Embed Size (px)
Citation preview

ThrombosisDr. Peter J. Lin
Director Primary Care Initiatives
Canadian Heart Research Centre

Copyright © 2017 by Sea Courses Inc.
All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means – graphic, electronic, or mechanical,
including photocopying, recording, or information storage and retrieval systems without prior written
permission of Sea Courses Inc. except where permitted by law.
Sea Courses is not responsible for any speaker or participant’s statements, materials, acts or omissions.



Platelet
Fibrin
Red blood cell

Fast Flowing
Platelets Stick First

Slow Flow
Coagulation First


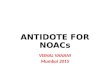
Stroke Burden Of Atrial Fibrillation
60%
20%
0%
20%
40%
60%
80%
100%
Disabling Fatal
QoL: quality of life.
1. Gladstone et al. Stroke. 2009;40:235; 2. Gage et al. Arch Intern Med. 1996;156:1829;
3. Solomon et al. Stroke. 1994;25:1721.
9
Impact of ischemic stroke in patients with AF (n=597)1
Many patients view QoL
following a severe stroke as
equal to or worse than
death2,3
Next

The Impact of Atrial Fibrillation (AF) in Canada
10
• Approximately 350,000 Canadians are living with AF1
‒ 25% of Canadians >40 years of age will develop AF2
• AF increases the risk of ischemic stroke by 3 to 5 times1,3
‒ AF-related strokes are associated with higher rates of morbidity and mortality
than non-AF-related strokes4,5
• With AF, annual stroke rate is 4.5%6
‒ About 16,000 AF-related strokes per year in Canada (about 20% of all strokes7)
1. Canadian Heart and Stroke Foundation. https://www.heartandstroke.ca/heart/conditions/atrial-fibrillation Accessed January 9, 2017. 2. Lloyd-Jones DM, et al. Circulation 2004;110:1042–6.
3. European Heart Rhythm Association, et al. Eur Heart J 2010;31:2369-429. 4. Dulli DA, et al. Neuroepidemiology 2003;22:118-23. 5. Marini C, et al. Stroke 2005;36:1115-9.
6. [No authors listed]. Arch Intern Med 1994;154:1449-57. 7. Wolf PA, et al. Stroke 1991;22:983-8.

Warfarin (Wisconsin Alumni Research Foundation)
• Warfarin is the most widely used coumarin derivative
• Originally found in sweet clover
Sweet clover


100% 50% 0% -50% -100%
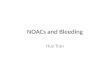
AFASAK-1 (n=671)
SPAF (n=421)
BAATAF (n=420)
CAFA (n=378)
SPINAF (n=571)
EAFT (n=439)
All Trials (n=2900)
Warfarin Better Warfarin Worse
64%
Stroke Prevention in AF 6 Trials of Warfarin vs. Placebo
13Hart RG, et al. Ann Intern Med 2007;146:857-67.
AFASAK: Atrial Fibrillation, Aspirin, AntiKoagulation; SPAF: Stroke Prevention in Atrial Fibrillation;
BAATAF: Boston Area Anticoagulation Trial for Atrial Fibrillation; CAFA: Canadian Atrial Fibrillation Anticoagulation;
SPINAF: Stroke Prevention in Nonrheumatic Atrial Fibrillation; EAFT: European Atrial Fibrillation Trial
Warfarin Has Been Shown to Reduce Stroke Risk in AF

Hylek EM, et al. NEJM 1996;335:540-546.
INR below 2.0 results in a higher risk of
stroke
Lowest Effective Intensity for Warfarin Therapy for Stroke Prevention in Atrial Fibrillation

Hylek, et al, studied the risk of intracranial hemorrhage in outpatients treated with warfarin. They determined that an intensity of anticoagulation expressed as a prothrombin time ratio (PTR) above 2.0 (roughly corresponding to an INR of 3.7 to 4.3) resulted in an increase in the risk of bleeding.
Adapted from: Hylek EM, Singer DE, Ann Int Med
1994;120:897-902
Risk of Intracranial Hemorrhage in Outpatients

