Embed Size (px)
Citation preview
DIFFERENTIAL DIAGNOSIS of
TOF PHYSIOLOGY
Satyam Rajvanshi
CYANOTIC CHD CLASSIFICATION
Cyanotic CHD CLASSIFICATION
Anatomico-pathological Physiological
Cyanotic CHD with Increased PBF• (5 Ts and 2 Ss)
– TAPVC – Single Ventricle – TGA – Single (Common)– Taussig-Bing Atrium– Tricuspid Atresia– Truncus Arteriosus
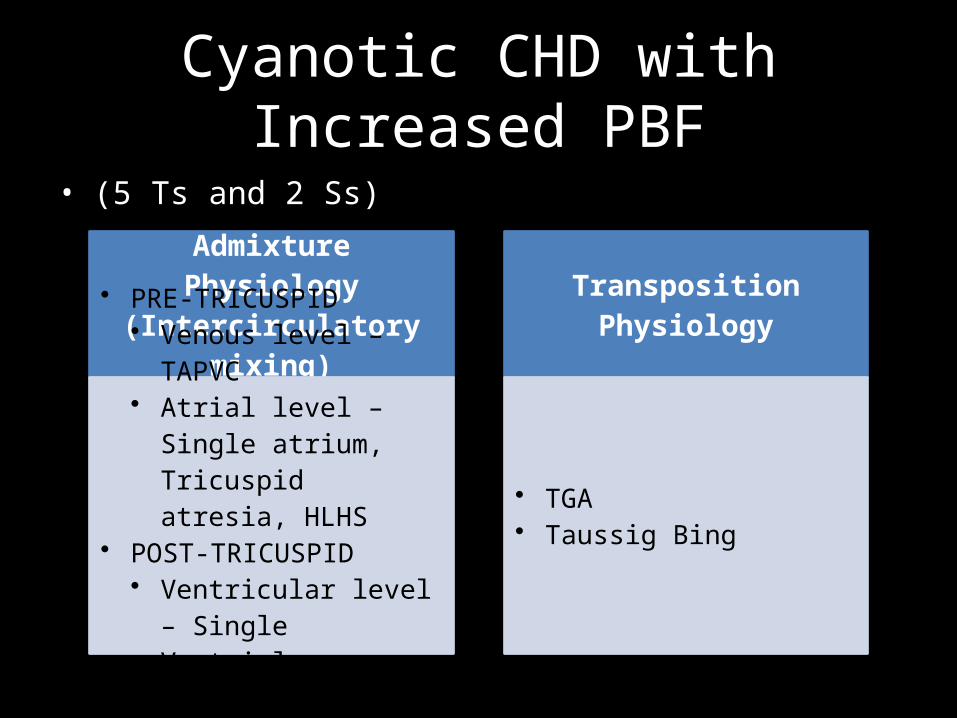
Cyanotic CHD with Increased PBF• (5 Ts and 2 Ss)
Admixture Physiology (Intercirculatory mixing)
• PRE-TRICUSPID• Venous level – TAPVC• Atrial level – Single
atrium, Tricuspid atresia, HLHS
• POST-TRICUSPID• Ventricular level – Single
Ventricle• Arterial level – Truncus
Transposition Physiology
• TGA• Taussig Bing
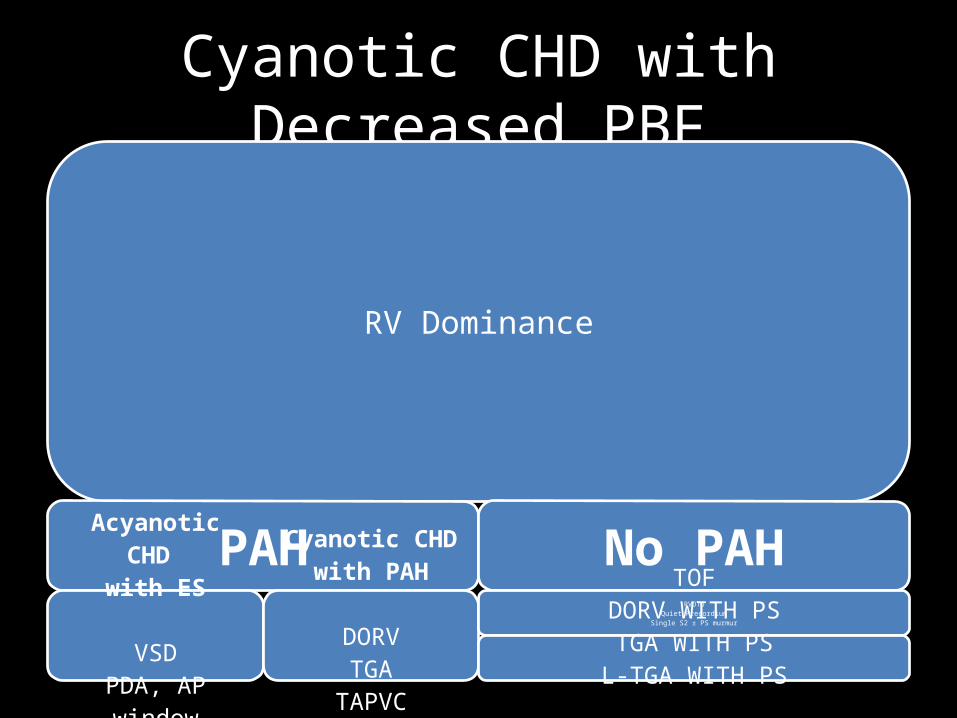
Cyanotic CHD with Decreased PBF
RV Dominance
PAHAcyanotic CHD
with ES
VSDPDA, AP window
ASD
Cyanotic CHD with PAH
DORVTGA
TAPVCTruncus
No PAHRVOTO
Quiet PrecordiumSingle S2 ± PS murmur
TOFDORV WITH PSTGA WITH PS
L-TGA WITH PS
ASD with PS
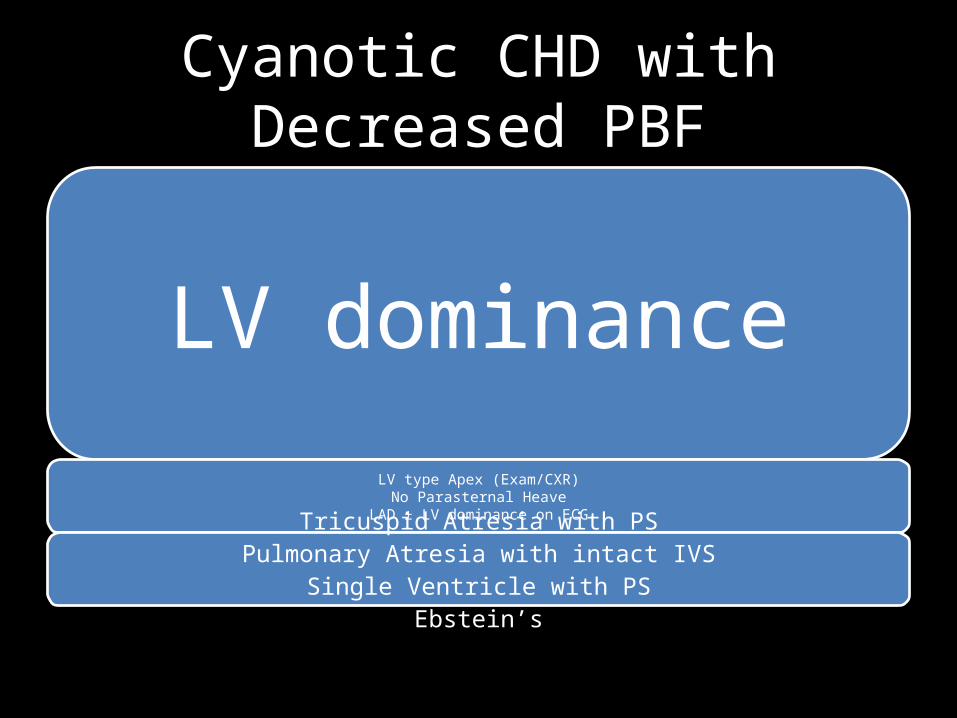
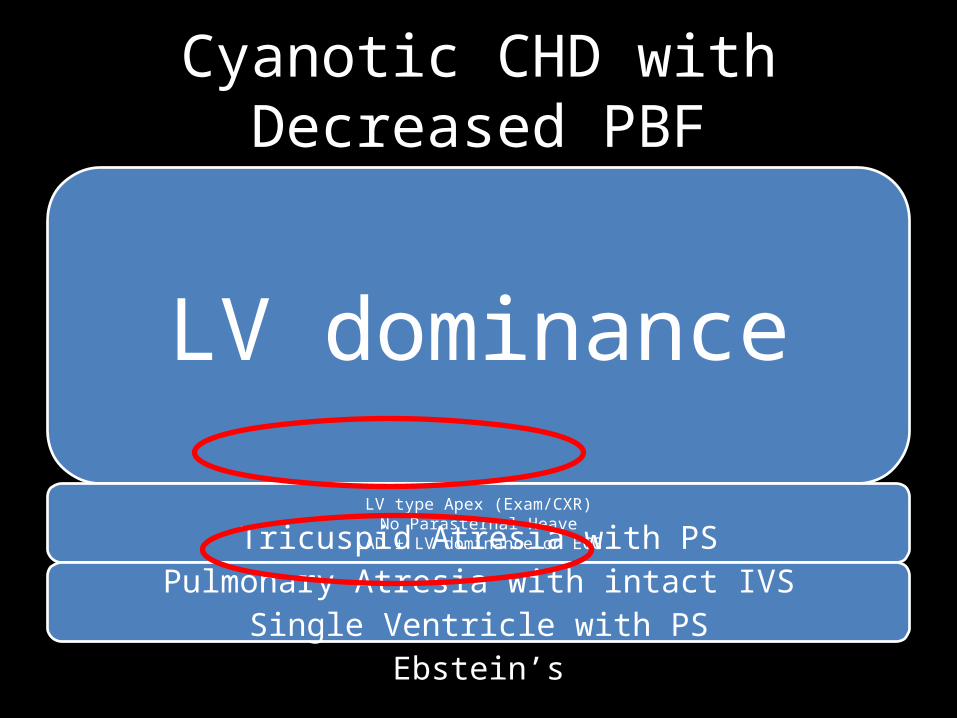
Cyanotic CHD with Decreased PBF
LV dominanceLV type Apex (Exam/CXR)
No Parasternal HeaveLAD ± LV dominance on ECG
Tricuspid Atresia with PSPulmonary Atresia with intact IVS
Single Ventricle with PSEbstein’s
Cyanotic CHD with Near Normal PBF
• Pulmonary AV Fistula• Unroofed coronary sinus into LA• Anomalous drainage of vena cava to LA

CCHD Physiological classification• TOF Physiology• Transposition Physiology• Admixture Physiology• Eisenmenger Physiology• Duct-dependent Physiology
– For PBF – Pulmonary atresia– For SBF – Aortic atresia/HLHS
