Embed Size (px)
Citation preview

2012 Update of the ESC Guidelines on the
Management of Atrial Fibrillation
Stefan H. Hohnloser
J.W. Goethe University
Frankfurt am Main
S.H.H. has served as a consultant, member of the steering committee, or speaker for:
Bayer Healthcare, BMS, Boehringer Ingelheim, Boston Scientific, Cardiome, Forest RI,
J&J, Medtronic, Pfizer, Portola, Sanofi aventis, St. Jude Medical
Antiarrhythmic drug therapy for the prevention
of atrial fibrillation recurrences

European Heart Journal
doi:10.1093/eurheartj/ehs253
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs253
2012 focused update of the ESC Guidelines for the
Management of Atrial Fibrillation An update of the 2010 ESC Guidelines for the Management of Atrial Fibrillation
Developed with the special contribution of the European Heart Rhythm Association
Authors/Task Force Members: A. John Camm (Chairperson) (UK)*, Gregory Y. H. Lip (UK), Dan Atar (Norway), Raffaele
De Caterina (Italy), Gerhard Hindricks (Germany), Stefan H. Hohnloser (Germany), Paulus Kirchhof (Germany/UK), Irene
Savelieva (UK)
ESC Committee for Practice Guidelines (CPG): Jeroen J. Bax (CPG Chairperson) (The Netherlands),
Helmut Baumgartner (Germany), Claudio Ceconi (Italy), Veronica Dean (France), Christi Deaton (UK),
Robert Fagard (Belgium), Christian Funck-Brentano (France), David Hasdai (Israel), Arno Hoes (The Netherlands), Paulus Kirchhof (Germany/UK),
Juhani Knuuti (Finland), Philippe Kolh (Belgium), Theresa McDonagh (UK), Cyril Moulin (France), Bogdan A. Popescu (Romania), Željko Reiner
(Croatia), Udo Sechtem (Germany), Per Anton Sirnes (Norway), Michal Tendera (Poland), Adam Torbicki (Poland), Alec Vahanian (France),Stephan
Windecker (Switzerland).
Document Reviewers: Panos Vardas (Review Coordinator) (Greece), Nawwar Al-Attar (France), Ottavio Alfieri† (Italy), Annalisa Angelini (Italy),
Carina Blömstrom-Lundqvist (Sweden), Paolo Colonna (Italy), Johan De Sutter (Belgium), Sabine Ernst (UK), Andreas Goette (Germany), Bulent
Gorenek (Turkey), Robert Hatala (Slovak Republic), Hein Heidbüchel (Belgium), Magnus Heldal (Norway), Steen Dalby Kristensen (Denmark),
Philippe Kolh† (Belgium), Jean-Yves Le Heuzey (France), Hercules Mavrakis (Greece), Lluís Mont (Spain), Pasquale Perrone Filardi (Italy), Piotr
Ponikowski (Poland), Bernard Prendergast (UK), Frans Rutten (The Netherlands), Ulrich Schotten (The Netherlands), Isabelle C. Van Gelder (The
Netherlands), Freek Verheugt (The Netherlands)

European Heart Journal (2010) 31, 2369-2429
Principles of antiarrhythmic drug therapy to maintain sinus rhythm
1. Treatment is motivated by attempts to reduce AF-related
symptoms.
2. Efficacy of antiarrhythmic drugs to maintain sinus rhythm is modest.
3. Clinically successful antiarrhythmic drug therapy may reduce rather
than eliminate recurrence of AF.
4. If one antiarrhythmic drug ‘fails’ a clinically acceptable response
may be achieved with another agent.
5. Drug-induced proarrhythmia or extra-cardiac side-effects are
frequent.
6. Safety rather than efficacy considerations should primarily guide
the choice of antiarrhythmic agent.

