-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
1/86
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
2/86
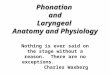
Relevant Anatomy
Fundamental components of speech
Theories of phonation
Glottic cycle
Factors affecting phonation
Objective evaluation of voice-Approach to
a patient with Hoarseness of voice
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
3/86
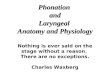
Situated at the upper endof trachea
Opposite 3rd6thcervicalvertebrae (males)
Higher in women andchildren
Infantssmaller, narrowlumen, funnel-shaped,
cartilages softer &
collapse easily
Larynx
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
4/86
Framework
Cartilages:
Thyroid cartilage
Cricoid cartilage
Aryetenoid cartilage
Corniculate and Cuneform
Vocal folds
Muscle
Intrinsic
Extrinsic
Nerve supply
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
5/86
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
6/86
THYROID CARTILAGE
Shield shaped cartilage Fused at midlineThyroid
notch ( 90* /120*)
Superiorly fusion absent-Thyroid notch
Posteriorly each ala has
superior and inferior horn Inferior horn articulates with
facet on cricoid cartilage-
Cricothyroid joint
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
7/86
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
8/86
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
9/86
Arytenoid cartilage
Paired catilages
Roughly Pyramidal in
shape Antero-lateral surfacehas vestibularligament,
thyroaryetenoid andvocalis muscle.
Posterior surface-muscular attachments
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
10/86
Corniculate cartilage:
cartilage of Santorini
Cuneform cartilage:
cartilage of Wrisberg
Are small pairedfibroelastic cartilages
Adds rigidity toaryepiglottic fold.
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
11/86
Extrinsic muscles
Elevators: elevates and displaces larynxanteriorly during
swallowing
Thyrohyoid
Stylohyoid Digastric
Geniohyoid
Mylohyoid
Stylopharyngeus
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
12/86
Extrinsic muscles
Depressors: displaces larynx downward duringinspiration
Omohyoid
Sternohyoid Sternothyroid
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
13/86
Intrinsic muscles
Muscles anatomicallyrestricted to larynx
Abductors:
Posterior cricoarytenoid
Adductors: Cricothyroid
Lateral cricoarytenoid
Interarytenoid
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
14/86
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
15/86
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
16/86
Posterior Cricoarytenoid
Attached to a depression onposterior surface of cricoid
lamina
and its fibers run obliquely superior andlateral and attach to
muscular process of
arytenoid. Contraction: abducts, elongates and
thins vocal fold.
Brings muscular process medially,posterior and inferior while
laterallyrotating and elevating vocal process.
Role in high pitch singing
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
17/86
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
18/86
Interarytenoid
Transverse and oblique fibres
Transverse fibres pass from posterior surface of onearytenoid to
the other
Contraction: brings together the arytenoid cartilages.
Assist closing post portion of glottis Only muscle having dual
innervation from Both RLN
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
19/86
Thyroarytenoid
T. internus T. externus
Contract - brings vocal process and adducts, shortenAnt
commissure closer to thickens and
each other lowers
the vocal fold
adducts true and false
vocal folds
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
20/86
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
21/86
Vocal cord
Antoine Ferrein coined the term
Located within larynx attached ant-thyroid cartilage and
post-arytenoid
cartilage
Male vocal folds -17.5 mm to25 mm
Female vocal folds -12.5 mm and17.5 mm
3-5 mm thickness
Folds are pearly white in color -more white in women than in
men.
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
22/86
Vocal Fold Vocal fold consists of five
layers:1. Squamous epithelium layer-
Very thin helps to hold the
shape of vocal cord.
2. Superficial layer of the laminapropria-loose fibres and
matrix
aka Reinkesspace
3. Intermediate layer-elastic &
collagenous fibres but more
than superficial layer
4. Deep layer-high concentration
of collagen bundles.
5. Vocalis: Main mass of the
vocal cord
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
23/86
Nerve Supply
Motor
Vagus
Sensory
Internal laryngeal nerve: supraglottis and the glottis
Recurrent laryngeal nerve: upper trachea and subglottis
SLN
RLN
Int
Ext Cricothyroid Muscle
Thyroarytenoid, Lateral cricoarytenoid,
Posterior cricoarytenoid, Interarytenoid
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
24/86
Theories of Nerve innervation
Semons law
Wagner & Grossman Theory
Modern theory
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
25/86
Semons Law
Rosenbach (1880) & Semon (1881)
In all progressive organic lesions, abductor fibres of
recurrent laryngeal nerve, which are phylogenetically
newer, are more susceptible and thus first to be
paralyzed compared to adductor fibres.
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
26/86
1ststage: only abductor fibres damaged; vocal folds
approximate in midline; adduction still possible
(paramedian position)
2ndstage: contracture of adductors; vocal folds
immobilized in median position
3rdstage: adductors become paralyzed; vocal fold
assumes cadaveric position
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
27/86
Abductors affected first ??