• Near-normal Physiology– Pulmonary AVFs
• Miscellaneous– Ebstein’s– ASD with PS– Unroofed CS into LA

• Symptom complex – guide to PHYSIOLOGY
• Examination – guide to ANATOMY(Physical findings)
• Radiology, ECG – add to BOTH
TOF PHYSIOLOGY?What is
TOF PHYSIOLOGY
• Cyanotic CHD with decreased PBF having 2 key components anatomically
– Severe PS – Decreasing PBF
– Large VSD – with right to left shunt due to outflow obstruction
(Acyanotic TOF not included)
TOF PHYSIOLOGY
• Cyanotic CHD with decreased PBF having 2 key symptoms Physiologically
– History of Spells
– History of Squatting
– No CHF symptoms
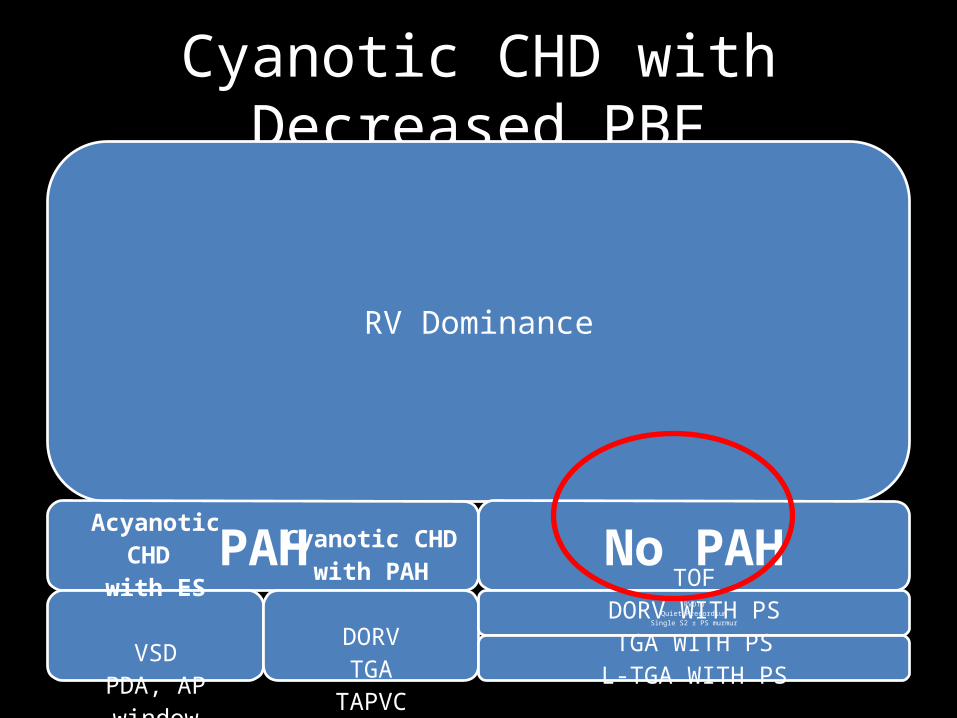
Cyanotic CHD with Decreased PBF
RV Dominance
PAHAcyanotic CHD
with ES
VSDPDA, AP window
ASD
Cyanotic CHD with PAH
DORVTGA
TAPVCTruncus
No PAHRVOTO
Quiet PrecordiumSingle S2 ± PS murmur
TOFDORV WITH PSTGA WITH PS
L-TGA WITH PS
ASD with PS
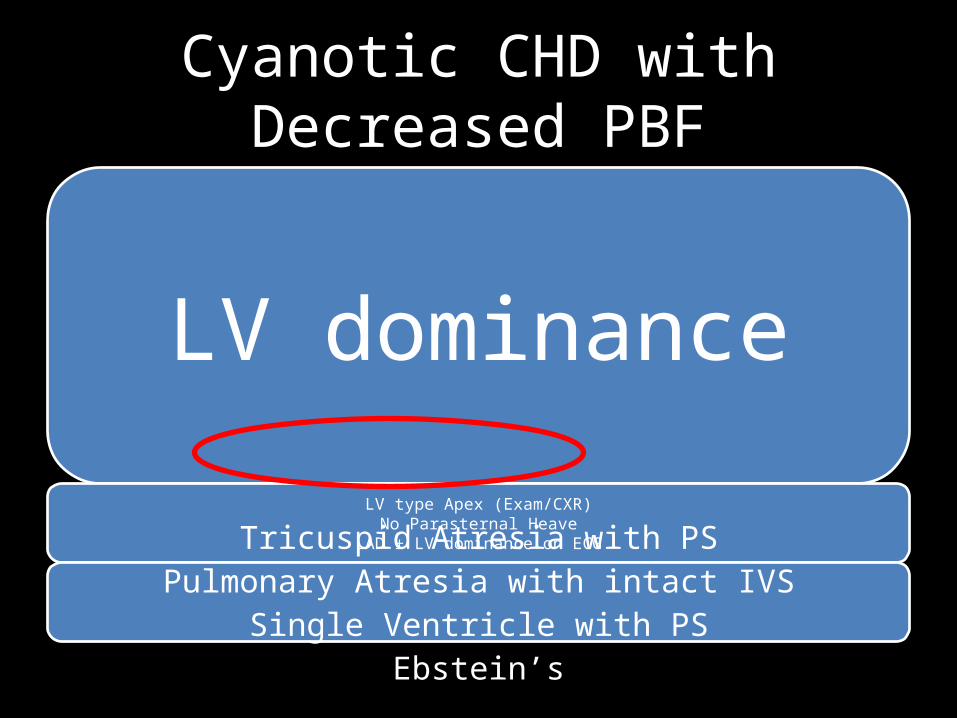
Cyanotic CHD with Decreased PBF
LV dominance
LV type Apex (Exam/CXR)No Parasternal Heave
LAD ± LV dominance on ECGTricuspid Atresia with PSPulmonary Atresia with intact IVS
Single Ventricle with PSEbstein’s
Cyanotic CHD with Decreased PBF
LV dominance
LV type Apex (Exam/CXR)No Parasternal Heave
LAD ± LV dominance on ECGTricuspid Atresia with PSPulmonary Atresia with intact IVS
Single Ventricle with PSEbstein’s

TOF
“Tetralogy of Fallot” History
• 1671: First reported by Niels Stenson a.k.a Nicholas Steno
• 1777; 1784; 1839; 1866; 1872Similar Case reports

• 1888:Etienne Louis Arthur Fallot– Anatomic diagnosis
at bedside– Confirmed at
postmortem– Coined term Tetralogie
(Fr.)