AF = atrial fibrillation; AV = atrioventricular; bpm = beats per minute; CYP = cytochrome P; ECG = electrocardiogram;
LV = left ventricular; NYHA = New York Heart Association.
Drug Dose Main contraindications and precautions
ECG monitoring AV nodal slowing
Disopyramide 100-250 mg t.i.d.
Contraindicated in systolic heart failure, SND, and AVB II and III without PM. Caution when using concomitant medication with QT-prolonging drugs.
QT interval None
Flecainide 100-200 mg b.i.d.
Contraindicated if creatinine clearance < 50 mg/mL, in coronary artery disease, reduced LV ejection fraction, heart failure.
QRS duration increase > 25% above baseline
None
Flecanide XL 200 mg o.d. Caution in the presence of conduction system disease.
Propafenone 150-300 mg t.i.d.
Contraindicated in coronary artery disease, heart failure.
QRS duration increase > 25% above baseline
Slight
Propafenone SR
225-425 mg b.i.d.
Caution in the presence of conduction system disease and renal impairment.
Changes from 2010 Guidelines
Suggested doses and main caveats for commonly used antiarrhythmic drugs
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs253

AF = atrial fibrillation; AV = atrioventricular; bpm = beats per minute; CYP = cytochrome P; ECG = electrocardiogram;
LV = left ventricular; NYHA = New York Heart Association.
Drug Dose Main contraindications and precautions
ECG features prompting lower dose or discontinuation
AV nodal slowing
d,l-Sotalol
80-160 mg b.i.d..
Contraindicated in the presence of significant LV hypertrophy, systolic heart failure, pre-existing QT prolongation, hypokalaemia, significant renal impairment Creatinine clearance < 50 mg/mL. Moderate renal dysfunction requires careful adaptation of dose.
QT interval > 500 ms
Similar to high-dose β-blockers
Amiodarone
600 mg o.d. for 4 weeks, 400 mg o.d. for 4 weeks then 200 mg o.d.
Caution when using concomitant medication with QT-prolonging drugs, heart failure. Dose of vitamin K antagonists and of digitoxin/digoxin should be reduced. Creatinine, liver enzymes, thyroid hormones, & lung function should be monitored
QT interval >500 ms 10–12 bpm in AF
Suggested doses and main caveats for commonly used antiarrhythmic drugs
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs253
Changes from 2010 Guidelines

AF = atrial fibrillation; AV = atrioventricular; bpm = beats per minute; CYP = cytochrome P; ECG = electrocardiogram;
LV = left ventricular; NYHA = New York Heart Association.
Drug Dose Main contraindications and precautions
ECG features prompting lowerdose or discontinuation
AV nodal slowing
Dronedarone 400 mg b.i.d. Contraindicated in NYHA class III–IV or unstable heart failure, during concomitant medication with QT-prolonging drugs, powerful CYP 3A4 inhibitors, if creatinine clearance < 30 mg/mL. Not advised in other forms of heart failure, unless no appropriate alternative. Cautious use in CHD. Regular monitoring of liver function.
Dose of digitoxin/digoxin should be reduced.
Elevations in serum creatinine of 0.1–0.2 mg/dL are common and do not reflect reduced renal function.
QT interval > 500 ms 10–12 bpm in AF
Suggested doses and main caveats for commonly used antiarrhythmic drugs
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs253
Changes from 2010 Guidelines

European Heart Journal (2010) 31, 2369-2429
Choice of antiarrhythmic for the patient with no or minimal structural heart disease
No or minimal structural heart disease
Adrenergically
mediated
β-blockers
Sotalol
Dronedarone Amiodarone
Dronedarone
Flecainide
Propafenone
Sotalol
Undetermined Vagally
mediated
Disopyramide

European Heart Journal (2010) 31, 2369-2429
Choice of antiarrhythmic for the patient with no or minimal structural heart disease
No or minimal structural heart disease
Adrenergically
mediated
β-blockers
Sotalol
Dronedarone Amiodarone
Dronedarone
Flecainide
Propafenone
Sotalol
Undetermined Vagally
mediated
Disopyramide

