Embed Size (px)
DESCRIPTION
Citation preview

Pumps & Pipes 1
Christie M. Ballantyne, M.D.Christie M. Ballantyne, M.D.
Center for Cardiovascular Disease PreventionCenter for Cardiovascular Disease PreventionMethodist DeBakey Heart CenterMethodist DeBakey Heart Center
Baylor College of MedicineBaylor College of MedicineHouston, TexasHouston, Texas
Atherosclerosis

Key Clinical Issues
1. What causes the development of atherosclerosis?
2. Why do some atherosclerotic plaques develop a thrombus leading to vessel occlusion and clinical symptoms (MI, stroke)
3. How do we identify early atherosclerosis which does not limit flow and does not cause symptoms?
4. How do we stop or reverse atherosclerosis?
5. How do we monitor whether therapy is successful?

How do you know if you are at risk for a heart attack?

Case
A 58-year-old former CEO, recently retired, concerned about his risk for heart disease because of a family history of heart disease. He exercises on a regular basis; diet and weight have fluctuated over the years with his stress and workload. His only medical problem is high blood pressure, which is controlled with medication.



Case
Physical examination: Blood pressure 142/80Height 6'2", Weight 210 lb
Labs: Total cholesterol 233Triglycerides 100HDL cholesterol 36LDL cholesterol 177
What is his risk for coronary heart disease?

Major Risk Factors That Modify LDL-C Goals
• Cigarette smoking• Hypertension: 140/90 mm Hg or on
antihypertensive medication• Low HDL-C: <40 mg/dL*• Family Hx of premature CHD: male first-degree
relative <55 years, female first-degree relative <65 years
• Age: men 45 years, women 55 years*High HDL-C (60 mg/dL) is a negative risk factor and
decreases by 1 the total number of risk factors
Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001;285:2486-2497.

Note: Risk estimates were derived from the experience of the Framingham Heart Study, a predominantly Caucasian population in Massachusetts, USA.
Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA. 2001;285:2486-2497.
Assessing CHD Risk in MenStep 1: Age
Years Points20-34 -935-39 -440-44 045-49 350-54 655-59 860-64 1065-69 1170-74 1275-79 13
Step 2: Total Cholesterol
HDL-C(mg/dL) Points
60 -1
50-59 0
40-49 1
<40 2
Step 3: HDL-Cholesterol
Systolic BP Points Points(mm Hg) if Untreated if Treated
<120 0 0120-129 0 1130-139 1 2140-159 1 2160 2 3
Step 4: Systolic Blood Pressure
Step 5: Smoking Status
Points at Points at Points at Points at Points at Age 20-39 Age 40-49 Age 50-59 Age 60-69 Age 70-79
Nonsmoker 0 0 0 0 0Smoker 8 5 3 1 1
Age
Total cholesterol
HDL-cholesterol
Systolic blood pressure
Smoking status
Point total
Step 6: Adding Up the Points
Point Total 10-Year Risk Point Total 10-Year Risk<0 <1% 11 8%0 1% 12 10%1 1% 13 12%2 1% 14 16%3 1% 15 20%4 1% 16 25%5 2% 17 30%6 2%7 3%8 4%9 5%10 6%
Step 7: CHD Risk
ATP III Framingham Risk Scoring
TC Points at Points at Points at Points at Points at(mg/dL) Age 20-39 Age 40-49 Age 50-59 Age 60-69 Age 70-79
<160 0 0 0 0 0160-199 4 3 2 1 0200-239 7 5 3 1 0240-279 9 6 4 2 1280 11 8 5 3 1

What is his Framingham Risk Score?
Age
Total cholesterol
HDL cholesterol
Systolic blood pressure
Smoking
Total:
8
3
2
2
0
15
PointsPoints
Risk of CHD event (MI or death): 20%Risk of CHD event (MI or death): 20%

High risk for CHD event: >20% over 10 years
Intermediate risk: 10–20%
Low risk: <10%

Current Approaches to "Risk Assessment" (Predicting Heart
Attack and Stroke)
1. Count risk factors
2. Equations to quantitate absolute 10-year risk or lifetime risk

What causes a heart attack?

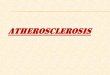
Endothelial Dysfunction in Atherosclerosis
Ross R. N Engl J Med 1999; 340:115–126.

Fatty-Streak Formation in Atherosclerosis
Ross R. N Engl J Med 1999; 340:115–126.

Formation of an Advanced, Complicated Lesion in Atherosclerosis
Ross R. N Engl J Med 1999; 340:115–126.

Unstable Fibrous Plaques in Atherosclerosis
Ross R. N Engl J Med 1999; 340:115–126.

Are there other tests to identify better who might have a heart
attack or stroke?

New Tests for Risk Assessment
• Blood tests related to inflammation
– High-sensitivity C-reactive protein (CRP)
– Lipoprotein-associated phospholipase A2 (Lp-PLA2)

LUMEN
MEDIA
INTIMA
LDL
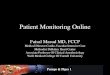
The Role of Lp-PLA2 in CVD
Lp-PLA2

Adhesion Molecules
LUMEN
MEDIA
INTIMA
Lp-PLA2
The Role of Lp-PLA2 in CVD
Oxidized LDL
Cytokines
Lyso-PC+
OxFA
LDL

LUMEN
MEDIA
INTIMA Lyso-PC+
OxFA
Lp-PLA2
Adhesion Molecules
CytokinesPlaque Formation
Foam Cell
Monocytes
Macrophage
The Role of Lp-PLA2 in CVD
Oxidized LDL
LDL

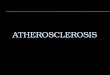
11.38
6.02 5.52
5.844.03
1.000.00
2.00
4.00
6.00
8.00
10.00
12.00
High Medium Low
Low
Medium
High
5.52
CRP, mg/L Lp-PLA 2
, g/L
Isch
emic
Str
oke
Haz
ard
Rat
io
95% CI 3.13–41.41,p<0.001
(>3) (1–3) (<1)
(422)
(310–422)
(<310)
6.02
2.854.27
Association of Lp-PLA2 and CRP with Incident Ischemic Stroke
4.36
Ballantyne CM et al. Arch Intern Med 2005;165:2479-2484.

• Ankle-brachial index (ABI)
• B-mode ultrasound of carotids (intima-media thickness)
• Electron beam computed tomography (EBCT)
• Exercise and nuclear stress tests
Noninvasive Assessments for Subclinical Atherosclerosis

• ARIC study – 16,000 individuals with 20 years of follow up
• 1.2 million SNPs per individual by end of year• Multiple imaging and blood tests on each
individual (100s to 1000s of data points per patient
• How to analyze and “mine” the data?
Biomarkers, Genes, Imaging and Prediction of MI and Stroke

ABCs of Prevention
A. Aspirin, ACE inhibitor
B. Blood pressure, beta-blocker
C. Cholesterol
D. Diet
E. Exercise

Intensity of lipid-modifying
therapy is dependent upon the
absolute risk for CHD events

Assessment of Therapeutic Efficacy
Prostate Cancer
Symptoms: urine flow
Blood tests: PSA
Imaging: ultrasound, MRI, CT
Invasive: biopsy
CAD
Symptoms: blood flow
"Stress" tests: to assess blood flow
Invasive: cath

Barriers to New Drug Development
• Lack of blood tests (biomarkers) to quantitate atherosclerosis
• No imaging tests to track progression/ regression in routine clinical practice