• 1894: Pierre Marie (French), first used term “Tetralogie de Fallot”
• 1924: Maude Abbott, first used term “Tetralogy of Fallot” &“Fallot’s Tetralogy”
Pathology
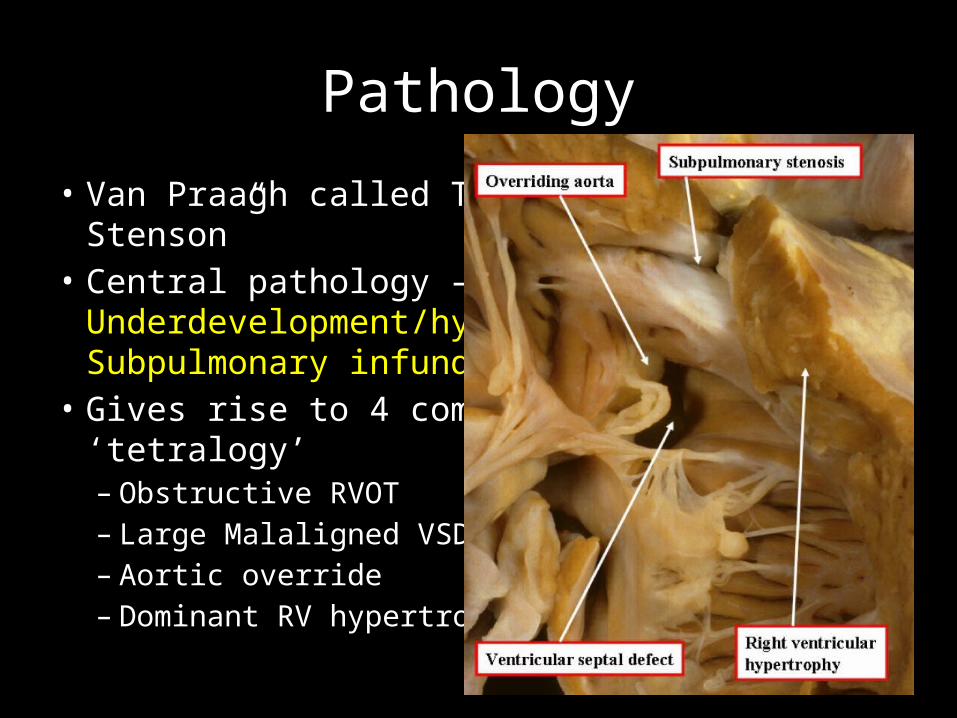
• Van Praagh called TOF “Monology of Stenson”• Central pathology –
Underdevelopment/hypoplasia of Subpulmonary infundibulum
• Gives rise to 4 components of ‘tetralogy’– Obstructive RVOT– Large Malaligned VSD– Aortic override– Dominant RV hypertrophy
Pathology
• Van Praagh called TOF “Monology of Stenson”• Central pathology –
Underdevelopment/hypoplasia of Subpulmonary infundibulum
• Gives rise to 4 components of ‘tetralogy’– Obstructive RVOT– Large Malaligned VSD– Aortic override– Dominant RV hypertrophy
TOF
• 1 in 3600 live births• M=F
Natural History
• Survival– 66% 1st yr– 50% 3rd yr– 25% 1st decade
• Poor survival with PA– 50% 1st yr– 10% 1st decade
Symptoms/Presentation• Cyanosis
– 1-2 weeks after birth– More severe the PS, earlier the presentation
• Hypercyanotic Spells– 2 months to 2 years of age
• Exertional dyspnoea– Older child
• Squatting– To alleviate a spell or dyspnoea
Physical Exam
• Physically underdeveloped
• Cyanosis (Depending on PBF)
• Pulse– NORMAL (irrespective of PS severity)– Wide PP – only in Large MAPCA/Severe AR
Physical Exam
• JVP– NORMAL (Height and waveform)
(RAP stays normal unless significant TR present)
Physical Exam
Palpation• RV impulse– Gentle; like normal neonatal RV; but stays like that
even as child grows– 4th LICS – 5th LICS & Subxyphoid (if Sub-Infundibular stenosis)
Physical Exam
Palpation• LV impulse– ABSENT (Conspicuous feature)– Absent even if MAPCAs present
Physical Exam
Palpation• 2nd / 3rd LICS– A2 maybe palpable– Left upper ICS (Not right) (due to hypoplastic PA)