European Heart Journal (2010) 31, 2369-2429
Choice of antiarrhythmic drug according to underlying pathology
ACEI = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blocker; CAD = coronary artery disease; CHF = congestive heart failure;
HT = hypertension; LVH = left ventricular hypertrophy; NYHA = New York Heart Association; unstable = cardiac decompensation within the prior
4 weeks. Antiarrhythmic agents are listed in alphabetical order within each treatment box. ? = evidence for ‘upstream’ therapy for prevention of atrial
remodelling still remains controversial.
? Prevention of remodeling
ACE/ARB/statin
β-blockade where appropriate
Treatment of underlying condition and ? Prevention/reversal
of remodelling - ACEI/ARB/statin. β-blockade where appropriate
HT CAD CHF
No LVH LVH Stable
NYHA I/II
NYHA III/IV
or ‘unstable’
NHYA II
Dronedarone Dronedarone
Sotalol
Dronedarone
Amiodarone Amiodarone Amiodarone
Dronedarone / Flecainide /
Propafenone / Sotalol
Minimal or no heart disease Significant underlying heart disease

Antiarrhythmic drug management
of non-permanent AF
Treatment of underlying condition and prevention of
remodelling – ACE-I / ARB / statins
CHF CHD
Significant structural heart disease Minimal or no structural heart disease
HHD
amiodarone
LVH No LVH
amiodarone
dronedarone / flecainide /
propafenone / sotalol
dronedarone
amiodarone
dronedarone
sotalol
AC
E-I
= a
ngio
tensin
convert
ing e
nzym
e inhib
itor;
AR
B =
angio
tensin
II re
cepto
r blo
cker;
CH
D =
coro
nary
heart
dis
ease; C
HF
= c
ongestive h
eart
failu
re; H
HD
=
hyp
ert
ensiv
e h
eart
dis
ease; LV
H =
left
ventr
icula
r hyp
ert
rophy.
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs253

Choice of an antiarrhythmic drug for AF control (I)
Recommendations Classa Levelb
The following antiarrhythmic drugs are recommended for rhythm control in
patients with AF, depending on underlying heart disease:
● amiodarone I A
● dronedarone I A
● flecainide I A
● propafenone I A
● d,I-sotalol I A
Amiodarone is more effective in maintaining sinus rhythm than sotalol,
propafenone, flecainide (by analogy) or dronedarone (LoE A), but because
of its toxicity profile should generally be used when other agents have failed
or are contraindicated (LoE C).
I A C
In patients with heart failure amiodarone should be the drug of choice. I B
Dronedarone is recommended in patients with recurrent AF as a moderately
effective antiarrhythmic agent for the maintenance of sinus rhythm. I A
In patients without significant structural heart disease, initial antiarrhythmic
therapy should be chosen from dronedarone, flecainide, propafenone, and
sotalol. I A
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs253

0 60 120 180 240 300 360
Cum
ula
tive incid
ence
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Cum
ula
tive incid
ence
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
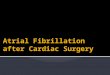
EURIDIS ADONIS
Time (days) Time (days)
1,237 patients (409 randomized to placebo, 828 to dronedarone)
EURIDIS & ADONIS: Primary Endpoint
HR = 0.78 (0.64 – 0.96)
P = 0.0138
HR = 0.73 (0.59 – 0.89)
P = 0.0017
Singh BN, et al. N Engl J Med. 2007;357:987-999.
0 60 120 180 240 300 360
Placebo
Dronedarone 400 mg BID

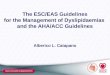
Hohnloser SH, et al. N Engl J Med. 2009;360:668-678.
Patients at risk:
Placebo 2,327 1,858 1,625 1,072 385 3
Dronedarone 2,301 1,963 1,776 1,117 403 2
Months
Placebo
Dronedarone
HR = 0.76
P < 0.001
0 6 12 18 24 30
0
10
20
30
40
50
Cu
mu
lative
in
cid
en
ce (
%)
0
10
20
30
40
50
2301
1858
1963
1625
1776
1072
1177
385
403
3
2
2327
Placebo
PlaceboDronedarone
MonthsPatients at risk
Dronedarone
HR=0.76P<0.001
0 6 12 18 24 30
Cu
mm
ula
tive
In
cid
en
ce
(%
)
0
10
20
30
40
50
2301
1858
1963
1625
1776
1072
1177
385
403
3
2
2327
Placebo
PlaceboDronedarone
MonthsPatients at risk
Dronedarone
HR=0.76P<0.001
0 6 12 18 24 30
Cu
mm
ula
tive
In
cid
en
ce
(%
)10 Outcome: Time to First Cardiovascular Hospitalization or Death
ATHENA: Morbidity/Mortality
Study in 4,628 Patients with AF

