Embed Size (px)
DESCRIPTION
Citation preview

Atrial Fibrillation-update
Fathi Maklady, MD , FRCPProfessor of Cardiovascular medicine
Suez Canal University

Atrial Fibrillation-update
• AF is the most common sustained cardiac arrhythmia In the general population.1-2%
• It is estimated to be doubled in the next 50Yrs as the population ages.


AF-Epidemiology
• -<0.5% age 40-50
• -2-4% age 50-60
• -6-8% age 60-70
• -10-15% age>80


AF-Definition
• Rapid and uncoordinated irregular atrial activation with loss of contribution of atrial contraction to ventricular filling ,The end result is a decrease in cardiac output.

AF-risk


AF-Risk
• Life time risk of developing AF is 25% in those reached the age of 4oYrs.
• Paroxysmal AF carries the same risk as persistent or permanent AF.
• Asymptomatic or silent AF accounts for about 30% ,and may cause cryptogenic stroke.













CV conditions associated with AF
• -Age• -Hypertension.• -Heart Failure.• -Tachycardiomyopathy.• -Valvular Heart disease.• -Coronary artery disease.• -Cong Heart disease.• -Cardiomyopathies.

CV conditions associated with AF
• Aging :due to isolation of atrial myocardium and conduction disturbance.
• Heart failure:-AF is found in 30-40% of HF Pts.• Pts with HF-NHHA 11-1V is found in 30% of AF
Pts.• Valvular HT disease are found in 30% of Pts
with AF due to Lt atrial distension.• Cardiomyopathy is found in 10% of AF Pts.

CV conditions associated with AF
• ASD is associated with AF in 10-15% of Pts.
• Other cong HT disease :single ventricle,transposition,fontan surgery.
• CAD is present In >20% of AF Pts.


Non CV conditions associated with AF
• Thyroid dysfunction: hyper-Hypo-subclinical.
• Obesity: is found in25% of AF Pts.
• Diabetes: is found in 20%.
• COPD :in 10-15%.
• CKD:in 10-15%
• OSA.

AF-Types
1. First diagnosed AF2. Paroxysmal: self terminated usually within
48h ,It may continue up to 7days.3. Persistent: when AF lasts longer than 7 days
or need termination by cardioversion.4. Long standing persistent :AF lasted more than
a year ,when it is decided to adopt rhythm control strategy.
5. Permanent AF:The presence of AF accepted by the patient ad physician ,and rhythm control is not pursued.



Evaluation of a Pt with AF

Evaluation of a Pt with AF
• History :very important



Evaluation of a Pt with AF
• Clinical Examination: -BP -Character of apex -LVH Or HF manifestation. -Valvular Ht disease. -Congenital Ht disease. -Other non cardiac problems eg,thyroid
dysfunction, COPD,Obesity…etc

Evaluation of a Pt with AF
1. Routine:FBC, SC, FBS,Electrolytes,LFTs
2. TSH
3. Echocardiography: structural or functional abnormalities.

AF-ECG Criteria
1. Shows absolutely irregular R-R interval (arrhythmia absoluta)
2. No distinct P wave.
3. Atrial cycle length 200-300 b/m

Predisposing Factors for Recurrence
• -Age.
• -Lt Atrial size.
• -Reduced LVF.
• Presence of CAD.
• Presence of valvular Ht disease. Duration of AF before cardioversion.
• Number of recurrence.

AF Management

AF Management
• The Goal:
1. Reduce Symptoms.
2. Prevent complications.

AF Management
1. Reduce symptoms: -Rhythm control by antiarhythmic,electric
cardioversion ,or ablation.
2. Preventing complications: -Antithrombotic therapy -Control of ventricular rate -Adequate therapy for concomitant
cardiac disease

AF Management
• Rate Control vs Rhythm Control














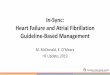
Prevention of Thromboembolic Complications













Non Warfarin Therapy






























In-Conclusion



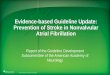
Copyright ©2011 American Heart Association
2011 Writing Group Members, et al. Circulation 2011;123:104-123
Therapy to maintain sinus rhythm in patients with recurrent paroxysmal or persistent atrial fibrillation


THANK YOU