Nerve fibres supplying abductors are in periphery of
recurrent laryngeal nerve
Muscle bulk for the abductors is less, more
susceptible
Phylogenetically, larynxs main function is
protection, so adductor functions are maintained
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
28/86
Wagner & Grossman Theory
In isolated paralysis of recurrent laryngeal nerve,
cricothyroid muscle (innervated by SLN) keeps
vocal cord in paramedian position due to adductor
function
In both RLN and SLN palsy, cord lies in
intermediate (cadaveric) position.
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
29/86
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
30/86
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
31/86
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
32/86
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
33/86
Subsystem Voice Organs Role in Sound Production
Air Pressure System Diaphragm, chest muscles,
ribs, abdominal muscles
Lungs
Provides and regulates air
pressure to cause vocal
folds to vibrate
Vibratory System Voice box (larynx)
Vocal folds
Vocal folds vibrate,
changing air pressure to
sound waves producing"voiced sound," which is
frequently described as a
"buzzy sound"
Varies pitch of sound
Resonating System Vocal tract: throat
(pharynx), oral cavity, nasal
passages
Changes the "buzzy sound"
into a person's recognizable
voice
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
34/86
Sound is produced when aerodynamic phenomena
cause vocal folds to vibrate rapidly in a sequence ofvibratory
cycles with a speed of about:
110 cycles per second or Hz (men) = Low pitch
180 to 220 Hz (women) = Medium pitch
300 Hz (children) = Higher pitch
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
35/86
PHONATION:
Physical act of sound production by means of
passive vocal fold interaction with the exhaled air stream.
Prerequisites:
Adequate respiratory support.
Appropriate glottal closure.
Favourable vibratory properties.
Favourable vocal fold shape.
Control of vocal fold length and tension are required.
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
36/86
THEORIES OF PHONATION
I. Neuromuscular theory / Clonic Theory /
Neurochronaxic Theory of Husson, 1953
II. Myoelastic Aerodynamic Theory of Van den Berg,
1958
III. Body- Cover theory/Two Mass Model
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
37/86
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
38/86
Myoelastic Aerodynamic Theory
Widely accepted theory- Van den berg
AERO - air pressure and flow
DYNAMIC - movement and change
MYO - muscular involvement ELASTIC - ability to return to
original state
States that interaction of
aerodynamic forces and
mechanical properties of the laryngeal tissues areresponsible
for inducing vocal fold vibration and
generating vocal sound.
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
39/86
Body- Cover theory
Hirano According to this, the vocal folds
consist of a multi-layered
vibrator with increasing stiffnessfrom the cover to the
body.
The cover is responsible for mostof the vibratory action of
thevocal folds
Theory can be applied only inmodal register but not in high
orlower pitch
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
40/86
Air is moved out of the lungs and towards the vocal folds.
Vocal fold vibrationsequence of Vibratory cycles/Glottic
cycles
The nose, pharynx and mouth amplify and modify sound,
allowing it to take on the distinctive qualities of voice
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
41/86
Glottic Cycle
Adduction of Vocal Folds by voice box muscles, andcartilage.
Expiration of air from lungs Subglottic pressure.
Air pressure increases below the glottis until folds forced
apart.
Subglottic pressure more than vocal fold resistance.
Air flow passes through narrowed glottis.
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
42/86
1 Column of air
pressure moves
upwards towards
vocal folds in
"closed" position.
2, 3Column of air
pressure opens
bottom of vibrating
layers of vocal folds;body of vocal folds
stay in place.
4, 5Column of airpressure continues
to move upwards,
now towards the top
of vocal folds and
opens the top.
610 The low
Pressure created behind
the fast-moving air
column produces a"Bernoulli effect"
which causes the
bottom to close,
followed by the top.
10Closure of the vocal
folds cuts off the air
column and releases a
pulse of air
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
43/86
Factors causing return of Vocal folds to
midline1. Air travels faster through the glottis when it is
narrow. This causes a local drop in air pressure
(Bernoulli effect)whichcauses the folds to be
sucked towards each other.
2. Elastic forces in vocal folds.
3. Transglottal pressure
4. Subglottic pressure
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
44/86
CHARACTERISTICS OF SOUND
SOURCE or GLOTTIC SIGNAL
Quality
Frequency
Amplitude
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
45/86
Quality
Depends on: Nature of vocal cords adduction during
phonation.
Regularity of mucosal waves of lamina propria.