Copyright ©2006 American Heart Association
Fuster, V. et al. Circulation 2006;114:e257-e354
Adjusted odds ratios for ischemic stroke and intracranial bleeding in relation to intensity of anticoagulation
INR 2-3
Warfarin Reduce Stroke Risk in AF 64%

Warfarin – mechanism of action
Vitamin K
Synthesis of functional
coagulation factors
VII
IX
X
II

Warfarin – mechanism of action
Vitamin K
Synthesis of non-functional
coagulation factors
VII
IX
X
II
Warfarin

Warfarin – mechanism of action

Food interactions
Green leafy vegetables counteract effects of warfarin
• Foods with high amounts of vitamin K, e.g:
‒ Cauliflower
‒ Green cabbage
‒ Seaweed (1350)
‒ Broccoli (270)
‒ Green tea
‒ Turnip greens
‒ Soybean oil (often used to fry foods in restaurants)
‒ Raw spinach
Vitamin K


0
2
4
6
8
10
12
14
16
18
1 5 9 13 17 21 25 29 33 37 41 45 49 53 57 61
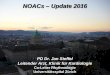
High Rates of Hemorrhage within 30 Days of Initiating Warfarin Therapy
22Gomes T, et al. CMAJ 2013;185:E121-7.
Incident rate of visits to hospital with hemorrhages in 30-day increments after the
start of warfarin therapy among older patients (≥ 66 yr) with AF
Rates are stratified by CHADS2 score at the start of treatment.
Inc
ide
nt
rate
of
he
mo
rrh
ag
e,
% p
er
pers
on
-year
Months
Overall Score 4-6Score 1

Clotting Cascade

II
VII
IX
X
protein C
protein S
• Vitamin K-dependent clotting factors have variable half-
lives
• Several days are required for maximal anticoagulant
effect of warfarin to be achieved
• Warfarin half-life is 2.5 days
Slow onset and offset of action
T½ 60 hours
4–6
24
48–72
8
30
Factors

Clotting Cascade
Direct Thrombin Inhibitor
(DTI)
Factor Xa inhibitor

26
Rate of Fatal Bleeding with NOACs
0.07
0.36 0.360.38
0.48
0.05
0.220.25
0.210.24
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
ARISTOTLE RE-LY
(D110 mg)
RE-LY
(D150 mg)
ENGAGE AF ROCKET-AF
Fa
tal B
lee
din
g E
ve
nts
(%
/ye
ar)
1. Apixaban (Eliquis) Product Monograph. Bristol-Myers Squibb Canada; 2. Dabigatran (Pradaxa) Product Monograph. Boehringer Ingelheim
Canada Ltd; 3. Giugliano et al. N Engl J Med. 2013;369:2093-104; 4. Rivaroxaban (Xarelto) Product Monograph.
Warfarin
Apixaban
Dabigatran 110 mg
Rivaroxaban
21 3
Fatal Bleeding is Reduced with NOACs vs. Warfarin with Rates <0.5%/year
Edoxaban
4
Dabigatran 150 mg
HR: 0.71
(0.25-1.95)
p=0.6183
HR: 0.61
(0.38-1.0)
p=0.0491
HR: 0.70
(0.44-1.12)
p=0.1338
HR: 0.55
(0.36-0.84)
p=0.006
HR: 0.50
(0.31-0.79)
p=0.003
2
*Not intended for cross study comparison

Other Bleeding Outcomes
27Giugliano RP, et al. N Engl J Med 2013;369:2093-104.
CRNM: clinically relevant nonmajor bleeding
Higher-dose edoxaban* vs. warfarin
0.55 (0.36-0.84)
p=0.006
0.47 (0.34-0.63)
p<0.001
1.23 (1.02-1.50)
p=0.03
0.51 (0.38-0.70)
p<0.001
0.86 (0.80-0.92)
p<0.001
Fatal
Intracranial
Gastrointestinal
Life-threatening
bleeding
Major or CRNM
*Dose reduced by 50% in selected pts
Warfarin betterEdoxaban better Hazard Ratio (95% CI)
1.0 2.00.10
Hazard ratio

