William James (1842–1910) and Carl Lange (1834–1900)had implied that emotions were derived from sensory inputs to the brain, but without anobvious cerebral localization. Walter Cannon (1871–1945) had noted subcortical areas whichon stimulation led to emotional release, and James Wenceslas Papez (1883–1858) had outlineda harmonious mechanism which he considered elaborated emotion. MacLean’s work took theimportant step of revealing how exterosensory inputs obtained access to limbic structures to allowfor the elaboration of their emotional content. However, with his concept of the triune brain,

Introduction and Preface to the Third Edition xxv
MacLean set the developed structures of the mammalian brain into a firm evolutionary mould, ina modified Jacksonian framework.
Since MacLean’s conceptualizations, the connectionist views of brain function have overtakenan outmoded modularity, and our knowledge of cortical–subcortical circuits, networks and thedeveloped understanding of limbic connectivity have altered our perspective on the limbic-systemconcept entirely (see Chapter 2). Perhaps fundamental has been the re-realization that the limbicareas of the brain are not, as often diagrammatically portrayed in the human brain, small andhidden, but are large and very prominent. Limbic connectivity, via the basal ganglia and frontalcortex, drives the organism forward in time and space. Importantly, emotion and limbic tonepervade many actions, and in the case of Homo sapiens, tinge most thinking.
One very important consequence of a biological approach to psychiatric disorders was theprogress of biological treatments (see Chapter 12). In the first part of the 20th century pellagra wasfound to be caused by a deficiency of nicotinic acid, phenylalanine deficiencies were identifiedin certain mentally handicapped children and endocrine replacement therapies, for examplethyroxine, became possible. Neurosurgical approaches to treating psychiatric disorders wereinitiated by the Portuguese neurologist Antonio Egas Moniz (1874–1955). In 1952, Jean Delay(1907–1987) and Paul Deniker (1917–1998) successfully gave chlorpromazine to psychotic patients.Soon after, antidepressant medications were developed and in 1949 John Cade (1912–1980)introduced lithium, the first prophylactic treatment in psychiatry. ‘Librium’, the first of thebenzodiazepines, was marketed in 1960. With these new and largely effective treatments, basedon medical models of normal and pathological behaviour, the future of biological psychiatrywas secure, and the societies followed. The Society for Biological Psychiatry and its journal werefounded in 1954 and the first World Congress of Societies of Biological Psychiatry was held in 1974.The World Federation of Societies of Biological Psychiatry today has 50 affiliated nationalities andnearly 5000 members.
Looking back on this history of fits and starts and forgotten lessons, one can even wonder if thefield of biological psychiatry can continue and evolve. In point of fact, it has, and quite exuberantly.In the 13 years since the last edition of this book, the field of neuroscience has exploded. The Societyfor Neuroscience annual meeting has gone from 400 attendees in 2000 to over 20 000 now, witheach attendee presenting new data. It is thus almost impossible for a clinical, biologically-orientedpsychiatrist to even keep up with all this new information. In this edition, we have done our bestto integrate new information with the older wisdom, thoroughly revamping and changing broadaspects of the text where needed. Many of the chapters have been completely restructured, andwe have included a new chapter on disorders of motivation and addiction (Chapter 9). There arefew authored books (not edited) that attempt to cover the full range of biological psychiatry witha single comprehensive voice. We apologize to anyone whose specific work is not directly cited,but we have tried to overview the important contemporary themes in this field. Understandinghow the brain organizes thoughts and consciousness is the most important scientific issue facinghumanity, and many believe that biological psychiatry is the most dynamic and interesting areain all of medicine and psychology, with profound philosophical implications. We hope the readerwill enjoy and be informed by this new edition.
M.R.T.M.S.G.
2402 Happy Acres Rd.Cedar Mountain, NC, USA


1Principles of Brain Functionand Structure: 1 Genetics,Physiology and Chemistry
INTRODUCTION
It has become fashionable periodically to ascribemuch psychopathology to the evils of mod-ern society, and the resurgence of this notionfrom time to time reflects the popularity ofthe simple. Often imbued with political over-tones, and rarely aspiring to scientific insights,such a view of the pathogenesis of psychiatricillness ignores the long tradition of both therecognition of patterns of psychopathology andsuccessful treatment by somatic therapies. Fur-ther, it does not take into account the obviousfact that humanity’s biological heritage extendsback many millions of years.
In this and the next chapter, consideration isgiven to those aspects of the neuroanatomy andneurochemistry of the brain that are importantto those studying biological psychiatry. Mostemphasis is given to the limbic system andclosely connected structures, since the under-standing of these regions of the brain has been offundamental importance in the development ofbiological psychiatry. Not only has a neurologi-cal underpinning for ‘emotional disorders’ beenestablished, but much research at the presenttime relates to the exploration of limbic systemfunction and dysfunction in psychopathology.
Biological Psychiatry 3e Michael R. Trimble and Mark S. George 2010 John Wiley & Sons, Ltd
GENETICS
Every cell in the human body contains thenuclear material needed to make any other cell.However, cells differentiate into a specific cellby expressing only partially the full geneticinformation for that individual. While it isbeyond the scope of this book to fully explainall of modern genetics, it is important tograsp several basic aspects that are involvedin building and maintaining the nervoussystem, and which may impact on psychiatricdiseases.
Modern genetic theories are based onknowledge of the deoxyribonucleic acid (DNA)molecule, its spontaneous and random muta-tions and the recombination of its segments.DNA is composed of two intertwined strands(the double helix) of sugar-phosphate chainsheld together by covalent bonds linked to eachother by hydrogen bonds between pairs ofbases. There is always complementary pairingbetween the bases, such that the guanine (G)pairs with cytosine (C), and the adenine (A)with thymine (T). This pairing is the basis ofreplication, and each strand of the DNAmolecule thus forms the template for thegeneration of another. Mammalian DNA is

2 Biological Psychiatry
SugarPhosphateBackbone
Base pair
Nitrogeousbase
Adenine
Thymine
Guanine
Cytosine
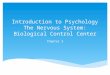
Figure 1.1 DNA replication and transcription. Dur-ing transcription, the DNA strands separate, and oneis transcribed. The primary mRNA transcript is acopy of the DNA strand, except that a U has beensubstituted for every T (reproduced with permissionfrom Professor Nick Wood)
supercoiled around proteins called histones(Figure 1.1). Recently it has been discovered thathistones can be modified by life experiences.The actual protein folding of the geneticmaterials changes as a function of histones ormethylation on the DNA. Early life experiencescan actually cause large strands of the DNA tobecome silent and not expressed (McGowanet al., 2008 ; Parent and Meaney, 2008).
On the DNA strand are many specific basesequences that encode for protein construction.Thus, proteins are chains of amino acids, andone amino acid is coded by a triplet sequence ofbases (the codon). For example, the codon TTCcodes for phenylalanine.
DNA separates its double helix in a reactioncatalysed by DNA polymerase. In the synthe-sis of protein, ribonucleic acid (RNA) is anintermediary. RNA is almost identical to DNA,except that uracil (U) replaces thymine, thesugar is ribose, and it is single-stranded. Thus,an RNA molecule is created with a complemen-tary base sequence to the DNA, referred to asmessenger RNA (mRNA). This enters the cyto-plasm, attaches to ribosomes, and serves as atemplate for protein synthesis. Transfer RNA(tRNA) attaches the amino acids to mRNA, lin-ing up the amino acids one at a time to form theprotein. The tRNA achieves this by having ananticodon at one end attach to the mRNA andthe amino acid at the other (see Figure 1.2). Cod-ing occurs between the start and stop codons.
Much is now known regarding the varioussequences of bases that form the genetic code. Intotal, chromosomal DNA in the human genomehas approximately 3 billion base pairs. There are20 amino acids that are universal constituents ofproteins, and there are 64 ways of ordering thebases into codons (Wolpert, 1984). Most aminoacids are represented by more than one triplet,and there are special techniques for starting andstopping the code. Although it was thoughtthat the only direction of information flow wasfrom DNA to RNA to protein, investigations oftumour cells have revealed retroviruses: RNAviruses that can be incorporated into host DNA.
The genetic programme is determined byDNA, and at various times in development,and in daily life, various genes will be turnedon or off depending on the requirements of theorganism. There is a constant interplay betweenthe genetic apparatus and chemical constituentsof the cell cytoplasm.
In the human cell there is one DNA moleculefor each chromosome, and there are some100 000 genes on 46 chromosomes. This consti-tutes only a small portion of the total genomicDNA, and more than 90% of the genomeseems non-coding. About 50% of human DNAconsists of short repetitive sequences thateither encode small high-abundance proteinssuch as histones, or are not transcribed. A lotof these are repetitive sequences dispersedthroughout the genome, or arranged as regionsof tandem repeats, referred to as satellite DNA.

Principles of Brain Function and Structure: 1 Genetics, Physiology and Chemistry 3
mRNA
Tyr
ArgArg Phe
Phe
3′
5′
30S
50S
Ribosome
Polypeptidechain
Leu
Figure 1.2 RNA translation. The mRNA (top) acts as a template that specifies the sequential attachment oftRNAs: amino acid complexes to make a protein shown in the bottom of the figure. Coding occurs betweenthe start codon (3
′) and ends at the stop codon (5
′) (reproduced with permission from Lowenstein et al., 1994;
Biol Psych, 2 Ed, p. 44)
Such repeats are highly variable betweenindividuals, but are inherited in a Mendelianfashion. These variations produce informativemarkers, and when they occur close to genesof interest are used in linkage analysis. Com-plimentary cDNA probes are produced usingmRNA as a template along with the enzymereverse transcriptase. The latter is present inRNA viruses; HIV is a well-known example.Reverse transcriptase permits these viruses tosynthesize DNA from an RNA template. It isestimated that 30–50% of the human genome isexpressed mainly in the brain.
Retroviruses enter host cells through inter-action at the host cell surface, there being aspecific receptor on the surface. Synthesis ofviral DNA then occurs within the cytoplasm, theRNA being transcripted into DNA by reverse
transcriptase, and the viral DNA becomingincorporated into the host’s genome.
Oncogenes are DNA sequences homologousto oncogenic nucleic acid sequences of mam-malian retroviruses.
In the human cell the chromosomes aredivided into 22 pairs of autosomes, plus the sexchromosomes: XX for females and XY for males.Individual genes have their own positions onchromosomes, and due to genetic variationdifferent forms of a gene (alleles) may exist ata given locus. The genotype reflects the geneticendowment; the phenotype is the appearanceand characteristics of the organism at any par-ticular stage of development. If an individualhas two identical genes at the same locus, onefrom each parent, this is referred to as being ahomozygote; if they differ, a heterozygote. If a

4 Biological Psychiatry
heterozygote develops traits as a homozygotethen the trait is called dominant. There aremany diseases that are dominantly inherited.If the traits are recessive then they will onlybe expressed if the gene is inherited fromboth parents. Dominant traits with completepenetrance do not skip a generation, appearingin all offspring with the genotype.
If two heterozygotes for the same recessivegene combine, approximately one in four of anychildren will be affected; two will be carriers,and one unaffected. When there is a defec-tive gene on the X chromosome, males aremost severely affected, male-to-male transmis-sion never occurs, but all female offspring of theaffected male inherit the abnormal gene.
Many conditions seem to have a geneticcomponent to their expression, but do nothave these classic (Mendelian) modes of inher-itance. In such cases polygenetic inheritance issuggested.
Mitochondrial chromosomes have been iden-tified. They are densely packed with no intronsand they represent around 1% of total cellularDNA. They are exclusively maternally trans-mitted. Unlike nuclear chromosomes, presentnormally in two copies per cell at the most,there are thousands of copies of the mitochron-drial chromosomes per cell.
In the gene there are coding sequences, calledexons, and intervening non-coding segmentsreferred to as introns. Some sequences occuraround a gene, regulating its function. It is notunusual for the genes of even small proteins
to be encoded in many small exons (under200 bases) spread over the chromosome. Mostgenes have at least 1200 base pairs, but arelonger because of introns. Further, importantsequences precede the initiation site (or 59),and the end of the gene (39). A model of ageneric gene is shown in Figure 1.3. The promo-tor region is at the 59 end, containing promotorelements and perhaps hormone binding sites.These activate or inhibit gene transcription. Thecoding region consists of sequences that willeither appear in the mature mRNA (exons) orbe deleted (introns).
During meiosis, the strands from the twochromosomes become reattached to each other,but each chromosome carries a different allele.There is then a new combination of allelesin the next generation, this exchange beingreferred to as recombination. The frequency of arecombination between two loci is a function ofthe distance between them: the closer they are,the less is the likelihood that a recombinationwill occur between them (Figure 1.4).
Linkage analysis places the location of aparticular gene on a chromosome; physicalmapping defines the linear order among aseries of loci. Genetic distance is measuredin centimorgans, reflecting the amount ofrecombination of traits determined by genes atthe two loci in successive generations.
In mutations, unstable mRNA is producedand cannot be translated into a functionalpolypeptide. Mutations may be referred toas point mutations (substitution of single
“CAAT BOX”−80 to −70 TRANSCRIPTION
INITIATIONSITE
POLYADENYLATIONSIGNALAATAAA
HORMONEBINDING SITES
(cAMP, etc)
5′ CONTROL ELEMENTS
3′ CONTROLELEMENTS
3′
CT
AAATATATEXON 1 EXON 2 EXON 3
−30 to −25“TATA BOX”
T
GC AATCT
5′
Figure 1.3 A ‘generic gene’. Three exons (white) and two introns (black) are shown (reproduced withpermission from Ciaranello et al., 1990; Biol Psych, 2 Ed, p. 46)

Principles of Brain Function and Structure: 1 Genetics, Physiology and Chemistry 5
Crossing–over and Recombination During Meiosis
12
3
ac
e
ac
ac
ac
ac
bd
f
bd
bd
bd
bd
ac
ac
bd
bd
e e f f
e f e f
e f e f
bd
f
bd
e
ac
e
ac
f
Gametes
Figure 1.4 The principle of crossover. If there aretwo genes A and C, the closer together they are,the more likely they are to remain together duringmeiosis (reproduced with permission from ProfessorNick Wood)
incorrect nucleotide), deletions, insertions,rearrangements or duplications.
Molecular cloning techniques allow for thestudy of gene structure and function. Restrictionendonucleases cut the DNA molecule at specificsites, allowing the fragments to be replicatedon a large scale by transfecting other organisms,which produces multiple copies of an insertedDNA section. Foreign fragments of DNAare inserted into a plasmid, a cosmid or abacteriophage vector capable of autonomousreplication in a host cell: the process of cloning.Recombinant DNA molecules are amplifiedby growth in the host (e.g. bacteria) andthen subsequently isolated and purified. Onceisolated, complementary DNA (cDNA) can bechemically sequenced, introduced into a hostcell to produce encoded protein, or hybridizedto genomic DNA to examine the structure ofthe genes encoding for the target protein.
Complementary DNAs are made frommRNAs, prepared from the tissue of interest,
and then propagated in vitro to form cDNAlibraries. A gene probe is a fragment of DNAthat detects its complementary sequence. Oftensuch cDNA probes are produced from animalprotein, and for most diseases they are notspecifically related to a disease gene, but maybe linked to it genetically.
The ‘lod’ score refers to the ‘log of the odds’and expresses the relative probability thattwo loci are linked as opposed to not linked.Thus, given a disease gene and a known DNAmarker, if they co-segregate together more thanby chance, they may be linked; the tighter thelinkage, the greater the probability. The logvalue of the relative probability of linkage is thelod score, and a positive score of >3 is usuallytaken as proof of linkage. This means that theodds are 1000 to 1 that the correlation is theresult of gene linkage, rather than chance. A lodscore of −2 excludes linkage.
Lod scores from independent family obser-vations are added together, overcoming theproblem of the small size of the human fam-ilies that are usually available for observation.Lod scores are calculated with available com-puter algorithms, and thus quantify probablelinkage, but are most effective for conditionswith Mendelian inheritance.
In modern genetics, restriction enzymes areused to split the DNA segments, which canthen be recognized by gene probes. Restriction-fragment-length polymorphisms (RFLP) areDNA fragments that differ in length betweenindividuals. Tandem repeated sequences varybetween individuals, and smaller sequencesof repeats are referred to as mini-satellites.Micro-satellites are very short sequences ofrepeated dinucleotides, usually GT, that areuseful for mapping (Figure 1.5).
These satellite sequences and mutations aredetected as RFLPs. The technique involvestaking tissue – the origin is immaterial – andsplitting the DNA into fragments. These arethen displayed by a hybridization blot method(Southern blot), which depends on the ability ofDNA to bind to nitrocellulose paper. The fixedDNA fragments are then hybridized with aradioactive DNA probe and detected bythe subsequent band pattern dependent on

6 Biological Psychiatry
Step 1: Digestion. Amplicons (PCR-amplified DNA segments) are cut ( ) with arestriction enzyme wherever a specific DNA sequence occurs.
Step 2: Visualization of cut and uncutamplicons on an electrophoretic gel.The size of the DNA fragment determinesthe distance it migrates on the gel; shortfragments travel farther than long fragments.
Step 3: Interpretation. Patient A: No copies of mutationHeterozygous for mutationHomozygous for mutation
Patient B:Patient C:
If the mutation is not present, the restrictionenzyme does not cut the amplicon and theoriginal length of the PCR fragment ismaintained (300 base pairs).
TAACGATGCTAGCGGA
Three outcomes are possible:
TAACGATGCTAGCGGA
300 bp
300 bp
300 bp
200 bp 100 bp 200 bp 100 bp
200 bp 100 bp300 bp
Patient A Patient B Patient C
If the mutation is present, the restrictionenzyme cuts the amplicon into twofragments of 100 and 200 base pairs
TAACGATG*TAGCGGA
TAACGATG
200 bp 100 bp
Restriction enzyme doesnot cut ampliconsfrom either allele.
Restriction enzyme cutsamplicons from both alleles.
Retriction enzyme cutsamplicons from one allele.
SizingStandard
PtA
PtB
PtC
300 bp200 bp
100 bp
bp = base pairsPt = Paitent
*TAGCGGA
Figure 1.5 Restriction fragment-length polymorphism method to test for genetic variants (reproduced withpermission from www.genetests.org and the University of Washington, Seattle)
the speed of migration with electrophoresis.Libraries of DNA probes are available fromacross the spectrum of the human genome.
Recently, the discovery of the polymerasechain reaction has revolutionized the analysis ofRFLPs. In this technique, sufficient high-quality
DNA is produced by biological amplificationusing DNA polymerase, increasing the speedand power of analysis.
The RFLPs are used as genetic markers forinherited diseases if they can be shown to belinked to a gene that is thought to be abnormal

Principles of Brain Function and Structure: 1 Genetics, Physiology and Chemistry 7
and responsible for the condition. Families inwhich there are several affected members areinvestigated and RFLPs are probed to detectonly those that are present in affected individu-als. When found, the chromosome on which theabnormal gene resides can be identified, and thelinked marker, which may be the gene itself, isused to detect genotypes likely to become phe-notypes. There have been three generations ofmarker loci used for genetic linkage mapping.The first was the RFLPs described above, fol-lowed by the micro-satellites. More recently thesingle-nucleotide polymorphisms (SNPs, pro-nounced ‘snips’) have been used for the samepurpose of tracking genetic variants in pedi-grees. A SNP is a silent genetic variation inwhich one nucleotide (AGTC) is replaced byanother, often not affecting the expression of thegene. These minor changes are useful in track-ing genetic changes over time and in differentpopulations.
Linkage studies are complicated by incom-plete penetrance, age of onset of disease, vari-able expression of that disease and geneticheterogeneity (more than one gene leading tothe phenotype).
The identity of a gene marker linked toHuntington’s chorea in 1983 provided the firstexample of the locating of an autosomal dom-inant gene in neuropsychiatry. This is knownto be on chromosome 4, and encodes a struc-turally unique protein of 348 kd (huntingtin).There is a specific trinucleotide repeat (CAG),which varies from 9 to 37 copies in normals,but can be massively expanded (>100 copies)in Huntington’s chorea. It is also possible topinpoint genes for specific enzymes and recep-tors; for example, the D2 receptor at 11q22, andtyrosine hydrolase at 11p15.5.
Despite now having mapped the entirehuman genome, as well as the genome ofmany other plants and animals, there has beenconsiderable difficulty in locating specific genesfor psychiatric illnesses. The initial break-throughs (see chapters on individual diseases)have not been replicated in many cases. Thisrelates partly to difficulties of clinical diagnosisand partly to problems of genetic modelling.Thus, the same data set is used to generate the
lod score that is used to construct the model forinheritance in the first place.
Building on the world of genomics (studyof genes), scientists are now investigatingthe world of proteomics (the study of theproteins an individual expresses, which changeover time). This is immensely richer thaneven genetics, as the proteins that the RNAtranscribes at any given moment are even morevariable than the ‘largely’ static genetic infor-mation. In the example above, in Huntington’sdisease the abnormal protein made by the genevariation is huntingtin; the build-up of toxicproteins then goes on to impair intracellulardynamics and receptor and neuronal function,resulting in disease. A surprising finding of theHuman Genome Project is that there are farfewer protein encoding genes than there areproteins in the human body. How can this be?Obviously there must be other factors – wherethe environment interacts with how genesmake proteins – that explain this paradox. Thewhole study of how the micro-environmentwithin the cell can impact back on which genesare expressed and when is called ‘epigenetics’.Some of the more interesting new theories aboutstress and trauma involve the lifelong effect ofthe social environment (childhood stress) ongene expression (see Chapters 6 and 8).
It is important to remember that genes codefor some facet of a disorder, and not a DSMcategory. Recently the concept of endopheno-types has emerged. This refers to a biomarkerwhich is intermediate between the genotype(pure gene) and the phenotype (the individualwith a disease). The endophenotype is closer tothe genetic variation, and represents a risk fac-tor or propensity for a behaviour that then leadsto the development of a syndrome (Chapter 4).For example, someone might inherit a gene thatcodes for a particular cognitive profile (abnor-mal sensory gating or startle or problems withexecutive function) which predisposes someoneto develop psychosis.
The genes that code for proteins make upabout 1.5% of the human genome, and at leastsome of the rest regulates gene expression. Thetranscription factors turn on DNA sequencescalled enhancers, which determine that genes

8 Biological Psychiatry
are expressed only where they are wanted andat the time that they are wanted. The enhancersare often hundreds of base pairs in length, andmay not be sited near the gene itself. They allowthe same gene to be used over and over in dif-ferent contexts, and from an evolutionary pointof view may allow individual traits to be modi-fied without changing the genes themselves. Inunderstanding genetics, the study of the role ofenhancers is in its infancy (Carroll et al., 2008).
BRAIN CHEMISTRY AND METABOLISM
In order to function adequately, the brainrequires energy which is derived from thecatabolism of the food we eat. The majornutrient for the brain is glucose, which, in theprocess of oxidization to carbon dioxide (CO2)and water gives up energy. This process resultsin the formation of adenosine triphosphate(ATP) from adenosine diphosphate (ADP).In the course of energy use through cellulartransport and biosynthesis the ATP is degradedto ADP (see Figure 1.6).
Glucose enters cells via transporters, andglucose utilization is higher in astrocytes thanneurones. Glycogen in the brain is stored mainlyin astrocytes, and the latter release energy toneurones via pyruvate and lactate. Glycogenturnover is rapid and coincides with synap-tic activity. Several neurotransmitters (such asthe monoamines) are glycogenolytic, releasingenergy from the astrocytes. Another important
function of astrocytes is to remove glutamatefrom the synaptic space, which is recycled viaglutamine back to neurones to replenish theglutamate pool. The metabolism of glucose inthe brain is highly temporospatially specific andlinked to neuronal-glial (the neutropil) activity,a property which has been used in the theories ofglucose PET imaging (see Chapter 4) and is alsoimportant for understanding functional MRI.
The oxidation of one molecule of glucosegenerally gives 36–38 moles of ATP (Siesjo,1978). It is obvious that ATP has a central rolein cellular metabolism, being the product ofoxidation and the substrate for further chemicalreactions requiring energy. It is composed of anitrogenous base (adenine), a five-carbon sugarand attached phosphate groups; it is one ofseveral triphosphonucleotides in the cell thatyield energy.
As noted, the main energy requirementsare those of cellular transport mechanismsand biosynthesis. The former includes themovement of both charged and uncharged par-
ticles across cell membranes and the transport ofmolecules intracellularly. Biosynthesis involvesthe formation of simple and complex moleculesrequired for cellular function, in addition tosuch energy storage molecules as glycogen.
A related molecule is adenosine 3,5-monophosphate (cyclic AMP), which has onephosphate molecule and forms a ring structurewith links between the sugar and phosphatemolecules. It is formed from ATP in a reaction
Glucose + 6 O2
6 CO2 + 6 H2 O
Oxidativemetabolism
Activetransport Biosynthesis
ATP
ADP + Pi
Figure 1.6 Showing the generation of ATP by means of oxidative metabolism with glucose as substrate.Oxidation of 1 mole of glucose yields 36–38 moles of ATP (reproduced with permission from Siesjo, 1978; BiolPsych, 2 Ed, p. 50)

Principles of Brain Function and Structure: 1 Genetics, Physiology and Chemistry 9
that utilizes adenyl cyclase as a catalyst. It isactivated by adrenaline and is known to beinvolved, via the intermediary phosphorylase,in the activation of glycogen. Further, cyclicAMP appears to act as an intermediary inmany other cellular reactions, including thosestimulated by hormonal or neurotransmitterstimuli (see below).
Chemical reactions in the body are facili-tated by enzymes, some of which themselves areactivated by coenzymes which transfer atoms orgroups of atoms from one molecule to another.Since the quantity of active enzyme presentis the essential ingredient that determines therate of a biochemical reaction in the presenceof appropriate substrates, activation and inhibi-tion of enzymes regulates the metabolic activityof cells. One method of inhibition of a partic-ular metabolic reaction is by feedback from aresulting metabolite (feedback inhibition).
THE METABOLISM OF GLUCOSE
Glucose and glycogen catabolism result in theproduction of ATP via the well-known tri-carboxylic acid (Krebs) cycle (see Figure 1.7).Glucose is first phosphorylated by hexokinase
to yield glucose-6-phosphate. This is converted,via the several intermediary steps of glycoly-sis, to lactic acid. This yields two molecules ofATP thus:
Glucose + 2 ADP + 2 phosphate→ 2 lactic acid + 2 ATP + 2 water
Lactic acid is converted to acetyl-coenzyme Avia pyruvic acid, and the former is oxidizedby the tricarboxylic acid cycle to citrate andultimately oxaloacetate, which itself is incorpo-rated with acetyl-coenzyme A to yield citrate.Hydrogen atoms that are generated react withoxygen to form water, and further moleculesof ATP are generated. Since other products ofdigestion undergoing catabolism also utilize thetricarboxylic acid cycle, it represents a final com-mon path, and almost two-thirds of all energyreleased in the breakdown of food occurs duringthe reactions of this cycle.
PROTEINS AND FATTY ACIDS
While glucose is the most important foodinvolved in metabolism, proteins and fattyacids are also involved. Protein is broken down
oxaloacetate
acetyl − coenzyme A
cis − aconitate
isocitrate
citrate
coenzyme A2H
H2O
L–malate
2H
2H + CO2
GTP +coenzyme A GDP + orthophosphate
oxalosuccinate
a − ketoglutarate
succinyl − coenzyme A
coenzyme A
succinate
fumarate
H2O
H2O
H2O
2H
CO2
Figure 1.7 The tricarboxylic acid cycle (Biol Psych, 2 Ed, p. 52)

10 Biological Psychiatry
Table 1.1 Some essential amino acids
HistidineArginineOrnithineValineMethionineLysinePhenylalanineTyrosineTryptophanHomocysteineCysteineGlycineAmino butyric acid
to amino acids, which can be oxidized throughthe tricarboxylic acid cycle. Degradation reac-tions common for several amino acids includedeamination, in which an amonia group isremoved, transamination, in which there isexchange between amino and ketonic acids ofamino and keto groups, and decarboxylation,in which a carbon dioxide radical is given up.Only some amino acids are broken down forenergy, others being involved in the synthesisof neurotransmitters, and most in the buildingof proteins.
There are only a limited number of aminoacids in living cells, some of the most importantbeing shown in Table 1.1.
Fats are hydrolysed to free fatty acidsand glycerol. The fatty acids are chains ofcarbon atoms terminated with a carboxylicacid ( COOH) group. Glycerides are esters(compounds formed by the interaction of anacid and an alcohol) of fatty acids and glycerol,and phospholipids are esters of fatty acidsand alcohol, the latter containing a phosphategroup. Sphingolipids have the base sphingosineinstead of glycerol, and sphingomyelines con-tain choline. The cerebrosides and gangliosidesare sphingolipids with a hexose, and in the caseof gangliosides, a polyhydroxy amino acid. Allof these are found in abundance in nerve tissue.
CELL MEMBRANES
Neurones, in common with other cells, arebounded by a membrane. It is now known that
this is a continuous double structure with twoelectron-dense layers separated by an interzone.The thickness is approximately 100 A, and sim-ilar membranes are seen in the cell, forming,for example, the endoplasmic reticulum or themitochondria.
They are mainly formed from lipids (whosecentral components are fatty acids) and proteins.One end is hydrophilic and the other hydropho-bic, and these align to form a structure suggestedto look like that shown in Figure 1.8. The insideis hydrophobic, and proteins seem embeddedin the structure, carrying out such functions asaiding active transport, forming the structure ofreceptors and enzyme activity. Channels in themembrane are thought to be protein aggregates,and they help regulate permeability. These areeither active (which can be open or closed) orpassive (which remain open all the time). Activechannels may be influenced by various stimuliincluding electrical or chemical ones such as theneurotransmitters.
The primary structures of sodium, potassiumand calcium channels have been revealed fol-lowing cloning, and they are all similar, withfour homologous transmembrane domains sur-rounding a central ion pore, which sits in thecentre of the square array.
In the technique of patch clamping, a smallmicropipette with a polished end is pushed intothe cell and then sucked. The membrane formsa tight seal on the pipette, and if it is then pulledthe small patch of membrane remains intact
Polar (hydrophilic) surface
Hydrophobicmembraneinterior
Figure 1.8 A schematic representation of a cellmembrane (reproduced from Shaw et al., 1982, bypermission of Butterworth & Co; Biol Psych, 2 Ed,p. 54)

Principles of Brain Function and Structure: 1 Genetics, Physiology and Chemistry 11
and is used to study receptor function in detail,including ion flow through channels.
In order that the cell is excitable, a poten-tial difference across it must exist (polarization).This membrane potential is positive on the out-side and negative on the inside. It is due toelectrolyte differences on the two sides of themembrane, and in most neurones is in the regionof 50–60 mV. This is referred to as the restingpotential; to generate the action potential themembrane must be depolarized by alterationof the ion distribution on the two sides of themembrane.
There are four main ions in the cells: sodium(Na+), potassium (K+), chloride (Cl2) andorganic anion (A2). Sodium and chloride are atlower concentrations on the inside of the cell;the other two have higher concentrations. Atrest, the potential is maintained by the actionof the sodium pump, which, at the expense ofenergy, forces the sodium out and draws thepotassium in. The resting potential acts as theenergy store of the cell, and neuronal action isdependent on it. The electrical signals of thenerve cells result from a change in the restingpotential with alteration of the distribution ofions on either side of the membrane.
The action potential is generated by depolar-ization, during which sodium flows into the celland, with slight delay, the potassium moves out.This process is initiated by the opening of thesodium channel, allowing sodium to flow in: aprocess that opens more sodium channels. Then,as sodium channels begin to close, the potassiumvoltage-regulated gated channels begin to openand repolarization occurs. The resulting phasesof the action potential are shown in Figure 1.9.
These action potentials are generated by suchstimuli as synaptic transmission, and propaga-tion of the current along the membrane proceedsas adjacent portions of the membrane becomedepolarized by electronic conduction. Gener-ally, the larger the diameter of the axon ofthe cell, the more rapid the current flow; how-ever, in myelinated axons (see below), wherethe resistance at the nodes of Ranvier is lowcompared with that at the internodes, currenttravels along intracellular fluid from node tonode, a process referred to as saltatory conduc-tion. Following the action potential there is abrief refractory period during which the sodiumchannels return to their closed state. The entireneuron firing and refractory period take 5–6 milliseconds, allowing neurone to potentially
+ 30
+ 10
− 10
− 30
− 50
− 70
− 90
0
Mem
bran
e po
tent
ial,
mV
Overshoot
Depolari-zation
Repolarization
After-hyperpolarization
After-depolarization
CFL
Vr
0 1 2
Time, msec
3 4
Figure 1.9 The action potential and its components. Vr, resting membrane potential; CFL, critical firing level(Biol Psych, 2 Ed, p. 55)

12 Biological Psychiatry
refire or oscillate at very high frequencies (sev-eral hundred events per second). This is in con-trast to the megahertz frequencies sometimesused in modern electronics or computers. How-ever, neurone also have the ability to amplifytheir signal; that is, once the axon is triggered, itcan spread to the full tree of the axon, and poten-tially interact with thousands of other neurone.Axonal information can travel at 0.5–50 m s−1.
Although the most important ions for thegeneration of the action potential are sodiumand potassium, others exert influences, such ascalcium and magnesium.
SYNAPSES
The main link between one neurone and thenext is the synapse, and in the human central
Dendrite
Mitochondria
Dendro-dendriticsynapse
Intrinsicneuron
Axon collateral
Axo-dendriticsynapse
Axo-axonicsynapse
Neuron (cell body, soma)
En passantneuronand synapse
Axo-somaticsynapse
Axon hillock
Initial segmentof axon
Myelin sheath
Axon terminal Vesicles
Axon
(A)
(A)
(C)
(D)
(B)(B)
Figure 1.10 Schematic representation of a neuron (Webster, 2002)

Principles of Brain Function and Structure: 1 Genetics, Physiology and Chemistry 13
nervous system (CNS) transmission is mainlychemical. However, it is recognized that elec-trical synapses occur (bridged junctions) withonly small gaps (around 20 A) separating thepresynaptic and postsynaptic membranes. Incontrast, chemical synapses (unbridged junc-tions) have a larger gap (200 A), the synapticcleft, and specialized vesicles are identifiablein the presynaptic terminals. Information flowacross the electrical synapse is more rapid thanacross chemical junctions, although the latterare more flexible.
Postsynaptic potentials are either inhibitory(IPSP) or excitatory (EPSP). The former preventthe initial area of the axon from reachingthe threshold required to generate an actionpotential (hyperpolarization) by increasing theinflux of potassium and chloride. These IPSPscan summate either temporally or spatially, andinteract with EPSPs to determine the ultimateexcitability of the postsynaptic cell. EPSPs resultfrom an influx of sodium via chemically gatedchannels, and the spike discharge is generatednot at the postsynaptic membrane, but at
the axon hillock, which has a low electricalthreshold (see Figure 1.10).
In addition to these postsynaptic events,presynaptic factors which control transmitterrelease also affect postsynaptic activity. Theseinclude presynaptic inhibition or facilitation viaactivity in synapses on the presynaptic boutons(axo-axonic synapses) and ionic influencessuch as calcium (Ca2) influx. The presynapticterminals come from interneurones, and theyprovoke an EPSP or IPSP in the terminal of theafferent nerve fibre. In the case of inhibition, thispartial depolarization reduces the amplitudeof the oncoming afferent action potential.Since the transmitter release is proportionalto the amplitude of the action potential, lesstransmitter is released and a smaller EPSPresults in the postsynaptic cell. Although firstdiscovered in relation to spinal cord afferents,this form of inhibition has been shown to existin many CNS areas. Varieties of presynapticconnections are shown in Figure 1.11. Wherethe neurone has receptors to its own transmitteron these terminals they are called autoreceptors.
VesiclesRe-uptaketransporter
Postsynapticreceptors
Postsynapticneuron
Presynapticterminal
Presynaptic autoreceptors
Cellbody
Secondarymessengercascade
Ca2+
Figure 1.11 Schematic representation of a generic excitatory synapse in the brain. This shows glutamatereleased by fusion of transmitter vesicles at the nerve terminal and diffusing across the synaptic cleft to activateAMPA and NMDA receptors. Glutamate also binds to metabotropic G-protein-coupled glutamate receptors,initiating secondary messenger intracellular signalling through the G-protein complex (Webster, 2002)

14 Biological Psychiatry
Calcium has been shown to be essential fortransmitter release. During depolarization of thepresynaptic terminal the calcium channels openand calcium moves into the cell. This allowsthe presynaptic vesicles that contain neuro-transmitters to bind to releasing sites on thepostsynaptic membrane. Control of calcium cur-rents by presynaptic receptors is thought to bean important mechanism of their action.
The amount of transmitter released is relatedto the calcium levels and the presynaptic input.The response is thus plastic, and further variedby the postsynaptic variation in ion channels.Single vesicles can release up to 5000 moleculesof a neurotransmitter.
A further consideration is the retrograde con-trol of presynaptic activity by diffusible messen-gers from the postsynaptic cell. Nitrous oxide(NO) is a gaseous messenger involved in long-term potentiation (LTP). NO is synthesized inthe postsynaptic cell following calcium influx atthe N-methy-aspartate (NMDA) receptor, anddiffuses back to the presynaptic terminals, alter-ing transmitter release. Other candidates arearachidonic acid and carbon monoxide. A possi-ble target for these messengers is the presynapticcalcium influx.
There are two types of communicationbetween cells: classical, with fast transmission,in which highly specialized regions of thepresynaptic cell make contact with discreteareas of the postsynaptic cell; and more diffuse,with transmitter released over a broader area.The latter is less readily removed, and trans-mission is slower. Transmitters such as aminesand opiates use this latter, slower method andset the level of a response.
RECEPTORS
In recent years much attention has been paidto the structure and function of receptors.These are proteins to which transmittersbind, and are located on the outer surface ofthe cell membranes. Two types are defined,the transmitter-gated ion channel (calledionotropic) and the G-protein-coupled receptor(called metabotropic). The former act very
quickly, while the latter initiate a series ofpostsynaptic intracellular events which altereither intracellular proteins or the DNA of thenucleus, altering gene expression. The latterwill lead to alteration of the configuration of thecell, for example by activating growth factorsor receptor activity (see Figure 1.12).
The genes for many receptors have beencloned and their polypeptide structures identi-fied. Many have a similar conformation, perhapssuggesting a common evolutionary precursor.Since the sequence of the amino acids is knownfor the Dopamine D1 receptor, it is possible tolook at which parts of the sequence will inter-act with the lipid-rich membrane, and at thehydrophobic and hydrophilic parts identified.The general model is of five subunits, a channel,a gate and a receptor bound in a pocket. Somereceptors have many subunits, and these areselected in different combinations to give differ-ent responses, the length of time the channel isopen and the number of ions that flow throughit (Sibley and Monsma, 1992).
G-protein-coupled receptors share a genericpattern of protein folding, with seven hydropho-bic transmembrane helices joined by alternatingintracellular and extracellular loops, an extracel-lular amino terminal and a cytoplasmic carboxylterminal. The protein folding of several recep-tors is shown in Figure 1.13.
The neurotransmitter binds with the receptorto form a transmitter–receptor complex, whichchanges the conformation of the latter. With thetransmitter-gated ion channels, opening up theionophore allows ion exchange to occur withconsequent changes of the membrane potential.An influx of negative ions such as Cl− leadsto IPSPs, while an influx of positive ions suchas Na+ will encourage EPSPs. Some ionophoresare specific for chloride or sodium, others areless selective. With the G-protein-coupled recep-tors, interaction of the transmitter and receptorprovokes alteration of intracellular metabolismby the stimulation of second messengers.
In addition to neurotransmitter receptors,there are receptors for other chemicals, someof which help with the early development ofneuronal systems, such as for nerve growthfactors (NGF) and steroid receptors. The latter

Principles of Brain Function and Structure: 1 Genetics, Physiology and Chemistry 15
Metabo-tropic
receptor
Iono-tropic
receptor
Ionchannels
Direct gating
Proteinkinaseactivity
Phosphorylation
(Minor direct action)
Gprotein
NT
SecondMessengers
GMP cAMP IP3
+ −
Membrane
Figure 1.12 The difference between ionotropic and metabotropic mechanisms. With the former, the neuro-transmitter combines with the receptor, leading to opening of the ion channel. With the latter, G-protein isactivated, leading to a secondary messenger cascade. The image also shows how the intracellular activationscan feed back, affecting ion channels (Webster, 2002)
are intracellular molecules which carry thesteroid to the nucleus.
Ligands (transmitters or synthesized chem-icals that act on receptors), which are ago-nists, antagonists, partial agonists (exhibitingless than a maximal response) and inverse ago-nists (leading to the opposite response to a fullagonist) have been identified, depending on thereceptor type.
There are several second messenger systems.Following contact between the receptor anda neurotransmitter, a G-protein is activated(a GTP-binding protein), which in turn activatesfurther proteins, leading to the conversion ofATP to cAMP.
One secondary messenger system is viaadenylate cyclase to cyclic AMP. There is anintermediary G-protein which binds with the
receptor–transmitter complex and alters itsconfiguration; it then links with adenylatecyclase and activates it, leading to cyclicAMP formation. An important feature of thissystem is amplification, whereby each activatedreceptor protein stimulates many moleculesof G-protein, which in turn activate manymolecules of adenylate cyclase, each furthergenerating many cyclic AMP molecules. Proteinkinases are enzymes which phosphorylate(add phosphorous to) proteins and helpphysiologically activate them (Figure 1.12).
Another second messenger system is viathe hydrolysis of a membrane phospholipid(phosphatidylinositol biphosphate), whichleads to the production of diacylglycerol and,via phospholipase C, inositol triphosphate (IP3).Diacylglycerol activates protein kinase C and

16 Biological Psychiatry
(a) (b) (c)
NH2
NH2
COOH
TM1 TM2 TM3 TM4 TM1 TM3 TM4 TM1
COOH
COOH
NH2
TM2TM2
TM2TM2
TM2
TM2
TM2
Figure 1.13 How transmembrane subunits are conceived. The subunits are embedded in the cell membrane.The example in (a) reflects the structure, for example, of a GABAa receptor. Below is shown pentamericstoichiometry of the domain receptors lining the central ion channel. (b) shows the structure of ionotropicglutamate receptors. (c) shows a subunit of an ATP receptor (Webster, 2002)
IP3 causes release of calcium from the endo-plasmic reticulum, which activates a proteinkinase called calmodulin-dependent proteinkinase. G-proteins can also elevate intracellularcalcium, thus indirectly activating kinases.Calcium is intimately related to these secondarymessenger systems, and a calcium-bindingprotein, calmodulin, mediates these eventsand release of neurotransmitters from synapticvesicles.
Thus, phosphorylation modifies the actionof intracellular enzymes and cell regulatoryproteins; signals mediated through second mes-sengers influence protein kinases and proteinphosphatases, which in turn modify the actionof genes via transcription factors in the cyto-plasm that bind to DNA. Genes encoding tran-scription factors have been referred to as thirdmessengers. Genes such as c-fos are activelyswitched on quickly, having binding sites forthe transcription factor CREB. The receptors forsteroid hormones are also transcription factors,acting in the cell cytoplasm.
Calcium Channels
Calcium channels are essential because theyallow the influx of calcium into the synapse,calcium being involved in the attachments ofvesicles to the synaptic membrane, which isessential for neurotransmitter release. Thus, cal-cium channels, and their proper functioning,can affect many different neurotransmitter sys-tems. Several different types of calcium channelhave been identified, some of which, such asthe T-type, or the subcomponent alpha-2-delta,have been implicated in the action of some anti-convulsant medications. There is evidence thatcalcium-channel blockers may be effective instabilizing mood in bipolar patients, particu-larly those who are treatment-resistant or arerapid-cycling.
Third Messengers and Other Proteins
Recent research has unravelled many otherintracellular proteins involved in either

Principles of Brain Function and Structure: 1 Genetics, Physiology and Chemistry 17
Table 1.2 Types of dopamine receptors
DA1 DA2 DA3 DA4 DA5
Coupled adenylate cyclase < phospholipase C > adenylate cyclaseChromosome 5 11 3 11 4Highest CNS <neostriatum> paleostriatum hypothalamusDensity nucleus accumbens archicerebellum frontal cortex hippocampus
olfactory tubercle hypothalamusAdenylate cyclase activate inhibits ? inhibits activatesPituitary no yes no yes noAffinity for DA micromol micromol nanomol submicromolar submicromolar
the biology of psychiatric disorders or theaction of psychotropic drugs, for exampleDARPP (dopamine- and cyclic-AMP-regulatedphosphoprotein) and CREB (cAMP-response-element binding) proteins. These form part ofa complex intracellular machinery, leading tolonger-term genetic and synaptic changes incells. It is now known that receptors underthe influence of these factors can actuallymove in and out of synapses. Genes encodingtranscription factors have been referred to asthird messengers. The receptors for steroidhormones are also transcription factors, actingin the cell cytoplasm. New research is focusingon whether these systems are abnormal inpsychiatric disorders, and if so, whether theymight be targets for novel therapies.
A single receptor in a homogenous cell popu-lation may couple differently to different effectorsystems, allowing for a range of activity fromnear antagonism to full agonism.
At the present time many different receptorshave been classified and subclassified, althoughthere is not universal agreement. It shouldbe noted that, when receptor binding studiesare presented, usually either receptor agonistaffinity (Kd) or receptor number (BMax) isreferred to. Receptor reactivity, a third butcrucial variable, is poorly investigated owingto the limitations of in vivo techniques. Some ofthe more relevant receptors for psychiatry arenow presented.
Dopamine
It is now accepted that there are five types ofdopamine receptor (DA1–5). They are all linkedwith a binding protein, and all have been cloned.
There are two subfamilies: DA1 and DA5, andDA2, DA3 and DA4 (see Table 1.2). The firstsubfamily of receptors couples with adenylatecyclase, and the other subfamily couples withphospholipase C, which then inhibits adeny-late cyclase.
The distribution of the D1 and the D2receptors is wide compared with the others, butthis does not relate to functional significance. D3has a limited distribution in the limbic striatum,especially in the olfactory tubercle and nucleusaccumbens, while D4 is found in the prefrontalcortex.
D2, D3 and D4 are also autoreceptors. Theymay inhibit DA cell firing, DA release orsynthesis.
Individual cells have been shown to containboth D1 and D2 receptors. D2 receptors havehigh affinity for traditional antipsychotic drugs,D1 less so. Interestingly, there are less abundantdopamine transporters in the frontal cortex,which suggests that dopamine may act differ-ently there than in the basal ganglia.
Receptors for Excitatory AminoAcids (EAA)
Glutamate and aspartate are the main EAAs.The glutamate receptors are of two main types,AMPA and NMDA. The former have fastkinetics and are coupled to a sodium channel;the latter are slower, having high calciumpermeability, which activates intracellularprocesses. Others include the kainate receptorand the trans-ACPD receptor. Excessive NMDAreceptor activity can lead to excess calciuminflux and neuronal death.

18 Biological Psychiatry
Table 1.3 Agonists and antagonists of adrenoceptors
α-1 α-2 β-1 β-2
Agonists Adrenaline Adrenaline Adrenaline AdrenalineNoradrenaline Clonidine Isoprenaline IsoprenalineMethoxamine Noradrenaline SalbutamolPhenylephrine Terbutaline
Antagonists Phenoxybenzamine Yohimbine Practolol PropranololPhentolamine AtenololPrazosin Metoprolol
Propranolol
The molecular structure of these receptors isknown, and subtypes have been defined. It isthought that NMDA receptors are involved insynaptic plasticity, and probably with LTP andmemory storage.
The NMDA receptor has within it a glycinebinding site, and occupancy of this is nec-essary to allow opening of the channel byglutamate. Phencyclidine, some anaestheticsand MK-801 have high-affinity binding for sitesin the ionic channel. The channel is normallyblocked by magnesium, which is removed ondepolarization.
Many glutamate synapses have two receptorsites – NMDA and non-NMDA – with an inter-action between them. If the non-NMDA receptorfires once, because of the presence of the magne-sium, the NMDA receptor ion channel remainsclosed. The latter is opened only by the cell fir-ing in bursts, with sufficient voltage change inthe post-synaptic neurone to remove the mag-nesium ion and allow an influx of sodium andcalcium.
Glutamate receptors are widely distributedin the cortex, and are linked to activity in theCA1 cells in the hippocampus.
Adrenoceptors
In the same way that dopamine receptors canbe subdivided, so can those for several otherneurotransmitters. The adrenergic receptorsare divided into three main subtypes: α1, α2and β. Each of these has three subtypes:α1a, α1b, α1d, α2a, etc. α1 receptors are postsynap-tic and excitatory, and α2 are both post- andpresynaptic and inhibitory. At the presynaptic
location they are involved in noradrenalinerelease, and their postsynaptic role is unde-termined. Relatively selective agonists andantagonists have been defined for all subtypes(see Table 1.3). The α1 receptor is believed to playa role in smooth muscle contraction and has beenimplicated in effecting blood pressure, nasalcongestion and prostate function. Althoughwidely expressed in the CNS, the central roleof the α1 receptor remains to be determined.Locomotor activation and arousal have beensuggested by some studies. Stimulation of the α1receptor may synergistically increase the activ-ity of the 5-HT neurone in the raphe nucleus,although stimulation of the α2 receptor mayhave the opposite effect. α1 receptors stimulatethe IP3 system; α2 inhibit adenylate cyclase.
The α2 receptor subtypes in the CNS inhibitthe firing of the noradrenaline neurone throughautoreceptors. This mechanism of action isbelieved to mediate the sedative and hypoten-sive effects of the α2 receptors agonist clonidine.Additionally, stimulation of the α2 receptorsdecreases sympathetic activity, which mayexplain the therapeutic utility of clonidine forsuppressing the heightened sympathetic stateof patients in opiate withdrawal.
The β receptor subtypes are more famous fortheir part in slowing cardiac rhythm and lower-ing blood pressure. The functions of the β recep-tors in the CNS, although widely distributed,are not well understood. It is not uncommonto use a β blocker, such as propranolol, to treatperformance anxiety or antipsychotic-inducedakathisia. Whether these benefits come from acentral or peripheral blockage (or both) of theβ receptor is not known. All β subtypes interactwith adenylate cyclase.

Principles of Brain Function and Structure: 1 Genetics, Physiology and Chemistry 19
Histamine Receptors
There are now four histamine receptors,although H4 is predominately in the peripheryand was only recently discovered. The H1receptor is the target for the classic antihis-tamines, which highlights its role in sedationand, conversely, arousal. Of great interest topsychiatrists is the role of H1 in weight gain.Recent analysis has shown that the potential togain weight with antipsychotic agents correlateswith their antagonism for the H1 receptor;examples include clozapine and olanzapine(Han et al., 2008; Nasrallah, 2008).
The H2 receptor is more traditionally associ-ated with the gut. Blockade of the H2 receptorhas been a widely used treatment for pepticulcer disease. The H3 receptor functions as aninhibitory receptor on the histamine neuroneas well as on other non-histamine nerve ter-minals. The role of this receptor is not clearlyunderstood, but may be involved in appetite,arousal and cognition.
5-HT Receptors
The original discovery of the 5-HT receptor ledto two subtypes: 5-HT1 and 5-HT2. Further dis-coveries, especially the application of molecular
cloning techniques, have resulted in multiplesubdivisions of these two receptors and theaddition of several new ones, for a total of 14.While the prospect of activating or blocking thevarious receptors for further refinement of psy-chopharmacological treatment is enticing, theclinical results, with a few exceptions, have beenlimited (see Table 1.4).
The 5-HT1 receptors make up the largest sub-type, with 5-HT1A, 5-HT1B, 5-HT1D, 5-HT1E and5-HT1F. 5-HT1A has received the most interestand seems to play a prominent role in depres-sion and anxiety. It is an autoreceptor on thecell body. Stimulation of this receptor reducescell firing and curtails the release of 5-HT. Howthis would improve mood is unclear, but block-ing this receptor has decreased the effectivenessof tricyclic antidepressants in rat models ofdepression. The anxiolytic buspirone is a partial5-HT1A agonist, which suggests that 5-HT1A hassome role in anxiety. The development and dis-tribution of buspirone is an example of specific5-HT-receptor targeting, which has had only amarginal effect on clinical practice.
The 5-HT1D receptor is also an autorecep-tor but is located on the nerve terminal at thesynapse. There it appears to function to sense the5-HT in the synaptic cleft and turn off releaseof more 5-HT when stimulated. The 5-HT1D
Table 1.4 5-HT receptor subtypes
Main type Sub-main site type Second messenger Agonist (AG)* antagonist (ANT)
5-HT1 a raphe; hippocampus ac buspirone (a)propranolol (ant)
b substantia nigra: globus pallidus ac propranol (ant)d basal ganglia ac metergoline (ant)
sumatriptan (ag)5-HT2 a cerebral cortex; caudate; limbic system IP3 ritanserin (ant)
ketanserin (ant)spiperone (ant)cyproheptadine (ant)mianserin (ant)methysergide (ant)metergoline (ant)
c choroid plexus IP3 m-CPP (ag)5-HT3 entorhinal cortex ion channel quizapine (ant)
ondansetron5-HT4 limbic system; basal ganglia; frontal cortex ac
*Only limited ones given. Note that drugs like quizapine (ag), L-tryptophan (ag), fenfluramine (ag), p-chloroamphetamine (ag), methysergide(ant) and metergoline (ant) act at multiple 5-HT receptors. Ac is adenylate cyclase, IP3 is phosphatidyl inositol.

20 Biological Psychiatry
receptor is stimulated by the antimigraine drugsumatriptan, although the importance of thiseffect in the overall efficacy of the medicationis unclear. Some researchers are exploring theeffectiveness of a 5-HT1D receptor antagonist forthe treatment of depression. The goal is to blockthe negative feedback mediated through the 5-HT1D receptor so that more 5-HT is released intothe synapse.
Other important 5-HT receptors for thepsychiatrist are 5-HT2A and 5-HT2C. The5-HT2A receptor has been identified as playingan important role in the ‘atypical-ness’ of thesecond-generation antipsychotic agents (cloza-pine, risperidone, olanzapine, etc). These neweragents have a greater capacity to block 5-HT2Athan the traditional agents like haloperidol andit is speculated that this results in the observeddecrease in extrapyramidal side effects (EPS)and greater cognitive improvements.
5-HT receptors are involved in the regulationof dopamine and acetylcholine release. 5-HT1Ais an autoreceptor on the cell body and reduces5-HT release; 5-HT3 activation stimulates stri-atal and mesolimbic dopamine release, and itis in mesolimbic areas that many of the 5-HT3binding sites are to be found. In contrast, thisreceptor decreases the release of acetylcholine.5-HT1D is also an autoreceptor, but at the nerveterminal, and also inhibits 5-HT release. Therehas been much interest in the 5-HT2A receptor,because it is involved in the action of the atypicalantipsychotics (Chapter 12).
GABA and Benzodiazepine Receptors
Multiple types of the GABA receptor exist. Thisreceptor is composed of three subunits, alpha,beta and gamma, each with its own isoforms.There are at least six for the alpha, four for thebeta, and two for the gamma. There seem tobe around 48 possible structures of the recep-tor, although it has to be noted that these havebeen identified with the techniques of molecularbiology, not pharmacology. These subunit typesdiffer with respect to their sensitivity for GABAand recognition sites for other molecules suchas the benzodiazepines. For the latter, bind-ing occurs at the alpha subunit, although itrequires the presence of the gamma subunit
for stabilization. Two types of benzodiazepinereceptors are described, BZ1 and BZ2, depend-ing on the alpha subunits from which theyare composed (Doble and Martin, 1992). Otherimportant modulators of the GABA receptorinclude neurosteroids and alcohol.
GABAa receptors are ligand-gated ion chan-nels composed of five subunits, the recognitionsite for GABA being present on the beta unit.Picrotoxin and bicuculline are antagonists, andthey contain a benzodiazepine and a barbitu-rate binding site. They are linked to chloridechannels.
GABAb receptors are coupled to G-proteinand activated by baclofen; they may decreasethe flow of calcium and are not linked to thebenzodiazepine recognition site. The distribu-tion of the subunits in the brain reveals GABAreceptors to be widespread; indeed, GABAis one of the most common neurotransmit-ters, occurring in over 30% of all synapses(Leonard, 1992). Ethanol enhances the functionof the GABA receptor. Long-term use ofethanol decreases the expression of the GABAreceptor, which may explain the tolerancethat develops with alcoholism. Whether thereceptor alterations contribute to the propensityfor seizures when the alcohol is withdrawnremains unclear. The steroid hormones canalso modulate GABA receptors (sometimescalled neurosteroids when they have effects onneurone). The distribution of GABA receptorswith different subunits varies widely in brain;alpha subunits localize especially with 5-HTand catecholamine neurone.
More recently, extra-synaptic GABA recep-tors have been identified, which are thoughtto act by using the overspill of GABA fromthe synapse, and provide tonic backgroundinhibition. This tonic conduction is activatedby low ambient levels of GABA. Research isunderway to find selective agents that act extra-synaptically. These compounds (e.g. gaboxadol)would increase inhibition and perhaps be usefulas a hypnotic or anticonvulsant.
Acetylcholine
Acetylcholine has four protein subunits (alpha,beta, gamma and delta). Muscarinic and

Principles of Brain Function and Structure: 1 Genetics, Physiology and Chemistry 21
nicotinic subtypes are recognized, and five mo-lecularly distinct muscarinic proteins (M1 –M5)have been cloned. They transduce their intra-cellular signals by coupling with G-proteins.
It was with the cholinergic receptor thatscientists first realized that one neurotransmit-ter (ACh) could have different receptors. Theinitial subtypes were identified and namedafter the drug that distinguished their effects.For example, nicotine will stimulate cholinergicreceptors in skeletal muscle but not the heart.Conversely, muscarine will stimulate the heartbut has no effect on skeletal muscle. Thus thetwo receptors can be identified by the actions ofdifferent drugs and the receptors were namedafter those drugs: nicotinic and muscarinic.Unfortunately, it has been hard to find a drugwith unique action on each receptor subtype, sowe have designations such as 1A, 2B and so on.
Many more subtypes of the nicotinic andmuscarinic receptors have been identified sincethe early days of receptor delineation, but thesignificance of these various subtypes remainsobscure. Clearly, ACh is important in cogni-tion and memory, as shown by the benefits ofinhibiting acetylcholinesterase as a treatment forAlzheimer’s disease (Chapter 12). Likewise theblockage of the muscarinic receptor by tricyclicantidepressants and antipsychotic medicationsresults in troublesome dry mouth, constipationand urinary hesitancy (which are genericallyreferred to as the anticholinergic side effects).However, the importance of one receptor sub-type over another has not been shown.
Other Receptors
Many other receptors and their subtypes havebeen identified in the CNS, although often theirfunctional significance is unknown.
Peptide and opiate receptors have been iden-tified. There are at least three classes of opiatereceptor (Reisine and Bell, 1993): delta, kappaand mu. The delta and kappa bind enkephalinsand endorphin, and the kappa receptors binddynorphins. Mu receptors are selectively sen-sitive to morphine. All three types couple toadenylate cyclase, inhibiting cAMP.
Receptors for substance P, enkephalins, pro-lactin, steroids, adenosine (A1 –A3) and even
some drugs such as imipramine, have also beendescribed. In the latter instance, it is the case thatthe imipramine, or another drug such as parox-etine, binds to the 5-HT transporter site. Sigmareceptors, once considered to be opiate recep-tors, are well represented in limbic structures,and have a high affinity for some neuroleptics.
The body and brain produce endogenousendocannabinoid substances. The cannabinoidreceptors are of two types: CB1 is foundin the brain and the heart, CB2 in immuneand hematopoetic cells. They work throughG-protein receptor mechanisms.
Transporters
Neurotransmitter transporters collect releasedtransmitters from the synaptic space, bring-ing them back to the presynaptic terminals.Transport is sodium-dependent, and theirregional distributions are consistent with thoseof their released neurotransmitters. Manydrugs, for example antidepressants, cocaineand amphetamine, act at such sites. The DNAstructures of many transporter sites have nowbeen identified, and while most seem to besituated on neurones, glial localization has alsobeen shown for some transmitters. Reversal offlow through the transporter from the cell backto the synaptic space is known to occur.
The genes coding for the 5-HT transporter (5-HTT), which removes 5-HT from the synapticcleft, have been identified. A polymorphism 5-HTTLPR in the promoter region has 22 basepair repeats, consisting of a short (s) and a long(l) version, which influences the function of thetransporter, the s variant leading to less 5-HTTmRNA and thus higher concentrations of 5-HTin the synaptic cleft.
NEURONES
The main types of cell in the CNS are theneurones and the glial cells. The neurone hasdendrites, an axon, the soma or cell body, andsites for synapses (see Figures 1.10 and 1.14).Essential metabolic molecules are synthesizedin the soma and transported to other regionsof the neurone. The difficult process of movingproducts down the long axon is accomplished

22 Biological Psychiatry
ImipramineCitalopram
Tryptophan Hydroxylaseinhibitor:
p-Chlorophenylalanine
Postsynapticcell
Cell body
Presynapticterminal
Tryptophan
5-HTP
5-HT
5-HT3 receptor2-methyl 5-HT (+)Ondansetron (−)
5-HTIA receptorBuspirone (+)WAY 100635 (−)
5-HT1B/1D receptorCPL 93129 (+)SB 224289 (−)
Vesicular uptake inhibitors
MAO inhibitorsIrreversible, non-selective: PhenelzineReversible, selective: Moclobemide (MAO-A, 'RIMA')
ReserpineTetrabenazine
5-HT2A/2C receptorLSD (+)Ritanserin (−)
Mitochondrion
Receptors
Transporter
Monoamineoxidase
Vesicle
Neuronal uptakeinhibitors
5-HT
5-HIAA
Tryptophan
hydroxylase
Figure 1.14 Example of the manufacture and distribution of 5-HT and various 5-HT receptors and sites ofdrug action (Webster, 2002)
by a microtubular system composed of a proteincalled tubulin. The larger axons are surroundedby a myelin sheath, which aids the speed ofelectrical conduction.
The glial cells vastly outnumber the neurones,and while they play a structural supportiverole, they are also involved in metabolic pro-cesses and the manufacture of myelin. Fivetypes are identified: astrocytes, oligodendro-cytes, microglia, Schwann cells and ependymacells, the latter of which line the inner surface ofthe brain.
The role of glial cells in cerebral activity isstill largely unknown, but astrocytes, whichare closely enmeshed with synapses, also havereceptors for some neurotransmitters, espe-cially glutamate and GABA. Astrocytes haveseveral functions within the CNS in addition totransmitter uptake and release. These includemetabolic support for the neurone, modulation
of synaptic transmission, phagocytosis(microglia) and gap-junction syncitiation forCa++ wave propagation for astrocytic glutamaterelease. By regulating glutamate metabolism theastrocytes are central for glutamate homeostasis.
The synaptic region of the neurone is highlyspecialized for the storage and release of neuro-transmitters. The latter are contained in storagevesicles along with ATP and proteins, and arethere protected from breakdown by intracyto-plasmic degradation enzymes. Release of thetransmitter into the synaptic cleft is by exocy-tosis, and quanta of transmitter are shed intothe synaptic cleft. This process requires cal-cium, which interacts with presynaptic releaseareas, facilitating fusion between the vesicleand cell membranes. Calcium enters the cellterminals through voltage-dependent calciumchannels. The interaction of transmitter withreceptors then takes place, and IPSPs or EPSPs

Principles of Brain Function and Structure: 1 Genetics, Physiology and Chemistry 23
are generated. The synaptic contacts can beto an opposing soma (axo-somatic), dendrite(axo-dendritic) or axon (axo-axonic), and theposition of contact has relevance for the postsy-naptic effect: the nearer to the axon hillock, thegreater the effect.
In contrast to the rather rigid anatomicalstructure shown in cartoons of the neurone,the neurone – especially the dendrites and thesynapses – must be seen as part of a dynamicsystem (Smythies, 2002). The electronic struc-ture of the dendrites is forever shifting: signalsspread from dendrites to soma and vice versa,and the electronic properties of the latter alterwith the resting membrane potential. Synapticresponses are often nonlinear, and related toprior activity.
The synapses themselves should be viewedas quite plastic; they are continually pruned andreplaced. Their receptors are modulated in num-ber and location, endocytosis- and exocytosis-redistributing membrane components, and thehighly regulated intracellular processes direct-ing cell growth, including synaptic modification(Smythies, 2002).
Neurodevelopment and Neurogenesis
It used to be believed that an individual wasborn with a fixed number of neurone and lostthem as they aged. New research has estab-lished that the brain is not such a fixed structure:although the rate of change and development isespecially prominent early in life, alteration ofthe structure of the brain in response to envi-ronmental factors remains a feature across theentire life span.
A single fertilized egg develops into100 billion neurone with 100 trillion connec-tions in a short amount of time. In utero, thisprocess is largely activity-independent andgenetically driven. After birth, interactions withthe environment begin to modify developmentand play a greater role. Unequivocally newlycreated neurone have been identified in thehippocampus of elderly subjects whose brainswere examined shortly after death.
Undifferentiated neural stem cells remain inthe CNS and continue to divide throughout life.They divide into more neural stem cells as well
as neural precursors that grow into neurone orglial cells. But they must migrate away from theinfluence of the stem cell before they can differ-entiate and only about half the cells successfullymove and transform.
Neurotrophic factors are chemicals that areessential for neuron survival and differentia-tion. Nerve growth factor (NGF) is a proto-typical neurotrophin, and NGF receptors arefound on cells which when activated lead torapid intracellular phosphorylation events. Pro-grammed cell death seems to be a processthat occurs across vertebrates and invertebratesalike, and the two main mechanisms are necrosisand apoptosis.
Clear evidence for adult neurogenesis hasbeen limited to the granule cells of the den-tate gyrus and olfactory bulb. Newly formedcells are identified by tagging them with amolecule such as bromodeoxyuridine (BrdU),a thymidine analogue that can be incorporatedinto newly synthesized DNA. A florescent anti-body specific for BrdU is then used to detectthe incorporated molecule and thus indicateDNA replication.
The rate of neurogenesis is modulated byvarious factors. It is known that enrichedenvironments and exercise will increase neu-rogenesis. Additional research suggests thatgonadal steroid hormones may also enhancenew cell production. There is more researchshowing the positive effects of oestrogen onmammal brains, but testosterone will stimulatenerve-cell production in songbirds (Duman,2005). Stress, on the other hand, has aninhibitory effect on neurogenesis. Extendedmaternal separation is a well-characterizedmodel of early-life stress for a rodent. As adults,such rodents will show protracted elevationsof CRF, ACTH and corticosterone (cortisolin a rat), as well as behavioural inhibition inresponse to stress. Rats exposed to prolongedmaternal separation will have a long-lastingblunting of neurogenesis (Fabricius et al., 2008).
Stem Cells
One potential way of rebuilding neurone is toimplant human embryonic stem cells that havebeen isolated from a very immature embryo,

24 Biological Psychiatry
placenta or bone marrow (only 100–200 cells).So far it has been difficult to get these immaturecells to differentiate into functioning neuronesoutside of the olfactory bulb and hippocampus.The problem may be the absence of biochemicalsignals that normally prompt the developingstem cell to migrate and differentiate.
As noted above, it used to be considered thatthe synapse was fixed and static. Indeed, manycartoons of synaptic function falsely reinforcedthis view. In fact, however, the synapse is aconstantly changing and dynamic concept andstructure. Synaptogenesis describes the exten-sive growth of axons and dendrites to makesynaptic connections – a process that primarilyoccurs early in life but continues even in adults.During development, the tips of axons and den-drites have growth cones that appear to reachout with finger-like structures, filopodia, and lit-erally pull the growth cone to its destination. Theaxon is guided in a specific direction by chemicalsignals that attract and repel the growth cone;that is, chemoattractants and chemorepellents.
Another important phase of neuronal celldevelopment is pruning or synaptic elimina-tion, which entails retraction and elimination ofexcessive connections. Some refer to this con-stant struggle of neurones to connect as ‘neuralDarwinism’. The evolution of cortical connec-tivity reflects an adaptation to sensory inputs ina constantly competitive fashion, with winnersand losers depending on the environmental sur-roundings of importance to the organism andinput to the brain (Edeleman, 1989). Disorderedpruning may be the pathological basis for suchconditions as autism and schizophrenia.
Apoptosis is referred to as programmed celldeath, which reflects the fact that the cells actu-ally carry genetic instructions to self-destruct,leaving no scars or damaged tissue.
Neurotrophic Factors
Neurotrophic or nerve-growth factors (NGFs)are best defined as any molecule that affects thenervous system by influencing the growth or dif-ferentiation of neurones or glia. Neurotrophicfactors are the stimulus behind neurogenesisand synaptogenesis (see Figure 1.15). NGFs
Limited supply ofneurotrophic factor
Apoptosis
Synaptogenesis
(a)
(b)
(c)
Figure 1.15 Neurotrophic factors mediate cell pro-liferation and elimination by promoting cell growth,stimulating synaptogenesis and preventing apopto-sis (reproduced with permission from Higgins andGeorge, 2007, Figures 7–8, p. 82)
mediate cell survival, and cells that do notreceive enough NGFs die. Target organs pro-duce NGFs and specific NGF receptors arepresent on nerve terminals which attract affer-ant input.
Several other growth factors have beendiscovered and are being studied, includingneurotrophin-3 (NT-3), glial cell-line-derivedneurotrophin factor (GDNF) and insulin-likegrowth factor (IGF) to name a few, but the oneof most interest is brain-derived neurotrophicfactor (BDNF).
NEUROTRANSMITTERS
A neurotransmitter is a substance that is man-ufactured by a cell, released into the synaptic

Principles of Brain Function and Structure: 1 Genetics, Physiology and Chemistry 25
cleft in response to stimulation and has a spe-cific effect on another cell. In the CNS this cell isa neurone, but peripherally it may be a secretorycell. Further, to qualify, the substance should,when applied experimentally, mimic the effectof the natural release, and some mechanismshould be available to remove it from the synap-tic cleft (Schwartz, 1981).
Although it was at first thought that a singleneurone used only one transmitter, it is nowknown that two or more transmitters can beidentified in many neurones, especially withthe coexistence of a peptide and an amine(see below). In fact, different neurotransmitterssometimes share the same vesicle. Further,while the criteria given for neurotransmitterstatus have been identified, the situation is notso clearly defined. Thus it is possible to seeall levels of chemical communication betweencells, from direct neurone–neurone contact,through to neurosecretory cells that release neu-rohormones either into the hypophyseal portalsystem, which influences pituitary cell output,or directly into the circulation via the posteriorpituitary gland (neurohypophysis). Receptorsfor some neurohormones have been identifiedin the brain, and the possibility of feedbackfrom release into the peripheral circulationexists. Finally, as in the autonomic system, neu-rones make contact with adrenal medullacells, directly influencing hormonal output.
The situation is further complicated by theconcept of neuromodulators. Thus, the action ofneurotransmitters is considered to be brief andto operate over a short distance. However, someneurotransmitter candidates, especially the pep-tides, lead to longer alterations of synaptic tone,modulating the environment of other ongoingneurotransmitter events.
Of the many potential transmitters, the syn-thesis of a few key ones is described.
Acetylcholine
This is synthesized from choline and acetylcoenzyme A, the reaction being catalysed bycholine acetyltransferase. Following release intothe synaptic cleft, it is broken down by acetyl-cholinesterase. It is the main transmitter used
by motor neurones in the spinal cord and isthe transmitter for all preganglionic autonomicneurones and for postganglionic parasympa-thetic neurones. In the CNS it is found in highconcentration in the caudate nucleus and hip-pocampus, and an ascending cholinergic systemhas been defined innervating the thalamus, thestriatum, the cerebellum, the limbic system andthe cerebral cortex. The basal nucleus of Meynertis an important CNS location of acetylycholine.
GABA
GABA is synthesized from L-glutamate, uti-lizing the enzyme glutamate decarboxylase(GAD). It is metabolized by GABA transaminaseto glutamic acid and succinic semialdehyde,which, following oxidation, enters the citricacid cycle. It is involved in the activity ofsome 30–50% of CNS neurones, especiallyof interneurones. The highest concentrationsof GABA are in the substantia nigra, globuspallidus, hippocampus, hypothalamus andcortex. In the spinal column it is in the spinalgrey matter. It is an inhibitory transmitter,and antagonists such as bicuculline provokeconvulsions. It is one of a group of amino acidtransmitters that have a ubiquitous distribution,some of which serve as substrates in metaboliccycles. These include glycine, beta-alanine,glutamate and aspartate.
Glycine
Glycine is another inhibitory transmitter, espe-cially in the spinal cord and brainstem. It inhibitsneuronal firing by gating chloride channels. Itcan modulate the action of glutamate at theNMDA receptor.
Serotonin (5-HT)
This is one of the amine neurotransmitters; oth-ers include dopamine and noradrenaline. It issynthesized from tryptophan under the influ-ence of the enzyme tryptophan hydroxylase,which converts it to 5-hydroxy-tryptophan. Thisis decarboxylated to 5-HT. It is metabolized to

26 Biological Psychiatry
5-hydroxyindole acetic acid (5-HIAA) by theenzyme monoamine oxidase.
The main nuclei containing 5-HT are theraphe nuclei of the brainstem, from which fibresascend and descend to influence many areas ofthe brain, especially the neocortex, limbic sys-tem, thalamus and hypothalamus. In the pinealgland, 5-HT is converted to melatonin.
Catecholamines
These are metabolized from tyrosine. Conver-sion to DOPA occurs under the influence of tyro-sine hydrolase. DOPA is then decarboxylated todopamine. In the presence of dopamine-betahydrolase this is converted to noradrenaline. Ina few areas, N-methylation of the latter resultsin adrenaline.
Breakdown involves two main enzymesystems: monoamine oxidase and catechol-O-methyl transferase. The former acts mainly in-traneuronally, the latter in the synaptic cleft. Themain metabolites of dopamine are homovanillicacid (HVA) and DOPAC, while noradrenaline(NA) breaks down to vanillomandelic add(VMA) and methoxyhydroxy-phenylglycol(MHPG).
Noradrenaline is the transmitter at post-ganglionic sympathetic neurones, but in thebrain the main synthesizing neurones are inthe brainstem, the locus coeruleus and relatednuclei. The ascending neurones terminatewidely to influence the cerebral cortex, limbicsystem and hypothalamus. Catechol O-methyltransferase, responsible for breaking down thecatecholamines, is regulated by the COMT gene,which has polymorphisms, and of importance isthe Met (methionine)–Val (valine) substitutionat codon 158 of chromosome 22q. The Met alleleis associated with low enzyme activity, and theVal with high activity.
Dopamine derives from nuclei in the brain-stem(notablythesubstantianigraandtheventraltegmental area), but its output is more restrictedthan noradrenaline or 5-HT. In particular, itinvolves the striatum and the limbic system. It isof interest that cortical dopamine projections inprimates suggest a functional specialization. Themajor influences are motor rather than sensory:
sensory association areas have more dopaminethan primary sensory regions, and auditoryassociation cortex has more than visual associa-tion areas (Lewis et al.,1986). A further locationof dopamine is in the tuberoinfundibular systemof the hypothalamus, which is involved in theregulation of prolactin release, with stimulationleading to inhibition.
Peptides
Many peptides that may have a central role,either as neurotransmitters or as neuromodula-tors, have been recognized. In contrast to classicneurotransmitters, they are large molecules andare composed of chains of aminoacids. A list ofthese is given in Table 1.5. At present the evi-dence that many are actually transmitters awaitsconfirmation. Moreover, attempts at developingtreatments based on peptides have been disap-pointing to date. Most peptides are formed by
Table 1.5 Potential peptide neurotransmitters
ACTH
AngiotensinBombesinBradykininCalcitoninCarnosineCCK (cholecystokinin)CRF (corticotrophin releasing factor)DynorphinBeta-endorphinMet-enkephalinLeu-enkephalinGastrinGlucagonGrowth hormoneLipotropinLHRHAlpha-MSHMotilinNeuropeptide YNeurotensinOxytocinProlactinSecretinSomatostatinSubstance PTRHVasopressinVIP

Principles of Brain Function and Structure: 1 Genetics, Physiology and Chemistry 27
cleavage of larger precursors and understandingof the functional significance of the fragments isquite incomplete.
An interesting feature of the peptides is theirwide distribution throughout the body, identicalones being found, for example, in the gut and thebrain. These include cholecystokinin, vasoactiveintestinal peptide (VIP) and gastrin. It can beseen that several are hormones.
Peptide receptors are coupled mainly withsecondary messenger systems.
Enkephalins
These were the first morphine-like (endorphin)substances to be discovered in the brain, beingpenta peptides. They were shown to possessopiate-like activity, along with other pep-tides such as beta-endorphin and dynorphin.Enkephalin neurones and opiate receptorshave been identified in the limbic system andstriatum, and receptors in such areas as thehippocampus, nucleus accumbens, thalamusand amygdala. They occur in several areasof the spinal cord, including the substantiagelatinosa. Beta-endorpin distribution is morerestricted, the highest concentration being inthe pituitary, which structure is almost devoidof enkephalins. Mu receptors are more relatedto sensory events, being found in the cerebralcortex, whereas the limbic system has anabundance of delta receptors.
Neurotensin
This is found in high concentrations in thehypothalamus, basal ganglia and amygdala. Itinhibits neuronal firing in the locus coeruleus,where neurotensin is abundant. Receptor sitesin the brain are widespread.
Substance P
This occurs in dorsal root ganglia, with termi-nals in the substantia gelatinosa, a region ofthe spinal cord thought to be involved in thepain pathways. It is found in high concentra-tions in the striatal–nigral system, the habenula,
the amygdala and the bed nucleus of the striaterminalis.
Cholecystokinin
This is found in high concentrations in thecortex, it and VIP being brain peptides wellrepresented within cells in the cortex. It is foundin the hypothalamus, and terminals are in theamygdala. It also is seen in the periaqueductalgrey region and, like substance P, in the dorsalroot ganglia cells.
Vasoactive Intestinal Peptide
Highest levels are found in the cerebral cor-tex, and terminals containing it are identifiedin the amygdala and the hypothalamus. In thebody it has several functions, including vasodi-lation and enhancing lipolysis and pancreaticsecretion.
Angiotensin
This has for some time been known to beinvolved in vasoconstriction and sodium reg-ulation by the kidney. It is found centrallyin several regions, including the hypothala-mus, and many angiotensin receptor sites havebeen identified. Complementing its peripheralaction, it is involved in the central regulation ofdrinking.
Releasing Factors
These are found in the median eminenceof the hypothalamus, and pass through theportal capillaries to influence hormonal releasefrom the anterior pituitary. They includethyrotropin-releasing hormone (TRH), a tripep-tide, the majority of which is found outside thehypothalamus. Somatostatin inhibits growthhormone release and is found in the amygdala,hippocampus and cortex, with terminals inthese sites and in the striatum. Luteinizinghormone-releasing factor (LHRH) stimulatesLH and FSH release, and is found primarily in

28 Biological Psychiatry
Precursor
CLASSICALTRANSMITTERS
Nuclear synthesis of propeptide
Axonal transport
PEPTIDES
SLOWRECEPTOR
EVENTS
Processing en route
Breakdown by peptidases
Distant actions
FAST SLOW
RECEPTOR EVENTS
NUCLEUS mRNA
Breakdown
Synthesis
Reuptake
Figure 1.16 Comparison of the manufacture andrelease of classical neurotransmitters and peptides(Webster, 2002)
the hypothalamus. Corticotropin-releasingfactor (CRF) releases ACTH. Various medica-tions modifying CRF were once consideredpromising candidates as anxiolytics or anti-depressants but were disappointing in clini-cal trials.
Other Central Peptides
The posterior pituitary hormones oxytocin andvasopressin seem to have a central role, withpathways projecting to some brainstem andlimbic-system structures. These two peptidesappear to act selectively in some animals interms of promoting or inhibiting interpersonalbonding (Stein and Ythilingum, 2009; Younget al., 2008). Active investigation involvesadministering synthetic oxytocin and observ-ing changes in interpersonal behaviour, andin disorders of bonding such as autism.Adrenocorticotrophic hormone (ACTH) isfound throughout the brain, especially in thehypothalamus, thalamus, periaqueductal greyand reticular formation.
Some of the differences between the pep-tide transmitters and the more classical onesare summarized by Hokfelt et al. (1980) and areshown in Figure 1.16. In particular, peptidesare produced in the cell soma and not synthe-sized at synaptosomes, unlike other transmit-ters, and there are no re-uptake mechanismsfrom the synaptic cleft. This may be compen-sated for by their effective action at much lower
Table 1.6 The coexistence of classical and peptide transmitters
Transmitter Peptide Location
Dopamine Enkephalin Carotid bodyDopamine CCK Ventral tegmental areaNoradrenaline Somatostatin Adrenal medullaNoradrenaline Enkephalin Adrenal medullaNoradrenaline Neurotensin Adrenal medulla5-HT Substance P Medulla oblongata5-HT TRH Medulla oblongataAdrenaline Enkephalin Adrenal medullaAcetylcholine VIP Autonomic ganglia, sweat glands

Principles of Brain Function and Structure: 1 Genetics, Physiology and Chemistry 29
concentrations, their more prolonged action andtheir intermittent rather than tonic release.
INTERRELATIONSHIPS AMONGTRANSMITTERS
Dale’s principle, namely that one neuronesynthesizes and releases only one neurotrans-mitter, has had to be modified in the lightof recent data. Although it has been knownfor some time that certain neurones probablyreleased both acetylcholine and noradrenaline,the coexistence of peptides and other neu-rotransmitters has been reported for severalneurone groups. A list is shown in Table 1.6.However, not all neurones possessing oneclassical transmitter contain the same peptide,and vice versa. The functional significance ofsuch arrangements has been a matter of specu-lation. For example, in one group of neuronesfrom sympathetic ganglia involved in sweatgland secretion, both acetylcholine and VIP arepresent (Hokfelt et al., 1980). It is suggested thatthe VIP may be the mediator of vasodilationaiding the acetylcholine-primed secretion. Afurther example is the coexistence of CCK ina subpopulation of dopamine neurones. Theseare mainly in the substantia nigra and relatedventral tegmental area (VTA), and project to thelimbic forebrain (Hokfelt et al., 1980).
Other examples of interaction include theinfluence of monoamine release by peptides,such as the association between substanceP and dopamine, the former acting as an
excitatory transmitter for some dopamine neu-rones (Iversen and Iversen, 1981), or peptidesinteracting with peptides as in the case of opiatereceptors located on substance P terminals.
TRANSMITTER DISPERSAL
Following interaction with the postsynaptic cell,transmitters are either broken down by enzymesystems in the synaptic cleft or taken back up bythe neurone for degradation for re-use. Someare lost by simple diffusion away from thecell. The intracellular enzymes, monoamine oxi-dase and catechol-O-methyl transferase, are ofimportance to the amine transmitters, and themajor extracellular mechanism for the degra-dation of acetylcholine is acetylcholinesterase.Peptides are degraded by peptidases.
CNS INFLAMMATION
Cytokines are produced by activated macro-phages, and are either proinflammatory (inter-feron, INF, and tumour necrosis factor, TNF)or anti-inflammatory (interleukin 4 or 10, IL4/IL10). A cascade of events leads to T-helper lym-phocyte activation, and these release cytokines.There are receptors for these cytokines in thebrain, and they have been shown to activatethe CRF system. The ratio between pro-inflammatory and anti-inflammatory cytokinescan be measured, and has been shown to relateto psychopathology.


2Principles of Brain Functionand Structure: 2 Anatomy
INTRODUCTION
This chapter concentrates on those areas of thebrain of most importance to biological psychia-try. After a brief introduction to neuroanatomy,the limbic system, the basal ganglia, the tha-lamus and some important cortical areas arediscussed. In the past it was common to refer todifferent areas of the brain using modular mod-els. However, theories using strict localizationof function to adequately explain behaviour,especially with regard to psychiatry, failed. Itthen became popular to consider systems, suchas the limbic system, but renewing localizationtheories with respect to ‘systems’ would alsolikely fail.
The most recent concepts of brain behaviourrelationships have to some extent developedfrom the era of artificial intelligence. Althoughsome have been led to adopt an unusual view,namely that cognition is similar in process toa computer algorithm and therefore there is nonecessity to understand the hardware (i.e. thebrain itself) in order to understand how thebrain works and how consciousness develops,this is clearly illogical. There are indeed manydifferences between brains and current mod-ern computers. While the latter are good atarithmetical computations, logical thinking andexhaustive memory searching, brains are bet-ter at pattern recognition and the use of con-text to interpret the whole (as in language,
Biological Psychiatry 3e Michael R. Trimble and Mark S. George 2010 John Wiley & Sons, Ltd
for example). Processing is in parallel, not insequence, hence the development of modelsreferred to as parallel distributed processing(PDP). As information is added to a computer,it gets slower; the exact opposite occurs withthe brain.
In PDP, information is no longer thought ofas being represented by a sequence of numbers,but by a pattern of activation. Information isstored in connections among processing units,each with a graded activity value, a probabilityof firing. There is a weighted connection withother units, and it is the pattern of the activationthat is relevant (Figure 2.1). Learning is thus achange in connection weights over time. Crucialto the development of these models has been theconcept of back propagation, which allows forcomputations in multilayer networks continu-ally adjusting connection weights depending onoutput patterns. The system can literally learnon its own, in keeping with the concept of neu-ral Darwinism (Edelman, 1989). As discussed inChapter 1, during development many neuronesdie, and competition leads to unique wiringrepertoires as the strengths of certain synapsesamplify, allowing organisms to respond to expe-rience. These circuits (maps) have intercon-nections with others, leading to higher-ordermaps that map maps, with parallel re-entrantsignalling between them. This allows differentproperties of an input, for example visual and

32 Biological Psychiatry
outputs
outputs
outputs
inputs
inputs(c)
(a) (b)inputs
Figure 2.1 Three types of network. (a) Feedforward,with one layer of weights connecting the input to theoutput units. (b) Feedforward, with two layers ofweights and one hidden layer of units between theinput and output units. (c) Recurrent, with recipro-cal connections (reproduced with permission fromChurchland and Sejnowski, 1992; Biol Psych, 2 Ed,p. 77)
tactile, to be connected in the response of higher-order networks, explaining such cognitive phe-nomena as categorization and generalization.
THE NEUROANATOMY OF EMOTION
Although great strides were made in neu-roanatomy and neurophysiology in the 19thcentury, little progress was made in under-standing how emotions were represented neu-rologically. William James suggested that theemotions are derived from sensory inputs tothe brain, which activate motor outputs, whichthe brain perceives as the emotion. We donot run away from something because we arefrightened; we experience fear because weare running away. However, there was noobvious cerebral location for the generationof emotion, although the sensory experienceswere known to be received cortically, namelyin the parietal regions of the brain.
The James-Lange hypothesis was soon testedand shown to be wrong from two avenues.
First, it was shown in animals that removal ofthe cortex of the brain on both sides did notabolish the expression of emotion. Second, itwas revealed that direct electrical stimulation ofvarious structures buried deep within the braincould lead to the release of emotion.
The Brain
The CNS axis is composed of several identifiablecomponents: the cerebrum, the cerebellum (thesmaller lobe at the posterior base of the cere-brum), the brainstem and the spinal cord. Infor-mation flows up the spinal cord from peripheralsensory receptors, which send signals to thebrain concerning the external and the internalenvironments of the organism; many such affer-ent nerve tracts have been identified within thespinal cord. Information travels to the musclesfrom the brain down the spinal cord, again inidentified pathways referred to as ‘efferent’. Inthe brainstem reside many of the nerves whichcontrol autonomic functions such as breathing,heart rate and so on, and several of the cranialnerves begin or terminate there.
Divisions of the Brain
The brain itself has been divided, purely onvisual anatomical grounds, into four main lobes:the frontal, the parietal, the occipital and thetemporal. Some also refer to the insula compo-nent as a lobe. The neocortex, so called becausein phylogenetic terms it is the most recent, isthat which is generally seen on surface inspec-tion of the brain. The gyrae and sulcae formthe irregular, undulating patterns of the corti-cal mantel, the former being composed of greyand white matter, the latter forming the spacesin between. The grey matter is formed by theneurones, and the white matter is composedof the fibre bundles of myelinated axons, whichstretch from one neurone population to another,interconnecting circuits of information.
Most sensory data initially terminate in a col-lection of nuclei situated subcortically in thethalamus. This is one of several identifiable sub-cortical collections of nuclei which are important

Principles of Brain Function and Structure: 2 Anatomy 33
to an understanding of the cerebral represen-tatives of emotion. Others include the basalganglia (striatal structures), the accumbens andthe limbic system, referred to by some as thelimbic lobe.
From the thalamus, information is passed onto the neocortex, arriving in a primary sensoryarea, such as one selective for vision or for touch.These are mainly in the occipital and parietalareas of the brain. There then occurs a cascade ofinformation flow, from these primary receptiveareas to the secondary, tertiary and then associ-ation cortices of the brain, during which transferthe representations are fused, amalgamated andcombined, such that while artificial stimulationof say the first visual receptive area will leadto the experience of flashes of light, stimula-tion in the temporal lobe association areas cansometimes lead to complex visual (and other)hallucinations. Information then flows to thelimbic related cortex (Figure 2.2). An exceptionto the above generalization is the olfactory sys-tem; this first enters the brain at one of the limbicnuclei, as will be discussed below.
Information flow out of the brain descendsfrom the motor areas of the neocortex, downthe pyramidal tracts to the spinal cord (thepyramidal system), where neurones emerge toinfluence movements by connecting with mus-cle cells. Other key structures which influencemovement and permit the smooth pursuit ofaction are the cerebellum and the basal ganglia,the motor paths of the latter being referred to asthe extrapyramidal motor system.
There is also much cross-talk within the brain,with some white matter commissures connect-ing areas within one hemisphere, and othersconnecting points across the hemispheres. Thelargest of the latter is called the corpus callosum.
The four main domains of the cerebral hemi-sphere of mammals are then the neocortex, thelimbic lobe, the thalamus and the basal ganglia.The neocortex (also referred to as isocortex) issix-layered, with extensive subcortical connec-tions, and provides the mantle for the structuresof the other three divisions. Within the limbiclobe, the most relevant structures are the amyg-dala and the hippocampus, and their afferent
(a) (b)
Figure 2.2 Input (a) and output (b) connections of the human entorhinalcortex (area 28). Area 35 is referredto as the perirhinal area. The input is multimodal and known to be associated with episodic memories. Theoutput connections are associated with memory consolidation in association cortices (courtesy of Dr vanHoesen)

34 Biological Psychiatry
and efferent connections. These and relatedstructures are referred to as allocortex (essen-tially ‘older cortex’). The very oldest cortex isreferred to as archicortex. The medial forebrainbundle is a continuum of interconnected neu-rones and pathways extending caudally to themidbrain and hind brain (Figure 2.3).
The term ‘agranular cortex’ refers to isocor-tex that lacks a clear layer 4 (internal granularlayer). The layers and columns of the isocor-tex have allowed neuroscientists to parcel outthe cortex into various regions. The numberhas varied from as low as four (Bayley andBonin) to over 150 (Vogt). The most popularscheme in use is that of Constantin Brodmann(see Figure 2.33), but it must be noted thatthis method does not take into account inter-subject variability, and only considers one thirdof the cortex, missing all the tissue buriedwithin the sulci. The Talairach Atlas is a widelyused three-dimensional atlas, taking its startingpoint for defining coordinates from the anterior
CINGULATE GYRUS
CINGULUM
S.C.
HippocampusHippocampal gyrus
AMYGDALA
PIT.
HYP.
M.L.M.A.
C.G.
G.
(1)
(2) SEPTUM
M.F.B.
FORNIX
A.T.
OLF.BULB
D.B.
Medial forebrain bundle
Figure 2.3 The main limibic structures as envi-sioned by MacLean. MacLean added the amygdala tothe limbic concept of Papez. MFB = Medial ForebrainBundle. AT, Anterior Thalamus; 1 and 2, ascendingpathways to the limbic lobe; CG, Central Grey ofmidbrain; G, dorsal tegmental nucleus of Godden;DB, Diagonal Band of Broca; Hyp, hypothalamus;LMA, Limbic Midbrain Area; M, Mamillary body;Pit, Pituiatry gland; SC, Superior Colliculus
commissure (0, 00). However, this too does nottake sulci into account, and cannot identify bor-ders between histologically defined areas (as perBrodmann). In imaging studies, it has becomefashionable to refer from the Talairach coordi-nates to a putative Brodmann area, transformingthe latter into a three-dimensional space. Thisextrapolation from individual results into amorphed three-dimensional atlas and then oninto a two-dimensional projection (Brodmann)should be viewed with caution. It is really littlemore than an educated guess (see Chapter 4).Recently, attempts have been made to defineborders within the brain more precisely usingchemical markers. Radioactive ligands are usedfor high-resolution quantitative in vitro recep-tor autoradiography, which outlines receptorarchitechtonics, allowing a neurochemical ‘fin-gerprint’ of brain areas to be developed.
The basal ganglia are a collection of struc-tures (the corpus striatum: the putamen and theglobus pallidus, connected with the substan-tia nigra and the subthalamic nucleus) whoseefferents remain largely within the forebrain,forming so-called parallel distributed circuits,whereby the termination of a loop in the cortexis near to or at the site of the cortical origin ofthe loop (see below) (Figure 2.4).
Figure 2.4 The circuits linking the frontal cortexwith the basal ganglia, the basal ganglia with thethalamus, and the thalamus with a re-entrant cir-cuit back to frontal cortex. Note: the temporal-limbicinputs to the circuitry

Principles of Brain Function and Structure: 2 Anatomy 35
The Limbic System
As already noted, James had no idea how emo-tions could be represented in the brain otherthan by suggesting the sensory neocortex asa site of integration of bodily sensations rep-resenting an emotional state. The concept thatcertain brain structures could form the founda-tion of an emotional brain system was a stunningdeparture for neurology, and the launch padof the disciplines of biological psychiatry andbehavioural neurology (that branch of neurol-ogy which tries to understand how neurologicaldisorders relate to behavioural changes).
Papez delineated his proposed cerebralmechanism of emotion in 1937. The keycomponents of his now-famous circuit werethe hippocampus, the cingulate gyri, themammillary bodies and the anterior thalamus.For him, the cingulate cortex was a receptivearea for experiencing emotion, in the same waythat the visual areas of the brain are receptivefor visual information. While the hypothalamuswas essential for the expression of emotion, theexperience required the cortex, ‘the stream offeeling’ depending on strong interconnectionsbetween the cortex and the hypothalamus.He summed this up with the famous quotethat ‘the hypothalamus, the anterior thalamicnuclei, the gyrus cinguli, the hippocampus andtheir interconnections constitute a harmoniousmechanism which may elaborate the functions
Fornix
Cingulategyrus
Anteriornucleus ofdorsalthalamus
Mamillo-thalamic tract
Mammillarybody Hippocampus
Parahippocampalgyrus
Figure 2.5 Circuit of Papez. A coloured version ofthis figure can be found on the colour plate
of central emotion, as well as participate inemotional expression’ (Figure 2.5).
The key structures of the limbic system,as originally outlined by MacLean but elab-orated on by others, are the amygdala andthe hippocampus, both neuronal aggregates ofconsiderable complexity, and their immediateconnecting structures, such as the orbital partof the frontal cortex and the so-called ventralstriatum: that part of the brain’s extrapyramidalsystem that relates to emotional motor expres-sion. In humans, on account of the migrationof the temporal lobes posteriorly, inferiorly andthen anteriorly, and the large increase in size ofthe corpus callosum in development, muchof the archicortex (evolutionary older cortex)lies folded and buried in the medial temporallobe in the hippocampus.
The cingulate gyrus surrounds the corpuscallosum, forming a C-shaped band, linkingposteriorly with the parahippocampal gyrusand connecting extensively with neocorticalstructures. The frontal lobes of the brain havemany demarcated subregions, but the orbital,medial and dorsolateral are the most frequentlyreferred to. The orbitofrontal cortex lies overthe floor of the anterior cranial fossa and hasintimate connections with the anterior insula,the amygdala, the ventral striatum and thesensory projection pathways. The ventromedialfrontal cortex is a part of the cingulate region.The insula is a large limbic structure, whichin contrast to most limbic components is notvisible from the medial surface of the brain,and lies laterally, but buried beneath folds ofneocortex (Figure 2.6). Many have found causeto cavil with the term ‘limbic system’. Someneuroanatomists now prefer to use the term‘limbic lobe’ after the original designation ofBroca, an aid to breaking down the conceptof an isolated system (Heimer et al., 2007). Itwas the development of new techniques inneuroanatomy, such as the use of horseradishperoxidase (HRP), histofluoresecence, autora-diography and improved silver-stainingmethods that led to a Renaissance in interest inand understanding of the structure, connectiv-ity and functions of the limbic lobe, especiallyits cortical–subcortical interactions, and the

36 Biological Psychiatry
Figure 2.6 The insula, buried beneath the cortex fol-lowing removal of the frontal and temporal polaropercula. The position of the amygdala, hippocam-pus and entorhinal cortex are shown (courtesy ofDr Gary van Hoesen). A coloured version of thisfigure can be found on the colour plate
relevance of these to an understanding of theneuroanatomy of emotion and behaviour.
Although Broca’s term was topographical,the limbic lobe may be differentiated from othercortical structures by cellular-staining meth-ods and susceptibility to certain disease pro-cesses. A recent definition of the limbic lobeis given by Heimer et al. (2007) as: ‘composedof the olfactory allocortex, hippocampal allo-cortex, and transitional cortical areas that inter-vene between these and larger isocortices. Thetransitional areas are numerous, and form thebulk of the limbic lobe, and depart in termsof structure in one or more ways from theisocortex. . . Limbic lobe cortical areas form thecingulate and parahippocampal gyri as wellas the bridging caudal orbitofrontal, medialfrontal, temporopolar, anteroventral insular andretrosplenial cortices. . . We also favour inclu-sion of the laterobasal–cortical complex of theamygdala. . .’ (Figure 2.7).
An extension of the original limbic systemconcept was suggested by Nauta and Domesick(1982). They included the posterior orbito-frontal cortex and the temporal pole, whichproject to the amygdala and hippocampus, andsome subcortical structures linked by recip-rocal pathways. These include the accumbens
Figure 2.7 Medial view of the human brain. The areas shown in darker colours represent limbic structures(courtesy of Dr L. Heimer). A coloured version of this figure can be found on the colour plate

Principles of Brain Function and Structure: 2 Anatomy 37
and such midbrain structures as the ventraltegmental area (VTA) and the interpeduncularnucleus. The inclusion of the latter has led tothe designation of a midbrain limbic area, themesolimbic system.
Nieuwenhuys (1996) has introduced theterm ‘greater limbic system’, which alsoincludes pontine and medullary neuronalgroups that relate to autonomic and somato-motor integration. He pointed out that this
BNST
PAG (1)
LTA6sc A6
PBN
va
C2SOLA29
6
12
va
15,5 cm fia.4
ve
se
ve
se + be
7
10A1
C1
sa
st
fld
fmt
f
Figure 2.8 Extended limbic circuitry. Note how the limbic connections output to diencephalic, midbrainand brain-stem structures. Abbreviations: A, amygdala; A1, A2, A5, A7, noradrenergic cell groups; A6, thenoradrenergic locus coeruleus; A6sc, the noradrenergic locus subcoeruleus; bc, branchial efferent fibres;BNST, bed nucleus of stria terminalis; C1, C2, adrenergic cell groups; f, fornix; fld, fasciculus longitudinalisdorsalis; fmt, fasciculus medialis telencephali; H, hippocampus; Hy, hypothalamus; L, L-region of Holstegeet al. (1986); LT, lateral pontine tegmentum; M, M-region of Holstege et al. (1986); PAG, periaquaductal grey;S, septum; se, somatic efferent fibres; ve, visceral efferent fibres; 1, loci for defence reactions, vocalizationand lordosis; 2, mesencephalic attack site; 3, pontine attack site; 4, mesencephalic locomotor region; 5, areareticularis superficialis ventrolateralis or ‘lateral medulla’, implicated in cardiovascular and respiratoryregulation; 6, dorsal respiratory group; 7, ventral respiratory group; 8, Kolliker-Fuse nucleus: pneumotaxiccentre; 9, dorsomedial swallowing area; 10, ventrolateral swallowing area; 11, pontine swallowing area;12, nucleus retroambiguus, containing loci for vocalization and lordosis (reproduced with permission fromR. Nieuwenhuys, and from Nieuwenhuys, 1996; Biol Psych, 2 Ed, p. 93)

38 Biological Psychiatry
‘system’ is composed of masses of thin andultrathin nerve fibres, and has embedded intoit neuronal groups related to monoamine andpeptide activity, and contains loci from whichintegrated patterns of behaviour can be elicited(see Figure 2.8).
It is important to recognize that anatomically,the limbic lobe is non-isocortical, not six-layered,and consists of allocortex and belts of agranularor dyslaminar (layer 4 missing, poorly orga-nized or atypical) transitional cortex. In otherwords, one possible definition of limbic cortexis those areas of cortex that are NOT isocortical(six-layered).
The inputs to the limbic system have beenshown to be both interoceptive (visceral) andexteroceptive (conveying information aboutthe environment). The former derive frommany structures that give information aboutthe internal state of the organism, and includemodulating influences from neurotransmitterpathways, which originate in the mid andhind brain, which help drive behaviour andmodulate mood, such as dopamine, 5-HTand noradrenaline. The exteroceptive afferentsderive from all sensory systems, and ultimatelypresent complex integrated sensory informa-tion to the cortex of the hippocampus and theamygdala (see Figure 2.2).
The Basal Ganglia
The demonstration that the basal gangliaextend all the way to the ventral surface ofthe brain, and that the inputs to the corpusstriatum involve not only the whole of thecortical mantle but also limbic structures,allowed for a differentiation between the ventaland dorsal striata, respectively receiving theirmain inputs from the limbic lobe and theneocortex (see Figures 2.9 and 2.10). A mainarea of the ventral striatum is referred to asthe accumbens, which is heavily afferentedfrom the cortical amygdala and hippocampus,and the prefrontal and temporal associationcortices. The main output from the ventralstriatum is to the ventral globus pallidus andthence to the thalamus, which then projectsback to the frontal cortex. This is but one of sev-eral cortico–striatopallidal–thalamic–cortical
DLPFCPremotor
Motor
Cd
Pu
Striatum(caudal)
Cd
PuCSh
Striatum(rostral)
Greater Lim
bicLobe
Isocortical Frontal Lobe
Figure 2.9 Diagram of the cortical projections (fromfrontal and limbic cortices), showing how the cortexprojects to the basal ganglia and how this processis continuous; in essence there is no discrete breakbetween the frontal inputs and limbic inputs. Itshould be noted that this figure helps to emphasizethat cortico-striatal projections come from the entirecerebral cortex. Cd = caudate nucleus; Pu = putamen;C = core and Sh = shell of accumbens (courtesy ofDr L. Heimer). A coloured version of this figure canbe found on the colour plate
re-entrant loops to have been defined, whichhave important regulatory properties govern-ing behaviour (Figure 2.11). The loop fromthe motor cortex (dorsal striatum) is involvedwith somatomotor activity, while the ventrallimbic–striatal circuits modulate reward andmotivation. Figure 2.12 shows a cartoon ofthese loops, and inserted are the indirect anddirect loops. Essentially these refer to twodifferent projections through the basal ganglia,which through inhibition and excitation balanceoutput from the globus pallidus internus tothe thalamus and hence back to the cortex.Disturbance of this balance results in symp-tomatology, such as the motor manifestationsof Parkinson’s disease or the compulsivephenomena of obsessive-compulsive disorder.There is a close anatomical association betweenthe globus pallidus interna and the substantianigra pars reticulata.

Principles of Brain Function and Structure: 2 Anatomy 39
Thalamus
Dorsalstriatum
Ventralstriatum
Ventralpallidum
(SI)
Amygdala
DA pathway fromventral tegmental area
(a) (b)
"Non-specific"thalamic nuclei
To mediodorsalnucleus
Dorsalpallidum
Thalamus
Neocortex
Allocortexfrontal-temporal
association cortex
DA pathway fromsubstantia nigra
''Non-specific"thalamic nuclei
To ventral anterior andventral lateral nuclei
Caudate-putamen Globus
pallidusMotorcortex
Anteriorcingulate and
prefrontalcortex
Allocortex
Olfactorytubercle
Ventralstriatum
Ventralpallidum
Ventrallateral
Mediodorsal
Figure 2.10 (a) Cartoons showing the classical distinction between the ventral and dorsal cortico-striato-pallido-thelamic re-entrant circuits. Image (b) emphasizes the parallel character of the re-entrant circuits(courtesy of Dr L. Heimer)
Figure 2.11 The basic anatomy of the cortico-striato-thalamic re-entrant loops

40 Biological Psychiatry
Figure 2.12 A similar anatomy to that in Figure 2.11, but emphasizing the external as well as the internalglobus pallidus connections, and the role of the subthalamic nucleus in regulating the output from the globuspallidus internus to the thalamus and hence the cortex. GPe = globus pallidus externus; GPi = globus pallidusinternus; STN = subthalamic nucleus and SN = substantia nigra
BLopt
(a) (b)
B
icf
f GP
ac
CeMe
Ant. cing.Orbltofr.Perirh. cortex
PirBLABMAHiEntIns
OB
A8
A9A10
EXTENDED AMYGDALA
CC
Periallo
&
Allocortex
Frontal
&
Temporal
Proisocortex
Figure 2.13 (a) The extended amygdala, connecting the central and medial nuclei of the amygdala withlimbic forebrain structures notably the bed nucleus of the stria terminalis. (b) Outputs from the extendedamygdala influencing autonomic and neuroendocrine function (courtesy of Dr L. Heimer)

Principles of Brain Function and Structure: 2 Anatomy 41
The so-called extended amygdala refers tothose components of the amygdala (central andmedial nuclei), which bridge its temporal lobecomponents, with the limbic forebrain and theventral striatum, and the hypothalamus, withits autonomic and endocrine influences (seeFigure 2.13). However, the outputs also flowthrough the stria terminalis posteriorly andthen loop anteriorly so as to from a ring-shapedstructure that encircles the internal capsule(Figure 2.14). The most relevant point to note isthat the amygdala is not an isolated temporallobe structure, but intimately linked with thebasal forebrain. The extended amygdala hasbeen distinguished from the laterobasal andcortical amygdala nuclei, especially by itsneurochemical differences and its outputs to thehypothalamus and brainstem autonomic andsomatomotor structures (Heimer et al., 2007).
BSTS/st
BSTM
BSTL
Med.Hyp.
Lat. Hyp.Ret. Form.
Co
Laterobasalcomplex
CeMe
Figure 2.14 The extended amygdala shown in iso-lation from the rest of the brain. Ce, Central andMe, Medial amygdaloid nucli; BSTL and BSTM, lat-eral and medial divisions of the extended amygdale;Co, cortical amygdala nucleus; BSTS/st, supracapsulapart of the bed nucleus (courtesy of Dr L. Heimer). Acoloured version of this figure can be found on thecolour plate
INDIVIDUAL ANATOMICALSTRUCTURES
Amygdala
The amygdala is located at the anterior partof the temporal lobes, in front of and abovethe temporal horn of the lateral ventricle (seeFigures 2.2 and 2.3). It abuts the rostral part ofthe hippocampus. It is a composite of severalneuronal aggregates and has two main compo-nents: a larger basolateral complex, which hasextensive connections with the neocortex andfrom which it receives polysensory informa-tion, and a central-medial division, extendingmedially, establishing continuity with thebed nucleus of the stria terminalis (extendedamygadala; see below). The laterobasal com-plex is cortical, whereas the centromedialnucleus is striato-pallidal-like. The basal nu-cleus has a high acetylcholine content, whichit receives from the basal nucleus of Meynert(see below).
The main afferent and efferent pathwaystraverse the stria terminalis and the ventralamygdalofugal pathway. The latter is a longitu-dinal association bundle linking to the ventralstriatum (see below) and the medial frontalcortex. There is also a caudal part going to thelateral hypothalamus and, via the MFB, to thebrainstem.
The uncinate fasciculus projects to the frontalcortex. The connections to the brainstem comealmost exclusively from the central nucleus,the fibres ending in structures that serve auto-nomic and visceral functions. These includethe catecholamine and 5-HT brainstem nuclei,the VTA and the substantia nigra, the centralgrey, the dorsal nucleus of the vagus and thenucleus of the solitary tract (NTS). There arealso connections to the midbrain and medullarytegmentum. The basolateral nuclei have corticaland ventral striatal links, and the medial andcentral groups connect to the hypothalamus.In the cortex, amygdaloid fibres are found inthe orbital and medial frontal lobe, the rostralcingulate gyrus and most of the temporal lobe(Price, 1981).
It is further appreciated that the amygdala hasextensive distributions to sensory cortical areas,especially visual cortex, which presumably

42 Biological Psychiatry
modify early sensory inputs (Amaral et al.,1992). The connections from the amygdala to thehippocampus are primarily via the entorhinalcortex (see below), which is a major source ofhippocampal afferents. There are direct connec-tions to the subiculum part of the hippocampus.Those to the hypothalamus may influence thecontrol of pituitary hormone release, especiallythe projections to the ventromedial nucleus,
which itself projects to the arcuate nucleus.Some of the widespread connections of theamygdala are shown diagrammatically inFigure 2.15.
GABA is an important inhibitory transmitterin the amygdala, and other neurotransmittersidentified within it include acetylcholine,histamine, dopamine (especially in the basolat-eral and central nuclei), noradrenaline, 5-HT,
Figure 2.15 The widespread connections of the amygdala (courtesy of Dr Asla Pitkanen)

Principles of Brain Function and Structure: 2 Anatomy 43
glutamate and peptides such as substance P,metenkephalin, somatostatin, VIP, CRF andneurotensin (Ben-Ari, 1981).
As noted above, the amygdala has exten-sive afferent and efferent connections. Whenthe amygdala speaks, the rest of the brain lis-tens. The amygdala provides affective valenceto sensory representations and is crucial forthe emotional tone of memories. The recipro-cal connections with the cortical structures itreceives information from, including even theprimary sensory cortical areas, allow for a directinfluence of emotional tone on cortical sensoryimpressions (Figure 2.16).
Hippocampus
The hippocampus is also situated in the tempo-ral lobe, but is an elongated structure composedof several subdivisions, together referred to asthe hippocampal formation (with the dentategyrus). The main outflow path of the hippocam-pus is called the fornix, which like several otherof the limbic components curves around thethalamus and then descends to the mammillarybodies of the hypothalamus, forming a cruciallink in the Papez circuit. In the human brain, theright hippocampus is larger than the left, butmuch of this relates to the uncus, that anterior
VISUAL THALAMUS
VISUALCORTEX
AMYGDALA
HEART RATE
BLOOD PRESSURE MUSCLE
Figure 2.16 The ‘fast’ and ‘slower’ routes to the amygdala in response to a frightening stimulus. The latteruses cortex, and is less direct than the former. For further explanation see page 75 (adapted from Le Doux JE,Scientific American, 1994, 270, 6, 50–57)

44 Biological Psychiatry
portion closely related to piriform cortex, amyg-dala and extended amygdala, and interlinkedwith emotion. The posterior hippocampus ismore uniquely human, related to the develop-ment of the temporal cortex, and the expansionof association cortices.
The hippocampal structures are closelylinked to the septal nuclei, sometimes referredto as the septohippocampal system. The expan-sion and development of the human brain hasled to separation of these two structures, butin lower animals they are closely linked. Gray(1982) likens this to a pair of joined bananas,
the joint being the septal area, with progressionfrom anterior to posterior accompanied by thestructures spreading laterally as they descendinto the temporal lobes. The main fibre systemsconnecting the two are the fimbria and thefornix, and the two hippocampi are inter-connected by the hippocampal commissures(Figure 2.17).
The structure of the hippocampus displays aconstant architectural pattern, and three maindivisions are recognized. These are the fas-cia dentata, Ammon’s horn and the subiculum(Figure 2.18).
1 Stria longitudinalis medialis 2 Stria longitudinalis lateralis 3 Indusium griseum 4 Fornix precommissuralis 5 Commissura anterior 6 Columna fornicis 7 Corpus amygdaloideum 8 Nucleus anterior thalami 9 Tractus mamillothalamicus10 Subiculum11 Ventriculus lateralis, cornu inferius12 Cornu ammonis (gyrus uncinatus)13 Limbus Giacomini14 Cornu ammonis (gyrus intralimbicus)15 Cornu ammonis (digitationes hippocampi)16 Corpus fornicis17 Fimbria hippocampi18 Gyrus dentatus19 Crus fornicis20 Commissura fornicis21 Site of corpus callosum22 Gyrus fasciolaris
Figure 2.17 The way in which the hippocampus loops round to join its opposite number in the hippocampalfornix. Relevant numbers: 5, anterior commisure; 7, amygdala; 8, anterior thalamic nucleus; 9, mamillothalamictract; 10, subiculum; 12, 14 & 15, Ammon’s horn; 16, fornix; 17, fimbria of the hippocampus; 18, dentate gyrus;20, commisure of the fornix (reproduced with permission from Nieuwenhuys et al., 1978)

Principles of Brain Function and Structure: 2 Anatomy 45
(a)
(b)
To: Associationand Limbic Cortices
Subiculum
Subiculum
CSTo: Association
and Limbic Cortices
CA1
FF
HF
To:MMB&AT
To: Septum
CA2
CA1
CA3
CA4
HFPC
DG
V
CSECEC
HIPPOCAMPAL CORTICAL OUTPUT
HIPPOCAMPAL CORTICAL INPUT
Figure 2.18 (a) Details of the hippocampal forma-tion. The inputs from the entorhinal cortex are shown.(b) Outputs from subiculum and CA1. AT, ante-rior thalamus; CS, collateral sulcus; DG, dentategyrus; EC, entorhinal cortex; FF, fimbria-fornix;HF, hippocampal fissure; MMB, mamillary bodies;PC, perirhinal cortex (reproduced from Heimer et al.,2007, Figure 4.8, p. 88; courtesy of Dr van Hoesen;Biol Psych, 2 Ed, p. 93)
The fascia dentata consists of a compact layerof granular cells, which forms a U-shape andembraces the pyramidal cells of Ammon’s horn(see Figure 2.19). The latter is sometimes sub-divided into four areas, CA1–4, the CA1 areain humans being particularly prominent andsusceptible to damage by anoxia (an alterna-tive name is Sommer’s sector). The subiculumis a transitional structure between CA1 and theparahippocampal gyrus. On sections it is foundwhere the neat structure of Ammon’s horn
breaks down as it merges with the six-layeredneocortex, and is an exit region for many hip-pocampal efferents.
The laminar organization of the hippocam-pus is derived from its regular cell layers,notably the pyramidal cells, granular cells andinterneuronal inhibitory basket cells.
Essentially the circuit of information flowfrom the neocortex is from the parahippocam-pal gyrus and entorhinal cortex via the perforantpath to the dentate gyrus, then from CA3 to theCA1 areas and the subiculum. The latter feedsinto the fornix, and back to the parahippocam-pal gyrus and neocortex. As noted, interoceptiveinformation flows via the fornix to and from thehypothalamus, septum, accumbens, thalamusand midbrain limbic areas. The CA3 region isrich in connectivity, and it forms an excellentfunnel for diverse exteroceptive and interocep-tive inputs to coalesce.
The intrinsic connections of the hippocampusare largely unidirectional. The granular cells ofthe dentate gyrus send mossy fibres to CA3,and the pyramidal cells of CA3 give rise tocollateral axons (Schaffer collaterals) to CA1.The pyramidal cells of the latter project to thesubiculum.
The principal outputs are back to the ento-rhinal cortex and to the ventral striatum (seebelow).
The main neurotransmitter associated withinhibition in the hippocampus is GABA, but thestructure receives dopaminergic, serotoninergicand noradrenergic afferents. Peptides such asVIP, CCK, neurotensin, somatostatin, substanceP and metenkephalin have been identified in thehippocampus (Roberts et al., 1984).
Parahippocampal Gyrus
The parahippocampal gyrus links posteriorlywith the descending cingulate gyrus. Anteriorlyit contains part of the cortical amygdala, whilethe entorhinal cortex forms a substantial com-ponent posterior to this. The entorhinal cortexinputs much integrated polysensory informa-tion to the hippocampus via the perforant path.
This structure is of central importance inthe limbic system. It is adjacent to the hip-pocampus and includes, progressing caudally,

46 Biological Psychiatry
the piriform, entorhinal and parahippocampalcortices. In Brodmann’s system, the entorhinalcortex is represented by area 28 (see below).It has extensive projections to the hippocampalformation via the perforant pathway and, mostimportantly, receives afferents from many cor-tical sites. Thus, the association cortices projectto this region, providing a direct limbic systeminput of visual, auditory and somatic informa-tion. Further, as noted, the amygdala projects tothe entorhinal area such that the hippocampusreceives, via the parahippocampal gyrus, mul-timodal sensory information derived from theexternal and internal world.
The subiculum also projects to the parahip-pocampal gyrus, and the latter in turn haswidespread limbic and association cortical pro-jections in frontal, parietal, temporal and occip-ital lobes (see Figure 2.19).
Septal Area
The septal nuclei are situated below the corpuscallosum, ventrally bounded by the olfactory
tubercle and the accumbens. The lateral bound-ary is made by the lateral ventricle, and thecaudal boundary by the third ventricle andhypothalamus (see Figure 2.20). In humans, thedorsal part is elongated by the development ofthe corpus callosum to form the septum pellu-cidum, which forms a glial and fibre attachmentto the corpus callosum. The septal nuclei of thehuman are often referred to as the precommis-sural septum.
The septal area is usually subdivided intomedial and lateral groups, and the medial septalarea is further divided into the medial septalnucleus and the nucleus of the diagonal band ofBroca. Both contain acetylcholine and project tothe hippocampus and entorhinal cortex via thefimbria and fornix. The lateral nuclei receivehippocampal afferents mainly from CA3 andthe subiculum. Since the lateral and medialseptal nuclei interconnect, a functional circuitis derived as follows: hippocampus–lateralseptum–medial septum–hippocampus. Theseptal area receives rich monoamine projections,especially dopamine, from the VTA via the
1
C Ca3
C 2 1'
1
2
pr
d.
V
a.
A
h
h
BC
f
b.
d
pr
p c.
a
a
Figure 2.19 The hippocampus within the hemispheres and after dissection (reproduced from Kovelman andScheibel, 1984; Biol Psych, 2 Ed, p. 85)

Principles of Brain Function and Structure: 2 Anatomy 47
cc
CLSd
LSv
LSi
VL
SI
ac BST
BST
MPO
MePO
ic
MS
Figure 2.20 The septal area. BST, bed nucleus of stria terminalis; C, caudate nucleus; LS, lateral septal nucleii;MePO, median preoptic nucleus; MPO, medial preoptic nucleus; MS, medial septal nucleus; VL, lateral ven-tricle; ac, anterior commissure; SI, substantia innominata; cc, corpus callosum (Biol Psych, 2 Ed, p. 88)
MFB. VIP, CCK, somatostatin, metenkephalin,neurotensin and substance P are all found inthe septum.
Extended Amygdala
Shown in Figure 2.20 are the bed nucleus ofthe stria terminalis and the substantia innomi-nata. There has been some confusion over theinnominata, the substance with no name, sinceneuroanatomical advances in recent years haveunravelled at least some important structures
within this complex. The ventral striatal terri-tory, located beneath the temporal limb of theanterior commissure, contains the accumbensand the basal nucleus of Meynert; the region ofthe innominata has thus been shown to containa collection of cholinergic and noncholinergicneurones referred to as the magnocellular basalforebrain complex, which also contains exten-sions of the basal ganglia and the amygdaloidcomplex (Heimer et al., 2007).
The extended amygdala has been definedby Alheid and Heimer (1988) as a collection of

48 Biological Psychiatry
cells forming a continuum from the amygdala(notably the centromedial nuclei) to the bednucleus of the stria terminalis and the inter-vening sublenticular portion of the substantiainnominata. The concept is of a broad sheetof interconnected neuronal structures whichreceives a rich monoamine input from ascend-ing midbrain afferents, but also, by its efferents,broadly influences hypothalamic, autonomicand somatomotor functions (see Figures 2.13and 2.14).
However, with outputs through the striaterminalis, the extended amygdala can be visu-alized as a ring formation encircling the internalcapsule and per definition is distinct from thebasolateral amygdala, is not a part of the limbiclobe, and is characterized by its projections tohypothalamic and brain-stem structures.
Cingulate Gyrus
This runs dorsal to the corpus callosum, follow-ing a C-shaped curve as it progresses posteri-orly. The anterior cingulate region is the areaoutlined by Brodmann as areas 23, 24, 25, 31and 33. The retrosplenial region is Brodmann’sareas 26, 29 and 30, and here the cingulategyrus becomes narrow and continuous withthe lingual gyrus, a dorsal extension of theparahippocampal gyrus. The cingulate cortexis continuous with the frontal cortex anteriorly,is rich in dopamine fibres and contains CCK andopiate receptors.
The cingulum has important connectionswith the parietal cortex, including an areareferred to as the precuneus, a part of thebrain involved in visuo-spatial processing andsomehow in an appreciation of our sense of self.However, the widespread cingulate connec-tions with the entorhinal area, the amygdala,the ventral striatum, the hypothalamus andother subcortical structures allow the cingulategyrus to have an important role in attention,motivation and emotion.
Insula
A large portion of the insular cortex is locatedin the depths of the Sylvian fissure, and it has a
key position linking the temporal pole with theposterior orbitofrontal cortex (see Figure 2.6).It is a bridging area in the continuous ring ofcortex that forms the limbic lobe. It has manyfunctions, including integration of limbic andcortical information, and forms a part of whatmay be called the ‘visceral cortex’. It links withthe frontal cortex anteriorly and with the hip-pocampal structures posteriorly, and receivesdirect input from brainstem structures such asthe tractus solitarius.
Thalamus
This, as with many other identifiable cellulargroups in the brain, is a collection of nuclei witha wide variety of motor and sensory functions.The anterior thalamic nucleus was identifiedby Papez as a part of his circuit. However,the thalamic nuclei are part of the re-entrantpathways from strital outputs to the cortex,the parallel, segregated cortico-basal ganglia-thalamocortical circuits that have becomeimportant to understanding the functionalanatomy of a range of neurological and psy-chiatric disorders (see below). The thalamusis usually considered to play a key role in thetransmission of somatic sensory impulses ontheir way to the cerebral cortex. It is composedof three main nuclear groups, the medial, lateraland anterior (Figure 2.21). The ventral pos-terolateral nucleus conveys medial lemniscaland spinothalamic information to the primaryand secondary sensory cortical areas. The basalganglia afferents project mainly to ventrolat-eral, ventroanterior, mediodorsal and so-calledintralaminar nuclei (located within whitematter laminae that transect the thalamus);these thalamic nuclei also receive cerebellarprojections. Reciprocal connections with thefrontal cortex are made by the ventral anteriorand mediodorsal nucleus, the anterior nucleusconnecting to the cingulate gyri as part of thePapez circuit. The reticular formation – thatloosely assembled, closely packed network ofneurones in the brainstem – activates manythalamic neurones, and continues by relay anddirect connection to influence all fields of thecortex; the midline intralaminar nuclei and

Principles of Brain Function and Structure: 2 Anatomy 49
Anterior To prefrontal cortex
From globus pallidus
To supplementary motor area
From globus pallidus
To motor cortex
From cerebellum
To somatic sensory cortex
From medial, spinal andtrigeminal lemnisci
From optic tract
To primary visual cortex
To primary auditory cortex
Inferior brachium
Ventral anterior
Reticular
Lateral dorsal
Ventral lateral
Intralaminar
Ventral posterior
Lateral posterior
Mediodorsal
Pulvinar
Lateral geniculate
Medial geniculate
(a) Nuclei (b) Connections of relay nuclei
Figure 2.21 Subdivisions of the thalamus (reproduced from Clarke et al., 2009, with permission of WileyBlackwell)
the thalamic reticular nuclei with their corticaloutputs thus influence cortical arousal.
The principal afferents from the thalamusto the cortex are glutaminergic. The cytoar-chitecture of the thalamus is unique, in thatthe GABA inhibitory neurone are not typicalinterneurons; rather they form a shell aroundthe nucleus, which is called the reticular nucleusand may have an important role in gating themassive sensory and cortical information pass-ing through the thalamus. This is probablyrelevant in regulating thalamocortical oscilla-tions and rhythms (Buzsaki, 2006).
Hypothalamus
The hypothalamus, positioned dorsal to thepituitary gland, is a site of convergence for muchlimbic-system and extended-amygdala activity.Posterior are the mammillary bodies and ante-rior are the optic chiasm and the preoptic area.The descending fornix divides the hypothala-mus into medial and lateral areas. The medialborder of the medial hypothalamus is formed bythe third ventricle, and several nuclear groupsare defined (Figure 2.22). Three zones areidentified: the periventricular, with essentially
neuroendocrine output (paraventricular andarcuate nuclei); the medial, connected to thelimbic system and extended amygdala; and thelateral zone, which contains many fibres of pas-sage of the monoamine brainstem and midbrainnuclei travelling with the MFB, but the fornix,stria terminalis and mammillothalamic tractsconnect anteriorly, and the mammillotegmentaltract posteriorly.
The suprachiasmatic nucleus is thought tobe a regulator of rhythmic activity, a sort ofbiological clock. The axons of neurones fromthe supraoptic and paraventricular nuclei areneurosecretory fibres travelling mainly to theposterior pituitary gland.
Several of the hypothalamic nuclei secreteneuropeptides, some of which release hor-mones. These are released into the hypophysialportal blood vessels, which carry them to theanterior pituitary where they stimulate orinhibit various pituitary hormones. A list ofsome of these and the accompanying releasinghormones is shown in Table 2.1.
The neurohormones are typically released ina pulsatile fashion. They are found in brainareas other than the median eminence and alsoinfluence the pituitary gland via secretion into

50 Biological Psychiatry
Interventricularforamen
(a)
(b)
Fornix
A
A
Anteriorcommissure
Laminaterminalis
Preopticnucleus
Supra-opticnucleus
Supra-chiasmaticnucleus
Arcuatenucleus
Optic chiasm
Middle lobe
Adenohypophysis
Dura mater
Sphenoidbone
Internal capsule
Fornix
Globus pallidus
MFB
LHN
Optic tract
ZI
Hypothalamicsulcus
DN
PVN
PNLHNDMN
Mammillo-thalamictract
VMNTN
MB
PVN
DMN
PER
VMN
Arc
Medial eminence
Infundibulum
Neurohypophysis
.
Figure 2.22 The hypothalamic nuclei: (a) sagital and (b) coronal sections. ARC = arcuate nucleus; DN =dorsal nucleus; DMN = dorsomedial nucleus; LHN = lateral hypothalamic nucleus; MB = mammillarybody; MFB = medial forebrain bundle; PER = periventricular nucleus; PN = posterior nucleus; PVN =paraventricular nucleus; TN = tuberomammilary nucleus; VMN = ventromedial nucleus and ZI = zonaincerta (reproduced from Clarke et al., 2009, with permission of Wiley Blackwell)

Principles of Brain Function and Structure: 2 Anatomy 51
Table 2.1 Hypothalamic releasing and inhibiting factors and pituitary hormones
Neurohormone Pituitary hormone
Thyrotropin-releasing hormone TSH, prolactinCorticotropin-releasing hormone (CRF) ACTH, beta-endorphinLH/FSH-releasing hormone LH, FSHGrowth hormone-releasing factor Growth hormoneMelanocyte-stimulating hormone-releasing factor MSHProlactin-inhibitory factor (PIF) ProlactinSomatostatin Growth hormone, TSHMSH-inhibiting factor MSH
the CSF. The extrapituitary influence is exertedon limbic system structures, the thalamus, theperiaqueductal grey region and the brainstemcatecholamine nuclei.
Monoamine transmitters are also presentin the hypothalamus, some of which impingeon the median eminence to influence hormonerelease. Indeed, catecholamines have beenlinked to the release of virtually all anteriorpituitary hormones. Of importance is theintrahypothalamic dopamine pathway with cellbodies in the arcuate nuclei. Here the dopamineis thought to inhibit prolactin release, dopaminebeing a prolactin-inhibitory factor (PIF). 5-HT isthought to stimulate both growth-hormone andprolactin release.
Habenula
The habenula is located in the dorsal dien-cephalon, in the sides of the third ventricle, andreceives afferents from the hypothalamus andthe ventral pallidum – part of the cortical basal
ganglia re-entrant circuits – especially thoseareas innervated by the accumbens shell. Themain efferents descend to the midbrain nuclei,which contain the monamine and cholinergicneurones. The habenula has been shown to beinvolved in stress responses, reward, learningand addiction (Figure 2.23) (Geisler, 2008).
Autonomic Nervous System
The arrangement of the autonomic system,responsible for much of the body’s homeostasis,is substantially different from that of thesomatomotor system. There are sympatheticand parasympathetic divisions, but both havepre- and post-ganglionic components. Theformer are located in the CNS, in the brainstemand spinal cord; the latter are located eitherdistant from the target organ (sympathetic) orclose to it (parasympathetic). The main featuresof the two systems are shown in Table 2.2.
Sympathetic preganglionic neurones arelocated in a cell column which lies in the lateral
Table 2.2 Classical comparisons of sympathetic and parasympathetic divisions of ANSa
SNS PSNS
Location of preganglionic somata Thoracolumbar cord Cranial neuroaxis;sacral cord
Location of ganglia (and postganglionic somata) Distant from target organ Near or in target organPostganglionic transmitter Noradrenaline AcetylcholineLength of preganglionic axon Relatively short Relatively longLength of postganglionic axon Relatively long Relatively shortDivergence of preganglionic axonal projection One to many One to fewFunctions Catabolic AnabolicInnervates trunk and limbs in addition to viscera Yes No
aLangley (1921) stressed the contrasting and distinguishing traits of the two divisions of the ANS. Since his time, most discussions haveidentified several contrasting features. Most of these distinctions apply generally but not universally. Although many of these distinctionshave blurred (e.g. transmitter) or may be completely unfounded (e.g. divergence), they are often discussed.

52 Biological Psychiatry
LHA
MR
LDTg
DR
Hb
VTA
Thalamussm fr
mfb
LSccPFC
Acbsh VP
Figure 2.23 The connections of the habenula. The habenula is part of the dorsal diencephalic circuit, convey-ing information from several forebrain nuclei to ascending brain-stem systems. HB, habenula; MFB, medialforebrain bundle; LHA, lateral hypothalamic area; PFC, prefrontal cortex; CC, corpus callosum; Fr, Fasciculusretroflexus; Acbsh, Accumbens shell; VP, ventral pallidum; MR and DR, medial and dorsal raphe; VTA, ventraltegmental area (reproduced with permission from Stefani Geisler)
Postganglionicfiber
Autonomicganglion
(a) (b) (c)
Figure 2.24 Differences between the somatic motor output and the sympathetic output to effector endpoints. (a) Motorneurones project directly to the muscles. (b) The sympathetic nervous system projects firstto preganglionic neurones, which then project to post-ganglionic motor neurones in para- and pre-vertebralautonomic ganglia. (c) The parasympethic nervous system has preganglionic neurones in brain-stem cranialnerve nuclei (and in spinal cord) that project to post-ganglionic motor neurones in ganglia located near orinside viscera (reproduced with permission from APA Press)

Principles of Brain Function and Structure: 2 Anatomy 53
Edinger-Westphal
Coronal'look-through'
dorsal nuc. of X
Brainsteam Slices With Vagus NerveConnections
solitary nuc.
nuc.ambiguus
Xthnerve
solitary tract
mesencephalic nuc.
main sensory V
vestibular nuc.motorV
III III
IV IV
VV V
VI VI
VII
XII
V
MID
BR
AIN
PO
NS
ME
DIU
LLA
cochlear nuc.
nuc. ambiguus
dorsal nuc. X
spinal nuc. of V
solitary nuc.
Figure 2.25 The autonomic nuclei that relate to control of autonomic function in the lower pons and medulla.Central to this arrangement are the nuclei related to the vagus nerve, the nucleus of the tractus solitaries, thenucleus ambiguous and the dorsal motor nucleus of the vagus. The section indicated on the right relates tothe slice of the arrow on the left
horn of the spinal grey matter between thefirst thoracic (T1) and the third lumbar (L3)segments. The post-ganglionic cells are in eitherparavertebral (adjacent to the spinal cord) orprevertebral (situated close to where majorabdominal arteries leave the aorta) ganglia. Thesympathetic postganglionic fibres then supplytarget organs such as skin and blood vessels(Figure 2.24).
Parasympatheric output stems from twocolumns of cells, one in the brainstem and one inthe spinal cord (S2–4). The brainstem, visceraldivision comprises a number of cell groupsadjacent to the central aqueduct, which sendefferents through cranial nerves to the head(III, VII and IX), thorax and abdomen (X – thevagus nerve), providing innervation thatcontrols pupil size, lacrymation and salivation,for example. The vagus innervates the digestive
tract and the two main nuclei are the dorsalmotor nucleus of the vagus and the ventral vagalnucleus (nucleus ambiguus) (see Figure 2.25).As shown in Table 2.2, the two divisions of theautonomic nervous system use different neu-rotransmitters at the post-ganglionic site, butmost preganglionic neurones are cholinergic.
There are extensive visceral afferent inputs tothe autonomic nervous system, many ending inthe nucleus of the solitary tract.
ASCENDING AND DESCENDINGLIMBIC-SYSTEM CONNECTIONS
Knowledge of the anatomy and functionalunity of the limbic system has altered radicallyin recent years. It is now accepted that a limbicforebrain–midbrain circuit exists which unites

54 Biological Psychiatry
the monoamine- and peptide-rich zones of themidbrain with rostral structures such as thehippocampus, amygdala and the accumbens,and a limbic midbrain area has been definedin the paramedian zone of the mesencephalon(Nauta and Domesick, 1982). The main con-necting structure is the MFB, a poorly definedfibre system with a loose arrangement, char-acteristic of brainstem reticular formation. Itreceives contributions from such structures asthe septal nuclei, accumbens, hypothalamus,olfactory tubercle, amygdala, bed nucleus ofstria terminalis and the orbitofrontal cortex.Caudally it projects to the VTA, the interpe-duncular nucleus, the raphe nuclei, the locuscoeruleus and the midbrain reticular formation.Nieuwenhuys (1996), with his concept of thegreater limbic system, emphasizes the caudalprojections to and from the rostral medulla, andfurther connections with the spinal cord whichinfluence autonomic function (Figure 2.8).Included are several regions from whichbehavioural and autonomic symptoms can beelicited by stimulation.
The final common pathway for emotionalexpression is through the autonomic nervoussystem, and some authors refer to the ‘emotionalmotor system’ (see below). The periaqueductalgrey matter (PAG) is situated immediatelybelow the superior colliculus, surroundingthe aqueduct between the third and fourthventricles. Stimulation leads to a variety ofexpressed emotions, especially threat and flight,and it is involved in pain perception (Bandlerand Keay, 1996). It receives projections from thelimbic lobe, and outputs both centrally, but alsoto the rostroventral medulla and spinal cord.
In the rostral medulla, and at the junctionbetween the medulla and the pons, lies agroup of neurone clusters that seem to directlycontrol autonomic function (see Figure 2.25).These include neurones regulating cardiac andrespiratory function and micturition. Some ofthe neurones (presympathetic cells) have directmonosynaptic inputs to the preganglionicsympathetic cells. The areas involved includethe C1, A5 and the nucleus ambiguus. Thenucleus ambiguus is part of the vagus nerveefferent motor system. The nucleus of the
tractus solitarius (NTS) receives afferent fibresfrom the vagus and glossopharyngeal nervesand is reciprocally connected to the nucleusambiguus, which, with the dorsal nucleus of thevagus, provides efferents to the vagus nerve,supplying the GI tract with autonomic nerves.The NTS also relays information rostrally tothe insula, hypothalamus and several otherstructures involved in monoamine regulationand limbic function. It is now appreciated thatthe majority of fibres in the vagus nerve areafferent, and this has been exploited in vagusnerve stimulation (see Chapter 12).
It is now known that there is an extensive sys-tem of interneurones at the spinal level whichinteract with the sympathetic and parasympa-thetic preganglionic neurones and use neuro-transmitters such as glycine and GABA. Thefinal output of the autonomic system is thereforeboth supraspinal and spinal and is dependenton visceral and somatic afferents as well asdescending influences from the cortex, hypotha-lamus and mesencephalon, ultimately reflectinglimbic and cortical information.
The ascending components of the limbicforebrain–midbrain circuit arise from theventral tegmental area (VTA), the raphe nucleiand the locus coeruleus. The VTA occupies thebasomedial midbrain, dorsal to the substantianigra, and is continuous rostrally with thelateral hypothalamus. It borders on the ventralperiaqueductal grey substance, the nucleusruber (red nucleus), the dorsal raphe nucleiand other nuclei of the limbic midbrain (seeFigure 2.26).
The ascending connections to the limbic fore-brain include the dopamine-rich cells whichinnervate the accumbens, olfactory tubercle,the extended amygdala, entorhinal area, hip-pocampus, frontocingulate cortex and septalarea. The catecholamine nuclei are found in rel-atively discrete areas of the brainstem, and werefirst identified using fluorescent histochemicaltechniques. On the basis of animal work theyhave been designated as Al, A2, . . . up to A13(Ungerstedt, 1971), and those arising from thesubstantia nigra and the VTA are referred to asA9 and A10 respectively. From these the major-ity of dopamine neurones that project to the

Principles of Brain Function and Structure: 2 Anatomy 55
L G B L G BIII
PC C
DD
R R
M M
V T A
S N S N
Figure 2.26 Location of the ventral tegmental area in the midbrain. C, nucleus of Cajal; D, nucleus ofDarkschewitsch; LGB, lateral geniculate body; M, mammillary bodies; P, posterior commissure; R, rednucleus; SN, substantia nigra; VTA, ventral tegmental area
limbic areas, striatum and cortex arise. Usingthis terminology, the locus coeruleus is A5 andA6. In a similar fashion the serotoninergic neu-rones are confined virtually to the brainstemraphe nuclei. The A10 projection also innervatesthe striatum and the thalamus and has connec-tions with the locus coeruleus and raphe nuclei,although not all paths are thought necessarily tobe dopaminergic (Nauta and Domesick, 1982).
The locus coeruleus lies ventrolateral to thefourth ventricle, and has widespread connec-tions to the neuroaxis, probably more extensivethan those of any other nucleus (Vertes, 1990). Itinnervates the spinal cord, the thalamus and thelimbic system, with a particularly dense projec-tion to amygdala and cortex. This distributionis in marked contrast to the relatively restrictedtermination of fibres from A9 and A10. Theascending catecholaminergic system is thoughtto exert a tonic modulatory influence on cor-tical neurones, and locus coeruleus neuronesare sensitive to sensory input, stress increasingtheir activity.
5-HT distribution is intermediate, being moreextensive than that of dopamine and projectingto the hippocampus and amygdala, parahip-pocampal gyrus, habenula, thalamus and cortex.
Raphe cells are unresponsive to arousingsensory stimuli, and high-frequency firingoccurs with repetitive movements and withfeeding. Their descending influences increasethe excitability of motor neurones and areantinociceptive (see Figure 2.27).
MACROSYSTEMS
Based on cytoarchitectural and neurochemicalproperties, functional basal forebrain anatom-ical systems can thus be identified, and havebeen referred to as macrosystems. These includethe ventral and dorsal striato pallidal system,the extended amygdala and the septal-preopticsystem.
Macrosystems are processing units thatreceive information from the cortex and projectto somatic and autonomic motor outputs inthe lateral hypothalamus or brainstem, or viare-entrant paths back to the cortex. They arehypothesized to detect the positive or negativevalence of stimuli and via their outputs theycompete and cooperate to influence resultingbehaviour (Heimer et al., 2007).
They have a common template, with largelycortical inputs, terminating predominately ininhibitory neurones (especially medium-sized

56 Biological Psychiatry
Nucleusaccumbens
(a)
(c)
(b)
Arcuatenucleus
Pituitary
Ventral tegmentalarea
Substantianigra
To hippocampus
Striatum
To hippocampus
Hypothalamus
To amygdala
Raphenuclei
Thalamus
To hippocampus
Locusceruleus
Medullaryretricularformation
Hypothalamus
To amygdala
Thalamus
Figure 2.27 Distribution of various monoamines output fibres arising from structures in the pontine area ofthe brain: (a) dopamine, (B) 5-HT, (c) noradrenaline (courtesy of Dr Ned Higgins)
(a) (b)
Figure 2.28 The connections underpinning the concept of basal forebrain macrosystems. (a) Outputs fromgreater limbic lobe structures, which converge in the reticular formation, and in addition to outputs from thecortex (CX) converge on motor effectors. (b) Re-entrant pathways returning to cortex (courtesy of Dr ScottZahm)

Principles of Brain Function and Structure: 2 Anatomy 57
spiny neurones), which project on to otherGABA neurones in structures such as thepallidum, extended amygdala and preopticarea, which then send projections back to thecortex via thalamo-cortical re-entrant pathways(see Figure 2.28). They also have projections toforebrain cholinergic and monoaminergic cellgroups, and influence somatomotor, autonomicand endocrine systems (Heimer et al., 2007).Since the thalamus, pivotal in this scheme, hasno direct motor outputs, and the striatum lacksdirect projections back to the cortex, funnellinginformation through the thalamus, the intrinsicmacrosystem circuitry modifies cortical activity.Since the macrosystems under considerationhere have substantial limbic inputs, they aresituated to synthesize multiple somatic andemotional information and thus regulate outputbehaviours.
THE BASAL GANGLIAAND THE RE-ENTRANT CIRCUITS
The term ‘basal ganglia’ usually refers to thecaudate nucleus, putamen and globus pallidusbut may also include the subthalamic nucleusand the substantia nigra. ‘Striatum’ refers to thecaudate nucleus and putamen, divided as theyare by the internal capsule. In lower animals theseparation is less complete, and the structure isreferred to as the caudatoputamen. The caudate
nucleus is a large curved nucleus which adheresthroughout its length to the lateral ventricles,anteriorly being continuous with the putamen.The putamen and globus pallidus are referredto as the lenticular nucleus.
The substantia nigra has two components, thepars reticulata and the pars compacta. The for-mer is a part of the pallidum, and uses GABA asits main efferent neurotransmitter; the pars com-pacta is the origin of the nigrostriatal dopaminepathway.
Recently, concepts of the organization ofthe basal ganglia have undergone profoundchanges. Previously discussed as if they usedserial processing, they are now viewed as beingparallel in nature, with structurally and func-tionally distinct circuits that act in parallel link-ing cortex, basal ganglia, thalamus and frontalcortex – the macrosystem template just referredto (Alexander et al., 1986; Heimer et al., 2007).Six such circuits are postulated, targeting dif-ferent areas of the frontal lobe. Representativestructures of three circuits especially involvedin regulating emotional behaviour are shown inFigure 2.29. These involve prefrontal, orbitaland medial frontal cortex. The features thatare shared by all the circuits are shown inFigures 2.11, 2.12 and 2.29. The cortical outputis glutaminergic, and projects to the striatum,with an enkephalin link to the globus pallidus.The latter structure is defined by at least two
Caudate(Ventromedial)
Globus Pallidus(Lateral Dorsomedial)
Thalamus(VA and MD)
Lateral OrbitalCortex
Anterior CingulateCortex
NucleusAccumbens
Globus Pallidus(Rostrolateral)
Thalamus(MD)
DorsolateralPrefrontal Cortex
Caudate(Dorsolateral)
Globus Pallidus(Lateral Dorsomedial)
Thalamus(VA and MD)
Figure 2.29 Organization of three frontal-subcortical circuits. VA, venral anterior; MD, medial dorsal (BiolPsych, 2 Ed, p. 98)

58 Biological Psychiatry
segments, the internal and the external. Theprojection to the internal segment utilizes GABAand connects with the thalamus, feeding backto frontal cortex. The globus pallidus externusloops with the subthalamic nucleus back to theinternal segment. The final thalamocortical linkreturns to the same area of cortex where theoriginal corticostriatal connection began.
Activation of the direct pathway throughthe internal pallidum excites the thalamocor-tical projection (via GABAergic inhibition of aninhibitory pathway), while that of the externalpallidum, which activates the STN, increasesinhibition of the thalamus, and the balancebetween the external and internal loops mod-ulates output to the cortex (see Figures 2.11and 2.12).
In this context, the basal ganglia facilitatemovement by a process of disinhibition.
The nigrostriatal pathways are dopaminer-gic, exciting the GABAergic striatal neuronesand inhibiting the projections to the internal andexternal pallidal segments. The net effect couldbe to enhance the output. Acetylcholine haseffects antagonistic to dopamine in the striatum.
Essentially all of the cortical mantelprojects to the basal ganglia structures (seeFigure 2.9). Thus, the caudate/putamen receiveswidespread, somatotopically organized projec-tions from the cerebral cortex and the corticalassociation areas, including temporal cortexprojecting to caudate. The main striatal structureof the ‘motor circuit’ is the putamen, that of the‘limbic circuit’ being the caudate and the ventralstriatum (see below). ‘All of cortex uses basalganglia mechanisms’ (Heimer et al., 2007, p. 43).
The cytoarchitecture of the striatum has func-tional significance. Striosomes, zones lackingacetylcholine, exhibit enkephalin-like, opiate-like, substance P-like and somatostatin-like reac-tivity, and are contrasted with the matrix. Thestriosomes seem more related to limbic inputs,the matrix to sensorimotor processing (Graybiel,1990). While the matrix outputs to the pal-lidum, the striosomes project largely to thepars compacta of the substantia nigra, perhapsmodulating dopamine input to the striatum. D1binding is greater in the striosomes, and D2greater in the matrix.
It seems that in the human striatum, strio-somes predominate (50%) (Saper et al., 1996),suggesting a profound limbic component, whichmust have functional significance. The mainneurones (70%) identified in the basal gangliaare called medium spiny neurones. The restare interneurones and contain neurotransmit-ters such as acetylcholine, neuropeptide Y andGABA.
The name of the spiny neurones relates tothe approximately 13 000 spiny dendrite pro-truberances, which have a head sticking out atthe end of a neck. Excitatory input (glutamate)synapses to the head, while the dopamine input(mainly from the substantia nigra) is to theneck. This arrangement allows the dopamineto modulate the glutaminergic input. Thismicrocontrol within the striatum is disturbed inmany basal ganglia diseases such as Parkinson’sdisease.
THE VENTRAL STRIATUM AND ‘LIMBICSTRIATUM’
Much attention has been focused on dopamine-rich structures lying ventral and medial to, andassociated with, the head of the caudate nucleus.The ventral striatum is contrasted with thedorsal striatum in the circuitry outlined abovemainly by its limbic inputs, and crucially by out-put to the mediodorsal nucleus of the thalamus,as opposed to the ventrolateral, ventromedialand centromedian nuclei (see Figure 2.10). Theaccumbens and the closely associated olfactorytubercle are the main nuclear groups of theventral striatum. The accumbens has a cau-dal boundary with the bed nucleus of the striaterminalis, which is difficult to establish, empha-sizing the interconnectedness with the extendedamygdala. Anteriorly it extends into the ventro-medial portion of the frontal lobe, and it lieslateral to the septal region (White, 1981) (seeFigure 2.30).
It has recently been appreciated that there aretwo components of the accumbens, a core anda shell (see Figure 2.31). The core is striatal andprojects to the ventral pallidum, and hence tothe loops of the thalamus and back to cortex. Theshell is essentially continuous with the extended

Principles of Brain Function and Structure: 2 Anatomy 59
Convergence of prefrontal cortical,limbic and dopamine inputs
Prefrontalcortex
HippocampusAmygdala
ML/IL Thalamus
RAPHE/5-HTVTA/dopamine
Motor /behavioral output
CPu
Acbac
OT
Figure 2.30 The connections of the accumbens,emphasizing the central position of the accumbens,which receives cortical and limbic input and haswidespread outputs that influence behaviour (cour-tesy of Dr Groenewegen)
Figure 2.31 Shell and core of the accumbens (cour-tesy of Dr L. Heimer)
amygdala and projects both to the globus pal-lidus and to the hypothalamus and brainstemmotor and autonomic nuclei. Further, the coreand the shell project directly to the VTA andthe substantia nigra reticulata. D1 receptors areabundant in the shell.
Substance P, enkephalin and CCK arefound in both ventral and dorsal striatum,while VIP, TRH and neurotensin are foundmainly in the accumbens. Other peptideslocated in the accumbens include somatostatin
and melanocyte-stimulating hormone (MSH)(Johannsson and Hokfelt, 1981). There are alsohigh concentrations of acetylcholine, glutamateand GABA.
Nauta repeatedly emphasized the cross-talkbetween the limbic system and the basal ganglia(Nauta and Domesick, 1982). This is of greatimportance for biological psychiatry, not leastbecause of the close links between motor andemotional behaviour (Trimble, 1981a). Directconnections exist between the hippocampus,amygdala, cingulate cortex and ventral stria-tum and the habenula, a nucleus at the caudalend of the midbrain which projects to the raphenuclei and has both limbic and pallidal affer-ents (Figure 2.23). Hypothalamic MFB efferentsimpinge on the VTA and substantia nigra. Fur-ther, indirect links by way of the substantianigra and raphe nucleus exist, both being influ-enced by the descending fibres of the MFB andthe fasciculus retroflexus from the habenula.In contrast, direct connections in the oppositedirection, from striatum to limbic system, arevery limited.
One further point of anatomical interest isthat three limbic projections converge on theanterior ventral component of the striatum,namely the dopaminergic fibres from the VTA,the projection from the amygdala and fibresfrom the frontal cortex (Figure 2.32).
nato
AC
Figure 2.32 Inputs to the accumbens overlappingfrom the ventral tegmental area (vertical lines)prefrontal cortex (horizontal lines) and amygdala(stipple). NA, nucleus accumbens; AC, anterior com-misure (courtesy of Dr L. Heimer)

60 Biological Psychiatry
THE ASCENDING CHOLINERGICSYSTEMS
The nuclear groups including the medial septalnucleus, the basal nucleus of Meynert and thenucleus of the diagonal band are all sites of ori-gin of cholinergic ascending systems that projectto the cerebral cortex and hippocampus (septal).The area forming a rostroventral extension of theglobus pallidus, the ventral pallidum, is coex-tensive with the basal nucleus of Meynert, and itis difficult to draw discrete boundaries betweenthese structures (see the discussion above con-cerning the substantia innominata). The maininputs to this cholinergic system come from thecortex, limbic system and hippocampus, and theefferents terminate in all layers of cortex. As withthe basal ganglia macrosystems the projection isback to the cortical areas from which their inputderives. Acetylcholine excites cortical neurones,modulating the effect of incoming information,and increased activity desynchronizes the elec-troencephalogram (EEG). Deficits of cholinergicinput, as associated with Alzheimer’s diseasefor example, lead to attentional, as opposed topure memory, deficits.
Additional cholinergic neurones arise fromthe mesencephalic reticular formation in thepedunculopontine and dorsolateral tegmentalnuclei. These are also part of an arousal systeminfluencing the thalamocortical system.
CORTICAL REGIONS OF INTEREST
As already noted, there are two main divisionsof cortex, the six-layered isocortex (neocortex)and the non-isocortex. The isocortex, especiallyin humans, has developed rapidly and exten-sively in the latter phases of evolution and isattributed a dominant role in human highercerebral processes. Much work of relevance forbiological psychiatry and neuropsychiatry hashighlighted the frontal and temporal areas ofthe cortex, although here further emphasis isgiven to parietal cortex.
The human isocortex has been divided intovarious areas dependent on microscopic differ-ences, such as those described by Brodmann(see Figure 2.33). The layer of cortex closest
to the pia mater contains mainly dendrites ofthe deeper-lying cells. The pyramidal cells, withlong axons that traverse the internal capsuleto form part of the pyramidal tract, are foundin layer 5. It is the granular cells of layer 4that mainly receive the thalamic sensory affer-ents, and this layer, in contrast to layer 5, isbest developed in primary sensory cortices. Thecerebral cortex is made up predominantly ofpyramidal cells, which use glutamate as theirneurotransmitter. Betz cells are large pyramidalcells found in the motor cortex of hominids.
The primary sensory somatocortex is locatedposterior to the central sulcus in the postcen-tral gyrus, equivalent to Brodmann’s areas 1to 3. More posterior, corresponding to areas 5and 7, is the somatic sensory association area.The visual receptive areas are the striate andperistriate cortex (area 17, the primary visualcortex, and areas 18 and 19, the visual associa-tion areas). The auditory cortical areas are in thesuperior temporal gyrus (Brodmann’s areas 41and 42). Heschl’s gyrus (the transverse tempo-ral gyrus) is located on the dorsal surface of thesuperior temporal gyrus. It forms the anteriorborder of the planum temporale and is part ofthe temporal operculum. It is also part of theprimary auditory cortex and receives auditoryinformation from the medial geniculate of thethalamus, and has efferents to the associationauditory cortex in the superior temporal gyrus.
The main motor cortex is situated in theprecentral gyrus, immediately rostral to the cen-tral sulcus (area 4), its main afferents comingfrom area 6, adjacent to it, which itself receivesprefrontal projections. Area 8, another regionanterior to the precentral gyrus, is referred toas the frontal eye field, and on stimulation eyemovements are provoked. The supplementarymotor area is Brodmann’s area 6. This is highlyinvolved in motor planning and pre-rehearsal.
It is now known that the cerebral cortexhas a columnar arrangement, which has func-tional significance. The cortical neurones formconnections within a column, but also ramifywith cells in adjacent columns. This arrange-ment allows for an amplifying effect on afferentimpulses, in the motor cortex permitting suf-ficient neurones to discharge for movement

Principles of Brain Function and Structure: 2 Anatomy 61
19
19
18
18
17
37
20
11
38
10
9
8
6 43 1 2
5
7
45
47
44 43
39
4241
22
21
40
8
6
9
10
4 31
25
7
19
18
17
1819
37
20
11
38
25
34
2836
35
33
3224
31
23
262930
27
Figure 2.33 The cortical areas as defined by the Brodmann system

62 Biological Psychiatry
and in the sensory cortex distinguishing twoclosely related stimuli. Further, by allowingfor the development of positive-feedback loopsand inhibition of neighbouring columns, thecolumns are self-excitatory, sharpening theireffect by surround inhibition. In the visual cor-tex, columns of orientation-selective cells havebeen identified, many of which are developedand present at birth.
A large proportion of intrinsic cortical neu-rones are GABAergic, many of which receivethalamic afferents. Cortical peptides includesomatostatin, VIP, CCK and neuropeptide Y.In the cortex, cholinergic neurones have beenshown to contain VIP.
The noradrenergic innervation of the neocor-tex is extensive and tangential to the colum-nar arrangement. The fibres run longitudinallythrough the cortical grey matter, in laminaaeVI, V and I, and branch widely, thus affect-ing activity over wide areas of cortex. Theyare activated by a novel stimulus, and interactwith the thalamocortical inputs impinging onpyramidal and interneuronal dendrites. VIP isalso released, which enhances the activity ofthe pyramidal neurones and influences cere-bral microcirculation. Thus VIP exerts specificlocal effects, possibly complementary in termsof information processing, with the influence ofmonoamines.
The frontal lobes are anatomically repre-sented by those areas of cortex anterior tothe central sulcus, including the main corti-cal representations for the control of motorbehaviour. The term ‘prefrontal cortex’ desig-nates the most anterior pole, an area sometimesreferred to as the frontal granular cortex orthe frontal association cortex (Brodmann’s areas9–15, 46 and 47; see Figure 2.33). The pre-frontal cortex is amongst the last to myelinate indevelopment. One definition of the prefrontalcortex is that region which receives projec-tions from the mediodorsal thalamic nucleus(Fuster, 1980). These are topographically orga-nized such that the medial part of that nucleusprojects to the medial and orbital frontal cortex,and the lateral to the lateral and dorsal cor-tex. The medial thalamic area receives afferents
from the mesencephalic reticular formation, andfrom the amygdala, entorhinal and inferior tem-poral cortex, whereas the lateral nuclear areaonly has afferents from the prefrontal cortex(Fuster, 1980).
Other important prefrontal connections aremade by the mesocortical dopamine projectionsfrom VTA. Unlike the subcortical dopamineprojections, these neurones lack autoreceptors(Bannon et al., 1982). Further links are to thehypothalamus (the orbital frontal cortex alonein the neocortex projects to the hypothalamus),the amygdala, the hippocampus, and the retro-splenial and entorhinal cortices. On the basis ofprimate data, Nauta (1964) suggested that theorbital frontal cortex makes connections withamygdala and related subcortical structures,whereas the dorsal cortex links more to thehippocampus and parahippocampal gyrus.Certainly there seems to be a comparablecircuit to the Papez circuit, but based on theamygdala instead of the hippocampus; thus:Amygdala–thalamus (mediodorsal nucleus)–orbitofrontal cortex–inferior temporal cortex–amygdala. In the same way that sensoryinformation from the primary sensory cortex,after passing to adjacent secondary areas,cascades to the anterior temporal areas (Jonesand Powell, 1970), the prefrontal cortex is also aprojection area for extensive somatic, auditoryand sensory information from parietal areas.
The prefrontal cortex has efferents to, butdoes not receive afferents from, the striatum,notably the caudate nucleus, globus pallidus,putamen and substantia nigra.
The flow of motor information is from pre-frontal to premotor to primary motor areas,with further loops to the basal ganglia and lat-eral thalamus via the circuits described above.Thus, with the exception of some primary sen-sory and motor areas, the prefrontal cortex isinterconnected with every other cortical region(Fuster, 1993).
The area of the prefrontal cortex that receivesthe dominant dorsomedial thalamic nucleusprojection overlaps with that from the dopamin-ergic VTA. The internal connectivity of theprefrontal cortical structures is complicated. In

Principles of Brain Function and Structure: 2 Anatomy 63
summary, the medial cortex shows few con-nections with orbital cortex and vice versa.The orbital networks mainly communicate witheach other, and such internal connectivity isthe case with medial frontal areas. The orbitalnetworks receive somatosensory and visceralinputs, including taste, and have been shownto possess cells which respond to taste andthe sight of food (Buckley et al., 2001; Rolls,2001). Output is to the basolateral amygdalaand accumbens. In contrast, the medial net-works have few olfactory inputs, and importantoutputs to the hypothalamus and periaque-ductal grey region (which has very limitedoutput from the orbital region), a descendingvisceral control.
The OFC with information from the accum-bens, amygdala and hippocampus may attributesalience to the environment. The lateral PFCreciprocally interacts with parietal cortex, sup-porting working memory and planning actionsequences, and since the OFC through intrin-sic connections influences the dorsolateral pre-frontal cortex (DLPFC), these structures along
with the ventral striatal re-entrant circuits pro-vide a cerebral substructure for coordinatedmotivated action plans.
THE CEREBELLUM
This structure lies posteriorly over the brain-stem, and its cortex is divided into the cen-tral vermis and the cerebellar hemispheres. Itreceives afferents from both peripheral sensereceptors and sensory and motor cortices, andprojects to the thalamus, spinal cord and thesame areas of cortex. Direct influences of thecerebellum on limbic system structures havebeen reported, notably at the hypothalamus,limbic midbrain and amygdala. These may bemediated via the fastigial nucleus of the vermis(Heath et al., 1978). Although traditionally con-sidered purely motor in function, recent workhas suggested that it plays an important rolein cognition and possibly also in emotionalbehaviour (Schmahmann, 1991). Attention hasalso recently focused on important projectionsfrom the cerebellum to the frontal cortex.


