Embed Size (px)
DESCRIPTION
Citation preview

1
Real-World Comparative Effectiveness and Safety of Rivaroxaban and Warfarin in Nonvalvular Atrial Fibrillation Patients
François Laliberté1; Michel Cloutier1; Winnie W. Nelson2; Craig I. Coleman3; Dominic Pilon1; CV Damaraju2; Jeffrey R. Schein2; Patrick Lefebvre1
1Analysis Group, Inc., Boston, MA; 2Janssen Scientific Affairs, LLC, Raritan, NJ; 3Univ of Connecticut & Hartford Hosp, Hartford, CT; AHA Scientific Session, November 16-20, 2013, Dallas, TX

2 2
Disclosures
● Financial support for the research was provided in whole by Janssen Scientific Affairs, LLC (JSA)
● François Laliberté, Michel Cloutier, Dominic Pilon, and Patrick Lefebvre are employees of Analysis Group Inc., a consulting company that has received research grants from JSA
● Craig I. Coleman is a Professor at University of Connecticut School of Pharmacy and Co-Director of the University of Connecticut/Hartford Hospital Evidence-Based Practice Center. He has received research grants from JSA and serves as a member of Janssen speaker bureau
● Winnie W. Nelson, CV Damaraju, and Jeffrey R. Schein are employees of JSA and stockholders of Johnson & Johnson

3 3
Background
● Chronic anticoagulants are regularly used in the prevention of stroke in patients with nonvalvular atrial fibrillation (NVAF)
● Until recently, warfarin and other oral vitamin-K antagonist (VKA) anticoagulants were the only oral anticoagulants available for stroke prevention
● Target-specific oral anticoagulants (e.g., rivaroxaban, dabigatran, apixaban) were approved for the prevention of stroke and systemic embolism in patients with NVAF
● The ROCKET-AF trial has demonstrated that rivaroxaban is effective in reducing the risk of stroke and systemic embolism
● The objective of this study was to assess real-world effectiveness, safety, and patients’ continued use of rivaroxaban and warfarin (i.e. persistence)

4 4
Methods - Data Source
Symphony Health Solutions Patient Transactional Datasets from May 2011 to July 2012
• Longitudinal patient data source with data from adjudicated medical and pharmacy claims
• Contains approximately 4.8 billion prescription claims across the U.S. for all payment types (e.g., commercials plans, Medicare Part D, assistance programs, and Medicaid)
• Linked with claims from hospital and physician practices for over 190 million patients
• Data de-identified in compliance with HIPAA

5 5
Methods - Study Sample
Inclusion criteria • Newly initiated on rivaroxaban or warfarin (at least 180 days of
clinical activity prior to the index date) • Age greater than or equal to 18 years • CHADS2 score ≥1 during the 180-day baseline period • ≥2 AF diagnoses (ICD-9-CM: 427.31) during baseline or follow-up
Exclusion criteria • Patients with the following conditions:
─ Valvular involvement ─ Pregnancy ─ Malignant cancer ─ Transient causes of AF

6 6
Methods - Study Design
● Retrospective matched-cohort design ensured groups were well balanced at baseline
● Each rivaroxaban user matched with up to 4 warfarin users based on propensity score
● The observation period spanned from the index date until: − End of clinical activity, or − End of data availability
● In addition, for clinical endpoints, observation period is further restricted to − Switch of anticoagulant, or − 14 days after treatment discontinuation

7 7
Methods - Study Endpoints
● Safety • Major bleeding • Gastrointestinal (GI) bleeding
● Effectiveness* • Composite stroke and systemic embolism
─ Ischemic stroke ─ Hemorrhagic stroke ─ Systemic embolism
• Venous thromboembolism (VTE) ─ Deep vein thrombosis (DVT) only ─ Pulmonary embolism (PE) with or without DVT
● Medication persistence to the index therapy
* Events identified during a hospitalization or emergency department visit

8 8
Statistical Methods
● Descriptive statistics to summarize the patient characteristics and compared using standardized differences
● Cox proportional hazard regressions to calculate hazard ratios (HRs) of bleeding (major and GI), composite stroke and systemic embolism, and VTE events between groups
● Kaplan-Meier estimates and HRs to compare the time to non-
persistence − Non-persistence defined as having a refill gap of 60 days or larger

9 9
Patients Characteristics
Characteristics
Matched Cohort
Rivaroxaban Warfarin Standardized Difference (N=3,654) (N=13,876)
Demographics Age, years, mean (SD) 73.3 (8.4) 73.7 (8.3) 4.6% Gender, female, n (%) 1,865 (51.0%) 7,159 (51.6%) 1.1%
Quan-Charlson comorbidity index 1.1 (1.3) 1.2 (1.4) 3.3% CHADS2 score 2.0 (1.0) 2.0 (1.0) 2.2% Selected baseline risk factors , n(%)
Age > 60 3,313 (90.7%) 12,681 (91.4%) 2.5% Prior stroke 357 (9.8%) 1434 (9.8%) 3.4% Hypertension 2,626 (71.9%) 9,761 (70.3%) 3.4% Hyperlipidemia 1,616 (44.2%) 6,032 (43.5%) 1.5% Diabetes 919 (25.2%) 3,599 (25.9%) 1.8% Heart failure 716 (19.6%) 2,858 (20.6%) 2.5%

10 10
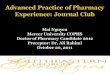
Hazard Ratios of Study Endpoints
†Event identified during a hospitalization or emergency department visit
0 1 2 3Rivaroxaban better Warfarin better
Rivaroxaban vs. Warfarin Hazard Ratios [95% CI]
Major bleeding
DVT only† PE with or without
DVT†
GI bleeding Composite stroke and
systemic embolism†
Hemorrhagic stroke†
Systemic embolism†
Ischemic stroke†
1.03 [0.68 - 1.56]
1.06 [0.40 - 2.80]
1.26 [0.98 - 1.62]
0.81 [0.58 - 1.15]
0.83 [0.59 - 1.18]
1.10 [0.12 - 9.86]
0.78 [0.17 - 3.50]
0.55 [0.25 - 1.21]

11 11
Treatment Persistence
60%
70%
80%
90%
100%
0 30 60 90 120 150 180
% o
f pat
ient
s per
sist
ent w
ith tr
eatm
ent
Time to event (days)
Warfarin User Cohort
Rivaroxaban User Cohort
85%
76%
81%
68%
HR = 0.66 (0.60-0.72), P<0.001

12 12
Limitations
● Claims database may contain inaccuracies or omissions in coded procedures, diagnoses, or pharmacy claims
● Propensity score matching only accounts for observable factors
● Despite matching, the observational nature of the analysis still carries the possibility of confounding
● Study was conducted when rivaroxaban was first available; use patterns may change over time

13 13
Conclusions
● This analysis suggests that rivaroxaban and warfarin do not differ significantly in real-world rates of composite stroke and systemic embolism, major bleeding, and GI bleeding
● Rivaroxaban was associated with a significantly higher treatment persistence compared with warfarin





![Single Dose Bioequivalence Study of Two Rivaroxaban Tablet ...€¦ · drug [3], rivaroxaban did not fulfil the waiver criteria for crushed bioequivalence testing. Therefore, after](https://img.pdfslide.us/doc/110x75/5f024c737e708231d403933a/single-dose-bioequivalence-study-of-two-rivaroxaban-tablet-drug-3-rivaroxaban.jpg)