Efficacy and Safety Benefits of NOACs vs. Warfarin from RCTs
Ruff CT, et al. Lancet 2014;383:955-62.
Ruff, Lancet, 2014, 383, 955
28
Stroke or systemic embolic events
Major bleeding
RR (95% CI) P
RE-LY (dabigatran 150 mg twice daily) 0.66 (0.53-0.82) 0.0001
ROCKET AF (rivaroxaban 20 mg once daily) 0.88 (0.75-1.03) 0.12
ARISTOTLE (apixaban 5 mg twice daily) 0.80 (0.67-0.95) 0.012
ENGAGE AF-TIMI 48 (edoxaban 60 mg once daily) 0.88 (0.75-1.02) 0.10
Combined (random) 0.81 (0.73-0.91) <0.0001
1.0 2.00.5Favours NOAC Favours Warfarin
Data are n/N, unless otherwise indicated. Heterogeneity: I2=47%; p=0.13. NOAC=non–vitamin K antagonist oral anticoagulants. RR=risk ratio.
RR (95% CI) P
RE-LY (dabigatran 150 mg twice daily) 0.94 (0.82-1.07) 0.34
ROCKET AF (rivaroxaban 20 mg once daily) 1.03 (0.90-1.18) 0.72
ARISTOTLE (apixaban 5 mg twice daily) 0.71 (0.61-0.81) <0.0001
ENGAGE AF-TIMI 48 (edoxaban 60 mg once daily) 0.80 (0.71-0.90) 0.0002
Combined (random) 0.86 (0.73-1.00) 0.06
Data are n/N, unless otherwise indicated. Heterogeneity: I2=83%; p=0.001. NOAC= non–vitamin K antagonist oral anticoagulants. RR=risk ratio.
1.02.00.5
Favours NOAC Favours Warfarin

Net Clinical Outcomes
29Giugliano RP, et al. N Engl J Med 2013;369:2093-104.
SEE: systemic embolic event
Higher-dose edoxaban* vs. warfarin
0.89 (0.83-0.96)
p=0.003
0.88 (0.81-0.97)
p=0.008
0.88 (0.81-0.96)
p=0.003
Stroke, SEE, death, major
bleeding
Disabling stroke, life-
threatening bleeding, death
Stroke, SEE, life-threatening
bleeding, death
Warfarin betterEdoxaban betterHazard ratio (95% CI)
1.00 1.500.50
Hazard ratio
0.75
*Dose reduced by 50% in selected pts

CHADS2 Score
1. JAMA. 2001;285(22):2864-2870. 2. Am J Med. 2010;123(6):484-488. 3. Can J Cardiol. 2012;28(2):125-136. 30
Quantifies stroke risk, aids in selection of antithrombotic therapy for risk
reduction
Letter Condition Points
C CHF 1
H Hypertension 1
A Age >75 years 1
D Diabetes 1
S2 Prior Stroke or TIA 2
CHADS2
score
Stroke rate per 100
patient-years
0 1.9
1 2.8
2 4.0
3 5.9
4 8.5
5 12.5
6 18.2

Can J Cardiol. 2016;32(10):1170-1185. 31
RECOMMENDATION:
We recommend that when
OAC therapy is indicated
for patients with non-
valvular AF, most patients
should receive dabigatran,
rivaroxaban, apixaban, or
edoxaban…in preference
to warfarin
(Strong Recommendation,
High-Quality Evidence).