Physical Exam
Palpation• Right sternoclavicular joint pulsation– Right sided Aortic arch
• No thrill due to RVOTO– BF goes uninterrupted to dilated Aorta

Physical Exam
Auscultation• Aortic area (2nd RICS)– Loud aortic EC from aortic root– Maximum in expiration
• Pulmonary area– Very delayed and soft P2– EC and P2 almost inaudible (Bicuspid PV – decreased mobility)
Physical Exam
Auscultation• 3rd LICS– Superficial murmur starting with S1
Duration and intensity decreases with severity of PS
• No S4 (RA contraction not forceful, RAP normal)
• No S3 (No RVF)
Physical Exam
Auscultation• Continuous murmurs– In case of Pulmonary atresia/MAPCAs
• AR murmur ±
• PR murmur ±
ECG
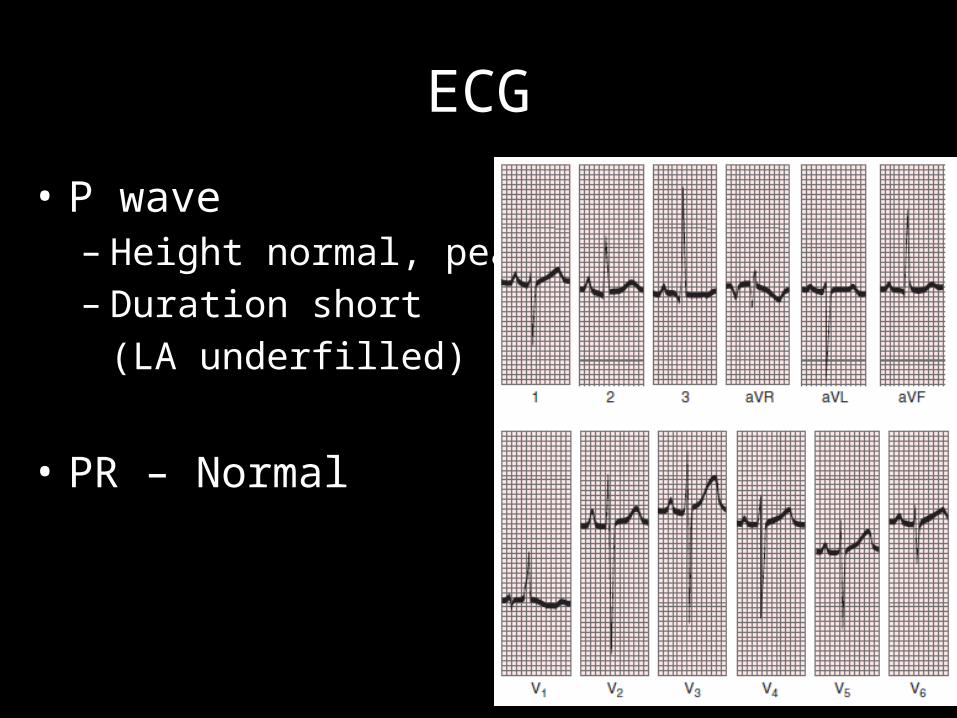
• P wave – Height normal, peaked– Duration short
(LA underfilled)
• PR – Normal
ECG
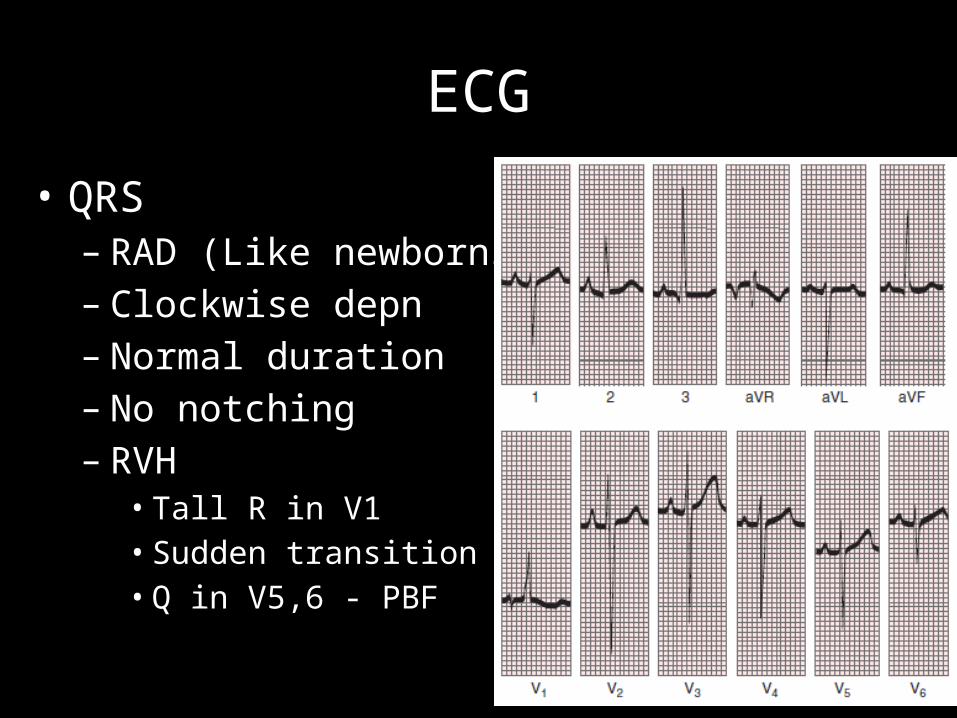
• QRS– RAD (Like newborns)– Clockwise depn– Normal duration– No notching– RVH• Tall R in V1• Sudden transition V1-2• Q in V5,6 - PBF
ECG
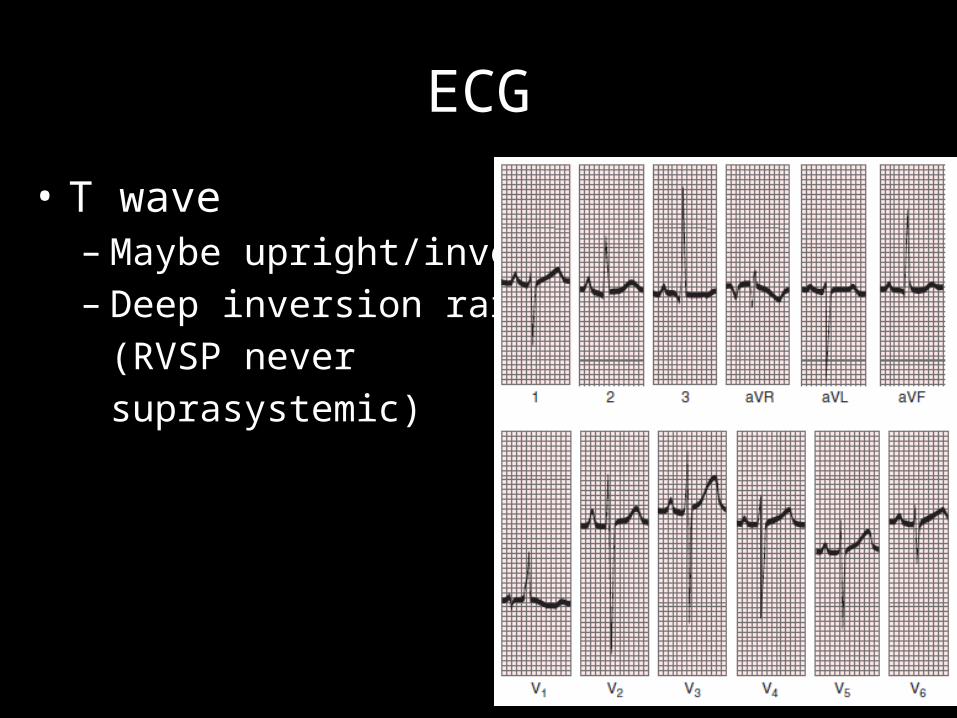
• T wave – Maybe upright/inverted – Deep inversion rare
(RVSP never suprasystemic)

CXR
CXR
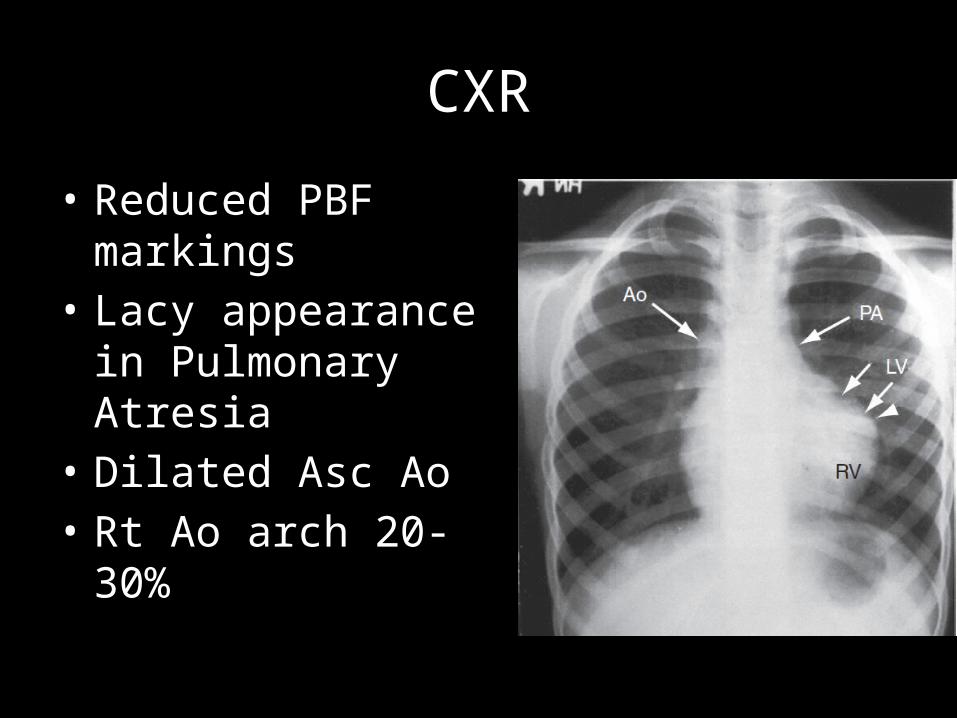
• Reduced PBF markings• Lacy appearance in
Pulmonary Atresia• Dilated Asc Ao• Rt Ao arch 20-30%
CXR
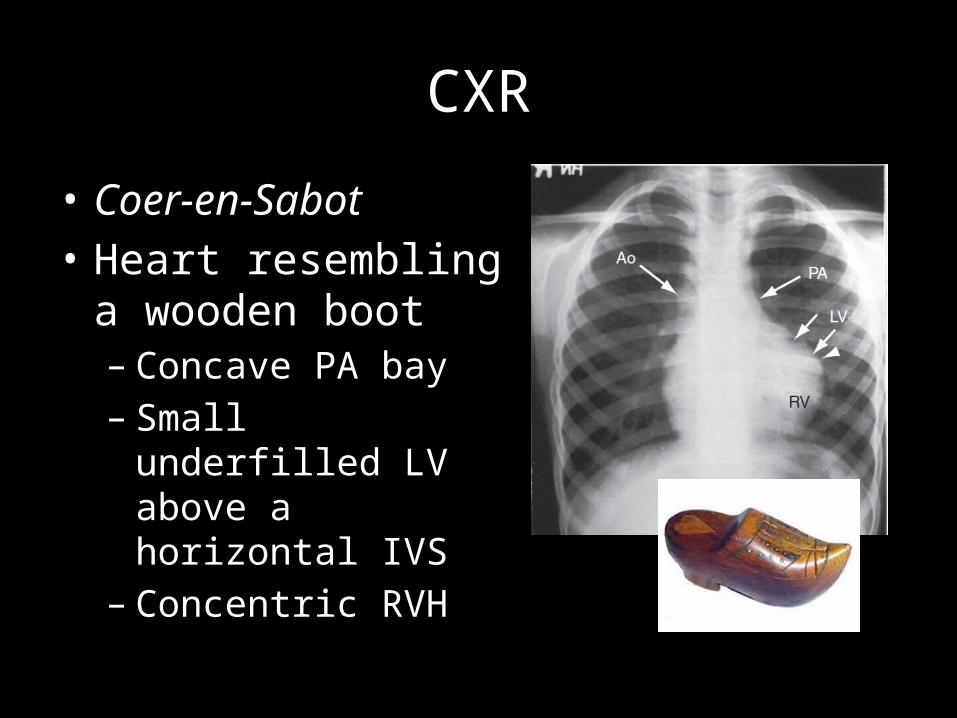
• Coer-en-Sabot• Heart resembling a
wooden boot– Concave PA bay– Small underfilled LV
above a horizontal IVS– Concentric RVH
CXR
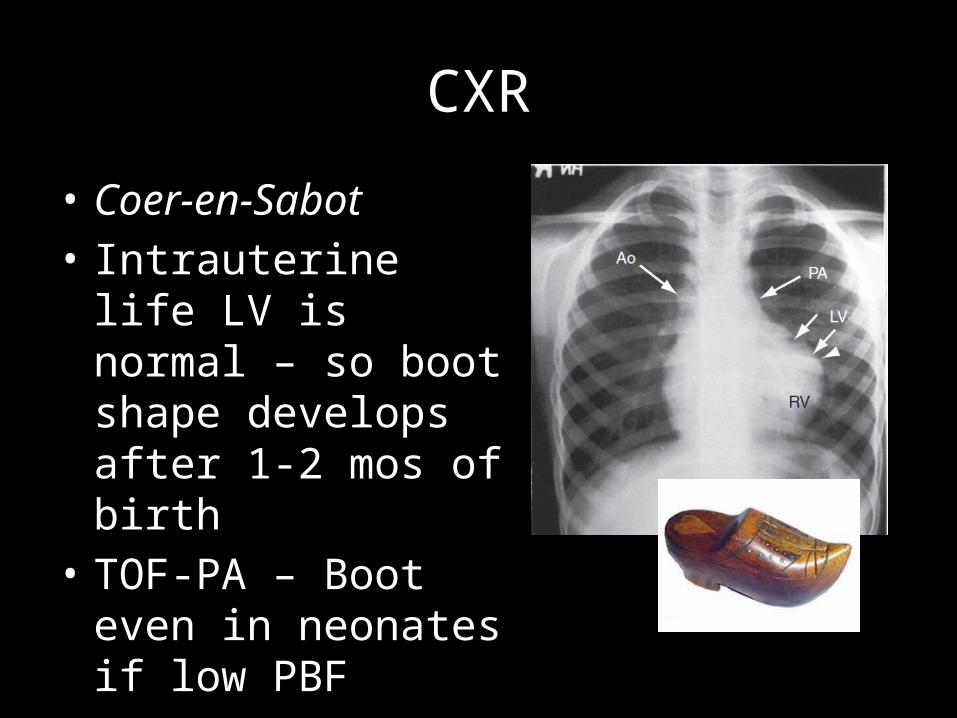
• Coer-en-Sabot• Intrauterine life LV is
normal – so boot shape develops after 1-2 mos of birth
• TOF-PA – Boot even in neonates if low PBF
DORV-VSD-PS
DORV
• Exact incidence unknown – Less than TOF
• Subaortic VSD 40-50% DORV