3Important Brain–Behaviour
Relationships
INTRODUCTION
Three clinical neuroscience discoveries in themiddle of the 20th century have revolutionizedour view of brain–behaviour relationships, withprofound therapeutic, conceptual and philo-sophical implications. The first was the devel-opment of the limbic system concept, the secondwas the discovery of so-called ‘pleasure path-ways’ in the brain and the third was the tranquil-izing antipsychotic effect of chlorpromazine.The first two are discussed in more detail inthis chapter.
The Limbic System and Beyond
Paul MacLean’s (1913–2007) original concept ofthe limbic system involved what he referred toas the ‘triune brain’. This was a three-layeredstructure, in which each layer had differingbehavioural repertoires, but all were intercon-nected (see Figure 3.1). There was the protorep-tilian complex, in humans referred to as thestriatal complex (basal ganglia), the paleomam-malian formation (the limbic system), and theneomammalian formation (the neocortex andits connections to the thalamic apparatus). Thistriune brain represented the achievements ofmillions of years of evolution of the neural axis,but also of behaviour.
Biological Psychiatry 3e Michael R. Trimble and Mark S. George 2010 John Wiley & Sons, Ltd
The striatal elements of the brain are involvedin mastering daily behavioural routines andsubroutines. These are repetitive and persevera-tive motor programmes but also include ritualsand communicative displays, best observedin reptiles, but obviously applicable to muchhuman behaviour.
The limbic system in MacLean’s scheme wasinvolved in three key mammalian behaviours,namely nursing and maternal care, audio-vocal communications – vital for maintainingmaternal–offspring contact – and play. Theseneuronal structures, rudimentary in reptiles,but developed extensively in mammals, lead toMacLean’s important dictum that ‘the historyof the evolution of the limbic system is thehistory of the evolution of the mammals, whilethe history of the evolution of the mammalsis the history of the evolution of the family’(MacLean, 1990).
A well-developed limbic system is thus acommon denominator in the brains of all mam-mals, and the evolutionary development of thelimbic system was an essential prerequisite forthe development of characteristic mammalianbehaviours. The key feature of being a mammalis of course the presence and need of a mother,and all that goes with having a mother. Areptile hatching from an egg must not cry outfor its mother or else it will be readily detected

66 Biological Psychiatry
N E O M A M M A L I A N
PA L E O M A M M A L I A N
REPTILIAN(Limbic System)
Figure 3.1 The triune brain. This diagram from Paul MacLean (1968) illustrates the evolution of the humanforebrain and how it expands along the lines of three basic formations that anatomically reflect an ancestralrelationship to reptiles, early mammals and late mammals (reproduced from Maclean, 1990). A colouredversion of this figure can be found on the colour plate
by predators and eaten either by them or byits mother. In contrast, a mammalian infantdepends on the separation cry for security andsuccour. Further, the development of family-,sibling- and later peer-relevant behaviours,including interpersonal bonding, relates to thephylogenetic and ontological development ofthese limbic structures.
MacLean outlined three main subdivisionsof the limbic lobe, which he referred to asan amygdalar division, a septal division anda thalamocingulate division (see Figure 2.3).These divisions had to do with feeling andexpressive states relating to self-preservation,to procreation and to maternal care andplay, respectively. MacLean’s contributions tounravelling the neural basis of emotional andsocial behaviour were central to a revolutionin the neurosciences that took neurology notonly towards mental illness, but also in thedirection of understanding normal as well asabnormal social behaviours. It was pointedout in Chapter 2 how in the past half-century,the underlying concepts of the limbic systemhave altered considerably, not least due to theanatomical explorations of neuroanatomists
such as Walle Nauta (1916–1994) and LennartHeimer (1930–2007).
A problem with the earlier conceptions of thelimbic system was the then-accepted anatomicalbelief that the hypothalamus was to be regardedas the principal subcortical projection of thelimbic system. Indeed, for some people, a rela-tionship to the hypothalamus became a definingfactor of a limbic structure (Heimer et al., 2007,p. 20). Now we know that the major outputsfrom the limbic system are to the basal ganglia.The former view led to an interesting but ratherdamaging conclusion, which had implicationsnot only for understanding brain–behaviourrelationships, but also for the developing spe-cializations of behavioural neurology and neu-ropsychiatry. Thus, those neurologists who, ahalf-century ago, might reluctantly have con-ceded that there was an underlying neurol-ogy of emotional behaviour, could acknowledgethat the limbic system–hypothalamic axis wasexplanatory enough for a neurology of the emo-tions (and hence psychiatry), but this was verydifferent from the neuroanatomy of neurologi-cal disorders. The latter involved essentially theneocortex and its main outputs, especially the

Important Brain–Behaviour Relationships 67
basal ganglia and the pyramidal motor system.A fundamental flaw in this scheme howeverwas that it did not correspond to many clin-ical observations. Included were the obviousbehavioural problems and psychiatric illnessesthat accompanied movement disorders (such asParkinson’s disease or Huntingtons’s chorea),and the obvious abnormal movements that werea part of the clinical picture of psychiatric disor-ders across the spectrum from anxiety (tremor)to schizophrenia (tics, dystonias, dyskinesiasand catatonias). Further, it failed to connect withcommon English and everyday observations,namely that emotion is six-sevenths motion(e-motion), and that we express our states ofdistress and emotion with motion, including ofcourse speech.
Nauta (1986) challenged the belief that cor-tical and subcortical systems were so distinctlyseparated, and noted how anatomical studieshad revealed not only that nearly all of theneocortex is connected to the basal ganglia byextensive efferent connections, but that therewas serial linkage between the limbic struc-tures, the basal ganglia and the neocortex (asdiscussed in Chapter 2). Further, it becameappreciated that the rostral parts of the basalganglia, far from being exclusively motor infunction, were actually innervated by the lim-bic system. There was in fact a much strongerconnectivity between limbic structures and thebasal ganglia than with the hypothalamus, over-throwing entirely the idea that the limbic systemwas a discrete system devoted to the hypotha-lamus and unable to influence the basal ganglia(motor systems) or the cortical mantle.
As has been discussed, Nauta and othersalso extended the influence of the limbic systemcaudally, through the medial forebrain bundle(a limbic traffic artery) and other structures tothe midbrain (limbic midbrain) and hind brain,including the cell structures we now know to bethe origin of the ascending monoamine systems.These innervate not only the ventral striatumitself but the frontal cortex and indeed, for someneurotransmitters like 5-HT, probably the wholeof the neocortex.
Nauta also noted how limbic efferentsinfluenced autonomic neurones and the cranial
nerves that innervate the muscles of facialexpression. Further, since the frontal lobes(especially the orbital and cingulate divisions)were also by this time revealed as being limbic-related, Nauta speculated that the fronto–limbicconnections enabled the frontal cortex to mon-itor and modulate the activities of thelimbic system.
The ventral striatum, which is a striatal struc-ture, is now seen as essentially limbic. Whatthis means, conceptually, is that the regions ofthe brain that modulate emotion and motivationhave direct access to its motor systems, downas far as the brainstem and beyond even to theneurones that control somatic and autonomicmuscular activity.
Pleasure Pathways
The second important neuroscience discoveryof the 20th century was that of James Olds(1922–1976) and Peter Milner in the early 1950s(Olds and Milner, 1954). For centuries, thebrain had been viewed as a passive recipient ofsensory impressions, which led in a Pavlov-typesequence to motor action, with, in some philoso-phies (the behaviouralists) the assumption oflittle else of relevance in between stimulus andresponse. And yet a growing undercurrentof knowledge was emphasizing the preparedbrain, the brain not as a receptacle and tabularasa, but as an active organ, a synthesizing andcreating brain. Proceeding from the psychologyof Freud and his successors, the very drivennessof human activity, by unconscious and in sometheories unknowable forces, became commoncurrency, but these hollow frames lackeda neurological basis, a neurobiology of theemotions and movement.
What Olds and Milner did was uncover cere-bral circuits for pleasure and reward, endowinghedonic tone to percepts and behaviour. Thisresearch was being conducted at the same timethat Papez and MacLean were unravelling theadditional neuroanatomical structures alreadydiscussed. The identification of such a neu-roanatomy of the emotions opened the possibil-ity of altering emotional expression, and henceof providing amelioration of neurobehavioral

68 Biological Psychiatry
disturbances by influencing such circuitry. Thediscovery of dopamine and other neuromodu-lators ushered in the era of psychopharmacol-ogy and heralded brain stimulation: the abilityto influence crucial neuroanatomical circuitry,whether indirectly across the scalp or directlyby application of electrodes to the brain itself.
IMPORTANT ANATOMICALSTRUCTURES FOR UNDERSTANDINGBEHAVIOUR
Hypothalamus and Peptides
The role of the hypothalamus in regulatingeating and drinking has been well investigated.Destruction of the ventromedial nuclei resultsin hyperphagia, and destruction of the lateralhypothalamus, to aphagia. Stimulation leadsto the opposite. In part the effects are due toalteration of activity in fibres of passage passingthrough the region, and it is now known thatdopamine projections from substantia nigraare involved. An interesting observation isthat CCK, injected in small amounts intraperi-toneally or intraventricularly, leads to satietyin hungry animals. Another example of thecentral and peripheral action of a peptideneurohormone is in the regulation of drinking:the hypothalamus contains cells sensitive toosmotic signals and sodium levels, howeverangiotensin 2, the active form of angiotensin,peripherally causes vasoconstriction and renalsodium retention, and centrally stimulatesdrinking. Findings such as these emphasizethat the brain is a target organ for hormonesreleased peripherally and centrally, and mayexplain the presence of central receptorsthat bind hormones, especially in limbic andhypothalamic structures.
The increasing relevance of peptides becomesclearer as peptide circuitry is worked out. Thisis similar to the catecholamine systems, wherethe cell bodies of the neurone originate from afew discrete sites but influence wide areas of thebrain. In the CNS, peptides can be divided intotwo groups depending on the origin of their cellbodies (Roberts et al., 1984): one group from the
hypothalamus, the other has extrahypothalamicas well as hypothalamic neurones. The hypotha-lamic ones project to a variety of mainly lim-bic structures, including the limbic forebrain,the amygdala, the thalamus and the VTA. Incontrast, the extrahypothalamic ones are lessdiverse, with local projections and longer fibrebundles suggesting more specific functions.
Some other specific roles for peptides canbe defined. Thus substance P is thought to beinvolved with sensory transmission, beingpresent in the dorsal roots of the spinal cord.Afferent fibres are seen in the substantiagelatinosa, an area known to be linked to painperception, and in other areas related topain such as the pain fibre-receptive region ofthe trigeminal nuclear complex (Iversen andIversen, 1981). Release of substance P leads tointense pain. Enkephalin has been shown toexist in proximity to substance P neurones, andopiates inhibit the release of substance P. Thissuggests functional links between this peptide,opiates and pain appreciation.
There is an extensive network of CRFfibres running from the central amygdala to thehypothalamus, the parabrachial nuclei and on tothe brainstem, notably the dorsomotor nucleusof the vagus. This transmitter and vasopressinseem linked with stress responses. CCK is alsofound in similar situations, and CCK antagonistshave anxiolytic properties. CCK is now thoughtto be involved in the neurobiology of panicattacks and anxiety (Harro et al., 1993). Oxytocinreceptors are plentiful in the forebrain, and thispeptide, along with vasopressin, has arousedmuch interest recently. Oxytocin stimulatesmaternal behaviour in animals, while vaso-pressin has been shown to relate to pair bonding,revealed in differences in behaviour betweentwo types of vole. The prairie vole formslongstanding pair bonds with a partner, whilethe montane vole does not, being more inde-pendent and promiscuous. Vasopressin infusedinto the cerebral ventricles of the male montanevoles increases their bonding behaviour, aneffect replicated by increasing (by DNA vectormanipulation) their central vasopressin recep-tors. In contrast, female vole partner preferenceseems related to oxytocin (Lim et al., 2004).

Important Brain–Behaviour Relationships 69
Orexin A and B (hypocretin 1 and 2) are foundin the lateral hypothalamus and regulate sleepand appetite. The latter is partly related to theefferent projections of orexin neurones, whichinclude the cholinergic and monoaminergic cellclusters. Orexin deficiency is found in CSF innarcolepsy, especially when accompanied bycataplexy.
Neuron clusters in the lateral hypothalamus,such as the tuberomammillary nucleus and acluster in the perifornical area, project widelyto thalamus, basal forebrain and cortex and areinvolved with the sleep–wake architecture. Theperifornical cells synthesize orexin, an excitatoryneuropeptide which is involved in maintainingwakefulness. Neurones from the ventrolateralpreoptic hypothalamic nucleus are reciprocallyconnected with the tuberomammillary nucleus,and also influence sleep–wake cycles via pro-jections to hindbrain ascending monoamine,histaminergic and cholinergic arousal systems.
Insula
The insula occupies such a key position inthe limbic lobe, anteriorly connected to theorbitofrontal cortex, and posteriorly to the pari-etal and temporal lobes, that it should not besurprising that it seems to play a part in manyneuropsychiatric disorders. This has becomeespecially apparent with brain-imaging stud-ies. Polysensory inputs make the insula a site ofmultimodal convergence, interrelating events ofthe external world with relevant internally gen-erated motivational states, but also providingaffective tone and hedonic valence to percep-tual experiences. In insula epilepsy, a variety ofsensory symptoms may occur, including gus-tatory and olfactory ones, but also epigastricgurgling, rising epigastric sensations, nauseaand even vomiting – truly visceral. The insula isalso involved in the processing of pain and inaddictive behaviours, being activated by salientvisual cues (Shelley and Trimble, 2004). Deficitsof emotional expression have been noted inpatients with insula lesions. The insula has beenregarded as the receptive cortex for visceralinputs, from vagus influences for example. One
of the important insula efferents is to the centralnucleus of the amygdala, with outputs to the bednucleus of the stria terminalis and thence to thehypothalamus (the extended amygdala). Thesedescending influences to the brainstem allow forreciprocal interplay on the afferent autonomictone. Further, since the insula receives infor-mation from sensory cortex and the sphlanch-nic vagal input reaches sensory cortex via thethalamus, there is scope for much integrationof autonomic and sensory information withinthe brain.
Cingulate Gyrus
The cingulate gyrus is an extensive structurein the human brain, but from a neuropsychi-atric point of view most attention has been paidto the anterior cingulate. It embraces corticalareas 23, 24 and 25 of Brodmann. The anteriorcingulate-related disorders have much to dowith motivation and movement, with the exten-sive dorsal and ventral striatal connections.
In the past the cytoarchitectural differencesbetween the anterior granular cortex (area 32)and the posterior agranular cortex (area 24)were emphasized, but other distinctions arealso realized. At least four functional divisionsare suggested: a viscero-motor region (includ-ing area 32), a cognitive-effector region, a motorregion (area 24) and a sensory processing region,as found progressing from anterior to posteriorcingulate, respectively (Figure 3.2).
In animal models, the cingulate cortex isone limbic area which has been shown to beassociated with vocalizations and primate callson stimulation. Release of autonomic activity,including changes of breathing and heart rate,sexual arousal and automated oral behav-iours, can also be observed. Cingulate epilepsyis characterized by brief episodes of alterationof consciousness, but signs may include vo-calization, rapid onset of motor activity (axialflexion and limb extension) and gesturalautomatisms (Devinsky and Luciano, 1993).
In humans, the cingulate has been shown tobe nociceptive, probably related to its thalamicafferents, and a wide variety of affectiveresponses, including fear, euphoria, depression

70 Biological Psychiatry
7070
60
60
50
50
40
40
30
30
30
Counting Stroop (Bush et al., Ref.3) Counting Stroop (Bush et al., Ref.17)
trends in Cognitive Sciences
Emotional Counting Stroop (Whalen et al., Ref.18)
20
20
20
10
10
10
0CognitivetaskEmotionaltask
Cognitivedivision
Affectivedivision
Cognitivedivision
Affectivedivision
0
70(a) (b)
7060
60
50
50
40
40
30
30
30
20
20
20
10
10
10
0
0
cc cc
Figure 3.2 Meta-analysis of the different imaging studies carried out, highlighting the differences betweenthe cognitive and affective divisions of the anterior cingulate. Note that the studies employing cognitive tasks,(a) commonly employing multitasking, cause activations in the upper cingulate (in circles), while studiesmanipulating emotion, (b) cause activation in the lower affective division (in rectangles) (reproduced fromBush et al., 2000). A coloured version of this figure can be found on the colour plate
and aggression, have been elicited by stimula-tion in individual patients, as have behaviourscharacterized by disinhibition, hypersexuality,tic-like movements and obsessive and/orcompulsive activity. Lesions of the anterior cin-gulate, which will lead to a pattern of behaviourcharacterized by emotional blunting anddecreased motivation, are considered as one ofthe frontal lobe syndromes (see Figure 3.3).
Area 25, the subgenual cingulate area, hasbecome a focus of considerable interest fol-lowing observations that increased activity inthis area is strongly associated with depression(Wu et al., 1992), and it has become a targetfor surgical ablation for intractable depressionand more recently for deep brain stimulation(see Chapter 12 and Figure 3.3). This area hasreciprocal connections with other frontal areas,with the hypothalamus, the ventral striatum,the amygdala and the autonomic outputs of thebrainstem (Johansen-Berg et al., 2008).
New target for depression provided by functional imaging
Figure 3.3 The position of the subgenial cingulatearea, which has become a target for deep brain stim-ulation (courtesy of Dr Wayne Drevets)

Important Brain–Behaviour Relationships 71
The posterior regions of the cingulate gyrushave been less studied. They are less involvedwith motor functions and have more to do withvisuospatial function and learning and mem-ory, the latter being linked to the cingulateprojections to the subiculum. Posteriorly, thecingulate gyrus blends with an area of parietalarea cortex now thought to be involved withself-consciousness, the precuneus (see below).
Hippocampus
The hippocampus only has major cortical con-nections with the entorhinal cortex, but hasextensive subcortical afferents and efferents,and thus is a conduit for multi-informationalcortical influences on behaviour and is alteredin structure or function in many neuropsychi-atric disorders. It has been estimated that thereis a 5% chance of a CA3 neurone synapsingwith another hippocampal neurone, emphasiz-ing the rich connectivity of the area and its rolein memory. Many of the structures surroundingthe hippocampus, such as the entorhinal, para-subicular and retrosplenial parts of the limbiclobe, are continuous with the hippocampus, ren-dering the hippocampus larger that it appearsfrom surface anatomy. The hippocampus isinvolved in many neuropsychiatric disorders.One paradigm is temporal lobe epilepsy, butchanges of structure or function have been notedin schizophrenia, the dementias and affectiveand anxiety disorders.
Thus it seems established that apoptosis (celldeath) occurs in the postnatal hippocampus,and that in animal models psychotropic drugssuch as antidepressants and electrical corticalstimulation (ECS) can stimulate neurogenesis.The plasticity within the structure is thereforesubstantial, perhaps interlinked with its centralrole in the modulation of so many behaviours,especially memory. A memory circuit, whichincludes the hippocampus, the fornix and thehypothalamic mammillary bodies, has longbeen identified, and bilateral removal of thehippocampi leads to a severe amnestic syn-drome, with complete failure to lay down newepisodic memories (anterograde memories).
A similar picture is seen after bilateral fornixdamage.
Another hippocampal function relates to itsfunction as a comparator of novel and familiarstimuli, matching to expectation or prediction,and in the initiation or inhibition of behaviouralstrategies as appropriate to the situation. Itbecomes linked therefore to emotions such asanxiety, and to motor responses as evoked byits ventral striatal outputs (Gray, 1982).
Parahippocampal Gyrusand Entorhinal Cortex
It was a puzzle for a long time how sensoryinputs gained access to the limbic structures;this was part of the problem of the conceptof the ‘isolated’ limbic system. In the 1960scortico–cortical connections were unravelled,which revealed the projections from primarysensory areas to frontal association cortices, tomultimodal cortical areas (parieto–temporo–occipital) and to temporal cortex. A cascade ofincreasingly complex sensory information thusreaches the limbic lobe from these primary,secondary and tertiary sensory inputs. Theseconvey further integrated data about the envi-ronment to the limbic lobe. The input targetsinclude the amygdala and the hippocampus,and the parahippocampal gyrus, overlayingthese structures, provides a relay. Extensive pro-cessing of information occurs, in which real-timeinformation about the environment integrateswith past-time stored data of memory.
The entorhinal cortex (Brodmann’s area 28),the anterior part of the parahippocampal gyrus,which can be identified with the naked eye insome brains by the surface warty protuberancescalled the verrucae hippocampi (which over-lie an island of multipolar neurones), may beviewed as the great gate through which neocor-tical information reaches the hippocampus andthence other limbic system structures. The mainconduit of this is the perforant pathway (seeFigures 2.2 and 3.4).
There is clear evidence that this region hasaccess to specific sensory and multimodalsensory representations. The links with the

72 Biological Psychiatry
PR
PaS
UN UF
GA
TN
OLFC
RS
PRG(35)
ITG
ENT(28)
CF
Figure 3.4 The ventromedial temporal lobe in theleft hemisphere. The anterior parahippocampal gyrusis shown with small wart-like elevations. CF, colletralfissure; ENT, enterhinal cortex; GA, gyrus ambi-ens; ITG, inferior temporal gyrus; OLFC, primaryolfactory cortex; PaS, parasubiculum; PR, perirhi-nal cortex; PRG, perirhinal gyrus; RS, rhinal sulcus;TN, tentorial notch; UF, uncle fissure; UN, uncus(courtesy of Dr van Hoesen)
amygdala, and hence the hypothalamus andforebrain limbic structures, imply that theentorhinal cortex is another meeting point forintegrating information regarding the affectiveand internal state of the organism with currentand past sensory information. The traffic istwo-way, however, both from sensory cortex tothe limbic system and vice versa, allowing forlimbic influences on sensory experiences.
Precuneus
The precuneus, occupying part of the medialparietal cortex, is continuous with the cortex ofthe posterior cingulate gyrus, and connectedwith the inferior parietal lobule (Figure 3.5).The precuneus links the limbic structures withthe parietal neural apparatus involved with thebody image and with exterior space. The poste-rior cingulate, the retrosplenial cortex and theprecuneus area of the medial parietal lobe havebeen suggested to be linked to a neural networkwhich correlates with autobiographical mem-ories and self-consciousness. The precuneusis one of the sites where increased metabolicactivity occurs while the brain is idling, when
PRECUNEUSCINGULATE GYRUS
FORNIX
HIPPOCAMPAL GYRU
AT
MS
Figure 3.5 The parahippocampal gyrus and the pre-cuneus. Note how the former has direct inputs to thelatter. M, mammillary body; AT, anterior thalamicnucleus (reproduced from MacLean, 1949)
the individual is self-reflecting, and activitydecreases when attention is engaged in othertasks. Further, activity decreases in states ofdiminished self-awareness, such as anaestheaia,dementia or sleep (Cavanna and Trimble, 2006).This so-called default cerebral circuitry linksthe precuneus with medial frontal areas.
Amygdala, Extended Amygdalaand Ventral Striatum
Two main divisions of the amygdala groupof nuclei have been noted: the projections ofthe basolateral amygdala and the continuousbridge of cells from the central and medial nucleithrough to the bed nucleus of the stria termi-nalis: the extended amygdala. The former haveextensive outputs to the ventral striatum, a ven-tral extension of the basal ganglia, with connec-tivity to frontal cortical structures, with a centralposition in the cortico–striato–thalamocorticalre-entrant circuits and with strong downstreamconnections to midbrain and hindbrain struc-tures. Here limbic and frontal projections (serv-ing cognitive executive functions) overlap, andthis ‘limbic loop’ of the re-entrant circuits seemswell suited for selecting appropriate adaptivebehaviours for action (Heimer et al., 2007).
The extended amygdala, which receivesinput from the laterobasal amygdala, projects

Important Brain–Behaviour Relationships 73
to hypothalamus and other autonomic outputstructures. It is thought to coordinate the activ-ities of multiple limbic regions in determiningautonomic behavioural output.
A further area of anatomical interest hasbeen the identification of two components ofthe accumbens, namely a core and a shell withdistinguishing neurochemistry and connectiv-ity (see Figure 2.31). The shell has basal gangliaconnections, is closely linked to the extendedamydala and has outputs to the hypothalamusand brainstem motor and autonomic structures.The shell has an abundance of D1 and mu-opioidreceptors, which may be relevant to a role of theshell in addiction (see Chapter 9).
Nauta emphasized the integration betweenthe limbic system and the basal ganglia (Nautaand Domesick, 1982), a project developed muchfurther by Heimer and colleagues (2007). Thus,the structures of the limbic system, especially theamygdala, so vital for emotional interpretationof sensory stimuli, have direct pathways influ-encing motor output, which are additional tothe somatic motor loops described above. Theextended amygdala projects directly to auto-nomic and endocrine outflow areas, but canalso modulate the circuitry of the motor loopsand hence pyramidal outflow by influences onthe gate setting of the VTA and substantia nigra.A further direct pathway is from the amygdalato prefrontal cortex, and hence to the motor areaM3 and pyramidal tracts.
The ventrostriatopallidal system is thus seennot only as a radical alteration of our traditionalviews of the basal ganglia but also as an expan-sion of cortical output. The entire cortex projectsto the basal ganglia, and all cortex uses basalganglia mechanisms (Heimer et al., 2007).
A reliable finding from f MRI studies is thatemotional stimuli enhance amygdala activity,especially such stimuli as fearful faces, andevidence is accumulating that the amygdala isalso associated with decision-making and thusthrough its output channels is central to guid-ing or even driving human behaviour. The lattermay include the social appraisal of the emotionalstate of others, and value judgments in complexsocial situations.
Autonomic Nervous System
The autonomic nervous system has long beenknown to regulate such bodily activities assweating, heart rate and respiratory rate, andto be involved in fear responses and the so-called ‘flight and fight response’. In the courseof phylogeny, the vagus nerve of mammalshas developed two efferents: a myelinated one,originating in the nucleus ambiguus, and anunmyelinated one, originating in the dorsalmotor nucleus of the vagus (see Figure 2.25). Themyelinated fibres provide the primary vagusregulation of the heart and bronchi, while theunmyelinated fibres provide the primary vagusregulation to subdiaphragmatic organs.
Unique to mammals is the neuroanatomicaland neurophysiological link in the brainstembetween the source nuclei of the nerves con-trolling the striated muscles of the face andhead, including the muscles of the middle ear,and the source nuclei of the myelinated vagus.Thus, in mammals there is a close connectionbetween the regulation of the facial muscles andthe visceral state. This provides a neurophysio-logical explanation for the covariation betweenfacial emotional expression and changes of bod-ily state and feelings. The sensory pathwaysfrom the trigeminal and the facial nerve providepotent input to the nucleus ambiguus.
With development, the infant has more andmore myelinated vagus fibres, as social commu-nication and facial expressions and responsesdevelop. There are facial-recognition areas inthe fusiform and superior temporal gyri, whichappear to detect intentionality of movement andmay modulate the amygdala, leading to flow ofneural activity to the appropriate output chan-nels (macrosystems) for the required responseto the facial expressions encountered. Thisexplains the amygdala and fusiform responsesto fearful faces shown with brain imaging.
The insula is central to this behaviour, withits vagus visceral afferents and outputs toamygdala, the bed nucleus of the stria termi-nalis (extended amygdala) and thence downto pontine and brainstem nuclei, influencingsome of the very same nuclei that provided

74 Biological Psychiatry
the autonomic input, including the nucleusambiguus (Porges, 2007).
Subthalamic Nucleus
This area of the basal ganglia circuitry hasexcited much interest recently as it has becomea target for DBS, especially in movement dis-orders. It lies close to the substantia nigra andis reciprocally connected to the globus pallidusexterna and interna. However, it is suggestedthat as with other basal ganglia structures it isdivided in its afferents and efferents, having adefinable limbic component, which is connectedto forebrain limbic structures and frontal corti-cal areas including the subgenual cingulate. Thismay explain why occasional patients suddenlydevelop emotional displays during subthalamicDBS (Bejjani et al., 1999).
SOME SPECIFIC BEHAVIOURS
Aggression
The relationship of the amygdala to aggres-sion seems well established, although a recip-rocal link with the hypothalamus and frontalcortex seems important. In one of the earli-est studies of brain–behaviour relationships,Kluver and Bucy (1939) and then Schreiner andKling (1956) tamed various aggressive felinespecies with bilateral amygdala lesions, an effectabolished by additional lesions in the ventro-lateral hypothalamus. The Kluver–Bucy syn-drome was one of the first limbic syndromes tobe recognized. The main features were an alter-ation of personality with loss of aggressivityand taming, a tendency to repetitively explorethe environment orally (hypermetamorphosis),hypersexuality and visual agnosia.
Aggression can be provoked by stimulationof the amygdala, the hypothalamus and thearea around the fornix in the diencephalon,and hypothalamic elicited aggression can beinhibited by stimulation of the ipsilateral frontalcortex (Siegel et al., 1975). Delgado (1966), usingimplanted intracerebral multilead electrodesto stimulate various regions of the brain in
monkeys, also recorded aggressive responsesfrom the ventral posterolateral nucleus of thethalamus and the central grey area. Rosvoldet al. (1954) demonstrated how amygdala lesionslead to loss of dominance in a social hierarchy.
Adamec, based on studies with kindling,introduced the concept of ‘limbic permeability’.Thus kindling is an experimental procedure inwhich small, brief, high-frequency currents arepassed across electrodes in an area of brain.At first no effects are seen, but after severaltrials, usually given on a daily basis, an after-discharge develops, and behaviour changes areseen. As the process continues, eventually theanimal, in spite of still receiving subthresholddoses, will have a generalized seizure. The asso-ciated changes in brain physiology, as yet notwell identified but thought to be related to LTP,are long-lasting, and the animal remains sus-ceptible to a seizure on passing the current forthe rest of its life. Kindling occurs best in limbic-system structures, especially from the amygdalaand hipocampus.
Adamec and Stark-Adamec (1983) used catsto kindle lasting behavioural changes, notablyaggressiveness or defensiveness. Limbic per-meability, the degree and facility of seizurepropagation from limbic to hypothalamic areas,could be related to these behaviour changes.
The frontal cortex is also part of the cir-cuitry that modulates aggressive responses.Stimulation of frontal cortex at the same timeas the hypothalamus increases the time to anaggressive episode in cats (Siegel et al., 1975),and in patients with epilepsy, very aggressivebehaviour interictally has been shown withMRI imaging to be associated with thinning ofthe left lateral frontal cortex (Tebartz van Elstet al., 2003).
The literature on the role of various trans-mitters in aggressive behaviour is confusingand highly species-dependent. It is furthercomplicated by the differing models ofaggression involved. Generally, decreasing theturnover of 5-HT, and increasing cholinergicor catecholaminergic drive, facilitates aggres-sive behaviour. Tricyclic antidepressants andmonoamine oxidase inhibitors (MAOI) arelikewise facilitatory (Eichelmann, 1979), as are

Important Brain–Behaviour Relationships 75
hormonal influences, for example the increasein aggression associated with testosterone.
In summary, while the spontaneous displayof aggression is obviously dependent onenvironmental stimuli from many sources, thecentral roles of the amygdala and the hypothala-mus in its neural organization seem establishedfrom animal studies. Since the frontal cortex hasintimate connections with the hypothalamusand the amygdala, these findings hint ata behavioural circuit, although the details,especially in humans, remain to be elucidated.
Anxiety and the Septohippocampal Link
The existence of a behavioural inhibition sys-tem which modulates anxiety responses hasbeen proposed (Gray, 1982). The neural counter-part of this is the septohippocampal circuit, andanxiolytic drugs are thought to act by inhibit-ing this system. Briefly, lesions of the septalarea or the hippocampus lead to a pattern ofbehaviours similar to that seen after giving anx-iolytic drugs, and stimulation of the septal areacreates the opposite effect. The septohippocam-pal system forms an extensive interconnectedneural network, and acts, with the associatedPapez circuit, as a comparator, generating pre-dictions about anticipated events and match-ing them to actual events. Mismatch allowsthe behavioural inhibition system to dominate,interrupting behaviour and generating a searchfor alternatives by increased arousal and atten-tion. The ascending monoaminergic systems,especially noradrenaline and 5-HT, modulateinformation flow into the hippocampus.
A shortcoming of this model is the lack ofreference to the amygdala. However, amygdalalesions dramatically influence anxiety responses(as in the Kluver–Bucy syndrome), and benzo-diazepine receptors are plentiful in the amyg-dala. Microinjections of benzodiazapines intothe amygdala, but not the hippocampus, reducefear (LeDoux, 1992).
Neural circuits for the conditioning of auto-nomic and fear responses have been workedout in animal models using auditory stimuli(LeDoux et al., 1988). There are essentially twopathways involved. The first is from auditory
cortex to inferior colliculus to medial geniculateto amygdala, extended amygdala and the auto-nomic and somatomotor outputs. This directsubcortical pathway does not involve corti-cal associations and is essentially rapid butcrude. The second circuit involves the neocor-tical auditory system, feeding to the amygdalavia association cortices, giving a more delayedroute, with refinement of the message. LeDouxtries to resolve the issue of the relative contri-butions of the amygdala and hippocampus bydrawing a distinction between fear and anxiety.The former relates more to interactions betweensensory processing areas and the amygdala, andaffective implications are assessed. Hippocam-pal inputs to the amygdala contribute cognitiveinformation, leading to anxiety for specific situ-ations (see Figure 2.16).
Memory
Other functions assigned to the hippocampus,in light of electrophysiological stimulation andlesion experiments, mainly relate to memory.Although severe memory problems afterhippocampal destruction were first defined inhumans, animal studies produced conflictingdata. Several competing theories now exist,although all ascribe to the hippocampus a role inhigher cognitive function. One suggestion is thatit is involved in the construction of spatial maps(O’Keefe and Nadel, 1978); an alternative is thatit subserves spatial memory. Its precise role inhuman memory is unclear, but relates either tothe consolidation of short-term memory or tothe retrieval of information once remembered.
Squire et al. (1989) have suggested that theCA1 and CA3 fields of the hippocampus areespecially involved in receiving and trans-mitting highly integrated information to andfrom the neocortex, sites of permanent memorybeing cortical.
The role of neuronal plasticity is crucial. TheNMDA receptor is related to the developmentof LTP (increased postsynaptic excitability aftera volley of impulses) in the CA1 region. Depo-larization of the non-NMDA glutamate receptoris required to open the NMDA channel, butonly with synergistic firing of adjacent synapses

76 Biological Psychiatry
or burst firing. This leads to synapse modifi-cation with strengthening of synaptic connec-tions and the potential for the laying down ofmemory traces. Acetylcholine is another neu-rotransmitter involved in the laying down ofepisodic memories.
The amygdala also plays a crucial role inmemory, notably for emotionally influencedmemories. Fear learning is inhibited by injec-tion of protein synthesis inhibitors into theamygdala. In laying down memory traces, thehippocampus and amygdala are thought to syn-chronize in the encoding of information, thehippocampus encoding through time and spacewhile the amygdala provides emotional valenceand contributes to reinforcement. Other crucialareas are the entorhinal and perirhinal cortices,the fornix and the mammillary bodies.
However, memory consolidation involves aprogression of trace migration from these allo-cortial structures to the neocortex, and frontal,cingulate and parietal areas are especiallyinvolved. The neural correlates of memoriesdecrease their dependence on the hippocampus,and become widely distributed in cortex. Withtime, due to the continued plasticity of thebrain and the recharging of memories throughrecall (each time different from the time before),remodelling occurs. Memory is actually onlyone way of forgetting.
Sexual Behaviour
The changes in sexual activity seen with theKluver–Bucy syndrome were confirmed inother species. The amygdala seems to beimportant in its regulation, and hypersexualityinduced by amygdala destruction can bereversed by septal lesions (Kling et al., 1960),supporting the role of the latter in pleasurablesexual experiences. Penile erection in monkeyscan be seen after stimulation of the septum(MacLean and Ploog, 1962), and electricalactivity is recorded here in female rabbits andhumans with orgasm (Heath, 1972; Sawyer,1957). The hypothalamus is clearly involved insexual behaviour, and lesions in the anteriorhypothalamus prevent the hormonal activationof sexual activity (Heimer and Larsson, 1966).
There are many steroid-binding sites inhypothalamic regions that interact with sys-temic hormones to modulate behaviour, furtherinterrelated with the influence of monoamineand peptide systems (Herbert, 1984).
Arousal, Sleep and the Reticular Formation
Arousal and consciousness are related to thetonic control of the ascending reticular forma-tion, extending from the medulla upwards tothe thalamus. On stimulation of this area there isdesynchronization of the EEG and behaviouralarousal. Lesions in this area lead to perma-nent sleep, although regions within it, such asthe median raphe, when destroyed lead to astate of permanent insomnia. Thus, the homo-geneous mass of reticular neurones referred tooriginally as the reticular activating system hasnow been shown to contain within it many dif-ferent neuronal groups, including the originsof the long-ascending monoamine and peptidepathways, and nuclei sensitive to sensory infor-mation from the cardiovascular and respiratorysystem. Some of its efferents descend to thespinal cord, influencing motor neurones andsensory afferents. Thus, the reticular formationreceives input fibres from adjacent ascendingand descending tracts and nuclei, the hypotha-lamus, the limbic system and cortex, and moder-ates arousal, conscious activity and sleep–wakecycles. Cholinergic transmission, especially viarelays in the thalamus, is important in arousaland in generating REM sleep (the period of sleepassociated with dreaming and cortical desyn-chronization on the EEG).
Motion, Emotion and Motivation
Even today, exploration of the neurobiologyof one of the most fundamental attributes ofbehaviour, namely what makes you tic(k), isin its infancy. The most significant advancesin this field have derived from the discover-ies of Olds and Milner (1954), and those ofNauta (1964, 1986; Nauta and Domesick, 1982),Heimer and others, who unravelled the essen-tial links between the limbic system and the

Important Brain–Behaviour Relationships 77
basal ganglia, revealing the role of the latter inmotivation. Thus, traditionally the basal gan-glia were viewed as being solely related tomotor behaviour. However, emotional displayinvolves motor patterns (hence e-motion), motorabnormalities are seen in patients with psy-chiatric illness as a part of their symptoma-tology (Trimble, 1981a) and motor disordersare frequently associated with psychopathol-ogy (Trimble, 1981a). Movement and emotionare linked in common speech (hence ‘a mov-ing experience’).
The extended amygdala and the accumbens(limbic basal ganglia) are central to theseconcepts. The limbic efferents to cerebral cortexrelate both to the development of memoriesand, especially from the amygdala, to theemotional valence of ongoing sensory stimuli.The hippocampal and amygdala outputsto the ventral striatum serve to gate infor-mation in cortico–striatal–pallidal–thalamiccircuits, and hence the outflow to both themotor pathways and also association andfrontal cortices. Further, autonomic activityis coordinated with this by the extensivenetwork of rostrocaudal connections from theextended amygdala through hypothalamus,periaqueductal grey, ventrolateral medullaand on to the efferent nuclei of the vagusnerve and sympathetic nervous system. TheseCNS sites seem to cooperate and coordinatevisceral and motor functions, allowing for acomprehensive emotional motor output, andthe term ‘emotional motor system’ has beenused to describe the autonomic components ofthis (Holstege, 1996).
In this scheme, the dorsal striatum is seen asbeing involved with neocortically derived motorbehaviours, and the ventral striatum is relatedto emotional arousal and expression. These stri-atal structures are filters of limbic and corticalinformation, permitting appropriate signals togain access to motor pathways (Mogenson et al.,1980). The role of dopamine is crucial here. Themesolimbic–prefrontal dopamine system lacksautoreceptors, has a higher cell-firing rate thanthe other dopamine neurones and is the onlyone to show an increased turnover in responseto stress.
The limbic output to the basal ganglia struc-tures is massive, and until this became realized(with the new anatomical investigations of thepast 40 years) there was a failure to understandthe neurology of behaviour in any complexity.‘A greater portion of behaviour is nondeter-ministic, an outcome governed by genetic pre-dispositions, societal norms, learning, rewardand motivation. It is this aspect of behaviourwith which the limbic lobe and basal forebrainare largely concerned . . . neural output deriva-tive of higher order, cortically derived cognitiverepresentations, is channelled from the greaterlimbic lobe through several macrosystems, eachof which may read messages differently andredistribute them back in altered form to thebrainstem and, via re-entrant circuits, back tothe cognitive apparatus. . .’ (Heimer et al., 2007,pp. 100, 104).
It is interesting in this context that disordersof motivation are barely considered in classi-fications of psychopathology. Yet essential tobehaviour is action, giving direction and changeto the status quo. Included would be impulse,desire and striving towards goals, individualmotivations being variously consciously avail-able or not. Patients with primary amotivationalstates are frequently encountered in clinicalpractice, and secondary disorders of motivationare noted in a wide variety of psychopatholo-gies (see Chapter 9). The unravelling of theneuroanatomy of the limbic forebrain allows foran understanding of these behaviours, whichcorrelate closely with that prime biological andnotably human force, the will, once seen as anindependent psychological faculty, now viewedas tightly bound with identifiable neuroanatom-ical and neurochemical substrates.
LIMBIC LOBE DISORDERS IN ACLINICAL CONTEXT
In clinical neurology it is customary to ascribecertain signature syndromes to various cor-tical lobes. Thus there are well-recognizedparietal-lobe syndromes, such as the apraxiasor the alexias, and there are the frontal-lobesyndromes (see below). However, few textsdescribe specific limbic-lobe disorders. An

78 Biological Psychiatry
exception is temporal-lobe epilpesy, which isdiscussed in detail in Chapter 10.
Limbic encephalitis is a rare disorder,secondary to certain viral infections, notablyrabies (rarely), and more commonly herpessimplex. Following a prodromal phase ofnonspecific symptoms, behavioural changesoccur with herpes simplex which includebizarre out-of-character behaviour, sometimeshallucinations, and also epileptic seizures. TheEEG may reveal unilateral or bilateral changesin temporal leads. The HSV-1 virus leads tomarked pathology in frontal and temporalareas, and the chronic state is characterizedby dense amnesia, irritability and aggression,distractibility, emotional blunting and featuresof the Kluver–Bucy syndrome. It is possibleto look for autoimmune antibodies to humanbrain intracellular or membrane antigens toestablish diagnosis.
A variant is seen in some patients with car-cinoma. This also presents with disturbancesof affect, depression, anxiety, and sometimeshallucinations and/or seizures. It is seen mostcommonly with bronchial oat-cell carcinomas,and pathology is noted in the amygdala, hip-pocampus, fornix and mammillary bodies. It isthought to be secondary to an immunologicalprocess, but the observations that such rela-tively selective pathologies target the limbiclobe suggests that their anatomical location andunderlying neuronal constitution have somespecific defining biological markers.
In the Urbach–Wiethe syndrome there isselective bilateral degeneration of the amygdala,and relatively selective temporal pole – medialtemporal limbic damage can be seen afterhead injuries.
RE-ENTRANT CIRCUITS IN ACLINICAL CONTEXT
The theory of the parallel cortical–subcorticalre-entrant circuits (see Figures 2.11 and 2.12) hashad an important impact on the understandingof several neuropsychiatric disorders. As shouldnow be clear, they are central not only to motorsystems, but also to a broad understanding
of the behavioural ramifications of limbicfunction and dysfunction. Altered activity inthe descending cortical–striatal–thalamic loopsinfluences motor output via the cascade ofinhibitory and excitatory neurotransmitterswhich regulate activity in these circuits. Ingeneral, the parallel distributed nature of thecircuits suggests that interventions or lesions atone of the nodal points (e.g. the pallidum) willlead to a similar clinical picture to a lesion atanother point within the same circuit. Secondly,the implication is that a lesion in one circuitwill be somewhat self-contained, and that theresulting behavioural effects will be different tothose noted with changes in an adjacent circuit.Quite how segregated such ‘basal ganglia loops’are in reality is however unclear, and thereis good evidence of cross-talk between them.Nonetheless, they have formed a paradigmwhich has been used effectively to explainmany clinical observations. This is illustrated forexample with the descriptions of three differentprefrontal syndromes, noted following lesionsof one of the three prefrontal described circuits,namely the dorso–lateral, the orbital and themedial frontal–cingulate circuit (Figure 2.29).
Thus, central to the above three syndromes isalteration of motor, emotional and motivationalbehaviours and involvement of the ventral stria-tum. In contrast, the syndromes related to thedorsal circuitry, such as Parkinson’s disease – inwhich the dopamine input to the dorsolat-eral caudate-putamen degenerates – present ini-tially with motor symptoms, some tremor andmuscle stiffening. However, because these dis-orders, as they progress or are influenced bytreatment, involve ventral striatal structures,behaviour problems then also emerge as a signif-icant part of the clinical picture. In Parkinson’sdisease, 40% of patients will develop depres-sive syndromes, and as the disease progresses,psychoses may appear. It is estimated that 30%of patients will have hallucinations, and about10–20% develop frank psychoses, often exacer-bated by dopamine agonists.
In a psychiatric context, these circuits havebeen used to help understand the underlyingneuroanatomy of several disorders. A paradigmis obsessive–compulsive disorder (OCD), often

Important Brain–Behaviour Relationships 79
linked to neurological disorders involving thesestructures and with alteration in fronto-basalganglia activity revealed using brain-imagingtechniques (see Chapter 6). Neurosurgical oper-ations and direct brain stimulation for OCD anda number of other neurological and psychiatricdisorders involve interfering with these circuits(see Chapter 12).
THE FRONTAL LOBES IN ACLINICAL CONTEXT
Recognition of the strategic importance ofthe frontal lobes in understanding humanbehaviour is often attributed to the observationsof John Martyn Harlow, who described thecase of the now famous Phineas Gage. Theunfortunate man had a tamping iron drivenat high velocity through the frontal part ofhis skull; he survived the injury but was leftwith severe personality changes. The site ofthe injury has recently been reconstructed, andshown to involve the ventromedial region ofboth frontal lobes, a part of the frontal cortexconnected with subcortical structures such asthe amygdala and hypothalamus; however,since the injury left the rest of the frontal lobesintact, Gage developed no speech or generalintellectual impairments. It was his socialjudgement that was affected, leaving him ‘nolonger Gage’ (Damasio et al., 1994).
It is now customary to refer to three ratherdistinct frontal-lobe syndromes, based onthe underlying neuroanatomy of any lesionsor functional disturbances. In reality, manypatients with frontal pathology show a com-bination of symptoms, partly based on theclinical fact that injuries such as head injuriesor tumours fail to obey natural lines of dissec-tion, but also on a relative fragility of the linksbetween anatomy and behaviour in general, andthe nature of the cortical–subcortical circuitry.In other words, the manifestations of a frontalsyndrome may differ with the extent of sub-cortical tissue involvement. Further, so-calledexecutive functions, while perhaps driven byactivation in the frontal areas, involve the brainin a much broader context. Motor knowledge,
the ability to perform and contain on-line acontinuous sequence of desired movements andtheir operation, implicates also executive atten-tion and memory: so-called working memory.In considering activity in frontal networks, it isimportant to consider their extensive input fromposterior cortical areas, notably linking sensoryassociation areas with motor equivalents, whichare reciprocated in what Fuster refers to as aperception–action cycle (Bodner et al., 2005;Fuster, 2004). Thus, the so-called corollary actionof frontal activity, the anticipatory monitoring ofongoing sensory and motor action in response toan action, with feedback and feed-forward loopshaving corrective and modulating attributions,is related to frontal efferent discharge to theassociation cortices of the parietal and temporalcortices via the longitudinal and arcuate fasci-culi. The additional reciprocal limbic–frontalconnectivity allows memory and motivationalcomponents of the cognitive hierarchy to beincorporated into an action sequence.
The three main syndromes of neuropsychi-atric interest are the orbital, the dorsolateraland the medial syndromes. The dorsolateralsyndrome, involving isocortex, with anatomi-cal conectivities to the thalamus, hypothalamus,amygdala and hippocampus, and prominentoutflows to the caudate nucleus, is often com-plex and can be variable in presentation. Itmay involve problems with motor facility andtemporal integration, leading to perseverationsand motor persistence, such that performingsequenced hand positions (such as the Luriathree-hand-position test) is impaired, or patientsmay have difficulty copying from design tem-plates with alternating patterns, such as mul-tiple loops. The mental inflexibility is revealedwith such tests as the Wisconsin card-sortingtest, in which sorting of cards into differentgroups is achieved only by the examinee detect-ing an undisclosed rule; the rule is then changedby the examiner, and the new one must be fol-lowed. The failure to shift the mental set withperseveration is then revealed in someone witha lesion involving this dorsolateral circuit.
Representations of the world must be heldon-line, prior to action (working memory), andwhen disturbed this leads to problems with

80 Biological Psychiatry
tasks of short-term and intermediate memory.There is poor spontaneous recall and a ‘forget-ting to remember’; however, recognition mem-ory and memory for implicit tasks (motor acts)remains intact. Language tasks such as word-listgeneration are impaired more following domi-nant hemisphere lesions, while design-fluencytasks (generating as many different designs ina one-minute time interval) are impaired withnondominant lesions.
With the dorsolateral syndrome, planning isimpaired, and shows up in tasks such as theTower of London test and variants, in whichpatients are asked to rearrange objects in as fewmoves as possible to achieve a specified pattern.Sometimes the inability to inhibit a responseis shown; the Stroop test is one such task, inwhich the patient has to state the colour of aword where the colour in which it is printed(say blue) is different from the word itself (saygreen). The natural tendency is to read ‘green’,which has to suppressed. They may be unableto inhibit a motor response; for example, whenasked to tap once in response to the exam-iner tapping twice, and tap twice when theexaminer taps once, they will tend to tap asthe examiner. Estimating answers to unusualquestions may be awry (‘How tall is the EmpireState Building?’), as may proverb interpretation,which becomes concrete.
Stimulus binding and environmental depen-dence are key features of the dorsolateral syn-drome, shown by poor attention with easydistractibility, poor planning abilities and con-cretization of thought. Attentional problemslead to a reduced digit span and failure on con-tinuous performance tasks. Further, a number ofpatients will show either utilization behaviouror imitation behaviour, where attention is capti-vated and dominated by environmental stimuli.In utilization behaviour, patients use objectsplaced in front of them even if they do notneed to. The classic example is giving a patient apair of glasses to wear when they already have apair on; they will put on the second pair withoutremoving the first. In imitation behaviour, thepatient copies even complex movements of theexaminer (such as picking up a patella hammer
that the examiner has used and tapping theexaminer with it).
The dorsolateral syndrome is summed upby the expression ‘executive function’. The term‘dysexecutive syndrome’ has become popular toshort-hand this clinical picture. Unfortunatelythis term suggests some overarching super-visory system, which fails to emphasize theflexible and dynamic nature of the neuronal sys-tems involved, and the important roles of thebasal ganglia and parietal cortex in integratingbehaviour.
The medial frontal syndrome is related tolesions involving the anterior cingulate cortex,with extensive connections to limbic and sub-cortical structures, and is associated with apathyand loss of drive for many or most of an indi-vidual’s daily activities. Affect is flattened, thereis an emotional emptiness, social contacts arediminished, and lack of interest in others and theself are seen. Self-neglect, reduced spontaneousbehaviour and speech, increased dependenceand sometimes abulia (complete loss of will)may be seen, with patients sitting doing nothingfor long periods of time, not getting bored at all.In bilateral cingulate lesions, akinetic mutismappears, with virtual lack of spontaneous inter-action with the world, in spite of being awakeand following events visually. The medial syn-drome is summed up by the expression ‘apathy’.
In the orbital frontal syndrome, patients likeGage display a lack of social concern and judge-ment. They are disinhibited, tactless and aggres-sive in social interactions, and lack insight intotheir coarseness. Their capacity for empathy isdiminished and they display poor risk assess-ment. This clinical picture is sometimes referredto as ‘pseudopsychopathic’. The key anatomicalconnectivities are again limbic and subcortical,especially the amygdala, hippocampus, thala-mus and hypothalamus. The orbital syndromeis summed up by the expression ‘disinhibition’.
Disturbed affect is common in people withfrontal lesions. This may be a lability, which tothe uninitiated may seem at times like a bipo-lar disorder. Depressive-like behaviour seemscommon, but testing may reveal the associatedcognitive stamps of a frontal lesion. However,

Important Brain–Behaviour Relationships 81
there are clear associations between disorders ofaffect and frontal activity, as revealed particu-larly with neuroimaging studies and discussedin Chapter 6.
LATERALITY
It is now well accepted that in the human brainthere is lateralization of functions within thecerebral cortex. Potentialities to lateralization,which are suggested in some other species, haveactualized in our evolution with huge conse-quences. Many aspects of speech are linked,in right-handed people, to the left hemisphere,while spatial and emotional processing is more afunction of the right hemisphere. This skewingof the brain’s functional allocation must havehad evolutionary advantages, placing represen-tations that did not need to be bilateral, as forexample those regulating vision or the motorfunctions of the two hands obviously do, inone or other hemisphere. This would minimizebrain size and energy consumption, and allowfor continued safety of the process of birth inmammals. Neurones with the same type of com-putational activity are placed together, aidingthe developing brain and minimizing the needfor long-distance connecting axons. It seems thatfunctional asymmetry in humans begins early inlife, blood flow showing a right-hemisphere pre-dominance until about age three, when a shift tothe left occurs. What is less clear is whether ornot the primitive cortical, limbic and subcorticalstructures of the brain also have lateralized func-tions, and if they do, how this may influence,or have influenced in the course of evolution,the overlying cortical development. The animalexperimental literature suggests that lateraliza-tion of even limbic and subcortical structures isindeed the case (Vallortigara, 2006a, 2006b).
Thus some suggestion of lateralization offunction can be found in species all the wayalong the phylogeny from fish to nonhuman pri-mates, which relates not only to basic behavioursbut also to everyday social repertoires, and theoverall conclusion seems to be that lateraliza-tion of function in the brain is found acrossmany vertebrate species. With regards to limbicstructures, there is good evidence from pri-mates, from human brain stimulation studiesand from patients with epilepsy of lateraliza-tion. It has been shown for example that inrhesus monkeys and marmosets there is a pop-ulation bias for the right hemisphere to controlemotional expressions. In humans, the rightamygdala is associated with fear and panic.Tachycardia recorded during seizures is asso-ciated with right-temporal-lobe epilepsy, andhuman micturition seems regulated by a groupof cortical and subcortical structures predom-inantly right-sided. There is evidence for lat-eralization of function in the human insula,especially with regards to the control of auto-nomic activity.
Several of the major neurotransmitter sys-tems in the brain, which drive and regulatebehaviour, seem asymmetrically distributedin animal and human brains, includingdopamine, acetylcholine and GABA (all with aleft-hemisphere predominance), and 5-HT andnoradrenaline (which have right-sided predom-inance). Separate processing abilities of the twohemispheres may relate to these observations,since such neurotransmitters, involved with theexpression of motor behaviour and attention,may link with the differing hemisphere capa-bilities, and the right hemisphere’s capacity inHomo sapiens for maintaining holistic, globalrepresentations, which are closely related toarousal and attentional mechanisms.


4Classifications and Clinical Investigations
INTRODUCTION
Although it is readily apparent in case confer-ences, it is often poorly appreciated that ourconcepts of disease are not immutable, and var-ious models may be proposed. It is customaryto assume that a disease has some independentexistence of its own, visiting our healthy bod-ies and altering them in some way. Physiciansnote these changes, establish the pattern thatthey assume, ascribe a diagnosis and prescribea remedy that will influence the disease process.Earlier theories using this model attributed dis-ease to the intrusion of spirits and evil forces,often as a punishment for wrongdoing. Latertheories were given the most powerful boostby the discovery of microorganisms, and theircure by antibiotics. However this led, in manyinstances, especially of infections, to diseasebeing seen as having a single cause, and, ideally,a single treatment.
Hippocrates (c. 460–c. 380 BC) introducedthe historical dimension to disease, and thefirst case histories in medicine were from thisera. A disease has signs and symptoms, abeginning, a course, a duration and an outcome.Recognition of diseases as independent entitiesdid not come until the 17th century, however,and the works of Baglivi and Sydenham, whofelt that diseases in their natural states weresubject to the same laws of observation anddescription as other natural phenomena. Thefinal step was made by Virchov, who combinedhis cellular pathology with the new knowledge
Biological Psychiatry 3e Michael R. Trimble and Mark S. George 2010 John Wiley & Sons, Ltd
of anatomicoclinical medicine, completingthe notion of disease as a local affection. Theresearch for classification systems as well asaetiology became predominant.
Entwined with the development of the con-cept of a disease as an independent local entityhas been the principle of reaction: Sydenham(1740), in spite of his attempts to study the nat-ural history of diseases, recognized this impor-tant element: ‘. . . a disease is nothing else butNature’s endeavour to thrust forth with all hermight the morbifick matter for the health ofthe patient. . .’ (p. 1). Thus intrinsic, as opposedto extrinsic, factors assume importance in thepathogenesis of symptoms. The reactions of theorganism were seen as healing.
This ‘biographic’ conception of disease standsin obvious contrast to the ‘ontological’ one, in thesense that it admits only diseased individuals,and not diseases per se. It has had a marked influ-ence in psychiatry. The testimony of individuals,as opposed to clinical observation, assumes withthis model an ever-increasing significance. Theintrospective techniques of the psychoanalyticmethod took this to its extreme, devaluing diag-nosis, elevating the subjective and, in most cases,allowing its practitioners the excuse not even tophysically examine their patients! The phrase‘reaction types’ became an accepted nomencla-ture, especially in the United States, under theinfluence of both psychoanalytic thinking andthe contributions of Adolf Meyer. Extreme con-clusions of this stance have been taken by some

84 Biological Psychiatry
authors, such as Szasz, who would deny thevery existence of psychiatric illness.
Finally, the technology of the 20th centurysaw statistics used in attempts to define disease.It was Galton who, in the 19th century, suc-cessfully applied mathematical and statisticalmethods to the measure of biological phenom-ena, and demonstrated how this could also bedone for psychological data. The use of sta-tistical models for the definition of normalitywas adopted by psychiatry, especially for per-sonality disorders, and the development of alarge range of rating scales of psychopathologyderived from these techniques.
SIGNS, SYMPTOMS, SYNDROMESAND DISEASE
In clinical medicine we recognize two fun-damental kinds of data. Symptoms are thosecomplaints of the patient that are spontaneouslyreported or are elicited by the clinical history.Signs are observed by the physician, the patient,or a friend or relative of the patient, and indicatethe presence of some abnormal functioning ofone or more body systems. A syndrome is a con-stellation of signs and symptoms which seemto coalesce to provide a recognizable entitywith defining characteristics. Syndromes maybe classified, and are the clinical representativesof illness. The latter implies some biologicalchange or variation of the organism, and thetask of medical science has been to explore this.A clear distinction has to be drawn between ill-ness and disease: illness is that with which thepatient presents, which only in part representsthe expression of disease. Biological psychia-try attempts to understand psychiatric illnessthrough defining syndromes and ultimately dis-eases, based on a knowledge of the associatedchanges of the structure and function of the cen-tral nervous system and their provoking factors.
At the present time, classification of diseasein medicine generally represents a potpourri ofnotions, some being defined by symptoms (suchas epilepsy, migraine or schizophrenia), othersby aetiology (such as syphilis) and still oth-ers by pathology (such as Alzheimer’s disease).
Indeed, with regard to the CNS, no attempthas been made to provide a comprehensiveclassification since that of Romberg in 1853. Ingeneral, in medicine progress has led from syn-drome delineation and the classification basedupon it to an understanding of pathology and anew classification. General Paresis of the Insane(GPI) is now classified as a syndrome of syphilis.Unfortunately, for many psychiatric syndromes,the underlying aetiologies and pathogeneses areunclear, and reliance on syndrome classificationhas led to a multitude of different classificationsystems. An important question is why psy-chiatry largely remains at the level of syndromeclassification, when much of medicine, and evenneurology, has moved beyond syndromes todisease classification. This is likely due to theuntil-recent inability to examine the main organof interest (namely the brain) while patients arealive, the lack of readily identifiable neuropatho-logical changes at autopsy, mistaken notionsabout the mind and brain, and the sheer com-plexity of the brain and its links to behaviours.Advances in brain-imaging techniques, com-bined with the search for endophenotypes andmore refined genetics, hold the promise thatbiological psychiatry may rapidly regain lostground. As Hughlings Jackson noted (Taylor,1958), there are two ways to classify flowers:as a gardener or as a botanist. At present westill use the techniques of the gardener, but areprogressing towards the position of the botanist.
CLASSIFICATION IN PSYCHIATRY
The two main diagnostic systems in use atpresent are the International Classification ofDiseases (ICD), which derives from the WorldHealth Organization, and the American Psy-chiatric Association’s Diagnostic and StatisticalManual of Mental Disorders, 4th edition TR(text revised). It is important to emphasizethat, although diagnostic fashion changes fre-quently, some of the categories that we usetoday were recognized by many earlier genera-tions, and have a degree of constancy over time.Further, the classifications discussed will them-selves soon be modified in the light of clinical

Classifications and Clinical Investigations 85
experience and the accumulation of knowledge,particularly as more biological correlates of clin-ical syndromes become manifest.
Kraepelin’s textbook of psychiatry wentthrough nine editions, and his views evolvedwith time and experience. Prognosis was anessential feature of his system, and this wasrelated to diagnosis. Dementia praecox andmanic–depressive psychosis were his twomain groupings, involutional melancholiaand paranoia being considered as separateentities. Three forms of dementia praecoxwere described, namely the hebephrenic, thecatatonic and the paranoid. These fundamentalcategories of psychopathology form the frame-work of the system in use today. The ideas ofthe Kraepelinian system were opposed to theunitary psychosis model, and reaffirmed thedisease concept firmly for psychiatry.
One more term should briefly be discussed,namely ‘endogenous’. The meaning of this isunclear though unfortunately it is still in pop-ular use. Aubrey Lewis (1971) pointed out thatthe term ‘endogenous’ is often merely a cloak forignorance. Its introduction was strongly linkedto the 19th century European degeneration the-ory, and Lewis felt its use ‘should be openlylinked to presumptive evidence of a powerfulhereditary factor in causation’ (p. 196).
Karl Jaspers (1883–1969)
Although Jaspers’ Allgemeine Psychopathologiewas first written in 1913 and went through nineeditions, the English translation did not becomeavailable until 1963. Nonetheless, the influenceof his thinking has been widespread, especiallyin Europe. His approach was strongly empirical,despite being rooted in the philosophical schoolof phenomenology. Jaspers developed a methodfor examining the mental state of another per-son, which, in its purest form, attempts todelineate psychic events as sharply as possible.Central to his theme is the distinction betweenthe psychological development of the individual(psychogenic development) and an organic dis-ease process. He also makes a clear distinctionbetween understanding a psychological process(Verstehen) (e.g. why someone is sad following
a loss) and providing a causal neurobiologi-cal explanation (Erklaren) (e.g. a tumour in thefrontal cortex causally explains the features of afrontal lobe syndrome).
Some quotations from his book (Jaspers, 1963)emphasize these issues:
Phenomenology . . . gives a concrete descriptionof the psychic states which patients actuallyexperience and presents them for observation(p. 55).
Form must be kept distinct from content . . .
from the phenomenological point of view it isonly the form that interests us. . . (p. 58).
Jaspers was clearly opposed to those who con-fused form and content, and he emphasizedhow the theories of Freud provided psycho-logical understanding but were not biologi-cally causal. Freud was concerned only withthe content of the mental state and not theunderlying causal neurobiology or endophe-notypes. Jasper’s approach differed from thatof Kraepelin in emphasizing a descriptive psy-chopathology rather than actual diseases. It wascontinued by Kurt Schneider (1887–1967), whofurther developed criteria to distinguish devel-opment from process and introduced what arenow referred to as the first-rank symptoms ofSchneider. From these developments diagnostictools such as the earlier ‘present-state examina-tion’ (PSE) of Wing and colleagues (1974) andthe currently-used Structured Clinical Interviewfor DSM IV (SCID) emerged.
Current Classifications
The classification schemes currently in use inpsychiatry are based almost entirely on symp-toms. Various operational definitions have beenintroduced and are widely employed, the basisof which is the completion of a checklist of symp-toms, signs and historical facts which must besatisfied before a diagnosis is made. ICD 10came into use in 1992, DSM IV in 1994. In thesection that follows, emphasis is given bothto DSM IV and ICD 10. A ‘text revision’ ofthe DSM IV, known as the DSM IV-TR, waspublished in 2000. The diagnostic categories

86 Biological Psychiatry
and the vast majority of the specific criteriafor diagnosis were unchanged, but the textsections giving extra information on each diag-nosis were updated, as were some of the diag-nostic codes, in order to maintain consistencywith the ICD. DSM V has had initial com-ments in 2010. DSM IV-TR adopts a multi-axialclassification, but this is not overemphasized.However, it is in keeping with the distinctiondrawn by Jaspers between personality disorderand psychiatric illness. Axis 1 refers to clinicalsyndromes, axis 2 covers developmental andpersonality disorders, and axes 3, 4 and 5 referto physical disorders, psychosocial stressors andglobal assessment of functioning respectively. Itis not intended that a comprehensive classifica-tion be given here, and attention is given to thedisorders that relate to subsequent chapters.
The newer versions of these ICD and DSMsystems, although perhaps slightly improved,still fundamentally represent committee-derived consensus about classifications ofsymptoms, and continue to fail to make theneeded leap, at some point, into diseasedefinitions based on firm understanding ofpathophysiology. The rest of medicine hasprogressed to disease classifications basedon endophenotypes defined by genetics, orbiomarkers such as imaging data, but ICD andDSM systems are fundamentally symptom-based systems. The updated versions of thesesystems, while perhaps necessary for someissues, are fundamentally incomplete in notmoving into a pathophysiological, endopheno-type approach, as is used in the rest of modernmedicine and neurology (see Chapter 13 for anattempt at a new classification scheme).
An example of this evolution has occurredin the area of multiple sclerosis (MS). Twentyyears ago MS was a disorder diagnosed onpurely clinical grounds, with lesions separatedin time and space. There were a few helpfulconfirmatory tests, but nothing definitive.The ability to give individual prognosis waslimited, and treatments were largely ineffective.Now the disease is almost 100% identifiablewith brain imaging, and other ancillarytests can exclude rare forms. This newfoundability to diagnose based on endophenotype
(imaging) (rather than mere constellation ofsigns and symptoms), coupled with morecomplete knowledge of the pathophysiology,has allowed for much-improved individualdiagnosis, prognosis and treatment monitoringfor those suffering from MS. It is hoped thatthis biological approach will gain favour in thepsychiatric classification schemes of the nearfuture. Currently, the larger symptom-basedapproaches are being progressively modifiedbased on new science information. For example,in DSM IV-TR there is a new section under‘Dementia’ entitled ‘Dementia with LewyBodies’. This incremental change is helpful,and may represent a gradual transformationof symptom-based into more endophenotype-and pathophysiologically-based systems.
Organic Mental Disorders
The muddles with regards to this category inearlier editions of the ICD and DSM have tosome extent been resolved, although much morework needs to be done to clarify this importantarea of psychiatric nosology.
The term ‘organic mental disorders’ of DSMIIIR has been replaced, and, as noted, some ofthese disorders are classified in the diagnosticsection with which they share phenomenology(for example, anxiety disorder due to a generalmedical condition). In this scheme, the underly-ing condition can be specified in axis 3. Delirium,dementia and amnestic and other cognitivedisorders are allocated a separate category. Sub-categories of dementia and amnestic disordersare then given.
There is a further overall category of mentaldisorders due to a general condition that havenot been specified elsewhere. This includes cata-tonia, personality change and mental disordernot otherwise specified, which embraces post-concussional disorder.
ICD 10 has a category labelled ‘organic’,including symptomatic mental disorders. Thisincludes the dementias, delirium and other men-tal and personality disorders due to brain dam-age and dysfunction and to physical disease.In the latter category are found the disorderssecondary to a general medical condition in the

Classifications and Clinical Investigations 87
DSM IV. The retention of the term ‘organic’ inICD 10 seems unfortunate, as it leads to a seman-tic muddle over the biological basis of othermental disorders, and the decision of DSM IV todrop this seems logical.
More concerning, perhaps, is the DSMapproach of requiring a separate designationof an axis 1 (psychiatric condition), a commenton axis 2, and then a separate listing of medicalconditions (axis 3). This Cartesian splitting ofthe psychiatric from the somatic forces an artifi-cial separation of what is the reality. Brain andbody are interconnected, as are brain and mind.Having a classification system that separatesthese realms runs the risk of perpetuating anunderinformed, incomplete and impoverishedview of diseases that affect the brain.
CLINICAL INVESTIGATION
It is not intended in this chapter to outlinethe basic or essential features of the neu-ropsychiatric examination, nor to discuss thevarious methods that are available for thequantification and documentation of the mentalstate. Accounts of these are given elsewhere(Cummings and Trimble, 2002; Roberts, 1984;Trimble, 1981a). Here some of the moreimportant clinical investigation techniques arepresented, including biochemical markers, EEGand brain-imaging techniques.
The importance of careful history-taking inthe evaluation of patients cannot be overem-phasized in psychiatry, as in other branches ofmedicine. This should, where possible, extend tothird-party accounts of the patient’s behaviour,and in particular must concentrate on change ofbehaviour. An understanding of the more regu-lar patterns of the patient’s activities is derivedfrom information about their past, including anyprevious change in behaviour that led to psychi-atric referral. Genetic diatheses must be soughtby careful questioning. The essence, however, isthe delineation of change; the identification ofthe point in time at which a process intervened.Personality – its style and development – has tobe dissociated from process. The manifestationsof the latter are then analysed for their form, not-ing the problems that occur if form and content
are confused. Diagnosis proceeds through docu-mentation of psychopathology, the combinationof signs and symptoms, and the application ofsome recognized nomenclature. As in medicinegenerally, the essential point of the initial patientevaluation in psychiatry is to draw up a differ-ential diagnosis so that a plan of investigationand treatment can be initiated.
In the clinical setting, the initial diagnosticprocess should be accompanied by a search foraetiology and if possible an understanding ofpathogenesis. As noted, many of the conditionsthat once formed a significant part of psychi-atric practice now have a clarified disease base,often associated with structural brain change.However, the fact that the signs and symptomsof psychiatric illness are reflections only of dis-turbed brain function, and alteration of functionarises either from intrinsic alteration of func-tion (functional disorder) or as a consequence ofstructural change (structural disorder), requiresus to examine the CNS in our patients.
Since psychiatry is a branch of medicine, itis reasonable to offer to psychiatric patients thesame facilities for medical investigation as theywould expect from other specialists. In partic-ular, their clinical evaluation should always beaccompanied by appropriate laboratory tests,many of which are routine. Thus all patientsshould have assessment of their basic haema-tology profile, an ESR measurement and certainbiochemical tests. The latter include urea andelectrolytes, liver function tests, calcium, phos-phate and thyroid function tests (T3, T4, TSH).The liver function tests are important since alco-hol intake is usually underestimated and under-revealed and may be significant in the patient’spathology. If alcoholism is suspected, estima-tion of red-cell transketolase activity may be ofvalue, as well as gamma glutamyl transpepti-dase (GGT) or carbohydrate-deficient transfer-rin (CDT). In many situations it may still bewise to test the patient’s syphilis serology. Thisis usually tested with a Treponemal enzymeimmunoabsorbant assay (EIA) combined with aTreponema pallidum haemaggultination assay(TPHA). The flourescent Treponemal antibodyabsorption (FTA-ABS) may be used as a confir-matory test. Depending on the clinical question,

88 Biological Psychiatry
and local policy, testing for human immunodefi-ciency virus (HIV) is often carried out. If the ini-tial antibody test or tests are positive, one shouldalso assess for the viral load and CD4 count.
Routine skull and chest X-rays are not nowrecommended unless there is a suspicion thatthey may be revealing (for example, whenthere are concerns about tuberculosis or occulttumours). Measurement of vitamin B12 and folicacid status, thyroid function studies and bloodglucose are often indicated, and in cases of‘funny turns’ an extended glucose tolerance testis often done. On occasion, rarer investigationswill be indicated, such as measurement ofplasma and urine osmolality, tests for LE cellsand antinuclear factors, C-reactive protein,further endocrine evaluation, and tests for infec-tious mononucleosis or other disorders suchas brucellosis. In a patient with chronic fatiguesyndrome, Lyme disease serology should beexamined. In patients with movement disordersand psychopathology, copper and caeruloplas-min and acanthocyte screening will help ruleout Wilson’s disease and neuroacanthocytosis.In patients with suspected autoimmune orvasculitis problems, one should order a testfor an anti-nuclear antigen (ANA) or anti-neutrophil cytoplasmic antigen (ANCA) (bothfor vasculitis), or anti-voltage gated potassiumchannel antibodies or anti-neuronal antibodies(both associated with limbic encephalitis as partof a primary autoimmune or paraneoplasticsyndrome).
Urine investigations include screening fordrugs if any state of intoxication is suspected,ruling out infections (especially in the con-fused elderly) and rarely testing for urinarycatecholamines in suspected phaeochromocy-toma or searching for metachromatic materialin suspected cases of metachromatic leucodys-trophy. Testing for porphyrins when porphyriais suspected still occasionally yields reward-ing results.
Serum-level monitoring of certain drugs hasnow become routine, especially for lithium andanticonvulsants. Antidepressant monitoringcan be of value, especially if a patient isresponding poorly to good oral doses of
the drug. Low levels may indicate a rapidmetabolism or poor compliance. In addition,measurement when there is a complaint oftoxic side effects on small doses may allowthe physician to determine if this is related tounexpectedly high levels, especially helpful inthe elderly, who often show reduced clearanceof drugs. Serum alcohol or barbiturate levelsare helpful in cases of suspected dependence.
One neuropeptide that is useful to assess isprolactin. This is elevated by drugs that blockdopamine receptors and thus may be helpfulin detecting compliance in patients on someneuroleptic drugs. Although there is toleranceto the initial higher levels of prolactin overfour weeks of treatment, a period of stabilityis reached which lasts for months thereafter(Brown and Laughren, 1981). Prolactin levelstend to be elevated in patients on intramusculartherapy (Chalmers and Bennie, 1978), andwhile not correlating with the serum levelsof the neuroleptics, may be a predictor of thedopamine blockade at the hypothalamopitu-itary axis. Patients who develop extrapyramidalside effects to these drugs tend to have higherprolactin levels (Kolakowska et al., 1979), andhyperprolactinaemia is often associated withsexual disorders, especially in men (Schwartzet al., 1982). Serum prolactin estimations willoften help differentiate epileptic from non-epileptic seizures and thus may be useful inthe investigation of intermittent behaviouraldisorders. Although there are some exceptions(frontal lobe seizures, simple partial seizures),a significantly raised prolaction 15–20 min-utes after the episode, in the presence ofnormal baseline prolactin, may be confirma-tory of an epileptic event (Dana-Haeri andTrimble, 1984).
The dexamethasone suppression test (DST)has a rather specific application to psychiatry.The details of this and some other neuroen-docrine tests are reviewed in Chapter 8.
Finally, lumbar puncture is of value inpsychiatric practice. Thus, in cases of suspectedcerebral syphilis, serological investigation isrequired, and in some cases of undiagnoseddementia the presence of, for example, an

Classifications and Clinical Investigations 89
oligoclonal immunoglobulin pattern may leadto a diagnosis of multiple sclerosis. Morerecently, CSF measures of amyloid-beta proteinand tau protein can be helpful in early diagnosisof Alzheimer’s disease.
Biochemical Investigations
In recent years the ability to measure sub-stances of biological importance in body fluids –plasma, saliva, CSF and urine – has increasedconsiderably. Further, the detection of smallquantities with reliable, quick and relativelyinexpensive techniques has been important inexpanding the use of biological tests in psychia-try. Gas chromatography and high-performanceliquid chromatography (HPLC) use the sep-aration of compounds on columns and theiranalysis by sensitive detectors. In the former, thesubstance to be measured is carried in a gaseousphase into a column in which the separationtakes place. Detectors at the end of the columnmeasure and quantify the compounds. A partic-ularly powerful detection method is mass spec-troscopy. In this technique the substance to bemeasured is ionized electrically or chemically,and the application of magnetic and electricalforces separates the fragments in relation totheir mass and electrical charge. In HPLC thecontents of the separation column are forced inunder high pressure, and their subsequent den-sity allows excellent separation of compoundswhen the sample is injected rapidly throughthem. Unlike gas chromatography, there is noneed to create gaseous derivatives. When com-bined with mass spectroscopy, HPLC is capableof quantifying picomolar concentrations.
Radioimmunoassay (RIA) has also beenimportant. Here a biologically radiolabelledcompound is combined with a very specificimmunoglobulin molecule – the complex –which is then quantified by competitive bindingto antibody. After an incubation period, whenthe binding of the labelled and unlabelledsubstances have equilibrated, the bound andthe unbound portions are separated. As the con-centration of the unlabelled portion increases,the amount of bound radioactivity decreases
and the appropriate quantitative calculationscan be made from standardized curves.
EMIT assay, fluorescent polarization immu-noassay and OPUS immunoassay are morenewly developed highly specific immunoas-says, which can be quickly performed on asmall amount (< 50 m l−1) of plasma or serum.
Many RIAs are available in kit form and arewidely used in the assessment of neurohor-mones. There are many difficulties, however,with RIA, not the least being the specificity ofthe antibodies, and often there are discrepanciesbetween the results obtained with biologicalassays (bioassay: the direct measurement ofchanges in isolated tissue responsive to thesubstance, for example a hormone) and theresults of RIA.
Another technique is the radioreceptorassay, in which binding to a specially preparedsuspension of receptors is calculated. Again, thebiologically active compound competes withknown radioactively labelled ligands for thereceptor, and the bound portion is assessed andcompared to a standard. This technique hasbeen especially helpful in the measurement ofserum drug levels.
The newest category of biochemical testinginvolves measuring specific genes. This can bedone either to test for a specific disease underquestion (e.g. Huntingtin Gene, HTT, in Hunt-ington’s disease), as a risk factor, or to determinepharmacological response (called genomicpharmacology). In the field of oncology, forexample, patients are routinely assayed for theBRAC1 gene, the results of which determine eachpatient’s prognosis and dictate the invasivenessof the treatment course. For diseases where thegenetics are well known, and with appropriatecounselling and physician overview, this testingcan help refine diagnosis and treatment. Aparticularly concerning area however involvesdirect-to-consumer (DTC) genetic testing thatpatients can order over the Internet. This areais ripe with fraud, with very little governmentoversight or regulation. Even when the tests arelegitimate, without proper interpretation by aphysician they often increase patient anxiety,and actually interfere with medical care.

90 Biological Psychiatry
EEG
The EEG signal
The signal finally reflected on the EEG trace rep-resents only an average of the electrical eventsgenerated by the dendrites of neurones in thesuperficial cortical layers. It thus represents thegraded sum of the excitatory and inhibitorypotentials from many thousands of neuroneslying under the recording electrode. Theoret-ically, if the cells are firing at random, thepotentials should average out. The fact that thereis a recordable rhythm implies that synchroniza-tion has occurred, suggesting the existence ofsome pacemaker. The thalamus is one structurefrom which EEG generators derive, although thegenesis of the synchrony required for the spikeof an epileptic focus is likely to be different fromthat leading to the generation of the normalalpha rhythm. The existence of multiple originsfor synchrony may be postulated, and similarwaveforms may not necessarily be derived bythe same mechanism.
EEG Traces
In the laboratory the patient has electrodesattached to the scalp, and usually 8 or 16 chan-nels are recorded. These are referred to by a stan-dardized notation known as the International10–20 system. It should be noted that an aver-age electrode spacing is some 5–6 cm, and, sincemuch cortex is buried in the sulci of the brain oris too medial to influence the surface EEG, in atypical examination only some 20% of the cor-tex is sampled, usually for only a small periodof time. Better recordings from such structuresas the medial temporal lobes can be obtainedby using special electrode placement such asnasopharyngeal or sphenoidal leads. The for-mer requires electrodes to be placed throughthe nares to rest in the nasopharynx under thebase of the skull. With sphenoidal electrodes,the tip is placed in the region of the fora-men ovale. Activation procedures for enhancingnormal and abnormal features of the EEG areusually employed and include hyperventilation,photic stimulation, sleep inducement or sleep
deprivation, and the administration of epilepto-genic agents such as pentylenetetrazol.
Interpretation of the recordings involvesrecognition not only of the type of waveformbut also of its voltage, frequency and polarity.The EEG is, in general, composed of relativelyhigh-voltage slow waves of up to 20 hertz (Hz,or cycles per second), and traditionally severaldifferent rhythms are recognized. The alpharhythm has an 8–13 Hz frequency, and tendsto appear in the relaxed-but-awake state. It ismost prominent occipitally, and is attenuatedor blocked by eye opening. Theta rhythm is4–7 Hz, and delta is below 4 Hz. Rhythms fasterthan 13 Hz are beta, and are more prominentfrontally. Many psychotropic agents such asbarbiturates or benzodiazepines increase beta.The mu rhythm is a central rhythm of the samefrequency as alpha which does not block witheye opening but does with movement.
Age is an important determinant of the nor-mal EEG, especially in early years. At birththeta and delta rhythms dominate, increasingin frequency with maturation, alpha becom-ing established around the age of 13. The fulladult pattern is not reached until the mid-twenties. Paroxysmal activity, including focalspikes or sharp waves, may be seen in nearly3% of normal children, increasing to nearly 10%if provocative techniques or sleep studies aredone (Eeg-Olofsson et al., 1971). Frontal andin particular posterior temporal theta activityis not infrequently recorded in younger peo-ple, and its presence is thought to reflect brainimmaturity. Its detection should not be inter-preted as evidence of epilepsy in patients having‘funny turns’.
An individual’s EEG is characteristic, andstudies of twins reveal important geneticdeterminants (Hill, 1950). The correlation withintelligence is poor. Level of awareness iscrucial to the EEG wave pattern, and markedchanges occur with the onset of sleep. Thus,in the drowsy state, alpha waves tend to comeand go, and as sleep supervenes, the rhythmsslow. Deeper sleep is characterized by deltaactivity, while in paradoxical sleep (REM) thereis fast desynchronized activity. During theorthodox, slow-wave stage, a number of other

Classifications and Clinical Investigations 91
EEG events may be observed. Sleep spindlesare bursts of low-voltage 13–15 Hz activity,and K-complexes – delta waves associated withspindles – may be seen. During a night’s sleep,REM activity occurs in four to six periods of upto 30 minutes approximately 90 minutes apart.Typically, the first REM period starts afterabout 90 minutes, and the total REM time forthe average adult is 20–25% of total sleep time.
Evoked Potentials
The electrical events generated by the brain fol-lowing a simple stimulus are small, and in thesea of background activity will not be detected.By the technique of averaging the results ofmany similar stimuli, the signal-to-noise ratio isenhanced and the so-called evoked potentialrecorded. Thus, visual, auditory or somato-sensory stimuli are repetitively presented, andafter each event the electrical activity of the brainis recorded. The averaged evoked potential isderived from computer analysis of the data andis a series of waveforms of negative and positivevoltage. The actual form of the event-relatedpotential varies with the sensory stimulus, itsmodality and the cognitive processes involvedin its perception. The first waves represent thearrival of the signals by the specific sensorypathways, the later waveforms reflecting activa-tion over slower, polysynaptic paths. The formerseem independent of the psychological state ofthe individual, while the latter vary with thestate of the subject and the meaning and rele-vance of the stimulus. The latency and ampli-tude of the early response seem related to thestrength of the stimulus, such that amplitudesincrease and latencies decrease with increasingstimulus intensity. This, however, is not invari-able, and in some subjects increased intensityleads to smaller responses (Shagass, 1972). Thepresentation of a stimulus and the evocation ofa response alter a subsequent evoked responsefor a short period of time. It has been suggestedthat alteration in the recovery of this changemay relate to psychopathology (Shagass, 1972).Changes in the waveforms of evoked poten-tials are widely used in the diagnosis of variousdiseases, an obvious example being multiple
sclerosis. Other, more specific tests have largelysuperseded the routine use of evoked potentialsin clinical, as opposed to research, biologicalpsychiatry.
In addition to the shorter ‘exogenous’ latencyresponses, a number of the ‘endogenous’ event-related slow potentials have been described.These include the P300 wave, the contingentnegative variation (CNV) and motor poten-tials such as the Bereitschaftspotential. The P300wave refers to a positive response componentseen some 300–500 ms after the stimulus, said torelate to a process of cognitive appraisal of thestimulus. It has a centroparietal distribution forall sensory modalities, and its latency increaseswith diminishing discrimination of presentedstimuli. It has been suggested that it may berelated to the laying down of memory traces(Karis et al., 1984).
The CNV is derived by giving a subject a stim-ulus, followed some brief time later by anotherwhich requires some response. The first servesas a warning stimulus in expectancy of the sec-ond (‘expectancy wave’ is an alternative name).The wave consists of a slow negative shift inpotential, especially in the vertex and frontalregions. Originally described by Walter and col-leagues in 1964, it relates to such psychologicalprocesses as motivation, attention and height-ened attention (see Figure 4.1). It is increasedby such factors as certainty that the stimuluswill occur and interest in the stimulus. It isdiminished by distraction and boredom, andits character may be altered in psychopathol-ogy. The CNV should not be confused with the‘readiness potential’ or Bereitschaftspotential,which is a similar slow negative potential thatarises about one second before voluntary move-ment. It is maximal in the precentral parietalregion, and may be broken down into a numberof separate components (Shibasaki et al., 1980).
Some Other Techniques
In recent years other sophisticated variations ofEEG recording have come into use, includingprolonged monitoring and computerized anal-ysis leading to continuous mapping of brainelectrical activity.

92 Biological Psychiatry
(a)
(b)
(c)
(d)
Click
Flashes
Flashes
Flashes terminated by button
Calibration
18µV1s
Click
Click
Figure 4.1 Contingent negative variation (CNV). Averages of responses to twelve presentations: (a) responsein frontovertical region to clicks; (b) flicker; (c) clicks followed by flicker; (d) clicks followed by flickerterminated by the subject pressing a button as instructed. The CNV appears following the conditionalresponse and submerges the negative component of the imperative response (reproduced with permissionfrom Walter et al., 1964)

Classifications and Clinical Investigations 93
There are two main forms of prolonged mon-itoring, namely videotelemetry and ambulatorymonitoring. In the former the patient is filmed bya video camera, usually in a specially designedlaboratory or ward, and the EEG is recordedsimultaneously. Both the picture and the EEGtrace are sent to an adjoining room where theyare displayed on a split screen to be viewedtogether. The EEG and the patient’s behaviourcan thus be correlated.
With ambulatory monitoring, the EEG isrecorded for a prolonged period of time usinga portable cassette recorder strapped to thepatient’s body. The technique requires the useof special head-mounted amplifiers that dimin-ish muscle and other artefacts. Although withthis method there is no accompanying visualimage of the patient, the apparatus can be wornat home or in the school without interference todaily activities.
A disadvantage of both these investigationsis the limited number of channels that can berecorded and the interference that still occurson the record at crucial times, such as duringa seizure.
The use of computerized EEG methodsallows profiles of the average amount of activityin various wavebands over time to be derived.The EEG record can be broken down intofrequency components which are quantifiedusing electronic filters and integrators, and elec-trical power determined according to selectedfrequency bands by using the mathematicaltechnique of Fourier analysis. This has beenparticularly useful in psychopharmacology,noting for example the influence of differentclasses of drugs on these measurements.
Brain electrical activity mapping (BEAM) is atopographic mapping technique that condensesinformation from the EEG or evoked potentialand presents it as a coloured map. Data are bro-ken down into a matrix of some 4000 elementsand a map is coded depending on the amountof electrical activity at each point. The resultingimage can be an average of a series of imagesfrom a group of patients, and these data canbe compared with those collected from another
group. Areas of statistical differences betweengroups can be displayed as coloured maps, atechnique known as statistical probability map-ping (SPM).
One of the limitations of EEG is that it isunclear which brain regions are contributingto the recordings on the scalp. LORETA (low-resolution electromagnetic tomography) is oneof several recent attempts to solve the inverseproblem (i.e. where within the brain are thedipoles that drive the surface EEG?) and ‘map’the surface EEG changes onto deeper brainstructures.
There is an exciting new application ofquantitative EEG over the prefrontal cortex asa potential early biomarker of antidepressantresponse. This method examines hemisphericdifferences in prefrontal coherence and activity(Bares et al., 2007; Cook et al., 2005; Hunter et al.,2006; Kopecek et al., 2007). One commercialcompany (Aspect Medical) has applied for FDAapproval to market this clinically.
Magnetoencephalography (MEG), whichmeasures extra-cranial magnetic fields derivedfrom the brain’s electrical potentials, hasbeen introduced. The magnetic fields are notinfluenced by the scalp as EEG potentials are,and are more localized. It is thus possible usingMEG to provide information from deeper cor-tical structures, which is at present impossiblewith the EEG without using depth electrodes.MEG has high spatial resolution and, sinceit detects tangential dipoles, can ‘look’ into asulcus. This, combined with coregistration ofMRI images, may provide a powerful techniquefor determination of structure–function brainrelationships. MEG has not fully penetrated intoroutine neurological or psychiatric practice asit requires an expensive magnetically shieldedroom, while EEG can be performed in a routinesetting. As with EEG, it is hard to determineexactly which regions in the brain under anelectrode causes the signal on the surface of thebrain. Some researchers are therefore combiningMEG, with its high temporal resolution, withMRI or PET to determine the brain source of theMEG surface signal.

94 Biological Psychiatry
Brain-imaging Techniques
Computerized Axial Tomography(CAT or CT) Scans
Both angiography and pneumoencephalogra-phy, widely used prior to the introduction ofthe CT scan, provided only indirect informa-tion and did not show brain tissue directly. Incontrast, the CT scan provides a computerizedreconstruction of the brain image and around1985 began transforming our ability to noninva-sively visualize the brain prior to autopsy.
A typical CT scanner is composed of anX-ray source, a detector, a computer for imageconstruction and an image display system.A fine beam of X-rays is generated and projectedthrough the patient’s head. The apparatus thenrotates through one or more degrees andanother projection is made. The process isrepeated until all points in a plane, around180◦, have been probed from many directions.During the passages of the X-ray photonsthrough the tissues of the head they will interactwith intrinsic electrons and be either scatteredor captured. In either case they will not reachthe detector on the opposite side of the head.The more important event is scattering, whichis dependent on tissue density. The final imagerepresents a matrix display, a kind of gridmap composed of many adjacent squares. Eachsquare represents the average density of thetissue in the area of the square and a volume oftissue lying underneath it. The small square asseen is called a pixel, and the volume of tissueit represents is the voxel.
It is obvious that if the voxel is composedof all the same tissue then the density reflectedin the pixel will faithfully reflect the quality ofthe represented area. However, if within thevoxel there are, in addition to the soft tissueelements, bone, fluid or air, the average readingwill be altered, which may lead to a misinter-pretation of the presence of pathology in thattissue. This is known as the partial volumeeffect, and is an important source of error inCT data. The depth of the voxel varies withdifferent machines from 2 to 13 mm. The usualmatrix is made up of a 160 × 160 or 320 × 320
matrix. Although the original scanners usedsingle beams, later models use multiple colli-mated beams and detectors and allow recon-struction of the X-ray data to produce sagittaland coronal, as well as axial, views. Even morecommon now are ‘rapid’ CT scanners with spi-ral techniques that make image acquisition moreefficient, reducing both the time of the scan andthe total radiation needed.
The units of density on one of the scales usedare referred to as Hounsfield units, named aftera pioneer of the CT technique. On this scale zerois the representative of water, air being +2500and brain tissue in the region of +15 to +18.An alternative is the EMI unit, which is half thevalue of the Hounsfield unit. Some machinesallow for direct assessment of densities in theselected region of interest (ROI).
The scan can be contrasted by using an iod-inated contrast medium, which, on account ofits efficient electron capture, deletes X-rays andincreases tissue radiodensity.
A grey scale, ranging from white to black,allows the ultimate visual display, and the scaleis set to allow maximum visualization of tissuesof interest. This procedure relates to windowwidth and level. The latter refers to setting thescale so that it is centred on the attenuation(X-ray absorption) value of most relevance, andthe width refers to the range of other tissue atten-uations to be included in the grey scale. Thus, ifthe window width is set at 20 and it is equallyweighted to either side of the level then 10 unitsabove and the same below will be included inthe grey scale. Values outside of this range willappear either as all white or as all black.
The advent of CT scans in 1985 dramati-cally altered neurological practice and had amajor indirect impact on psychiatry. However,because CT involves radiation, and is less sen-sitive than MRI for many clinical questions,it is now largely restricted to trauma unitsand trauma evaluations. CT scans are useful inimaging the two ‘B’s – bone and blood – wherethey are not supposed to be. Thus emergencyroom physicians use CT scans after road trafficaccidents or other trauma to investigate skullfractures, subdural hematomas or haemorhagicstrokes. Some newer units combine CT scans

Classifications and Clinical Investigations 95
with PET cameras; these are increasingly usedin cancer diagnosis and monitoring.
Magnetic Resonance Imaging (MRI) Scans
The elegant demonstration of the brain’s struc-ture by the CT scan has been superseded by MRI.While more expensive, MRI is a more pow-erful and diverse technology and has largelyreplaced conventional CT technology except insome clinical situations following trauma.
Although the technique, also referred to asnuclear magnetic resonance (NMR), has beenused in spectroscopy for some time, the for-mation of images derives from the work ofLauterbur (1973), who used the term ‘zeug-matography’. The principle involves the exam-ination of the physicochemical environment ofproton nuclei in tissue based on the inherentelectromagnetic forces that exist in such electri-cally charged particles.
Briefly, any object that has charge and veloc-ity produces a magnetic field perpendicular toit. A charged nuclear particle spinning in thebody’s tissues thus produces a magnetic field,although in this case the field is referred to asthe angular magnetic moment, with a vectorperpendicular to the axis of rotation. A chargednuclear particle, spinning about its axis, acts likea tiny bar magnet; before the application of anexternal magnetic field, the sum total magne-tization of many of these spinning in humantissues is zero, since their direction of move-ment is random. On application of an externalmagnetic force the tiny magnets are aligned, justas an ordinary compass needle will align in theEarth’s magnetic field. The alignment is parallel(or antiparallel) to the external field. The protonsin such a setting actually spin, like a spinningtop, around the alignment of the applied field, aprocess referred to as precession. Protons, whichpossess their own inherent specific precession,once aligned can be excited by the momentaryapplication of a radio signal broadcast at theirown specific frequency (the Larmour frequency)from a radiofrequency transmitter. This processmay be likened to a tuning fork: if we havesix guitar strings tuned to different frequenciesand a tuning fork for one of those frequencies is
struck nearby, only that string will resonate; ifwe have a series of guitars, all the strings of thatfrequency will respond. So it is with protons inhuman tissue. If now the tuning fork is silenced,the guitars will continue to give off a sound,and this can be picked up by a receiver andmeasured (see Figure 4.2).
The procedure of imaging makes use of thefact that waves emitted from the nuclei differin both frequency and amplitude, the formerlocating the position of the particular nucleus inthe body and the latter reflecting the number ofnuclei present at that position. Thus, within thestatic externally applied magnetic field, energyis imparted to the parallel protons, excitingthem to a higher energy level by radiofre-quency waves of exactly the right frequency,and after the signal is finished, electromagneticenergy of the same frequency will be given off,detected by a receiver coil. After the applicationof the radiofrequency pulse, the magnetizationreturns exponentially to its pre-excitement level,a process referred to as relaxation. This may bedefined by two time constants, referred to as T1and T2, where T1 is always greater than T2.
The T1, or spin-lattice, relaxation time, repre-senting relaxation along the longitudinal axis, isthe time taken for the protons to recover theirpreviously aligned position in the static fieldafter excitation in this axis by a 180◦ pulse. Inpractice, due to the configuration of most scan-ners, a so-called inversion recovery image isused to give a T1-weighted image.
The T2 relaxation time, representing relax-ation in the transverse plane (hence transverserelaxation time), is the exponential time con-stant which results from decay of coherence,due to the interaction of the spinning nuclei.It relates to energy exchange between protons,and is also referred to as the spin–spin relax-ation time. T2 is thus a measure of the lengthof time for which the tissue maintains its tem-porary transverse magnetization, perpendicularto the external magnetic field, following a 90◦
pulse. The spin echo is proportional to the pro-ton density and T2, and is frequently used forT2 measurement.
Thus, each tissue has a specific T1 and T2value, essentially reflecting the physicochemical

96 Biological Psychiatry
C C
C C
(a)
(b)
Aligned
hello
hello
Excited
Emission
NS
NS
NS
Figure 4.2 (a) The principle of resonance. If a tuning fork is struck, an adjacent one of the same tone willvibrate and emit sound (upper). This will persist after the first tuning fork is removed (lower). (b) Principlesof MRI (Biol Psych, 2 Ed, p. 127)
environment of the proton nuclei, especially thewater density of the tissue. T1 relates to the inter-actions of protons with surrounding nuclei; T2depends on interactions of protons with eachother. In the brain, the proton behaviour mea-sured relates to the hydrogen nucleus, mostcommonly of CNS water. Thus the spinningatomic nucleus will behave like a spinning toponly if it has an odd atomic mass or number, anatom with an even number being nonmagnetic.While NMR spectroscopy can image 1H, 13C,
15N, 19F, 23Na and 31P, most clinical and researchimaging at present is largely confined to hydro-gen nuclei.
In practice, the requirements for clinicalbrain imaging are a large superconducting boremagnet, a radiofrequency transmitter coil thatmay also act as a receiver, a computer and adisplay system. The actual imaging techniqueinvolves a series of choices for sequencingrelated to the direction and timing of theradiofrequency pulses delivered, the data being

Classifications and Clinical Investigations 97
spatially encoded to provide information onproton density and T1 and T2 times. The echotime refers to the time taken to generate the echosignal after the initial 90◦ pulse, while the repe-tition time states the pulse signal to be repeated.Since it is an electronic process, reconstructioncan be done in any direction, and is usually sliceencoding. Inversion recovery and spin-echotechniques are the most widely employed. Byexploiting differences between the relaxationtimes of different tissues, heightened contrast
between them is achieved, and hence betterimages. The use of contrast media such asgadolinium DTPA further aids tissue differen-tiation. These cross the blood–brain barrier insmall quantities and alter the relaxation timeof tissues, inversion recovery images beingparticularly sensitive (Figure 4.3).
A static magnet activates all protons, andgradient magnets activate specific cuts. Thederived images have a low spatial resolution, insome machines as low as 0.8 mm square. Most
PD T2
TI MRA
Figure 4.3 Contrasting MRI images. (Provided by Dr Mark George.) Selected images from a healthy brainMRI, all at the same level through the head. Proton density (PD, top left), T1-weighted (T1, bottom left),T2-weighted (T2, top right), and MR angiography (MRA, bottom right) scans have varying image contrast thatreveals specific information about various structures in the brain. The T1 scan is considered the ‘Rembrandt’as it shows high-resolution anatomy in health, and depicts the brain as one would see it at dissection, withthe skull present, grey matter as grey, white matter bright, and CSF dark. In contrast, the T2 scan is usefulto detect pathology, and things are ‘non-obvious’. The skull is sometimes not even imaged, and grey matteris bright, white matter is dark, and the CSF is very bright, almost radioactive. The proton density scanis a hybrid between these two. In the MRA scan, bottom right, blood flowing in arteries or veins is verybright (reproduced with permission from Christopher P. Hess MD, PhD; Purcell, Derk D. BRAIN: CT, MRI:noninvasive imaging of the central nervous system [Internet]. Version 46. Knol. 2008 Aug 6. Available from:http://knol.google.com/k/christopher-p-hess-md-phd/brain-ct-mri/biWBkaDv/wqrGdg)

98 Biological Psychiatry
pathological conditions increase the length of T1
and T2, free water having even higher values.Since on T1 images increasing the time dark-ens the image, and on T2 images it lightens theimage, on T1 images, CSF and pathological areasare relatively darkened, and the opposite is trueon T2 images. Both T1 and T2 are shorter in
white matter than in grey, but the signal frombone is very weak and is not well visualized onimages. This conveys an enormous advantagefor imaging in neuropsychiatry since the bonystructures of the cranial vault, which on CTimaging so often obscure the structures of inter-est, such as the temporal lobes, are not present.
Table 4.1 Advantages and disadvantages of MRI
Advantages Disadvantages
No radiation Noise discomfortMinimal risk1 ClaustrophobicGood grey/white discrimination Limited discrimination between pathologiesLess degradation of image with movement Length of scan timeNo bone artefacts Artefacts from ferromagnetic material (e.g. tooth filling,
air sinuses)Clear structural imagesPotential for functional imagingAbility to visualize several planes
1Only patients with cardiac pacemakers, intracranial magnetic clips or in the first trimester of pregnancy should not be scanned.
Image time-series Kernel Design matrix Statistical parametric map (SPM)
Randomfield theory
Statisticalinference
General linear modelSmoothing
Normalisation
Template
Parameter estimates
Realignment
p <0.05
Figure 4.4 Method of statistical parametric mapping. This schematic depicts the transformations that startwith an imaging data sequence and end with a statistical parametric map (SPM). An SPM can be regardedas an ‘X-ray’ of the significance of regional effects. On the left, voxel-based analyses require the data to be inthe same anatomical space; this is effected by realigning the data. After realignment, the images are subjectto nonlinear warping so that they match a spatial model or template that already conforms to a standardanatomical space. After smoothing, the statistical model is employed to estimate the parameters of a temporalmodel and derive the appropriate univariate test statistic at every voxel. The test statistics (usually t orF-statistics) constitute the SPM. The final stage (right) is to make statistical inferences on the basis of the SPMand Random Field Theory and characterize the responses observed using the fitted responses or parameterestimates (courtesy of Dr Mark George)

Classifications and Clinical Investigations 99
A disadvantage is that calcified lesions are notwell visualized. A summary of the advantagesand disadvantages of MRI is given in Table 4.1.
There is the potential to use quantitativeinformation from the scans, especially actualT1 and T2 measurements for studying structuralchanges, and, with higher-strength magnets, toimage other atoms such as 31P.
It is possible to reconstruct images inthree dimensions (see Figures 4.4 and 4.5).Echo-planar imaging (‘fast MRI’) and the useof low-flip-angle techniques which tip protonsrapidly through very small angles (FLASH,or fast low-angle shots) are leading to imageacquisition in short times compared with olderconventional imaging.
The real expense of an MRI machine is thatit requires a large superconducting magnet tocreate a static magnetic field big enough fora human body. A conventional electromagnetwould require enormous energy, and generatea great deal of heat, to produce the magneticfield. By cooling the entire electromagnet tonear zero degrees kelvin, the electricity isable to flow with less resistance (supercon-duct), requiring much less energy and notcreating heat. However, the scanner must be
Figure 4.5 A diffusion-weighted scan, which is verysensitive to acute changes in water content, andincreasingly used for detection of acute strokes (cour-tesy of Dr Mark George)
‘refrigerated’ with liquid helium or hydrogen.A breakthrough in superconducting materialswould fundamentally reduce the cost of MRIscanners and expand their use. Unfortunately,there is nothing on the short-term materialshorizon that might cause this change in the nextdecade.
MRI has so fundamentally transformedmedicine in general, and neuropsychiatry inparticular, that in 2003 Sir Peter Mansfield andDr Paul Lauterbur were awarded jointly theNobel Prize in Physiology or Medicine (notphysics) for their pioneering work with MRI.There is a dizzying array of MRI methods inuse in psychiatry research and clinical practice,most of which are discussed below, though it iscertain that this list will continue to grow. Thetechniques are artificially divided into thosethat are used to assess structure and those thatindirectly measure brain function.
Structural MRI
As noted above, conventional MRI is used togather structural information about the size andshape of the brain. The T1 scans are anatomicallycorrect (sometimes called the ‘Rembrandts’ ofscanning because they resemble the tissue theyimage). The T2 and other proton-density scansare not anatomically correct but instead con-vey crucial information about subtle changesin water density associated with pathologicalstates. For example, small areas of ischemia ordemyelination are invisible on T1 scans but arevisible on T2 scans. These are referred to as‘white matter hyperintensities’. There is a robustresearch literature on the potential relation-ship between these and new-onset, late-onsetdepression, sometimes referred to as ‘vasculardepression’ (see Chapter 8). Many biologicalpsychiatry researchers have used MRI scans toinvestigate the size or shape (morphology) ofkey brain regions like the amygdala and hip-pocampus. Early research on regional brain sizeor shape required trained researchers to actu-ally manually and somewhat laboriously outlineand sample each region for each subject, a pro-cess resembling the work of medieval monkscopying illuminated manuscripts. More com-monly now scans are manipulated by computers

100 Biological Psychiatry
and boundaries are determined by sophisticatedthresholding algorithms. One of the more popu-lar recent computerized techniques is referred toas voxel-based morphometry or VBM. Briefly, ina given patient, the brightness level of a region,say the right amygdala, might be a constant X.If we were to take this subject, and severalothers, and morph their brains into a commonatlas (a process called stereotactic normaliza-tion), then for example for those subjects witha small right amygdala, their overall brightnesscounts would have to be stretched into a largercommon space and the overall brightness or sig-nal intensity would be diluted. For those witha large right amygdala, their brightness levelwould be crowded into a smaller common spaceregion and their relative brightness would thusincrease. Researchers can thus use VBM to per-form whole brain comparisons of the size of thebrain in one group compared to another, or tocompare a group over time to examine increasesor decreases in regional brain size or shape. ThisVBM method is being used extensively in stud-ies examining plasticity or changes over timewith interventions and treatments. Because itis relatively easy to perform, and does calcu-lations on the entire brain (literally thousandsof comparisons), researchers struggle to makesure that results are not false positives resultingfrom the statistical complexity of the data. Thisproblem of how to correct for multiple statisti-cal comparisons plagues much of MRI imagingresearch (Figure 4.4).
Another new technique, called diffusiontensor imaging (DTI), yields indirect infor-mation about the structure of white-matterfibres and local water diffusion (diffusion-weighted imaging, DWI). Remember that aparticle will move randomly inside a confinedspace (called Brownian motion): the same istrue of water molecules in the brain, but thebrain has hydrophobic compartments andbarriers, most notably myelin. By imagingwater molecules repeatedly as they migrateover time, researchers can examine their localmigrations and then determine whether themovement is purely random or is constrainedand thus directional. Water will tend to movemore freely within a myelin sheath rather thanacross a sheath. Thus diffusion imaging uses
the local migration of water to infer informationabout local neuronal integrity. One of the firstevents following ischemia or trauma is a lossof cell membrane integrity, when water movesmore randomly than in healthy functioningtissue. Thus DWI is now becoming the imagingmodality of choice in assessing acute ischemicstrokes (see Figure 4.5). The membrane integrityof a given portion of brain is called the fractionalanisotropy (FA). Building on this concept ofwater diffusion, one can compute the averagedirection of water movement for a given brainvoxel. Thus each voxel can be given a vectorvalue of the direction and magnitude of waterflow. This vector is called a tensor, hence diffu-sion tensor imaging. This indirectly correlateswith the white-matter fibre tracts in that voxel.Creatively, one can then ‘connect the dots’. Thatis, each voxel has a vector pointing to anothervoxel, and then to another. By mathematicallytracing these vectors one can create images of‘likely’ fibre tracts in the brain. There are how-ever many different mathematical algorithmsfor fibre-tract tracing, and each different rulethen highlights different pathways. It is impor-tant to remember that these are not real fibresbeing imaged, rather they are mathematicalanalogues. Figure 4.6 shows a diffusion tensorimage, where this directional information forthe entire brain is contained in the colours.Red shows water (and fibres) flowing right toleft, blue shows water travelling head to toe,and green denotes vectors pointing anterior toposterior. Reassuringly, the corpus callosum isred, internal capsule blue, and arcuate fasciculusgreen. By planting a ‘seed’ one can obtain theo-retical fibre tracts (shown in Figure 4.6). Whilethese are compelling images, it is important toremember that they are simply mathematicalvectors of aggregate water direction and arenot the actual white-matter fibres. However,they do provide interesting indirect informationabout structural connectivity and directionality.
Functional MRI
Different types of MRI scanning can also beused to assess the function of the brain, not justits size, shape and structure. There are currentlythree main approaches: those that assess generalblood flow or perfusion, those that examine

Classifications and Clinical Investigations 101
Figure 4.6 Structural MRI scan shown in 3D, with diffusion information superimposed and DTI tractsarising from brainstem. To generate the DTI tracts, ‘seeds’ were placed in the brainstem with a computermodel (courtesy of Dr Mark George). A coloured version of this figure can be found on the colour plate
subtle changes in tissue haemoglobin use duringperformance of a task, and finally the classicaluse of MRI as MR spectroscopy, where one candirectly measure chemical composition.
One MR technique for measuring large-scaleblood flow is called MR angiography, whereblood molecules are magnetically tagged, andthen reimaged as they flow through large vessels(arteries and arterioles). In biological psychiatryMR angiography can be used to image a vas-culitis, arteriovenous malformation or infectionwhere there is a change in vessel integrity (suchas herpes simplex encephalitis). For actualcalculation of regional blood flow, investigatorsinitially used bolus injections of contrast agentsand measured their flow through large vessels.More recently physicists have devised methodsof magnetically labelling blood and then mea-suring the speed and quantity of its flow intoother brain regions, a technique called arterial
spin-labelling or ASL. Large-vessel blood flowchanges as a function of heart rate and canbe modified by certain drugs, such as cocaine.ASL or perfusion is not sensitive enough toreflect subtle changes in regional brain activityassociated with higher cognitive processes,however.
By far the most common MRI research tech-nique (in terms of publications) is examiningchanges in tissue haemoglobin concentrationbefore and then during various activities.Briefly, the brain uses oxygen, which is carriedby haemoglobin (oxyhaemoglobin). After theoxygen leaves the haemoglobin, the deoxy-haemoglobin has a different magnetic signal.When a brain region becomes active it ini-tially becomes anaerobic and sends chemicalsignals that cause a fairly rapid compensa-tion response, and the full region is floodedwith oxyhaemoglobin to replenish it. This

102 Biological Psychiatry
compensation takes about 3–6 seconds (calledthe haemodynamic response) and is not spa-tially precise. As Malonek and Grinvald (1996)wrote, ‘the entire garden row is flooded forwant of one thirsty rose’. Serially measuring theoxy/deoxy haemoglobin ratio is referred to asblood oxygenation level-dependent functionalMRI, or BOLD fMRI. This technique hasallowed an explosion of research concerningwhat regions are ‘activated’ or ‘deactivated’during various mental states. However, it isstill not clear how local brain activity relates tothe BOLD signal. That is, a brain region thatis working very hard to inhibit or gate anotherregion would have increased BOLD signal andwould be an ‘activation’ even though its activity
VBM DBM TBM
CorticalMapping
ShapeModeling
CINGSRSIRS
Parcellation
is to inhibit other brain regions. Importantly,the change in BOLD signal with a task is onlyabout 3% of the background signal, so it is nota large effect. Thus, researchers will typicallyhave a subject perform a task, then rest, andthen repeat the task and rest numerous timesover a typical 10 minute scan. The images arethen digitally manipulated through a series ofsteps in order to generate the final statisticalmap of the regions that have changes inactivity correlating with the behaviour. Thesesteps involve correcting for small movementthat might have occurred in the scanner,lining up all the images and then morphingor spatially normalizing the scans into acommon brain atlas. There are several common

Classifications and Clinical Investigations 103
statistical software packages that researchersuse: statistical parametric mapping (SPM),FMRIB Software Library (FSL) and Analysisof Functional Neuroimages (AFNI). BOLDMRI scans are then spatially smoothed andstatistical tests are performed comparing brainactivity during a task with the control or restcondition. Essentially the raw images undergo aseries of statistical procedures which first of allstereotactically reorganize the brain image intostandard stereotactic space; the resultant imagehas noise variance smoothed, and analysis ofcovariance is used to remove the contribution ofunderlying global activity. The SPMs are thencreated by statistical analysis, using t maps,comparing repeated measurements betweengroups of images on a pixel by pixel basis(see Figure 4.7) (Friston et al., 1991, 1996).
Typically the areas that are statistically sig-nificantly different during the task comparedto the control condition are displayed in colourand then on top of a grey-scale structural MRI.It is important to realize that the size of theactivation is totally a function of where one
draws the statistical threshold, which is notat all consistent in the literature. Some othernotes of caution are needed in order to makesense of this ‘blobology’ literature, where it iseasy to be enthralled by a coloured ‘blob’ inthe brain. Is the merged and displayed imagetrue to all of the data, or have the investigatorsconveniently masked out activations in otherregions? This post-hoc masking and selectivepresentation of results is deceptive, borderingon dishonesty. An alternative way to analysethese data is to perform a correlation analysis,seeking evidence of a distributed brain systemwith high covariance.
In the early days of BOLD fMRI, the signalswere weak, with smaller magnets. One couldonly find statistically significant task activationsby pooling data from multiple subjects whowere all doing the same task and control con-dition. These were thus group statements, andone could not use them for individual diagnosisor prognosis. More recently, with higher fieldstrengths and multiple receiver coils combinedinto one unit (multichannel head coils), it has
Figure 4.7 (a) The concept of inter- and intra-subject averaging, following spatial normalization. All scans arefirst fitted into a standard space, and subsequent comparison of pixel values is based upon standard parametricstatistical techniques. Areas of significant difference between groups are illustrated as statistical maps in threeformats. These are (left to right): T-maps, orthogonal projections showing areas of significant difference orsurface renderings onto a standard brain template (reproduced with permission from Dr K. Friston, WellcomeDepartment of Cognitive Neurology, Queen Square). (b) Six major types of analysis of structural images,showing some of the main types of data used in each case. Voxel-based morphometry (VBM; top-left panels)compares anatomy voxel by voxel to find voxels (shown here in blue) where the tissue classification (grey,white matter, CSF) depends on diagnosis or other factors. Results are typically plotted in stereotaxic space(lower panel), and their significance is assessed using random field or permutation methods. Deformation-based morphometry (DBM) can be used to analyse shape differences in the cortex or brain asymmetries(coloured sulci; red colours show regions of greatest asymmetry). Tensor-based morphometry (TBM) uses3D warping fields with millions of degrees of freedom (top) to recover and study local shape differences inanatomy across subjects or over time (red colours indicate growth rates in the corpus callosum of a youngchild). Other methods focus on structures such as the cerebral cortex, which can be flattened to assist theanalysis (bottom left), or the lateral ventricles (shape modelling). If anatomic structures are represented asparametric surface meshes, their shapes can be compared, their variability can be visualized and they canbe used to show where grey matter is lost (e.g. in Alzheimer’s disease; bottom-left panel, red colours denotegreatest grey-matter loss in the limbic and entorhinal areas). Fine-scale anatomical parcellation (lower right)can be used to compare structure volumes across groups, or to create hand-labelled templates that can beautomatically warped onto new MRI brain datasets. This can create regions of interest in which subsequentanalyses are performed (reproduced from Lawrie et al., 2003, with permission of Oxford University Press).A coloured version of this figure can be found on the colour plate

104 Biological Psychiatry
become possible to make reliable and repeat-able within-individual BOLD maps for somecognitive, sensory and motor tasks. This within-individual BOLD fMRI mapping is now FDAapproved and used by neuroradiologists forpre-surgical planning of motor, sensory, visualand to some degree language areas. CurrentlyBOLD scans are not able to make individualdiagnoses, although they can predict, better thana polygraph and above chance, when someoneis lying (Kozel et al., 2005).
The third form of functional MRI involvesusing the MRI to image chemical spectra and iscalled magnetic resonance spectroscopy (MRS).Whereas MRI provides largely spatial informa-tion based on hydrogen or water content, MRSdetails chemical information. The principle isthe same as that for structural imaging, exceptthat the peaks for water are removed from thespectrum, and no tomographic reconstructiontechniques are applied. The resolution is not asgood as in conventional MRI, around 1 cm, andimage acquisition is typically much longer.
31P MRS reveals a number of peaks, and sincephosphorus is essential for energy metabolism,several directly reflect on, for example, the activ-ity of ATP, ADP, Pi: inorganic orthophosphate.
Proton (1H) MRS gives a more complicated spec-trum than 31P imaging, partly because nearly allbrain metabolites contain protons. Amino acids,inositol and creatine are all represented, and itis therefore possible to obtain information onexcitatory and inhibitory amino acids (e.g. glu-tamate and GABA) and membrane precursors(choline/phosphocholine). The main localiza-tion of n-acetyl aspartate (NAA) is in neurone,and its value will fall with neuronal degenera-tion (Figure 4.8).
There are other spectra, including those for13carbon, 19fluorine, 23sodium and 7lithium, andtheir value in CNS research is at present underinvestigation.
Cerebral Blood Flow (CBF) and Metabolism
Several techniques described above for brainimaging provide essentially anatomical data,and to the present have given information aboutstructural changes in the brain. In contrast,CBF and metabolism reflect on the functionof the brain. It is important to emphasize thatthe resulting images are based on compli-cated mathematical modelling, itself based on
Choline
Creatine
4.8
−0.24.3 3.3 2.3 1.3
CHEMICAL SHIFT (PPM)
0.3
INT
EN
SIT
Y
NAA
Figure 4.8 MRS from a 6 cm volume in the hippocampus. Signals measured are from NAA, creatine andcholine (Biol Psych, 2 Ed, p. 133)

Classifications and Clinical Investigations 105
suppositions about the biochemical activity ofthe brain in nondiseased states, and that theresolution of current machines is far less thanfor MRI. Although assessment of whole-brainCBF has been available for many years, it wasthe development of regional analysis in the1960s and the combination of these techniqueswith computed imaging to provide PET thatrevolutionized our knowledge in this area.
The use of radioactive isotopes to aid indiagnosis initially involved the administrationof gamma ray-emitting compounds such astechnetium 99 to outline blood–brain barrierdefects and enhance the visualization of, forexample, cerebral tumours. The first successfulmeasurement of CBF was with the nitrousoxide technique, introduced by Kety andSchmidt (1948).
The second-generation methods, rapidlydeveloped, relied on the rates that isotopes werecleared from the brain, traced by recordingthe decline in radioactivity over the scalp withscintillation counters. The isotopes were givenby either inhalation or intracarotid injection,and included 85-krypton and 133-xenon. Thenumber of detectors available has increased,and it is now possible to image regional CBF(rCBF) from many areas on both sides of thebrain. In practice, a tracer is given, and the‘clearance curve’ of its arrival and eliminationfrom the region is plotted. By comparison totheoretical values obtained from a physiologicalmodel, the CBF is derived. The initial slopeindex (ISI) is an early flow index frequentlyused. Tracer is monitored for approximately10 minutes after administration and calculationsof both grey- and white-matter flow are derived.The spatial resolution of the technique is lim-ited, and interference from the contralateralhemisphere reduces the sensitivity, especiallyfor detecting asymmetries. Early artefacts, suchas the problem of contamination of blood fromextracerebral sources, have been overcome, buthaemoglobin values, due to the affinity of xenonfor haemoglobin, and the arterial CO2 tensionhave to be taken into account in analysis. CO2is a potent vasodilator of cerebral vessels, andhyperventilation, for example due to anxiety,may lower the PaCO2 and the CBF.
In normal healthy adults, the mean CBF isaround 50 ml/100 g of brain tissue per minute,the values for grey and white matter beingapproximately 80 and 20 ml/100 g per minuterespectively. Normally a tendency to greatervalues frontally is found, as is a slow decreasewith advancing age (Frackowiak et al., 1980).
CBF, especially xenon inhalation, has manyadvantages: it is a noninvasive procedure, itis quick to perform, it is possible to repeatimages after a short time interval and, especiallycompared to PET, it is inexpensive. Its limita-tions are the low spatial resolution (2–4 cm),its inability to provide three-dimensionalimaging and its failure to give information ondeep cerebral structures. It has been largelyreplaced by three-dimensional SPECT and PETtechnology (see below).
PET
As noted above, the main source of cerebralenergy is glucose, but provided that thereis coupling between oxygen consumptionand ATP production, energy metabolism canbe deduced from measuring oxygen use.Although under normal conditions there iscoupling between the CBF and the cerebralmetabolic rate of oxygen use (CMRO2), and thusassessment of CBF may provide informationregarding metabolism, in pathological statesor with hypercapnia or hyperventilation therelationship is lost. Measurement of CMRO2using the technique of Kety and Schmidt waspossible, but, with the autoradiographic workof Sokoloff et al. (1977) and the technology ofcomputed tomography, the development ofPET has allowed for the assessment of both CBFand metabolism, in vivo, on a regional basis.
In PET, radioactive isotopes of biological sub-stances are created by a cyclotron, which firesprotons at a nucleus of, for example, carbon. Thelatter gains protons and becomes unstable, beingan ‘antiparticle’ to a negatively charged elec-tron. When in tissue, it combines immediatelywith an electron, the two particles convertingtheir mass into radiation energy. They subse-quently annihilate. The latter gives rise to therelease of two coincident gamma rays of equal

106 Biological Psychiatry
DETECTOR DETECTOR
Accepted by coincidence detection
REGION OFCOINCIDENCE
DETECTION
Rejected by coincidence detection
Figure 4.9 Release of coincidence rays following positron annihilation, and detection of coincidence rays bythe scanner (Biol Psych, 2 Ed, p. 135)
energy which travel at 180◦ to each other (seeFigure 4.9).
The presence of these rays is picked up bythe detectors of the scanner, positioned suchthat they only record coincident events, thesebeing separated from other nonsimultaneouslyreleased gamma rays. Thus the decay event isknown to have taken place on a line connectingthe two detectors, a process called coincidencedetection. Detection cameras are placed in a ringaround the patient’s head, the exact structurebeing dependent on the system used. Comput-erized reconstruction of the image is performedusing technology similar to that of CT scanning.However, it is essential to recognize a funda-mental difference between the two techniques,namely that in CT, rays from an external sourceare passed through the patient’s brain, while inPET, rays are emitted from the brain, detectedand quantified. Further, the image of PET isindeed an image, and one of tissue-tracer distri-butions. It is not an anatomical map as providedby MRI and CT.
The spatial resolutions of the machines vary,but typically are between 7 and 15 mm. For
technical reasons related to the finite range of thedecay of positrons, the maximum resolution is inthe region of 2–3 mm. In order to obtain accuratereadings from a structure, it should have a sizetwice that of the resolution of the machine.
The main biologically interesting positronemitters created include carbon-11, nitrogen-13,fluorine-18 and oxygen-15. In practice, since allbut fluorine-18 have short half-lives, the patienthas to be in close proximity to the cyclotronfor the investigations to be carried out. Withfluorine-labelled isotopes, with a half-life of110 minutes, the substance can be transportedto the patient over considerable distances.
Depending on the isotope used, PETprovides information on several parameters,including cerebral blood volume, CBF, cerebralmetabolism and neuroreceptor function.
At present there are two main systems forimaging metabolism, one based on oxygen andthe other on glucose or deoxyglucose. In theoxygen-15 technique, the patient continuouslyinhales trace amounts of oxygen-15-labelled car-bon dioxide (CO2) and oxygen. The CO2 israpidly converted in the lungs to H15
2 O and

Classifications and Clinical Investigations 107
is distributed throughout the arterial tree, about20% reaching the brain, where it equilibratesrapidly with tissue water. Since this is removedcontinuously by the venous system, at steadystate the concentration of radioactivity mea-sured will reflect both the delivery to and thedecay from the tissue. Thus, at steady state, itis possible, using mathematically derived for-mulae with various corrections, to calculate theblood flow.
Similarly, the 15O is delivered to the brainattached to haemoglobin, and is there usedto fuel the Krebs cycle for the production ofATP, the radioactive oxygen appearing in wateras a result of the metabolism. Again, withsophisticated mathematics and correction forsources of error (Lammertsma et al., 1981), it ispossible to define the oxygen-extraction frac-tion (OEF) – the fraction of available oxygenextracted from the blood – and from this andthe CBF the CMRO2 is calculated.
The fluorodeoxyglucose (FDG) method relieson the ingenious yet simple principle developedby Sokolof et al. (1977). Glucose, when admin-istered, is taken up into tissue and rapidlymetabolized to CO2 and H2O and cleared fromthe brain. However, deoxyglucose is takenup and phosphorylated to deoxyglucose-6-phosphate, but this is not metabolized furtheras there are no available enzymes for its furtherdegradation. In addition there is no functionaldephosphorylase, so it cannot re-enter theprecursor pool. As a consequence it getstrapped in the tissue, and its presence is directlymeasured and quantified since the radioactivedeoxyglucose emits positrons, which lead to theproduction of coincidence annihilation gammarays detected by the scanner. In contrast to theshort half-life of 15O (123s), that of FDG is inthe region of 110 minutes; hence its use entailsa longer study and requires careful control andmonitoring of the patient’s state during theuptake period. The metabolic handling of thisanalogue of glucose has then to be equated withthat of glucose if the derived measurementsare to be used to reflect neuronal metabolism.The relationship has been found constant undermany conditions, mathematically referred to
as the lumped constant, but the latter has beenderived essentially from animal models andmay break down in certain pathological states,leading to erroneous calculations.
Interpretation of the data accumulated withPET is subject to a multitude of errors, which atpresent are probably responsible for the confu-sion in some of the data, especially with regardto psychiatric illness. Some of these are listed inTable 4.2.
Innovations of PET technology have beenprogressing rapidly. State-of-the-art camerascan collect data in seconds from many contigu-ous transaxial planes and have a resolutionapproaching 5 mm. Many measurements canbe taken in one session, scanning every fewminutes. Activation tasks, which will increaseactivity in specified areas of cerebral function,have been used to study responses to pharma-cological or behavioural stimuli. The techniquerequires at least two data sets generated inconditions that differ for the specific functionexamined. Motor tasks might be simple repeat-ing of a specific movement, while cognitivetasks might include the administration of apsychological test such as the Stroop test.
Positron-emitting radioligands are used toexamine neuroreceptor and neurotransmitterfunction. The ligand must be selective for areceptor and have high affinity, with goodblood–brain barrier penetration. Typicalcompounds in use include 11C flumazenil forbenzodiazepines, 11C methyl spiperone and 11Craclopride for dopamine, 11C carfentanil foropiates, and 18F ritanserin for 5-HT. Carbon-and fluorine-labelled L-dopa are now availableto detect the precursor pool of dopamine.Newer compounds, for other systems, andreceptor subtypes are in development. One ofthe more exciting areas is the development andtesting of amyloid ligands for the diagnosis andstudy of Alzheimer’s disease. The most widelyused at present is the Pittsburgh Compound B(PIB), which is being used in several large trialsfor diagnosis, correlation with clinical diseaseburden and as a potential surrogate marker fornew drug development. These amyloid ligandsare not yet commercially available. A dopamine

108 Biological Psychiatry
Table 4.2 Potential artefacts in the interpretation ofPET. (From De Lisi and Buchsbaum, 1986)
Compound as tracer
1. Half-life and breakdown rate of label2. Purity of the compound3. Differences between oxygen and glucose4. Differences between labels, e.g. 18F/11C
Experimental conditions
1. Variation in anxiety and emotional state ofsubject
2. Psychiatric state of patient3. Task performed during the uptake period4. Variation in sensory inputs, e.g. eyes
open/closed5. Prolonged uptake period with inconstant
physiological changes6. Variation in blood sampling procedures7. Failure to control for age and sex
Instrumentation
1. Limited resolution2. Non-uniform resolution3. Scatter and partial volume effects4. Inadequate number of planes sampled5. Need to standardize adequately to phantoms6. Variation in head size and shape7. Head movement8. Change in distribution of tracer compound
during the scan procedure from first to lastslice
Data analysis
1. Inaccuracy of models for describing bio-chemical kinetics
2. No appropriate model for some substances3. Kinetic constants used derived from animals4. Differences in the kinetics between white
and grey matter5. Difficulties in matching some slices among
individuals6. Undersampling of anatomical structures7. Overinterpretation of assumed anatomical
details8. Computerized methods failing to account for
anatomical differences among individuals9. Accounting for cortical folding
10. Lack of serial determinations of data in thesame individual over time, so normal varia-tion unknown
D4 agonist and 5-HT1a antagonist, the WAYligand, is available and is used for research.
Single-Photon-Emission Tomography(SPECT or SPET)
This technique has proved to be more usefulthan its early detractors predicted. Instead ofpositron-emitting isotopes, SPET uses single-photon emitters. The image is obtained by arotating gamma camera. This rotates through360◦, and a series of images are acquired rep-resenting the sum of radioactivity along a lineparallel to the hole in the detecting collima-tor. These are reconstructed by filtered back-projection. Multidetector cameras are now inuse, which give much better resolution (8 mm),as are safe, reliable tracers. The latter include133xenon, 123-p-iodo-N-isopropylamphetamine,99mTcHMPAO and several neuroreceptor lig-ands. 99mTcHMPAO has proven of particularvalue. Once given, it is taken up by neurones,where it remains for a few hours, giving asnapshot of cerebral activity at the time ofadministration (George et al., 1991, 1992).
The advantages of SPECT over PET includeits more ready availability and its low cost.The tracers generally have longer physical andbiological half-lives, not requiring an on-sitecyclotron. However, quantification of data ismuch more complicated, ratios between dif-fering brain areas often being used, with onestructure, such as the cerebellum, being usedas a standard reference. Multiple rapid imagesof the type now available for PET studies arenot possible, although sophisticated activationprotocols can be performed.
As with PET, several SPECT ligands are use-ful clinically, although they are not widely used.β-CIT SPECT is used to assess dopamine func-tion in Parkinson’s disease. In general, it is moredifficult to create specific ligands for SPECTthan it is for PET, because of the need to couplethe ligand with one of the technetium transporttracers, as opposed to simply inserting a labelledcarbon or oxygen molecule.
As discussed above, it is easy to overinterpretbrain-imaging results, and many patients andclinicians wish that brain imaging could do more

Classifications and Clinical Investigations 109
than it can in terms of making diagnoses andguiding treatments. As will be discussed in thechapters that follow, there are several promis-ing areas in psychiatry where brain-imagingtechniques are starting to aid clinically (notjust as a research tool). In classical neurologicaldisorders such as multiple sclerosis, brain imag-ing has revolutionized diagnosis and treatmentmonitoring. One example of the likely misuseof brain imaging is in the claims that brainSPECT scans can diagnose ADHD, and pre-dict which treatment a patient should receive(Amen and Carmichael, 1997). Unfortunately,there are no class I data showing that thisis the case and many published trials showthat brain imaging is not clinically useful inADHD (Zametkin and Liotta, 1998). Biologicalpsychiatrists should attempt whenever possi-ble to practice evidence-based medicine, andin areas where there is no data and there ispotential harm from radiation exposure, ‘first dono harm’.
Near-Infrared Spectroscopy (NIR)
This approach uses a fairly small and oftenportable machine and a movable wand, muchlike an ultrasound machine. Unlike ultrasound,the fibre-optic wand transmits energy in theelectromagnetic spectrum (from about 800 to2500 nm), which interacts uniquely with tissueand is able to penetrate through bone (skull). Itcan thus examine changes in haemoglobin con-centration in the cortical tissue just below theskull. As with fMRI and PET, brain regions thatbecome activated have relatively rapid changesin local oxygen and haemoglobin concentra-tions. The advantages of NIR are that it is non-invasive, relatively inexpensive and portable.Its main disadvantage is that it can only revealinformation about the cortical regions directlyunder the wand, and thus cannot provide a fullimage of brain activity. It is currently mostly aresearch tool.
Transcranial Magnetic Stimulation (TMS)
A common method in science to help under-stand causality is to eliminate something, and
then see if the behaviour or disease changes.Thus, researchers ‘knock out’ genes and exam-ine the effects on the animal or system they arestudying. Building on the knowledge providedby PET and fMRI, many biological psychia-trists and cognitive neuroscientists are startingto use TMS as a knockout method. TMS is atechnique in which a powerful small electro-magnet is placed on the scalp (George andBelmaker, 2006). The brief but powerful mag-netic field passes unimpeded into the outerlayers of the brain and induces electrical cur-rents in the cortex. This noninvasive approachcan temporarily ‘activate’ brain regions, makingthem temporarily unavailable for normal cogni-tive processing (Muggleton et al., 2006; Stewartet al., 2001; Walsh and Cowey, 2000). Thus, TMScan be used as a research tool to ‘knock out’or interrupt a brain region and observe thechanges in behaviour. This is easiest to demon-strate over language areas, where brief TMS canproduce a temporary speech arrest resemblinga Broca’s aphasia.
Cognitive Neuroscience
The introduction of the new imaging techniqueshas led to a revolution in understanding ofbrain–behaviour relationships, and the rapiddevelopment of this discipline. Using MRI tech-niques it has been possible to confirm andexpand data about areas of cerebral cortex thatrespond to sensory stimulation, and relation-ships between multiple brain areas of activa-tion. This in part has stimulated the approachtowards circuits and parallel distributed pro-cessing (PDP) as a model of brain function.One interesting application of functional MRIhas been to note signal changes during men-tal imagery. The brain uses much the sameregions when imagining doing an action as itdoes actually doing it.
Despite all the advances in brain imaging andbrain-stimulation knockout techniques, there isstill inadequate understanding of some of themore important and basic questions. How doesone form a mental image? What is the brain basisof consciousness? While these questions remainlargely unanswered, many recent studies are

110 Biological Psychiatry
beginning to emphasize, for example, the roleof the precuneus in studies of ‘self awarenessof mental acts’. Thus, in addition to designingever more clever experiments or paradigmsin an attempt to understand self-awarenessor consciousness, others are attempting totackle this question using different statisticalapproaches and novel imaging methods. Oneof these approaches is called resting BOLDfMRI. In these studies, rather than the usual‘task–rest–task. . .’ paradigms, subjects areinstructed to simply ‘do nothing’. Serial BOLDscans over 5–10 minutes are then analysed forbrain regions that either positively or negatively
change with each other over time. This is anattempt to examine functional connectivity.Some have speculated that these functioningcircuits become dysregulated in disease statesor with different levels of ‘consciousness’ orself-awareness. The main regions of interest arethe medial frontal cortex and the precuneus.
It is beyond the scope of this work to reviewall of brain imaging. But suffice it to say thatover the past 20 years PET and fMRI datahave allowed numerous cognitive operationsto be mapped, for example the brain regionsassociated with memory, language and evenemotional recognition of faces (Figure 4.10)
Medial Views
Front Front
(a)
(b)
Figure 4.10 (a) Statistical parametric maps (O15 PET) of the brain regions activated during transient sadnessinduced by remembering sad events and viewing sad faces. The control task consisted of rememberingneutral events and viewing neutral faces. Note that anterior limbic structures (septum, anterior cingulate)and left prefrontal cortex are activated. All points in dark tone represent significant increases in activity (p <
0.01) (courtesy of Dr Mark George). (b) Three consecutive coronal slices through the brain of the group brainactivation that occurs when healthy subjects are unconsciously exposed to ultra-brief (subliminal) picturesof human faces which look fearful. The subjects were unaware after the imaging study that they had evenbeen exposed to anything unusual. Note that the ‘early warning system for danger’, the amygdala, bilaterallyshow activation during the time the subjects are exposed to the fearful faces, compared to when they are not.This was one of the first demonstrations of the rapid fear response system of the amygdala (reproduced fromWhalen et al., 1998). A coloured version of this figure can be found on the colour plate

Classifications and Clinical Investigations 111
(George et al., 1993). While confirming muchthat was previously known, these studieshave enriched our knowledge of potentialneuronal networks, and have emphasized theholistic nature of cerebral activity associatedwith cognitive tasks. Interestingly, although
referred to as cognitive, many of the areasinvestigated might better be referred to asemotional, but such studies are now explor-ing the fundamentals of human thinkingfrom decision making to rationality andconsciousness.


5Personality Disorders
GENERAL INTRODUCTION
Here, and in the following chapters on theaffective disorders and the psychoses, thebiological underpinnings of psychopathologywill be reviewed. Following an introduction toeach topic, genetics, metabolic and biochemicalfindings, neurochemical and neuropathologicalinformation, and the literature on neuro-logical illness – including the abnormalitiesfrom special investigations – will be referredto. Each chapter ends with a discussion ofoutstanding issues.
INTRODUCTION TO THE CONCEPTOF PERSONALITY
We see the personality in the particular wayan individual expresses himself, in the wayhe moves, how he experiences and reacts tosituations, how he loves, grows jealous, howhe conducts his life in general, what needs hehas, what are his longings and aims, what arehis ideals and how he shapes them, what valuesguide him and what he does, what he createsand how he acts (Jaspers, 1963, p. 428).
It is thus by the personality traits that we knowsomeone; they are enduring and give an air ofpredictability to a person. In common parlancethere is little difficulty in understanding a per-son’s personality in these terms. It follows that
Biological Psychiatry 3e Michael R. Trimble and Mark S. George 2010 John Wiley & Sons, Ltd
over time people have given certain personalitystyles names, and that scientists have attemptedto quantify various attributes of personality.A popular concept for example has been that ofthe axis of introversion–extroversion, and useof the Eysenk Personality Inventory (EPI) formeasurement. Another well-validated scale hasbeen the Minnesota Multiphasic PersonalityInventory (MMPI). There are many others; someattend to specific aspects of personality, such asobsessionality, while others, like the MMPI, arebroad in scope. An additional approach has beenthe scheme developed by Robert Cloninger,where personality is defined on three axes,which loosely relate to neuropharmacology.The axes are impulsivity and risk-taking,interpersonal reactivity and harm avoidance.They were originally thought to relate to themajor monoamine systems, with dopaminelevels correlating with risk-taking, 5-HT withinterpersonal reactivity and noradrenaline withharm avoidance (Cloninger, 1987; Cloningeret al., 1993, 1996a, 1996b; Svrakic et al., 1993).
With such assessments, it should be possibleto define normality within a population,and hence reflect on abnormality. Thus, inpsychopathology, two ways of defining anabnormal personality, a statistical method andone based on ideal types, have arisen. Jasperspreferred the former, as did Kurt Schneider(1959), who defined abnormal personalities asthose who ‘. . .suffer from their abnormalityor through whose abnormality society suffers’

114 Biological Psychiatry
(p. 4). The alternative, invoking a kind ofPlatonic reality, suggests that ideal Pygmalioncreations exist in nature; this is the way ofDSM IV-TR.
The diagnostic criteria for the personality dis-orders, and other psychopathologies discussedin this book, can be found in DSM IV-TR, ICD 10and the Structured Clinical Interview for DSMIII-R Personality Disorders SCID-IIP (for per-sonality). Caution about the use of such manualshas already been given. The types discussed inthis chapter cover the following:
Psychopathic personality is a term used bySchneider to embrace several differing abnor-mal personality patterns, but generally nowimplies antisocial personality traits. In the ICDit is referred to as the dissocial personality, andin DSM IV-TR as antisocial personality disor-der (ASPD). It manifests mainly as sociopathy.Sociopathic personality or antisocial personal-ity are alternative terms. It is characterizedby ‘disregard for and violation of the rightof others’ (DSM IV-TR). It usually becomesapparent in early life, often with conduct dis-order at school, a continuing history of poorinterpersonal relationships, a poor work recordand continuing marital difficulties. Drug abuse,alcoholism, pathological lying and prison con-victions may be recorded, and sociopaths tendto display more than accepted sexual devia-tion, somatization and outbursts of physicalviolence. A characteristic feature is the tendencyto remit over the years, either in early or midadulthood.
Obsessional personality, also referred to asthe anankastic personality disorder in ICD 10,and obsessive–compulsive personality disorder(OCPD) in DSM IVTR is characterized by a life-long tendency to meticulousness and punctual-ity, and feelings of doubt leading to excessivecaution. Patients have a reluctance to delegatetasks to others, and insist on tasks being carriedout only in certain ways. It is better referred to asthe anankastic personality disorder, as this savesconfusion with obsessive–compulsive disorder(OCD) (see Chapter 6).
Histrionic personality has links to the antiso-cial personality disorder, and in many ways iscontrasted with the anankastic. Jaspers (1963)
defined the type thus: ‘hysterical personalitiescrave to appear, both to themselves and oth-ers, as more than they are and to experiencemore than they are ever capable of’ (p. 443). Thecharacteristic traits are excessive dependence;suggestibility; shallow, labile affects; impulsive-ness; verbal exaggeration and excessive gesturaldisplay; seductiveness in the presence of rela-tive frigidity; and self-dramatization. Patientsprefer to be the centre of attention, and long forappreciation. There is a tendency to take over-doses of medication or make other attempts atself-harm, and there is some association withsomatization. The validity of this category hasbeen established by factor analysis (Lazare et al.,1970), from which studies its traits are clearlydistinguished from the anankastic personality.In particular, the impulsivity and the tendencyto approximate and exaggerate of the histrionicpersonality stand in contrast to the calculationsand deliberations of the anankast. In contrast tosociopaths, who tend to be male, histrionic per-sonalities are commoner in females. There areclear overlaps with both dissocial and borderlinepersonalities.
Borderline personality was first introduced inDSM III. In the ICD 10 it is a subcategory ofthe emotionally unstable personality disorders.The essential feature is ‘a pervasive pattern ofinstability of interpersonal relationships, self-image, and affects and marked impulsivity. . .’(DSM IV TR, p. 710). There is marked identitydisturbance, impulsivity and recurrent attemptsat self-harm. Patients display transient episodesof paranoid ideation, and may have dissociativesymptoms.
Paranoid personality is distinguished by con-tinued suspiciousness, mistrust and excessivesensitivity. Jealousy, transient ideas of reference,litigiousness and a tendency to avoid intimacyare all features, and individuals often take upminor concerns or causes with tenacious vigour,collecting vast amounts of documentary evi-dence to support them.
Schizoid personality features describe peoplewho have little affective or social contact, with atendency to detachment and eccentricity. Whilewell recognized, the DSM IV-TR has split thisinto three groups, the schizoid, the schizotypal

Personality Disorders 115
and the avoidant. The schizotypal appears toinclude oddities of behaviour, thinking, per-ception and speech with unusual beliefs andideas of reference, and the avoidant emphasizeshypersensitivity and social withdrawal in spiteof yearning for acceptance. The schizoid person-ality disorder defines those who appear cold,seem to experience no pleasure and are solitary.They seem insensitive to praise or criticism, andto social norms.
Other Personality Types
In addition to the above groupings, which findsome concordance in the different systems, var-ious other types are described, although thecriteria are often less than clear. Anxious person-ality (ICD 10) defines those who display lifelonganxiety, and under stress readily develop anx-iety or panic disorder. Narcissistic personalityrefers to those with a grandiose sense of self-importance or uniqueness; preoccupation withfantasies of unlimited success; exhibitionisticneed for constant attention and admiration;characteristic responses to threats of self-esteem;and characteristic disturbances in interpersonalrelationships. Also noted are frequent depressedmoods and transient psychotic states.
DSM III included the category of the pas-sive aggressive personality, those who habituallyexpress covert aggression. Both ICD 10 and DSMIV-TR describe the dependent personality disor-der. These individuals have a pervasive needto be taken care of that leads to submissiveand clinging behaviour and fears of separation.ICD 10 refers to the explosive personality, in whichliability to intemperate outbursts of anger areseen in people otherwise not prone to antiso-cial behaviour, under the emotionally unstablepersonality disorders.
Links between Personalityand Psychiatric Illness
A form of depression less severe than majoraffective disorder is now referred to as dys-thymic disorder, involving prolonged andpersistent lowness of mood beginning early in
life. This is associated with chronic psychosocialstresses and ‘personality disorder . . . mergesimperceptibly into this condition’ (AmericanPsychiatric Association, 1987, p. 221). Patientswith personality styles referred to as avoidantor dependent personalities display lifelonganxiety with bouts of panic and exacerbationunder stress.
Thus, in these typologies there is not alwaysa clear separation between personality styleand certain categories of psychiatric illnessthat used to be referred to as neurotic, aword removed from DSM IV, but which haslongstanding psychiatric understanding. If thequantitative approach to personality disordersis taken, separation between individuals takeson less clear boundaries, personality disorderrelating to a statistical deviation from thenorm. Schneider’s model blurs the distinctionbetween the neuroses (anxiety disorders inparticular) and personality disorders, definingpersonality disorders as dispositions throughwhich either the individual themself or societysuffers. Some other models of psychopathologyconfuse boundaries even further. For example,the Meyerian reaction types, which minimizedendogenous variables at the expense of ‘reac-tions’ to environmental events, drew no cleardistinctions between personality idiomorphs,neurosis and psychosis. Freudian psychoanal-ysis also failed in this regard, the pathogenesisof all forms of psychopathology being similarin that they represent deviant childhooddevelopments with libidinous fixations andlater regressions.
In contrast, Jaspers’ model emphasizes cleardistinctions between personality and illness, notonly phenomenologically, but also developmen-tally. Illness is a new feature, either skewingthe development of personality or altering thematured individual, leading to phenomena thatcannot be understood in terms of that individ-ual’s normal development. As Slater and Roth(1969) pointed out, this was an extremely usefulclinical distinction, enabling clearer delineationof such illnesses as schizophrenia, and theirdistinction from the excessive reactions of var-ious personalities. Further, it led to success indistinguishing various primary mood disorders

116 Biological Psychiatry
from secondary mood changes; the endogenousfrom other forms. This breakdown into primaryand secondary is useful. Secondary depressionis that which occurs in the presence of pre-existing psychiatric disorders or chronic medicalillnesses (Feighner et al., 1972; Goodwin andGuze, 1984), amongst which are to be includedpersonality disorders.
Thus, concepts of personality and neurosisseem to have been historically intertwined byseveral groups of authors, often writing fromdifferent perspectives. The blurred boundaryhas had many consequences. For one, terminol-ogy became a labyrinth of confusion. Neuroticdepression and its distinction from endoge-nous depression became an area of intenseresearch, the outcome of which is not clearto this day. Variants of terms such as depres-sive reaction, psychogenic reaction, depressivepersonality and dysthymia added to the con-fusion, and people with abnormal personalitieswere wrongly classified as having psychiatricillnesses.
This last point is more fundamental than isoften appreciated, and itself has had conse-quences for biological psychiatry. First, if theillness represents the outcome of a process thenit may be possible to identify that process biolog-ically. Hence the search for biological markersin psychiatry. In some cases these markers willbe identifiable as abnormal tissue pathogens,for example as in an encephalitis. In others,the neurochemical constituents alone may be atvariance, and detection of the change rests inidentifying variation from the normal expectedrange. If patients with personality disordersare confused in a group with those having aparticular illness then the sought abnormalityor biomarker will be diluted and not found.This problem sometimes arises with researchinto depressive illness, where patients withpersonality disorders are wrongly categorizedas having a major affective disorder or dys-thymia. A similar problem arises in drug trials,where heterogeneous populations masqueradefor homogeneous ones, and real differencesbetween active drugs and placebos may beminimized. Attempts, such as the DSM III andits successors, to more rigidly define categories
and provide exclusions as well as inclusions arehelpful for some areas of psychiatric research,but are still quite imperfect.
A second consequence relates to the imageof psychiatry with nonmedical people. Patientswith personality disorders often developdepressive symptoms in the setting of socialstress, and may be thought, by the uninitiated,to have what psychiatrists refer to as majoraffective disorder. As many such peoplerespond, albeit temporarily, to manipulationof their social environment, it is assumed thatall psychopathology can likewise be remedied.This thinking, combined with lay confidence inthe nonbiological therapies that characterizedpsychiatry a generation ago, has led to markeddistractions in attempts to understand thebiological bases of psychopathology.
DSM IV-TR recognizes clusters of personal-ities which have some identifiable overlappingfeatures. Cluster A embraces the schizoid, para-noid and schizotypal – the odd and the eccen-tric; cluster B the antisocial and impulsive, theflamboyant and the erratic; and cluster C thedependent, the anxious and fearful. This line ofthinking leads on to consideration of personalitytraits and their relationship to states. Traits arepersistent underlying attitudes, while states aretemporary or permanent manifestations, andwill take two forms. Trait exaggeration is oneform, in which a flowering of the premorbid per-sonality is seen. The other is symptoms that arisede novo. Thus, traits and states do not always gohand in hand; the development of OCD or aconversion disorder (somatoform disorder) isnot necessarily dependent on the premorbidpersonality, as predicted by some theories.
With regard to depressive symptoms,some authors described so-called depressivepersonalities (Schneider’s (1959) depressivepsychopaths) as people who are continuallypessimistic, with constant anxiety about them-selves and their world. This style, however, isnot found in DSM IV-TR. Cyclothymic disorder,appearing with affective disorders, replacesboth depressive and cyclothymic personalitydisorder, emphasizing the illness rather than thepersonality. There is some literature supportingthe link between cyclothymic personality and

Personality Disorders 117
manic–depressive illness, notably the findingof an excess of cyclothymic personalities amongthe relatives of manic–depressive patients(Kallmann, 1954), and evidence of cyclothymicbehaviour in between illness episodes inmanic–depressive patients (Winokur andTanna, 1969) (see Chapter 8).
The strongest associations between personal-ity traits and psychopathology are encounteredbetween types of OCPD and OCD. In Kringlen’s(1965) study, over 70% of patients with OCDhad such a personality style. Another postulatedrelationship is between the symptoms of conver-sion (somatoform disorder) and the hystericalpersonality. However, clinical estimates notethat only 18–21% of patients with conversionsymptoms conform to this style (Merskey andTrimble, 1979), supported in studies of similarpopulations using standardized rating scales toassess personality (Wilson-Barnett and Trimble,1985). There is an association between schizoty-pal personality disorder and OCD (Sobin et al.,2000). Dependent personality disorder has linkswith panic disorder and agoraphobia (Hoffartet al., 1995), and avoidant personality disorderlinks with social phobia.
In a study of 660 patients, axis 1 and 2diagnoses were assessed and associationsbetween personality disorder and psychosiswere examined with logistic regression analysis.Among the associations noted were schizotypaland schizoid personalities with schizophrenia,paranoid personality with delusional disor-der, histrionic personality with brief reactivepsychosis and OCPD with major depression(Cuesta et al., 1999; Peralta and Cuesta, 1999).
In summary, the links between personal-ity styles and psychiatric illnesses are not soclear and much is clinical lore. In some clinicalsettings, notably the anxiety and affective disor-ders, disentangling the constitutional elementsin the clinical picture is difficult, especially withlimited patient contact. It is often only with timethat the personality vulnerabilities of patientsbecome exposed and the nature of the co-morbidpsychopathology becomes clearer. The linkshowever are of profound importance clinicallyand conceptually. For example, cluster A meldswith the concept of a schizophrenia spectrum of
disorders, the latter falling at the more extremeend of the former, and broaches the subject ofendophenotypes related to cognitive and emo-tional styles. Certain cognitive and behaviouraldispositions may increase the risk for axis 1disorders, such as substance abuse, or neuro-logical disorders, such as head injuries, whichthen impact further on personality dimensions.It is unclear when some personality attributesbecome axis 1 disorders, what may be the geneticlinks, and to what extent treatment of an axis 1profile leads to changes which alter the axis 2designation (e.g. treating an anxiety disorderand the effects on the comorbid anxious person-ality disorder).
Personality Styles
The above distinctions of different personalityconstellations lead to consideration of the differ-ent styles of thinking and perceiving of emotionby different individuals. Shapiro, in a book titledNeurotic Styles, outlined the differences betweenfour different ways of responding to the worldas seen in obsessive–compulsive, paranoid, hys-terical and impulsive personalities (Shapiro,1999). The theme was that each style was char-acteristic, and although the book was writtenfrom a psychoanalytic era, the implication wasthat the styles of thinking related to underlyingpsychological structures, the mode of thinkingitself being interlinked with the psychopathol-ogy. An act carried out by say an obsessionalpersonality guarantees their next act, which willseem to them the most rational way of proceed-ing. ‘The paranoid person is not simply visitedby apprehensions and defensive suspicions; hesearches actively and does not rest until he haslocated clues to new dangers’ (Shapiro, 1999,p. 20). Shapiro draws attention for example tothe rigid thinking of the obsessional, which canalso emerge after cerebral trauma, with a nar-rowed focused attention which implies a lackof cognitive flexibility. Paranoid personalitieshave an acuteness of attention; this is contin-uous and always a searching for something.‘Significant’ cues are seized from their context,a subjective world emerges which is endowedwith special significance and reality is distorted.

118 Biological Psychiatry
The hysterical style is one of impressions andsuperlatives (‘Wow! It’s wonderful.’), with lackof factual detail, and poor concentration skills.‘Hysterical attention is easily captured . . . theirline of thought is easily interrupted by transientinfluences’ (Shapiro, 1999, p. 115). This leadsto an inadequate memory and a poverty ofknowledge. Their cognitive style is thus impres-sionistic, immediate and global. Their emotionallife is one of lability, emotional outbursts being afeature, but outbursts which they almost disownas something which has been visited on them.Psychopathic traits include insincerity and aproclivity to lying, impulsivity, and cognitivelya lack of planning, concentration and logicalobjectivity.
This line of thinking is an elaboration onJaspers, in that it suggests different cognitiveanlages which define behaviour, underlying notintelligence, but the way the world and its con-tingencies are reflected upon and respondedto. In the context of biological psychiatry, theunderpinnings of this would be related to neu-robiological principles, and hence the relevanceof examining personality changes in neurolog-ical disorders and looking for neuroanatomicaland neurophysiological profiles that relate todifferent personality styles. Unfortunately thishas not been well researched, in part becauseof a reluctance on behalf of many even withinthe psychiatric community to accept conceptsof personality disorder, or if they are accepted,to attribute the personality disorder entirely tosociological variables.
Of the many attempts to quantitativelyexamine the structure of personality by theuse of rating scales and statistical analysis andinterpretation, the rating scales of Eysenk arestill most widely used. Of all the personalitydisorders, antisocial personality disorder hasbeen the most researched, and Hare’s Psy-chopathology Checklist is widely used. Withfactor analysis, two main factors are identified,the first relating to charm, glibness, pathologicallying, lack of guilt, lack of empathy and thelike, the second to a need for stimulation, easyboredom, poor behaviour control, impulsivityand irresponsibility (Guay et al., 2007; Hare,1999; Neumann et al., 2007). Using Cloninger’s
method, antisocial personality has been shownto be associated with somatization disorder andsubstance abuse (Battaglia et al., 1996; Cloningeret al., 1993; Svrakic et al., 1993).
GENETICS
General Findings
There is considerable evidence that genetic fac-tors are of importance in personality disorders.The early studies are well reviewed by Slaterand Roth (1969) and McGuffin (1984). Ani-mal studies have permitted the selective breed-ing of anxiety-prone rats (Broadhurst, 1975).These show greater corticosterone, ACTH andprolactin responses to stress, and lower 3H-diazepam binding in various cortical structuresand the hippocampus than non-anxious coun-terparts (Gentsch et al., 1981).
In humans, the familial prevalence of anxietyis high, over 50% of first-degree relatives suffer-ing from the same disorder. The clinical ratingsof personality are more similar in monozygous(MZ) twins than in dizygous (DZ) pairs, evenin MZ twin pairs reared apart from an earlyage. In the study of Shields (1962), MZ twinsreared apart were more alike than MZ twinsraised together, leading to the suggestion thatthe common environment of the twins is less rel-evant for this aspect of personality developmentthan genetic factors. Shields (1954) showed thatMZ twin schoolchildren resembled one anotherwith regards to the pattern of what was thenreferred to as neurosis, the mean concordancerate taken from several studies of neurotic iden-tical twins being given as 61% by Tienari (1963).In the latter’s own study of 21 identical twinpairs classified as neurosis cases, only 5 hada normal co-twin, 13 pairs having a co-twinwith either neurotic personality, a neurosis oran immature personality. With regards to theclinical picture, the tendency towards concor-dance was clearest with phobic and obsessionalcases (91%).
One problem with many of these clinical stud-ies is the vagueness of classification of the indexdisorders, and in many instances the diagnoses

Personality Disorders 119
were purely given on a retrospective analysis,case notes being relied on for the historical data.Further information comes from studies usingrating scales of psychopathology to quantifysymptomatology. Gottesman (1962) gave theMMPI to twins and derived a hereditabilityindex for the scales. The highest values were forSi (social introversion) and Pd (psychopathicdeviation), while only low values were reportedfor Hy (hysteria). Likewise there is evidencefor genetic factors in the personality dimen-sions extraversion–introversion using the EPI,estimates of hereditability values being 50%.
Torgersen et al. (2000), using twin and patientregistries, interviewed 92 MZ and 129 DZ twinpairs using the SCID-IIP. The best-fitting modelshad a heritability of 0.60 for personality disor-ders generally, with 0.37 for cluster A, 0.60 forcluster B and 0.62 for cluster C. Among the spe-cific disorders, the heritability given was 0.79 fornarcissistic, 0.78 for obsessive–compulsive, 0.69for borderline, 0.67 for histrionic, 0.61 for schizo-typal, 0.57 for dependent, 0.54 for self-defeating,0.29 for schizoid, 0.28 for paranoid and 0.28 foravoidant personality disorders. Family environ-mental influences were very limited, and theresults were more strongly influenced by geneticeffects – more than almost any axis 1 disorder.
One of the more interesting and controversialareas of personality and genetics in the recentliterature has revolved around whether certainvariants of the dopamine receptor, specificallythe D4 variant, are associated with increasednovelty-seeking or impulsivity. Initial studiesfound such an association (Cloninger, 2008),which has more recently been challenged(Paterson et al., 1999; Soyka et al., 2002; Thomeet al., 1999). More studies are needed.
Genetics of Specific Personality Disorders
There is good evidence that genetic factorscontribute to individual personality disorders.Most investigated has been antisocial personal-ity disorder (sociopathy). Concordance betweenMZ twins with regards to criminality has beenreported by several groups (Christiansen, 1974;Lange, 1929), supported by adoption studieswhich show higher rates of offences in adopted
children in cases where the natural father isknown to the police (Hutchings and Mednick,1975). Baker et al. (2007) reported in a largesocioeconomically and ethnically diverse sam-ple of 605 families of twins or triplets that mea-sures of antisocial behaviour such as conductdisorder, ratings of aggression, delinquencyand psychopathic traits obtained through childself-reports and teacher and caregiver ratingsrevealed a common antisocial behaviour factorthat was strongly heritable (heritability at 0.96).Family studies confirm associations betweenantisocial personality disorder and somatizationdisorder and substance abuse, linked by heri-table personality traits of high novelty seekingand low self-directedness (Cloninger, 2005).
Torgersen (2000) reviewed the literature onthe genetics of borderline personality disorder(BPD) and concluded that it was too early to sayto what extent BPD is influenced by genes. How-ever, since traits similar to it, such as noveltyseeking, are found in BPD and are themselvesinfluenced by genes, and because personalitytraits generally show a strong genetic influence,this should also be true for BPD. He opinedthat the effect of genes on the developmentof BPD is likely substantial while the effectof common family environment may be closeto zero (Torgersen, 2000). Molecular geneticstudies have linked BPD with a monoamineoxidase allele and with 5-HT transporter poly-morphisms (Ni et al., 2009).
Histrionic personality disorder overlapswith BPD, but is over-represented in females.Some imply that this is gender stereotyping,or that it is merely the feminine counterpart ofmale antisocial personality disorder. There areno adequate studies of the genetics, but usingthe Dissociative Experiences Scale (DES) Janget al. (1998) reported additive genetic influencesaccounting for 48% and 55% of the variancemeasuring pathological and nonpathologicaldissociative experiences respectively. Heritabil-ity estimates did not differ by gender. Thegenetic correlation between these measureswas estimated at 0.91, suggesting commongenetic factors underlying pathological andnonpathological dissociative states. Genetic andenvironmental correlations between the DES

120 Biological Psychiatry
scales and measures of personality disordertraits (Dimensional Assessment of PersonalityPathology: Basic Questionnaire) were alsoestimated (Livesley and Jang, 2008). Significantgenetic correlations were found betweenthe DES scales and cognitive dysregulation,affective lability and suspiciousness, suggestingthat the genetic factors underlying particularaspects of personality disorder also influencedissociative capacity. This same group reportedthat 45% of the variance for the trait narcissismcould be explained genetically, an even higherfigure being given by Torgersen (2000).
Chromosomal Abnormalities
Some further evidence for a contribution ofgenetic factors to personality developmentderives from patients with chromosomal abnor-malities. The contention that patients with tri-somy 21 (mongolism) or a translocation variantare friendly and jovial is hard to evaluate,especially in the presence of learning disability.
People with Y chromosome abnormalities,notably XYY males, tend to be taller thannormals, are overrepresented in prison pop-ulations and show poor impulse control andaggressivity. They have difficulty interpretingemotional expressions of others. Neither heightnor socioeconomic class explained such obser-vations (Dorus, 1980). Other studies, of patientswith variability in length of the Y chromosome,although supportive of an association withexcessive criminality and aggression, are notconclusive (Dorus, 1980). XYY males show anexcess of neurological problems, including EEGabnormalities, mild to moderate ventricularenlargement on pneumoencephalography,a tendency to clumsiness, incoordinationand hyperacrivity, and occasionally epilepsy(Hakola and Iivanainen, 1978).
In comparison, disorders of the X chromo-some present different behavioural profiles.Klinefelter’s syndrome (XXY) is linked withhyposexuality, sexual deviancy, lack of self-assertiveness and immaturity. Puberty is oftendelayed and developmental language defectsare common (Money, 1975; Walzer et al., 1978).There are smaller amygdala volumes on MRI.
In contrast, lack of one X chromosome inTurner’s syndrome (XO) leads to a specificvulnerability for visuoconstructive cognitivedeficits, and patients are reported to bephlegmatic, showing an inertia of emotionalarousal (Money, 1975). Recent studies haveshown that Turner’s syndrome females havedifficulty processing emotional information andidentifying emotional expressions, but mainlyfrom the eye regions of the face. They havebeen reported to have increased amygdala andorbitofrontal cortical size bilaterally, and lossof the normal correlation between the fusiform(face recognition) cortex and the left amygdalawhen presented with facial expressions of fearand anger (Skuse, 2006, 2007). The clinicalfindings and the more recent brain-imagingstudies thus suggest that different chromosomalaberrations lead to differing personality pro-files; the amygdala seems especially involvedin this research. Some authors have implieda specific link between the development ofthis structure and the X chromosome; loosely,the volume of the amygdala is inverse to thenumber of X chromosomes (Aleman et al., 2008;van Rijin et al., 2008).
Genetic Alleles
The new genetic studies have looked atassociations between specific gene allelesand temperament. Early studies suggestinglinks between the short version of the 5-HTtransporter promotor (5-HTTLPR) and anxietyhave not been well replicated, although it hasbeen associated with suicidality. Several studiespoint to a role of 5-HT transporter promoterpolymorphism (s allele carriers) in amygdalaactivation during emotion perception, account-ing for up to 10% of the phenotypic variance(Aleman et al., 2008). Other relevant findingsinclude reduced anterior cingulate–amygdalacoupling (s allele) (Pezawas et al., 2005) andaltered amygdala–ventromedial prefrontalcortex coupling, which might imply geneticliabilities in s allele carriers to emotionaldysregulation in settings of stress. Rhodes et al.(2007) have recently reported in a combinedPET/MRI investigation a negative correlation

Personality Disorders 121
between 5-HTT (transporter) availability andamygdala activity, further implicating 5-HTin amygdala reactivity. Other polymorphisms(e.g. the COMT val/met polymorphism, andvariants of the tryptophan hydroxylase gene)may also be implicated, although as yetresults are inconsistent (Aleman et al., 2008).Meyer-Lindenberg et al. (2006) reported thatlow activity of a variant of the MAOA gene(associated with antisocial, including aggres-sive, behaviour) was correlated with increasedamygdala arousal to emotional stimuli. Asnoted above, novelty seeking has been associ-ated with dopamine-related genes (transporter:DAT 1; receptor: DRD4) (Sabol et al., 1999).Some investigators have reported complexinteractions between personality types, such asnovelty seeking, and several polymorphisms,such as the dopamine receptor (DRD4), the5-HT transporter promotor region 5-HTTLPRand catechol O-methyltransferase (Sabol et al.,1999). Such studies are in their infancy, but areseeking to find associations between geneticpolymorphisms, certain personality variablesand eventually activation of cerebral circuitry.
Another interesting area of current researchinvolves CLOCK genes, which are involved incircadian rhythm regulation and sleep needs(von Schantz, 2008). Different polymorphismsare associated with different needs for sleepand the amount that people ‘fidget’. Most inter-estingly, they may be linked to, or moderate,bipolar disorder (Benedetti et al., 2008; Imbesiet al., 2009).
It may be concluded, as it was by Slaterand Roth (1969), that ‘heredity factors play animportant role in the development of personal-ity’ (p. 68).
SOMATIC VARIABLES
In the past, measurement of bodily featuresrelating to personality types was fashionable.An early enthusiast was Cesare Lombroso(1836–1909), who identified types, notablycriminals, by their physiognomy. To ourknowledge this interesting line of investigationpetered out, but perhaps it has found renewedinitiative, albeit in a far more sophisticated
fashion, with brain imaging – looking atbrains instead of scalps and facial features.Weinstein et al. (1999) reported that schizotypalpersonality-disorder patients showed moreminor physical anomalies and dermatoglyphicasymmetries than a normal group, raising com-parisons with similar findings in schizophrenia(see Chapter 7). Yang et al. (2008) have reportedan increase in minor physical abnormalities insociopathy. ‘Minor physical anomalies’ refers todysmorphic features such as subtle deviationsof facial structure, finger length and minorearlobe changes such as a Darwin’s tubercle.
METABOLIC AND BIOCHEMICALFINDINGS
Platelet MAO Activity
One of the peripheral markers that has beenstudied in personality disorders is platelet MAOactivity. This is thought to reflect central brainMAO activity, to some degree, and is readilystudied. The enzyme MAOB is present in humanplatelets, and its activity, and that of centralMAO, is thought to be under genetic control,although the mechanism of the inheritance isnot clear. Levels are relatively stable over time,with a tendency to increase with advancing age.
It has been suggested that reduced plateletMAO may represent a marker of genetic vul-nerability for psychopathology (Murphy et al.,1974). In non-patient studies, there is an associ-ation between platelet MAOB activity and per-sonality variables. Murphy et al. (1977) noted aninverse relationship with higher MMPI scores,and higher ratings on a sensation-seeking scalein men only. Plasma amine oxidase activity helda similar relationship, while another enzyme,dopamine beta hydroxylase, showed no corre-lation to personality scales. Volunteers with thelowest MAO activity had elevation of most ofthe MMPI subscales, showing profiles similar topatients with psychiatric illness and low MAOactivity. Comparable data are reported by others(Fowler et al., 1980; Schooler et al., 1978), empha-sizing the association, in particular, betweenlow MAO activity in platelets and sensation-seeking, the correlations to extraversion on the

122 Biological Psychiatry
EPI, for example, being much weaker (Orelandet al., 1984).
Other studies indicate that children with lowplatelet MAO activity are more active at birthand are more likely to display neurotic traitsin early childhood and that adults with lowplatelet MAO are more likely to be impulsive,monotony avoiders and aggressive. Buchsbaumet al. (1976) noted those with low platelet MAOhave more psychiatric contacts, attempt suicidemore frequently, have a higher family incidenceof psychopathology, have a greater number ofconvictions and use illicit drugs more than thosewith high MAO activity.
In animals, a correlation between low MAOactivity and brain 5-HT and its metabolites isreported, notably in a strain of mouse with highanxiety, irritability and aggression (Orelandet al., 1984), and in primates, low MAO plateletactivity relates to exploratory sensation-seekingactivity. Biochemically, the relationship to5-HT activity in the brain, confirmed in humanautopsy material (Adolfsson et al., 1978),suggests that, while in no way being a specificmarker for any personality type, plateletMAO activity, especially MAOB, may indicatevulnerabilities to certain personality attributesand psychiatric illness. In one follow-up studyof low-MAO subjects, Coursey et al. (1982)reported that they had more psychopathologyand job instability than high-MAO counterparts,and Perris et al. (1984) noted that low-MAO sub-jects reported less life events prior to the devel-opment of depressive disorders than others.
CSF 5-HIAA
There are several studies showing relationshipsbetween aggressive, violent or impulsivebehaviour and lower levels of 5-HIAA inthe CSF. In patients, aggression scores arecorrelated negatively with the metabolite level,and a less significant but positive correlationhas been noted for MHPG (Brown et al., 1979).Low 5-HIAA seems to be associated with ahistory of suicide attempts, especially by violentmeans (Brown et al., 1982), and to be lower inincarcerated murderers and those convicted of
homicide compared with controls (Linnoila andMartin, 1983). The literature on links between 5-HT and depression (see Chapter 8) is paralleledby these studies linking suicide to low 5-HTturnover. Indeed, this relationship has beenobserved many times, and is one of the mostreplicated in the whole of biological psychiatry.Patients with low 5-HT turnover are more likelyto die from suicide at follow-up, and similarbiochemical findings are noted in impulsivealcoholic offenders and people with aggressivepersonality disorders without depression. Inpost mortem samples of brains from those whohave committed violent suicide, 5-HT levels areinterpreted as low (Stanley and Mann, 1983).Thus, the low 5-HT release relates not only todepressed affect but also to aggression, impul-sivity and suicidal behaviours. Stanley et al.(2000) have reconfirmed the link between hos-tility, aggression and low 5-HT concentrations,to the extent of noting an inverse relationshipbetween the 5-HT levels and measures takenof aggression (Sher et al., 2006; Stanley et al.,2000). These clinical data receive substantialsupport from investigations of rodents whichlink low 5-HT with enhanced aggression, andof nonhuman primates, in which reducedamounts of 5-HT are associated with severeforms of aggression and a greater frequency ofhigh-risk behaviour (Mehlman et al., 1994). Onehypothesis put forward to explain this suggeststhat the 5-HT link to aggression is mediated vianeuronal excitability in the amygdala. In thismodel, 5-HT is viewed as an activating systemfor inhibiting behaviour, which is impairedwhen 5-HT levels are low (Keele, 2005).
Impulsivity is one feature shown by many ofthese patients, suggesting an association withthe personality attributes noted with low MAOlevels reported above. A further link betweenthe studies is that alcoholism itself is associatedwith low platelet MAO levels (Oreland et al.,1984) and abstinent alcoholics also have low 5-HIAA CSF levels (Ballenger et al., 1979; Linnoilaand Martin, 1983); impulsive aggression andlifetime aggression in such subjects are relatedto the low 5-HIAA.