Choice of an antiarrhythmic drug for AF control (II)
Recommendations Classa Levelb
If one antiarrhythmic drug fails to reduce the recurrence of AF to a clinically
acceptable level, the use of another antiarrhythmic drug should be
considered. IIa C
Dronedarone should be considered in order to reduce cardiovascular
hospitalizations in patients with non-permanent AF and cardiovascular risk
factors. IIa B
ß-blockers should be considered for rhythm (plus rate) control in patients
with a first episode of AF. IIa C
Short-term (4 weeks) antiarrhythmic therapy after cardioversion may be
considered in selected patients e.g., those at risk for therapy-associated
complications. IIb B
aClass of recommendation. bLevel of evidence.
AF = atrial fibrillation; LoE = level of evidence.
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs253

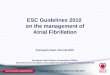
635 patients, mean age 64 years, flecainide 4 weeks vs long-term therapy
Primary outcome: time to persistent AF or death, monitored by telemetric ECG S
urv
iva
l p
rob
ab
ility
Time to event (days)
Short- vs long-term AAD Rx after cardioversion
Kirchhof et al, www.thelancet.com Published online
June 18, 2012 DOI:10.1016/S0140-6736(12)60570-4 1

Timefrom 1 month to event (days)
Su
rviv
al p
rob
ab
ility
Short- vs long-term AAD Rx after cardioversion
Short-term AAD Rx after cardioversion prevents approximately 80% of AF
recurrences, although long-term therapy is statistically more effective.
Landmark analysis after 1 month
Kirch
ho
f e
t a
l, w
ww
.th
ela
nce
t.co
m P
ub
lish
ed
on
line
June 1
8, 2012 D
OI:
10.1
016/S
0140
-6736(1
2)6
0570-4
1

Choice of an antiarrhythmic drug for AF control (III)
Recommendations Classa Levelb
Dronedarone is not recommended for treatment of AF in patients with NYHA
class III and IV, or with recently unstable (decompensation within the prior
month) NYHA class II heart failure. III B
Dronedarone is not recommended in patients with permanent AF III B
Antiarrhythmic drug therapy is not recommended for maintenance of sinus
rhythm in patients with advanced sinus node disease or AV node
dysfunction unless they have a functioning permanent pacemaker. III C
aClass of recommendation. bLevel of evidence.
AF = atrial fibrillation; LoE = level of evidence.
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs253

N Engl J Med 2011;365:2268-76
PALLAS: First co-primary outcome (stroke, MI, SEE, CV death)
Dronedarone
Placebo
0 1 3 6
0 1 3 6
Months
Cu
mu
lative
Ha
za
rd
1.0
0.8
0.6
0.4
0.2
0.0
0.04
0.03
0.02
0.01
0.00
Placebo 1617 1445 908 377
Dronedarone 1619 1421 930 353
No. at Risk
Median follow-up
3.5 months
HR 2.29 (1.34-
3.94; p = 0.002)

PALLAS: Second co-primary outcome (unplanned CV hospitalization or death)
Dronedarone
Placebo
0 1 3 6
Months
0 1 3 6
Cu
mu
lative
Ha
za
rd
1.0
0.8
0.6
0.4
0.2
0.0
0.12
0.08
0.04
0.00
No. at Risk
Placebo 1617 1429 882 361
Dronedarone 1619 1389 879 334
Median follow-up
3.5 months
HR 1.95 (1.45-
2.62; p < 0.001)
N Engl J Med 2011;365:2268-76

Summary of Recommendations Regarding the Use of Dronedarone
Recommendations Classa Levelb
Dronedarone is recommended in patients with recurrent AF as a moderately
effective antiarrhythmic agent for the maintenance of sinus rhythm. I A
Dronedarone should be considered in order to reduce cardiovascular
hospitalizations in patients with non-permanent AF and cardiovascular risk
factors. IIa B
Dronedarone is not recommended for treatment of AF in patients with NYHA
class III and IV, or with recently unstable (decompensation within the prior
month) NYHA class II heart failure. III B
Dronedarone is not recommended in patients with permanent AF III B
aClass of recommendation. bLevel of evidence.
AF = atrial fibrillation; LoE = level of evidence.
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs253