1. Incomplete adductionBreathy voice
2. Insufficient vocal cord adduction for vibration but
sufficient
to produce audible turbulent airWhisper
3. Irregular mucosal waveform vibrationHoarse
4. Vocal cords strongly adducted + raised subglottal air
pressurePressed or Strained voice
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
46/86
Frequency
Number of vibratory cycles/ sec (measured in Hertz)
Frequency with:
Length of vocal cord Thinning and stiffening of vocalis
muscle
Jitter or Pitch perturbationshort term variance in
frequency of vocal cord vibration
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
47/86
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
48/86
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
49/86
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
50/86
MODAL REGISTERAka Heavy voice
Speech and singing frequency (F0100 to 300Hz)
Vocal foldscomplete adduction, triangular in cross
section
Larynxpulled down; PharynxNormal
Vibration slowly and whole length.
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
51/86
PULSE REGISTER
Aka Glottal fry, Vocal fry or Creaky voice
Reflects pulsatile nature of laryngeal sound generated
Occurs during lowest frequency (F020 to 60Hz)
Feature of normal speech
Larynxnormal; Pharynxnormal
Vocal cordlong closed phase
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
52/86
Modification of Glottic signalRaw Glottic Signal Modified into
speech by
RESONANCE ARTICULATION
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
53/86
VOCAL RESONANCE
TYPES
ORAL RESONANCE NASAL RESONANCE
AFFECTED BY:
1. Degree of jaw movt.
2. Mouth opening
3. Tongue raising4. Pharygeal
constriction
AFFECTED BY:
Velopharyngeal sphincter
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
54/86
ARTICULATION
Synchronized movements of the organs of articulation
(e.g.Palate, Tongue, Lips) to change Glottal soundRecognizable
speech
Described by SOURCE FILTER MODEL
SOURCE LARYNX
FILTERSLips , Tongue, Palate ,Pharynx
( Forms Consonants and Vowels)
Articulatory movement are of two typesVowels and Consonants
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
55/86
VOWELS
These are sounds in which
there is no obstruction to
flow of air as it passes
from larynx to lips. Eg : A, E, I, O, U
Different vowels are
produced by :
Height of tongue
raising in mouth
Part of tongue raised
Position of lips (spread or
rounded)
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
56/86
CONSONANTS
Sounds produced when there is more definitiveobstruction to air
by one or more articulator in theoral tract
Eg : P, B, M, W, F, T, S, Z, R
Different consonants are produced by :
- Place of articulation- Manner of articulation
- State of larynx
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
57/86
CONSONANTS
Bilabial
Dental
Labiodental
Alveolar
PalatalVelar
Glottal
Based on place
of articulation
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
58/86
CONSONANTS BASED ON PLACE OF
ARTICULATION
BILABIAL
Articulation
between Upperand lower lip
P, B, M,W
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
59/86
LABIODENTAL
Top teeth and lower
lip
F, V
CONSONANTS BASED ON PLACE OF
ARTICULATION
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
60/86
DENTAL
Tongue tip and top
teeth occlusion
th in th ink
th in th at
CONSONANTS BASED ON PLACE OF
ARTICULATION
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
61/86
ALVEOLAR
Tongue tip touching ridge
behind the teeth
T, D, N, S, Z, R, ch, dj
CONSONANTS BASED ON PLACE OF
ARTICULATION
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
62/86
PALATAL
Articulation of
middle tongue withhard palate
Y
CONSONANTS BASED ON PLACE OF
ARTICULATION
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
63/86
VELAR
Articulation ofposterior tongue and
soft palate
K, G, ng
CONSONANTS BASED ON PLACE OF
ARTICULATION
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
64/86
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
65/86
CONSONANTS BASED ON STATE
OF LARYNX Consonants are paired- here only difference is whether
their
articulation is accompanied by voicing or not.
Eg: p and b, t and d, k and g, s and z
Can be either:
Voiced b, d, g, z
Voicelessp , t, k, s, hno vibration of vocal cords
h does not have a voiced twin so in connected
speech,vocalization is not continuous.
Phonation is switched on and off to signal voiceless
consonants.
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
66/86
Workup
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
67/86
Workup
ANY PATIENT WITH HOARSENESS OF TWOWEEKS DURATION OR LONGER
MUST
UNDERGO VISUALIZATION OF THE VOCAL
CORDS
EVALUATION OF A PATIENT WITH
HOARSENESS INCLUDES THE FOLLOWING:-
- History
- Clinical examination
- Investigations
HOARSENESS
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
68/86
History
Duration
Character of onset ( Sudden / gradually progressive)
Constant or intermittent Vocal nodule/ Chr. laryngitis
Associated symptoms: Cough/ dyspnoea/ dyphagia/ fever
Diurnal variation:
Chronic laryngitis-worse in morning Malignancy- worse in
evening
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
69/86
Potential triggering factors (Vocal abuse, URTI,
Change in medications, Exposure to known allergens)
Exacerbating and ameliorating factors, such as
improvement with voice rest, or fatigue with use
Other head and neck symptoms (eg, dysphagia,otalgia,
odynophagia)
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
70/86
History
Past H/o:
History of past surgery involving the neck (especially
thyroid, carotid, and cervical spine), base of skull, or
chest
History of trauma or endotracheal intubation
History of reflux or sinonasal disease
Medical comorbidities which may affect voice (eg,
rheumatoid arthritis or tremor)
Psychological stress
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
71/86
Personal H/o:
History of smoking and alcohol use
H/o weight loss.