Personality Disorders 123
More recent work on this association hasconfirmed the link between hostility, aggressionand low 5-HT concentrations, to the extent ofnoting an inverse relationship between 5-HIAAlevels and the measures taken of aggression(Stanley et al., 2000).
Coccaro et al. (1994) have investigated famil-ial relationships. Thus, reduced 5-HIAA in theCSF is associated with a family history of depres-sion in healthy probands and a family history ofalcoholism in depressed patients. They reportedthat the prolactin response to a fenfluraminechallenge (which releases 5-HT and prolactin)was blunted in association with an increasedrisk of impulsive personality disorder traits infirst-degree relatives of patients with a DSM IIIdiagnosis of personality disorder.
These data are compatible with some ofthe animal data, and emphasize the relation-ship of 5-HT and its metabolites to certainaspects of human behaviour. The genetic evi-dence and the links to MAO activity suggest thatsome personality variables, notably impulsivity,sensation-seeking, aggressiveness and prone-ness to alcoholism, have biochemical correlates,notably with the serotonergic system and itsregulation through MAO.
NEUROPHYSIOLOGICALAND NEUROLOGICAL DATA
Psychophysiological (autonomic) underarousal,as indicated by reduced resting heart rate andskin conductance levels and poor classicalconditioning, is one of the most replicatedfindings in antisocial populations (Glenn andRaine, 2008; Raine et al., 1994). Autonomicunderarousal can be shown in infants andyoung children with a disinhibited tempera-ment that suggests a predisposition to juveniledelinquency and adult aggressive behaviour.Psychophysiological measures, taken at the ageof 15 years, have been related to criminalityassessed at a later age (24 years). Thus crimi-nality is somehow associated with autonomicunderarousal, and the differences are not medi-ated by social, demographic or educationalfactors (Baker et al., 2007, 2008; Yang et al., 2008).
EEG
The frequency of EEG abnormalities in patientsreferred to as aggressive or psychopathic wasestablished long ago (Hill, 1952). In particular,bilateral theta activity in temporal and cen-tral regions was reported. These data werereinforced by Williams (1969), whose studiesrevealed a far higher incidence of abnormalEEGs in aggressive psychopaths than in individ-uals selected for stability, such as flying person-nel, and by Stafford-Clarke and Taylor (1949),who found over 70% of motiveless murderers tohave abnormalities. Monroe (1970), reporting on70 psychiatric patients, noted, with activation,that those who demonstrated high-amplitudeparoxysmal slow waves were more likely tobe seriously aggressive to themselves or others.Patients diagnosed as suffering from episodicdyscontrol frequently have EEG abnormalities,again the majority being temporal lobe in origin(Bach et al., 1971), and higher levels of violencehave been reported with left-focal abnormali-ties (Pillmann et al., 1999; Shelley et al., 2008).One interesting feature of these studies is thata normal EEG reflected on good personalitystructure, with a suggestion that cerebral dys-rythmias may impede the natural process ofpsychological maturation (Shelley et al., 2008).
These data are supplemented by observa-tions that psychiatric patients with no history ofepilepsy but a temporal lobe focus on the EEGare more likely to be aggressive (Treffert, 1964;Tucker et al., 1965), and by depth-electrodestudies, which indicate that feelings of dyscon-trol and rage are primarily associated withdischarges in the amygdala and hippocampusin both epileptic and non-epileptic patients(Heath, 1982).
In a more systematic study of the behaviouralcorrelates of rhythmic midtemporal discharge,an abnormality frequently associated withpsychopathology, Hughes and Hermann (1984)noted a relationship between the frequency ofsuch discharges and abnormal MMPI profiles.Further, patients with BPD have a high fre-quency (46%) of EEG abnormalities, includingnonfocal spike- or sharp-wave activity, diffuse

124 Biological Psychiatry
slowing and, on occasions, posterior temporalspike-wave discharges (Cowdry et al., 1986).
These data suggest links between cerebraldysrhythmia and certain personality features,and the emphasis is on impulsive aggressivebehaviour. The association is particularly withposterior, often bilateral, temporal paroxysmaldischarges. The aetiology of the dysrhythmiasis unclear, but may reflect maturational fac-tors, possibly genetically determined, earlierbrain damage or a functional disturbance ofbrainstem–limbic system structures.
Evoked potential studies have also been car-ried out, although attempts to correlate changesto personality variables have not been reliablyreproduced (Shagass, 1972). The CNV has beenshown to be of higher amplitude in two studiesof psychopathic patients (Howard et al., 1984),although the meaning of this is unclear. In‘go’/‘no-go’ tasks indicating response inhibi-tion, the differential frontal negative potentialrecorded at 400 ms between the two trials isdiminished in psychopaths (Kiehl et al., 2000;Shane et al., 2008). In odd-ball stimulus detectiontasks, psychopaths show larger fronto-centralnegative waves (N550) during target detectionthan nonpsychopaths.
Early childhood abuse, stress and lifetimeassaultative violence have been linked to elec-trophysiological abnormalities. Thus an increasein fronto-temporal EEG abnormalities with anemphasis on the left side has been reported inabused children, and dysrhythmic abnormal-ities have been noted in 77% of those withincestuous relationships (Ito et al., 1998).
Neurological Disorders
Substantial evidence that personality and thebrain are closely entwined stems from observa-tions of patients with various neurological con-ditions or who have suffered trauma to selectedregions of the brain. Generally, any brain lesionmay disrupt personality, and some authors referto an ‘organic personality change’ (Lishman,1987). This includes irritability and restlessness,lassitude, poor concentration, loss of initiativeand excessive emotionality. There may be poortolerance for change, withdrawal, insecurity and
anxiety. With more severe damage, extremesof this picture are seen, with social disorga-nization, loss of interest in the self, explosiveirritability, shallowness of affect and a bluntingof emotional responses. In such situations, anexacerbation of pre-existing personality traitsis seen, for example aggressive people exhibit-ing outbursts of anger, and perhaps violence,with minimal provocation. While many of thesefeatures are nonspecific, their recognition isimportant.
The most direct evidence that the brainis intimately involved in the structure of thepersonality comes from the observations onpatients with frontal-lobe damage. This hasbeen discussed in Chapter 3, where the mainelements of the frontal-lobe syndromes havebeen presented. These include reduced activity,lack of drive, loss of appropriate affect withindifference and blunting, inability to planappropriately, impulsivity with irritabilityand aggression, and marked impairment ofrelationships with others. One recognized formof this has been termed ‘pseudopsychopathic’,reflecting the similarity of the behaviour to thatform of personality disorder.
In contrast, changes of personality related totemporal-lobe pathology are different. The rela-tionship between temporal-lobe pathology andpersonality change is noted in Chapter 3, andthe subject of personality disorders in relationto epilepsy is discussed in Chapter 10, wherethe arguments in favour of a ‘temporal-lobesyndrome’ and the relation to aggression arerehearsed. The noted association between per-sonality disorders and epilepsy crystallized withthe introduction of the EEG, which led to a fullerunderstanding and identification of temporal-lobe epilepsy. It was suggested that patientswith such an origin of their seizures were morelikely to show personality changes. Such clinicalinformation seemed in keeping with the grow-ing literature on the role of the temporal lobes inanimal behaviour, in particular the descriptionof the Kluver–Bucy syndrome. Alterations ofaggressive potential, affective tone and motoriclife were a part of the syndrome, and havebeen described in association with other limbic-system conditions where the burden of the

Personality Disorders 125
pathology is in the temporal lobes, such asencephalitis.
The interictal behaviour syndrome oftemporal-lobe epilepsy emphasizes alterationsin sexual behaviour, hyperreligiosity andhypergraphia, namely the tendency towardsextensive and often compulsive writing(Waxman and Geschwind, 1975). In somepatients the syndrome appeared before anyseizures, and when present, even in the absenceof further evidence, might suggest dysfunctionat this specific anatomical site. They contrastedthis picture both with the frontal-lobe syndromeand with the Kluver–Bucy syndrome, havingsome characteristics almost opposite to thelatter. The religiosity, the excessive interest inthe cosmic and supernatural, the conviction thatthe person has some special significance in theworld or some messianic mission, the meticu-lous attention to detail, the hypergraphia (withdetailed accounts of events being recorded,often with a moral or religious theme), thedisturbed sexuality, are all features of the fullsyndrome. Waxman and Geschwind suggestedthis related to ongoing interictal abnormalelectrical activity in the limbic system, a themetaken up by Bear and Fedio (1977). In theirstudies of patients with temporal-lobe epilepsy,using a behavioural rating scale constructedfrom literature descriptions of abnormalitiesrecorded in association with the condition, theyreported that many items correlated with thelength of seizure history. Their interpretationof the findings was that the epileptic focussomehow led to enhanced associations betweenaffect and stimuli, a so-called ‘functionalhyperconnection’ (p. 465) between neocorticaland limbic structures, possibly inhibiting eventsthat normally prevent fortuitous sensory andaffective connections. This can be seen asthe opposite of the Kluver–Bucy syndrome.In the latter the limbic dysfunction leads tofailure to attribute stimuli their appropriateemotional significance, with hypermetamor-phosis, emotional blunting, diminished fear andaggression, and inappropriate sexual behaviour(limbic agnosia).
The above data reinforce the crucial impor-tance of temporal-lobe epilepsy in unravelling
the neurological basis of personality, with a piv-otal role of the limbic system and related struc-tures in determining personality dispositions.
Radiological Studies
Brain-imaging studies have contributed sig-nificantly to studies of personality disorders,although most of the data has been carried out inantisocial and borderline personality disorder.
With regards to BPD, initial CT studiesyielded no useful information. Driessen et al.(2000) studied 21 female patients with BPDand a similar group of healthy controls usingthe Childhood Trauma Questionnaire and MRIvolumetric measurements. They reported thatin comparison with controls, the personalitydisorders had bilaterally smaller amygdala andhippocampal volumes. The volumes of thehippocampus were negatively correlated withthe extent and the duration of self-reportedearly trauma (Brunner et al., 2009; Tajima et al.,2009; Whittle et al., 2009; Zanetti et al., 2007).Herpertz et al. (2001) have shown with fMRIthat the amygdala of females with borderlinepersonality is more reactive when viewingaversive emotional pictures (increased BOLDsignal bilaterally). There is also increased signalfrom the fusiform gyrus. One study usingproton spectroscopy has shown reduced NAAlevels in the left dorsolateral prefrontal cortexin borderline patients (Tebartz van Elste, 2003).
Functional imaging with PET has not shownconsistent results, although the most frequentlyreported finding is decreased activity indorsolateral prefrontal cortex. Examining thehypothesis that impulsivity and aggressivityare linked with the borderline profile, Soloffet al. (2000) gave fenfluramine challenge (5-HT-releasing compound) and compared theresults to placebo (Soloff et al., 2000). Uptake ofFDG with fenfluramine was greater in controlscompared with patients in prefrontal cortex,including medial and orbital regions bilaterally(BA 10–11), left superior temporal gyrus andright insular cortex. In a later study, againwith PET but with a 5-HT receptor ligand(18F-altanserin), Soloff et al. (2007) reportedincreased binding in the hippocampus in BPD.

126 Biological Psychiatry
Most recently investigators have used fMRI,with a variety of innovative activation tasks, totry and understand the brain deficits in BPD.To date, investigators have asked BPD patientsto remember painful life events (Buchheim et al.,2008; Vollm et al., 2007), react to emotional faces(Minzenberg et al., 2007; Wingenfeld et al., 2008)or attempt to bond or self-sooth (Driessen et al.,2008; Silbersweig et al., 2007; Vollm et al., 2007).
Interpreting these data is difficult. The stud-ies are done on small numbers, and severalhave used only female patients. However, thereis evidence of fronto-limbic dysfunction withalteration of amygdala size and function in bor-derline patients. The increased amygdala andassociated fusiform gyrus activation, the lat-ter of which processes complex facial stimuli,might imply an increased reactivity to emo-tional events, and the smaller hippocampi couldlink with similar findings in some disorders,including depression and post-traumatic stressdisorder (see Chapters 6 and 8).
With regards to antisocial personalitydisorder, Raine et al. (1994) have reporteda series of studies examining functional andstructural brain correlates. In an early PET studythey reported that murderers have reducedmetabolism in the lateral and medial prefrontalcortex compared with controls, and thenshowed that the findings applied to murdererswho had no early psychosocial deprivation(i.e. no childhood abuse, family neglect). Thisgroup have also shown an 11% reduction inprefrontal grey-matter volume in the absence ofobserved brain lesions in psychopathic antiso-cial individuals compared with controls (Raineet al., 2000). They also observed in antisocialsubjects a 23% increase in estimated callosalwhite-matter volume, a 7% increase in callosallength, a 15% reduction in callosal thickness,and increased functional inter-hemisphericconnectivity. These deficits predicted groupmembership independent of psychosocialrisk factors. Unsuccessful psychopaths (oneswho get caught!) in their studies have a 22%reduction in prefrontal grey-matter volumecompared with those deemed successful, buton ratings, higher total as well as subfactor psy-chopathy scores (arrogant/deceptive, affective
and impulsive/unstable) were all associatedwith low prefrontal grey volume (Yang et al.,2008, 2009). In a recent meta-analysis ofimaging data and other variables found inpsychopathy, Raine has reported decreasedfrontal cortical size (especially orbital andmiddle prefrontal gyrus) (Figure 5.1), greatestin violent psychopaths, higher rates of cavumseptum pellucidum, and a decreased amygdalasize of 17% (Yang et al., 2008).
These studies seem concordant with otherevidence from neurological patients, EEG stud-ies and neuropsychology (see below) that brain
Figure 5.1 Coronal MRI scan showing the seedingpoints in a study by Raine and colleagues, who exam-ined MRI-defined prefrontal white and grey matter insubjects with antisocial personality disorder, healthyage- and gender-matched controls, and controls withmatched substance abuse. The antisocial-personality-disorder group had markedly smaller prefrontalgrey-matter volumes (Raine and Yang, 2006; Yanget al., 2005a, 2005b, 2007) (reproduced with permis-sion from Raine et al., 2000). A coloured version ofthis figure can be found on the colour plate

Personality Disorders 127
structural deficits are found in those referredto as psychopaths or who have antisocialbehaviour disorders, and that the burden ofthe abnormalitiy is largely prefrontal. Thecorpus-callosal findings suggest this may bedevelopmental. Raine suggests that these brainstructural abnormalities may underlie the lowarousal, poor fear conditioning, lack of con-science and decision-making deficits that havebeen found to characterize antisocial, psycho-pathic behaviour. Although these differencesemerge in many group studies of antisocial per-sonality subjects, it is unclear how they shouldbe used in forensics or whether they might rep-resent endophenotypes or biological markers(Raine et al., 1994; Raine and Yang, 2006). It isalso particularly unclear whether brain-imagingstudies help establish an individual diagnosis.
There are few studies of cerebral imagingin other personality types. Raine et al. (2002)looked at patients with schizotypal/paranoidpersonalities and reported reduced prefrontalgrey volumes and poorer frontal functioningon frontal neuropsychological tasks comparedto controls, although they discussed this morein the context of the findings in schizophreniathan in the context of personality disorders.There are some imaging findings in schizotypalpersonality disorder, discussed in Chapter 7.
Neuropsychological Findings
Ruocco (2005) carried out a meta-analysis ofthe neuropsychological data of patients withborderline personalities and reported that, incomparison with healthy comparison groups,on selected neuropsychological tests of atten-tion, cognitive flexibility, learning and memory,planning, speed of processing, and visuospa-tial abilities, the borderline patients did worseacross all neuropsychological domains. Therewas a suggestion that these deficits were morestrongly lateralized to the right hemisphere.
There are several studies of neuropsycho-logical performance in psychopaths, who alsoshow quite diffuse neuropsychological deficits.Meta-analysis particularly implicates deficits offrontal tasks. Impairments on dorsolateral pre-frontal executive function tasks of planning
ability and set shifting have been shown, aswell as on tasks such as the ‘go’/‘no go’, whichsuggest ventromedial prefrontal deficits (Yanget al., 2008).
SOME OUTSTANDING ISSUES
It seems to be the case that in comparisonwith the affective disorders or the schizophre-nias, investigation of the personality disordershas been relatively neglected, certainly froma neurobiological perspective. There are sev-eral reasons for this, including difficulty withthe overall concept, problems with definitionsof any subtypes, a debate about the statisticalas opposed to the unitary nature of individualtypes, and disagreement about when a personal-ity disposition becomes a disorder. For example,why is psychopathy diagnosed more in malesand histrionic personality identified more infemales? Is it simply a matter of cultural bias, oris it related to hormonal, genetic and other bio-logical variables? Added to these are the linesthat are drawn between personality disorder(DSM IV axis 2) and any comorbid isomorph(axis 1). It may be that with the next editionsof the diagnostic manuals some of these issueswill be resolved, especially if biological markerscan be identified which help differentiation. Inview of the distress which certain personalitytypes bring to themselves, and also to society,much more work with personality disorders ofall dimensions would seem a priority (Hiller andFichter, 2004; Soeteman et al., 2008; van Asseltet al., 2007).
There are other reasons why research in theseareas lags behind the volume of work in the restof biological psychiatry. First, it is most difficultto parse out whether a biological change (e.g.lack of regional brain volume) is fundamental toa personality disorder or arises from living a lifewith the behaviour flowing from the personalitydisorder. For example, an antisocial personalitypatient engages in impulsive behaviour, whichleads to a head injury, which damages theorbitofrontal or prefrontal cortex, which thenresults in even more impulsive behaviour. Andthe cycle continues.

128 Biological Psychiatry
Second, some researchers and funding orga-nizations are concerned about asking about thegenetic underpinnings of personality as this getsuncomfortably close to issues of genetic deter-minism and even eugenics. Nevertheless, thesearch for genetic, epigenetic and endopheno-typic variables underlying behaviour and itsdisorders is a central aspect of modern biologicalpsychiatry research.
There seem to be clear associations, andperhaps similar neurobiological underpin-nings, between some cluster A variables(especially schizotypal personality disorder)and schizophrenia, but the true nature of thisrelationship is unknown. Nonetheless, this isof more than theoretical significance: it haspreventative and treatment implications. It isnot known at what age schizotypal personalitydisorder begins to reveal itself, or what might bethe potential factors that aid or protect againstthe glide of the mental state to psychosis. Thesame may be said for other associations, suchas anankastic tendencies and OCD, or even thepersonality profiles that increase the risk formajor depressive disorder.
In classical descriptions of personality thereis a tendency to imply that personalities (asopposed to illnesses) are stable over time.A person’s personality is biologically derivedthrough genetic and epigenetic factors, butmatures sometime in the mid to late teens,although any parent will note personalityfeatures in their children from a much youngerage (even within the uterus before birth?). Thereare few long-term follow-ups of personalitydisorders, but many individuals with antisocialpersonality disorder seem to ‘mature’ with age,usually by about 40. It is not clear whetherthis relates to myelination of cerebral pathways(unlikely), or to some enrichment of lifestylethat may accrue with some social success, orsimply to a ‘burn out’ and a wish to spend lesstime in prison or alone. However, some forms ofpsychopathic behaviour seem to be integratedwithin an individual’s biological and neuro-logical makeup, and the neurophysiologicaland brain-imaging data reviewed above seemcrucial to understanding the pervasive and per-sistent nature of the behaviours. Recall above
how the opposite sometimes occurs, when mildpersonality traits seen throughout a lifetimebecome more florid later in life, associated witha dementia or other disease process.
There is much evidence that personalityand its variants have a strong genetic basis,and yet this has hardly been a subject of muchdiscussion outside of small interested groups,and the implications are carefully avoided.Interactions between genetic endowmentand environmental influences need parsingout much more carefully than has been thecase up until now, especially with the vastimprovement that has occurred with the newgenetic studies. Measuring the sociologicalvariables lags far behind the modern precisionof measuring genetic markers. A good exampleis the difficulty in adult patients of determiningaccurately the amount of childhood physicalor sexual abuse. Nevertheless, much behaviourwhich has been assumed to be environmentallydriven seems to have a stronger genetic basisthan is generally credited (witness the datafor antisocial personality disorder). This entirearea becomes more complicated because anindividual with a genetic bias for a personalitytype will then often grow up in an environmentwith parents who also express these tendencies;the dysfunctional family will interact with thegenetics, further changing behaviour (Hewittet al., 1997; Moffitt et al., 2005; Rutter, 1994;Rutter and McGuffin, 2004). These are referredto as gene–environment interactions and theybecome enormously complex with respect tobehaviours that can persist through severalgenerations. Meaney and colleagues havedeveloped animal models of parenting in rats,selecting for mothers who lick and groom theirpups. One can select for good mothers, andthen subject the pups to early life stressorsby temporarily taking them away from themother (separation). This early separation canthen make the adult rat have a lifelong ‘anxietydisorder.’ However, when the pup is returnedfrom the separation the mother tends to lickand groom it, and a good mother can almostundo the stress of the separation, which is thentransmitted in a protective way to the nextgeneration. Postweaning isolation or separation

Personality Disorders 129
reduced exploratory behaviour in the offspringof high-licking and grooming mothers, whereassocial enrichment enhanced exploration oflow-licking and grooming offspring (Cameronet al., 2008; Champagne and Meaney, 2007;Champagne et al., 2008; Szyf et al., 2008). Inter-estingly, these effects were also transmittedto the next generation of offspring. Thus,maternal licking and grooming exhibited ahigh degree of plasticity in response to changesin environment beyond the postnatal period,which then transmitted a behavioural responseto novelty and maternal care across generations.
Many features that we subsume underthe term ‘personality’ would seem to bemore closely associated with non-isocorticalstructures, because affective tone is set more bythe limbic lobe and its connectivity than by theisocortex. However, cortical structures modu-late and interact with limbic regions to regulate
behaviour and personality. The studies combin-ing brain imaging and genetics are beginning toshow close associations between some person-ality variables and monamine levels, especially5-HT regulation and neuroanatomy, notably theamygdala and its intimate connectivity. Will, asa behavioural domain, and its relationship tobehavioural dispositions and to tendencies toact (motion) in one direction or another, derivefrom extraconscious limbic and subcorticalactivity. These ideas link to such fundamentalsocial behaviours as empathy (being moved),and how close it is possible to get to another(moving). The frontal–subcortical axis is notonly central to many behavioural disorders butdetermines these personality propensities, justas the temporal–subcortical axis reflects on ouremotional harmonies (emotion), and togetherthey allow for not only fear and despondencybut also creativity and joy.


6Anxiety Disorders
INTRODUCTION
Historically, and from a clinical point of view,there are close links between the anxiety disor-ders and personality disorders (see Chapter 5).The term ‘neurosis’, originally introduced as asynonym for nervous diseases, was abandonedby DSM III and its successors, and terms such as‘reactive’ and ‘neurotic depression’ have fallenout of fashion. The blurred boundary betweenthe personality disorders and the neuroses wascleaved by DSM III and the divisions betweenaxis 1 and axis 2 disorders.
In anxiety disorders, the predominantsymptom is anxiety not associated with anotherpsychiatric disorder. In DSM IV-TR, the fol-lowing subcategories are given, with their ICDequivalents in brackets: agoraphobia withoutpanic disorder (agoraphobia), social phobia(social phobia), specific phobias (isolatedphobia), panic attack, panic disorder with orwithout agoraphobia (panic disorder) and gen-eralized anxiety disorder (generalized anxietydisorder). ICD 10 has also mixed anxiety anddepressive disorder as subcategories, whileDSM IV-TR has anxiety disorder due to ageneral medical condition, substance-inducedanxiety disorder and anxiety disorder nototherwise specified (NOS).
Obsessive–compulsive disorder (obsessive–compulsive disorder, OCD), and reactions tosevere stress and adjustment disorders are theother two main groupings. Post-traumatic stress
Biological Psychiatry 3e Michael R. Trimble and Mark S. George 2010 John Wiley & Sons, Ltd
disorder (post-traumatic stress disorder, PTSD)is included under the latter. ICD 10 has a subcat-egory of acute stress reaction, with symptomslasting only a few days. The equivalent in DSMIV, acute stress disorder, with symptoms verysimilar to post-traumatic stress disorder, can lastup to four weeks.
This listing and lumping of the different dis-orders is somewhat confusing and unsatisfying.Recall the review of the anatomy of fear andanxiety in Chapter 3.
Both the amygdala and the hippocampusare involved, and there may be a distinctionbetween the neuroanatomy of fear and anxiety.Fear relates more to interactions between pri-mary sensory processing areas such as thethalamus and the amygdala. Hippocampalinputs to the amygdala contribute cognitiveinformation as well as a link to cortical struc-tures and memory, leading to anticipatory andmore global anxiety (see Figures 2.16 and 6.1).Flowing from this anatomy, it thus makes senseto categorize generalized anxiety disorder andpanic disorder as conditions that arise fromhardwired fear and anxiety circuitry. Fear ofpotentially harmful events or stimuli obviouslyhas important survival value. The specific pho-bias, including social phobia, also belong withinthis grouping of fear and anxiety. PTSD can beseen as an overreaction of this circuitry, in apathological manner which then feeds forwardin a destructive way, leading to avoidance

132 Biological Psychiatry
Emotionalstimulus
Quickanddirty
Thalamus
Slowand
accurate
Amygdala
Sensorycortex
Figure 6.1 Diagram of fear circuitry. In contrast togeneral anxiety, fear neuroanatomy arises in responseto an external threat (shown as an emotional stim-ulus). This information goes through the LGN ofthe thalamus for visual information. There are thentwo pathways: a slow and accurate pathway, whichinvolves normal cortical evaluation of the threat, anda quick and dirty pathway, which sends informationdirectly to the amygdala for certain threats that havelikely had evolutionary importance, such as fearful orthreatening human faces, or snakes and large preda-tors (reproduced with permission from Higgins andGeorge, 2007)
behaviours and social withdrawal. But like theother anxiety disorders, PTSD likely arises froma common neural substrate involving fear andanxiety regulation. The one condition that doesnot appear to belong in this category, reasoningfrom the underlying anatomy as well as fromthe clinical descriptions and symptoms, is OCD.In OCD, anxiety is secondary to the persistentthoughts (obsessions) or an inability to performcompulsions, or both. The anxiety is not aprimary motivator. Moreover, the underlyingneuroanatomy is distinct, as is discussed below.OCD will therefore be discussed separately, butwithin this chapter, as is PTSD, on account of itsconceptual importance but also the controversyit has occasioned.
The phobic disorders reflect persistent andirrational fears resulting in avoidance behavi-our. Phobias as such are extremely common,although in the majority they are not disabling.
Simple phobias include fear of spiders, snakes,thunderstorms, flying, subways, needlesand animals. These are usually less sociallyincapacitating than agoraphobia, which ischaracterized by a fear of going into crowdedplaces, often combined with a fear of beingalone. In this condition, individuals graduallyrestrict their activities, until, in its most floridform, they become housebound. They use manytechniques to avoid going out, and if they haveto venture outside it is invariably with a friend,a spouse or a dog. In one form of the disorder,panic attacks occur. These may be only on goingout, or occur in places such as the supermarket(the agora), or they may arise spontaneouslyat home. This may be in relationship to thethought of going out, or on going near the frontdoor, or may suddenly come on out of theblue. Associated with the agoraphobia there isoften a history of an anxious personality anda tendency to develop affective disorder. Itshould be noted that agoraphobic symptomsoften arise in the setting of a major affectivedisorder, and in these cases the diagnosis iswith the affective disorders. Social withdrawaland isolation are hallmarks of depression, andshould be differentiated from agoraphobia inthe absence of other depression symptoms.
Social phobia is a fear of embarrassment orhumiliation in social situations, which thusbecome avoided as the individual restrictssocial contacts. There is anticipatory anxiety atthe thought of social encounters, often confinedto certain situations only, such as eating orspeaking in public.
Generally, simple phobias have a better prog-nosis than others, especially if they start inchildhood. Agoraphobia, which is commonerin women, tends to come on in the third orfourth decade of life, and may be very resistantto treatment, not the least problem being thepatient’s reluctance to leave home to attend theclinic for consultation.
In generalized anxiety disorder the patienthas anxiety of at least one month’s durationwithout phobic symptoms or panic attacks.The manifestations of anxiety are multiple,

Anxiety Disorders 133
and affect every bodily system. Further, sinceanxiety is such a common symptom, and manyof the symptoms are somatic, many patientswith anxiety disorders are misdiagnosed andinappropriately treated, sometimes for manyyears. Common symptoms include palpitations,sometimes associated with anterior chest painover the heart; dyspnea and a sense of chokingor a feeling that the patient will not be ableto take in a sufficient breath; and dry mouth,with unpleasant, often metallic tastes andabdominal tension, sometimes associated withnausea or actual vomiting. Other symptoms areconstipation or diarrhoea; retention of urineor frequency of urination; poor concentrationand memory difficulties; dizziness, vertigo,faint feelings and, on occasions, blackoutswhich resemble epileptic seizures; increasedmuscle tone with pain; tremor; fatigue andloss of energy; and sensory symptoms such astingling, especially of the hands, diminishedvision or a generalized hyperacusis in whichsounds are distorted and magnified, sometimesaccompanied by photophobia. On examination,patients with anxiety show sweating, oftenhave cold extremities, and may show flushing.The resting pulse, respiration rate and bloodpressure may be elevated and increased centralbody movement or restless hand movementswith a tremor may be noted.
Panic attacks are frequent episodes, of a dis-crete nature, of panic associated with appre-hension and fear. Their paroxysmal nature, theirsudden onset and the absence often of anyobvious precipitating factor may readily leadto a diagnosis of epilepsy. They often resem-ble one form of complex partial seizure (seeChapter 10).
A variant of this is the phobic-anxiety deperson-alization syndrome (omitted from the diagnosticmanuals), in which depersonalization or dere-alization forms a prominent part of the picture.This is a much more pervasive disorder, withgeneralized anxiety, affective symptoms and adanger of death by suicide. In some patients,between the more extreme manifestations, thedepersonalization may persist. When severe it
may lead patients to feel like automata, or asif they have left their bodies, sometimes withautoscopy. Autoscopy is when a person, whilebelieving themselves to be awake, sees theirbody and the world from a location outsidetheir self.
Post-traumatic stress disorder has a long anddistinguished history, and in the past wasreferred to as accident neurosis, compensationneurosis or some other variant (Trimble, 1981b).Many physicians come across this in a medi-colegal setting and are familiar with thearguments over the role of financial gain in theproduction or prolongation of the symptoms.The characteristic symptoms involve combi-nations of psychological re-experiencing ofa traumatic event with or without physicalaccompaniments, avoidance phenomena andpersistent symptoms of arousal.
The essential features of OCD are theobsessions – persistent ideas, thoughts orimages that invade conscious experience againstthe wishes of the patient – and compulsions –repetitive semipurposeful motor acts. Both theobsessions and the compulsions are somehowalien to the individual (ego-dystonic) and areresisted. Often the thoughts are offensive andrepugnant, and the compulsions are senselessstereotyped actions, from which no pleasure isderived, although there is often relief of tension.OCD implies the persistence of obsessionsand compulsions, in the absence of anotherpsychiatric disorder. The contents of the ritualsmost commonly found are cleaning, avoiding,repeating and checking, and some authors notethat the recognition of the senselessness of thephenomena is more relevant than resistance tothem (Stern and Cobb, 1978). Variants includethe intrusion of vivid imaginary, scenes ofunacceptable events, ruminations on trivia,convictions of a magical nature (for example,that to carry out one act will prevent another),fears of dirt, disease and contamination, andrituals of counting or performing certain actsin specific ways or in a special order. Althoughdepressive symptoms are common, it is essen-tial to distinguish whether the depression

134 Biological Psychiatry
is secondary, or whether the obsessionalsymptoms derive from a primary affectivedisorder in an anankastic personality.
GENETICS
Modern genetics in this area is tending to iden-tify endophenotypes and there is some overlapwith the genetics underlying the depressions(Merikangas and Low, 2005). Controlled familystudies reveal that all of these anxiety subtypesare familial, and twin studies suggest that thefamilial aggregation is attributable in part togenetic factors. Panic disorder and its spec-trum have the strongest magnitude of familialclustering and genetic underpinnings. Childrenof parents with anxiety disorders are at anincreased risk of developing mood and anxi-ety disorders, but there is far less specificity
of the manifestations of anxiety in childrenand young adolescents. Although there havebeen many studies designed to identify genesunderlying these conditions, to date no specificgenetic loci have been identified and repli-cated in independent samples. Several familystudies have detected a higher rate of panicdisorder in the relatives of affected probandsthan in relatives of control subjects. The relativerisk to first-degree relatives of panic-disorderprobands ranges between 2.6- and 20-fold, withone meta-analysis finding an eightfold increasein risk (Middeldorp, 2005). Twin studies haveshown a heritability of 30–60%. There are twostudies suggesting, but not proving, suscepti-bility loci (markers D4S413 (Kaabi et al., 2006),which also harbours the neuropeptide gene, andD9S271 (Thorgeirsson et al., 2003)). For OCD, thetwin studies have found a higher heritability
1.9
2.3
2.7
3.1
3.4
3.8
4.2
0.0
0.5
1.0
1.5
2.0
2.5
3.0
(a)
(c)
(b)
Figure 6.2 Genetic variation impacts key brain regions involved in anxiety, increasing vulnerability todysregulation. Shown are thresholded maps (p < 0.05) reflecting differences in grey-matter volume in 5-HTTLPR s-allele carriers compared to the l/l genotype, with medial sagital views (a) and coronal images (b)and (c) representing the statistical thresholds for the colour on the images. Note the volume reductions in theallele carriers in the bilateral perigenual anterior cingulate cortex and amygdala (reproduced from Pezawaset al., 2005). A colour version of this figure can be found on the colour plate

Anxiety Disorders 135
than panic, at 80% (Carey et al., 1980), with ashared genetic diathesis involving Gilles de laTourette’s syndrome. Hu et al. (2006) found agenetic linkage of OCD to the short variant ofthe 5-HT transporter gene. Twin studies for theother anxiety disorders again show heritability(20–40% for agoraphobia and social phobia).
As discussed above, another approach tounderstanding the genetics of a disorder is tofind an endophenotype for the behaviour andexamine whether genetic differences correlatewith differences in behavioural tendencies.Figure 6.2 shows that subjects with differencesin the 5-HT transporter (5-HTT LPR) havedifferences in grey-matter volume in theanterior cingulate and amygdala (Pezawas,2005). Moreover, an individual’s genotype forthe 5-HT transporter may also affect how theyprocess fearful stimuli and respond to stress.That is, individuals with the s genotype for the5-HT transporter may be more vulnerable tostress than those with the l genotype.
SOMATIC VARIABLES
Psychophysical variables associated with gen-eralized anxiety have been investigated, notablymonitoring autonomic activity (Lader, 1969).Lower skin conductance, more spontaneousfluctuations, increased sweating and dimin-ished habituation of autonomic indices tostimulation, monitoring such variables asblood pressure, the EMG and forearm bloodflow, have been reported. The galvanic skinresponse (GSR) is the sudden increase in skinconductance that can be observed with appro-priate stimuli, and, since it can be abolishedby atropine, it is thought to be dependent onthe activity of sweat glands. Its habituation isdelayed in those with anxiety states, the habit-uation being negatively correlated with ratingsof anxiety (Lader, 1969). Tsunoda et al. (2008)explored whether social anxiety is associatedwith preattentive emotional responses tofacial expressions. Skin conductance responsesdiffered between a group with high socialanxiety and one with low social anxiety. Theformer showed significantly greater differencesin their responses between masked fearful and
happy faces than the latter. These findingssuggest that the predisposition to social anxietyrelates to the hard fear wiring in the ‘quick anddirty’ amygdala circuit.
Abnormalities of psychophysiologicalresponses have been shown in PTSD. Trau-matized patients show increased autonomicreactions to specific stimuli related to earlierpsychological trauma. They also show failureof habituation to an acoustic startle responseand delayed extinction of fear conditioning(Blechert et al., 2007; van der Kolk, 1994).
There has been interest in an associationbetween panic disorder and mitral valve pro-lapse. The latter may present with symptomssimilar to anxiety, although the emphasis is onpalpitations and chest pain. Whether the occur-rence of the two conditions when seen togetheris coincidence, genetic or reflects some underly-ing autonomic dysfunction associated with bothis not clear.
METABOLIC AND BIOCHEMICALFINDINGS
In contrast to the affective disorders and thepsychoses, there is a dearth of informationregarding metabolic and biochemical links withthe anxiety disorders. As suggested with theabove findings, the autonomic system, and inparticular adrenaline, was a focus of interest.Normals show increased stress-related increasesin plasma catecholamines. Adrenaline infusionsprovoke somatic symptoms of anxiety or exacer-bate anxiety in anxious patients (Breggin, 1964).Further, noradrenaline stimulates the produc-tion of lactic acid and free fatty acids, both ofwhich are raised in anxiety states. Isoprenaline,a beta-receptor agonist, when infused provokestachycardia more readily in the anxious (Frolichet al., 1969).
Several groups have noted increased urinaryor plasma catecholamines in anxious subjects.The difficulty with the plasma assessments fromearlier studies was the insensitivity of the assayprocedures, and thus more studies have beendone on urine. Excretion of both adrenaline andnoradrenaline are noted in anxiety-provokingsituations, increased adrenaline relating to

136 Biological Psychiatry
threatening or uncertain situations and nora-drenaline to states of challenge, including thoseleading to anger or aggression (Schildkraut andKety, 1967). Mathew et al. (1980a) have reportedthat both noradrenaline and adrenaline areincreased in patients with generalized anxietydisorder compared with controls, decreasingafter a course of biofeedback. Raised urinarycatecholamines are found on PTSD (Young andBreslau, 2004).
The lactic acid link was followed by Pitts andMcClure (1967) on the grounds that lactate wasresponsible for the anxiety. In their studies theygave anxious patients and normals intravenoussodium lactate, and nearly all the former (93%)developed severe anxiety, starting within a fewminutes of the infusion. This was not seen tothe same extent in the normals (20%), or fol-lowing glucose–saline infusions. Since lactatecombined with calcium chloride was much lesseffective in provoking anxiety they suggestedthat the lactate bound with calcium, which low-ered calcium levels and thus interfered withneurotransmission.
These observations have been replicated byseveral groups, the main clinical conclusionbeing that lactate provokes anxiety, and morespecifically panic in susceptible patients. It wasearlier thought that the effect of lactate was aperipheral one, and that infused lactate did notpenetrate the CNS. However, it has been shownusing MRS that panic patients respondingto lactate show higher brain lactate levelsbefore, during and after infusion comparedwith nonresponders. This raises the possibilityof direct CNS effects of lactate. In humans,hyperventilation with subsequent hypocapnia,which is typically seen in lactate-induced panic,may either enhance peripheral uptake or leadto endogenous increases of brain lactate (Dageret al., 1994). These data fit with the replicatedobservation that giving panic patients 5% CO2to breath will also provoke panic attacks. Sinceinfusions of sodium bicarbonate also inducepanic in the prone, theories have been devel-oped to explain why CO2, bicarbonate and lacticacid should all be so provocative. Since CO2 is acommon metabolite of lactate and bicarbonate,it has been suggested that CO2 leads to cerebral
hypercapnia, which leads to hyperventilationand panic (Papp et al., 1993). Patients withspecific phobias do not exhibit this sensitivityto CO2 (Anthony et al., 1997), while lactate(and yohimbine) activates flashbacks in PTSD(Southwick et al., 1997).
There are reports that platelet MAO isincreased in patients with panic disorder(Gorman et al., 1985). In animals, a correlationbetween low MAO activity and brain 5-HT andits metabolites is reported, notably in a strainof mouse with high anxiety, irritability andaggression (Oreland et al., 1984); in primates,low MAO platelet activity relates to exploratorysensation-seeking activity. Tryptophan deple-tion caused increased anxiety and CO2-inducedpanic in patients with panic disorder, butnot controls. A blunted prolactin responseto fenfluramine has been reported in PTSD,suggestive of 5-HT dysrregulation, whichreceives some support from the response ofthis condition to SSRIs and the sensitivity totryptophan depletion.
There are few hormonal investigations ofpatients with anxiety disorders. Clinically,phaeochromocytomas, which secrete cate-cholamines, can present with intermittentepisodes of anxiety. The absence of thyroidhormone at crucial stages of early life isknown to markedly alter development. Theclinical picture of thyrotoxicosis has long beenrecognized to simulate anxiety states, andassessment of thyroid function is still requiredin the evaluation of anxiety states. In view of theoverlap, the reports of blunted TSH responsesto TRH in panic-disorder patients are of interest(Roy-Byrne et al., 1985a). Basal levels of TSHseem only slightly diminished and routinethyroid-function tests are within normal limitsin panic-disorder patients.
There is one report of a blunted growth-hormone response to intravenous clonidinein OCD patients, who also displayed higherMHPG and noradrenaline plasma levels thancontrols (Siever et al., 1983). The similarity ofthe clonidine response to that seen in affectivedisorders (see Chapter 8) suggests a biologicalaffinity between the two, the authors suggest-ing an association with increased presynaptic

Anxiety Disorders 137
and decreased postsynaptic noradrenergicresponsiveness. In PTSD, studies have revealedelevated urinary catecholamines in comparisonto patients with other psychiatric disorders(van der Kolk, 1994).
Generally patients with anxiety or panicdisorder show normal cortisol suppressionwith the DST (Roy-Byrne et al., 1985b), and sup-pression does not relate to anxiety symptomsin depressed patients (Saleem, 1984). Similarly,patients with PTSD and OCD show normalDST suppression (Lieberman et al., 1985). Inchronic PTSD, low-baseline, normal-rangeand elevated-baseline cortisol have all beenreported, which may reflect on the heterogene-ity of patients or differences between trait andstate. Low cortisol has been observed in normalindividuals under chronic stress as well as withchronic medical conditions, which may reflecton neuroanatomical (hypothalamic) or geneticinfluences.
Some of these data have led to specificexamination of the HPA axis in PTSD (Shalevet al., 2008; Yehuda and Golier, 2009; Yehudaet al., 2007). Stress initiates autonomic changesand alters activity in the hypothalamo–pituitary–adrenal (HPA) axis. The neurone ofthe paraventricular nucleus of the hypotha-lamus contain releasing hormones such ascorticotrophin factor (CRF), which increasesthe pituitary release of ACTH (corticotrophin),stimulating adrenal cortisol secretion. BluntedACTH responses to CRF and elevated CSFcorticotrophin are reported in PTSD (Bremneret al., 1997). Plasma CRF levels are also high (deKloet et al., 2008). These data, along with the lowcortisol levels, are thought to relate to an HPAaxis oversensitivity to the feedback of cortisol,the low cortisol levels thus reflecting chronicchanges to the HPA axis. This is secondary to anincreased sensitivity of glucocorticoid receptorsin target tissues. Such feedback is initiated viathe hypothalamus, amygdala, hippocampusand pituitary, all areas with high concentrationsof cortisol receptors (Rodrigues et al., 2009;Ruby et al., 2008). However, the hippocampusis central to this concept, the acute hormonalchanges occurring with psychological traumarelating to abnormal memory consolidation
in PTSD, supported by the hippocampalimaging data reported below. CRF receptorantagonists are currently under investigationfor the treatment of anxiety disorders, althoughresults from early clinical trials have beendisappointing.
NEUROCHEMICAL INVESTIGATIONS
The three main areas of neurochemical investi-gation relating to the anxiety disorders are theassociation of anxiety with abnormal adrenergicor 5 H-T activity and the link with benzodi-azepine receptors.
The interest in adrenergic mechanisms relatesto the early observations that drugs such as thebeta stimulants provoked many of the periph-eral effects of anxiety and the finding that thesewere blocked by specific beta-receptor antago-nists. In particular, drugs such as propranololdiminish the heart rate, inhibit palpitations,decrease tremor and inhibit the release of freefatty acids. In addition, the beta blockers havea long and respectable clinical use in anxiety.One hypothesis to emerge is that in anxietythere is an increased sensitivity of adrener-gic, specifically beta receptors. Some suggestthis is a peripheral phenomenon supporting theJames–Lange hypothesis (Chapter 2), but this isnot supported by several findings. First, in gen-eral, catecholamine-related compounds used tostimulate and block the anxiety symptoms crossthe blood–brain barrier, and may thus be exert-ing their effects centrally. Second, the availableevidence with regards to panic disorder does notshow increased responsiveness. Thus, Gormanet al. (1983) have shown that propranolol pre-treatment fails to prevent lactate-induced panicattacks, and Nesse et al. (1984) report that panicpatients actually decrease their heart rate afteran infusion of the beta-stimulant isoprotera-nol. Third, panic disorder responds better toimipramine than propanolol (Kathol et al., 1981).Fourth, many of the infusion investigations werenot carried out under double-blind conditions,and it is uncertain to what extent the infusionsthemselves acted as a nonspecific stressor.
In contrast, alternative theories emphasizethe primacy of central mechanisms in anxiety

138 Biological Psychiatry
and panic, and sometimes are seen as rivals tothe peripheral theory. The origins of this go backto Cannon (1927). He acknowledged the workof others who previously had shown that decor-ticate animals could still experience anxiety; hisown investigations showed that emotions couldbe generated by stimulation of CNS structures,and the experience of anxiety was not dependenton peripheral changes. The extended amygdalais one of the macrosystems considered impor-tant for these behaviours. For this theory, thesomatic manifestations experienced in anxietyare an effect, not the cause, and it follows thatthe biochemical changes such as those of thecatecholamines are also secondary.
In panic disorder there is evidence of down-regulation of beta adrenergic receptors, and in-creased sensitivity to the hypotensive responseto clonidine, suggesting increased sensitivityof presynaptic alpha-2 receptors, but bluntedclonidine growth hormone responses, suggest-ing subsensitive postsynaptic alpha-2 receptors(Nutt and Lawson, 1992). These data implicatebrain noradrenergic systems in panic disorder.
Gorman et al. (1989) postulated a neu-roanatomical basis of panic disorder involvingthe locus coeruleus, chemosensitive areas of themedulla, the limbic system and the frontal cor-tex. Patients with generalized anxiety disorderalso show blunted growth-hormone responses.
Central monoamine activity in anxiety-panicdisorder has been studied, with particular refer-ence to noradrenaline and the locus coeruleus,which when stimulated provokes anxiety inanimals. Drugs that increase locus-coeruleusfiring, and thus release of noradrenaline, suchas yohimbine, provoke anxiety in humans(Helmberg and Gershon, 1961), while thealpha-2 agonist clonidine, which reduces locuscoeruleus activity, is anxiolytic, albeit modestly(Hoehn-Saric, 1982; Uhde et al., 1985). Similardown-regulation of activity is seen with tricyclicantidepressants, also effective in some anxietypatients (Nyback et al., 1975), propranololand benzodiazepines.
A possible estimate of central catecholamin-ergic activity is measurement of the MHPGin urine and plasma. Ko et al. (1983) reported
that plasma levels of this metabolite correlatedhighly with rated anxiety in patients with thephobic anxiety syndrome, and both clonidineand imipramine inhibited a panic-inducedMHPG increase. In a more extensive investi-gation of alpha-2-receptor function in anxiety,Charney et al. (1984a) gave yohimbine tohealthy subjects and drug-free patients withagoraphobia or panic attacks. In the patientsthe rise of plasma MHPG levels correlatedwith patient-rated anxiety, nervousness andthe frequency of reported panic attacks; thiswas interpreted as evidence for impairedpresynaptic noradrenergic regulation in thepatients. This is supported by the observationof diminished yohimbine platelet binding inpanic-disorder patients (Cameron et al., 1984).
Patients with PTSD show decreased alphaadrenergic platelet receptors (Perry et al., 1990)and increases in MHPG to yohimbine challenge(Southwick et al., 1993). Bremner et al. (1993)hypothesized that PTSD is associated with anincreased responsiveness of the locus coeruleus,and increased release of noradrenaline in lim-bic and other areas innervated by that nucleargroup in response to stressful stimuli.
Another putative neurotransmitter group ofinterest in anxiety is the purinergic system. Thuscaffeine is anxiogenic, even provoking anxiety innormal controls at high levels (Uhde et al., 1985).Caffeine is an inhibitor of adenosine, itself apotent neuromodulator which has anticonvul-sant effects, and antagonists are proconvulsant.
Buspirone, a 5-HT1A agonist has been shownto be effective in treating generalized anxietydisorder, suggesting involvement of the 5-HTsystem, supported by the observations that theSSRIs are helpful for this condition and panicdisorder (see Chapter 12).
Understanding of the benzodiazepine recep-tor has been of importance. There are hints ofan association between central benzodiazepine-receptor binding and anxious traits in animals,and in patients the benzodiazepines are mostsuccessful in the treatment of anxiety disorders.The discovery of the benzodiazepine receptorwas a landmark in our understanding of theanxiety disorders, and is of great significance

Anxiety Disorders 139
for biological psychiatry. Thus, the possi-bility of discovering abnormalities of brainstructure and function in patients with majorpsychopathology has been a continuousendeavour, but the anxiety disorders have beensomewhat excluded. Indeed, the concept ofbiological therapies for anxiety disorders hasbeen criticized, and use of medications suchas the benzodiazepines has been discouraged.The concept of endogenous anxiety has beenignored, and the essentially biological natureof the anxiety disorders has been sacrificed onthe Cartesian shrine. In other words, many stillsuggest that anxiety is ‘mind-based’ rather thanbiologically ‘brain-based’. That is, compared tothe schizophrenias or the depressions, whichare now readily treated with psychotropicmedications, many anxiety-disorder patients,their families and even their physicians still failto acknowledge the neurobiological basis ofanxiety disorders.
It has to be of interest therefore that benzo-diazepine receptors exist in profusion in thehuman brain; that in animal models, anxietylevels can be related to such receptors; andthat in humans, benzodiazepines are anxiolytic.Further, benzodiazepine receptors are foundin high concentration in such structures asthe temporal, frontal and visual cortices,and the cerebellum and their antagonistsprovoke anxiety in animals and humans. Theseantagonists displace radioactively labelledbenzodiazepines from their binding sites andreverse their behavioural and physiologicaleffects. Two commonly used compounds arebeta-carboline-3-carboxylate (beta-CCE) andRo 15–1788, which appear anxiogenic whengiven alone. A derivative of beta-CCE has beengiven to humans and shown to provoke severeanxiety (Dorrow et al., 1983). These data raisethe possibility that an ‘endogenous anxiolytic’exists within the brain, and Sandler (1983)proposed the name ‘tribulin’ for this. Thereare other endogenous anxiogenic compounds,most notably the gut protein, CCK; this isalso found in the brain and can provokepanic attacks when given intravenously(Eser et al., 2008a, 2008b).
The search is still on for a truly active ‘endoge-nous benzodiazapine’. In many instances, thediscovery of a receptor that interacts withexternal medications preceded the discovery ofthe internal endogenous ligand. For example,opiate receptors were found long before theendorphins were uncovered. It is unclear if thereare endogenous benzodiazapine compoundsor whether the receptor’s activity involvesother compounds and the modification of thereceptor by, for example, CCK.
Among the disorders that are classi-fied under the ‘anxiety’ moniker the role of5-HT has been most clearly established inobsessive–compulsive behaviours. This stemsfrom the observations that patients withobsessive–compulsive disorder respondedpreferentially to clomipramine, a tricyclic drugwith a high selectivity for 5-HT, comparedwith other tricyclics, even in the absence of anassociated depression (Thoren et al., 1980a). Ithas now been shown that the response is betterin patients with higher pretreatment levels ofCSF 5-HIAA and HVA (Thoren et al., 1980b), inthose whose 5-HIAA levels fall the most duringtreatment and in those whose blood 5-HTdecreases (Hanna et al., 1993). Further, severalof the selective 5-HT reuptake inhibitors (SSRI)have been shown to be efficacious in OCD (seeChapter 12).
CSF 5-HIAA, although relating to responsein some studies, with higher levels beforetreatment being indicative of a better response(Swedo et al., 1992; Thoren et al., 1980b), has notbeen reliably different at baseline comparedwith controls. CSF MHPG does not relate toOCD symptoms (Swedo et al., 1992). Symptomsof OCD can be exacerbated by the 5-HT partialagonist m-chlorophenylpiperazine (m-CPP),but symptoms are not exacerbated by trypto-phan depletion (Berney et al., 2006). The criticalrole of 5-HT in modulating OCD symptoms (aswell as trichotillomania) was demonstrated byRapoport et al. (1992) in both human studiesand dogs with canine acral lick dermatitis.These double-blind crossover studies comparedclomipramine with desipramine, and fluoxetinewith fenfluramine against placebo. Only the

140 Biological Psychiatry
5-HT-uptake-blocking drugs were effective.The authors proposed that canine acral lickdermatitis was an animal model for OCD(Rapoport, 1992; Rapoport et al., 1992).
Other findings associated with OCD includea normal prolactin response to TRH, normalalpha-2 noradrenergic responsivity, normaldexamethasone suppression, reduced pro-lactin release with fenfluramine, and anelevated growth-hormone response to theacetylcholinesterase inhibitor pyridostigmine(Lucey et al., 1993), the latter finding suggestingcholinergic supersensitivity.
CSF studies have revealed elevated vaso-pressin and oxytocin in some OCD patients,especially those with no personal or familyhistory of tics (Altemus et al., 1992; Leckmanet al., 1994). These findings are of particularinterest, since the limbic forebrain containsmany sites rich in vasopressin and oxytocinreceptors, and in animal models vasopressinhas been shown to be associated with groomingbehaviours and with maintaining conditionedresponses to aversive stimuli (Insel, 1992).
There arises from these data good evidencethat the serotonergic system is important inOCD, although other systems are also involved.An attempt has been made to examine receptorsubtypes that may be involved by using selec-tive agonists. The effect of mCPP on increasingobsessional symptoms can be blocked by meter-goline, an antagonist of the 5-HT1a, 5-HT1c,5-HT1d and 5-HT2 receptors. MK-212, a selec-tive agonist of the 5-HT1b, 5-HT1c and 5-HT2receptor, provokes a blunted prolactin responsein patients with OCD, but does not increasesymptomatology (Bastini et al., 1990). The 5-HT1a receptor agonist isapirone seems to haveno such effects (Lesch et al., 1991), and thereseems to be no alteration of platelet 5-HT2 recep-tors (Pandey et al., 1993). A working hypothesistherefore is that further examination of the 5-HT1d subsystem may be worthwhile.
NEUROPHYSIOLOGICALAND NEUROLOGICAL DATA
The Kluver–Bucy syndrome, with diminishedanxiety as a central feature, has already
been described. It might be anticipated thatstimulation of medial temporal structures leadsto anxiety. Such is indeed the case. Heath (1982)correlated changes in various brain sites withemotions using intracerebral EEG recordings,and noted, in some patients, how the affect fearrelated to subcortical discharges. This has beenreplicated by several other groups, includingGloor et al. (1982) and Wieser (1983). The formerrecorded from, and stimulated, electrodesimplanted in neocortical and allocortical sites inpatients awaiting neurosurgery. Of 35 patients,50% exhibited some kind of experiental phe-nomenon with recorded activity, fear being thecommonest. The responses required limbic-system discharges and could not be evoked bypurely cortical discharges. Particularly involvedwas the amygdala, a structure also identified inthe studies of Wieser, who stimulated variousbrain regions, again using implanted electrodes,and reported fear on activation of the amygdalaand periamygdaloid area.
The evidence from patients with epilepsypoints in a similar direction. Williams (1956)recorded the ictal emotional experiences of 100patients with epilepsy, and noted fear in 61. Itwas seen mainly with an anterior or midtempo-ral location of the seizure origin. Cases of partial-status epilepticus, with an origin in the temporallobes and fear as a clinical manifestation, aredescribed (Henriksen, 1973), and clinically onoccasion it can be very difficult to distinguish apanic attack from an epileptic aura of fear.
There are several single case reports ofpatients with focal right-temporal lesionspresenting with panic attacks (Drubach andKelly, 1989), and Fontaine et al. (1990) reportedsignificantly more temporal-lobe abnormalitiescompared with controls on MRI.
IMAGING
Structural Studies
As mentioned above in the imaging studies ofthe SERT transporter, the anatomical studies inpanic, PTSD and GAD have largely focused onhippocampal or amygdala volumes. This areais problematic in that these disorders involve

Anxiety Disorders 141
stress, repeated over time, and we know thatstress hormones feed back in health and canactually change hippocampal size. This hasbeen shown in studies of Cushing’s disease(Belanoff et al., 2001; Dubrovsky, 1993; Starkmanet al., 1999). Thus, there is a chicken-and-eggparadox as to what came first, small volumes ornormal volumes which have then changed whilesubjects live a life of repeated stress (Maheuet al., 2008; Sapolsky, 1996; Yehuda, 1997).
Structural imaging in OCD has failed tofind consistent differences between controls.Luxenberg et al. (1988) noted decreased volumeof the caudate nuclei, a finding replicated byRobinson et al. (1995). These data were notsupported by the study of Kellner et al. (1991).Garber et al. (1989) reported increased T1 valuesof right-frontal white matter.
In the realm of PTSD, some studies havefound focal areas of abnormal signal activityin the medial temporal and parahippocampalareas on the right side. Bremner et al. (1995) havecompared hippocampal volumes in Vietnamcombat veterans with PTSD and controls, andreported smaller right hippocampal volumesin the PTSD group. A most interesting recentstudy examined the subject in reverse: Grafmanand colleagues (Koenigs and Grafman, 2009;Koenigs et al., 2008) built on work showingthat PTSD is associated with hypoactivity inthe ventromedial prefrontal cortex (vmPFC),hyperactivity in the amygdala and reduced vol-ume in the hippocampus (discussed below). It isunknown whether these functional neuroimag-ing findings reflect the underlying cause or asecondary effect of the disorder. To investi-gate the causal contribution of specific brainareas to PTSD symptoms, Grafman and col-leagues studied a unique sample of VietnamWar veterans who suffered brain injury andemotionally traumatic events. They found a sub-stantially reduced occurrence of PTSD amongthose individuals with damage to one of tworegions of the brain: the ventromedial pre-frontal cortex (vmPFC) and an anterior temporalarea that included the amygdala. These resultssuggest that the vmPFC and amygdala arecritically involved in the pathogenesis of PTSD(Koenigs et al., 2008).
Functional Studies
A large body of functional imaging literaturenow confirms our ideas about the neural cir-cuitry of the anxiety disorders. Researchers havetypically taken either control subjects or anxietypatients and then exposed them to situationsthat provoke their anxiety, and compare brainactivity during the anxiety to brain activityat rest. These studies have been enormouslyhelpful in destigmatizing the illnesses and inelucidating the relevant neuroanatomy.
In OCD patients, Baxter et al. (1988) initiallyfound increased metabolism in the left orbitalfrontal region and caudate nuclei. These find-ings have received some replication, althoughothers implicate more widespread frontalinvolvement (Swedo et al., 1989b). Treatmentwith either selective 5-HT agents or behaviourtherapy tends to decrease levels of metabolismin fronto-basal ganglia circuits (Benkelfat et al.,1990; Baxter et al., 1992).
Provocation studies, in which obsessive–compulsive behaviours are invoked duringscanning, also show increases of CBF infronto-basal ganglia, thalamic and cingulateareas during activated behaviours (McGuireet al., 1994; Rauch et al., 1994).
These data seem consistent with the hypoth-esis that the underlying neuroanatomy ofobsessive–compulsive behaviours involvesthe fronto-basal ganglia–thalamic circuitsdiscussed in Chapter 3. Frontal or caudateoveractivity will lead to increased inhibitionof the globus pallidus–thalamic pathway, thusreleasing activity in thalamic outflow back to thecortex. Another way to achieve the same effectwould be by a lesion in the globus pallidus orthe anterior limb of the internal capsule, or theanterior cingulate. These approaches are beingusing therapeutically with gamma-knife anddeep-brain stimulation. The 5-HT effects maybe mediated by the substantial serotoninergicafferents to the basal ganglia.
Two early PET studies of lactate-inducedpanic disorder suggested that there was rightparahippocampal and bitemporal activationrespectively, and that similar bilateral abnor-malities were also seen in patients with

142 Biological Psychiatry
anticipatory anxiety (Reiman et al., 1989). Thesefindings were later attributed to increasedtension in extracranial muscles associated withthe anxiety (Drevets et al., 1992). It does appearhowever that intense anxiety and panic doactivate fear and anxiety circuits involving theamygdala and hippocampus.
Studies using PET in generalized anxietypatients suggest differences from controls withhigher occipital-lobe, right posterior temporal-lobe, right precentral frontal-lobe and leftinferior frontal-lobe metabolism, and decreasedactivity in the basal ganglia. Treatment withbenzodiazepines resulted in decreased meta-bolic rates in cortical, limbic and basal gangliaareas (Wu et al., 1991).
In simple phobia there have been neg-ative studies as well as positive activationdata. Fredrikson et al. (1993), in patients withsnake phobias, showed activation of visualassociation cortex and thalamus, while Rauchet al. (1995), in patients with small-animalphobia, demonstrated activation of anteriorcingulate, insular, anterior temporal, posteriormedial orbitofrontal, somatosensory cortexand thalamus. The latter study was carefulto exclude teeth-clenching as an artefact(Rauch et al., 1995).
These data do suggest widespread involve-ment of limbic and somatosensory cortex invarious anxiety conditions, with an emphasison the right, especially for panic disorder.
OBSESSIVE–COMPULSIVE DISORDER
Clinically this syndrome would seem the ‘mostneurological’ of the conditions discussed inthis chapter, and in some patients the qualityof the thoughts and compulsions are of psy-chotic intensity. The syndrome seems ratherarbitrarily in the past to have been labelled aneurosis, with the supposed assumption thatin doing so its pathogenesis was understood inpsychodynamic terms.
Tuke (1894) was one of the earliest writersto recognize the cerebral underpinnings ofthe condition and since then the evidencefor the neurological associations of OCD hasstemmed from the clinical associations with
such disorders as encephalitis lethargica,Parkinson’s disease, Gilles de la Tourette’ssyndrome and the remarkable response of somepatients to selective neurosurgical lesions.
The encephalitis pandemics of the earlypart of this century led to the rich variety ofneuropsychiatric symptomatology describedby von Economo (1931). These includedobsessive and compulsive behaviours (Neal,1942). Many patients had postencephaliticParkinson’s disease, and in some the compul-sive behaviour was ‘awakened’ by L-dopa ther-apy (Sacks, 1973). The association betweenParkinson’s disease and obsessive–compulsivetraits has been frequently mentioned, interms of either rigid, moralistic and inhibitedpremorbid personality profiles or the develop-ment of obsessive–compulsive symptoms inassociation with the motor manifestations ofthe disease (Todes and Lees, 1985). Obsessionalslowness – the extreme time required by somepatients to carry out acts – may be likened tofailure of executive motor planning, similar tothat which must underlie Parkinson’s disease.
Swedo et al. (1989a) have drawn attention tothe high prevalence of obsessive–compulsivesymptoms in patients with Sydenham’s chorea,a known disorder of the basal ganglia. Gillesde la Tourette’s syndrome is characterizedby multiple tics, including vocal tics, whichusually manifest before the age of 15 years(Trimble, 1981a). Although these wax and wanewith time, the condition once established seemslifelong. Some of its manifestations are respon-sive to drugs that block dopamine receptorssuch as haloperidol, pimozide and sulpiride.The richness of the condition, however, extendsfar beyond the tics, and the motor symptomsinclude a great variety of complicated move-ments, many of which have a compulsivequality. Further, some 30–50% of patients haveobsessive–compulsive phenomena, equivalentin severity to OCD as defined by the DSMIII (Trimble and Robertson, 1986). Thesesymptoms are closely interlinked with someof the central features of the syndrome, suchas coprolalia and echophenomena, suggestingclose biological links between the motoric andpsychological phenomena.

Anxiety Disorders 143
‘PANDAS’ refers to paediatric autoim-mune neuropsychiatric disorders associatedwith streptococcal infections and representsa group of disorders somehow linked withbasal ganglia autoantibodies. The latter cross-react with human brain tissue, with highbinding specificity to caudate and putamen,and seem associated with a spectrum ofpost-streptococcal movement and relatedpsychiatric disorders, Sydenham’s chorea beinga paradigm. The streptococci are thought toactivate antigen-specific T- and B-cells, whichcross the blood–brain barrier and lead tofocal cytotoxicity basal ganglia disorders. Suchantibodies can be identified in up to 40% ofpatients with OCD.
Follow-up studies of patients with OCDreveal that about 10% go on to develop Gillesde la Tourette’s syndrome, and that those whodo have an earlier onset of OCD. The prognosisof OCD is worse if there is a lifetime history oftic disorder (Leonard et al., 1993).
The evidence that gamma-knife surgery isinfluential in the relief of obsessive–compulsivephenomena is reviewed in Chapter 12, andpoints to anterior cingulate lesions as beingan important target area. The observationsof Talairach et al. (1973), in which patients’brains were stimulated electrically, showedthat excitation of the cingulate area provokedforced integrated motor behaviour, similar innature to compulsive movements. Such obser-vations, combined with the known anatomicalconnections of the cingulate gyrus to thefrontal cortex, and the role of the latter in theregulation of sensory–motor integration andmotor planning (Stuss and Benson, 1984), implya potential neuroanatomical circuit involvedin OCD.
Other evidence for a neurological involve-ment in OCD comes from observations ofincreased birth abnormalities (Capstick andSeldrup, 1977), especially in patients with morebizarre rituals, and case reports of the conditiondeveloping after a head injury (Hillbom, 1960;McKeon et al., 1984). There is a long historyof an association between epilepsy and formsof obsessional thinking, sometimes reflectedin hypergraphia, associated mainly with
temporal-lobe epilepsy (see Chapter 10), andEEG studies of obsessive–compulsive patientsreveal significant abnormalities in 6–60%(Flor-Henry, 1983). Evoked potential investi-gations show shorter latencies and reducedamplitude of the N200 component of the visualevoked response (Ciesielski et al., 1981) topatterned stimulation, similar to that seen inpsychotic patients. Shagass et al. (1984) reportedhigh-amplitude somatosensory N60 waves inthe disorder, again found in schizophrenicpatients, and a lower-amplitude P90. Thesedata were taken to support notions of excessivearousal in these patients, but, in addition,implicate and support a suggestion of Flor-Henry that there is a deficit of left-frontalinhibition, leading to an inability to inhibitverbal ideational representations and theirmotor counterparts.
Insel et al. (1982) report that patients withOCD have abnormal sleep patterns and short-ened REM latencies, similar to patients withaffective disorder, reinforcing the clinical andbiochemical links between the two. There areseveral case reports of patients with lesionsin the basal ganglia developing OCD, thepallidum being particularly involved (Laplaneet al., 1989).
Neuropsychological studies consistently sug-gest problems with executive function, implyingfrontal involvement and related deficits canbe found in Gilles de la Tourette’s syndrome(Flor-Henry, 1983). Set-shifting problems andimpaired inhibition rather than planning anddecision-making ones are reported. Patientswith OCD also show problems with learningand memory. These psychological profilesare thought to relate to attentional deficitswith aberrant fronto-cingulate basal-gangliafunction, and are likely to be trait- ratherthan state-linked. (de Geus et al., 2007a, b;van ’t Ent et al., 2007).
POST-TRAUMATIC STRESS DISORDER
This disorder also has a rather special placein the anxiety-disorder pantheon. In DSM IV-TR it is virtually the only disorder definedby its cause (post-concussional disorder being

144 Biological Psychiatry
another), and there is considerable controversyover its validity, the relevance of the pretrau-matic personality and the role of the traumaitself. Since it is post-traumatic, since traumaoften implies accidents and since the latter usu-ally imply that someone is responsible, thereis a considerable social dimension to its pres-ence. These arguments are rehearsed elsewhere(Trimble, 2004), but they serve to emphasize thesocial nature of syndrome construction, and theimportance of moving to endophenotypes andbiological markers as a basis for classification.The imaging studies are noted above.
There are some neuropsychological inves-tigations of patients with PTSD, but the dataare confounded by co-morbidities such assubstance abuse, head injury and depression.Memory is central to the condition, traumaticmemories being so vividly re-experienced.However, psychogenic amnesia is also adiagnostic feature, but one which can easily beconfused with a post-traumatic amnesia of ahead injury. There have been studies combininghippocampal imaging with learning tasks, butwith inconclusive results.
SOME OUTSTANDING ISSUES
The anxiety disorders discussed in this chapterrepresent a heterogeneous group of conditions,but underling the majority, the affect of anxietyis central. This does not apply to OCD, whichclinically and biologically reveals a differentprofile. The genetics, neuroanatomy, diseasecourse and treatments of OCD are differentfrom say those of panic disorder. From a neuro-chemical perspective, the links to 5-HT seem thegreater with OCD, while the anatomical under-pinning is the fronto-basal ganglia circuitry.Further, in a different treatment area, severeOCD was amenable to neurosurgery, whichtoday has been replaced by the successes ofDBS (Cecconi et al., 2008; Greenberg et al., 2008).The various targets have involved thisneuronal network.
There is a more common basis for gener-alized anxiety disorder, the phobic states and
panic disorder, although some differential maybe suggested. In these, increased autonomicarousal can be shown, and the anxious-proneshow increased adrenergic activity when pro-voked. GABA systems seem to be more relevantfor generalized anxiety, but less involved inpanic attacks. Panic disorder shows a closeraffinity with the biochemistry of lactic acid andCO2 provocation, and there is more evidence of5-HT involvement in panic than with phobias.
These distinctions have been supported bythe neuroanatomical findings. Reflecting recenttrends in biological psychiatry, since the last edi-tion of this book there has been much less inter-est in studying urine, CSF and blood hormonalprofiles following chemical provocation stud-ies, and a shift towards genetics and imaging.In contrast to OCD, the anatomical basis ofthe other classified anxiety disorders hinges onthe temporal–limbic axis, especially involvingthe hippocampus and amygdala. Not only doanxious people show increased amygdala reac-tivity to emotionally arousing stimuli, but thisstructure is involved in the aetiology of socialphobia and panic disorder. Other anatomicalsites of primary relevance (revealed from ani-mal studies) include the locus coeruleus. Whilethere is also amygdala reactivity in PTSD, thisdisorder seems to have a different profile of bio-logical markers. The hippocampus seems morerelevant to the pathogenesis of this disorder,although it is unclear whether these anatom-ical findings relate to a state or a trait. Thefindings relating to the HPA axis would alsoseem unique amongst the anxiety disorders.How relevant these findings are for explainingco-morbidities and, as with all the disordersdiscussed in this chapter, for trying to unravelthe close links between the personality dispo-sitions and disorders and the axis 1 disordersis far from clear. The advance of combininggenetics with brain imaging is likely to throwmore light on these questions in the comingyears. One major difficulty for research in thearea of the anxiety disorders is the substan-tial clinical co-morbidities and overlap. Evenpure samples of PD or GAD, if followed long

Anxiety Disorders 145
enough, will often eventually have overlap-ping co-morbidites. The key concepts for futureresearch will likely involve identification ofanxiety-disorder endophenotypes.
The past trend to ignore the genetic, biolog-ical and neuroanatomical bases of the anxiety
disorders, especially amongst those with littleinclination towards neuroscience, is reflective ofthe same situation with regards to the addictions(see Chapter 9). This has retarded research inthis area and hindered the development of moreeffective biological therapies.


7The Schizophrenias
INTRODUCTION
Definition and Classification
Many of the illnesses referred to in the past as‘neuroses’ have melted away into more clearlydefined neurological conditions with a recog-nizable structural basis. So it is with Kraepelin’sconcept of dementia praecox. Although for himit represented a disease, whose origins mayoften be found in early life, its pathogenesis andphysiological accompaniments largely eludedhim. Bleuler, recognizing the heterogeneity ofthe condition, used the term ‘disease group . . .
about analogous with the group of the organicdementias’ (Bleuler, 1924, p. 373), while Slaterand Roth (1960) refer to schizophrenia as a term‘for a group of mental illnesses characterizedby specific psychological symptoms’ (p. 237).Gradually over time some aetiological factorshave become clarified.
Schizophrenia therefore should be consid-ered not as a single disease, but, like epilepsy(or the epilepsies), as a group of syndromes,recognized by a collection of signs and symp-toms, which have diverse pathogeneses. It issuggested that the symptoms represent theoutcome of abnormal cerebral functioning,itself provoked by disease processes, some ofwhich we readily recognize. However, it isimportant to understand that, as time passes,and as the cerebral basis of schizophrenicsymptoms becomes clearer, the clinical diag-nostic category will get whittled down, and
Biological Psychiatry 3e Michael R. Trimble and Mark S. George 2010 John Wiley & Sons, Ltd
preferred pathological diagnoses will begiven. This is one process whereby medicineadvances, and the principle is as important inpsychiatry as in other areas. Thus, Parkinson’sdisease, dementia (the dementias) and epilepsy(the epilepsies) are no longer thought of asclearly defined entities with a common cerebralpathology, but as recognizable conditionson clinical grounds, perhaps with commonunderlying functional changes that helpexplain the symptom pattern, but with severalpathological antecedents.
The concept that schizophrenia (or more aptlythe schizophrenias) is a single disease entity hascaused much confusion in psychiatry, even lead-ing some authors to the fanciful conclusion thatit does not exist (Szasz, 1976). There remainarguments over the precise definitions, if onlybecause they are operational and clinical, butthis is common with many conditions. How todefine epilepsy is likewise an elusive problem(see Chapter 10). The use of the plural in thechapter title and intermittently in the text how-ever emphasizes that the schizophrenias shouldproperly be viewed as a collection of disorderswith differing pathogeneses.
This view is not that developed by Kraepelin,who, while acknowledging the differing clin-ical pictures that may arise, noted the samebasic disturbances suggestive of a commonunderlying process. Bleuler (1911), who intro-duced the term schizophrenia ‘to show that thesplit of the several psychic functions is one of its

148 Biological Psychiatry
most important characteristics’ (p. 5), extendedthe range of the observed psychopathology,referred to the group of schizoprenias andintroduced Freudian psychodynamics into hisideas. He suggested that many of the typicalsymptoms were determined by ‘psychic’ causesand distinguished various types, includingprimary, secondary and basic. The symp-toms delineated by Kraepelin were mainlysecondary, derived by a reaction of the sickmind to the illness, primary ones being directlycaused by the disease process. Basic symptoms,present at all times, were alteration of affect andvolition, ambivalence and autism. The theorywas elaborated further, particularly by Jung, toinclude the idea that the psychic cause couldset an organic process in motion, thus beingaetiological. In addition, Bleuler considerablywidened the boundaries of the disorder toinclude personality changes and other subtlechanges of mental function, atypical maniasand melancholias, anergia, obstinacy andmoodiness. Simple schizophrenia was addedto the classification, which included many ofthese marginal cases, and the idea of latentschizophrenia was accepted. Bleuler’s influencewas profound, not only in central Europe,but also in the USA through the writings ofAdolf Meyer.
An important step was taken by KurtSchneider. Influenced by both Kraepelin andJaspers, he was especially concerned withsymptoms, and was dissatisfied with the waythat Bleuler defined such concepts as primaryand basic ones. He introduced the terms ‘firstrank’ and ‘second rank’, quite different fromthe divisions of other, previous writers. Thefirst-rank symptoms, shown in Table 7.1, wereintroduced for pragmatic diagnostic use, and ‘ifthis symptom is present in a non-organic psy-chosis, then we call that psychosis schizophrenia. . . the presence of first rank symptoms alwayssignifies schizophrenia, but first rank symptomsneed not always be present in schizophrenia’(Schneider, 1957, p. 44).
Schneider had no presumption of a commonstructure for these phenomena, although hediscussed them in terms of the lowering of a‘barrier’ between the self and the surrounding
Table 7.1 The first-rank symptoms of Schneider(after Schneider, 1957, p. 43)
The hearing of one’s thoughts spoken aloud inone’s head
The hearing of voices commenting on what one isdoing at the time
Voices arguing in the third personExperiences of bodily influenceThought withdrawal and other forms of thought
interferenceThought diffusionDelusional perceptiona
Everything in the spheres of feeling, drive andvolition which the patient experiences asimposed on them or influenced by others
aAn abnormal significance attached to a real perception without anycause that is understandable in rational or emotional terms.
world. Other symptoms were termed second-rank, and were considered much less importantfor diagnosis.
The first-rank symptoms assumed impor-tance for the diagnosis of schizophrenia, espe-cially in the UK, and were employed widely inresearch, for example the Present State Exam-ination (PSE) being biased to detect them forthat diagnostic category. Their influence on theDSM III and its successors is clear.
The International Pilot Study of Schizophre-nia was a transcultural investigation of1202 patients in nine countries: Colombia,Czechoslovakia, Denmark, India, Nigeria,China, the USSR, the USA and the UK (WorldHealth Organization, 1973). The main ratinginstrument was the PSE. The symptom profilesand the rank order of the most frequentsymptoms were similar across countries, andwhile no single symptom was present in allpatients from all cultures, the conclusion wasthat when psychiatrists diagnose schizophreniathey have the same condition in mind. Lack ofinsight, delusional mood, ideas of reference,flatness of affect, auditory hallucinations andpassivity experiences were commonly recordedand although first-rank symptoms were presentin only one-third, when recorded they almostinevitably led to a diagnosis of schizophrenia.The Americans and Russians differed the most,having a broader concept of the conditionthan the others. This difference in part led to

The Schizophrenias 149
the tightening up of the diagnostic criteria inthe DSM III.
The ICD 10 refers to schizophrenic disordersas a group in which there is a disturbance of thepersonality, distortion of thinking, delusions, asense of outside influence, disturbed percep-tion, an abnormal affect out of keeping withreality, and autism. Thought, perception, mood,conduct and personality are all affected by thesame illness, but the diagnosis is not restricted toone with a deteriorating course. The main typesrecognized are undifferentiated, hebephrenic,catatonic and paranoid, but residual and simpletypes were also included.
It is necessary for symptoms to have beenpresent for a month or more for a diagno-sis of schizophrenia to be given. For a moreacute episode, the term acute schizophrenia-likepsychotic disorder is used.
DSM IV-TR includes characteristic symp-toms, such as hallucinations, delusions andthought disorder, but emphasizes also socialand occupational dysfunction. The problemsmust have been present for at least six months.Illnesses lasting for a shorter time are referredto as schizophreniform disorder. Such Schneide-rian symptoms as voices keeping a runningcommentary on the patient’s behaviour, or twoor more voices conversing with each other,are specifically associated with a diagnosisof schizophrenia.
DSM IV-TR gives the following subtypes: dis-organized, catatonic, paranoid, undifferentiatedand residual. The disorganized type is character-ized by incoherence, an inappropriate bluntedaffect associated with mannerisms, social with-drawal and odd behaviour, and by an absenceof well-systematized delusions. This is equatedwith the hebephrenia of the ICD 10. In the cata-tonic type there is marked motor disturbance,sometimes fluctuating between the extremesof excitement and stupor. The paranoid typeemphasizes preoccupation with delusions orhallucinations. The undifferentiated type is forthose not classified in these groups, and theresidual is for patients who have a history of atleast one past episode but have minimal psy-chotic symptoms in the presence of continuedevidence of the illness.
Missing from the DSM IV-TR criteria are themotor disorders seen in schizophrenia (otherthan the catatonia), which form an integral partof the syndrome. These include stereotypies,negativisms, automatic behaviours, posturingand catalepsy. In addition, tremors, tics andchoreoathetosis have all been identified – notas a consequence of treatment but as a partof the disorder (Trimble, 1981a). Further, theemphasis on current or recent symptomsdetracts from the essential nature of schizophre-nia, which, in the majority of cases, pursues achronic course.
The history, typically, is of a patient, who maywell have demonstrated early developmentallanguage and behaviour problems, who mani-fests bizarre behaviour in late teens and earlyadulthood with a loss of academic potential.Initially, a bewildering variety of psychopatho-logical states, including anxiety states, maniasand depressions, may be recorded, but eventu-ally the longitudinal course becomes apparentand the cognitive and psychotic symptoms out-lined above manifest.
DSM IV-TR notes that psychotic disorder canbe due to a wide variety of general medicalconditions. This excludes disorders that onlypresent as delirium, and is subdivided depen-dent on whether the predominant symptomsare delusions or hallucinations.
Both the DSM IV-TR and the ICD 10 have thecategory schizoaffective, a term that is a sourceof considerable controversy. It was first intro-duced to refer to a psychosis with an admixtureof affective and schizophrenic symptoms that isprecipitated by emotional stress. Sitting betweenthe two Kraepelinian pillars of psychosis, thisdiagnostic category is not accepted by many, itsvery existence suggesting a return to a unitarypsychosis theory (see below). However, fam-ily and genetic data support the concept thatsome form of schizoaffective subtype exists,though its prognosis is related more to theaffective disorders (Procci, 1976). Some use theterms ‘schizodepressive’ and ‘schizomanic’ toreflect this; DSM IV-TR refers to the bipo-lar and the depressive types. It is diagnosedonly when definite schizophrenic and definiteaffective symptoms are present simultaneously.

150 Biological Psychiatry
It must be distinguished from post-treatmentschizophrenic depression.
The schizoaffective subtype may describethe same patients referred to as having cycloidpsychosis (Leonhard, 1957). The features arepsychotic episodes which resolve completelyand are associated with confusion and per-plexity, mood and motor changes, pan-anxietyand delusions.
Kraepelin’s original concept, of a dementiapraecox, embedded the idea of a progression.There have now been several follow-up studies,particularly with brain imaging (see below), thatrather support his views. Thus it is estimatedthat some 50–70% of cases take a progressivecourse, which includes not only the psychoticsymptoms but also the cognitive changes andloss of the ability to function independently at ahigh level in society.
Paranoid Disorders
The word ‘paranoid’ has been used in psy-chiatry for many years, but its meaning hasshifted from a general term for madness to amore precise technical expression (Lewis, 1970).Kraepelin initially classified paranoia asa separate entity from dementia praecox;it represented the insidious development of adelusional system in the presence of an intactpersonality. He used the term ‘paraphrenia’to refer to those who have a paranoid illnessdeveloping later than dementia praecox.Lewis (1970), after a careful consideration of theworld literature, gave the following definition:‘A paranoid syndrome is one in which thereare delusions of self reference which maybe concerned with persecution, grandeur,litigation, jealousy, love, envy, hate, honour,or the supernatural, and which cannot beimmediately derived from a prevailing morbidmood such as mania or depression’ (p. 11).He felt that the adjective ‘paranoid’ could beapplied to a personality disorder with similarfeatures, except that dominant ideas shouldreplace delusions.
ICD 10 uses the term ‘persistent delusionaldisorders’, and DSM IV-TR ‘delusional disor-der’ for these syndromes. Patients develop a
single delusion or a related set of delusions,not necessarily so bizarre in content, in theabsence of criteria for schizophrenia. Such delu-sions often arise in middle age, can contain ideasabout the individual’s body and should last atleast one month. In many patients, these disor-ders are persistent, but psychosocial functioningmay remain adaptable. DSM IV-TR recognizesseveral types, namely erotomanic, grandiose,jealous, persecutory, somatic and mixed. Thelitigious variant is also well known to lawyers.
An important addition to this group is thepsychotic disorder due to a general medical con-dition. Prominent symptoms are hallucinationsand delusions not due to delirium or dementia.
Endophenotypes
The term ‘endophenotypes’ refers to a marker ofan illness that might be closer to the underlyinggenetic mechanisms than the actual phenotype,as for example specified by DSM IV-TR andICD 10. It was introduced in 1972 by Gottesmanand Shields and represents a neurobiologicaltrait that is related to the illness in question. Theconcept has assumed particular prominence inthe genetics of schizophrenia and is one wayto deconstruct the phenotype into componentparts for a potentially more powerful geneticanalysis. Most studies have highlighted cogni-tive and brain-imaging variables.
GENETICS
The contribution of genetics to schizophreniahas been long recognized, but is often curiouslyneglected in some pathogenic explanations ofthe disorder. It has been reviewed in detailby many authors (McGuffin, 1984; Slater andRoth, 1960; and more recently Gur et al., 2007;Norton et al., 2006; Porteous, 2008; Riley andKendler, 2006; Tandon et al., 2008; van Winkelet al., 2008). In brief, the twin studies showimpressive differences in rates of concordancebetween monozygous (MZ) and dizygous (DZ)pairs, and the adoption data indicate that thereis a greater incidence of schizophrenia andschizophrenic spectrum disorders in those who,

The Schizophrenias 151
Table 7.2 Classic twin studies in schizophrenia
Study Concordance
Monozygous (%) Dizygous (%)
Kringlen (1967) 45 15Pollin et al. (1969) 43 9Tienari (1971) 35 13Fischer (1973) 56 26Gottesman and Shields (1972) 58 12Kendler and Robinette (1983) 40 6Mean 46.1 13.5
adopted to normal parents, have a biologicalparent with the condition. Table 7.2 summarizesthe data, indicating concordance rates from 35to 58% in MZ and from 6 to 26% in DZ pairs.
While there were several criticisms ofthe early data, for example the method ofascertainment of the zygosity and the clinicaldiagnostic criteria for the schizophrenia, laterstudies have attempted to overcome these.Some authors (Gottesman and Shields, 1972;Kendler and Robinette, 1983) noted that themore severe the illness, the more likely theconcordance in MZ pairs, and Kallmann (1946),whose own series noted a 91.5% concordancefor MZ twins living together, reported arising familial incidence of the condition assubjects approach a genetic relationship withindex cases. Thus, compared to a percentageexpectation of 0.9% for the general population,the equivalent figure for half-sibs was 7.1%, forparents 9.2%, for full-sibs 14.2%, for children16.4%, for DZ co-twins 14.5% and for childrenof two schizophrenic parents 39.2%. Aftera review of the data, Slater concluded ‘theevidence is very strong that the geneticalconstitution of an individual contributes alarge part of his total potentiality of becomingschizophrenic’ (Slater and Roth, 1969, p. 246).McGuffin (1984) calculated that the heritabilityof the condition was 0.66, genetic factors thusaccounting for two-thirds of the variance invulnerability to the disorder. A similar figure(68%) has been given by Kendler (1983), whonotes that this is similar to that for diabetesand hypertension, and rather in excess ofthat for epilepsy, peptic ulcer and coronaryartery disease.
There is some suggestion that schizophrenicprobands resemble their affected relatives withregards to subtype, although there is muchoverlap, and twin and adoption studies whichmight clarify this issue have not been conducted.Leonhard (1980) has suggested, on the basis offamily studies, that periodic catatonia has a highgenetic loading, and Perris (1974) noted the samefor cycloid psychosis. Winokur (1977) reportedthat paranoia may also be genetically separate.
McGuffin et al. (1984) examined the heritabil-ities of a twin population using six different setsof operational criteria for schizophrenia. Thoseof Feighner and the RDC criteria gave the high-est heritability, while the Schneiderian criteriahad a heritability value of zero. Dworkin andLenzenweger (1984) examined the case histo-ries of MZ twins in whom at least one hadschizophrenia and assessed concordance forpositive and negative symptoms. Their resultssuggested that negative symptoms may have thegreater genetic component. Similar conclusionshave emerged from the studies of Tsaung (1993).
With regards to interpretation, the contentionthat environmental factors are so important,in that the environments of MZ twins are saidto be more alike than those of DZ pairs, hasbeen discounted by the adoption studies.Heston (1966) showed that the adopted childrenof schizophrenic mothers, removed from themshortly after birth, had a higher incidence ofthe illness than the adopted children of non-schizophrenic mothers. These findings havebeen replicated and extended by a seriesof studies on Danish patients, including inves-tigation of the relatives of adopted childrenwho later became schizophrenic (Kety, 1983;

152 Biological Psychiatry
Kety et al., 1994). These studies have notonly shown the higher incidence of schizophre-nia among the biological relatives but alsoan overrepresentation of the schizophreniaspectrum of disorders. Further, there wasan overrepresentation of schizophrenia orschizophrenia-spectrum disorders in thebiological relatives of adopted schizophrenicpatients, significantly greater than amongthe relatives of nonschizophrenic adoptedcontrols. In addition, in investigations of pater-nal half-siblings of schizophrenic probands,the incidence of schizophrenia was higherthan in control cases, ruling out intrauterinecontributions to the congenital effects.
Replication studies (Kendler et al., 1981),particularly improving the criteria forschizophrenia-spectrum disorders, have beenconducted. The prevalence of schizotypal per-sonality disorder was significantly higher in thebiological relatives of schizophrenic adopteesthan controls, but this was not the case for delu-sional disorder of the nonschizophrenic typeor for anxiety disorder. These adoption studies,particularly the careful analysis of the Danishpatients, have confirmed the genetic contribu-tion to schizophrenia and identified the conceptof the schizophrenia spectrum more clearly.
Gottesman and Bertelsen (1989) observed thatthe risk for schizophrenia and related disorderswas similar in the offspring of schizophrenicMZ twins and those of their nonschizophrenicco-twins, suggesting that the discordance ratein MZ twins may in part be explained by anunexpressed genetic diathesis.
With regards to the mode of inheritance,several authors favour polygenic as opposed tomonogenic transmission (Kendler, 1983), math-ematical models failing to provide evidence forthe latter. To date, no consistent traditionalgenetic markers linking to schizophrenia havebeen identified. However, the identification ofsuch markers will only be successful if thereis a major gene effect (either single or a smallnumber) or if there is a subgroup with such acomponent. HLA markers have been claimed,but the results of different studies are variable.McGuffin et al. (1981), after review of the
available literature, noted that the mostpersistent genetic marker to date was HLA A9with paranoid schizophrenia, and the moreconsistent associations (found by more thanone group) relate to HLA A9 and B5.
There are several important negative-linkagestudies to regions of chromosomes 2, 5, 9, 11, 12and 22 and to the D2, D3, D4, 5-HT2 and GABAasubunits (Macciardi et al., 1994; Waddingtonet al., 1992; Su et al., 1993). No mutation of theD1 receptor gene has been found.
Crow (1988) suggested that the pseudoau-tosomal locus of the X or Y chromosomes isimportant. This is a region of the distal seg-ment of the short arm of the Y chromosome thatin meiosis exchanges genetic material with theshort arm of the X chromosome. Genes thereare therefore transmitted in an autosomal ratherthan sex-linked way. Further, genes of the pseu-doautosomal locus do not seem subject to Xinactivation. His theory is based on a numberof observations, notably that the age of onset ofschizophrenia is earlier in males, that pairs offirst-degree relatives with psychosis are morelikely to be the same sex, that in parent–childpairs with psychosis the mother is twice aslikely to be affected than the father and thatconcordance by sex is paternally rather thanmaternally inherited. Further, sex-chromosomeaneuploides such as XXY, XX, but not XO,are associated with an increased incidence ofschizophrenia. No direct evidence of such link-age has yet been found (Crow et al., 1994), butCrow’s theory has developed to include a searchfor the gene responsible for handedness andcerebral dominance, which may be located atthe pseudoautosomal region (Crow, 1991).
The substantial evidence for genetic influ-ences on the development of schizophreniahas led to several studies of high-risk people.These include the Edinburgh group (Lawrieet al., 2008a, 2008b; Owens and Johnstone, 2006),NAPLS (the North America Prodrome Longi-tudinal Study) (Addington et al., 2007) and theEPOS (the European Prediction of PsychosisStudy). Each of these studies has taken subjectswith at least one parent with schizophrenia andfollowed them longitudinally, gathering data

The Schizophrenias 153
at inception before there was any diagnosisof the disorder. They are assessed at variousintervals, and those who develop the disorderare then compared with those who do noton many different variables. The studieshave included psychological and behaviouralvariables, neurocognitive profiles and imaging,although each study has varied with regards toentry criteria and measurements selected. Somehave included healthy normal controls andsome alternative high-risk groups such as thosewith learning disability (or mental handicap).Assessments have included such ratings as theStructured Interview for Schizophrenia (SIS),the Structured Interview for Prodromal Syn-dromes (SIPS) and tasks of verbal abilities andworking memory. The results of these studiesare awaited with interest. These massive projectsoffer some promise, but caution is needed inlight of the amount of genetic work done todate that has not shown real progress. Oneproblem is that as sample sizes have increased,the signals heralded from earlier studies seemto have weakened rather than getting stronger(Weinberger, 2009). The genome-wide studiesare in fact revealing overlaps in the revealedgenetics of schizophrenia and bipolar disorder.At present, if differences can be suggested, it isbetween susceptibility for bipolar disorder andgenes involved in calcium ion-channel function,and the zinc-finger transcription factor inschizophrenia. Two promising position candi-dates in schizophrenia are NRG1 (neuregulin)and DTNBP1 (protein-coding dystrobrevin-binding protein 1). The deletions of the neurexingene (involved in the development of synapses)may represent a discontinuity with bipolardisorder and the potential genetic links betweenthe latter and the genes coding for the GABAareceptor and calcium channels may turn out tobe significant (Kirov et al., 2009).
It needs to be emphasized however that thegenetic variations noted so far in these disordersexplain only a small amount of the variabilityof the phenotype, and the limitations of thetechnique with regards to the statistics involvedand the definition of phenotypes as discussed inChapter 4 need to be taken into account.
Landis and Insel (2008) described only cau-tious optimism toward the results in this areaat present.
SOMATIC VARIABLES
Abnormalities in muscle endplates in schizo-phrenic patients have been reported. Usingmuscle biopsies stained for motor neuronesand terminals, Crayton and Meltzer (1976)reported the size and dispersion of terminalbulbs to be abnormal in psychotic patients, withlarger and more variable endplate arborizationand low density of endplate neural structures.Although similar findings were seen in somemanic–depressive patients and no associationwas noted with type or length of illness, theauthors felt the findings might indicate regener-ative processes of previously denervated fibres,reflecting perhaps altered CNS physiology.These data are in keeping with other evidenceof disturbed muscle pathology in psychoticpatients. A number of authors have noted anincrease in serum creatine phosphokinase inacute psychoses. This does not simply reflectthe use of intramuscular injections or methodsof restraint since elevations are found in aproportion of first-degree relatives and there issome correlation with the alpha-motor neu-rone abnormalities noted on biopsy. Further,mean creatine kinase levels during a hospitaladmission are also elevated (Meltzer 1980).
Schizophrenics have been shown in severalstudies to present with an excess of majorphysical abnormalities, but the contribution ofmental handicap to the ensuing clinical pictureis unclear. Minor physical and dermatoglyphicabnormalities are overrepresented and a num-ber of these abnormalities are linked to the firsttrimester of foetal development (Guy et al., 1983;Weinberg et al., 2007). These seem unrelated tosymptomatology or to the presence or absenceof neurological soft signs. Dysmorphic craniofa-cial features are also increased in schizophrenia,including brachycephaly (McGrath et al., 2002).
The velo-cardiofacial syndrome (DiGeorgesyndrome or chromosome 22q11.2 deletion

154 Biological Psychiatry
syndrome) is associated with an increasedrisk for schizophrenia and with alterations ofcerebral structure, especially temporal-lobesize (Debbane et al., 2009; Eliez, 2007; Greenet al., 2009; Schaer and Eliez, 2007).
METABOLIC AND BIOCHEMICALFINDINGS
One early finding that has been replicated wasof abnormal nitrogen balance in patients withperiodic catatonia (Gjessing, 1947). Thus, phasesof stupor and excitement were associated withnitrogen retention, with later compensatoryincreased excretion. In such patients it wasclaimed that alteration of nitrogen input, byreducing protein intake, altered the course ofthe illness.
The concept that endogenous neurotoxinsexist, derived from the abnormal metabolismof various chemicals, was encouraged by obser-vations of psychoses resembling schizophreniathat could be provoked by the ingestion of vari-ous psychotropic drugs, such as LSD, mescalineand amphetamine. Attempts were made to iden-tify abnormal compounds in the blood and urineof schizophrenics, with some authors reportingsuccess, although much of the early data wasnot replicated. From these ideas arose thetransmethylation hypothesis (Smythies, 1976).Several hallucinogenic compounds were seen tobe closely related chemically to the endogenouscatecholamines and indolamines, which werenotably methylated derivates. It was suggestedthat abnormal transmethylation of thesecompounds might produce hallucinogenicmethylated monoamines related to the patho-genesis of at least some forms of schizophrenia.Administration of methyl donors such asmethionine to schizophrenics gave variableresults but, especially when combined with amonoamine oxidase inhibitor, led to the exac-erbation of symptoms in some 40% of patients.These studies did not, however, distinguishbetween an acute organic brain syndrome andtrue exacerbation of schizophrenic symptoms(Wyatt et al., 1971).
A related theme is the possibility that 5-HTis involved in schizophrenia. Thus, methionine
may inhibit the uptake of tryptophan into thebrain by competitive blockade (Smythies, 1976)and schizophrenia may in part reflect defectivetryptophan metabolism. However, supplemen-tary tryptophan loading in patients has pro-vided only equivocal results, and to date therole of indolamines in the psychoses remains tobe clarified.
Administration of the 5-HT agonistmetachlorophenylpiperazine (MCPP) toschizophrenic patients increases positive symp-toms (Krystal et al., 1993). In controls there is noeffect, suggesting a propsychotic rather than apsychotogenic effect. These data suggest a rolefor serotonergic mechanisms in schizophrenia.This has been supported by observations thatpipamperone, a selective 5-HT2 antagonist, isantipsychotic, and some newer antipsychoticssuch as risperidone are selective 5-HT2 receptorantagonists (see Chapter 12).
Platelet MAO activity in schizophrenia hasbeen studied by many authors. In general, thevalues are low, although, since similar dataare noted in some other psychiatric conditions,it is not specific for schizophrenia (Delisiet al., 1982; Siever and Coursey, 1985). Patientswith paranoid symptoms probably have thelower levels, and in studies of normal adultsan inverse correlation between the paranoiascore on the MMPI and MAO levels has beennoted. Several authors link low values to hallu-cinations and delusions, others to poor out-come. Baron et al. (1980) identified studentswith abnormally high or low levels of MAOand found that 70% of those with low levelsand none with high levels had a diagnosis ofborderline schizophrenia. This same group alsoreported that schizophrenic patients with a highgenetic load have reduced levels in contrastto those with nonfamilial schizophrenia, andrelatives with low MAO are more often affectedwith schizophrenia-spectrum disorders thanhigh-MAO relatives (Baron et al., 1984).
Reveley et al. (1983) examined MAO in MZtwins discordant for schizophrenia, normal MZand DZ twins, and controls. The MZ pair witha schizophrenic co-twin had significantly lowervalues than did the healthy MZ twins and theother controls, the MZ schizophrenics having

The Schizophrenias 155
only slightly lower values than their healthyco-twins.
Although some authors have failed to findlow MAO in schizophrenic patients, and fur-ther show that neuroleptic treatment may itselflower MAO (Owen et al., 1981), the consistencyof the data and the findings in twins, rela-tives and volunteers suggests some association,genetically determined, between MAO and vul-nerabilities to these behaviour patterns, and arein agreement with the adoption studies that bothschizophrenia and related spectrum disordersneed to be considered together.
Low-platelet MAO has been implicated inboth the transmethylation and the dopamine(see below) hypotheses of schizophrenia in thesense that reduced MAO activity may reflect animpaired capacity to degrade monoamines ortheir abnormal metabolites, thus increasing theload of these substances in the brain.
The Dopamine Hypothesis
The predominant biochemical hypothesis ofschizophrenia has been the dopamine hypothe-sis, and a considerable amount of research workhas been carried out investigating dopamineand its metabolites in patients. The hypothesisemerged in the wake of the introduction of thephenothiazines in the 1960s, stemming fromrecognition of the similarity of a psychosisinduced by amphetamine to schizophrenia, andthat in small doses they can activate symptomsin patients, and the discovery that the principalmode of action of the phenothiazines is to blockdopamine receptors. The ability of neurolepticdrugs to block dopamine receptors correlatedbetter than other biochemical effects with theirefficacy in the control of psychotic symptoms(Snyder et al., 1974). The dopamine hypothesiswhich emerged thus suggested that schizophre-nia was the result of overactivity of dopamineneurotransmission in the CNS and that neu-roleptics acted by reducing this. However, theevidence was largely circumstantial, and overtime modifications have had to be made.
In animal models, behavioural distur-bances provoked by dopamine agonists givensystemically or by injection into the limbic
forebrain were reversed by neuroleptic drugs(Anden, 1975), and the ability of these com-pounds to inhibit dopamine-sensitive adenylcy-clase stimulation is proportional to their clinicalpotency, with notable exceptions, namely thebutyrophenones. However, the recognitionof different classes of dopamine receptorsand the fact that the main receptor linked toadenylcyclase activity is the D1 have helpedexplain this apparent discrepancy.
Generally the evidence that neuroleptics actat dopamine receptors in the limbic system isstrong (Scatton and Zivkovic, 1984). Electro-physiologically their iontophoretic applicationantagonizes the depression of cellular activityinduced by the application of dopamine ago-nists, and binding studies show that a varietyof neuroleptics specifically bind to dopaminesites within the limbic system. Further, theyincrease the metabolism and turnover ofdopamine, an effect related to the feedback acti-vation of neurones following the postsynapticreceptor blockade.
Early on it was noted that some neurolepticdrugs were less frequently associated withextrapyramidal side effects. The latter werethought to occur with the blockade of dopaminereceptors in the striatum, and the reason whysome drugs, notably thioridazine, clozapine andsulpiride, did not do this required explanation.Some evidence pointed to differential effectsat limbic and nonlimbic sites (ventral anddorsal striatum, respectively), either due toanticholinergic properties (strong with thior-idazine and clozapine, anticholinergic effectsbeing greater in nonlimbic striatal areas) ordue to preferential action on different receptorsubpopulations at the two sites (Scatton andZivkovic, 1984; see also Chapter 12), drugssuch as sulpiride acting mainly at the limbicreceptors. It seems that the effects of neurolepticdrugs on psychotic symptoms relate to changesof dopamine turnover in the limbic forebrain atleast, while the development of extrapyramidalsymptoms is related to the dorsal striatum(Crow et al., 1979a). Further, the antipsychoticeffect most likely relates to blockade of selec-tive dopamine receptors, especially D2, D3and D4.

156 Biological Psychiatry
An effective demonstration of the antipsy-chotic effect of dopamine antagonism has beenprovided by Crow et al. (1979a). Patients withacute schizophrenia took part in a double-blindtrial of treatment with flupenthixol, comparingthe alpha isomer, which blocks the dopaminereceptor, to the beta isomer, which does not.The former had a significant effect comparedto placebo, although this was confined toonly certain symptoms, referred to by theauthors as ‘positive’. Thus, using the Krawieckascale, the improvements were seen on scoresfor delusions, hallucinations and speechincoherence, but not on poverty of speech oraffective flattening.
One problem for the dopamine theoryrelates to the time course of the clinicaleffect. Prolactin, which is elevated by blockingdopamine receptors (the prolactin inhibitoryfactor probably being dopamine), rises muchfaster than the noted clinical improvements,which do not become manifest for two or threeweeks after commencing treatment. In contrast,the extrapyramidal effects often arise within 48hours. This paradox has some explanation interms of adaptive effects to the acute blockadein dopamine systems. Thus, cerebrospinalfluid (CSF) studies indicate that the initialrise of dopamine turnover diminishes aftertime (van Praag, 1977b), as does the plasmalevel of HVA (Pickar et al., 1984), and similartolerance of the biochemical effects has beenobserved in animals. However, it seems that thetolerance relates more to dopamine receptorsin the caudate areas, less to those in the limbicforebrain and not at all to those in the frontalcortex (Scatton and Zivkovic, 1984). The latterfinding may relate to the lack of autoreceptorsin frontal areas. Reuptake of dopamine infrontal cortex is via the NA transporter.
Another line of evidence has been to observethe effects of drugs known to increase dopamineactivity on the symptoms of schizophrenia.Paradoxically, administration of the dopamineagonists L-dopa and apomorphine seems toimprove symptoms in some patients (Buchananet al., 1975; Tamminga et al., 1977). In somereports the effect is on such symptoms as apa-thy, isolation and blunted affect (Gerlach and
Luhdorf, 1975); in others it is on hallucinationsand delusions (Tamminga et al., 1977). How-ever, several carefully conducted trials havefailed to replicate these findings (Ferrieret al., 1984b; Syvalahti et al., 1986). It is sug-gested that any observed effect is due to inhi-bition of dopamine release by interaction withpresynaptic receptors.
More direct evidence of abnormal dopamineactivity in schizophrenia has been hard todemonstrate. If dopamine is overactive in theCNS then low basal levels of prolactin maybe expected, but studies have generally beennegative. In contrast, provocation tests usingapomorphine and measurements of eithergrowth hormone (raised by dopamine ago-nists) or prolactin have been more successful.Growth-hormone responses have been reportedto be greater in patients with first-rank symp-toms (Whalley et al., 1984), with delusions,hallucinations and thought disorder (Meltzeret al., 1984), and to be both increased (Meltzeret al., 1984) and blunted in association with neg-ative symptoms and in chronic schizophrenia(Ferrier et al., 1986). Prolactin baseline levels andapomorphine-induced prolactin suppressionhave been shown to correlate inversely withthe presence of positive symptoms (Johnstoneet al., 1977; Ferrier et al., 1984b), especiallyin patients with normal ventricular size onCT scans (Kleinman et al., 1982b). Althoughthe interpretation of such findings may beeasily blurred by the effects of medicationon hormonal release, these studies were ondrug-free patients, and the results tend tosupport the hypothesis that at least somesymptoms in schizophrenia are related todopaminergic mechanisms, notably hallucina-tions, delusions and thought disorder, similarto the ones shown to respond preferentially todopamine-antagonist drugs.
Other estimates of dopamine activity haverelated to peripheral markers. Plasma dopaminehas been reported to be elevated in some studies(Bondy et al., 1984). Measurement of dopaminebeta-hydrolase, the enzyme that convertsdopamine to noradrenaline, has providedinconsistent results (Castellani et al., 1982),as have measurements of plasma HVA.

The Schizophrenias 157
Other markers have included the reporting ofreduced platelet cyclic-AMP production (Kafkaet al., 1979) and elevated spiperone binding tolymphocytes apparently unrelated to treatment(Bondy et al., 1984). Further evidence that linksdopamine to schizophrenia comes from CSFand post-mortem studies, and is discussedbelow (see Table 7.3).
PET ligand-binding studies have mainlyused tracers that bind to one or more of thedopamine receptors. There is discrepancyof results, partly based on technical factorssuch as the ligand used. There are morenegative findings with normal D2 densities inschizophrenia (Martinot, 1990; Farde et al., 1990;Pilowsky et al., 1995) than positive ones (Tuneet al., 1992), failing to provide direct evidencefor increased dopamine-receptor activity inschizophrenia. Fletcher et al. (1996) have usedapomorphine as a dopamine agonist to showthat in schizophrenia, using a verbal fluencyactivation task, there is impaired activationin the cingulate cortex, which is enhanced byapomorphine. Their data suggest a regionalfunctional deficit in schizophrenia, which canbe modulated by dopamine. Research continueswith dopamine PET imaging, with some studies
Table 7.3 Main arguments for and against thedopamine hypothesis
For:
1. Amphetamine-induced psychosis produces aschizophrenia-like illness
2. Amphetamine exacerbates schizophrenia3. Drugs that block dopamine receptors are antipsy-
chotic in relationship to their blocking potential4. Post-mortem and endocrine studies5. Animal models of dopamine agonism resem-
ble psychosis, and are reversed by dopamine-blocking agents
Against:
1. Time course between administration of adopamine blocker and clinical response
2. Dopamine agonists have an inconsistent effecton psychosis
3. Direct evidence of increased dopamine activityis poor
suggesting an important role for dopamine inschizophrenia (Howes et al., 2009; Howes andKapur, 2009) and others not (Valli et al., 2008).
Catechol-O-methyl-Transferase (COMT) isone of several enzymes that degrade thecatecholamines, such as dopamine or nora-drenaline. A series of studies have now fairlyconsistently found that individuals with certainCOMT gene variants (specifically the valvariant) carry an increased risk of developingschizophrenia, and the val variant of theCOMT gene is associated with both structuraland functional brain changes within patientswith schizophrenia (van Haren et al., 2008;Lawrie et al., 2008a; Ross et al., 2006; Roffmanet al., 2006). These findings raise suspicion thatan abnormality in catecholamine metabolismis fundamental to schizophrenia pathogenesis,at least in some subjects (Gur et al., 2007;Benes, 2007; Keshavan et al., 2007; van Harenet al., 2008).
The Noradrenergic Hypothesis
An alternative to the dopamine hypothesis isthe noradrenergic hypothesis, suggested byStein and Wise (1971) and revived recently byYamamoto and Hornykiewicz (2004). This wasbased on the idea that the central noradrenergicpathways, then shown to be related to a centralreward system, might degenerate and lead to atleast some of the symptoms of schizophrenia.Generally the data are less favourable for thishypothesis, although several studies indicatea role of noradrenergic mechanisms in somesymptoms of schizophrenia. This has beenreviewed in detail (Kleinman et al., 1985).No noradrenergic abnormalities have beenreported in urine of schizophrenic patients,although there is one report of increased levelsin the plasma of drug-free patients (Ackenheilet al., 1979). Neither plasma nor urine 3-methoxy-4-hydroxyphenylglycol (MHPG) orvanillylmandelic acid (VMA) levels have beenconsistently abnormal in schizophrenia, moststudies showing no difference from controls.CSF and neurochemical data are discussedbelow. Attempts to assess the functions ofalpha-2 adrenergic receptors have been done

158 Biological Psychiatry
either by direct measurement of plateletbinding or by changes of metabolites afterchallenge with clonidine. Alpha-2 receptorshave been reported as increased in plateletsin only a minority of subjects, probably thosewho are schizoaffective (Kafka et al., 1980),while others have noted decreased binding ina group with negative symptoms and poorresponse to treatment (Rosen et al., 1985), withsubsensitivity of MHPG release to a clonidinechallenge (Sternberg et al., 1982).
The Glutamate Hypothesis
It has been known for some time that phen-cyclidine and ketamine, drugs which areantagonists at the NMDA receptor, increasesymptoms in schizophrenia. Glutamate isubiquitous in cerebral cortex, and is the mainexcitatory neurotransmitter regulating activityin the cortical-basal ganglia thalamic re-entrantcircuits. This relates not only to motor controlbut also to sensory gating. The NMDA receptorsare therefore hypothesized to be hypofunctionalin schizophrenia. Serum glutamate levels arelow at the onset of the disorder (Palominoet al., 2007), as are serine levels in serum andCSF, serine being modulatory at the NMDAreceptor. Attempts to use this hypothesis todevelop new treatment strategies include trialsof the glutamate agonist D-serine, which isreleased by glutamate from astrocytes. Patho-logical studies in support of this hypothesis arediscussed below.
Other Studies
Early investigations of endocrine function inschizophrenia yielded inconsistent results andwere aimed in particular at examination of thethyroid and adrenal glands. Schizophrenia-likepsychoses have been described in associationwith several endocrinopathies, including hypo-and hyperthyroidism and hypoparathyroidism(Lishman, 1987). The prolactin and growth-hormone data, utilized more as a methodof challenging hypothalamic–pituitary (HPAaxis) function than to implicate the hormonal
changes themselves as pathogenic, have beendiscussed. Few other studies of endocrinefunction in schizophrenia have been carried outrecently, although there are reports of lower LHand FSH levels in chronic schizophrenia, withan inverse relationship to positive symptoms,while negative symptoms have been inverselyrelated to testosterone levels (Alias, 2008).There seems to be loss of normal episodicsecretion of LH, possibly reflecting disturbedhypothalamic or limbic-system function (Ferrieret al., 1982). Further evidence for this is thefinding of blunted FSH and prolactin responsesto thyrotropin-releasing hormone in similarpatients (Ferrier et al., 1983).
In contrast to what is seen in the affectivedisorders, the number of schizophrenic patientsshowing abnormal dexamethasone suppressionis low, unless there is coexistent depression(Munro et al., 1984).
Finally, following the discovery of enkeph-alins, attempts have been made to examinepeptide function in schizophrenia, largely bygiving peptides to patients and estimating clin-ical changes. Table 7.4 lists some of the sub-stances tried to date, but the results have beendisappointing.
Of growing importance has been thecannabinoid group of compounds, especiallythe social use of cannabis. It is acknowledgedthat the strength and the availability of cannabispreparations has increased, and it is knownthat patients with psychotic disorders are morelikely to abuse illicit drugs. Schizophrenicpatients are often heavy cannabis users, and
Table 7.4 Some peptides used as treatments inschizophrenia
Peptide Author
CCK Lostra et al. (1984)Albus et al. (1984)
Des-tyrosinegamma-endorphin
van Praag et al. (1982)
Des-enkephalingamma-endorphin
van Praag et al. (1982)
Beta-endorphin Berger et al. (1980b)Thyroid-releasing
hormonePrange et al. (1979)

The Schizophrenias 159
the administration of tetrahydrocannabinolincreases the reporting of psychotic symp-toms in healthy volunteers and schizophrenicpatients in remission (Henquet et al., 2008;Tandon et al., 2008; d’Souza et al., 2005).
Several long-term follow-up studies havebeen reported in which populations have beenexamined over several years and their drugusage noticed or monitored. A Swedish cohortof over 50 000 conscripts noted that cannabisuse by the age of 18 was associated with a 2.4-fold increase in a diagnosis of schizophrenia(Andreasson et al., 1987). A longer follow-up ofthe same population (27 years) reported a doserelationship between the amount of cannabisuse at entrance and the later risk of developingthe disorder (Zammit et al., 2002). A Netherlandsstudy (three-year follow-up of nearly 5000 peo-ple) confirmed these findings and noted thatthose who had reported any psychotic symp-toms at baseline were more likely to go onto develop schizophrenia if they were cannabisusers (van Os et al., 2002). Arseneault et al. (2002)followed 759 people in a cohort from birthto young adulthood. Cannabis use by age 15increased the risk of developing psychosis. In ameta-analysis of the data, the increased risk ofdeveloping a psychosis with cannabis use wasgiven as 1.4 (odds ratio), and the dose responsewas confirmed (odds ratio 2.84). Most stud-ies in this area had adjusted for confoundingfactors such as the use of other drugs and psy-chotic symptoms at baseline (Moore et al., 2007).One problem with interpreting these results ina causal way is that evidence that the inci-dence of schizophrenia is increasing pari passuis not yet reliably available. However, elevatedanandamide (a cannabinoid agonist) has beenreported in CSF (Leweke et al., 2007), as hasincreased density of CB1 receptors in prefrontalcortex (Dean et al., 2001).
NEUROCHEMICAL INVESTIGATIONS
In order to explore further the dopamineand related neurochemical hypotheses inschizophrenia, many neurochemical investiga-tions have been conducted. The CSF data will
be discussed first, followed by neurochemicalpathological data.
CSF
The main metabolite assessed in CSF to test thedopamine hypothesis is HVA, although it is sug-gested that the main source of this is nigrostriataldopamine and not mesolimbic and mesocorticaldopamine. Nonetheless, the anatomical prox-imity and the overlap between these systemssuggests that at least some of it reflects limbic-system dopamine function. In general, eitherthe baseline CSF values or the accumulationof metabolite after probenecid administrationhave been sampled. The latter technique inhibitsthe exit of HVA and related compounds fromthe CSF, diminishing the gradient that existsbetween ventricular and spinal CSF values.Theoretically this should provide a more accu-rate determination of metabolite turnover andconcentration, but it too has methodological dif-ficulties. Not the least is that the results arerelated to the CSF probenecid levels.
One of the early baseline studies of HVA wasthat of Rimon et al. (1971), who reported normalvalues, except that patients with paranoidsymptoms had elevated levels. Generally, how-ever, the baseline data have failed to show dif-ferences between schizophrenics and controls,although Sedvall and Wode-Helgodt (1980)reported that high HVA levels were associatedwith a family history of schizophrenia. Theprobenecid studies likewise have tended tobe negative with singular exceptions. Thereare reports of decreased accumulation inpatients with Schneiderian first-rank symptoms(Bowers, 1973; Post et al., 1975) and a suggestionthat those with low values have poorer progno-sis (Bowers, 1974). These data are compatiblewith increased dopamine-receptor sensitivity,which subsequently decreases dopamineturnover. Some support for this comes froma study in which the relationship betweenapomorphine-induced growth-hormone releaseand CSF–HVA levels was assessed in drug-freeschizophrenic patients. An inverse relationshipwas found, those patients with low HVAhaving a higher release of hormone (Zemlan

160 Biological Psychiatry
et al., 1985). Thus low HVA was associatedwith higher dopamine-receptor activity, and inaddition with first-rank symptoms and thoughtdisorder. Pickar et al. (1990) also reportednegative correlations between HVA ratings ofpsychosis and positive symptoms.
Both CSF levels of DOPAC and dopamineitself are reported as normal in schizophrenia(Berger et al., 1980a; Gattaz et al., 1983b), as areprolactin levels (Rimon et al., 1981).
With regard to the noradrenergic hypothe-sis, MHPG levels are consistently reported asnormal (Kleinman et al., 1985), although thereare reports of increased levels of noradrenaline(Gomes et al., 1980; Lake et al., 1980), especiallyin paranoid subtypes, and of MHPG correlatingwith negative symptoms (Pickar et al., 1990).
A variety of other substances have been mea-sured in the CSF of schizophrenic patients, someof the more important ones being shown inTable 7.5.
Brain Neurochemistry
Most studies in this area relate to testing thedopamine hypothesis. Studies on post-mortembrains are difficult to interpret. Not only arethey derived from patients that have usuallybeen on medication or have used a large dose of
psychotropic drugs to kill themselves, but alsorapid post-mortem biochemical changes occur.Several groups have set up centres designedspecifically for collection of brains and appropri-ate storage after death, control specimens beingtreated in the same manner. It seems likely thatpeptides and receptors are much more stablethan monoamines and their metabolites. Gen-erally the areas of brain examined have beenthose with a high level of the neurotransmitterunder investigation, and studies have mainlyconcentrated on the limbic system and relatedstructures. For all of these reasons, ligand PETimaging is somewhat better, although it also hasproblems, primarily that not all substances, par-ticularly peptides, can be measured with PET.
The majority of post-mortem neurochem-istry studies show normal values for bothdopamine concentrations and HVA, notablyin the caudate nucleus, putamen and nucleusaccumbens. However, Bird et al. (1979) reportedincreased concentrations of dopamine in thenucleus accumbens and the anterior perfo-rated substance. In an extended study onover 50 schizophrenic brains, with controls,Mackay et al. (1982) confirmed the significantelevations, especially in patients with earlyonset of illness. Owen et al. (1978) reportedincreases in dopamine in the caudate nucleus,but not in the putamen or nucleus accumbens,
Table 7.5 Some CSF studies in schizophrenia
Compound Result Reference
Dopamine beta-hydrolase Normal Lerner et al. (1978)Dopamine sulphate Increased: negative symptoms Risby et al. (1993)5-HIAA Normal Post et al. (1975)
Gomes et al. (1980)Roy et al. (1985)
Cyclic-AMP Decreased Biedermann et al. (1977)Increased Gomes et al. (1980)
Cyclic-GMP Decreased Gattaz et al. (1983a)GABA Normal (↓ young females) van Kammen et al. (1982)Angiotensin-converting enzyme Decreased Beckmann et al. (1984)Neurotensin Decreased (subgroup only) Widerlov et al. (1982)Glutathione Decreased: also in prefrontal
cortex (MRS)Do et al. (2000)
Kynurenic acid Decreased, correlated withgrey-matter densities
Schroeder et al. (2008)
Copper Decreased Tyrer et al. (1979)D-serine Decreased Bebdikov et al. (2007)

The Schizophrenias 161
and a significant decrease in HVA in thecaudate. Farley et al. (1977) reported increasesin dopamine only in the septal region of chronicparanoid patients. The cingulate has beenrarely examined, but Wyatt et al. (1995) havereported decreased DOPAC levels in anteriorcingulate cortex.
Reynolds (1983, 1987) has attempted to assesslaterality effects in relation to neurochemistry inschizophrenia. Comparing patient brains to con-trols, dopamine was increased in the amygdalaof the schizophrenics, selective for the left side.In one study, the increase of dopamine in theamygdala was found to correlate with decreas-ing levels of GABA binding in the hippocampus(Reynolds et al., 1990).
Dopamine-receptor binding, with suchcompounds as haloperidol, spiperone, flu-penthixol and apomorphine, has also beeninvestigated. Studies of the dopamine receptorin vivo with PET imaging have shown high inter-individual variability, which links to person-ality variables (Farde et al., 1990; Karlssonet al., 1995; Karlsson et al., 2002) and to cognition(Cervenka et al., 2008). Most of the studies inschizophrenia show increased binding in someareas, although the interpretation of this has ledto much debate. In summary, most studies of D2receptors show increases of caudate binding (13of 16) (Clardy et al., 1994), others show increasesin the putamen and/or nucleus accumbens.The contribution of prescribed neurolepticdrugs to these findings continues to be animportant controversy, although some authorsexamined groups of drug-naıve patients (Owenet al., 1978) or patients drug-free for a long time(Lee and Seeman, 1980). However, these verysame changes can be observed in rat brainsgiven long-term neuroleptics (Clow et al., 1979).
Other dopamine receptors have been lessstudied. D1 receptors seem normal (Seemanet al., 1987), similar to data from animals receiv-ing neuroleptic drugs. However, D4 bindingin the striatum has been reported as increased(Seeman et al., 1993).
It remains unclear what it is that drives theincrease in dopamine activity. Early work hadsuggested a link through GABA. Decreased ter-minals of GABA in the hippocampus correlate
with increased dopamine levels and are linkedto the observation of increased GABAa-receptoractivity. Attention has now centred on asubgroup of GABA neurones, the parvalbumin-containing cells. Parvalbumin, along withcalretinin and calbindin, is a calcium-bindingprotein, which develops at between three andsix months of foetal development. Decreasedparvalbumin cells are found in the frontalcortex and hippocampus in schizophrenia. Thisall suggests GABAergic deficits, which it ispostulated lead to disturbed neuronal rhythmic(oscillatory) expression in key structures (thehippocampus, but also areas of frontal cortex),and to altered dopamine release.
Glutamate is also linked with this story. Glu-tamate input to dopamine-releasing cells (from,for example, the hippocampus and the pedun-culopontine areas) normally induces bursts ofspikes within the VTA, which are disrupted bya deficit of glutamate. Glutamate can be identi-fied within neurones by looking at transporters(EAAT3 or VGluT1 – the neuronal and vesicu-lar transporter respectively), and recent studieshave shown decreases of these in post-mortemmaterial, especially in the left-temporal area(Nudmamud-Thanoi et al., 2007; Reynolds andHarte, 2007). These are associated behaviourallyto novelty detection, which under normal cir-cumstances activates the VTA and accumbens,interlinked with behavioural reward, and whichin schizophrenia is thought to become disrupted(Lodge et al., 2009; Sohal et al., 2009).
Glutamic acid decarboxylase levels arereported as decreased in prefrontal cortx(Volk et al., 2000). The changes in GABAare supported by decreases in reelin mRNA,reelin being a protein released by GABAergicneurones, and decreased GABA transportersin DLPFC neurone (Costa et al., 2001; Akbarianet al., 1995).
Several studies of glutamate binding havebeen carried out. Measurement of glutamatelevels in CSF had earlier yielded conflictingresults, but the psychotomimetic agent phen-cyclidine (PCP) was known to be an NMDA-receptor antagonist, leading to the hypothesisthat glutamate transmission may be reducedin schizophrenia. Decreased kainate and

162 Biological Psychiatry
glutamate binding have been reported (Kerwinet al., 1988; Deakin et al., 1989), especiallyin the left temporal lobes, as has reducedrelease of both glutamate and GABA fromsynaptosomes from temporal cortex followingapplication of the agonists kainic acid or NMDA(Sherman et al., 1991). Data from frontal areasare equivocal, especially for GABAa receptors,although they suggest, if anything, increasedglutamate binding in orbitofrontal areas. Thesedata argue for decreased cortical excitatorytransmission in some areas of the limbic systemin schizophrenia.
Noradrenaline and its metabolites have al-so been examined. Decreased levels of nora-drenaline have been reported in the putamen(Crow et al., 1979b); others have reportedno differences (Bird et al., 1979; Winbladet al., 1979) and others selective increases (Farleyet al., 1977). MHPG is reported to be elevated inthe hypothalamus and nucleus accumbens byone group (Kleinman et al., 1982a). Dopaminebeta-hydrolase and monoamine oxidase appearnormal.
Binding of 5-HT receptors to various brainregions has been variable. Low 5-HT2 bindingto frontal cortex has been noted by some groups,especially if patients who commit suicide areexcluded from the sample (Laurelle et al., 1993),
although the contribution of chronic neuroleptictreatment to these effects remains unclear.
Peptides have also been studied. Levels ofangiotensin-converting enzyme were reducedin the substantia nigra and globus pallidus(Arregui et al., 1980). Opioid and naloxonebinding is probably normal (Owen et al., 1985).Ferrier et al. (1984a), in an extensive studyof peptide distribution in limbic structuresin schizophrenic and control brains, reportedthat CCK was reduced in temporal cortex,especially in the hippocampus and amygdalaof patients with negative symptoms (type 2 ofCrow); somatostatin was likewise decreased inhippocampus in the same group, while VIP wasincreased in the amygdala of those with positivesymptoms (type 1 of Crow). No changes wereseen for neurotensin, while substance P wasincreased in the hippocampus. A fuller review ofthe post-mortem findings of peptides in schizo-phrenia is given by Caceda et al. (2006, 2007).
Several other compounds have been assessedin various brain regions, and many of these aresummarized in Table 7.6.
Neuropathological Data
A related area of research has been neuropatho-logical studies of the brains of patients who had
Table 7.6 Some post-mortem biochemical findings
Chemical Result Author
Dopamine Increased D2, D3, D4/transporter normal
Review, see Guillin et al. (2007)
GABA Probably normal Cross et al. (1979)Glutamic acid decarboxylase Normal Bird et al. (1979)5-HT Increased: Putamen Crow et al. (1979a)
5-HT1a frontal cortex Gurevich and Joyce (1997)Abi-dargham (2007)
5-HT2 probably normalLower:Hypothalamus Winblad et al. (1979)Medulla oblongataHippocampusFrontal cortex Bennett et al. (1979)
Tryptophan Normal Crow et al. (1979b)Cathechol-O-methyl transferase Normal Crow et al. (1979b)Tyrosine hydrolase Normal Crow et al. (1979b)Choline acetyl transferase Normal Bird et al. (1979)Muscarinic receptors Decreased Dean et al. (2002)Neurotrophins BDNF Variable results Buckley et al. (2007)

The Schizophrenias 163
‘the schizophrenias’. Although many studiesover the years have been carried out, all ofthem detecting changes in some brains exam-ined, such data are often criticized on account ofthe lack of consistency of the findings. However,similar criticisms would apply to pathologicalstudies of such disorders as the dementias orthe epilepsies if it were supposed that they rep-resented the outcome of only a single process.
Earlier studies had shown abnormalitiesin thalamic, hypothalamic, periventricular,periaqueductal and basal forebrain areas(Nieto and Escobar, 1972; Stevens, 1982). Sincethat time other investigators have examinedpost-mortem collections of brains and whilemost detect some abnormalities, there aredifferences between types of pathology andareas affected. The most consistent abnormal-ities have been noted in hippocampal andrelated structures.
Overall, the volumes of schizophrenic brainsare reduced (Pakkenberg, 1987). This is asso-ciated with negative symptoms (Johnstoneet al., 1994), and an excess of nonspecific focalpathology can be seen, often in basal-gangliastructures (Bruton et al., 1990). The length ofthe sylvian fissure on the left is decreased(Falkai, 1992).
There are reports of abnormal gyral pat-terns, especially in the frontotemporal areas,with associated cytoarchitectural abnormalities(Jacob and Beckman, 1989) confirmed with MRIstructural imaging.
Structural disorganization of hippocampalpyramidal cells (Kovelman and Scheibel, 1984;Bogerts et al., 1985), reduced hippocampalmossy cell-fibre staining (Goldsmith andJoyce, 1995), decreased hippocampal volumesand cell loss (Falkai and Bogerts, 1986) andabnormalities or reduced volumes of thesubiculum and hippocampal CA regions haveall been reported (Arnold et al., 1995). In theentorhinal cortex, smaller neurones, displacedpre-alpha and pre-beta cells, and reducedneuronal number and density have been noted(Arnold et al., 1991). The changes reported arein both the left (Kovelman and Scheibel, 1984;Bogerts et al., 1985) and the right hemispheres(Conrad et al., 1991).
Crow and colleagues (Brown et al., 1986),in a comparison of brains from patientsmeeting strict criteria for affective disorderand schizophrenia, noted that the latter hadlarger temporal horns of the lateral ventricleand thinner parahippocampal gyri. The greaterdifferences were noted in the left hemisphere.
Some of these reports suggested thatgliosis was a typical pathological reaction inschizophrenic brains. However, most studiesfail to find gliosis, supporting the sugges-tions of Kovelman and Scheibel (1984) thatthe pathological changes instead representdevelopmental anomalies.
Other neuropathological findings includediminished neuronal density in some layersof the frontal, cingulate and motor cortices(Benes et al., 1986), higher numbers of longvertical axones in cingulate cortex, possiblyrepresenting increased input of associativeaxons (Benes et al., 1987), and abnormalarrangement of cells and decreases of smallinterneurones (possibly inhibitory) in cingulatecortex (Benes and Bird, 1987; Benes et al., 1991).Increased neuronal density has been reportedin hippocampus and prefrontal cortex (Selemonet al., 1995), while reduced dendritic spinedensity of pyramidal neurone in the DLPFC hasbeen found. These findings add evidence to thegrowing appreciation that the schizophreniasmay be neurodevelopmental disorders, andthat abnormalities in cortical cytoarchitextureand connectivity may be key facets of theunderlying pathophysiology.
Akbarian et al. (1993) reported reducednumbers of NADPH-diaphorase-stained cellsin superficial and increased numbers in deeplayers of the dorsolateral prefrontal cortex.The stain specifically identifies cells of theembryological subplate area, the findingssuggesting anomalous migration of cells. Inanother study, decreased gene expression forglutamic acid decarboxylase in prefrontal cor-tical neurones was found. This occurred in theabsence of any cell loss, suggesting a functionaldown-regulation of neurotransmitter geneexpression (Akbarian et al., 1995). This mayrelate to the reported decrease in glutamic aciddecarboxylase levels in prefrontal cortex and

164 Biological Psychiatry
decreased GABA axon terminals. The changesin GABA are supported by decreases in reelinmRNA. As with many studies, the contributionof medication to these effects is unknown.
There are reported decreases of neuronesin medial dorsal nucleus of the thalamus andnucleus accumbens (Pakkenberg, 1990), sub-stantia innominata (Stevens, 1982) and cerebel-lum (Jeste et al., 1985). The thalamic findingsare of interest in view of the increasing evi-dence from imaging studies of thalamic abnor-malities in schizophrenia. Some evidence hasemerged for abnormalities of glutamate recep-tors (NMDA) and transporters in this structure,but also in other areas such as the caudate, hip-pocampus, DLPFC and cingulate gyrus (Watiset al., 2008).
A selective reduction in glial cells in cingulatecortex (Brodmann’s area 24) has been shown inschizophrenia patients relative to comparisonsubjects, calling into question whether cingulatechanges are specific only for affective disorders(Stark et al., 2004).
Recently, direct measurement of proteinexpression in brain areas has been carriedout (proteomic studies) using electrophoresisor specialized mass-spectrometry techniques.These can identify the profile of many hundredsof proteins, but to date have not yieldeduseful clinical information. Likewise there area growing number of studies in which geneexpression in various cortical areas has beenlooked at, again with heterogenous results.The frontal cortex and genes that link withneurotransmitter function have been moststudied. Genes related to myelin-formingoligodendrocytes and metabolic enzymes,as well as synaptic marker proteins such assynaptophysin, spinophilin (markers at pre-and post-synapyic terminals, respectively) anddysbindin, have all been reported to be reducedin some areas, notably hippocampus (Weickertet al., 2007). The mRNA that encodes GAD67 (glutamic acid decarboxylase), an enzymethat synthesizes GABA, is reduced in theDLPFC. This is reported particularly for theparvalbumin-expressing neurones, which havebeen shown in several studies to be reduced
in schizophrenia in the hippocampus and pre-frontal cortex.
While the pathological studies achieve somedegree of agreement, there is also quite a bit ofconfusion. This relates to several factors. Agonalchanges, prior drug prescriptions and statisticalanalysis of such databases are problematic. Itis also necessary to take into account the meth-ods selected for analysis and the heterogenouspopulation. There seems to be evidence for cellloss or disarray, or both, in frontal and tempo-ral areas, but also for alterations of cell density,which may better reflect cell size rather thanloss. However, the abnormalities are relatedto the structures implicated in the anatomy ofschizophrenia, especially the prefrontal areas,medial temporal (especially hippocampal struc-tures) and thalamus. Glutamate and GABAsystems are becoming very relevant as attentionhas been directed to underlying anatomical cir-cuitry. The enthusiasm for post-mortem studieshas waned in recent years, overtaken partic-ularly by the advances in brain imaging, butnewer methods of protein and gene analysis arealso ascendant and may lead to important find-ings, especially if they can be coordinated withimaging and genetic data.
NEUROPHYSIOLOGICALAND NEUROLOGICAL DATA
EEG
Soon after the introduction of the electroen-cephalogram, reports of abnormalities inschizophrenia appeared. Hill (1950) reviewedthese as follows: EEGs suggestive of epilepsywere most often seen in catatonia, althoughgeneralized nonparoxysmal dysrhythmias andother paroxysmal phenomena were also found.Since then, there have been many reports ofEEG abnormalities in schizophrenic patients.In a comparison with patients suffering fromaffective disorder, Abrahams and Taylor (1979)noted that the proportion of EEG abnormalitieswas twice as great in the schizophrenics, whohad more temporal abnormalities. Slow-waveasymmetries, slow bursts, spikes and sharp

The Schizophrenias 165
waves were the recorded changes, and theytended to be more frequent on the left side. Inpatients with temporal-lobe EEG changes thislaterality was associated with formal thoughtdisorder and emotional blunting, but notfirst-rank symptoms. Although patients wereon medications, this did not correlate with theEEG findings.
Investigations of patients using electrodesimplanted within the brain have clearlydemonstrated abnormalities in schizophrenics,again notably within the limbic system. In aseries of studies, Heath (1982) investigated 63patients with psychosis, 38 being diagnosed asschizophrenic. Spiking was seen in the septalregion. This is defined by Heath as an area bor-dered dorsally by the base of the anterior horn ofthe lateral ventricle and the head of the caudatenucleus, and ventrally by the free surface of thegyrus rectus of the frontal lobe. It includes septalnuclei, the accumbens, olfactory tubercle andthe diagonal band, as well as parts of the gyrusrectus. It has extensive frontal and temporal con-nections. The abnormalities occurred when, andonly when, the patients were actively psychotic.In many cases changes were not observed onsurface recordings, and neither were similarfindings noted in chronic-pain control patients.Violence and aggression were associated withhippocampal and amygdala discharges. Somepatients showed activation in sensory-relaynuclei in association with hallucinations (forexample, medial geniculate recordings) andoften cerebellar discharges. Similar findings,especially with regards to the septal region,have been reported by others (Rickles, 1969).
Examination of the spectral power of EEG fre-quencies in schizophrenia reveals more fast betaactivity, more theta and delta, and less alphathan normals (Itil, 1975). Psychotic childrenand those with a high risk for schizophreniashow a similar pattern of changes. Generallythese patterns are ‘normalized’ by antipsychoticmedication.
Fenton et al. (1980) noted the changes to bemaximal over temporal derivations in acuteschizophrenic patients, while chronic patientsshowed more diffuse slow-wave power, notably
theta and delta, diffusely or maximally fron-toparietally.
Stevens and Livermore (1982) used teleme-tered EEG recordings during psychoticbehaviour of schizophrenic patients. They iden-tified so-called ‘ramp patterns’, characterizedby a monotonic decline in power from lowestto highest frequencies, which can be seenin epileptic patients during subcortical spikeactivity. These were seen only in recordingsfrom schizophrenic patients in their sample,and not in controls. Patients with catatonicepisodes showed them in the right temporalregion, while 50% of paranoid patients withauditory hallucinations had left-sided ramps,with increased slow activity. Psychotic eventsrecorded clinically were associated withsuppression of left temporal alpha frequencies.
Evoked-potential studies in schizophreniaare numerous, and the results complicatedto interpret. Several reviews are available(Shagass, 1972; Flor-Henry, 1983). Generally,evoked potentials show greater variabilityand amplitudes are decreased; a subgroup ofpatients show a ‘reducing’ pattern of decreasingamplitude with increasing stimulus intensity.Flor-Henry (1983) summarized a review bystating ‘the evoked potential characteristics inschizophrenia consistently implicate the lefthemisphere, and particularly the left temporalregion’ (p. 215). The contingent negative varia-tion (CNV) also tends to be reduced, maximallyover frontal areas.
Studies using brain electrical activity map-ping (BEAM) EEG have shown increasedfrontal delta and diminished left temporalP300 amplitudes (Morihisa et al., 1983; Morstynet al., 1983).
More recent studies have investigatedrhythmic oscillations and synchronizationsbetween neural networks. Such oscillationsundergo changes during development and areclosely related to GABA and glutamate activity.As noted, there are suggestions of decreasedGABA neurones in cortical structures inschizophrenia, especially those neurone whichexpress parvalbumin (chandelier neurones)with thalamic afferents. Alteration of this input

166 Biological Psychiatry
can disrupt inhibition and hence oscillatorypatterns (Lodge et al., 2009; Sohal et al., 2009).
Using MEG it has been shown that responsesrecorded from auditory cortex in schizophreniato rhythmic auditory trains or to visual stimuliare different from controls, with decreases ofhigher frequencies (40 Hz, gamma) and excessof lower ones (20 Hz, beta). Gamma and betaoscillations have different source generators,the latter coming from deeper cerebral areas.This disruption of gamma oscillations inschizophrenia is in keeping with theoriesof disruption of GABA/glutamate activity,and with disturbed cognition, especially withworking memory (Rotarka-Jagiela et al., 2009;Haenschel et al., 2009; Haenschel et al., 2007).
Radiological Studies
A common saying throughout the 1900s wasthat ‘schizophrenia was the graveyard ofneuropathologists’. That is, numerous neu-ropathologists had worked for many years tofind neuropathological evidence correlatingwith the behavioural changes observed by pa-tients and clinicians, all to no avail. A modernupdate of that saying might be that ‘schizophre-nia is the graveyard of neuroimagers’. However,what is different with the modern methods isthat many, in fact most, published imagingstudies do in fact find differences betweenpatients with schizophrenia and controls.Nonetheless, often the studies are methodologi-cally flawed or are of small sample size and theresults do not replicate.
MRI
The earlier findings with CT are reviewed inprevious editions of this book, but remain bothinteresting and valid. MRI has become the pre-dominant research method. There are well over1000 studies, and they have served to confirmmuch of the earlier CT data, but in addition haveprovided new findings. A summary is given inTable 7.8.
With MRI it has been possible to confirm thatthe cerebral cortex is smaller than in controls
Table 7.7 Some features of ventricular enlargementof schizophrenia
Early brain damage or birth complicationPoorer premorbid adjustmentMore negative symptomsLess positive symptomsCognitive declinePoorer response to treatmentMore minor neurological signsDecreased CSF–HVADecreased frontal CBF
(Zipursky et al., 1992), even at the onset of theillness (Degreef et al., 1991). The degree of losscorrelates with the severity (Young et al., 1991)and duration of the schizophrenic symptoms(Waddington et al., 1991). Ventricular enlarge-ment has been confirmed in many reports, againat the onset of the illness (Degreef et al., 1991).The relationship of this to positive and negativesymptoms is unclear (Table 7.7).
One of the significant advantages of MRIis the production of high-resolution images oftemporal-lobe structures. Reduced temporal-lobe volume and increased size of thetemporal horn of the lateral ventricle is a well-replicated finding (Suddath et al., 1989;Kawasaki et al., 1993). Smaller superiortemporal-lobe gyri on the left have been notedby several authors, with correlations to clinicalphenomena, namely auditory hallucinations(Barta et al., 1990), thought disorder (Shentonet al., 1992) and reduced P300 amplitude(McCarley et al., 1993). These findings are ofparticular interest since the superior temporalgyrus contains the planum temporale andHeschl’s gyrus (primary auditory cortex) andmerges into Wernicke’s area, and is thereforeintimately involved with language and themanipulation of symbolic knowledge.
Suddath et al. (1990) studied 15 MZ twinsdiscordant for schizophrenia, and found theaffected twin to show larger lateral and thirdventricles, and smaller hippocampi with de-creased grey-matter volume, an effect greater onthe left. No such differences were found in nor-mal twin pairs. In a further study of twin pairs,they noted a significant relationship between theleft hippocampal volume, and rCBF activation

The Schizophrenias 167
Table 7.8 Summary of MRI findings in schizophrenia
Region of interest Findings
Cerebrum Volume loss in cerebral cortex and abnormal relaxation timesCerebellum InconclusiveVentricles Enlarged lateral and third ventriclesTemporal lobes Abnormal relaxation times and volume loss in grey matterSuperior temporal gyrus Smaller – especially on the leftMesial temporal structures Abnormal relaxation times and smaller
amygdala–hippocampus–parahippocampus in particular the left side;associations between hippocampal size and prefrontal cortex activity;reduced NAA in left hippocampus with MRS
Frontal lobes Smaller and abnormal relaxation times; decreased phospholipid turnoverCaudate nucleus Various reports, smaller and largerThalamus SmallerSeptum pellucidum Enlarged and higher incidence of cavum septum pellucidumCorpus callosum Thinner/thicker/longer/shape distortion or normalCingulate gyrus Smaller on both sidesGender effects Brain abnormalities more in malesProgression Ventricular enlargement – nonprogressive > progressive
Brain volume loss – cortical thinningClinical correlation Positive symptoms: mesial temporal structures and superior temporal gyrus
Negative symptoms: ventricular enlargement and frontal lobe abnormalities
in the prefrontal cortex with the Wisconsin card-sorting test with differences between healthyand affected twins. In the affected twins, pre-frontal activation was correlated to both rightand left hippocampal volumes.
Individual structures in the temporal lobehave also been examined. The hippocampi havebeen reported smaller, a finding that is morerobust on the left (Breier et al., 1992; Weinbergeret al., 1992; Bogerts et al., 1993), and in onestudy correlated with the severity of positivesymptoms (Bogerts et al., 1993). The amygdala,a much more difficult structure to measurethan the hippocampus, is also probably reducedin size on the left (Barta et al., 1990; Shentonet al., 1992) or bilaterally (Breier et al., 1992). Theparahippocampal gyrus is also smaller on theleft (Shenton et al., 1992; Kawasaki et al., 1993)or bilaterally (McCarley et al., 1993).
The frontal cortex has also been investigated.Abnormal relaxation times of both T1 and T2have been reported, in some studies correlatedwith the severity of negative symptoms (Bessonet al., 1987; Williamson et al., 1992). The pre-frontal cortex is also smaller (Breier et al., 1992),the size correlating with reduction of prefrontalactivation during the Wisconsin card-sorting
test (Weinberger et al., 1992), but also with non-deficit symptoms (Buchanan et al., 1993). How-ever, unlike the findings with the temporallobes, many of the investigations of frontal areasare negative (Suddath et al., 1990).
Other MRI findings include increased thirdventricular enlargement, which is correlatedwith the degree of cognitive deficit (Bornsteinet al., 1992); variable abnormalities of thecorpus callosum in thickness, length or shape(Casanova et al., 1990), which findings can-not yet be resolved; smaller cingulate gyri(Blackwood et al., 1991); and less grey-mattervolume in areas of heteromodal associationcortex such as the dorsolateral prefrontal cortex,the inferior parietal area and the superiortemporal gyrus (Schlaepfer et al., 1994).
Several of the MRI studies have noted greatereffects in male patients (Waddington et al., 1991;O’Callaghan et al., 1992). Most now agree thatthe bulk of ventricular enlargement is earlyin the disease course and reaches a plateau(Borgwardt et al., 2009; Delisi, 2008).
A particularly interesting MRI methodinvolves diffusion tensor imaging (DTI), whichallows one to test white-matter fibre integrityand potential anatomic connectiveness. DTI

168 Biological Psychiatry
studies in schizophrenia have repeatedly foundabnormalities in white-matter fibre tracts.Included are the uncinate fasciculus. As withmost findings in schizophrenia, it is not clearif these changes are primary, or simply reflectproblems elsewhere in the brain and are ‘Wal-lerian degeneration-like’ (Delisi et al., 2006a)
A summary of the morphological MRIfindings is that nearly all reported studieshave found abnormalities of morphology inschizophrenia (Tables 7.7 and 7.8). Smaller brainsize, third and lateral ventricular atrophy andincreased size of the temporal horns are robustfindings. Abnormalities of the left temporallobe seem to be reported more than findings onthe right, especially with decreases in size ofthe superior temporal gyrus and hippocampus,which seem inversely correlated with the pres-ence of positive symptoms. The frontal lobes arealso abnormal. These data substantially supportthe neuropathological data presented above,and emphasize the relevance of abnormalitiesof the limbic system, especially on the left, inthe pathology of schizophrenia.
Unfortunately, contemporary meetings of theAmerican Psychiatric Association or the USSociety of Biological Psychiatry, or other forumsrelated to schizophrenia research, are filled withposter after poster of imaging studies, but oftenwithout an ability to extrapolate the findingsinto a comprehensive understanding of the ill-ness. The vast and ever-growing literature how-ever can be distilled down into a few keyfindings that appear to be replicated and tendto transcend the different methods (CT, MRI):
1. Enlargement of the lateral ventricles, partic-ularly the left, and the temporal horn.
2. Diffuse grey-matter reductions and thinningbilaterally.
3. Reduced white-matter integrity (particularlynow as seen with DTI).
4. Reduced size of the entire temporal cortex,superior temporal gyrus and hippocampus.
There are also multiple reports of increasedbrain asymmetries, abnormalities of the cavumseptum pelllucidum and corpus callosum, andenlargement of the caudates with medications,particularly the antipsychotic medications.
Studies of individuals at first onset of psy-chosis and then following them through thefirst phases of the illness have shown that withtime there is a decrease in size of the left parahip-pocampal gyrus, bilateral cingulate gyri and leftfusiform and orbitofrontal gyri.
Recent longitudinal studies have shown thatmany of the abnormalities are progressive, withleft ventricular expansion, bilateral hemisphericvolume decreases, changes in the cerebellumand corpus-callosum thinning. Relatives fromhigh-risk families who may be exhibiting pro-dromal symptoms also have measurable brainchanges as a group. The high-risk individu-als had reduced apparent diffusion coefficient(ACD) DTI values in the left parahippocampalgyrus, lingual gyrus and superior and mid-dle frontal gyri compared to controls (Delisiet al., 2006a).
The interested reader is referred to severalrecent reviews of this massively expanding andcomplex area (Abi-Dargham and Guillin, 2007;Delisi et al., 2004, 2006a, 2006b). A recentsummit of the experts in this area concluded‘(1) that progressive brain change associatedwith schizophrenia is a real phenomenon, (2)that it is widespread in the brain, but that (3) itvaries among individuals in how widespread orsevere it is and it varies in the timing. (4) It wasgenerally agreed that there is much evidence tosuggest that in the majority of patients it occursearly in the illness and levels off. (5) Althoughthe underlying cause is not known, it could bepartly genetic and cannot wholly be accountedfor by pharmacological treatment. (6) It clearlyhas clinical implications; and (7) its unknowncause is a likely future target for pharmaceuticalintervention’ (Borgwardt et al., 2009).
CBF and PET Studies
Ingvar and Franzen (1974) initially reported thatschizophrenic patients had normal mean hemi-sphere blood flows, but demonstrated a shiftin distribution such that higher levels were lesscommon in frontal structures and more com-mon in postcentral structures when comparedwith controls. This ‘hypofrontality’ has becomea well-replicated finding using several different

The Schizophrenias 169
imaging techniques. However, like most areaswith functional brain imaging, there is a prob-lem with causality. Does the hypofrontalityoccur because the patients with schizophre-nia are not activating the prefrontal cortex aswell – that is, they are not doing the task aswell – as controls? Or is it primary? We still donot understand this basic problem, which con-tinues to plaque the early PET studies and themore recent fMRI BOLD-activation studies.
Several early studies used xenon inhalationto measure CBF and used brain-activation par-adigms. For example, Gur et al. (1983a, 1983b),in medicated patients, assessed cerebral activityduring verbal and spatial tasks. No hypo-frontality was seen, but schizophrenic patients,unlike controls, showed no changes in hemi-sphere activation during the verbal task, anda greater increase than expected in left hemi-sphere activity when carrying out the spatialtask. Further investigations on unmedicatedpatients (Gur et al., 1985) showed higherresting left hemisphere flow. Further, moreseverely affected patients showed decreasesof anterior left hemisphere activity duringspatial tasks, a pattern rarely found in normals.Their data, they suggested, supported ahypothesis of left-hemisphere overactivationin schizophrenia, and the differences betweenmedicated and unmedicated patients suggestedthat medication helps restore symmetricalblood flow, the main effect being on theleft hemisphere.
Weinberger et al. (1986) have specificallytested frontal-lobe function by administeringpatients the Wisconsin card-sorting test duringxenon-133 inhalation. Controlled cognitivetasks, such as a number-matching test, werealso used, patients being drug-free for aminimum of four weeks. During the number-matching task no differences were notedbetween patients and controls, but with thefrontal-lobe task the clear increases seen incontrols were not seen in frontal regions inthe schizophrenic patients. The changes wereregionally specific, in particular involving thedorsolateral aspect of the prefrontal associationcortex. These data, they suggested, indicatethat patients with schizophrenia have a specific
physiological dysfunction of prefrontal cortex.In later studies (Berman et al., 1986), similarresults have been obtained in patients offmedication and in twin studies, only theaffected MZ twin shows hypofrontality onactivation (Berman et al., 1992). Further, sinceschizophrenic patients and controls did notdiffer on a continuous-performance task withregards to CBF, the abnormalities recordedwere thought to be independent of medicationstatus and of state factors such as attention andmental effort.
There have been many SPECT- and PET-activation studies in schizophrenia. The earlierPET investigations were largely with glucose,but more recently oxygen and ligand studieshave yielded the more interesting results. Acaveat to most of these studies is that theyinvariably use patients that have been on neu-roleptic medications, even if they were free frommedication at the time of testing. Generally,hypofrontality has been reported (Buchsbaumet al., 1990; Siegel et al., 1993), although thereis considerable overlap with control values,and there are several negative studies, espe-cially in acute-onset medication-free patients(Sheppard et al., 1983). Hypofrontality does notseem to correlate with ventricular dilatation andis increased by neuroleptic medication (Delisiand Buchsbaum, 1986). The hypofrontality is inpart a reflection of hyperoccipitality, and is moreprominent in medial rather than lateral frontalcortex (Siegel et al., 1993).
Increased anterior temporal-lobe activity hasbeen shown with deoxyglucose PET (Delisiet al., 1989) and oxygen (Liddle et al., 1992).
Hallucinations have been associated withincreased blood flow in Broca’s area withSPECT (McGuire et al., 1993) and PET (Cleghornet al., 1992), and with lower metabolism in theregion of Wernicke’s area and increased activityin the anterior cingulate regions and stria-tum with fluorodeoxyglucose PET (Cleghornet al., 1992).
Based on factor analysis of patients’ symp-toms in schizophrenia, Liddle (1987) proposedthree clusters, respectively referred to as psy-chomotor poverty, reality distortion and dis-organization syndromes. The former involves

170 Biological Psychiatry
poverty of speech, affect and movement; realitydistortion comprises hallucinations and delu-sions; and the disorganization syndrome refersto formal thought disorder and inappropri-ate affect. While each syndrome can coexist inthe same individual, they were postulated torepresent independent functional systems, cor-responding to limbic and subcortical distributedbrain systems.
Using 15O2-PET and SPM, Liddle et al. (1992)identified separate neuroanatomical profilesfor the three clusters shown in Table 7.9(Liddle et al., 1992). These data, especially forthe reality-distortion factor, have receivedpartial replication (Kaplan et al., 1993). Fristonet al. (1992) have identified the left parahip-pocampal region as being the centralneuroanatomical substrate of schizophrenia,abnormalities here being associated withdysfunction in distributed limbic-associationareas, the pattern of distribution dependenton the presenting behavioural syndrome. Theprimacy of the hippocampus and cingulateregion has also been discussed by Tammingaet al. (1992).
Friston et al. (1992) point out a resolu-tion to the conflicting data with regardsto hypofrontality. Thus, a patient can haveregional hypofrontality (associated with psy-chomotor poverty in the psychomotor-povertysyndrome) and hyperfrontality (in the anteriorcingulate in the disorganisation syndrome).
There is little conformity of data with regardsto basal ganglia findings in psychotic patients,
high, normal and low values being noted(Volkow et al., 1985; Gur, 1986; Buchsbaumet al., 1992). Increased values in basal gangliaregions following neuroleptic treatment arereported from several PET studies (DeLisiand Buchsbaum, 1986; Gur, 1986; Cleghornet al., 1992). These data are in keeping with theknown high dopamine content of these regionsof the brain and their possible abnormalities inpatients with psychosis.
Following an analysis of 50 male schizo-phrenics and controls using SPM, Andreasen(1995) has highlighted the thalamus and whitematter connecting to the frontal lobes as possi-ble key areas of abnormality. More recently therole of the thalamus has been emphasized byBuchsbaum and colleagues (Hazlett et al., 2008;Byne et al., 2009).
Examination of the dopamine hypothesishas been further enhanced by the developmentof selective radioactive dopamine ligands(e.g. fallypride and 11c NPA for the D2/D3receptor), although none are selective for justthe D2 receptor. In the past much attentionwas given to striatal activity, but with theseligands linked to higher-resolution scanners(as low as 2 mm), extrastiatal dopamine hasbeen examined. The thalamus has becomea centrepiece, especially the dorso-medialnucleus. There are several studies suggesting adecreased size and/or activity of this nucleus(Byne et al., 2006) and decreased dopaminebinding (Buchsbaum et al.,2006). Interestingly,the majority of studies, but not all, report
Table 7.9 PET findings in the syndromes of schizophrenia (Liddle et al., 1992)
Syndrome cluster Clinical features PET
Psychomotor poverty Poverty of speech, affect, movement Decreased: prefrontal L parietalIncreased: caudate
Reality distortion Hallucinations and delusions Increased: L – parahippocampal; ventralstriatum
Decreased: R – post-cingulate;post-temporal
Disorganization Thought disorder; inappropriate affect Increased: ant cingulate, mediodorsalthalamus
Decreased: R frontotemporal, Broca’sarea; R, L angular gyrus
Increased/decreased refers to cerebral blood flow compared with controls.