• PS 40-70% Subaortic VSD
DORV-PS
• History• Physical Exam• CXR
Same as TOF
DORV-PS
• Exceptions- If restrictive VSD present (Subaortic stenosis)• Long decrescendo systolic murmur at LPS area
(obligatory flow murmur)• ECG - LVH

DORV-PS
• Differentiation from TOF- ECG
- PR Prolonged- Counterclockwise depn- RVH but no sudden
transition
D-TGA – VSD – PS
D-TGA
• 1 in 2500-5000 live births• M>F 4:1
• VSD is most common communication
• PS (LVOTO) present in 15%
Symptoms/Presentation
• Cyanosis– Since birth – 1st day of life
• Hypercyanotic Spells– May be present occasionally
• Squatting– Rare
Natural History
• Mortality rate in TGA without PS– 30% 1st week– 50% 1st month– 90% 1st year
• Better survival with PS – may survive adolescence
Physical Exam
• Birth weight > normal (Contrast to other CHDs)
• Deep Cyanosis
• Scalp & Arm varicose veins (Systemic volume overload with desaturated blood)
• Pulse– Full volume bounding pulse– Warm extremities
• JVP– Elevated RAP with dominant A wave
(Systemic volume overload with desaturated blood)
• Palpation– RV impulse gentle at birth– Soon after 1 week – Prominent RV impulse
(Systemic volume overload with desaturated blood)– Rt sternoclavicular impulse – Rt arch
(11-16% in TGA-VSD-PS)
Just like TOF
• Auscultation– Just like TOF
ECG
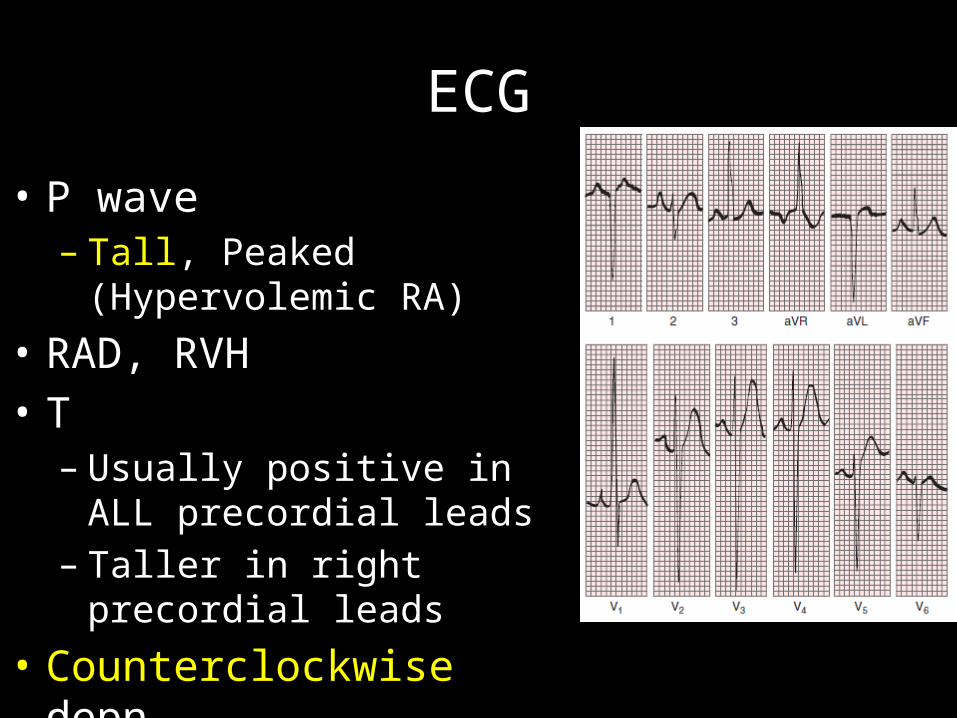
• P wave – Tall, Peaked (Hypervolemic RA)
• RAD, RVH• T– Usually positive in ALL
precordial leads– Taller in right precordial leads
• Counterclockwise depn
CXR
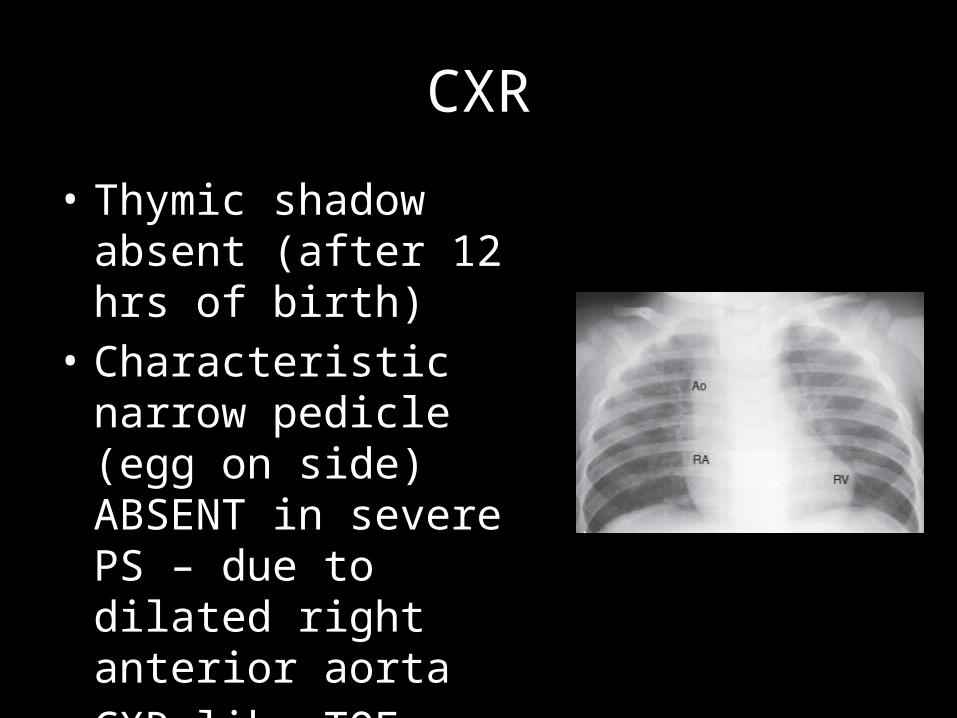
• Thymic shadow absent (after 12 hrs of birth)
• Characteristic narrow pedicle (egg on side) ABSENT in severe PS – due to dilated right anterior aorta
• CXR like TOF
L-TGA – VSD – PS