European Heart Journal (2010) 31, 2369-2429
Choice between ablation and antiarrhythmic drug therapy
for patients with and without structural heart disease
†More extensive LA ablation may be needed; *usually PVI is appropriate.
AF = atrial fibrillation; CAD = coronary artery disease; CHF = congestive heart failure; HT = hypertension; LVH = left ventricular hypertrophy;
NYHA = New York Heart Association; PVI = pulmonary vein isolation. Antiarrhythmic agents are listed in alphabetical order within each treatment box.
CHF
Stable
NYHA III
NYHA III/IV
or unstable
NHYA II
Dronedarone Dronedarone
Sotalol Dronedarone
Catheter
ablation for AF
Amiodarone
CAD Hypertension
with LVH
Relevant underlying
heart disease
Dronedarone
Flecainide
Propafenone
Sotalol
Amiodarone
Paroxysmal
AF
Persistent
AF
Catheter
ablation for AF*
No or minimal heart disease
(including HT without LVH)

Antiarrhythmic drugs and/or left atrial ablation
for rhythm control in AF
* = usually PVI is appropriate ‡ = more
extensive LA ablation may be needed;
* = not recommended in LVH;
ǂ caution with coronary heart disease;
HF = heart failure.
No or minimal structural heart disease
Paroxysmal Persistent
amiodarone
dronedarone,
flecainide,
propafenone,
sotalol
Catheter
ablation
Patient choice
‡
*
Patient choice
Relevant structural heart disease
HF
dronedaroneǂ, sotalol *
Due to AF
Catheter ablation ‡
No Yes
amiodarone
Patient choice
Yes
No
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs253

European Heart Journal
doi:10.1093/eurheartj/ehs253
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs253
2012 focused update of the ESC Guidelines for the
Management of Atrial Fibrillation An update of the 2010 ESC Guidelines for the Management of Atrial Fibrillation
Developed with the special contribution of the European Heart Rhythm Association
Authors/Task Force Members: A. John Camm (Chairperson) (UK)*, Gregory Y. H. Lip (UK), Dan Atar (Norway), Raffaele
De Caterina (Italy), Gerhard Hindricks (Germany), Stefan H. Hohnloser (Germany), Paulus Kirchhof (Germany/UK), Irene
Savelieva (UK)
ESC Committee for Practice Guidelines (CPG): Jeroen J. Bax (CPG Chairperson) (The Netherlands),
Helmut Baumgartner (Germany), Claudio Ceconi (Italy), Veronica Dean (France), Christi Deaton (UK),
Robert Fagard (Belgium), Christian Funck-Brentano (France), David Hasdai (Israel), Arno Hoes (The Netherlands), Paulus Kirchhof (Germany/UK),
Juhani Knuuti (Finland), Philippe Kolh (Belgium), Theresa McDonagh (UK), Cyril Moulin (France), Bogdan A. Popescu (Romania), Željko Reiner
(Croatia), Udo Sechtem (Germany), Per Anton Sirnes (Norway), Michal Tendera (Poland), Adam Torbicki (Poland), Alec Vahanian (France),Stephan
Windecker (Switzerland).
Document Reviewers: Panos Vardas (Review Coordinator) (Greece), Nawwar Al-Attar (France), Ottavio Alfieri† (Italy), Annalisa Angelini (Italy),
Carina Blömstrom-Lundqvist (Sweden), Paolo Colonna (Italy), Johan De Sutter (Belgium), Sabine Ernst (UK), Andreas Goette (Germany), Bulent
Gorenek (Turkey), Robert Hatala (Slovak Republic), Hein Heidbüchel (Belgium), Magnus Heldal (Norway), Steen Dalby Kristensen (Denmark),
Philippe Kolh† (Belgium), Jean-Yves Le Heuzey (France), Hercules Mavrakis (Greece), Lluís Mont (Spain), Pasquale Perrone Filardi (Italy), Piotr
Ponikowski (Poland), Bernard Prendergast (UK), Frans Rutten (The Netherlands), Ulrich Schotten (The Netherlands), Isabelle C. Van Gelder (The
Netherlands), Freek Verheugt (The Netherlands)