The Schizophrenias 171
that the left side is the more affected (Kessleret al., 2009). The thalamus is looped with thebasal ganglia and with frontal cortex, themedio-dorsal nucleus being a relay betweensensory and cognitive systems representing anadditional way in which dopamine may beinvolved in the pathogenesis of schizophrenia.There is in normals usually a tight correlationbetween frontal and medio-dorsal thalamicactivity, which is lost in schizophrenia (Hazlettet al., 2008).
The Viral Hypothesis
As noted in earlier chapters, the possibility thatviral infections of the limbic system are asso-ciated with some cases of psychosis has hada long history. There are several reasons tosearch for viruses, including the known excessof winter births in schizophrenia (Fuller Torreyet al., 1977), the schizophrenia-like presentationsof some patients with known encephalitis, thediscovery of slow viruses which affect the ner-vous system, but whose effects are delayed formany years (Fuller Torrey and Peterson, 1973),and the reporting by some authors of evidencefor viral activity in schizophrenic patients.
A second line of evidence has been to exam-ine serum and CSF for abnormal antibody titres,or to seek impaired immunological function inschizophrenic patients. Scattered early reportsof decreased delayed hypersensitivity, priorto the introduction of neuroleptic drugs, areof interest, implying possible immunologicaldysfunction which cannot be attributed to theseagents (Delisi, 1984). Estimations of lympho-cyte characteristics, including the percent-ages of B- and T-cells, have produced variabledata, as has the quantitative assessment ofvarious immunoglobulin classes. OligoclonalIgG bands appear normal (Roos et al., 1985).Reports of raised cytomegalovirus antibodylevels in CSF in up to 70% of patients (Albrechtet al., 1980) have not consistently been replicated(Shrikhande et al., 1985; Alexander et al., 1992)and post-mortem brain studies using stainingfor these viruses have also been negative(Stevens et al., 1984).
There is thus minimal evidence that viralillness is aetiologically related to schizophrenia,and the variable findings, in particular theabnormal features of the immunological system,may reflect immunosuppression related tomedications.
The search for a viral aetiology has turnedinto a quest to implicate prenatal infection, andthe influenza virus has attracted most attention.As noted above, there is good evidence that thereis an excess of winter births in schizophrenia.From over 50 studies, the number that confirmthis effect outways negative results. The effectmay be more robust in females and those with-out a family history, and exposure to the A2influenza virus has been most strongly impli-cated (Mednick et al., 1988; O’Callaghan, 1991;Adams et al., 1993; Takei et al., 1994). Infantsin their second trimester of foetal developmentwere said to be vulnerable to later developingschizophrenia, timing which fits well with someof the neuronal development abnormalities dis-cussed above (Jacob and Beckman, 1989) and theobserved excess of minor physical abnormalitiesnoted in schizophrenics.
This view has its detractors, however. Theyclaim that the largest cohorts do not revealthe effect, that there are statistical objectionsto the handling of the data and that prospec-tive studies are negative (Crow, 1994). In theNational Child Development Study in the UK,in which all children born in a specified weekin 1958 were followed at regular intervals, noexcess of schizophrenia was noted in children ofmothers who suffered influenza in the 1957 epi-demic (Crow, 1994). A further problem seemsto be that the influenza virus fails to cross theplacental barrier.
Another way to examine this theory, orat least the theory that chronic infection hassomething to do with the slow progression ofschizophrenia, has been to examine the inflam-matory cytokine profiles. The implication is thatthere is a mild but chronic immune process thatalters certain brain structures and may alterneurochemical expression. Thus the proinflam-matory cytokines (INF, TNF) shift the balanceof the metabolism of tryptophan from 5-HT

172 Biological Psychiatry
towards kynurenine, a compound which hasbeen shown elevated in CSF in schizophreniaand is a NMDA-receptor antagonist.
Associations with Neurological Disease
The most comprehensive survey of the rela-tionship of schizophrenia-like psychoses toneurological conditions is that of Davison andBagley (1969). It has already been pointed out(in Chapter 3) that a variety of pathologiesthat affect the limbic system may lead to a
disorder with a phenomenological appearanceof a schizophreniform psychosis, the mostconvincing data so far being collected forepilepsy, in particular temporal-lobe epilepsy(see Chapter 10).
Table 7.10 lists the neurological conditionsthat have been associated with a schizophreni-form psychosis, giving the expected number andthe actual number in the early published litera-ture. Taken from Davison and Bagley’s review,it indicates a higher than expected frequency, inparticular for Huntington’s chorea, narcolepsy,
Table 7.10 Comparison of the relative proportions of CNS disorders with psychosis in the1958–1967 literature and their prevalence in the general population (from Davison and Bagley,1969, p. 149)
CNS disorder Prevalence in Distribution of psychotic casesgeneral population in 1958–1967 literature
(per 100 000)a
Expected number Actual number
Trauma – – 532Epilepsy 548 211 276Huntington’s chorea 4 2 86b
Cerebrovascular disease 450 173 42b
Parkinsonism 114 44 20b
Narcolepsy – – 19b
Choreoathetosis – – 19b
Cerebral glioma 8.3 3 19b
Benign cerebral tumour 30 12 17Pituitary adenoma 5.4 2 17b
Postmeningitis/encephalitis – – 16Multiple sclerosis 80 30 11b
Congenital disorders – – 8General paresis 24 9 5Hepatic encephalopathy – – 5Wilson’s disease – – 4Cerebellar degeneration 7 3 3Other cerebral degeneration – – 3Cerebral lipoidosis – – 3Hypoglycaemia – – 3Motor neurone disease 11 4 2Cerebral reticulosis – – 2Torsion spasm – – 2Leber’s optic atrophy – – 1Phenylketonuria – – 1Schilder’s disease – – 1Friedreich’s ataxia – – 1Myotonia congenital – – 1
aPrevalence figures taken from Brewis et al. (1966).bIndicates probable significant difference.

The Schizophrenias 173
cerebrovascular disease, cerebral gliomas andpituitary adenomata. A lower than expectedincidence occurs with Parkinson’s disease andmultiple sclerosis.
The conclusion with regards to tumoursin particular emphasizes temporal-lobe anddiencephalic locations. A survey of theworld literature on psychiatric symptomatol-ogy in Huntington’s chorea reveals an excessof schizophrenia-like and paranoid condi-tions, the psychopathology often emergingbefore the onset of the movement disorder(Trimble, 1981a). It is of interest that thiscondition is associated with relative overac-tivity of dopamine function, in contrast toParkinson’s disease, in which the incidence ofpsychosis is said to be rare, unless provokedby dopaminergic medications such as L-dopaor bromocriptine. Wilson’s disease, in whichcondition the main pathological findings aremultilobular cirrhosis of the liver and cerebralchanges maximal in the putamen, caudatenucleus and globus pallidus, is also notassociated with an excess of schizophrenia-likesymptoms. Sydenham’s chorea and idiopathicbasal ganglia calcification (Cummings, 1985)are sporadically reported to be associated witha schizophreniform psychosis.
In contrast to some of the other conditionsmentioned, multiple sclerosis is a white-matterdisease affecting in particular periventricularstructures, and its psychopathology, whichincludes emotional lability, affective disorderand a characteristic euphoria (Trimble, 1981a),is markedly different. On the other hand,metachromatic leucodystrophy is an autosomalrecessive disorder due to a deficiency of aryl-sulphatase A which leads to an accumulationof sulphated sphingolipids. In the juvenile andadult-onset forms metachromatic leucodys-trophy presents with behavioural symptoms,which include personality changes, demen-tia and a schizophrenia-like illness (Hydeet al., 1992).
Davison and Bagley (1969) particularlyemphasized diencephalic, brainstem and tem-poral lobe locations of pathology. Midline cere-bral malformations, especially cavum septum
pellucidum, agenesis of the corpus callosumand aqueduct stenosis, are also overrepresentedin patients presenting with schizophrenia (Scottet al., 1993).
There is additional literature emphasizingneurological impairments and signs which maybe found in patients at risk for schizophreniaor those with the condition. Offspring ofschizophrenic parents, thus representing ahigh-risk group for the later development of thedisorder, have an increased number of preg-nancy and birth complications. The high-risksubjects who have a psychiatric breakdownhave the greatest number of such complications,and show abnormal electrodermal galvanicskin responses with shorter latency, slowerhabituation and greater resistance to extinction(Parnas et al., 1981). Further, infants at riskfor schizophrenia show increased evidence ofneurological dysfunction, with neurological softsigns, poor motor coordination and perceptualdeficits (Marcus et al., 1985). Schizophrenicpatients have lower birth weights than expected(Parnas et al., 1981), and cerebral dysfunction,as shown by neurological signs, EEG abnor-malities or a history of seizures, is overreportedin patients with infantile psychosis (Kolvinet al., 1971).
Data from the National Child DevelopmentStudy showed children who later developedschizophrenia to have early language, readingand motoric disturbances, and these abnormal-ities are seen earlier and more frequently inmales (Crow, 1994). Similar findings are beingreported in more recent studies of high-risk peo-ple which emphasize neuromotor developmentand cognition, especially memory/learning.Interestingly, such studies suggest that familyand environmental variables are largely sec-ondary or indirect associations. Nonspecificaffective symptomatology prior to the onset ofthe disorder seems to be of more importancethan most psychotic phenomena (Owens andJohnstone, 2006).
Patients diagnosed as schizophrenic fre-quently show neurological abnormalities onroutine testing. These affect up to 60% ofpatients and cannot be solely ascribed to

174 Biological Psychiatry
medication or undiagnosed neurological illness(Woods and Short, 1985); they may also bedetected in a high proportion of relatives(Kinney et al., 1986). Potential frontal-lobe signs,such as the grasp reflex, and perseveration areespecially reported (Cox and Ludwig, 1979),while Fuller Torrey (1980) reported abnormalface–hand tests (particularly pronounced inthe right hand, suggesting left-hemisphereinvolvement) and graphesthesia. Minor motorand sensory disturbances, more recognizablechoreoathetotic, dystonic and tic-like presen-tations, gait disturbances, difficulties withcoordination and smooth performance ofmotor activities, reflex changes (increased ordecreased) and the presence of infantile reflexessuch as palmomental reflexes, mirror move-ments and variable Babinski responses, have allbeen reported (Claude and Bourguignon, 1927;Quitkin et al., 1976; Tucker and Silberfarb, 1978;Keshavan et al., 1979). These have an inverserelationship to IQ levels (Quitkin et al., 1976),but no apparent association to prognosis.
Abnormalities of eye blinking (Stevens, 1978),either decreased or increased, or episodic rapidparoxysms of blinking, have been noted inschizophrenia, the paroxysms being associ-ated with psychotic episodes. Disturbed eyetracking, including abnormal smooth-pursuiteye movements and saccadic eye movements,are also reported. These movements are madeas the fovea tracks a moving object. Saccadesare fast but ballistic movements that bringthe fovea and the target together, while thesmooth-pursuit eye movements are responsiblefor fixation of slower-moving targets, andthus are continuous with the fovea sitedon the target. Saccadic movements can bevoluntarily executed, whereas smooth-pursuitmovements require stimulus activation andare maintained by attention to the target. Upto 85% of schizophrenic patients are reportedto show abnormal smooth-pursuit tracking,similar abnormalities being noted in 34% ofrelatives (Holzman et al., 1984). This does notappear to be related to inattention, motivationor drug effects, and higher concordance forthe abnormality is shown for MZ as opposedto DZ twins. Saccadic abnormalities have also
been described in schizophrenia (Mialet andPichot, 1981).
Neuropsychological Disturbancesin Schizophrenia
That patients with schizophrenia have alteredneuropsychological performance on a varietyof tests has been known for many years and thefindings have been reviewed by several authors(Flor-Henry, 1983; Cutting, 1990). The CognitiveNeuroscience Treatment Research to ImproveCognition in Schizophrenia (CNTRICS) grouphas summarized the literature in specificdomains and has issued recommendationsabout standardized tests or measures of atten-tion, social cognition and working memory(Barch et al., 2009a, 2009b; Carter et al., 2009;Nuechterlein et al., 2009). In general, all whohave looked for it have noted intellectualdecline of some sort in schizophrenic patients,reflecting Kraepelin’s (1919) summary that pro-found dementia occurs in 75% of patients withhebephrenia and 59% of those with catatonia.The Halstead–Reitan test battery, designed toidentify patients with brain damage, fails todiscriminate between schizophrenic patientsand those with known neurological damage(Heaton and Crowley, 1981), and decrementsare more likely to be found in those with longerhospitalizations and chronic illness (Goldsteinand Halperin, 1977). The decline does notappear to be related to neuroleptic medication;in fact, cognitive testing is often seen to improvein patients receiving these drugs (Heaton andCrowley, 1981).
Patients with simple schizophrenia showthe most markedly dilapidated cognition,while those with a delusional form of thedisorder may be least impaired (Robertson andTaylor, 1985). Schizophrenic patients demon-strate average reading and spelling abilities inthe setting of lower IQ and memory scores,the former tasks reflecting premorbid ability;similar patterns are noted in the dementias(Dalby and Williams, 1986).
Other studies emphasize altered attention,psychomotor speed and problem-solving(Goldberg et al., 1993), and the concept of

The Schizophrenias 175
deterioration of working memory has becomeimportant. This involves the memory capacityto hold information for short periods of time,usually seconds. It is required for guidingfuture behaviour from representations of theoutside world, rather than for responding toimmediate stimuli (Goldman-Rakik, 1994).It provides temporal and spatial continuitybetween past experience and present actions.In animal studies it is impaired by frontallesions, which produce decrements on delayedresponse tasks. During such delays, increasedneuronal firing is found in Brodmann’s area46 of primate brains. This is equivalent to partof the middle frontal gyrus in humans, and inprimates is anterior to area 8, lesions of whichproduce smooth-pursuit eye deficits, similar tothose reported in schizophrenia. Since patientswith schizophrenia can also be shown to beimpaired on delayed-response tasks, it has beensuggested that these frontal impairments arecentral to the psychology of schizophrenia.
Liddle and Morris (1991) presented cogni-tive data on their patients, separated into thethree syndromes discussed above. Psychomo-tor poverty was associated with impairment ofabstract thinking and long-term memory; disor-ganization syndrome with impaired concentra-tion and new learning; while reality distortionwas associated only with impairment of figureground perception. Frontal-lobe tasks were per-formed badly by those in the psychomotor-poverty and disorganization groups, but weredone better by patients in the reality-distortiongroup. The disorganization syndrome was asso-ciated with impaired verbal fluency.
Johnstone et al. (1978) have drawn attentionto age disorientation in chronic schizophrenicpatients, affecting approximately 25%, in whichthey usually underestimate their age. Thosewith this problem are more likely to have had ayounger first admission to hospital and a longerduration of stay. This same group has drawnattention to the ‘dementia’ of dementia praecox.They thus note that there appears to be a sub-group of patients with schizophrenia who notonly show intellectual impairment but on CTscan demonstrate evidence of structural braindamage. These patients often display ‘negative
features’ such as poverty of speech, retardationand affective changes, while patients with ‘pos-itive features’ such as hallucinations, delusionsand thought disorder are less likely to show acognitive decline.
Laterality effects have also been examined.Schizophrenic patients perform abnormallyon tests of aphasia. On a battery of neuropsy-chological tasks including subsets from theHalstead–Reitan and the Luria–Nebraskabatteries, schizophrenic patients (the majoritydrug-free) not only displayed marked impair-ments but had maximal abnormalities on testsrelated to frontotemporal functions bilater-ally (Taylor and Abrams, 1984). In a morecomprehensive evaluation, Flor-Henry (1983)compared large numbers of schizophrenicand affective-disorder patients and notedasymmetric frontotemporal dysfunction, theleft side being more impaired than the right inthe schizophrenic sample. When an analysis ofcovariance was carried out, looking at depres-sion, mania, schizophrenia and control patients,a continuum of increasing cerebral disorgani-zation was seen, depression showing minimalchanges, while schizophrenia showed maximal.
Recently much attention has been paid tothe potential for cognitive abnormalities to beendophenotypic variants, and deficits of execu-tive function and working memory have beenthe focus of attention (Gur et al., 2007). The lat-ter is capacity-limited; in other words, thereis an inverted U-shaped curve of efficiency innormals, closely linked to increased activationof the dorsolateral prefrontal cortex. Abnor-malities of working memory have been wellrecorded, schizophrenic patients operating at orbeyond efficiency being unable to maintain per-formance within their expected capacity. Duringworking-memory tasks and imaging they showeither hyperfrontality or hypofrontality in acomplex relationship with task difficulty andperformance (Karlsgodt et al., 2009). Unaffectedsibs of patients also show difficulties with work-ing memory, including unaffected MZ twins(Prata et al., 2008a, 2008b; Filbey et al., 2008;Toulopoulou et al., 2006) and genetic links havebeen probed. The latter have included an asso-ciation with the disrupted-in-schizophrenia 1

176 Biological Psychiatry
(DISC1) gene (Matsuzaki and Tohyama, 2007;Ishizuka et al., 2006; Callicott et al., 2005).
Another strategy has been to use high-risksubjects. Neuropsychological impairments havebeen shown in those who later develop the dis-order, more severe than that seen in those whogo on to develop bipolar disorders, and work-ing memory again is highlighted. Performanceabnormalities on verbal tasks, including verballearning and fluency, are most often reportedin those who later convert to schizophrenia.However, these early cognitive problems do notclearly correlate with later psychotic symptoms,except weakly with negative features. What ismore relevant is the identification of abnormalthinking, reflecting abnormal cognitive struc-ture in these high-risk people. In addition tothese cognitive variables, other strong predic-tors are high scores on the SIPS and SIS, bizarrethinking, schizotypal personality disorder, sus-piciousness, poor social functioning and poorsocial skills. These findings link with otherssuch as deficits of facial recognition and emo-tional discrimination of faces in schizophrenia,correlated with abnormal early evoked poten-tials, suggesting processing problems occur atan early stage of sensory processing.
Of particular interest is the potential link andoverlap with findings from patients with autism,who show many similarities to and differencesfrom schizophrenia. The largest similarities arein the problems with social cues, face processing,empathy and understanding the actions of oth-ers, called ‘theory of mind’ (Anckarsater, 2006;Rapoport et al., 2009; Vollm et al., 2006).
SOME OUTSTANDING ISSUES
The evidence reviewed clearly indicates a sig-nificant genetic contribution towards the devel-opment of schizophrenia. However, it is clearthat this contribution to schizophrenia doesnot explain all the variance, and environmentalvariables have been persistently sought. Indi-vidually, these environmental factors are ofunknown effect size and several have been sug-gested, although exactly how they interact withthe genetic liability is unclear.
Further, the consensus that what is inheritedis a schizophrenia spectrum, as opposed toschizophrenia per se, has gained ground, andcertain biological markers, for example plateletMAO activity or dysfunction of eye move-ments, may reflect upon underlying geneti-cally determined biochemical or neurocircuitrypropensities to develop psychosis under certainconditions. The search for the gene(s) responsi-ble for the schizophrenias continues. Some obvi-ous candidates, especially relating to dopamineregulation, seem to have been ruled out. Theconsensus has been to look for co-acting loci, andthere have been many reports of linkage find-ings or results from genome-wide scans, withquite heterogenous results; some 30–40 suscep-tibility genes have been identified at thresholdsignificance. In part this may reflect the factthat genetic markers are themselves only prox-ies for the risk variant. But there are otherconfounding factors, including the problem ofthe quality of genotype analysis, the statisticalrequirements of such potentially large data setsand the delineation of the phenotype. What arethe features of a subset of cases that show anenhanced genetic signal? The strategy of lookingat endophenotypes, and away from DSM IV-TR-defined categories, seems a promising wayforward, but to date no endophenotypes relatedto schizophrenia have yielded any secrets togenetics. However, recent attempts to combinegenetics with brain imaging are proving inter-esting, examining the genetic contributions tothe cerebral structural, functional changes andendophenotypic variance.
There was hope that the newer generation ofgenome-wide studies might prove more power-ful than linkage and candidate gene strategies.That promise has not been fulfilled as yet. Thelatest genome-wide studies if anything tendto suggest similarities, rather than differences,between bipolar affective disorders and theschizophrenias (Esslinger et al., 2009; Keshavanet al., 2007; Tan et al., 2008; van Haren et al., 2008;Lin and Mitchell, 2008; Thaker, 2008; van Oset al., 2008) (see Chapter 8).
To date, and so many years after Slater’s stud-ies, the picture remains that there may be severalor many genes of small effect contributing to the

The Schizophrenias 177
schizophrenia spectrum. Essentially we may belearning that, with only a few exceptions suchas Huntington’s disease, there are no genes formental illness per se, but rather genetic effectsthat relate to information processing in thebrain and subsequent cognitive and behaviouralstrategies, the endophenotypes, which providea substrate for the later development of the phe-notype. No longer is a statistical relationship be-tween genes and a DSM IV-TR diagnosis beinglooked for, but rather the relationship betweenthe neurobiological effects of genes and the pro-cesses that lead to any particular phenotype.
With regards to environmental agents, thereis evidence that some schizophrenic patientsdemonstrate increased early brain damage,either through perinatal or uterine insults.Murray et al. (1985) advocate it would be use-ful to divide schizophrenia into familial and spo-radic cases. The sporadic cases are thusassociated with increased ventricular size(highly replicated) and environmental traumasreflective of perinatal damage or early headinjury. The genetic predisposition, if strong, willpromote the disorder, while, in the presence ofa lesser genetic vulnerability, the environmentalinsult becomes necessary for the full expressionof the illness. Where there is no geneticvulnerability, as in, for example, some cases ofepilepsy, the cerebral pathology itself directlyprovokes the schizophrenia-like symptoms.
More recent discussion of environmentaleffects has concerned epigenetic and pharma-cological influences. The former should includeuterine and neonatal events on cerebral devel-opment, synaptogenesis and synaptic pruning,as well as early psychosocial stressors (Parentand Meaney, 2008). Alternative environmentalinsults have been sought, in particular neu-rological conditions, head injury or infection,for example with viruses. However, recentresearch has centred on the use of psychoactivedrugs, especially cannabis. The emphasisfrom CNS disorders is on those which affecttemporal-lobe, basal-ganglia and diencephalicfunction. Temporal-lobe disorders, in particularsuch conditions as epilepsy affecting limbicstructures, seem to be more associated withhallucinations, while basal-ganglia disorders
lead more to disturbances of motoric activity,motivation and cognition via the fronto-striatalre-entrant networks.
The pathological and MRI studies reviewedreinforce a neuroanatomical approach, empha-sizing medial temporal structures in associationwith hallucinations, paranoia and thoughtdisorder, and the basal-ganglia frontal axiswith negativism and motor signs. Such findingsemphasize that the ‘anatomy of schizophrenia’(Stevens, 1973) is predominantly related toallocortical and subcortical structures, particu-larly those of the limbic lobe (entorhinal cortex:hippocampus), the thalamus and the relatedbasal ganglia.
In cerebral development, neuronal migrationis from the ventricular zone outwards to thecortical plate. Younger neurones thus migratethrough more mature ones, and the migration isdirected by previously formed radial glial fibres.In the human entorhinal cortex, these migra-tions are complete by six months of gestation;the hippocampus and temporal neocortex aresomewhat later, the hippocampus not reachingadult volume until about the age of two years,and continuing to myelinate well into adult life(Benes et al., 1994).
The upper layers of the entorhinal cortex,especially layer 2, containing pre-alpha cells,are sites of origin of the glutamate projectionsto the hippocampus, and receive a dopaminer-gic input. It is important to note that duringnormal development, the ventricular volumeis reduced, and so abnormal development willlead to increased volumes. Further, the develop-ment of the left hemisphere is later than the right,and any damage that influences early develop-ment of these structures is therefore more likelyto impact on the left.
The parts of the entorhinal cortex involvedin pathological studies of schizophrenia areintimately connected with the insula and theorbitofrontal cortex, and it is of interest thatthese entorhinal areas are not found in otheranimals, including other primates.
Some authors have drawn attention to thelikeness of some schizophrenic symptoms tofrontal-lobe disorders. In particular this in-volves the dorsolateral prefrontal cortex, and the

178 Biological Psychiatry
symptoms include those seen following frontalinjury, such as affective changes, impairedmotivation, poor insight and other ‘defect’symptoms frequently seen in schizophrenia.Indeed, the evidence for frontal-lobe dysfunc-tion in schizophrenic patients is clear, and hasbeen noted not only in the neuropathologicalstudies but also in EEG, evoked-potential data,neuropsychological studies (especially those ofworking memory), testing for soft neurologicalsigns, and more recently imaging techniquessuch as PET and MRI.
The pathological studies of frontal corticalareas are more limited, but do suggest somechanges, which either represent evidence ofmore generalized pathology in schizophrenicbrains or are a localized contribution to thedevelopment of the psychopathology.
The orbitofrontal and temporal pole areasare connected by the uncinate fasciculus, andlesions at such sites may impair higher-ordercognitive processes and lead to disorderedsocial communication. Recent data clearlysuggest that abnormal hippocampal structureis associated with functional impairment offrontal-lobe activity, supporting a suggestionthat the temporal/limbic changes may beprimary. Alternatively, disturbances of frontalprojections to the parietal and temporal associ-ation areas may impair sensory representationsin these areas, explaining positive symptoms,setting the frontal lobes as crucial for thedevelopment of both positive and negativesymptoms. More recent imaging studies haveconcerned changes in white-matter tracts andhave identified alterations in white matter,including the corpus callosum, the uncinatefasciculus and the anterior limb of the internalcapsule. It is quite unclear whether these arepart of the structural alterations that relateto schizophrenia or are secondary to otherneuronal loss. It does seem to be the case thatmany of the structural (and functional) changesoccur early on in the disorder, are not secondaryto antipsychotic drug prescriptions and may beseen in the high-risk group before diagnosis.
The evidence for two distinct syndromesin schizophrenia has been pursued by Crowand colleagues (Crow, 1980). The suggestion
is that there is both a neurochemical and aneuropathological contribution to schizophre-nia, with two syndromes. Thus, the type Isyndrome (equivalent to acute schizophrenia) ischaracterized by positive symptoms (delusions,hallucinations and thought disorder) and isrelated to change in dopaminergic transmission.The type II syndrome (equivalent to the defectstate) is characterized by negative symptoms(affective flattening and poverty of speech) andis associated with intellectual impairment andstructural changes in the brain. Current thoughtalso involves a continuum model and includesconsideration of the schizophrenia spectrum. Itis established that abnormalities of cognitionand thinking are present well before the onsetof the actual psychosis. The high-risk studiesall come to similar conclusions, namely thata prodromal state can be identified linked tounusual thinking and cognitive problems, espe-cially with working memory and verbal tasks,which, if identified early, may be more amenableto treatment strategies than the fully-developedsyndrome. However, the studies beg the ques-tion as to whether the identified pattern shouldbe seen as part of the schizophrenia, especiallyas it also includes those who achieve a diagno-sis of schizotypal personality disorder. In otherwords, should the syndrome schizophrenia(s)not include such preludes? The role of envi-ronmental factors in the actual descent into psy-chosis remains unclear, although neurochemicalinvasions, especially from psychoactive drugssuch as cannabis, are clearly implicated.
There is certainly considerable evidence thatstructural changes are likely to be found insome schizophrenic brains and that cerebralatrophy on the whole is related to more negativesymptoms. Positive symptoms, in particular thefirst-rank symptoms of Schneider, have beenrelated to abnormal dopaminergic transmission.The dopamine hypothesis has in part stoodthe test of time. Dopamine is closely linkedto disorders of motivation (see Chapter 9), aprominent part of the schizophrenia clinicalpicture, and the known interactions betweenbrain areas such as the frontal cortex, theaccumbens and the midbrain dopamine areas(VTA) as part of the underlying anatomy of

The Schizophrenias 179
schizophrenia are supported by pathologicaland MRI findings. Patients with positivesymptoms show increased growth-hormoneresponses to apomorphine, decreased baselineprolactin, low CSF–HVA accumulation andminimal heritability (first-rank symptoms), andtend to have less cerebral atrophy. Further, thepathological and PET data reviewed suggestthat temporal-lobe, including parahippocampalgyrus, abnormalities may be more related tosuch symptoms. These data certainly supporta particular relationship between positivesymptoms, relatively normal brain structure,abnormalities of dopamine and possiblytemporal-lobe dysfunction.
In contrast, negative symptoms appear morerelated to periventricular abnormalities, cere-bral atrophy and environmental insults, and areperhaps related to dopamine dysfunction, but ina different way (as the disorder progresses anddisorder of motivation becomes more appar-ent). Experimental support for defining twosubtypes has derived from intercorrelations ofpatients’ symptoms, which indicate generallythat positive symptoms correlate positively, asdo negative symptoms, although the internalconsistency is much greater for negative symp-toms (Andreasen and Olsen, 1982).
The important contribution of abnormalitiesof dopamine to schizophrenia has been per-sistently argued. But it is well known that theantipsychotic effects of neuroleptic drugs are notconfined to schizophrenia, and they amelioratepsychotic symptoms in mania and acute organicbrain syndromes. Further, because such medica-tions alleviate some symptoms of schizophreniadoes not mean that dopamine itself has theprimary role in pathogenesis. While it has beennoted that the dopamine-blocking effect ofthese drugs is the most important for helpingthe psychosis, it should be remembered thatanticholinergic drugs alleviate the symptoms ofParkinson’s disease, even though the primarypathology in that condition relates to dopamineand not acetylcholine. Other neurochemicalhypotheses have obviously been entertained,and as noted involve serotonergic, other cate-cholaminergic, peptidergic and glutaminergicabnormalities. Mackay (1980) has argued
that a chronic dopamine deficit is relatedto schizophrenia, rather than overactivity,highlighting the reported low CSF–HVA levels.This reduced dopamine turnover leads not onlyto reduced presynaptic dopamine accumulationbut also to a compensatory postsynapticdopamine-receptor proliferation. In his theory,both positive and negative symptoms thusrelate to a defect of dopaminergic function,the positive symptoms emerging as a resultof a switch from a deficit to an increase inpresynaptic release of dopamine, the latterinteracting with the excessive number ofpostsynaptic dopamine receptors and leadingto the florid positive symptoms.
An alternative is that abnormally low pre-frontal dopamine activity is related to deficitsymptoms and excess dopamine activity in sub-cortical structures relates to positive symptoms.The mainly negative PET dopamine ligand-binding studies to date were disappointing forthose in favour of the dopamine hypothesis,although attention is now being directed toalternative dopamine receptors, especially D2,D3 and D4. The importance of frontal dopamineactivity is highlighted by the data that relateit to working memory, and the links to COMTalleles, genes associated with an enzyme closelylinked with dopamine metabolism and shownto be associated with cognitive performance(Lawrie et al., 2008a Roffman et al., 2006; vanHaren et al., 2008).
Decreased D2 and D3 receptor occupancy iswell replicated in several brain areas. Thesefindings have been enhanced by the develop-ment of selective radioactive dopamine ligands(e.g. fallypride and 11c NPA for the D2/D3receptor, although none are selective for just theD2 receptor). In the past much attention wasgiven to striatal activity, but with these ligands,extrastiatal dopamine can be estimated. The tha-lamus, especially the dorso-medial nucleus isimportant (Andreasen et al., 1994). Several stud-ies suggesting a decreased size and/or activityof this nucleus (Siegel et al., 1993; Shihabud-din et al., 2001), along with decreased dopaminebinding are reported. Lower prefrontal corti-cal dopamine has been shown to correlate withincreased striatal release. This may be mediated

180 Biological Psychiatry
by the reduced excitatory feedback from frontalcortex (glutamate) to the inhibitory GABA neu-rones in the VTA, thus increasing firing andhence output of dopamine from the VTA tostriatal structures such as the accumbens.
While dopamine remains a key transmit-ter in the schizophrenia story, it is obviouslyinvolved in a variety of psychopathologies, anda question remains as to its biological func-tion in regulating behaviour aside from its rolein motor programming. The findings relatedto disorders of motivation (Chapter 9) suggestit is related to novel reward detection in theenvironment and is interlinked with hedonia.It somehow attributes motivational salience toneural events, influencing attention and the sub-sequent behavioural repertoires. This in itselfdoes not lead to psychotic symptoms, but theabnormal attribution of salience to environmen-tal and somatic representations may lead overtime to cognitive restructuring (Kapur, 2006).This may vary with pre-existing or consequentstructural neuronal and circuitry changes, andsuch hypotheses need to be integrated with theaccumulating knowledge of brain morphologi-cal changes.
The current status of the dopamine hypothe-sis suggests that D2/D3 receptors are still centralto the theories, decreased receptor occupancybeing well replicated in several brain areas.Attention has moved to extrastriate regions andtheir involvement not only with the anatomyof the cortical–striatal–thalamic re-entrant cir-cuits, but with reciprocal relationships betweenGABA and dopamine, and the link throughglutamate.
It remains unclear what it is that drivesthe increase in dopamine activity. Early workhad suggested a link through GABA, espe-cially with a subgroup of GABA neurones, theparvalbumin-containing cells. Disturbed neu-ronal rhythmic expression in key structures is adeveloping story.
The known importance of the balancebetween GABA and glutamate within theCNS for coordinating neuronal firing andoscillations, and the importance of glutamatein the regulation of the cortical–subcorticalre-entrant circuits, has led to looking at GABA
as well as glutamate as possible substrates.Thus, glutamate input to dopamine-releasingcells (from, for example, the hippocampus andthe pedunculopontine areas) normally inducesbursts of spikes within the VTA, which aredisrupted by a deficit of glutamate. Thesetheories put more emphasis on the possiblerelevance of cortical changes as primary in thedisorder.
Crow (1993) has persistently argued againstthe Kraepelinian dichotomy, pointing out thatoverlaps of schizophrenia and affective disor-ders occur phenomenologically and genetically(the proportion of relatives of schizophrenicsthat have an affective disorder is increased).In his continuum (see Figure 7.1), whichextends from unipolar depression at one endto schizophrenia with a defect state at theother, variations of sociability and emotionalityare expressed.
Murray et al. (1992) on the other hand arguethat there is a congenital schizophrenia, witha primary genetic defect and/or a primaryenvironmental insult such as a viral infection,and abnormal neuronal maturation in crucialCNS sites. These patients show personality andsocial impairments in childhood, and developthe more severe cognitive impairments andnegative symptoms. In contrast, patients withadult-onset schizophrenia, which includes sev-eral syndromes, do not have the classic dementia
UP BP
elation
mood-incongruentdelusions
nuclear symptomsmood change
flat affect(+) (−)
SA S+A S+DS−A
Figure 7.1 The continuum concept of psychotic ill-ness. UP, unipolar affective illness; BP, bipolar; SA,schizoaffective psychosis; S, schizophrenia with andwithout significant mood disturbance (+ and – A),and with defect state (S+D) (reproduced with per-mission from Crow, 1993; Biol Psych, 2 Ed, p. 223)

The Schizophrenias 181
Table 7.11 Evidence for laterality in schizophrenia
Neurological examination Increased abnormalities in right-side sensory testing; increasedleft-handedness
Neuropsychology Association with poor performance on language tasksEEG Dominant hemisphere abnormalities on routine testing, power spectra,
with telemetry, evoked potentials and BEAM studiesCT studies Density changes; new onset casesMRI studies Especially positive symptoms: left superior temporal gyrus changesPET studies Variable: recent thalamic findingsNeurochemistry Increased dopamine, left amygdala; decreased GABA and glutamate, left
hippocampusNeuropathology Parahippocampal gyrus abnormalities in some studies onlyNeurology Epilepsy and head-injury studies
praecox and are more likely to have relapsing,remitting psychosis with positive and affec-tive symptoms.
The search for virus infections has not beenrewarding and the evidence that intrauterineinfection with the influenza virus is important isat present quite unclear. However, one impor-tance of the infective theory relates to somehistorical considerations of schizophrenia: it hasbeen suggested that schizophrenia was uncom-mon in the medical literature prior to the 19thcentury, implying, rather like AIDS encephali-tis, that it may have been a new disease, andthat an environmental agent, such as a virus,must have become prevalent around that time.The alternative is that it is an old conditionwhich has been ubiquitous and always present.The problem then is to explain its persistencein view of the low fecundity of schizophrenicpatients (Hare, 1979). This paradox remainsunresolved.
Finally, substantial evidence has accumu-lated suggesting that at least in some formsof schizophrenia, the major disturbance is in thedominant hemisphere (see Table 7.11). Becauseone of the cardinal features of schizophrenia isa disturbance of thought and language and thedominant hemisphere is known to be involvedin modulating such activities, it is hardly sur-prising that the weight of evidence suggests thatthe dominant hemisphere is primarily involved,and this continues to be the case. It is clear thatto implicate the left hemisphere alone would
be nonsensical. In fact, Cutting (1990) made astrong case for the nondominant hemispherehaving a primary role in the symptomatology,a view recently supported by Crow and hiscolleagues (Crow et al., 2007, 2009; Crow 2009).Nonetheless, the role of the dominant hemi-sphere is of outstanding importance, perhapsearly on in the disorder, or in providing thekey harmonic that reverberates through thedeveloping phenomenology. The findings frompathology, and the progressive nature of theimaging data, have initiated a discussion asto whether schizophrenia should be viewed asa progressive disorder, as Kraepelin originallyenvisaged, or even as a degenerative disorder:a ‘dementia’ in our current-day terminology.Although at first sight the degenerative hypoth-esis seems possible (schizophrenia being viewedas a dementia praecox), this is an unlikelyhypothesis. The early age of onset vis-a-visthe dementias, the subtle nature of the patho-logical changes and the eventual defect stateas opposed to a continued progressive declineargue against it.
In summary, the current perspective onschizophrenia is to view it as a neurode-velopmental disorder, with a clear geneticcomponent. The final clinical picture howevermust be viewed as a spectrum, reflectingalterations in the structure of the cognitiveand perceptual abilities of those who becomepatients, these being yoked with aberrantneuroanatomy and neurophysiology.


8Affective Disorders
INTRODUCTION
A difficulty in reviewing the literature onaffective disorders is the various classificationsthat have been used by investigators. Althoughfor the present the DSM IV-TR seems likelyto be influential, much biological informationhad been accumulated prior to its introduction,and in some areas the lack of consistency ofresults reflects the lack of similarity of patients.A recurring theme is the confusion betweendepression as an illness and a reaction oran ordinary state of misery or grief. Lewis(1934) gave as a definition of the depressivestate ‘a condition in which the clinical pictureis dominated by an unpleasant affect, nottransitory, without evidence of schizophrenicdisorder or organic disorder of the brain,and in which, moreover, the affective changeappears primary. . .’ (p. 277). This concept, theessential criterion being the disturbance ofmood, continues to be embodied in DSM IV-TR,the mood being referred to as a prolongedemotion (American Psychiatric Association,1987). Episodes of more transient mood changeor chronic minor changes of mood are referredto as dysthymic disorder, which replacesdepressive neurosis, depressive personality andsimilar categories. The issue of ‘reaction’, whichhas so long pervaded this area, is not discussed.
Winokur (1982), whose own classification dis-tinguishes a primary (bipolar/unipolar) from asecondary depression, has given support for theconcept of neurotic depression, citing positive
Biological Psychiatry 3e Michael R. Trimble and Mark S. George 2010 John Wiley & Sons, Ltd
criteria for its diagnosis. These include youngerage, poorer response to treatment, family historyof alcoholism and personality problems. Thesethen are patients with lifelong personality disor-ders who recurrently display depressive symp-toms, more often than not DSM TR IV dysthymicdisorder. They represent an entirely differentproblem from those in whom the depressiveprocess is referred to as endogenous depression.
A more widely accepted distinction, adoptedby the DSM III and originally made by Leonhard(1957), is that between unipolar and bipolarforms of affective illness. While the latterare readily identifiable, biological differencesbetween the two are emerging, and the failureto identify manic episodes in a patient’s historymay provide a further source of error.
In summary, there is still much confusionregarding the nosological status of subtypes ofdepressive illness, although the entity referredto as endogenous depression seems well rec-ognized and more homogeneous than others.The DSM III and successors have disbandedthe concept of neurotic depression, the evi-dence for which emphasizes the importanceof personality vulnerabilities for its expression,but confusion with the endogenous form stillabounds in clinical practice and research. Thisconfounds attempts to expose the biological sub-strates of the depressive process, and often leadsto inappropriate treatments. This is not to saythat patients with other forms of depressivesymptoms do not require treatment, or are not

184 Biological Psychiatry
meaningful subjects for research. In fact, sonumerous are these patients, and so chronicoften are their disorders, that more effectiveremedies urgently need to be sought for them,particularly psychotropic agents.
The nosologic confusion can be seen in thecurrent attempts to describe bipolar disorder.While there is little debate concerning bipolar1, where patients must have had a clear manicepisode, controversy begins with attempts todefine ‘softer’ bipolar disorder. Akiskal andBenazzi (2006) have argued for a bipolar 2 disor-der, where recurrent depressions alternate withperiods of hypomania or cyclothymia. Theyhave also proposed a bipolar 3 diagnosis, wheredepressions exist alongside a volatile tempera-ment or a strong family history of bipolar moodswings (Akiskal, 2007; Benazzi and Akiskal,2008; Fountoulakis and Akiskal, 2008; Gondaet al., 2009; Rihmer et al., 2007). Even more con-fusing is the ‘unipolar’ patient who developsmania or hypomania while being treated with anantidepressant, a form of iatrogenic bipolar dis-order. Clearly, the nosology continues to evolve.
Unipolar major depression is a surprisinglycommon disorder, with many studies findinga 20% lifetime incidence and a 5% pointprevalence. Bipolar disorder is less common inits purer form (i.e. not the spectrum extensionsdiscussed above), with many studies estimatinga 1% lifetime incidence. Because the affectivedisorders are so common, often developinginto chronic forms with associated otherillnesses such as diabetes and pain syndromes,major depression is currently the leadingcause of disease burden in North Americaand other high-income countries, and thefourth-leading cause worldwide. In the year2030 it is predicted to be the second-leadingcause of disease burden worldwide after HIV,according to the World Health Organization(Mathers and Loncar, 2006).
GENETICS
As with most other conditions reviewed in thisbook, the affective disorders have an important
genetic component to their pathogenesis. This isparticularly so for bipolar illness.
Family studies reveal that the risk for affectiveillness is increased severalfold in first-degree rel-atives of probands over that expected by chance(Gershon, 1983). Further, while bipolar patientsoften have relatives with unipolar illness, theconverse is uncommon. Estimates, based oncombined data from several studies, put therisk at 20% for first-degree relatives of bipolarprobands and 7% for first-degree relatives ofunipolar patients (McGuffin, 1984).
Winokur (1982) has identified three typesof unipolar illness based on familial patterns:familial pure depression disease (FPDD), witha family history of depression; depressive spec-trum disease (DSD), with a familial history ofalcoholism or antisocial personality; and spo-radic depressive disease (SDD), with negativefamily history.
The concept of a genetic spectrum for bipo-lar disorders emerges with the reporting ofan increased frequency of schizoaffective disor-der and cyclothymic personality in relatives ofprobands (Gershon, 1983). Studies of schizoaf-fective patients tend to show both affectiveillness and schizophrenia in the relatives (Angstet al., 1979), greater for affective illness, and Per-ris (1974) reported that in cycloid psychosis anincreased frequency of the same condition wasseen in relatives.
Twin data give a concordance rate, bycombining studies, of 69% for monozygotic(MZ) and 13% for dizygotic (DZ) pairs(McGuffin, 1984). Most of the investigationswere carried out prior to the acceptance ofthe unipolar/bipolar distinction, but Bertelsenet al. (1977) calculated the pairwise concordancerates for MZ twins to be 0.43 for unipolarand 0.74 for bipolar illness, the correspondingfigures for DZ pairs being 0.19 and 0.17. Theconcordance was particularly noted for females,and the differences between the unipolar andbipolar rates were significant, supporting thefamilial data that the bipolar form carries thegreatest heritability.
Price (1968) reported 67% concordancein 12 pairs of MZ twins raised apart. This

Affective Disorders 185
and the adoption study of Mendlewicz andRainer (1977), in which the rate of affectiveillness was significantly greater in biological(28%) as opposed to adoptive (7%) parentsof probands separated in early life, furthersupport the genetic contribution to the illnesses.
A single autosomal dominant gene withreduced penetrance and variable expressivitywas supported by Slater (Slater and Roth,1969), while others have suggested X-linked(Winokur and Tanna, 1969) and multifactorialmodels, implying underlying quantitativeliability to an affective disorder, greater forbipolar illness (Gershon, 1983). The X-linkedhypothesis seems unlikely, in that father–sontransmission of affective disorder is frequentlyseen, although it received initial support fromlinkage studies with colour blindness andglucose-6-phosphate dehydrogenase deficiency(Mendlewicz et al., 1980), known to be sex-linked. These data have not been consistentlyreplicated (Gershon, 1983) and no X-linkage hasbeen demonstrated.
Linkage studies of bipolar disorder to datehave not revealed reliable markers. The earlystudies in Old Order Amish pedigrees identify-ing the short arm of chromosome 11 have notbeen replicated. The gene for tyrosine hydrolaseis located at this site, but reports of a positiveassociation between tyrosine hydrolase RFLPsand bipolar illness have been mainly negative.Lack of association has also been reported forthe D1, D2, D4 and 5-HT1A receptor genes, fordopamine beta-hydrolase, and for sites on chro-mosome 5 in the region of the glucocorticoid andbeta-2 adrenergic receptors (Curtis et al., 1993;Debruyn et al., 1994; Mirow et al., 1994; Nothenet al., 1992). No mutations have been found onthe D1 receptor gene.
One study of the tryptophan hydrolase genedemonstrated a significant association betweenthat genotype and low CSF 5-HIAA levels. Theclinical associations were with suicide attemptsbut not impulsivity (Nielsen et al., 1994).
In the last decade more than 15 differentcandidate genes have been identified for mooddisorders with at least partial replication, usinggenome-wide approaches and single-nucleotide
polymorphisms (SNPs) (for review see Haydenand Nurnberger, 2006). Those of interest includebrain-derived neurotropic factor (BDNF),COMT and DISC1, a candidate gene involvedin cortical development which is also associatedwith schizophrenia.
Particular interest has recently focused onthe gene for the 5-HT transporter, called theSERT gene. The protein re-takes 5-HT into thesynaptic cleft and terminates its function. Thegene, found on chromosome 17, can have sev-eral variations – either in length, or with SNPs.The promotor region for this gene can alsohave variations with short or long repeats (5-HTTLPR). Studies on the 5-HT transporter havecombined neuroimaging and genetic methods.For example, a voxel-based morphometry studyfound less grey matter in perigenual anteriorcingulate cortex and amygdala for short allelecarriers of the 5-HTTLPR polymorphism thanfor subjects with the long/long genotype(Munafo et al., 2008; Pezawas et al., 2005).
Other recent interest involves a new fam-ily of genes called circadian locomotor outputcycles kaput, or CLOCK, genes. These genesencode proteins regulating circadian rhythm.The CLOCK protein, found in all animals, evenfruit flies, affects both the persistence and lengthof the circadian cycle. Recent studies have sug-gested that CLOCK-gene abnormalities maypredispose to developing bipolar disorder, ordetermine its age of onset (Kishi et al., 2009;Severino et al., 2009; Shi et al., 2008). Many havelong suspected that bipolar disorder is a diseaseof circadian cycles, as sleep–wake disturbancessometimes trigger cycles and the mood stateresponds to circadian manipulations. Not onlymight these findings explain this commonality,they would suggest that treatment may involveaggressively re-regulating sleep–wake cycles(McClung, 2007a, 2007b; Wood et al., 2009).
In addition to findings of high rates of familialincidence of mood disorders, some studies havealso found that family member risk and overallpopulation risk have increased in those bornin more recent decades. This ominous trend,referred to as an age-period-cohort effect, mayreflect sampling and reporting biases, but may

186 Biological Psychiatry
also be caused by other factors such as increas-ing prevalences of prior comorbid disorders(Kessler and Walters, 1998).
There is a great deal of interest in using thenew power of genetics to potentially better parseour diagnoses and provide better disease clas-sifications. However, several recent large-scalegenome-wide analyses suggest that even bipo-lar disorder and schizophrenia share commongenetic linkages, calling into question our clear-est distinction, in effect challenging the Krae-pelinean dichotomy (Czeizel, 2009; Lichtensteinet al., 2009; Maher et al., 2008; O’Donovan et al.,2008). These studies tend not to support the dis-tinction of bipolar disorder from schizophrenia,at least in terms of genetic predisposition.
METABOLIC AND BIOCHEMICALFINDINGS
Early metabolic studies found abnormalities ofelectrolyte distribution in affective disorder, inparticular retention of sodium intracellularly(including bone) during depressive episodes(Coppen and Shaw, 1963), with increased lossduring recovery. In mania even more markedchanges were reported (Coppen et al., 1965).Some interpreted these data as a reflection ofdietary changes consequent to the change ofmood. No evidence has shown that the brain isalso involved, or that the changes somehow leadto an alteration of cell membrane excitability.
Naylor et al. (1970) examined erythro-cyte electrolytes in affective disorder andreported falling sodium levels with recovery.The activity of sodium/potassium-activatedATPase, thought to reflect sodium pumpbehaviour, is lower in the depressive phase ofa manic–depressive psychosis, and possiblyin the manic phase as well, with increasedactivity on recovery. These data do suggestimpaired handling of electrolytes in associationwith affective disorder, reflected in part byalteration of membrane transport (El-Mallakhand Wyatt, 1995). Studies of calcium suggestthis is not influenced by the illness, and data onmagnesium are inconsistent.
The essential trace element vanadium hasbeen studied in relation to the electrolyte
changes. It is an inhibitor of Na+/K+ ATPase.It is reported to be raised in hair but notblood, in mania, and in blood and serum indepression, with a fall on recovery. Substancesthat lower vanadium concentration, such asascorbic acid and EDTA, are therapeutic inmania and depression (Naylor et al., 1984).Lithium responders are reported to have lowererythrocyte Na+/K+ ATPase and to showthe greatest increases in activity when onlithium compared with nonresponders (Nayloret al., 1976).
Platelet MAO activity has been reported inaffective disorders, although results show vari-ability. It is of interest, however, that severalgroups have reported increased values, particu-larly in unipolar (Reveley et al., 1981) as opposedto bipolar patients, in which reduced values aremore frequently reported. This seems a traitas opposed to a state finding, and low lev-els are also noted in first-degree relatives ofbipolar patients (Leckman et al., 1977). How-ever, there are reports of significant positivecorrelations between scores on depressive rat-ing scales and MAO activity (Mann, 1979). Someauthors report an increase in MAO activity withage and link this to the increasing incidence ofdepressive disorders in later life. MAOI drugslower MAO activity, the effect of lithium treat-ment is unclear, whilst ECT has no effect (Mann,1979). The variability of results, especially withbipolar patients, presumably reflects differentpatient populations and different techniques ofmeasurement of MAO with differing substrates.
Sandler et al. (1975) gave a tyramine conju-gation test to untreated patients with severedepression. Following an oral load, most tyra-mine is degraded by MAO to its main metabo-lite p-hydroxyphenylacetic acid, but some 15%is conjugated. In the patients the secretion ofconjugated tyramine was significantly low, sug-gesting increased MAO activity. Sandler et al.have since gone on to suggest that the tyra-mine test may be a possible biological markerof depressive illness, useful in diagnosis andin predicting response to tricyclic drugs (Haleet al., 1989). This deficit persists after recoveryfrom illness, and is noted in both bipolar andunipolar patients (Harrison et al., 1984).

Affective Disorders 187
With regards to central monoamines, in con-trast to the literature on schizophrenia, that onthe affective disorders has been dominated notby dopamine, but by noradrenaline and 5-HT.
The 5-HT (Serotonin) Hypothesis
The main biochemical hypotheses relating to theaffective disorders were inspired by the revolu-tion in psychopharmacology of the 1960s. Earlyobservations were that reserpine, a drug thatdepletes monoamines, led to a depressive ill-ness in some 20% of patients taking it (mainlyhypertensives); that MAOI drugs, initially usedto treat tuberculosis, were mood-elevating andincreased monoamine levels; and that the otherclass of antidepressants, the tricyclic drugs, also,by a different mechanism, elevated functionallevels especially of noradrenaline and 5-HT. Oneemerging hypothesis was therefore that deple-tion of monoamine levels related to depres-sive illness. While investigators in the UnitedStates provided many data on catecholamines,in Europe the serotonin (5-HT) hypothesis wasmore vigorously pursued.
Pharmacological Evidence
In order to test the 5-HT hypothesis, patientswere treated with amine precursors, notablytryptophan and 5-hydroxytryptophan (5-HTP).In normals, both compounds led to elevationof mood, minimal with the former and moredramatic with the latter (Wirz-Justice, 1977).In depressed patients, L-tryptophan had alimited antidepressant effect, enhancing thatof either clomipramine (a relatively selectiveinhibitor of 5-HT uptake) (Walinder et al., 1976)or an MAOI (Coppen et al., 1963) when giventogether. 5-HTP has antidepressant propertiesalone, or when given with clomipramine (vanPraag et al., 1974) or an MAOI. In contrast,parachlorophenylalanine, a drug that selectivelydepletes 5-HT, reverses the antidepressant effectof both tricyclic and MAOI antidepressants, butsuch an effect was not observed with the cate-cholamine depleter alpha-methyl-paratyrosine(Shopsin et al., 1976).
Tryptophan in the plasma has been measuredby several groups. It exists in a free and boundform (unlike other amino acids that are notbound to plasma protein), and entry across theblood–brain barrier is competitive with otheramino acids. Since the rate-limiting enzymefor 5-HT formation, tryptophan-5-hydrolase, isnot saturated under ordinary conditions, thelevel of tryptophan in the plasma can influencecentral 5-HT synthesis. Results of plasma tryp-tophan studies are not consistent, with reportsof decreased total (Riley and Shaw, 1976) or nor-mal total but reduced free (Coppen and Wood,1978) and normal free levels (Møller et al., 1979),even when unipolar and bipolar patients wereexamined separately (Møller et al., 1979). A sea-sonal variation exists, possibly related to theseasonal variations of depressive illness. Study-ing the ratio of plasma tryptophan to thoseof five other amino acids, Meyer et al. (1981)reported lower ratios, but mainly in samplestaken within 72 hours of hospital admission inunipolar depressed patients. Improvements indepression, rated on the Hamilton scale, cor-related significantly with an increasing ratio,suggesting lowered brain availability of trypto-phan in the depressive phase. In a later studythey reported normal platelet and whole-blood5-HT in depressed patients, but lower plateletlevels in patients who made a suicide attempt(Mann et al., 1992).
In summary, there is a suggestion that lowerplasma tryptophan levels are associated withsome aspect of depressive illness, but furtherinvestigations are required to establish theirsignificance.
Delgado and colleagues pioneered the devel-opment of the tryptophan depletion technique,where subjects drink an amino-acid drink thatleads to around an 80% depletion of plasmatotal and free tryptophan (TRP), resulting in amoderate but significant reduction of central5-HT metabolism (Delgado et al., 1991, 1994;Miller et al., 1992). If subjects tolerate the proce-dure (it induces nausea and vomiting in many),healthy controls often experience mood shiftsand many of the behaviours of a depressiveepisode (Delgado et al., 1994). As would bepredicted, patients with prior episodes of

188 Biological Psychiatry
depression are more likely to report a transient‘depression’ following this technique, as arefirst-degree relatives of patients with mooddisorders (Allen et al., 2009; Delgado et al.,1991). Some researchers have used this as anacute treatment for mania (Applebaum et al.,2007) or the antidepressant discontinuationsyndrome, where patients continue to havevertigo, sensory dyskinesias and headachesafter stopping SSRIs (Delgado, 2006).
Another way to examine this issue is theuse of platelet-binding studies. Platelets takeup and store 5-HT in a manner thought similarto synaptosomes, and have therefore beenused as a model for central 5-HT terminals.Early reports found decreased Vmax (maximumtransport rate) through the platelet membranein manic–depressive, depressive, unipolar,bipolar and schizoaffective patients (Meltzeret al., 1981). It is unclear from the data whethervalues return to normal with recovery or therelationship to response with tricyclic drugs.Imipramine and related compounds are potentinhibitors of the active transport of 5-HT intoplatelets (Todrick and Tait, 1969), although thesite of this action may not be identical to thatof the 5-HT transporter under all conditions.Thus imipramine labels a low-affinity sitethat is unrelated to the 5-HT transporter, butparoxetine binding is more specific. Othercompounds used include labelled ketanserinand LSD. Decreased imipramine binding sites(Bmax) have also been reported in severalstudies in a variety of depressive subgroups(Briley et al., 1980; Lewis and McChesney, 1985),including unipolar, bipolar and FPDD patients,although considerable overlap with controlvalues is seen, and it is unclear whether this is astate- or trait-dependent marker.
Brusov et al. (1985) have identified plasmalow-molecular-weight compounds that inhibitboth the imipramine binding and 5-HT uptakeof platelets, suggesting possible endogenouscompounds that may regulate 5-HT plateletand synaptosome activity and play a role inaffective illness. The issue is more complex,however, since seasonal variations of both5-HT uptake and platelet binding have beenreported, with lower levels in the winter and
spring, accounting for some of the variabilityin the results (Egrise et al., 1986). The results ofparoxetine-binding studies in depression andseasonal affective disorder are negative (Ozakiet al., 1994), and results with LSD binding areinconclusive (McBride et al., 1994). However, ameta-analysis of platelet imipramine bindingconcluded that Bmax for binding is significantlydecreased in depressed patients, an effect notrelated to the taking of antidepressant drugs(Ellis and Salmond, 1994).
Another haematological marker is red-blood-cell choline. This is reported elevatedin some unipolar patients, possibly thosethat do not show altered imipramine binding(Wood et al., 1983).
Attempts to identify changes in urinarymetabolites of 5-HT in depression have notbeen consistent. Only about 5% of urinaryamine metabolites are of central origin, withthe exception of the catecholamine derivativeMHPG, the urine being too remote from CNSactivity to provide meaningful data. Furtherevidence for the 5-HT hypothesis from CSF andbrain-binding studies is discussed below.
The Noradrenaline Hypothesis
Pharmacological Evidence
Although most antidepressant drugs influencecatecholamine uptake (there are exceptions, forexample iprindole, mianserin and the selec-tive 5-HT agents), the evidence that precursorloading with, for example, dihydroxypheny-lalanine and L-dopa in depression improvesthe response of other drugs, or is antidepres-sant, is poor. Further, alpha-methylparatyrosinedoes not reverse the antidepressant effect ofimipramine (Shopsin et al., 1976). However, L-dopa may switch a patient from the depres-sive to the manic phase of a bipolar illness,and alpha-paramethyltyrosine does the oppo-site (Murphy et al., 1971). Some antidepressantsare reported to be selective for noradrenergicsystems (for example maprotiline), although thisdoes not necessarily reflect on their mode ofantidepressant action.

Affective Disorders 189
Biochemical Evidence
Tyrosine levels in blood have been evaluated,but there is little consistency between studies.
Plasma noradrenaline levels have beenreported as increased in affective disorder byseveral groups (Lake et al., 1982; Roy et al.,1985), notably in those with major affectivedisorder, especially those unipolar patients withmelancholia (Roy et al., 1985). The increasedlevels fall with ECT (Cooper et al., 1985). Esleret al. (1982) measured the rate of entry ofnoradrenaline to plasma from sympatheticnerves (‘noradrenaline spillover’) with tritiatednoradrenaline and showed higher levels andspillover in patients with endogenous depres-sion characterized by retardation or agitation.This suggested increased sympathetic tone,although interestingly, in this and some ofthe other studies, the raised levels were notaccompanied by elevated blood pressure. In asmall number of patients, tricyclic drugs ledto a drop in both noradrenaline levels andspillover. Plasma adrenaline (Esler et al., 1982)and dopamine beta-hydrolase (Friedman et al.,1984) tended to be normal.
Various strategies have been adopted totest catecholamine-receptor function. Theseinclude the tyramine pressor test, clonidinechallenge, and estimation of the alpha adren-ergic receptors on platelets and the betareceptors on lymphocytes. Some of theseassess both presynaptic autoreceptor andpostsynaptic autoreceptor function (e.g. theeffect of clonidine on blood pressure), othersare postsynaptic (e.g. yohimbine on sedationor blood pressure, or the effects of clonidine ongrowth hormone release).
The tyramine test involves assessing changesin blood pressure after a tyramine load. Theblood pressure is elevated in depressed patientsin some studies (Ghose et al., 1975) but notothers. Clonidine, an α-2 adrenergic agonist,leads to a fall in blood pressure by acting oncentral α-2 receptors, and also lowers plasmanoradrenaline and MHPG. Results in depressedpatients are variable, although one group(Siever and Uhde, 1984) has reported decreasedresponse to the MHPG decrement in major
depressive disorder. This is compatible withother evidence of blunted postsynaptic alpha-receptor activity reported in clonidine studies(see below). Tricyclic antidepressants attenuatethe physiological responses of clonidine onMHPG and blood pressure (Charney et al.,1981), one postulated mechanism being thatthe increased synaptic neurotransmitter levelsafter treatment lead to negative feedback andreduction of neuronal firing and autoreceptorsubsensitivity. Interestingly, similar effects werenot observed with mianserin, indicating thatnot all antidepressants act in this way (Charneyet al., 1984b).
Platelet alpha-2 receptors have been exam-ined using agonist ligands such as clonidineand antagonists such as dihydroergocryptine oryohimbine. Of the studies to date, some showa difference, with increased binding (Garcia-Sevilla et al., 1981; Healy et al., 1983), but themajority are negative. Using an alternative tech-nique, that of examining the functional responseof platelets, Garcia-Sevilla et al. (1986) studiedplatelet aggregation to adrenaline hydrochlo-ride and found it increased in patients withmajor affective disorder, the effect being dimin-ished by lithium. In contrast, Siever and Coursey(1985) reported decreased prostaglandin-E1-stimulated cyclic AMP production in platelets,an indication of subsensitivity, while othershave reported no change.
Antidepressants (long-term), lithium andECT reduce the sensitivity of the α-2 autorecep-tor in both animal models and patient studies(Healy et al., 1983). These attempts to findalteration of α-2-receptor function in depressiveillness and changes with treatment stem fromhypotheses that implicate the receptor in theaetiology of depression, at least in a subgroupof patients, enhanced α-2-autoreceptor activitybeing associated with reduced noradrenalineoutput. However, while there is some evidenceto support these ideas, results are not reliablyconsistent. Further, the platelet data presupposethat the platelet α-2 receptor replicates the CNSreceptor. This is unlikely, as centrally the α-2receptor is both pre- and postsynaptic.
Studies of the β receptor, using lympho-cyte binding, are also inconclusive, although

190 Biological Psychiatry
decreased responsiveness of cyclic AMP oradenylate cyclase to isoprenaline challengeshave been reported in manic and depressedpatients (Extein et al., 1979; Pandey et al., 1979).This effect is observed in both major depressivedisorders and dysthymia (Mazzola-Pomiettoet al., 1994). These data suggest downregulationof the receptor, possibly a response to highcirculating noradrenaline levels.
Increased urinary noradrenaline andnormetadrenaline and lower dihydroxypheny-lacetic acid (DOPAC) levels have been reportedin unipolar depressed patients (Roy et al., 1986a).However, the main urinary metabolite studiedhas been MHPG, some 20–60% deriving fromcentral sources. The earlier studies, particularlyfrom Schildkraut et al. (1984), found low levels,especially in a subgroup of patients with thedepressed phase of a bipolar illness, and higherlevels in manic or hypomanic episodes. Similarfindings were not found with VMA, adrenalineor normetadrenaline. Estimates of MHPG levelsin unipolar depression have been variable, someauthors reporting low levels (Maas et al., 1972),others finding no change, but a wide variationsuggesting subtypes with both high and lowlevels (Schildkraut et al., 1984). Patients withlow excretion rates have been found to be par-ticularly responsive to treatment with tricyclicdrugs (Maas et al., 1972; Hollister et al., 1980).This is more consistent for imipramine, nortryp-tiline and desipramine than for amitryptiline,for which higher excretion rates are reportedin responders (Modai et al., 1979), possiblyreflecting pharmacological differences betweenthe drugs, especially on noradrenergic systems.
Wiesel et al. (1982) reported on urinaryexcretion values of MHPG, HVA, 5-HIAA andDOPAC in healthy volunteers. Those with afamily history of psychiatric morbidity hadincreased variance of MHPG levels. This corre-lated positively with CSF levels and suggestedthat altered noradrenergic metabolism mightbe related to vulnerability to psychopathology.
Other Biochemical Hypotheses
In addition to the above hypotheses, which havedominated depression research in recent years,
both dopamine and choline hypotheses havehad supporters. Further, biochemical findingsrelating to other systems have been reportedand are of interest.
The dopamine hypothesis has been stronglysupported by Randrup et al. (1975). It is basedon pharmacological evidence that neurolepticdrugs block dopamine receptors and areeffective antimanic agents; that a ‘depression’is not infrequently seen in patients on thesedrugs; that some neuroleptics, especially insmall doses, may be antidepressant; on thefacts that many antidepressants act, at leastto some extent, on dopamine uptake systemsand that L-dopa, in some patients, may beantidepressant or may precipitate a manicphase; and on animal pharmacology that linkscertain behaviours (especially stereotypy) toincreased central dopamine activity.
Some support for this derives from CSF dataand the association of depressive illness withParkinson’s disease (see below), although thereis, to date, relatively little direct evidence toimplicate dopamine in the primary pathogene-sis of affective disorders.
Cholinergic mechanisms have been impli-cated by Janowsky et al. (1980). In particularthey discuss the relative balance betweencholinergic and adrenergic tone, with depres-sion representing a cholinergic and mania anadrenergic excess. The evidence is as follows:animal data show that cholinergic agentsinhibit self-stimulation; many, especially ofthe older, first-generation, antidepressants,have considerable anticholinergic properties;cholinomimetics such as physostigmine pro-duce an ‘inhibitory syndrome’ of lethargyand psychomotor retardation and may reversemania, sometimes provoking a switch to adepressed phase; and precursors such as deanoland choline may provoke depressive symptoms(Tammingar et al., 1976). Patients with affectivedisorder are reported to be more sensitive to thebehavioural effects of physostigmine (Janowskyet al., 1980), and some show elevated levels ofred-cell choline (Wood et al., 1983) or reducedacetylcholinesterase levels (Mathew et al., 1982).
GABA has recently been implicated fol-lowing observations that the anticonvulsant

Affective Disorders 191
sodium valproate may have antimanic prop-erties (Emrich et al., 1984) and that someprecursor drugs, such as progabide, maypossess antidepressant properties (Morselliet al., 1980). However, other anticonvulsantsthat act at the benzodiazepine-GABA receptor,such as phenobarbitone, clonazepam, tiagabineand vigabatrin may be associated with depres-sion. Plasma GABA has been reported low ineuthymic bipolar patients and CSF data offersome support for these findings (Berrettini et al.,1983). Several groups have found abnormalbrain GABA levels in patients with depressionusing MR spectroscopy (Sanacora et al., 2002,2006). To date it has not been possible toreconcile these findings, but the possibilitythat low trait GABA reflects a susceptibilityfor the development of depression, which thenbecomes manifest with an increase of GABAand subsequent alteration of monoamine status,has been suggested.
Urinary cyclic AMP has been reported tobe decreased in depression and increased inmania (Paul et al., 1971b), and in rapid-cyclingpatients there appears to be an increase in cyclicAMP levels during the switch from depressionto mania (Paul et al., 1971a). With treatment,values tend to return to normal (Abdulla andHamadah, 1970). It is difficult to interpret thesedata since some 50% of urinary cyclic AMPderives from the kidneys. However, they mayreflect altered receptor function in affective dis-orders, a suggestion supported by observationsthat antidepressant drugs and lithium decreasenoradrenaline-stimulated cyclic AMP. The inhi-bition of ADH-activated cyclic AMP is a possibleexplanation for one of the side effects of lithium,namely polyuria.
The phenylethylamine hypothesis statesthat this compound, structurally related toamphetamine and the catecholamines, is aneuromodulator that is deficient in depressiveillness. It is excitatory in animals, and isdegraded by MAOB to phenylacetate. The latterand beta-phenylethylamine are reported lowin patients with major depressive disorders(Sabelli et al., 1983).
Peptides have also been implicated. Initialobservations that some, for example TRH or
beta-endorphin (Kline et al., 1977), may possessantidepressant properties have not led as yetto any therapeutic advances. Marangell andcolleagues (1997) demonstrated rather con-vincingly that administering TRH intrathecallycould induce almost complete symptom remis-sion in a group of highly treatment-resistantdepressed patients. Unfortunately, the effects ofa single intrathecal injection lasted only 24 hoursand then the depression returned. Plasma beta-endorphin levels have been reported as normalin patients with unipolar major affectivedisorder (Alexopolous et al., 1983).
Low levels of folic acid have been reported inassociation with a variety of neuropsychiatricconditions, especially in patients with epilepsy.There are several reports of depressive illnessbeing associated with low levels (Trimbleet al., 1980), not explained away in termsof diet or institutionalization, in outpatientsand in community studies (Edeh and Toone,1985). Reynolds et al. (1984) have drawnattention to the fact that the methyl donor SAMis antidepressant, that folate megaloblasticanaemia is more frequently associated withaffective disorder than is B12 deficiency, and thatfolic acid is reported to improve mood, notablyin patients with folate deficiency. The fact thatSAM and folate are intimately connected withmonoamine metabolism may mean that CNSmethylation is intimately involved with theregulation of mood.
As in other psychiatric disorders likeschizophrenia, researchers have recently begunfocusing on the glutamate system in mood dis-orders (Kugaya and Sanacora, 2005; Sanacoraet al., 2008). Animal models of depression tran-siently respond to glutamatergic manipulation(Banasr et al., 2008; Engin et al., 2009). Smallopen-label trials of the N-methyl-d-aspartate(NMDA) glutamate-receptor antagonistketamine, used in general anaesthesia, haveproduced rapid, albeit transient, antidepressanteffects. Double-blind studies are underway totest this novel hypothesis, and to devise waysof extending the effect beyond the acute stage(24–48 hours).
BDNF has been a compound of interestrecently. The brain is more dynamic than

192 Biological Psychiatry
previously thought and contains undevelopedstem cells that can migrate and mature intoneurone or glial cells. There is evidence thatthis process is disrupted in depression andcorrected with successful treatment. Structuralimaging studies and post-mortem analysisof depressed patients have documentedsubtle volumetric loss in several importantstructures such as the hippocampi, prefrontaland orbitofrontal cortex, cingulate gyrus andcerebellum (Lenze et al., 1999; Sheline et al.,1999). Additionally, microscopic examinationshave shown decreased cortical thickness as wellas diminished neural size in similar regions.One possible explanation is that HPA axisactivation is neurotoxic to the brain. Anotherpossibility involves a disruption of normalnerve growth. The prospect that depression isrelated to problems with nerve-growth factorshas opened up a new way of conceptualizingits pathophysiology. That is, a failure ofneurogenesis and growth-factor proteins suchas BDNF may cause subtle shrinkage of thebrain, which is a part of the neurobiology ofdepression.
BDNF is one of a family of neurotrophinsthat regulate the differentiation and survival of
neurone. There are a multitude of growth-factorproteins maintaining and stimulating nervegrowth, but at this point BDNF is the mostwidely studied in depression. Figure 8.1 showsan example of the effects of BDNF on seroton-ergic neurone in the rat cortex. Saline or BDNFwas infused directly into the rat frontal cortexfor 21 days. Then the animals were sacrificedand the cortex at the site of the infusion wasstained for 5-HT neurone. Note the profoundarborization of the 5-HT axons in the cortex ofthe rat exposed to BDNF.
Thus, growth-factor proteins such as BDNFprovide ongoing maintenance of neurone inthe brain. Disruption of these nerve-growthfactors results in reduced size of neurone aswell as some cell loss. It is difficult to assessthe quantity and quality of BDNF in livinghumans, so the evidence connecting BDNFand depression is indirect. In rats almost alleffective antidepressants have been shown toincrease BDNF, including lithium. Many ofthe brain-stimulation techniques (ECT, TMS,VNS), oestrogen and even exercise also raiseBDNF levels. A post-mortem analysis of suicidesubjects found a marked decrease in BDNFin the prefrontal cortex and hippocampus in
Figure 8.1 BDNF infused directly into the rat frontal cortex results in a supranormal branching of 5-HTaxons (adapted from Mamounas et al., (1995); from Higgins and George, 2007)

Affective Disorders 193
suicide subjects compared to controls (Dwivediet al., 2003). Serum BDNF levels in depressedpatients prior to treatment are significantlyless than in healthy subjects. After eight weeksof antidepressant treatment, serum BDNFlevels increased significantly and were nolonger different from controls (Gonul et al.,2005). Studies in rats have demonstrated thatfluoxetine stimulates neurogenesis in about thesame amount of time as it takes for humansto respond to the treatment. The rats givenfluoxetine did not generate new neurone at arate any different from placebo after five days,but did separate from placebo by 28 days. Ofparticular interest, it also took 28 days for therats to change their behaviour, demonstrating agreater willingness to move into open, lightedareas to eat (Santarelli et al., 2003). At this pointit is still unclear whether BDNF changes indepression are causal or secondary.
Hormonal Data
With the development of new techniques forthe accurate measurement of small quantitiesof hormones, a plethora of data appearedassessing neurohormonal function in affec-tive disorders. Raised plasma cortisol levelsand corticosteroid excretion rates have beenobserved in patients with depression. Mostinterest has centred around cortisol and the dex-amethasone suppression test (DST). Reviewsare readily available (Arana and Baldessarini,1985; Braddock, 1986; Dahl et al., 1992).
Following investigation of over 400 patients,Carroll et al. (1981) defined a standardizedprotocol and suggested that the test may be‘a specific laboratory test for the diagnosisof melancholia’. The object of the test is tosuppress ACTH with a dose of dexamethasone,and most laboratories have adopted a scheduleas shown in Table 8.1, or a variant of it. Normalsubjects show a diurnal rhythm of secretion ofcortisol, with inhibition during the nocturnalhours. They suppress cortisol for 24–48 hoursafter dexamethasone.
The use of 1 mg of dexamethasone givesthe most sensitivity, although doses up to 8mg have been used in some studies. The most
Table 8.1 Schedule for the dexamethasone suppres-sion test
Day 1 Day 2
2300 0800 1600 2300↑ ↑ ↑ ↑
Dex 1 mg oral Cortisol determinations
Nonsuppression: cortisol >5 mg per 100 ml (157 nmol/l)
practical time to take the sample for cortisolmeasurement is at 1600 hours, although theuse of additional times may increase the rateof positivity. Using a plasma cortisol criterionvalue of >5 mg per 100 ml, Carroll et al. (1981)gave an overall test sensitivity (true-positiverate) of 43% and a specificity (true-negative rate;that is, 100% minus false-positive rate) of 96%.The diagnostic confidence for a diagnosis ofmelancholia with values above this level was96%, although that for ruling out melancholia atlevels below this was only 54%. In other words,a positive result had much more significancethan a negative result.
In a review of over 5000 cases, Arana andBaldessarini (1985) found the sensitivity to be44% and the specificity 93% when distinguish-ing major depression from normal controls, butthe latter fell to 76.5% in comparison to all otherpsychiatric disorders. However, DST specificityremained high when major depression was com-pared with bereavement (90.5%), anxiety andpanic (88.2%), schizophrenia (86.9%) and alco-holism not active or in acute withdrawal (80.0%).
In contrast to these data, other authors havebeen more critical, and in particular have notedhigh levels of positivity in other psychiatric con-ditions. Some of these are shown in Table 8.2.
Age and gender do not seem related to theresults, although higher levels of positivity arereported in older patients. The DST responseis not affected by the use of antidepressant orneuroleptic medications or lithium. There area number of conditions that give false-positiveresults, shown in Table 8.3.
The data with some psychiatric populationsother than depression are often confused by theinclusion of patients with associated affectivesymptoms, which increases the rate of positivity.The results in schizophrenia are influenced by

194 Biological Psychiatry
Table 8.2 Abnormal DST results and psychiatric diagnoses
Psychiatric condition Result (%) Reference
Melancholia 45 Carroll et al. (1981), Arana and Baldessarini (1985)Mania 0–40 Rabkin et al. (1985)Schizophrenia 0–20 Coppen et al. (1983), Munro et al. (1984)Panic disorder 25 Roy-Byrne et al. (1985b)Obsessive–compulsive 2 Checkley (1985)Anorexia nervosa 36–100 Rabkin et al. (1985)Bulimia 35–67 Lindy et al. (1985)Borderline personality 8 Krishnan et al. (1984)Normals 4–27 Carroll et al. (1981), Braddock (1986)
Table 8.3 False-positive DST
Medications BenzodiazepinesAnticonvulsantsBarbituratesReserpineAlpha-methyl dopaMethadoneMorphineSpironolactoneIndomethacinCyproheptadine
Drugs Alcohol; excess caffeineDiseases Diabetes mellitus
DementiaCerebral tumourCardiac failureCushing’s disease
Metabolic DehydrationOther Pregnancy
Acute medical illness ortrauma
acute psychosis and hospital admission, both ofwhich increase the nonsuppression rate. False-negative results are seen in Addison’s diseaseand hypopituitarism.
Although no specific clinical features of themelancholia have been associated with the pos-itive result, some findings are clinically rele-vant. There are several reports that the DSTreverts to normal after treatment, and that fail-ure to do so, or reversion back to a positiveresponse after normalization, is a bad prog-nostic factor (Arana and Baldessarini, 1985)and may signal an increased risk of suicide(Targum et al., 1983a). In a meta-analysis of theDST as a predictor of outcome, Ribeiro et al.(1993) noted that while baseline DST did not
predict response to antidepressant treatment,or outcome after hospital discharge, persistentnonsuppression after treatment was associatedwith a high risk of early relapse and pooroutcome after discharge. Coppen et al. (1985)have suggested that if higher cutoff points (forexample 10 mg per 100 ml) are taken then pre-diction of response may be improved. In addi-tion, endogenicity, as assessed by the Newcastlescale, may be relevant (Coppen et al., 1983), asmay severity of depression as measured by theHamilton rating scale (Meador-Woodruff et al.,1986). Patients with psychotic depression andbipolar illness have higher levels of nonsuppres-sion (Arana and Baldessarini, 1985), as shownin Table 8.4.
Some have reported that abnormal DSTs areassociated with a family history of depression(Mendlewicz et al., 1982), although others do notfind this (Rudorfer et al., 1982). There are severalreports suggesting that patients with secondarydepression have lower rates of suppression than
Table 8.4 Nonsuppression in DST and affectivestate (from Arana and Baldessarini, 1985)
Nonsuppression (%)
Normal control 7.2Acute grief 9.5Dysthymic disorder 22.9Major depressive
disorder43.1
Melancholia 50.2Psychotic affective,
includes bipolardisorder
68.6
With suicide intent 77.8

Affective Disorders 195
those with primary depressive illness, and in asmaller number of studies, psychotic depres-sives yield a higher rate than nonpsychotics(Rabkin et al., 1985).
The abnormal responses are not due to anunusually rapid clearance of the dexametha-sone by patients with melancholia (Carroll et al.,1981) and the circulating half-life of the cortisolis normal (Butler and Besser, 1968). Depressedpatients seem to have an increased number ofcortisol secretory episodes with an increasedtime per day of release (Sachar et al., 1973).
ACTH levels are higher and dexamethasoneplasma levels lower in DST-positive patients,in spite of the normal dexamethasone clearance(Arana and Baldessarini, 1985). One expla-nation of the raised ACTH levels is that thehypothalamic–pituitary–adrenal axis is ‘set’ ata higher level in the nonsuppressors. Holsboeret al. (1985) have given corticotrophin releasingfactor (CRF) to nonsuppressing depressedpatients, and repeated the investigation onrecovery when suppression was normal. Nodifferences in the profiles of ACTH, cortisol orcorticosterone output were noted in the twoconditions. This implies that the hypersecretionof steroids in depression is not the result ofexcessive hormonal reserves in the pituitaryor adrenal glands. However, blunted ACTHresponses to CRF in depressed patients arereported by a number of authors (Gold et al.,1988), suggesting downregulation of pituitaryCRF receptors (Dinan, 1994), with an abnor-mality above the pituitary. Hypersecretion ofCRF leads to downregulation of pituitary CRFreceptors and decreased ACTH in response toCRF. Whalley et al. (1986) measured the numberof glucocorticoid receptors on lymphocytes inpatients with depression, schizophrenia andcontrols. The number of receptors was signifi-cantly lower in the depressed patients, even inthose who had not received psychotropic medi-cation. This suggests that in depression theremay be changes in steroid-receptor sensitivity,which if they also occurred in the brain wouldlead to dexamethasone nonsuppression.
Other studies support the concept of reducedglucocorticoid-receptor activity, helping toexplain why patients with affective disorders
do not become cushingoid in the presence ofraised glucocorticoid levels (Dinan, 1994).
Although studies of these peripheral mark-ers may not reflect central receptor activity, onehypothesis is that there are reduced central glu-cocorticoid receptors. In animal models, Sapol-sky et al. (1985) showed that excessive exposureto steroids reduces the number of hippocampalneurones, suggestive of a direct toxic effect.
Others have assessed adrenal hyperrespon-siveness, showing increased cortisol response toACTH. This may be related to adrenal hypertro-phy, since there are several studies showing anincreased size of the adrenal gland in patientswith affective disorder (Nemeroff et al., 1992;Szigethy et al., 1994).
In relation to other biological markers,patients with dexamethasone nonsuppressionhave higher platelet MAO activity (Schatzberget al., 1985) and higher plasma MHPG (Jimersonet al., 1983).
Among the factors that may influence theDST must be included the method of cortisolanalysis and patient compliance. Thus part ofthe variation in the data may reflect the useof radioimmunoassay as opposed to a competi-tive protein-binding assay, the latter appearingto be more reliable (Meltzer and Fang, 1983).HPLC and mass spectrometry are rarely used,but will be even more accurate. Poor compliancemay be one reason why inpatient studies showhigher rates of nonsuppression than outpatientinvestigations, although severity of the illness isa more likely explanation. Some authors havesuggested that weight loss is a critical vari-able, although others have failed to replicatethis (Keitner et al., 1985).
A summary of the abnormal glucocorticos-teroid responses in patients with depressionis shown in Table 8.5. The abnormal suppres-sion has been interpreted in terms of a simpleresponse to stress, although an alternative isthat it reflects abnormal limbic–hypothalamicfunction. The lower levels of abnormality inassociation with anxiety disorders and bereave-ment are against this being a nonspecific stressresponse. Further, an abnormal DST does notrelate to an excess of life events as assessed bythe Bedford College Life Events and Difficulties

196 Biological Psychiatry
Table 8.5 Abnormalities of the hypothalamic–pituitary–adrenal axis in patients with depression(glucocorticoids)
Cortisol hypersecretionIncreased urinary free cortisolIncreased CSF corticotrophin-releasing factorIncreased circulating ACTHAbnormal circadian rhythms of cortisolAbnormal dexamethasone suppressionDecreased glucocorticoid-receptor sensitivityDecreased release of ACTH to CRHIncreased adrenal-gland size
Schedule, although patients with severe lifeevents in a six-month period prior to the onsetof depression have higher urinary-free cortisollevels than those without (Dolan et al., 1985a)and acute stress will elevate postdexametha-sone cortisol levels (Baumgartner et al., 1985). Itis unlikely that the raised cortisol levels have acausative role in the depressive illness sincecortisol itself tends to provoke euphoria ormood elevation when given to patients, andin Cushing’s disease, although depression iscommon, it is not universal, being severe inless than 20% of patients (Cohen, 1980). How-ever, Dinan (1994) has argued that activationof the hypothalamic–pituitary–adrenal axis inbiologically predisposed individuals is centralto depression, altering monoamine responses,which are therefore secondary.
A more attractive hypothesis is that theabnormal DST reflects altered CNS function,especially neurotransmitter action in hypotha-lamic and related limbic pathways, and is thusa marker of some more fundamental biologicalchange. This has been explored by Carrollet al. (1980), whose data suggest a cholinergicmechanism. They noted that physostigmine, aninhibitor of anticholinesterase, allowed normalsubjects to escape from suppression, an effectthat could be blocked by atropine.
Patients with organic mental disorders havebeen investigated, and generally high levelsof nonsuppression are reported. In particular,the DST does not seem to differentiate reliablybetween depressive illness and dementia (Sparand Gerner, 1982). It is abnormal in patients afterthe acute phase of a cerebrovascular accident,
and this relates both to the presence of majordepression and to greater lesion volume on CTexamination (Lipsey et al., 1985).
Cortisol plasma levels may also be stimulatedby amphetamine and methylamphetamine. Asthis can be blocked by alpha adrenergic antago-nists, the effect is thought to be mediated nora-drenergically. This response seems blunted indepressed patients (Checkley, 1979). Clonidineappears to normalize the hypercortisolaemia ofdepression (Siever and Uhde, 1984), providingsupport for a role of adrenergic mechanisms.
Some conclusions regarding the ever-accumulating information on the DST aregiven in Table 8.6. In recent years this area hasagain become prominent as researchers havedeveloped potential antidepressant compoundswhich directly alter ACTH activity (Gomezet al., 2006; Keller et al., 2008; Schatzberg andLindley, 2008).
Other Neurohormonal Data
Several other neuroendocrine responses in de-pression have been assessed. These include thethyroid-stimulating-hormone (TSH) responseto thyroid-releasing hormone (TRH), growth-hormone responses to dopamine agonists,insulin, L 5-HTP and clonidine, and prolactinresponse to tryptophan, D-fenfluramine andbuspirone.
In the TRH test, 200–500 mg of IV-TRH aregiven, and blood samples are taken over the
Table 8.6 Some conclusions regarding the DST inpsychiatry
1. An abnormal DST is found in somepatients
2. This suggests hypothalamic–pituitaryaxis dysfunction
3. It is most abnormal in anorexia nervosa4. It is often abnormal in depression, espe-
cially endogenous, melancholic andpsychotic subtypes
5. It is state- rather than trait-dependent6. It may help differentiate anxiety disor-
ders from depression7. It may predict relapse after treatment

Affective Disorders 197
next hour for the assessment of TSH values.Some 40–50% of patients with depressionshow blunted responses (Extein et al., 1981;Calloway et al., 1984). One group, studying145 medication-free depressed patients, gavethe specificity of the test as 93% with asensitivity of 56%, and predictive value of amaximum TSH response (the peak level afterinfusion–baseline) of <7 m IU/ml as 91%for major unipolar depression (Extein et al.,1981). The response tends to normalize withtreatment (Extein et al., 1982). Claims thatthis test may distinguish different subgroupsof affective disorder have not been upheld.Further, although cortisol excess itself leadsto impaired TSH release, not all patientswith blunting on this test are dexamethasonenonsuppressors. About 30–40% of patientsare abnormal on both dexamethasone andTRH tests, although this does not identify anyparticular diagnostic group. Interestingly, asubgroup of patients with blunted responseshave an elevated free-thyroxine index (FTI),some, while not being clinically hyperthyroid,having values in the hyperthyroid range(Calloway et al., 1984). Abnormal responses arealso reported in alcoholism, anorexia nervosaand acute starvation. In depression, it is thoughtthat the blunted responses reflect decreasedTRH-receptor sensitivity.
Because of the observed endocrine changesin depressed patients, other investigatorshave given multiple neuroendocrine chal-lenges to look for a more generalizedhypothalamic–pituitary defect in the disorder.Brambilla et al. (1978) gave TRH and LHRHto 16 patients with primary affective disorder,and 79% had some demonstrable abnormality.Winokur et al. (1982), using TRH, LHRH, DSTand insulin challenge tests in patients withprimary unipolar depression and controls,reported abnormalities in 96.2% of patients andonly 29% of controls.
Both growth hormone and prolactin havebeen studied because of the relationship oftheir release to underlying neurotransmitters.Growth hormone is affected by a number offactors including stress, fasting and diet, butis thought to be released under the influence
of growth-hormone releasing factor (GHRF,somatostatin) from the hypothalamus. Releaseof growth hormone is altered by drugs thatact on the adrenoceptor, being stimulated byclonidine, methoxamine and phenyephrine(alpha agonists), an effect potentiated bypropranolol. This suggests that alpha receptorsare excitatory and beta receptors inhibitory. Thegrowth-hormone response to apomorphine isrelated to dopamine-receptor stimulation, andit can be blocked by dopamine antagonists suchas chlorpromazine. Other neurotransmittersalso probably involved in growth-hormonerelease include 5-HT and GABA, although theirinfluence is weaker.
Growth-hormone responses have been stud-ied in depression. Impaired release is reportedafter metamphetamine (Checkley, 1979), insulinhypoglycaemia (Mueller et al., 1969), clonidine(Checkley, 1985; Siever and Uhde, 1984) anddesmethylimipramine (Glass et al., 1982), a tri-cyclic drug that selectively blocks the re-uptakeof noradrenaline. Responses to apomorphineare not reliably altered, supporting a major rolefor alpha-adrenergic mechanisms in affectivedisorder with decreased alpha-2-receptorresponsiveness, probably at the hypothalamus.GHRF itself has provided mixed results (Skareet al., 1994). Katona et al. (1985) have reportedthat patients with blunted growth-hormoneresponses to clonidine are more likely to beDST nonsuppressors, suggesting a commonunderlying mechanism for these changes.
Wieck et al. (1991) gave women with ahistory of affective psychosis the apomor-phine challenge test four days post partum.Growth-hormone responses were significantlygreater in those that developed a recurrentpsychotic illness, suggesting that in this groupat least, hypothalamic dopamine receptors hadincreased sensitivity.
Prolactin release, regulated by prolactin-inhibitory factor (PIF), itself thought to bedopamine, is stimulated by dopamine antag-onists and inhibited by dopamine agonists.Tryptophan, 5-HTP, 5-HT and GABA also stim-ulate its release. The response to tryptophan isthought to result from activation of postsynaptic5-HT1A receptors and the 5-HT2 receptor.

198 Biological Psychiatry
More selective 5-HT receptor agonists includegepirone and buspirone for the 5-HT1A site.Stimulation leads to a rise in GH and ACTH.
Baseline prolactin levels are consistently nor-mal in depressed populations. In one study, thedegree of suppression following apomorphinehas been reported impaired in major depres-sion and schizoaffective disorder, the degree ofdepression as rated on the Hamilton scale corre-lating with the degree of suppression (Meltzeret al., 1984), although in this investigation base-line levels were elevated. While this may suggesta role of dopaminergic systems, blunted pro-lactin responses have also been reported aftermethadone (Judd et al., 1982) and tryptophan(Heninger et al., 1984), suggesting both peptideand serotonergic abnormalities.
Studies with buspirone (a 5-HT1A agonist)in depressed patients failed to reveal alteredGH, cortisol or prolactin (postsynaptic 5-HT1A)release compared with controls (Cowen, 1994;Meltzer and Maes, 1994), but did attenuatehypothermic responses (presynaptic 5-HT1Aeffect) (Cowen, 1994). One conclusion of thesedata is that there is decreased 5-HT1A autorecep-tor function in depression (Cowen, 1994). Thismay reflect decreased release of 5-HT and com-pensatory downregulation of the autoreceptor.
In contrast to the many studies in depression,neuroendocrine challenges in mania are few.Prolactin responses to buspirone seem normal(Yatham, 1994).
A summary of some of these neurohormonalfindings in affective disorder is found inTable 8.7. In general, taking into considerationthe methodological problems associated with
Table 8.7 Summary of neurohormonal data
Hypersecretion of cortisolLoss of normal circadian cortisol cycleIncreased urinary excretion of cortisol and
metabolitesAbnormal response to dexamethasoneBlunting of growth hormone output to
alpha-adrenergic stimulantsBlunting of TSH responses to TRHBlunted prolactin responses to several agentsBlunted ACTH responses to CRF
Table 8.8 Some important methodologicalconsiderations
Influence of age and sexInfluence of circadian, monthly and annual
cycle of hormone activityInfluence of stress, diet and associated illnessMany hormones are released in a pulsatile
fashionInfluence of nicotine and alcohol intakeInfluence of psychotropic drugsVariability of assay proceduresLack of specificity for receptors of drugs
these data (see Table 8.8), they offer supportfor adrenergic and serotoninergic involvementin major affective disorders, the most robustfindings relating to studies of the α adrenergicreceptor in depressive disorders.
NEUROCHEMICAL INVESTIGATIONS
There have been a considerable number of inves-tigations of CSF in the affective disorders, themajority examining the noradrenergic, 5-HTand BDNF hypotheses. In contrast to the studiesin schizophrenia, the neuropathological studiesare few in number.
CSF
The main metabolites investigated, in studieswith or without the probenecid technique,have been 5-HIAA and MHPG. Overall, morestudies report lower levels of 5-HIAA than nodifferences compared with controls. Many ofthe early studies did not use the probenecidmethod, and were dismissed on account ofmethodological problems. First, much 5-HIAAreleased from the brain is removed from theCSF by an active transport system, giving a3:1 gradient from ventricular to lumbar fluid.Second, factors such as diet, time of day andpatient height and posture were often not takeninto account. Third, the spinal cord was knownto contribute to the 5-HIAA pool, furtherdiminishing the relevance of lumbar-fluidfindings.

Affective Disorders 199
Using the probenecid technique, severalgroups have shown diminished accumulationof 5-HIAA, further lessened by the adminis-tration of antidepressants (Post and Goodwin,1978) but elevated by L-tryptophan and 5-HTP(Takahashi et al., 1975). In addition, the lowlevels seem to persist on clinical recoveryin both baseline (Coppen et al., 1972) andprobenecid (van Praag, 1980a) studies. In aseries of investigations, van Praag (1980a), usingthe probenecid method, reported low levelsof 5-HIAA to characterize some 40% of cases,although he did not report any psychopatho-logical differences between these and otherpatients. In contrast, Banki et al. (1981) reportedanxiety, insomnia, retardation, fatigability andsuicide to be more prevalent in a subpopulationof patients with low 5-HIAA. The low levels arenoted in patients with an absence of significantadverse life events in the six months prior toonset of their illness (Roy et al., 1986b).
A relationship between suicide and low5-HIAA has been replicated by most studiesthat have examined it. Asberg and colleagues(Asberg et al., 1976; Lidberg et al., 1985) reported5-HIAA as lower in those who attempt suicide,even in nondepressed subjects, and in thosewho have murdered sexual or familial partnersor their children. They have also reported ina follow-up study of depressed patients thatthose with low values are more likely to diefrom suicide in the ensuing 12 months. Sincesimilar findings are reported in schizophrenicswho attempt suicide (Ninan et al., 1984), inalcoholic impulsive violent offenders (Linnoilaet al., 1983b) and in patients with aggressionwho have borderline personality disorderswithout depressive illness (Brown et al., 1982),one interpretation is that the low 5-HT turnoveris related to impulse control and aggression,rather than to depression per se. Of related inter-est is the study of Higley et al. (1992) in rhesusmonkeys, where high rankings for aggressionwere negatively correlated with CSF 5-HIAA,and positively with CSF noradrenaline.
There has been one investigation of ventricu-lar fluid metabolites in depression. Bridges et al.(1976), in a study of patients with chronic or
persistently resistant depression having resec-tive brain surgery, reported severely depressedpatients to have the lowest and agitated patientsto have the highest 5-HIAA levels.
In contrast, results of 5-HIAA levels in maniahave been contradictory, some studies reportingincreased and others decreased values.
CSF catecholamine or catecholamine metabo-lite levels have been studied with less consistentresults. In keeping with the urine investiga-tions, some authors report low levels of MHPG(Post et al., 1973) and others show normal results(Post et al., 1985) and no relationship to suicide.Low HVA levels have been reported in sub-groups of patients, notably those with retarda-tion (van Praag, 1977a) or who attempt suicide(Roy et al., 1992). This observation is consis-tently reported in probenecid studies and seemsrobust. In contrast, agitation and psychosis arereported to be related to increased HVA levels(Banki et al., 1981).
Estimates of noradrenaline levels have pro-duced inconsistencies, although there are tworeports of elevations in mania (Gerner et al.,1984; Post et al., 1985) associated with paradoxi-cally decreased dopamine beta-hydroxylase lev-els (Post et al., 1985). Lower adrenaline levelshave also been reported in depressed patients,returning to normal with recovery (Christensenet al., 1980).
There are several reports of CSF data combin-ing with other biological markers. In particular,DST nonsuppressors show lower HVA and apoor association with adverse life events (Royet al., 1986b).
Lower CSF GABA has been noted in sev-eral studies (Berrettini et al., 1983; Gerner et al.,1984), as has lower CSF somatostatin (Rubinowet al., 1985), especially in dexamethasone non-suppressors (Doran et al., 1986). This suggests afunctional interdependence of CRF on somato-statin, possibly at the level of the hypothalamus,and receives some support from observations ofhigher CSF cortisol in depression (Traskmanet al., 1980), associated with nonsuppression ofthe DST.
Other CSF changes reported include lowerAVP (Gjerris, 1988), lower pregnenolone

200 Biological Psychiatry
(George et al., 1994a) and decreased S-adenosylmethionine (Bottiglieri et al., 1990).
Brain Neurochemistry
The CSF data provide limited support forchanges in catecholamines in depressive illness,especially in relation to motor activity. The datafrom brain neurochemical studies in this areaare minimal. Those reported lend weight tochanges in the 5-HT system, and are largelyderived from studies of brains of patients whohave committed suicide. These data are difficultto interpret methodologically, especially sincepsychotropic drugs are often the main cause ofdeath in such patients, and there are difficultieswith controlling for post-mortem degradation.
Most studies of cortical 5-HT and 5-HIAA inpost-mortem brains reveal no changes, findingsfrom the brainstem being more consistent inshowing lower levels than controls (Lloyd et al.,1974; Shaw et al., 1967). In a study of bipolarpatients, Young et al. (1994) reported decreased5-HIAA and HVA levels in cortex, and increasednoradrenaline turnover, reflected in increasedMHPG/NA ratios.
Attempts to examine binding sites havemainly used labelled imipramine, amitriptylineor paroxetine, and this use of different ligandsmay be important. Results are very variable(Lawrence et al., 1990) and no conclusions canbe drawn. There are several studies supportingthe early findings of increased frontal bindingof 3H-spiperone, suggesting raised 5-HT2receptors at this site (Stanley and Mann, 1983),but results using 5-HT1A ligands are conflicting.
It has already been noted that an impor-tant variable with regards to 5-HT functionrelates perhaps more to violence and impul-sivity than to depression. The changes in 5-HT2binding seem more consistent in studies of vio-lent suicides (Arora and Meltzer, 1989; Stanleyand Mann, 1983). These data are interpretedas reflecting low 5-HT turnover, with compen-satory increase in postsynaptic binding sites.
In other studies, brain MAO, noradrenalinelevels and muscarinic cholinergic binding havebeen studied with negative results. One grouphas reported low dopamine levels in the caudate
nucleus (Birkmeyer et al., 1977), and others haveshown significantly increased beta-adrenergicreceptor binding to frontal cortex (Mann et al.,1986), increased clonidine (alpha-2) bindingin suicide patients (Meana et al., 1992) andincreased frontal benzodiazepine binding sites(Cheetham et al., 1988).
MR spectroscopy allows one to noninva-sively assess brain chemistry. Using this tech-nique some investigators have found abnormalcholine metabolism in bipolar affective-disorderpatients in the caudate (Moore et al., 2000).As mentioned above, MRS studies have alsofound abnormal low GABA activity in depres-sion (Kaufman et al., 2009; Sanacora et al., 2002).
NEUROPHYSIOLOGICALAND NEUROLOGICAL DATA
Electrophysiological Studies
Some of the earliest reports of EEG traces inaffective disorder found a higher than expectedincidence of abnormalities. For example, Fin-ley and Campbell (1941) found abnormalitiesin 33% of 137 manic–depressive patients, andsimilar data were given by others (Davis, 1941).As with schizophrenia, attention was drawnto the presence of abnormally high frequencies(20–50 Hz).
Abrams and Taylor (1979) analysed therecords of 27 schizophrenic and 132 affective-disorder patients, noting that in contrast to themore extensive and temporal location of theabnormalities in schizophrenia, the affectiveshad more parieto/occipital changes (24%). Incases where the abnormalities were lateralized,71% were right-sided. This did not relate to age,severity of illness or medication.
Two waveforms in particular have beenassociated with affective symptoms. Thesix-per-second rhythmic waves, also referred toas rhythmic midtemporal discharges (RMTD),are associated with an increased risk forpsychopathology, including high hypochon-driasis and depression scores on the MMPI(Hughes and Hermann, 1984) (see Figure 8.2).Small sharp spikes (SSS), brief-durationsmall-amplitude spikes that are sometimes

Affective Disorders 201
27 6 5 4 3
89101112
181716151420 19
21Eye M.
T.C.: 0·3s
H.F.: 70Hz
140µV
1s
13 ECG
1
Figure 8.2 Rhythmic midtemporal discharges. Note trains of notched waves, maximal in the left temporalregions (leads 7 12, and 18) (courtesy of Dr Colin Binnie, Institute of Psychiatry)
exclusively temporal in location and manifestin drowsy states or light sleep, have beenassociated with neurovegetative symptoms,affective disorders and a tendency to suicide(Small, 1970) (see Figure 8.3). In particular,related symptoms included mood swings, anx-iety, insomnia, concentration difficulties andfeelings of hopelessness. Further, in patientswith bipolar affective disorder, 43% show SSS,which may be significantly related to a familyhistory of affective disorder (Small et al., 1975).
Struve et al. (1979) reported a highly signifi-cant positive relationship between paroxysmalEEG abnormalities and suicidal ideation andacts, and assaultive/destructive acts, unrelatedto medication. Both SSS and RMTD wereincluded in the paroxysmal events that wereassociated with suicide. The relevance of thesefindings for such conditions as episodic dyscon-trol and the association between epilepsy andaffective disorder and suicide is not clear.
However, they do emphasize the importance ofparoxysmal electrophysiological events beyondepilepsy, and that ‘all that spikes is not fits’(Stevens, 1979).
Data from power spectra analyses have beenreported in detail by Flor-Henry (1983). Heconfirms the increased amount of 20–50 Hzactivity, notably bilaterally in the temporalregions for both mania and depression, andin the left parietal region in mania. In hisstudies there was a significant reduction ofright parietal alpha energy in both states,thought to reflect abnormal activation ofthe nondominant hemisphere. Examininginterhemispheric organization by means ofan EEG measure of left/right-hemisphericenergy oscillations, at rest and during certaincognitive tasks that activated one or otherhemisphere, he reported that the organizationis most disturbed and bilateral in schizophre-nia, is intermediate and in the dominant

202 Biological Psychiatry
27 6 5 4 3
89101112
181716151420 19
21Eye M.
T.C.: 0·3s
H.F.: 70Hz
140µV
1s
13 ECG
1
Figure 8.3 Small sharp waves (benign epileptiform transients of sleep). Note the short-duration spikes. Amagnification of those from channels 6 and 7 is shown below. These are predominant in the temporal regionsand seen during drowsiness or stages 1 and 2 sleep (courtesy of Dr Colin Binnie, Institute of Psychiatry)
hemisphere only in mania, and is normal indepression.
The evoked-potential literature is confusingand difficult to interpret. Shagass et al. (1981),in studies where potentials were evokedby four different kinds of sensory stimuli,claimed to show differences between psychoticdepressives and schizophrenics. They reportedthat the amplitudes of earlier peaks were higherin the latter, while later peaks (P90, N130 andP185) were higher in the former. However, inboth groups most amplitudes were lower thancontrols. The data were interpreted as suggest-ing some impairment of sensory processingin depression, although less than that seen inschizophrenia. Laterality differences have beenreported, but the results are inconsistent, some
suggesting nondominant- (Flor-Henry, 1983)and others dominant-hemisphere (Shagasset al., 1979) abnormalities.
Davidson and colleagues, working over sev-eral decades now, have suggested that pre-frontal EEG laterality measures can distinguisha sad from a normal affect, melancholic dis-position from controls, and depression fromhealth (Davidson, 1995). Similarly, Korb andcolleagues (2008) have proposed that a measureof laterality and prefrontal EEG power (calledcordance) can distinguish depressed patientsfrom controls. More ambitiously, they also sug-gest that serial measures of cordance can be usedto determine who will eventually respond to agiven antidepressant medication, and that EEGchanges can be observed in eventual responders

Affective Disorders 203
as early as one to two weeks after beginningto take a medication, before clinical symptomsbegin to change (Cook et al., 2005; Hunter et al.,2006).
Sleep Studies
One biological marker of depression that hasbecome of interest is polygraphically definedsleep changes. Some disorder of sleep has longbeen held to be a key symptom of depres-sion, notably early-morning waking and noc-turnal restlessness in endogenous depression.The major changes of sleep in depression areshown in Table 8.9.
One consistent observation is the shorteningof the time from the onset of sleep to the firstREM period (REM latency). This falls by about30%, and is associated with an increase in thelength of the first REM period and decreasedstages 3 and 4 sleep. The REM period is said tobe more dense, with an increased number of eyemovements per minute. Patients show increasedwaking during the night, and will complain ofboth early-morning wakening and poor sleepquality.
The shortened REM latency does not seemspecific for depression, and has been reported insuch conditions as narcolepsy, anorexia nervosa,some schizophrenics and in normals followingartificial REM deprivation (Gillin et al., 1985).However, in depression it has good sensitivity
Table 8.9 Sleep and affective disorder
Patient symptoms Difficulty getting off to sleepPoor sleepEarly morning wakingIncreased waking
Duration Decreased total timeNon-REM sleep Increased stage 1
Decreased stages 3 and 4REM sleep Decreased REM latency
Increased REM time in earlyhours
Decreased REM in late hoursTreatment Sleep deprivation
Selective REM deprivationAntidepressants, some of which
suppress REM
(60–70%) and high specificity (80–97%), and isassociated with some other biological markers.Latencies are briefer in patients who are cortisolnonsuppressors (Mendlewicz et al., 1984; Rushet al., 1982).
Benca et al. (1992) conducted a meta-analysisof sleep disorders, reviewing data from over7000 patients. While most psychiatric groupsshowed reduced total sleep time, accounted forby decreases of non-REM sleep, percentage REMwas increased in affective disorders. Decreasedlatency was seen in several disorders, but over-all the findings for this and other parameterswere more consistently disturbed in depressedpatients.
The meaning of these changes is unclear.They seem to identify a pattern of depressionreferred to as endogenous, and may be pre-sumed to be a reflection of the underlyingbiochemical abnormality associated with thecondition. Manipulation of sleep, for exampledeprivation, has an antidepressant effect, and,in patients switching from depression to mania,a change in sleep pattern heralds the change inmood and motoric behaviour. Several hypothe-ses have been advanced (Gillin et al., 1985). SinceREM sleep is regulated by monoamines andis influenced by cholinergic medications (REMlatency can be shortened by physostigmine), onesuggestion is that it reflects a disturbed choliner-gic/aminergic balance. Another is that the shortlatency represents a ‘phase advance’, a shift ofdiurnal rhythms. This is particularly interest-ing given the new data on CLOCK genes andbipolar disorder discussed above.
Radiological Studies
CT and MRI
Early CT data revealed a subgroup of patientswith affective disorder that had ventriculardilatation and cerebral atrophy (Dolan et al.,1985b; Nasrallah et al., 1982a). Increasedventricular size has been reported in groupstudies of patients with manic–depressiveillness (Pearlson and Verloff, 1981), psychoticdepression with delusions (Targum et al.,1983b), mania (Nasrallah et al., 1982b), young

204 Biological Psychiatry
manics (Nasrallah et al., 1982b) and elderlydepressives (Jacoby and Levy, 1980b).
MRI data have confirmed and extended thesefindings. There are several reports of increasedsubcortical white-matter intensity lesions in theelderly with depression (Coffey et al., 1993) andin bipolar disorder (Strakowsi et al., 1993). Inthe elderly, this may be related to vascular dis-ease, and is more prominent in the frontal areas(Coffey et al., 1993). It seems that the presenceof atrophy in the elderly may predispose to thedevelopment of affective disorder.
Other findings in depression includedecreased caudate volumes (Krishnan et al.,1992), decreased temporal-lobe size (Hauseret al., 1989) and decreased brainstem andcerebellar vermis volumes (Shah et al., 1992). Inbipolar disorder a similar reduction of temporalvolumes has been reported (Altschuler et al.,1991), but with increased caudate volumes(Aylward et al., 1994). However, it is clear thatfewer studies of MRI have been conducted inaffective disorder than in schizophrenia, andsome of these data await confirmation. Harveyet al. (1994) found no volumetric differencesbetween bipolars and controls.
Dolan et al. (1990) reported increased frontalT1 values in unipolar but not bipolar patients,possibly related to lithium treatment in thelatter. Rangel-Guerra et al. (1983) reported thatbipolar patients had higher T1 values thancontrols, which decreased following lithiumtreatment.
Using phosphorous MRS in patients withbipolar disorder, Kato et al. (1993) reportedincreased phosphomonoester peaks in frontalcortex, which decreased when patients wereeuthymic. In contrast, Deicken et al. (1995)noted lower phosphomonoester values andhigher diester values in both frontal lobes inmedication-free bipolar patients.
In a combined PET/MRI study of mooddisorders, Drevets and colleagues (2008)demonstrated that the mean grey-matter vol-ume of the subgenual cingulate area (sgACC,Brodmann’s area 25) cortex is reduced insubjects with major depressive disorder andbipolar disorder, irrespective of mood state.Neuropathological assessments of sgACC
tissue acquired post mortem from subjects withmajor depressive disorder or bipolar disorderconfirmed the decrement in grey-matter volumeand revealed that this abnormality was likelydue to reduced glia, not neurone. In PET studiesthe metabolic activity was elevated in thisregion in the depressed relative to the remittedphases of the same major-depressive-disordersubjects, and several studies have suggested thateffective antidepressant treatment is associatedwith a reduction in sgACC activity (Mayberget al., 1997, 1999). The white-matter fibre tractsprojecting to this area are now a target for deep-brain stimulation in treatment-resistant majordepressive disorder (Mayberg et al., 2005).
Another finding using structural imagingis increased amygdala size in patients withchronic affective disorder and bipolar disorder.Notwithstanding the difficulties of measuringamygdala size volumetrically, this has beenreplicated in several studies (Altshuler et al.,2000; Hauser et al., 2000). Whether this relatesto trait or state is unclear at the present time,although the amygdala contains islands of smallundifferentiated neurone, and it could be relatedto neuronal plasticity.
CBF and PET Studies
Early SPECT and PET findings in depressionwere variable, but most suggested reducedCBF maximally frontally (Baxter et al., 1985;Mathew et al., 1980b). There are reports that theabnormalities are maximal on the left (Baxteret al., 1989; Buchsbaum et al., 1986) and nor-malize with treatment. Other findings includedecreased caudate metabolism (Buchsbaumet al., 1986).
More recent studies with higher-resolutionscanners have examined regional metabolismmore discretely. Biver et al. (1994) reporteddecreased dorsolateral frontal and parietal cor-tical fluorodeoxyglucose uptake, but increasedactivity in orbital frontal lobe.
Similar data are reported by Bench et al.(1993) using oxygen PET and statistical para-metric mapping (SPM). Decreased rCBF wasseen in depression in the left dorsolateralprefrontal cortex, left anterior cingulate and left

Affective Disorders 205
angular gyrus. These findings seemed unrelatedto treatment conditions. Interestingly, therewere region-specific correlations to symptompatterns, anxiety and agitation relating toincreased activity in posterior cingulate andinferior parietal lobules bilaterally, and psy-chomotor retardation correlating negativelywith flow in the left superior temporal gyrusand areas of the left parietal and left inferiorfrontal and dorsolateral prefrontal cortex. Cog-nitive function was correlated positively withleft medial frontal flow. Following recoveryfrom depression, maximal changes occurred inthe left anterior cingulate, left angular gyrusand left dorsolateral prefrontal cortical regions.
A common abnormality of the left dorso-lateral prefrontal cortex therefore emerges instudies of both schizophrenia and depression.Since in schizophrenia this is not activated byfrontal tasks such as the Wisconsin card-sortingtest, but in depression it can be, Berman et al.(1993) have argued that the pathophysiology ofthe abnormality differs between the two condi-tions. It seems to relate to a common symptompattern shared between the diagnoses, namelypsychomotor retardation.
The involvement of the cingulum is of partic-ular interest (Drevets et al., 2008). It is related toattentional mechanisms, which are disturbed indepression; to pain appreciation; and it is cen-tral to the limbic circuitry modulating emotion.In studies where sleep deprivation has beenattempted to treat patients with depression,increased cingulate activation predicts a goodresponse (Wu et al., 1992). In a series of studies,Mayberg et al. (1997, 1999) have suggested thatthe subgenual anterior cingulate may representa final common pathway involved in depressionpathogenesis and treatment response.
In PET studies using SPM it has beenshown that the cingulum can be activated bythe STROOP test, which involves selectingappropriate responses and inhibiting others.Patients with depression fail to activate thecingulate gyrus with this task, but activate thedorsolateral prefrontal cortex (George et al.,1994d). Another activation task used by Georgeet al. (1994c) is a facial emotion-recognition task,separating the response for identity recognition
from that for emotional expression recognition.There is now a large literature using this formof activation to probe affective circuits in healthand depression. In the original study, depressedsubjects had a deficit in matching faces foremotional content, and failed to activate theright insula as seen in controls with this task.More recent work with these facial emotion-activation tasks has focused on amygdala aswell as cingulate and prefrontal activation(George et al., 1995c, 1998; Minzenberg et al.,2007).
In an attempt to understand the role of someof these structures in emotion, investigatorshave imaged healthy volunteers in differentemotional states using oxygen PET and morerecently BOLD fMRI. George et al. (1994b, 1994c)reported that transient sadness activated theamygdala, the anterior temporal lobes, the cin-gulate gyrus and the orbital and prefrontalcortex bilaterally. These same areas are activatedby intravenous procaine, a drug that activateslimbic structures and causes dysphoria. In con-trast, transient happiness produces decreasedactivity in temporoparietal cortex bilaterally andright frontal cortex. Thus, while these volun-teer studies help to outline further an anatomyof mood, the direction of the changes notedrequires explanation. George et al. speculatedthat perhaps a chronic increase in limbic activ-ity overwhelms the normal regulatory role ofthe prefrontal cortex, and the overall circuitdecreases in activity with the onset of a depres-sion in mood-disorder patients.
Procaine-induced euphoria is associated withactivation of the amygdala, basal forebrain andanterior cingulate (Ketter et al., 1994). UsingSPM and PET, George et al. (1994b) examinedrCBF in mania. They reported increased activ-ity in right temporal structures. The only otherstudy of PET in mania was that of Baxter et al.(1985), which reported global hypermetabolism.
There are few receptor studies. D’haenenand Bossuyt (1994), using ketanserin and IBZMSPECT, reported frontal asymmetries withthe former, and increased uptake of the latterin depression. Wong et al. (1985), using PET,did not initially find increased D2 receptorsusing methylspiperone in bipolar patients, but

206 Biological Psychiatry
more recently they have (Pearlson et al., 1995);thus the findings with IBZM are difficult tointerpret. However, Ebert et al. (1994) reportedthat responders to sleep deprivation showeda decrease of D2 receptor occupancy aftertreatment. Newer studies have imaged 5-HT1Areceptors directly (Cannon et al., 2006, 2007;Drevets et al., 2007). Other studies do not imagea receptor directly, but rather image the brainin groups where different receptor geneticvariants exist (Burnet et al., 1999; Munafo et al.,2008; Pezawas et al., 2005). Using 11cWAY, the5-HT1A receptor has been shown to be reducedin the raphe and medial temporal cortex indepressed especially bipolar subjects (Savitz etet al. 2009).
Another new form of functional brainimaging involves examining the ‘resting state’.Patients are placed in the MRI scanner andgiven no specific task. Over a period of time thescanner measures small variations in regionalbrain activity. These serials scans can then beanalysed, looking for regional covarations, orfunctional connectivity at rest. Several studieshave now been carried out with this techniquein depressed patients, implicating disruptedcortico-limbic connectivity (Anand et al., 2005a,2005b; Greicius et al., 2007).
Consistent with the structural studiesmentioned above, amygdala activity has beenshown to be enhanced in patients with mania ordepression, or with anxiety disorders (Drevets,2003). There do not appear to be consistentimaging differences between unipolar andbipolar depression.
Neurological Data
It is clear that depression can be associated witha wide range of somatic illnesses, includingendocrine disorders (particularly adult-onsetdiabetes), malignancy, viral disorders, hepaticand pancreatic disease, electrolyte disordersand the collagenoses (Hall, 1980). Further, manypeople with chronic illness become despondentand demoralized. These states, often associatedwith some symptoms of a major depressive ill-ness, are sometimes referred to as secondarydepression or depressive reactions, but in mostinstances their phenomenology has not been
well specified, and their response to conven-tional antidepressant treatments not evaluated.Again it is of importance to understand thedefinition of a depressive illness and to differen-tiate it from understandable reactions to adversecircumstances and human misery. Failure to doso leads to confusion over biological data col-lected in supposed major affective disorder andto unnecessary prescription of antidepressantdrugs, which themselves carry morbidity. Thissaid, it is important to aggressively treat comor-bid depression after attempts have been madeto address the underlying condition, as this canhave beneficial effects on quality of life as wellas the primary illness.
Secondary mania, although rarer, has beennoted with several CNS conditions, includingpostencephalitic states, Huntington’s chorea,tumours, epilepsy, following head injury andwith cerebellar atrophy (Krauthammer andKlerman, 1978; Yadalam et al., 1985). Euphoricmood changes were commonly described ingeneralized paralysis of the insane (GPI), anda ‘eutonia’ and ‘empty’ euphoria accompaniesthe periventricular demyelination of multiplesclerosis. Most studies reveal that the focallesions that lead to secondary mania areright-sided and involve the orbitofrontal cortex,caudate nuclei, thalamus or basotemporalareas (Table 8.10). This is in contrast to manystudies which have found that left-sided lesionspredispose to depression, particularly those inthe frontal cortex.
A number of drugs may precipitate, pro-voke or exacerbate a depressive illness, andthe role of reserpine in originally providing
Table 8.10 Disorders associated withsecondary mania
Cerebrovascular accidentsEpilepsyParkinson’s disease with dopamine agonist
therapyIdiopathic basal ganglia calcification (Fahr’s
disease)Huntington’s diseaseTraumatic brain injuryMultiple sclerosisFrontal-lobe degenerationsCerebral syphilis

Affective Disorders 207
Table 8.11 Some drugs commonly associated withaffective disorders
Depression AlcoholAnticonvulsantsBarbituratesBenzodiazepinesButyrophenonesDigitalisDisulfiramFenfluramine and appetite
suppressantsMethyl dopaMetronidazoleNonsteroidal anti-inflammatory
drugsOral contraceptivesPhenothiazinesPropranolol and other beta blockersReserpine
Mania Amphetamine and other stimulantsBromocriptineL-dopaMAOI antidepressantsSteroidsTricyclic antidepressants
an insight for the biochemical theories has beenmentioned. A short list of commonly used drugsassociated with causing or exacerbating depres-sion is shown in Table 8.11; more extensivereviews are available (Hall, 1980; Whitlock andEvans, 1978).
Depressive illness is common with neu-rological disorders, and the literature hasbeen reviewed elsewhere (Cummings, 1985;Cummings and Trimble, 1995; Trimble, 1981a).The association is more than just an accom-paniment to chronic illness, and touchesupon the biochemical and neuroanatomicalunderpinnings of affective expression. Theconditions most considered are head injuries,cerebrovascular disease, epilepsy, multiplesclerosis and Parkinson’s disease. Depressivesymptoms in dementia are discussed inChapter 11. It is germane to note that headinjuries, often of a relatively trivial nature,may provoke depressive symptoms, often inthe setting of a post-traumatic stress disorder.The contributions of neuronal, personality andpsychosocial influences to the final picture havebeen discussed elsewhere (Trimble, 1981b).
Lesion location has been shown to be important,especially with early-onset depression. Leftdorsolateral frontal and left basal ganglialesions are particularly implicated (Jorgeet al., 1993).
With regard to tumours, meningiomas,especially frontal meningiomas, are notori-ously liable to induce a picture of typicalmajor depressive disorder. Both temporal-and frontal-lobe tumours are likely to presentwith changes of affect, including euphoria,hypomanic-like features, lability, depressionand irritability, with a tendency to be com-moner with dominant-hemisphere pathology(Cummings, 1985; Lishman, 1987). However,parietal and diencephalic tumours are alsoreported to lead to affective change, especiallyhypomanic swings with diencephalic lesions(Greenberg and Brown, 1985).
The association between basal-ganglia disor-ders and depression is of particular interest. InParkinson’s disease some 30–60% of patientshave a depressive illness, not entirely due tothe limitations of the chronic disability. Thesubject has been well reviewed by Cummings(1992). The clinical picture may be dominatedby anxiety, although all typical depressive fea-tures are seen. No consistent relationship toage of onset is noted, although some suggestit is commoner with early-onset disease. Thereis a correlation between depressive symptomsand motor impairment, but no consistent rela-tionship between for example Hoehn and Yahrstaging and depression ratings.
Biological associations have been reported.A relationship between right-sided hemi-Parkinsonism and severity of depression hasbeen noted (Starkstein et al., 1990), as hasgreater depression in ‘off’ phases in patientsdisplaying ‘on–off’ phenomena (Brownet al., 1984).
The depression associated with Parkinson’sdisease is often reported to occur prior to theonset of the motor disorder, responds to ECT,and has been associated with decreased CSF5-HIAA levels (Mayeux et al., 1984).
PET studies have shown decreased CBF in thefrontal and cingulate areas, in regions that over-lap with the abnormalities shown in primarydepressive illness (Ring et al., 1994).

208 Biological Psychiatry
Huntington’s chorea also often presentswith disorders of affect, including psychotic-depressive and hypomanic pictures. Again thiscan be dissociated from the motor disability,and may be seen prior to the onset or diagnosisof the chorea. Further, a high frequency ofsuicide is reported, even in those with noknowledge of their diagnosis. In a comparisonbetween the frequencies of major affectivedisorder in this condition and in Alzheimer’sdisease, Mindham et al. (1985) reported that theHuntington’s disease patients showed twice theincidence, emphasizing some special relation-ship, as opposed to the depressive symptomsmerely being a prodrome to the dementia.PET studies reveal decreased orbital andinferior prefrontal cortical metabolism relatedto depression in this condition (Mayberg, 1994).
Other basal-ganglia disorders associated withaffective change, either depressive or euphoric,include Wilson’s disease, Sydenham’s choreaand the blepharospasm–oromandibular–dystonia syndrome (Bruegel’s or Meige’ssyndrome) (Trimble, 1981a).
Cerebrovascular accidents (CVA) regularlyleave neuropsychiatric sequelae, and depressionis common. A controlled study in compari-son with similarly disabled orthopaedic con-trols revealed a significantly higher level ofdepression in the CVA patients (50% against13% for controls), suggesting the mood changeis not a simple reaction to disability (Folsteinet al., 1977).
In a series of studies, Robinson and colleagueshave explored this using CT evaluation of lesionextent and site (Robinson and Szetela, 1981;Robinson et al., 1984; Starkstein and Robinson,1993). In patients with CVA they noted 27%to have a major depressive disorder and 20% adysthymic disorder. They found that in the dom-inant hemisphere, the nearer the lesions to thefrontal pole, the more severe the depression. Inthe nondominant hemisphere, the further awayfrom the frontal pole, the higher the frequencyof the depression. There was no association withaphasia, although others have noted depressionto be more prevalent in association with Broca’saphasia (Benson, 1979). On follow-up, the majordepressive disorder persisted in 60%, and others
developed a new depressive syndrome. Thecorrelation to the left frontal pole persisted. Asimilar relationship was confirmed in a series ofonly left-handed patients. Subcortical atrophyidentified by brain imaging and a family historyof depression seem predisposing risk factors.
Using PET and methylspiperone, Maybergand colleagues (1988) reported increasedbinding (5-HT2 receptor) in uninjured brainareas in patients with CVAs, but only forright-hemisphere strokes. In left-hemispherelesions, the ratio of ipsilateral to contralateralbinding in temporal cortex was correlatedwith depression scores. These data requirereplication, but suggest that the mechanismof post-stroke depression is different betweenthe two hemispheres. Mayberg and colleaguesspeculated on the possible reasons for the asso-ciation of lesion site to severity of depression,citing their own animal work. They producedexperimental stroke lesions in rats and notedgreater post-lesion decline in catecholaminelevels with anterior as opposed to posteriorcortical lesions. They suggested that a frontallesion interrupts more arborizing monoamineprojection pathways than does a posteriorlesion, leading to greater destruction of axonesand more catecholamine depletion.
Patients with affective disorder have beenexamined for clinical neurological abnormali-ties. Generally these are noted with a lowerfrequency than in schizophrenia, and no specificpattern emerges (Manschreck and Ames, 1984).
Neuropsychological Disturbancesin Affective Disorder
There is no doubt that a marked cognitiveimpairment can accompany depressive illness,and that complaints of poor memory, impairedconcentration and difficulty with planning,decision-making and abstracting abilities bypatients are common. The term ‘pseudode-mentia’ has been used to specify this (Caine,1981; Wells, 1979). It can be argued that thisstate is better referred to as one of ‘reversibledementia’, and categorized as a subcorticaldementia (see Chapter 11).

Affective Disorders 209
The presentation can so resemble dementiathat many patients are misdiagnosed as hav-ing Alzheimer’s disease, and left untreated.The importance of the recognition of pseu-dodementia is that it is a reversible state ofcognitive decline, and improves in associationwith improvement of the depressive illness.
Although there are other causes of pseudo-dementia, which include hypomania, hysteriaand schizophrenia (Trimble, 1981a), that asso-ciated with depression is the commonest, andsome degree of cognitive impairment is foundin most cases. Important clues to help distin-guish pseudodementia from dementia include:a past history of affective disorder; the relativelyacute onset, with little evidence of decline priorto the development of affective symptoms; thepatient’s distress and complaints about cogni-tive function (as opposed to the lack of insightoften seen in dementia); the response to ques-tions in the mental-state examination (patientsoften using ‘don’t know’ as an answer, whereasin dementia the answers are more evasive,skirting the correct but lost answer); and theperformance on more structured psychologicaltasks, which do not reveal the focal deficits ofAlzheimer’s disease and produce patchy, incon-sistent impairment.
Pseudodementia is one of the most commonproblems leading to an inappropriate diagnosisof dementia, and follow-up studies of patientswith dementia often reveal a subgroup that hasnot declined or has even improved over time.Depressive illness is then often diagnosed ret-rospectively (Marsden and Harrison, 1972; Ronet al., 1979).
In addition to the clinical features, CT andEEG evaluation are essential, both often beingwithin normal limits. However, since a sub-group of patients with depressive illness hascerebral atrophy, confusion will occur if CT dataare taken in isolation.
There is no clear pattern of cognitive impair-ment that emerges, but often the patients’subjective complaints are worse than theirperformance on objective tests. When patientswith depressive illness are compared withcontrols on cognitive-test batteries they tend toshow impairments of attention, lack of speed
in mental processing, poor attention to detail(Caine, 1981), difficulty in abstraction andmemory difficulties, especially on tasks thatrequire effort, motivation and active processing.
There is some suggestion of morenondominant-hemisphere dysfunction, withgreater impairment of performance as opposedto verbal abilities, especially for spatial infor-mation (Weingartner and Silberman, 1985).Although not entirely consistent, the litera-ture from investigations adopting differenttesting strategies does suggest predominantlynondominant frontotemporal dysfunction indepressive illness (Flor-Henry, 1983; Taylor andAbrams, 1984). These impairments seem greaterwith more severe depression, and improvewith treatment and clinical response of thedepression.
SOME OUTSTANDING ISSUES
It seems clear that much biological informationabout the affective disorders has been accu-mulated in recent years. Although there aremany conflicting data, there is also a growingbody of consistency, and some of the earlierdifficulties have been overcome by improvedtechnology, better patient selection and clari-fication of hypotheses to be tested. However,new problems have arisen with the wealth ofinvestigations now available to the investigator,and the complexities of interpreting empirically-derived data, often collected without referenceto any clear underlying hypothesis.
Classification is still quite unsatisfactory, andcontinues to be a potential source of data con-flict. Although the DSM IV and DSM IV-TRhave provided a reasonable attempt to unifythe researchers’ ideals, this attempt fails, per-haps in the sense of being too broad for iden-tifying truly homogeneous groups. The lossof the reactive–endogenous dichotomy is wel-comed, not only because of the inconsistencyand confusion surrounding the word ‘reactive’,but because it has falsely assumed a classifi-cation based on aetiology. Despite the origi-nal scheme of Mobius, in which ‘endogenous’was contrasted with ‘exogenous’ on grounds

210 Biological Psychiatry
of causation, the evidence that depressions aresomehow either provoked by external circum-stances or the result of a mysterious internalprocess does not stand up. There are many stud-ies employing life-event methodology whichshow that antecedent life events do not predictclinical pattern (Paykel and Hollyman, 1984),although the fact that human adversity maylead to depressive symptoms hardly requiresscientific validation. The important questionsare, why do some people develop a depressiveillness, and what are the constitutional, neuro-physiological and neurochemical correlates ofvulnerability, resilience and presentation? Theconfusion that continually arises when moodchanges based primarily on underlying per-sonality disorders are mistaken for depressiveillness has already been discussed, but cannotbe overemphasized.
Most authors seem to identify a core ofpatients that suggests a biological syndrome,and in the past the term ‘endogenous’ hasbeen used to describe them. In DSM IV-TR‘major depressive episode’ is a substitute. Therelationship to bipolar-disorder depression stillrequires clarification, and to date neurobiolog-ical differences between them have not beenidentified. While clinically they are identical inphenomenology, there may be important bio-logical differences. Further, the affiliation withdysthymic disorder should be questioned.
The genetic studies have so far not revealedany specific genes of major effect, and there areconsiderable problems with phenotypic identifi-cation. Depressive disorder and the depressivephase of a bipolar disorder may be confusedclinically, and the introduction of the bipo-lar spectrum throws up additional confusions.The profile of the prospective candidates insome studies suggests differences from those ofschizophrenia, and if this turns out to be the caseit raises problems for those who might supporta continuum hypothesis for the psychoses.
With regards to the similarities anddifferences between patients with bipolardisorder and schizophrenia, it has become clearthat the long-term prognosis of bipolar disordercan also be poor, and that many patientsremain unwell (subclinically with cognitive
problems and mood instability) in betweentheir episodes of depression or hypomania.Their neurocognitive deficits seem differentfrom those identified in schizophrenia. Further,for bipolar disorder, an identifiable prodromehas not been identified and endophenotypeshave hardly been investigated.
The differences between the schizophreniasand those bipolar disorders which may be iden-tified at the present are shown in Table 8.12.
The relative lack of data in mania is imme-diately obvious. This stems in part from thefact that it is less common, and manic patients,because of their clinical state, are often poorresearch subjects. Much information is hiddenunder the term ‘bipolar disorder’, patients occa-sionally being examined in both a depressedand a manic phase. The main hypotheses tested,as in depressive illness, relate to the variousmonoamine hypotheses.
The initial monoamine theories were simple,depression relating to a deficit of catecholamineor 5-HT activity or turnover. In the UnitedKingdom the data have concentrated more onthe latter, while in the United States it is the for-mer which became predominant. More recentlydiscussions have shifted to GABA, BDNF andgrowth factors, as well as G-protein-coupledreceptors (Mathew et al., 2008; Sanacora et al.,2008). As shown in Table 8.13, evidencereviewed in this chapter provides supportfor the involvement of both transmitters, butthis is hardly surprising. Few would upholdany suggestion that neurotransmitters actin isolation, and the various feedback andregulatory events that exist between them, nowincluding the neuromodulators, are graduallybeing unravelled.
Schildkraut and Kety’s (1967) originalhypothesis was that some or all depressionwas associated with ‘a relative deficiencyof noradrenaline at functionally importantadrenergic receptor sites in the brain, whereaselations may be associated with any excess ofsuch amines’ (p. 8). Maas went on to suggesttwo types of depression, A and B, the formerhaving disordered noradrenaline and thelatter abnormal 5-HT systems. Another cate-cholamine, dopamine, has also been involved,

Affective Disorders 211
Table 8.12 Some putative differences between the schizophrenias and the affective disorders
Schizophrenias Affective disorders
Birth/obstetricproblems
Positive Negative
Neurocognitivechanges
Widespread/working memory Subtle/not widespread/attentionaldeficits
Anatomy Volume loss/amydala decreased Less volume loss/amygdalaincreased/area 25 involved
Neurochemistry Dopamine/glutamate GABA/5-HTTreatments Dopamine antagonists 5-HT/noradrenalin uptake
inhibitorsCourse Slowly progressive Progressive in a small numberRisk for cardio-vascular
diseaseGreatly increased (1–5×) Increased ??
Life expectancy Reduced up to 20 years Reduced
Table 8.13 Evidence for the 5-HTand catecholamine hypotheses
5-HT Noradrenaline
Precursor drug studies + –Reversal by inhibitors + ×Chemistry of antidepressants + +Selective uptake inhibitors + +SSRI + –Plasma precursors ? +Platelet studies + ?Urine studies × +Hormone release studies × +CSF data + –Post-mortem studies + –Association with neurology + +
+, reasonable supportive evidence; – , little supportive evidence;×, inadequate or no data.
although there has been less enthusiasm todevelop a ‘dopamine hypothesis’, even thoughtwo antidepressant medications developedspecifically on this hypothesis (nomifensine,buproprion) have good efficacy and may workthrough dopamine-related effects. After carefulconsideration of all the data, van Praag (1980b)concluded that dopamine deficiency character-izes vital depressions and is linked to the motorfeatures of the illness. This is consistent with theobserved associations with Parkinson’s disease,common neurotransmitter abnormalities beingimplicated in both conditions. He furtheraccepted that ‘within the group of vital depres-sive patients with central monoamine disorders,
it is either the 5-HT system or the noradrenalinesystem that is predominantly disturbed’ (p. 51).
Others have speculated on the role of cat-echolamines in relation to brain-reward sys-tems, deficiencies leading to lack of pleasure(the clinical counterpart being anhedonia), orhave invoked animal evidence that links learnedhelplessness (an animal model of depression) tocatecholamine systems (Willner, 1983).
Van Praag (1980a) has also considered indetail the role of 5-HT. He pointed out thesubstantial evidence for at least a subgroupof patients having a 5-HT-deficiency syndromethat seems to persist when the depressive illnesshas abated. It is thus a trait factor, linked to sus-ceptibility to develop depression and with poorcontrol over aggression. The 5-HT deficienciesare unlikely to be secondary to increased sen-sitivity of the postsynaptic 5-HT receptor. First,the precursor loading studies with increased5-HT function alleviate depressive symptoms,and second, the limited binding studies of brainor platelets do not support the hypothesis.
Other transmitter hypotheses have been putforward. The ‘permissive amine hypothesis’,originally suggested by Prange et al. (1974),stated that central 5-HT deficiency related toa vulnerability to affective illness; loweredcatecholamines correlated with depression andraised values with mania. Cholinergic mech-anisms have been implicated (Janowsky et al.,1980), and a cholinergic–adrenergic imbalancesuggested. Depression was seen as a state of

212 Biological Psychiatry
cholinergic dominance, mania one of adrenergicexcess. The evidence for involvement of thecholinergic system at present is very limited,being mainly of an indirect nature from theeffects of drugs that influence the cholinesystem and mood.
Recently attention has shifted from neu-rotransmitter levels and turnover to the roleof receptors, both pre- and postsynaptic. Theinvestigations of Sulser (1984) revealed thatnearly all treatments effective in depressiveillness lead to decreased activity (downreg-ulation) of the postsynaptic noradrenergicreceptor. This applies to antidepressant drugsand relates to the adenylate cyclise-linked betareceptor. This downregulation is dependent onan intact presynaptic 5-HT neuronal input, andcan be reversed by 5-HT depletion. Further,the time course of these events correlatesbetter with the known clinical effects ofantidepressants, emerging over days ratherthan acutely. Much of the receptor-bindingand neurohormonal data reviewed above havebeen aimed at testing hypotheses relating toalteration of monoamine-receptor activity indepressive illness. At present interpretation isdifficult, but a summary is given in Table 8.14.The blunted growth-hormone responses, espe-cially to clonidine, support decreased alpha-2noradrenergic-receptor activity (the growth-hormone effect is probably mainly mediated bypostsynaptic hypothalamic receptors), whichcould be accounted for by increased presynapticnoradrenergic output but decreased efficiencyof the noradrenergic system. The decreasedreceptor sensitivity may explain some ofthe other neurohormonal findings, includingthe abnormalities of cortisol and failure tosuppress with dexamethasone. However, theway in which different receptors may interact,
the primacy of any changes (in other wordswhether a receptor modification succeeds orleads to synaptic changes of neurotransmitteractivity) and the whole area of linking moretraditional monoamine hypotheses to receptortheories are unresolved.
The introduction of the SSRI antidepressantshas led to a renewed search for the mecha-nisms of action of antidepressants and the roleof 5-HT and its receptors. Increased responsiv-ity of 5-HT2 receptors can lead to decreased5-HT1A function, and a primary abnormality ofthe former can therefore explain some of theneurochemical abnormalities discussed in thischapter. However, raised cortisol can lead toa similar picture by reducing 5-HT1A function,leading Deakin et al. (1991) to suggest that the5-HT1A abnormalities may be primary. Antide-pressants are thought to reverse this deficit.However, the relative contribution of the 5-HT1A autoreceptor, as opposed to the postsy-naptic receptor, is unclear. It seems that SSRIs(and MAOIs) initially lead to a flooding of thesynapse with 5-HT, following which the sys-tem seems to close down. There is then, over atime course compatible with the delayed actionof these drugs, a resumption of activity but afurther decrease of 5-HT1A responsivity. Thisdecrease of autoreceptor sensitivity enhances5-HT release and normalizes 5-HT2 receptorfunction.
With greater use of brain-imaging studies,the discussion has shifted to circuits and inter-collated brain regions. That is, depression mayinvolve an abnormality of a specific neuromod-ulator in a specific region of circuitry. Involve-ment of the subgenual cingulate is a goodexample of this thinking and much attentionis now focusing on cortical–limbic regulatorycircuits.
Table 8.14 Sensitivity of neuronal receptors in depression and effect of antidepressants
Adrenergic 5-HT
Alpha Beta 1a (auto) 1a (postsynaptic) 2
Presynaptic Postsynaptic
Depression ↑? ↓ ↑ ↓ ↓ ↑Antidepressants ↓ ↑? ↓ ↓ ↑ ↓

Affective Disorders 213
Laterality has been discussed in relation toaffective disorder, as it has for schizophrenia.Generally the evidence is less convincing,but important observations have been made.Flor-Henry (1983), starting from his ownobservations that patients with psychosis andepilepsy awaiting temporal lobectomy are morelikely to have a manic–depressive picture if theyhave a nondominant-hemisphere focus, haspersistently argued for a role of that hemispherein the regulation of mood. The most persuasivedata come from the EEG and psychometrystudies of patients with depressive illness andpatients with secondary mania. Observationsof patients with CVA affecting either one orthe other hemisphere (Gainotti, 1972), studiesof split-brain patients and direction of gazein response to stimuli (to the left in affectivedisorder and to the right in schizophrenia, the
direction implying activation of the oppositehemisphere (Myslobodsky et al., 1979)) have allbeen used to support the concept. Certainly theproposition that the nondominant hemispherein health is concerned with emotional behaviouris convincing (Bear, 1986), and its link to affec-tive disorders is thus a reasonable postulate.However, not all findings support this, espe-cially the recent data from CVA, epilepsy (seeChapter 10) and imaging in primary depression.The latter emphasize frontal-basal-ganglia cir-cuitry in the anatomy of depression, especiallythe prefrontal cortex (George et al., 1994d).Distinctions between mania and depressionare emerging, both with respect to changes ofcerebral blood flow at key frontolimbic sites(increased in mania, decreased in depression)and with regards to laterality (right side inmania, left in depression).


9The Addictions and Disorders
of Motivation
INTRODUCTION
Most commentators agree that addiction to avariety of psychoactive drugs is one of the mostpressing problems facing Western society at thepresent time. The problem embraces not only thehuge cost of managing the direct consequencesof substance abuse, and the criminal activitywhich seems to go hand-in-hand with obtainingillegal substances, but also the associated socialmorbidity in terms of unemployment, familybreakdown and early mortality. In the UnitedStates, the National Institute on Drug Abuse(NIDA) estimates that the total cost of substanceabuse is more than $484 billion per year. TheWorld Health Organization (WHO) estimatesthat there are currently 2 billion alcohol abusers,1.3 billion tobacco users and 185 million usersof illicit drugs worldwide; in 2001, these threecategories together contributed to 12.4% of totaldeaths. According to the US National Epidemi-ologic Survey on Alcohol and Related Condi-tions (NESARC), the one-year point prevalenceof DSM IV substance-use disorders (excludingnicotine) is 9.35% in the United States, repre-senting 19.4 million adults.
Such pressures call out for a coordinatedapproach to the addictions, and there is a desireto understand the problem from a neurobiolog-ical perspective in order to seek new avenues oftreatment. Yet this area of biological psychiatry
Biological Psychiatry 3e Michael R. Trimble and Mark S. George 2010 John Wiley & Sons, Ltd
had suffered from neglect until quite recently,stemming from the almost entirely socialapproach to management of the addictions intimes past, and to an unfortunate fragmentationof interests and funding bureaucracies. Forexample, those interested in alcohol abuse(funded in the USA by the National Instituteon Alcohol Abuse and Alcoholism, NIAAA)have lacked interest in opiate addiction (whichis funded separately and competitively throughthe NIDA). Both groups have historically failedto grasp how important it is to understandaddiction and the processes leading to it. Thereneeds to be a better global understanding of themore fundamental aspects of human behaviour,which are not substance-specific but interlinkwith substance abuse, from lethargy and apathyto drive and motivation; that is, ‘what makes youtick’. Indeed, it may not be an exaggeration tostate that understanding disorders of motivationlies at the heart of psychiatry in general and bio-logical psychiatry in particular – and yet neitherDSM nor ICD in any of their respective classifi-cations recognizes disorders of motivation as anindependent group of conditions. ‘Substance-related disorders’ are however identified inDSM IV-TR, including dependence, intoxicationand withdrawal, and the various abused sub-stances are grouped under 11 classes, from alco-hol to anxiolytics and from caffeine to cannabis.

216 Biological Psychiatry
There is also acknowledgement that abuse canoccur outside of this list, and that more thanone drug can be involved – polydrug abuse.
The central features of dependence arerepeated compulsive self-administration, whichcan be associated with tolerance (needingincreased quantities with diminished effect fromthe same amount consumed), withdrawal symp-toms (physical and psychological) and craving(a strong subjective drive to use the substance).For dependence, there needs to be clinicallysignificant impairment or distress, althoughabuse without any dependence but with directharmful effects of the drug is also recognized.
Until recently, many psychiatrists, and cer-tainly those involved in driving social policy,have viewed drug dependency simply as asocial problem with social causes and socialsolutions in spite of the evidence from genet-ics, the obvious fact that the abused substanceshave psychoactive and hence neurochemicalproperties, and the developing understandingof the underlying neuroanatomy of drive andmotivation, which clearly have identifiable neu-robiological substrates.
DISORDERS OF MOTIVATION
Addiction is not only a brain-based disorder,it is central to an understanding of a widerspectrum of conditions referred to here to as‘disorders of motivation’. These are listed inTable 9.1. In all of these disorders there isan alteration of goal-directed behaviour anda change of desire and striving. Motivationhas direction and intensity, and implicatesinitiation of activity and persistence of suchactivity. In general terms, motivation can beincreased or decreased. It is closely linked with
the word ‘will’, which is now conceptuallymoving from a philosophically-bound constructor a psychological faculty to a neurobiologicalattribute discussed in terms of frontal-lobeactivity and executive functions. The word‘motivation’ implies motion, moving towardor away, giving direction and change to thestatus quo. ‘Will’ expresses a desire, a subjectivetone of inclination. Individual motivations arevariously available to the self-reflecting con-sciousness. Altered motivation as a feature ofhypomania and mania is manifest by increasedgoal-directed activity and pursuit of (high-risk)pleasurable activity; in impulsive disordersindividuals fail to resist environmentally-bounddirected activities (e.g. pyromania); in the obses-sions and compulsions there is the persistentdirecting of activity to focal (pointless) goalsand an inability to stop actions (or thoughts).Other disorders that have been includedin this spectrum include the Kluver–Bucysyndrome (with apathy; see Chapter 5) and theGastaut–Geschwind syndrome (with drivenhypergraphia and religiosity; see Chapter 10).A pure apathy syndrome, with diminishedemotional responses to goal-directed events,must not be confused with depression (althoughsome apathy is often seen in depression), andthe pure apathy syndrome does not respondto antidepressants. The right-hemisphere syn-drome is seen following strokes, and emotionalindifference is a central feature, with apathyor even abulia (see below) as key components.Drug-induced causes of apathy would includethe obtunding sometimes seen with somepsychotropic drugs, notably antipsychotics,benzodiazepines and the SSRIs. The dopaminedysregulation disorder associated with L-dopaabuse in Parkinson’s disease is a disorder ofincreased motivation.
Table 9.1 Disorders of motivation
Decreased Increased
Apathy Addiction (substance addiction)Abulia Hypomania/maniaAkinetic mutism Impulse-control disordersNegative symptoms (depression, schizophrenia, dementias) Obsessive–compulsive disorderEmotional indifference/right-hemisphere syndrome Gilles de la Tourette’s syndromeDrug-induced (antipsychotics, benzodiazapines, SSRI) Drug-induced (L-DOPA, stimulants)

The Addictions and Disorders of Motivation 217
The underlying anatomy of these disordersbrings the subject close to the limbic/basal-ganglia neuroanatomy discussed in Chapter 2,and lays a foundation for seeking a neurobi-ology of fundamental behavioural attributeswhich drive normal social interactions, andwhich become misapplied paradigmatically indisorders of motivation and, for the purposes ofthis chapter, in addictive behaviours.
CONDITIONING
Traditional Pavlovian conditioning involvesan external stimulus, initially neutral (theconditioned stimulus (CS)), being paired withan unconditioned (biologically significant) one(unconditioned stimulus (US)); the result isthe conditioned response (CR). Novel stimulithus become paired with innate biologicalresponses, enlarging the repertoire of ananimal’s behaviour. However, it is the casethat such pairings are not singular, and theconditioned stimulus may attach to several asso-ciations, including an affect. With instrumentalconditioning, a contingency is set up betweena behaviour and a reinforcing outcome, thereward strengthening the association betweenthe stimulus and the response, reflective of habitlearning. However, the flexibility of the systemis such that motivational states influence goaldirection, such that both Pavlovian and instru-mental conditioning are influenced by centralstates of ‘affect’. Thus, Pavlovian-conditionedstimuli that signal an emotionally significantoutcome can enhance responding: cues gainmotivational significance.
In experimental psychology, stimuli thatrepeatedly lead to approach behaviours areconsidered rewarding, reflecting the positivevalence of the organism to the particular circum-stance. Such stimuli can either incite or reinforceactions, by invoking memories of previousreward experiences, or increasing the proba-bility that a behaviour will be repeated. Theunderlying neuroanatomy, as revealed throughanimal investigations, involves the amygdala,the accumbens, the insula and the prefrontalcortex (orbito-frontal and medial). This under-scores the importance that understanding the
new neuroanatomy of the basal forebrainhas had in unravelling the biological basis ofmotivational behaviours generally, and addic-tions specifically.
All addictive drugs decrease the amountof stimulation needed in a brain-reward stim-ulation paradigm. The ventral striatum inparticular, along with the connections to andfrom the basolateral amygdala, has been shown,in animal models and in human imaging studies(see below), to be the anatomical core of notonly pathological addictive behaviours butalso quotidian-motivated activities. Two of themain nuclear components of the amygdala(the basolateral and the central nucleus)and their afferents and efferents, at least inanimal models, seem to play different roles inconditioned behaviours. The basolateral nuclei,with an important role in emotional memory,allow a conditioned stimulus (sensory inputsfrom the thalamus and cortex) to access thevalency of an unconditioned stimulus, whilethe central nucleus via the extended amygdalamacrosystem, the accumbens core and themedial forebrain bundle affects arousal and theoverall response through downstream brain-stem activation of autonomic and somatomotoroutputs. There is also reverberation back to thelimbic forebrain, with influence on the VTA,substantia nigra, the raphe nuclei, the locuscoeruleus and the cholinergic nuclei. Cardinalet al. (2002c) sums this up as follows: ‘we areremarkably close to this situation with thesuggestion that the central nucleus of the amyg-dala encodes or expresses Pavlovian stimulus-response associations, while the basolateralamygdala encodes or retrieves the affectivevalue of the predicted unconditioned stimulus’(p. 333) (see also Cardinal et al., 2002a, 2002b,2003; Robbins and Arnsten, 2009).
The accumbens and its striatal circuitryare central, being involved with stimulus-reinforcement associations and attributingmotivational effects to stimuli (Cardinal et al.,2002). The accumbens shell is considered mostrelevant, relaying information to the accumbenscore to translate motivation into action, thuspotentiating the behaviours, but also havingoutputs to the hypothalamus and brainstem.