L-TGA
• 1 in 13000 live births• M>F 1.5:1
• VSD 80% L-TGA
• PS 50% L-TGA80% of PS a/w VSD
Symptoms/Presentation
• Cyanosis appearance according to PS severity• Spells and squatting uncommon• Older adults – Stokes-Adams & Syncope
(High degree AV blocks)
Natural History
• Better survival with VSD-PS – may survive adolescence
Physical Exam
• Like TOF
• Pulse– Normal– Bradycardia/Blocks
• JVP– Normal– 1st /2nd /3rd degree AV blocks
• Palpation– IVS almost vertical and parallel to left sternal border– Morph. RV – anterior & left position forming apex –
Systolic RV Impulse– Morph. LV – posterior & right position behind
sternum – LV Impulse non-palpable (even if enlarged)
– Ao EC & A2 palpable 2nd LICS
• Auscultation– Just like TOF– In case of blocks• Soft S1 – in 1st degree AVB• Variable S1 – High degree AVB
ECG
• AV Blocks maybe present– CHB – ventricular activation sequence normal;
QRS narrow• LAD (d/t LAFB)• RVH

• Q /q– Present in right precordial leads / absent in left
(Septal activation right to left directed)– Present in III, avf (III>avf) / absent in I, aVL
(Septal activation superiorly directed)• T– Usually positive in ALL precordial leads
• Clockwise depn
CXR
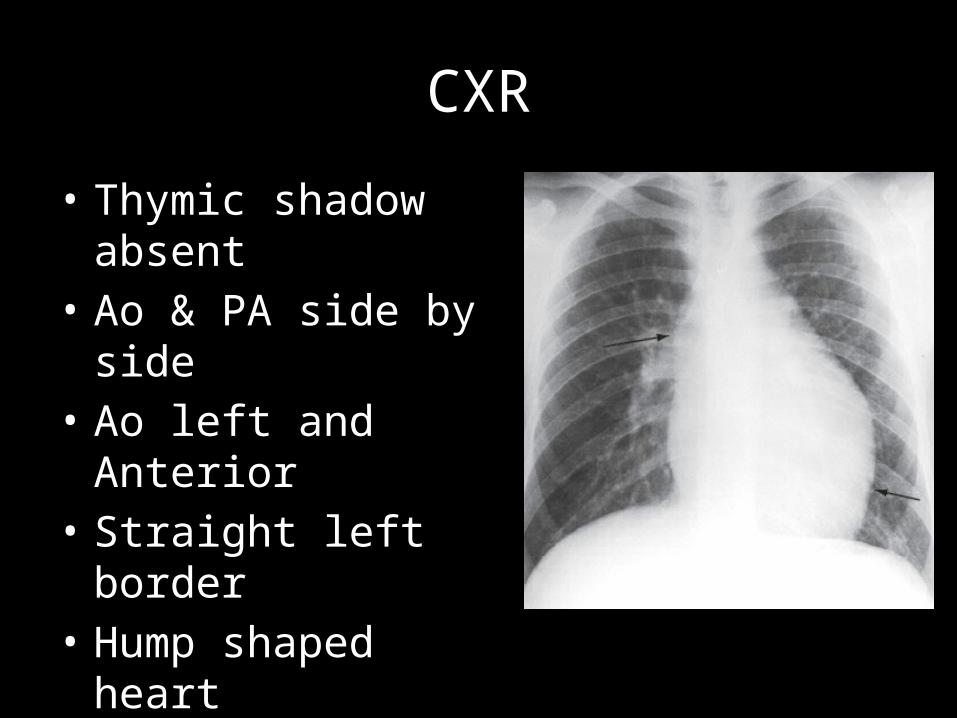
• Thymic shadow absent• Ao & PA side by side• Ao left and Anterior• Straight left border• Hump shaped heart• RPA and LPA at same
level
TRICUSPID ATRESIA – PS
Tricuspid Atresia (TA)
• 1 in 17000 live births
• 90% TA – No TGA
• 90% have Restrictive VSD – Physiologically PS
• 10% TA– TGA
• 90% have no PS – Increased PBF

Symptoms/Presentation
• Just like TOF

Natural History
• TA-NRGA-PS– 80% mortality in 1st yr– Already restrictive VSD – decreases in size and
closes! (Like a PM-VSD!)