Despite Increasing Use of NOACs in AF Globally, Many Patients Still Remain Untreated or Inappropriately Treated
32Camm AJ, et al. Heart 2017;103:307-14.
Evolution in Baseline Treatment for Patients Enrolled in Sequential Cohorts of GARFIELD-AF
Proportion of newly
diagnosed patients
with AF not prescribed
OAC
0
10
20
30
40
50
60
70
80
90
100
Cohort 1 Cohort 2 Cohort 3 Cohort 4
Pro
po
rtio
n o
f P
ati
en
ts o
n
Tre
atm
en
t, %
2010-2011
(n=5311)
2011-2013
(n=11,562)
2013-2014
(n=11,343)
2014-2015
(n=10,923)
12.4
30.2
4.2
53.2
11.5
26.1
13.8
48.5
12.9
20.1
26.3
40.8
12.4
16.6
37.0
34.0
VKA ± AP Fxa/DTI ± AP AP None
57.4%
29.0%
GARFIELD-AF: Global Anticoagulant Registry in the Field–Atrial Fibrillation; AP: antiplatelet; DTI: direct thrombin inhibitor; Fxa: factor Xa inhibitor; VKA: vitamin K antagonist
Proportion of newly
diagnosed patients
with AF prescribed
OAC
71.0%
42.6%

Total Drug Exposure (AUC) with Declining Renal
Function
≥80 50-79 30-49 <30
AU
C R
atio
vs.
No
rma
l R
en
al Fu
nc
tio
n
0
1
2
3
4
5
6
7
≥80 50-79 30-49 <30 ≥80 50-79 30-49 <30
Rivaroxaban4Apixaban1 Dabigatran2
Creatinine Clearance (mL/min)
Normal Renal Function: ≥80 mL/min; Mild Renal Impairment: 50-79 mL/min
Moderate Renal Impairment: 30-49 mL/min; Severe Renal Impairment: <30 mL/min
33
1. Apixaban (Eliquis) Product Monograph. Bristol-Meyers Squibb Canada; 2. Dabigatran (Pradaxa) Product Monograph.
Boehringer Ingelheim Canada Ltd.; 3. Edoxaban (Lixiana) Product Monograph. Progress Therapeutics; 4. Rivaroxaban (Xarelto)
Product Monograph. Bayer Inc.
≥80 50-79 30-49 <30
Edoxaban3

Common Methods for Assessing Renal
Function • Cockcroft-Gault
– Estimates CrCl based on age, weight, sex and creatinine
– Recommended equation for drug dose adjustments in
patients with renal impairment
• Modification of Diet in Renal Disease (MDRD)
– Estimates GFR based on age, race, sex and creatinine
– More accurately estimates renal function vs. Cockcroft-Gault
– Loses precision in patients with normal renal function and
might falsely suggest CKD
CKD: chronic kidney disease; CrCl: creatinine clearance; GFR: glomerular filtration rate.
1. Macle et al. Can J Cardiol. 2015;31:1207-18. 34
Kate’s eGFR according to MDRD:
52 mL/min/1.73 m2

Equations compared to Inulin
35Clin J Am Soc Nephrol 4: 899–906, 2009. doi: 10.2215/CJN.05371008
Cockcroft-Gault MDRD
GFR
REAL GFR
Calc GFR

Equations compared to Inulin
36Clin J Am Soc Nephrol 4: 899–906, 2009. doi: 10.2215/CJN.05371008
Cockcroft-Gault MDRD

Equations compared to Inulin
37Clin J Am Soc Nephrol 4: 899–906, 2009. doi: 10.2215/CJN.05371008
Cockcroft-Gault MDRD

Stroke Prevention in Patients with Renal
Impairment
How should we be treating patients with AF and renal impairment?

Therapeutic Choices for the Prevention of Stroke in Patients with CKD
*Consider Dabigatran 110 mg BID if age >80 or if the patient is at higher risk of bleeding, including elderly ≥75 years with ≥1 risk factor;
†Consider Apixaban 2.5 mg BID if 2 of 1) age ≥80 years, 2) body weight ≤60 kg, or 3) creatinine ≥133 μmol/L; ‡ARISTOTLE included a small
number of patients (1.5%) with a CrCl as low as 25 ml/min; ‖Dose adjusted warfarin has been used, but data regarding safety and
efficacy is conflicting; ¶No published studies; product monographs suggest the drug is contraindicated for this level of renal function.
1. Apixaban (Eliquis) Product Monograph. Bristol-Myers Squibb Canada; 2. Dabigatran (Pradaxa) Product Monograph. Boehringer
Ingelheim Canada Ltd.; 3. Edoxaban (Lixiana) Product Monograph. Progress Therapeutics; 4. Rivaroxaban (Xarelto) Product Monograph.
Bayer Inc; 5. Warfarin (Coumadin) Product Monograph. Bristol-Myers Squibb Canada.39
CrCl
(mL/min)
Apixaba
n1Dabigatran2 Edoxaban3 Rivaroxaban4 Warfarin5
>50 5 mg BID 150 mg BID* 60 mg daily 20 mg daily Dose
adjusted
for
INR 2.0-3.030-49
5 mg BID
(consider
2.5 BID)†
150 mg BID* 30 mg daily 15 mg daily
15-29 Limited
data‡
No RCT
data
Limited
data
No RCT
data
No RCT
data‖
<15
or dialysis
No RCT
data¶
No RCT
data¶
No RCT
data¶
No RCT
data¶
No RCT
data‖