218 Biological Psychiatry
The accumbens core then ‘mediates aspects ofpreparatory behaviour . . . not consummatorybehaviour. . .’ (Cardinal et al., 2002c, p. 337).The shell is sensitive to psychoactive drugs. Inaddition, exposure to unconditioned stimuli ornovelty causes local release of dopamine. Theextended amygdala may then play a specialrole here, its output being directly through themedial forebrain bundle, that neuronal pleasurehighway which so excited researchers in the1950s on account of its role in self-stimulationexperiments in which animals would continueto stimulate in preference to other rewards,to the limits of exhaustion. Finally, the dorsal
striatum, involved in habit learning, also showsincreased dopamine release during second-order reinforcement schedules, suggestingthat it is related to the compulsive nature ofdrug-seeking. It seems that as the drug-seekingbehaviour becomes established, the neuronalsubstrate may migrate from the accumbensshell to the core and then to the dorsal striatum:behaviourally, a shift from motivations to habits(Figures 9.1 and 9.2) (Hyman et al., 2006, 2007).
Cortical influences are from the orbito-frontal cortex, with its reciprocal connectionsto the basolateral amygdala, its afferents frompolymodal sensory cortex, and its accumbens
Figure 9.1 A schematic of the involvement of the amygdala (BLA) and the hippocampus, and the roleof the prefrontal cortex, in the process of conditioned reinforcement, showing how habits depend on theinteraction between prefrontal cortex and the dorsal striatum. Acb, accumbens; VTA, ventral tegmental area;SNc, substantianigra pars compacta; VGP, ventral pallidum; DGP, dorsal pallidum; BNST, bed nucleus ofstria terminalis; NE, noradrenaline; CRF, corticotrophin-releasing factor (reproduced from Squire et al., 2008)

The Addictions and Disorders of Motivation 219
PFC
VTANA
A H
Acute use Chronic use
PFC
NA VTAVTA
Dorsal stiatum
PFC
NA
Amygdala Amygdala
NucleusAccumbens
Hippocampus
Hippocampus
CoreShell
Figure 9.2 The greater involvement of the dorsal striatum in the behavioural effects of chronic use of drugsof addiction (reproduced with permission from Higgins and George 2007)
and hypothalamic influences relating to moti-vational state; it has been shown to containneurones that are responsive to the rewardvalue of stimuli such as food. The insula, as vis-ceroreceptive cortex, is thought to be importantin storing or retrieving memory of the sensoryvalue of stimuli, and the anterior cingulate,responsive to emotionally significant stimuli,including drug-associated cues, plays somepart in action selection. Dopamine has beenshown to be critical for learning, and dopamineantagonists block the reinforcing propertiesof addictive drugs, but not the drug-seekingbehaviour, supporting some of the above-notedanatomical dissociations between the differentphases of the addictive process.
Social preferences, while being in part genet-ically determined, including drug addictions,are learned behavioural intentions, and asso-ciated social cues (such as drug-taking para-phenalia in the addictions) become conditionersfor the establishment of conditioned responses.Drug cues elicit craving; the drugs, the social
surroundings and the related rituals becomelinked initially to intense pleasure, a learningprocess involving the hippocampus as well asthe circuits already outlined above. Alterationof activity in these structures and their efferentswith drug use leads to tolerance and cravingfollowing withdrawal of the drug. The latterintentions exert a control over future actionsand become associated with dysphoria ratherthan euphoria, and lead on to associated moodchanges and anhedonia.
GENETICS
By far the largest amount of work in genet-ics and addictions has been carried out onalcoholism, in part because alcohol has been areadily available substance for wide abuse overseveral generations. For example, it is hard to dogenetic studies of ectasy, LSD or even metham-phetamine addiction as these substances haveonly become available in recent times. Thereare no pedigrees of people addicted to these

220 Biological Psychiatry
substances as they did not exist a couple ofgenerations ago; it is hard to know if one’sparents would have become addicted to a sub-stance that has just been created or just becomeavailable. Moreover, many patients have poly-substance abuse, or abuse different substancesin various phases of their lives, so pure pedi-grees are difficult to examine by the substance ofabuse (e.g. cocaine, morphine, etc). Future workin understanding the addictions will requireidentification of genes that either have a role inaltered substance-specific vulnerabilities such asvariation in drug metabolism or drug receptors,or that moderate the role of shared vulnerabili-ties predisposing to addiction such as variationin reward or stress resiliency, or both.
The genetic studies of alcoholism will bereviewed in this section, followed by a dis-cussion on whether or not there are genes, orpolymorphisms, that bias toward an overalladdictive endophenotype. Many patients withdepression or bipolar disorder also haveproblems with addictions. The genetic studiesin those disorders have been discussed inChapter 8. Also, there are genetic crossoverswith personality disorders (see Chapter 5), par-ticularly antisocial personality disorder (ASPD)and borderline personality disorder (BPD).Finally, the impulsivity factor in Cloninger’spersonality schema is associated with increasedtendency to addictions.
Addictions are among the most heritable ofpsychiatric disorders, as shown in studies oflarge, carefully characterized cohorts of twins,including epidemiologically ascertained cohortsfrom Virginia, USA, and Australia. Heritabilitiesrange from 0.39 (for hallucinogens) to 0.72 (forcocaine). The addiction liability of a substancegenerally predicts its heritability moderatelywell. That is, cocaine and opiates, among themost addictive of substances, are also amongthe most heritable. Hallucinogens are amongthe least addictive, and are also the least her-itable. These data point toward an inheritanceof variation in the core neurobiological basis ofaddiction discussed above, such as the path-ways that mediate reward, behavioural control,obsessionality, compulsivity or stress and anxi-ety response.
Genetics of Alcoholism
Some individuals do not become addicted to asubstance because they simply do not experi-ence pleasure when ingesting it. For example,a human variant of the GABAa receptor hasbeen linked to sensitivity to alcohol andbenzodiazepines in relatively small datasets.Additionally, two outstanding examples ofverified human ‘addiction genes’ encode forenzymes that catalyse consecutive steps inalcohol metabolism: alcohol dehydrogenase(ADH) and aldehyde dehydrogenase 2 (ALD).ADH metabolizes ethanol to acetaldehyde, atoxic intermediate, which is in turn converted toacetate by ALD. The most important functionalloci at these genes are His47Arg in the ADHgene and Glu487Lys in the ALD gene. Eitherhigher activity of ADH (conferred by the His47allele) or lower activity of ALD (conferredby the Lys487 allele) leads to accumulationof acetaldehyde following an alcohol load.Acetaldehyde accumulation causes the aversiveflushing reaction that discourages further alco-hol intake, much like the effects of disulfiram(a drug that is used to prevent relapse) andcertain antiprotozoal drugs, such as metron-idazole, that inhibit ALD. In several East Asiancountries, such as Japan, where both His47 andLys487 are highly abundant, most of the pop-ulation carries a heterozygous or homozygousgenotype that is protective against alcoholism.The protective effect seems to vary acrossenvironments and the effects of genotypes areadditive. Interestingly, each of these protectivealleles apparently represents a single ancientmutation, which likely did not evolve to protectagainst alcoholism. Researchers think that thecommon gene variants might have conferredsome other effect on fitness, such as protectionagainst severe infectious diseases by proto-zoans, that are sensitive to inhibition of alcoholmetabolism, either because of their localizationin the gut or because of their lack of intrinsicaldehyde dehydrogenase (Goldman et al., 2005).
In addition to genes that make it unlikely tobecome addicted because of a change in how thesubstance is metabolized, there are others thatapparently predispose individuals to develop

The Addictions and Disorders of Motivation 221
an addiction. This might be referred to as thegenetics of risk-taking. Behavioural control is aname for the ability to inhibit the immediatepursuit of pleasurable stimuli and for the devel-opment of structured patterns of behaviour thatproduce long-term rewards. In children, deficitsin developing behavioural control can lead tovarious problems, including substance use andabuse. For example, in the Virginia twin cohort,a common factor encompassing externalizingdisorders such as ASPD and conduct disor-der (CD) accounted for 71% of the geneticliability to alcoholism and 67% of the inheri-tance of vulnerability to illicit drug abuse ordependence. Several genes that influence impul-sivity and externalization have also been found.Polymorphisms in both the DRD4 gene andthe dopamine transporter have been linked toattention-deficit hyperactivity disorder (ADHD)and CD. Monoamine oxidase A (MAOA) metab-olizes dopamine, and a rare stop-codon variantof this gene was linked to impulsive behaviouramong males in a Dutch family. An abundantMAOA variable-number tandem-repeat locusis linked to antisocial behaviour in children.5-HT is the neurotransmitter that is most consis-tently implicated in aggression and impulsivityby neurochemical and neurobehavioural stud-ies in humans and other species. The 5-HTreceptor 1B (HTR1B) gene is located at the siteof several mouse alcohol quantitative trait loci(QTLs) on chromosome 9, and mice in whichthis gene had been knocked out were moreaggressive and had a preference for alcohol.HTR1B was linked to ‘antisocial alcoholism’ ina Finnish family sample that was ascertainedthrough criminal alcoholic probands, and ina south-western Native American communitysample. However, replication of the associationof HTR1B with impulsivity or aggression hasbeen variable and no functional locus polymor-phism is known.
There are thus genes that can protectagainst developing substance abuse, as well asgenes that can push one to become addicted.There are also other interesting combinations:Thorgeirsson et al. in 2008 reported on a genevariant of the nicotinic acetylcholine receptoron chromosome 15q24 that both increases the
likelihood of becoming nicotine dependent andindependently increases the risk of developinglung cancer or peripheral arterial disease.The findings provide a case study of a gene–environment interaction, highlighting the roleof nicotine addiction in the pathology of otherserious diseases (Stefansson et al., 2009).
METABOLIC AND BIOCHEMICALFINDINGS
Different drugs of addiction have differingneurochemical effects, but they may all lead toa similar effect on the neuroanatomical systemsdescribed above. All addictive drugs increasethe activity of dopamine in the accumbens,either directly or indirectly. Some argue thatthis may be a final common pathway for allof the addictions. Cocaine blocks dopamine,5-HT and noradrenaline transporters, leadingto increased release of these monoamines,resulting in increased prefrontal dopamine andaccumbens activity, driving motor output. Onwithdrawal, increased CRF release has beenshown usually associated with adverse events.Amphetamine likewise potentiates monoamineactivity by increasing release, also leading tomotor activation. Alcohol, opiates, cannabi-noids and nicotine also modulate activity inthe accumbens but via different pathways. Forexample, opiates increase dopamine by remov-ing the GABAergic tonic inhibitory activityon ventral tegmental dopamine cells (GABAinterneurones having mu opiate receptors),while alcohol acts more directly on GABAreceptors in the ventral tegmental area. Nicotineacts on nicotinic acetylcholine receptors in theventral tegmental area, releasing dopamine.Phencyclidine antagonizes excitatory glutamateinput to the accumbens, impinging on GABAer-gic inhibition of dopamine. Cannabinoidsinteract with ventral tegmental area cannabi-noid receptors (Figure 9.3) (Higgins and George,2007; Hyman et al., 2006). Of the dopaminereceptors, D1, D2 and D3 are all involved,although D3 receptors, found almost exclusivelyin the accumbens shell, are probably of mostrelevance since virtually all significant addic-tive drugs lead to increased dopamine-shell

222 Biological Psychiatry
PFC
Endorphinpathways
+
Opiates
_+
__
_
NicotineAlcohol Opiates
Alcohol
Dopamine
Stimulants
PCP
CocaineAmphetamineMethylphenidate
VTA+
Nicotine
GABA
Glutamate
NAc
Figure 9.3 The pathways and sites of action of substance-abuse drugs on cerebral structures (reproducedwith permission from Higgins and George 2007, p. 114, Figure 9.9)
activation. The precise role of dopamine remainsunclear. It seems essential for reward-relatedlearning but it does not directly relate to hedonicresponses; thus it may be essential for motiva-tion (Hyman et al., 2006). However, addictiveagents differ from conventional reinforcingstimuli in a lack of habituation, and repeatedexposure does not lead to satiation. Naturalrewards lead to brief firing of dopamine cells,whereas drugs of addiction elevate dopaminerelease for much longer periods of time. Absti-nence with several drugs is associated withreduced dopamine transmission in the accum-bens (Table 9.2). This is an anhedonic state lead-ing to the need for the drug, satisfaction of whichamplifies the incentive properties of the drug.
Other brain changes that may relate tothese neurochemical intrusions of the addictive
Table 9.2 Neurotransmitters implicated in the moti-vational effects of withdrawal from drugs of abuse
Decreased Increased
Dopamine Corticotrophin-releasing factorOpioid peptides5-HTGABA
drugs include alteration of activity of ven-tral tegmental area and accumbens glutamatereceptors, and morphological and molecularneuronal alterations. In animal models, an in-crease of the density of dendritic spines inmedium spiny neurones and increased den-dritic branching have been shown in theaccumbens (shell and core) and medial frontalcortex with amphetamine, nicotine and cocaine,but decreases have been shown with morphine.These changes persist following drug with-drawal. More recently, research has examinedintracellular mechanisms associated withlearning and addiction, including the role ofthe transcription factors such as CREB and Fos,which bind to the promoter region of somegenes and may alter the long-term activityof cells (McClung and Nestler, 2003). It isunclear whether the intracellular mechanismsthat are altered in substance use are specificto addictive states, or whether they representintrinsic natural processes that are hijackedby the drugs in the process of creating andmaintaining dependency. This matters in termsof whether therapies that block or modifythese processes will be specific anti-addictiontherapies, or whether they are nonspecific and

The Addictions and Disorders of Motivation 223
affect many intracellular systems, with resultantside effects.
NEUROPHYSIOLOGICALAND NEUROLOGICAL DATA
EEG
Although the EEG has been used to investigateaddictions, there are all the problems mentionedabove in terms of specificity of any particulardrug. There is also the confound of whether thechanges predict substance abuse or arise fromthe use of the drug or other secondary factorsassociated with abuse and dependence (likedelirium tremens, head injury, poor nutritionand vasculitis (cocaine)). There is EEG evidenceof altered brain functional connectivity withchronic opioid abuse, with increased local anddecreased remote functional connectivity inabusers (alpha and beta bands). Pathologicalgambling has also been shown to be associatedwith EEG dysfunction (Regard et al., 2003).An increased P300 wave can be elicited withopiates in comparison with neutral stimuliin addicts, suggesting that drug cues acquirevalence that enhances their attention. Such cue-related evoked-potential changes with drugsin addicts have also been shown for othersubstances (Lubman et al., 2007). Cocaine crav-ing elevates plasma cortisol levels, and withquantitative EEG it has been shown that cueexposure increases beta activity and decreasesdelta power in the frontal cortex.
Radiological and Brain-imaging Studies
Researchers and clinicians have used the fullgamut of neuroimaging tools described inChapter 4 to understand and characterize theaddictions. To organize the discussion of thislarge body of studies, the imaging studies arepresented as follows. There are group andeven individual studies that characterize thepredisposition or tendency to become addicted,or which speak to disorders of motivation orimpulse control. These studies, for want of abetter term, are described as imaging studies of
addictive temperament or disordered motiva-tion or impulse control. There are also imagingstudies characterizing the brain changes thatarise as a function of chronic substance abuseor dependence. Finally, there are newer studiesattempting to actually image the brain whilesubjects are craving, which use the results topredict response or find new treatments.
Imaging Studies of Addictive Temperamentor Disordered Motivation or ImpulseControl
The above review of the neurochemical andneuroanatomical bases of addictive behavioursreceives considerable support from brain-imaging studies examining individuals with an‘addictive temperament’ or problems with im-pulse control.
Imaging studies in the amotivational statehave consistently revealed problems withmedial and orbito-frontal activation, similar tothe changes seen in the famous orbito-frontalpatient Phineas Gage. In one of the first modernstudies in this area, Bench et al. (1993) scanned40 depressed patients using PET. They thenanalysed the scans with a factor analysis. Highloadings for psychomotor retardation anddepressed mood correlated negatively withrCBF in the left dorsolateral prefrontal cortexand left angular gyrus. These data indicate thatsymptomatic specificity may be ascribed toregional functional deficits in major depressiveillness. Other imaging studies focusing on thesymptom of apathy or psychomotor retardationhave similarly found decreased prefrontalactivity (see discussion in Chapters 7 and 8).
A most interesting and controversial litera-ture revolves around whether abnormal pre-frontal or orbito-frontal structure or functionpredates and predisposes substance abuse, useand dependence, along with other impulsivebehaviours. For example, Raine et al. (1994) haveperformed a series of imaging and psychophys-iology studies in impulsive or psychopathicpatients, many of whom have substance-abuseproblems. In one such study, they measuredMRI prefrontal grey- and white-matter volumes

224 Biological Psychiatry
in 21 antisocial patients and in three controlgroups, comprising 34 healthy subjects (controlgroup), 26 subjects with substance dependence(substance-dependent group) and 21 psychi-atric controls. The ASPD group showed an11.0% reduction in prefrontal grey-matter vol-ume in the absence of ostensible brain lesions,and reduced autonomic activity during a stres-sor. The authors speculate that this prefrontalstructural deficit may underlie the low arousal,poor fear conditioning, lack of conscience anddecision-making deficits that have been found tocharacterize antisocial, psychopathic behaviour,and may represent a risk factor in developingsubstance abuse and dependence.
There is thus some brain-imaging evidence tosupport the idea of a functional neuroanatomyof apathy or abulia, and that disorders of pre-frontal and orbito-frontal cortex might predis-pose patients to develop disorders of substanceabuse.
There are imaging studies of hypermotivatedstates. Tics are involuntary, brief, stereotypedmotor and vocal behaviours often associatedwith irresistible urges. They are states of‘hypermotivation’ and are a defining symptomof the classic neuropsychiatric disorder Gillesde la Tourette’s syndrome, and constitute anexample of disordered human volition. Sternet al. (2000) used event-related [(15)O]H(2)Opositron-emission tomography techniquescombined with time-synchronized audio andvideotaping to determine the duration of,frequency of and radiotracer input during ticsin each of 72 scans from 6 patients with Gillesde la Tourette’s syndrome. This permitted avoxel-by-voxel correlational analysis withinstatistical parametric mapping of patterns ofneural activity associated with the tics. Theyfound that tics were correlated with increasedactivity in the medial and lateral premotorcortices, anterior cingulate cortex, dorsolateral-rostral prefrontal cortex, inferior parietal cortex,putamen and caudate, as well as primary motorcortex, Broca’s area, superior temporal gyrus,insula and claustrum. In an individual patientwith prominent coprolalia, such vocal tics wereassociated with activity in prerolandic andpostrolandic language regions, insula, caudate,
thalamus and cerebellum, while activity in sen-sorimotor cortex was noted with motor tics.These researchers concluded that aberrant activ-ity in the interrelated sensorimotor, language,executive and limbic circuits might account forthe initiation and execution of diverse motorand vocal behaviours that characterize tics inGilles de la Tourette’s syndrome, as well as forthe urges that often accompany them (Sternet al., 2000).
Imaging Studies of the Consequencesof Abuse
While the studies above are somewhat theoret-ical, and controversial, there is a much largerand noncontroversial body of imaging studiesdetailing the damage that chronic substance-abuse dependence might produce in the brain.To summarize this literature, it is easiest to statethat there is no real consensus on long-termbrain damage associated with tobacco (exceptfor the associated cardiovascular changes andrisk of cancer), cannabis, benzodiazepinesand opiates.
There are however many studies detailingthe damage caused by alcohol, cocaine and toa lesser extent MDMA (ecstacy). It is very clearthat chronic alcohol use causes brain damage,and that the entire brain volume shrinks. MRIstudies have documented ventricular volumeenlargement as well as deficits in grey- andwhite-matter volumes in alcoholics as comparedto nonalcoholic subjects (for review see Georgeet al., 2002; Mann et al., 2001). This cellular lossis greater in older alcoholics than younger alco-holics, even after the duration and amount ofalcohol consumed are taken into consideration.The loss in both grey and white matter is differ-ent than that found in other neurodegenerativedisorders such as Alzheimer’s disease, in whichthe cell loss is grey matter alone. In addition, thegrey- and white-matter loss in alcoholics is mostpronounced in the frontal lobes. Interestingly,some but not all of the brain-volume loss associ-ated with alcoholism has been found to reversewithin a few weeks of abstinence.
While many studies have evaluated brainstructure in alcoholic men, alcoholic women

The Addictions and Disorders of Motivation 225
have received less research attention. Womenmay be more vulnerable to the brain effectsof alcohol, given that while they develop alco-holism later in life, they often manifest adverseconsequences of alcoholism sooner than domale alcoholics, a phenomenon often referred toas ‘telescoping’. For example, two early studiesusing CT found that male and female alcoholicshad a similar effect on ventricle:brain ratiodespite the fact that the women had less dailyalcohol consumption. This led to the hypothesisthat women may be more vulnerable to thetoxic effects of alcohol. Hommer and colleagues(2001) evaluated 43 alcohol-dependent menand 36 alcohol-dependent women, as well as39 healthy control subjects. They found thatthe alcoholic women had greater white- andgrey-volume loss as well as increased sulcaland ventricular volumes compared to controlfemales. Furthermore, the difference in brain-volume loss, particularly in the grey matter, wasgreater in the females than the males. However,Pfefferbaum and colleagues (2001) performedvolumetric MRI measurements on age- andlength of sobriety-matched alcoholic men andwomen as well as age-matched healthy controls.While the alcoholic women showed no differ-ences in brain-volume indices in comparison tohealthy control women, alcoholic men showedvolume deficits compared to nonalcoholicmen (Mann et al., 2001a). These findings areconsistent with a PET study in which alcoholicmen had deficits in energy utilization whichwere not found in alcoholic women. Thus, whilesome studies have supported the idea thatwomen are more vulnerable to the detrimentalbrain effects of alcohol than are men, moreresearch is needed to conclusively settle theissue. The role of diet and other comorbidconditions needs further exploration as well.
In addition to examining brain structure,neuroimaging technology has also been utilizedto examine brain function in alcoholism. Thesestudies have evaluated brain activity afterimmediate cessation of alcohol use, as well asafter sustained abstinence. Unfortunately thereare relatively few neuroimaging studies in closetemporal proximity to alcohol withdrawal.Volkow and colleagues (1992) used PET scans
in recently-abstinent alcoholics (6–32 days) andhealthy controls and found that alcoholics hadlower overall brain metabolic rates. In a follow-up study in 1994, 10 alcoholic men were seriallyscanned using glucose PET at 8, 16 and 30 daysafter their last use of alcohol. These scans werethen compared over time with scans from 10age-matched nonalcoholic healthy controls. Onthe scan 8 days after alcohol cessation, alcoholicsshowed lower brain metabolism in numerousbrain regions compared to the control group;over the period of abstinence, brain metabolismimproved significantly (Volkow et al., 1994).Berglund and Risberg (1981) found a significantglobal reduction in CBF in 12 subjects in thefirst two days of withdrawal with the 133Xeinhalation method. However, they reportedrelatively high temporal and low parietal flowscoupled with aggravated symptoms of alcoholwithdrawal. Caspari et al. (1993) studied 15 alco-holics with perfusion single-photon-emission-computed tomography (SPECT) during day 1or 2 of acute alcohol withdrawal and again threeweeks later. During acute alcohol withdrawal,relative perfusion was elevated in the bilateralinferior temporal regions and reduced in thebilateral superior temporal regions.
To evaluate the role of the pattern of alco-hol use on regional brain activity, George et al.(1999) studied 14 adults with brain perfusionSPECT on days 7–9 following their last drinkand 2–3 days since their last detoxification med-ication. Seven healthy adults were scanned ascontrol subjects. The alcoholics, compared tocontrols, had widely reduced relative activityin cortical secondary-association areas and rel-atively increased activity in the medial tempo-ral lobes. Thus, while functional neuroimagingstudies examining the basal ‘resting’ state of thebrain following alcohol cessation have demon-strated that chronic alcohol use globally reducesneuronal activity for several weeks, the limbicarea seems to exhibit increased activity duringthis period.
Chronic cocaine causes selective vasocon-striction and can lead to white-matter abnor-malities and strokes. Since the development ofalkaloidal ‘crack’ cocaine in the 1980s, therehas been a significant rise in the number of

226 Biological Psychiatry
case reports describing both ischemic and hem-orrhagic stroke associated with cocaine use.The exact mechanism of cocaine-induced strokeremains unclear but there are likely to be a num-ber of factors involved, including vasospasm,cerebral vasculitis, enhanced platelet aggrega-tion, cardioembolism and hypertensive surgesassociated with altered cerebral autoregulation.The use of MDMA (ecstasy), a popular recre-ational drug, has been related to ischemic andhemorrhagic cerebrovascular events, as wellas atrophy.
Imaging Studies of Craving
Researchers have been able to induce craving forsubstances while subjects are inside the fMRIor PET scanner. Interestingly, and consistentwith the neuroanatomy discussed above, thereis a large convergence of these studies. Cravinginvolves a common neurobiology regardless ofthe object being craved, be it chocolate, a lovedone or crack cocaine. These studies are summa-rized in Figure 9.4. Some groups are using thiscraving signal induced within the fMRI scanner
R L R L
Drugs Feelings
1. Acute Effects of Cocain on Human Brain Activity and Emotion. Neuron 1997;19:591-611.2. Alcohol Promotes Dopamine Release in the Human Nucleus Accumbens. Synapse 2003; 49: 226-31.3. SPECT Imaging of Srtiatal Dopamine Release After Amphetamine Challenge. J Nuc Med 1995;36:1182-90.4. Role of Dopmaine in the Therapeutic and Reinforcing Effects of Methylphenidate in Humans:Results from Imaging Studies. Eu Neuropsychophar 2002; 12:557-66.5. Nicotine-induce Limbic Cortical Activation in the Human Brain: a Functional MRI Study. Am J Psych 1998;155:1009-15.
6. Reward, Motivation, and Emotion Systems Associated with Early-Stage Intense Romantic Love. J Neurophysiol 2005;94:327-337. 7. Intensely Pleasurable Responses to Music Correlate with Activity in Brain Regions Implicated in Reward and Emotion. PNAS 2001;98:11818-23. 8. Humor Modulates the Mesolimbic Reward Centers. Neuron 2003;40:1041-48. 9. Functional Imaging of Neural Responses to Expectancy and Experience of Monetary Gains and Losses. Neuron 2001;30:619-39.10. The Neural Basis of Altruistic Punishment. Science 2004;305:1254-8.11. Beautiful Faces Have Variable Reward Value:fMRI and Behavioral Evidence. Neuron 2001;32;537-551.12. A Neural Basis for Social Cooperation. Neuron 2002; 35:395-405.13. Changes in Brain Activity Related to Eating Chocolate. Brain 2001;124:1720-33.
Drugs Feelings
1. Cocaine2. Alcohol3. Amphetamines4. Methylphenidate5. Nicotine
6. Romantic love 7. Listening to music 8. Humor 9. Expectation of $$$10. Inflicting punishment11. Looking at beautiful faces12. Social cooperation13. Eating chocolate
a. Nucleus accumbens
ab
b. Ventral tegmental area
Figure 9.4 Summary of craving studies, showing how the same structures are involved in addiction andcraving irrespective of the substance or object of desire (reproduced with permission from Higgins andGeorge 2007, p. 111)

The Addictions and Disorders of Motivation 227
to screen potential treatments before they areused in a large-scale clinical trial (George et al.,2001; Myrick et al., 2008).
Associations with Neurological Disease
Patients with primary amotivational states arefrequently encountered in clinical practice, andsecondary disorders of motivation are noted ina wide variety of psychopathologies (Table 9.3).The latter merge with apathy and flattenedaffect, and with anergia (as seen in the chronicfatigue syndrome or in hypothyroidism). Theparadigm of a primary motivational state isabulia, in which the patient literally has no will.Patients will sit in a chair all day long doingnothing. Whereas in apathy, patients cannot bebothered to do things, in abulia there is simplyno desire. Further, when asked if they ever feelbored, patients with abulia simply say, ‘no’.The latter disorder is most frequently encoun-tered in patients with basal-ganglia disorders,especially those which damage or destroyanterior cingulate and striatal connections.Abulia may be seen in Parkinson’s disease, butalso following strokes to the basal ganglia andhead injuries which impinge on fronto-striatalstructures. Secondary disorders of decreasedmotivation are seen in the schizophrenias (withnegative symptoms), in some depressions (withapathy and anhedonia) and in such disordersas the emotional indifference of a Kluver–Bucysyndrome. Apathy may be a feature of pituitaryand hypothalamic disease (e.g. adenomas orcraniopharyngiomas) and has been associatedwith alteration of the morphology of the accum-bens in HIV patients. Bhatia et al. (1993) studiedthe behavioural and movement disordersreported in 240 patients with lesions affectingthe caudate nucleus, putamen and globus
Table 9.3 Neuropsychiatric disorders where thereis alteration of motivation
Parkinson’s disease and variantsBasal-ganglia lesionsFrontal-lobe disordersObsessive–compulsive disorderGilles de la Tourette’s syndromeEncephalitis
pallidus (lentiform nucleus). Dystonia was themost frequent movement disorder recorded(36%), but the most common behaviouraldisturbance was the syndrome of abulia (13%),mainly noted with caudate lesions (28%).Depression was a relatively nonspecific finding.
Increased states of motivation occur in asso-ciation with hypomanic and mania drivenness;the intensely driven motor behaviour of Gillesde la Tourette’s syndrome, which is oftenassociated with comorbid OCD; the latter toomay be viewed as another dysregulation ofmotivation.
The main conditions leading to alteration ofmotivation therefore involve frontal- or basal-ganglia function, and imply either overactiv-ity or underactivity in the cortico–striatal–pallidal–thalamic re-entrant circuits describedin Chapters 2 and 3.
Neuropsychological Disturbances
All the addictive substances or their metabo-lites cross the blood–brain barrier and willlead to acute toxicity, with interference witha subject’s ability to perform neuropsychologi-cal tests. These effects should be short-lived andwill abate as the drug is washed out from thebrain. However, there is growing evidence oflonger-term use leading to alterations of cog-nition. Unfortunately, obtaining data is verydifficult. Many people are polydrug abusers;their pre-ingestion cognitive abilities will belargely unknown, and their drug histories unre-liable. Some drugs such as cocaine may leadon to neurological disorders from vasculitis orseizures, which themselves alter cognition. Sincethe individual drugs have differing chemicalprofiles, some neuropsychological differences oflong-term use may be expected, but are hard toidentify under the generalized cognitive blunt-ing that is often reported.
Cannabis use has been associated withmemory and attentional deficits and an amo-tivational state. Chronic cocaine ingestionimpairs executive function, psychomotor speedand manual dexterity, which effects persist afterperiods of abstinence. Amphetamine abuseis reported to lead to poor decision-making(akin to orbital-frontal deficits) and impaired

228 Biological Psychiatry
spatial working memory, while opiate abuseleads to delayed decision-making and a similarworking-memory problem. A common themeunderlying these findings, especially with stim-ulants, is disruption of monoamine influencesin association with disordered frontal-lobefunction.
The increased use of ecstasy has attractedconsiderable interest, and it has been associatedwith deficits of immediate and delayed mem-ory and attention, the former correlating withdiminished 5-HT turnover as measured by CSF5-HIAA levels, even after periods of abstinence(Quednow et al., 2006, 2007).
Chronic alcohol abuse has been reportedto impair cognition across several domains,with mild to moderate difficulties of executivefunction and visuospatial abilities, but relativesparing of episodic memory. Alcohol has beenshown to inhibit neurogenesis, which may havesomething to do with these cognitive deficits.The neurocognitive deficits have been shown tobe partially reversible with abstinence (Gilmanand Hommer, 2008). Interestingly, in the serialfunctional imaging studies in abstinent alco-holics, which show a gradual return of func-tion over the course of at least one month(George et al., 1999), the areas most affectedpersistently following chronic alcohol use arenot primary motor or sensory but rather mul-timodal association areas used in higher cogni-tive tasks.
The cognitive impairments identified in thesestudies may have profound consequences, notonly making the road to rehabilitation moredifficult, but also, by decreasing impulse control,unfortunately fostering the tendency to continuethe illicit drug-taking.
SOME OUTSTANDING ISSUES
Drugs are not the only rewarding factors inour lives, and many social stimuli from food togambling to sex are reinforcing. As with drugs,surrounding environmental contexts assumesignificance to enhance the chance of a behav-ioural sequence, but there are differencesbetween addictive drugs and natural rewards
from a cultural point of view. Drug rewardsmay seem overwhelming of other ones, narrow-ing the behavioural repertoire, and ultimatelydepriving the individual of a healthy life.However, some addictions, like that of theworkaholic, have equal drive, motivation andbehavioural consequences, but are channelledin a socially accepted manner.
The reviewed literature suggests that similarcerebral and neurochemical systems underliethese behaviours, whether drug-driven or not.This raises the important questions of whena behaviour becomes pathological, and whatare the neurobiological correlates of the patho-genesis. Genetic influences are clearly importantin the ease with which addictive behavioursare acquired, as may be the risk for comorbidpsychiatric disorders such as bipolar disorderor schizophrenia. These two categories of psy-chopathology are frequently comorbid withsubstance abuse, and substance abuse is oftena precursor to the later psychopathology,perhaps initially providing self-medication fordeveloping symptoms (such as benzodiazepine,alcohol or cigarette use to calm anxiety).Also, cannabis use is often a precursor to thedevelopment of schizophrenia (see Chapter 7).The underlying neurobiology of addictivebehaviours outlined in this chapter revealscircuits and neurotransmitters that cross overwith major psychopathology. Not only can thisenlighten the understanding of the biology ofthe specific psychiatric disorder, but unravel-ling the neurochemical and neuroanatomicalassociations which are common with addictivebehaviours will enhance preventative andtreatment possibilities.
The role of the limbic forebrain anddopamine is so important in driving behaviourthat damage to such structures may be expectedto have profound clinical effects. Indeed it does,but disorders of motivation find no place insuch diagnostic manuals as the DSM IV-TR,and as such are poorly recognized clinicallyand are underdiagnosed. Understanding of theneuroanatomy of the limbic forebrain allowsfor a better comprehension of these behav-iours, which are intimate with that primeforce, referred to as the ‘will’, once seen as

The Addictions and Disorders of Motivation 229
an independent psychological faculty, nowviewed as tightly bound with identifiableneuroanatomical and neurochemical substrates.Such abrogation of traditional philosophy manyfind uncomfortable.
A reclassification scheme of psychopathologyfocusing on the spectrum of disorders of moti-vation would aid the field in numerous ways. Itis difficult to educate, diagnose and treat amo-tivational disorders (e.g. abulia) if they are notlisted in classification schemes such as DSM IV-TR. Additionally, focusing on the overarchingproblem of disordered motivation might alsoimprove understanding of some other condi-tions, such as the eating disorders (which unfor-tunately, due to space issues, are not covered inthis text). One might also place catatonia underthe umbrella of disordered motivation, with thehypothesis being that the catatonic patient iswell motivated but is unable to translate thisinto subsequent movement. These suggestionsarise from imaging studies showing that cata-tonic patients have widespread and active brainmetabolism, which requires inhibition (e.g. ben-zodiazepines) in order that normal behaviourcan resume (de Tiege et al., 2003).
More recent human studies, a spin-off fromthe direct studies of drug addiction, havecombined brain imaging, notably fMRI, andsocial reward tasks (for money or other positivereward pairings – attractive faces as opposedto unattractive ones). Studies using fMRI haverevealed how the accumbens is reliably acti-vated in states of expectancy, in euphoria andwith craving for not only drugs of addiction butalso sexual cues (see Figure 9.4) (Breiter et al.,1997). This line of research is leading to under-standing of human motivation in a more generalway, which when combined with genetics willprofile the brain associations of motivationsand their subsequent behaviours in some detail.Although much of the work in unravelling the
neurobiology has come from animal studies, thebasics seem to hold for humans. At the presenttime, investigators are attempting to definean integrative model of addictive behaviourswhich includes the ventral tegmental area,accumbens, hippocampus and amygdala(related to salience attribution); the cingulategyrus–prefrontal, orbitofrontal cortex andaccumbens (related to craving and expectation);and loss of top-down regulation associated withfrontal cortex changes (with bingeing and lossof control) (Kalivas and Volkow, 2002). Manyattempts at therapy now specifically targetdifferent aspects of the complex behavioursassociated with addiction, which map rathernicely on to these various circuits.
The work with drugs of addiction is alsoleading to an understanding of basic mecha-nisms of learning, the development of long-termpotentiation, the role of glutamate receptors, theimportance of dopamine and the links betweenepisodic and emotional cues to learning andmemory. Persistence of relapse long after stop-ping an addictive drug suggests long-term brainadaptations. These have been likened to thesetting up of memory traces, responding torenewed presentation of past salient externaland internal cues.
In view of the importance to neuroscience andto society of studying addicts and their propen-sities, it is disappointing that, until recently, rel-atively little funding has been given or directedresearch carried out. Since all drugs of addic-tion lead to a final common neurochemical andneuroanatomical pathway, it is strange that his-torically specialists in alcohol addiction seemto be divorced from those interested in cocaineand so on. Further, so many of those involvedin treatments seem uninterested in the basicanatomy and chemistry, and still consider thatthe problem is one of only a social dimension,devoid of any neurobiological substrate.


10Epilepsy
INTRODUCTION
The longstanding relationship between epi-lepsy and psychiatry has already been noted.The links have been explored by a numberof authors (Temkin, 1971) and stem back toat least the ancient Greek tradition. It is onlyin the 20th century that chronic epilepsy hasbecome more the province of neurology thanpsychiatry. However, there are four reasonswhy psychiatrists need to know about epilepsyanditscomplications.First, thehistoryof itsasso-ciation with psychiatry emphasizes the changingnature of ideas with regards to neuropsychiatricconditions, both their supposed pathogenesisand their psychopathological manifestations.Second, in any psychiatric setting, patients withepilepsy, particularly chronic epilepsy withcontinuing uncontrolled seizures, are still seen.Third, some forms of epilepsy, particularlytemporal-lobe epilepsy, are associated withcognitive and emotional sequelae which closelyresemble psychopathology seen in non-epilepticpatients. Finally, many drugs and stimulationdevicesusedinthemanagementofepilepsyhavealso been used to treat psychopathology, fromthe bromides and barbiturates to, more recently,lamotrigine and vagus nerve stimulation.
PREVALENCE AND CLINICALCHARACTERISTICS
Defining epilepsy is, as with schizophrenia, dif-ficult. The often-quoted definition of Hughlings
Biological Psychiatry 3e Michael R. Trimble and Mark S. George 2010 John Wiley & Sons, Ltd
Jackson, of ‘occasional, sudden, rapid and localdischarges of grey matter’ (Taylor, 1958, p. 100),emphasizes the acute paroxysmal nature of thedisorder, but fails to distinguish it from othersimilar disorders such as migraine or acutepanic attacks. Further, it misses the point thatthe seizure is but one manifestation of theunderlying anatomico/physiological disorderof the brain which leads to the potential to haveseizures. Thus, while it is accepted that the car-dinal clinical symptom of epilepsy is the seizure,and it is usual to accept that epilepsy requiresrecurrent seizures as opposed to a single seizurebefore the diagnosis can be made, it has to beemphasized that epilepsy refers to a heteroge-neous group of conditions, and, like schizophre-nia, clear evidence for organic brain dysfunctionbecomes evident the more it is looked for. How-ever, in a number of cases, even with moderntechnology, recurrent seizures are found in theabsence of identifiable neuropathology.
CLASSIFICATION
It is important to distinguish the classification ofseizures from that of epilepsy. An abbreviatedversion of the classification of seizures is givenin Table 10.1. Although this classification datesback to 1981, it is still generally accepted and nonew version has yet been published.
Partial seizures are those in which the clinicaland EEG changes suggest a focal onset, andthe classification is based mainly on whether or

232 Biological Psychiatry
Table 10.1 Revised ILAE classification of epilepticseizures (1981)
I. Partial (focal, local) seizuresA. Simple partial seizures (consciousness
not impaired)B. Complex partial seizures (with impair-
ment of consciousness; may sometimesbegin with simple symptomatology)
C. Partial seizures evolving to secondarilygeneralized seizures (this may be gener-alized tonic–clonic, tonic or clonic)
II. Generalized seizures (convulsive or noncon-vulsive)
III. Unclassified epileptic seizures
not consciousness is impaired in the attack. In asimple partial seizure, consciousness is retained.Various forms are recognized, for examplefocal motor seizures (when accompanied bya march these are referred to as Jacksonian);seizures with somatosensory or special sensorysymptoms; with autonomic symptoms; or withpsychic symptoms such as dysphasia, dysmne-sia (for example deja vu), cognitive, affective,illusory or hallucinatory experiences. This lastgroup of symptoms is usually accompanied byimpairment of consciousness, and therefore isoften associated with complex partial seizures.In these, the impairment of consciousness isoften the first clinical sign, although simplepartial seizures may evolve into the complexvariety. In patients presenting to psychiatricclinics, complex partial seizures are the com-monest seizure type, and they usually, butnot inevitably, give a history of progression tooccasional generalized motor seizures.
Generalized seizures are those in which thefirst clinical changes suggest bilateral abnor-malities with widespread disturbances of bothhemispheres. Absence seizures (petit mal) areusually associated with regular 3 Hz spike andslow-wave activity on the EEG, althoughvariants of this with 2–3 Hz activity may beseen. Myoclonic seizures typically present withmyoclonic jerking, and are sometimes asso-ciated with clearly delineated EEG changes.Tonic–clonic seizures are the classical grandmal attacks with associated EEG abnormalities.
Finally, seizures that cannot be classified into theabove groupings are included as unclassifiedseizures.
Classic tonic–clonic seizures are unmistak-able. There is sudden loss of consciousness, oftenwithout warning, and tonic muscular contrac-tions are followed by clonic ones. Following theattack, the patient is unrousable for a time, andthere follows a period of postictal confusion. Ifthe attack has a focal origin prior to its general-ization then the patient may experience an aura,namely a brief feeling or sensation immediatelybefore the attack, which represents the originof the epileptic activity. These auras need tobe distinguished from prodomata, which occurseveral hours or even days before a seizure, andserve to warn the patient that one is forthcom-ing. Prodromal symptoms are often changes ofmood, but may also be headaches or changesof appetite.
Generalized seizures that present as absenceattacks impair consciousness briefly and arevirtually unaccompanied by motor signs. Theyoccur primarily in children and in many casescease before the age of 20, although in about 50%of patients this form of seizure is replaced bygeneralized tonic–clonic seizures. In the gener-alized absence seizure there is sudden arrest ofattention, some blinking and eye-fluttering andperhaps pallor with subsequent amnesia.
The symptoms of focal attacks correspond tothe site of origin of abnormal electrical activity,the commonest disturbances seen in psychiatricpractice relating to a temporal-lobe location.There may be disturbance of thought, percep-tion, behaviour, affect and, in complex partialattacks, consciousness. Hallucinations may beformed and complex, as opposed to those whicharise from seizures of primary sensory cortex,which are usually simple, for example a flash oflight. Characteristically in epilepsy the halluci-nation is constant and with repeated episodes iscarefully reproduced. Any recognized emotionmay occur, although the commonest experienceis fear, which is intense, and is often associatedwith a fear of death. Ictal fear may be commonerwith right temporal lesions (Hermann et al.,1992), and associated with the development ofparanoid states (Devinsky et al., 1991). The only

Epilepsy 233
aura that has been reliably shown to have lat-eralizing significance is that of deja vu to theright temporal lobe (Palmini and Gloor, 1992).Depression is uncommon but well documented(Robertson and Trimble, 1983), although rageand outbursts of anger are rare. Cursive seizuresrefer to running during attacks; gelastic seizuresare laughing attacks, while those associated withcrying, which are rarer, are called dyscrasticseizures. In uncinate seizures, the patient expe-riences an unpleasant smell or taste, usuallyunidentifiable, and this may be accompanied bychewing movements and lip-smacking.
Automatisms, which may occur with partialor generalized seizures, refer to ‘all kinds ofdoings after epileptic fits, from slight vagariesup to homicidal actions’ (Jackson, quoted inTaylor, 1958, p. 122). Characteristically, themotor activity is automatic and occurs duringa state of altered consciousness, for which timethere is amnesia. During automatisms, whichgenerally last less than 15 minutes, patientscarry out complex quasi-purposeful behaviour;violence is unusual, but if the patient is inter-fered with during the automatism, aggressionmay result. The neurophysiological basis forautomatisms is thought to be bilateral involve-ment of the amygdaloid–hippocampal region(Fenton, 1972).
Myoclonic seizures are sudden, brief jerk-likecontractions which may be generalized or con-fined to one or more muscle groups. They maybe solitary or repetitive, and may be triggeredby action. They commonly occur late at night orearly in the morning, and in some people heralda generalized tonic–clonic seizure.
Status epilepticus denotes recurrent epilepticseizures without return of consciousness be-tween attacks. Persistent focal seizures arereferred to as epilepsia partialis continua, andwhen complex partial seizures are continuous(complex partial-seizure status), prolongedstates of behaviour disturbance may be seen.These occur with detectable but minimalalteration of higher cognitive function, andassociated hallucinations and delusions mayclosely resemble those of schizophrenia. Incontrast, during absence status, prolongedalteration of cognitive function occurs with
intermittent prolonged stupor. Occasionally itmay present as a psychotic illness, with hal-lucinations and delusions, intermingled witha fluctuating confusional state and associatedEEG changes.
Although approximately 1 in 20 peoplemay have a seizure during their lifetime, theprevalence of epilepsy is far less, being around0.5% for the general population. The currently-used classification of the epilepsies is shown inTable 10.2 (ILAE, 2006).
Terms found in earlier classifications ofepilepsy, such as ‘primary’ and ‘secondary’,have been omitted and the main dichotomy sep-arates epilepsies with generalized seizures fromthose with partial or focal seizures, the latterbeing referred to as localization-related partialor focal epilepsies. The term ‘cryptogenic’ wasintroduced to reflect disorders in which theaetiology was assumed to be symptomatic butwas hidden or occult. Subsequent discussionshave revealed the unsatisfactory nature ofthe term, and indeed of the classificationscheme generally, but as yet no revised versionhas been published (Engel, 2006a, 2006b).Of particular relevance for psychiatrists arethe localization-related symptomatic seizures,further designated by the area of localizationaffected. For example, frontal-lobe epilepsiesoften present as brief episodes of behaviouralchange with minimal or no postictal confusion.
Table 10.2 Classification of epilepsies (ILAE, 1989)
1. Localization-related (focal, local, partial)epilepsies and syndromesIdiopathic with age-related onset, e.g. benign
epilepsy of childhoodSymptomatic, e.g. frontal lobe, temporal lobeCryptogenic, presumed symptomatic with
unknown aetiology2. Generalized epilepsies or syndromes
Idiopathic, e.g. juvenile myoclonic epilepsyCryptogenic and/or symptomatic, e.g. West’s
syndromeSymptomatic
3. Epilepsies and syndromes undetermined asto whether they are focal or generalized
4. Special syndromes, e.g. febrile convulsions

234 Biological Psychiatry
There may be deviation of the head and eyes,sometimes referred to as an adversive seizure.The sudden onset of some frontal seizures, fol-lowed by sometimes bizarre motor movementsoften of the lower limbs (cycling-like), may leadthese attacks to be diagnosed as pseudoseizures(they are in fact pseudopseudoseizures!).
Under temporal-lobe epilepsies there is acategory with particular emphasis on hip-pocampal and amygdala pathology. Theseepilepsies characteristically present with partialseizures, alteration of consciousness and oftenautomatisms.
Some distinctive syndromes are included inthe classification of epilepsies. West’s syndrome(infantile spasms) consists of a characteristicpicture of infantile spasms in association withhypsarrhythmia on the EEG. The onset is inthe first year of life, and the spasms are flexoror extensor, or both. Males are affected morecommonly than females, and a symptomaticsubgroup is recognized with clear evidence ofpre-existing brain damage.
Lennox–Gastaut syndrome occurs in chil-dren up to the age of about 8 and presents with avariety of seizures, focal, myoclonic, atonic andabsence, with a markedly disturbed EEG andassociated learning disability.
Benign childhood epilepsy is a syndrome thataffects children between 3 and 16 years of age. Ithas a good prognosis, and presents with simplepartial seizures, which may or may not lead tosecondary generalized attacks, and an EEG withcharacteristic centrotemporal spikes.
Juvenile myoclonic epilepsy (Janz’s syn-drome) presents in late childhood or earlyadolescence with myoclonic jerks, especiallyin the early mornings, which may or may notprogress to generalized tonic–clonic attacks.
Landau–Kleffner syndrome (LKS) is a child-hood disorder consisting of an aquired aphasiaassociated with paroxysmal EEG changes, usu-ally bitemporal. The latter changes are often seenin slow-wave sleep, and for this reason this dis-order may be closely linked with the syndromeof continuous spike and waves in slow-wavesleep (CSWS, also known as electrical statusepilepticus of slow-wave sleep, ESES). In the
latter, up to 85% of sleep may be infiltratedby the EEG changes, and severe behaviouralchanges follow. In LKS permanent disruptionof linguistic processing may occur.
Rasmussen’s encephalitis is a chronic hemi-spheric encephalitis, of unknown aetiology butsometimes following blunt trauma, associatedwith seizures.
The prognosis of epilepsy is dependent uponthe aetiology, the age of onset of the conditionand the setting in which outcome is examined.While in the majority of patients the outlook isfavourable, and some 55–68% of patients withnew-onset disorder will become seizure-free,and if children are followed into adulthood,over 60% will have gone into long-term remis-sion (Beghi et al., 2009; Hauser and Beghi, 2008).The most striking association with failure oftreatment to control the attacks is the presenceof additional neurological or psychiatric illness(Shorvon and Reynolds, 1982). In particular,patients with combined partial and generalizedseizures and those with symptomatic epilepsyshow a poorer prognosis.
Sudden unexpected death in epilepsy(SUDEP) occurs with an incidence around 0.09–2.7 per 1000 person years, and the causes areunknown.
Why patients have seizures when they dois not clear, although ‘reflex epilepsy’, whereseizures are provoked by sensory or motorevents, has been well described. Visually-evoked seizures, by photic stimulation, andmusicogenic seizures, in which attacks aretriggered by patterned tones, are well-knownexamples. ‘Psychogenic seizures’, where sei-zures are evoked by specific mental activity, alsooccur. Fenwick (1981) divides these into primaryand secondary types. In the former, a directact of will precipitates seizures, for exampleintense concentration or sudden alteration ofattention. In the latter there is precipitation bya mental act without the deliberate intention ofthe patient. Examples include attacks broughton by mental arithmetic, or solving Rubik’scube. (The use of the term ‘psychogenic’ hereis clearly different from its use signifying oneform of non-epileptic (pseudo)seizure.)

Epilepsy 235
GENETICS
The division of epilepsy into idiopathic andsymptomatic groups recognizes that in manypatients there is no known or suspected aetiol-ogy other than potential hereditary disposition.It has been shown that there is an increased inci-dence of seizures in siblings of epileptic patients(6–12%) (Andermann, 1980), and the concor-dance rate for MZ (12–100%) is higher thanfor DZ (0–35%) twins (Newmark and Penry,1980). Further, an abnormal EEG is commonin close relatives of epileptic patients, particu-larly showing generalized spike-and-wave dis-charges (Newmark and Penry, 1980).
The hereditability of epilepsy depends toa considerable extent on the seizure type ofthe proband, being greatest for generalized-seizure disorders and least for partial and symp-tomatic seizures. However, most studies suggesta slight increase in positive family histories ofpatients with symptomatic seizures, emphasiz-ing an environmental–genetic interaction.
Of particular interest has been the discov-ery of a specific pathological lesion, namelymesial temporal sclerosis, in some patients whohave simple and complex partial seizures. It isoften unilateral, and specifically there is scle-rosis of the hippocampus and related struc-tures of the temporal lobe, with neuronal lossand increased glial elements. Many patientswho develop this have a history of febrileconvulsions in childhood, and similar lesionscan be produced in primates by experimen-tally provoking seizures (Meldrum, 1976). Ithas been suggested that the pathology rep-resents damage to the temporal lobe whichoccurs secondary to anoxic episodes at vulner-able periods during life. Since children withfebrile convulsions are likely to have a posi-tive family history for epilepsy (Newmark andPenry, 1980), it seems they inherit a loweredseizure threshold. This renders them prone tofebrile convulsions and to the resulting struc-tural damage. The latter then leads to an evengreater chance of the development of complexpartial seizures in adult life, emphasizing thecomplexities of environmental and genetic inter-actions in these conditions.
There are a number of Mendelian epilepsysyndromes such as progressive myoclonicepilepsies (e.g. Unverricht–Lundborg disease),and the association between epilepsy andfor example metabolic abnormalities such asstorage disorders. A number of specific epilepsysyndromes have been shown to have geneticlinkage. These include juvenile myoclonicepilepsy and familial forms of frontal- andtemporal-lobe syndromes. Autosomal domi-nant nocturnal frontal-lobe epilepsy seems adiscrete syndrome linked with genes codingfor subunits of the cerebral nicotinic receptor(Picard and Brodtkorb, 2007).
SYMPTOMATIC EPILEPSY
Some of the underlying pathologies and meta-bolic defects related to seizures and epilepsyare outlined in Table 10.3.
There is variation with age. Neonatal seizuresmay be caused by prenatal events such as cere-bral malformations, rubella embryopathy,toxoplasmosis and perinatal birth damage fromhypoxia or trauma. Postnatal events includemetabolic changes such as hypoglycaemia,hypocalcaemia, hypomagnesaemia, infectionssuch as meningitis, and a number of inbornerrors of metabolism which become expressedearly in life.
Early-childhood epilepsy (starting aroundthe age of three) is more likely to be idiopathic,while in adult life, tumours and cerebrovasculardisease become prominent causes. Dysembry-oplastic neuroepithelial tumours (DNT) arebenign tumours with mixed glial and neuronalcell types thought to be developmental inorigin. They are often misdiagnosed as gliomas,and are easily treated by surgical resection.
Head injury is a common cause at any age,and is most likely to be responsible if the dura ispenetrated or if the injury produces coma and apost-traumatic amnesia of more than 24 hours.Early seizures following injury increase theprobability of the later development of epilepsy(Jennett, 1975), and the usual pattern is of focalor secondary generalized attacks. Fifty per centof patients who develop post-traumatic epilepsy

236 Biological Psychiatry
Table 10.3 Some causes of seizures and epilepsy
Developmental Heterotopias and dysplasiasGenetic Autosomal, dominant,
nocturnal, frontal-lobeepilepsy
Metabolic causes Hypoglycaemia,hypomagnesaemia, fluidand electrolytedisturbances, acuteintermittent porphyria,amino acid disorders
Trauma Head injuries, especiallypenetrating wounds andbirth injuries
Neurologicalcauses
Tumours, cerebrovascularaccidents, degenerative andstorage disorders,demyelinating diseases,Sturge–Weber and othermalformations, tuberosesclerosis, infections such ascytomegalovirus,toxoplasmosis, meningitis,cysticercosis and syphilis
Drug withdrawal Especially alcohol and thebarbiturates
Vitamindeficiency
Pyridoxine
Poisons Lead, strychnineTemperature Fever
have their first attack within 12 months of injury,although in some patients onset is delayed forseveral years: the relative risk remains elevatedfor some 10 years or longer with severe injury(Annegers et al., 1998). Genetic factors may beimportant here, but evolving neurophysiologi-cal and neurochemical events are presumablyalso involved. This model has relevance forschizophrenia, where the interaction of geneticand early environmental insults does not nec-essarily lead to the expression of the clinicalcondition for a number of years.
Cortical dysgenesis has been shown to havean important association with epilepsy inperhaps up to 20% of patients with intractableseizures. This can take the form of gyralabnormalities or heterotopias. The gyral patternis shown to be disorganized with thickeningof individual gyri; there is disturbance of
the white/grey boundary, and clumps ofheterotopic cells may be seen. These abnormal-ities may not be seen with CT, but are readilyapparent on MRI. Microdysgenesis, essentiallymicroscopic islands of ectopic neurones anddisturbed cortical layering, has also been shownon pathological examination of brains fromsome epileptic patients.
The aetiology of these dysgeneses is unclear,but some are familial, with presumed geneticbasis.
BIOCHEMICAL FINDINGS
In contrast to affective disorder and schizophre-nia, there have been relatively few clinicalinvestigations relating to the biochemical under-pinnings of the epileptic process. However,since epilepsy is associated with hypersyn-chronization of large numbers of neurones,reduced inhibition or increased excitation vianeurochemical processes is considered relevantto pathogenesis. Experimental investigationshave looked at alterations of monamine andacetylcholine activity, but GABA and the excit-atory amino acids such as glutamate and aspar-tate have attracted most attention.
In general, catecholamine agonists raise theseizure threshold, while antagonists lower it(Trimble and Meldrum, 1979). In particular,drugs such as chlorpromazine may precipi-tate seizures, although dopamine agonists suchas apomorphine are not therapeutically valu-able. Experimentally, some antiepileptic drugsincrease CNS 5-HT levels, while others decreaserelease, so 5-HT may have some effect on reg-ulation of the seizure threshold, although datafrom patients are variable, reflecting either anincrease, no change, or a decrease of activity(Reynolds, 1981).
The evidence for the role of GABA is sub-stantial, although it largely derives from animalstudies. Some antiepileptic agents such assodium valproate, benzodiazepines, gabapentintiagabine and vigabatrin are GABA agonists,and GABA antagonists such as picrotoxin andbicuculline are proconvulsant. Both glutamateand aspartate provoke excitatory neuronal

Epilepsy 237
activity and they can be inhibited by certainantiepileptics (Chapman et al., 1983). Recent evi-dence has suggested that these excitatory aminoacidsmaybeendogenousneurotoxins, increasedrelease of which may provoke neuronal damagevia a calcium-dependent mechanism. Since thedepolarized NMDA receptor allows the flow ofcalcium into the cell, a cascade of events leads toan amplification of excitation at many synapsesand such excessive activation might underlieseizure generation. The relevance of the calciuminflux for cell toxicity and thus progressive neu-ronal damage in recurrent seizures is however aconsiderable focus of interest, and is one modelfor seeking out drugs which decrease glutamateactivity and which thus may be neuroprotective.
The role of voltage-gated ion channels andthe regulation of calcium currents are relevant.The former determines the excitability of neu-rones, and sodium currents are largely respon-sible for the generation of action potentials.Voltage-gated currents are related to the gener-ation of seizures, and a number of antiepilepticdrugs act at the sodium channel. The influx ofcalcium through voltage-gated calcium chan-nels activates calcium-dependent potassiumchannels and regulates a number of calcium-dependent intracellular processes, includingtransmitter release. Low-voltage calcium chan-nels are referred to as T-type channels and playa role in the action of ethosuximide. Voltage-gated calcium channels are controlled by sub-units, one of which, the alpha-2-delta subunit,is a binding site for the antiepileptic drugsgabapentin and pregabalin.
INVESTIGATION AND DIFFERENTIALDIAGNOSIS
Following history-taking and neurologicalexamination, it is customary to request routinehaematology and electrolytes, also estimatingcalcium and, less nowadays, serology. Thesedays the imaging technique of choice is either aCT or an MRI scan. High-resolution MRI scans,with specific sequences such as FLAIR, willyield evidence of structural lesions in a muchlarger proportion of patients than routine imag-ing, and detection of tumours, malforations
and migration defects has important treatmentimplications. An EEG is helpful; it may aid withdiagnosis, but it also forms a baseline for anyfuture investigations.
Any suggestion from clinical examination orthe EEG that the seizures are focal should alertthe clinician to the possibility of an intracra-nial lesion being present, and brain imagingfor such patients is mandatory. The finding ofintracranial pathology will obviously requirefurther investigation under the appropriate spe-cialist, using more sophisticated radiologicaltechniques.
Where there is doubt about the epilepticnature of the seizures, the possibility of non-epileptic (pseudo)seizures arises. Further psy-chiatric exploration will become necessary torule out psychopathology, and possibly admis-sion to a specialized unit where prolongedobservation with videotelemetry or ambulatorymonitoring can be carried out.
With careful neuropsychiatric investigationsit is possible to reach a diagnostic conclusionin the majority of patients who present diffi-culties. However, there are patients, especiallyamong those seen at special referral centres,for whom diagnosis is difficult and a primarypsychiatric diagnosis is most likely. Currentestimates suggest that up to 20% of patientsin a tertiary referral epilepsy clinic diagnosedas having epilepsy may suffer from alternativeconditions.
PSYCHIATRIC DISORDERS IN EPILEPSY
Classification
One way to classify the psychiatric disordersof epilepsy is in relation to the seizure itself.Ictal (peri-ictal) disorders are directly related tothe seizure, while interictal disorders are unre-lated in time to the seizure. A third categoryis of disorders which, due to brain damageor disease, lead to both seizures and psychi-atric illness. In this would be included manycauses of learning disability (mental handicap),and some epileptic syndromes such as thoseof West and Lennox–Gastaut. It would also

238 Biological Psychiatry
cover organic mental disorders such as autismand the disintegrative psychosis of childhood,and cerebrovascular disease and Alzheimer’sdisease in adults.
The international classifications of epilepsyreviewed above takes no account of psy-chopathology. Further, classifications such asthe DSM IV and ICD 10 are inadequate whendealing with such neurally-based disorders.In response, to examine this issue, the Com-mission on the Psychobiology of Epilepsyof the ILAE has published guidelines for aclassification of the psychiatric disorders ofepilepsy (Table 10.4). This is multiaxial, takesinto account comorbidities, and recognizes thatthe syndromes are phenomologically discrete(Krishnamoorthy et al., 2007). It acknowledgescomorbidity, namely that people with epilepsycan get as anxious or obsessional as anyone else,
and can be awarded a DSM IV TR category.However it also notes the disorders which seembound in with the epilepsy, giving an organicvariation to the clinical picture. The mainones are the interictal psychoses, the interictaldysphoric disorder, the Gastaut–Geschwindinterictal personality disorder and the postictalpsychoses. Other relevant information recorded(apart from relationship to the seizure) includesrelationship to the EEG change (Forced Nor-malization) and relationship to antiepilepticdrug prescription.
Ictally-related Psychiatric Disorders
No one doubts that acute disruption of cerebralactivity, as occurs with the electrical eventsof the seizure, may disturb cortical func-tion sufficiently to provoke acute psychiatric
Table 10.4 The commission on psychobiology of epilepsy classification of psychiatric disorders in epilepsy
Category Clinical features Key conclusions in draft classification proposal
The problem ofco-morbidity
• Anxiety and phobic disorders• Minor and major depression• Obsessive compulsive disorder• Other somatoform, dissociative
and neurotic disorders
No different from the range of commonmental disorders prevalent in thecommunity and in clinic/hospitalpopulations. Classification should be asper ICD-10 and DSM-IV TR
Psychopathology aspresenting symptomof epileptic seizures
Altered awareness, confusion,disorientation, memorydisturbances, anxiety, dysphoria,hallucinations and paranoidsyndromes
Complex partial, simple partial andabsence status and other epilepsysyndromes can be diagnosed; clinicallysupported by EEG
Interictal psychiatricdisorders that arespecific to epilepsy
• Cognitive dysfunction includingmemory complaints
• Psychoses of epilepsy• Affective/somatoform disorders
• Personality disorders
• Anxiety and phobias specific toepilepsy
• May be general or specific; diagnosedwith standard neuropsychological tests
• To be classified based on therelationship to seizure-prodromal,inter-ictal, post-ictal and alternating
• Hyperethical, viscous, labile, mixedand other
• Both trait accentuation and disorder tobe coded
• Fear of seizures recognized as a distinctand disabling entity
Other information ofrelevance
• Relationship to AED therapy• Relationship to EEG change
Coded as not documented; associatedwith institution and/or withdrawalwith specified time periods for bothpresence or absence of associated EEGchange documented

Epilepsy 239
syndromes. Many of the manifestations ofsimple and complex partial seizures outlinedabove are psychological symptoms which,in other settings, would clearly be describedas psychopathology. In addition, prodromalsymptoms, predominantly dysphoric, and thepsychiatric presentations of both generalizedabsence and complex partial seizure status, areincluded in this category.
Postictal confusion occurs immediately fol-lowing the seizure, when there is usually stilldisruption of the EEG, mainly with diffuse slowfrequencies and little normal activity. Patientspresent with a variety of behaviours, the under-pinnings of which are clearly-defined confu-sional states. These are short-lived, rarely lastingmore than an hour, but occasionally can persistfor days or longer, especially in the learning-disabled. Recurrent seizures, which do not allowfor mental-state recovery between attacks, canalso lead to prolonged states of obtunding.
Typical emotional experiences include fearand depression. The severity of the latter rangesfrom mild to severe, and in some patients sui-cidal ideation is reported. Ictal depression lastslonger than other ictal epileptic experiences, andmay persist for longer than 24 hours.
Ictally-driven psychoses may beschizophrenia-like, especially in complexpartial-seizure status, although more often theyrepresent an obvious organic brain syndromewith a variety of hallucinatory and delu-sional experiences and evidence of cognitivedisruption in association with a disturbed EEG.
Postictal states such as the above should notbe confused with the later-developing postic-tal syndromes, although the syndromes mayemerge from the repeated acute states. In manycases however the postictal syndromes comeon several hours or more following the seizure,when the acute confusion of the immediate pos-tictal phase has passed.
Logsdail and Toone (1988) conducted a sur-vey of patients with postictal psychoses. Mosthad complex partial seizures with secondarygeneralization, and the majority had an increasein seizures prior to the onset of psychosis, usu-ally as a cluster. A lucid interval, from one to sixdays, was clearly described in 80% of cases. On
Table 10.5 Clinical features of postictal psychoses
Clusters of seizuresLucid intervalVariable alteration of consciousnessMixed affective stateFear of impending deathReligious hallucinations and delusionsTime-limited (days to weeks)
follow-up, after several years, 21% had becomechronically psychotic. These postictal psychoticstates have a number of features which are hall-marks and when present lead to the diagnosis.These are shown in Table 10.5. Notable are thereligious hallucinations and delusions, the fearof impending death and the relative absenceof clouding of consciousness. The EEG often isnot so abnormal, and may show an improvedpattern on the interictal state, suggesting linksbetween this state and Forced Normalization(see below). The level of consciousness is veryimportant clinically since if patients have com-mand hallucinations to commit suicide, theycan plan such acts and carry them out. This isin contrast to any self-harm, which occurs in theimmediate postictal phase of confusion, whensuch directed actions are not possible.
Kanemoto and colleagues (2002) noted 2% ofall patients attending an epilepsy centre had apostictal psychosis, but that in the subgroupwith temporal-lobe epilepsy, the figure was11%. In their series, the ‘lucid interval’ rangedfrom less than 24 hours to 7 days, and the psy-chosis itself from 12 hours to more than 1 month.They have stressed the close link with psychicauras such as deja vu and ictal fear.
Kanner and colleagues (2004) have stud-ied the postictal behavioural disorders in somedetail. They have noted in addition to the psy-choses (7%) a spectrum which includes anxi-ety (45%) and dysphoric/depressive symptoms(45%) and hypomania (22%). These presenta-tions were associated with a past history ofdepression and anxiety; they are often not rec-ognized to be related to the ictus (with the timeinterval after the attack not being immediate)and are usually untreated, even though theycan be very distressing for patients.

240 Biological Psychiatry
The pathophysiology of the postictal psy-choses is unknown. Logsdail and Toone (1988)hypothesized that postictal psychosis resultsfrom increased postsynaptic dopamine sensitiv-ity. Ring et al. (1992) tested this hypothesis usingsingle-photon-emission computed tomography(SPECT) and the D2 ligand [123I]IBZM. Theynoted that patients with epilepsy and psychoseshad decreased binding to the ligand, suggestingthat there was increased release of endoge-nous dopamine in the psychotic state. Othershave suggested that the disorder represents arestricted limbic-status epilepticus, but limitedfunctional imaging studies have produced con-tradictory results (Kannemoto et al., 2002). TheSPECT data with IBZM suggest increased activ-ity in the right fronto-temporal area.
Interictal Psychiatric Disorders
There are few reliable epidemiological studiesof the psychopathology of epilepsy. Manyare carried out only on selected populations,and both the classifications of the epilepsyand the psychopathology may be hard toverify. Most point to a higher prevalence ofinterictal psychopathology with localization-related temporal-lobe epilepsy and in patientswith difficult-to-control seizures. The general-practice survey of Edeh and Toone (1985)revealed 48% of patients to be classified as casesusing the Clinical Interview Schedule. Patientswith focal epilepsies had more psychopathol-ogy than those with generalized epilepsies; in atemporal-lobe group, 36% had an affective dis-order, and 8% an affective or organic psychosis.
Jalava and Sillanpaa (1996) examineda prospective population-based cohortover a span of 35 years, and noted thatpatients with epilepsy, in comparison withcontrols, had a fourfold risk of developingpsychiatric disorders.
The rates of psychopathology are greater ifselected populations are examined, such as thelearning-disabled or those in tertiary-referralspecial clinics. Further, it has recently beenshown that the relationship, at least with depres-sion, is two-way. In other words, people withdepression have an increased risk for seizuredisorders, and vice versa (Hesdorffer et al., 2006).
Personality Disorders
This at one time was a most controversialissue. The main arguments revolved aroundwhether any personality changes seen are sec-ondary to an organic brain syndrome, preferen-tially affecting the temporal lobes and especiallylimbic structures, or whether they are due tosecondary factors such as recurrent headinjuries, social stigmatization and the long-term prescription of anticonvulsant drugs.Amidst the theorizing, several advances in theneurosciences revealed the important role ofthe frontal lobes in regulating behaviour, andfrontal-lobe syndromes, essentially personalitydisorders, were described in animals andhumans. Further, a temporal-lobe syndrome,namely the Kluver–Bucy syndrome, wasdescribed after bilateral damage to the temporallobes, which presented as an alteration of per-sonality traits, with calming of emotions, visualagnosis and alterations of sexual behaviour.
Many studies in this area have used the MMPIto detect personality change, and while someshow differences between epileptic patients anda normal population, many fail to show sta-tistical differences between temporal-lobe andgeneralized epilepsy subgroups (Trimble, 1991).Interestingly, several of these ‘negative’ resultsshow nonsignificant but higher levels of psy-chopathology in a temporal-lobe group, raisedparanoia or schizophrenia scales being quitecommon. In some studies, scores for psychoticbehaviour are higher in those with combinedpsychomotor and generalized seizures or thosewith bilateral foci. In addition, in a meta-analysisof MMPI studies in the literature (Hermann andWhitman, 1984), patients with epilepsy werecompared to others with chronic medical dis-orders. Epileptic patients who were classifiedas abnormal by the MMPI showed more severepsychopathology than other groups, suggestingthat while chronic illness may be one variable,patients with epilepsy were more susceptible tosevere problems.
To overcome the shortcomings of the MMPI,Bear and Fedio (1977) developed a ratingscale of 18 behavioural features, drawn fromthe literature, thought to be associated with

Epilepsy 241
temporal-lobe epilepsy. Their scale was appliedto epileptic patients with a temporal-lobefocus, neurological control patients and healthycontrols. They reported that the temporal-lobegroup scored significantly higher on sev-eral subscales, notably humourless sobriety,dependency, obsessionality, and religious andphilosophical concerns. This study has hadpartial replication from other groups (Hermannand Riel, 1981; Hermann et al., 1982), who alsohighlighted a sense of personal destiny, depen-dence, paranoia and philosophical interests inpatients with a temporal-lobe origin of attackswhen compared with those with generalizedseizures. Psychopathology has been reported tobe especially overrepresented in patients withauras of ictal fear, being more often classified,using Goldberg’s sequential diagnostic systemfor the MMPI, as psychotic. An aura of ictal fearimmediately suggests a periamygdaloid, andhence limbic, focus for the onset of the seizure.
Other evidence that patients with limbic-related epilepsies may be more prone topsychopathology derives from Nielsen andKristensen (1981). They also applied the Bear–Fedio scale to patients with temporal-lobeepilepsy, and noted that those with a medio-basal EEG focus showed significantly morehypergraphia (a tendency towards extensiveand compulsive writing), elation, guilt andparanoia than those with a lateral focus. Adamec(1989) applied the Bear–Fedio inventory to 114patients with epilepsy, and to other groupswith psychiatric illness and no epilepsy, normalcontrols and patients with chronic illness otherthan epilepsy. Cluster analysis revealed a clus-ter with psychiatric illness and seizures that wasdistinguished from the nonpsychiatry-seizurepatient cluster by the presence of depressionand metaphysical symptoms, and the reportingof ‘limbic’ auras such as jamais vu, time changesand formed images. Thus several studies haveused a limbic marker (auras or EEG findings)to identify patients with limbic epilepsy, andnoted an association between the latter andpsychopathology (Trimble, 1991).
The importance of these and related findingsfor biological psychiatry and neuropsychiatrycannot be overemphasized. Generally, the data
suggest that patients with epilepsy do showabnormal personality profiles, although themain argument relates to whether a subgroupwith temporal-lobe epilepsy may be identified.While the results do not support the conceptthat a specific ‘epileptic personality’ exists inall patients with temporal-lobe epilepsy, theydo suggest that patients with temporal-lobelesions, particularly those with medially-sitedlimbic lesions, are more susceptible to severepsychiatric disturbances, notably scoring highon such parameters as religiosity, emotionalityand paranoia. This should be seen as represent-ing the outcome of an organic process in thelimbic system.
The view that there is a specific interictal syn-drome of temporal-lobe epilepsy receives mostsupport from clinical evidence and has beenstrongly made by Geschwind and colleagues(Geschwind, 1979; Waxman and Geschwind,1975). They have drawn attention in particularto disorders of sexual function, plasticity ofbehaviours, religiosity, hypergraphia, philo-sophical concern and irritability (see Table 10.6),and disturbances of mood, often short-lived,are noted. Further, there are nascent intellectualinterests, with preoccupation with religious,moral and philosophical themes. Finally, thereare altered interpersonal dispositions, whichinclude increased preoccupation with detail(obsessionality), circumstantiality of speechand a tendency to prolong social encounters,referred to as viscosity. Such diagnostic man-uals as the DSM IV-TR are of no help inunderstanding this syndrome, since it andother well-defined syndromes of epilepsy (e.g.postictal psychosis) will not be found therein.
The hypergraphia of this syndrome fre-quently leads to a written output that ismeticulous, obsessional and carried out with
Table 10.6 Features of the Gastaut–Geschwindsyndrome
HypergraphiaHyposexualityHyperreligiosityIncreased concern with philosophical mattersIrritabilityMood labilityViscosity

242 Biological Psychiatry
a compulsion. The content is often moral orreligious. Repetition of words and sentencesmay be seen. Variants include excessivedrawing or painting, or the hiring of a thirdparty to write down information. There is somesuggestion that hypergraphia is associatedwith nondominant-hemisphere temporal-lobedisturbances (Trimble, 1986c).
Rao et al. (1992) examined viscosity, anotherfeature of this syndrome. This refers to astickiness of thought processes, and to an‘interpersonal adhesiveness’, or increased socialadhesion. Patients display circumstantiality,have difficulty terminating conversations, andtend to prolong interpersonal encounters, forexample interviews with physicians, beyondwhat is indicated by social cues. They reportedthis trait to be commoner in patients with a leftor bilateral seizure foci, and suggested it repre-sented a subtle interictal language disturbance.
Religiosity
The ‘heightened religiosity’ of epilepsy hasbeen recognized since the 19th century bythe French and German alienists (Trimble,2007b). Studies have found that ‘religiosity trait’scores can distinguish between patients withtemporal-lobe epilepsy, normal controls andpatients with other psychiatric or neurologicalconditions, including extra-temporal focalepilepsy and generalized epilepsy. Ecstatic ictalexperiences, in some cases accompanied byvisions of a religious nature, have been reportedin patients with EEG evidence of temporal-lobedischarges (Saver and Rabin, 1997), and suddenreligious conversions have been reported in thepostictal period, noted above.
Trimble and Freeman (2006), using the Bear–Fedio scale in addition to other scales thatassess aspects of individual religious experi-ences and behaviour, examined three experi-mental groups. The first consisted of 28 peoplewith temporal-lobe epilepsy and a prominentdevotion to religion, identified clinically. Thesecond consisted of 22 people with temporal-lobe epilepsy who had no religious affiliations.In the third group were 30 regular churchgoers
without known epilepsy. The purpose of thestudy was to examine in more detail the psy-chological profile of those patients with epilepsyand religiosity, and, by comparing them with theother epilepsy sample, to examine the underly-ing epilepsy variables that might be related tothe religious experiences.
They were able to reconfirm the originalfindings of Geschwind and his school, and showthat the temporal-lobe religious group not only,as expected, endorsed the religiosity subscaleof the Bear–Fedio scale, but also revealed otherelements of the Gastaut–Geschwind syndrome(see Figure 10.1). Notably, the religious groupalso scored highly on the subscales of emo-tionality, philosophical interests, anger andsadness, dependence and hypergraphia. Theywere also rated by a significant other to havemore paranoia and mental viscosity than thenonreligious sample. Thus, the profile thatemerged in the religious patients with epilepsywas true to the original clinical descriptions ofthe Gastaut–Geschwind syndrome, and empha-sized hypergraphia, philosophical interests andemotionality linked with the hyperreligiosity.
When the two groups of patients withtemporal-lobe epilepsy were compared, thosewith the religiosity were noted to more oftenhave had a history of episodes of postictalpsychosis (although they were not psychoticat the time of interview) and more electroen-cephalogram changes that were bilateral thanthose without the religiosity.
The ordinary churchgoers were different intheir backgrounds from the epilepsy patients(more females, of an older age, who were morelikely to be married, and with a better educa-tional level and occupational status), but theyalso differed in their religious behaviours. Thepatients with epilepsy and religiosity were morelikely to belong to a religion not regarded asmainstream (i.e. Church of England or Catholic),Seventh Day Adventism being popular. Thequestion ‘How often have you felt as though youwere very close to a powerful spiritual force thatseemed to lift you outside?’ was endorsed sig-nificantly more by those with epilepsy and reli-giosity than the non-epilepsy churchgoers, butinterestingly, there was no significant difference

Epilepsy 243
Self-reported behavioral profiles
4.5
3.5
2.5
Mea
n T
rait
Sco
re
Hyp
erga
raph
ia
Rel
igio
sity
Obs
essi
onal
is
Gui
lt
Sad
ness
Par
anoi
aTraits
Total Score4540353025
151050
20
Pat
ient
s w
ith
Patients withhyperreligiosity
Patients with noreligiosity
Group
Sco
re
Phi
loso
phic
al
Dep
ende
nce
Vis
cosi
ty
21.5
0.50
1
3
4
t-test
Figure 10.1 Profiles on the Bear–Fedio self-reported rating scale, comparing patients with epilepsy withand without religiosity. This confirms the original Bear–Fedio syndrome, with high ratings on religiosity,hypergraphia, emotionality and philosophical ideas * = p < 0.05
in response to the question that asked if theyhad had any religious experience. Neither wasthere any difference in responses to questionswhich asked about the frequency or duration ofthe religious experiences that they had.
With regards to the actual religious experi-ences, the epilepsy religious sample reportedmore experiences of the feeling of the pres-ence of some external being, either of evil orof great spirituality, associated with feelings ofdeath or dying and intense fear. The experienceswere ineffable and noetic, not simply an aware-ness. There was identification, of and with thatessence, and ecstasy and miracles were featuresof the descriptions.
These results lead to some relevant con-clusions. First, temporal-lobe epilepsy can beassociated with an identifiable constellationof behavioural dispositions, which have beenidentified for years, but are now better doc-umented with rating-scale assessments. Thisconstellation in its full form is referred to asthe Gastaut–Geschwind syndrome. Second,patients with epilepsy and hyperreligiosityhave often experienced postictal psychotic
states, underscoring the potential links betweentheir psychological profile and that of anepilepsy-related psychosis.
From the neurological point of view, it wasthe patients with temporal-lobe epilepsy andbilateral disturbances of function (as revealedthrough the electroencephalogram) in their tem-poral lobes who reported the most intense reli-gious experiences, especially endorsing itemsto do with the inner subjective nature of theirexperiences, their ineffability and the spatial–temporal component.
In a further investigation, in which the vol-umes of the hippocampus and the amygdalawere measured, using MRI, in patients withepilepsy whose interictal behaviour was ratedusing the Bear–Fedio scale, Wuerfel et al. (2004)found that patients who met the criteria forhyperreligiosity had significantly lower meanright hippocampal volumes than those reportedas not religious. While in itself this findingwas interesting, confirmation of the anatomi-cal association emerged when the actual scoreson religiosity were correlated with hippocam-pal size. Thus, there was a significant negative

244 Biological Psychiatry
association between religiosity scores and hip-pocampal size, on the right side only. Further,this correlation was found for both patient self-ratings and on the independently obtained carerratings; the smaller the right hippocampus, thegreater the expressed religiosity. These data sug-gest that the right-sided limbic structures maybe of central importance to the development ofthese personality attributes.
Personality Changes in Juvenile MyoclonicEpilepsy (JME)
Although most of the discussion of the personal-ity changes in epilepsy has revolved around theinterictal syndrome of temporal-lobe epilepsy,the personality associations with one of thegeneralized epilepsies was described by Janz(2002). These include poor sleep habits, goingto bed early and waking late, and a personalityprofile characterized by ‘unsteadiness, lack ofdiscipline, hedonism and indifference towardstheir illness’. These patients were prone to moodswings, were suggestible, and could react withundue sensitivity. These characteristics often ledto poor compliance with treatment regimes, andmade management difficult.
Several studies have used rating scales toassess groups of patients with JME, althoughlittle has come from them, being few in numberand using standardized ratings of psycho-pathology, which, as with the temporal-lobe-epilepsy studies, may be inappropriate. It ishowever of interest that studies of cognition inpatients with JME suggest that they do less wellon frontal-lobe tasks than matched patientswith temporal-lobe epilepsy (Trimble, 2000).
Aggression
As emphasized in Chapter 3, neurophysio-logical studies in aggression strongly point toalteration of the limbic system, in particularamygdala function. Since this area of the brain isfrequently damaged in patients with temporal-lobe epilepsy, it may be expected that theywould display more aggression than thosewith other forms of epilepsy. This is an area of
considerable controversy. While ictal violence,recorded using videotelemetry, has beenclearly described (Delgado-Escueta et al., 1981),the problems of recording and quantifyinginterictal aggressive behaviour, almost entirelyseen in an interpersonal setting, have led toconsiderable variability of results in clinicalstudies. Hermann and Whitman (1984) notedthe high risk factors for aggression in epilepsy,which include organic cerebral disease, lowsocioeconomic status and poor environmentalupbringing. Fenwick (1986) noted the evidencefrom intracranial implanted electrode studies,which suggests that the amygdala is involvedin the mediation of aggression in man, furthercommenting that an amygdalectomy improvesaggressive behaviour in those series where it hasbeen tried. In addition, patients with temporal-lobe epilepsy who undergo temporal lobectomyshow improvement of seizures and improve-ment of behaviour, most notably aggression.His conclusion was that a relationship betweenseizure discharges and aggressive behaviourhad been shown, although the relationship wasmore between poor impulse control and braindamage than the seizure process itself.
In a study using MRI imaging, Tebartz vanElste and colleagues (2000) noted that patientswith epilepsy and severe aggression (referredto as intermittent explosive disorder) had asignificantly higher incidence of encephaliticbrain disease and left-handedness, more bi-lateral EEG abnormality and less frequenthippocampal sclerosis than controls. In theaggressive patients a subgroup showed severeamygdala atrophy. In a further analysis,voxel-based morphometry revealed reductionsof grey-matter density over large areas of theleft extratemporal neocortex, maximal in theleft frontal neocortex (Woermann et al., 2000).
A related condition is the episodic dyscontrolsyndrome (Fenwick, 1986; Monroe, 1970), a syn-onym for episodic dyscontrol. This presents assudden episodes of spontaneously released vio-lence, often in the setting of minimal provoca-tion, which tend to be short-lived. They may beprovoked by small amounts of alcohol, and afterthe events, patients may feel remorse. Generally,the condition is associated with nonspecific

Epilepsy 245
abnormalities that are also seen in epilepsy,for example evidence of brain damage, lowsocioeconomic status and a disturbed upbring-ing. Evidence of minimal neurological damage,with soft neurological signs and abnormal EEGs,is often found, although there is no evidence thatthese episodes have the same pathophysiologyas epileptic seizures.
Affective Disorders
Many people with epilepsy are miserableand unhappy, but this does not equate to adepressive illness. Further, many patients sufferfrom a chronic dysphoria, often provoked orexacerbated by the long-term administrationof anticonvulsant drugs. However, interictaldepressive states are frequent in epilepticpatients, and postictal affective states arebecoming increasingly recognized. Severalauthors have commented on the frequency ofsuicide in epileptic patients (Blumer, 2004),the risk being approximately five times thatexpected, highest for those with temporal-lobeepilepsy. In patients assessed for self-poisoning,epileptic patients are overrepresented (Mackay,1979), and frequent use of barbiturates for thispurpose is noted. Anticonvulsant medicationsthat act at the GABA receptor complex arehighly implicated (Trimble, 1997).
Epidemiology
Assessing the frequency of epilepsy and depres-sion from selected clinic samples gives a biastowards the more severely affected patients andalso those on the most medication. In commu-nity studies, Edeh and Toone (1987) reportedthat 22% of unselected patients with epilepsywere rated as having a depressive disorder.A Canadian community health survey exam-ined 253 people with epilepsy using a ratingscale to identify a history of depression, noteda lifetime prevalence of depression at 22%; thiswas compared with 12% in the general popula-tion (Tellez-Zenteno et al., 2005).
More recently, Ettinger et al. (2004) assesseddepression in 775 people with epilepsy, and
compared the incidence with patients withasthma, and also with healthy controls. In thisstudy, a rating-scale assessment was againused (Centers of Epidemiological Studies –Depression Instrument). Symptoms of depres-sion were significantly more frequent in theepilepsy group (36.5%) than in those withasthma (27.8%) and the controls.
Several studies have noted a correlationwith seizure frequency. In an epidemiologicalstudy, Jacoby et al. (1996) noted that depressionoccurred in 4% of seizure-free patients, in10% of patients with less than one seizure amonth, and in 21% patients with higher seizurefrequency. O’Donoghue et al. (1999) noted thatpatients with epilepsy with continuing seizureswere significantly more likely to suffer fromdepression than those in remission (33% vs 6%).
There are a number of studies from selectedpatient groups, for example tertiary centres, andfrom those awaiting surgery for epilepsy, whichnote in these populations an even higher fre-quency of depression (Jones et al., 2005; Victoroffet al., 1994). Another finding, which has beenverified, is the association between depressivesymptomatology and quality of life in peoplewith epilepsy. Depressive symptoms tend to bethe most important predictor of quality of life,and were a more powerful predictor than theactual seizure frequency (Gilliam et al., 1997).
Some studies have shown patients withtemporal-lobe epilepsy to be more prone todepression than other groups, but other investi-gations have failed to confirm this. Quiske et al.(2000) found that patients with temporal-lobeepilepsy who had mesial temporal sclerosiswere more likely to report depression. Ingeneral terms, there is greater agreement thatpatients with complex partial seizures aremore likely to have a depressive disorder(Robertson, 1998).
There are also studies linking frontal-lobedysfunction to the depression of epilepsy.These have emerged from investigations usingbrain imaging (PET or SPECT) and neuropsy-chological batteries. Hermann et al. (1991) notedthat patients with temporal-lobe epilepsy anddepression were more likely to perform poor-ly on frontal-lobe neuropsychological tasks,

246 Biological Psychiatry
especially with a left-sided seizure focus.Schmitz et al. (1997) noted similar frontalchanges and localizations using SPECT, andBromfield et al. (1990), using PET, reportedthat patients with temporal-lobe epilepsy andassociated depression revealed bilateral reduc-tions of frontal-lobe metabolism. Theodore et al.(2007) have reported decreased 5-HT1A bindingin the ipsilateral hippocampus of depressedepilepsy patients, unrelated to the presenceof medial temporal sclerosis or laterality offocus. These data relate well to the findings innon-epileptic bipolar patients (Chapter 8).
Although these studies, of necessity, were ona limited number of patients, the concordancebetween the findings does support an anatomi-cal association between temporal-lobe epilepsy,depression and frontal-lobe dysfunction.
With regard to the temporal-lobe associa-tion with depression, it is of interest that thereare a number of studies outside the field ofepilepsy which suggest that hippocampal vol-ume loss is associated with affective disor-ders (see Chapter 8). Although further researchin this area is needed, neuroimaging studiesare revealing an underlying neurocircuitry ofdepression in psychiatric patients without a neu-rological disorder. This neurocircuitry includesthe hippocampus, in keeping with the findingsin subgroups of patients with epilepsy.
Recent data have suggested a bidirectionalrelationship between epilepsy and several co-morbid conditions. In other words there is anincreased risk of patients with anxiety, depres-sion or schizophrenia developing epilepsy afterthe psychiatric disorder (Hesdorffer et al. 2006).This has led to a renewed interest in these bio-logical links.
The Relationship of Antiepileptic Drugsto Depression
There is an older literature which linksbarbiturate-related drugs to depression, butmore recent data suggest that it is possible todistinguish between AEDs with the potentialto have positive effects on mood, such ascarbamazepine, lamotrigine and valproic acid,and these older compounds. The AEDs most
associated with this effect seem to be thosewhich act at the benzodiazepine–GABA recep-tor complex, and include tiagabine, gabapentintopiramate and vigabatrin. Since in psychiatricpractice it is known that benzodiazepines andother GABA agonists are associated clinicallywith depression, and that abnormalities of CSFGABA have been reported in patients withdepression (Trimble, 1996), the link betweensudden cessation of seizures (Forced Normal-ization), GABAergic agents and the onset ofdepression seems reasonably secure. Further,these studies have revealed that patients withepilepsy and a prior history of an affective dis-order are the more likely to develop depressionin these circumstances.
Bipolar Disorder and Epilepsy
It used to be confidently stated that bipolar dis-order was rare in patients with epilepsy (Wolf,1982). Such statements were made prior to theuse of standardized diagnostic manuals such asthe DSM IV, and were also based upon clini-cal impression rather than assessment on ratingscales. It was accepted however that in the con-text of the postictal state, patients could developa postictal psychosis, the features of which wereoften manic or hypomanic, although more gen-erally the presentation was one of a mixedaffective state, often with psychotic features.Kanner et al. (2004) noted postictal hypomanicsymptoms in 22% of patients, often with asso-ciated psychotic phenomenology. In the studyof Ettinger et al. (2005), bipolar symptoms wererevealed in 12.2% of the epilepsy patients, whichwas twice as much as in patients with asthma,and seven times as much as in the healthy com-parison group. Of those who in the screeningprocess were rated as potential patients withbipolar symptoms, nearly 50% were rated by aphysician as having a bipolar disorder.
These data raise some doubts about the pre-vious suggestions that bipolar disorder is rare inpeople with epilepsy, and about our knowledgeof the association between these two disor-ders. However, the older discussions relatedmore to classical manic–depressive disorder,

Epilepsy 247
as opposed to the more recently developed con-cepts of the bipolar spectrum, which is currentlythe focus of psychiatric interest.
Interictal Dysphoric Disorder (IDD)
The issue of phenomenology of depression inepilepsy is very much a matter of debate. Ingeneral terms, it is reasonable to hypothesizethat patients with epilepsy can experience formsof mood disorder identical to those of patientswithout epilepsy and classifiable with standard-ized diagnostic manuals. However, it is equallyreasonable to assume that the underlying brainpathology can influence the expression of mood-disorder symptoms, making less evident someaspects and emphasizing others.
Comorbid anxiety symptoms have been iden-tified in 73% of patients with epilepsy anddepression (Robertson et al., 1987). This is veryimportant clinically, since they may worsen thequality of life of depressed patients and signifi-cantly increase the risk of suicide (Kanner, 2006).
Mendez et al. (1986) investigated the clini-cal semeiology of depression in 175 patientswith epilepsy, and reported that 22% couldbe classified as having atypical features. Inparticular, classic endogenous-type depressivesymptoms, such as feelings of guilt, ‘Gefuhl derGefuhllosigkeit’ and a circadian pattern of symp-tom severity were rarely reported. Kanner et al.(2000) showed that 71% of patients with refrac-tory epilepsy and depressive episodes severeenough to need a psychopharmacological treat-ment failed to meet criteria for any DSM IV axis1 diagnosis. A study of 199 consecutive patientswith epilepsy revealed that 64% failed to meetany DSM IV criteria using two structured clin-ical interviews, namely the Structured ClinicalInterview for DSM IV Axis I (SCID-I) and theMini International Neuropsychiatric Interview(MINI) (Kanner et al., 2004).
The peri-ictal cluster of symptoms may tosome degree account for the atypical featuresof affective disorders in epilepsy, but the possi-bility that in some cases the mood disorder ofepilepsy has unique characteristics has plausi-bility. Kraepelin (1923) and then Bleuler (1949)
Table 10.7 Main symptom clusters of the interictaldysphoric disorder
Labile depressivesymptoms
Labile affectivesymptoms
Specific symptoms
Depressed mood Fear Euphoric moodsAnergia Anxiety Paroxysmal
irritabilityPainInsomnia
were the first authors to describe a pleomor-phic pattern of symptoms in epilepsy, includingaffective symptoms with prominent irritabil-ity intermixed with euphoric mood, fear andanxiety, as well as anergia, pain and insom-nia. Blumer (2000) coined the term ‘interic-tal dysphoric disorder’ (IDD) to refer to thistype of depressive disorder in epilepsy. It ischaracterized by eight key symptoms groupedin three major categories (Table 10.7): labiledepressive symptoms (depressive mood, aner-gia, pain, insomnia), labile affective symptoms(fear, anxiety) and supposedly ‘specific’ symp-toms (paroxysmal irritability, euphoric moods).Blumer used the term ‘dysphoria’ to stressthe periodicity of mood changes and the pres-ence of irritability and outbursts of aggressivebehaviour as key symptoms. The dysphoricepisodes are described as occurring withoutexternal triggers and without clouding of con-sciousness. They begin and end rapidly andrecur fairly regularly in a uniform manner,occurring every few days to every few monthsand lasting a few hours up to two days.
The theoretical framework suggested byBlumer goes beyond a narrow IDD profile,and he speculated that affective symptomsin epilepsy exist along a continuum, from adysphoric disorder with fleeting symptoms to amore severe disorder with transient psychoticfeatures, to an even more debilitating disorderwith prolonged psychotic states. It seems pos-sible that IDD patients have several features incommon with a specific subset of non-epilepticcyclothymic subjects, where depressive periodsand labile–angry–irritable moods dominate theclinical picture. In a recent study investigatingthe prevalence and psychopathological features

248 Biological Psychiatry
of IDD in patients with epilepsy comparedwith a group of patients with migraine (Mulaet al., 2008) it was diagnosed in 20% of patients,making it one of the most common mooddisorders in epilepsy.
Seizures and Laterality
In his classic study, Flor-Henry (1969, 1983)examined 50 patients with temporal-lobeepilepsy awaiting temporal lobectomy who atone time had been psychotic, and comparedthem with 50 nonpsychotic cases with thesame form of epilepsy. Where the lateralizationcould be determined, he noted that 18% werelateralized to the right hemisphere, and themajority of those had manic–depressive psy-choses. He suggested that affective disorderswere more likely to reflect nondominant-hemisphere pathology. While generalizedtonic–clonic seizures were more often theonly ictal manifestations in the affective-disorder group, the occurrence of psychomotorseizures was lowest. Flor-Henry suggestedthis implied that infrequently-released seizureswere somehow related to the expression of thepsychopathology. This is in keeping with theobservations of decreased seizure frequencyprior to the onset of a depressive illness (Betts,1974), a finding noted in 43% of patients in thestudy of Robertson (1986).
The suggested link of affective disorder withthe nondominant hemisphere in Flor-Henry’sstudies has been criticized not only on thegrounds that the patients selected were allawaiting temporal-lobe surgery, but also be-cause of the small numbers. It has receivedpartial support from some studies (for exampleTaylor, 1975), but was not confirmed by others(Altschuler et al., 1990; Robertson, 1986). If any-thing, the studies tend to suggest an associationto a left-sided focus. Part of the confusion relatesto diagnostic issues: Flor-Henry was referringto bipolar patients, others to depressive illness.Further, surface-electrode EEG is quite anunreliable method of establishing laterality.The instructive case study of Hurwitz et al.(1985) supports this. He described a casestudy of a patient with bilaterally independent
foci. During right temporal discharges shereported euphoria, but with left-sided changesdepression was noted. The association betweenmania and euphoria and right-sided cerebrallesions is discussed further in Chapter 8.
Other Findings
Low serum, red cell and CSF folate levels havebeen reported in a high proportion of patientswith epilepsy (Reynolds, 1976), associated withthe taking of anticonvulsant drugs, in par-ticular phenobarbitone, phenytoin and prim-idone. While the deficiency rarely leads toa megaloblastic anaemia, there are severalstudies which show a high incidence of lowfolate levels in epileptic patients with mentalsymptoms (Reynolds, 1976). Psychoses anddementia are often reported, but several studiesnote the link with depression (Edeh and Toone,1985; Robertson, 1986; Rodin and Schmaltz,1983; Trimble et al., 1980). Reynolds (1986) haspointed out that folate deficiency and depres-sion have also been reported in non-epilepticpatients, not wholly explained by poor diet, andthat S-adenosylmethionine (SAM), a methyldonor involved in folate metabolism, has anti-depressant properties.
Interictal Psychosis
A difficulty with the literature on psychosisand epilepsy is that few authors specify theirprecise diagnostic criteria for psychosis, andrecognized research criteria are rarely quoted.Many continental authors refer to ‘organic brainsyndromes’ in the context of epileptic psy-chosis, whereas British authors tend to use thisphrase to refer to a psychosis in the setting ofunclear consciousness. Generally authors distin-guish between schizophrenia-like presentationsand manic–depressive presentations. Further,a clear dissociation between ictal and interictalpsychoses is not always clear, and issues such asForced Normalization must be accommodatedin any overall concept of understanding thepsychoses of epilepsy.
Perez and Trimble (1980) used the present-state examination (PSE) of Wing to document

Epilepsy 249
the phenomenology of 24 epileptic patientsprospectively referred with a psychosis in clearconsciousness. Of the sample, 50% were cate-gorized as having a schizophrenic psychosis,92% having a profile of nuclear schizophrenia(NS), the diagnosis being based on the first-ranksymptoms of Schneider. The syndrome profileof patients with schizophrenia-like symptomsand epilepsy, when compared to those withschizophrenia and no epilepsy, shows fewsignificant differences, emphasizing the simi-larity of the clinical presentation of these twodisorders. Similar findings have been reportedin a retrospective study by Toone et al. (1982b).
Some differences between process schizo-phrenia and the schizophrenia-like psychosesof epilepsy were emphasized by Slater andBeard (1963), who noted the retention of affec-tive warmth in the latter, patients showing lesspersonality deterioration. They reported on 69patients with a schizophrenia-like illness andepilepsy, and suggested, on statistical grounds,that the association was more than just coin-cidence. They noted an absence of premorbidschizoid personality traits and an absence offamily history of psychiatric disturbance thatmight suggest a predisposition to schizophre-nia. Forty-six had a psychosis that was highlytypical of paranoid schizophrenia, and 12 had ahebephrenic presentation. Eleven of their serieshad a chronic psychosis that had been precededby recurrent short-lived confusional states. Themean onset of the psychosis was 29.8 years,which occurred after the epilepsy had beenpresent for a mean of 14.1 years. In 25% of thecases, the psychotic symptoms appeared as thefrequency of generalized seizures was falling,and there was a preponderance of temporal-lobeabnormalities on neurological investigations.
Epidemiology
Stefansson et al. (1998), in a case-control study,compared the prevalence of nonorganic psy-chiatric disorders in patients with epilepsy tothose with other somatic diseases, the groupsbeing taken from a disability register in Iceland.Although the difference in psychiatric diagnosesoverall was not significant, there was a higher
rate of psychoses, particularly schizophreniaand paranoid states, among males with epilepsy.
Qin et al. (2005), in a study from Denmark,have confirmed the increased risk of schizo-phrenia and schizophrenia-like psychoses inepilepsy; in this study a family history ofpsychoses and a family history of epilepsy weresignificant risk factors for psychosis. Bredkjaeret al. (1998) in a record-linkage study looked forassociations between epilepsy from the nationalpatient register of Denmark and the equivalentpsychiatric register. The incidence of nonor-ganic, nonaffective psychoses, which includedschizophrenia and schizophrenia-spectrumdisorders, was significantly increased in epi-lepsy, even when patients with learning dis-ability or substance misuse were excluded.
Higher prevalence rates for psychoses werefound in studies of much more select popula-tions such as hospital case series. Thus, Gureje(1991), in patients attending a neurologicalclinic, quoted that 37% were psychiatric cases,and that 29% of these were psychotic. Mendezet al. (1993), in a retrospective investigation,reported that interictal psychotic disorderswere found in over 9% of a large cohort ofpatients with epilepsy, in contrast to just over1% in patients with migraine.
Risk Factors
Risk factors for interictal psychosis are shownin Table 10.8. The pathogenesis of psychosis inepilepsy is likely to be heterogeneous and theliterature on risk factors is highly controversial.Studies are difficult to compare because of vary-ing definitions of the epilepsy, the psychiatricdisorder and the investigated risk factors.
There is some evidence for a genetic predispo-sition for the psychoses of epilepsy. The intervalbetween age at onset of epilepsy and age at firstmanifestation of psychosis has been reported assimilar in several studies – around 11–15 years.This interval has been used to postulate the eti-ologic significance of the seizure disorder andsuggest a kindling-like mechanism.
There is a clear excess of temporal-lobeepilepsy in most case series of patients withepilepsy and psychosis, and focal seizure

250 Biological Psychiatry
Table 10.8 Risk factors for interictal psychosis
Age of onset Early adolescenceInterval Onset of seizures – psychosis
Around 14 yearsSeizure type Complex partial, automatisms,
visceral aurasSeizure
frequencyDeclining, but poor control over
the yearsSeizure focus Temporal/limbicNeurology Sinistrality
GangliogliomasEEG Forced Normalization in a
subgroupTemporal mediobasal focus
(sphenoidal)
symptoms that indicate ictal mesial temporalor limbic involvement are overrepresentedin patients with psychosis. There are severalstudies showing that psychoses in generalizedepilepsies differ from psychoses in temporal-lobe epilepsy (Trimble, 1991). The formerare more likely to be of short duration andconfusional. There is also a general consensusthat psychoses are less common in patients withneocortical extratemporal epilepsies.
Stevens and Hermann (1981) suggested thefollowing important variables: age of onset,an abnormal neurological examination, autom-atisms and visceral auras, sphenoidal spikeactivity on EEG, and the presence of multifocalspikes. While some of these may reflect merelymore cerebral disturbance, the automatismswith specific auras and the high incidence ofsphenoidal spike activity would suggest theinvolvement of medial temporal structuresin the psychosis. In particular, the study ofpatients with auras of fear by Hermann et al.(1982) showed that patients with temporal-lobeepilepsy and such auras displayed markedlyraised elevations of some MMPI scales, es-pecially for schizophrenia.
In support of these findings, in a study specif-ically looking at hippocampal and amygdalavolumes, Tebartz van Elst et al. (2002) exam-ined 26 patients with epileptic psychoses, 24with temporal-lobe epilepsy and no psychosis,and 20 healthy controls. The psychotic patientshad significantly increased amygdala sizes in
comparison with the other two groups, whichwere bilateral, and not related to the lateralityof the focus, or the length of epilepsy history.No hippocampal differences were noted in thisstudy. In a complementary study on the samegroups, Rusch et al. (2004) was unable to findany neocortical–cortical volumetric differences.
Schmitz and Trimble (2007) identified thefollowing risk factors for developing psychosisin epilepsy: complex partial and absenceseizures, multiple seizure types, poor seizurecontrol and a history of generalized statusepilepticus. Age of onset of epilepsy in latechildhood and early adolescence emerges fromseveral studies (see Toone, 1981), while otherdata suggest that the relationship is not betweentemporal-lobe epilepsy and partial seizures,but between temporal-lobe pathology andcomplex partial seizures that lead to secondarygeneralized attacks.
In a follow-up study of 249 patients withtemporal-lobe epilepsy who had earlier hada temporal lobectomy, Roberts et al. (1990)reported on 25 that had a schizophrenia-likepsychosis before or after surgery. They notedassociations of the psychosis with pathologicallesions affecting the medial temporal lobe,which were developmental and present foetallyor perinatally, and led to an early onset ofepilepsy. Gangliogliomas seemed to be overrep-resented pathologically.
In the only other pathological study ofepileptic psychosis, Bruton et al. (1994) reportedthat psychosis was associated with larger cere-bral ventricles, excessive periventricular gliosisand more focal cerebral damage than nonpsy-chotic controls, and that brains from patientswith schizophrenia-like psychosis had morewhite-matter softenings. However, most oftheir small number of patients did not have theschizophrenia-like psychosis defined by Slater.
Laterality
Flor-Henry (1969) suggested that a left-sidedtemporal-lobe focus was more likely to be asso-ciated with a schizophrenia-like psychosis, con-trasting this with the right-sided abnormalitylinking with an affective disorder. The evidence

Epilepsy 251
for the former is more substantial than the lat-ter, although there are negative studies (Schmitzand Wolf, 1991).
Studies supporting the laterality hypothesisof epilepsy-related psychosis have been madeusing surface EEG, depth-electrode recordings,computed tomography, neuropathology, neu-ropsychology, positron-emission tomography(PET) and more recently MRI. Trimble (1991)summarized the earlier literature; of 14 stud-ies with 341 patients, 43% had left, 23% right,and 34% bilateral abnormalities. This is a strik-ing bias toward left lateralization. However,lateralization of epileptogenic foci was not con-firmed in all controlled studies. Again, it maybe that certain symptoms rather than any syn-drome are associated with a specific side offocus. Trimble (1991) pointed out that a specificgroup of hallucinations and delusions, definedby Schneider, and referred to as first-rank symp-toms, which usually (but by no means exclu-sively) signify schizophrenia, may be relevant.He suggested that these may be signifiers oftemporal-lobe dysfunction, representing as theydo disturbances of language and symbolic rep-resentation. In this sense he equated them toa Babinski sign for a neurologist, pointing toa location and lateralization of an abnormal-ity in the CNS. These laterality findings havereceived support from brain-imaging studies.Using PET and oxygen-15, Trimble and col-leagues (Trimble, 1986a) have reported data onpatients with complex partial seizures, compar-ing a psychotic with a nonpsychotic subgroup.Generally, psychotic patients showed lower val-ues for oxygen metabolism, but maximal differ-ences were seen in the left hemisphere, acrossthe entire temporal cortex. The majority of thissample had schizophrenia-like psychoses withSchneiderian symptoms.
Mellers (1998), using a verbal fluency activa-tion paradigm and HMPAO SPECT, comparedpatients with schizophrenia-like psychoses ofepilepsy with schizophrenia, epilepsy and nopsychoses. The psychotic epilepsy patientsshowed lower blood flow in the superior tem-poral gyrus during activation than the othertwo groups. Using MR spectroscopy, Maieret al. (2000) were able to compare hippocampal–
amygdala volumes and hippocampal N-acetylaspartate (NAA) levels in patients withtemporal-lobe epilepsy and schizophrenia-likepsychoses of epilepsy, temporal-lobe epilepsyand no psychoses, schizophrenia and noepilepsy, and matched normal controls. Thepsychotic patients showed significant left-sidedreduction of NAA; this was more pronouncedin the psychotic epilepsy group. Regionalvolume reductions were noted bilaterally in thisgroup, and in the left hippocampus–amygdalain the schizophrenic group.
Flugel et al. (2006) examined 20 psychoticand 20 nonpsychotic cases with temporal-lobeepilepsy using magnetization transfer imaging.They reported significant reductions of the mag-netization transfer ratio (an index of signal loss)in the left superior and middle temporal gyri inthe psychotic patients; this was unrelated to vol-ume changes, and best revealed in a subgroupwith no focal MRI lesions.
Summarizing these data, it appears thatseveral authors, using independent sam-ples and differing techniques, show a linkbetween dominant-hemisphere pathology inpatients with temporal-lobe epilepsy and aschizophrenia-like psychosis. It should be notedthat the emphasis is on Schneiderian symptoms,presentation being with positive symptoms,and lack of deterioration and negative features.
Antagonism and the Concept of ForcedNormalization
An earlier idea that schizophrenia and epilepsyhad an inverse relationship has caused confu-sion. Essentially, this antagonism, observationsof which led von Meduna to introduce convul-sive seizures as a therapy for schizophrenia,was between seizures and the symptoms ofpsychosis, rather than between epilepsy andschizophrenia (Wolf and Trimble, 1985).
Landolt (1958) recorded changes in the EEGduring preseizure dysphoric episodes and lim-ited periods of frank psychosis lasting days orweeks in epileptic patients. He noted improve-ment in EEG activity during such episodes andreferred to this as ‘Forced Normalization’. He

252 Biological Psychiatry
defined Forced Normalization thus: ‘the phe-nomenon characterized by the fact that, with therecurrence of psychotic states, the EEG becomesmore normal, or entirely normal, as comparedwith previous and subsequent EEG findings.’Forced Normalization was thus essentially anEEG phenomenon. He suggested that similarchanges could be provoked by anticonvulsantdrugs, and noted that, at the end of a psychoticepisode, the EEG returned to being abnormal.Although initially he discussed this in relation totemporal-lobe epilepsy, he later drew attentionto its occurrence with generalized epilepsies,in particular the precipitation of psychosis inpatients with generalized absence seizures byethosuximide. Although Forced Normalizationis generally associated with psychosis, variantforms include prepsychotic dysphorias, depres-sive, manic, hypochondriacal and twilight states(Wolf and Trimble, 1985). A preferred term isperhaps ‘paradoxical normalization’. Thus, as ageneral rule in epilpesy, if the behaviour deteri-orates, so does the EEG. However, in the case ofForced Normalization, the EEG improves butparadoxically the behaviour becomes worse.
The clinical counterpart of forced normaliza-tion is referred to as alternative psychosis, inwhich less attention is paid to EEG phenom-ena and more to the presence or absence ofseizures in association with the psychosis. Clin-ically, such states can be very problematic, sincecontrol of seizures leads to an even more dis-turbing and often difficult-to-control problem,namely the development of a psychosis. Thissometimes has a schizophrenia-like presenta-tion, but more often it appears as a paranoidor even manic psychosis. In lesser forms, theproblem may merely present as an exacerba-tion or precipitation of behavioural problemsas seizures remit. The disturbed behaviour maylast days or weeks. It is often terminated by aseizure, and the EEG abnormalities then return.
Mechanisms
There appears to be some association betweenthe development of an epileptic focus in oneor other temporal lobe, expressed around earlyadolescence, and the development of a later
psychiatric illness. The evidence implicates thedominant hemisphere in patients who developa schizophrenia-like psychosis with positivesymptoms, and suggests that in some patientsthere is an inverse relationship between theexpression of the seizures and the expressionof the psychosis. The latter is not only notedwith Forced Normalization, but is also seen inpatients with chronic psychosis, some of whomdevelop the psychosis as their seizure frequencydeclines. This holds for affective disorder (Flor-Henry, 1969) and for the schizophrenia-likeconditions (Slater and Beard, 1963).
Most authors have used EEG or functionalimaging to assess the side and site of theepileptic focus associated with psychopathol-ogy, which implies some disturbance of CNSfunction. This is supported by the inverserelationship to seizures and by the early obser-vations of authors such as Heath (1962) andKendrick and Gibbs (1957) of abnormal EEGdischarges from deep limbic sites in patientswho have psychosis, whether or not epilepsyis present. Heath, in work which is now barelyquoted, but is important as it is unlikely ever tobe repeated, emphasized the involvement of theseptal region (the area we would now call theaccumbens) in the development of psychosis,and showed that, while during interictal periodsepileptic patients show paroxysms of abnormalactivity, particularly in the hippocampus andamygdala, as psychosis becomes apparentthese spread to involve the septal region.Schizophrenic patients also show spiking andslow-wave activity, primarily in this area, butto a lesser extent in the hippocampus andamygdala. The spiking is relatively infrequentin schizophrenic patients, but in epilepticpsychosis there are dramatic high-amplitudespikes frequently associated with pronouncedslow-wave activity. Thus, although differenceswere noted in the electrical patterns, the sameanatomical regions are involved in psychosiswhether or not the patient has epilepsy.
There are two main contrasting hypothesesto explain the development of the psychoses ofepilepsy. The first, supported by the above, sug-gests that they are truly epileptic in origin andshould be referred to as ‘epileptic psychoses’.

Epilepsy 253
The second says that they are a manifesta-tion of organic neurological damage, and notspecifically of epilepsy. The former view hasbeen most strongly expressed by Flor-Henry(1969), supported by the observations of thelink between seizure frequency and psychosisand the depth-electrode data. Slater and Beard(1963) advocated the second hypothesis, notinga significant proportion of psychotic patientshad a defined organic basis for their epilepsy;a similar view was taken by Kristensen andSindrup (1978) and Bruton et al. (1994).
CT and MRI studies do not add furtherinformation. Thus, patients with epilepsy tendto show a high frequency of abnormalities,with or without psychosis. Toone et al. (1982a)and Conlon et al. (1990) reported a tendencytowards the reporting of more left-sidedstructural abnormalities in patients with schizo-phreniform psychosis of epilepsy, and halluci-nations were exclusively reported in those withleft-sided CT lesions. The studies with SPECT,PET and MRS quoted above lend furthersupport to the concept that the psychosesare associated with disturbed function asopposed to structure. In general, patients withlocalization-related epilepsies, in particulartemporal-lobe epilepsy, show hypometabolicareas at the site of the seizure focus, asdemonstrated on the EEG. However, the extentof the underlying pathology, assessed duringtemporal lobectomy, tends to be much smallerthan the zone of hypometabolism. This suggestsa widespread functional disturbance in the asso-ciated brain regions of such patients. Further,these hypometabolic areas become hyperme-tabolic during an ictus. They do not appear tobe dependent on seizure frequency, durationor clinical expression. In epileptic psychosis,these functional disturbances tend to be greater,and with schizophrenia-like presentations theyinvolve the left side more than the right.
Neuropathological data (Stevens, 1986)do not clarify the situation much further.Thus, a common finding in epilepsy is mesialtemporal sclerosis, with pyramidal cell loss inthe CA1 area of the hippocampus. Althoughmost common in patients with temporal-lobeepilepsy, this is also seen following status
epilepticus. It is suspected to be aetiological forpartial seizures with a temporal-lobe origin,but may also occur as a secondary consequenceof recurrent seizures. Mesial temporal sclerosishas been reported occasionally in brains fromschizophrenic patients who have never hadseizures, and in epilepsy is associated withpathology elsewhere, such as Purkinje cell lossin the cerebellum.
Patients with epilepsy and psychosisare reported to have gliosis and degenerativechanges in such areas as the pallidum, the brain-stem, the tegmentum and the periaqueduc-tal and periventricular regions of the basalforebrain, similar to the changes observed inpatients with schizophrenia (Bruton et al., 1994)(see Chapter 7).
Thus, mesial temporal sclerosis alone is insuf-ficient for the development of psychosis, andother areas, in particular periventricular andforebrain sites which receive projections fromthe amygdala and hippocampus, would seemimportant. Further evidence for this stems fromclinical observations that patients who have hadtemporal lobectomy sometimes develop psy-chosis postoperatively, which clearly implicatesother areas of the brain than the medial tempo-ral structures in the overall pathogenesis of thepsychoses (Trimble, 1991).
Symonds (1962) pointed to the ‘epileptic dis-order of function’. It was, he suggested, not theloss of neurones in the temporal lobe that wasresponsible for the psychosis, but the disorderlyactivity of those that remained. One possibilityis that chronic temporal-lobe ictal lesions lead tokindling of activity in other regions of the brain,especially forebrain limbic areas – changeswhich lead to the gradual development ofthe psychosis. Such a hypothesis fits with theintracerebral recording studies of Heath (1962),as well as observations that it is difficult tokindle epileptic seizures in certain parts of thelimbic system, particularly those that are cate-cholaminergic such as the dopamine-rich areasof the limbic forebrain. In such sites, kindledbehaviour changes rather than seizures are seen(Stevens and Livermore, 1978). The data of Ringet al. (1993) with IBZM binding (a D2 ligand) tobasal ganglia structures in psychotic epileptic

254 Biological Psychiatry
patients compared with controls are in supportof this hypothesis. These data are important forunderstanding the pathogenesis of schizophre-nia since the temporal-lobe-epilepsy modelof schizophrenia-like psychosis is one for the‘positive symptoms’ of psychosis, and drawsattention to the medial temporal lobes andforebrain limbic system in the development ofsome schizophrenic symptomatology.
COGNITIVE DETERIORATIONAND EPILEPSY
It has long been recognized that some patientswith epilepsy undergo dilapidation of theirintellect, in particular showing disturbancesof memory, which later may progress tointellectual deterioration and dementia. Insome cases this may be related to a progressiveencephalopathy. It may reflect an underlyingneuropathology, such as a lipid storage disor-der, which leads to both seizures and intellectualdeterioration. Examples of epileptic syndromessuch as West’s syndrome have been notedalready. Alternatively, recurrent head injuries,bouts of anoxia and intracranial bleeds may overtime lead to deterioration. Some dementias,such as Alzheimer’s disease, are associated withseizures, and links between Down’s syndrome,early dementia and seizures are noted (Brown,2004). Autism and autistic-spectrum disorderssuch as Asperger’s syndrome are associatedwith a later development of seizures in about25% of cases, comorbidity depending upon theage and type of disorder. Major risk factorsfor seizure occurrence are learning disabilityand additional neurological disorders. Autismwith regression has been reported in one-thirdof children with previously normal or nearly-normal development. Epilepsy may be present,resulting in so-called autistic epileptiformregression (Canitano, 2007).
Attention has been drawn to anticonvulsant-induced encephalopathies, sometimes seenwith phenytoin and sodium valproate, in thelatter being associated with hyperammone-mia. Diagnosing an anticonvulsant-inducedencephalopathy can be difficult, since it may
produce a typical picture of dementia, some-times associated with focal neurological signsand dyskinesias, in association with a raisedCSF protein. Since this represents one possiblereversible cause of dementia, it should alwaysbe considered in patients with epilepsy who,for unclear reasons, are becoming cognitivelyimpaired.
Most studies of non-institutionalized epilep-tic patients show a near-normal distribution ofthe IQ, with skewing at the lower end of thescale. On formal testing, people with epilepsyoften show memory disturbances, particularlyfor more recent events, and there is some evi-dence of a laterality effect, patients with left-sided foci having memory deficits for verbalmaterial and right-sided lesions for nonverbalmaterial. Other selective deficits include impair-ment of attention, poor perceptuomotor scores,deficient arithmetical and reading ability, and ageneralized slowing of cognitive processes. Ref-erences to the latter have long been noted, andhave been described as viscosity and stickinessof thought, referring to the prolonged speed ofcerebration noted in some patients with epilepsy(Trimble and Thompson, 1985).
Factors influencing cognitive performance inepilepsy include length of seizure history, pres-ence of hippocampal sclerosis, an early age ofonset of seizures, an increasing frequency ofseizures and associated neuropsychiatric hand-icaps such as depressive illness (Jokeit andEbner, 2004). With regard to seizure types,generalized absence seizures seem less dam-aging than generalized tonic–clonic seizures,and patients with partial seizures seem morelikely to show impairments of memory function.Patients with frontal epilepsies reveal deficitson testing frontal executive functions (Helm-staedter, 2004).
The more subtle adverse effects of anti-convulsant drugs on neuropsychologicalabilities have become appreciated (Trim-ble and Reynolds, 1984). Phenobarbitone,phenytoin and more recently topiramate havebeen most implicated, and carbamazepinethe least. Topiramate seems to produce inaround 7% of patients a reversible aphasia-likesyndrome, associated with left-sided onset

Epilepsy 255
of seizures (Mula et al., 2003). Polytherapyitself, particularly with older anticonvulsants,would appear detrimental, and significantimprovements in both cognitive performanceand affective symptoms can be brought aboutin patients by rationalizing polytherapy, or bysubstituting patients on polytherapy with moresedative compounds such as carbamazepine asmonotherapy (Thompson and Trimble, 1982a).
SOME OUTSTANDING ISSUES
The last 30 years have seen a sea change withregards to the acceptance that epilepsy andpsychopathology can be closely biologicallylinked. This has been due in part to a shift inneurological thinking, many neurologists nowaccepting that there is a neuroanatomy of emo-tion, and that the limbic circuitry is involvedin many neurological disorders. Temporal-lobe epilepsy remains a paradigm. Further,as special epilepsy centres and clinics havedeveloped, the behavioural syndromes ofepilepsy have not only become more apparentto treating physicians, but have been the subjectof much more scientifically-based research. Theneuroanatomy outlined in Chapters 2 and 3has also opened up the underlying mechanismswhereby such behavioural changes arise; thecircuitry is clear, especially with regards tolimbic-based syndromes.
Better definitions of some of the epilepsy-related behavioural syndromes are required.The characteristics, frequency and comorbidi-ties of the IDD are unclear, as is its relationshipto atypical depressions and bipolar disorder.This has very important implications. Thus, it isknown that many patients with bipolar disorderin the absence of epilepsy respond to antiepilep-tic medications (see Chapter 12), although this isnot a class effect, and is limited mainly to carba-mazepine, sodium valproate and lamotrigine. Infact, antiepileptic drugs that are GABA agonistsare likely to provoke or maintain depressivesymptoms and not be mood-stabilizing. Onepossibility is that the non-epilepsy mood-disordered patients respond because theyhave atypical bipolar disorders – for which
there is some evidence – and that the effect ofthe antiepileptic drugs has to do with theirinfluence at limbic structures. Carbamazepine,sodium valproate and lamotrigine all have aneffect on the amygdala, are central in regulatingmood and are involved in the neurobiology ofmany epilepsy syndromes.
The relationship between the interictal psy-choses of epilepsy and schizophrenia have beenpartially sorted out, but more work is needed toexamine neurobiological similarities and differ-ences in greater detail. The underlying pathol-ogy is different, an absence of gliosis in thehippocampus and related structures character-izing schizophrenia. Thus, the site of the pathol-ogy, the timing of the lesions developmentally,and the consequent functional changes in thebrain may all be crucial to the later develop-ment of any behaviour changes in both epilepsyand schizophrenia.
The recent evidence then, especially frombrain-imaging studies, suggests that Slater’soriginal hypothesis regarding the structuralbasis for the syndromes was part right but partwrong. The interictal psychoses seem differentfrom schizophrenia, especially with regards tothe admixture with affective symptoms andthe long-term social prognosis, which is better.While hippocampal changes may relate toboth disorders, the increased amygdala size –bilateral and around 17–20% – and the lesservolumetric changes in the hippocampus inthe epileptic psychoses suggest the two psy-chopathological states are biologically quitedifferent. While the laterality findings withregards to the functioning of the left hemisphereseem to hold up, the data point away fromfundamentally cortical abnormalities in thesepsychoses, and show the amygdala and relatedstructures to be central in pathogenesis.
This raises questions as to the relationship ofthe schizophrenia-like syndromes of epilepsy todisturbances of affect, and the way the conceptof the IDD fits into this scheme, since Blumerconsiders a spectrum of IDD which includespsychotic presentations. However, these clini-cal and pathological differences perhaps reflecton the prognosis of the various disorders, andshould be telling us something about the role

256 Biological Psychiatry
of the amygdala vis-a-vis the hippocampus inpsychotic states.
The phenomenon of Forced Normalization isstill held in doubt by a number of physicians, inspite of considerable evidence for its occurrenceclinically and a neurobiological explanation,namely switching off the cortical expression ofthe EEG and diverting electrochemical forcesthrough limbic–limbic forebrain structures. Itis certainly found less often than made outby Landolt, and specific studies are few andfar between. It is difficult to document casesprecisely, EEG recordings being difficult toobtain at the right times. However, studieswhich systematically analyse the aetiologyin consecutive case series identify ForcedNormalization or alternative psychoses asaccounting for about 10% of psychotic cases(Schmitz et al., 1999). The importance of thecondition cannot be overemphasized, eitherclinically or theoretically. The concept bringspsychiatry uncomfortably close to neurologyfor some people, revealing a close biologicallink between seizures and psychosis. It alsoaffects treatment. Thus, if, in some patients,suppression of seizures provokes psychopathol-ogy, it reinforces the fact, often ignored ormisunderstood, that seizures and epilepsy arenot synonymous, and that an understandingof the epileptic process and its treatment goesfar beyond the control of seizures. In clinicalpractice, to ignore the fact that some patientsmanifest these problems as their seizures come
under control can lead to the continuationof severe behaviour disturbances, with all ofthe social disruption that then emerges, and afailure to manage the epilepsy appropriately.
The term ‘dementia of epilepsy’ is alsocontroversial. It is clear that some syndromes(such as ESES) reveal a direct relationshipbetween seizures and a dementia syndrome,perhaps reversible. But the controversy wasover whether or not a slow cognitive declineoccurred due to the direct effect of seizuresdamaging neurones. This seems accepted, withthe understanding of the toxic effects of calciuminflux with excess neuronal excitability, andclinical evidence of cognitive decline over thelong term in some patients.
Finally, the Gastaut–Geschwind syndromehas been much debated. However, the conceptthat an organic brain syndrome secondary toa temporal-lobe/limbic disorder of functioncould manifest has to be seen alongside theready acceptance of the Kluver–Bucy syn-drome and a raft of frontal-lobe behaviouralsyndromes. The presence of such featuresas hyperreligiosity and hypergraphia, deepfeelings of personal destiny and epiphanicexperiences leads the interested to the bor-derlands of brain–behaviour relationships,and touches on fundamental neuroscienceissues that are coming to the forefront ofresearch, namely neuroaesthetics, neurotheol-ogy and the neurology of human consciousness(Trimble, 2007b).

11The Dementias
INTRODUCTION
Progress in our understanding of the neuro-pathological and neurochemical bases of thedementias has been substantial in the last twodecades. New forms of dementia have been dis-covered, and the fundamental molecular biol-ogy, especially with regards to tau and amyloidprotein, has been valuable in directing potentialdiagnostic methods and interventions.
DEFINITION
Dementia refers to a syndrome. Over the years,many authors have attempted definitions, andmost agree on the following characteristics: itis acquired and chronic, thus distinguishing itfrom learning disability and acute organic brainsyndromes, and in most cases it is irreversible,being secondary to structural changes in thebrain. Further, it is distinguished by a decline inintellectual capabilities, in addition to changesin other areas of behaviour, notably emotionaland motor. The emphasis is on social declineand failure to cope with an independent life.
Lishman (1987) defined dementia as ‘anacquired global impairment of intellect, mem-ory and personality but without impairment ofconsciousness’ (p. 6).
Cummings and Benson (1992) refer to ‘anacquired persistent impairment of intellectualfunction with compromise in at least three of thefollowing spheres of mental activity; language,
Biological Psychiatry 3e Michael R. Trimble and Mark S. George 2010 John Wiley & Sons, Ltd
memory, visuospatial skills, emotion or per-sonality, and cognition (abstraction, calculation,judgement, etc.)’ (p. 1).
ICD 10 refers to dementia as a syndrome‘due to disease of the brain, usually of a chronicor progressive nature, in which there is dis-turbance of multiple higher cortical functions,including memory, thinking, orientation, com-prehension, calculation, learning capacity,language and judgement. Consciousness is notclouded’ (p. 45). ICD and DSM IV-TR bothsubclassify according to type (dementia inAlzheimer’s disease, etc.).
DSM IV-TR notes the essential feature ofdementia to be the development of multiplecognitive deficits, which include memoryimpairment and at least one of aphasia, apraxia,agnosia or a disturbance in executive function-ing. These deficits must be severe enough toimpair occupational or social functioning. ButCummings and Benson (1992) consider this toorestrictive: it excludes patients in early phasesof dementia who still function well, it failsto include dementias such as Pick’s diseasewhere memory disturbances appear late and itdoes not include the dementias associated withpsychiatric illness.
One feature of the various definitions is theirdescriptive nature, the concept being, initiallyat any rate, clinical. Another is the global natureof the impairments; this distinguishes dementiafrom persistent focal brain syndromes such asaphasias or amnesias. Although several of the

258 Biological Psychiatry
dementias present with signs of focal brain dam-age, their resulting incapacity is clearly muchmore extensive than purely focal dysfunctionwould allow.
PREVALENCE
Most agree that dementia is posing one of themost rapidly increasing medical problems in theWestern world. This is on account of the risingage of the population, the tendency towards anuclear family structure, leaving many elderlypeople without the support of the extendedfamily, and an increased awareness of diagnosis.
Prevalence rates rise with age, some 6% ofthe population over 65 being affected (Kay et al.,1970), essentially doubling with every five-yearincrease of age over 65. Over 75 the preva-lence increases rapidly, to around 40% by theage of 95. In geriatric units, over one-third ofpatients show evidence of mental impairment,and many in retirement communities and res-idential homes are affected. The prevalence ishigher in women than in men, except in thosewith younger onset, when this is reversed. Theincidence rate is variously estimated at around0.5–7.0% per annum, again dependent on age.
Although the majority of cases, between 22and 60%, are diagnosed as Alzheimer’s dis-ease (Cummings and Benson, 1992), these esti-mates are invariably made on selected referralpatients, the diagnosis being clinical and rarelysupported by post-mortem confirmation. Thesecond most common diagnosis is multi-infarctdementia (MID), accounting for around 10% ofcases. However, the growing recognition andimportance clinically of dementia syndromessuch as fronto-temporal dementia and dementiawith Lewy bodies, along with increased clinicalacumen, is altering these earlier estimates.
DIAGNOSIS AND CLASSIFICATION
Not all dementias show the same presentation,and one of the advances in recent years hasbeen in the identification of different subtypes,based on clinical presentation, which appears toconform to underlying pathological processes.
In the classical picture, memory disorder is theinitial complaint, especially for new events. Thisemerges gradually, although the family mayreport a dramatic behavioural event early onin the condition which signalled to them thatsomething was wrong with their relative. Overtime, other features of intellectual impairmentbecome apparent, including a lack of spontane-ity, concrete thinking and an impairment ofabstract reasoning. Disorientation is a frequentearly cognitive sign, patients easily losing theirway, often in familiar surroundings.
As the disorder progresses, thought disordermay emerge, with delusions, often of persecu-tion, and illusions or hallucinations, usually of afleeting nature. Ultimately patients may becomefloridly psychotic.
Affective symptoms are present early inmany cases, with lability of affect, tearfulness,withdrawal and frank depressive symptoms.In some presentations, distinction from majoraffective disorder may be difficult (see below).Hypochondriacal complaints, often with bizarrepresentations, may arise.
Focal symptoms such as aphasia or apraxiaare common, and as the disorder progressesabnormal neurological signs may appear. Motorsigns, in particular Parkinsonism, can lead toa poverty of facial expression and posturaldisorders, and add to the slowness of movementand impaired ability to act. The development ofParkinsonism (suggestive of either Parkinson’sdisease with dementia or Lewy-body demen-tia), or of lateralizing signs (suggestive ofcerebrovascular or fronto-temporal dementia),assumes clinical importance. Premorbid per-sonality traits are exaggerated, irritability andaggression common, but the focal deficits maygive rise to a more clearly defined change ofpersonality, for example frontal-lobe pathologyleading to disinhibition and perseveration.As time progresses, apathy, personal neglectand vacuousness come to dominate theclinical picture.
Identification of dementia in its early stagescan be difficult. Often the patient is well sup-ported by a relative, who, while noting thefailing powers of their companion, will coverup for any deficits. The loss of such support, for

The Dementias 259
example with the death of a spouse, may leadto a crisis, but by this time the disorder is welladvanced.
It is clear that in the diagnosis of demen-tia, especially in the early stages, the witnessaccount of a third party, especially one whoknows the patient well, is essential. A full men-tal status and neurological evaluation are thenfollowed by a series of special investigations.These include specialized neuropsychometry,with assessment of both the premorbid and thecurrent level of functioning, skull and chestX-ray, and now MRI scanning, EEG investiga-tions and, where necessary, more specializedtechniques such as SPECT, PET or angiography.Laboratory investigations include haematologyand electrolytes, B12 and folate levels, serology,thyroid-, liver- and renal-function tests, and anESR. CSF is becoming of value, usually showingelevation of proteins, but also biological mark-ers. Examination of the CSF will help excludean inflammatory process.
The above introduction is a starting point,from the clinical point of view, for detecting thedevelopment of a dementia. Unlike in the otherchapters of this book, diagnostic entities willhere be discussed separately, as it has becomeclear that clinical, pathological and in some casesmolecular biological differences can be made.Soon it may be possible to classify the dementiaswithin a genetic, molecular and neuroanatom-ical biological framework, which will overrideclinical considerations.
ALZHEIMER’S DISEASE
This is the most commonly diagnosed of thedementias. Described in 1907 by Alzheimer, itis now used by many to refer to a demen-tia which is not confined to any particular agegroup but increases in incidence with age. It isoften referred to as dementia of the Alzheimertype (DAT). In life, the diagnosis is still madeby exclusion, there being as yet no confirmatorytest, although with brain imaging and biologi-cal markers case identification is more certain(see below).
Familial cases have been described suggest-ing an autosomal dominant inheritance, and
there are several reports of identical twinswith the disorder, confirmed histologically(Kilpatrick et al., 1983). In such reports thecases usually present in the presenile period(under 65). There tends to be an increase incases among relatives of probands, especiallywith a presenile onset, and, further, relativeshave an excess of Down’s syndrome, lymphomaand immune-system disorders (for examplerheumatoid arthritis, lupus erythematosus)compared to that expected from a control group(Heston et al., 1981). The link with Down’ssyndrome is the more interesting in that it isnow established that, if patients with the tri-somy 21 survive long enough, they will almostcertainly develop a dementia, the pathologicalfeatures of which are typical for Alzheimer’sdisease. Mosaicism for trisomy 21 can presentwith no or minimal manifestations of Down’ssyndrome, and it may be an underdiagnosedcause of early-onset Alzheimer’s disease.
Studies of the molecular genetics ofAlzheimer’s disease have, to date, revealedseveral candidate genes linked with the rarerearly-onset familial disorder. These are thosefor the amyloid-beta precursor protein (APP),presenilin-1 (chromosome 14) and presenilin-2.The latter two form the catalytic core in gamma-secretase complexes, and mutations lead toabnormal formation of APP and to an accu-mulation of the beta-amyloid in the brain (seeFigure 11.1). However, these account for lessthan 5% of all Alzheimer’s disease cases. Suscep-tibility genes associated with the sporadic formsof the disease include apolipoprotein E (Apo E)alleles, which are associated with late-onset andfamilial Alzheimer’s disease. The genes for ApoE are localized to chromosome 19, and Apo E isfound in plaques, tangles and amyloid deposits.Intracellularly it is thought to stabilize tauprotein, which binds perihelical filaments, andhence stabilizes minitubules (see below). Thereare three alleles: Apo E 2, 3 and 4. The latter ispresent in about 15–20% of the population, butthe E4–E4 genotype occurs in about 1%, and in40% of patients with Alzheimer’s disease. Thus,homozygosity for Apo E E4 leads to an eightfoldrisk for the disease, and most homozygoteswill develop Alzheimer’s disease before the age

260 Biological Psychiatry
APPI
II
III
IV
NEXTRACELLULAR
SECRETASES
SECRETASES
N
671
Normal cleavage sequence
Abnormal cleavage sequence in Alzheimer’s disease
N
a-secretase(i)
(ii)
(i)
(ii)
g -secretase
b-secretase
b-AMYLOID 42-43 amino acids
g-secretase
Soluble APP
Soluble APP
672
687 688
712 713
714 715713
688
751/770
751/770
672
672
671 751/770
751/770
687 688 712 713 714
CYTOPLASM
695, 751 or 770amino acids
C
Membraneb-amyloidsequence(Ab4)
b a g
b a g
(or 692 - 693)
Figure 11.1 Schematic representation of possible cleavage sites of APP by secretases leading to the productionof beta-amyloid protein. Section I shows APP molecules in aminoacid chain lengths (695, 751 or 770); muchis extracellular. Section II is an enlargement of the beta-amyloid sequence. Section III shows the cleavage,normally of APP, by alpha-secretase releasing extracellular APP. The remaining molecule is broken downby gamma-secretase, yielding two short proteins that are broken down. In Section IV beta- rather thanalpha-secretase splits off the extracellular APP to leave insoluble beta-amyloid (Webster et al., 2002, p. 390)
of 80. Several other genetic associations havebeen reported but not confirmed.
Although it may present in the fourth decade,the disease typically comes on later, and is morecommon in women. It progresses slowly over
5 to 10 years, with early signs of amnesia andlack of spontaneity. The course is steady, withthe emergence of additional intellectual deficits,and finally extrapyramidal signs, seizures andadvanced dementia. Focal neuropsychological

The Dementias 261
disorders are prominent, and the presentationwith aphasia or disorientation is seen. Depres-sive symptoms, irritability and aggression maybe early signs, and slight infections or cen-trally active medications may provoke an acuteorganic brain syndrome.
The memory disturbance in Alzheimer’sdisease has been studied in detail by Kopelman(1985). He compared this condition toKorsakoff’s psychosis and normal controlson a battery of memory tasks, and providedevidence that in the dementia, primary (short-term) memory was impaired, and there wasalso an increase in the rate of forgetting. Sec-ondary (long-term) memory was also impaired,Alzheimer’s patients showing a higher rate offalse-positive errors. However, like Korsakoff’spatients, those with the dementia, if allowed,could acquire memory by prolonged exposureto the stimulus material. Thus the Alzheimer’s-disease patients showed defects in both memorysystems: notably primary memory capacity andretention, and secondary memory acquisition.Tests of working memory (such as digit span)are retained, at least early on. One interpretationgiven by Kopelman was that these data supportthe clinical impression that the forgetfulnessof these patients is due to a failure to takein information. Delayed memory recall is themost sensitive measure of the disorder, butwith progression, semantic memory declines.Further, the existence of these multiple memorydeficits may explain the failure of cholinergicreplacement therapy, which primarily acts onsecondary memory systems. The retrogradeamnesia with loss of memory for faces andevents from the distant past that patientsdevelop remains unaccounted for.
Language disturbances are almost universal.Anomia is the commonest impairment, fol-lowed by comprehension difficulties. Speechis characterized by being fluent but irrelevant,with a high incidence of semantic jargon(Appell et al., 1982). A consistent relationshiphas been reported between the impairment oflanguage and the severity of the dementia, butnot to duration of symptoms (Cummings et al.,1985). The pattern of the aphasia resemblestranscortical sensory aphasia, albeit usually
with a diminished output, being fluent andparaphasic, and with the ability to repeatremaining intact. In the later stages of theillness, echolalia, palilalia and verbigerationmay occur, and finally mutism.
The personality in Alzheimer’s diseaseremains relatively preserved in the early phasesof the illness, and patients may retain socialgraces, in spite of severe impairments. Thismay be quite deceptive, the patient makinggood cognitive deficits by employing politereplies to questions and avoiding further inter-rogation. Sim (1979) outlined some of theearly behavioural patterns seen in Alzheimer’sdisease in response to questions. These were:(a) perseverative movements, such as snappingof the fingers, indicating the answer to aquestion is on the tip of the patient’s tongue;(b) the offering of entirely irrelevant answers;(c) simply smiling in response to a question inthe hope that an alternative, less demandingone will be asked; (d) a display of anger, ora reply such as ‘I’m not a child to be askedthese silly questions’; (e) tearfulness; (f) a fullcatastrophic reaction, patients acting violently,with anger or tearfulness.
Wells (1979) noted such features as over-expression of satisfaction with trivial achieve-ments, the increased reference to diaries andcalendars for everyday events, and the aban-donment of interest in hobbies and other topics,patients noting that this is so that others, forexample the younger generation, can keep upwith them. Gradually changes become obvious,and in the later stages features of frontal- ortemporal-lobe disease appear. Fragments of theKluver–Bucy syndrome may be recognized.
The EEG is invariably abnormal, with reduc-tion of alpha rhythm, and later rhythmical thetaand delta discharges – particularly over frontaland temporal regions – or diffuse slowing beingrecorded. There is some correlation between thedegree of the dementia and the degree of slow-ing of the background rhythms. Of importanceis the observation that, except in some condi-tions such as fronto-temporal dementia, the EEGtends to deteriorate over time in most formsof dementia. The investigation is thus essen-tial for assessing difficult cases with regards to

262 Biological Psychiatry
clarifying diagnosis over time, and may givean impression of the rate of the progression ofthe disease (Gordon, 1968). There are severalreports that the P300 of the evoked potentialshows increased latency and diminished ampli-tude, greater than that seen in aging (St Clairet al., 1985), although to date no diagnosticallyspecific findings have been noted.
The CT or MRI scan usually, but not always,reveals enlarged ventricles and enlarged corticalsulci. Nonetheless, like the EEG, the CT or MRIscan is an essential technique in investigatingthe disorder. First, it will reliably rule out manyother causes of dementia (see below), some ofwhich are potentially reversible. Second, it is ofhelp in assessing the course of the condition indifficult-to-diagnose or established cases. Third,a normal scan in the presence of severe dementiashould alert the physician to the possibility thatthe problem is a pseudodementia (apparently adementia but actually a severe depression), stillone of the commonest causes of a misdiagnosisof dementia.
Generally, brain atrophy as shown on the CTor MRI scan tends to correlate with the degreeof dementia, although using planimetric mea-surements considerable overlap is seen whencomparing patients with Alzheimer’s diseaseand age-matched controls (Jacoby and Levy,1980a), and correlations to cognitive tasks vary.Dementia associated with more severe atrophyhas a poorer prognosis (Fox et al., 1975), espe-cially with marked parietal atrophy (Jacoby andLevy, 1980a). The latter is in keeping with theclinical data, implying a shorter survival in thosewith low scores on parietal tests (McDonald,1969) and lower attenuation densities in theright parietal region (Naguib and Levy, 1982).
MRI studies have shown smaller cortical vol-umes and larger ventricular size. Hippocampalloss of volume on MRI is particularly impor-tant (although not specific, being seen also inLewy-body dementia and some cases of fronto-temporal dementia), and the finding of mesialtemporal atrophy predicts those high-risk peo-ple with mild cognitive impairment (see below)who convert to Alzheimer’s disease (Figure 11.2)(Korf et al., 2004; Scher et al., 2007). More recentMRI methods segment grey matter, white matter
and CSF, allowing for quantification of brainatrophy, calculating the boundary shift in brainstructures on repeated scanning.
CBF and PET have also yielded interestingdata. Mean-hemisphere CBF is decreased withincreasing cognitive deterioration, especiallygrey-matter flow. Further, some correlationsto cognitive tasks have been detected, withdecreased temporal CBF with impaired memoryscores, and a reduction in occipito-parieto-temporal areas with verbal and symboliclanguage defects. In addition, a positive correla-tion between rCBF reduction in the postcentralareas and increasing EEG abnormalities hasbeen shown in patients with post-mortemhistological confirmation of their diagnosis(Johannesson et al., 1977). In Alzheimer’sdisease, SPECT abnormalities are maximal inthe postcentral region, predominantly in thearea of the parietal lobes.
The PET studies confirm the decreasedCBF, but also note low oxygen and glucoseuptake. In general they confirm that the extentof the abnormalities reflects the degree ofthe dementia (Frackowiak et al., 1981), and inAlzheimer’s disease reveal early abnormalitiesin the parieto-temporal regions and laterfrontal-lobe involvement, with relative preser-vation of metabolic activity in the primarymotor and sensory areas. Some groups are evenusing FDG PET as a disease marker, comparingan individual’s scan against a gender- andage-matched healthy database (a jack-knife orindividual-to-group comparison), looking forindividual reductions greater than one standarddeviation compared to the group, especially inthe parietal cortex (Small et al., 2000).
Recently it has become possible to visualizeamyloid with PET using tracers such as F-18FDDNP and C11PIB – called the Pittsburghcompound. It is possible to look at amyloid-betadeposition in the brain, although F-18 FDDNPvisualizes both beta-amyloid plaques andneurofibrillary tangles (see below). Correlationshave been shown between the binding of thelatter tracer and the degree of dementia (Kepeet al., 2006; Shoghi-Jadid et al., 2005).
Much interest has been generated by theneuropathological findings of Alzheimer’s

The Dementias 263
Alzheimer’s Disease FrontoTemporal Dementia Huntington’s Disease
Figure 11.2 Hallmark pathological changes seen in several of the dementias. On the top-left a transverseT1-weighted MRI scan shows the characteristic atrophy of the parietal cortex in a patient with Alzheimer’sdisease (arrow). Below that, a coronal MRI scan shows the hippocampal atrophy (arrow and outlined). In thecentre panel, in contrast, are images from a patient with fronto-temporal dementia showing the prominentfrontal atrophy (arrows on the transverse (top) and sagittal images (below)). The images on the right depict thecharacteristic atrophy of the caudate nucleus, with relative preservation of the rest of the brain in Huntington’schorea. The top-right image shows the caudate atrophy (arrow), with the bottom-right image showing thecaudate of a healthy control (fronto-temporal dementia courtesy of Dr Donna Roberts, MUSC; Alzheimer’sdisease from www.medscape.com; Huntington’s chorea from Ruocco et al., 2006)
disease. Macroscopically there may be atrophy,especially in the temporoparietal region,and histologically there is loss of neurones,proliferation of astrocytes and the presenceof senile plaques and neurofibrillary tangles.Granulovacuolar degeneration, in particular inthe hippocampal pyramidal cells, is also seen.Tangles appear as coils of parallel bundleswhich stain intensively with silver; on electronmicroscopy they are seen to be made up ofpaired helical filaments. The tangle is composedof hyperphosphorylated tau protein, whichderives from microtubles. The latter normallyare both a transport system and provide struc-tural support for the neurone, but in Alzheimer’s
disease the tau protein is abnormally phos-phorylated and less soluble. It becomes unableto bind to microtubules, presumably alteringmicrotubule structure. Alzheimer’s disease isthus one of the tauopathies, others being shownin Table 11.1.
The plaques are degenerating nerve termi-nals, astrocytes and microglia with an amyloidcentre. Amyloid is seen as playing a central rolein the pathology of Alzheimer’s disease. Beta-amyloid is a protein of 39–43 amino acids, and isa fragment of the larger precursor protein APP.The latter is cleaved by beta and gamma secre-tases, but is also actually prevented from this byalpha secretase. It is an insoluble 40/42 amino

264 Biological Psychiatry
Table 11.1 The tauopathies
1. Alzheimer’sdisease
2. Sporadic Progressive supranuclear palsyCorticobasal degenerationPick’s diseaseNeurofibrillary form of senile
dementia3. Familial
acid, and accumulates in plaques and cerebralblood vessels (amyloid angiopathy).
Tau protein is involved in the polymerizationon neurotubules and tau accumulates in theneurones in several disorders, referred to col-lectively as the tau-opathies. Abnormal tau isfound in neurofibrillary tangles, in Pick bodies,and can also be identified in astrocytes insome conditions. Microtubules are stabilizedby tau–tubulin interactions. In Alzheimer’sdisease, tau pathology is most likely secondary;the proximate cause is unknown. However,amyloid-beta protein precursor is somehowinvolved.
There is some relationship between the site ofpathology and clinical presentation. Forstl et al.(1994) reported that misidentifications (e.g. Cap-gras phenomena) were associated with lowerneurone counts in the CA1 region of the hip-pocampus, but delusions and hallucinationswere found in those patients with less cell lossin the parahippocampal gyrus and more in theraphe nucleus.
The tangles are in the cell body, usually closeto the axon hillock, and the plaques are oftenlocated near to blood vessels. This situation ofthe tangles may lead them to block the nor-mal movement of the macromolecules from theneurones to the terminal.
These changes are maximal in the cortex,especially in the temporo-parieto-ocipital regionand in limbic-related cortex, hippocampus andamygdala, but also occur in some brainstemnuclei such as the locus coeruleus. Most tan-gles are seen in the entorhinal cortex, and theamygdala is also affected (lateral but not centro-medial nuclei), but primary sensory corticesare least affected. The earliest site of tangle
formation is in the entorhinal cortex and CA1hippocampus, and a staging system of the pro-gression of the disorder has been developed byBraak and Braak (Braak and Braak, 1997; Braaket al., 1994a, 1994b). Plaques in noncortical struc-tures are most numerous in the mammillarybodies
Although plaques and tangles are an essentialfeature of the pathology of Alzheimer’s disease,they are not exclusive to that condition. Tanglesare found, albeit in smaller numbers, in associa-tion with normal aging, and with such patholo-gies as dementia pugilistica, postencephaliticParkinson’s disease, progressive supranuclearpalsy (the Steele–Richardson syndrome), sub-acute sclerosing panencephalitis and Down’ssyndrome. This raises the question as to whetheror not they represent some nonspecific responseto a variety of insults. Plaques, too, havebeen seen in Down’s syndrome, Creutzfeldt–Jakob disease and with lead encephalopathy(Cummings and Benson, 1992).
What is unclear at present is the relationshipbetween the findings that relate to Apo E E4, tauprotein and the development of amyloid abnor-malities, tangles and plaques. The E4 allele is anormal polymorphism in the population whichconfers increased risk of Alzheimer’s disease,but it is possible that the Apo E2 allele con-fers protection. The relationship may involveenhanced aggregation or decreased clearanceof amyloid-beta peptides, since Apo E enhancesthe proteolytic clearance of soluble beta-amyloidfrom the brain, and this ability is dependentupon the Apo E isoform.
The other line of pathological research hasbeen the discovery of the neurochemical defectsin Alzheimer’s disease. The first to be definedwas an abnormality of cholinergic mechanisms.Thus, it is now known that in Alzheimer’sdisease there is a widespread loss of presy-naptic cholinergic activity, notably in the hip-pocampus, amygdala and neocortex (Bowenand Davison, 1986). The principal abnormalitydetected is a deficit of the synthesizing enzymecholine acetyl transferase, and a significant rela-tionship exists between the decline in activityand an increasing number of plaques (Perry andPerry, 1980). This contrasts with the presence

The Dementias 265
of normal muscarinic cholinergic (M1)-receptoractivity. It is thought that the loss reflects degen-eration of cholinergic neurones from the nucleusbasalis, the projections of which are widespread.These cortical cholinergic deficits are not foundin some other dementias, for example multi-infarct dementia or Huntington’s chorea, butdo occur in Creutzfeldt–Jakob disease and alco-holic dementia (Bowen and Davison, 1986).
Although some have suggested thatAlzheimer’s disease is a disorder of cholinergicinnervation (Coyle et al., 1983), several otherneurotransmitter deficits have now beendescribed (see Table 11.2). These includediminished noradrenergic and serotonergicinnervation to the cortex, with associated neu-ropathological findings in the locus coeruleusand raphe nuclei (Adolfsson et al., 1979; Mannet al., 1980). Low levels of GABA, dopamine(Adolfsson et al., 1979), dopamine beta hydro-lase (Cross et al., 1981), somatostatin (Francisand Bowen, 1985) and neurotensin withan increase in substance P (Perry and Perry,1982) have all been reported. A low uptake of5-HT by neocortical biopsy tissue has also beennoted (Benton et al., 1982), as has decreased5-HT4 receptor binding to frontal and temporalcortices (Cross et al., 1984). All these changesmay have relevance for the symptomatologyof the disease, and are relevant in terms ofdefining therapies. Not all neurotransmittersare reduced, however, and some peptidessuch as cholecystokinin and VIP seem normal(Rossor et al., 1980). NMDA binding is variablebut often normal.
Decreased glutamate terminals in cortical andhippocampal areas from Alzheimer’s-disease
Table 11.2 Summary of some neurotransmitter andreceptor changes in Alzheimer’s disease
Transmitter Receptor
Acetylcholine ↓ NNoradrenaline ↓ NDopamine ↓ N5-HT ↓ NGlutamate ↓ ↑Somatostatin ↓ ↓GABA ↓ ?
brains have been reported, suggesting dysfunc-tion of excitatory amino-acid-release pathwaysfrom neocortical neurones (Bowen and Davison,1986; Hardy et al., 1987). Such data implicate thecortex as a possible site of the primary pathol-ogy, loss of descending projections leading tosecondary changes in subcortical structures.
Bowen and colleagues argue that since cogni-tive decline can be related to reduced synthesisof acetylcholine and other monoamine abnor-malities have not been so clearly related to thecognitive changes, these latter changes are notthe primary neuropathological events in the dis-ease (Francis et al., 1985).
CSF studies in general have led to conflictingresults with regard to monoamine findings.However, the search for biomarkers has seena renewed interest in CSF data (see below). Onthe basis of genetic clinical and biochemicalfindings, several forms of Alzheimer’s diseaseare being defined. Rossor et al. (1984) examinedbrains of Alzheimer’s-disease patients and con-trols, and noted various changes in the former,including decreased choline acetyl transferase,GABA, noradrenaline and somatostatin levels.However, older patients, dying in their ninthand tenth decades, had a relatively purecholinergic deficit with additional decreases insomatostatin, reductions being confined to thetemporal cortex. There was no cholinergic lossin the frontal cortex. The younger patients hadmore widespread changes with regard to acetyl-choline and the other neurotransmitters. Rossoret al. suggested that Alzheimer’s disease in thoseunder 80 may be a distinct form. Bondareff et al.(1981) also provided data showing that neuronaldropout in the locus coeruleus characterizesa subgroup with a younger age, more severedisease and earlier death. Mahendra (1984) hasdeveloped the concept further. He suggests thatone type of Alzheimer’s dementia is character-ized by earlier onset, signs and symptoms ofparietal lobe and language disorders, and cor-tical and subcortical pathology. In the other, oflater onset, the pathology is restricted to subcor-tical sites, and the presence of the parietal-lobesigns is minimal. The genetic studies seem toprovide some support for these ideas. Some ofthe differences are shown in Table 11.3.

266 Biological Psychiatry
Table 11.3 Summary of some changes in Alzheimer’s disease and normal aging
Old age Alzheimer’s early onset Alzheimer’s late onset
Plaques in cortex + + + + ++Tangles in cortex – + + + ++CAT decrease ± + + + ++ (temporal)↓ cells in locus coeruleus + + + +↓ cells in nucleus basalis – + + + −Noradrenaline ↓ – ++ +GABA ↓ + + + + +5-HT ↓ + + + + +Somatostatin ↓ – ++ + (temporal only)Cholecystokinin − − −VIP − − −Genetics − 14,21 19 (chromosome number)Apo E E4 – ? +
–, no change; + through +++, significant change; CAT = choline acetyl transferase.
In spite of this growing knowledge of thepathology and chemistry of Alzheimer’s dis-ease, the aetiology remains obscure. The sug-gestion that it represents premature aging isnot compatible with the evidence from clinical,radiological and pathological comparisons ofelderly people and patients with dementia. Thepresence of plaques and tangles, and possiblebiochemical links between them, may suggest acommon genetic defect that leads to their for-mation, the consequent disruption of neuronalactivity then leading to the clinical picture. Oth-ers suggest that the plaques are due to degen-eration from their cells of origin in the nucleusbasalis, the latter being the crucial site of pathol-ogy. Rossor (1981) has proposed that the diseaseshould be conceptualized as a ‘disorder of theisodendritic core’. The ‘isodendritic core’ refersto the fact that cells of the locus coeruleus, sub-stantia nigra, substantia innominata and septalnuclei all share a generalized pattern of den-dritic spread, intermingling with other neuronalelements, thus forming a continuous isoden-dritic core from the spinal cord to the basalforebrain. This idea links Alzheimer’s diseaseand Parkinson’s disease, each of which repre-sents a different region of loss of the core, andmay explain the frequent presence of extrapyra-midal motor symptoms in Alzheimer’s diseaseand the high frequency of cognitive impairmentin Parkinson’s disease. While tangles are not aregular feature of the latter, profound losses ofneurones in the nucleus basalis are seen.
At one time, the cortical/subcortical locationof the pathology of the dementias led to the sug-gestion that there were two types of dementia,one primarily cortical, presenting with focal cor-tical signs such as aphasia and apraxia, and theother subcortical, with dilapidation of cognition,memory problems and slowing. This placedAlzheimer’s disease firmly with the corticaldementias. However, the pathological studieshave emphasized the subcortical basis for muchof the neurochemical change in Alzheimer’s dis-ease, and the dichotomy is no longer held tobe valid.
Pathogenic agents discussed have includedaluminium intoxication, immunological abnor-malities and slow viruses, although noconvincing data have supported such ideas.Certainly to date there are no substantialreports of transmission of a similar disease fromAlzheimer’s-disease brain tissue to animals,and the immunological abnormalities reportedmay well be secondary (Cummings andBenson, 1992).
Biomarkers
In the context of this section, ‘biomarkers’ refersto possible clinically-useful biological mark-ers of Alzheimer’s disease, as opposed to, forexample, genetic linkages. The latter conferrisk factors but not state markers. The idea isto better identify the disorder, especially with

The Dementias 267
treatment in mind, and possibly to monitorprogress. There are several candidates, and theyrelate to amyloid and tau. CSF beta-amyloid islow and total tau protein is high, the combina-tion having high sensitivity and specificity forAlzheimer’s disease. Either alone is less usefulsince although CSF amyloid-beta1– 42 differenti-ates Alzheimer’s disease from healthy controls,it is much less discriminating against some othertypes of dementia (Schipper, 2007, 2009). Theremay be some association of the combination toApo E E4 status.
DEMENTIA OF FRONTAL-LOBE TYPE
Pick described a form of dementia in 1892associated with a circumscribed atrophy of thefrontal and temporal lobes. Neary and col-leagues (1988) suggested that this was one formof a wider spectrum of dementing illness inwhich the primary pathology was frontal. Thesepatients present a clinical picture suggestiveof progressive frontal damage, an absence ofAlzheimer’s pathology and decreased frontal-lobe CBF with brain imaging. They have fewneurological signs. As a group, patients withdementia of frontal-lobe type are younger thanpatients with Alzheimer’s disease, and a fam-ily history of dementia is reported in 46%. Inthe familial variant with autosomal dominantinheritance, around 20% have mutations in theMAPT gene which encodes tau protein,
This is a clinical designation, not a patho-logical diagnosis. Clinical features are shownin Table 11.4. Pick’s disease itself is much lesscommon than Alzheimer’s disease. It is morecommon in females. Inheritance is said to bethrough a single autosomal dominant gene,although most cases are sporadic.
There are distinguishing features thatreflect the underlying pathology and separatefronto-temporal dementia from Alzheimer’sdisease (see Table 11.5). Thus abnormalities ofbehaviour, emotional changes and aphasia arefrequently the presenting features, as opposedto memory impairments. Some have notedelements of Kluver–Bucy syndrome at onestage or another of the disease (Cummings
Table 11.4 Clinical diagnostic features of fronto-temporal dementias (adapted from Brun et al., 1994)
Behaviour disorderAffective symptomsSpeech disorderSpatial orientation and praxis preserved
Physical signs:Early: incontinence, primitive reflexesLate: akinesia, rigidity
Investigations:EEG: normalImaging: predominantly fronto-temporal changeNeuropsychology: failure on frontal tests
Supportive features:Onset before 65 in 80%Positive family history 20% autosomal
dominant inheritanceBulbar palsy
and Benson, 1992). Interpersonal relationshipsdeteriorate, insight is lost, and the jocularityof frontal-lobe damage may even suggest amanic picture. The aphasia is reflected in word-finding difficulties, empty, flat, nonfluentspeech and paraphasias. With progression thecognitive changes become apparent, includingmemory deterioration, but several highercortical functions are intact – for example, apatient may continue to play bridge or evento work at a technical job. Cases are des-cribed of an output of creativity, such aspainting or poetry, and obsessions, hoarding,compulsive eating and unusual rituals maybe seen (Mendez and Shapira, 2008, 2009).Ultimately, extrapyramidal signs, incontinenceand widespread cognitive decline are seen.
The EEG tends to remain normal in fronto-temporal dementias, even when the behaviourchanges are advanced, and the CT or MRI mayprovide confirmatory evidence of lobar atro-phy (see Figure 11.2). Likewise, the PET pictureshows diminished metabolism in the frontaland temporal areas. Neuropsychological test-ing will reveal appropriate abnormalities onfrontal-executive tasks.
Pathologically, the brunt of the change infrontotemporal dementias is borne by the frontaland temporal lobes, and mainly takes the formof neurone loss with gliosis and spongiformchanges. In some cases there is predominant

268 Biological Psychiatry
Table 11.5 The differential diagnosis of dementia (from Trimble, 1981, p. 118)
Alzheimer’sdisease
Dementia offrontal type
Creutzfeldt–Jakob’disease
Arteriosclerotic Hydrocephalic
Early signs Memory Behaviourchange,aphasia,incontinence
Neurological signsand symptoms
Acute focaldeficit
Memory, psy-chomotorshowing,ataxia,incontinence
Focal deficits ++ + + ++ – –Orientation
difficultiesEarly Late – – –
Personalitychange
Late Early Early Late Early
Extrapyramidalsigns
+ – + + ±
CBF Posteriorhemisphere
Anteriorhemisphere
Multiple areas ofhypoperfusion
Multiple areasof hypoper-fusion
EEG Abnormal Often normal Always abnormal Abnormal AbnormalOther features ‘Mirror sign’ Hyperalgesia Myoclonus Pseudobulbar
signsVentricular
enlargement
–, no change; + through +++, significant change.
tau pathology, in others ubiquitin changes arein evidence, and in a third group there is nodistinguishing pathology. Mutation of the taugene has been identified in most familial caseswith tau pathology, although this is only theminority of cases with familial fronto-temporaldementia. Cases with tau-gene mutation canbe distinguished from typical Pick pathologywith the characteristic ‘balloon’ cell, which con-tains disorganized neurofilaments and neuro-tubules, and also the Pick bodies, which aresilver-staining and are also composed of neu-rofilaments, tau protein and tubules. The latterare particularly prominent in the mediotempo-ral and limbic frontal areas. Plaques and tanglesare not a feature of this disease, and the aetiologyis unknown.
FOCAL CORTICAL ATROPHIES
Pick’s disease is one of a number of focal atro-phies that lead to a dementia syndrome. Theclinical picture is related to the site and speed ofthe developing pathology. Semantic dementiais a subtype of fronto-temporal dementiawhich presents with predominant language
impairments, with the same demographicfeatures and MRI evidence of atrophy of the leftanterior temporal lobe. There is an anomia buta fluent aphasia, and often a reading difficultywith an inability to read words with irregularspellings (such as yaught). Progressive nonflu-ent aphasia is associated with left perisylvianatrophy. There is a variant associated withmotor-neurone disease, with bulbar palsy,weakness, wasting and muscular fasciculations.Corticobasal degeneration has cortical andbasal-ganglia pathology, with an associatedextrapyramidal syndrome; in some cases thecortical presentation may be mainly parietal.The pathology resembles Pick’s disease. Othervariants are with a posterior atrophy, but withAlzheimer-like pathological changes.
Progressive subcortical gliosis is a disorderwith a primarily frontal presentation and gliosisof frontal and subcortical structures.
DEMENTIA WITH LEWY BODIES
This is a syndrome of dementia with extrapyra-midal rigidity, associated with Lewy bodies asa pathological finding. Lewy bodies occur with

The Dementias 269
or without associated plaques or tangles. Theyare identified with alpha-synuclein antibodiesand are typically found in the substantia nigrain Parkinson’s disease, but in dementia withLewy bodies they are scattered throughout thecortex, especially in the parahippocampal gyrusand temporal, frontal and insular cortices. Theyare round hyaline bodies with a pale peripheralhalo, found in the cell cytoplasm. The presenta-tion of the dementia is often with hallucinationsor delusions, and it may be much more commonthan as yet diagnosed. The distinction betweenParkinson’s disease with dementia and demen-tia with Lewy bodies can be difficult, but thelatter has a far shorter history of Parkinsonismbefore the onset of the dementia. Other sugges-tive signs of dementia with Lewy bodies includethe presence of REM-sleep behaviour disorder,early autonomic dysfunction and sensitivity toneuroleptic drugs.
In comparison with Alzheimer’s disease,basal-ganglia imaging with ligands for thedopamine transporter (FP-CIT) will often beabnormal, while imaging of medial temporalstructures is normal.
VASCULAR DEMENTIAS
The concept of vascular dementia has under-gone significant changes in recent years,most notably with the recognition that chronicischaemic changes in the brain are rarely, if ever,responsible for dementia. It is now thoughtthat multiple cerebral infarctions are a commoncause of dementia, and that separation of thistype of deterioration from Alzheimer’s disease ispossible on clinical grounds and has therapeuticand prognostic relevance. However, ischaemicchanges are frequently found in association withAlzheimer’s disease or Lewy-body dementia,and may contribute to the clinical picture.
The vascular dementias comprise three maingroups: first, multi-infarct dementia (MID) asso-ciated predominantly with multiple corticalinfarcts; second, MID with mainly subcorticalinfarcts; and third, that type which affects whitematter diffusely, Binswagner’s disease. In realitythe first two types are frequently combined.
The pattern of the presentation relates tothe occurrence of multiple infarcts, their siteof extracranial origin and their location in theCNS. The most common cause is emboli fromthe extracranial arteries and the heart, and typi-cally the progression is of a stepwise dementia,often with a history of hypertension and evi-dence of recurrent strokes. On examination theremay be evidence of focal deficits in neurologicalfunction, and increased muscular tone, hyper-reflexia and Babinski responses may be found.A pseudobulbar state may be apparent, andemotional lability present. Unlike Alzheimer’sdisease, there is an equal sex preponderance.
The Hachinski score is now an acceptedmethod for helping establish a diagnosis, and isused widely in research (Hachinski et al., 1975).Application of this scale, the features of whichare shown in Table 11.6, leads to a score: theischaemia score. If over seven, the diagnosis ismore likely to be MID, while a score of underfour suggests parenchymatous dementia. Thereare criticisms of the method and the scale, espe-cially with regard to identification of early cases.Follow-up studies have been carried out whichsuggest that four features, namely abrupt onset,stepwise deterioration, focal neurological symp-toms and a history of hypertension, are the bestdiscriminators for MID.
In the cortical presentations of MID, thesigns and symptoms depend on the site of thelesions. The middle cerebral-artery territory ismost involved, leading to aphasias, apraxias,
Table 11.6 The Hachinski scale (from Hachinskiet al., 1975)
Abrupt onset 2Stepwise deterioration 1Fluctuation 2Nocturnal confusion 1Relative preservation of personality 1Depression 1Somatic complaints 1Emotional lability 1Hypertension 1History of stroke 2Focal symptoms 2Focal signs 2Other arteriosclerotic signs 1

270 Biological Psychiatry
visuospatial problems and other signs andsymptoms of cortical pathology. In contrast,the subcortical variant affects the basal ganglia,thalamus and internal capsule. It is usually theconsequence of infarction of tissue suppliedby the lenticulostriate arteries of the middlecerebral artery and other small perforatingvessels from the posterior communicating andposterior cerebral arteries.
The pattern of the disorder is progressive,with acute deterioration in the mental and cog-nitive state of the patient, followed by recovery.The latter is rarely to the state prior to the infarct,so a continuous but interrupted decline occurs.Patients often retain insight to their difficul-ties, and personality is quite preserved initially.Affective changes are common, and these mustbe distinguished from the lability of pseudob-ulbar palsy. Psychotic episodes with paranoiddelusions may be seen, and may be the onlyor initial sign of an infarct. Hypochondriacalcomplaints may be an early sign. The cogni-tive state is one of memory impairment, psy-chomotor slowing and general dilapidation ofperformance. As the condition advances, motorsymptoms are clear, including a Parkinsoniansyndrome.
The pathology in MID reveals areas of soften-ing and cavitation, and when these are multiplein the basal ganglia the condition is referred toas a lacunar state.
The EEG usually shows severe changes, andfocal slow activity is not uncommon. The CTand MRI scan reveal multiple infarcts, bilaterallydistributed, some of which may be seen in thebasal ganglia.
With PET, clearer differences betweenvascular and nonvascular cases have beennoted (Frackowiak et al., 1981). In contrast to thefronto-parietal distribution of Alzheimer’s dis-ease, MID showed more scattered areas of focalinfarction, although in mild dementia the pari-etal areas were involved in both groups. In gen-eral, a low frontal pattern was characteristic ofthe Alzheimer’s-disease group. Of importancewere the findings that changes in oxygen uptakein the MID patients were coupled to the CBF,the ratio of extracted oxygen (OER) remainingin the normal range. This demonstrates that
the pathology is not related to ischaemia wherethe OER increases, and raises doubts about thefeasibility of using agents that increase bloodflow in treatment. One possible consequenceof this finding is that episodes of hypotensionmay cause ischaemia in zones of decreasedperfusion.
‘Binswagner’s encephalopathy’ refers to aform of dementia of vascular aetiology withpredominantly white-matter changes. The cere-bral cortex appears well preserved, and patientshave a past history of hypertension. The presen-tation is of a slowly-developing dementia, oftenin the presenium, with a history compatiblewith multiple small strokes. Neurological signs,pseudobulbar lability and psychopathology areseen. The latter includes affective changes, para-noid delusions and hallucinations.
Pathologically there is loss of myelin andgliosis, and accompanying blood vessels arearteriosclerotic (Janota, 1981). The EEG isusually abnormal, with generalized slowingor focal changes, and the CT scan may revealdecreased white-matter attenuation. MRI showsincreased T2 signal from periventricular areasand associated white-matter hemisphere lesionsThe white-matter changes are reflected by lowoxygen uptake with a PET scan (Frackowiaket al., 1981).
‘Leucoaraiosis’ refers to small areas of white-matter change that can be seen on CT, or betterwith MRI, and are commonly visualized in theelderly. These may represent either increasedwater content of myelin without alteration offunction, or myelin loss, and thus their pres-ence has a poor correlation with cognition. Itis associated with hypertension, but may resultfrom hypoperfusion, and there is a genetic linkin some cases. Cerebral autosomal dominantarteriopathy with subcortical infarcts and leu-coencephalopathy (CADASIL) is related to amutation on chromosome 19 (notch-3 gene)which affects the smooth muscle of the wallsof affected cerebral blood vessels. It has a youngage of onset, with recurrent ischaemic attacts,and there is often a history of migraine. How-ever, there may be a history of psychiatricdisorder, especially depression, preceding theobvious vascular lesions by a number of years.