– Acquired Pulmonary atresia without embryological collaterals – fatal!
Physical Exam
• Like TOF• No left precordial bulge – RV underdeveloped
• Pulse– Normal
• JVP– Height increased– A prom – PFO/Restrictive ASD/Decr LV compliance– V prom – MR
• Palpation– IVS almost vertical and parallel to left sternal border– Systolic LV Impulse (present even if low PBF)– RV Impulse non-palpable
• Auscultation– Single S1 (M1)– Single S2 (A2); P2 soft & delayed – maybe heard– LVS4 if unrestrictive VSD/LVH– Obligatory VSD holosystolic murmur• 3rd-4th LICS• Radiates to 2nd LICS• Duration shortens in closing VSD
ECG
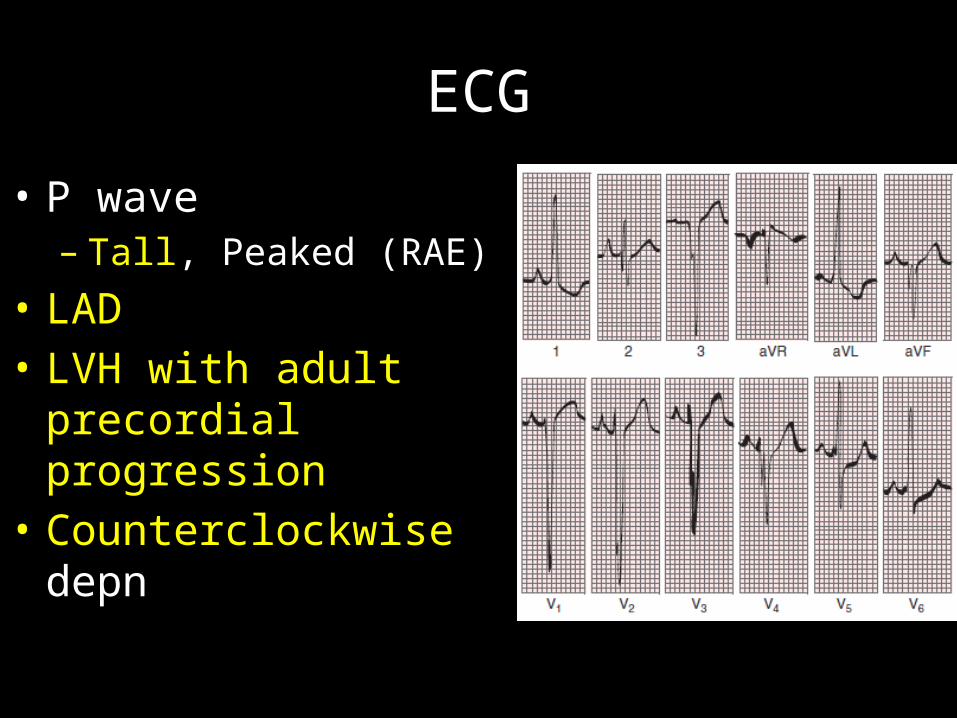
• P wave – Tall, Peaked (RAE)
• LAD• LVH with adult precordial
progression• Counterclockwise depn
CXR
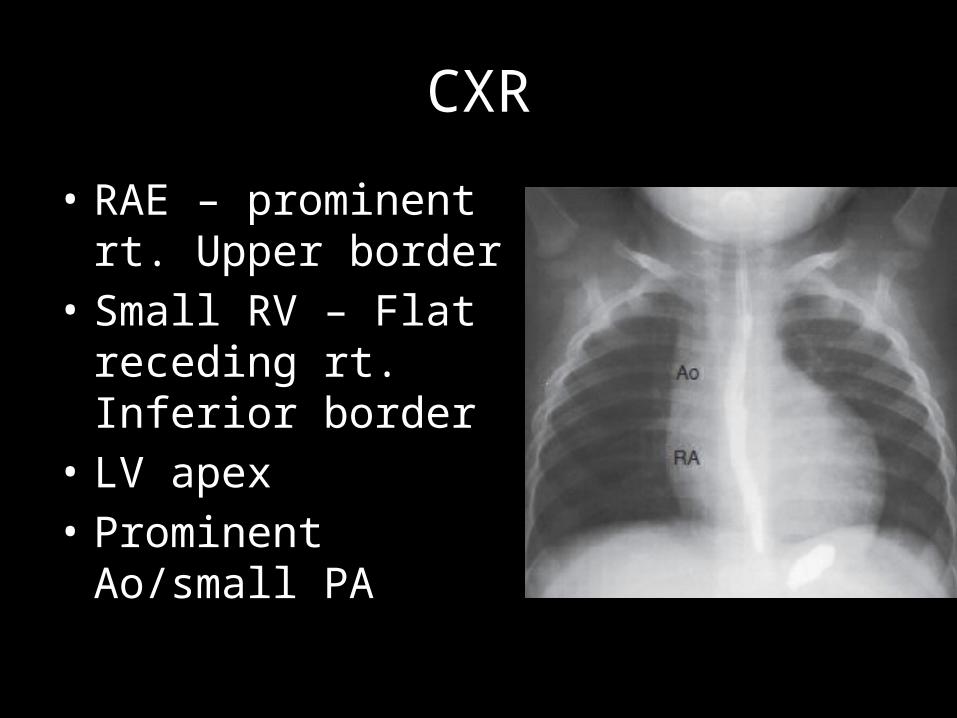
• RAE – prominent rt. Upper border
• Small RV – Flat receding rt. Inferior border
• LV apex• Prominent Ao/small PA
SINGLE VENTRICLE – PS
Single ventricle (SV)
• 1 in 20000 live births• M>F 2-4:1
• 80% SLV• 10% SRV• 10% Indeterminate
• SLV OC inverted (right); Noninverted (left)TGA present (Ao from OC; PA from SLV)
Symptoms/Presentation
• Cyanosis since birth
• Spells and squatting maybe present