Patients with AF and eGFR
≤30 mL/min
Patients with AF and eGFR
>30mL/minWarfarin
Apixaban
Dabigatran
Rivaroxaban
Edoxaban
CCS Guidelines Recommend NOACs for Eligible AF Patients
with eGFR ≥30 mL/min
40CCS: Canadian Cardiovascular Society; eGFR: estimated glomerular filtration rate.
1. Verma et al. Can J Cardiol. 2014:30;1114-30.

Dabigatran2
Dosing Algorithms in AFApixaban1
41
1. Apixaban (Eliquis) Product Monograph. Bristol-Meyers Squibb Canada; 2. Dabigatran (Pradaxa) Product Monograph.
Boehringer Ingelheim Canada Ltd.; 3. Edoxaban (Lixiana) Product Monograph. Progress Therapeutics; 4. Rivaroxaban
(Xarelto) Product Monograph. Bayer Inc.
Edoxaban3 Rivaroxaban4

Apixaban Dosing Algorithm
eCrCl: estimated creatinine clearance.
1. Apixaban (Eliquis) Product Monograph. Bristol-Meyers Squibb Canada. 42
Return to slide
Patient has risk factor for stroke
Estimate CrCl
≥25
mL/min
5 mg
BID
2.5 mg
BID
<15 mL/min
Not
recommendedCheck Age
Check
Weight
Check
Serum
Creatinine
≥80 years ≤60 kg≥133
micromol/L
If ≥2
features
If ≤1
features
≥15-24
mL/min
No dosing
recommendation
can be made*
*In patients with eCrCl
15-24 mL/min, no dosing
recommendation can
be made as clinical
data are very limited
Use 2.5mg bid(2 or more)
Age 80Weight 60kgCreatinine 133

Dabigatran Dosing Algorithm
Return to slide 431. Dabigatran (Pradaxa) Product Monograph. Boehringer Ingelheim Canada Ltd.
Patient has risk factor for
stroke
Estimate CrCl
<30 mL/min 30-50 mL/min>50
mL/min
Age
<75 years
Age
75-79
years
Age
≥80 years
150
mg
BID
110
mg
BID
150mg BID
Contra-indicated
150 mg BID
[Patients
with ≥1 risk
factor for
bleeding –
110 mg BID]
150
mg
BID
Is the patient at higher risk
of bleeding?
NoYes
110
mg
BID
Use 110mgBleeding risk Age > 80

Edoxaban Dosing Algorithm
*except amiodarone and verapamil.
1. Edoxaban (Lixiana) Product Monograph. Progress Therapeutics44Return to Slide
Patient has risk factor for stroke
Estimate CrCl
>50 mL/min
60 mg
OD
30-50 mL/min
30 mg OD
<30 mL/min
Not
recommended
Check
Weight
≤60 kg
Check
Medications
Concomitant
P-gp inhibitor?*
30 mg OD
30 mg OD
Use 30mg eGFR 30-50Weight 60Drug Pglycoprotein blockers
Cyclosporine, Dronedarone, Ketoconazole, Quinidine, Erythromycin