The Dementias 271
The causes of the vascular occlusionsresponsible for the vascular dementias arelegion (Cummings and Benson, 1992). Includedare haematological conditions, inflammatorydisorders and infections, and cardiac disease, allof which may lead to emboli, and the prominentrole of hypertension has been noted above.This is of utmost relevance for evaluation andtreatment. Thus, since vascular dementia is asecondary form of dementia, elicitation of anyunderlying pathology is of prime importance,especially if the condition is treatable in itsown right. This underlines the importance of afull and proper evaluation and investigation ofpatients with dementia. Ruling out cardiovas-cular disease, and especially hypertension, mayrequire specialized investigations and repeatedestimations of blood pressure. Rarer causessuch as systemic lupus erythematosus, giant cellarteritis, atrial myxomas and sarcoid should bethought of, as well as the commoner diabetes,and emboli from silent myocardial infarctionsand atrial fibrillation. While survival may relateto the underlying condition, it seems that it islonger in Alzheimer’s disease (5–10 years) thanin MID.
OTHER FORMS OF DEMENTIA
The primary dementias of Alzheimer and Pickcan be distinguished from dementia associatedwith other CNS conditions such as Huntington’schorea and Parkinson’s disease, and from thesecondary dementias such as those due to vas-cular (for example MID), infective (for examplesyphilis, AIDS), traumatic, metabolic, neoplas-tic and metabolic causes. In addition, one formof dementia, potentially reversible, is now clin-ically identifiable secondary to hydrocephalus.Some of these conditions are described here (seeTable 11.7).
Huntington’s Chorea
The main features of this disease are dementia,chorea and a family history of a similar disorder.There is a high frequency of associated psy-chopathology, notably depression, personality
Table 11.7 Some treatable causes of dementia (fromTrimble, 1981, p. 125)
Traumatic Head injury, hydrocephalus afterhead injury, subdural
Infective Neurosyphilis, chronic meningitis,parasitic and fungal infections,AIDS – secondary infections
Deficiencies Vitamin B12, folic acidNeoplasia Primary or metastaticIntoxications Barbiturates, anticonvulsants,
alcoholMetabolic Hormonal (thyroid, parathyroid,
adrenal)Wilson’s diseaseRenal failureHepatic failurePulmonary or cardiac failure
Dynamic HydrocephalusOther Embolic: Sarcoid: SLE
Whipple’s diseaseLyme diseaseBehcet’s diseaseGiant cell arteritisSystemic vasculitides
disorder and a schizophrenia-like or paranoiddisorder (Trimble, 1981a). The condition hasan age of onset typically in the fourth or fifthdecade, although juvenile forms are seen. Psy-chiatric states are the earliest manifestations ofthe disease in about one-third of patients, andmemory disturbance occurs early, though it isqualitatively different from that of Alzheimer’sdisease. In Huntington’s chorea there are bothencoding and retrieval deficits.
Huntington’s chorea is a genetic disorder,with an autosomal dominant pattern of inher-itance, and a gene abnormality on the shortarm of chromosome 4. It is known that CAGrepeats are expanded, and the abnormal proteinis referred to as huntingtin. In normal chro-mosomes, there are 9–39 CAG repeats, but inHuntington’s chorea there are usually over 40.The number is related to the age of onset of thedisease, larger numbers relating to earlier onset.
Gradual atrophy of the neostriatum isthe hallmark of the condition, and mediumspiny projection neurones (containing GABAand substance P) degenerate first and mostseverely. The small spiny cells are inhibitoryGABA neurones, with a high density of NMDA

272 Biological Psychiatry
receptors. Nuclear inclusions that label forubiquitin and huntingtin are seen. The latter isa widely-distributed protein, and is involvedin intracellular transcription and transport.It also has anti-apoptotic properties. Thereare decreased concentrations of GABA andglutamic acid decarboxylase, with a relativeincrease of dopamine function. CSF GABAis also decreased. Some neurotransmittersare increased in levels, including 5-HT andpeptide Y (Beal et al., 1988). Receptor studiesreveal reduced binding in the basal ganglia forNMDA, dopamine, GABA and acetylcholine(Young et al., 1988). One hypothesis is thatNMDA excitotoxicity is involved in pathogen-esis, although how this relates to the geneticfindings is unknown.
CT and MRI will reveal loss of bulk inthe head of the caudate, and PET studiesshow decreased metabolism in the caudate,even before structural changes are visible(Figure 11.2). Presymptomatic patients oftenshow subtle motor impairments, subtle clum-siness, brief choreiform movements and ocularmotor impairment, and on imaging it may bepossible to show a decrease in size of the corpusstriatum. Genetic testing for CAG repeats isdefinitive, and it is now possible to estimate theyears to clinical diagnosis from the current ageof the patient and the CAG-repeat length.
CNS Syphilis
Although rare, this condition is still encounteredas a cause of dementia in the Western world,and it is advisable to test serology appropriatelyin all cases. In its florid form, GPI presentsas a progressive deterioration with associatedpsychopathology. The latter may resemblemanic illness, schizophrenia or a depressiveillness. The disorder starts insidiously, some10–15 years after the primary infection, butsoon loss of judgement and delusions, some-times with the well-known grandiosity, appear.It may resemble the euphoria of the frontal-lobesyndrome, but the grandiosity is quite distinc-tive from the mood-congruent behaviour ofmania. On examination, apart from the abnor-mal mental state, tremor of the lips, tongue andoutstretched hands may occur. Dysarthria is
common. The typical Argyll–Robertson pupilis seen in about 50% of cases. If associated withtabes dorsalis, neurological features of this, suchas loss of vibration and position sense in thelimbs, will be found. Convulsions may occur.
Pathologically there is marked atrophy withneuronal loss and gliosis, and iron pigment inthe microglia and perivascular spaces is specificfor the disease (Catterall, 1977). Treponema pal-lidum can be seen in the cortex in about 50%of cases.
In the CSF there is elevation of total proteinand lymphocyte count, a paretic (first-zone) risein the Lange colloidal gold curve and positiveserology. An oligoclonal antibody pattern is alsoseen. Blood screening with WR or the VDRLis essential, but these give both false-positiveand negative results. The treponema pallidumimmobilization test (TPI) and the fluorescentantibody test (FTA) are much more reliable.After treatment, the VDRL and the WR usu-ally become normal, but this may take severalyears. The FTA, however, may remain positive,but prior to relapse the clinical manifestationsare normally preceded by further CSF changes,notably a rise in cells and protein, and increasingantibody titres.
Another spirochete that is associated withdementia is borrelia burgdorferi, which causesLyme disease. As with treponema pallidum, thisorganism can invade many organs, includingthe brain, leading to inflammatory changes.
HIV Encephalopathy
This condition, also referred to as the AIDS–dementia complex, is caused by the virusHTLV-111 (HIV, human immunodeficiencyvirus), which invades T-helper lymphocytesand damages them. Briefly, the T-helper cellspromote immunological responses to infection.They have a surface glycoprotein which bindsto the envelope glycoprotein of HIV. The HIV isa retrovirus, one which destroys cells it invadesby transcribing its own RNA into the DNA ofthe host cell using the enzyme reverse transcrip-tase. The depletion of T-helper (T4) lymphocytesleads to loss of the infected person’s immunolog-ical competence; neurotoxins are secreted andsecondary ‘opportunistic’ infections develop,

The Dementias 273
many of which affect the brain, for exampletoxoplasmosis or cryptococcal meningitis. Analternative expression is the development ofcertain tumours, for example CNS lymphoma.The pathological hallmarks of HIV dementia aremicroglial nodules and multinucleated giantcells which are HIV-infected macrophages.
It is known that the virus itself is neurotropicand can be isolated from the brains and CSF ofpatients. It may lead to an acute encephalopa-thy, associated with malaise, mood changes andseizures. However, an insidious dementia mayoccur with initial features of psychopathologysuch as lethargy, loss of libido, affective changesand cognitive blunting. Eventually, neurologi-cal signs become clear, the EEG changes oftenshowing bilateral slowing, and MRI may revealevidence of atrophy and periventricular white-matter lesions. The CSF may show a rise of thewhite-cell count and protein. In the final stages,mutism, dementia, incontinence and paraplegiamay result. Highly-active antiretroviral therapy(HART), introduced in the mid-1990s, has ledto a remarkable decline in the incidence of HIV-associated dementia.
The virus is a blood-borne pathogen, andhigh-risk patients are intravenous drug abusers,homosexuals and haemophiliacs. It is identifiedby testing for HIV antibodies, the viral loadand an abnormal ratio of T4 to T8 lymphocytes.Less than 400 T4 cells per cu mm is consideredabnormal.
Creutzfeldt–Jakob Disease and Prions
The original descriptions of this condition wereof a dementia with pyramidal and extrapyrami-dal manifestations. It is a rare cause of demen-tia, males being affected more than females.Rarely, familial cases are described, and autoso-mal dominant inheritance is suggested (Masterset al., 1979).
Although sudden onset is seen, usually, in theinitial phase, there may be only vague somaticcomplaints followed by mood and personal-ity changes. The progression of the disordermay be fairly rapid, many patients dying withinsix months of the diagnosis. Soon the demen-tia is apparent, and localized cortical deficitssuch as aphasia or apraxia may occur. The
accompanying signs are those of extrapyrami-dal and pyramidal dysfunction, but cerebellarabnormalities and frontal-lobe features may alsobe seen. Muscle wasting, convulsions (particu-larly myoclonic jerking), delusions and halluci-nations form part of the clinical picture. A startleresponse to sudden loud noises is an interestingsign that may help provide a clue to diagnosis.
Several different forms of the dementia havebeen described. These include a cerebellar form,an amyotrophic form with marked lower motor-neurone signs, and the amaurotic variant ofHeidenhain. However, some prefer not to splitthe disorder in this way, regarding the diseaseas a single entity with various presentations.
The CSF is usually unremarkable, although14-3-3 protein may be elevated. The EEG isalways abnormal, with increased slow-waveactivity and diminution of the alpha rhythm. Apattern of slow sharp-wave discharges is seen,which may be locked to the myoclonic jerks.Although these may be seen in other conditionssuch as metabolic encephalopathies, SSPEand some viral encephalitides, their presencewith the above clinical picture confirms thediagnosis of Creutzfeldt–Jakob disease. TheCT and MRI scans may be normal, althoughthey mostly show atrophy and ventriculardilatation, while on PET there are multifocalareas of hypometabolism (Cummings andBenson, 1992). Biopsies of the tonsils canidentify prion protein, and a brain biopsy willconfirm the diagnosis.
Of interest has been the transmission ofthe condition from human brain material toprimates. The first degenerative condition of thehuman CNS to be transmitted to primates wasKuru. This disorder, found among aborigines inNew Guinea, causes a pathological state similarto the human disease in the primate brains. InCreutzfeldt–Jakob disease this consists of neu-ronal loss and gliosis, and status spongiosus –the microscopic appearance of vacuolesleading to a spongiform picture. Abnormalproteinaceous particles representing prionscan be detected. This disorder has now beentransmitted to several species, and there arereports of man-to-man inoculation duringneurosurgical procedures (Bernoulli et al., 1977)and from human growth hormone extracts. The

274 Biological Psychiatry
pathological agent responsible is a prion (smallproteinaceous infectious agent). The humanprion diseases include Creutzfeldt–Jakobdisease (sporadic and familial forms), Kuruand the Gerstmann–Straussler–Scheinker syn-drome, and are referred to as transmissiblecerebral amyloidoses. The latter is an autosomaldominant disorder which presents in the thirdor fourth decade with cerebellar symptoms,with later onset of extrapyramidal featuresand dementia (Collinge et al., 1990). Familialfatal insomnia, with progressive insomnia,autonomic dysfunction and dementia is anotherprion disorder with pathological changeslargely in the thalamus.
Variant Creutzfeldt–Jakob disorder ap-peared in the UK, and is thought to be relatedto ingestion of beef from cows with bovinespongiform encephalopathy. It differs fromother forms of Creutzfeldt–Jakob disease by anearlier age of onset (mean 28 years) and pre-sentation initially with behavioural problems.It produces a characteristic MRI picture withhigh signal bilaterally in the posterior thalamus(the pulvinar sign). Homozygosity at codon 129has been noted in most cases, the gene being onchromosome 20.
Prions are resistant to heat, ultraviolet andionizing radiation and formaldehyde treatment,but are inactivated by agents that hydrolyse pro-teins. There is no associated nucleic acid, andthey do not evoke an inflammatory reaction.They are thought to be glycoproteins, essentiallyisoforms of normal host-membrane glycopro-teins (prion proteins), which are broken downby proteases. PrP 27–30 has been identified asthe infective agent (Prusiner, 1987). The cDNAhas been found, and has been shown to be asingle gene on the short arm of chromosome20 that codes for the normal membrane protein.In the prion disorders, the protease-resistantinsoluable isoform of the protein accumulates(PrPsc/PrPres/PrPp), a process which is autocat-alytic; in other words, the abnormal protein actsas a template for its further production.
Although clearly genetic, with mutationsleading to autosomal dominant disease, priondiseases can also be transmitted by inoculationof exogenous prion protein.
It is now recognized that multiple mutationsof the gene that encodes the prion protein (PrPor PRNP) can occur, and over 50 different muta-tions have been reported in the familial cases.The commonest mutation is reported at codon200. Since prion diseases can have very vari-able presentations, the extent to which otherdementias may be prion-related has yet to bedetermined.
Hydrocephalic Dementias
Although not exactly understood, the dynam-ics of CSF flow are as follows. The major-ity is produced by the choroid plexi of theventricular system, and flow is from the lat-eral and third ventricles, through the Sylvianaqueduct to the fourth ventricle, and then outfrom the interstices of the brain to the sub-arachnoid space. It then goes either upwards,over the surface of the brain to be absorbedinto the saggital sinus, or downwards overthe spinal cord. Interference with this flowpattern can lead to hydrocephalus, with accu-mulation of excess CSF within the ventricularsystem. Two main varieties of hydrocephalusare recognized: obstructive and non-obstructive(see Table 11.8).
The non-obstructive conditions refer tothose traumatic, destructive or degenerativestates that lead to ventricular enlargement. Theobstructive varieties are of two main types. Innoncommunicating hydrocephalus, the CSFflow is impeded within the ventricular system,leading to increased pressure in the ventriclesand secondary enlargement. Such states havelong been recognized in childhood, but it is nowclear that a variety of processes may lead tosimilar pathology in adulthood, and dementia is
Table 11.8 Hydrocephalic dementias (after Benson,1975)
Non-obstructive Degenerative, e.g. Alzheimer’sdisease
Destructive, e.g. arterioscleroticObstructive Noncommunicating with
ventricular obstructionCommunicating – normal-
pressure hydrocephalus

The Dementias 275
one result. Pathologies include tumours, intra-cranial haemorrhage, colloid cysts of the thirdventricle, ectatic basilar artery and periventric-ular inflammation. The link between stenosisof the aqueduct, a very vulnerable site, and aschizophreniform illness has been noted (seeChapter 8). In communicating hydrocephalusthere is no obstruction of the flow within theventricular system or its exits, but a failure ofabsorption of the CSF back into the saggitalsinus through blockage occurs. Either the fluidis unable to reach the convexity of the brainor absorption through the arachnoid villi isabnormal. There are several causes of this,including cerebral trauma, previous meningitis,neoplasia or, most commonly, subarachnoidhaemorrhage. Normal-pressure hydrocephaluswas described by Adams et al. (1965), andreferred to a dementia seen several years aftera head injury or subarachnoid haemorrhagewith characteristic clinical features. Theseinclude gait disturbance and incontinence, anda normal CSF pressure. The dementia wasoften of recent onset, and was more related toa psychomotor slowing than to memory andhigher cognitive deficits. Patients lost initiative,became apathetic, and in some cases theirbehaviour resembled a state of depression.
It is now recognized that the clinical picturecan be varied. Spasticity, especially of the lowerlimbs (feet glued to the floor), difficulty in initi-ating movement, frontal-lobe signs, and incon-tinence and ataxia in the presence of dementiashould alert to the possibility of this diagno-sis, even in the absence of the above associatedevents in the patient’s history, idiopathic casesbeing well recognized.
The EEG is usually abnormal, showing dif-fuse slowing, and a CT or MRI scan revealslarge ventricles, often maximally blown in thefrontal and temporal regions, in the presenceof normal or small cortical sulci. Isotope cis-ternography will reveal the abnormal patternof flow, and monitoring intracranial CSF pres-sure may help identify patients who will benefitfrom shunting.
The possibility of shunting the CSF to eitherthe atrium of the heart or the peritoneal cavityhas been tested, but with variable success.
FURTHER CAUSES OF DEMENTIA
The causes of dementia are legion, and someof the more common ones have alreadybeen defined. Every physician is looking toexclude a treatable cause, some of which areshown in Table 11.7. Tumours, especiallymeningiomas, must always be ruled out. Bothfolic acid and vitamin B12 deficiencies canlead to neuropsychiatric change and dementia,and this can occur in the absence of ananaemia. Nicotinic acid deficiency can leadto a pellagra-like state with dermatologicalchanges, gastroenterological symptoms anddementia. Anticonvulsant drugs, notablyphenytoin, in epileptic patients have beenimplicated with an encephalopathy (Trimbleand Reynolds, 1976) and the dementia ofchronic alcoholism is recognized (Ron et al.,1979). Intoxication with psychotropic drugscan lead to cognitive dulling, for example withlithium, and rarely major tranquillizers can pro-voke or exacerbate a dementia-like syndrome.Creutzfeldt–Jakob-like symptoms are describedwith tricyclic antidepressant intoxicationand lithium.
Hormone disturbances can lead to demen-tia, especially hypothyroidism, which is usuallyaccompanied by other signs of myxoedema.Thyroid function tests will be abnormal, serumcholesterol raised and thyroid antibodies maybe present in the serum.
More pervasive causes of dementia includethose secondary to such cerebral insults astrauma and anoxia, and the dementia of demye-linating conditions such as multiple sclerosis.
SOME OUTSTANDING ISSUES
Differential Diagnosis
It used to be suggested that to try and diagnosethe cause of dementia in life is a futile exercise. Itwas asserted that the post-mortem diagnosis isthe only valid one, and that clinical diagnosis isoften at variance with this. It was further impliedthat dementia is irreversible and that treatmentsare ineffective, and hence the diagnosis is purelyan academic exercise.

276 Biological Psychiatry
There are several reasons why such viewsare no longer tenable. Thus, the dementias dodiffer in their clinical presentation. While thebroader issue of cortical and subcortical demen-tia is discussed below, it seems that there aresome forms of dementia that primarily presentwith cortical destruction, with apraxias andaphasias, while in others there is gradual cogni-tive slowing, difficulties with planning a futureevent and impairment of the grasp of complexissues – often initially with minimal memoryimpairment. Alzheimer’s and fronto-temporaldementia can be distinguished in many cases,the latter showing behavioural complicationsin the presence of a relatively well-preservedmemory and absence of the parietal signs. EEGand MRI data aid this distinction. An impor-tant sequel to this is to allow for and expectmore florid behavioural problems with frontaldementias, which has consequences not only formanagement, but also medicolegally.
Both of these forms of dementias must be dis-tinguished from a cortical aphasia syndrome,which may be very difficult in the so-calledangular gyrus syndrome, or following an infarctin the dominant hemisphere of a left-handedpatient, in whom the clinical picture of theaphasia can be misleading. The angular gyrussyndrome is caused by a lesion of the left hemi-sphere in the region of that gyrus. Patients havecombinations of fluent aphasias, apraxias, alexiaand parts of Gerstmann’s syndrome, compris-ing acalculia, right–left disorientation, fingeragnosia and agraphia. Such focal syndromes aremost likely, particularly if they are due to a vas-cular cause, to be nonprogressive, and thus carrya very different prognosis to the dementias.
Distinguishing primary parenchymatousdementias from secondary dementias is ofutmost importance, especially in view of thenumber of reversible causes that exist. Theseparation of the different types of vasculardementia has prognostic and treatment impli-cations. The number of toxic, metabolic andhormonal causes should be remembered, andpatients with dementia should be offered thesame medical facilities for investigation asother patients, irrespective of their age. Thedistinction of an acute organic brain syndrome(delirium) from dementia can sometimes be
difficult, but the possibility that an establisheddementia may be exacerbated by such a statemust always be borne in mind, and significantimprovements of the mental state can beseen with resolution of the offending causes(infections, drug treatments, etc.).
The relevance of careful clinical investiga-tion is apparent with follow-up studies. Thecommonest missed condition is depression andthe best discriminator of this diagnosis is aprevious history of depressive illness, and affec-tive features on admission. Psychometric tests,with marked verbal/performance discrepancy(but not memory tasks), radiological evidenceof cerebral (particularly cortical) atrophy andEEG abnormalities are of maximum value indiscriminating between those with and withoutreversible dementia.
For some conditions, specific treatments areneeded. For example, cerebrosyphilis requiresantibiotics, usually large doses of penicillin,although steroids are often given in additionto prevent the Herxheimer reaction. This isan acute febrile state with intensification ofsymptoms that comes on soon after treatment.A patient with hydrocephalus should bereferred to an interested surgeon for consid-eration of shunting, and tumours will requiresimilar referral. Attempts should be madeto correct any endocrine or metabolic causesdiscovered, and intoxicants, especially anyunnecessary drugs, should be removed. Itshould be remembered that the aging brain,especially one affected by a dementing process,is easily decompensated by such factors, andan acute organic brain syndrome thus compli-cates the underlying deficits. Respiratory andurinary-tract infections are notorious offenders,although in patients that have ceased to care forthemselves and have no one to look after them,nutritional deficiencies may be paramount.
Subtle head injuries may occur, eithercausing a dementia syndrome, for examplewith the development of subdural haematomas,or exacerbating an existing condition. Alco-hol dependency or misuse should never beoverlooked; many elderly early dementedpatients take an excess, with poor food intake,worsening confusion and potentiating fallsand head injuries. Diagnosis of MID should

The Dementias 277
lead to a search for the site of origin of anyemboli, and any hypertension requires cautioustreatment. Stopping smoking is important.Treating cardiac arrythmias and using lipid-lowering agents and aspirin helps preventfurther strokes, and may even protect againstdementia (Erkinjuntti and Gauthier, 2009;Gouw et al., 2008). Some advocate even moreaggressive anticoagulant treatment – an area ofconsiderable unresolved controversy. In a fewselected cases, where the problem relates tocarotid artery stenosis, carotid endarterectomyhas been tried, although the evidence that thisbrings lasting benefit in many cases is not clear.
Reversible/Irreversible
In older definitions of dementia, the criterionthat it shall be an irreversible syndrome is oftennoted. One distinguishing feature between adelirium and a dementia was thus thought to bethe acute reversible nature of the former and thechronic irreversibility of the latter. However,the feature of irreversibility can no longer beaccepted. This arises from the structural impair-ment, and if the pathogenesis is functional(altered neuronal function) then the possibil-ity of reversibility can be entertained. There aremany examples of reversible dementia notedabove, and early treatment may prevent signifi-cant morbidity, or prevent secondary structuralchanges from developing.
Dementia/Pseudodementia
The presentation of a major affective disorderwith a picture resembling dementia has alreadybeen discussed (Chapter 8). It has also beennoted that follow-up studies indicate thatpatients diagnosed with dementia who do notdeteriorate tend to have an affective disorderin retrospect. Although the term ‘pseudode-mentia’ refers to this condition, it is arguablyincorrect. Thus, if it has the hallmarks of demen-tia, it should be so diagnosed, recognizing thatdementia is the beginning not the end of thediagnostic process. Depression, in addition toseveral other conditions, is a cause of reversibledementia. Others include mania, the depressive‘pseudodementia’ of Ganser’s syndrome,
hysteria, simulation and anxiety disorders. Theacknowledgement that these conditions mustbe considered in the differential diagnosis ofdementia will hopefully lead to their presencebeing sought and the correct diagnosis of apotentially treatable condition being made.
Cortical/Subcortical
In this chapter, reference has been made to sub-cortical dementia. It has been suggested thatdamage to subcortical nuclei (basal ganglia,thalamus) and deep white matter may lead to adementia syndrome, the presentation of whichdiffers from those disorders that mainly influ-ence cortex. Albert et al. (1974) described thefeatures of subcortical dementia as emotionaland personality changes, memory disorder, adefective ability to manipulate acquired knowl-edge and a slowness in the rate of informationprocessing. In contrast to the cortical dementias,aphasias, apraxias and similar symptoms arenot seen. This clinical picture may be seenin progressive supranuclear palsy (Steele–Richardson syndrome), Parkinson’s disease,Huntington’s chorea, Wilson’s disease, somevascular dementias and the AIDS–dementiacomplex. The dementia of depression alsohas similar features. Albert et al. supportedthis concept by quoting evidence that surgicallesions of the basal ganglia impair performanceand problem-solving tasks, and that stimulationof subcortical structures impairs cognitive per-formance. They also noted the similarity of thesymptom complex of subcortical dementia tothe behavioural syndrome seen in patients withfrontal-lobe damage. Pointing to the uniquereciprocal connections between the frontalcortex and the limbic system, they also referredto this as frontolimbic dementia.
The concept of the subcortical dementiasis most strongly advocated by Cummingsand Benson (1992). They give as prominentclinical features ‘mental slowness, inertia andlack of initiative, forgetfulness, dilapidationof cognition, and mood disturbance’ (p. 95).The memory changes are more of forgetfulnessand difficulty of spontaneous recall, and thecognitive state may demonstrate a difficultywith processing of complex problems, ‘failing

278 Biological Psychiatry
to synthesize the elements properly to achievethe correct answer. . .’ (p. 10). They also includeas causes hydrocephalus and toxic/metabolicdisorders that disrupt basal gangia function,and note that many conditions may leadto a combined picture of both cortical andsubcortical deficits.
The concept of subcortical dementias hasnot gained universal acceptance. This stemsin part from a traditional reluctance to viewsome subcortical structures, such as the basalganglia, as anything but motor in function,and the long-held view that ‘higher’ cognitivefunction is the prerogative only of the cortex.Further, the pathological studies viewed abovehave led to a questioning of the value of theterm ‘subcortical’ in the context of pathology ofmost syndromes. Anatomically the close linksbetween the basal-ganglia structures and cortexare well established (Chapter 2) and disruptionof cerebral circuits in pathology involves cor-tical and subcortical structures. However, theconcept does emphasize that disruption of cog-nition can be the result of damage to the deepernuclear structures of the brain and that demen-tia has presentations other than the classical oneseen in association with Alzheimer’s disease.
Senile/Presenile
The term ‘senile dementia’ referred arbitrarilyto patients developing dementia over the ageof 65. If no other underlying condition wasfound, it was labelled parenchymatous seniledementia, and was thought to present in asimilar fashion to the presenile dementia ofAlzheimer, but in a milder form. Those whowish to uphold differences between the lat-ter and parenchymatous senile dementia notethe genetic difference, and comment clinicallyon the relative absence of focal cortical signs,extrapyramidal disorder and seizures in thesenile group. Others have argued there wereneuropathological differences, noting the higherdensity of plaques and tangles in the tem-poral neocortex, amygdala and hippocampusfrom brains of Alzheimer’s disease patients. Thealternative view, that the senile dementia andAlzheimer’s disease were the same condition,
emerged from the early neurochemical studies,in which cholinergic deficits were seen irrespec-tive of age (Bowen et al., 1979).
The concept of presenile/senile based onarbitrary age limits was poorly conceived, andthe unravelling of different pathologies – forexample of fronto-temporal dementia, with dif-ferent age of onset from classical Alzheimer’sdisease – plus potential classifications that aremoving towards a pathological (tauopathies) oreven a genetic basis render it redundant.
Dementia, Aging and Mild CognitiveImpairment
A related issue is the extent to which disor-ders such as Alzheimer’s disease merely rep-resent accelerated aging. This view is almostcertainly incorrect. It is true that elderly peopledevelop cognitive impairments, notable slow-ing and memory difficulty, but cognition isoften intact in advanced old age, and the otherdisturbances found in Alzheimer’s disease arenot seen.
The concept of mild cognitive impairment(earlier called ‘benign senescent forgetfulness’)refers to a transitional state between the cogni-tive changes of normal aging and early demen-tia. Thus, on history taking, those who later geta diagnosis of Alzheimer’s disease reveal cogni-tive problems before the diagnosis is made, butnot all aging people with memory complaintswill go on to develop dementia. The conceptof mild cognitive impairment is thus defininga high-risk group. On cognitive testing mem-bers of this group perform below age–educationnorms on at least one cognitive test (>1.5 stan-dard deviations), but they have no impairmentsof activities of daily living, and function inde-pendently. The prevalence increases with age,but the conversion to dementia is given atbetween 2.7 and 15% per year, perhaps reveal-ing the difficulty of defining mild cognitiveimpairment in practice. Further, some distin-guish different forms, for example an amnesticvariety. Prognostic studies suggest poor verbalmemory, cerebral or regional brain atrophy onMRI (especially in hippocampus and entorhinalcortex), and progression of the latter over time,

The Dementias 279
as well as decreased glucose uptake in poste-rior cingulate/temporoparietal areas, are signif-icant. The Apo E allele status is also relevant.
A confounding factor is that depression isalso comorbid with mild cognitive impairment,and with the considerable publicity given toAlzheimer’s disease, concern, worry and hypo-chondriacal issues can cloud the picture.
Neuropathological data reveal that plaquesand tangles are common in the brains of elderlynondemented people, and even Lewy bodiesare reported, but plaques are usually in smallernumbers and tangles are only rarely foundin the cortex. There seems to be a commonmechanism underlying several degenerativedisorders, with aggregation and deposition ofmisfolded insoluble proteins, which lead toamyloid deposition. These changes seem toaccumulate slowly over the years, but how themisfolded proteins lead to neurodegenerationremains to be discovered. Cell loss is seen,but, compared to Alzheimer’s disease, it is lessextensive, and where there is a reduction ofdentritic arborization an increase in synapticcontact is noted (Tomlinson, 1982). Pathologicalfollow-up studies suggest that those withamnestic mild cognitive impairment are mostlikely to progress to Alzheimer’s disease, butsome develop other disorders such as Lewy-body dementia (Jicha et al., 2008; Josephs et al.,2009; Whitwell et al., 2007).
Some decline in muscarinic binding sitesoccurs with aging, but choline acetyltransferaseactivity is not characteristically diminished, andnor is the ability to synthetize acetylcholine.The losses of noradrenaline and somatostatinseen in Alzheimer’s disease are not a featureof aging (Rossor et al., 1984) (see Table 11.3).The CSF changes shown in Alzheimer’s diseaseare not as yet defined in mild cognitive impair-ment and are not found in normal aging. Oneinterpretation of this is that in spite of someneuronal loss and diminution of biochemicalactivity with aging, the remaining neurones cancope with the demands on them by increas-ing their activity, while the neurones in mildcognitive impairment in those who progress toAlzheimer’s disease do not possess this reservecapacity.
The introduction of mild cognitive impair-ment in many ways simply shifts the problemof when the process of dementia begins, andthe borders between it, healthy aging and earlyAlzheimer’s disease remain unclear. Further, wedo not know what the first step in any pathol-ogy is, or where it begins. Amyloid precursorprotein is a normal synaptic constituent, and thefirst problems may therefore be synaptic.
Mixed Types and Thresholds
In spite of attempts to clearly distinguish varioustypes of dementia, mixed types are frequentlyseen. Thus Pick’s and Alzheimer’s pathologyhave been seen in the same brain (Smith andLantos, 1983), and the existence of low attenu-ation areas on CT scans or areas of increasedT2 signed intensity on MRI in patients with pre-sumed Alzheimer’s disease are common (Coffeyand Figiel, 1991; Jacoby and Levy, 1980a). Theacute onset of Alzheimer’s disease followinghead injury or illness is reported (Hollanderand Strich, 1970), and several pathogenic influ-ences seem to be linked to the formation of bothplaques and tangles. The presence of plaques innormal aging and their correlation broadly withthe cognitive performance has led to the sug-gestion that there are thresholds beyond whichdementia occurs. Thus, aging processes providethe nidus upon which other insults operate toincrease the changes and eventually throw thebrain into ‘brain failure’, analogous to the devel-opment of cardiac failure. The insults could bemany, including a vascular episode, minor headinjury or anoxia. In spite of the attractivenessof these ideas to explain some of the clinicalphenomena, they are not supported by the bio-chemical evidence accumulated to date.
Incidence Rates
Finally, since the population is getting older,and the incidence rates rise with age, will every-one who reaches the age of 120 be demented?One study of an elderly community living inCache county, Utah noted a peak in incidence inthe 90–92 age group, with a decline thereafter(Onyike et al., 2007; Tschanz et al., 2006).


12Biological Treatments
INTRODUCTION
Most of the treatment modalities used in biolog-ical psychiatry attempt to modify brain circuitryand behaviour. They can be grouped into oneof several types. By and large they generallyapproach the allocortex.
There are treatments that directly interactwith the brain and cause direct physical changes.Included in this class are the old and newbrain-stimulation techniques: electroconvulsivetherapy (ECT), vagus-nerve stimulation (VNS),deep-brain stimulation (DBS) and transcranialmagnetic stimulation (TMS).
In contrast, there are treatments where thereis an indirect physical intervention. This classincludes the talking therapies (psychoanalysis,cognitive behavioural therapy), various formsof biofeedback, and even techniques like aro-matherapy. We also include in this indirectphysical class the indirect medications used astreatments.
Psychopharmacology, or allopathy, has beena cornerstone of biological psychiatry and willcontinue to be so for the next decade at least.We will discuss psychopharmacology first, anddeal with the newer direct physical treatmentsat the end of the chapter.
PHARMACOLOGY: PHARMACOKINETICSAND PHARMACODYNAMICS
Of the several ways that drugs are adminis-tered to patients, the oral route is the most
Biological Psychiatry 3e Michael R. Trimble and Mark S. George 2010 John Wiley & Sons, Ltd
common. Following absorption from the gas-trointestinal tract, the drug passes to the livervia the portal system, where metabolism mayoccur, usually by oxidation, reduction, hydroly-sis or conjugation. This metabolism is referred toas ‘first-pass metabolism’, and drugs which aregiven intramuscularly, intravenously or with askin patch avoid this ‘first-pass’ effect. For oralcompounds, the rate of absorption of a drugfrom the stomach depends upon a number offactors, including the concentration of the activecompound, the carrying medium with whichthe compounds are given (including whether ornot they are taken with food), the pH of thegastrointestinal tract, associated disease of thegut and other active medications which maycompete with uptake across the gastrointestinalcell membranes.
Ionization is an important factor determininguptake, since only non-ionized drug crosses cellmembranes freely, and, unless specific transportmechanisms exist, the rate of movement is pro-portional to the concentration of the drug acrosscell membranes. The proportion of ionized tonon-ionized drug is dependent on both pHand its dissociation constant. It is immediatelyapparent how oral ingestion may lead to a widevariation in the amount of drug finally absorbedfrom the gut, and thus how oral dose does notnecessarily relate to serum levels and can changeover time even within the same individual.
Some drugs increase the activity of enzymesresponsible for their metabolism or for the

282 Biological Psychiatry
metabolism of other drugs within the liver.Barbiturates, phenytoin, carbamazepine andsteroids are particularly implicated; carbama-zepine is known to induce its own metabolism.
Cytochrome P450 plays a major role in oxida-tive metabolism, and at least 19 forms exist inthe human liver. Individual isoenzymes maymetabolize different drugs, and inhibition of themetabolism of one drug by another using thesame isoenzymes may result in high serum lev-els of the inhibited drug, and toxicity. Inductionof the enzymes that metabolize one drug byanother will lead to lower serum levels of thefirst. Although some 75% of drug metabolism isthrough the CYP system, much is not poly-morphically expressed (e.g. CYP3A4/5) andthe main polymorphisms of relevance, in otherwords those genetic variables that influencedrug metabolism in humans, and may deter-mine alterations of speed of metabolism, areCYP 2D6, 2C19 and 2C9.
From the bloodstream, drugs become widelydistributed throughout the body. The distri-bution is initially determined by the relativeblood flow of the various organs and the pres-ence of the blood–brain barrier, which protectsthe brain from the effects of many neurotoxiccompounds. Further, many drugs are bound toplasma proteins, especially albumin; the pres-ence of the drug in plasma thus occurs in bothbound and unbound (free) forms.
Many psychotropic drugs are secondaryor tertiary amines and weak bases, and areabsorbed better from the duodenum than thestomach. Since lipid solubility is important forpassing through the blood–brain barrier, thesedrugs are highly lipid-soluble, but are alsooften highly protein-bound. P-glycoproteinsare transporter proteins within the brain whicheffectively prevent drugs getting into it, andform part of the blood–brain barrier. They areencoded by selective genes (ABCB1) and studiesare underway to see which genotypes mayrelate to response to psychotropic medications.P-glycoprotein status may be one cause oftreatment nonresponsiveness.
Excretion of drugs is usually via the kidney,although the liver and other organs such as thelung may also be involved.
The half-life of a drug refers to the time ittakes for its concentration to decrease in theplasma by 50%. The quicker the metabolismand elimination, the shorter the half-life. ‘Zero-order’ kinetics refers to a situation in which thereis an exponential relationship between the doseof a drug and its serum levels (see Figure 12.1),while in ‘first-order’ kinetics the relationship isone of equivalence.
Zero-order kinetics occurs because the en-zymes responsible for drug metabolism andexcretion become saturated at levels requiredfor the therapeutic effects. Phenytoin is one drugthat follows such kinetics, whereas the majorityof psychotropic medications show first-orderkinetics. Knowledge of the half-life of a drugis useful, since it is recommended that the doseinterval be equivalent to the half-life. The steadystate, namely that in which the serum level ofthe drug reaches a steady plateau, excretionbeing in balance with intake, is approximatelyequivalent to four or five half-lives.
Since factors which influence drug metab-olism include genetics, age, diet, coexistentmedications and coexistent disease, carefulconsideration of pharmacokinetic principles isrequired, particularly in certain patients. Theseinclude those with diseases of the liver, kidneyand heart, as well as the young and the elderly.In children, absorption from the stomach isfaster than in adults, which may lead to higherpeak drug concentrations and thus an increasedrisk of adverse effects. Plasma–protein bindingis reduced because of lower albumin and glob-ulin contents of the blood, values comparable tothose of adults being reached between the agesof 10 and 15. The enzyme systems responsiblefor drug degradation are faster than those ofadults in early childhood, and decrease slowlywith age, such that adult clearance valuesdevelop around puberty. The increased metab-olism of drugs in childhood means dosing re-quirements need careful adjustment.
In elderly patients, the body composition hasaltered, with a generally leaner body mass andan increase in adipose tissue. This means thatlipid-soluble drugs are more extensively dis-tributed, particularly in elderly women, as thefraction of the total body weight composed of

Biological Treatments 283
200 P.He.
THERAPEUTICRANGE
P.Ho. R.B.J
150
200 400 500 600300
Dose of phenytoin (mg/day)
Ser
um p
heny
toin
con
cent
ratio
n (µ
M)
100
100
50
0
Figure 12.1 An example of zero-order kinetics. Dose/serum-level relationship for phenytoin in threepatients in whom steady-state concentrations were measured at several doses of the drug. Each pointrepresents the mean ±SD of three to seven separate estimations. The curves were fitted by computer using theMichaelis–Menten equation. The therapeutic range suggested by Buchthal et al. (1960) has been drawn in toillustrate the steepness of the relationship within this range. Note: 4 mM = 1 mg/ml (Biol Psych, 2 Ed, p. 326)
adipose tissue increases more in women than inmen. Alteration of gastrointestinal-tract activity,with reduction of gastroparietal cell functionand impaired acid secretion with an elevatedpH, leads to impaired absorption of certaindrugs. Hepatic and renal activity may also bealtered. In particular, the hepatic microsomalenzymes responsible for oxidative metabolism,principally hydroxylation and n-dealkylation,may be diminished in this age group, lead-ing to reduced clearance and higher steady-state plasma concentrations with multiple drugdosage. Further, reduced hepatic blood flowoccurs, on account of reduced cardiac output,with a further decline of clearance. Elderlypatients may have diminished plasma albuminwith reduced total protein binding, and elimi-nation of drugs by renal clearance is increasedsince there is a fall of glomerular filtration rateand decreased tubular secretion and absorption
capacity of the renal tubules. All of these factorsmean alterations in the volume of the drugdistribution (the hypothetical volume relatingthe amount of drug in the body to the plasmaconcentration at all times after the attainmentof distribution equilibrium) and reduced clear-ance, with considerable danger of drug toxicityif dosages employed for younger patients arenot modified.
‘Pharmacodynamics’ is a term that refers tothe biochemical, physiological and behaviouraleffects of drugs, which in many cases bearno direct relation to pharmacokinetics. ‘Behav-ioural toxicity’ refers to specific side effects ofdrugs, leading to impaired performance. Theseproblems, frequently encountered in clinicalpractice, include a whole spectrum from minormood changes, impairment of psychomotor per-formance, fatigue and drowsiness, through tosevere agitation and psychoses.

284 Biological Psychiatry
ANTIDEPRESSANTS
These are divided into two major categories:the monoamine oxidase inhibitors (MAOI) andnon-MAOI drugs. The non-MAOI medicationsare traditionally further divided into tricyclicand nontricyclic, while the MAOIs may besubdivided either by chemical structure intohydrazines and nonhydrazines, in reference totheir enzyme selectivity as MAOA or MAOBinhibitors, or in relation to their reversibility ofenzyme inhibition.
MAOI Antidepressants
These compounds, the first of which was iso-niazid, were introduced for the treatment oftuberculosis, but were soon recognized to beenergizing in their effects. The early forerun-ners were all hydrazines, and were notablebecause of their hepatotoxicity and the ‘cheesereaction’. The mechanism of the latter is asfollows. Monoamine oxidase is widely dis-tributed throughout the body, and togetherwith catechol-O-methyl transferase (COMT) isresponsible for the detoxification of absorbedprimary amines. Some sympathomimeticamines, in particular tyramine, exert a hyper-tensive effect by releasing noradrenaline fromtissue. Although the main problem is tyramine,other amines and amine precursors such astyrosine, histamine and dopamine may also beinvolved, and such products may derive fromprotein-containing foods that have undergonedegradation, or from other drugs.
MAOIs will minimize the degradation ofthese amines in the gut wall, and thus oneexplanation for the ‘cheese effect’ relates toan increased presence of these amines in thecirculation. Alternatively, inhibition of MAOin adrenergic nerve endings delays the metab-olism of tyramine and noradrenaline, and thusincreases their effects.
It is now known that MAO exists in both Aand B forms. The substrates for MAOA includenoradrenaline and 5-HT, while phenylethy-lamine is a substrate for MAOB. Tyramine anddopamine are substrates for both forms, butit has been suggested that selective inhibitionof only one form of MAO may minimize
the chances of a hypertensive reaction. Thesymptoms of this reaction include headache,sweating, nausea, vomiting and a rise in bloodpressure that can lead to cerebral bleeding. Thefoods most often involved contain tyramine,although fatalities have almost always beenassociated with cheese.
Currently-marketed hydrazine deriva-tives include isocarboxide, nialamide andphenelzine; the nonhydrazine groups includetranylcypramine and pargyline. The selectivecompounds include deprenyl for MAOB andclorgyline, cimoxatone and moclobemide forMAOA. The place of MAO drugs in thetreatment of depression has been evaluatedin several reviews (Tyrer, 1976; Pare, 1985).Generally they are recommended for patientswith ‘atypical depressions’, although the exactfeatures that respond are often less than clearlydefined. Tyrer (1976) suggested that the clinicalprofile most commonly associated with a goodresponse includes hypochondriasis, somaticanxiety, irritability, agoraphobia, social phobiasand anergia. A poor result is associated withguilt, depressed mood, ideas of referenceand nihilistic delusions. Most clinicians agreethat a patient with typical major affectivedisorder and endogenous features is the leastappropriate for this class of drugs, while addi-tional anxiety or phobic symptoms, or mixedanxiety–depressive states, may respond. Thepresence of somatic symptoms, of the phobicanxiety–depersonalization syndrome and ofpanic attacks suggests a good response. Follow-ing administration there is often a delay beforeimprovement, sometimes of days or evenweeks, although this is less with the nonhy-drazine drugs. These compounds suppressREM sleep, and the onset of the clinical improve-ment often coincides with the change in sleeppattern. Dosage is particularly important, andsome negative results of earlier trials stemmedfrom inadequate prescriptions. It is usual tostart with doses in the medium range and thenincrease after one or two weeks, depending onthe patient’s response. However, doses of upto 90 mg of phenelzine, 20–40 mg of tranylcy-promine and 50 mg of isocarboxazid may benecessary. Once treatment has been started itmay continue for several years if necessary,

Biological Treatments 285
and apart from the limitations of interactionswith foodstuffs and other drugs, long-term sideeffects appear to be rare.
The drugs are metabolized by acetylation,and the speed (fast and slow) at which this iscarried out is a polygenetically inherited trait.In the United Kingdom, some 40% of the popu-lation comprises fast acetylators, but the clinicalrelevance of this is unclear.
MAOI drugs may be combined with tricyclicor other antidepressants in certain clinicalsituations. Although this may lead to unwantedeffects, especially hypotension, used carefullysuch combinations can be useful, particularlywith resistant depressions. In general, a patienton a tricyclic antidepressant may be started onan MAOI, but more caution needs to be exer-cised when patients are already on the latter andneed to be given additional tricyclic therapy.Both drugs may be started simultaneously, butit is wise to start each drug at a lower dose thanwould be used when given alone. It has beensuggested that clomipramine, ecstasy (MDMA3,4 methylenedioxymethamphetamine), me-peridine, tramadol, dextromethorphan andSt John’s wort should not be combined withan MAOA inhibitor. Selective 5-HT reuptakeinhibitors (SSRIs) should be used with caution,and after a washout period.
Apart from the hyper- and hypotensive re-actions, other side effects noted include tremor,weakness, dizziness, hyperreflexia, irritability,ataxia, impotence, hypotension, micturitionproblems, sweating, hyperpyrexia, rashes and,rarely, convulsions. The drugs are contraindi-cated in liver disease, congestive heart failureand following cerebrovascular accidents. Thehypertensive complications respond to alphaadrenergic blocking drugs, such as phen-tolamine or chlorpromazine.
The newer generation of MAOI drugs cur-rently being investigated shows selectivity forone or other of the enzymes. Most work has beencarried out with selegeline, which appears topossess antidepressant properties (Mendlewiczand Youdim, 1983), which can be shown toinhibit platelet MAOB, an effect that may berelated to the clinical response. The selectivityfor MAOB is probably related to lack of thehypertensive effect with tyramine and lack
of postural hypotension as a side effect. Themain use of selegeline is in Parkinson’s disease;a transdermal delivery product is available,which is also approved for depression. Asimilar agent is rasagiline.
Reversible inhibitors of monoamine oxidase(RIMAs) are selective MAOA inhibitors thatare themselves inhibited in action by the pres-ence of high levels of natural substrate. Thus,high released or ingested endogenous amineswould continue to be peripherally metabolized,and not provoke a hypertensive reaction. MAOin the brain would continue to be inhibited,exerting the therapeutic effect. Several of thesecompounds have been tested (toloxatone, bro-faromine). The only one clinically available ismoclobemide.
There is no dietary restriction with moclobe-mide: an average meal contains 25 mg of tyra-mine, and doses of up to 100 mg of the latter havebeen given with moclobemide safely. How-ever, caution is advised with clomipramine ordeprenyl, and a serotoninergic syndrome hasbeen reported in combination with SSRIs. Thestarting dose is 300 mg, with target doses of450–600 mg, and single daily dosing is possible.Moclobemide has a half-life of 1–4 hours, andis generally nonsedative. It is unclear whetherthese compounds are effective for the atypicalpresentations that are responsive to the earliergeneration of MAOIs, their use at present beingfor depression and social phobias.
Non-MAOI Antidepressants
The first of these to be synthesized and usedwas imipramine, followed shortly by amitripty-line. These two drugs are probably still the mostwidely used of the non-SSRI antidepressants.The early members of this group were all varia-tions of the tricyclic nucleus, but more recentlydrugs have been developed with nontricyclicstructures.
Tricyclic Drugs
Traditionally, the tricyclic drugs were thoughtto act by inhibition of monamine uptake intothe presynaptic neurone, thus enhancing theavailability of monoamines within the synaptic

286 Biological Psychiatry
Table 12.1 Properties of some antidepressant drugs
Inhibition of uptake Affinities for receptor
5-HT NA DA Muscarinic anticholinergic Anti-histaminic
Amitriptyline ++ + + + ± + + + + + +Clomipramine + + + + – ++ ±Imipramine ++ + ± + +Maprotiline – + + + ± ± +Desipramine + + + + – + –Nortriptyline + + + + ± + +Bupropion – – ++ – –L-tryptophan – – – – –Mianserin – + + – ++Viloxazine – + + – –Paroxetine + + + – – ± –Fluvoxamine + + + – – – –Sertraline + + + – – – –Citalopram + + + – – – +Escitalopram + + + _ _ _ _Fluoxetine + + + – – – –Trazadone + – – – ±Iprindole – – ± – –Dothiepin + + ± ± + + +Protriptyline + + + + ± + + + ±Lofepramine – ++ – + ?Venlafaxine ++ ++ ± – –Nefadozone ++ ++ – – –Mirtazepine + _ _ ± +
cleft. Further, it was taught that drugs which aretertiary amines have more of an effect on 5-HTuptake, while the secondary amines are morepotent with regards to catecholamine uptake.The spectrum of action of this group and ofsome other antidepressants in relationship tobiochemical effects is shown in Table 12.1.
Lofepramine is a tricyclic antidepressantwhich is metabolized in vivo into desipramine;hence its pharmacological and clinical profile issimilar to the other tricyclic drugs, but it has anapparently excellent safety profile, including inoverdose.
Anticholinergic effects are noted, particularlywith amitriptyline, clomipramine and protripty-line. These relate not only to their side effects,but also to their clinical efficacy if patients findthem difficult to take. Antihistaminic effects alsovary as shown.
Nontricyclic Drugs
In view of the problematic side effects of the tri-cyclic drugs, many alternative antidepressants
have been marketed. Most investigated are theSSRIs, developed largely on the basis of the5-HT hypothesis of depression (see Chapter 8).
Trazadone
This is a triazolopyridine with an addedphenylpiprazine group. It has no anticholiner-gic properties and is free from cardiovascularside effects, but is a 5-HT2 antagonist, a 5-HTuptake inhibitor and an alpha-2 adrenoceptorantagonist. It is thus serotoninergic. It israpidly and completely absorbed followingoral administration and its metabolites areinactive. The half-life is about four hours, andits clinical dosage is approximately twice thatof tricyclic drugs, up to a maximum of 600 mgper day. It has similar efficacy to tricyclicantidepressants, but is sedative, and relativelysafe when taken in overdose. It is reported toprovoke priapism in males (Scher et al., 1983)and may increase libido in females (Gartrell,1986). Nefazodone is chemically related totrazadone. In addition to its effects inhibiting

Biological Treatments 287
the uptake of 5-HT and noradrenaline, it blocks5-HT2 receptors.
Amoxapine
This is a demethylated metabolite of the antipsy-chotic drug loxapine, a tricyclic drug of thedibenzoxazepine class. It is rapidly absorbed fol-lowing oral administration, and has a half-lifeof eight hours. It has minimal anticholinergicproperties, but does block dopamine receptors,which contributes to its side-effect profile. Thisincludes extrapyramidal reactions and hyper-prolactinaemia, but in addition seizures may bea problem.
L-tryptophan
Some of the literature that relates to the antide-pressant properties of tryptophan is discussedin Chapter 8. It is an essential amino acid,and its antidepressant effects, potentiated inparticular by MOAI drugs, form part of theevidence for implication of 5-HT mechanisms indepression. It possesses no anticholinergic, anti-adrenergic or dopaminergic properties, with ahalf-life of around four hours. It may, in addi-tion, be usefully combined with tricyclic drugs,in particular amityriptyline and clomipramine.It has few side effects other than drowsiness,although it has been linked to the developmentof an eosinophilic myalgia syndrome, whichhas limited its availability, although it is readilyavailable as a nonprescription product.
Venlafaxine
This selectively blocks the reuptake of 5-HTand noradrenaline. It has no muscarinic or his-taminic effects. It has a half-life of between
one and six hours, and an active metabolite.It is given twice daily, with a dose range of75–300 mg. Nausea, anorexia and insomnia arethe main side effects.
While it does not affect cardiac conduction,there are reports of increased blood pres-sure with the drug, especially with higherdoses. A once-daily preparation of the majormetabolite des-venlafaxine has a half-life of11 hours and the recommended dose range is50–400 mg daily.
Selective Serotonin Reuptake Inhibitors(SSRIs)
The main SSRIs in clinical practice are citalo-pram, escitalopram, fluoxetine, fluvoxamine,paroxetine and sertraline (see Table 12.2). Asnoted below, they block the 5-HT transporter,but this effect occurs in a matter of hours, theactivity of the 5-HT neurones slowly recoveringover the next 14 days (Montigny and Blier,1985).
Fluoxetine is a bicyclic drug with high selectiv-ity for inhibition of 5-HT uptake and virtuallyno effect on catecholamine neurones. It is theleast potent of the SSRIs for the inhibition of 5-HT uptake. It is highly protein-bound (95–99%)and has an active metabolite, norfluoxetine giv-ing a long half-life of 6–14 days. It reducesREM sleep and increases REM latency. Thereis a 90 mg extended-release formulation of thiscompound to be given once per week.
Fluvoxamine is a single-ringed compoundwith no anticholinergic properties which israpidly absorbed after oral administration andhas a half-life of approximately 15 hours. Itis extensively metabolized and its metabolitesalso have no effect on the catecholamine uptake
Table 12.2 Some properties of SSRI antidepressants
Drug 5-HT* 5-HT/NA** Half-life Active metabolite Protein binding
Citalopram 2.6 1500 36 hours None 50%Escitalopram 1.2 2000 30 hours None 60%Fluoxetine 25 20 1–3 days 7–15 days 94%Fluvoxamine 6.2 180 15 hours none 77%Paroxetine 1.1 320 20 hours none 95%Sertraline 7.3 190 25 hours 66 hours 99%
*Impramine = 100: inhibition of uptake.**Ratio of 5-HT to noradrenaline uptake inhibition.

288 Biological Psychiatry
process. Gastrointestinal side effects appearto be a particular problem, although it hasminimal effect on the EEG profile (Saletuet al., 1983). It has a half-life of approximately15 hours, and can therefore be given on a once-daily basis.
Paroxetine is one of the more highly selectiveof the group for 5-HT, and has no active metabo-lites. It does however inhibit its own clearance;its half-life therefore increases with higher dose.Agitation as a side effect is not reported.
Sertraline has long-acting metabolites, andsexual side effects have been more prominent.It too is highly protein-bound (98.5%) and has ahalf-life of 13–45 hours.
Citalopram is sold as a racemic mixture, con-sisting of 50% R-(−)-citalopram and 50% S-(+)-citalopram. Only the S-(+) enantiomer has thedesired antidepressant effect, so it has been mar-keted by itself as escitalopram.
The main advantage of the SSRIs is the lackof cardiac effects, weight gain or sedation. Themain side effects that limit their use are nausea,diarrhoea, agitation or increased anxiety, anddelayed orgasm and reduced sexual drive.Others are mainly CNS-related, includinginsomnia, dizziness, tremor and extrapyrami-dal reactions (see below). The SSRIs do show aneffect on dopamine uptake, this being strongestfor sertraline and weakest for fluvoxamineand citalopram.
The metabolites of citalopram, fluvoxamine,paroxetine and sertraline are inactive, and thepotential for interactions with other drugs istherefore less than with fluoxetine. It is recom-mended that at least a four-week interval isallowed when switching from fluoxetine toan MAOI.
The dose prescribed depends on the prod-uct, but, unlike the tricyclics, there is oftenlittle to be gained when treating depression byincreasing the dose if a response is not obtainedwith the recommended prescription. Markedlyhigher doses of the SSRIs do have clinical ben-efits in patients with OCD. Some of the SSRIsare now being introduced as extended-releasepreparations.
Clinically the SSRIs have also been used totreat OCD, social phobia, migraine, bulimia and
panic disorder, the indications varying in differ-ent countries.
Some Other Novel or More RecentlyIntroduced Antidepressants
Viloxazine has minimal anticholinergic proper-ties. It is rapidly absorbed after oral adminis-tration, with maximal blood levels between 1and 4 hours and a half-life of 2–5 hours.In animal models it is a stimulant, and is aweak inhibitor of noradrenergic uptake. Ithas limited antihistaminic and anticholinergicproperties, but is mildly sympathomimetic. Itsmain disadvantages are nausea and vomiting,but, of the antidepressants, it has minimalconvulsant potential (Trimble, 1978). However,its use in epilepsy is inhibited because ofits adverse pharmacokinetic interaction withcarbamazepine (Pisani et al., 1984).
Mianserin is a tetracyclic compound whosemain mode of action appears to be as an antag-onist at the presynaptic alpha-adrenoceptor. Ithas antihistaminic but only minimal anticholin-ergic and serotonergic activity. Its biochemistryconfers certain advantages, for example mini-mal anticholinergic side effects and thus car-diotoxicity, although it is epileptogenic.
It is rapidly absorbed following oral admin-istration, peak plasma concentrations occurringin 2–3 hours. Its half-life is 10–17 hours, and it ishighly protein-bound. It possesses antidepres-sant activity at doses between 30 and 120 mgdaily, and it is customary to prescribe it as asingle night-time dose.
Blood dyscrasias have been noted, includingagranulocytosis, which are usually reversiblebut are an indication for blood monitoring.
Maprotiline is a tetracyclic drug which hasselectivity for blocking noradrenergic reuptake.It is low in anticholinergic effects, and mayeven have cardiac antiarrhythmic properties.It is well absorbed after oral administration,peak plasma levels being reached between 6 and19 hours, with a half-life around 30 hours. Thismakes it ideal for single daily administration.It has antidepressant effects equivalent to tri-cyclic drugs, but seizures are a specific problem,particularly at higher doses (Trimble, 1980).

Biological Treatments 289
Iprindole is a weak inhibitor of both nora-drenaline and 5-HT uptake, with relatively weakantidepressant action. Like mianserin, its lack ofeffect on traditional monoamine systems is onepiece of evidence which has led to questioningof the classical neurotransmitter hypothesis ofaffective disorder.
Bupropion has a single-ring novel structurethat has no effect on 5-HT or noradrenaline up-take, and does not inhibit monoamine oxidase. Itmay block dopamine reuptake and has a chem-ical structure which resembles amphetamine.It is not associated with weight gain or sexualdysfunction but at higher doses it provokes sei-zures. It has comparable efficacy in depressionto the SSRIs and is also used for nicotine crav-ing. It is available as a slow-release preparation.
Mirtazapine has a tetracyclic chemical struc-ture. It is a noradrenergic, being an antagonistat alpha-2 receptors, and is a specific seroton-ergic agent acting as an antagonist of 5-HT2and 5-HT3 receptors (NaSSA). It has minimalanticholinergic, 5-HT-related or adrenergic sideeffects, but antihistaminic effects (drowsinessand weight gain) are prominent. The alpha-2receptors, located in the locus coeruleus, controlthe firing rate of serotonergic neurones; the drugthus increases hippocampal 5-HT release.
Novel drugs with antidepressant action in-clude the 5-HT1A agonist buspirone, the tricyclictianeptine, the phosphodiesterase-inhibitorrolipram and the 5-HT–noradrenaline-reuptakeinhibitor (SNRI) duloxetine. Tianeptine isdescribed as a selective 5-HT-reuptakeenhancer (SSRE) since, unlike conventionaltricyclic antidepressants or SSRIs, tianeptineenhances the reuptake of 5-HT instead ofinhibiting it. It does not bind to adrenergic ordopaminergic receptors or transporters but mayinfluence glutaminergic transmission, and itseffects on the stress-induced neuronal changesin the hippocampus in particular have been afocus of interest.
The Mode of Actionof Antidepressant Drugs
The mode of action of tricyclic drugs has tra-ditionally been related to their ability to inhibit
monoamine uptake within neurones of the CNS,or to influence the uptake and distributionof other neurotransmitters. This is shown byexample in Figure 12.2, which shows variouscompounds that influence the glutamate sys-tem and Figure 1.14 for the 5-HT system. Cer-tainly this is a common biological activity thatmost of them share. However, it occurs acutely,while their therapeutic effect may take sev-eral weeks to become apparent. In addition,compounds such as mianserin and iprindoleminimally inhibit amine uptake in vivo. Atten-tion has been paid to the chronic effects ofthese and other antidepressant treatments onthe sensitivity of catecholamine receptors, inparticular downregulation of β-receptor activ-ity. This leads to a decrease in glycogenolysisin the postsynaptic cell, small changes at thereceptor being magnified through the coupler,effector and amplifier system of the postsynapticcell membrane into larger dynamic changes. It isknown that an intact 5-HT system is required forthe beta-receptor changes to occur. These datahave led to hypotheses that relate depressive ill-ness to a supersensitivity at these receptor sites,itself related to decreased intrasynaptic levelsof neurotransmitters, such as 5-HT. The mecha-nism of the downregulation and subsensitivityof noradrenergic receptors by antidepressants isunclear, but it could be related to a change ofaffinity, a reduction of density or interferencewith cyclic AMP coupling or activity.
However, several antidepressants, such asmianserin, paroxetine, citalopram and fluo-xetine, fail to downregulate beta receptors,implying that these changes alone are notsufficient. Another theory relates to the alpha-2adrenergic receptor, since long-term but notshort-term antidepressant treatment reducedthe sensitivity of the alpha-2 autoreceptor. Thefunctional effect of this is to increase noradrener-gic impulse flow and turnover with behaviouralactivation (Charney et al. 1983). Although someantidepressants, for example amitryptiline,desipramine and imipramine, have been shownto reduce alpha-2 autoreceptor sensitivity, atpresent information on other drugs, particularlyin patient studies, is limited. Nonetheless, thesefindings are in keeping with a hypothesis that

290 Biological Psychiatry
Presynapticterminal
Glial cell
Glial uptake
Glycine site
AMPA receptorGlutamate
AMPANBQX (–)
GlutamateKainateDomoic acid
LY382884 (–)
Kainate receptor Metabotropic receptor NMDA receptor
Gp I Il GlutamateNMDAAspartate
ifenprodil (–)Mg++(–) 7CK (–)
MK801 (–)Ketamine (–)
AP5 (–)
mGlu1 2 4 55 3 7 8
III
Postsynapticcell
Neuronal uptakeGLUTAMINE
GLUCOSE
GLUTAMATE
Figure 12.2 Synaptic cleft, showing the influence of some drugs on the glutamate system (reproduced withpermission from Webster, 2002)
hypersensitivity of the presynaptic receptors indepression is associated with decreased releaseof neurotransmitters and upregulation of thepostsynaptic beta receptor. Antidepressantsthus regulate the presynaptic receptor andnormalize the postsynaptic receptor. The asso-ciation of these findings to the decreased post-synaptic alpha-2 activity in depressed patients(Siever and Uhde, 1984) is unclear. It is ofinterest that mianserin is an alpha-2 presynapticreceptor antagonist, an action which may berelevant to its antidepressant action.
There has been much interest in serotonergicmechanisms since the introduction of the SSRIs.It is not known how these drugs work, butsome findings are secure. All types of antide-pressant therapy, including ECT, MAOI andlithium, increase 5-HT neurotransmission. Theeffects of antidepressant action can be reversed
by reducing brain 5-HT through the techniqueof tryptophan depletion (Delgado et al., 1990).Following administration of an SSRI there is con-siderable acute release of 5-HT into the synapticcleft, and this is followed by a dramatic decreaseof related neuronal activity. Gradually the func-tions of the neurones resume, and the 5-HT2receptors are normalized (see Figure 12.3).
There is considerable debate over wherethese effects take place, and what is primary.It has been speculated (see Chapter 8) that indepression, with reduced 5-HT turnover, thereis decreased transmission at the pre- and postsy-naptic 5-HT1A receptors and the 5-HT2 receptoris upregulated. With SSRIs, the biological effectis seen mainly at the raphe nuclei, which have ahigh density of 5-HT1A autoreceptors. One spec-ulation is that SSRIs block the transporter at theraphe, increasing the release of 5-HT around the

Biological Treatments 291
(b)
(a)
(c)
5-HT 5-HT
5-HT
5-HT 5-HT
SSRI SSRI
SSRI SSRI
5-HT transporter5-HT1A receptor
5-HT1B receptor5-HT1A receptor(desensitised)
5-HT
Figure 12.3 Schematic representation of the effectsof SSRI drugs on 5-HT neurones. (a) 5-HT is releasedfrom neurones within the raphe nuclei and takenup by the 5-HT transporter. (b) Blockade of thetransporter increases the concentration of 5-HT andactivates the 5-HT1A autoreceptors, which hyper-polarises the neurone, reducing 5-HT release fromforebrain terminals. (c) The increased extracellular5-HT concentration with continuous treatment desen-sitises the raphe 5-HT1A autoreceptors, allowing the5-HT neurones to recover cell-firing and the terminalrelease of 5-HT (reproduced with permission fromWebster, 2002, p. 445)
raphe, probably from the local dendrites, whichthen acts as an agonist, activating the autorecep-tor, and decreasing cell firing and the release of5-HT. With continued treatment there is desensi-tization of the autoreceptor (leading to increased5-HT synaptic transmission) and resumptionof normal firing. Further, postsynaptic 5-HT1Areceptors in the hippocampus and 5-HT2 re-ceptors are also normalized (see Figure 12.3).
The 5-HT1A receptor is the main 5-HTinhibitory receptor, and is found in high
concentrations in the raphe but also in thepregenual cingulum, temporal cortex, anteriorcingulum, orbitofrontal cortex and olfactorycortex. It can be quite reliably imaged withligands such as 11C-WAY and 18-F MPPFand is reduced in depression, panic disorderand social-anxiety disorder, all of which areconditions that respond to SSRIs. As noted, theeffect of the SSRIs at the 5-HT1A raphe receptorsis partly responsible for their action, somehowleading to a resetting of the neuronal systemwith eventual increased release of 5-HT into thesynaptic space (Neumeister et al., 2006). 5-HT1Apartial agonists (gepirone, vilazedone) are thusbeing examined as potential antidepressantswhen combined with SSRIs, to see if the effectof the latter can be advanced or enhanced.
The importance of the 5-HT1A receptor fortherapeutics goes beyond the antidepressantshowever, since some of the atypical antipsy-chotics (ziprazidone, quetiapine, clozapine) alsopossess 5-HT1A partial agonist activity, althoughothers (sertindole, risperidone) have low affin-ity, as do the first-generation antipsychotics.Since some of the atypical antipsychotics havean effect on mood stabilization (see below), the5-HT1A receptor activity may be relevant to theirtherapeutic effect.
The role of the 5-HT transporter (5-HTTLRP)in clinical antidepressant response is beinginvestigated. Thus, those with the 5-HTTLRP ssallele have a threefold decrease in transportersand 5-HT uptake (Hariri et al., 2002). Onimaging, these depressed subjects with theshort allele have been shown to have moreresponsive amygdala to angry and fearful facesthan do the long-allele ll carriers, and showenhanced startle responses. At present, inves-tigations into drug-responsiveness and pheno-typic status are ongoing.
Tricyclic drugs may not act in the sameway; one suggestion is that their response ismore via the hippocampal postsynaptic 5-HT1Areceptors. In any case, enhanced responsivity offorebrain 5-HT neurones seems to be a commonresponse to long-term treatment with both theSSRIs and tricyclic drugs.
Most antidepressants decrease the receptordensity of 5-HT2 receptors in the frontal

292 Biological Psychiatry
cortex, an effect which distinguishes themfrom ECT, which increases 5-HT2 receptors.As a generalization, therefore, antidepressantsand ECT downregulate alpha-2, beta and5-HT1 receptors, but their action on the 5-HT2receptor differs.
One major difficulty for the discovery of newantidepressant treatments has been to find ananimal model for depression that closely resem-bles the human condition. The most widely usedare the forced swim test, in which animals areplaced in water and the length of time theystruggle before giving up is measured, and thelearned helplessness model, a state provokedby enforced foot shock. Further, for two gener-ations drugs which act on monoamine systemshave been targeted for investigation, but thetrend has been to develop drugs with morethan one monoamine target, with minimal effectat other receptors, which may relate to sideeffects. However, antidepressants have an effecton glutamate receptors, tricyclics, ECT, MAOIsand some SSRIs, decreasing NMDA receptorfunction (Kilts, 1994). Sigma receptors modu-late several central neurotransmitters, includingglutaminergic and monoaminergic systems, andthey have been considered possibly relevant forthe action of some antidepressants. Fluvoxam-ine is the most potent sigma-receptor agonist;sertraline has low affinity or may even be anantagonist; and venlafaxine has no effect.
The CRF system has been a longstandingfocus of interest, although disappointing interms of new medications that act within it. Es-sentially, stress leads some people to depres-sion, and the hypothalamic–pituitary–adrenal(HPA) axis is involved in this relationship. Inanimals, CRF increases locomotor activity andenhances stress-induced freezing. Increasedactivity of the HPA axis leads to increased cor-tisol release, decreasing central glucocorticoidreceptors and potentially doing harm to somecerebral structures, notably the hippocampus.Chronic increased CRF secretion may underliethese HPA axis changes noted in depression.However, CRF-receptor antagonists to datehave been ineffective in depression and anxietyclinical trials.
Observations that structural changes inthe brain may accompany depression, in partrelated to the altered HPA-axis activity, notablyin the amygdala, hippocampus and prefrontalcortex (see Chapter 8), have coincided withfindings from animal models that several psy-chotropic agents, especially antidepressants,may induce synaptogenesis or neurogenesis.Neuroplasticity has become an exciting areaof research, and may be one mechanism ofantidepressant action.
Attention is also now focussing on transcrip-tion factors that mediate between receptor activ-ity and cellular genetic expression. CREB, thetranslocation of glucocorticoid receptors to thecell nucleus and alteration of m-RNA expressionafter antidepressant administration in animalmodels are all current areas of research.
There are several genetic candidates whichmay link outcome of treatment with antide-pressants, including genes related to the 5-HTtransporter, polymorphisms of 5-HT-receptorgenes and the val/met polymorphism of theBDNF gene (Lee et al., 2009; Kim et al., 2008).
Some General Principles of Treatment
Although many of the newer drugs seemto have equivalent clinical efficacy with theestablished tricyclic drugs, their main benefitmay lie in having less side effects, particularlythose related to anticholinergic activity. Manyof them, for example mianserin and the SSRIs,are much safer in overdose. Some 15% of allfatal poisonings are due to tricyclic drugs, and3.3% of tricyclic overdoses have a fatal out-come. Amitriptyline and related tricyclics areresponsible for approximately 1.66 deaths bysuicide per 10 000 patients prescribed the drug,whereas the comparable figure for mianserin isaround 0.13; historically before the widespreaduse of SSRIs 82% of deaths from antidepressantoverdose were due to two drugs, amitryptilineand dothiepin (Henry et al., 1995). There are alsomajor differences between the drugs in regardto their sedative properties, some of whichare related to their antihistaminic action. Themore sedative compounds include amitripty-line, trimipramine, dothiepin, clomipramine,

Biological Treatments 293
mianserin and mirtazepine, while less sedativeare protriptyline and some of the newerselective 5-HT uptake inhibitors and their suc-cessors. The clinical implications of this are thatpatients with depression that require sedation,either because of anxiety, agitation or insomnia,may do better on the more sedative compounds,whereas those with psychomotor retardationrequire less sedation. If insomnia is prominentthen the whole of the prescribed dose should begiven at night-time, so that maximum sedationis obtained without the need for additional hyp-notic drugs. Some patients, especially the elderlyor those with heart or urinary problems, will beunable to tolerate the anticholinergic propertiesof some of the drugs, and those with minimalanticholinergic activity will be required.
Choice of antidepressant needs therefore totake into account the clinical pattern of thedepression, the age of the patient and addi-tional medical diagnoses. It is helpful to take adrug history from the patient and to find out ifany close relative has had a depressive illnessand, if so, to which drug they have responded.If a patient has been reliably treated before ona particular compound and has suffered fewside effects from it, it is logical to start on thesame preparation, unless there are contraindi-cations. Potential suicide risk may be one ofthese, and drugs which are safe in overdosesuch as the SSRIs have obvious advantages.Venlafaxine is more associated with seizures,and citalopram leads to a prolonged QT inter-val following overdose, related to its metabolitedidesmethylcitalopram.
It is wise, especially if the patient has pre-viously experienced side effects or has someassociated medical problem such as a seizuredisorder, to start on low doses and build up theprescription over the ensuing one or two weeks.Polypharmacy should be avoided, however, andno patients should require an additional hyp-notic to an antidepressant if a sedative antide-pressant can be given as a single night-time dose.Useful combinations, apart from those withMAOI drugs, include L-tryptophan (if available)and clomipramine, or clomipramine and lithiumin intractable cases. Some preparations are stillavailable which combine antidepressants and
phenothiazines, for example motival, which isfluphenazine and nortriptyline. If possible, theseshould be avoided. In non-responding patients,higher than usual doses may be prescribed, theincrements being given until side effects occuror a clinical response is obtained. Once started,an antidepressant should be continued, if suc-cessful, for 6–12 months.
Pharmacology
Serum-level monitoring of antidepressant drugscan be undertaken. It is usually carried out usinggas–liquid chromatography, although radio-immunoassay and mass spectrometry are alsoused. With regards to the tricyclic drugs,following absorption they are metabolized bymethylation and hydroxylation in the liver,before passing into the circulation, where theyare strongly protein-bound. Tertiary tricyclics,for example imipramine and amitriptyline,are demethylated to secondary amines, whichthemselves possess antidepressant properties.They are absorbed well and rapidly, peakplasma concentration occurring in 2–6 hours,although marked variation between patients isnoted in terms of the serum levels for identicaldoses of medication. The half-lives are variable,from 8 hours for imipramine to over 80 hoursfor protriptyline. They are highly bound toplasma protein, with about 10% circulating asfree drug.
Most of the studies that have examinedthe relationship between clinical response andserum levels have measured total rather thanfree levels. Further, since the presence of meta-bolites has to be taken into account, it is hardlysurprising that the results obtained are difficultto interpret. Some authors have claimed thata therapeutic window exists, such that levelsbelow or above this lead to poor results. This hasmainly been noted with nortriptyline (Sørensenet al., 1978). In contrast, for imipramine, therelationship is linear, levels below 150 ng ml−1
(540 nmol l−1) being less effective (Glassmanet al., 1977). In general it may be said thathigh levels of drugs are more likely to leadto side effects, while patients with low levelsrespond poorly.

294 Biological Psychiatry
Table 12.3 CYP enzymes inhibited by differentpsychotropic drugs
CYP isoenzyme Antidepressants Antipsychotics
CYP1A2 FluvoxamineCYP2C9/10/19 Fluoxetine Thioridazine
Sertraline ClozapineFluvoxamineMoclobemide
CYP2D6 Fluoxetine ThioridazineParoxetine HaloperidolSertraline Clozapine
OlanzapineRisperidone
CYP3A4 Fluoxetine ChlorpromazineSertraline ThioridazineNefazodone Haloperidol
RisperidoneThioridazine
In practice, measurement of serum levels ishelpful in patients not responding as expectedon good clinical doses of the drug, or in patientsapparently experiencing side effects on smalldoses. It may also be useful in monitoringcompliance where this is suspect. Interactionsbetween tricyclic drugs and others show that
barbiturates and some other anticonvulsantslower, while major tranquillizers raise, theserum levels of antidepressants, these effectsmainly occurring by alteration of activity ofmetabolizing enzymes in the liver.
The SSRIs tend to have nonlinear pharma-cokinetics, but this has little clinical relevance,and to date no relationships have been shownbetween serum levels and either clinicalresponse or side effects.
The cytochrome 450 isoenzymes 1A2, 2C,2D6 and 3A4 are important in the meta-bolism of psychotropic drugs, especially 2D6.Fluoxetine, paroxetine and sertraline havesimilar inhibitory effects on the 2D6 enzyme,and increased levels of some concomitantlyprescribed drugs, for example tricyclic drugsor some antipsychotics, may be expected.Sertraline and fluoxetine inhibit 3A4, whichmediates the metabolism of carbamazepine,and thus may increase levels of the latter if bothclasses are coprescribed. A list of enzymes isshown in Tables 12.3 and 12.4.
A general list of side effects with antidepres-sants is shown in Table 12.5. Some of these occur
Table 12.4 CYPs enzymes involved in psychotropic drug metabolism
CYP1A2 CYP2C9/10 CYP2C19 CYP2D6 CYP3A4
Antidepressants Anticonvulsants Antidepressants Antidepressants AntidepressantsAmitriptyline Phenytoin Amitriptyline Fluoxetine AmitriptylineClomipramine Antipsychotics Citalopram Paroxetine ClomipramineImipramine Thioridazine Clomipramine Mianserin DesipramineTrazodone Olanzapine Imipramine Venlafaxine ImipramineFluvoxamine Moclobemide Trazodone NorclomipramineAntipsychotics Anticonvulsants Nefazodone NortriptylineChlorpromazine Mephenytoin Amitriptyline TrimipramineHaloperidol Esobarbital Clomipramine NefazodoneClozapine Mephobarbital Desipramine FluoxetineOlanzapine Imipramine SertralineZiprasidone Norclomipramine Venlafaxine
Nortryptiline AntipsychoticsTrimipramine HaloperidolMaprotiline ClozapineSertraline RisperidoneAntipsychotics ZiprasidoneChlorpromazine IloperidoneThioridazine QuetiapineHaloperidol AnticonvulsantsOlanzapine CarbamazepineRisperidoneIloperidoneQuetiapine
CYP; Cytochrome, Data from [23–25, 29].

Biological Treatments 295
Table 12.5 Some side effects of non-MAOI antide-pressant drugs
Sedation DyskinesiaDry mouth Myopathy, neuropathyPalpitations and
tachycardia, changeson the ECG
Convulsions
Visual difficulties AtaxiaPostural difficulties DeliriumPostural hypotension AgitationNausea, vomiting,
heartburn,G. I. bleeding
Transient hypomania
Constipation DepersonalizationGlaucoma AggressionUrinary retention,
impotence, delayedejaculation
Jaundice (cholestatic)
Paralytic ileus Weight gainGalactorrhoea Impairment of cognitive
functionSweating RashesFever Extrapyramidal reactionsTremor Psychosis
frequently but may be tolerable, for exampledry mouth, while others are rarer and canbe very discomforting, such as dyskinesias orseizures. Some may be used therapeutically, forexample the hypnotic effect. As noted, gener-ally the SSRIs have less side effects than tricyclicantidepressants.
Much attention in the past has been paidto some specific side effects, in particular car-diac and neurological problems. Tricyclic drugsincrease the atrioventricular conduction time(Burrows et al., 1976) and can convert a par-tial to a complete heart block. In overdose theyprovoke a variety of arrhythmias, these beingthe commonest cause of death from overdose.The antidepressants with minimal anticholiner-gic effects, including the newer selective-uptakeinhibitors, are safer in this regard. In one study,a comparison between fluoxetine and amitripty-line, an increased heart rate and prolongation ofthe P–R interval and QRS complex were notedwith the tricyclic drug but not with fluoxetine(Fisch, 1985). Venlafaxine has been associatedwith a mildly increased blood pressure, espe-cially in doses above 300 mg per day,
Nearly all the non-MAOI antidepressantslower the seizure threshold and may precipitate
seizures, with the possible exception of vilox-azine and nomifensine (Trimble, 1978). Themechanism of this side effect is not understood,although it may be related to interference withmonoamine or GABA activity. Thus patientswith organic neurological disease, who mayhave a lowered seizure threshold, should beprescribed tricyclic drugs with caution. Themanagement of epileptic patients is discussedbelow.
Impairment of cognitive function and perfor-mance on psychological tests probably occurswith most of the non-MAOI drugs, althoughthis has not been well evaluated. Most stud-ies are single-dose or short-term in volunteers,and while patient data tend to show improve-ment of cognitive function on antidepressanttherapy, this may well be due to the relief ofthe cognitive effects of the depression ratherthan the antidepressant per se. Evidence fromhealthy volunteers suggests differences betweendrugs, for example imipramine, amitriptylineand mianserin give the most detrimental effects,while nomifensine and viloxazine are associatedwith the least problems (Thompson and Trim-ble, 1982b). The SSRIs are also more beneficialin this regard and there are reports of alertingeffects with some of them (sertraline, fluoxetine,paroxetine).
Flu-like reactions have been described withseveral compounds, including zimelidine andnomifensine, with headaches, joint pains andelevation of liver enzymes. The 5-HT syndromeis a potentially life-threatening adverse effectthat may occur following therapeutic use ofSSRIs, notably with inadvertent interactionswith other agents such as the MAOIs or withoverdoses. It is related to excess 5-HT activityin the CNS and peripheral nervous system.The main symptoms, which can be mild andcome on quite quickly, are flu-like, but includetachycardia, mydriasis, myoclonic jerks andincreased superficial reflexes on neurologicalexamination. When more severe, there is hyper-tension and fever, and behavioural agitation.Severe cases may lead to rhabdomyolysis,seizures, renal failure and rarely disseminatedintravascular coagulation. There are similaritiesin the presentation of this syndrome and theneuroleptic malignant syndrome (see below),

296 Biological Psychiatry
although CPK changes are usually not raised inthe 5-HT syndrome.
Weight gain is a particularly difficult problemfor patients, and this is not solely attributable toan increase in appetite. With the SSRIs weightmay initially be lost, then regained later intreatment, in some cases leading to weightgain. A withdrawal syndrome on stoppingantidepressants after long-term treatment hasbeen reported. Symptoms include anxiety,panic, abdominal cramping, vertigo, dysas-thesias, vomiting and diarrhoea. In addition,insomnia with nightmares, some restlessness,and occasionally hypomanic, manic or evenpsychotic pictures have been described. Theseflu-like withdrawal syndromes generally tendto occur in patients who have been on higherdoses for long periods of time and who stoptheir drugs suddenly. They can be avoided bycareful reduction of dosage and by warning thepatient at the time of initial prescription not tosuddenly stop taking their medication. With theSSRIs they are reported most with paroxetine,and are also noted with venlafaxine.
It has been known for many years that para-doxical excitation and increased motor activitycan be seen with the prescription of antide-pressants, and that this may lead the immobiledepressed but suicidal patient to become activeand act on their suicidal ideation. Similar acti-vation has been reported with some of theSSRIs, and there is a continuing controversyas to whether they may induce suicide in somepatients. There are analyses which suggest thatthe odds ratio of suicide attempts is increasedwith the SSRIs compared with placebo, but notagainst tricyclic agents (Fergusson et al., 2005),and some epidemiological data note that the sui-cide rate has fallen with increasing use of SSRIprescriptions (Gibbons et al., 2005). The FDAinserted a black-box warning concerning thesein children and adolescents, and prescriptionsfell. These data imply a need to closely observepatients as they are started on antidepressantsfor signs of increasing suicidal ideation.
ANTIPSYCHOTIC DRUGS
The term ‘antipsychotic’ for this group of drugsimplies that their most important action is to
lyse psychotic symptoms. Other terms that havebeen used for this class include ‘major tranquil-izer’ (to be contrasted with ‘minor tranquilizer’)and ‘neuroleptic’ (a compound that tranquilizesbut does not sedate).
These drugs naturally fall into four groups:phenothiazines, butyrophenones, thioxanthinesand others. The phenothiazines have a tricyclicnucleus in which different configurations of theside chain lead to alteration of their properties.Three subgroups are recognized, one with analiphatic side chain, such as chlorpromazine,one with a piperidine side chain, such as thior-idazine, and one with piperazine side chains,such as trifluoperazine. The thioxanthines havea structure similar to the phenothiazines andinclude clopenthixol, flupenthixol, thiothixineand related drugs.
The butyrophenones, such as haloperidol,and related diphenylbutylpiperidines, such aspimozide, fluspiriline and penfluridol, have adifferent chemical structure, and some drugs,for example fluspiriline and penfluridol, arelong-acting oral preparations. Other antipsy-chotics include molindone, reserpine, tetra-benazine, oxypertine, loxapine and the so-calledatypicals, which include clozapine and thesubstituted benzamides, such as sulpiride.
The distinguishing property of all the stan-dard antipsychotic drugs is their ability to blockdopamine receptors. In addition they may evokeextrapyramidal symptoms of various types.They all inhibit apomorphine-induced stereo-typy and agitation in animal models; provokean acute increase in dopamine turnover withraised HVA levels in areas such as the corpusstriatum, nucleus accumbens, olfactory tubercleand frontal cortex; block the stimulation ofdopamine-sensitive adenylate cyclase; and dis-place receptor binding with H3 dopamine or H3spiroperidol at postsynaptic dopamine receptorsites. The relative receptor binding profiles forsome of these drugs are shown in Table 12.6.
The most potent dopamine-receptor antag-onist used clinically is benperidol, whilepimozide is the most specific. With few excep-tions, the ability of these drugs to block thereceptor correlates with their clinical antipsy-chotic action. Since the majority readily pro-voke extrapyramidal effects, it has been

Biological Treatments 297
Table 12.6 Receptor-binding properties of neuroleptics
DA 5-HT Alpha adrenergic Histamine ACh
Benperidol + + + + + ± ± – –Droperidol + + + + + + + – –Haloperidol + + + + + – ± – –Pimozide + + + + + – – – –Bromperidol + + + + + – ± – –Fluspiriline + + + + + + – – –Thiothixine + + ++ + ± + –Trifluoperazine + + ++ ± ± ± –Perphenazine + + ++ + – + –Flupenthixol + + ++ + + ± –Fluphenazine + + + + + + –Penfluridol + + + – – – –Chlorprothixine + + + ++ ++ ++ ++Clozapine + + + ++ ++ + + + + + +Risperidone + + + + + + ++ ++ –Thioridazine ++ + ++ + ++Chlorpromazine ++ ++ + + + + + + ++Sulpiride + – – – –Promazine ± + + + + + + + + + +Quetiapine + + + + +Ziprasidone + ++ ++ + _Olanzapine + + + ++ + + +Aripiprazole + + + + _
suggested that the antipsychotic potential isdue to antagonism of dopamine receptors inthe mesolimbic or mesocortical areas of thebrain, while the motor effects relate to thenigrostriatal system. There are a few drugs thatappear to possess minimal potential to evokeextrapyramidal effects, especially thioridazineand clozapine. One explanation for this has beenthe anticholinergic potential of these drugs,which may counteract the tendency to provokeextrapyramidal symptoms. Alternatively, it hasbeen suggested that some, especially the atyp-icals, preferentially act on dopamine receptorsin mesolimbic areas, rather than at the stria-tum. Although studies examining dopaminemetabolites do not confirm a preferentialincrease in levels when comparing mesolimbicto striatal structures for various neuroleptics,those examining the disappearance or releaseof dopamine from selective sites do supporta suggestion of a more preferential action inmesolimbic areas for these compounds (Leysenand Niemegeers, 1985; Scatton and Zivkovic,1984). Since for example sulpiride does not haveanticholinergic properties, it would seem that
the most likely explanation for these differingclinical effects of some of the antipsychoticsrelates to differential blockade of dopaminereceptors in limbic as opposed to striatal areas.
These biochemical differences have given riseto the concept of atypical neuroleptics. Thesedrugs weakly antagonize dopamine-inducedstereotypies, but do not induce catalepsy. Theydo not lead to an upregulation of D2 receptorsin striatal structures or to the development oftolerance of increased dopamine turnover withchronic treatment. Clozapine is the paradigm.
When typical neuroleptics are given chroni-cally, it is shown in animal models that toler-ance occurs, and in patients initially elevatedHVA levels in the CSF tend to decrease aftera few weeks of drug administration (Post andGoodwin, 1975). However, it seems that thistolerance is observed in the striatum but notin mesolimbic and mesocortical dopaminergicsystems (Scatton and Zivkovic, 1984), possiblyexplaining the clinically effective antipsychoticaction of these drugs, which persists over time.
It should be noted that of the varioussubclasses of dopamine receptors described,

298 Biological Psychiatry
Table 12.7 D1 and D2 receptor-site antagonism
D1 D2
Pimozide + + + ++Butaclamol + + ++ + + ++Chlorpromazine ++ + + +Thioridazine ++ + + +Flupenthixol + + ++ + + +Haloperidol ++ + + ++Sulpiride − + + +Clozapine ++ ++Fluphenazine + + + + + +Risperidone ± + + +Quetiapine + +Aripiprazole + +Ziprasidone ++ ++Olanzapine ++ ++
antagonism of the D2 receptor is related to manybehavioural effects. Table 12.7 shows a compari-son of the antagonism at D1 and D2 receptors forsome neuroleptic drugs. However, clozapineshows equal occupancy at the D1 and D2receptors, and has a potent effect at D4 receptors(Seeman, 1992). Risperidone has high affinity forD2, D4, 5-HT2 and alpha-adrenergic receptors,but acts only weakly at the D1 site. Quetiapineis antagonistic at the D1 and D2 dopaminereceptor, the alpha-1 and alpha-2 adrenergicreceptor, the histamine H1 receptor and the5-HT1A and 5-HT2 5-HT receptor subtypes. PETdata have shown that the D2 receptor occupancyof quetiapine rapidly dissociates, which theoret-ically may minimize the risk of extrapyramidaland prolactin-related side effects. Ziprasidonehas a high affinity for D1 and D2, 5-HT2Aand alpha-adrenergic receptors and a mediumaffinity for histaminic receptors. Amisulpirideis quite specific for D2 and D3 receptors, butlike other benzamides activates the endogenousGABA receptor. Olanzapine is structurally sim-ilar to clozapine, and has a higher affinity for5-HT2 receptors than D2 receptors, with loweraffinity for histamine, cholinergic muscarinicand alpha-adrenergic receptors. Aripiprazole isa partial D2 and 5-HT1A agonist, and a 5-HT2Aantagonist with moderate affinity for his-tamine and alpha-adrenergic receptors, and noappreciable affinity for cholinergic muscarinicreceptors. Zotepine and sertindole are other
atypicals with both D2 and 5-HT2 antagonisteffects, which are marketed in some countries.
In general, the rank order of the potency ofthe drugs for interaction with the D1 receptoris unrelated to any of the behavioural testsof measuring dopaminergic activity, and asyet the relationship of this receptor to CNSfunction is undetermined. However, the D2-receptor binding does correlate with effects onbehavioural tests of dopaminergic function,and probably relates to their antipsychoticfunction. Following treatment with these drugs,it has been shown in animal models that thenumber of D2-receptor binding sites increases,and on drug withdrawal slowly revert topretreatment values (Leysen and Niemegeers,1985). Other effects mediated by the D2 receptorare dopamine-activated locomotion, prolactinrelease, dopamine-induced vomiting andimpaired learning, noted following adminis-tration of dopamine antagonists. The alpha-1adrenergic blockade is related to cardiovascularproblems including hypotension, tachycardiaand sedative effects; the latter may be enhancedby any antihistaminic effect.
Although the effects of clozapine at the D4receptor have stimulated considerable interestas a significant potential interaction site toexplain its properties, it also antagonizes 5-HT2receptors. This, and the fact that other atypicalsalso antagonize the 5-HT2 system, has ledto a renewed interest in the role of 5-HT inschizophrenia.
SPECT and PET data have shown that clinicalresponse to neuroleptics in schizophrenia is notdirectly related to the amount of D2 blockade(Pilowsky et al., 1992), although low occupancy(<50%) is more likely in nonresponders andthe occurrence of extrapyramidal side effects ismore likely with high occupancy (Nordstromet al., 1993).
Following oral administration, chlorpro-mazine is easily absorbed and metabolized bythe liver, with peak plasma level occurring in1–3 hours. Its half-life is 17 hours. Some meta-bolites, such as the sulfoxide, have little phar-macological activity, while others, for examplethe hydroxy derivatives, are more potent. Itis strongly protein-bound, and preferentially

Biological Treatments 299
accumulates in the brain with a brain:plasmaratio of about 5:1. After termination of treat-ment, excretion of the drug or one of its meta-bolites may continue for several months.
Haloperidol is less rapidly absorbed, maxi-mal concentrations occurring around 5 hours,with a half-life of 13–20 hours. It is 90% protein-bound, and does not induce its own metabolism.Pimozide has a half-life of over 50 hours, andit is possible to give the drug on less than adaily basis. Once-weekly treatment has beentried successfully in maintenance therapy forpsychotic patients.
Clozapine is well absorbed, with peakplasma levels at 1–4 hours. It is 95% protein-bound, and metabolized through the liver witha half-life of about 14 hours. It is started atlow doses (25 mg once or twice daily) andincreased as necessary up to 300–600 mg a day.Because of the problem of agranulocytosis, itis essential to monitor blood counts, and therisk of seizures is increased with larger doses(5–10% over 600 mg). Other drugs which maybe associated with agranulocytosis such ascarbamazepine should be avoided. The inci-dence of extrapyramidal reactions, especiallytardive kinesia, is low, although there arereports of the neuroleptic malignant syndromeassociated with this drug, and akathisia iscommon. Patients often nonresponsive to otherantipsychotics have been reported to respond toclozapine; in particular, patients with negativesymptoms have done well. There may be arelationship between a low ratio of CSF HVA to5-HIAA and better response (Pickar et al., 1992).
Risperidone is also rapidly absorbed, witha half-life of about 24 hours. It has an activemetabolite, 9-hydroxyrisperidone. It seems tohave maximal antipsychotic efficiency at dosesof 6–10 mg daily, but with increasing dosesit provokes Parkinsonism, and dystonias andakathisia are reported. Ziprasidone has a shorthalf-life of 2–4 hours, quetiapine 6 hours,olanzapine 20–50 hours and aripiprazole6 days. The latter also has an active metabolite,dehydro-aripiprazole. The incidence of sideeffects with these drugs varies, but generallythe extrapyramidal ones are less than with theolder compounds. Quetiapine is available as a
sustained-release preparation, while paliperi-done is an extended-release preparation, beingthe main active metabolite of risperidone.
The dose of antipsychotic prescribed needs tobe titrated for individual patients against theirsymptoms, but in some cases large doses arenecessary. With drugs that are alpha-adrenergicblockers, for example chlorpromazine, cloza-pine and risperidone, such doses may lowerblood pressure and monitoring of the latter maybe necessary. It is usual in clinical practice tostart patients on oral medications, and oftenonce-daily prescription is possible. Followingcontrol of psychotic symptoms with oral ther-apy, especially if the patient has schizophrenia,a change to intramuscular preparations maybe preferred.
Esterified drugs, mostly dissolved in oil,are given intramuscularly, and released over avarying period of time, up to about four weeks.They include the older decanoate preparationsof haloperidol, fluphenazine, flupenthixol,and clopenthixol and fluspiriline. These drugsprovoke the same incidence of extrapyramidalproblems as do oral preparations, althoughthe onset may be more rapid (Ayd, 1974). Itmay have been expected that the use of intra-muscular preparations would have increasedcompliance and thus response. However, earlytrials comparing patients on injectable prepara-tions to oral pimozide suggest little differencein relapse rate (McCreadie et al., 1980), and thegrowth in the use of intramuscular therapieswaned with the introduction of the atypicals.Recently however, a number of the latter havebecome available as intramuscular preparations(risperidone, olanzapine, ziprazadone) andsome have been developed with different deliv-ery systems, such as oral olanzapine, whichdissolves on the tongue. In schizophrenia, oncetreatment has been started, it probably needsto be continued indefinitely. Discontinuation oftherapy leads to relapse in approximately 20%of patients in six months and 45% of patientsat one year (Curson et al., 1985). It is estimatedthat some 60–65% of patients will relapse overa 24-month period if not taking drugs, com-parable data for those in maintenance therapybeing 35%. Poor response to treatment relates to

300 Biological Psychiatry
younger age of onset of illness, prominent initialnegative symptoms, impairment of cognitiveperformance and an enlarged ventricular:brainratio on the CT or MRI scan.
A relationship between clinical response toserum levels of antipsychotics or plasma pro-lactin has not been demonstrated in schizophre-nia (Kolakowska et al., 1985). Maintenance withlow dose may reduce the long-term incidence ofside effects. Low doses of these drugs have beenused in other conditions, for example depres-sive illness, borderline personalities and anxietydisorders, although the use of those with a highpotential for extrapyramidal or metabolic sideeffects should be discouraged. The preferen-tial response of monosymptomatic psychosesto pimozide has been reported (Riding andMunroe, 1975), and for aggression, in particu-lar in patients with brain damage, clopenthixolmay have special value.
Antipsychotics are also used in the manage-ment of acute or chronic organic brain syn-dromes, and may be used in alcohol withdrawalstates, although their potential to lower seizurethreshold is a problem in this setting. Theiruse in the management of personality disor-ders remains controversial, and their use in theelderly is discouraged unless the indications foruse are very clear. An increased risk of cere-brovascular disease, stroke and bone fractureshas been reported with the atypicals in the geri-atric population. They should be used sparinglyand with caution in elderly patients.
There has been an accepted tendency touse atypical antipsychotic medications in themanagement of bipolar-spectrum disorders. Inthe past, on account of the high prevalenceof extrapyramidal side effects of the first gen-eration drugs, this was not considered goodpractice, except in the rapid resolution of acutemanic behaviours. The atypicals also have goodacute antimanic efficacy, and all are acceptablefor use in acute states, with the exception ofclozapine. The more difficult question relates totheir chronic use to prevent manic relapses. Thelicences for use vary across countries, but theprofile of effects is similar in clinical trials, evenfor side effects; again the exception is clozapine.Quetiapine seems to have the lowest potential
to provoke extrapyamidal reactions. In clinicalpractice, an atypical antipsychotic or valproicacid is added to lithium, but no study has testedthe hypothesis that two drugs are better thanone in this situation. Several of the atypicalantipsychotics have been shown to have antide-pressant effects in bipolar depression, and theyare thus now used widely for bipolar patientswho struggle with depression.
In some cases it is necessary to tranquillizepatients rapidly, and intramuscular or intra-venous doses may be given. In these situations,changeover to oral therapy should be carriedout as soon as possible. Side effects, such asacute dystonias, seem to be rare.
Side Effects
The side effects of the antipsychotics aresimilar to those listed for antidepressants(Table 12.5). Of particular interest, however, arethe extrapyramidal syndromes, which includedystonias, akinesia, akathisia, Parkinsonismand tardive syndromes.
In general, these disorders fall into twogroups, as shown in Table 12.8. In practice, someadmixture of symptoms is seen, and the divisionmay not be so clear. The acute disorders includeacute dystonias, akathisia, akinesia and Parkin-sonism. The chronic ones are mainly tardivedystonia and tardive dyskinesia. Acute dystoniais one of the earliest extrapyramidal side effectsand usually occurs within the first two or threedays of treatment. Typically, the movementsare uncoordinated and spasmodic, and mayinvolve the body, the limbs, the head and theneck. The jaws may be tightly clenched together,the tongue may be forcibly protruded and facial
Table 12.8 Extrapyramidal effects of psychotropicdrugs
Acute Chronic
Dystonia Tardive dyskinesiaAkathisia Tardive dystoniaAkinesiaParkinsonismRabbit syndrome

Biological Treatments 301
grimaces occur. Retrocollis, torticollis, antecol-lis, oculogyric crises or opisthotonos may all beseen. Males are preferentially affected and somesuggest that up to 50% of patients may developsome form of reaction following treatmentwith high-potency neuroleptics (Winslow et al.,1986). There are repeated spasms of muscleswith hypertonicity between attacks, and the con-dition can be distressing and painful. Dystonia isusually treated by intramuscular or intravenousadministration of an anticholinergic drug suchas benztropine or orphenadrine, althoughbenzodiazepines are also effective; it is thoughtto be caused by increased dopamine turnoverthat occurs following acute administration ofdopamine antagonists, stimulating dopaminereceptors not blocked by the action of the drugsand thus provoking the movement disorder.
Much more common is akinesia, which isusually seen within 24 hours of starting thedrugs. Patients have diminished spontaneousmovements, reduced facial expression andmay complain of fatigue. Muscle tone is notincreased, and the clinical picture may be mis-taken for an increasing apathy of depression orschizophrenia. It is usually helped by loweringthe dose of the antipsychotic or adding ananticholinergic drug.
Akathisia is sometimes less acute, but occursvery frequently, affecting over 50% of patients.It is characterized by a subjective sense of rest-lessness and presents as motor hyperactivity,with shifting posture and inability to sit orstay still for more than a few moments. It thusresembles agitation, and may lead to a mistakendiagnosis of agitated depression, or a deterio-ration of the psychosis if unrecognized. Somepatients have added orofacial dyskinesia; thusboth disorders can occur in the same patient.Akathisia usually responds to a reduction ofdose or to the administration of anticholinergicor benzodiazepine drugs. Since similar clinicalpictures have been reported in patients follow-ing L-dopa therapy in Parkinson’s disease, it isthought that it somehow relates to abnormalitiesof dopamine transmission in the basal ganglia.
The classical picture of Parkinsonism, withincreased muscle tone, rigidity, increased sali-vation, and gait and posture disturbances, may
be seen in patients prescribed antipsychoticdrugs, and over 60% of patients may have mildsymptoms. In contrast to idiopathic Parkinson’sdisease, tremor tends to occur late in the pictureand is less common than rigidity and akinesia.Akathisia may also be associated with theParkinsonian picture. The Parkinsonism tendsto come on gradually, and may be preceded bycomplaints of weakness or limb pains. Femalesare more affected than males. A variant is theso-called ‘rabbit syndrome’, in which rapidchewing-like movements of the lips occur,which resemble a rabbit eating. This is to bedistinguished from tardive dyskinesia.
It has been suggested that the incidence ofParkinsonism, and indeed some of the otherextrapyramidal syndromes, may be diminishedby the administration of routine prophylac-tic anticholinergic drugs. However, it may beargued that since anticholinergic drugs mayexacerbate some motor disorders (for exampletardive dyskinesia), provoke a toxic psychosis,delay gastric emptying and, by neurochemicalantagonism of the dopamine blocking poten-tial of the antipsychotic drugs, diminish theirtherapeutic potential, such routine prescriptionshould be avoided. It is clinically accepted thatthe atypical antipsychotic drugs provoke less inthe way of Parkinsonism and other extrapyra-midal side effects than the older compounds
Other conditions seen after varying timeintervals following introduction of neu-roleptic drugs include the blepharospasm–oromandibular–dystonia syndrome (Meige’sor Bruegel’s syndrome), catatonic reactionsand the neuroleptic malignant syndrome. Theblepharospasm–oromandibular–dystonia syn-drome is characterized by prolonged spasmsof the jaw and mouth, usually in associationwith blepharospasm, which is seen both as anidiopathic form and following neuroleptic treat-ment. Females are more affected than males,and the onset is usually in the sixth decade. Thedystonia can be extremely painful, the teethbeing forced together and sometimes damaged,or alternatively tongue biting can occur. Themouth may be forced into an open positionfor varying periods, which if severe may leadto difficulties with speaking and eating, and

302 Biological Psychiatry
sometimes jaw dislocation. Tongue protrusion,lip pouting and occasionally dystonic posturingin other parts of the body may also be noted. Thepathogenesis is unknown, but again it is thoughtto be related to abnormalities of dopamineactivity within the basal ganglia. It is one ofa group of tardive dystonias, which includeother forms of dystonic posturing, spasmodicdysphonia and abnormal vocalizations, whichsometimes are in association with tics, a tardiveform of Gilles de la Tourette’s syndrome.
Catatonic reactions involve posturing, waxyflexibility, withdrawal, mutism and associatedParkinsonism, which may be severe and life-threatening, and can be misinterpreted as anexacerbation of the underlying psychosis.
The neuroleptic malignant syndrome is one ofthe most serious of the extrapyramidal compli-cations, presenting as hyperpyrexia and rigidity.It may emerge from a catatonic reaction andbe associated with a variety of other abnor-mal involuntary movements. Autonomic distur-bances including cardiovascular and respiratorydifficulties, perspiration, salivation and inconti-nence may be seen, and death may occur fromrespiratory, cardiac, hepatic or renal failure.It can develop quite suddenly and has beendescribed following a single injection of anantipsychotic. Its appearance may be facilitatedby the combined administration of lithium. Itspathogenesis is not understood, but presum-ably relates to dopamine-receptor blockade inthe basal ganglia and hypothalamus. In viewof its high mortality (5–30%), attention to thepatient’s medical state is extremely important.Leucocytosis and elevated creatine kinase levelsin the presence of abnormal liver-function testsare often found. Treatment with bromocryp-tine, dantrolene, amantadine and ECT have allbeen tried.
Tardive Dyskinesia
This condition is a chronic disorder sec-ondary to the administration of antipsychotics,although idiopathic forms with an identicalclinical picture are noted. In addition, ithas been associated with the taking of antihis-tamines, anticholinergic drugs, anticonvulsants,
particularly phenytoin, and the tricyclic antide-pressants. It usually comes on after aboutthree months of therapy, and its appearance isgradual. In some patients, the first movementsare noted following reduction of drug dosage.This withdrawal dyskinesia is frequently seenin patients who have been on neurolepticmedication for a long period of time.
The characteristic features of tardive dyski-nesia are persistent abnormal muscular move-ments, predominantly affecting the tongue andperioral region, but, in addition, choreiform andathetoid movements in the limbs, and occa-sionally the trunk. There is smacking of thelips with masticatory jaw movements and pro-trusion of the tongue, often in combination.Sometimes the only clinical manifestation isincreasing writhing movements of the lips. Inother patients, blepharospasm, blinking, tics,abdominal movement and laryngeal spasmsmay also be noted. More rarely, particularlyin younger patients, a to-and-fro clonic-typemovement of the spine is seen. Although it issometimes stated that the condition does notcause much stress, and it is true that patientsoften lightly dismiss the dyskinesia, puttingtheir problems down to ‘denture difficulties’,it is nevertheless very uncomfortable in somepatients and may be socially quite disabling.
Tardive dyskinesia is found more frequentlyin patients receiving antipsychotics than in con-trol populations, is commoner in females andis found with increasing frequency with age.Younger patients tend to have involvement ofthe extremities and trunk, occasionally withbizarre postures and ballistic movements withgait abnormalities and rocking, while in theelderly a perioral distribution with associatedlimb movements is the more frequent picture. Insome cases the dyskinesia is persistent, althougha withdrawal dyskinesia will tend to disappearover weeks to months, following cessation ofthe neuroleptic. Present estimates suggest thatabout 50% of patients with tardive dyskine-sia will remain unchanged at follow-up. Noconvincing association between duration, doseand type of antipsychotic drug treatment hasemerged, but these pictures are seen less fre-quently with the atypicals. There is a suggestion

Biological Treatments 303
that patients who develop tardive dyskinesia aremore likely to show impairments on psycholog-ical testing (Struve and Willner, 1983; Wegneret al., 1985) and an increased incidence of CT-scan changes, including ventricular dilatation(Owens et al., 1985).
The pathogenesis of tardive dyskinesia hasyet to be clarified. The facts that it is com-monly related to drugs whose principal action isdopamine antagonism and that it is a tardive dis-order have led to the suggestion that it is relatedto the development of postsynaptic dopamine-receptor supersensitivity. This is supported byobservations that similar movements may beseen following L-dopa therapy for Parkinson’sdisease and that L-dopa itself may exacerbatethe movements of tardive dyskinesia. However,there are serious shortcomings to the conceptthat the condition is simply related to someform of receptor-disuse supersensitivity. Theseinclude the discrepancies between the develop-ment of the clinical syndrome and the time ofthe increase in dopamine receptors following thebeginning of treatment, which can be shown tooccur rapidly in animal models. Further, all ani-mals given neuroleptics develop supersensitiv-ity, whereas only some 20% of patients developthe persisting dyskinesia. In addition, in animalmodels where increased receptor sensitivity isshown, no equivalent of tardive dyskinesia hasbeen seen. The receptor changes tend to revert tonormal after withdrawal, but again, in patients,persistence of the syndrome can continue formany years. Finally, in patient post-mortemstudies, no difference in binding has been shownwith respect to either D1 or D2 receptors in thebrain when patients with schizophrenia withor without movement disorders are compared(Waddington et al., 1985).
An alternative hypothesis relates to analteration of GABA, since significant reductionsin GAD activity have been shown in the globuspallidus, subthalamus and substantia nigra ofprimates receiving long-term neuroleptic ther-apy (Gunne et al., 1984). This deficit appearedrelated to abnormal orofacial movements in theanimals. The hypothesis receives some supportfrom early suggestions that GABA agonistsmay improve some of the symptoms of tardive
dyskinesia in patients (Casey et al., 1980). Thesedata have recently been replicated using vigaba-trin in studies in which dyskinetic schizophrenicpatients were reported to show lower CSFGABA levels than those without dyskinesias(Thaker et al., 1987). Although no consistentabnormalities or neuropathological changes atpost mortem have been described, there areseveral reports of microscopic changes in somebasal-ganglia areas, including the substantianigra in patients receiving long-term neurolep-tics (Christensen et al., 1970), perhaps suggestingthat the clinical picture arises from the com-bination of some form of intrinsic neuronaldamage in these crucial regions of the brain andlong-term dopamine-receptor blockade.
A large number of drugs have been tried inthe treatment of tardive dyskinesia, but successhas been limited. Most of the studies have beencontinued for a few weeks only, and the major-ity are not double blind. Antipsychotic drugs,especially an atypical, are the most effectivemethod of suppressing the symptoms, althoughin the long term it seems hardly logical touse them. Anticholinergic drugs exacerbate thesymptoms, and withdrawal should be under-taken if they are concurrently prescribed in apatient with the syndrome (Burnett et al., 1980).
Other Side Effects
Agranulocytosis, due to a direct toxic effectof phenothiazines on the bone marrow, mayoccur, and depression of the white-cell countis often encountered. The estimated incidenceof this with clozapine is 1–2% of patients. Thismainly occurs within four months of treatment,and is reversible in most cases on stopping thedrug. Photosensitivity may be a problem withchlorpromazine, and may lead to a pattern ofcontact dermatitis or skin eruptions on expo-sure to sunlight. Retinal pigmentation has beendescribed with thioridazine. Combinations oflithium and haloperidol may lead to an organicpsycho-syndrome.
Cardiac arrhythmias are noted withpimozide, necessitating an EEG examinationprior to commencing therapy. The finding of aprolonged QT interval, or prescription of other

304 Biological Psychiatry
drugs that may increase the QT interval, whichincludes other antipsychotics, are contraindi-cations to its use. The concern over cardiacconduction problems has lead to the failure ofsome antipsychotics reaching clinical practice.Ziprasidone leads to a prolongation of the QTinterval and should not be given to patientswith a QT interval >500 ms or with otherdrugs which have an action on this ECG period(such as methadone, some tricyclic drugs,lithium). Torsade de points is a ventriculartachycardia associated with a long QT interval,which may lead to loss of consciousness, andrarely to death. Sudden death in patients onantipsychotic drugs has been reported, and thismay be due to cardiac problems. Findings atpost mortem are usually negative.
A withdrawal syndrome has been seen afterlong-term treatment with the antipsychotics,with insomnia, anxiety, restlessness and thealready-mentioned movement disorders. Adepressive illness has been reported to occurin some patients treated with antipsychotics,although the exact relationship between themedication and the depression is unclear,since postpsychotic depression is a well-recognized clinical entity. One suggestion isthat suppression of the psychotic symptomspermits the expression of pre-existent affectivesymptoms.
One problem that has emerged with theatypical antipsychotics relates to metabolicabnormalities. These include weight gain,hyperlipidaemia, glucose intolerance, increasedinsulin levels and type-2 diabetes mellitus. Thelatter has been reported to lead to episodes ofketoacidosis, a medical emergency which canlead to death. Weight gain is reported less withrisperidone, aripiprazole and ziprasidone, andmore for clozapine and olanzapine, the lattertwo having the higher risk for diabetes (Jinet al., 2006). In prospective studies the risk fordiabetes with typical agents is also shown tobe increased, but not in all studies, and less sothan with the atypical antipsychotics.
What is unclear is whether schizophreniaitself raises the risk for diabetes, and its relation-ship to weight gain. The metabolic syndrome,which represents a clinical picture of abdom-inal obesity, raised triglyceride and lowered
HDL-cholesterol levels, hypertension and raisedfasting glucose, puts patients at high risk forcardiovascular disease and diabetes mellitus,and is overrepresented in psychiatric patients,including those diagnosed with schizophrenia.In many cases the diabetes develops beforeweight gain, and it may emerge soon afterthe onset of therapy. It is unclear at presentto what extent patients beginning to take atyp-ical antipsychotics should be screened for themetabolic syndrome, but attention to familyhistory, weight, fasting blood sugar, the lipidprofile and blood pressure would seem sensi-ble, and the vulnerable should be notified of therisk and appropriately monitored.
Antipsychotic Drugs in Development
Asenpaine is a novel atypical drug which hashigher affinity for several 5-HT and D3 andD4 receptors. The trend has been to developD2 antagonists or partial agonists with high-affinity antagonism for other receptors such as5-HT (5-HT1A, 5-HT2a 5−HT2c, 5-HT3, etc.) orfor noradrenaline, or selective agonists at D1or D4, nicotinic and GABAa receptors. How-ever, other potential treatments include COMTinhibitors such as tolcapone, and drugs that acton the glutaminergic system such as glycine, D-serine, D-cycloserine and ampakine. Of these,only the co-agonists glycine and D-serine showany promise; these seem effective on negativeas opposed to positive symptoms (Tuominenet al., 2006).
Another strategy is to target symptoms,especially those derived from endophenotypicresearch (such as cognition), or negative symp-toms, moving away from using DSM IV-TR approaches to patient selection. Geneticresearch may in the future allow molecularlibraries of potential targets for pharmaceuticalsto be established, with genetic profiling ofpatients most likely to respond.
ANXIOLYTICS AND HYPNOTICS
Three main groups are included: barbiturates,benzodiazepines and others. They are the mostwidely used drugs in psychiatry, and possess

Biological Treatments 305
sedative and anticonvulsant properties in addi-tion to being anxiolytic. The main differencesbetween the barbiturates and the benzodi-azepines reside in the lack of suicide potentialwith the latter and the greater tendency toaddiction with the former.
Barbiturates include phenobarbitone, buto-barbitone and amylobarbitone. They are rapidlyabsorbed from the GI tract and are power-ful hepatic enzyme inducers. Their duration ofaction is around eight hours, but their gener-alized effect on the brain leads to respiratorydepression, which may cause death in over-dose. Since the introduction of the benzodi-azepines they have been used far less frequently,although occasional patients still benefit fromthe prescription of a hypnotic barbiturate invery selected circumstances. Although pheno-barbitone at one time was an important drug inthe management of epilepsy, its use these daysis not encouraged.
The benzodiazepines have a common struc-ture, but differ with respect to their metabolites(see Figure 12.4). Ultimately, they are conju-gated with glucuronic acid, and a number of themetabolic products themselves are active com-pounds. However, some of the benzodiazepines(particularly the short-acting ones) tend not tohave active intermediaries. Many of the longer-acting ones have desmethyldiazepam as theiractive metabolite, which has a half-life of some50 hours. However, benzodiazepines differ bothwith regards to their half-life and with theirpotential for anxiolytic, anticonvulsant, muscle-relaxant, sedative and amnesic effects. Some
Table 12.9 Half-life of different benzodiazepines
Hours
Temazepam 8Oxazepam 8Lorazepam 12Medazepam 6–20Flurazepam 10–20Chlordiazepoxide 24Diazepam 30Chlorazepate 30–60Nitrazepam 48Triazolam 2Clonazepam 53Clobazam 18
of these differences are shown in Tables 12.9and 12.10.
On the basis of their half-lives, they maybe divided into long, intermediate and shortduration of action. Some of these pharmacoki-netic differences are shown in Table 12.11. Ingeneral, those with a long duration of actiontend to be prescribed as anxiolytics, while thosein the short-acting class are hypnotics. Theclearance of many of these drugs is increasedwith age, although oxazepam, lorazepam andtemazepam show only minor differences in theirkinetics with advancing years. The metabolismof lorazepam and oxazepam is little influencedby liver disease.
The discovery of the benzodiazepine recep-tor led to a clearer understanding of theirmode of action (Braestrup and Nielsen, 1982).The benzodiazepine binding site, thought torepresent part of the GABA–receptor chlorideionophor complex, is in some way relatedto the behavioural actions of these drugs,
Chlordiazepoxide(Librium)
Medazepam(Norbium)
Diazepam(Valium)
Temazepam(Normison)
(Metabolites) (Metabolites)
Oxazepam . . . Lorazepam(Serenid D) (Ativan)
Desmethyldiazepam
Desmethylchlordiazepoxide Demoxepam (Metabolites)
Chlorazepate(Tranxene)
Figure 12.4 The pathway of benzodiazepine metabolism (Biol Psych, 2 Ed, p. 358)

306 Biological Psychiatry
Table 12.10 Differential effects of different benzodiazepines
Drug Anxiolytic Anti-convulsant Muscle relaxing Sedative Amnesic
Lorazepam ++ + + + + + + + +Diazepam ++ + + + + ++ +Temazepam + ± + + + + ±Clonazepam ± + + + ++ + ±Nitrazepam + ++ + + + + ±Clobazam ++ + + + + ± ±
Table 12.11 Pharmacokinetic differences amongbenzodiazepines
Long Intermediate Short
Chlordiazepoxide Alprazolam BrotizolamClorazepate Bromazepam MidazolamClobazam Flunitrazepam TriazolamDiazepam LorazepamFlurazepam LormetazepamKetazolam NitrazepamMedazepam OxazepamPrazepam Temazepam
although it does not explain all of their effects.For example, meprobamate and alcohol, botheffective anxiolytics, do not bind to the receptor.This is one element of the argument whichhas led Gray (1982) to suggest that at leastthe anxiolytic effect of the benzodiazepines isrelated to enhancement of the GABA trans-mission, probably at selective sites within theCNS, but that interaction with other neuro-transmitter systems, in particular the ascendingmonoamines, is also involved (Iversen, 1983).Benzodiazepine antagonists counteract some
of the effects of benzodiazepines, and provokeanxiety in humans (Dorrow et al., 1983). Res-piratory depression does not appear to be acomplication of benzodiazepine therapy, andafter overdose, if taken alone, benzodiazepinesrarely result in death.
The existence of multiple potential configura-tions of the benzodiazepine–GABA receptor hasallowed further understanding of the spectrumof benzodiazepine effects. These range from fullagonism to partial agonism, to antagonism andinverse agonism, as illustrated in Figure 12.5.This has allowed partial agonists to be devel-oped, such as abecarnil and bretazenil, althoughas yet none have found clinical approval. Thediffering profile of benzodiazepines is reflectedin two compounds, namely clobazam and alpra-zolam. Clobazam is a 1,5-benzodiazepine, inwhich the nitrogen on the heterocyclic ringis moved from the 4 to the 5 position. Thisappears to confer a better therapeutic poten-tial of the drug with regards to its anticon-vulsant effect, the drug possessing minimalsedative, myorelaxant and cognitive side effects
The spectrum of benzodiazepine activity
Agonism Antagonism Inverseagonism
AnxiogenicProconvulsant
AnxiolyticAnticonvulsant
Full
DiazepamLorazepamAlprazolam
FlumazenilBretazenilAbercarnil
DMCMB-CCM
Partial FullPartial
Figure 12.5 The spectrum of benzodiazepine effects (reproduced from Cummings and Trimble, 1995; BiolPsych, 2 Ed, p. 361)

Biological Treatments 307
(Trimble, 1986b). Alprazolam is a triazoloben-zodiazepine, which in addition to its anxiolyticproperties is reported to be effective in the con-trol of panic disorder and may possess antide-pressant properties (Judd et al., 1986). It appearsthat most benzodiazepines are ineffective forpanic attacks, while tricyclic antidepressants,SSRIs, MAOI drugs and alprazolam are thera-peutically useful. Alprazolam is antidepressantfor patients with reactive or neurotic depression(Imlah, 1985) and mania has been reported as aside effect (Arana et al., 1985).
Concern has been expressed about benzodi-azepine dependence. This has been reportedafter as short a time as six weeks of treat-ment, although it tends to occur in patients whohave been on high doses for prolonged periods.Withdrawal symptoms may occur, particularlyif the dose of the drug is withdrawn at aninappropriate rate. The withdrawal syndromein many cases actually represents a return ofearlier anxiety, although some authors have sug-gested that perceptual distortions and feelingsof depersonalization are characteristic (Ashton,1984). Withdrawal seizures are certainly onemanifestation, although again, in the clinical set-ting, they probably reflect too rapid a decreasein dose. The presence of the withdrawal syn-drome suggests how effective these compoundsare biologically, and thus how they should beused judiciously in clinical practice. It has beenreported that premorbid personality character-istics may be important in predicting thosepatients who will show withdrawal reactions,those with passive and dependent personal-ity traits being more susceptible than thoseshowing premorbid conscientiousness, rigidityor even premorbid anxiety proneness (Tyreret al., 1983).
Other side effects include oversedation,problems with concentration and memory, andin the elderly, ataxia and confusion, particularlywith the longer-acting and more sedative com-pounds. The shortest-acting benzodiazapines,such as midazolam, are powerful amnesticagents and are commonly used in brief surg-eries and procedures. Longer-term confusionalstates have been reported in the elderly, evenafter brief exposure to the shortest-acting
agents. Depression has been reported, but it isalso seen following long-term benzodiazepinewithdrawal (Olajide and Lader, 1984). Releaseof aggression has also been noted in bothanimals and humans.
Other anxiolytics include meprobamate,which is absorbed rapidly, induces its ownmetabolism and has a half-life of about 12 hours.It is approximately halfway between the bar-biturates and the benzodiazepines in termsof producing tolerance, sedation and corticaldepression. Other hypnotics include chloralhydrate, dichloralphenazone, glutethamide,paraldehyde and chlormethiazole. The lattermay be particularly useful in the managementof alcohol withdrawal syndromes.
The azapirones are nonbenzodiazepineanxiolytics which include gepirone, ipsapirone,binospirone and buspirone. They act as agonistsat the 5-HT1A receptor, and seem also to possessantidepressant properties (see above). The roleof the 5-HT receptors in anxiety is actively underinvestigation at present, and some 5-HT2 antag-onists such as mianserin and ritanserin maydiminish anxiety. It is thought that the downreg-ulation of 5-HT2 receptors by antidepressantsmay be related to the anxiolytic effects of thesedrugs. 5-HT3 antagonists such as ondansetronmay be effective in some anxiety states, althoughthe clinical use of the later is as an antiemetic.
Buspirone is well absorbed and widely dis-tributed throughout the body. It has a half-lifeof approximately 2–3 hours, and although aweak dopamine antagonist, does not appear tobe antipsychotic, and lacks sedative, muscle-relaxant and anticonvulsant effects.
Zopiclone is a cyclopyrrolone that acts atsubunits of the benzodiazepine A receptor,with sedative and anticonvulsant properties. Itis one of a group of drugs, including zaleplonand zolpidem, which were thought to have lessaddictive potential than the benzodiazepines,but cases of dependence are reported. Thesedrugs have short half-lives (3–6 hours) and areused as hypnotics. Dysgeusia is a particularproblem with zopiclone, and a tentativeassociation with carcinoma has been suggested.A related drug, alpidem, is not hypnotic buthas anxiolytic properties.

308 Biological Psychiatry
When using anxiolytics, doses of drugs haveto be based on clinical judgement, and for tran-quillization once-daily or twice-daily regimescan be used. Although some patients developtolerance to these drugs, requiring increasingdoses over time, this is not usual and manypatients continue to get clinical benefit on smalldoses. However, it is important that they shouldnot be given for longer than is necessary, andthat when withdrawal is undertaken it shouldbe done slowly and with care.
Recently, increased knowledge of theheterogeneity and complexity of the GABAreceptor, especially regarding extrasynapticreceptors, has led to a resurgence of interestin GABA agonists as psychotropic agents,but beyond anxiolysis, with even potentialantipsychotic effects. More subtype-selectivebenzodiazepines are being explored.
With regard to hypnotics, there has been agrowing interest in cerebral rhythms, especiallycircadian ones controlled by the suprachi-asmatic nucleus of the hypothalamus. Thisnucleus receives light stimuli via the eye,and regulates a number of bodily rhythmsincluding temperature and sleep–wake cycles.Melatonin receptors (M1 and M2) are found inthe supachiasmatic nucleus, and act throughadenylate cyclase to regulate oscillations ofneuronal activity. Melatonin levels are high atnight-time and low in the daytime.
Melatonin itself can induce sleep, and is usedby many people as a hypnotic. Ramelteon selec-tively binds to M1 and M2 receptors. Agomela-tine is an M1 and M2 agonist with high affinityfor the 5-HT2c receptor, and no affinity for 5-HT or dopamine transporters, or histaminicand muscarinic receptors. The 5-HT2c receptoreffect is thought to release noradrenaline anddopamine in frontal cortex, contributing to anantidepressant effect. This compound increasesslow-wave sleep and is nonsedative.
BETA-ADRENERGIC BLOCKERS
Beta-adrenergic blockers, such as propranolol,are widely used in the management of car-diovascular disorders, and clinically decrease
the heart rate, lower the blood pressure andmay cause bronchial constriction. Their usein the management of anxiety disorders hasbeen advocated, one suggestion being that theyinfluence the somatic symptoms such as pal-pitations, sweating and diarrhoea, as opposedto psychic symptoms (Tyrer and Lader, 1974).However, improvement of psychic symptomshas also been reported (Kathol et al., 1980), andthe suggestion that their effect is primarily onperipheral receptors may need revision. Somebeta-blockers such as practolol, with little abilityto cross the blood–brain barrier, also appear tobe effective anxiolytics. They are of little valuein agoraphobia and panic attacks and do notinfluence lactate-induced panic (Gorman et al.,1983). There has been interest in their use inschizophrenia, but the results of various trialsare contradictory. They are contraindicated inpatients with respiratory and cardiac disorders,where beta blockade may lead to deteriorationof the clinical state, and are poorly tolerated bysome people, who develop a severe malaise andlethargy, which, if unrecognized, may be takenfor further symptoms of the underlying psy-chiatric disturbance. A withdrawal syndromehas been described with abrupt termination oftreatment. Their use as single doses (40 mg ofoxprenolol) to quell stage fright and other brief-lived episodes of stress-induced anxiety maybe helpful, but generally in the managementof patients with anxiety, benzodiazepines arepreferred, particularly by patients (Tyrer andLader, 1974).
LITHIUM
Lithium carbonate was first introduced for thetreatment of manic–depressive illness in 1949and is the drug of choice for prophylactic man-agement of manic–depressive psychosis. Fol-lowing ingestion, it is absorbed rapidly, peakconcentrations occurring in 1–2 hours, with ahalf-life of approximately 24 hours. It is mainlyexcreted in the urine, and thus patients withrenal disease readily become intoxicated. Sinceit is reabsorbed with sodium into the proximalrenal tubules, any drug that leads to a nega-tive sodium balance, such as a diuretic, will

Biological Treatments 309
lead to increased retention of lithium. This alsooccurs with alteration of the diet, heavy sweat-ing and diseases that reduce sodium intake. Fora hypertensive patient, a beta-blocker or cloni-dine is preferred, and thiazide diuretics shouldbe avoided.
Its mode of action is still unknown in spiteof its widespread use, but it does reduce thesodium content of the brain, increase central5-HT synthesis and noradrenaline turnover,increase platelet 5-HT uptake (Coppen et al.,1980), and reduce urinary noradrenaline,MHPG, VMA and whole-body noradrenalineturnover (Linnoila et al., 1983a). Lithium alsoaffects the PI intracellular transduction system,perhaps interfering with neurotransmitter-stimulated PI metabolism. This may thusdownregulate, for example, an overactivedopamine system. Since dopamine-inducedstimulation of PI can also be inhibited bydopamine antagonists, one explanation forthe effects of both neuroleptics and lithiumin mania is through this common mechanism.Rangel-Guerra et al. (1983) reported using MRI,that T1 proton relaxation time was reducedfrom elevated levels in 20 patients with bipolaraffective disorder following lithium therapy of900 mg per day for 10 days.
The main indication for lithium is in bipolaraffective disorder, although it is now known tobe useful in the management of recurrent unipo-lar affective disorder. It may also be used in theacute treatment of affective disorder, especiallymania, when it is usually started in combi-nation with an antipsychotic. Other uses oflithium include recurrent aggressive disorders,migraine, cluster headaches, cycloid psychosesand organic mental disorders with secondaryaffective symptoms. In one trial (Coppen et al.,1978), lithium was found to be superior tomianserin in the long-term maintenance treat-ment of depressive illness.
Lithium has a number of toxic effects, whichare shown in Table 12.12. Although these areminimized by regular monitoring of serumlithium levels, with a suggested nontoxic rangeof 0.6–1.5 mmol l−1, severe toxicity has beendescribed at lower levels, and coexistent med-ication such as phenytoin, carbamazepine and
Table 12.12 Toxic effects of lithium
Neuropsychiatric DrowsinessConfusionPsychomotor retardationRestlessnessStuporHeadacheWeaknessTremorAtaxiaMyasthenia gravis syndromePeripheral neuropathyChoreoathetoid movementsCerebellar syndromeDysarthriaDysgeusiaBlurred visionSeizuresDizziness, vertigoImpaired short-term memory
and concentrationGastrointestinal Anorexia, nausea, vomiting
DiarrhoeaDry mouth, metallic tasteWeight gain
Renal Microtubular lesionsImpairment of renal
concentrating capacityCardiovascular Low blood pressure
ECG changesEndocrine Myxoedema
HyperthyroidismHyperparathyroidism
Other Polyuria and polydipsiaGlycosuriaHypercalcinuriaRashes
haloperidol may be related to this. Ibuprofen,indomethacin, mefenamic acid, diclofenacand piroxicam inhibit lithium excretion, anddiuretics cause lithium retention, which mayincrease serum levels. Patients with cardiacor renal disease, or in other situations thatmay interfere with the clearance of lithium,will obviously need regular monitoring, andprior to starting therapy it is customary toassess renal and hepatic function. Thyroidfunction is also checked since hypothyroidism,sometimes associated with goitre or evenadvanced myxoedema, has been observed.Lithium therapy may decrease thyroxine andT3 and increase TSH levels, which may lead to

310 Biological Psychiatry
abnormalities of thyroid-function tests even inthe absence of clinical signs of hypothyroidism.If lithium-maintenance therapy is essential thensupplementary thyroxine treatment will berequired if the patient develops myxoedema.
Although a teratogenic effect of lithium inhumans has not been demonstrated, there arereports of a high incidence of congenital mal-formations in babies born to mothers who takelithium, and it should probably be discontinuedif possible during pregnancy.
One of the commonest side effects relatesto altered renal function, with polyuria andpolydipsia. Urinary-concentrating ability isimpaired, which may be exacerbated by com-bination with neuroleptics. The polyuria mayresult in compensatory increases in antidiuretichormone secretion, although occasionally apicture of nephrogenic diabetes insipidus isseen. In spite of these findings, long-termfollow-up does not suggest that serious renaldamage occurs with prolonged therapy.
Severe intoxication may lead to an organicbrain syndrome with hyperactive reflexes,seizures and tremor. On occasion, unilateralneurological abnormalities have been reported,which may be interpreted as an alternativeneurological diagnosis. If toxicity results incoma, dialysis should be considered, especiallyif clearance is in any way delayed. On stoppingthe drug, the serum concentration usually fallsby about half each day, and after routine therapywithdrawal symptoms including irritability andemotional lability have been described (Kingand Hullin, 1983). For reasons that are not clear,lithium is the only medication that appearsto have a distinct anti-suicide effect. This wasnoted by Baldessarini in a large meta-analysis(22 studies, 6000 patients) and has now beenconfirmed in several studies, one involving alarge California health-maintenance organiza-tion (HMO) (21 000 patients). In the HMO study,bipolar patients on valproic acid had a suiciderate three times higher than those taking lithium.
ANTICONVULSANTS
These compounds are also referred to as anti-epileptic drugs, although there is no evidence
that they affect the underlying processes ofepilepsy. They are antiseizure agents, but havea much broader clinical spectrum, and someare used widely in neuropsychiatry beyondepilepsy, particularly for mood stabilization inbipolar patients. Some of the anticonvulsantdrugs presently in use are shown in Table 12.13.The older barbiturate-related compounds andphenytoin have been largely replaced by drugssuch as carbamazepine and sodium valproate,and newer agents which include gabapentin,lamotrigine, levetiracetam, oxcarbazepine,pregabalin, tiagabine, topiramate, vigabatrinand zonisamide.
As a generalization, the four main modes ofaction are by blockade of voltage-dependentsodium channels, antagonism of excitatoryaminoacid receptors, potentiation of GABAtransmission and blockade of calcium channels(see Table 12.14). New findings with gabapentinand pregabalin are that these agents inhibitthe action of the alpha-2-delta component ofthe calcium channel and that levetiracetambinds to a synaptic vesicle protein, SV2A. Thesenew findings may lead to the development ofdifferent antiseizure agents.
Phenytoin is highly plasma-bound andcleared from the plasma by hepatic metabolism.Varying serum levels may be noted amongstdifferent patients on the same dose, and smallincrements in prescription can lead to rapidlyescalating serum levels on account of its zero-order pharmacokinetics (Figure 12.1). In spiteof its long use, its mechanism of action is stillunclear, although there are suggestions that itmay interact with sodium or calcium channelsin excitable neurones, thus limiting the potentialfor high-frequency neuronal discharges. It is amembrane stabilizer and also possesses somebenzodiazepine binding, and thus has someinfluence at the GABA receptor, particularly athigher concentrations.
Primidone is partially converted to pheno-barbitone, although the primidone componentitself probably exerts independent anticonvul-sant activity. Phenobarbitone also influencesthe transcellular transport of sodium, cal-cium and potassium ions and influences theneurotransmitter release of GABA, glutamate

Biological Treatments 311
Table 12.13 Some anticonvulsant drugs in current use
Name Half-life (hours) Recommendedserum level(mmol l−1)
Indications
Carbamazepine 8–45 16–50* Generalized seizures: simple or complex partialseizures; secondary generalized seizures
Clobazam 22 – As for carbamazepineClonazepam 20–40 – Myoclonic epilepsyEthosuximide 30–100 300–700 Generalized absence seizuresPhenobarbitone 36 6–180* Generalized or simple partial seizuresPhenytoin 22 40–80* Generalized seizures: simple or complex partial
seizuresPrimidone 3–12 – Generalized: complex or simple partial seizuresSodium valproate 10–15 – Generalized absence seizures: myoclonic
epilepsy; simple or complex partial seizuresNewer AgentsGabapentin 5–7 – Intractable, partial and generalized seizuresLamotrigine 22–36 – Intractable, partial and generalized seizuresLevetiracetam 6–9 – Intractable partial aand generalised seizuresOxcarbazepine 8–15 – Adjunctive therapy for partial seizuresPregabalin 5–6 – Intractible partial and generalised seizuresTiagabin 4–13 – Intractible partial and generalised seizuresTopiramate 20–30 – Intractible partial and generalised seizuresVigabatrin 5–7 – Intractable, partial and generalized seizuresZonisamide 50–70 – Intractible partial and generalised seizures
*Conversion factor for µg/ml: carbamazepine 4.2, phenobarbitone 4.3, phenytoin 4.0.
Table 12.14 The principal modes of action of anticonvulsant drugs (adapted from Perucca, 2002)
Blockade of Antagonism of Potentiation of Blockade ofvoltage dependent excitatory GABA calcium channelssodium channels aminoacid receptors transmission (channel type)
Older AEDsBenzodiazepines − − + −Carbamazepine + − − −(L)Ethosuximide − − − +(T)Phenobarbital − − + −Phenytoin + − − ?Valproic acid + − + +(T)
Newer AEDsFelbamate + + + +Gabapentin/Pregabalin +(?) − +(gbp) +Lamotrigine + − − +(L,N,P)Levetiracetam − − − +(N)Oxcarbazepine + − − +(L)Tiagabine − − + −Topiramate + + + +(L)Vigabatrin − − + −Zonisamide + − − +
gbp = gabapentin.

312 Biological Psychiatry
and aspartate. Further, it enhances GABApostsynaptic inhibition, interacting at thebenzodiazepine–GABA receptor.
Carbamazepine is structurally related to thetricyclic antidepressants, and has a mode ofaction different from phenytoin and pheno-barbitone. This drug also acts at the sodiumchannel, but in addition its biochemical actionsinclude partial agonism of adenosine recep-tors; it acutely increases the firing of the locuscoeruleus and decreases CSF somatostatin andHVA accumulation after probenacid (Post andUhde, 1986; Post et al., 1986). Further, in animalmodels, carbamazepine is shown to be rela-tively more effective than other anticonvulsantsin inhibiting the seizures developed from amyg-dala kindling, suggesting some limbic-systemselectivity for the drug (Albright and Burnham,1980). Sodium valproate is a GABA agonist insome animal models, but clinically this is notthought important, and the mechanism of itsantiseizure action is unknown at the presenttime. It also reduces sodium and potassiumconductance, reducing the excitability of nervemembranes. The role of benzodiazepines inthe management of epilepsy has been largelyrestricted to acute use in status epilepticus (e.g.midalozam). However, clonazepam, clobazamand nitrazepam have been used for oral therapy.Clonazepam finds more use in childhood, butis markedly sedative in contrast to clobazam,a nonsedative 1,5-benzodiazepine. Clobazamhas effective antiepileptic properties in a sub-group of patients who are nonresponsive toother drugs, and is used as adjunctive ther-apy. Gabapentin probably acts at extrasynapticGABA receptors.
Gabapentin and pregabalin have a novelmechanism of action, not influencing directlypostsynaptic GABA receptors, and binding tothe alpha-2-delta subunit of the calcium chan-nel. This leads to a decrease in the release ofmonoamines and glutamate. Lamotrigine wasoriginally developed as a folate antagonist, butis now thought to act by reducing the releaseof excitatory amino acids from presynaptic ter-minals. Oxcarbazepine is structurally related tocarbamazepine; it is a 10-keto analogue, possess-ing an extra oxygen atom on the dibenzazepinering. This reduces the liver-enzyme induction,
and decreases the risk of some side effects,including the agranulocytosis that is occasion-ally associated with carbamazepine. Vigaba-trin was the first important designer drug forepilepsy, being developed as a suicide inhibitorof GABA transaminase, the main enzyme thatmetabolizes GABA in neurones and glial cells.It reliably increases GABA in the CSF and CNS,an effect detected by MRS (Preece et al., 1994).It was later shown to lead to irreversible par-tial loss of vision (scotoma) in about 30% ofpatients, an effect of GABA on the retina, whichhas markedly restricted its use. Despite thisconcern, it is currently being investigated asan anti-craving drug for cocaine users. Drugssuch as tiagabine, topiramate and zonisamidehave several mechanisms of action that may berelevant to their antiseizure effects.
All of the newer drugs are advocated foruse in intractable epilepsy, usually as add-ontherapy, although several are licensed for use inmonotherapy, their availability depending onthe country of use.
The side effects of anticonvulsants are many;they are given often for many years andin combination with other anticonvulsants.Table 12.15 sets out the neuropsychiatric sideeffects, attributed to the older generation ofdrugs, although many are still in use in variouscountries. These include an encephalopathy anddeterioration of intellectual function, as well asapathy, depression, dysphoria, irritability andoccasionally hyperactivity, which are particu-larly seen in association with the barbituatesand polytherapy. Chronic dyskinesias are occa-sionally seen, while an acute dystonic reactionhas been noted with carbamazepine. Sodiumvalproate has been associated with liver failurein a small number of young patients, and alsoproduces a reversible alopecia and weight gain.Carbamazepine may be associated with waterintoxication and hyponatraemia, althoughthe mechanism of this is not clear. This is incontrast to the polyuria provoked by lithium,and emphasizes the different pharmacologicalprofiles of lithium and carbamazepine, eventhough both have mood-stabilizing effects.
The profile of the side effects with the newerdrugs is given in Table 12.16. Some exacerbate oreven initiate generalized (especially myoclonic)

Biological Treatments 313
Table 12.15 Chronic toxic effects of some anticon-vulsant drugs (reproduced from Reynolds, 1975)
Nervous system Cerebellar atrophy (?)Peripheral neuropathyEncephalopathyOther mental symptoms,
depression, agitation,psychoses
Haemopoieticsystem
Folic acid deficiencyCoagulation defectsAgranulocytosisAplastic anaemia
Skeletal system Metabolic bone diseaseVitamin D deficiency
Connective tissue Gum hypertrophyFacial skin changesWound healingDupytren’s contracture
Skin HirsutismPigmentationHair lossAcne
Liver Enzyme induction; failureEndocrine system Pituitary–adrenal
Thyroid–parathyroidHyperglycaemia
(diabetogenic)Other metabolic
disordersVitamin B6 deficiency(?)
Immunologicaldisorders
LymphotoxicityLymphadenopathySystemic lupus
erythematosusAntinuclear antibodiesImmunoglobulin changes(?)Immunosuppression
seizures (vigabatrin, lamotrigine). Behaviouralproblems have limited the use of some, inparticular the exacerbation or precipitation ofaggression, depression and psychoses. Suchadverse reactions may be linked with the phe-nomenon referred to as ‘Forced Normalization’(see Chapter 10). They may occur with all ofthe drugs, but are particularly prominent withGABAergic agents such as vigabatrin, topira-mate, gabapentin and tiagabine, and attemptedor completed suicide has been reported. Thelink between anticonvulsant drugs and suicidehas been of such concern that in the USA theFDA has instructed all companies marketingthese drugs to include a warning about suicidein their data and information sheets. Ofparticular concern has been the use of some of
these compounds ‘off label’ in patients withmood disorders.
Topiramate has been associated with cogni-tive blunting, and particularly with a reversibleaphasia-like syndrome, presenting with word-finding difficulties.
Interactions between anticonvulsants andother drugs, or between different anticonvul-sants, may present problems in management. Ofparticular importance are the drugs that elevatephenytoin levels and might lead to phenytointoxicity (see Table 12.17), and interactions withpsychotropic drugs (Tables 12.3 and 12.4). Thereis some evidence that patients on phenytoin,because of induced hepatic enzymes, will havelower serum levels of antidepressants, andthat thus prescription of the usual dose maybe subtherapeutic. Serum levels of neurolep-tics may likewise be significantly lower inpatients treated with anticonvulsants than incontrols. Carbamazepine intoxication can alsobe caused by cimetidine, dextropopoxyphene,erythromycin and verapamil, and SSRIs. Of thenew drugs, only lamotrigine has significantinteractions. Its metabolism is inhibited bysodium valproate, so when it is given with thatdrug, the dose of lamotrigine that is needed ismuch lower. Some of the hepatic enzyme induc-ers, such as carbamazepine, oxcarbazepineand topiramate, will lower serum oestrogenlevels, and contraceptive protection maybe lost unless high-dose oestrogen pills areprescribed.
It is generally accepted that in epilepsy, newlydiagnosed patients should be treated by theprescription of only one anticonvulsant drugif possible. Upwards of 80% of new patientswith appropriate serum-level monitoring andadequate serum levels will be satisfactorily con-trolled on monotherapy. It is not clear thataddition of a second drug will lead to bettermanagement of seizures in those who continueto have attacks, with exceptions. Recent researchhas suggested that patients who have furtherseizures are likely to do so within a year of pre-sentation with the first attack, and it is thus tosome extent predictable who is likely to sufferfrom chronic uncontrolled seizures. It is suchpatients who are liable to receive polytherapy,and, in the long term, to suffer neuropsychiatric

314 Biological Psychiatry
Tab
le12
.16
Sum
mar
yof
the
mai
nsi
de
effe
cts
ofth
ene
wer
gene
rati
onof
anti
conv
ulsa
ntd
rugs
(ad
apte
dfr
omPe
rruc
a,20
02)
Felb
amat
eG
abap
enti
n+La
mot
rigi
neLe
veti
race
tam
Oxc
arba
zepi
neT
iaga
bine
Top
iram
ate
Vig
abat
rin
Zon
isam
ide
Nau
sea
Diz
zine
ssD
izzi
ness
Diz
zine
ssFa
tigu
eD
izzi
ness
Diz
zine
ssV
isua
lfiel
dco
nstr
icti
on(3
0%)**
*
Fati
gue
Vom
itin
gFa
tigu
eB
lurr
edvi
sion
Fati
gue
Hea
dac
heFa
tigu
eSo
mno
lenc
eSo
mno
lenc
eH
ead
ache
Som
nole
nce
Dip
lopi
aH
ead
ache
Diz
zine
ssH
ead
ache
Men
tals
low
ing
Diz
zine
ssD
izzi
ness
Beh
avio
ural
dis
ord
ers**
Inso
mni
aSo
mno
lenc
eA
taxi
aT
rem
orIm
pair
edco
ncen
trat
ion
Som
nole
nce
Ata
xia
Inso
mni
aSo
mno
lenc
eN
ervo
usne
ssSe
dat
ion
Ner
vous
ness
Wei
ghtg
ain
Ano
rexi
aB
ehav
iour
ald
istu
rban
ces
Ata
xia
Ata
xia
Beh
avio
ural
dis
turb
ance
s**N
ause
aIm
pair
edco
ncen
trat
ion
Som
nole
nce
Fati
gue
Nau
sea
Tre
mor
Hea
dac
heH
ypon
atra
emia
Pare
sthe
siae
Diz
zine
ssM
enta
lslo
win
gW
eigh
tlos
sW
eigh
tgai
nFa
tigu
eM
ildsk
inra
shes
Abd
omin
alpa
inD
ysno
mia
/an
omia
Beh
avio
ural
dis
turb
ance
sIm
pair
edco
ncen
trat
ion
Apl
asti
can
aem
ia(1
:5,0
00)
Nau
sea
Dep
ress
ion
Wei
ghtl
oss
Dep
ress
ion
Mild
skin
rash
esSe
riou
shy
pers
ensi
tivi
tyre
acti
ons
Ano
rexi
aPs
ycho
sis
Agi
tati
onIr
rita
bilit
yH
epat
otox
icit
y(1
:26,
000)
Stev
ens-
John
son
synd
rom
e(1
:1,0
00)*
Nau
sea
Con
fusi
onA
taxi
aD
ysno
mia
/an
omia
Oth
erse
riou
shy
pers
ensi
tivi
tyre
acti
ons
Oth
erse
riou
shy
pers
ensi
tivi
tyre
acti
ons
Fati
gue
Nap
hrol
ithi
asis
(1–2
%)
Pare
sthe
sias
Skin
rash
esM
etab
olic
acid
osis
Dep
ress
ion
Nep
hrol
ithi
asis
(1–2
%)
* Hig
her
inci
den
cein
child
ren
(1,1
00to
1,30
0).
**E
spec
ially
inpa
tien
tsw
ith
lear
ning
dis
abili
tyor
ahi
stor
yof
beha
viou
rald
isor
der
s.**
* Inc
iden
ceof
sym
ptom
atic
visu
alfi
eld
cons
tric
tion
isab
out1
–3%
.+
Sim
ilar
for
preg
abal
in.
N.B
.Sui
cid
alit
yan
dse
lf-h
arm
have
been
linke
dw
ith
AE
Dpr
escr
ipti
ons
(see
text
).

Biological Treatments 315
Table 12.17 Anticonvulsant interactions
(a) Clinically significant interactions with carba-mazepine and phenytoin
Drugs which maycause elevation ofanticonvulsantlevels ofcarbamazepine orphenytoin
AllopurinolCarbamazepine*†ChloramphenicolChlorpromazineCimetidineCo-trimoxoleDextropropoxypheneDiltiazemDisulfiramErythromycinImipramineMetronidazoleMiconazoleSulphonamidesThioridazineTopiramateTroleandomycinVerapamilViloxazine
Drugs which havetheir effectreduced byphenytoin orcarbamazepine
AmitriptylineDexamethasoneDiazepamDoxepinHaloperidolHydrocortisoneOral contraceptivesPethidinePhenobarbitonePrimidonePrednisoloneSodium valproateTheophyllineWarfarin
(b) Other significant anticonvulsant interactions
Sodium valproate Levels reduced bycarbamazepine andphenytoin
Increases free phenytoinlevels
Increases lamotriginelevels
Increases phenobarbitonelevels
*Phenytoin levels can be increased or decreased when carbamazepineis added.†Carbamazepine induces its own metabolism.
complications and become candidates for eithersurgical resection or treatment with VNS.
A number of new anticonvulsant drugs arein development, which are either structural
variables of existing compounds or novel chem-icals. The structural variables include (withmarketed product in brackets): breviracetam(levetiracetam), which in addition to bindingat the SV2A protein interacts with voltage-gated sodium channels; eslicarbazepine, thel-isomer of oxcarbazepine; and fluorofelbamate(felbamate). The new compounds include:lacosamide, an amino acid which enhancesthe slow inactivation of sodium channels;retiagabine, which acts on voltage-gatedK-channels, increasing the M-current andstabilizing resting and subthreshold membranepotentials; and ganaxolone, a neurosteroid.
The question of which anticonvulsant drugto use for which type of seizure is often a mat-ter of clinical choice, but some guidelines areclear. In some instances, for example the useof steroids or ACTH for infantile spasms andthe almost exclusive use of ethosuximide forgeneralized absence seizures, there is high speci-ficity. However, for the majority of seizures,there is more overlap, as noted in Table 12.13.There is some evidence that carbamazepine hassuperiority over the other drugs for the man-agement of complex partial seizures, but asidefrom this the choice of prescription relates toside effects and the patient’s tolerability. Pheny-toin is particularly unsuitable for a number ofpatients because of its side effects, includingcognitive dulling, hirsutes, gum hypertrophyand acne, with coarsening of the facial features.Teratogenic effects also occur with anticonvul-sant drugs, and several follow-up pregnancyregisters have been set up to examine this. Therate of major malformations is higher in chil-dren born to women who were on polytherapyduring the pregnancy, and sodium valproate inparticular has been associated with major mal-formations, especially spina bifida. This restrictsthe use of this drug in women. Another gender-related problem is the polycystic ovary syn-drome. Polycystic ovaries (PCO) are diagnosedwhen more than ten 2–8 mm ovarian cystsare found on abdominal examination. The syn-drome is diagnosed when the cysts are associ-ated with hyperandrogenism (hirsuitism, acneand male pattern baldness), along with raisedserum androgen.

316 Biological Psychiatry
During pregnancy, serum levels of anticon-vulsants may fall, and they thus need to becarefully monitored if control of the epilepsyproves difficult. The best clinical use and thefull spectrum of side effects of the new drugsare still being evaluated.
Ever since carbamazepine’s introduction forthe management of epilepsy it has been reportedto have psychotropic properties, and its use asa mood stabilizer in manic–depressive illnesshas been widely investigated and reviewed(Post and Uhde, 1986). It appears to be aseffective as conventional neuroleptics in theacute management of mania, and to be equiva-lent to lithium in the long-term prophylaxis ofbipolar affective disorder. Although some tri-als have been carried out on patients who arelithium-resistant, neither this nor the presenceof EEG abnormalities is related to a benefi-cial clinical response. Rapid-cycling patientsand those with secondary mania may respondwell. Some patients respond to a combination ofcarbamazepine and lithium, but not to eitherdrug alone. Carbamazepine is also used inschizoaffective disorders, in the managementof aggression and episodic dyscontrol, and insome schizophrenic patients. Trials in the lattercondition are sparse and the indications for itsuse are not clear.
Other anticonvulsants seem to possessmood-stabilizing properties. However, this isnot a class effect, and it has been most revealedthrough studies in patients with affective dis-orders with sodium valproate and lamotrigine.The latter drug seems better for type-2 asopposed to type-1 bipolar disorder, especiallytreating the depressed phase, and because of theproblem of rashes with rapid increases of serumlevels it is not suitable for acute disorders. Asummary of the data on anticonvulsant use inpsychiatric conditions is given in Table 12.18.
Dosage of the drugs will vary with each indi-vidual, although generally it is wise to startwith a small dose and increase gradually untilsatisfactory serum levels are achieved. Manyanticonvulsants can be given on a once-dailyor twice-daily regime; some are available asextended-release preparations and compliancemay be enhanced by this prescription.
Table 12.18 A summary of the effects of anticonvul-sant drugs in psychiatric disorders
Depression Mania Bipolar Anx’yprophylaxis
Carbamazapine 0 + + 0Oxcarbazapine 0 + 0 0Valproate 0 + ? 0Lamotrigine 0 0 + 0Gabapentin 0 – – 0Topiramate 0 – 0 0Tiagabine 0 – 0 0Pregabalin 0 0 0 +
0 = no evidence of effect.+ = effect shown.− = no studies.
DRUGS FOR THE TREATMENTOF DEMENTIA
Many drug therapies have been used for failingbrains, but most of those advocated in the pastare symptomatic and of little value. Severaldrugs are reported to improve blood flow ormetabolism, although the evidence that theyhelp dementia is minimal. The futility of merelyincreasing blood flow in Alzheimer’s disease orMID has been demonstrated by the PET stud-ies. Cycladenate, isoxsuprine, co-dergocrinemesylate, pentifylline and naftidrofuryl are pastexamples. Hydergine, an ergot alkaloid, appearsto possess mixed dopamine agonist–antagonistproperties, and has been reported in severalshort-term trials (up to 8 mg daily) to improvebehaviour, rather than cognition (MacDonald,1982). Piracetam, thought to enhance acetyl-choline release, is another compound for whichclaims have been made.
Among the most important drugs used inmanagement are the psychotropics. Depressionor a depressive component often responds toantidepressants, although choice of drug isdifficult. Their anticholinergic properties mayincrease cognitive problems and lead to urinaryretention. Imipramine, starting with as smalla dose as 10 mg a day, has been popular; theSSRIs however are also of value. ECT is notcontraindicated.
Of the antipsychotics, the atypicals aredrugs of choice, but warnings over side effects(especially stroke with typical antipsychotics

Biological Treatments 317
and olanzapine and risperidone), maximized inthe elderly, must be heeded. Benzodiazepinesshould be used with caution, and certainly nopatient should be on more than two at the sametime. For nocturnal sedation, the shorter-actingdrugs are preferred, while in the daytime,drugs whose pharmacokinetics are minimallyinfluenced by aging and which have minimaleffect on cognition are needed. Oxazepam andclobazam are examples. Chlormethiazole canprovide a useful alternative to the benzodi-azepines, but barbiturates should be avoided.
The demonstration of the significant reduc-tion in the density of muscarinic and nicotinicreceptors in the brain of Alzheimer’s-diseasepatients led to the development of receptor ago-nists. However, since other transmitter systemsare involved in the pathology, the acetylcholineabnormalities, while they may link to memorychanges, do not necessarily reflect on the otherbehavioural changes so characteristic of demen-tia. Further, as Kopelman (1985) has shown,even the memory deficits are more pervasivethan those provoked by artificial disruption ofacetylcholine activity.
Treatments have either been with cholineprecursors such as choline, deanol or lecithin, orwith anticholinesterases. The main drugs avail-able are tacrine, donazepil, rivastigmine andgalantamine. Rivastigmine and galantamine(extended release) are given once daily, but thereis no evidence that either is more potent than theother. Both are available as a transdermal prepa-rations. It is inadvisable to use more than one ofthese drugs at a time. Side effects include nauseaand vomiting, anorexia, tremor, weight lossand fatigue. The gastrointestinal effects can beminimized by taking the prescription with food.
Memantine is a partial NMDA antagonist.It may be better tolerated than the anti-cholinesterases, and can be combined withthem. Other therapeutic strategies sometimesemployed include giving L-dopa and a decar-boxylase inhibitor (sinemet, madopar) to helpmotor impairments.
Problems inhibiting trials of such treatmentswere until recently lack of any in vivo diagnostictechnique for the vast majority of people withdementia, and the inclusion into trials of such
heterogenous pathological subtypes. Furthercomplicating the area is the lack of a reliablebiomarker that predicts disease progression.Also, the assessment techniques are variable,but a standard assessment scale in clinical trialsis the ADAS-Cog (0–70, a higher score implyinggreater impairment). None of the drugs rec-ommended in Alzheimer’s disease are licensedfor the other dementias, although they maybring benefit, and trials are underway. Anti-cholinesterase inhibitors may however make thesymptoms of fronto-temporal dementia worse.
Future strategies are concentrating more onamyloid-related changes, and ways to deal witheither its accumulation or its resorption. Thera-pies in development include those evolved froma better understanding of the cascade of molec-ular events underlying amyloid deposition, andconcepts derived from the developing geneticsof the disorder. Strategies include inhibition ofbeta- and gamma-secretases, amyloid-loweringagents (tarenflurbil) and decreasing the pro-duction or deposition of β amyloid. Immunetherapies are being investigated; these target β
amyloid, and include immunization with syn-thetic β amyloid or monoclonal antibody infu-sion. Targeting tau is another potential strategy.Varenicline is an antismoking drug which tar-gets nicotinic anticholinergic receptors, and isone of a group of new nicotinic receptor com-pounds which are being tried in the dementias.
MEDICATIONS FOR THE ADDICTIONS
Researchers have made good progress overthe past decade in developing several medica-tions useful in the treatment and managementof the addictions. These can be divided intomedications useful in detoxification, and thosedesigned to block craving and prevent relapse.
Each of the substances of abuse has its owncharacteristic withdrawal pattern, and the drugsused in managing withdrawal are substance-dependent. For example, opiate withdrawal istypically managed by replacing the short-actingopiate with slower-acting agents such asmethadone. More recently, clinicians have usedbuprenorphine. For many years alcohol with-drawal was accomplished by administering

318 Biological Psychiatry
benzodiazapines, particularly to block alcohol-withdrawal seizures. However, some worriedthat it made little clinical sense to replacean addictive compound (alcohol) with amedication that might itself be addictive. Morerecent studies have now shown that alcoholwithdrawal can be treated with nonbenzodi-azapine GABAergic compounds such as carba-mazepine, valproic acid and other nonaddictingmedications such as beta-blockers. Cocainewithdrawal is managed with amantadine,bromocriptine or clonidine.
Classically, alcohol-relapse prevention hasbeen accomplished with self-help groupscombined with disulfiram, which interacts withalcohol to create nausea and flushing. Thereis now intense interest in developing specificanticraving medications for alcoholism. Theseinclude acamprosate, naltrexone, buproprionand verenacline. These agents may also be ofvalue for various other addictions. Pharmaco-logical agents such as GABA agents (topiramate,tiagabine, baclofen and vigabatrin) and agonist-replacement agents (modafinil, disulfiram,methylphenidate) seem to be the most promis-ing in treatment of cocaine dependence. Trials ofantipsychotics are largely negative. Preliminaryresults of human studies with an anticocainevaccine, N-acetylcysteine, and ondansetron arepromising, as are several compounds in pre-clinical development. While opioid dependencehas more treatment agents available than otherabused drugs, none are curative. They can, how-ever, markedly diminish withdrawal symptomsand craving, and block opioid effects due tolapses. The most effective withdrawal methodis substituting and then tapering methadoneor buprenorphine. Alpha-2 adrenergic agentssuch as clonidine can ameliorate untreatedsymptoms or substitute for agonists if not avail-able. Shortening withdrawal by precipitating itwith narcotic antagonists has been studied, butthe methods are plagued by safety issues andpersisting symptoms. Neither the withdrawalagents nor the other methods are associatedwith better long-term outcome, which appearsmostly related to post-detoxification treatment.Excluding those with short-term habits, the bestoutcome occurs with long-term maintenance on
methadone or buprenorphine accompanied byappropriate psychosocial interventions. Thosewith strong external motivation may do well onthe antagonist naltrexone. Currently, optimumduration of maintenance on either is unclear.
BRAIN-STIMULATION THERAPIES
The device-based treatments involving brainstimulation have certain advantages over classi-cal oral medications. Because the devices deliverfocal electricity to specific brain regions, thereare less or no systemic side effects, and there isless worry about drug–drug interactions.
Convulsive Therapy
Although the original observations of vonMeduna led to the introduction of convul-sive therapy with camphor, electroconvulsivetherapy (ECT) was introduced by Cerlettiand Bini for the treatment of schizophrenia.However, it was clear that it gave better resultsin depressive illness, the main indication ofits use today. Although it was eclipsed by thesuccessful introduction of antidepressants inthe 1960s, more recently there has been anupsurge of interest. This has stemmed partlyfrom the realization that antidepressant drugsmay be ineffective in severe affective disorder,and further from the troublesome side effectsof psychotropic drugs that can be seen withlong-term treatment – sometimes required inpsychotic patients – for example the extrapyra-midal complications of neuroleptic drugs. Itscurrent place in therapy has been extensivelyreviewed (Fink, 1986; Malitz and Sackheim,1986; Coffey, 1993). The conclusions of an NIHconsensus-development conference stated:‘ECT is demonstrably effective for a narrowrange of severe psychiatric disorders in a limitednumber of diagnostic categories; delusional andsevere endogenous depression and manic andcertain schizophrenic syndromes’ (ConsensusDevelopment Conference Statement, 1986).
Fink (1986) refers to the changes in behaviourthat occur consequent on ECT, dividing theminto those which are seizure-dependent andthose which are subject-dependent.

Biological Treatments 319
The seizure-dependent effects are a directresult of the seizure or the seizure-inductionmethod and include neurophysiological andhormonal consequences, the majority of whichare usually transient, returning to pretreatmentlevels within days or a few weeks of theseizures. The subject-dependent effects arerelated to the state of the patient at the timeof administration of the seizure, one of themost persistently observed consequences beingelevation of mood in severely depressedpatients, an effect particularly noted in patientswho are suicidal or psychotic.
Stimulus parameters have received consid-erable attention, as has the issue of unilateralor bilateral electrode placement. Waveforms,either sine waves or brief pulse stimuli (shortcurrent bursts with lower energy content), havebeen compared, as have different stimulusintensities. At present there is no evidence ofa difference in therapeutic outcome betweenhigh- and low-energy stimuli, although thelatter provoke less acute cognitive and electro-physiological abnormalities (Weiner, 1986).Caffeine is proconvulsant, and increasesseizure duration.
The issue of whether unilateral ECT is aseffective as bilateral ECT has been the subject ofconsiderable investigation. Memory disruptionis considerably greater with bilateral electrodeplacement, as are other side effects such aspostseizure confusion and headache. Unilateralnondominant-hemisphere seizure dischargeseems to be associated with less intracerebralcurrent and less postictal suppression of thecontralateral hemisphere, and with treatementabout six times higher than seizure threshold isroughly equivalent to bilateral ECT.
Although its use has been established formany years, several double-blind controlled tri-als of ECT have been carried out (see Crowand Johnstone, 1986). The majority of thesehave been in affective disorder, and demon-strate a significant benefit for ECT. A consistentpredictor of response has been the presence ofdelusions, although clinically ‘endogenicity’ hasbeen a valuable guide.
Generally, while the prognosis seemsunrelated to the pretreatment DST status,
normalization of an abnormal DST suggests agood clinical outcome and failure to normalizeshould be cause for concern. Prolactin has beenshown to rise following the seizure (Trimble,1978), elevations being greater for bilateralas opposed to unilateral electrode placement.Abrahams and Schwartz (1985) have reportedan inverse relationship between the prolactinrelease at 15 minutes of the first four treatmentsand clinical outcome. Those with good responseshowed lower peak prolactin elevations thanpoor responders.
Trials against simulated ECT have alsobeen reported for schizophrenia (Taylor andFleminger, 1980), demonstrating the benefit ofthe seizure, and successful use of nondominant-hemisphere unilateral ECT in manic episodeshas been shown (Small et al., 1986). Other situa-tions where ECT has occasionally been helpfulhave been in the management of Parkinson’sdisease, organic mental disorders (particularlyassociated with severe affective disorder),delirium and epilepsia partialis continua (whereit is used in order to bring the seizure to an end).
The mechanism of action of ECT is notknown. Changes of brain function evolve overtime, reflected in the usual clinical practice ofadministering therapy two or three times aweek. The antidepressant effect was initiallythought to be directly related to the seizureactivity (Ottosson, 1960), cumulative seizureduration being an important variable. Maletsky(1978) estimated that if total seizure time wasless than 201 seconds, no response was noted;most patients respond after 1000 seconds,with little additional improvement beyondthis being noted. However, seizures for ECT,while necessary, are not sufficient. For example,Sackeim and colleagues have shown in severalstudies that generalized seizures triggered byelectrodes over the parietal lobe are ineffective,as are some inadequate doses of prefrontaltreatment. Clearly the therapeutic effects ofECT must involve an interplay between localcharge density in certain prefrontal regionsand the results of the actual seizure. This lineof reasoning then directly intersects with theother brain-stimulation techniques that areinfluencing brain activity in these same regions.