Natural History
• SLV 50% mortality before 14 yrs
• SRV 50% mortality before 4 yrs

Physical Exam
• Like TOF
• Pulse– Normal
• JVP– Normal– V prom – if Rt AV valve regurgitant

• Palpation– Systolic LV Impulse at apex– 3rd LICS – palpable impulse due to inverted OC maybe
present
• Auscultation– Like TOF
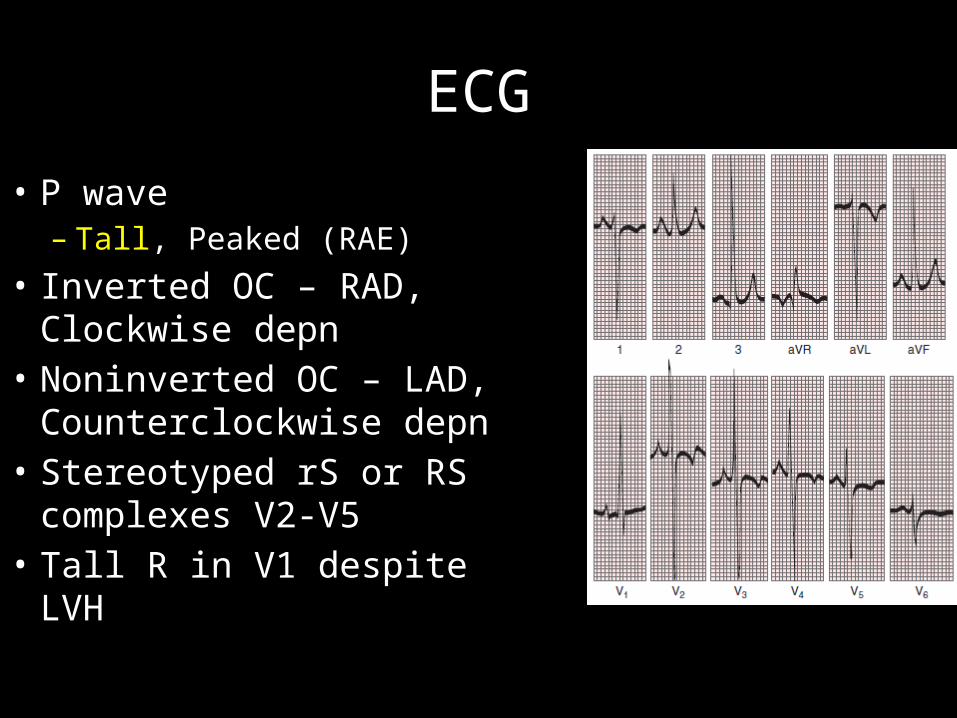
ECG
• P wave – Tall, Peaked (RAE)
• Inverted OC – RAD, Clockwise depn
• Noninverted OC – LAD, Counterclockwise depn
• Stereotyped rS or RS complexes V2-V5
• Tall R in V1 despite LVH
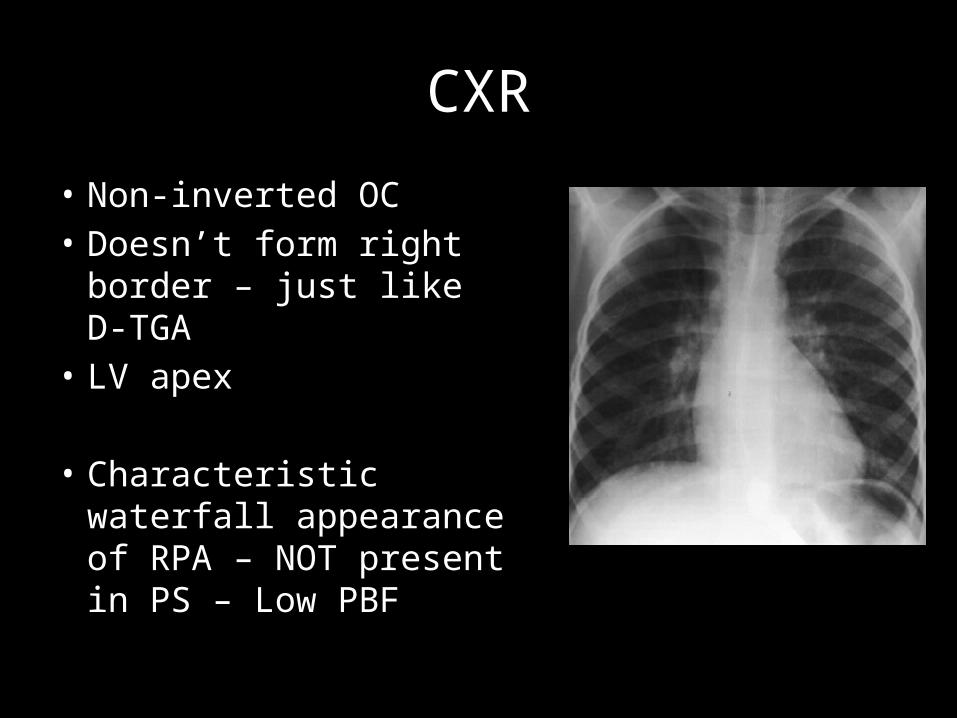
CXR
• Non-inverted OC• Doesn’t form right
border – just like D-TGA• LV apex
• Characteristic waterfall appearance of RPA – NOT present in PS – Low PBF
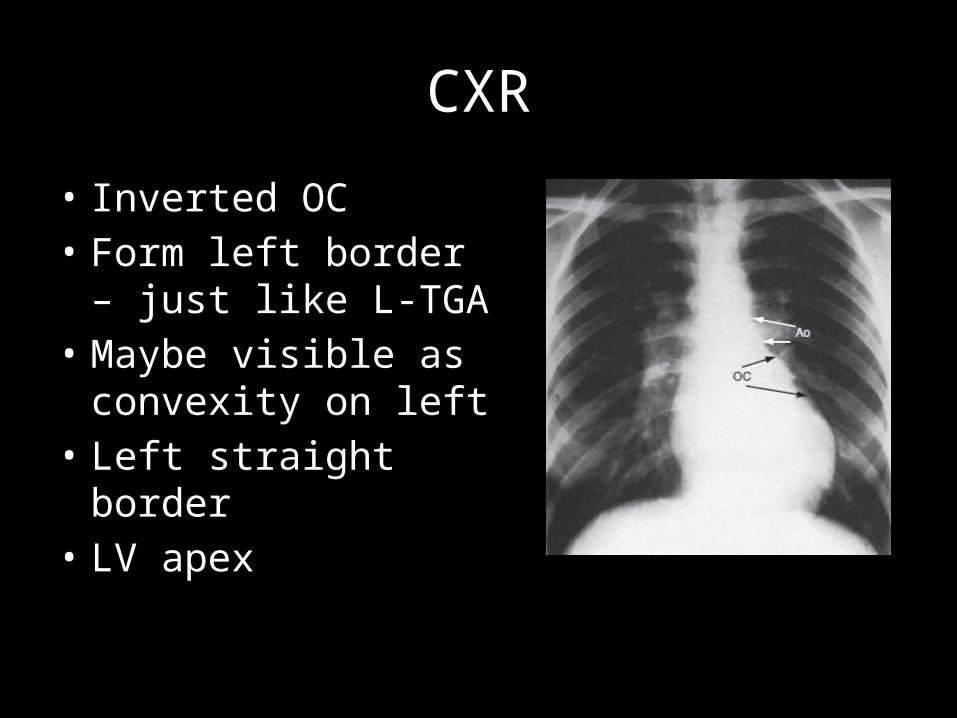
CXR
• Inverted OC• Form left border – just
like L-TGA• Maybe visible as
convexity on left• Left straight border• LV apex
APPROACH?
• Incidence acccording to age and natural history– Age of presentation?– Survival?
• PRESENTATION– Timing of cyanosis appearance?– Characteristic spells/squatting?
• Physical Exam– LV or RV predominent?
• ECG– LAD/RAD– Clock/Counterclock– LVH/RVH– AV Blocks
• CXR– Less helpful– LV/RV apex– Left Straightening