Occupation, hobbies, and habits impacting voice use
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
72/86
Differential diagnosis of hoarseness
Voice quality Differential diagnosis
Breathy Vocal cord paralysis
Abductor spasmodic dysphoniaFunctional dysphonia
Hoarse Vocal cord lesion
Muscle tension dysphoniaReflux laryngitis
Low-pitched Reinke's edema
Vocal abuse
Reflux laryngitis
Vocal cord paralysis
Muscle tension dysphonia
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
73/86
Differential diagnosis of hoarseness
Voice quality Differential diagnosis
Strained Adductor spasmodic dysphonia
Muscle tension dysphoniaReflux laryngitis
Tremor Parkinson disease
Essential tremor of the head and neck
Spasmodic dysphonia
Muscle tension dysphonia
Vocal fatigue Muscle tension dysphoniaVocal cord paralysis
Reflux laryngitis
Vocal abuse
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
74/86
Examination of the nose for patency, obstructing
lesions, foreign body, or evidence of allergy
Examination of the oral cavity for mass lesions,
mucosal abnormalities, tonsil size, and motorfunction of the
palate and tongue
Palpation of the neck for mass lesions
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
75/86
LARYNGEAL EXAMINATION
INDIRECT LARYNGOSCOPY
FLEXIBLE LARYNGOSCOPY
RIGID LARYNGOSCOPY
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
76/86
INDIRECT LARYNGOSCOPY
AdvantagesQuick
Inexpensive
Minimum
Equipment
Disadvantages
Gag
Non physiologic
No permanent
image capability
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
77/86
DIRECT LARYNGOSCOPY
70 or 90-degreetelescope.
Advantages:
Best optic image Magnifies image
Video documentation
Disadvantages:
Gag,
Non physiologic
Expensive
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
78/86
FLEXIBLE LARYNGOSCOPY
Advantages:Well tolerated
Physiologic
Video documentationpossible
Disadvantages:
Time consuming
Expensive
Resolution limited by
fiberoptics
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
79/86
RIGID LARYNGOSCOPY
Advantages:Best images
Video
documentation
Disadvantages:
Expensive
Nonphysiologic
Gag
Requirement of
General Anaesthesia
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
80/86
VIDEOSTROBOSCOPY
Done to evaluate the vibratory patterns of the vocal folds
thatoccur too rapidly to be visualized by the unaided human
eye.
Is an illusion of slow motion
Light source - flashing Xenon tube
Permits accurate visualization of epithelial abnormalities
whichare missed out on IDL due to fast vibrations
Evaluation criteria include:
1. Symmetry
2. Amplitude
3. Periodicity
4. Mucosal wave propagation
5. Glottal closure.
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
81/86
OTHER TESTS
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
82/86
OTHER TESTS
LABS: TFT
PLAIN FILMS: Chest xray, Lateral Neck, Foreign body r/o.
CT SCAN: Cancer, Unknown diagnosis, Persistent or
recurrent pain and hoarseness, trauma.
MRI : R/o Multiple cranial neuropathies- Evaluate skull base
and brainstem.
LARYNGEAL EMG
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
83/86
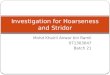
LARYNGEAL EMG One of the most specific and sensitive test to
determine the presence
of vocal fold paralysis. Differentiate Bilateral vocal fold
fixation and Neurogenic Vocal fold
paralysis
To confirm the presence of dystonia and in identifying which
muscles
are most involved. MyogenicNormal frequency of firing but
decreased amplitude (A)
NeurogenicDecreased frequency but occasional normal
amplitudes
(B)
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
84/86
PANENDOSCOPYINDICATIONS
To do biopsy of suspicious lesions
Laryngeal cancerTumour extend, any secondaries
Hoarseness patients without any diagnosis at the end of all
routine investigations.
Persistent or recurrent vocal symptoms
Patients with malignancies with new onset of hoarsenss.
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
85/86
References Ballengers 16thedition
Scott brown 7thedition
Cummings 5thedition OCNA 40 (2007) 991-1001
NCVS.org-national centre for voice and speech.
Voiceproblem.org ( Washington voice consortium)
-
8/10/2019 Physiology of Phonation and Approach to a Pt With
Hoarseness
86/86
Thankyou