320 Biological Psychiatry
ECT has an anticonvulsant effect, greater withbilateral as opposed to unilateral treatment.With the former, this averages 87% during acourse of treatment, but it does not seem to bepersistent over long periods of time after theend of ECT (Nobler and Sackheim, 1993).
In animal models a consistent effect is down-regulation of presynaptic 5-HT1A, alpha-2 andbeta-adrenergic receptor sites, and enhancedbehavioural responses to 5-HT, possibly relatedto increased numbers of 5-HT2 receptors, havebeen noted. Dopamine-related behaviours arealso shown to be enhanced by repeated seizures(Green, 1986). Other reported changes includeincreased release of GABA and increasedGABAb binding, increased opioid binding andincreased limbic neuropeptide-Y and TRH lev-els (Mikkelsen et al., 1994; Nutt and Glue, 1993).Both the GABA and the opiate changes mayexplain the inherent anticonvulsant propertiesof ECT. While some of the effects, especially onthe adrenergic receptors, which may reflect onincreased synaptic noradrenergic activity, aresimilar to the effects of other antidepressants,the effects of ECT at the 5-HT2 receptor arethe opposite.
In man, Slade and Checkley (1980) exam-ined growth-hormone responses to clonidineand methylamphetamine in patients with affec-tive disorder before and after a course of ECT.No significant changes were noted. The effectsof ECT on neuroendocrine responses to apomor-phine have also been reported but are variable.
ECT increases CSF 5-HIAA and HVA(Rudorfer et al., 1988), and enhances the pro-lactin response to fenfluramine, suggestingincreased 5-HT activity (Shapira et al., 1992).
The effects of ECT on CBF using SPECTand PET show consistent increases immedi-ately, with postictal hypoperfusion. The latteris not evenly distributed over the cortex, and isrelated to the site of electrode placement. Fur-ther, it persists after a full course of treatment,and the degree of acute reduction, especially infrontal cortex, predicts response, nonrespondersshowing no CBF decline (Rubin et al., 1994).
Contraindications to the use of ECT are few,but include the presence of intracranial tumoursand a recent cerebrovascular accident. Since
an increase in CSF pressure occurs during theseizure discharge, ECT is best avoided in con-ditions where raised intracranial pressure issuspected. It carries with it minimal risk ofmortality, and the morbidity is more related tocomplications of the accompanying anaestheticthan to the therapy itself.
Two recent developments with ECT deservenote. Sackeim and colleagues have begun usingultrabrief pulse ECT, where the pulse widthapproaches the minimum necessary to causedepolarization. Importantly, right unilateralultrabrief ECT appears as effective as bilateralregular-pulse ECT, without any of the associatedcognitive side effects (Sackeim et al., 2008).
The other trend with ECT has been in study-ing the relapse rates following a course oftreatment and which maintenance medicationswork best. Most studies find a 50% relapse rate atsix months, even with aggressive maintenance-medication treatment (Petrides et al., 2001).
Transcranial Magnetic Stimulation (TMS)
This is perhaps the most interesting of thenew brain-stimulation techniques, because theskull does not need to be opened in order tostimulate the brain, and to date there appearto be only limited side effects (George, 2002;George and Belmaker, 2000; George et al., 2002).TMS involves creating a powerful electricalcurrent near the scalp. The electricity flowingin an electromagnetic coil resting on thescalp creates an extremely potent (near 1.5Tesla) but brief (microseconds) magnetic field.Although skin and bone act as resistors toimpede electrical currents, magnetic fields passunimpeded through the skull and soft tissue.The importance of this is that the TMS magneticfield enters the surface of the brain withoutinterference. There it encounters nerve cellswith resting potentials, and induces electricalcurrents to flow. Thus, electrical energy isconverted to magnetic fields, which are thenconverted back into electrical currents in thebrain (Bohning, 2000). TMS is thus sometimescalled ‘electrodeless electrical stimulation’.
The magnetic field acts to bridge the skull.Although magnetic fields do have biological

Biological Treatments 321
effects on tissue, the vast majority of TMS effectslikely derive not from the magnetic fields butrather from the induced electrical currents gen-erated in the brain. TMS, with powerful butextremely brief magnetic fields, differs fromwearing (or sleeping on) constant low-field mag-nets. TMS directly electrically stimulates thebrain, while constant weak magnets do notinduce currents.
The idea of using TMS, or something akinto it, to alter neural function goes back to atleast the early 1900s. Pollacsek and Beer, psy-chiatrists working in Vienna at the same timeas Freud, filed a patent to treat depressionand neuroses with an electromagnetic devicethat looks surprisingly like modern TMS (Beer,1902). The modern TMS era began in 1985 whenBarker and colleagues, working in Sheffield, UK,created a focal electromagnetic device with suf-ficient power to induce currents in the spine(Barker et al., 1985, 1987). They quickly realizedthat their device could also directly and non-invasively stimulate the human brain. It couldonly stimulate the surface of the brain, how-ever, as the magnetic field falls off sharply withdistance from the coil. Several researchers areworking on more powerful TMS devices thatmight stimulate deeper.
A single pulse of TMS, applied over themotor cortex, produces a jerk-like movementin the hand, arm, face or leg, depending onwhere the coil is positioned. A single pulseapplied over the back of the brain can produce aphosphene. However, that is about the extentof the immediate positive effect that single-pulse TMS can produce. TMS pulses applied inrhythmic succession are referred to as repetitiveTMS or rTMS. rTMS can create behaviours notseen with single pulses, including the potentialrisk of causing an unintended seizure. Twentyseizures have occurred in the history of itsuse, twelve unintended, out of an unclear totalamount of use. All seizures have occurred dur-ing stimulation, rather than later, and have beenself-limited, with no sequelae. rTMS seizuresare more likely to occur with certain combi-nations of TMS intensity, frequency, durationand interstimulus interval (Wassermann, 1997;Wassermann et al., 1996).
Much research is underway to determineexactly which neurone TMS effects, and the cas-cade of neurobiological events that follows stim-ulation. Different factors such as gyral anatomy(how the brain is shaped), the distance fromthe skull to the brain (brain atrophy) and theorientation of nerve fibres relative to coil areall important.
One of the more interesting rTMS effects isthat for brief periods of time, during stimula-tion, rTMS can block or inhibit a brain func-tion. That is, rTMS over the motor area thatcontrols speech can temporarily render the sub-ject speechless (motor aphasia), only while thedevice is firing. Cognitive neuroscientists haveused this knockout aspect or ‘temporary lesion-ing’ ability of rTMS to re-explore and test thelarge body of information gleaned from yearsof studying stroke patients. Additionally, twopulses of TMS in quick succession can provideinformation about the underlying excitability ofa region of cortex. This diagnostic technique,called paired-pulse TMS, can demonstrate thebehaviour of local interneurons in the motor cor-tex and serve as an indirect measure of GABAor glutamate activity.
Single nerve cells form themselves intofunctioning circuits over time through repeateddischarges. Externally stimulating a singlenerve cell with low-frequency electrical stim-ulation can cause long-term depression, wherethe efficiency of links between cells diminishes.High-frequency stimulation over time cancause the opposite effect, called long-termpotentiation. These behaviours are thought tobe involved in learning, memory and dynamicbrain changes associated with networks. Avery exciting aspect of TMS research, and ofthe other brain-stimulation techniques, is theexamination of whether or not one can useexternal brain stimulation to change braincircuits over time in a manner analogous tolong-term depression or long-term potentiation.Although this is still controversial and not fullyresolved, there are a number of rTMS studiesshowing inhibition or excitation lasting for upto several hours beyond the time of stimulation.The clinical implications here are profound:one could begin to use TMS or other techniques

322 Biological Psychiatry
to change learning and memory, or resculptbrain circuits. Some basic physiological studiesindicate that one can best change a circuit whilethe behaviour is ongoing, and the cells involvedin the various neural pathways are acting asa circuit (Barnes et al., 1994; Bartsch and vanHemmen, 2001; Stanton and Sejnowsky, 1989).It is an important question whether rTMSshould be delivered while patients are thinkingabout important topics or abreacting (Amatet al., 2008). Thus, in the near future one mightcombine rTMS with modified forms of talkingor cognitive behavioural therapy.
Animal and cellular studies with TMS rein-force that it is a powerful technique able to alterneuronal function. One stumbling block in usingTMS in animals is that it is hard to make TMScoils that are the same size relative to humans.Small coils simply explode. Thus, most animalTMS studies have not really used focal TMSas in humans, especially small-animal studies.Nevertheless, studies have shown that rTMSenhances apomorphine-induced stereotypyand reduces immobility in the Porsolt swim test(Fleischmann et al., 1996), and induces electro-convulsive shock (ECS)-like changes in rodent-brain monoamines, beta-adrenergic receptorbinding and immediate early gene induc-tion (Ben-Sachar et al., 1997). Most recently,researchers have found that rTMS can induceneurogenesis (Jennum and Klitgaard, 1996).
A critically important area that will ulti-mately guide clinical parameters is to combineTMS with functional imaging to directly moni-tor TMS effects on the brain, and to thus under-stand the varying effects of different TMS useparameters on brain function. Since it appearsthat rTMS at different frequencies has divergenteffects on brain activity, combining TMS withfunctional brain imaging will better delineatenot only the behavioural neuropsychology ofvarious psychiatric syndromes, but also some ofthe pathophysiologic circuits in the brain. In con-trast to imaging studies with ECT, which havefound that ECT decreased global and regionalactivity (Nobler et al., 2001), most studies usingserial scans in depressed patients undergoingrTMS have found increased activity in the cin-gulate and other limbic regions (Shajahan et al.,
2002; Teneback et al., 1999). However, two stud-ies have now found divergent effects of rTMSon regional activity in depressed patients, deter-mined both by the frequency of stimulation andthe baseline state of the patient (Mitchel, 2002;Speer et al., 2000). That is, in patients with globalor focal hypometabolism, high-frequency pre-frontal stimulation increases brain activity overtime. Patients with focal hyperactivity have beenshown to have reduced activity over time fol-lowing chronic daily low-frequency stimulation.Although these two small sample studies havenumerous flaws, they simultaneously show thepotential, and the complexity, surrounding theissue of how to use rTMS to change activity indefined circuits. They also point out an obviousdifference with ECT, where the net effect of theECT seizure is to decrease prefrontal and globalactivity (Nobler et al., 2001).
Therapeutic Uses of rTMS
Although there is controversy, and much morework is needed, certain brain regions have con-sistently been implicated in the pathogenesis ofdepression and mood regulation (see Chapter 8).These include the medial and dorsolateral pre-frontal cortex, the cingulate gyrus, and otherregions commonly referred to as limbic (amyg-dala, hippocampus, parahippocampus, septum,hypothalamus, limbic thalamus, insula)and related cortex (anterior temporal pole,orbitofrontal cortex). A widely-held theory overthe last decade has been that depression resultsfrom a dysregulation of these prefrontal corticaland limbic regions (see Chapter 8) (George et al.,1994a, 1995a; Mayberg et al., 1999). The veryfirst uses of rTMS as an antidepressant werenot influenced by this regional neuroanatomicliterature, and stimulation was applied overthe vertex (Beer) (Kolbinger et al., 1995; Grisaruet al., 1994). However, working within theprefrontal cortical limbic dysregulation theoryoutlined above, and realizing that theories ofECT action emphasize the role of prefrontal cor-tex effects (Nobler et al., 2000), in 1995 Georgeand Post performed the first open trial ofprefrontal rTMS as an antidepressant, followedimmediately by a crossover double-blind study.

Biological Treatments 323
Their reasoning was that chronic, frequent, sub-convulsive stimulation of the prefrontal cortexover several weeks might initiate a therapeuticcascade of events both in the prefrontal cortexand in connected limbic regions, thereby caus-ing the dysregulated circuits to rebalance andnormalize, alleviating depression symptoms(George and Wassermann, 1994). The imagingevidence previously discussed now shows thatthis hypothesis was largely correct: prefrontalrTMS sends direct neural information toimportant mood-regulating cerebral regionssuch as the cingulate gyrus, orbitofrontal cortex,insula and hippocampus. Thus, beginning withthese prefrontal studies, modern TMS wasspecifically designed as a focal, nonconvulsive,circuit-based approach to therapy.
Since the initial studies, there has been contin-ued high interest in rTMS as an antidepressanttreatment. There are now over 30 publishedrandomized controlled clinical trials (RCTs) indepression, and 5 independent meta-analysesof the published or public rTMS antidepres-sant literature, each differing in the publicationsincluded and the statistics used (Burt et al.,2002; Holtzheimer et al., 2001; Kozel and George,2002; Martin et al., 2002; McNamara et al., 2001).These largely conclude that daily prefrontalTMS delivered over several weeks has antide-pressant effects greater than sham treatment.Several studies have compared rTMS to ECT,without finding differences in efficacy in smallsample studies. rTMS was clearly better toler-ated than ECT, with no cognitive side effects andno need for repeated general anaesthesia. In asimilar but slightly modified design, Pridmore(2000) reported a study comparing the antide-pressant effects of standard ECT (three timesa week) versus one ECT a week followed byrTMS on the other four weekdays. At threeweeks he found that both regimens producedsimilar antidepressant effects. An Israeli grouprecently published that relapse rates in thesix months following ECT versus rTMS weresimilar (Dannon et al., 2002). In sum, these stud-ies suggest that rTMS clinical antidepressanteffects are in the range of other antidepressants,and persist as long as the clinical effects fol-lowing ECT.
A multisite industry-sponsored RCT of 301patients with major depression, medication-free, has recently been published (O’Reardonet al., 2007). rTMS was delivered five timesper week at 10 Hz frequency and 120% ofmotor threshold, for a period of 4–6 weeks.Active rTMS was significantly superior to shamTMS. rTMS was well tolerated, with a lowdropout rate for adverse events (4.5%). Theadverse events observed were mild, and limitedto transient scalp discomfort or pain. Therewere no seizures. These data resulted in FDAapproval in October 2008 of rTMS as a treatmentfor depression.
Although the literature suggests that pre-frontal rTMS has an antidepressant effect greaterthan sham, and that the magnitude of this effectis in the range of other antidepressants, manyissues are not resolved. Work done to date hasshown clear evidence that prefrontal rTMS pro-duces immediate (George et al., 1999; Li et al.,2002; Nahas et al., 2001; Paus et al., 2001; Strafellaet al., 2001) and longer-term (Teneback et al.,1999) changes in mood-regulating circuits. Thus,the original hypothesis about its antidepressantmechanism of action is still the most likely expla-nation. What remains unclear is which specificprefrontal or other brain locations might be besttargeted for treating depression, and whetherthis can be determined with a group algorithmor needs individual imaging guidance. For themost part, the coil has been positioned usingthe rule-based algorithm to find the prefrontalcortex that was used in the early studies (Georgeet al., 1995b). However, this method was shownto be imprecise in the particular prefrontalregions stimulated directly underneath the coil,depending largely on the subject’s head size(Herwig et al., 2001). Additionally, most stud-ies have stimulated with the intensity neededto cause movement in the thumb (called themotor threshold). There is now increasing recog-nition that higher intensities of stimulation areneeded to reach the prefrontal cortex, especiallyin elderly patients, where prefrontal atrophymay outpace that of motor cortex, the site atwhich the motor threshold is measured (Kozelet al., 2000; McConnell et al., 2001; Mosimannet al., 2002; Padberg et al., 2002). There is only

324 Biological Psychiatry
limited data on using rTMS as a maintenancetreatment in depression.
rTMS as a Treatment for Other PsychiatricConditions
rTMS has also been investigated as a possibletreatment for a variety of neuropsychiatricdisorders. In general, the published literaturein these conditions is much less extensive thanfor rTMS as an antidepressant, and thereforeconclusions about the clinical significance ofeffects must remain tentative until large-samplestudies are conducted. Hoffman and colleagueshave used repeated daily session of low-frequency rTMS over the temporal lobes to treathallucinations in patients with schizophrenia(Hoffman et al., 1998). Some but not all groupshave replicated these effects (d’Alfonso et al.,2002; Fitzgerald et al., 2006; Hoffman et al., 1998,2000; Jin et al., 2006; Rollnik et al., 2000).
Several studies have shown promise in usingrTMS to treat OCD. In the initial study in thefield, Greenberg et al. (1997) found that a singlesession of right-prefrontal rTMS decreasedcompulsive urges for eight hours. Mood wasalso transiently improved, but there was noeffect on anxiety or obsessions. Two otherstudies have examined possible therapeuticeffects of rTMS in OCD. A double-blind studyusing right-prefrontal slow (1 Hz) rTMS and aless-focal coil failed to find statistically signif-icant effects greater than sham (Alonso et al.,2001). In contrast, a recent open study in a groupof 12 OCD patients, refractory to standard treat-ments, who were randomly assigned to right- orleft-prefrontal fast rTMS, found that clinically-significant and sustained improvement wasobserved in one-third of patients (Sachdevet al., 2001). Finally a recent group stimulatedthe supplemental motor area (SMA) and foundclinical improvements in OCD and Gilles de laTourette’s syndrome (Mantovani et al., 2006).
Mood-regulating circuits in the brain highlyoverlap with the neural pathways involved inpain regulation, especially the regions involvedin determining the subjective discomfort of thepain. Thus, some researchers have begun explor-ing whether rTMS might have a therapeutic
role in treating acute or chronic pain. There arereports that rTMS over either prefrontal cor-tex or motor cortex can acutely decrease painin healthy adults or patients with chronic pain(Lefaucheur et al., 2001; Pridmore and Oberoi,2000). A recent RCT found that a single 20-minute session of left-prefrontal rTMS given topatients in the recovery room following surgeryreduced self-administered morphine use by 40%(Borckardt et al., 2006).
Overall, rTMS is a promising new therapy,as well as research tool. The bulk of clinicalwork to date has been in depression, whereit is now FDA-approved, but research showsthat it has potential applications in several otherpsychiatric disorders.
Vagus-nerve Stimulation (VNS)
TMS is non-invasive, focal and largely limitedto different cortical sites, and is given intermit-tently. VNS is in some sense the opposite ofthis as it is invasive, requiring surgical implan-tation of a device in the chest wall and a wire inthe neck. The brain region stimulated is alwaysthe same initial route: the vagus nerve in theneck. It is also a permanent implant in that itcannot easily be implanted and then removedwithout surgery. VNS has been approved foralmost 15 years as a treatment for epilepsy(Ben-Menachem et al., 1994; George et al., 1994b;Salinsky et al., 1996; Uthman et al., 1993; VagusNerve Stimulation Study Group, 1995) and isalso approved for the chronic treatment of recur-rent treatment-resistant depression.
The vagus nerve helps regulate the body’sautonomic functions, which are important ina variety of emotional tasks. For reasons thatare unclear, most people are more familiar withthe vagus nerve’s efferent functions, where itserves as the messenger for signals from thebrain to the viscera. Traditionally, the vagusnerve has been considered a parasympatheticefferent nerve (controlling and regulating auto-nomic functions such as heart rate and gastrictone). The afferent role of the vagus has beenunderemphasized in the traditional literature.The vagus is actually a mixed nerve, composedof about 80% afferent sensory fibres carrying

Biological Treatments 325
information to the brain from the head, neck,thorax and abdomen (Foley and Dubois, 1937).
Over the past 100 years several differentresearchers have convincingly demonstratedthe extensive projections of the vagus nervevia its sensory afferent connections in thenucleus tractus solitarius (NTS) to diverse brainregions (Ammons and Blair, 1983; Bailey andBremer, 1938; Otterson, 1981; Rutecki, 1990;Zardetto-Smith and Gray, 1990). Reasoningin part from this body of literature, Zabarademonstrated an anticonvulsant action of VNSon experimental seizures in dogs (Zabara, 1992).Zabara hypothesized that VNS could prevent orcontrol the motor and autonomic componentsof epilepsy. Penry and others ushered in themodern clinical application of VNS in 1988,using an implanted device to treat epilepsy(Penry and Dean, 1990; Uthman et al., 1993).
Although the route of entry into the brainis constrained, VNS offers the potential formodulating and modifying function in manybrain regions, through trans-synaptic connec-tions (Henry, 2002; George et al., 2000; Nemeroffet al., 2006). Briefly, incoming sensory (affer-ent) connections of the vagus nerve providedirect projections to many of the brain regionsimplicated in neuropsychiatric disorders. Theseconnections provide a basis for understandinghow VNS might be a portal to the brainstem andconnected limbic and cortical regions. Thesepathways likely account for the neuropsychi-atric effects of VNS, and they invite additionaltheoretical considerations for potential researchand clinical applications. Functional imagingstudies in patients with implanted VNS stim-ulators have largely confirmed this importantneuroanatomy of the vagus (Bohning et al., 2001;Chae et al., 2003; Conway et al., 2006; Henry et al.,1998, 1999; Lomarev et al., 2002; Mu et al., 2004).
VNS Methods
VNS has been commercially available for thetreatment of resistant partial-onset seizures inEurope since 1994, and in the USA since 1997.The surgery for implanting the VNS generatorin the chest is much like inserting a cardiac pace-maker. In both VNS and cardiac pacemakers, a
subcutaneous generator sends an electrical sig-nal to an organ through an implanted electrode.With VNS, the electrical stimulation is deliveredthrough the generator, an implantable, multi-programmable, bipolar pulse generator (aboutthe size of a pocket watch) that is implanted inthe left chest wall to deliver electrical signals tothe left vagus nerve through a bipolar lead. Theelectrode is wrapped around the vagus nervein the neck, and is connected to the genera-tor subcutaneously. The VNS generator can becontrolled by a personal computer or PDA con-nected to an infrared wand. As a safety feature,the generator is designed to shut off in the pres-ence of a constant magnetic field. Each patientis thus given a magnet that, when held over thepulse generator, turns off stimulation. When themagnet is removed, normal programmed stim-ulation resumes. This allows patients to controland temporarily eliminate stimulation-relatedside effects during key behaviours like pub-lic speaking (voice tremor) or heavy exercising(mild shortness of breath).
Therapeutic Uses of VNS
VNS has been most extensively studied asa treatment for epilepsy. Two double-blindstudies have been conducted in patientswith epilepsy, with a total of 313 treatment-resistant completers (Ben-Menachem et al., 1994;Handforth et al., 1998). In this difficult-to-treatgroup, the average decline in seizure frequencywas about 25–30% compared to baseline. Inter-estingly, the longer the treatment was applied,the better the clinical response rates.
Most epilepsy patients with VNS have notbeen able to reduce or withdraw antiepilepticmedications. Thus VNS, as now delivered, hasnot been shown to be a substitute for anticon-vulsant medications, although in some patientsthe dosage levels or numbers of anti-epilepticmedications have been decreased with the addi-tion of VNS. VNS is increasingly being used inchildren with epilepsy, in part because of its lackof negative cognitive effects, which are commonto other anticonvulsants (Helmers et al., 2001).
There are several different programmablevariables in determining how to deliver VNS.

326 Biological Psychiatry
These ‘use parameters’ include the pulse widthof the electrical signal (130, 250, 500, 750,1000 µs), the intensity (0.25–4 mA is clini-cally tolerated), the frequency of stimulation(1–145 Hz), the length of stimulation (7–270seconds) and the length of time betweentrains of stimuli (0.2 seconds to 180 minutes).In general, the initial epilepsy studies usedsettings that derived from the animal studieswhere anticonvulsant effects were found. Thesestudies compared efficacy in two groups,based on different use parameters. There was ahigh-stimulation group (30 Hz, 30 seconds on,5 minutes off, 500 µs pulse width) and a low-stimulation group (1 Hz, 30 seconds on, 90–180minutes off, 130 µs pulse width). The majority ofthe VNS epilepsy efficacy and safety data comefrom trials with use parameters similar to thoseused in the high-stimulation group. Similarly,most of the data from other neuropsychiatricdisorders (depression, anxiety) involve VNS atuse parameters similar to those used in the ini-tial epilepsy studies. It is difficult to imagine thatthese use parameters are the maximally effec-tive choices, or that the same parameters workequally well in all conditions and all patients.Epilepsy physicians commonly switch nonre-sponding patients to use-parameter settings thatare different from their current settings. How-ever, there has been no clear demonstration thatchanging settings improves efficacy. Furtherwork toward understanding the translationalneurobiology of these use-parameter choices,and how they relate to clinical symptoms, is thekey area for future growth of the field.
There is a long history in biological psychi-atry where anticonvulsant medications (e.g.carbamazepine) or devices (e.g. ECT), have beenfound to have mood-stabilizing or antidepres-sant effects. In early 1998, there were severallines of evidence to suggest that VNS mighthave antidepressant effects. Anecdotal reportsof mood improvement in VNS-implantedepilepsy patients, knowledge of vagus functionand neuroanatomy, brain-imaging studies,work in animals and CSF studies all supportedan initial pilot clinical trial in treatment-resistantdepression (George et al., 2000).
In June 1998, the first depression patient wasimplanted at MUSC in Charleston, launchingan open study of VNS for the treatment ofchronic or recurrent treatment-resistant depres-sion (called D-01). This study involved four sites(MUSC, Charleston; Columbia PI, NY; UTSW,Dallas; Baylor, Houston) and initially involved30 subjects (Rush et al., 2000), with a later exten-sion of 30 more subjects to clarify the effectsize and look for response predictors (Sackeimet al., 2001b). The study design involved select-ing patients with treatment-resistant, chronicor recurrent major depressive episodes (MDEs)(unipolar or nonrapid cycling bipolar) and thenadding VNS to a stable regimen of antidepres-sant medications or no antidepressant medica-tions. No stimulation was given for the first twoweeks following implantation, creating a single-blind placebo phase and allowing for surgicalrecovery. All patients met eligibility criteria byfailing at least two adequate treatment trials inthe current episode.
Ten weeks of VNS therapy were pro-vided, with medications held constant. Of 59completers (1 patient improved during therecovery period), the response rates were 30.5%for the primary Hamilton Rating Scale forDepression (HRSD28) measure, 34.0% for theMontgomery–Asberg Depression Rating Scale(MADRAS) and 37.3% for the Clinical GlobalImpression-Improvement score (CGI-I of 1 or 2).VNS was well tolerated in this group, with sideeffects similar to those encountered by epilepsypatients. The most common side effect wasvoice alteration or hoarseness (60.0%, 36/60),which was generally mild and related to theintensity of the output current. There were noadverse cognitive effects (Sackeim et al., 2001a).
The only response predictor was priortreatment-resistance. VNS as used in this openstudy was more effective in depressed patientswho were less treatment-resistant.
These encouraging initial results served asthe basis for a US multisite double-blind trial ofVNS for chronic or recurrent, low-to-moderatetreatment-resistant depression. In this trial,active VNS failed to show a statistically signifi-cant difference in acute response from the sham

Biological Treatments 327
group (Rush et al., 2005). The sham responserate was 10%, with the active response 15%.
The longer-term response rates for VNS-implanted depression patients are encourag-ing (Nahas et al., 2005) and appear better thanwould be expected in this population (Rushet al., 2006). A parallel but nonrandomized com-parison found that patients with VNS implantedhad better outcomes at one year than a groupreceiving treatment as usual (George et al., 2005).These data served as the basis for FDA approvalof VNS for the chronic (not acute) treatmentof chronic recurrent depression. Thus, VNS isFDA approved, although there is no double-blind evidence for VNS as an antidepressantin patients with depression. There are how-ever open (Harden et al., 2000) and double-blind(Elger et al., 2000) studies showing that VNS hasantidepressant effects in epilepsy patients withcomorbid depression.
In conclusion, VNS has an important rolein the treatment of epilepsy. However, theonly clinical effects that have been shownwith double-blind studies are in epilepsy forseizure control and depression occurring in thesetting of epilepsy. There are many areas wheremore information would facilitate its adoption.Compared to psychotherapy, medications andeven ECT, VNS requires a different approach totreating depression. Whereas other treatmentscan be begun and sampled and then easily aban-doned if not effective, VNS, with the installationof an implant, requires careful considerationprior to initiating therapy. Currently there isno non-invasive method of VNS that couldbe tried prior to a permanent implant. Thus,it is crucial to determine from available datawho will likely respond (or not). Additionally,because of the relatively large initial capital costof implanting a VNS generator, data are neededto convince payers that VNS is cost-effective.An initial implantation fee of around US$20 000(device and surgery) is about equal to one weekof hospitalization, or a course of outpatientECT. VNS would thus be cost-effective in thoserecurrent chronically-ill patients where implan-tation results in clinical improvements thateliminate the need for hospitalization, ECT or
more frequent and aggressive outpatient medi-cation management. Another radical differencebetween VNS and medication treatments is thatVNS facilitates almost 100% adherence. Thedevice, once implanted, cycles on and off with-out problems for several years. Many studieshave shown that even the best patients skip andforget medications, with resultant problems intheir clinical course. VNS is thus a most inter-esting new approach to treating depression, butmore information is critically needed.
Resective or Ablative Brain Surgery(Psychosurgery)
The early experiments of Fulton and Jacobsen(1935) demonstrated that primates with destruc-tion of the frontal lobes became more placid andless anxious. Moniz (1936) became the first tosever connections between the frontal lobes andother areas of the limbic system in psychiatricpatients, which led Freeman and Watts (1947) todevelop a standardized leucotomy technique.
The early operations were radical frontal leu-cotomies in which a large section of white matterwas severed between the frontal lobes and therest of the brain, but since that time the operationhas been remarkably refined. Restricted frontalleucotomy was followed by orbital undercuttingin which only the medially-situated frontotha-lamic fibres were destroyed. Other selectivelesions include cingulectomy, in which the ante-rior 4 cm of the cingulum is removed, andsubcaudate tractotomy, in which lesions areplaced beneath the head of the caudate nucleus.Stereotactic techniques have been used to placelesions with greater accuracy, and during somesurgical procedures stimulation is carried out.This provokes subjective experiences in patients,but is also used to evaluate autonomic changessuch as alteration of heart rate, blood pressureand forearm blood flow in order to locate sitesfor surgical destruction. In one procedure, mul-tifocal leucocoagulation, patients have lesionsmade through chronically-implanted electrodesafter various intervals of time, and the changein symptoms is continuously observed. When

328 Biological Psychiatry
clinical status improves, further lesions are with-held. In cingulotomy, lesions are placed bilater-ally in the cingulum bundle, and capsulotomytargets the anterior limb of the internal capsule.A stereotactic gamma unit in which radioac-tive cobalt rays are directed at a selected targetusing the gamma knife, can be used for the lat-ter operation, which avoids the necessity of acraniotomy (Mindus and Nyman, 1991).
The main frontolimbic connections that aresevered pass from the lower medial quadrant ofthe frontal lobe to the septal and nucleus accum-bens regions, thalamus and hypothalamus.Additional target areas are the frontocingularconnections passing to the cingulate gyrusand hippocampus. The subcaudate pathwayinterrupts frontal and temporal connections,in addition to the ascending monamine pro-jections from the ventral tegmental area to thefrontal cortex.
In capsulotomy, fibres between the frontalcortex and the limbic system and basal gangliaare lesioned.
Although the very early techniques had amortality of around 6% and a high morbidity,the modified and restricted operations canbe carried out safely. Mitchell-Heggs et al.(1976) presented data on 66 patients who hada limbic leucotomy; 73% were improved at6 weeks and 76% at 16 months. The best resultswere in obsessional neurosis, anxiety anddepression, although six of seven schizophrenicpatients also responded, particularly if theschizophrenic symptoms were accompaniedby anxiety, depression or obsessional states. Inthis follow-up, no intellectual deterioration wasnoted, and adverse personality changes werereported as minimal. Clinical improvementsoccurred gradually, for up to a period of a year.Patients with good premorbid personalitiesdid better than those with poor preoperativeadjustment. Patients with obsessional illnessseemed to do particularly well with stereotacticlimbic leucotomy.
Bridges et al. (1994) have reported on theresults of a large series of patients after subcau-date tractotomy, with 40–60% of patients goingon to live normal or near-normal lives. Therewas a 1% postoperative suicide rate, compared
with 15% in cases of affective-disorder controls.Similarly, the follow-up data with capsulo-tomy (Mindus and Nyman, 1991) reveal 70%symptom-free or ‘much improved’ at 1–7 yearsof follow-up.
Postoperatively, marked frontal-lobe oedemacan be seen on the MRI scan and a characteristicfrontal slow-wave activity is seen on the EEG.The amount of this shortly after the operationcorrelates with a beneficial clinical outcome oneyear later (Evans et al., 1981).
The indications for brain surgery for psy-chaitric disorders have been clarified. Patientsshould have had a severe psychiatric illness, bepotentially suicidal and have been ill for an aver-age of 10 years. Further, they must have beenshown to have failed to respond to all alternativeforms of therapy, including a good trial withavailable psychotropic medications. The bestresponses are seen in patients suffering fromdepression and obsessional neurosis, with goodpremorbid personalities, and from a stable homeenvironment. Some schizophrenic patients dowell, showing a reduction in the number oftheir psychotic episodes and a reduced need forphenothiazine medication. Psychopathy is anabsolute contraindication, and patients who areaddicted to drugs or alcohol are not suitable.Complications include cerebral haemorrhage,postoperative suicide, postoperative seizures,personality changes, urinary and faecal inconti-nence, increased weight, sleep disturbance anddiabetes insipidus.
Other neurosurgical procedures used to ame-liorate psychopathology include unilateral orbilateral amygdalotomy in patients with aggres-sion, especially lesions of the medial amygdalain the relief of aggressive behaviour distur-bances associated with epilepsy (Narabayashi,1971). Thalamotomy has been used for obses-sional illness, while placing lesions in thehypothalamus and stria terminalis has beentried for aggression.
Deep-brain Stimulation (DBS)
Instead of permanently resecting or lesioning anarea of the brain, one can stimulate the regionelectrically with an electrode and temporarily

Biological Treatments 329
‘knock out’ its function. Because of its morefavourable safety profile compared to resectivesurgery, and the potential for withdrawing thestimulator if the effects are not satisfactory, DBShas replaced resective brain surgery for OCDor depression. Typically the DBS electrodesare small wires with exposed terminals at thevery end of the wire. These contacts are placedneurosurgically with MRI and CT image guid-ance. Once the wires are in place the electrodesare connected to external generators implantedunder the skin in the chest. For the treatment ofParkinson’s disease and dystonia, the DBS elec-trodes are implanted in the suthalamic nucleus(STN) or the globus pallidus interna (Gpi).The electricity is delivered at high frequency(>100 Hz) constantly. The anti-tremor effectsare immediate in PD, while the anti-dystoniaeffects take weeks or months to emerge, evenwith constant high-frequency stimulation.
DBS has been studied for both OCD anddepression. The evidence base for DBS in OCDis slightly greater than that for depression, butfor both conditions the number of publishedcases is less than 100. For OCD, researchershave followed the neurosurgical literatureand have implanted the electrodes in theanterior limb of the internal capsule, whichthen approaches the nucleus accumbens. TheFDA refers to this electrode placement as theALICNA; depending on which of the fourelectrode positions one uses, the same electrodecan interfere with different brain regions.ALICNA implantation of refractory OCD hasbeen granted a humanitarian device exemption
by the US FDA. In the early OCD studies of theALICNA location, researchers were struck bythe antidepressant effects, and some have usedthis electrode location for treatment-resistantdepression. Another location for depressioninvolves implanting in the white-matter fibresimmediately lateral to the subgenual cingulate.Further research is needed for these invasiveand risky procedures, which are not yet clinicaltreatments.
SLEEP-DEPRIVATION THERAPY
It has been observed for some time that ifa patient with a depressive illness is keptawake for the whole night, elevation of moodoccurs. This is often only transient, althoughthere are anecdotal reports of some patientshaving a sustained benefit. The technique canbe used to help with diagnosis, the alterationof mood confirming the presence of an affec-tive disorder.
Wu et al. (1992) reported that over 50% ofpatients with an affective disorder will showa response to deprivation, and in bipolarpatients transient hypomania can be seen inup to 30%. They postulated that in sleep, anendogenous substance is released that causesdepression, in contrast to an alternative theorythat an endogenous antidepressant substanceis released in wakefulness. In other studiesit has been shown using PET that increasedcingulate activity before deprivation predictsthe antidepressant response (Ebert et al., 1994).


13Epilogue: Progress toward
a Neuroanatomically,Biological-psychiatrically InformedClassification Scheme in Psychiatry
It is over 20 years since the first edition of Biologi-cal Psychiatry was published in 1987. The secondedition followed in 1996. In the decade that haspassed since there have been substantial devel-opments in the field, which the authors of thisedition believe justified the present endeavourto update knowledge. It is however worth tak-ing a glimpse back in time to see just what hashappened since the first edition, and to makesome comments on the prides and pitfalls thathave come to pass.
One of the most important advances has beenthe development of brain-imaging technologies.These were still in relative infancy at the timeof writing the first edition, but as outlined inChapter 4, the power of PET and MRI in variousformats has transformed research and theoret-ical approaches to biological psychiatry. Thefirst two editions contained much informationon monoaminergic and other transmitter func-tion, revealed by chemical challenge tests andblood measurements of hormones, CSF studiesand a deal of neuropathology, with an empha-sis on the findings from neurochemistry. Manyof these data have been omitted from this cur-rent text, summaries of the results being given,
Biological Psychiatry 3e Michael R. Trimble and Mark S. George 2010 John Wiley & Sons, Ltd
and the fuller complement of references can befound in earlier editions. This is not to criticizethese research endeavours. Psychiatrists withan interest in biological psychiatry used thebest techniques available to test their hypothe-ses, and the quite diverse methods neverthelessallow certain outcomes to form a continuingbasis on which to build further hypotheses. Inaddition, they led to a refinement of therapies,especially in neuropsychopharmacology.
The field of genetics had progressed by thesecond edition, but was yielding few resultsnot predicted from the earlier edition. Thisthird edition finds much more space devotedto genetics and brain imaging, and the sectionon neuroanatomy has re-emphasized theimportance of understanding advances in thosefields to the overall enterprise of uniting brainand behaviour, in sickness and in health. Thepreface to the first edition noted ‘one challengefor biological psychiatry is to unite informationwe now have regarding functional changes inthe brain in psychopathology with that whichwe now know about brain–behaviour rela-tionships and brain structure’ (p. xi). It seemsthat the challenge can now be met, and the

332 Biological Psychiatry
following conclusions are put forward, not onlyto stimulate discussion and debate, but in asincere attempt to raise important issues, someof which open up vistas of opportunity forfuture progress.
The first edition was bound into DSM III; bythe second it was DSM IV; now we have DSMIV-TR. It may come as some surprise, but ofthe 176 diagnostic criteria sets that appear inboth DSM IV and ICD 10, only one, namelytransient tic disorder, has identical DSM IV andICD 10 definitions. Throughout the text we havemade some comments about the failure of suchcommittee-driven manuals as the DSM or theICD system to provide an adequate method withwhich to understand psychopathology, and webelieve that it is now the time, with the immi-nent threat of DSM V and ICD 11, to moveclassification away from the sociological to thebiological; from the phenotype to the endophe-notype; from the epigenetic to the genetic; andunderlying all of these, from the phenomeno-logical to the anatomical. Hints at the possiblestructure of such a classification scheme haveemerged throughout this book, and to a largeextent have been made possible by the powerof the new developments in neuroscience thathave unveiled intimate knowledge of cerebralanatomy. As discussed in Chapter 2, a fullerunderstanding of the neuroanatomy of the lim-bic forebrain has exposed some of the difficultiesof the older conceptions of the limbic system.This allows us, along with data culled fromthe new brain-imaging techniques discussed inChapter 4, to progress towards a classificationof psychopathology founded in neuroanatomy.
Attempts in this direction are not new.Yakovlev introduced his evolutionary view ofthe brain, citing three layers or levels of anatom-ical distinction, an inner core surrounding thecentral CSF space, an intermediate level and anouter layer. The latter essentially was neocortex,but of interest was his bringing together of thebasal ganglia and the limbic structures of thebrain within his middle layer. Based on theseevolutionary anatomical principles, Cummingshas developed clinical counterparts, namelyautonomic disorders as a consequence of inner-layer abnormalities, while signature cortical
syndromes such as aphasias and apraxiasemerge from damage to the outer layer. How-ever, alteration of structure and function of themiddle layer results in paradigmatic neuro-psychiatric disorders from Parkinson’s diseaseto schizophrenia, which involve the cortical–subcortical circuits outlined in Chapter 2 andclinically lead to a confluence of motor and psy-chological symptoms, disorders of motivationbeing central.
We believe that a similar but more preciseanatomical framework can be given this clas-sification. We start out by asking not what ishappening in the brain, but where in the brain isit happening? An outline of the scheme is givenin Table 13.1.
We begin with anatomy. The outline is notto suggest that the related phenotype involvesonly the anatomical structure in column one,but that this is the fons et origo of the disor-der and most likely, even with progression ofthe disorder, to be the site of maximum neu-roanatomical and neurophysiological change.It is becoming clear that the unfolding of thecerebral, neuronal and glial structures has agenetic basis, and in the future the second col-umn may be replete with relevant genotypeswhich underpin the anatomical variants, but atpresent the cells are largely blank. The majorpsychopathological categories lend themselvesto an influence from one or more of the mainneurotransmitters, which drive behaviour andset our emotional tone. The identified ones atpresent are dopamine, GABA, glutamate, 5-HT,noradrenaline and acetylcholine. As other neu-romodulators become identified, the list willprobably fractionate, for example with differentGABA, cholinergic or 5-HT subtypes, and evennew potent chemopathologies, perhaps linkedto intracellular dynamics. Again, we do not wishto naively suggest that the neurotransmitter isthe cause of the phenotype, only that knowl-edge to date had pointed in certain directions;but ask not whether transmitter X is abnormalin the brain, we are urging to ask where!
We do not wish to imply that we supportan old-fashioned modular view of brain func-tion, a return to phrenology, with regards tocognition or disorders. Indeed throughout the

Epilogue 333
Table 13.1 A Proposed First Pass at a neuroanatomically, biological-psychiatrically informed classificationscheme in psychiatry. Note that for all of the major psychiatric disorders, one can begin by understanding therelevant neuroanatomy, and how the disorder is an imbalance of the function or behaviour resulting fromthat region, falling along a spectrum often from hyperfunction to hypofunction of the behaviour. For example,both the addictions and apathy syndromes flow from a dysfunction of a medial frontal–cingulate–basalganglia–nucleus accumbens circuit involved in appetitive drives. These behaviours prominently involvedopamine, without clear-cut genetic factors, can sometimes involve structural damage of the circuit, and mayor may not be progressive or lateralized. We posit that a nosology that is neuroanatomically based, buildingout from known brain functions, would refocus our field back on brain systems and would aid in futureunderstanding of the diseases within the field of biological psychiatry
Anatomy Genetics Neurotransmitters Structure Progressiveness Laterality Behaviour
Non-isocortical
Amyg 5-HT 5-HT/GABA/BDZ N N ? GAD/panicHC APO E ACH Y Y N Alzheimer’s
N N Y N Bilat. Amnesticdisorder
HC/ParaHC Y DA Y Y L PsychosisOF/BG Y DA/5-HT N N N Compulsive and
obsessiveMedF/Cing/BG N DA Y Y or N ? Hyper/
hypomotivation+/− tics
MedF (B 25) Y 5-HT N N ? DepressionBG Y GABA Y Y Bilat. Huntington’sBG Y DA Y Y Bilat. Parkinson’sIsocortical
FT Y ? Y Y R/L FT dementiasParietal N N Y Y/N R/L Signature
syndromes(aphasia, etc.)
Y, yes; N, no; R, right; L, left; DA, dopamine; BG, basal ganglia; FT, front-temporal; OF, orbitofrontal; ?, uncertain; MedF, mediofrontal;Cing, cingulum; B, Brodmann; Amyg, amygdala; HC, hippocampus; ParaHC, parahippocampal gyrus
book we have espoused a view of circuitry anddistributed function. However, we opine that atthe outset of any disorder identification of anycircuitry involved will likely be unclear, but thiswill become apparent as the disorder matures,as genetic unfolding of cortical anatomy contin-ues (into late life?), and under environmentalimpressions.
Whether or not there are structural changesand whether or not they are progressive is vitalto understanding prognosis. For years it wassuggested that schizophrenia and epilepsy werenot progressive disorders, and in some cases thisis so. However, these two variables we believeshould be part of a multiaxial classification,ending arguments over progression, but per-haps requiring new phenotypic designations.
Finally, in our list of variables we have includedlaterality. In spite of over 150 years of neuro-science progress since Broca first suggested lat-erality as being important for the developmentof psychological syndromes, and Flor-Henry’srejuvenation of the theme in the 1960s, no psy-chopathological classification scheme includesthis, although some isocortical signature syn-dromes are clearly lateralized. Much imagingresearch fails to discuss laterality, even whenfindings are clearly lateralized, and we knowthat the two hemispheres of the human brainsubserve widely divergent functions.
As a clear example, we take OCD. Forquite unclear reasons this has been categorizedunder anxiety disorders, and yet as we showin Chapter 6, this is untenable. In comparison

334 Biological Psychiatry
with generalized anxiety disorder and panicdisorder, the sex ratio is different, the envi-ronmental triggers to symptoms are different,the genetics are different, the neurocognitiveprofile is different, the somatic/neurologicalassociations are different, and the anatomy isdifferent. In contrast to the underling amyg-dala and hippocampal associations with theother anxiety disorders, OCD primarily reflectsfrontal–basal ganglia dysfunction. It is a behav-ioural reflection of a different circuitry. Thereare obvious subdivisions of this designation, forexample with associated tics (now referred to asGilles de la Tourette’s syndrome), or with bodyimage distortions (dysmorphic syndromes).
With regards to current concepts of schizo-phrenia, it has been clear for decades that asimple phenomenologically-based classificationis inadequate for both neuroscientific andclinical understanding. There is considerableevidence that the earliest anatomical changesin many people so classified by DSM IV arein the left medial temporal areas, affectingprincipally hippocampus and surroundingcortical structures. In a majority there is slowprogression and then a defect state remains.Secondary changes involve distributed anatom-ical and functional brain changes, which maybe genetically linked, and are contributed to bythe neurotransmitter dopamine. The geneticsof cerebral development combined with thefocus of the initial pathology would explainthe unfolding of the clinical syndrome throughendophenotype deviance and tertiary cognitiveembodiment. This hippocampal–temporal dis-order is different from another, which at presentis referred to as Alzheimer’s dementia, where
the pathology is different, the genetics aredifferent, the spread of the anatomy with timeis different, the neurocognitive changes are dif-ferent, and the main neurotransmitter involvedis acetylcholine. This pattern of unfolding of theclinical picture is again contrasted with thoseprogressive or halting disorders that primarilyinvolve frontal areas, or parietal cortex. Thereare syndromes which begin in basal gangliaand then spread to involve cortex, and so theclassification can be developed.
We believe that such an approach to classifi-cation helps with the issue of spectrums. Thusit is now fashionable to discuss the schizophre-nia spectrum or the bipolar spectrum, whichembrace both DSM IV axis 1 and axis 2 cate-gories. The spectrum however reflects on thebiological variability, which our anatomically-based view provides, temperament to psychosislinking anatomy with progression, as a disorderunfolds in time and neurological space.
We offer this neuroanatomical approachto an understanding of psychopathology as athoughtful challenge to the next committeeswho will revise existing manuals. We believethat the days of purely symptom-derivedclassifications in psychiatry are numbered,and go further to imply that, up to now, theyhave inhibited so much intelligent thought andresearch funding, and ossified our urge for anunderstanding of the brain in psychopathologyin favour of the simple flexibility of check-listdiagnoses. Like an emperor with no clothes,they have no substance (biological validity),but parading nakedly around the fringes ofacademic circles, seemingly unashamed, theyhave garnered the multitudes to worship them.

References
Abdulla, Y.H. and Hamadah, K. (1970) 3,5 cyclic adenosine monophosphate in depression andmania, Lancet, i, 378–81.
Abi-Dargham, A. and Guillin, O. (2007) Preface, International Review of Neurobiology, 78, xiii–xvi.Abrahams, R. and Schwartz, C.M. (1985) ECT and prolactin release: relation to treatment response
in melancholia, Convulsive Therapy, 1, 38–42.Abrams, R. and Taylor, M.A. (1979) Differential EEG patterns in affective disorder and schizophre-
nia, Archives of General Psychiatry, 36, 1355–8.Adamec, R.E. (1989) Kindling, anxiety and personality. In T.E. Bolwig and M.R. Trimble (eds.), The
Clinical Relevance of Kindling, Wiley, Chichester, pp. 117–35.Adamec, R.E. and Stark-Adamec, C. (1983) Limbic kindling and animal behaviour, Biological
Psychiatry, 18, 269–93.Adams, F. (1939) The Genuine Works of Hippocrates, Williams and Wilkins, Baltimore.Adams, R.D., Fisher, C.M., Hakim, S. et al. (1965) Symptomatic occult hydrocephalus with normal
CSF pressure. A treatable syndrome, New England Journal of Medicine, 243, 117–26.Addington, J., Cadenhead, K.S., Cannon, T.D. et al. (2007) North American prodrome longitudinal
study: a collaborative multisite approach to prodromal schizophrenia research, SchizophreniaBulletin, 33, 665–72.
Adolfsson, R., Gottfries, C.-G., Oreland, L. et al. (1978) Monoamine oxidase activity and serotonergicturnover in human brain, Progress in Neuropsychopharmacology, 2, 225–30.
Adolfsson, R., Gottfries, C.-G., Roos, B.E. et al. (1979) Changes in brain catecholamines in patientswith dementia of the Alzheimer type, British Journal of Psychiatry, 135, 216–23.
Akiskal, H.S. (2007) The emergence of the bipolar spectrum: validation along clinical-epidemiologicand familial-genetic lines, Psychopharmacology Bulletin, 40, 99–115.
Akiskal, H.S. and Benazzi, F. (2006) The DSM-IV and ICD-10 categories of recurrent (major)depressive and bipolar II disorders: evidence that they lie on a dimensional spectrum, Journal ofAffective Disorders, 92, 45–54.
Albert, M.L., Feldman, R.G. and Willis, A.L. (1974) The ‘subcortical dementia’ of progressivenuclear palsy, Journal of Neurology, Neurosurgery and Psychiatry, 37, 121–30.
Albright, P.S. and Burnham, W.I. (1980) Development of a new pharmacological seizure model:effects of anticonvulsants on cortical and amygdala-kindled seizures in the rat, Epilepsia, 21,681–9.
Aldencamp, A.P. (2004) Antiepileptic drug treatment and epileptic seizures: effects on cognitivefunction. In M.R. Trimble and B. Schmitz (eds.), The Neuropsychiatry of Epilepsy, CambridgeUniversity Press, Cambridge, pp. 256–265.
Biological Psychiatry 3e Michael R. Trimble and Mark S. George 2010 John Wiley & Sons, Ltd

336 References
Aleman, A., Swart, M. and Van Rijn, S. (2008) Brain imaging, genetics and emotion, BiologicalPsychology, 79, 58–69.
Alexander, G.E., DeLong, M.R. and Strick, P.L. (1986) Parallel organisation of functionally segre-gated circuits linking basal ganglia and cortex, Annual Review of Neuroscience, 9, 357–81.
Alexopoulos, G.S., Inturrisi, C.E., Lipman, R. et al. (1983) Plasma immunoreactive beta-endorphinlevels in depression, Archives of General Psychiatry, 40, 181–3.
Alheid, G.F. and Heimer, L. (1988) New perspectives in basal forebrain organisation of specialrelevance for neuropsychiatric disorders, Neuroscience, 27, 1–39.
Allen, J.J., McKnight, K.M., Moreno, F.A. et al. (2009) Alteration of frontal EEG asymmetry duringtryptophan depletion predicts future depression, Journal of Affective Disorders, 115, 189–95.
Alonso, P., Pujol, J., Cardoner, N. et al. (2001) Right prefrontal TMS in OCD: a double-blind,placebo-controlled study, American Journal of Psychiatry, 158, 1143–5.
Altemus, M., Piggott, T., Kalogeras, K.T. et al. (1992) Abnormalities in the regulation of vasopressinand corticotrophic releasing factor secretion in obsessive–compulsive disorder, Archives ofGeneral Psychiatry, 49, 9–20.
Altschuler, L.L., Devinsky, O., Post, R.M. et al. (1990) Depression, anxiety and temporal lobeepilepsy, Archives of Neurology, 47, 284–8.
Altschuler, L.L., Conrad, A., Hauser, P. et al. (1991) Reduction of temporal lobe volume in bipolardisorder, Archives of General Psychiatry, 48, 482–3.
Altschuler, L.L., Bartzokis, G., Grieder, T. et al. (2000) An MRI study of temporal lobe structures inmen with bipolar disorder or schizophrenia, Biological Psychiatry, 48, 147–62.
Amaral, D.G., Price, J.L., Pitkanen, A. et al. (1992) Anatomical organisation of primate amygdaloidcomplex. In Aggleton (ed.), The Amygdala, Wiley Liss, New York, NY, pp. 1–66.
Amat, J., Paul, E., Watkins, L.R. et al. (2008) Activation of the ventral medial prefrontal cortexduring an uncontrollable stressor reproduces both the immediate and long-term protectiveeffects of behavioral control, Neuroscience, 154, 1178–86.
Amen, D.G. and Carmichael, B.D. (1997) High-resolution brain spect imaging in ADHD, Annals ofClinical Psychiatry, 9, 81–6.
American Psychiatric Association (1987) Diagnostic and Statistical Manual of Mental Disorders, 3rdedition revised, APA, Washington, DC.
American Psychiatric Association (1994) DSM-IV-TR: Diagnostic and Statistical Manual of MentalDisorders, APA, Washington, DC.
American Psychiatric Association (2000) DSM-IV-TR: Diagnostic and Statistical Manual of MentalDisorders, APA, Washington, DC.
Ammons, W.S. and Blair, R.W.F.R.D. (1983) Vagal afferent inhibition of primate thoracic spinotha-lamic neurons, Journal of Neurophysiology, 50, 926–40.
Anand, A., Li, Y., Wang, Y. et al. (2005a) Activity and connectivity of brain mood regulating circuitin depression: a functional magnetic resonance study, Biological Psychiatry, 57, 1079–88.
Anand, A., Li, Y., Wang, Y. et al. (2005b) Antidepressant effect on connectivity of the mood-regulating circuit: an fMRI study, Neuropsychopharmacology, 30, 1334–44.
Anckarsater, H. (2006) Central nervous changes in social dysfunction: autism, aggression, andpsychopathy, Brain Research Bulletin, 69, 259–65.
Anden, N.E. (1975) Animal models of brain dopamine function. In W. Birkmayer andO. Hornykiewicz (eds.), Advances in Parkinsonism, Roche, Basle, pp. 169–77.
Andermann, E. (1980) Genetic aspects of epilepsy. In P. Robb (ed.), Epilepsy Updated: Causes andTreatment, Medical Year Book, Chicago, pp. 11–24.
Andreasen, N.C., Arndt, S., Swayze, V. et al. (1994) Thalamic abnormalities in schizophreniavisualized through magnetic resonance image averaging, Science, 266(5183), 294–8.

References 337
Andreasson, S., Allebeck, P., Engstrom, A. et al. (1987) Cannabis and Schizophrenia: a longitudinalstudy of Swedish conscripts, Lancet, ii, 1483–6.
Andre-Obadia, N., Peyron, R., Mertens, P. et al. (2006) Transcranial magnetic stimulation for paincontrol: double-blind study of different frequencies against placebo, and correlation with motorcortex stimulation efficacy, Clinical Neurophysiology, 117, 1536–44.
Angst, J., Felder, W. and Lohmeyer, B. (1979) Schizoaffective disorders: results of a geneticinvestigation, Journal of Affective Disorders, 1, 139–53.
Annegers, J.F., Hauser, W.A., Coan, S.P. et al. (1998) A population based study of seizures aftertraumatic head injuries, New England Journal of Medicine, 338, 20–24.
Anthony, M.M., Brown, T.A. and Barlow, D.H. (1997) Response to hyperventilation and 5.5%carbon-dioxide inhalation of subjects with types of specific phobia, panic disorder or no mentalillness, American Journal of Psychiatry, 154, 1089–95.
Appell, J., Kertesz, A. and Fishman, M. (1982) A study of language functioning in Alzheimer’spatients, Brain and Language, 17, 73–91.
Applebaum, J., Bersudsky, Y. and Klein, E. (2007) Rapid tryptophan depletion as a treatment foracute mania: a double-blind, pilot-controlled study, Bipolar Disorders, 9, 884–7.
Arana, G.W. and Baldessarini, R.J. (1985) The dexamethasone suppression test for diagnosis andprognosis in psychiatry, Archives of General Psychiatry, 42, 1193–204.
Arana, G.W., Pearlman, C. and Shader, R.I. (1985) Alprazolam induced mania, American Journal ofPsychiatry, 142, 368–3.
Arora, R.C. and Meltzer, H.W. (1989) Serotonergic measures in the brains of suicide victims,American Journal of Psychiatry, 146, 730–6.
Asberg, M., Traskman, L. and Thoren, P. (1976) 5-HIAA in the CSF: a biochemical suicide predictor,Archives of General Psychiatry, 33, 1193–7.
Ashton, H. (1984) Benzodiazepine withdrawal: an unfinished story, British Medical Journal, 288,1135–40.
Ayd, F.J. (1974) Side effects of depot fluphenazines, Comprehensive Psychiatry, 15, 277–84.Aylward, E.H., Roberts-Twiddie, J.V., Barta, P. et al. (1994) Basal ganglia volumes and acute white
matter hyperintensities in patients with bipolar disorders, American Journal of Psychiatry, 151,687–94.
Bach, Y., Rita, G., Lion, J.R. et al. (1971) Episodic dyscontrol: a study of 130 violent patients, AmericanJournal of Psychiatry, 127, 1473–8.
Bailey, P. and Bremer, F. (1938) A sensory cortical representation of the vagus nerve, Journal ofNeurophysiology, 1, 405–12.
Baker, L.A., Jacobson, K.C., Raine, A. et al. (2007) Genetic and environmental bases of childhoodantisocial behavior: a multi-informant twin study, Journal of Abnormal Psychology, 116, 219–35.
Baker, L.A., Raine, A., Liu, J. et al. (2008) Differential genetic and environmental influences onreactive and proactive aggression in children, Journal of Abnormal Child Psychology, 36, 1265–78.
Ballenger, J.C., Goodwin, F.K., Major, L.F. et al. (1979) Alcohol and central serotonin metabolism inman, Archives of General Psychiatry, 36, 224–7.
Banasr, M., Chowdhury, G.M., Terwilliger, R. et al. (2008) Glial pathology in an animal modelof depression: reversal of stress-induced cellular, metabolic and behavioral deficits by theglutamate-modulating drug riluzole, Molecular Psychiatry (epub ahead of print, PMID: 18825147).
Bandler, R. and Keay, K.A. (1996) Columnar organization in the midbrain periaqueductal gray andthe integration of emotional expression, Department of Anatomy and Histology, Institute forBiomedical Research, The University of Sydney, NSW, Australia, Progress in Brain Research, 107,285–300.
Banki, C.M., Vojnick, M. and Molnar, G. (1981) CSF biochemical examinations, Biological Psychiatry,18, 1033–44.

338 References
Bannon M.J., Reinhard, J.F., Bunney, E.B. et al. (1982) Unique response to antipsychotic drugs is dueto absence of terminal autoreceptors in mesocortical dopamine neurones, Nature, 296, 444–6.
Barch, D.M., Berman, M.G., Engle, R. et al. (2009a) CNTRICS final task selection: working memory,Schizophrenia Bulletin, 35, 136–52.
Barch, D.M., Braver, T.S., Carter, C.S. et al. (2009b) CNTRICS final task selection: executive control,Schizophrenia Bulletin, 35, 115–35.
Bares, M., Brunovsky, M., Kopecek, M. et al. (2007) Changes in qEEG prefrontal cordance as apredictor of response to antidepressants in patients with treatment resistant depressive disorder:a pilot study, Journal of Psychiatric Research, 41, 319–25.
Barker, A.T., Freeston, I.L., Jalinous, R. et al. (1987) Magnetic stimulation of the human brain andperipheral nervous system: an introduction and the results of an initial clinical evaluation,Neurosurgery, 20, 100–9.
Barker, A.T., Jalinous, R. and Freeston, I.L. (1985) Non-invasive magnetic stimulation of the humanmotor cortex, Lancet, i, 1106–7.
Barnes, C.A., Jung, M.W., McNaughton, B.L. et al. (1994) LTP saturation and spatial learningdisruption: effects of task variables and saturation levels, Journal of Neuroscience, 14, 5793–806.
Baron, M., Levitt, M. and Perlman, R. (1980) Low platelet MAO activity: a possible biochemicalcorrelate of borderline schizophrenia, Psychiatry Research, 3, 329–35.
Baron, M., Levitt, M., Greuen, R. et al. (1984) Platelet MAO activity and genetic vulnerability toschizophrenia, American Journal of Psychiatry, 141, 836–42.
Bartsch, A.P. and van Hemmen, J.L. (2001) Combined Hebbian development of geniculocorticaland lateral connectivity in a model of primary visual cortex, Biological Cybernetics, 84, 41–55.
Bastini, B., Nash, F. and Meltzer, H.Y. (1990) Prolactin and cortisol responses to MK-212, a serotoninagonist, in obsessive–compulsive disorder, Archives of General Psychiatry, 47, 833–9.
Battaglia, M., Przybeck, T.R., Bellodi, L. et al. (1996) Temperament dimensions explain the comor-bidity of psychiatric disorders, Comprehensive Psychiatry, 37, 292–8.
Baumgartner, A., Graf, K.J. and Kurten, I. (1985) The dexamethasone suppression test in depression,in schizophrenia and during experimental stress, Biological Psychiatry, 20, 675–9.
Baxter, L.R., Phelps, M.E., Mazziotta, J.C. et al. (1985) Cerebral metabolic rates for glucose in mooddisorders, Archives of General Psychiatry, 42, 441–7.
Baxter, L.R., Schwartz, J.M., Mazziotta, J.C. et al. (1988) Cerebral glucose metabolic rates in non-depressed patients with obsessive–compulsive disorder, American Journal of Psychiatry, 145,1560–3.
Baxter, L.R., Jeffrey, M.S., Phelps, M.E. et al. (1989) Reduction of prefrontal cortex glucosemetabolism common to three types of depression, Archives of General Psychiatry, 46, 243–50.
Baxter, L.R., Schwartz, J.M., Bergman, K.S. et al. (1992) Caudate glucose metabolic rate changeswith both drug and behaviour therapy for obsessive–compulsive disorder, Archives of GeneralPsychiatry, 49, 681–96.
Beal, M.F., Mazurek, M.F., Ellison, D.W. et al. (1988) Somatostatin and its neuropeptide Y concen-trations in pathologically graded cases of Huntington’s disease, Annals of Neurology, 23, 562–9.
Bear, D. (1986) Hemispheric asymmetries in emotional function: a reflection of lateral specialisationin cortical–limbic connections. In B.K. Doane and K.E. Livingstone (eds.), The Limbic System:Functional Organization and Clinical Disorders, Raven Press, New York, NY, pp. 29–42.
Bear, D. and Fedio, P. (1977) Quantitative analysis of interictal behaviour in temporal lobe epilepsy,Archives of Neurology, 34, 454–67.
Beer, B. (1902) Uber das Auftretten einer objectiven Lichtempfindung in magnetischen Felde,Klinische Wochenzeitschrift, 15, 108–9.
Beghi, E., Carpio, A., Forsgren, L. et al. (2009) Recommendation for a definition of acute symptomaticseizure, Epilepsia (epub ahead of print), Mario Negri Institute, Milan, Italy.

References 339
Beghi E. and Sander, J.W. (2007) The natural history and prognosis of epilepsy. In J. Engel andT. Pedley (eds.), Epilepsy: A Comprehensive Textbook, 2nd edition, Lippincott Williams & Wilkins,New York, NY, pp. 65–70.
Bejjani, B.P., Damier, P., Arnulf, I. et al. (1999) Transient acute depression induced by high-frequencydeep-brain stimulation [see comments], New England Journal Of Medicine, 340, 1476–80.
Belanoff, J.K., Gross, K., Yager, A. et al. (2001) Corticosteroids and cognition, J Psychiatr Res, 35,127–45.
Ben-Ari, Y. (1981) Transmitters and modulators in the amygdaloid complex: a review. In Y. Ben-Ari(ed.), The Amygdaloid Complex, Elsevier, North Holland, pp. 163–74.
Benazzi, F. and Akiskal, H.S. (2008) How best to identify a bipolar-related subtype among majordepressive patients without spontaneous hypomania: superiority of age at onset criterion overrecurrence and polarity?, Journal of Affective Disorders, 107, 77–88.
Benca, R.M., Obermeyer, W.H., Thisted, R.A. et al. (1992) Sleep and psychiatric disorders: ameta-analysis, Archives of General Psychiatry, 49, 651–68.
Bench, C.J., Friston, K.J., Brown, R.G. et al. (1993) Regional cerebral blood flow in depression mea-sured by positron emission tomography: the relationship with clinical dimensions, PsychologicalMedicine, 23, 579–90.
Benedetti, F., Dallaspezia, S., Colombo, C. et al. (2008) A length polymorphism in the circadianclock gene Per3 influences age at onset of bipolar disorder, Neuroscience Letters, 445, 184–7.
Benes, F.M. (2007) Searching for unique endophenotypes for schizophrenia and bipolar disorderwithin neural circuits and their molecular regulatory mechanisms, Schizophrenia Bulletin, 33,932–6.
Benjamin, J., Osher, Y., Kotler, M. et al. (2000) Association of tridimensional personality question-naire (TPQ), and three functional polymorphisms: dopamine receptor D4 (DRD4), serotonintransporter promotor region (5-HTTLRP) and catechol O-methyltransferase (COMT), MolecularPsychiatry, 5, 96–100.
Benkelfat, C., Nordahl, T.E., Semple, W. et al. (1990) Local cerebral glucose metabolic rates in OCD,Archives of General Psychiatry, 47, 840–8.
Ben-Menachem, E., Manon-Espaillat, R., Ristanovic, R. et al. (1994) Vagus nerve stimulation fortreatment of partial seizures: 1. a controlled study of effect on seizures, Epilepsia, 35, 616–26.
Ben-Sachar, D., Belmaker, R.H., Grisaru, N. et al. (1997) Transcranial magnetic stimulation inducesalterations in brain monoamines, Journal of Neural Transmission, 104, 191–7.
Benson, D.F. (1975) The hydrocephalic dementias. In D.F. Benson and D. Blumer (eds.), PsychiatricAspects of Neurolgoic Disease, Grune and Stratton, New York, NY, pp. 83–97.
Benson, D.F. (1979) Aphasia, Alexia and Agraphia, Churchill Livingstone, Edinburgh.Benton, J.S., Bowen, D.M., Alien, S.J. et al. (1982) Alzheimer’s disease as a disorder of isodendritic
core, Lancet, i, 456.Berman, K.F., Doran, A.R., Picker, D. et al. (1993) Is the mechanism of prefrontal hypofunction in
depression the same as schizophrenia?, British Journal of Psychiatry, 162, 183–92.Berney, A., Sookman, D., Leyton, M. et al. (2006) Lack of effects on core obsessive–compulsive symp-
toms of tryptophan depletion during symptom provocation in remitted obsessive–compulsivedisorder patients, Biological Psychiatry, 59, 853–7.
Bernouilli, C., Siegfried, J., Baumgartner, G. et al. (1977) Danger of accidental person-to-persontransmission of Creutzfeld–Jakob disease by surgery, Lancet, i, 478–9.
Berrettini, W.H., Numberger, J.I., Hare, T.A. et al. (1983) Reduced plasma and CSF GABA inaffective illness: effect of lithium carbonate, Biological Psychiatry, 18, 185–94.
Bertelsen, A., Harvald, B. and Hauge, M. (1977) A Danish twin study of manic depressive disorders,British Journal of Psychiatry, 130, 330–51.

340 References
Betts, T.A. (1974) A follow-up study of a cohort of patients with epilepsy admitted to psychiatriccare in an English city. In P. Harris and C. Mawdsley (eds.), Epilepsy: Proceedings of the HansBerger Centenary Symposium, Churchill Livingstone, Edinburgh, pp. 326–38.
Bhatia, K.P., Bhatt, M.H. and Marsden, C.D. (1993) The causalgia-dystonia syndrome, Brain, 116,843–51.
Birkmeyer, W., Jellinger, K. and Riederer, P. (1977) Striatal and extrastriatal dopaminergic functions.In A.R. Cools et al. (eds.), Psychobiology of the Striatum, Elsevier, North Holland, pp. 141–52.
Biver, F., Goldman, S., Delvenne, V. et al. (1994) Frontal and parietal metabolic disturbances inunipolar depression, Biological Psychiatry, 36, 381–8.
Bleuler, E. (1911) Dementia Praecox or the Group of Schizophrenics (Translated by J. Zenkin, 1950),New York International University Press.
Bleuler, E. (1924) Textbook of Psychiatry (Translated by A.A. Brill, 1924), Dover Publications.Bleuler, E. (1949) Lehrbuch der Psychiatrie, 8th edition, Springer-Verlag, Berlin.Blumer, D. (2000) Dysphoric disorders and paroxysmal affects: recognition and treatment of
epilepsy-related psychiatric disorders, Harvard Review Psychiatry, 8, 8–17.Blumer, D. (2004) Suicide. In M.R. Trimble and B. Schmitz (eds.), The Neuropsychiatry of Epilepsy,
Cambridge University Press, Cambridge, pp. 107–116.Bodner, M., Shafi, M., Zhou, Y.D. et al. (2005) Patterned firing of parietal cells in a haptic working
memory task, European Journal of Neuroscience, 21, 2538–46.Bohning, D.E. (2000) Introduction and overview of TMS physics. In M.S. George and R.H.
Belmaker (eds.), Transcranial Magnetic Stimulation in Neuropsychiatry, American PsychiatricPress, Washington, DC.
Bohning, D.E., Lomarev, M.P., Denslow, S. et al. (2001) Feasibility of vagus nerve stimulation-synchronized blood oxygenation level-dependent functional MRI, Investigative Radiology, 36,470–9.
Bondareff, W., Mountjoy, C.Q. and Roth, M. (1981) Selective loss of neurones of origin of adrenergicprojection to cerebral cortex in senile dementia, Lancet, i, 783–4.
Borckardt, J.J., Weinstein, M., Reeves, S.T. et al. (2006) Post-operative left prefrontal repetitive tran-scranial magnetic stimulation (RTMS) reduces patient-controlled analgesia use, Anesthesiology,105, 557–562.
Borgwardt, S.J., Dickey, C., Pol, H.H. et al. (2009) Workshop on defining the significance ofprogressive brain change in schizophrenia: December 12, 2008 American College of Neuropsy-chopharmacology (ACNP) All-Day Satellite, Scottsdale, Arizona, The Rapporteurs’ Report,Schizophrenia Research.
Bottiglieri, T., Godfrey, P., Flynn, T. et al. (1990) CSF S-adenosylmethionine in depression, Journalof Neurology, Neurosurgery and Psychiatry, 53, 1096–8.
Bowen, D.M. and Davison, A. (1986) Biochemical studies of nerve cells and energy metabolism inAlzheimer’s disease, British Medical Bulletin, 42, 75–80.
Bowen, D.M., Spillane, J.A., Curzon, G. et al. (1979) Accelerated ageing or selective neuronal lossas an important cause of dementia, Lancet, i, 11–13.
Boylan, L.S., Flint, L.A., Labovitz, D.L. et al. (2004) Depression but not seizure frequency predictsquality of life in treatment-resistant epilepsy, Neurology, 62, 258–61.
Braak, H. and Braak, E. (1997) Frequency of stages of alzheimer-related lesions in different agecategories, Neurobiol Aging, 18, 351–7.
Braak, E., Braak, H. and Mandelkow, E.M. (1994a) A sequence of cytoskeleton changes related tothe formation of neurofibrillary tangles and neuropil threads, Acta Neuropathol, 87, 554–67.
Braak, H., Braak, E., Yilmazer, D. et al. (1994b) Amygdala pathology in Parkinson’s disease, ActaNeuropathol, 88, 493–500.

References 341
Braddock, L. (1986) The dexamethasone suppression test: fact and artefact, British Journal ofPsychiatry, 148, 363–74.
Braestrup, C. and Nielsen, M. (1982) Anxiety, Lancet, ii, 1030–4.Brambilla, F., Smeraldi, F., Sacchetti, E. et al. (1978) Deranged anterior pituitary responsiveness to
hypothalamic hormones in depressed patients, Archives of General Psychiatry, 35, 1231–8.Bredkjaer, S.R., Mortensen, P.B. and Parnas, J. (1998) Epilepsy and non-organic non-affective
psychosis: national epidemiologic study, British Journal of Psychiatry, 172, 235–8.Breggin, P.B. (1964) The psychophysiology of anxiety, Journal of Nervous and Mental Diseases, 139,
558–68.Breiter, H.C., Weisskoff, R.M., Kennedy, D.N. et al. (1997) Acute effects of cocaine on human brain
activity and emotion, Neuron, 19, 591–611.Bremner, J.D., Davis, M., Southwick, S. et al. (1993) Neurobiology of PTSD. In J.M. Oldham et al.
(eds.), Review of Psychiatry 12, APA Press, Washington, DC, pp. 183–214.Bremner, J.D., Randall, P., Scott, T.M. et al. (1995) MRI-based measurement of hippocampal volume
in patients with combat-related PTSD, American Journal of Psychiatry, 152, 973–81.Bremner, J.D., Innis, R.B., Salomon, R.M. et al. (1997) PET measurement of cerebral metabolic
correlates of depressive relapse, Archives of General Psychiatry, 54, 364–74.Bridges, P.K., Bartlett, J.R., Sepping, P. et al. (1976) Precursors and metabolites of 5-HT and
dopamine in the ventricular CSF of psychiatric patients, Psychological Medicine, 6, 399–405.Bridges, P.K., Bartlett, J.R., Hale, A.S. et al. (1994) Psychosurgery: stereotactic subcaudate tracto-
tomy, British Journal of Psychiatry, 165, 599–611.Briley, M.S., Langer, S.Z., Raisman, R. et al. (1980) Tritiated imipramine binding sites are decreased
in platelets of untreated depressed patients, Science, 209, 303–5.Broadhurst, P.L. (1975) The Maudsley reactive and non-reactive strain of rats, Behaviour and
Genetics, 5, 299–319.Bromfield, E., Altschuler, L. and Leiderman, D. (1990) Cerebral metabolism and depression in
patients with complex partial seizures, Epilepsia, 31, 625.Brown, S.W. (2004) Dementia and epilpesy. In M.R. Trimble and B. Schmitz (eds.), The Neuropsy-
chiatry of Epilepsy, Cambridge University Press, Cambridge, pp. 135–51.Brown, W.A. and Laughren, T.P. (1981) Tolerance to the prolactin-elevating effect of neuroleptics,
Psychiatry Research, 5, 317–22.Brown, G.L., Ballanger, J.C., Minichello, M.D. et al. (1979) Human aggression and its relationship
to CSF 5HIAA, 3MHPG and HVA. In M. Sandler (ed.), Psychopharmacology of Aggression, RavenPress, New York, NY, pp. 131–48.
Brown, G.L., Ebert, M.H., Goyer, P.F. et al. (1982) Aggression, suicide and serotonin: relationshipto CSF amine metabolism, American Journal of Psychiatry, 139, 741–6.
Brown, R.G., Marsden, C.D., Quinn, N. et al. (1984) Alterations in cognitive performance and affect-arousal state during fluctuations in motor function in Parkinson’s disease, Journal of Neurology,Neurosurgery and Psychiatry, 47, 454–65.
Brun, A., Englund, B., Gustafson, L. et al. (1994) Clinical and neuropathological criteria forfronto-temporal dementia, Journal of Neurology, Neurosurgery and Psychiatry, 57, 416–18.
Brunner, R., Henze, R., Parzer, P. et al. (2009) Reduced prefrontal and orbitofrontal gray matterin female adolescents with borderline personality disorder: is it disorder specific?, Neuroimage,49(1), 114–20.
Brusov, O.G., Fomenko, A.M. and Katasonov, A.B. (1985) Human plasma inhibitors of plateletserotonin uptake and imipramine receptor binding: extraction and heterogeneity, BiologicalPsychiatry, 20, 235–44.
Bruton, C.J., Stevens, J.R. and Frith, C. (1994) Epilepsy, psychosis and schizophrenia, Neurology, 44,34–42.

342 References
Buchheim, A., Erk, S., George, C. et al. (2008) Neural correlates of attachment trauma in borderlinepersonality disorder: a functional magnetic resonance imaging study, Psychiatry Research, 163,223–35.
Buchsbaum, M.S., Coursey, R.D. and Murphy, D.L. (1976) The biochemical high risk paradigm:behavioural and familial correlates of low platelet MAO activity, Science, 194, 339–41.
Buchsbaum, M.S., Wu, J., Delisi, L.E. et al. (1986) Frontal cortex and basal ganglia metabolic ratesassessed by PET with 18F-2-deoxyglucose in affective illness, Journal of Affective Disorders, 10,139–52.
Buchsbaum, M.S., Christian, B.T., Lehrer, D.S. et al. (2006) D2/D3 dopamine receptor binding with[F-18]fallypride in thalamus and cortex of patients with schizophrenia, Schizophrenia Research,85(1–3), 232–44.
Buckley, M.J., Booth, M.C., Rolls, E.T. et al. (2001) Selective perceptual impairments after perirhinalcortex ablation, Journal of Neuroscience, 21, 9824–36.
Burnet, P.W., Sharp, T., Lecorre, S.M. et al. (1999) Expression of 5-HT receptors and the 5-HTtransporter in rat brain after electroconvulsive shock, Neuroscience Letter, 277, 79–82.
Burnett, G.B., Prange, A.B., Wilson, I.C. et al. (1980) Adverse effects of anticholinergic antiparkin-sonian drugs in tardive dyskinesia, Neuropsychobiology, 6, 109–20.
Burrows, G.D., Vohra, J., Hunt, D. et al. (1976) Cardiac effects of different tricyclic antidepressantdrugs, British Journal of Psychiatry, 129, 335–41.
Burt, T., Lisanby, S.H. and Sackeim, H.A. (2002) Neuropsychiatric applications of transcranialmagnetic stimulation, International Journal of Neuropsychopharmacology, 5, 73–103.
Bush, G., Luu, P. and Posner, M.I. (2000) Cognitive and emotional influences in anterior cingulatecortex, Trends in Cognitive Sciences, 4, 215–222.
Bush, G., Whalen, P.J., Shin, L.M. et al. (2006) The counting Stroop: a cognitive interference task,Nature Protocols, 1(1), 230–3.
Butler, P.W.P. and Besser, G.M. (1968) Pituitary–adrenal function in severe depressive illness,Lancet, i, 1234–6.
Buzsaki, G. (2006) Rhythms of the Brain, Oxford University Press, London.Byne, W., Kidkardnee, S., Tatusov, A. et al. (2006) Schizophrenia-associated reduction of neuronal
and oligodendrocyte numbers in the anterior principal thalamic nucleus, Schizophrenia Research,85(1–3), 245–53.
Byne, W., Hazlett, E.A., Buchsbaum, M.S. et al. (2009) The thalamus and schizophrenia: currentstatus of research, Acta Neuropathologica, 117, 347–68.
Caceda, R., Kinkead, B. and Nemeroff, C.B. (2006) Neurotensin: role in psychiatric and neurologicaldiseases, Peptides, 27, 2385–404.
Caceda, R., Kinkead, B. and Nemeroff, C.B. (2007) Involvement of neuropeptide systems inschizophrenia: human studies, International Review of Neurobiology, 78, 327–76.
Caine, E. (1981) Pseudodementia: current concepts and future directions, Archives of GeneralPsychiatry, 38, 1359–64.
Callicott, J.H., Straub, R.E., Pezawas, L. et al. (2005) Variation in disc1 affects hippocampal structureand function and increases risk for schizophrenia, Proceedings of the National Academy of ScienceU S A, 102, 8627–32.
Calloway, S.P., Dolan, R.J., Fonagy, P. et al. (1984) Endocrine changes and clinical profiles indepression: the TRH test, Psychological Medicine, 14, 759–65.
Cameron, O.G., Smith, C.B., Hollingsworth, P.J. et al. (1984) Plasma alpha-2 adrenergic receptorbinding and plasma catecholamines, Archives of General Psychiatry, 41, 1144–8.
Cameron, N.M., Shahrokh, D., del Corpo, A. et al. (2008) Epigenetic programming of phenotypicvariations in reproductive strategies in the rat through maternal care, J Neuroendocrinol, 20,795–801.

References 343
Canitano, R. (2007) Epilepsy in autism spectrum disorders, European Child and Adolescent Psychiatry,16, 61–6.
Cannon, W.B. (1927) The James–Lange theory of emotion: a critical examination and an alternativetheory, American Journal of Psychology, 39, 106–24.
Cannon, D.M., Ichise, M., Fromm, S.J. et al. (2006) Serotonin transporter binding in bipolar disorderassessed using [11c]DASb and positron emission tomography, Biological Psychiatry, 60, 207–17.
Cannon, D.M., Ichise, M., Rollis, D. et al. (2007) Elevated serotonin transporter binding in majordepressive disorder assessed using positron emission tomography and [11c]DASb: comparisonwith bipolar disorder, Biological Psychiatry, 62, 870–7.
Capstick, N. and Seldrup, J. (1977) Obsessional states: a study in the relationship betweenabnormalities occurring at the time of birth and the subsequent development of obsessionalsymptoms, Acta Psychiatrica Scandinavica, 56, 427–31.
Cardinal, R.N., Daw, N., Robbins, T.W. et al. (2002a) Local analysis of behaviour in the adjusting-delay task for assessing choice of delayed reinforcement, Neural Networks, 15, 617–34.
Cardinal, R.N., Parkinson, J.A., Lachenal, G. et al. (2002b) Effects of selective excitotoxic lesions ofthe nucleus accumbens core, anterior cingulate cortex, and central nucleus of the amygdala onautoshaping performance in rats, Behavioral Neuroscience, 116, 553–67.
Cardinal, R.N., Parkinson, J.A., Hall, J. et al. (2002c) Emotion and motivation: the role of theamygdala, ventral striatum, and prefrontal cortex, Neuroscience & Biobehavioral Reviews, 321–52.
Cardinal, R.N., Parkinson, J.A., Marbini, H.D. et al. (2003) Role of the anterior cingulate cortex inthe control over behavior by Pavlovian conditioned stimuli in rats, Behavioral Neuroscience, 117,566–87.
Carey, G., Gottesman, I.I. and Robins, E. (1980) Prevalence rates for the neuroses: pitfalls in theevaluation of familiality, Psychological Medicine, 10(3), 437–43.
Carroll, B.J., Greden, J.F., Haskett, R.F. et al. (1980) Neurotransmitter studies of neuroendocrinepathology in depression, Acta Psychiatrica Scandinavica, 61, Suppl. 280, 183–200.
Carroll, B.J., Feinberg, M., Greden, J.F. et al. (1981) A specific laboratory test for the diagnosis ofmelancholia, Archives of General Psychiatry, 38, 15–22.
Carroll, S.B., Prud’homme, B. and Gopel, N. (2008) Regulating evolution, Scientific American, 35–45.Carter, C.S., Barch, D.M., Gur, R. et al. (2009) CNTRICS final task selection: social cognitive and
affective neuroscience-based measures, Schizophrenia Bulletin, 35, 153–62.Casey, D., Gerlach, J., Magelund, G. et al. (1980) Gamma acetylenic GABA in tardive dyskinesia,
Archives of General Psychiatry, 37, 1376–9.Caspari, D., Trabert, W., Heinz, G. et al. (1993) The pattern of regional cerebral blood flow during
alcohol withdrawal: a single photon emission tomography study with 99TC-HMPAO, ActaPsychiatrica Scandinavica, 87(6), 414–417.
Catterall, R.D. (1977) Neurosyphilis, British Journal of Hospital Medicine, 17, 585–604.Cavanna, A.E. and Trimble, M.R. (2006) The precuneus: a review of its functional anatomy and
behavioural correlates, Brain, 129, 564–83.Cecconi, J.P., Lopes, A.C., Duran, F.L. et al. (2008) Gamma ventral capsulotomy for treatment of
resistant obsessive–compulsive disorder: a structural MRI pilot prospective study, NeuroscienceLetter, 447, 138–42.
Cervenka, S., Backman, L., Cselenyi, Z. et al. (2008) Associations between dopamine D2-receptorbinding and cognitive performance indicate functional compartmentalization of the humanstriatum, Neuroimage, 40, 1287–95.
Chae, J.H., Nahas, Z., Lomarev, M. et al. (2003) A review of functional neuroimaging studies ofvagus nerve stimulation (VNS), Journal of Psychiatric Research, 37, 443–55.
Chalmers, R.J. and Bennie, E.H. (1978) The effect of fluphenazine on basal prolactin concentrations,Psychological Medicine, 8, 483–6.

344 References
Champagne, D.L., Bagot, R.C., van Hasselt, F. et al. (2008) Maternal care and hippocampalplasticity: evidence for experience-dependent structural plasticity, altered synaptic functioning,and differential responsiveness to glucocorticoids and stress, Journal of Neuroscience, 28, 6037–45.
Champagne, F.A. and Meaney, M.J. (2007) Transgenerational effects of social environment onvariations in maternal care and behavioral response to novelty, Behavioral Neuroscience, 121,1353–63.
Chapman, A., Meldrum, B. and Mendes, E. (1983) Acute anticonvulsant activity of structuralanalogues of valproic acid and changes in brain GABA and aspartate content, Life Sciences, 32,2023–31.
Charney, D.S., Heninger, G.R., Sternberg, D.E. et al. (1981) Presynaptic adrenergic receptor sensi-tivity in depression, Archives of General Psychiatry, 38, 1334–40.
Charney, D.S., Heninger, G.R. and Sternberg, D.E. (1983) Alpha-2 adrenergic receptor sensitivityand the mechanism of action of antidepressant therapy, British Journal of Psychiatry, 142, 265–75.
Charney, D.S., Heninger, G.R. and Breier, A. (1984a) Noradrenergic function in panic anxiety,Archives of General Psychiatry, 41, 751–63.
Charney, D.S., Heninger, G.R. and Sternberg, C.E. (1984b) The effect of mianserin on alpha-2adrenergic receptor function in depressed patients, British Journal of Psychiatry, 144, 407–16.
Checkley, S.A. (1979) Corticosteroid and growth hormone responses to methyl amphetamine indepressive illness, Psychological Medicine, 9, 107–15.
Checkley, S.A. (1985) Biological markers in depression. In Granville–Grossman (ed.), RecentAdvances in Clinical Psychiatry, Churchill Livingstone, Edinburgh, pp. 201–4.
Cheetham, S.C., Crompton, M.R., Katona, C.L.E. et al. (1988) Brain GABA-A benzodiazepinebinding sites and glutamic acid decarboxylase activity in depressed suicide victims, BrainResearch, 460, 114–23.
Christensen, E., Møller, J.E. and Faurbye, A. (1970) A neuropathological investigation of 28 brainsfrom patients with dyskinesia, Acta Psychiatrica Scandinavica, 46, 14–23.
Christensen, N.J., Vestergaard, P., Sorensen, T. et al. (1980) CSF adrenaline and noradrenaline indepressed patients, Acta Psychiatrica Scandinavica, 61, 178–82.
Christiansen, K.O. (1974) The genesis of aggressive criminality. In J. De Wit and W.W. Hastings(eds.), Determinants and Origins of Aggressive Behaviour, Moulton, The Hague, pp. 233–53.
Ciesielski, K.T., Beech, H.R. and Gordon, P.K. (1981) Some electrophysiological observations inobsessional states, British Journal of Psychiatry, 138, 479–84.
Cloninger, C.R. (1987) A systematic method for clinical description and classification of personalityvariants, Archives of General Psychiatry, 44, 573–88.
Cloninger, C.R. (2005) Antisocial personality disorder: a review. In M. Maj, H.S. Akiskal, J.E.Mezzich and A. Okasha (eds.), Personality Disorders, John Wiley and Sons, New York, NY, pp.125–169.
Cloninger, C.R. (2008) The psychobiological theory of temperament and character: comment onFarmer and Goldberg (2008), Psychological Assessment, 20, 292–9; Discussion 300–4.
Cloninger, C.R., Svrakic, D.M. and Przybeck, T.R. (1993) A psychobiological model of temperamentand character, Archives of General Psychiatry, 50, 975–90.
Cloninger, C.R., Przybeck, T.R., Svrakic, D.M. et al. (1994) The Temperamental Character Inventory, AGuide to its Development and Use. Washington University Center for Psychobiology of Personality,St Louis.
Cloninger, C.R., Adolfsson, R. and Svrakic, D.M. (1996a) Mapping genes for human personality,Nature Genetics, 12, 3–4.
Cloninger, C.R., Przybeck, T.R. and Svrakic, D.M. (1996b) The tridimensional personality question-naire: US normative data, Psychological Reports, 69, 1047–57.

References 345
Coccaro, E.F., Silverman, J.M., Klar, H.M. et al. (1994) Familial correlates of reduced centralserotonergic system function in patients with personality disorder, Archives of General Psychiatry,51, 318–24.
Coffey, C.E. (1993) The Clinical Science of ECT, American Physiological Society Press,Washington, DC.
Coffey, C.E. and Figiel, G.S. (1991) Neuropsychiatric significance of subcortical encephalomalacia.In B.J. Carroll and J.E. Barrett (eds.), Psychopathology and the Brain, Raven Press, New York, NY.pp. 243–63.
Coffey, C.E., Wilkinson, W.E., Weiner, R.D. et al. (1993) Quantitative cerebral anatomy in depres-sion, Archives of General Psychiatry, 50, 7–16.
Cohen, S.I. (1980) Cushing’s syndrome: a psychiatric study of 29 patients, British Journal ofPsychiatry, 136, 120–4.
Collinge, J., Owen. F., Poulter, M. et al. (1990) Prion dementia without characteristic pathology,Lancet, 336, 7–10.
Conlon, P., Trimble, M.R. and Rogers, D. (1990) A study of epileptic psychosis using MRI, BritishJournal of Psychiatry, 156, 231–5.
Consensus Development Conference Statement (1986) Electroconvulsive Therapy, 5(11), NIH.Conway, C.R., Sheline, Y.I., Chibnall, J.T. et al. (2006) Cerebral blood flow changes during vagus
nerve stimulation for depression, Psychiatry Research, 146, 179–84.Cook, I.A., Leuchter, A.F., Morgan, M.L. et al. (2005) Changes in prefrontal activity characterize
clinical response in SSRI nonresponders: a pilot study, Journal of Psychiatric Research, 39,461–6.
Cooper, S.J., Kelly, J.G. and King, D.J. (1985) Adrenergic receptors in depression, British Journal ofPsychiatry, 147, 23–9.
Coppen, A.J. and Shaw, D.M. (1963) Mineral metabolism in melancholia, British Medical Journal, ii,1439–44.
Coppen, A. and Wood, K. (1978) Tryptophan and depressive illness, Psychological Medicine, 8,49–57.
Coppen, A., Shaw, D.M. and Farrell, M.B. (1963) Potentiation of the antidepressive effect of a MAOIby tryptophan, Lancet, ii, 79–81.
Coppen, A.J., Malleson, A. and Shaw, D.M. (1965) Effects of lithium carbonate on electrolytedistribution in man, Lancet, i, 682–3.
Coppen, A., Prange, A.J., Whybrow, P.C. et al. (1972) Abnormalities of indoleamines in affectivedisorders, Archives of General Psychiatry, 26, 474–8.
Coppen, A., Ghose, K., Rao, R. et al. (1978) Mianserin and lithium in the prophylaxis of depression,British Journal of Psychiatry, 133, 206–10.
Coppen, A., Swade, S. and Wood, K. (1980) Lithium restores abnormal platelet 5-HT transport inpatients with affective disorders, British Journal of Psychiatry, 136, 235–8.
Coppen, A., Abou-Saleh, M., Milln, P. et al. (1983) DST in depression and other psychiatric illness,British Journal of Psychiatry, 142, 498–504.
Coppen, A., Milln, P., Harwood, J. et al. (1985) Does the DST predict antidepressant treatmentsuccess?, British Journal of Psychiatry, 146, 294–6.
Coursey, R.D., Buchsbaum, M.S. and Murphy, D.L. (1982) Two year follow up of subjects andtheir families defined as at risk for psychopathology on the bases of platelet MAO activities,Neuropsychobiology, 8, 51–6.
Cowdry, R.W., Pickar, D. and Davies, R. (1986) Symptoms and EEG findings in the borderlinesyndrome, International Journal of Psychiatry and Medicine, 15, 201–11.
Cowen, P. (1994) Antidepressant drugs and brain 5-HT function in humans, Neuropsychopharma-cology, 10, 45S.

346 References
Coyle, J., Prince, D.L. and DeLong, M.R. (1983) Alzheimer’s disease: a disorder of cholinergicinnervation, Science, 219, 1184–90.
Crayton, J.W. and Meltzer, H.Y. (1976) Motor endplate alterations in schizophrenic patients, Nature,264, 658–9.
Cross, A.J., Crow, T.J., Perry, R.H. et al. (1981) Reduced dopamine beta hydrolase activity inAlzheimer’s disease, British Medical Journal, 1, 93–4.
Cross, A.J., Crow, T.J., Johnson, J.A. et al. (1984) Studies of neurotransmitter receptor systems inneocortex and hippocampus in senile dementia of the Alzheimer type, Journal of the NeurologicalSciences, 64, 109–17.
Crow, T.J. (1988) Sex chromosome for psychosis in the case of the pseudo-autosomal locus, BritishJournal of Psychiatry, 153, 675–83.
Crow, T.J. (1991) The search of the psychosis gene, British Journal of Psychiatry, 158,611–14.
Crow, T.J. (2009) A theory of the origin of cerebral asymmetry: epigenetic variation superimposedon a fixed right-shift, Laterality, 1–15.
Crow, T.J. and Johnstone, E.C. (1986) Controlled trials of ECT. In S. Malitz and H.A. Sackeim (eds.),ECT, Annals of the New York Academy of Sciences, Vol. 462, pp. 12–29.
Crow, T.J., Johnstone, E.C. and Owen, F. (1979a) Research on schizophrenia. In Recent Advances inClinical Psychiatry, Churchill Livingstone, Edinburgh, pp. 1–36.
Crow, T.J., Baker, H.F., Cross, A.J. et al. (1979b) Monoamine mechanisms in chronic schizophrenia:post-mortem neurochemical findings, British Journal of Psychiatry, 134, 249–56.
Crow, T.J., Delisi, L.E., Lofthouse, R. et al. (1994) An examination of linkage of schizophrenia andschizoaffective disorder to the pseudoautosomal region (Xp 22.3).
Crow, T.J., Paez, P. and Chance, S.A. (2007) Callosal misconnectivity and the sex difference inpsychosis, International Review Psychiatry, 19, 449–57.
Crow, T.J., Close, J.P., Dagnall, A.M. et al. (2009) Where and what is the right shift factor or cerebraldominance gene? A critique of Francks et al. (2007), Laterality, 14, 3–10.
Cuesta, M.J., Peralta, V. and Caro, F. (1999) Premorbid personality in psychoses, SchizophreniaBulletin, 25, 801–11.
Cummings, J.L. (1985) Clinical Neuropsychiatry, Grune and Stratton, New York, NY.Cummings, J.L. (1992) Depression and Parkinson’s disease: a review, American Journal of Psychiatry,
149, 443–54.Cummings, J.L. and Benson, D.F. (1992) Dementia: A Clinical Approach, 2nd edition, Butterworths,
London.Cummings, J.L. and Trimble, M.T. (1995) A Concise Guide to Neuropsychiatry and Behavioural
Neurology, APA Press, Washington, DC.Cummings, J.L. and Trimble, M.R. (2002) A Concise Guide to Neuropsychiatry and Behavioural
Neurology, 2nd edition, APA Press, Washington, DC.Cummings, J.L., Benson, F., Hill, M.A. et al. (1985) Aphasia in dementia of the Alzheimer type,
Neurology, 35, 394–7.Curson, D.A., Barnes, T.R.E., Bamber, R.W. et al. (1985) Long-term depot maintenance of chronic
schizophrenic out patients, British Journal of Psychiatry, 146, 464–80.Curtis, D., Sherrington, R., Brett, P. et al. (1993) Genetic linkage analysis of manic depression in
Iceland, Journal of the Royal Society of Medicine, 86, 506–10.Czeizel, A.E. (2009) The unitary nature of functional psychoses, Lancet, 373, 809.Dager, S.R., Marro, K.I., Richards, T.L. et al. (1994) Preliminary application of MRS to investigate
lactate induced panic, American Journal of Psychiatry, 151, 57–63.Dahl, R.E., Kaufman, J., Ryan, N.D. et al. (1992) The dexamethasone test in children and adolescents,
Biological Psychiatry, 32, 109–26.

References 347
d’Alfonso, A.A., Aleman, A., Kessels, R.P. et al. (2002) Transcranial magnetic stimulation of leftauditory cortex in patients with schizophrenia: effects on hallucinations and neurocognition,Journal of Neuropsychiatry Clinical Neuroscience, 14, 77–9.
Damasio, H., Grabowski, T., Frank, R. et al. (1994) The return of Phineas Gage: clues about thebrain from the skull of a famous patient, Science, 264, 1102–5.
Dana-Haeri, J. and Trimble, M.R. (1984) Prolactin and gonadotrophin changes following partialseizures in epileptic patients with and without psychopathology, Biologice Psychiatry, 19(3),329–36.
Dannon, P.N., Dolberg, O.T., Schreiber, S. et al. (2002) Three and six-month outcome followingcourses of either ECT or rTMS in a population of severly depressed individuals: preliminaryreport, Biological Psychiatry, 51, 687–90.
Davidson, R.J. (1995) Cerebral asymmetry, emotion, and affective style. In R.J. Davidson andK. Hugdahl (eds.), Brain Asymmetry, MIT Press, Cambridge, MA, pp. 361–88.
Davies, R.K. (1979) Incest: some neuropsychiatric findings, International Journal of PsychiatricMedicine, 9, 117–21.
Davis, P. (1941) Electroencephalograms of manic-depressive patients, American Journal of Psychiatry,98, 430–3.
Deakin, J.F.W., Guimaraes, F.S., Wang, M. et al. (1991) Experimental tests of the 5-HT receptorimbalance theory of affective disturbances. In S.N. Sandler et al. (eds.), 5-HT in Psychiatry, OxfordUniversity Press, Oxford, pp. 143–57.
Debbane, M., van der Linden, M., Gex-Fabry, M. et al. (2009) Cognitive and emotional associationsto positive schizotypy during adolescence, Journal of Child Psychological Psychiatry, 50, 326–34.
Debruyn, A., Mendelbaum, K., Sandkuijl, L.A. et al. (1994) Nonlinkage of bipolar illness to tyrosinehydrolase, tyrosinease and D2 and D4 dopamine receptor genes on chromosome 11, AmericanJournal of Psychiatry, 151, 102–6.
de Geus, E.J., van ’t Ent, D., Wolfensberger, S.P. et al. (2007a) Intrapair differences in hippocampalvolume in monozygotic twins discordant for the risk for anxiety and depression, BiologicalPsychiatry, 61, 1062–71.
de Geus, F., Denys, D.A., Sitskoorn, M.M. et al. (2007b) Attention and cognition in patients withobsessive–compulsive disorder, Psychiatry Clinical Neuroscience, 61, 45–53.
Deicken, R.F., Calabrase, G., Merrin, E.L. et al. (1995) Basal ganglia phosphorous metabolism inchronic schizophrenia, American Journal of Psychiatry, 152, 126–9.
de Kloet, C.S., Vermetten E., Geuze E., et al. (2008) Elevated plasma corticotrophin-releasinghormone levels in veterans with posttraumatic stress disorder, Progress in Brain Research, 167,287–91.
de la Fuente, J.M., Tugendhaft, P. and Mavroudakis, N. (1998) Electroencephalographic abnormal-ities in borderline personality disorder, Psychiatry Research, 77, 131–8.
Delgado, J.M.R. (1966) Aggressive behaviour evoked by radio stimulation in monkey colonies,American Zoologist, 6, 669–81.
Delgado, P.L. (2006) Monoamine depletion studies: implications for antidepressant discontinuationsyndrome, The Journal of Clinical Psychiatry, 67, Suppl. 4, 22–6.
Delgado, P.L., Charney, D.S., Price, L.H. et al. (1990) Serotonin function and the mechanism ofantidepressant action, Archives of General Psychiatry, 47, 411–18.
Delgado, P.L., Price, L.H., Miller, H.L. et al. (1991) Rapid serotonin depletion as a provocativechallenge test for patients with major depression: relevance to antidepressant action and theneurobiology of depression, Psychopharmacology Bulletin, 27, 321–30.
Delgado, P.L., Price, L.H., Miller, H.L. et al. (1994) Serotonin and the neurobiology of depression:effects of tryptophan depletion in drug-free depressed patients, Archives of General Psychiatry,51, 865–74.

348 References
Delgado-Escueta, A., Mattson, R.H., King, L. et al. (1981) The nature of aggression during epilepticseizures, New England Journal of Medicine, 305, 711–16.
Delisi, L.E. (2008) The concept of progressive brain change in schizophrenia: implications forunderstanding schizophrenia, Schizophrenia Bulletin, 34, 312–21.
Delisi, L., Wise, C.O., Bridge, T. et al. (1982) Monamine oxidase and schizophrenia. In E. Usdin andI. Hanin (eds.), Biological Markers in Psychiatry and Neurology, Pergamon Press, New York, NY,pp. 79–96.
Delisi, L.E., Sakuma, M., Maurizio, A.M. et al. (2004) Cerebral ventricular change over the first 10years after the onset of schizophrenia, Psychiatry Research, 130, 57–70.
Delisi, L.E., Szulc, K.U., Bertisch, H. et al. (2006a) Early detection of schizophrenia by diffusionweighted imaging, Psychiatry Research, 148, 61–6.
Delisi, L.E., Szulc, K.U., Bertisch, H.C. et al. (2006b) Understanding structural brain changes inschizophrenia, Dialogues in Clinical Neuroscience, 8, 71–8.
de Tiege, X., Bier, J.C., Massat, I. et al. (2003) Regional cerebral glucose metabolism in aki-netic catatonia and after remission, Journal of Neurology, Neurosurgery and Psychiatry, 74,1003–4.
Devinsky, O., Cox, C., Witt, E. et al. (1991) Ictal fear in temporal lobe epilepsy, Journal of Epilepsy, 4,231–8.
Devinsky, O. and Luciano, D. (1993) The contributions of cingulate cortex to human behavior. InB.A. Vogt and M. Gabriel (eds.), Neurobiology of Cingulate Cortex and Limbic Thalamus, Birkhauser,Boston, MA.
Dinan, T.G. (1994) Glucocorticoids and the genesis of depressive illness, British Journal of Psychiatry,164, 365–71.
Doble, A. and Martin, I.L. (1992) Multiple benzodiazepine receptors, TIPS, 13, 16–18.Dolan, M. and Park, I. (2002) The neuropsychology of antisocial personality disorder, Psychological
Medicine, 32, 417–27.Dolan, R.J., Galloway, S.P., Fonagy, P. et al. (1985a) Life events, depression and hypothalamic
pituitary–adrenal axis function, British Journal of Psychiatry, 147, 429–34.Dolan, R.J., Calloway, S.P. and Mann, A.H. (1985b) Cerebral ventricular size in depressed subjects,
Psychological Medicine, 15, 873–8.Dolan, R.J., Poynton, A.M., Bridges, P.K. et al. (1990) Altered magnetic resonance white matter T1
values in patients with affective disorder, British Journal of Psychiatry, 157, 107–10.Doran, A.R., Rubinow, D.R., Roy, A. et al. (1986) CSF somatostatin and abnormal response to
dexamethasone administration in schizophrenic and depressed patients, Archives of GeneralPsychiatry, 43, 365–9.
Dorrow, R., Horowski, R., Paschelke, G. et al. (1983) Severe anxiety induced by FG 7142, Lancet, ii,98–9.
Dorus, E. (1980) Variability in the Y chromosome and variability in human behaviour, Archives ofGeneral Psychiatry, 37, 587–94.
Drevets, W.C., Videen, T.O., MacLeod, A.K. et al. (1992) PET images of blood flow changes duringanxiety: correction, Science, 256, 1696.
Drevets, W.C. (2003) Neuroimaging abnormalities in the amygdala in mood disorders, Annals ofthe New York Academy of Sciences, 985, 420–44.
Drevets, W.C., Thase, M.E., Moses-Kolko, E.L. et al. (2007) Serotonin-1a receptor imaging inrecurrent depression: replication and literature review, Nuclear Medicine and Biology, 34,865–77.
Drevets, W.C., Price, J.L. and Furey, M.L. (2008) Brain structural and functional abnormalitiesin mood disorders: implications for neurocircuitry models of depression, Brain Structure &Function, 213, 93–118.

References 349
Driessen, M., Herrmann, J., Stahl, K. et al. (2000) Magnetic resonance imaging volumes of thehippocampus and the amygdala in women with borderline personality disorder and earlytraumatization, Archives of General Psychiatry, 57, 1115–22.
Driessen, M., Wingenfeld, K., Rullkoetter, N. et al. (2008) One-year functional magnetic resonanceimaging follow-up study of neural activation during the recall of unresolved negative life eventsin borderline personality disorder, Psychological Medicine, 1–10.
Drubach, D.A. and Kelly, M.P. (1989) Panic disorder associated with right paralimbic lesion,Neuropsychiatry, Neuropsychology and Behavioural Neurology, 4, 282–9.
D’souza, D.C., Abi-Saab, W.M., Madonick, S. et al. (2005) Delta-9-tetrahydrocannabinol effects inschizophrenia: implications for cognition, psychosis, and addiction, Biological Psychiatry, 57,594–608.
Dubrovsky, B. (1993) Effects of adrenal cortex hormones on limbic structures: some experimentaland clinical correlations related to depression, J Psychiatry Neurosci, 18, 4–16.
Duman, R.S. (2005) Neurotrophic factors and regulation of mood: role of exercise, diet andmetabolism, Neurobiological Aging, 26, Suppl. 1, 88–93.
Dwivedi, Y., Rizavi, H.S., Conley, R.R. et al. (2003) Altered gene expression of brain-derivedneurotrophic factor and receptor tyrosine kinase B in postmortem brain of suicide subjects,Archives of General Psychiatry, 60, 804–15.
Dworkin, R.H. and Lenzenweger, M.F. (1984) Symptoms and the genetics of schizophreniaimplications for diagnosis, American Journal of Psychiatry, 141, 1541–6.
Ebert, D., Feistel, H., Kaschka, W. et al. (1994) SPECT assessment of cerebral dopamine D2receptor blockade in depression before and after sleep deprivation, Biological Psychiatry, 35,880–5.
Edeh, J. and Toone, B.K. (1985) Antiepileptic therapy, folate deficiency, and psychiatric morbidity:a general practice survey, Epilepsia, 26, 434–40.
Edelman, G.M. (1989) The Remembered Present, Basic Books, New York, NY.Eeg-Olofsson, O., Petersen, I. and Sellden, U. (1971) The development of the EEG in normal children
from the age of 1 through 15 years, Neuropaediatrie, 2, 375–404.Egrise, D., Rubinstein, M., Schoutens, A. et al. (1986) Seasonal variation of platelet serotonin binding
in normal and depressed subjects, Biological Psychiatry, 21, 283–92.Eichelmann, B. (1979) Role of biogenic amines in aggressive behaviour. In M. Sandler (ed.),
Psychopharmacology of Aggression, Raven Press, New York, NY, pp. 61–93.Elger, G., Hoppe, C., Falkai, P. et al. (2000) Vagus nerve stimulation is associated with mood
improvements in epilepsy patients, Epilepsy Research, 42, 203–10.Eliez, S. (2007) Autism in children with 22q11.2 deletion syndrome, Journal of the Amenice Academic
of Child and Adolescent Psychiatry, 46, 433–4; Author Reply 434–4.Ellis, P.M. and Salmond, C. (1994) Is platelet imipramine binding reduced in depression?, Biological
Psychiatry, 36, 292–300.El-Mallakh, R.S. and Wyatt, R.J. (1995) The Na, K-ATPase hypothesis for bipolar illness, Biological
Psychiatry, 37, 235–44.Emrich, H.M., Dose, M. and von Zerssen, D. (1984) Action of sodium valproate and of oxycar-
bazepine in patients with affective disorders. In H.M. Emrich et al. (eds.), Anticonvulsants inAffective Disorders, Excerpta Medica, Oxford, pp. 45–55.
Engel, J. (2006a) ILAE classification of epilepsy syndromes, Epilepsy Research, 70, Suppl. 1, S5–S10.Engel, J. (2006b) Report of the ILAE classification core group, Epilepsia, 47, 1558–68.Engel, J., Fejerman, N., Berg, A.T. et al. (2007) Classification of the epilepsies. In J. Engel and T.
Pedley (eds.), Epilepsy: A Comprehensive textbook, 2nd edition, Lippincott Williams & Wilkins,New York, NY, pp. 767–72.
Engin, E., Treit, D. and Dickson, C.T. et al. in Neuroscience, 162(4), 1438–9.

350 References
Erkinjuntti, T. and Gauthier, S. (2009) The concept of vascular cognitive impairment, Frontiers ofNeurology and Neuroscience, 24, 79–85.
Eser, D., Baghai, T.C., Schule, C. et al. (2008a) Neuroactive steroids as endogenous modulators ofanxiety, Current Pharmaceutical Design, 14, 3525–33.
Eser, D., Wenninger, S., Baghai, T. et al. (2008b) Impact of state and trait anxiety on the panicresponse to CCK-4, Journal of Neurological Transmission, 115, 917–20.
Esler, M., Turbott, J., Schwartz, R. et al. (1982) The peripheral kinetics of norepinephrine indepressive illness, Archives of General Psychiatry, 39, 295–300.
Esslinger, C., Walter, H., Kirsch, P. et al. (2009) Neural mechanisms of a genome-wide supportedpsychosis variant, Science, 324, 605.
Ettinger, A., Reed, M., Cramer, J. and the Epilepsy Impact Project Group (2004) Depression andcomorbidity in community-based patients with epilepsy or asthma, Neurology, 63, 1008–14.
Ettinger, A.B., Reed, M.L., Goldberg, J.F. et al. (2005) Prevalence of bipolar symptoms in epilepsyvs other chronic health disorders, Neurology, 65, 535–40.
Extein, I., Tallman, J., Smith, C.C. et al. (1979) Changes in lymphocyte beta adrenergic receptors indepression and mania, Psychiatric Research, 1, 191–7.
Extein, I., Pottash, A.L.C. and Gold, M.S. (1981) Relation of TRH test and DST abnormalities inunipolar depression, Psychiatry Research, 4, 49–53.
Extein, I., Pottash, A.L.C., Gold, M.S. et al. (1982) TSH response to TRH in unipolar depressionbefore and after clinical improvement, Psychiatry Research, 6, 161–9.
Fabricius, K., Wortwein, G. and Pakkenberg, B. (2008) The impact of maternal separation on adultmouse behaviour and on the total neuron number in the mouse hippocampus, Brain StructureFunction, 212, 403–16.
Farde, L., Wiesel, F.-A., Stone-Elander, S. et al. (1990) D2 dopamine receptors in neuroleptic-naiveschizophrenic patients, Archives of General Psychiatry, 47, 213–19.
Feighner, J.P., Robins, E., Guze, S.B. et al. (1972) Diagnostic criteria for use in psychiatric research,Archives of General Psychiatry, 26, 57–63.
Fenton, G.W. (1972) Epilepsy and automatism, British Journal of Hospital Medicine, 7, 57–64.Fenwick, P. (1981) Precipitation and inhibition of seizures. In E.H. Reynolds and M.R. Trimble
(eds.), Epilepsy and Psychiatry, Churchill Livingstone, Edinburgh, pp. 242–63.Fenwick, P. (1986) Aggression and epilepsy. In M.R. Trimble and T. Bolwig (eds.), Aspects of Epilepsy
and Psychiatry, John Wiley and Sons, Chichester, pp. 31–60.Fergusson, D., Doucette, S., Glass, K.C. et al. (2005) Association between suicide attempts and
selective serotonin reuptake inhibitors: systematic review of randomised controlled trials,British Medical Journal, 330, 396.
Filbey, F.M., Toulopoulou, T., Morris, R.G. et al. (2008) Selective attention deficits reflect increasedgenetic vulnerability to schizophrenia, Schizophrenia Research, 101, 169–75.
Fink, M. (1986) Convulsive therapy and epilepsy research. In M.R. Trimble and E.H. Reynolds(eds.), What is Epilepsy?, Churchill Livingstone, Edinburgh, pp. 217–28.
Finley, G.W. and Campbell, C.M. (1941) Electroencephalography in schizophrenia, American Journalof Psychiatry, 98, 374–84.
Fisch, C. (1985) Effect of fluoxetine on the electrocardiogram, Journal of Clinical Psychiatry, 46, 42–4.Fitzgerald, P.B., Benitez, J., Daskalakis, J.Z. et al. (2006) The treatment of recurring auditory
hallucinations in schizophrenia with rTMS, World Journal of Biological Psychiatry, 7, 119–22.Fleischmann, A., Sternheim, A., Etgen, A.M. et al. (1996) Transcranial magnetic stimulation down-
regulates beta-adrenoreceptors in rat cortex, Journal of Neural Transmission, 103, 1361–6.Flor-Henry, P. (1969) Psychosis and temporal lobe epilepsy, Epilepsia, 10, 363–95.Flor-Henry, P. (1983) Cerebral Basis of Psychopathology, John Wright, Bristol.

References 351
Flugel, D., Cercignani, M., Symms, M.R. et al. (2006) Diffusion tensor imaging findings andtheir correlation with neuropsychological deficits in patients with temporal lobe epilepsy andinterictal psychosis, Epilepsia, 47, 941–4.
Foley, J.O. and Dubois, F. (1937) Quantitative studies of the vagus nerve in the cat: I. the ratio ofsensory and motor studies. Journal of Comparative Neurology, 67, 49–67.
Folstein, M.F., Maiberger, R. and McHugh, P.R. (1977) Mood disorder as a specific complication ofstroke, Journal of Neurology, Neurosurgery and Psychiatry, 40, 1018–20.
Fontaine, R., Breton, G., Dery, R. et al. (1990) Temporal lobe abnormalities in panic disorder: anMRI study, Biological Psychiatry, 27, 304–10.
Forstl, H., Burns, A., Levy, R. et al. (1994) Neuropathological correlates of psychotic phenomena inconfirmed Alzheimer’s disease, British Journal of Psychiatry, 165, 53–9.
Fountoulakis, K.N. and Akiskal, H.S. (2008) Focus on bipolar illness, CNS Spectrums, 13, 762.Fowler, C.J., von Knorring, L. and Oreland, L. (1980) Platelet MAO in sensation seekers, Psychiatry
Research, 273–9.Fox, J.H., Topel, J.L. and Huckman, M.S. (1975) Use of computerized axial tomography in senile
dementia, Journal of Neurology, Neurosurgery and Psychiatry, 38, 948–53.Frackowiak, R.S.J., Lenzi, G.L., Jones, T. et al. (1980) Quantitative measurements of regional CBF
and oxygen metabolism in man using 15 O and PET: theory, procedure and normal values,Journal of Computer Assisted Tomography, 4, 727–36.
Frackowiak, R.S.J., Pozzilli, C., Legg, N.J. et al. (1981) Regional cerebral oxygen supply andutilisation in dementia, Brain, 104, 753–8.
Francis, P.T. and Bowen, D.M. (1985) Relevance of reduced concentrations of somatostatin inAlzheimer’s disease, Biochemical Society Transactions, 13, 170–1.
Francis, P.T., Palmer, A.M., Sims, N.R. et al. (1985) Neurochemical study of early onset Alzheimer’sdisease, New England Journal of Medicine, 313, 7–11.
Fredrikson, M., Wik, G., Greitz, T. et al. (1993) Regional cerebral blood flow during experimentalphobic fear, Psychophysiology, 30, 126–30.
Freeman, W. and Watts, J.W. (1947) Psychosurgery during 1936–46, Archives of Neurology andPsychiatry, 58, 417–25.
Friedman, M.J., Stolk, J.M., Harris, P.Q. et al. (1984) Serum dopamine–beta-hydrolase activity indepression and anxiety, Biological Psychiatry, 19, 557–70.
Friston, K.J., Frith, C.D., Liddle, P.F. et al. (1991) Comparing functional (PET) images: the assessmentof significant change, Journal of Cerebral Blood Flow and Metabolism, 11, 690–9.
Friston, K.J., Liddle, P.P., Firth, C.D. et al. (1992) The left median temporal region and schizophrenia,Brain, 115, 367–82.
Friston, K.J., Holmes, A., Poline, J.B. et al. (1996) Detecting activations in PET and fMRI: levels ofinference and power, Neuroimage, 4, 223–35.
Frolich, E.D., Tarazi, R.C. and Dunstan, H.F. (1969) Hyperdynamic beta-adrenergic circulatorystate, Archives of Internal Medicine, 123, 1–7.
Fulton, J.F. and Jacobsen, C.G. (1935) The functions of the frontal lobes, a comparative study inmonkeys, chimpanzees and men, Advances in Modern Biology, 4, 113–23.
Fuster, J.M. (1980) The Pre-frontal Cortex, Raven Press, New York, NY.Fuster, J.M. (1993) Frontal lobes, Current Opinion in Neurobiology, 3, 160–5.Fuster, J.M. (2004) Upper processing stages of the perception-action cycle, Trends in Cognitive
Sciences, 8, 143–5.Gainotti, G. (1972) Emotional behaviour and hemispheric side of the lesion, Cortex, 8, 41–55.Garber, H.J., Anarth, J.V., Chiu, L.C et al. (1989) Nuclear magnetic resonance study of OCD,
American Journal of Psychiatry, 146, 1001–5.

352 References
Garcia-Sevilla, J.A., Athanasios, P.Z., Hollingsworth, P.J. et al. (1981) Platelet alpha 2 adrenergicreceptors in major depressive disorder, Archives of General Psychiatry, 38, 1327–33.
Garcia-Sevilla, J.A., Guimon, J., Garcia-Valleto, P. et al. (1986) Biochemical and functional evidenceof supersensitive platelet alpha-2 adrenoceptors in major affective disorder, Archives of GeneralPsychiatry, 43, 51–7.
Gartrell, N. (1986) Increased libido in women receiving trazadone, American Journal of Psychiatry,143, 781–2.
Geisler, S. (2008) The lateral habenula: no long neglected, CNS Spectrums, 13, 484–9.Gentsch, C., Lichtsteiner, M. and Freer, H. (1981) 3-H diazepam binding sites in Roman high- and
low-avoidance rats, Experientia, 37, 1315–16.George, M.S. (2002) Advances in brain stimulation: guest editorial, The Journal of ECT, 18, 169.George, M.S. and Belmaker, R.H. (2000) Transcranial Magnetic Stimulation in Neuropsychiatry,
American Psychiatric Press, Washington, DC.George, M.S. and Belmaker, R.H. (2006) TMS in Clinical Psychiatry, American Psychiatric Press,
Washington, DC.George, M.S. and Wassermann, E.M. (1994) Rapid-rate transcranial magnetic stimulation (rTMS)
and ECT, Convulsive Therapy, 10(4), 251–3.George, M.S., Ring, H.A., Costa, D.C. et al. (1991) Neuroactivation and Neuroimaging with SPET,
London, Springer-Verlag.George, M.S., Ring, H.A., Costa, D.C. et al. (1992) Demonstration of human motor cortex activation
using SPECT, Journal of Neural Transmission, 87, 231–6.George, M.S., Ketter, T.A., Gill, D.S. et al. (1993) Brain regions involved in recognizing facial
emotion or identity: an oxygen-15 PET study, Journal of Neuropsychiatry Clinical Neuroscience, 5,384–94.
George, M.S., Ketter, T.A. and Post, R.M. (1994a) Prefrontal cortex dysfunction in clinical depression,Depression, 2, 59–72.
George, M.S., Ketter, T.A. and Post, R.M. (1994c) Activation studies in mood disorders, PsychiatricAnnals, 24, 648–52.
George, M.S., Ketter, T.A. and Post, R.M. (1994d) Prefrontal cortex dysfunction in clinical depres-sion, Depression, 2, 59–72.
George, M.S., Post, R.M., Ketter, T.A. et al. (1995a) Neural mechanisms of mood disorders. In A.J.Rush (ed.), Current Review of Mood Disorders, Current Medicine, Philadelphia.
George, M.S., Wassermann, E.M., Williams, W.A. et al. (1995b) Daily repetitive transcranial mag-netic stimulation (RTMS) improves mood in depression, Neuroreport, 6, 1853–6.
George, M.S., Ketter, T.A., Parekh, P.I. et al. (1995c) Depressed subjects have abnormal righthemisphere activation during facial emotion recognition, Journal of Neuropsychiatry ClinicalNeuroscience, 9, 55–63.
George, M.S., Ketter, T.A. and Post, R.M. (1996) What functional imaging studies have revealedabout the brain basis of mood and emotion. In J. Panksepp (ed.), Advances in Biological Psychiatry,Jai Press, Greenwich, CN, pp. 63– 113.
George, M.S., Huggins, T., McDermut, W. et al. (1998) Abnormal facial emotion recognition indepression: serial testing in an ultra-rapid-cycling patients, Behavioral Modification, 22, 192–204.
George, M.S., Stallings, L.E., Speer, A.M. et al. (1999a) Prefrontal repetitive transcranial magneticstimulation (rTMS) changes relative perfusion locally and remotely, Human Psychopharmacology,14, 161–70.
George, M.S., Teneback, C.C., Malcolm, R.J. et al. (1999b) Multiple previous alcohol detoxificationsare associated with decreased medial temporal and paralimbic function in the postwithdrawalperiod, Alcohol Clinical Experiment Research, 23, 1077–84.

References 353
George, M.S., Sackeim, H.A., Rush, A.J. et al. (2000) Vagus nerve stimulation: a new tool for brainresearch and therapy, Biological Psychiatry, 47, 287–95.
George, M.S., Anton, R.F., Bloomer, C. et al. (2001) Activation of prefrontal cortex and anteriorthalamus in alcoholic subjects on exposure to alcohol-specific cues, Archives of General Psychiatry,58, 345–52.
George, M.S., Myrick, H., Li, X. et al. (2002a) Assessing the brain sequelae of alcoholism usingbrain imaging. In B.A. Johnson, P. Ruiz and M. Galanter (eds.), Alcoholism: A Practical Handbook,Lippincott Williams & Wilkins, New York, NY, pp. 94–9.
George, M.S., Nahas, Z., Kozel, F.A. et al. (2002b) Mechanisms and state of the art of transcranialmagnetic stimulation, The Journal of ECT, 18, 170–81.
George, M.S., Rush, A.J., Marangell, L.B. et al. (2005) A one-year comparison of vagus nervestimulation with treatment as usual for treatment-resistant depression, Biological Psychiatry, 58,364–73.
George, R., Salinsky, M., Kuzniecky, R. et al. (1994b) Vagus nerve stimulation for treatment ofpartial seizures: 2. long-term follow-up on first 67 patients exiting a controlled study, Epilepsia,35, 637–43.
Gerner, R.H., Fairbanks, L., Anderson, G.M. et al. (1984) CSF neurochemistry in depressed, manicand schizophrenic patients compared with that of normal controls, American Journal of Psychiatry,141, 1533–40.
Gershon, E. (1983) The genetics of affective disorders. In L. Grinspoon (ed.), Psychiatry Update,Vol. 2, APA, Washington, DC, pp. 434–56.
Geschwind, N. (1979) Behavioural changes in TLE, Psychological Medicine, 9, 217–19.Ghose, K., Turner, P. and Coppen, A. (1975) Intravenous tyramine pressor response in depression,
Lancet, i, 1317–18.Gibbons, R.D., Hur, K., Bhaumik, D.K. et al. (2005) The relationship between antidepressant
medication use and rate of suicide, Archives of General Psychiatry, 165–72.Gilliam, F., Kuzniecky, R., Faught, E. et al. (1997) Patient validated content of epilepsy specific
quality of life measurement, Epilepsia, 38, 233–6.Gilliam, F.G., Barry, J.J., Hermann, B.P. et al. (2006) Rapid detection of major depression in epilepsy:
a multicentre study, Lancet Neurology, 5, 399–405.Gillin, J.C., Sitaram, N., Wehr, T. et al. (1985) Sleep and affective illness. In R.M. Post and J.C.
Ballenger (eds.), Neurobiology of Mood Disorders, Williams and Wilkins, Baltimore, pp. 157–89.Gilman, J.M. and Hommer, D.W. (2008) Modulation of brain response to emotional images by
alcohol cues in alcohol-dependent patients, Addiction Biology, 13, 423–34.Gjerris, A. (1988) Baseline studies on transmitter substances in CSF in depression, Acta Psychiatrica
Scandinavica, 73, Suppl. 346.Gjessing, R. (1947) Biological investigations in endogenous psychoses, Acta Psychiatrica Neurologica
Scandinavica, Suppl. 47.Glass, I.B., Checkley, S.A., Shur, E. et al. (1982) Effect of desipramine upon central adrenergic
function in depressed patients, British Journal of Psychiatry, 141, 372–6.Glassman, A.H., Perel, J.M., Shostak, M. et al. (1977) Clinical implications of imipramine plasma
levels for depressive illness, Archives of General Psychiatry, 34, 197–204.Glenn, A.L. and Raine, A. (2008) The neurobiology of psychopathy, Psychiatric Clinics North America,
31, 463–75, vii.Gloor, P., Olivier, A., Quesney, L.F. et al. (1982) The role of the limbic system in experiential
phenomena of TLE, Annals of Neurology, 12, 129–44.Goldman-Rakic, P.S. (1994) Working memory dysfunction in schizophrenia, Journal of Neuropsychi-
atry Clinical Neuroscience, 6, 348–57.

354 References
Gold, P., Kling, M.A., Demitrack, M.A. et al. (1988) Clinical studies with CRH. In D. Gentenand D. Pfaff (eds.), Current Trends in Neuroendocrinology, Vol. 8, Springer Verlag, Berlin,pp. 238–56.
Gomez, R.G., Fleming, S.H., Keller, J. et al. (2006) The neuropsychological profile of psychotic majordepression and its relation to cortisol, Biological Psychiatry, 60, 472–8.
Gonda, X., Fountoulakis, K.N., Rihmer, Z. et al. (2009) Towards a genetically validated newaffective temperament scale: a delineation of the temperament phenotype of 5-HTTLPR usingthe Temps-A, Journal Of Affective Disorders, 112, 19–29.
Gonul, A.S., Akdeniz, F., Taneli, F. et al. (2005) Effect of treatment on serum brain-derivedneurotrophic factor levels in depressed patients, European Archives of Psychiatry and ClinicalNeuroscience, 255(6), 381–6.
Good, K., Lawrence, N.S., Thomas, C.J. et al. (2003) Dosage-sensitive X-linked locus influences thedevelopment of amygdala and orbitofrontal cortex and fear recognition in humans, Brain, 126,2431–46.
Goodwin, D.W. and Guze, S.B. (1984) Psychiatric Diagnosis, 3rd edition, Oxford University Press,Oxford.
Gordon, E.B. (1968) Serial EEG studies in presenile dementia, British Journal of Psychiatry, 114,779–80.
Gorman, J.M., Levy, G.F., Liebowitz, M.R. et al. (1983) Effect of acute beta adrenergic blockade onlactate-induced panic, Archives of General Psychiatry, 40, 1079–82.
Gorman, J., Liebowitz, M.R., Fyer, A.J. et al. (1985) Platelet MAO activity in patients with panicdisorder, Biological Psychiatry, 20, 852–8.
Gorman, J.M., Liebowitz, M.R., Fyer, A.J. et al. (1989) A neuroanatomical hypothesis for panicdisorder, American Journal of Psychiatry, 146, 148–61.
Gottesman, I.I. (1962) Differential inheritance of the psychoneuroses, Eugenics Quarterly, 9, 223–7.Gottesman, I.I. and Bertelsen, A. (1989) Confirming unexpressed genotypes for schizophrenia,
Archives of General Psychiatry, 46, 867–72.Gottesman, I.I. and Shields, J. (1972) Schizophrenia and Genetics: A Twin Study Vantage Point,
Academic Press, London.Gouw, A.A., van der Flier, W.M., Fazekas, F. et al. (2008) Progression of white matter hyperinten-
sities and incidence of new lacunes over a 3-year period: the leukoaraiosis and disability study,Stroke, 39, 1414–20.
Gray, J.A. (1982) The Neuropsychology of Anxiety: An Enquiry into the Functions of the Septo-hippocampalSystem, Oxford University Press, New York, NY.
Graybiel, A.M. (1990) Neurotransmitters and modulators in the basal ganglia, TINS, 13,244–54.
Greicius, M.D., Flores, B.H., Menon, V. et al. (2007) Resting-state functional connectivity in majordepression: abnormally increased contributions from subgenual cingulate cortex and thalamus,Biological Psychiatry, 62, 429–37.
Green, A.R. (1986) Changes in GABA biochemistry and the seizure threshold. In S. Malitz and H.A.Sackeim (eds.), ECT, Annals of the New York Academy of Sciences, Vol. 462, pp. 105–18.
Green, T., Gothelf, D., Glaser, B. et al. (2009) Psychiatric disorders and intellectual functioningthroughout development in velocardiofacial (22q11.2 deletion) syndrome, Journal of AmericanAcademics of Child and Adolescence Psychiatry, 48(11), 1060–8.
Greenberg, D.B. and Brown, G.L. (1985) Mania resulting from brain stem tumour, Journal of Nervousand Mental Diseases, 173, 434–6.
Greenberg, B.D., George, M.S., Dearing, J. et al. (1997) Effect of prefrontal repetitive transcranialmagnetic stimulation (rTMS) in obsessive compulsive disorder: a preliminary study, AmericanJournal of Psychiatry, 154, 867–869.

References 355
Greenberg, B.D., Askland, K.D. and Carpenter, L.L. (2008) The evolution of deep brain stimulationfor neuropsychiatric disorders, Frontiers in Bioscience, 13, 4638–48.
Griesinger, W. (1867) Mental Pathology and Therapeutics (Translated by C. Lockhart Robertson andJ. Rutherford), New Sydenham Society, London.
Grisaru, N., Yarovslavsky, U., Abarbanel, J. et al. (1994) Transcranial magnetic stimulation indepression and schizophrenia, European Neuropsychopharmacology, 4, 287–288.
Groenewegen, H.J. (1997) Cortical-subcortical relationships and the limbic forebrain. In M.R.Trimble and J. Cummings, Behavioural Neurology, Butterworth-Heinemann, pp. 29–48.
Guay, J.P., Ruscio, J., Knight, R.A. et al. (2007) A taxometric analysis of the latent structure ofpsychopathy: evidence for dimensionality, Journal of Abnormal Psychology, 116, 701–16.
Gunne, L.M., Haggstrom, J.E. and Sjoquist, B. (1984) Association with persistent neuroleptic-induced dyskinesia of regional changes in brain GABA synthesis, Nature, 304, 347–9.
Gur, R.E., Calkins, M.E., Gur, R.C. et al. (2007) The consortium on the genetics of schizophrenia:neurocognitive endophenotypes, Schizophrenia Bulletin, 33, 49–68.
Gureje, O. (1991) Interictal psychopathology in epilepsy: prevalence and pattern in a Nigerianclinic, British Journal of Psychiatry, 158, 700–5.
Guy, J.D., Majorski, L.V., Wallaco, C.J. et al. (1983) The incidence of minor physical abnormalitiesin male schizophrenics, Schizophrenia Bulletin, 9, 571–82.
Hachinski, V.C., Linnette, D., Zilhka, E. et al. (1975) Cerebral blood flow in dementia, Archives ofNeurology, 32(9), 632–7.
Haenschel, C., Bittner, R.A., Haertling, F. et al. (2007) Contribution of impaired early-stage visualprocessing to working memory dysfunction in adolescents with schizophrenia: a study withevent-related potentials and functional magnetic resonance imaging, Archives in General Psychi-atry, 64, 1229–40.
Haenschel, C., Bittner, R.A., Waltz, J. et al. (2009) Cortical oscillatory activity is critical for work-ing memory as revealed by deficits in early-onset schizophrenia, Journal of Neuroscience, 29,9481–9.
Hakola, H.P.A. and Iivanainen, M. (1978) Pneumoencephalographic and clinical findings of theXYY syndrome, Acta Psychiatrica Scandinavica, 58, 360–6.
Hale, A.S., Hannah, P., Sandler, M. et al. (1989) Tyramine conjugation test for prediction of treatmentresponse in depressed patients, Lancet, i, 234–6.
Hall, K.C.W. (1980) Depression. In R.C.W. Hall (ed.), Psychiatric Presentations of Medical Illness,MTP, Press, Lancaster, pp. 37–63.
Han, M., Deng, C., Burne, T.H. et al. (2008) Short- and long-term effects of antipsychotic drugtreatment on weight gain and H1 receptor expression, Psychoneuroendocrinology, 33, 569–80.
Handforth, A., Degiorgio, C.M., Schachter, S.C. et al. (1998) Vagus nerve stimulation therapy forpartial-onset seizures: a randomized active-control trial, Neurology, 51, 48–55.
Hanna, G.L., Yuwiler, A. and Cartwell, D.P. (1993) Whole-blood serotonin during clomipraminetreatment of juvenile obsessive–compulsive disorder, Journal of Child and Adolescent Psychophar-macology, 3, 223–9.
Harden, C.L., Pulver, M.C., Ravdin, L.D. et al. (2000) A pilot study of mood in epilepsy patientstreated with vagus nerve stimulation, Epilepsy and Behavior, 1, 93–9.
Hardy, J., Cowburn, R., Barton, A. et al. (1987) Glutamate deficits in Alzheimer’s disease, Journal ofNeurology, Neurosurgery and Psychiatry, 50, 356–9.
Hare, R.D. (1999) Psychopathy as a risk factor for violence, Psychiatric Quarterly, 70, 181–97.Hariri, A.R., Mattay, V.S., Tessitore, A. et al. (2002) Genetic variation and the response of the human
amygdale, Science, 297, 400–3.Harrison, W.M., Cooper, T.B., Stewart, J.W. et al. (1984) The tyramine challenge test as a marker for
melancholia, Archives of General Psychiatry, 41, 681–5.

356 References
Harro, J., Vasar, E. and Bradwejn, J. (1993) CCK in animal and human research on anxiety, TIPS,14, 244–9.
Hart, S.D. and Hare, R.D. (1997) Psychopathy: assessment and association with criminal conduct.In D.M. Stoff, J. Breiling and M.D. Maser (eds.), Handbook of Antisocial Behavior, John Wiley andSons, New York, NY, pp. 22–35.
Harvey, I., Persand, R., Ron, M.A. et al. (1994) Volumetric MRI measurements in bipolars comparedwith schizophrenics and healthy controls, Psychological Medicine, 24, 1–11.
Hauser, P., Altschuler, L.L., Berrettini, W. et al. (1989) Temporal lobe measurement in primaryaffective disorder by MRI, Journal of Neuropsychiatry and Clinical Neuroscience, 1, 128–34.
Hauser, P., Matochik, J., Altshuler, L.L. et al. (2000) MRI-based measurements of temporal lobeand ventricular structures in patients with bipolar I and bipolar II disorders, Journal of AffectiveDisorders, 60, 25–32.
Hauser, W.A. and Beghi, E. (2008) First seizure definitions and worldwide incidence and mortality,Epilepsia, 49, Suppl. 1, 8–12.
Hayden, E.P. and Nurnberger, J.I., Jr (2006) Molecular genetics of bipolar disorder, Genes, Brain,and Behavior, 5, 85–95.
Hazlett, E.A., Buchsbaum, M.S., Zhang, J. et al. (2008) Frontal-striatal-thalamic mediodorsal nucleusdysfunction in schizophrenia-spectrum patients during sensorimotor gating, Neuroimage, 42,1164–77.
Healy, D., Carney, P.A. and Leonard, B.E. (1983) Monoamine related markers of depression:changes following treatment, Journal of Psychiatric Research, 17, 251–60.
Heath, R.G. (1962) Common characteristics of epilepsy and schizophrenia, American Journal ofPsychiatry, 118, 1013–26.
Heath, R.G. (1972) Pleasure and brain activity in man, Journal of Nervous and Mental Diseases, 154,3–18.
Heath, R.G. (1982) Psychosis and epilepsy: similarities and differences in the anatomic–physiologicsubstrate. In W.P. Koella and M.R. Trimble (eds.), Temporal Lobe Epilepsy, Mania and Schizophreniaand the Limbic System, Karger, Basle, pp. 106–16.
Heath, R.G., Dempesy, C.W., Fontana, C.J. et al. (1978) Cerebellar stimulation: effects on septalregion, hippocampal and amygdala of cats and rats. Biological Psychiatry, 13, 501–29.
Heimer, L. and Larsson, E. (1966) Impairment of mating behaviour in male rats following lesionsin the pre-optic and anterior hypothalamic continuum, Brain Research, 3, 248–63.
Heimer, L., van Hoesen, G.W., Trimble, M. et al. (2007) Anatomy of Neuropsychiatry, Academic Press,San Diego, CA.
Heinz, A., Braus, D.F., Smolka, M.N. et al. (2005) Amygdala pre-frontal coupling depends on agenetic variation of the serotonin transporter, Nature Neuroscience, 8, 20–1.
Helmberg, G. and Gershon, S. (1961) Autonomic and psychic effects of yohimbine, Psychopharma-cologia, 2, 93–106.
Helmers, S.L., Wheless, J.W., Frost, M. et al. (2001) Vagus nerve stimulation therapy in pediatricpatients with refractory epilepsy: retrospective study, Journal of Child Neurology, 16, 843–8.
Helmstaedter, C. (2004) Behavioural and neuropsychological effects of frontal lobe epilepsy. InM.R. Trimble and B. Schmitz (eds.), The Neuropsychiatry of Epilepsy, Cambridge University Press,Cambridge, pp. 164–88.
Heninger, G.R., Charney, D.S. and Sternberg, D.E. (1984) Serotinergic function in depression,Archives of General Psychiatry, 41, 398–402.
Henquet, C., di Forti, M., Morrison, P. et al. (2008) Gene–environment interplay between cannabisand psychosis, Schizophrenia Bulletin, 34, 1111–21.
Henriksen, G.F. (1973) Status epilepticus partialis with fear as a clinical expression: report of a caseand ictal EEG findings, Epilepsia, 14, 39–46.

References 357
Henry, T.R. (2002) Therapeutic mechanisms of vagus nerve stimulation, Neurology, 59, S15–S20.Henry, J.A., Alexander, C.A. and Sener, E.K. (1995) Relative mortality from overdose of antide-
pressants, British Medical Journal, 310, 221–4.Henry, T.R., Bakay, R.A., Votaw, J.R. et al. (1998) Brain blood flow alterations induced by therapeutic
vagus nerve stimulation in partial epilepsy: I. acute effects at high and low levels of stimulation,Epilepsia, 39, 983–90.
Henry, T.R., Votaw, J.R., Pennell, P.B. et al. (1999) Acute blood flow changes and efficacy of vagusnerve stimulation in partial epilepsy, Neurology, 52, 1166–73.
Herbert, J. (1984) Behaviour and the limbic system with particular reference to sexual andaggressive interactions. In M.R. Trimble and E. Zarifian (eds.), Psychopharmacology of the LimbicSystem, Oxford University Press, Oxford, pp. 51–67.
Herbert, J.D., Hope, D.A. and Bellack, A.S. (1992) Validity of the distinction between generalizedsocial phobia and avoidant personality disorder, Journal of Abnormal Psychology, 101, 332–9.
Hermann, B.P. and Riel, P. (1981) Interictal personality and behavioural traits in temporal lobe andgeneralized epilepsy, Cortex, 17, 125–8.
Hermann, B.P. and Whitman, S. (1984) Behavioural and personality correlates of epilepsy: a review,methodological critique, and conceptual model, Psychological Bulletin, 95, 451–92.
Hermann, B.P., Dickmen, S., Swartz, M.S. et al. (1982) Interictal psychopathology in patients withictal fear: a quantitative investigation, Neurology, 32, 7–11.
Hermann, B.P., Seidenberg, M., Haltiner, A. et al. (1991) Mood state in unilateral temporal lobeepilepsy, Biological Psychiatry, 30, 1205–18.
Hermann, B.P., Wyler, A.R., Blumer, D. et al. (1992) Ictal fear, Neuropsychiatry, Neuropsychology,Behavioural Neurology, 5, 205–10.
Herpertz, S.C., Dietrich, T.M., Wenning, B. et al. (2001) Evidence of abnormal amygdala functioningin borderline personality disorder: a functional MRI study, Biological Psychiatry, 50, 292–8.
Herwig, U., Padberg, F., Unger, J. et al. (2001) Transcranial magnetic stimulation in therapy studies:examination of the reliability of ‘standard’ coil positioning by neuronavigation, BiologicalPsychiatry, 50(1), 58–61.
Hesdorffer, D.C., Hauser, W.A., Ludvigsson, P. et al. (2006) Depression and attempted suicide asrisk factors for incident unprovoked seizures and epilepsy, Annals of Neurology, 59, 35–41.
Heston, L.L. (1966) Psychiatric disorders in foster home reared children of schizophrenic mothers,British Journal of Psychiatry, 112, 819–25.
Heston, L.L., Mastri, A.R., Anderson, E. et al. (1981) Dementia of the Alzheimer type, Archives ofGeneral Psychiatry, 38, 1085–90.
Hewitt, J.K., Silberg, J.L., Rutter, M. et al. (1997) Genetics and developmental psychopathology: 1.phenotypic assessment in the virginia twin study of adolescent behavioral development, Journalof Child Psychology Psychiatry, 38, 943–63.
Higgins, E.S. and George, M.S. (2007) The Neuroscience of Clinical Psychiatry: The Pathophysiology ofBehavior and Mental Illness, Lippincott, Baltimore, MD.
Higley, J.D., Mehlman, P.T., Taub, D.M. et al. (1992) CSF monoamine and adrenal correlates ofaggression in free-ranging rhesus monkeys, Archives of General Psychiatry, 49, 436–41.
Hill, D. (1950) Psychiatry. In D. Hill and G. Parr (eds.), Electroencephalography, MacDonald, London,pp. 319–63.
Hill, D. (1952) EEG in episodic psychotic and psychopathic behaviour, Electroencephalography andClinical Neurophysiology, 4, 419–42.
Hillbom, E. (1960) After-effects of brain injuries, Acta Psychiatrica Neurologica Scandinavica, 35,Suppl. 142.
Hiller, W. and Fichter, M.M. (2004) High utilizers of medical care: a crucial subgroup amongsomatizing patients, Journal of Psychosomatic Research, 56, 437–43.

358 References
Hoehn-Saric, R. (1982) Neurotransmitters in anxiety, Archives of General Psychiatry, 39, 735–42.Hoffart, A., Thornes, K. and Hedley, L.M. (1995) DSM IIR Axis I and II disorders in agoraphobic
patients with and without panic disorder before and after psychosocial treatment, PsychiatryResearch, 56, 1–9.
Hoffman, R., Boutros, N., Berman, R. et al. (1998) Transcranial magnetic stimulation and halluci-nated ‘voices’, Biological Psychiatry, 43, 93–310.
Hoffman, R.E., Boutros, N.N., Hu, S. et al. (2000) Transcranial magnetic stimulation and auditoryhallucinations in schizophrenia, Lancet, 355, 1073–5.
Hokfelt, T., Johansson, O., Ljungdahl, A. et al. (1980) Peptidergic neurones, Nature, 284, 515–21.Hollander, D. and Strich, S.J. (1970) Atypical Alzheimer’s disease with congophilic angiopathy,
presenting with dementia of acute onset. In G.E.W. Wolstenholm and M. O’Connor (eds.),Alzheimer’s Disease and Related Conditions, Ciba Symposium, Churchill, London, pp. 105–24.
Hollister, L.E., Davis, K.L. and Berger, P.A. (1980) Subtypes of depression based on excretion ofMHPG and response to nortriptyline, Archives of General Psychiatry, 37, 1107–10.
Holsboer, F., Gerkoen, A., Stall, G.K. et al. (1985) ACTH, cortisol and coricosterone output afterovine corticotropin-releasing factor challenge during depression and after recovery, BiologicalPsychiatry, 20, 276–86.
Holtzheimer, P.E., Russo, J. and Avery, D. (2001) A meta-analysis of repetitive transcranial magneticstimulation in the treatment of depression, Psychopharmacology Bulletin, 35, 149–69.
Hommer, D., Momenan, R., Kaiser, E. et al. (2001) Evidence for a gender-related effect of alcoholismon brain volumes, American Journal of Psychiatry, 158, 198–204.
Howard, R.C., Fenton, G.W. and Fenwick, P.B.C. (1984) The CNV, personality and antisocialbehaviour, British Journal of Psychiatry, 144, 463–74.
Howes, O.D. and Kapur, S. (2009) The dopamine hypothesis of schizophrenia: Version III The finalcommon pathway, Schizophrenia Bulletin, 35, 549–62.
Howes, O.D., Montgomery, A.J., Asselin, M.C. et al. (2009) Elevated striatal dopamine functionlinked to prodromal signs of schizophrenia, Archives of General Psychiatry, 66, 13–20.
Hu, X.Z., Rush, A.J., Charney, D. et al. (2007) Association between a functional serotonin transporterpromoter polymorphism and citalopram treatment in adult outpatients with major depression,Archives of General Psychiatry, 64, 783–92.
Hughes, J.R. and Hermann, B.P. (1984) Evidence for psychopathology in patients with rhythmicmid-temporal discharges, Biological Psychiatry, 19, 1623–34.
Hunter, A.M., Leuchter, A.F., Morgan, M.L. et al. (2006) Changes in brain function (quantitativeEEG cordance) during placebo lead-in and treatment outcomes in clinical trials for majordepression, American Journal of Psychiatry, 163, 1426–32.
Hurwitz, T.A., Wada, J.A., Kosaka, B.D. et al. (1985) Cerebral localisation of affect suggested bytemporal lobe seizures, Neurology, 35, 1335–7.
Hutchings, B. and Mednick, S.A. (1975) Registered criminality in the adoptive and biologicalparents of registered male criminal adoptees. In R.R. Fieve, D. Rosenthal and H. Brill (eds.),Genetic Research in Psychiatry, Johns Hopkins Press, Baltimore, pp. 105–16.
Hyman, S.E. (2007) The neurobiology of addiction: implications for voluntary control of behavior,American Journal of Bioethics, 7, 8–11.
Hyman, S.E., Malenka, R.C. and Nestler, E.J. (2006) Neural mechanisms of addiction: the role ofreward-related learning and memory, Annual Review of Neuroscience, 29, 565–98.
ILAE (1985) Proposal for classification of the epilepsies and epileptic syndromes, Epilepsia, 26,268–78.
Imbesi, M., Yildiz, S., Dirim Arslan, A. et al. (2009) Dopamine receptor-mediated regulation ofneuronal ‘clock’ gene expression, Neuroscience, 158, 537–44.

References 359
Imlah, N.W. (1985) An evaluation of alprazolam in the treatment of reactive or neurotic depression,British Journal of Psychiatry, 14, 515–19.
Insel, T.T. (1992) Oxytocin, Psychoneuroendocrinology, 17, 1–35.Insel, T.R., Gillin, J.C., Moore, A. et al. (1982) The sleep of patients with obsessive–compulsive
disorder, Archives of General Psychiatry, 39, 1372–7.Ishizuka, K., Paek, M., Kamiya, A. et al. (2006) A review of disrupted-in-schizophrenia-1 (disc1):
neurodevelopment, cognition, and mental conditions, Biological Psychiatry, 59, 1189–97.Ito, Y., Teicher, M.H., Glod, C.A. et al. (1993) Increased prevalence of electroencephalographic
abnormalities in children with psychological, physical and sexual abuse, Journal of Neuropsychi-atry and Clinical Neuroscience, 5, 401–8.
Ito, Y., Teicher, M.H., Glod, C.A. et al. (1998) Preliminary evidence for aberrant cortical developmentin abused children: a quantitative EEG study, Journal of Neuropsychiatry and Clinical Neuroscience,10, 298–307.
Iversen, S. (1983) Where in the brain do benzodiazepines act? In M.R. Trimble (ed.), BenzodiazepinesDivided, John Wiley and Sons, Chichester, pp. 167–85.
Iversen, S.D. and Iversen, L. (1981) Substance P: a new CNS transmitter, Hospital Update, May,497–506.
Jacoby, R. and Levy, R. (1980a) Computed tomography in the elderly: II. Senile dementia, BritishJournal of Psychiatry, 136, 256–69.
Jacoby, R. and Levy, R. (1980b) Computed tomography in the elderly: III. Affective disorder, BritishJournal of Psychiatry, 136, 270–5.
Jacoby, A., Baker, G.A., Steen, N. et al. (1996) The clinical course of epilepsy and its psychosocialcorrelates: findings from a UK community study, Epilepsia, 37, 148–61.
Jalava, M. and Sillanpaa, M. (1996) Concurrent illnesses in adults with childhood-onset epilepsy:a population based 35 year follow-up study, Epilepsia, 37, 1155–63.
Jang, K.L., Paris, J., Zweig-Frank, H. et al. (1998) Twin study of dissociative experience, Journal ofNervous and Mental Disease, 186, 345–51.
Janota, I. (1981) Dementia, deep white matter damage and hypertension: Binswanger’s disease,Psychological Medicine, 11, 39–48.
Janowsky, D.S., Risch, S.C., Parker, D. et al. (1980) Increased vulnerability to cholinergic stimulationin affective disorder patients, Psychopharmacology Bulletin, 16, 29–31.
Janz, D. (2002) The psychiatry of idiopathic generalized epilepsy. In M.R. Trimble and B.Schmitz (eds.), The Neuropsychiatry of Epilepsy, Cambridge University Press, Cambridge,pp. 41–61.
Jaspers, K. (1963) General Psychopathology (Translated by J. Hoenig and M.W. Hamilton), ManchesterUniversity Press, Manchester.
Jennett, B. (1975) Epilepsy after Non-missile Head Injuries, Heinemann, London.Jennum, P. and Klitgaard, H. (1996) Effect of acute and chronic stimulations on pentylenetetrazole-
induced clonic seizures, Epilepsy Research, 23, 115–22.Jicha, G.A., Parisi, J.E., Dickson, D.W. et al. (2008) Age and apoE associations with complex
pathologic features in Alzheimer’s disease, Journal of Neurological Science, 273, 34–9.Jimerson, D.C., Insel, T.R., Reus, V.I. et al. (1983) Increased plasma MHPG in dexamethasone
resistant depressed patients, Archives of General Psychiatry, 40, 173–6.Jin, Y., Potkin, S.G., Kemp, A.S. et al. (2006) Therapeutic effects of individualized alpha fre-
quency transcranial magnetic stimulation (rTMS) on the negative symptoms of schizophrenia,Schizophrenia Bulletin, 32, 556–61.
Johannesson, G., Brun, A., Gustaffson, L. et al. (1977) EEG in presenile dementia related to cerebralblood flow and autopsy findings, Acta Neurologica Scandinavica, 56, 89–103.

360 References
Johansen-Berg, H., Gutman, D.A., Behrens, T.E. et al. (2008) Anatomical connectivity of the sub-genual cingulate region targeted with deep brain stimulation for treatment-resistant depression,Cereb Cortex, 18, 1374–83.
Johannsson, O. and Hokfelt, T. (1981) Nucleus accumbens; transmitter neurochemistry withspecial references to peptide-containing neurones. In R.B. Chronister and J.F. de France (eds.),The Neurobiology of the Nucleus Accumbens, Haer Institute, Brunswick, NJ, pp. 147–72.
Johnson, S., Summers, J. and Pridmore, S. (2006) Changes to somatosensory detection and painthresholds following high frequency repetitive TMS of the motor cortex in individuals sufferingfrom chronic pain, Pain, 123, 187–92.
Johnstone, E.C., Crow, T.J., Frith, C.D. et al. (1978) The dementia of dementia preacoc, ActaPsychiatrica Scandanavica, 57, 305–24.
Jokeit, H. and Ebner, A. (2004) The risk of cognitive decline in patients with refractory temporallobe epilepsy. In M.R. Trimble and B. Schmitz (eds.), The Neuropsychiatry of Epilepsy, CambridgeUniversity Press, Cambridge, pp. 152–163.
Jones, E.G. and Powell, T.P.S. (1970) An anatomical study of converging sensory pathways withinthe cerebral cortex of the monkey, Brain, 93, 793–820.
Jones, J.E., Hermann, B.P., Barry, J.J. et al. (2005) Clinical assessment of axis 1 psychiatric morbidityin chronic epilepsy: a multicentre investigation, Journal of Neuropsychiatry of Clinical Neurosciences,17, 172–9.
Jorge, R., Robinson, R., Arndt, S. et al. (1993) Comparison between acute and delayed-onsetdepression following traumatic brain injury, Journal of Neuropsychiatry and Clinical Neurosciences,5, 43–9.
Josephs, K.A., Ahlskog, J.E., Parisi, J.E. et al. (2009) Rapidly progressive neurodegenerative demen-tias, Archives of Neurology, 66, 201–7.
Judd, L.L., Risch, C., Parker, D.C. et al. (1982) Blunted prolactin response, Archives of GeneralPsychiatry, 39, 1413–16.
Judd, F.K., Norman T.R. and Burrows, G.D. (1986) Pharmacological treatment of panic disorder,International Clinical Psychopharmacology, 1, 3–16.
Juengling, F.D., Schmahl, C., Hesslinger, B. et al. (2003) Positron emission tomography in femalepatients with borderline personality disorder, Journal of Psychiatric Research, 37, 109–15.
Kaabi, B., Gelernter, J., Woods, S.W. et al. (2006) Genome scan for loci predisposing to anxietydisorders using a novel multivariate approach: strong evidence for a chromosome 4 risk locus,American Journal of Human Genetics, 78, 543–53.
Kalivas, P.W. and Volkow, N.D. (2005) The neural basis of addiction: a pathology of motivationand choice, American Journal of Psychiatry, 162, 1403–13.
Kallmann, F. (1946) The genetic theory of schizophrenia, American Journal of Psychiatry, 103, 309–22.Kallmann, F. (1954) Genetic principles in manic–depressive psychosis. In J. Zubin and P. Hoch
(eds.), Depression: Proceedings of the American Psychopathological Association, Grune and Stratton,New York, NY.
Kanemoto, K. (2002) Post-ictal psychoses revisited. In M.R. Trimble and B. Schmitz (eds.), TheNeuropsychiatry of Epilepsy, Cambridge University Press, Cambridge, pp. 117–34.
Kanner, A.M. (2006) Depression and epilepsy: a new perspective on two closely related disorders,Epilepsy Currents, 6, 141–6.
Kanner, A.M., Kozac, A.M. and Frey, M. (2000) The use of sertraline in patients with epilepsy: is itsafe?, Epilepsy Behavior, 1, 100–5.
Kanner, A.M., Soto, A. and Gross-Kanner, H. (2004) Prevalence and clinical characteristics ofpostictal psychiatric symptoms in partial epilepsy, Neurology, 62, 708–13.
Karis, D., Fabini, M. and Donchin, E. (1984) P300 and memory, Cognitive Psychology, 16, 177–216.

References 361
Karlsgodt, K.H., Sanz, J., van Erp, T.G. et al. (2009) Re-evaluating dorsolateral prefrontal cortexactivation during working memory in schizophrenia, Schizophrenia Research, 108, 143–50.
Karlsson, P., Farde, L., Halldin, C. et al. (2002) PET study of D(1) dopamine receptor bind-ing in neuroleptic-naive patients with schizophrenia, American Journal of Psychiatry, 159,761–7.
Karlsson, P., Smith, L., Farde, L. et al. (1995) Lack of apparent antipsychotic effect of the D1-dopamine receptor antagonist Sch39166 in acutely ill schizophrenic patients, Psychopharmacology(Berl), 121, 309–16.
Kathol, R.G., Noyes, R., Slyman, D.J. et al. (1980) Propranolol in chronic anxiety disorders, Archivesof General Psychiatry, 37, 1361–5.
Kathol, R.G., Noyes, R., Slyman, D.J. et al. (1981) Propranolol in chronic anxiety disorders. In D.F.Klein and J. Rabkin (eds.), Anxiety, New Research and Changing Concepts, Raven Press, New York,NY, pp. 81–93.
Kato, T., Takahashi, S., Shioiri, T. et al. (1993) Alterations in brain phosphorous metabolismin bipolar disorder detected by in vivo 31P and 7LI MRS, Journal of Affective Disorders, 27,53–60.
Katona, C.L.E., Hale, A.S., Theodorus, S.L. et al. (1985) Which depressives have blunted growthhormone responses to clonadine? Abstracts, Autumn Quarterly Meeting of the Royal College ofPsychiatrists, 6–7.
Kaufman, R.E., Ostacher, M.J., Marks, E.H. et al. (2009) Brain GABA levels in patients with bipolardisorder, Progress in Neuro-psychopharmacology and Biological Psychiatry, 33, 427–34.
Kay, D.W.K., Foster, E.M., McKenchnie, A.A. et al. (1970) Mental illness and hospital use in theelderly: a random sample followed up, Comprehensive Psychiatry, 11, 26–35.
Keele, N.B. (2005) The role of serotonin in impulsive and aggressive behaviors associated withepilepsy-like neuronal hyperexcitability in the amygdala, Epilepsy and Behavior, 7, 325–35.
Keitner, G.I., Brown, W.A., Qualls, C.B. et al. (1985) Results of DST in psychiatric patients with andwithout weight loss, American Journal of Psychiatry, 142, 246–8.
Keller, J., Shen, L., Gomez, R.G. et al. (2008) Hippocampal and amygdalar volumes in psychoticand nonpsychotic unipolar depression, American Journal of Psychiatry, 165, 872–80.
Kellner, C.H., Jolley, R.R., Holgate, R.C. et al. (1991) Brain MRI in obsessive–compulsive disorder,Psychiatric Research, 36, 45–9.
Kendler, K.S. (1983) Overview: a current perspective on twin studies of schizophrenia, AmericanJournal of Psychiatry, 140, 1413–25.
Kendler, K.S. and Robinette, C.D. (1983) Schizophrenia in the National Academy of Sciences,American Journal of Psychiatry, 140, 1557–63.
Kendler, K.S., Gruenberg, A.M. and Strauss, T.S. (1981) An independent analysis of the Danishadoption study of schizophrenia, Archives of General Psychiatry, 38, 973–87.
Kendrick, J.F. and Gibbs, F.A. (1957) Origin, spread and neurosurgical treatment of the psychomotortype of seizure discharge, Journal of Neurosurgery, 14, 270–84.
Kepe V., Huang, S.C., Small, G.W. et al. (2006) Visualizing pathology deposits in the living brain ofpatients with Alzheimer’s disease, Methods Enzymology, 412, 144–60.
Keshavan, M.S., Prasad, K.M. and Pearlson, G. (2007) Are brain structural abnormalities useful asendophenotypes in schizophrenia?, International Review of Psychiatry, 19, 397–406.
Kessler, R.C. and Walters, E.E. (1998) Epidemiology of DSM III-R major depression and minordepression among adolescents and young adults in the national comorbidity survey, Depressionand Anxiety, 7, 3–14.
Kessler, S.R., Garrett, A., Bender, B. et al. (2004) Amygdala and hippocampal volumes in Turner’ssyndrome: a high resolution MRI study of X-monosomy, Neuropsychologia, 42, 1971–8.

362 References
Kessler, R.M., Woodward, N.D., Riccardi, P. et al. (2009) Dopamine D2 receptor levels in striatum,thalamus, substantia nigra, limbic regions, and cortex in schizophrenic subjects, BiologicalPsychiatry, 65(12), 1024–31.
Ketter, T.A., George, M.S., Ring, H.A. et al. (1994) Primary mood disorders: structural and restingfunctional studies, Psychiatric Annals, 24, 637–42.
Kety, S.S. (1983) Mental illness in the biological and adoptive relations of schizophrenic adoptees,American Journal of Psychiatry, 140, 720–7.
Kety, S.S. and Schmidt, C.F. (1948) The nitrous oxide method for the quantitative determination ofcerebral blood flow in man: theory procedure and normal values, Journal of Clinical Investigation,27, 476–83.
Kety, S.S., Wender, P.H., Jacobsen, B. et al. (1994) Mental illness in the biological and adoptiverelatives of schizophrenic adoptees, Archives of General Psychiatry, 51, 442–55.
Kiehl, K.A., Hare, R.D., Liddle, P.F. et al. (1999) Reduced P330 responses in criminal psychopathsduring a visual oddball task, Biological Psychiatry, 45, 1498–1507.
Kiehl, K.A., Smith, A.M., Hare, R.D. et al. (2000) An event-related potential investigation of responseinhibition in schizophrenia and psychopathy, Biological Psychiatry, 48, 210–21.
Kilpatrick, C., Burns, R. and Blumbergs, P.C. (1983) Identical twins with Alzheimer’s disease,Journal of Neurology, Neurosurgery and Psychiatry, 46, 421–5.
Kilts, C.D. (1994) Recent pharmacologic advances in antidepressant therapy, American Journal ofMedicine, 97 (Suppl. 6A), S3–S12.
Kim, B., Choi, E.Y., Kim, C.Y. et al. (2008) Could HTR2a T102c and DRD3 SER9gly predict clinicalimprovement in patients with acutely exacerbated schizophrenia? Results from treatmentresponses to risperidone in a naturalistic setting, Hum Psychopharmacol, 23, 61–7.
King, J.R. and Hullin, R.P. (1983) Withdrawal symptoms from lithium, British Journal of Psychiatry,143, 30–5.
Kirov, G., Rujescu, D., Ingason, A. et al. (2009) Neurexin 1 (NRXN1) deletions in schizophrenia,Schizophrenia Bulletin , 35, 851–4.
Kishi, T., Kitajima, T., Ikeda, M. et al. (2009) Association study of clock gene (clock) and schizophre-nia and mood disorders in the Japanese population, European Archives of Psychiatry and ClinicalNeuroscience, 259(5), 293–7.
Kline, N.S., Li, C.H., Lehmann, H.E. et al. (1977) Beta endorphin induced changes in schizophrenicand depressed patients, Archives of General Psychiatry, 34, 1111–14.
Kling, A., Orbach, J., Schwartz, N.B. et al. (1960) Injury to limbic system and associated structuresin cats, Archives of General Psychiatry, 3, 391–420.
Kluver, H. and Bucy, P.C. (1939) Preliminary analysis of functions of the temporal lobes in monkeys,Archives of Neurology, 42, 979–1000.
Ko, G.N., Elsworth, J.D., Roth, R.H. et al. (1983) Panic induced elevation of plasma MHPG levels inphobic anxious patients, Archives of General Psychiatry, 40, 425–30.
Koenigs, M. and Grafman, J. (2009) Posttraumatic stress disorder: the role of medial prefrontalcortex and amygdala, Neuroscientist, 15(5), 540–8.
Koenigs, M., Huey, E.D., Raymont, V. et al. (2008) Focal brain damage protects against post-traumatic stress disorder in combat veterans. Nature Neuroscience, 11, 232–7.
Kolakowska, T., Orr, M., Gelder, M. et al. (1979) Clinical significance of plasma drug and prolactinlevels during acute chlorpromazine treatment: a replication study, Psychological Medicine, 135,352–9.
Kolakowska, T., Williams, A.O., Jambor, K. et al. (1985) Schizophrenia with good and poor outcome,British Journal of Psychiatry, 146, 348–57.
Kolbinger, H.M., Hoflich, G., Hufnagel, A. et al. (1995) Transcranial magnetic stimulation (TMS) inthe treatment of major depression: a pilot study, Human Psychopharmacology, 10, 305–10.

References 363
Kopecek, M., Sos, P., Brunovsky, M. et al. (2007) Can prefrontal theta cordance differentiate betweendepression recovery and dissimulation?, Neuroendocrinology Letters, 28, 524–6.
Kopelman, M.D. (1985) Multiple memory deficits in Alzheimer-type dementia, PsychologicalMedicine, 15, 527–41.
Korb, A.S., Cook, I.A., Hunter, A.M. et al. (2008) Brain electrical source differences betweendepressed subjects and healthy controls, Brain Topogr, 138–46.
Korf, E.S., Wahlund, L.O., Visser, P.J. et al. (2004) Medial temporal lobe atrophy on MRI predictsdementia in patients with mild cognitive impairment, Neurology, 63, 94–100.
Kotler, M., Cohen, H., Segman, R. (1997) Excessive dopamine D4 receptor (DRD4) exon 111 sevenrepeat allele in opiod dependent subjects, Molecular Psychiatry, 2, 251–4.
Kovelman, J.A. and Scheibel, A.B. (1984) A neurohistological correlate of schizophrenia, BiologicalPsychiatry, 19, 1601–22.
Kozel, F.A. and George, M.S. (2002) Meta-analysis of left prefrontal repetitive transcranial magneticstimulation (rTMS) to treat depression, Journal of Psychiatric Practice, 8, 270–5.
Kozel, F.A., Johnson, K.A., Mu, Q. et al. (2005) Detecting deception using functional magneticresonance imaging, Biological Psychiatry, 58, 605–13.
Kozel, F.A., Nahas, Z., Debrux, C. et al. (2000) How the distance from coil to cortex relates to age,motor threshold and possibly the antidepressant response to repetitive transcranial magneticstimulation, Journal of Neuropsychiatry And Clinical Neurosciences, 12, 376–84.
Kraepelin, E. (1904) Lectures on Clinical Psychiatry, William Wood, New York, NY.Kraepelin E (1923) Psychiatrie: Band 3, Johann Ambrosius Barth, Leipzig.Krauthammer, C. and Klerman, G.L. (1978) Secondary mania, Archives of General Psychiatry, 35,
1333–9.Kringlen, E. (1965) Obsessional neurotics, British Journal of Psychiatry, 111, 709–22.Krishnamoorthy, E.S., Trimble, M.R. and Blumer, D. (2007) The classification of neuropsychiatric
disorders in epilepsy: a proposal by the ILAE Commission on Psychobiology of Epilepsy,Epilepsy Behavior, 10, 349–53.
Krishnan, K.R.R., McDonald, W.M., Escalona, P.R. et al. (1992) MRI of the caudate nuclei indepression, Archives of General Psychiatry, 49, 553–7.
Kristensen, O. and Sindrup, E.H. (1978) Psychomotor epilepsy and psychosis, Acta NeurologicaScandinavica, 57, 361–70.
Krystal, J.H., Seibyl, J.P., Price, L.H. et al. (1993) M-CPP effects in neuroleptic free schizophrenics,Archives of General Psychiatry, 50, 624–35.
Kugaya, A. and Sanacora, G. (2005) Beyond monoamines: glutamatergic function in mood disor-ders, CNS Spectrums, 10, 808–19.
Lader, M.H. (1969) Psychophysiological aspects of anxiety. In M.H. Lader (ed.), Studies of Anxiety,Headley Bros., Kent, pp. 53–61.
Lake, C.R., Pickar, D., Ziegler, M.G. et al. (1982) High plasma norepinephrine levels in patientswith major affective disorders, American Journal of Psychiatry, 139, 1315–16.
Lammertsma, A.A., Jones, T., Frackowiak, R.S.J. et al. (1981) A theoretical study of the steady-statemodel for measuring rCBF and oxygen utilisation using oxygen-15, Journal of Computer AssistedTomography, 5, 544–50.
Landis, S. and Insel, T.R. (2008) The ‘neuro’ in neurogenetics, Science, 322, 821.Landolt, H. (1958) Serial electroencephalographic investigations during psychotic episodes in
epileptic patients and during schizophrenic attacks. In Lorenz de Haas (ed.), Lectures on Epilepsy,Elsevier, London, pp. 91–133.
Lange, J. (1929) Verbrechen als Schicksal, Thomas, Leipzig.Lapierre, D., Braun, C.M. and Hodgkins, S. (1995) Ventral frontal deficits on psychopathy:
neuropsychological test findings, Neuropsychologia, 33, 139–51.

364 References
Laplane, D., Levasseur, M., Pillon, B., Dubois, B. et al. (1989) Obsessive–compulsive and otherbehavioural changes with bilateral basal ganglia lesions, Brain, 112, 699–725.
Lauterbur, P.C. (1973) Image formation by induced local interactions: examples employing NMR,Nature, 242, 190–1.
Lawrence, K.M., De Paermentier, F., Cheetham, S.C. et al. (1990) Brain 5-HT uptake sites labelledwith 3H-paroxetine in antidepressant-free depressed suicides, Brain Research, 526, 17–22.
Lawrie, S.M., Hall, J., McIntosh, A.M. et al. (2008a) Neuroimaging and molecular genetics ofschizophrenia: pathophysiological advances and therapeutic potential, British Journal of Pharma-cology, 153, Suppl. 1, S120–4.
Lawrie, S.M., McIntosh, A.M., Hall, J. et al. (2008b) Brain structure and function changes during thedevelopment of schizophrenia: the evidence from studies of subjects at increased genetic risk,Schizophrenia Bulletin, 34, 330–40.
Lazare, A., Klerman, G.L. and Armor, D.J. (1970) Oral, obsessive and hysterical personality patterns,Journal of Psychiatric Research, 7, 275–90.
Leckman, J.F., Gershon. E.S., Nichols, A.S. et al. (1977) Reduced MAO activity in first degreerelatives of individuals with bipolar affective disorders, Archives of General Psychiatry, 34, 601–8.
Leckman, J.F., Goodman, W.K., North, W.G. et al. (1994) Elevated CSF oxytocin inobsessive–compulsive disorder, Archives of General Psychiatry, 51, 782–92.
LeDoux, J.E. (1992) Emotion and the amygdala. In Aggleton, J.P. (ed.) The Amygdala, Wiley Liss,New York, NY, pp. 339–51.
LeDoux, J.E., Iwata, J., Cicchetti, P. et al. (1988) Differential projections of the central amyg-daloid nucleus mediate autonomic and behavioural correlates of conditioned fear, Journal ofNeuroscience, 8, 2517–29.
Lee, H.Y., Kim, D.J., Lee, H.J. et al. (2009) No association of serotonin transporter polymorphism (5-HTTVNTR and 5-HTTLPR) with characteristics and treatment response to atypical antipsychoticagents in schizophrenic patients, Progress in Neuro-psychopharmacol Biological Psychiatry, 33,276–80.
Lefaucheur, J.P. (2004) Transcranial magnetic stimulation in the management of pain, Supplementsto Clinical Neurophysiology, 57, 737–48.
Lefaucheur, J.P., Drouot, X. and Nguyen, J.P. (2001) Interventional neurophysiology for paincontrol: duration of pain relief following repetitive transcranial magnetic stimulation of themotor cortex, Neurophysiologie Clinique, 31, 247–52.
Leonard, B.E. (1992) Fundamentals of Psychopharmacology, John Wiley and Sons, Chichester.Leonard, H.L., Swedo, S.E., Lenane, M.C. et al. (1993) A 2–7 year follow up study of 54
obsessive–compulsive children and adolescents, Archives of General Psychiatry, 50, 429–39.Leonhard, K. (1957) Aufteilung der Endogenen Psychosen, Akademie Verlag, Berlin.Leonhard, K. (1980) Contradictory issues in the origin of schizophrenia, British Journal of Psychiatry,
136, 437–44.Lenze, E., Cross, D., McKeel, D. et al. (1999) White matter hyperintensities and gray matter lesions
in physically healthy depressed subjects, American Journal of Psychiatry, 156(10), 1602–7.Lesch, E.P., Hoh, A., Disselkamp-Tietze, J. et al. (1991) 5-HT1a receptor responsivity in obsessive–
compulsive disorder, Archives of General Psychiatry, 48, 540–7.Leweke, F.M., Giuffrida, A., Koethe, D. et al. (2007) Anandamide levels in cerebrospinal fluid of
first-episode schizophrenic patients: impact of cannabis use, Schizophrenia Research, 94, 29–36.Lewis, A. (1934) Melancholia: a clinical survey of depressive states, Journal of Mental Science, 80,
277–378.Lewis, A. (1970) Paranoia and paranoid: a historical perspective, Psychological Medicine, 1, 2–12.Lewis, A. (1971) ‘Endogenous’ and ‘exogeneous’: a useful dichotomy, Psychological Medicine, 1,
191–6.

References 365
Lewis, D.A. and McChesney, C. (1985) Tritiated imipramine binding distinguishes among subtypesof depression, Archives of General Psychiatry, 42, 485–8.
Lewis, D.A., Campbell, M.J., Foote, S.L. et al. (1986) The dopaminergic innervation of primate neo-cortex is widespread, yet regionally specific, Society of Biological Psychiatry Abstracts, Washington,DC, May, p. 1.
Leysen, J. and Niemegeers, C.J.E. (1985) Neuroleptics. In A. Lagtha (ed.), Handbook of Neurochemistry,Vol. 9, Plenum, New York, NY, pp. 331–61.
Li, D. and He, L. (2007) Meta-analysis supports association between serotonin transporter (5-HTT)and suicidal behavior, Molecular Psychiatry, 12, 47–54.
Li, X., Teneback, C.C., Nahas, Z. et al. (2002) Lamotrigine inhibits the functional magnetic resonanceimaging response to transcranial magnetic stimulation in healthy adults, Biological Psychiatry,51.
Lichtenstein, P., Yip, B.H., Bjork, C. et al. (2009) Common genetic determinants of schizophreniaand bipolar disorder in Swedish families: a population-based study, Lancet, 373, 234–9.
Lidberg, L., Tuck, J.R., Asberg, M. et al. (1985) Homicide, suicide and CSF 5-HIAA, Acta PsychiatricaScandinavica, 71, 230–6.
Lieberman, J.A., Kane, J.M., Sarantakos, S. et al. (1985) Dexamethasone suppression tests in patientswith obsessive–compulsive disorder, American Journal of Psychiatry, 142, 747–51.
Lim, M.M., Wang, Z., Olazabel, D.E. et al. (2004) Enhanced partner preference in a promiscuousspecies by manipulating the expression of a single gene, Nature, 429, 754–7.
Lin, P.I. and Mitchell, B.D. (2008) Approaches for unraveling the joint genetic determinants ofschizophrenia and bipolar disorder, Schizophrenia Bulletin, 34, 791–7.
Linnoila, M. and Martin, P.R. (1983) Benzodiazepines and alcoholism. In M.R. Trimble (ed.),Benzodiazepines Divided, John Wiley and Sons, Chichester, pp. 291–306.
Linnoila, M., Karoum, F., Rosenthal, N. et al. (1983a) ECT and lithium carbonate, Archives of GeneralPsychiatry, 40, 677–80.
Linnoila, M., Virkkunen, M., Scheinin, M. et al. (1983b) Low CSF 5-HIAA concentration differenti-ates impulsive from non-impulsive violent behaviour, Life Science, 33, 2609–14.
Lipsey, J.K., Robinson, R.G., Pearlson, G.D. et al. (1985) The DST and mood following stroke,American Journal of Psychiatry, 142, 318–22.
Lishman, A. (1987) Organic Psychiatry, 2nd edition, Blackwell, Oxford.Livesley, W.J. and Jang, K.L. (2008) The behavioral genetics of personality disorder, Annual Review
of Clinical Psychology, 4, 247–74.Lloyd, K.G., Parley, I.J., Deck, J.H.N. et al. (1974) Serotonin and 5-HIAA in discrete areas of the
brainstem of suicide victims and control patients, Advances in Biochemical Psychopharmacology,11, 387–97.
Lodge, D.J., Behrens, M.M. and Grace, A.A. (2009) A loss of parvalbumin-containing interneuronsis associated with diminished oscillatory activity in an animal model of schizophrenia, TheJournal of Neuroscience, 29, 2344–54.
Logsdail, S.J. and Toone, B.K. (1988) Post-ictal psychoses: a clinical and phenomenological descrip-tion, British Journal of Psychiatry, 152, 246–52.
Lomarev, M., Denslow, S., Nahas, Z. et al. (2002) Vagus nerve stimulation (VNS) synchronizedbold fMRI suggests that VNS in depressed adults has frequency/dose dependent effects, Journalof Psychiatric Research, 36, 219–27.
Lucey, J.V., Butcher, G., Clare, A.W. et al. (1993) Elevated growth hormone responses topyridostigmine in obsessive–compulsive disorder, American Journal of Psychiatry, 150,961–2.
Luxenberg, J.S., Swedo, S.E., Flament, M.F. et al. (1988) Neuroanatomical abnormalities in OCDwith quantitative X-ray CT, American Journal of Psychiatry, 145, 1089–93.

366 References
Maas, J.W., Fawcett, J.A. and Dekirmenjian, H. (1972) Catecholamine metabolism, depressiveillness and drug response, Archives of General Psychiatry, 26, 252–62.
Macciardi, F., Petronis, A., van Tol, H. et al. (1994) Analysis of the D4 dopamine receptor genevariant in an Italian schizophrenic kindred, Archives of General Psychiatry, 51, 288–93.
MacDonald, R.T. (1982) Drug treatment of senile dementia. In D. Wheatley (ed.), Psychopathology ofOld Age, Oxford University Press, Oxford, pp. 113–37.
Mackay, A. (1979) Self poisoning: a complication of epilepsy, British Journal of Psychiatry, 134,277–82.
MacLean, P.D. (1990) The Triune Brain in Evolution: Role in Paleocerebral Functions, Plenum Press,New York, NY.
MacLean, P.D. and Ploog, D.W. (1962) Cerebral representation of penile erection, Journal ofNeurophysiology, 25, 29–55.
Mahendra, B. (1984) Dementia, MTP Press, Lancaster.Maher, B.S., Riley, B.P. and Kendler, K.S. (2008) Psychiatric genetics gets a boost, Nature Genetics,
40, 1042–4.Maheu, F.S., Mazzone, L., Merke, D.P. et al. (2008) Altered amygdala and hippocampus function in
adolescents with hypercortisolemia: a functional magnetic resonance imaging study of cushingsyndrome, Development And Psychopathology, 20, 1177–89.
Maier, M., Mellers, J. and Toone, B. (2000) Schizophrenia, temporal lobe epilepsy and psychosis,Psychological Medicine, 30, 571–80.
Maletsky, B.M. (1978) Seizure duration and clinical effect in ECT, Comprehensive Psychiatry, 19,541–50.
Malitz, S. and Sackeim, H.A. (eds.), (1986) ECT, Annals of the New York Academy of Sciences,p. 462.
Malonek, D. and Grinvald, A. (1996) Interactions between electrical activity and cortical microcir-culation revealed by imaging spectroscopy: implications for functional brain mapping, Science,272, 551–4.
Mamounas, L.A., Blue, M.E., Siuciak, J.A. et al. (1995) Brain derived neurotrophic factor promotesthe survival and sprouting of serotonergic axons in rat brain, Journal of Neuroscience, 15(2),7929–39.
Mann, J. (1979) Altered platelet MAO activity in affective disorders, Psychological Medicine, 9,729–36.
Mann, J.J. and Malone, K.M. (1997) Cerebrospinal fluid amines and higher-lethality suicideattempts in depressed in-patients, Biological Psychiatry, 41, 162–71.
Mann, D.M.A., Lincoln, J., Yates, P.O. et al. (1980) Changes in monoamine containing neurones ofthe human CNS in senile dementia, British Journal of Psychiatry, 136, 533–41.
Mann, J.J., Stanley, M., McBride, A. et al. (1986) Increased serotonin-2 and beta adrenergic receptorbinding in the frontal cortices of suicidal victims, Archives of General Psychiatry, 43, 954–9.
Mann, J.J., McBride, A., Anderson, G.M. et al. (1992) Platelet and whole blood serotonin content indepressed inpatients, Biological Psychiatry, 23, 243–57.
Mann, K., Agartz, I., Harper, C. et al. (2001) Neuroimaging in alcoholism: ethanol and braindamage, Alcoholism: Clinical and Experimental Research, 25, S104–9.
Manschreck, T.C. and Ames, D. (1984) Neurological features and psychopathology in schizophrenicdisorders, Biological Psychiatry, 19, 703–19.
Mantovani, A., Lisanby, S.H., Pieraccini, F. et al. (2006) Repetitive transcranial magnetic stimulation(rTMS) in the treatment of obsessive–compulsive disorder (OCD) and Tourette’s syndrome (TS),International Journal of Neuropsychopharmacology, 9, 95–100.
Marangell, L.B., George, M.S., Callahan, A.M. et al. (1997) Effects of intrathecal thyrotropin-releasinghormone (protirelin) in refractory depressed patients, Archives of General Psychiatry, 54, 214–22.

References 367
Marsden, C.D. and Harrison, M.J.G. (1972) Outcome of investigation of patients with preseniledementia, British Medical Journal, ii, 249–52.
Martin, J.L.R., Barbanoj, M.J., Schlaepfer, T.E. et al. (2002) Transcranial magnetic stimulation fortreating depression (Cochrane Review), The Cochrane Library, Oxford, Update Software.
Masters, C.L., Harris, J.O., Gajdusek, D.C. et al. (1979) Creutzfeldt–Jakob disease: patterns ofworldwide occurrence and significance of familial and sporadic clustering, Annals of Neurology,5, 177–88.
Mathers, C.D. and Loncar, D. (2006) Projections of global mortality and burden of disease from2002 to 2030, Plos Medicine, 3, E442.
Mathew, R.J., Ho, B.T., Kralik, P. et al. (1980a) COMT and catecholamines in anxiety and relaxation,Psychiatry Research, 3, 85–91.
Mathew, R.J., Meyer, J.S., Semchuk, K.M. et al. (1980b) CBF in depression, Lancet, i, 1308.Mathew, R.J., Ho, B.T., Khan, M.M. et al. (1982) True and pseudocholinesterases in depression,
American Journal of Psychiatry, 139, 125–7.Mathew, S.J., Manji, H.K. and Charney, D.S. (2008) Novel drugs and therapeutic targets for
severe mood disorders, Neuropsychopharmacology: Official Publication of the American College ofNeuropsychopharmacology, 33, 2080–92.
Matsuzaki, S. and Tohyama, M. (2007) Molecular mechanism of schizophrenia with reference todisrupted-in-schizophrenia 1 (Disc1), Neurochemistry International, 51, 165–72.
Mayberg, H.S. (1994) Functional imaging studies in secondary depression, Psychiatric Annals, 24,643–7.
Mayberg, H.S., Robinson, R.G., Wong, D.F. et al. (1988) PET imaging of cortical S2 serotoninreceptors after stroke: lateralized changes and relationship to depression, American Journal ofPsychiatry, 145(8), 937–43.
Mayberg, H.S., Brannan, S.K., Mahurin, R.K. et al. (1997) Cingulate function in depression: apotential predictor of treatment response, Neuroreport, 8, 1057–61.
Mayberg, H.S., Liotti, M., Brannan, S.K. et al. (1999) Reciprocal limbic–cortical function andnegative mood: converging PET findings in depression and normal sadness, American Journal ofPsychiatry, 156(5), 675–82.
Mayberg, H.S., Lozano, A.M., Voon, V. et al. (2005) Deep brain stimulation for treatment-resistantdepression, Neuron, 45, 651–60.
Mayeux, R., Stern, Y., Cote, L. et al. (1984) Altered serotonin metabolism in depressed patients withParkinson’s disease, Neurology, 34, 642–6.
Mazzola-Pomietto, P., Azorin, J.-M., Tranoni, V. et al. (1994) Relation between lymphocyteβ-adrenergic responsivity and the severity of depressive disorders, Biological Psychiatry, 35,920–6.
McBride, P.A., Brown, R.P., de Meo, M., Keilp, J. et al. (1994) Relationship of platelet 5-HT2receptor indices to major depressive disorder, personality traits and suicidal behaviour, BiologicalPsychiatry, 35, 295–308.
McClung, C.A. (2007a) Clock genes and bipolar disorder: implications for therapy, Pharmacoge-nomics, 8, 1097–100.
McClung, C.A. (2007b) Role for the clock gene in bipolar disorder, Cold Spring Harbor Symposia onQuantitative Biology, 72, 637–44.
McClung, C.A. and Nestler, E.J. (2003) Regulation of gene expression and cocaine reward by creband deltafosb, Nature Neuroscience, 6, 1208–15.
McConnell, K.A., Nahas, Z., Shastri, A. et al. (2001) The transcranial magnetic stimulation motorthreshold depends on the distance from coil to underlying cortex: a replication in healthyadults comparing two methods of assessing the distance to cortex, Biological Psychiatry, 49(5),454–9.

368 References
McCreadie, R.G., Dingwall, J.M., Wiles, D.H. et al. (1980) Intermittent pimozide versusfluphenazine as maintenance therapy in chronic schizophrenia, British Journal of Psychiatry, 137,510–17.
McDonald, C. (1969) Clinical heterogeneity in senile dementia, British Journal of Psychiatry, 115,267–71.
McGowan, P.O., Meaney, M.J. and Szyf, M. (2008) Diet and the epigenetic (re)programming ofphenotypic differences in behavior, Brain Research, 1237, 12–24.
McGrath, J., El-Saadi, O., Grim, V. et al. (2002) Minor physical anomalies and quantitative measuresof the head and face in patients with psychosis, Archives of General Psychiatry, 59, 458–64.
McGuffin, P. (1984) Genetic influences on personality, neurosis and psychosis. In P. McGuffin, M.F.Shanks and R.J. Hodgson (eds.), The Scientific Principles of Psychopathology, Grune and Stratton,London, pp. 191–228.
McGuffin, P., Farmer, A.E. and Yonance, A.H. (1981) HLA antigens and subtypes of schizophrenia,Psychiatry Research, 5, 115–22.
McGuffin, P., Farmer, A.E., Gottesman, I.I. et al. (1984) Twin concordance for operationally definedschizophrenia, Archives of General Psychiatry, 41, 541–5.
McGuire, P.K., Bench, C.J., Frith, C.D. et al. (1994) Functional anatomy of obsessive–compulsive phenomena, British Journal of Psychiatry, 164, 459–68.
McKeon, J., McGuffin, P. and Robinson, P. (1984) Obsessive–compulsive neurosis following headinjury: a report of four cases, British Journal of Psychiatry, 144, 190–2.
McNamara, B., Ray, J.L., Arthurs, O.J. et al. (2001) Transcranial magnetic stimulation for depressionand other psychiatric disorders, Psychological Medicine, 31, 1141–6.
Meador-Woodruff, J.H., Grunhaus, L., Haskett, R.F. et al. (1986) Post-dexamethasone cortisol levelsin major depressive disorder, Society of Biological Psychiatry Abstracts, 177, Washington, DC, 7–11May.
Meana, J.J., Barturen, F. and Garcia-Sevilla, J.A. (1992) α2-adrenoceptors in the brain of suicidevictims, Biological Psychiatry, 31, 471–90.
Mehlman, P.T., Higley, J.D., Faucher, I. et al. (1994) Low CSF 5-HIAA concentrations and severeaggression and impaired impulse control in non-human primates, American Journal of Psychiatry,151, 1485–91.
Meldrum, B.S. (1976) Neuropathology and pathophysiology. In J. Laidlaw and A. Richens (eds.),A Textbook of Epilepsy, Churchill Livingstone, Edinburgh, pp. 314–54.
Meltzer, H.Y. and Fang, V.S. (1983) Cortisol determination and the DST, Archives of GeneralPsychiatry, 40, 501–5.
Meltzer, H.Y. and Maes, M. (1994) Effects of buspirone on plasma prolactin and cortisol levels inmajor depressed and normal subjects, Biological Psychiatry, 35, 316–23.
Meltzer, H.Y., Ross-Stanton, J. and Schlessinger, S. (1980) Mean serum creatine kinase activity inpatients with functional psychoses, Archives of General Psychiatry, 37, 650–5.
Meltzer, H.Y., Arora, R.C., Baber, R. et al. (1981) Serotonin uptake in blood platelets of psychiatricpatients, Archives of General Psychiatry, 38, 1322–6.
Meltzer, H.Y., Kolakowska, T., Fang, V.S. et al. (1984) Growth hormone and prolactin response toapomorphine in schizophrenia and the major affective disorder, Archives of General Psychiatry,41, 512–19.
Mendez, M.F. and Shapira, J.S. (2008) The spectrum of recurrent thoughts and behaviors infrontotemporal dementia, CNS Spectrums, 13, 202–8.
Mendez, M.F. and Shapira, J.S. (2009) Altered emotional morality in frontotemporal dementia,Cognitive Neuropsychiatry, 14, 165–79.
Mendez, M.F., Cummings, J.L. and Benson, D.F. (1986) Depression in epilepsy: significance andphenomenology, Archives of Neurology, 43, 766–70.

References 369
Mendez, M.F., Doss, R.C., Taylor, J.L. et al. (1993) Relationship of seizure variables to personalitydisorders in epilepsy, Journal of Neuropsychiatry Clinical Neuroscience, 5, 283–6.
Mendlewicz, J. and Rainer, J.D. (1977) Adoption-studies supporting genetic transmission in manicdepressive illness, Nature, 268, 327–9.
Mendlewicz, J. and Youdim, M.B.H. (1983) L-deprenil: a selective MAOB inhibitor, in the treatmentof depression: a double-blind evaluation, British Journal of Psychiatry, 142, 508–11.
Mendlewicz, J., Linkowski, P. and Wilmotte, J. (1980) Linkage between glucose-6-phosphatedehydrogenase deficiency and manic depressive psychosis, British Journal of Psychiatry, 137,337–42.
Mendlewicz, J., Charles, G. and Franckson, J.M. (1982) The dexamethasone suppression test inaffective disorders: relationship to clinical and genetic subgroups, British Journal of Psychiatry,141, 464–70.
Mendlewicz, J., Kerkhofs, M., Hoffman, G. et al. (1984) DST and REM sleep in patients with majordepressive disorder, British Journal of Psychiatry, 145, 383–8.
Merikangas, K.R. and Low, N.C. (2005) Genetic epidemiology of anxiety disorders, Handbook ofExperimental Pharmocology, 163–79.
Merskey, H. and Trimble, M.R. (1979) Personality, sexual adjustment and brain lesions in patientswith conversion symptoms, American Journal of Psychiatry, 136, 179–82.
Meyer, M.K., Shea, A., Hendrie, H. C et al. (1981) Plasma tryptophan and five other amino acids indepressed and normal subjects, Archives of General Psychiatry, 38, 642–6.
Meyer-Lindenberg, A., Buckholtz, J.W., Kolachana, B. et al. (2006) Neural mechanisms of geneticrisk for impulsivity and violence in humans, Proceedings of the National Academic of Science U SA, 103, 6269–74.
Miczek, K.A., Altman, J.L., Appel, J.B. et al. (1975) Para-chlorophenylalanine, serotonin, and killingbehavior, Pharmacology, Biochemistry and Behavior, 3, 355–61.
Middeldorp, C.M., Cath, D.C., van Dyck, R. et al. (2005) The co-morbidity of anxiety and depressionin the perspective of genetic epidemiology: a review of twin and family studies, PsychologicalMedicine, 35, 611–24.
Middeldorp, C.M., Cath, D.C. and Boomsma, D.I. (2006) A twin-family study of the associa-tion between employment, burnout and anxious depression, Journal of Affective Disoder, 90,163–9.
Middeldorp, C.M., Hottenga, J.J., Slagboom, P.E. et al. (2008) Linkage on chromosome 14 in agenome-wide linkage study of a broad anxiety phenotype, Molecular Psychiatry, 13, 84–9.
Mikkelsen, J.D., Woldbye, D., Kragh, J. et al. (1994) ECS increases the expression of neuropeptideY mRNA in the piriform cortex and the dentate gyrus, Molecular Brain Research, 23, 317–22.
Miller, H.L., Delgado, P.L., Salomon, R.M. et al. (1992) Acute tryptophan depletion: a method ofstudying antidepressant action, The Journal of Clinical Psychiatry, 53, Suppl, 28–35.
Mindham, R.H.S., Steele, C., Folstein, M.F. et al. (1985) A comparison of the frequency of major affec-tive disorder in Huntington’s disease and Alzheimer’s disease, Journal of Neurology, Neurosurgeryand Psychiatry, 48, 1172–4.
Mindus, P. and Nyman, H. (1991) Normalisation of personality characteristics in patients withincapacitating anxiety disorders after capsulotomy, Acta Psychiatrica Scandinavica, 83, 283–91.
Minzenberg, M.J., Fan, J., New, A.S. et al. (2007) Fronto-limbic dysfunction in response to facialemotion in borderline personality disorder: an event-related fMRI study, Psychiatry Research,155, 231–43.
Mirow, A.L., Krisatbjanarson, H., Egeland, J.A. et al. (1994) A linkage study of distal chromosome5q and bipolar disorder, Biological Psychiatry, 36, 223–9.
Mitchel, P. (2002) 15 Hz and 1 Hz TMS have different acute effects on cerebral blood flow indepressed patients, International Journal of Neuropsychopharmacology, 5, S7–S.08.

370 References
Mitchell-Heggs, N., Kelly, D. and Richardson, A. (1976) Stereotactic limbic leucotomy: a follow upat 16 months, British Journal of Psychiatry, 128, 226–40.
Modai, I., Apter, A., Golomb, A.M. et al. (1979) Response to amitriptyline and urinary MHPG inbipolar depressed patients, Neuropsychobiology, 5, 181–4.
Moffitt, T.E., Caspi, A. and Rutter, M. (2005) Strategy for investigating interactionsbetween measured genes and measured environments, Archives of General Psychiatry, 62,473–81.
Mogenson, G.J., Jones, D.L. and Yim, C.Y. (1980) From motivation to action: functional interfacebetween the limbic system and the motor system, Progress in Neurobiology, 14, 69–97.
Møller, S.E., Kirk, L. and Honore, P. (1979) Free and total plasma tryptophan in endogenousdepression, Journal of Affective Disorders, 1, 69–76.
Money, J. (1975) Human behavioural cytogenetics: review of psychopathology in three syndromes:47XXY, 47XYY and 45X, The Journal of Sex Research, 11, 181–200.
Moniz, E. (1936) Tentatives Operatroires dans le Traitment de Certaines Psychoses, Masson, Paris.Monroe, R. (1970) Episodic Behaviour Disorders, Harvard Press, Harvard.Montigny, C. de and Blier, P. (1985) Electrophysiological aspects of serotonin neuropharmacol-
ogy. In A.R. Green (ed.), Neuropharmacology of Serotonin, Oxford University Press, Oxford,pp. 181–92.
Moore, C.M., Breeze, J.L., Gruber, S.A. et al. (2000) Choline, myo-inositol and mood in bipolardisorder: a proton magnetic resonance spectroscopic imaging study of the anterior cingulatecortex, Bipolar Disorders, 2, 207–16.
Morselli, P.L., Bossi, L., Henry, J.F. et al. (1980) On the therapeutic action of SL76002, a newGABA-mimetic agent, Brain Research Bulletin, 5, Suppl. 2, 411–15.
Mosimann, U.P., Marre, S.C., Werlen, S. et al. (2002) Antidepressant effects of repetitive transcranialmagnetic stimulation in the elderly: correlation between effect size and coil–cortex distance,Archives of General Psychiatry, 59, 560–1.
Mu, Q., Bohning, D.E., Nahas, Z. et al. (2004) Acute vagus nerve stimulation using different pulsewidths produces varying brain effects, Biological Psychiatry, 55, 816–25.
Mueller, F.S., Heninger, G.R. and MacDonald, R. (1969) Insulin tolerance test in depression, Archivesof General Psychiatry, 21, 587.
Muggleton, N.G., Postma, P., Moutsopoulou, K. et al. (2006) TMS over right posterior parietalcortex induces neglect in a scene-based frame of reference, Neuropsychologia, 44, 1222–9.
Mula, M., Jauch, R., Cavanna, A. et al. (2010) Interictal dysphoric disorder and periictal dysphoricsymptoms in patients with epilepsy, Epilepsia, [Epub ahead of print].
Mula, M., Trimble, M.R., Thompson, P. et al. (2003) Topiramate and word-finding difficulties inpatients with epilepsy, Neurology, 60, 1104–7.
Munafo, M.R., Brown, S.M. and Hariri, A.R. (2008) Serotonin transporter (5-HTTLPR) genotypeand amygdala activation: a meta-analysis, Biological Psychiatry, 63, 852–7.
Murphy, D.L., Brodie, H.K.H., Goodwin, F.R. et al. (1971) Regular induction of hypomania byL-dopa in bipolar manic depressive patients, Nature, 229, 135–6.
Murphy, D.L., Belmaker, R. and Wyatt, R.J. (1974) Monoamine oxidase in schizophrenia and otherbehavioural disorders, Journal of Psychiatric Research, 11, 221–47.
Murphy, D.L., Belmaker, R.H., Buchsbaum, M. et al. (1977) Biogenic amine related enzymes andpersonality variables in normals, Psychological Medicine, 7, 149–57.
Myslobodsky, M., Mintz, M. and Tomer, R. (1979) Asymmetric reactivities of the brain andcomponents of hemispheric imbalance. In J. Gruzelier and P. Flor-Henry (eds.), HemisphereAsymmetries of Function in Psychopathology, Elsevier, North Holland, pp. 125–48.
Naguib, M. and Levy, R. (1982) Prediction of outcome in senile dementia: a CT study, British Journalof Psychiatry, 140, 263–7.

References 371
Nahas, Z., Lomarev, M., Roberts, D.R. et al. (2001) Unilateral left prefrontal transcranial magneticstimulation (TMS) produces intensity-dependent bilateral effects as measured by interleavedbold fMRI, Biological Psychiatry, 50(9), 712–20.
Nahas, Z., Marangell, L.B., Husain, M.M. et al. (2005) Two-year outcome of vagus nervestimulation (VNS) therapy for major depressive episodes, Journal of Clinical Psychiatry, 66,1097–104.
Nasrallah, H.A. (2008) Atypical antipsychotic-induced metabolic side effects: insights fromreceptor-binding profiles, Molecular Psychiatry, 13, 27–35.
Nasrallah, H.A., McCalley-Whitters, M. and Jacoby, C.G. (1982a) Cortical atrophy in schizophreniaand mania: a comparative CT study, Journal of Clinical Psychiatry, 43, 439–41.
Nasrallah, H.A., McCalley-Whitters, M. and Jacoby, C.G. (1982b) Cerebral ventricular enlargementin young manic males, Journal of Affective Disorders, 4, 15–19.
Nauta, W.J.H. (1964) Some efferent connections of the prefrontal cortex in the monkey. In J.M.Warren and K. Akert (eds.), The Frontal Granular Cortex and Behaviour, McGraw Hill, New York,NY, pp. 397–407.
Nauta, W.J.H. (1986) Circuitous connections linking cerebral cortex limbic system and corpusstriatum. In B.K. Doane and K.E. Livingstone (eds.), The Limbic System, Raven Press, New York,NY, pp. 43–54.
Nauta, W.J.H. and Domesick, V.B. (1982) Neural associations of the limbic system. In A. Beckman(ed.), The Neural Basis of Behaviour, Spectrum Inc., New York, NY, pp. 175–206.
Naylor, G.J., McNamee, H.B. and Moody, J.P. (1970) Erythrocyte sodium and potassium indepressive illness, Journal of Psychosomatic Research, 14, 173–7.
Naylor, G.J., Dick, D.A.T. and Dick, E.G. (1976) Erythrocyte membrane cation carrier, relapse rateof manic depressive illness and response to lithium, Psychological Medicine, 6, 257–63.
Naylor, G.J., Smith, A.H.W., Bryce-Smith, D. et al. (1984) Tissue vanadium levels in manic depressiveillness, Psychological Medicine, 14, 767–72.
Neal, J.B. (1942) Encephalitis, H.K. Lewis, London.Neary, D., Snowden, J.S., North, B. et al. (1988) Dementia of the frontal lobe type, Journal of
Neurology, Neurosurgery and Psychiatry, 51, 353–61.Nemeroff, C.B., Krishnan, K.C.R., Reed, D. et al. (1992) Adrenal gland enlargement in major
depression: a CT study, Archives of General Psychiatry, 49, 384–7.Nemeroff, C.B., Mayberg, H.S., Krahl, S.E. et al. (2006) VNS therapy in treatment-resistant depres-
sion: clinical evidence and putative neurobiological mechanisms, Neuropsychopharmacology, 31,1345–55.
Nesse, R.M., Cameron, O.G., Curtis, G.C. et al. (1984) Noradrenergic function in patients withanxiety, Archives of General Psychiatry, 41, 771–6.
Neumann, C.S., Hare, R.D. and Newman, J.P. (2007) The super-ordinate nature of the psychopathychecklist-revised, Journal of Personality Disorder, 21, 102–17.
Neumeister, A., Hu, X.Z., Luckenbaugh, D.A. et al. (2006) Differential effects of 5-HTTLPR geno-types on the behavioral and neural responses to tryptophan depletion in patients with majordepression and controls, Archives of General Psychiatry, 63, 978–86.
Newmark, M.E. and Penry, J.K. (1980) Genetics of Epilepsy: A Review, Raven Press, New York, NY.Ni, X., Chan, K., Bulgin, N. et al. (2006) Association between serotonin transporter gene and
borderline personality disorder, Journal of Psychiatric Research, 40, 448–53.Ni, X., Sicard, T., Bulgin, N. et al. (2007) Monoamine oxidase a gene is associated with borderline
personality disorder, Psychiatric Genetics, 17, 153–7.Ni, X., Chan, D., Chan, K. et al. (2009) Serotonin genes and gene–gene interactions in borderline
personality disorder in a matched case-control study, Progress in Neuro-Psychopharmacology andBiological Psychiatry , 33, 128–33.

372 References
Nielsen, H. and Kristensen, O. (1981) Personality correlates of sphenoidal EEG foci in temporallobe epilepsy, Acta Neurologica Scandinavica, 64, 289–300.
Nielsen, D.A., Goldman, D., Virkkunen, M. et al. (1994) Suicidality and 5-HIAA concentrationassociated with tryptophan hydrolase polymorphism, Archives of General Psychiatry, 51, 34–8.
Nieuwenhuys, R. (1996) The greater limbic system, the emotional motor system and the brain.In H.J. Groenewegen, R. Bandler, C.B. Saper (eds.), The Emotional Motor System, Elsevier,Amsterdam.
Ninan, P.T., van Kammen, D.P., Scheinin, M. et al. (1984) CSF 5-HIAA levels in suicidalschizophrenic patients, American Journal of Psychiatry, 141, 566–9.
Nobler, M.S. and Sackeim, H.A. (1993) ECT stimulus dosing. In C.E. Coffey (ed.), The ClinicalScience of ECT, APA Press, Washington, DC, pp. 229–52.
Nobler, M.S., Sackeim, H.A., Prohovnik, I. et al. (1994) Regional cerebral blood flow in mooddisorders: III. Treatment and clinical response. Archives of General Psychiatry, 51, 884–97.
Nobler, M.S., Roose, S.P., Prohovnik, I. et al. (2000) Regional cerebral blood flow in mood disorders.V: Effects of antidepressant medication in late-life depression, American Journal of GeriatricPsychiatry, 8, 289–96.
Nobler, M.S., Oquendo, M.A., Kegeles, L.S. et al. (2001) Decreased regional brain metabolism afterECT, American Journal of Psychiatry, 158, 305–8.
Nordstrom, A.-L., Farde, L., Wiesel, F.A. et al. (1993) Central D2-dopamine receptor occupancy inrelation to antipsychotic drug effects, Biological Psychiatry, 33, 227–36.
Norton, N., Williams, H.J. and Owen, M.J. (2006) An update on the genetics of schizophrenia,Current Opinion in Psychiatry, 19, 158–64.
Nothen, M.M., Erdmann, J., Korner, J. et al. (1992) Lack of association between dopamine D1 andD2 receptor genes and bipolar affective disorder, American Journal of Psychiatry, 149, 199–201.
Nudmamud-Thanoi, S., Piyabhan, P., Harte, M.K. et al. (2007) Deficits of neuronal glutamatergicmarkers in the caudate nucleus in schizophrenia, Journal of Neural Transmission, Suppl., 281–5.
Nuechterlein, K.H., Luck, S.J., Lustig, C. et al. (2009) CNTRICS final task selection: control ofattention, Schizophrenia Bulletin, 35, 182–96.
Nutt, D.J. and Glue, P. (1993) The neurobiology of ECT animal studies. In C.E. Coffey (ed.), TheClinical Science of ECT, APA Press, Washington, DC, pp. 213–35.
Nutt, D. and Lawson, C. (1992) Panic attacks, British Journal of Psychiatry, 160, 154–64.Nyback, H., Walters, J.R., Aghajanian, G.K. et al. (1975) Tricyclic antidepressants: effect on the
firing rate of noradrenergic neurones, European Journal of Pharmacology, 32, 302–12.O’Donoghue, M.F., Goodridge, D.M., Redhead, K. et al. (1999) Assessing the psychosocial conse-
quences of epilepsy: a community-based study, Br J Gen Pract, 49, 211–14.O’Donovan, M.C., Craddock, N., Norton, N. et al. (2008) Identification of loci associated with
schizophrenia by genome-wide association and follow-up, Nature Genetics, 40, 1053–5.O’Keefe, J. and Nadel, L. (1978) The Hippocampus as a Cognitive Map, Oxford University Press,
Oxford.Olajide, D. and Lader, M. (1984) Depression following withdrawal from long-term benzodiazepine
use: a report of four cases, Psychological Medicine, 14, 937–40.Olds, J. and Milner, P. (1954) Positive reinforcement produced by electrical stimulation of septal
area and other regions of rat brain, Journal of Comparative and Physiological Psychology, 47, 419–27.Onyike, C.U., Sheppard, J.M., Tschanz, J.T. et al. (2007) Epidemiology of apathy in older adults: the
Cache County study, American Journal of Geriatric Psychiatry, 15, 365–75.O’Reardon, J.P., Solvason, H.B., Janicak, P.G. et al. (2007) Efficacy and safety of transcranial magnetic
stimulation in the acute treatment of major depression: a multi-site randomized controlled trial,Biological Psychiatry, 62, 1208–16.

References 373
Oreland, L., von Knorring, L., von Knorring, A.L. et al. (1984) Studies on the connection betweenalcoholism and low platelet MAO. In S. Parvez et al. (eds.), Alcohol, Nutrition and the NervousSystem, International Science Press, Utrecht.
Otterson, O.P. (1981) Afferent connection to the amygdaloid complex of the rat with someobservations in the cat: III. Afferents from lower brainstem, Journal of Comparative Neurology,202, 335.
Ottosson, J.O. (1960) Experimental studies in the mode of action of ECT, Acta Psychiatrica Scandi-navica, 35, Suppl. 135, 1–141.
Owen, F., Bourne, R.C., Crow, T.J. et al. (1981) Platelet MAO in acute schizophrenia: relationship tosymptomatology and neuroleptic medication, British Journal of Psychiatry, 139, 16–22.
Owens, D.G. and Johnstone, E.C. (2006) Precursors and prodromata of schizophrenia: findingsfrom the Edinburgh high risk study and their literature context, Psychological Medicine, 36,1501–14.
Owens, D.G.C., Johnstone, E.C., Crow, T.J. et al. (1985) Lateral ventricular size in schizophrenia:relationship to the disease process and its clinical manifestations, Psychological Medicine, 15,27–41.
Ozaki, N., Rosenthal, N.E., Mazzola, P. et al. (1994) Platelet paroxetine binding, 5-HT-stimulatedCa++ response, and 5-HT content in winter seasonal affective disorder, Biological Psychiatry, 36,458–66.
Padberg, F., Zwanzger, P., Keck, M.E., et al. (2002) Repetitive transcranial magnetic stimulation(rTMS) in major depression: relation between efficacy and stimulation intensity, Neuropsy-chopharmacology, 27, 638–45.
Palmini, A. and Gloor, P. (1992) The localising value of auras in partial seizures, Neurology, 42,801–8.
Palomino, A., Gonzalez-Pinto, A., Aldama, A. et al. (2007) Decreased levels of plasma glutamate inpatients with first-episode schizophrenia and bipolar disorder, Schizophrenia Research, 95, 174–8.
Pandey, G.N., Dysken, M.W., Garter, D.L. et al. (1979) Beta adrenergic receptor function in affectiveillness, American Journal of Psychiatry, 136, 675–8.
Pandey, S.C., Kim, S.W., Davis, J. et al. (1993) Platelet S2 receptors in obsessive–compulsive disorder, Biological Psychiatry, 37, 367–72.
Papp, L.A., Klein, D.F. and Gorman, J.M. (1993) Carbon dioxide hypersensitivity, hyperventilation,and panic disorder, American Journal of Psychiatry, 150(8), 1149–57.
Pare, C.M.B. (1985) The present state of MAOI, British Journal of Psychiatry, 146, 576–84.Parent, C.I. and Meaney, M.J. (2008) The influence of natural variations in maternal care on play
fighting in the rat, Developmental Psychobiology, 50, 767–76.Paterson, A.D., Sunohara, G.A. and Kennedy, J.L. (1999) Dopamine D4 receptor gene: novelty or
nonsense?, Neuropsychopharmacology, 21, 3–16.Paul, M.I., Cramer, H. and Bunney, W.E. (1971a) Urinary adenosine 3,5 monophosphate in the
switch process from depression to mania, Science, 171, 300–5.Paul, M.I., Cramer, H. and Goodwin, F.K. (1971b) Urinary cyclic AMP excretion in depression and
mania, Archives of General Psychiatry, 24, 327–33.Paus, T., Castro-Alamancos, M.A. and Petrides, M. (2001) Cortico–cortical connectivity of the
human mid-dorsolateral frontal cortex and its modulation by repetitive transcranial magneticstimulation, European Journal of Neuroscience, 14, 1405–11.
Paykel, E.S. and Hollyman, J.A. (1984) Life events and depression: a psychiatric view, Trends inNeurosciences, 7, 475–80.
Pearlson, G.D. and Verloff, A.E. (1981) CT scan changes in manic-depressive illness, Lancet,ii, 470.

374 References
Pearlson, G.D., Wong, D.F., Tune, L.E. et al. (1995) In vivo D2 dopamine receptor density in psychoticand non-psychotic patients with bipolar disorder, Archives of General Psychiatry, 52, 471–7.
Penry, J.K. and Dean, J.C. (1990) Prevention of intractable partial seizures by intermittent vagalnerve stimulation in humans: preliminary results, Epilepsy, 31, S40–3.
Peralta, V. and Cuesta, M.J. (1999) Dimensional structure of psychotic symptoms: an item levelanalysis of SAPS and SANS symptoms in psychotic disorders, Schizophrenia Pesearch, 38,13–26.
Perez, M.M. and Trimble, M.R. (1980) Epileptic psychosis: diagnostic comparison with processschizophrenia, British Journal of Psychiatry, 137, 245–9.
Perris, C. (1974) A study of cycloid psychosis, Acta Psychiatrica Scandinavica, Suppl., 253.Perris, H., von Knorring, L., Oreland, L. et al. (1984) Life events and biological vulnerability,
Psychiatry Research, 12, 111–20.Perry, E.K. and Perry, R.H. (1980) The cholinergic system in Alzheimer’s disease. In P.J. Roberts
(ed.), Biochemistry of Dementia, John Wiley and Sons, Chichester, pp. 135–83.Perry, B.D., Southwick, S.M., Yehuda, R. et al. (1990) Adrenergic receptor regulation in post-
traumatic stress disorder. In E.L. Giller (ed.), Biological Assessment and Treatment of PTSD, APAPress, Washington, DC, pp. 84–114.
Petrides, G., Fink, M., Husain, M.M. et al. (2001) ECT remission rates in psychotic versus nonpsy-chotic depressed patients: a report from core, Journal of ECT, 17, 244–53.
Pezawas, L., Meyer-Lindenberg, A., Drabant, E.M. et al. (2005) 5-HTTLRP polymorphism impactshuman cingulate-amygdala interactions: a genetic susceptibility mechanism for depression,Nature Neuroscience, 8, 828–34.
Picard, F. and Brodtkorb, E. (2007) Familial frontal lobe epilpesies. In J. Engel and T. Pedley (eds.),Epilepsy: A Comprehensive Textbook, 2nd edition, Lippincott Williams & Wilkins, New York, NY,pp. 2495–502.
Pickar, D., Labarca, T., Linnoila, M. et al. (1984) Neuroleptic induced decrease in plasma HVA andantipsychotic activity in schizophrenic patients, Science, 225, 954–6.
Pickar, D., Woen, R.R., Litman, R.E. et al. (1992) Clinical and biologic response to clozapine inpatients with schizophrenia, Archives of General Psychiatry, 49, 345–53.
Pillmann, E., Rohde, A., Ullrich, S. et al. (1999) Violence, criminal behaviour, and the EEG: signifi-cance of left hemisphere focal abnormalities, Journal of Neuropsychiatry and Clinical Neuroscience,11, 454–7.
Pilowsky, L.S., Costa, D.C., Ell, P.J. et al. (1992) Clozapine, SPET and D2 dopamine receptorblockade hypothesis of schizophrenia, Lancet, 340, 199–202.
Pisani, F., Narbone, M.C., Fazio, A. et al. (1984) Increased serum carbamazepine levels withviloxazine in epileptic patients, Epilepsia, 25, 482–3.
Pitts, F. and McClure, J.N. (1967) Lactate metabolism in anxiety neurosis, New England Journal ofMedicine, 277, 1329–36.
Pope, A. and Keck, M.E. (2001) TMS as a therapeutic tool in psychiatry: what do we know aboutneurobiological mechanisms?, Journal of Psychiatric Research, 35, 193–215.
Porges, S.W. (1995) Orienting in a defensive world: mammalian modifications of our evolutionaryheritage: a polyvagal theory, Psychophysiology, 32, 301–18.
Porges, S.W. (2007) The polyvagal perspective, Biological Psychology, 74, 116–43.Porteous, D. (2008) Genetic causality in schizophrenia and bipolar disorder: out with the old and
in with the new, Current Opinion in Genetics and Development, 18, 229–34.Post, R.M. and Goodwin, F.K. (1975) Time dependent effects of phenothiazines on dopamine
turnover in psychiatric patients, Science, 190, 488–9.Post, R.M. and Goodwin, F.K. (1978) Approaches to brain amines in psychiatric patients, Handbook
of Psychopharmacology, 13, 147–85.

References 375
Post, R.M. and Uhde, T.W. (1986) Anticonvulsants in nonepileptic psychosis. In M.R. Trimbleand T.G. Bolwig (eds.), Aspects of Epilepsy and Psychiatry, John Wiley and Sons, Chichester, pp.177–212.
Post, R.M., Gordon, E.K., Goodwin, F.K. et al. (1973) Central norepinephrine metabolism in affectiveillness: MHPG in the CSF, Science, 179, 1002–3.
Post, R.M., Jimerson, D.C., Ballenger, J.C. et al. (1985) CSF norepinephrine and its metabolites inmanic depressive illness. In R.M. Post and J.C. Ballenger (eds.), Neurobiology of Mood Disorders,Williams and Wilkins, Baltimore, pp. 539–51.
Post, R.M., Rubinow, D.R., Uhde, T.W. et al. (1986) Dopaminergic effects of carbamazepine, Archivesof General Psychiatry, 43, 392–6.
Prange, A., Wilson, I., Lynn, C.W. et al. (1974) L-tryptophan in mania: contribution to a permissivehypothesis of affective disorder, Archives of General Psychiatry, 30, 52–62.
Prata, D.P., Mechelli, A., Fu, C.H. et al. (2008a) Effect of disrupted-in-schizophrenia-1 on pre-frontalcortical function, Molecular Psychiatry, 13, 915–7.
Prata, D.P., Mechelli, A., Fu, C.H. et al. (2008b) The Disc1 Ser704Cys polymorphism is associatedwith prefrontal function in healthy individuals, Molecular Psychiatry, 13, 909.
Preece, N.A., Jackson, G.D., Houseman, J.A. et al. (1994) NMR detection of elevated cortical GABAin the vigabatrin-treated rat in vivo, Epilepsia, 35, 431–6.
Preter, M. and Klein, D.F. (2008) Panic, suffocation false alarms, separation anxiety and endogenousopioids, Progress in Neuropscholopharmacol and Biological Psychiatry, 32, 603–12.
Price, J. (1968) The genetics of depressive disorder. In A. Coppen and A. Walk (eds.), British Journalof Psychiatry Special Publication, No. 2, pp. 37–54.
Price, J.L. (1981) The efferent projections of the amygdaloid complex in the rat, cat and monkey. InY. Ben-Ari (ed.), The Amygdaloid Complex, Elsevier, North Holland, pp. 121–32.
Pridmore, S. (2000) Substitution of rapid transcranial magnetic stimulation treatments for electro-convulsive therapy treatments in a course of electroconvulsive therapy, Depress Anxiety, 12(3),118–23.
Pridmore, S. and Oberoi, G. (2000) Transcranial magnetic stimulation applications and potentialuse in chronic pain: studies in waiting, Journal of the Neurological Sciences, 182, 1–4.
Procci, W.R. (1976) Schizoaffective psychosis: fact or fiction, Archives of General Psychiatry, 33,1167–78.
Prusiner, S.B. (1987) Prions and neurodegenerative disease, New England Journal of Medicine, 317,1571–81.
Qin, P., Xu, H., Laursen, T.M. et al. (2005) Risk for schizophrenia and schizophrenia-like psychosisamong patients with epilepsy: population based cohort study, British Medical Journal, 331, 23.
Quednow, B.B., Jessen, F., Kuhn, K.U. et al. (2006) Memory deficits in abstinent MDMA (ecstasy)users: neuropsychological evidence of frontal dysfunction, Journal of Psychopharmacol, 20, 373–84.
Quednow, B.B., Kuhn, K.U., Hoppe, C. et al. (2007) Elevated impulsivity and impaired decision-making cognition in heavy users of MDMA (‘ecstasy’), Psychopharmacology (Berl), 189, 517–30.
Quiske, A., Helmstaedter, C., Lux, S. et al. (2000) Depression in patients with temporal lobe epilepsyis related to mesial temporal sclerosis, Epilepsy Research, 39, 121–5.
Rabkin, J.G., Steward, J. and Klein, D.F. (1985) Overview on the relevance of the DST to differentialdiagnosis. In R.M.A. Hirschfeld (ed.), Clinical Utility of the Dexamethasone Suppression Test, NIH,MD, pp. 12–33.
Raine, A. and Yang, Y. (2006) Neural foundations to moral reasoning and antisocial behavior, Socialand Affective Neuroscience, 1, 203–13.
Raine, A., Venables, P.H. and Williams, M. (1990) Relationships between central and autonomicmeasures of arousal at age 15 years and criminality at age 24 years, Archives of General Psychiatry,47, 1003–7.

376 References
Raine, A., Buchsbaum, M.S., Stanley, J. et al. (1994) Selective reductions in prefrontal glucosemetabolism in murderers, Biological Psychiatry, 36, 365–73.
Raine, A., Phil, D., Stoddard, J. et al. (1998) Prefrontal glucose deficits in murderers lackingpsychosocial deprivation, Neuropsychiatry Neuropsychology and Behavioural Neurology, 11, 1–7.
Raine, A., Lencz, T., Bihrle, S. et al. (2000) Reduced prefrontal gray matter volume and reducedautonomic activity in antisocial personality disorder, Archives of General Psychiatry, 57, 119–27.
Raine, A., Lencz, T., Yaralian, P. et al. (2002) Prefrontal structural and functional deficits inschizotypal personality disorder, Schizophrenia Bulletin, 28, 501–13.
Raine, A., Lencz, T., Taylor, K. et al. (2003) Corpus callosum abnormalities in psychopathic antisocialindividuals, Archives of General Psychiatry, 60, 1134–42.
Randrup, A., Munkvad, I., Fog, R. et al. (1975) Mania, depression and brain dopamine. In L. Valzelli(ed.), Current Development in Psychopharmacology, Vol. 2, Spectrum Publications, New York, NY,pp. 207–48.
Rangel-Guerra, R.A., Perez-Payan, H., Minkoff, L. et al. (1983) NMR in bipolar affective disorders,American Journal of Neuroradiology, 4, 229–32.
Rao, S.M., Devinsky, O., Grafman, J. et al. (1992) Viscosity and social cohesion in temporal lobeepilepsy, Journal of Neurology, Neurosurgery and Psychiatry, 55, 149–52.
Rapoport, J.L. (1992) Animal models of obsessive compulsive disorder, Clinical Neuropharmacol, 15,Suppl. 1, Pt A, A261–2.
Rapoport, J.L., Ryland, D.H. and Kriete, M. (1992) Drug treatment of canine acral lick: an animalmodel of obsessive–compulsive disorder, Archives of General Psychiatry, 49, 517–21.
Rapoport, J., Chavez, A., Greenstein, D. et al. (2009) Autism spectrum disorders and childhood-onset schizophrenia: clinical and biological contributions to a relation revisited, Journal of theAmerican Academy of Child and Adolescent Psychiatry, 48, 10–18.
Rauch, S.L., Jenike, M.A., Alpert, N.M. et al. (1994) Regional CBF measured during symptompreoccupation in OCD using O15-labelled CO2 and PET, Archives of General Psychiatry, 51,62–70.
Rauch, S.L., Savage, C.R., Alpert, N.M. et al. (1995) A positron emission tomographic study ofsimple phobic symptom provocation, Archives of General Psychiatry, 52, 20–8.
Reiman, E.M., Raichle, M.E., Robins, E. et al. (1989) Neuroanatomical correlates of a lactate inducedanxiety attack, Archives of General Psychiatry, 46, 493–500.
Reisine, T.D. and Bell, G.I. (1993) Molecular biology of opiate receptors, TINS, 16, 506–10.Reveley, M.A., Glover, V., Sandler, M. et al. (1981) Increased platelet MAO activity in affective
disorders, Psychopharmacology, 73, 257–60.Reveley, M.A., Reveley, A.M., Clifford, C.A. et al. (1983) Genetics of platelet MAO activity in
discordant schizophrenia and normal twins, British Journal of Psychiatry, 142, 560–5.Reynolds, E.H. (1976) Neurological aspects of folate and vitamin B12 metabolism, Clinics in
Haematology, 5, 661–96.Reynolds, E.H. (1981) Biological factors in psychological disorders associated with epilepsy. In E.H.
Reynolds and M.R. Trimble (eds.), Epilepsy and Psychiatry, Churchill Livingstone, Edinburgh,pp. 264–90.
Reynolds, G.P. and Harte, M.K. (2007) The neuronal pathology of schizophrenia: molecules andmechanisms, Biochemical Society Transactions, 35, 433–6.
Reynolds, E.H., Carney, M.W.P. and Toone, B.K. (1984) Methylation and mood, Lancet, ii, 196–7.Rhodes, R.A., Murthy, N.V., Dresner, M.A. et al. (2007) Human 5-HT transporter availability
predicts amygdala reactivity in vivo, Journal of Neuroscience, 27, 9233–7.Ribeiro, S., Tandon, R., Greenhaus, L. et al. (1993) The DST as a predictor of outcome in depression:
a meta analysis, American Journal of Psychiatry, 150, 1618–29.Riding, B.E.J. and Munroe, A. (1975) Pimozide in monosymptomatic psychosis, Lancet, ii, 400–1.

References 377
Rihmer, Z., Gonda, X., Akiskal, K.K. et al. (2007) Affective temperament: a mediating vari-able between environment and clinical depression?, Archives of General Psychiatry, 64,1096–7.
Riley, B. and Kendler, K.S. (2006) Molecular genetic studies of schizophrenia, European Journal ofHuman Genetics, 14, 669–80.
Riley, G.J. and Shaw, D.M. (1976) Total and non-bound tryptophan in unipolar illness, Lancet, ii,1249.
Ring, H.A., Trimble, M.R., Costa, D.C. et al. (1992) Effect of vigabatrin on striatal dopaminereceptors: evidence in humans for interactions of GABA and dopamine systems, Journal ofNeurololgy, Neurosurgery and Psychiatry, 55, 758–61.
Ring, H.A., Trimble, M.R., Costa, C.D. et al. (1993) Striatal dopamine receptor binding in epilepticpsychoses, Biological Psychiatry, 35, 375–80.
Ring, H.A., Bench C., Trimble, M.R. et al. (1994) Depression in Parkinson’s disease, British Journalof Psychiatry, 165, 333–9.
Robbins, T.W. and Arnsten, A.F. (2009) The neuropsychopharmacology of fronto-executive func-tion: monoaminergic modulation, Annual Review of Neuroscience, 32, 267–87.
Roberts, G.W., Polak, J.M. and Crow, T.J. (1984) Peptide circuitry of the limbic system. In M.R.Trimble and E. Zarifian (eds.), Psychopharmacology of the Limbic System, Oxford University Press,Oxford, pp. 226–43.
Roberts, G.W., Done, D.J., Bruton, C. et al. (1990) A ‘mock up’ of schizophrenia, Biological Psychiatry,28, 127–43.
Roberts, J.K.A. (1984) Differential Diagnosis in Neuropsychiatry, John Wiley and Sons, Chichester.Robertson, M.M. (1986) Ictal and interictal depression in patients with epilepsy. In M.R. Trimble
and T. Bolwig (eds.), Aspects of Epilepsy and Psychiatry, John Wiley and Sons, Chichester, pp.211–32.
Robertson, M.M. (1998) Forced normalisation and the aetiology of depression in epilepsy. InM.R. Trimble and B. Schmitz (eds.), Forced Normalisation and Alternative Psychoses of Epilepsy,Wrightson Biomedical Publishing, Petersfield, pp. 143–67.
Robertson, M.M. and Trimble, M.R. (1983) Depressive illness in patients with epilepsy: a review,Epilepsia, 24, Suppl. 2, S109–16.
Robertson, M.M., Trimble, M.R. and Townsend, H.R.A. (1987) The phenomenology of depressionin epilepsy, Epilepsia, 28, 364–72.
Robinson, R.G. and Szetala, B. (1981) Mood change following left hemisphere brain injury, Annalsof Neurology, 9, 447–53.
Robinson, R.G., Starr, L.B. and Price, T.R. (1984) A two year longitudinal study of mood disordersfollowing stroke, British Journal of Psychiatry, 144, 256–62.
Robinson, D., Wu, H., Munne, R.A. et al. (1995) Reduced caudate nucleus volume in OCD, Archivesof General Psychiatry, 52, 393–8.
Rodin, E. and Schmaltz, S. (1983) Folate levels in epileptic patients. In M. Parsonage et al. (eds.),Advances in Epileptology: The 14th Epilepsy International Symposium, Raven Press, New York, NY,pp. 143–53.
Rodrigues, S.M., Ledoux, J.E. and Sapolsky, R.M. (2009) The influence of stress hormones on fearcircuitry, Annual Review of Neuroscience, 32, 289–313.
Roffman, J.L., Weiss, A.P., Goff, D.C. et al. (2006) Neuroimaging-genetic paradigms: a new approachto investigate the pathophysiology and treatment of cognitive deficits in schizophrenia, HarvardReview Of Psychiatry, 14, 78–91.
Rollnik, J.D., Huber, T.J., Mogk, H. et al. (2000) High frequency repetitive transcranial magneticstimulation (rTMS) of the dorsolateral prefrontal cortex in schizophrenic patients, Neuroreport,11(18), 4013–15.

378 References
Rollnik, J.D., Wustefeld, S., Dauper, J. et al. (2002) Repetitive transcranial magnetic stimulation forthe treatment of chronic pain: a pilot study, European Neurology, 48, 6–10.
Rolls, E.T. (2001) The rules of formation of the olfactory representations found in the orbitofrontalcortex olfactory areas in primates, Chem Senses, 26, 595–604.
Ron, M.A., Acker, W. and Lishman, W.A. (1979) Dementia in chronic alcoholism. In J. Obiols et al.(eds.), Biological Psychiatry Today, Elsevier, North Holland, pp. 1146–50.
Ross, C.A., Margolis, R.L., Reading, S.A. et al. (2006) Neurobiology of schizophrenia, Neuron, 52,139–53.
Rossor, M.N. (1981) Parkinson’s disease and Alzheimer’s disease as disorders of the isodendriticcore, British Medical Journal, 283(ii), 1588–90.
Rossor, M.N., Iversen, L.L., Mountjoy, C.Q. et al. (1980) AVP and ChAT in brains of patients withAlzheimer-type senile dementia, Lancet, ii, 1367–8.
Rossor, M.N., Iversen, L.L., Reynolds, G.P. et al. (1984) Neurochemical characteristics of early andlate onset types of Alzheimer’s disease, British Medical Journal, 288(i), 961–4.
Rosvold, H.E., Mirsky, A.F. and Pribram, K.H. (1954) Influence of amygdalectomy on socialbehaviour in monkeys, Journal of Comparative and Physiological Psychology, 47, 173–80.
Rotarska-Jagiela, A., Oertel-Knoechel, V., Demartino, F. et al. (2009) Anatomical brain connectivityand positive symptoms of schizophrenia: a diffusion tensor imaging study, Psychiatry Research,174(1), 9–16.
Roy, A., Pickar, D., Linnoila, M. et al. (1985) Plasma norepinephrine levels in affective disorders,Archives of General Psychiatry, 42, 1181–5.
Roy, A., Pickar, D., Douillet, P. et al. (1986a) Urinary monoamines and monoamine metabolitesin sub-types of unipolar depressive disorder and normal controls, Psychological Medicine, 16,541–6.
Roy, A., Pickar, D., Linnoila, M. et al. (1986b) CSF monoamine and metabolite levels and the DSTin depression, Archives of General Psychiatry, 43, 356–60.
Roy, A., Karoum, F. and Pollack, S. (1992) Marked reduction in indices of dopamine metabolismamong patients with depression who attempt suicide, Archives of General Psychiatry, 49,447–50.
Roy-Byrne, P., Uhde, T.W., Gold, P.W. et al. (1985a) Neuroendocrine abnormalities in panicdisorder, Psychopharmacology Bulletin, 21, 546–50.
Roy-Byrne, P., Bierer, L.M. and Uhde, T.W. (1985b) The DST in panic disorder, Biological Psychiatry,20, 1237–40.
Rubin, E., Sackhein, H.A., Nobler, M.S. et al. (1994) Brain imaging studies of antidepressanttreatments, Psychiatric Annals, 24, 653–8.
Rubinow, D.R., Gold, P.W., Post, R.M. et al. (1985) Somatostatin in patients with affective illnessand normal volunteers. In R.M. Post and J.C. Ballenger (eds.), Neurobiology of Mood Disorders,Williams and Wilkins, Baltimore, MD, pp. 369–87.
Ruby, N.F., Hwang, C.E., Wessells, C. et al. (2008) Hippocampal-dependent learning requiresa functional circadian system, Proceeding of the national Academic of Sciences’ U S A, 105(15),593–8.
Rudorfer, M.V., Hwu, H. and Clayton, P.J. (1982) DST in primary depression: significance of familyhistory and psychosis, Biological Psychiatry, 17, 41–8.
Rudorfer, M.V., Risby, E.D., Hsiao, J.K. et al. (1988) ECT alters human monoamines in a differentmanner from antidepressant drugs, Psychopharmacology Bulletin, 24, 396–9.
Ruocco, A.C. (2005) The neuropsychology of borderline personality disorder: a meta-analysis andreview, Psychiatry Research, 137, 191–202.
Ruocco, A.C. et al. (2006) Clinical presentation of juvenile Huntington disease, Arquivos de Neuro-Psiquiatr, 64(1), doi: 10.1590/S0004-282X2006000100002.

References 379
Rusch, N., Tebartz van Elst, L., Baeumer, D. et al. (2004) Absence of cortical gray matter abnormal-ities in psychosis of epilepsy: a voxel-based MRI study in patients with temporal lobe epilepsy,Journal of Neuropsychiatry Clinical neuroscience, 16(2), 148–55.
Rush, A.J., Giles, D.E., Roffwarg, H.P. et al. (1982) Sleep EEG and DST findings in out patients withunipolar major depressive disorders, Biological Psychiatry, 17, 327–41.
Rush, A.J., George, M.S., Sackeim, H.A. et al. (2000) Vagus nerve stimulation (VNS) for treatment-resistant depressions: a multicenter study, Boilogical Psychiatry, 47, 276–86.
Rush, A.J., Marangell, L.B., Sackeim, H.A. et al. (2005) Vagus nerve stimulation for treatment-resistant depression: a randomized, controlled acute phase trial, Biological Psychiatry, 58,347–54.
Rush, A.J., Trivedi, M.H., Wisniewski, S.R. et al. (2006) Bupropion-SR, sertraline, or venlafaxine-XRafter failure of SSRIs for depression, New England Journal of Medicine, 354, 1231–42.
Rutecki, P. (1990) Anatomical, physiological and theoretical basis for the antiepileptic effect ofvagus nerve stimulation, Epilepsia, 31, S1–36.
Rutter, M. (1994) Psychiatric genetics: research challenges and pathways forward, American Journalof Medical Genetics, 54, 185–98.
Rutter, M. and McGuffin, P. (2004) The social, genetic and developmental psychiatry centre: itsorigins, conception and initial accomplishments, Psychological Medicine, 34, 933–47.
Sabelli, H.C., Fawcett, J., Gusovsky, F. et al. (1983) Urinary phenyl acetate: a diagnostic test fordepression, Science, 220, 1187–8.
Sabol, S.Z., Nelson, M.L., Fisher, C. et al. (1999) A genetic association for cigarette smoking behavior,Health Psychology, 18, 7–13.
Sachar, E.J., Hellman, L., Roffwarg, H. et al. (1973) Disrupted 24 hour patterns of cortisol secretionin psychotic depression, Archives of General Psychiatry, 28, 19–24.
Sachdev, P.S., McBride, R., Loo, C.K. et al. (2001) Right versus left prefrontal transcranial magneticstimulation for obsessive–compulsive disorder: a preliminary investigation, Journal of ClinicalPsychiatry, 62, 981–4.
Sackeim, H.A., Keilp, J.G., Rush, A.J. et al. (2001a) The effects of vagus nerve stimulation on cogni-tive performance in patients with treatment-resistant depression, Neuropsychiatry NeuropsycholBehavioral Neurology, 14, 53–62.
Sackeim, H.A., Rush, A.J., George, M.S. et al. (2001b) Vagus nerve stimulation (VNS) for treatment-resistant depression: efficacy, side effects, and predictors of outcome, Neuropsychopharmacology,25, 713–28.
Sackeim, H.A., Prudic, J., Nobler, M.S. et al. (2008) Effects of pulse width and electrode placementon the efficacy and cognitive effects of electroconvulsive therapy, Brain Stimulation, 1, 71–83.
Sacks, O. (1973) Awakenings, Duckworth, London.Saleem, P.T. (1984) Dexamethasone Suppression Test in depressive illness: its relation to anxiety
symptoms, British Journal of Psychiatry, 144, 181–4.Saletu, B., Grunberger, J. and Rajna, P. (1983) Pharmaco-EEG profiles with antidepressants, British
Journal of Clinical Pharmacology, 15, S 369–84.Salinsky, M.C., Uthman, B.M., Ristanovic, R.K. et al. for the Vagus Nerve Stimulation Study Group
(1996) Vagus nerve stimulation for the treatment of medically intractable seizures: results of a1-year open-extension trial, Archives of Neurology, 53, 1176–80.
Sanacora, G., Fenton, L.R., Fasula, M.K. et al. (2006) Cortical gamma-aminobutyric acid concen-trations in depressed patients receiving cognitive behavioral therapy, Biological Psychiatry, 59,284–6.
Sanacora, G., Mason, G.F., Rothman, D.L. et al. (2002) Increased occipital cortex GABA concentra-tions in depressed patients after therapy with selective serotonin reuptake inhibitors, AmericanJournal of Psychiatry, 159, 663–5.

380 References
Sanacora, G., Zarate, C.A., Krystal, J.H. et al. (2008) Targeting the glutamatergic system to developnovel, improved therapeutics for mood disorders, Nature Reviews: Drug Discovery, 7, 426–37.
Sandler, M. (1983) Benzodiazepines: studies on a possible endogenous ligand. In M.R. Trimble(ed.), Benzodiazepines Divided, John Wiley and Sons, Chichester, pp. 139–47.
Sandler, M., Bonham Carter, S., Cuthbert, M.F. et al. (1975) Is there an increase in monoamineoxidase activity in depressive illness?, Lancet, i, 1045–8.
Santarelli, L., Saxe, M., Gross, C. et al. (2003) Requirement of hippocampal neurogenesis for thebehavioral effects of antidepressants, Science, 301, 805–9.
Saper, C. (1996) The role of the cerebral cortex in cerebral expression. In G. Holstege, R. Bandlerand C.B. Saper (eds.), The Emotional Motor System, Elsevier, Amsterdam.
Sapolsky, R.M. (1996) Why stress is bad for your brain, Science, 273, 749–50.Sapolsky, R.M., Krey, L.C. and McEwen, B.S. (1985) Prolonged glucocorticoid exposure reduces
hippocampal neurone number, Journal of Neuroscience, 5, 1222–7.Saver, J.L. and Rabin, J. (1997) The neural substrates of religious experience, Journal of Neuropsychi-
atry and Clinical Neuroscience, 9, 498–510.Savitz, J., Lucki, I. and Drevets, W.C. (2009) 5-HT(1A) receptor function in major depressive
disorder, Progress Neurobiology, 88, 17–31.Sawyer, C.H. (1957) Triggering of the pituitary by the CNS. In P. Bullock (ed.), Physiological Triggers,
Waverly Press, Baltimore, MD, pp. 164–74.Scatton, B. and Zivkovic, B. (1984) Neuroleptics and the limbic system. In M.R. Trimble and
E. Zarifian (eds.), Psychopharmacology of the Limbic System, Oxford University Press, Oxford, pp.174–97.
Schaer, M. and Eliez, S. (2007) From genes to brain: understanding brain development in neu-rogenetic disorders using neuroimaging techniques, Child Adolescent Psychiatric Clinic of NorthAmerica, 16, 557–79.
Schatzberg, A.F. and Lindley, S. (2008) Glucocorticoid antagonists in neuropsychiatric [corrected]disorders, European Journal Of Pharmacology, 583, 358–64.
Schatzberg, A.F., Rothschild, A.J., Gershon, B. et al. (1985) Toward a biochemical classification ofdepressive disorders, British Journal of Psychiatry, 146, 633–7.
Schmahmann, J.D. (1991) An emerging concept: the cerebellar contribution to higher functions,Archives of Neurology, 48, 1178–87.
Scarpa, A. and Raine, A. (1997) Psychophysiology of anger and violent behavior, Psychiatric Clinicsof North America, 20, 375–94.
Scher, M., Krieg, J.N. and Juergens, S. (1983) Trazadone and priapism, American Journal of Psychiatry,140, 1362–3.
Scher, A.I., Xu, Y., Korf, E.S. et al. (2007) Hippocampal shape analysis in Alzheimer’s disease: apopulation-based study, Neuroimage, 36, 8–18.
Schildkraut, J.J. and Kety, S.S. (1967) Biogenic amines and emotion, Science, 156, 21–30.Schildkraut, J.J., Orsulak, P.J., Schatzberg, A.F. et al. (1984) Urinary MHPG in affective disorders.
In R.M. Post and J.C. Ballenger (eds.), Neurobiology of Mood Disorders, Williams and Wilkins,Baltimore, MD, pp. 519–628.
Schipper, H.M. (2007) The role of biologic markers in the diagnosis of Alzheimer’s disease,Alzheimers Dement, 3, 325–332.
Schipper, H.M. (2009) Apolipoprotein E: implications for Alzheimer’s Disease neurobiology,epidemiology and risk assessment, Neurobiol Aging (epub ahead of print, PMID: 19482376).
Schmitz, B. and Trimble, M.R. (2007) Psychoses. In P. Engel et al., Epilepsy: A Comprehnesive Textbook,2nd edition, Lippincott Williams & Wilkins, New York, NY.
Schmitz, B. and Wolf, P. (1991) Psychoses in epilepsy. In O. Devinsky and W.H. Theodore (eds.),Epilepsy and Behaviour, Wiley-Liss, New York, NY, pp. 97–128.

References 381
Schmitz, B. and Wolf, P. (1995) Psychosis with epilepsy: frequency and risk factors, Journal ofEpilepsy, 8, 295–305.
Schmitz, B., Moriarty, J., Costa, D.C. et al. (1997) Psychiatric profiles and patterns of cerebral bloodflow in focal epilepsy: interactions between depression, obsessionality, and perfusion related tothe laterality of the epilepsy, Journal of Neurological Neurosurgery Psychiatry, 62, 458–63.
Schmitz, B., Robertson, M. and Trimble, M.R. (1999) Depression and schizophrenia in epilepsy:social and biological risk factors, Epilepsy Research, 35, 59–68.
Schneider, K. (1957) Primary and secondary symptoms in schizophrenia. In S.R. Hirsch andM. Shepherd (eds.), Themes and Variations in European Psychiatry, John Wright, Bristol, pp. 40–6.
Schneider, K. (1959) Clinical Psychopathology (Translated by M.W. Hamilton and E.W. Anderson),Grune and Stratton, New York, NY.
Schooler, C., Zahn, T.P., Murphy, D.I. et al. (1978) Psychological correlates of monoamine oxidaseactivity in normals, Journal of Nervous and Mental Disease, 166, 177–86.
Schreiner, L. and Kling, A. (1956) Rhinencephalon and behaviour, American Journal of Psychiatry,184, 486–90.
Schwartz, J.H. (1981) Chemical basis of synaptic transmission. In E.R. Kandel and J.H. Schwartz(eds.), Principles of Neural Science, Elsevier, North Holland, pp. 106–20.
Schwartz, M.F., Bauman, J.E. and Masters, W.H. (1982) Hyperprolactinaemia and sexual disordersin men, Biological Psychiatry, 17, 861–76.
Seeman, P. (1992) Dopamine receptor sequences: therapeutic levels of neuroleptics occupy D2
receptors, clozapine occupies D4, Neuropsychopharmacology, 7, 261–84.Severino, G., Manchia, M., Contu, P. et al. (2009) Association study in a Sardinian sample between
bipolar disorder and the nuclear receptor REV-ERBalpha gene, a critical component of thecircadian clock system, Bipolar Disorders, 11, 215–20.
Shagass, C. (1972) Evoked Brain Potentials in Psychiatry, Plenum Press, New York, NY.Shagass, C., Roemer, R.A., Straumanis, J.J. et al. (1979) Evoked potential evidence of lateralised
hemispheric dysfunction in the psychoses. In J. Gruzelier and P. Flor-Henry (eds.), HemisphereAsymmetries of Function in Psychopathology, Elsevier, North Holland, pp. 293–316.
Shagass, C., Roemer, R.A., Straumanis, J.J. et al. (1981) Differentiation of depressive andschizophrenic psychoses by evoked potentials, Advances in Biological Psychiatry, 6,173–9.
Shah, S.A., Doraiswany, P.M., Hussain, M.M. et al. (1992) Posterior fossa abnormalities in majordepression, Acta Psychiatrica Scandinavica, 85, 474–9.
Shajahan, P.M., Glabus, M.F., Steele, J.D. et al. (2002) Left dorso-lateral repetitive transcranialmagnetic stimulation affects cortical excitability and functional connectivity, but does not impaircognition in major depression, Progress in Neuropsychopharmacology and Biological Psychiatry, 26,945–54.
Shalev, A.Y., Videlock, E.J., Peleg, T. et al. (2008) Stress hormones and post-traumatic stress disorderin civilian trauma victims: a longitudinal study: part I. HPA axis responses, International JournalNeuropsychopharmacol, 11, 365–72.
Shane, M.S., Stevens, M., Harenski, C.L. et al. (2008) Neural correlates of the processing of another’smistakes: a possible underpinning for social and observational learning, Neuroimage, 42, 450–9.
Shapira, B., Lerer, B., Kindler, S. et al. (1992) Enhanced serotonergic responsivity following ECT inpatients with major depression, British Journal of Psychiatry, 16, 233–9.
Shapiro, D. (1999) Neurotic Styles, New York, NY, Basic Books.Shaw, D.M., Camps, F.E. and Eccleston, E.G. (1967) 5-hydroxytryptamine in the hind-brains of
depressive suicides, British Journal of Psychiatry, 113, 1407–11.

382 References
Sheline, Y.I., Sanghavi, M., Mintun, M.A. et al. (1999) Depression duration but not age predictshippocampal volume loss in medically healthy women with recurrent major depression, Journalof Neuroscience, 19, 5034–43.
Shelley, B.P. and Trimble, M.R. (2004) The insular lobe of Reil – its anatamico-functional,behavioural and neuropsychiatric attributes in humans – a review, World Journal of BiologicalPsychiatry, 5, 176–200.
Shelley, B.P., Trimble, M.R. and Boutros, N.N. (2008) Electroencephalographic cerebral dysrhyth-mic abnormalities in the trinity of nonepileptic general population, neuropsychiatric, andneurobehavioral disorders, Journal of Neuropsychiatry of Clinical Neuroscience, 20, 7–22.
Shen, D., Liu, D., Liu, H. et al. (2004) Automated morphometric study of brain variation in XXYmales, Neuroimage, 23, 648–53.
Sher, L., Mann, J.J., Traskman-Bendz, L. et al. (2006) Lower cerebrospinal fluid homovanillic acidlevels in depressed suicide attempters, Journal of Affective Disorder, 90, 83–9.
Shi, J., Wittke-Thompson, J.K., Badner, J.A. et al. (2008) Clock genes may influence bipolar disordersusceptibility and dysfunctional circadian rhythm, American Journal of Medical Genetics. Part B:Neuropsychiatric Genetics, 147b, 1047–55.
Shibasaki, J., Barrett, G., Halliday, E. et al. (1980) Components of the movement-related corticalpotential and their scalp topography, Electroencephalography and Clinical Neurophysiology, 49,213–26.
Shields, J. (1954) Personality differences and neurotic traits in normal twin schoolchildren, EugenicsReview, 45, 213–46.
Shields, J. (1962) Monozygotic Twins Brought Up Apart and Brought Up Together, Oxford UniversityPress, London.
Shihabuddin, L., Buchsbaum, M.S., Brickman, A.M. et al. (2001) Diffusion tensor imaging inKraepelinian and non-Kraepelinian Schizophrenia, Biological Psychiatry, 49, 19–67.
Shoghi-Jadid, K., Barrio, J.R., Kepe, V. et al. (2005) Imaging beta-amyloid fibrils in Alzheimer’sdisease: a critical analysis through simulation of amyloid fibril polymerization, Nuclear MedicalBiology, 32, 337–51.
Shopsin, B., Friedman, E. and Gershon, S. (1976) Parachlorophenylalanine reversal of tranyl-cypramine effects in depressed patients, Archives of General Psychiatry, 33, 811–19.
Shorvon, S.D. and Reynolds, E.H. (1982) Early prognosis of epilepsy, British Medical Journal, ii,1699–701.
Sibley, D.R. and Monsma, F.J. (1992) Molecular biology of dopamine receptors, TIPS, 13, 61–9.Siegel, A., Edinger, H. and Dotto, M. (1975) Effects of electrical stimulation of the lateral aspects of
the pre-frontal cortex upon attack behaviour in cats, Brain, 93, 473–84.Siegel, B.V.J., Buchsbaum, M.S., Bunney, W.E.J. et al. (1993) Cortical-striatal-thalamic circuits and
brain glucose metabolic activity in 70 unmedicated male schizophrenic patients, American Journalof Psychiatry, 150, 1325–36.
Siesjo, B.K. (1978) Brain Energy Metabolism, John Wiley and Sons, Chichester.Siever, L.J. and Coursey, R.D. (1985) Biological markers for schizophrenia and the biological
high-risk approach, Journal of Nervous and Mental Disease, 173, 4–16.Siever, L.J. and Uhde, T.W. (1984) New studies and perspectives on the noradrenergic receptor
system in depression: effects of the alpha-2 adrenergic agonist clonidine, Biological Psychiatry,19, 131–56.
Siever, L.J., Insel, T.R., Jimerson, D.C. et al. (1983) Growth hormone response to clonidine inobsessive–compulsive patients, British Journal of Psychiatry, 142, 184–7.
Silbersweig, D., Clarkin, J.F., Goldstein, M. et al. (2007) Failure of frontolimbic inhibitory function inthe context of negative emotion in borderline personality disorder, American Journal of Psychiatry,164, 1832–41.

References 383
Sim, M. (1979) Early diagnosis of Alzheimer’s disease. In A. Glen and L.J. Whalley (eds.), Alzheimer’sDisease, Churchill Livingstone, Edinburgh, pp. 78–85.
Skare, S.S., Dysken, M.W. and Billington, C.J. (1994) A review of the GHRH stimulation test inpsychiatry, Biological Psychiatry, 36, 249–65.
Skuse, D. (2006) Genetic influences on the neural basis of social cognition, Philosophical Transactionsof the Royal Society London B Biological Science, 361, 2129–41.
Skuse, D.H. (2007) Rethinking the nature of genetic vulnerability to autistic spectrum disorders,Trends Genet, 23, 387–95.
Slade, A.P. and Checkley, S.A. (1980) A neuroendocrine study of the mechanism of action of ECT,British Journal of Psychiatry, 137, 217–21.
Slater, E. and Beard, A.W. (1963) The schizophrenia-like psychoses of epilepsy, British Journal ofPsychiatry, 109, 95–150.
Slater, E. and Roth, M. (1960) Clinical Psychiatry, 1st edition, Bailliere Tindall and Cassell, London.Slater, E. and Roth, M. (1969) Clinical Psychiatry, 3rd edition, Bailliere Tindall and Cassell, London.Small, J.G. (1970) Small sharp spikes in a psychiatric population, Archives of General Psychiatry, 22,
277–84.Small, J.G., Small, I.F., Milstein, V. et al. (1975) Familial associations with EEG variants in manic
depressive disease, Archives of General Psychiatry, 32, 43–8.Small, J.G., Milstein, V., Klapper, M.H. et al. (1986) ECT for manic episodes. In S. Malitz and H.A.
Sackeim (eds.), ECT, Annals of the New York Academy of Science, Vol. 462, pp. 37–49.Small, G.W., Ercoli, L.M., Silverman, D.H. et al. (2000) Cerebral metabolic and cognitive decline in
persons at genetic risk for Alzheimer’s disease, Proceedings of National Academy of Sciences, U SA, 97(11), 6037–42.
Smith, D.A. and Lantos, P.L. (1983) A case of combined Pick’s disease and Alzheimer’s disease,Journal of Neurology, Neurosurgery and Psychiatry, 46, 675–7.
Smolka, M.N., Buhler, M., Schumann, G. et al. (2007) Gene–gene effects on central processing ofaversive stimuli, Molecular Psychiatry, 12, 307–17.
Smythies, J.R. (1976) Recent progress in schizophrenia research, Lancet, ii, 136–9.Smythies, J. (2002) The Dynamic Neuron, MIT Press, Cambridge, MA.Snyder, S.H., Banerjee, S.P., Yamamura, H. I et al. (1974) Drugs, neurotransmitters and schizophre-
nia, Science, 184, 1243–53.Sobin, C., Blundell, M.L., Weiller, F., Gavigan, C. et al. (2000) Evidence of a schizotypy subtype in
OCD, Journal of Psychiatry Research, 34, 15–24.Soeteman, D.I., Hakkaart-Van Roijen, L., Verheul, R. et al. (2008) The economic burden of personality
disorders in mental health care, Journal of clinical Psychiatry, 69, 259–65.Sohal, V.S., Zhang, F., Yizhar, O. et al. (2009) Parvalbumin neurons and gamma rhythms enhance
cortical circuit performance, Nature, 459(7247), 698–702.Sokoloff, L.M., Reivich, C., Kennedy, M.H. et al. (1977) The 14C deoxyglucose method for the
measurement of local cerebral glucose utilisation, Journal of Neurochemistry, 28, 897–916.Soloff, P.H., Meltzer, C.C., Greer, P.J. et al. (2000) A fenfluramine-activated FDG-PET study of
borderline personality disorder, Biological Psychiatry, 47, 540–7.Soloff, P.H., Price, J.C., Meltzer, C.C. et al. (2007) 5HT2A receptor binding is increased in borderline
personality disorder, Biological Psychiatry, 62, 580–7.Sørensen, B., Kragh-Sørensen, P., Larsen, N.E. et al. (1978) The practical significance of nortriptyline
plasma control: a prospective evaluation under routine conditions in endogenous depression,Psychopharmacology (Berl), 59(1), 35–9.
Southwick, S.M., Krystal, J.H., Morgan, A. et al. (1993) Abnormal noradrenergic function inpost-traumatic stress disorder, Archives of General Psychiatry, 50, 266–74.

384 References
Soyka, M., Preuss, U.W., Koller, G. et al. (2002) Dopamine D 4 receptor gene polymorphism andextraversion revisited: results from the Munich gene bank project for alcoholism, Journal ofPsychiatric Research, 36, 429–35.
Spar, J.E. and Gerner, R. (1982) Does the DST distinguish dementia from depression?, AmericanJournal of Psychiatry, 139, 238–40.
Speer, A.M., Kimbrell, T.A., Wasserman, E.M. et al. (2000) Opposite effects of high and lowfrequency rTMS on regional brain activity in depressed patients, Biological Psychiatry, 48(23),1133–41.
Spiegelhalder, K., Hornyak, M., Kyle, S.D. et al. (2009) Cerebral correlates of heart rate variationsduring a spontaneous panic attack in the fMRI scanner, Neurocase, 1–8.
Squire, L.R., Shimamura, A.P. and Amaral, D.G. (1989) Memory and the hippocampus. In J. Byrneand W. Berry (eds.), Neural Models of Plasticity, Academic Press, New York, NY, pp. 208–40.
Stafford-Clarke, D. and Taylor, F.H. (1949) Clinical and EEG studies of prisoners charged withmurder, Journal of Neurology, Neurosurgery and Psychiatry, 12, 325–30.
Stanley, M. and Mann, J.J. (1983) Increased serotonin-2 binding sites in frontal cortex of suicidevictims, Lancet, i, 214–16.
Stanley, B., Molcho, A., Stanley, M. et al. (2000) Association of aggressive behavior with alteredserotonergic function in patients who are not suicidal, American Journal of Psychiatry, 157, 609–14.
Stanton, P.K. and Sejnowsky, T.J. (1989) Associative long-term depression in the hippocampusinduced by Hebbian covariance, Nature, 339, 215–18.
Stark, A.K., Uylings, H.B., Sanz-Arigita, E. et al. (2004) Glial cell loss in the anterior cingulatecortex, a subregion of the prefrontal cortex, in subjects with schizophrenia, American Journal ofPsychiatry, 161, 882–8.
Starkman, M.N., Giordani, B., Gebarski, S.S. et al. (1999) Decrease in cortisol reverses human hip-pocampal atrophy following treatment of Cushing’s disease, Biological Psychiatry, 46, 1595–602.
Starkstein, S.E. and Robinson, R.G. (1993) Depression in cerebrovascular disease. In S.E. Starksteinand R.G. Robinson (eds.), Depression in Neurologic Disease, Johns Hopkins Press, Baltimore, MD,pp. 28–49.
Starkstein, S.E., Preziosi, T.J., Bolduc, P.L. et al. (1990) Depression in Parkinson’s disease, Journal ofNervous and Mental Disease, 178, 27–31.
St Clair, D.M., Blackwood, D.H.R. and Christie, J.E. (1985) P3 and other long latency auditoryevoked potentials in presenile dementia, Alzheimer-type and the alcoholic Korsakoff syndrome,British Journal of Psychiatry, 147, 702–6.
Stefansson, S.B., Olafsson, E. and Hauser, W.A. (1998) Psychiatric morbidity in epilepsy: a casecontrolled study of adults receiving disability benefits, Journal of Neurology, Neurosurgery andPsychiatry, 64, 238–41.
Stefansson, H., Ophoff, R.A., Steinberg, S. et al. (2009) Common variants conferring risk ofschizophrenia, Nature, 460, 744–7.
Stein, D.J. and Ythilingum, B. (2009) Love and attachment: the psychobiology of social bonding,CNS Spectrums, 14(5), 239–42.
Stern, R.S. and Cobb, J.P. (1978) Phenomenology of obsessive compulsive neurosis, British Journalof Psychiatry, 132, 233–9.
Stern, E., Silbersweig, D.A., Chee, K.Y. et al. (2000) A functional neuroanatomy of tics in tourettesyndrome, Archives in General Psychiatry, 57, 741–8.
Stevens, J.R. (1979) All that spikes is not fits. In C. Shagass, S. Gershon and A.J. Friedhoff (eds.),Psychopathology and Brain Dysfunction, Raven Press, New York, NY, pp. 183–98.
Stevens, J.R. (1986) Epilepsy and psychosis: neuropathological studies of six cases. In M.R. Trimbleand T. Bolwig (eds.), Aspects of Epilepsy and Psychiatry, John Wiley and Sons, Chichester, pp.117–45.

References 385
Stevens, J.R. and Hermann, B.P. (1981) Temporal lobe epilepsy, psychopathology and violence; thestate of the evidence, Neurology, 31, 1127–32.
Stevens, J.R. and Livermore, A. (1978) Kindling in the mesolimbic dopamine system: animal modelof psychosis, Neurology, 28, 36–46.
Stewart, L., Walsh, V., Frith, U. et al. (2001) TMS produces two dissociable types of speechdisruption, Neuroimage, 13, 472–8.
Strafella, A.P., Paus, T., Barrett, J. et al. (2001) Repetitive transcranial magnetic stimulation of thehuman prefrontal cortex induces dopamine release in the caudate nucleus, Journal of Neuroscience,21, RC157.
Strakowski, S.M., Woods, B.T., Tohen, S.M. et al. (1993) MRI subcortical hyperintensities in maniaat first hospitalisation, Biological Psychiatry, 33, 204–6.
Struve, F.A. and Willner, A.E. (1983) Cognitive dysfunction and tardive dyskinesia, British Journalof Psychiatry, 143, 597–600.
Struve, F.A., Saraf, K.R., Arko, R.S. et al. (1979) Relationships between paroxysmal electroen-cephalographic dysrythmia and suicide ideation and attempts in psychiatric patients. In C.Shagass, S. Gershon and A.J. Friedhoff (eds.), Psychopathology and Brain Dysfunction, RavenPress, New York, NY, pp. 199–221.
Stuss, D.T. and Benson, D.F. (1984) Neuropsychological studies of the frontal lobes, PsychologicalBulletin, 95, 3–28.
Su, Y., Burke, J., O’Neill, A. et al. (1993) Exclusion of linkage between schizophrenia and the D2dopamine receptor gene region, Archives of General Psychiatry, 50, 205–11.
Sulser, F. (1984) Regulation and function of noradrenaline receptor in systems in brain, Neurophar-macology, 23(2B), 255–61.
Svrakic, D.M., Whitehead, C., Przybeck, T.R. et al. (1993) Differential diagnosis of personalitydisorders by the seven-factor model of temperament and character, Archives of General Psychiatry,50, 991–9.
Swedo, S.E., Rapoport, J.L., Cheslow, D.L. et al. (1989a) High prevalence of obsessive–compulsivesymptoms in patients with Sydenham’s chorea, American Journal of Psychiatry, 146, 246–9.
Swedo, S.E., Schapiro, M.B., Grady, C.L. et al. (1989b) Cerebral glucose metabolism in childhoodonset OCD, Archives of General Psychiatry, 46, 518–23.
Swedo, S.E., Leonard, H.L., Kraesi, M.J.P. et al. (1992) CSF neurochemistry in children andadolescents with obsessive–compulsive disorder, Archives of General Psychiatry, 49, 29–36.
Sydenham, T. (1740) The Whole Works, 11th edition, J. Pechey, Ware, London.Symonds, C. (1962), The schizophrenia-like psychoses of epilepsy: discussion, Proceedings of the
Royal Society of Medicine, 55, 311.Szasz, T.S. (1976) Schizophrenia: the sacred symbol of psychiatry, British Journal of Psychiatry, 129,
308–16.Szigethy, E., Conwell, Y., Forbes, N.T. et al. (1994) Adrenal weight and morphology in victims of
completed suicide, Biological Psychiatry, 36, 374–80.Szyf, M., McGowan, P. and Meaney, M.J. (2008) The social environment and the epigenome,
Environmental and Molecular Mutagenesis, 49, 46–60.Tajima, K., Diaz-Marsa, M., Montes, A. et al. (2009) Neuroimaging studies in borderline personality
disorder, Actas Espanolas de Psiquiatria, 37, 123–7.Takahashi, S., Kondo, H. and Kato, N. (1975) Effect of L-5HTP on brain monoamine metabolism
and evaluation of its clinical effect in depressed patients, Journal of Psychiatric Research, 12,177–87.
Talairach, J., Bancaud, J., Geier, S. et al. (1973) The cingulate gyrus and human behaviour,Electroencephalography and Clinical Neurophysiology, 34, 45–52.
Tamminga, R.C., Smith, R.C. et al. (1976) Depression associated with oral choline, Lancet, ii, 905.

386 References
Tan, H.Y., Callicott, J.H. and Weinberger, D.R. (2008) Intermediate phenotypes in schizophreniagenetics redux: is it a no brainer?, Molecular Psychiatry, 13, 233–8.
Tandon, R., Keshavan, M.S. and Nasrallah, H.A. (2008) Schizophrenia, ‘just the facts’: what weknow in 2008: 2. Epidemiology and etiology, Schizophrenia Research, 102, 1–18.
Targum, S.D., Rosen, L. and Capodanno, A.E. (1983a) The dexamethasone suppression test insuicidal patients with unipolar depression, American Journal of Psychiatry, 140, 877–9.
Targum, S.D., Rosen, L.N., Delisi L.E. et al. (1983b) Cerebral ventricular size in major depressivedisorder: association with delusional symptoms, Biological Psychiatry, 18, 329–36.
Taylor, D.C. (1975) Factors influencing the occurrence of schizophrenia-like psychosis in patientswith TLE, Psychological Medicine, 5, 249–54.
Taylor, J. (1958) Selected Writings of John Hughlings Jackson, Basic Books, New York, NY.Taylor, M.A. and Abrams, R. (1984) Cognitive impairment in schizophrenia, American Journal of
Psychiatry, 141, 196–201.Taylor, P. and Fleminger, J.J. (1980) ECT for schizophrenia, Lancet, i, 1380–3.Tebartz van Elst, L., Woermann, F., Lemieux, L. et al. (2000) Affective aggression in patients with
temporal lobe epilepsy: a quantitative magnetic resonance study of the amygdala, Brain, 123,234–43.
Tebartz van Elst, L. and Thiel, T. (2001) Subtle prefrontal neuropathology in a pilot MRS study inpatients with borderline personality disorder, Journal of Neuropsychiatry and Clinical Neuroscience,13, 511–14.
Tebartz van Elst, L., Hesslinger, B., Thiel, T. et al. (2003) Frontolimbic brain abnormalities in patientswith borderline personality disorder: a volumetric magnetic resonance imaging study, BiologicalPsychiatry, 54, 163–71.
Tellez-Zenteno, J.F., Patten, S.B. and Wiebe, S. (2005) Pychiatric comorbidity in epilepsy: apopulation-based analysis, Epilepsia, 46, Suppl. 8, 264.
Temkin, O. (1971) The Falling Sickness, Johns Hopkins Press, Baltimore, MD.Teneback, C.C., Nahas, Z., Speer, A.M. et al. (1999) Two weeks of daily left prefrontal rTMS
changes prefrontal cortex and paralimbic activity in depression, Journal of NeuropsychiatryClinical Neuroscience, 11, 426–35.
Thaker, G.K. (2008) Neurophysiological endophenotypes across bipolar and schizophrenia psy-chosis, Schizophrenia Bulletin, 34, 760–73.
Thaker, G.K., Tamminga, C.A., Alphs, L.D. et al. (1987) Brain GABA abnormality in tardivedyskinesia, Archives of General Psychiatry, 44, 522–31.
Theodore, W.H., Hasler, G., Giovacchini, G. et al. (2007) Reduced hippocampal 5HT1A PET receptorbinding and depression in temporal lobe epilepsy, Epilepsia, 48, 1526–30.
Thome, J., Weijers, H.G., Wiesbeck, G.A. et al. (1999) Dopamine D3 receptor gene polymorphismand alcohol dependence: relation to personality rating, Psychiatr Genet, 9, 17–21.
Thompson, P.J. and Trimble, M.R. (1982a) Anticonvulsant drugs and cognitive functions, Epilepsia,23, 531–44.
Thompson, P.J. and Trimble, M.R. (1982b) Non-MAOI antidepressant drugs and cognitive function:a review, Psychological Medicine, 12, 539–48.
Thoren, P., Asberg, M., Cronholm, B. et al. (1980a) Clomipramine treatment ofobsessive–compulsive disorder: I. Controlled clinical trial, Archives of General Psychiatry,37, 1281–5.
Thoren, P., AAsberg, M., Bertilsson, L. et al. (1980b) Clomipramine treatment ofobsessive–compulsive disorder: II. Biochemical aspects, Archives of General Psychiatry,37, 1289–94.
Thorgeirsson, T.E., Geller, F., Sulem, P. et al. (2008) A variant associated with nicotine dependence,lung cancer and peripheral arterial disease, Nature, 452, 638–42.

References 387
Tienari, P. (1963) Psychiatric illness in identical twins, Acta Psychiatrica Scandinavica, 391,Suppl. 171.
Todes, C.J. and Lees, A.J. (1985) The premorbid personality of patients with Parkinson’s disease,Journal of Neurology, Neurosurgery and Psychiatry, 48, 97–100.
Todrick, A. and Tait, A.C. (1969) The inhibition of human platelet 5HT uptake by tricyclicantidepressive drugs, Journal of Pharmacy and Pharmacology, 21, 751–62.
Tomlinson, B.E. (1982) Plaques, tangles and Alzheimer’s disease, Psychological Medicine, 12, 449–59.Toone, B. (1981) Psychoses of epilepsy. In E.H. Reynolds and M.R. Trimble (eds.), Epilepsy and
Psychiatry, Churchill Livingstone, Edinburgh, pp. 113–37.Toone, B.K., Dawson, J. and Driver, M. (1982a) Psychoses of epilepsy: a radiological evaluation,
British Journal of Psychiatry, 140, 244–8.Toone, B.K., Garralda, M.E. and Ron, M.A. (1982b) The psychosis of epilepsy and the functional
psychoses: a clinical and phenomenological comparison, British Journal of Psychiatry, 141,256–61.
Torgersen, S. (2000) Genetics of patients with borderline personality disorder, Psychiatrical Clinicsof north America, 23, 1–9.
Torgersen, S., Lygren, S., Oien, P.A. et al. (2000) A twin study of personality disorders, ComprehensivePsychiatry, 44, 416–25.
Toulopoulou, T., Quraishi, S., McDonald, C. et al. (2006) The Maudsley family study: premorbidand current general intellectual function levels in familial bipolar I disorder and schizophrenia,Journal of Clinical and Experimental Neuropsychology, 28, 243–59.
Traskman, L., Tybring, G., AAberg, M. et al. (1980) Cortisol in the CSF of depressed and suicidalpatients, Archives of General Psychiatry, 37, 761–7.
Treffert, D.A. (1964) The psychiatric patient with an EEG temporal lobe focus, American Journal ofPsychiatry, 120, 765–71.
Trimble, M. (1978) Serum prolactin in epilepsy and hysteria, British Medical Journal, 2, 1682.Trimble, M.R. (1980) New antidepressant drugs and the seizure threshold, Neuropharmacology, 19,
1227–8.Trimble, M.R. (1981a) Neuropsychiatry, John Wiley and Sons, Chichester.Trimble, M.R. (1981b) Post-traumatic Neurosis, John Wiley and Sons, Chichester.Trimble, M.R. (1986a) PET in epilepsy. In M.R. Trimble and T. Bolwig (eds.), Aspects of Epilepsy and
Psychiatry, John Wiley and Sons, Chichester, pp. 147–60.Trimble, M.R. (1986b) Recent contributions of benzodiazepines to the management of epilepsy,
Epilepsia, 27, Suppl. 1.Trimble, M.R. (1986c) Hypergraphia. In M.R. Trimble and T. Bolwig (eds.), Aspects of Epilepsy and
Psychiatry, John Wiley and Sons, Chichester, pp. 75–87.Trimble, M.R. (1988) Biological Psychiatry, 1st edition, John Wiley and Sons, Chichester.Trimble, M.R. (1991) The Psychoses of Epilepsy, Raven Press, New York, NY.Trimble, M.R. (1996) Biological Psychiatry, 2nd edition, John Wiley and Sons, Chichester.Trimble, M.R. (1997) Clinical consequences of pharmacology. In J. Engel and T. Pedley (eds.),
Epilepsy: A Comprehensive Textbook, 2nd edition, Lippincott Williams & Wilkins, New York, NY,pp. 2161–70.
Trimble, M.R. (1998) Forced normalisation and the role of anticonvulsants. In M.R. Trimble andB. Schmitz (eds.), Forced Normalisation and Alternative Psychoses of Epilepsy, Wrightson BiomedicalPublishing, Petersfield, pp. 169–78.
Trimble, M.R. (2000) Cognitive and personality profiles in patients with juvenile myoclonicepilepsy. In M.R. Trimble and B. Schmitz (eds.), Juvenile Myoclonic Epilepsy: The Janz Syndrome,Wrightson Biomedical Publishing, Petersfield, pp. 101–9.

388 References
Trimble, M.R. (2007a) Personality disorders in epilepsy. In S.C. Schachter, G.L. Holmes et al.,Behavioral Aspects of Epilepsy, Demos, New York, NY, pp. 253–60.
Trimble, M.R. (2007b) The Soul in the Brain: The Cerebral Basis of Language, Art and Belief , JohnsHopkins Press, Baltimore, MD.
Trimble, M.R. and Freeman, A. (2006) An investigation of religiosity and the Gastaut–Geschwindsyndrome in patients with temporal lobe epilepsy, Epilepsy and Behavior, 9, 407–14.
Trimble, M.R. and Meldrum, B.S. (1979) Monoamines, epilepsy, and schizophrenia. In J. Obiolset al. (eds.), Biological Psychiatry Today, Elsevier, Amsterdam, pp. 470–5.
Trimble, M.R. and Reynolds, E.H. (1976) Anticonvulsant drugs and mental symptoms: a review,Psychological Medicine, 6, 169–78.
Trimble, M.R. and Reynolds, E.H. (1984) Neuropsychiatric toxicity of anticonvulsant drugs. InW.B. Matthews (ed.), Recent Advances in Clinical Neurology, Churchill Livingstone, Edinburgh,pp. 261–80.
Trimble, M.R. and Robertson, M.M. (1986) The psychopathology of tics. In C.D. Marsden (ed.),Movement Disorders, Vol. 2, Butterworths, Kent, pp. 406–20.
Trimble, M.R. and Thompson, P. (1985) Neuropsychiatric aspects of epilepsy. In I. Grant andK. Adams (eds.), Neuropsychological Assessment of Neuropsychiatric Disorders, Oxford UniversityPress, Oxford, pp. 321–48.
Trimble, M.R., Corbett, J.A. and Donaldson, J. (1980) Folic acid and mental symptoms in childrenwith epilepsy, Journal of Neurology, Neurosurgery and Psychiatry, 43, 1030–4.
Tsaung, M.T. (1993) Genotypes, phenotypes, and the brain, British Journal of Psychiatry, 163,299–307.
Tschanz, J.T., Welsh-Bohmer, K.A., Lyketsos, C.G. et al. (2006) Conversion to dementia from mildcognitive disorder: the Cache County study, Neurology, 67, 229–34.
Tsunoda, T., Yoshino, A., Furusawa, T. et al. (2008) Social anxiety predicts unconsciously provokedemotional responses to facial expression, Psychological Behavior, 93, 172–6.
Tucker, G., Detre, T., Harrow, M. et al. (1965) Behaviour and symptoms of psychiatric patients andthe EEG, Archives of General Psychiatry, 12, 278–86.
Tuke, D.H. (1894) Imperative ideas, Brain, 17, 179–97.Tuominen, H.J., Tiihonen, J., Wahlbeck, K. (2006) Glutamatergic drugs for schizophrenia, Cochrane
Database Syst Rev, doi: CD003730.Tyrer, P. (1976) Towards rational therapy with MAOI, British Journal of Psychiatry, 128, 354–60.Tyrer, P.J. and Lader, M.H. (1974) Response to propranolol and diazepam in somatic and psychic
anxiety, British Journal of Psychiatry, 2, 14–16.Tyrer, P.J., Owen, R. and Dawling, S. (1983) Gradual withdrawal of diazepam after long-term
therapy, Lancet, i, 1402–6.Uhde, T.W., Boulenger, J.-P., Vittone, B. et al. (1985) Human anxiety and noradrenergic function.
In P. Pichot (eds.), Psychiatry: The State of the Art, Vol. 2, Plenum, New York, NY, pp. 693–8.Ungerstedt, U. (1971) Stereotaxic mapping of the monoamine pathways in the rat brain, Acta
Physiologica Scandinavica, 197, Suppl. 367, 1–48.Uthman, B.M., Wilder, B.J., Penry, J.K. et al. (1993) Treatment of epilepsy by stimulation of the
vagus nerve, Neurology, 43, 1338–45.Vagus Nerve Stimulation Study Group (1995) A randomized controlled trial of chronic vagus
nerve stimulation for treatment of medically intractable seizures, Neurology, 224, 230.Valli, I., Howes, O., Tyrer, P. et al. (2008) Longitudinal PET imaging in a patient with schizophrenia
did not show marked changes in dopaminergic function with relapse of psychosis, AmericanJournal of Psychiatry, 165, 1613–14.
Vallortigara, G. (2006a) Cerebral lateralization: a common theme in the organization of thevertebrate brain, Cortex, 42, 5–7.

References 389
Vallortigara, G. (2006b) The evolutionary psychology of left and right: costs and benefits oflateralization, Developmental Psychobiological, 48, 418–27.
van Asselt, A.D., Dirksen, C.D., Arntz, A. et al. (2007) The cost of borderline personality disorder:societal cost of illness in BPD-patients, European Psychiatry, 22, 354–61.
van der Kolk, B.A. (1994) The body keeps the score: memory and the evolving psychobiology ofpost-traumatic stress, Harvard Review of Psychiatry, 1, 253–65.
van Haren, N.E., Bakker, S.C. and Kahn, R.S. (2008) Genes and structural brain imaging inschizophrenia, Current Opinion in Psychiatry, 21, 161–7.
van Os, J., Rutten, B.P. and Poulton, R. (2008) Gene–environment interactions in schizophrenia:review of epidemiological findings and future directions, Schizophrenia Bulletin, 34, 1066–82.
van Praag, H.M. (1977a) Significance of biochemical parameters in the diagnosis, treatment andpresentation of depressive disorders, Biological Psychiatry, 12, 101–31.
van Praag, H. M (1977b) The significance of dopamine for the mode of action of neuroleptics andthe pathogenesis of schizophrenia, British Journal of Psychiatry, 130, 463–74.
van Praag, H.M. (1980a) Central monoamine metabolism in depressions: 1. Serotonin and relatedcompounds, Comprehensive Psychiatry, 21, 30–43.
van Praag, H.M. (1980b) Central monoamine metabolism in depressions: 11. Catecholamines andrelated compounds, Comprehensive Psychiatry, 21, 44–54.
van Praag, H.M., van den Burg, W., Bos, E. et al. (1974) 5HTP in combination with clomipraminein ‘therapy resistant’ depression, Psychopharmacologia, 38, 267–9.
van Rijn, S., Aleman, A., Swaab, H. et al. (2006) Klinefelter’s syndrome and schizophrenia-spectrumpathology, British Journal of Psychiatry, 189, 459–61.
van Rijn, S., Aleman, A., Swaab, H. et al. (2008) Effects of an extra X chromosome on languagelateralization: an fMRI study with Klinefelter men (47,XXY), Schizophrenia Research, 101, 17–25.
van ’t Ent, D., Lehn, H., Derks, E.M. et al. (2007) A structural MRI study in monozygotic twinsconcordant or discordant for attention/hyperactivity problems: evidence for genetic and envi-ronmental heterogeneity in the developing brain, Neuroimage, 35, 1004–20.
van Winkel, R., Stefanis, N.C. and Myin-Germeys, I. (2008) Psychosocial stress and psychosis:a review of the neurobiological mechanisms and the evidence for gene–stress interaction,Schizophrenia Bulletin, 34, 1095–105.
Vertes, R.P. (1990) Fundamentals of brainstem anatomy. In W.R. Klemm and R.P. Vertes (eds.),Brainstem Mechanisms of Behaviour, John Wiley and Sons, Chichester, pp. 33–104.
Victoroff, J.I., Benson, F., Grafton, S.T. et al. (1994) Depression in complex partial seizures: elec-troencephalography and cerebral metabolic correlates, Archives of Neurology, 51, 155–63.
Volkow, N.D., Hitzemann, R., Wang, G.J. et al. (1992) Decreased brain metabolism in neurologicallyintact healthy alcoholics, American Journal of Psychiatry, 149(8), 1016–22.
Volkow, N.D., Wang, G.J., Hitzemann, R. et al. (1994) Recovery of brain glucose metabolism indetoxified alcoholics, American Journal of Psychiatry, 151, 178–83.
Vollm, B.A., Taylor, A.N., Richardson, P. et al. (2006) Neuronal correlates of theory of mind andempathy: a functional magnetic resonance imaging study in a nonverbal task, Neuroimage, 29,90–8.
Vollm, B., Richardson, P., McKie, S. et al. (2007) Neuronal correlates of reward and loss in cluster Bpersonality disorders: a functional magnetic resonance imaging study, Psychiatry Research, 156,151–67.
von Economo, C. (1931) Encephalitis Lethargica (Translated by K.O. Newman), Oxford UniversityPress, Oxford.
von Schantz, M. (2008) Phenotypic effects of genetic variability in human clock genes on circadianand sleep parameters, Journal of Genetics, 87, 513–19.

390 References
Waddington, J.L., Youssef, H.A., Molloy, A.G. et al. (1985) Association of intellectual impairment,negative symptoms, and aging with tardive dyskinesia: clinical and animal studies, Journal ofClinical Psychiatry, 46, 29–33.
Waddington, J.L., Weller, M.P., Crow, T.J. et al. (1992) Schizophrenia, genetic retrenchment andepidemiologic renaissance, Archives of General Psychiatry, 49, 990–4.
Walinder, J., Skott, A., Carlsson, A. et al. (1976) Potentiation of the antidepressant action ofclomipramine by tryptophan, Archives of General Psychiatry, 33, 1384–9.
Walsh, V. and Cowey, A. (2000) Transcranial magnetic stimulation and cognitive neuroscience,Nature Reviews Neuroscience, 1, 73–9.
Walzer, S., Wolff, P.H. and Bowen, D. et al. (1978) A method for the longitudinal study ofbehavioural development in infants and children: the early development of XXY children,Journal of Child Psychology and Psychiatry, 19, 213–29.
Wassermann, E.M. (1997) Report on risk and safety of repetitive transcranial magnetic stimulation(RTMS): suggested guidelines from the international workshop on risk and safety of rTMS (June1996), Electroencephalo Clinical Neurology, 108, 1–16.
Wassermann, E.M., Cohen, L.G., Flitman, S.S. et al. (1996) Seizures in healthy people with repeatedsafe trains of transcranial magnetic stimuli, Lancet, 347, 825–6.
Watis, L., Chen, S.H., Chua, H.C. et al. (2008) Glutamatergic abnormalities of the thalamus inschizophrenia: a systematic review, Journal of Neural Transmission, 115, 493–511.
Waxman, S.G. and Geschwind, N. (1975) The interictal behaviour syndrome of temporal lobeepilepsy, Archives of General Psychiatry, 32, 1580–6.
Webster, N.J., Green, K.N., Peers, C. et al., Institute for Cardiovascular Research, Universityof Leeds, Leeds, UK (2002) Altered processing of amyloid precursor protein in the humanneuroblastoma SH-SY5Y by chronic hypoxia, Journal of Neurochemistry, 83(6), 1262–71.
Wegner, J.T., Catalano, F., Gibralter, J. et al. (1985) Schizophrenics with tardive dyskinesia, Archivesof General Psychiatry, 42, 860–5.
Weickert, C.S., Webster, M.J., Gondipalli, P. et al. (2007) Postnatal alterations in dopaminergicmarkers in the human prefrontal cortex, Neuroscience, 144, 1109–19.
Weinberg, S.M., Jenkins, E.A., Marazita, M.L. et al. (2007) Minor physical anomalies in schizophre-nia: a meta-analysis, Schizophrenia Research, 89, 72–85.
Weinberger, D.R. (2009) Janssen Lecture, Institute of Psychiatry, London, 4 November; and personalcommunication.
Weiner, R.D. (1986) Electrical dosage, stimulus parameter and electrode placement, Psychopharma-cology Bulletin, 22, 499–502.
Weingartner, H. and Silberman, S. (1985) Cognitive changes in depression. In R.M. Post andJ. Ballenger (eds.), Psychobiology of Mood Disorders, Williams and Wilkins, Baltimore, MD, pp.121–35.
Weinstein, D.D., Diforio, D., Schiffman, J. et al. (1999) Minor physical anomalies, dermatoglyphicasymmetries, and cortisol levels in adolescents with schizotypal personality disorder, AmericanJournal of Psychiatry, 156, 617–23.
Weissman, J.D., Epstein, C.M. and Davey, K.R. (1992) Magnetic brain stimulation and brain size:relevance to animal studies, Electroencephalo Clinical Neurology, 85, 215–19.
Wells, C.E. (1979) Pseudodementia, American Journal of Psychiatry, 136, 895–900.Whalen, P.J., Rauch, S.L., Etcoff, N.L. et al. (1998) Masked presentations of emotional facial
expressions modulate amygdala activity without explicit knowledge, Journal of Neuroscience, 18,411–18.
Whalley, L.J., Borthwick, N., Copolov, D. et al. (1986) Glucocorticoid receptors and depression,British Medical Journal, 292, 859–61.

References 391
White, L.E. (1981) Development and morphology of human nucleus accumbens. In R.B. Chronisterand J.F. de France (eds.), The Neurobiology of the Nucleus Accumbens, Haer Institute, Brunswick,NJ, pp. 198–209.
Whitlock, F.A. and Evans, L.E.J. (1978) Drugs and depression, Drugs, 15, 53–71.Whittle, S., Chanen, A.M., Fornito, A. et al. (2009) Anterior cingulate volume in adolescents with
first-presentation borderline personality disorder, Psychiatry Research, 172, 155–60.Whitwell, J.L., Jack, C.R., Jr, Parisi, J.E. et al. (2007) Rates of cerebral atrophy differ in different
degenerative pathologies, Brain, 130, 1148–58.Wieck, A., Kumar, R., Hirst, A.D. et al. (1991) Increased sensitivity of dopamine receptors and
recurrence of affective psychosis after childbirth, British Medical Journal, 303, 613–16.Wiesel, F., Fyro, B., Nyback, H. et al. (1982) Relationship in healthy volunteers between secretion
of monoamine metabolites in urine and family history of psychiatric morbidity, BiologicalPsychiatry, 17, 1403–13.
Wieser, H.G. (1983) Electroclinical Features of the Psychomotor Seizure, Gustav Fischer, Stuttgart.Williams, D. (1956) The structure of emotions reflected in epileptic experiences, Brain, 79, 29–67.Williams, D. (1969) Neural factors related to habitual aggression, Brain, 92, 503–20.Willner, P. (1983) Dopamine and depression: a review of recent evidence, Brain Research Reviews, 6,
225–36.Wilson-Barnett, J. and Trimble, M.R. (1985) An investigation of hysteria using the IBQ, British
Journal of Psychiatry, 146, 601–8.Wing, J.K., Cooper, J.E. and Sartorius, N. (1974) Description and Classification of Psychiatric Symptoms,
Cambridge University Press, Cambridge.Wingenfeld, K., Rullkoetter, N., Mensebach, C. et al. (2008) Neural correlates of the individual
emotional stroop in borderline personality disorder, Psychoneuroendocrinology, 34(4), 571–86.Winokur, G. (1977) Delusional disorder, Comprehensive Psychiatry, 18, 511–21.Winokur, G. (1982) The development and validity of familial subtypes in primary unipolar
depression, Pharmacopsychiatrica, 15, 142–6.Winokur, G. and Tanna, V.L. (1969) Possible role of X-linked dominant factor in manic depressive
disease, Diseases of the Nervous System, 30, 87–94.Winokur, A., Amsterdam, J., Caroff, S. et al. (1982) Variability of hormonal responses to a series of
neuro-endocrine challenges in depressed patients, American Journal of Psychiatry, 139, 39–44.Winslow, R.S., Stillner, V., Coons, D.J. et al. (1986) Prevention of acute dystonic reactions in patients
beginning high-potency neuroleptics, American Journal of Psychiatry, 143, 706–10.Wirz-Justice, A. (1977) Theoretical and therapeutic potential of indolamine precursors in affective
disorders, Neuropsychobiology, 3, 199–233.Woermann, F., Tebartz van Elst, L., Koepp, M.J. et al. (2000) Reduction of frontal neocortical grey
matter associated with affective aggression in patients with temporal lobe epilepsy: an objectivevoxel-by-voxel analysis of automatically segmented MRI, Journal of Neurology, Neurosurgery andPsychiatry, 68, 162–9.
Wolf, P. (1982) Manic episodes in epilepsy. In H. Akimoto, H. Kazamatsuri, M. Seino and A.A.Ward, Jr (eds.), Advances in Epileptology: XIIIth Epilepsy International Symposium, Raven Press,New York, NY, pp. 237–40.
Wolf, P. and Trimble, M.R. (1985) Biological antagonism and epileptic psychosis, British Journal ofPsychiatry, 146, 272–6.
Wolpert, L. (1984) DNA and its message, Lancet, ii, 853–6.Wong, D.F., Wagner, H.N., Pearlson, G. et al. (1985) Dopamine receptor binding of C-11-3-N-
methylspiperone in the caudate in schizophrenia and bipolar disorder, PsychopharmacologyBulletin, 21, 595–8.

392 References
Wood, P.L., Suranyi-Cadotte, B., Schwartz, G. et al. (1983) Platelet 3H-imipramine binding and redblood cell choline in affective disorders, British Medical Journal, 18, 715–20.
Wood, J., Birmaher, B., Axelson, D. et al. (2009) Replicable differences in preferred circadian phasebetween bipolar disorder patients and control individuals, Psychiatry Research, 166, 201–9.
World Health Organization (1973) Report of the International Pilot Study of Schizophrenia, WHO,Geneva.
World Health Organization (1993) The ICD-10 Classification of Mental and Behavioural Disorders:Diagnostic Criteria for Research, WHO, Geneva.
Wu, J.C., Buchsbaum, M.S., Hershey, T.S. et al. (1991) PET in generalised anxiety disorder, BiologicalPsychiatry, 29, 1181–99.
Wu, J.C., Gillin, J.C. et al. (1992) Effect of sleep deprivation on brain metabolism of depressedpatients, American Journal of Psychiatry, 149, 538–43.
Wuerfel, J., Krishnamoorthy, E.S., Brown, R.J. et al. (2004) Religiosity is associated with hippocampalbut not amygdala volumes in patients with refractory epilepsy, Journal of Neurology, Neurosurgeryand Psychiatry, 75, 640–2.
Wyatt, R.J., Termini, B.A. and Davis, J. (1971) Biochemical and sleep studies of schizophrenia: areview of the literature 1960–1970, Schizophrenia Bulletin, 4, 10–66.
Yadalam, K.G., Jain, A.K. and Simpson, G. (1985) Mania in two sisters with similar cerebraldisturbance, American Journal of Psychiatry, 142, 1067–9.
Yamamoto, K. and Hornykiewicz, O. (2004) Proposal for a noradrenaline hypothesis of schizophre-nia, Prog Neuropsychopharmacol Biol Psychiatry, 28, 913–22.
Yang, Y., Raine, A., Lencz, T. et al. (2005a) Prefrontal white matter in pathological liars, BritishJournal of Psychiatry, 187, 320–5.
Yang, Y., Raine, A., Lencz, T. et al. (2005b) Volume reduction in prefrontal gray matter inunsuccessful criminal psychopaths, Biological Psychiatry, 57, 1103–8.
Yang, Y., Raine, A., Narr, K.L. et al. (2007) Localisation of increased prefrontal white matter inpathological liars, British Journal of Psychiatry, 190, 174–5.
Yang, Y., Glenn, A.L. and Raine, A. (2008) Brain abnormalities in antisocial individuals: implicationsfor the law, Behavioral Scientific Law, 26, 65–83.
Yang, Y., Raine, A., Colletti, P. et al. (2009) Abnormal temporal and prefrontal cortical gray matterthinning in psychopaths, Molecular Psychiatry, 14, 561–2, 555.
Yatham, L.N. (1994) Buspirone induced prolactin release in mania, Biological Psychiatry, 35, 553–6.Yehuda, R. (1997) Stress and glucocorticoids, Science, 275, 1662–3.Yehuda, R. and Golier, J. (2009) Is there a rationale for cortisol-based treatments for PTSD?, Expert
Review of Neurotherapeautics, 9, 1113–15.Yehuda, R., Morris, A., Labinsky, E. et al. (2007) Ten-year follow-up study of cortisol levels in aging
holocaust survivors with and without PTSD, J Trauma Stress, 20, 757–61.Young, A.B., Greenamayr, J.T., Hollingsworth, Z. et al. (1988) NMDA receptor losses in putamen
from patients with Huntington’s disease, Science, 241, 981–3.Young, K.A., Liu, Y. and Wang, Z. (2008) The neurobiology of social attachment: a comparative
approach to behavioral, neuroanatomical, and neurochemical studies, Comp Biochem Physiol CToxicological Pharmacology, 148(4), 401–10.
Young, L.T., Warsh, J.J., Kish, S.J. et al. (1994) Reduced brain 5-HT and elevated NA turnover andmetabolites in bipolar affective disorder, Biological Psychiatry, 35, 121–7.
Young, A. and Breslau, N. (2007) Troublesome memories: reflections on the future, Journal ofAnxiety Disorder, 21, 230–2.
Young, E.A. and Breslau, N. (2004) Saliva cortisol in posttraumatic stress disorder: a communityepidemiologic study, Biological Psychiatry, 56, 205–9.

References 393
Zabara, J. (1985a) Peripheral control of hypersynchronous discharge in epilepsy, Electroencephalog-raphy and Clinical Neurophysiology, 61, S162.
Zabara, J. (1985b) Time course of seizure control to brief, repetitieve stimuli, Epilepsia, 26, 518.Zabara, J. (1992) Inhibition of experimental seizures in canines by repetitive vagal stimulation,
Epilepsia, 33, 1005–12.Zametkin, A.J. and Liotta, W. (1998) The neurobiology of attention-deficit/hyperactivity disorder,
Journal of Clinical Psychiatry, 59, Suppl. 7, 17–23.Zammit, S., Allebeck, P., Andreasson, S. et al. (2002) Self-reported cannabis use as a risk factor for
schizophrenia in swedish conscripts of 1969: historical cohort study, British Medical Journal, 325,1199.
Zanetti, M.V., Soloff, P.H., Nicoletti, M.A. et al. (2007) MRI study of corpus callosum in patientswith borderline personality disorder: a pilot study, Progress in Neuropsychopharmacol BiologicalPsychiatry, 31, 1519–25.
Zardetto-Smith, A.M. and Gray, T.S. (1990) Organization of peptidergic and catecholaminergicefferents from the nucleus of the solitary tract to the rat amygdala, Brain Research Bulletin, 25,875.
Zifkin, B.G., Guerrini, R. and Plouin P. (2007) Reflex seizures. In J. Engel and T. Pedley (eds.),Epilepsy: A Comprehensive Textbook, 2nd edition, Lippincott Williams & Wilkins, New York, NY,pp. 2559–72.
Zilboorg, G. (1941) A History of Medical Psychology, W.W. Norton, New York, NY.


Index
References to tables are given in bold type.
5-HIAA see hydroxyindoleacetic acid5-HT see serotonin
abecarnil 306abulia 227accumbens 38, 58–59, 217acetylcholine 25, 188
receptors 20–21see also cholinergic systems
action potential 11acute schizophrenia-like psychotic disorder
149addictive disorders 215
benzodiazepines 307brain damage 224–226conditioning 217–219cravings 226–227electroencephalographic data 223genetic factors 219–220imaging studies 223–226medication for 317–318neurological disease and 227see also alcoholism
adenosine 3,5-monophosphate(AMP) 8
adenosine diphosphate (ADP) 8adenosine triphosphate (ATP) 8adrenaline 135adrenoceptors 18, 289adrenocorticotropic hormone (ACTH) 193,
194–195, 195–196affective disorders
aetiology 190–193, 210–212noradrenaline hypothesis 188–189
Biological Psychiatry 3e Michael R. Trimble and Mark S. George 2010 John Wiley & Sons, Ltd
permissive amine hypothesis 211serotonin 187–188
cerebrospinal fluid investigations 198–203cerebrovascular accidents and 208classification 183–184, 209–210computerized axial tomography (CAT)
203–204electroconvulsive therapy (ECT) 319electroencephalagraphic (ECG) studies
200–203epilepsy and 245genetics 184–186hormonal data 193–196, 196–198magnetic resonance imaging (MRI)
203–204metabolic factors 186–187neurochemistry 200neurological data 206–207neuropsychological disturbances 208–209neurotransmitters and 212pharmacological treatment
antidepressants see antidepressantslithium 309–310
sleep deprivation therapy 329sleep studies 203see also bipolar disorder; depression
aggression 122–123epilepsy and 244–245neurophysiological factors 74
agoraphobia 132agranular cortex 34agranulocytosis 303AIDS-dementia complex 272–273akathisia 301

396 Index
akinesia 301alcohol dehydrogenase (ADH) 220alcoholism 20, 220–221
brain damage 224–225cognitive impairment 228drug therapies 318genetics 220–221see also addictions
aldehyde dehydrogenase 2 (ALD) 220Allgemeine Psychopathologie 85alpha rhythm 90Alzheimer’s disease 258, 259–260
aetiology 265biomarkers 266–267brain atrophy 262classification 265–266, 266diagnosis 276electroencephalography (EEG) 261–262genetic factors 259personality 261–262personality effects 261progression 260–261see also dementia
ambulatory monitoring 93amines 282amino acids 10
DNA coding 2γ-aminobutyric acid see GABAamoxapine 287amphetamine 221amygdala 40, 41–42, 81, 120
aggression and 74anticonvulsant drugs 255anxiety and 140–141epilepsy and 244extended 41, 47–48, 72–73, 77function 72–73role in conditioning 217role in memory 76schizophrenia 167
amygdalofugal pathway 41amylobarbitone 305amyloid beta cleavage 259, 260amyloid plaques 263anankastic personality disorder see obsessive
personality disorderangiotensin 27, 68angular gyrus syndrome 276animals, transcranial stimulation 322
anomia 260anticonvulsant drugs 248, 255, 310–316, 311
depression and 246interactions 315modes of action 311pharmacology 293–296prescription guidelines 313, 315side-effects 312–313, 314toxic effects 313
antidepressant drugs 189, 286amoxapine 287animal experiments 292buproprion 289dementia and 316iprindole 289maprotiline 288–289mianserin 288mirtazapine 289mode of action 289–292monoamine oxidase inhibitors (MAOI)
284–285principles of treatment 292–293selective serotonin reuptake inhibitors
(SSRI) 285, 287–288serum-level monitoring 88side effects 294–295, 295toxicity 292trazadone 286–287tricyclic 285–286, 289, 291–292, 292, 295L-tryptophan 287venlafaxine 287viloxazine 288–289see also depression
antipsychotic drugs 296–300butyrophenones 296dementia and 316–317novel 304phenothiazines 296side-effects 300–302, 303–304
tardive dyskenesia 302–303antisocial personality disorder see sociopathyanxiety
epilepsy and 247functional studies 141–142genetic factors 118, 134–135metabolic effects 135–137neurochemical studies 137neurophysiological factors 75somatic variables 135

Index 397
see also generalized anxiety disorder;phobic disorders
anxiety disordersbrain imaging studies 140–142pharmaceutical treatment 305–308
anxiolytic drugs 305–308anxious personality 115apathy 227apolipoprotein E (ApoE) 259, 264apomorphine 156apoptosis 71arousal 76aspartate 17astrocytes 22autism 254autistic spectrum disorders, seizures 254automatisms 233autonomic nervous system, function 73–74autonomic nervous system (ANS) 51–53, 53azapirones 307
baclofen 20barbiturates 305basal ganglia 34, 38–41, 57–58, 207
disorders 208see also globus pallidus
Bear-Fedio scale 240–241religiosity 242–243
behavioural control 221benzodiazepines 138–139, 305–306, 312
modes of action 311side-effects 307
beta (adrenergic) blockers 137, 308Betz cells 60Binswagner’s disease 269biochemical assays 89bipolar disorder 184
distinguished from schizophrenia 210, 211epilepsy and 246genetics 184, 185lithium 308–310, 309prevalence 184sleep-deprivation therapy 329
blepharospasm-oromandibular-dystoniasyndrome 301
Bleuler, Eugen 147–148blinking 174blood flow imaging 101
blood oxygen level-dependent functionalMRI (BOLD) 102–104, 110
blood tests 88blood-brain barrier 282BOLD MRI 102–104, 110borderline personality disorder 114, 125brain
anatomy 32–34amygdala 41–43basal ganglia 38–41cerebellum 63cholinergic systems 60cingulate gyrus 48cortex 60–63extended amygdala 47–48hippocampus 43–45hypothalamus 49–51insula 48limbic system 35–38parahippocampal gyrus 45–46septal area 46–47thalamus 48–49
blood flow 104–105see also cerebral blood flow imaging
glucose metabolism 9imaging see brain imaginginformation processing 31–32lateralization of function 81macrosystems 55–57metabolism 8–9
imaging 105–106, 106–107pleasure pathways 67–68protein metabolism 9–10see also amygdala; hippocampus
brain electrical activity mapping (BEAM) 93,165
brain imaginganxiety 140–141cerebral blood flow (CBF) 104–105computerized axial tomography (CAT)
94–95magnetic resonance imaging (MRI) 95–99near infrared spectroscopy (NIR) 109positron emission tomography (PET)
105–108single-photon emission tomography
(SPECT) 108–109transcranial magnetic stimulation 109
brain surgery 70, 327–328

398 Index
brain-derived neurotrophic factor (BDNF)191–193
bretazenil 306Brodmann areas 33, 60, 61brofaromine 285buprenorphine 317buspirone 198, 289, 307butobarbitone 3, 305
caffeine 138calcium 14, 16, 22–23calcium channels 237cAMP 191cannabis 158–159, 177, 228capsulotomy 328carbamazepine 254, 255, 311, 312, 315carcinoma 78cardiac arrhythmia 303–304catatonic reactions 302catechol-O-methyl-transferase (COMT) 157catecholamines 26, 51, 135, 188
affective disorders and 199, 211epilepsy and 236–237receptor function tests 189
caudate nucleus 57CCK 68cell membranes 10–12central nervous system (CNS) 32
cell types 21–23inflammation 29
cerebellum 63cerebral blood flow (CBF) imaging 104–105,
204–205alcoholism 225schizophrenia 168–169
cerebral cortex 60–62, 166cerebral dysrhythmia 123–124cerebrospinal fluid (CSF)
affective disorders and 198–200Creutzfeldt-Jakob disease and 273–274flow dynamics 274–275personality disorders and 122–123schizophrenia 159–160
cerebrosyphilis 272, 276cerebrovascular accidents (CVA) 208chloride 11chlorpromazine 303Cholecystokinin (CCK) 27, 162cholinergic systems 60
anxiety and 138see also acetylcholine
chromosomes 2, 3–4abnormality
Alzheimer’s disease and 259schizophrenia 152
abnormality and personality disorders 120mitochondrial 4
cingulate gyrus 48, 69–71, 205behavioural role 69–71
circadian locomotor output cycles kaput(CLOCK) 185
citalopram 288classification 83–84
future direction 332–333see also diagnosis
clinical examination 87–89clobazam 306, 311clonazepam 311clonidine 189cloning 5clozapine 297, 299, 303CMRO2 105cocaine 221
medications 318neurophysiological effects 225–226
codons 2complementary DNA (cDNA) 5computerized axial tomography (CAT)
94–95affective disorders 203–204personality disorders 125–126
conditioning 217–219conduct disorder (CD) 221contingent negative variation (CNV) 91, 92corpus callosum 33cortex 60–63
Brodmann areas 33, 61cortical aphasia 276cortical atrophy 268cortico-striato-thalamic loops 39corticotrophin releasing factor (CRF) 195craving 226–227Creutzfeldt-Jakob disease (CJD) 273–274CT scans see computerized axial tomographycyclic AMP (cAMP) 157, 191cyclothymic disorder 116CYP see cytochrome P450cytochrome P450 282, 294–295

Index 399
Dale’s principle 29deep-brain stimulation (DBS) 74, 328–329dementia 254
aetiology 271, 275classification 258–259, 277–278cortical atrophy 268definition 257–258diagnosis 259, 268, 275–277epilepsy and 254, 256frontal-lobe 267–268hydrocephalic 274–275Lewy bodies 268–269mixed types 279pharmaceutical treatment 316–317prevalence 258pseudodementia and 208–209, 277reversibility 277subcortical 277syphilis 272vascular 269–271see also Alzheimer’s disease; Huntington’s
choreadependent personality 117dependent personality disorder 115depression 277
aetiology 190–193, 210–212serotonin 187–188
classification 210–211contrasted with unhappiness 183epilepsy and 245–246neurological data 206–207pharmacological treatment see
antidepressant drugsantiepileptic drugs and 246
prefrontal cortex 205prevalence 184as result of antipsychotic withdrawal 304transcranial magnetic stimulation (TMS)
323vagus nerve stimulation (VNS) 326see also affective disorders; antidepressants
desmethylimipramine 197dexamethasone suppression test (DST) 88,
137, 193–195, 194diagnosis
basic procedure 87–89analytic (biochemical) techniques 89
Diagnostic and Statistical Manual of MentalDisorders (DSM-IV) 84–85, 85–86,332
dementia 257depression 183, 210personality disorders 114, 116–117schizophrenia 149, 150
diffusion tensor imaging (DTI) 100disease
classification 85–86concept 83–84
disinhibition 80Dissociative Experiences Scale (DES) 119DNA 1–2dopamine 17–18, 51, 56, 160–161
schizophrenia and 178–179affective disorders and 190receptor agonists 296–297role in addiction 221–223role in conditioning 219schizophrenia and 155–157see also 5-hydroxytryptamine
dorsal striatum 218dorsolateral syndrome 79–80Down’s syndrome, Alzheimer’s disease and
259drug addiction see addictionsdrugs
excretion 282metabolism 282oral administration 281–282
DST see dexamethasone suppression testdyskinesia 302–303dysthymic disorder 115dystonia 300–301
electrical cortical stimulation (ECS) 71electroconvulsive therapy (ECT) 318–320electroencephalography (EEG) 90–93, 140
addictions 223affective disorders 200–203Alzheimer’s disease 261–262epilepsy 237, 251–252evoked potentials 91frontal-lobe dementia 267–268hydrocephalic dementia 274P300 wave 91personality disorders 123–124ramp patterns 165

400 Index
electroencephalography (EEG) (Continued)schizophrenia 164–165vascular dementia 270
emotion 76–77encephalopathies 254endophenotypes 7, 150enkephalins 27, 68, 158entorhinal cortex 71, 177–178epigenetics 7epilepsy 140, 164, 206, 231
aetiology 235–236psychoses 252–253
biochemistry 236–237classification 233–234cognitive deterioration 254–255diagnosis 237electroconvulsive therapy 320epidemiology 245–246fatal 234genetics and heritability 235personality effects 124–125related disorders 237–238
affective 245, 247aggression 244–245bipolar disorder 246–247ictal 238–240interictal dysphoric disorder 247–248personality 240–242, 244psychosis 248–254see also religiosity
religiosity and 242–244seizures 231–234temporal-lobe 241vagus nerve stimulation (VNS) 325, 326variation with age 235–236
episodic dyscontrol syndrome 244–245ethosuximide 311evoked potential 165, 202executive function 79exons 4eye tracking 174Eysenk personality tests 118
factor analysis 118Fahr’s disease 206fatty acids 9–10fear responses 73, 131felbamate 311, 314fluoxetine 193, 287, 289
fluvoxamine 287–288focal seizures 232folic acid 191Forced Normalization 251–252, 256, 313forced swim test 292fornix 43, 49free-thyroxine index 197frontal cortex 62
aggression and 74dysfunction 79–81, 124
functional magnetic resonance imaging100–104
G-protein-coupled receptors 13, 14GABA (γ-aminobutyric acid) 25, 42–43,
190–191, 199agonist compounds 308, 313epilepsy and 236receptors 20schizophrenia and 180tardive dyskinesia and 303
gabapentin 310, 311, 312, 314Gage, Phineas 79Galton, Francis 83–84galvanic skin response 135gamma knife therapy 143ganaxolone 315gas chromatography (GC) 89Gastaut-Geschwind syndrome 239, 242, 243,
256general paresis of the insane (GPI) 84generalized anxiety disorder (GAD)
132–133, 144genetics 331
addictions 219–220Alzheimer’s disease 259DNA 2–3epilepsy 235heritability 4personality and 118–119polymerase chain reaction 6–7schizophrenia 150–153, 176–177
genomics 89Gilles de la Tourette syndrome 142, 224,
227glial cells 22gliosis 163globus pallidus 38, 40glucocorticosteroids 195

Index 401
glucose 8, 9–10glutamate 17–18, 161, 236–237, 290
schizophrenia and 158glycerides 10glycine 25glycogen 8
habenula 51, 52, 52Hachinski scale 269–270haemodynamic response 102hallucinogens 220Halstead-Reitan tests 174Harlow, John Martyn 79head injury 235, 276–277heterozygotes 3–4high-performance liquid chromatography
(HPLC) 89highly-active antiretroviral therapy (HART)
272–273hippocampus 43–45
anxiety and 140–141behavioural role 71epilepsy 243–244memory and 75–76schizophrenia 168
Hippocrates 83histamine, receptors 19history-taking 87histrionic personality disorder 114, 119HIV encephalopathy 272–273homovanillic acid (HVA) 26, 159–160hormones 136–137Hounsfield units 94Human Genome Project 7Huntington’s chorea 7–8, 173, 206, 208, 263,
271–272hydergine 316hydrocephalic dementia 274–2755-hydroxyindoleacetic acid (5-HIAA)
139–140, 200affective disorders 198–199personality disorders and 122–123
5-hydroxytryptamine (5-HT) see serotoninhyperphagia 68hypnotics 305–308hypothalamo-pituitary-adrenal (HPA) axis
137hypothalamus 49, 49–51, 50, 66
function 68–69, 76
hydrazines 284hysterical personality style 118
illness 84imipramine 188, 200infants, neurological development 73–74initial slope index (ISI) 105innominata 47inositol triphosphate 15insular cortex 36, 48, 69
behavioural role 69interictal psychosis 248–252International Classification of Diseases (ICD)
84–85, 332dementia 257organic disorders 86–87schizophrenia 149, 150
International Pilot Study of Schizophrenia148
introns 4ion channels 11, 237iprindole 289isocarboxide 284isocortex 60isodendritic core 266
James, William 32, 35James-Lange hypothesis 32, 137Jaspers, Karl 85juvenile myoclonic epilepsy (JME) 244
kidneys 27, 283kindling 74Klinefelter’s syndrome 120Kluver-Bucy syndrome 74, 76, 125, 140, 240
L-dopa 156lacosamide 315lactic acid 9, 136lamotrigine 311, 314Landau-Kleffner syndrome 234laterality
affective disorders 213interictal psychosis 247–248schizophrenia 175, 181tests 175
Lennox-Gastaut syndrome 234leucoaraiosis 270–271leucotomies 327levetiracepam 311, 314Lewis, Aubrey 85

402 Index
Lewy bodies 268–269ligands 15limbic encephalitis 78limbic lobe 33, 35, 36–37
disorders 77–78see also limbic system
limbic permeability 74limbic system 34, 35–38, 65–67
connections 53–55greater 37–38, 37schizophrenia 165sensory input 71–72see also limbic lobe
linkage analysis 4lithium (carbonate) 308–310liver 283locus coeruleus 55lod score 5lofepramine 286Lombroso, Cesare 121long-term potentiation (LTP) 75, 75–76,
94low-resolution electromagnetic tomography
(LORETA) 93lumbar puncture 88–89
MacLean, Paul 65macrosystems 55–57magnetic resonance angiography 101magnetic resonance imaging (MRI)
advantages and disadvantages 98affective disorders 200, 203–204Alzheimer’s disease 262physical principles 95–96schizophrenia 166–168static magnet 97–99structural 99
magnetic resonance spectroscopy (MRS) 104magnetoencephalography (MEG) 93mammals 65–66mania 186, 206, 216maprotiline 288–289MDMA 226, 228medial frontal syndrome 80meiosis 4melatonin 308memantine 317memory 75–76
Alzheimer’s disease and 261
neurophysiological aspects 75–76schizophrenia and 175–176
mesial temporal sclerosis 235messenger RNA 3metachlorophenylpiperazine (MCPP) 154methadone 317α-methylparatyrosine 188Meyer, Adolf 83MHPG (3-methoxy-4-hydrophenylglycol)
138, 157, 160mianserin 189, 288, 288–289mild cognitive impairment 278Milner, Peter 67Minnesota Multiphasic Personality
Inventory (MMPI) 113, 240mirtazapine 289mitochondria 4moclobemide 285mongolism 120monoamine oxidase inhibitors (MAOI)
284–285, 295monoamine oxidase (MAO) 26, 121–122,
221, 284affective disorders and 186–187anxiety and 136see also 5-hydroxytryptamine; dopamine;
noradrenalinemonoamine transmitters 51, 56mood stabilizers 316motivation disorders 76–77, 77, 216–217,
216–217diagnosis 229neurological disease and 227
motor cortex 60mu rhythm 90multi-infarct dementia 258multiple sclerosis 86, 173mutation 4–5myoclonic seizures 233
N-methyl-d-aspartate (NMDA) 191narcissistic personality 115National Child Development Study 173National Institute on Drug Abuse 215neocortex 33neostriatum 271nerve growth factors (NGF) 14–15, 23, 24neurofibrillary tangles 263neurogenesis 23

Index 403
neuroleptic drugs 155–156neuroleptic malignant syndrome 302neuronal plasticity 75–76neurones 12
cell membranes 10–12cortical 62growth and replication 23resting potential 11
neuropsychological disturbances 208–209neurosis 131neurotensin 27neurotransmitters 21, 24–25, 81
acetylcholine 20–21, 25, 188Alzheimer’s disease and 265behavioural role 68catecholamines see catecholaminesenkephalins 27, 68, 158GABA see GABAglycine 25interrelationships 29serotonin see serotonin
neurotrophic factors see nerve growth factorsnialamide 284nigrostriatal pathways 58nomifesine 295noradrenaline 26, 56, 162, 199, 284
affective disorders and 188–190schizophrenia and 157–158
nortryptyline 293–294
obsessive personality disorder 114, 117obsessive-compulsive disorder (OCD)
78–79, 117, 133–134, 142–143,144
Olds, James 67oncogenes 3opiate receptors 21–22orbital syndrome 79orbitofrontal cortex (OFC) 63orexin 69organic mental disorders 86–87oxcarbazepine 311, 314oxygen-extraction fraction (OEF) 107oxytocin 28, 68
P300 wave 91paediatric autoimmune neuropsychiatric
disorders (PANDAS) 143panic attacks 132, 133
panic disorder 134neurochemical aspects 138
Papez circuit 35, 43–45parahippocampal gyrus 45–46, 71
schizophrenia 170parallel distributed processing (PDP) 31,
109–110paranoid personality disorder 114paranoid schizophrenia 150parasympathetic nerves 51–53Parkinsonism 301Parkinson’s disease 78, 206, 227, 258, 269paroxetine 288paroxymal activity 90partial volume effect 94parvalbumin 161, 180passive-aggressive personality disorder
115patch clamping 10–12patient history 87, 149Pavolian conditioning 217–219PCR see polymerase chain reactionpeptides 26, 162
role in behaviour regulation 68–69periaqueductal grey matter 54–55personality disorders 113–115
Alzheimer’s disease 261brain imaging studies 125–127diagnostic problems 127–129electroencephalography (EEG) 123–124epilepsy and 240–242genetic factors 118–122neurological disorders and 124–125neuropsychological analysis 127psychiatric disorder and 115–117stability over time 128
personality styles 117–118personality traits 116phaeochromatocytomas 136pharmacodynamics 283pharmacokinetics 281–283, 282–283phenelzene 284phenobarbital 311phenobarbitone 254, 305, 311phenylethylamines 191phenytoin 254, 310phobic disorders 132phobic-anxiety depersonalization syndrome
133

404 Index
photosensitivity 303physostigamine 190Pick’s disease 267pimozide 299platelets 188pleasure, neural pathways 67–68polycystic ovaries 315polymerase chain reaction (PCR) 6–7positron emission tomography (PET)
105–108, 142addictions 223–224affective disorders 204–206Alzheimer’s disease 262artefacts 108dementia 270schizophrenia 168–171
positron emitters 106post-traumatic stress disorder (PTSD)
131–132, 133, 135, 136–137, 137,143–144
brain imaging 141neurochemistry 138
precuneus 72prefrontal cortex 205presenilin-1 259present-state examination 248primidone 310–312prions 274procaine 205prolactin 88, 156, 197, 319prolactin-inhibitory factor (PIF) 197protein kinase C 15–16proteins 2, 9–10
phosphorylation 16receptors see receptor proteins
proteomics 7, 164pseudodementia 208–209, 277pseudopsychopathy 80psychogenic seizures 234psychopathic personality 114psychosis 149
epilepsy and 239, 248–252, 255laterality 250–251mechanisms 252–254risk factors 249–250
see also antipsychotic drugs; schizophreniapsychosurgery 70, 327–328psychotropic drugs 316–317purinergic system 138
putamen 58pyramidal cells 60
radioimmunoassay (RIA) 89radioreceptor assay 89ramp patterns 165Raphe cells 55Rassmussen’s encephalitis 234re-entrant circuits, 39, 57–59
disorders 78–79receptor proteins 14–16
acetylcholine 20–21adrenergic 18antidepressant drugs 289benzodiazepine 138–139, 305dopamine 17histamine 19serotonin 19–20, 290–291
religiosity 125, 242–244reserpine 206resonance 96resting potential 11restriction fragment-length polymorphisms
(RFLP) 5, 6retroviruses 3reversible inhibitors of monoamine oxidase
(RIMA) 285risperidone 299RNA (ribonucleic acid) 2, 3
S-adenosyl methionine (SAM) 191schizoaffective disorder 149schizoid personality 114–115schizophrenia 128, 205
aetiology 158–159dopamine hypothesis 155–157, 160,
178–179glutamate hypothesis 158noradrenergic hypothesis 157–158viral hypothesis 171–172, 180
associated diseases 172–174bipolar disorder and 210, 211brain morphology 167, 167–168, 170, 177classification 180–181
type I and II syndromes 178definition 147–150electroencephalogram (EEG) studies
164–165environmental factors 177

Index 405
epilepsy and 248–249antagonism 251–252
genetics 150–153, 176–177laterality 181long-term studies 152–153magnetic resonance imaging (MRI)
studies 166–168metabolic findings 154–155neurochemical studies 160–161neuropathology 162–164neuropsychological disturbances 174–176paranoid 150positron emission tomography 168–171somatic variables 153–154winter births and 171–172see also psychosis
schizophreniform disorder 149Schneider, Kurt 85, 148secondary mania 206seizures 233, 234, 250
autistic spectrum disorders 254classification 232–233, 232
selective serotonin uptake inhibitors (SSRI)212, 285, 287–288, 290–291, 296
self-help groups 318semantic dementia 268senile dementia 278sensory somatocortex 60septal area 46–47, 75serotonin 55, 200, 212, 221, 265
affective disorder and 187–188, 197–198,211–213
anxiety and 139receptors 19–20, 19schizophrenia and 154transport 291see also selective serotonin reuptake
inhibitorsserotonin receptors 185, 205–206sertraline 288sexual behaviour 76single-nucleotide polymorphism (SNP) 7single-photon emission tomography
(SPECT) 108–109, 169, 225sleep 76, 203sleep deprivation therapy 329sociopathy 114, 119
brain imaging studies 126sodium 11
sodium valproate 311, 312sphingolipids 10statistical probability/parametric mapping
(SPM) 93, 98, 103, 110, 204–205status epilepticus 233stem cells 23–24stria terminalis 41, 47–48striatum 57–58stroke 216, 225–226Stroop test 80, 205structural magnetic resonance imaging
99–100Structured Interview for Prodromal
Syndromes 153–154subcortical dementia 277subiculum 45substance dependence see addictive
disorderssubstance P 27, 59, 68substantia innominata 47substantia nigra 57subthalamic nucleus 74sudden unexpected death in epilepsy
(SUDEP) 234suicide 199, 310sulpiride 155suprachiasmatic nucleus 49Sydenham’s chorea 142symptom (definition) 84synapses 12–14
calcium channels 16growth 24
syndrome (definition) 84syphilis 272, 276
Talairach Atlas 34tardive dyskenesia 302–303tau protein 263tauopathies 263–264temperament see personalitytemporal lobe, schizophrenia 166tensor-based morphometry (TBM) 100,
102–103thalamus 32–33, 48–49, 90, 179–180thioridazine 297thyroid-stimulating hormone (TSH) 196–197thyrotropin-releasing hormone (TRH) 27tiagabine 314tics 224

406 Index
toloxatone 285tonic-clonic seizures 232topiramate 254, 313, 314Tourette’s syndrome 142, 224, 227Tower of London test 80toxicity, behavioural 283tractus solaritus 54transcranial magnetic stimulation (TMS) 109,
320–322therapeutic uses 322–323
transfer RNA 2transmitters, aggression and 74trazadone 286–287triune brain 65, 66L-tryptophan 287Turner’s syndrome 120twin studies
affective disorder 184–185anxiety 118bipolar disorder 184electroencephalography 90panic disorder 134–135schizophrenia 166–168
tyramine 186–187tyramine pressor test 189tyrosine 26, 189
uncinate fasciculus 41Urbach-Wiese syndrome 78urine testing 88utilization behaviour 80
vagus 53, 73vagus-nerve stimulation (VNS) 324–327vanadium 186vascular dementia 269–271vascular depression 99
vasoactive intestinal peptide (VIP) 27,29, 59
vasopressin 27–28venlafaxine 287ventral globus pallidus 389ventral striatum 58–59ventral tegmental area (VTA) 37, 54, 55videotelemetry 83vigabatrin 313, 314Virchov, Rudolf 83viruses 2, 3
dementia and 271–272schizophrenia and 171–172, 181
voles 68voxel-based morphometry (VBM) 100,
102–103voxels 94
weight gain 296, 304West’s syndrome 234white matter hyperintensity 99will 129, 216
see also motivation disordersWilson’s disease 173withdrawal symptoms
antidepressants 296antipsychotics 304benzodiazepines 307
World Health Organization 215
X-rays 88see also computerized axial tomography
zimelidine 295ziprasidone 304zonisamide 314zopiclone 307

Fornix
Cingulategyrus
Anteriornucleus ofdorsalthalamus
Mamillo-thalamic tract
Mammillarybody Hippocampus
Parahippocampalgyrus
Figure 2.5 Circuit of Papez
Figure 2.6 The insula, buried beneath the cortex following removal of the frontal and temporal polaropercula. The position of the amygdala, hippocampus and entorhinal cortex are shown (courtesy of Dr Garyvan Hoesen)

Figure 2.7 Medial view of the human brain. The areas shown in darker colours represent limbic structures(courtesy of Dr L. Heimer)
Striatum(caudal)
Striatum(rostral)
Greater Lim
bicLobe
Isocortical Frontal Lobe
Figure 2.9 Diagram of the cortical projections (from frontal and limbic cortices), showing how the cortexprojects to the basal ganglia and how this process is continuous; in essence there is no discrete break betweenthe frontal inputs and limbic inputs. It should be noted that this figure helps to emphasize that cortico-striatalprojections come from the entire cerebral cortex (courtesy of Dr L. Heimer)

BSTS/st
BSTM
BSTL
Med.Hyp.
Lat. Hyp.Ret. Form.
Co
Laterobasalcomplex
CeMe
Figure 2.14 The extended amygdala shown in isolation from the rest of the brain. Ce, Central and Me,Medial amygdaloid nucli; BSTL and BSTM, lateral and medial divisions of the extended amygdale; Co,cortical amygdala nucleus; BSTS/st, supracapsula part of the bed nucleus (courtesy of Dr L. Heimer)
N E O M A M M A L I A N
PA L E O M A M M A L I A N
REPTILIAN(Limbic System)
Figure 3.1 The triune brain. This diagram from Paul MacLean (1968) illustrates the evolution of the humanforebrain and how it expands along the lines of three basic formations that anatomically reflect an ancestralrelationship to reptiles, early mammals and late mammals (reproduced from Maclean, 1990)

7070
60
60
50
50
40
40
30
30
30
Counting Stroop (Bush et al., Ref.3) Counting Stroop (Bush et al., Ref.17)
trends in Cognitive Sciences
Emotional Counting Stroop (Whalen et al., Ref.18)
20
20
20
10
10
10
0 CognitivetaskEmotionaltask
Cognitivedivision
Affectivedivision
Cognitivedivision
Affectivedivision
0
70(a) (b)
7060
60
50
50
40
40
30
30
30
20
20
20
10
10
10
0
0
cc cc
Figure 3.2 Meta-analysis of the different imaging studies carried out, highlighting the differences betweenthe cognitive and affective divisions of the anterior cingulate. Note that the studies employing cognitivetasks, commonly employing multitasking, cause activations in the upper cingulate (in circles), while studiesmanipulating emotion cause activation in the lower affective division (in rectangles) (reproduced from Bushet al., 2000)

Figure 4.6 Structural MRI scan shown in 3D, with diffusion information superimposed and DTI tractsarising from brainstem (courtesy of Dr Mark George)

VBM DBM TBM
CorticalMapping
ShapeModeling
CINGSRSIRS
Parcellation
Figure 4.7 (a) The concept of inter- and intra-subject averaging, following spatial normalization. All scans arefirst fitted into a standard space, and subsequent comparison of pixel values is based upon standard parametricstatistical techniques. Areas of significant difference between groups are illustrated as statistical maps in threeformats. These are (left to right): T-maps, orthogonal projections showing areas of significant difference orsurface renderings onto a standard brain template (reproduced with permission from Dr K. Friston, WellcomeDepartment of Cognitive Neurology, Queen Square). (b) Six major types of analysis of structural images,showing some of the main types of data used in each case. Voxel-based morphometry (VBM; top-left panels)compares anatomy voxel by voxel to find voxels (shown here in blue) where the tissue classification (grey,white matter, CSF) depends on diagnosis or other factors. Results are typically plotted in stereotaxic space(lower panel), and their significance is assessed using random field or permutation methods. Deformation-based morphometry (DBM) can be used to analyse shape differences in the cortex or brain asymmetries(coloured sulci; red colours show regions of greatest asymmetry). Tensor-based morphometry (TBM) uses3D warping fields with millions of degrees of freedom (top) to recover and study local shape differences inanatomy across subjects or over time (red colours indicate growth rates in the corpus callosum of a youngchild). Other methods focus on structures such as the cerebral cortex, which can be flattened to assist theanalysis (bottom left), or the lateral ventricles (shape modelling). If anatomic structures are represented asparametric surface meshes, their shapes can be compared, their variability can be visualized and they canbe used to show where grey matter is lost (e.g. in Alzheimer’s disease; bottom-left panel, red colours denotegreatest grey-matter loss in the limbic and entorhinal areas). Fine-scale anatomical parcellation (lower right)can be used to compare structure volumes across groups, or to create hand-labelled templates that can beautomatically warped onto new MRI brain datasets. This can create regions of interest in which subsequentanalyses are performed (reproduced from Lawrie et al., 2003, with permission of Oxford University Press)

Medial Views
Front Front
(a)
(b)
Figure 4.10 (a) Statistical parametric maps (O15 PET) of the brain regions activated during transient sadnessinduced by remembering sad events and viewing sad faces. The control task consisted of remembering neutralevents and viewing neutral faces. Note that anterior limbic structures (septum, anterior cingulate, medialtemporal (?amygdala)) and left prefrontal cortex are activated. All points in dark tone represent significantincreases in activity (p < 0.01) (courtesy of Dr Mark George). (b) Three consecutive coronal slices through thebrain of the group brain activation that occurs when healthy subjects are unconsciously exposed to ultra-brief(subliminal) pictures of human faces which look fearful. The subjects were unaware after the imaging studythat they had even been exposed to anything unusual. Note that the ‘early warning system for danger’, theamygdala, bilaterally show activation during the time the subjects are exposed to the fearful faces, comparedto when they are not. This was one of the first demonstrations of the rapid fear response system of theamygdala (reproduced from Whalen et al., 1998)

Figure 5.1 Coronal MRI scan showing the seeding points in a study by Raine and colleagues, who examinedMRI-defined prefrontal white and grey matter in subjects with antisocial personality disorder, healthy age-and gender-matched controls, and controls with matched substance abuse. The antisocial-personality-disordergroup had markedly smaller prefrontal grey-matter volumes (Raine and Yang, 2006; Yang et al., 2005a, 2005b,2007) (reproduced with permission from Raine et al., 2000)
1.9
2.3
2.7
3.1
3.4
3.8
4.2
0.0
0.5
1.0
1.5
2.0
2.5
3.0
(a)
(c)
(b)
Figure 6.2 Genetic variation impacts key brain regions involved in anxiety, increasing vulnerability todysregulation. Shown are thresholded maps (p < 0.05) reflecting differences in grey-matter volume in 5-HTTLPR s-allele carriers compared to the l/l genotype. Note the volume reductions in the allele carriers inthe bilateral perigenual anterior cingulated cortex and amygdala (reproduced from Pezawas et al., 2005)