Rivaroxaban Dosing Algorithm
1. Rivaroxaban (Xarelto) Product Monograph. Bayer Inc. 45Return to Slide
Patient has risk factor for stroke
Estimate CrCl
30-49 mL/min >50 mL/min
20 mg
OD15 mg
OD
<30 mL/min
Not
recommended
Rivaroxaban is the only NOAC that prospectively studied a reduced dose based solely on renal function7
Use 15mg eGFR 30-50

Dose Considerations for the NOACs
NOAC Usual Starting Dose Dose Adjustment Criteria
Apixaban1 5 mg BID
2.5 mg BID if any 2 of the following criteria:
- Age ≥80 years
- Body weight ≤60 kg
- Creatinine ≥133 μmol/L
Dabigatran2 150 mg BID
110 mg BID if:
- Age ≥80 years
- At higher risk of bleeding, including elderly
≥75 years with ≥1 risk factor
Edoxaban3 60 mg QD
30 mg QD if:
- CrCl 30 to 50 mL/min
- Body weight ≤60 kg
- Concomitant use of P-gp Inhibitors except
amiodarone and verapamil
Rivaroxaban4 20 mg QD 15 mg QD if CrCl 30 to 49 mL/min
1. Apixaban (Eliquis) Product Monograph. Bristol-Myers Squibb Canada; 2. Dabigatran (Pradaxa) Product Monograph. Boehringer
Ingelheim Canada Ltd; 3. Edoxaban (Lixiana) Product Monograph. Progress Therapeutics; 4. Rivaroxaban (Xarelto) Product
Monograph. Bayer Inc. 46

Bleeding Risks for Invasive/Surgical Procedures
1. Macle et al. CJC. 2016;32:1170-85;
2. 2016 CCS AF Guidelines Corrigendum (Nov 29, 2016). 47
REQUIRES Anticoagulation Interruption1,2
High risk
• Any surgery or procedure with neuraxial (spinal or
epidural) anesthesia
• Neurosurgery (intracranial or spinal)
• Cardiac surgery (e.g. CABG, heart valve
replacement)
• Major intra-abdominal surgery
• Major vascular surgery (e.g. aortic aneurysm repair,
aortofemoral bypass)
• Major orthopedic surgery (e.g. hip or knee
replacement)
• Lung resection surgery
• Urological surgery (e.g. prostatectomy, bladder
tumour resection)
• Extensive cancer surgery (e.g. pancreas, liver)
• Intestinal anastomosis surgery
• Reconstructive plastic surgery
• Selected procedures (e.g. kidney biopsy, prostate
biopsy, cervical cone biopsy, pericardiocentesis,
colonic polypectomy)
DOES NOT REQUIRE Anticoagulation Interruption1,2
Low risk
• Dental extractions (1 or 2 teeth), endodontic (root
canal) procedure,
• subgingival scaling or other cleaning
• Cataract surgery
• Dermatologic procedures (e.g. biopsy)
• Gastroscopy or colonoscopy without biopsies
• Coronary angiography
• Permanent pacemaker insertion or internal
defibrillator placement (if bridging anticoagulation is
not used)
• Selected procedures (e.g. thoracentesis,
paracentesis, arthrocentesis)
REQUIRES Anticoagulation Interruption1,2
Intermediate risk
• Other intra-abdominal surgery (e.g. laparoscopic
cholecystectomy, hernia repair)
• Other general surgery (e.g. breast)
• Other intrathoracic surgery
• Other orthopedic surgery
• Other vascular surgery
• Non-cataract ophthalmologic surgery
• Gastroscopy or colonoscopy with biopsies
• Selected procedures (e.g. bone marrow biopsy,
lymph node biopsy)
• Complex dental procedure (e.g. multiple tooth
extractions)

Pre-operative Management of Patients
Receiving a NOAC
48
Low Risk of BleedingIntermediate or
High Risk of Bleeding
1 Day Before 3 Days Before
Dabigatran1
30 to ≤50 mL/min
SKIP 6 DOSES
Apixaban1
≥30 mL/min
SKIP 2 DOSES
Dabigatran1
≥50 mL/min
SKIP 2 DOSES
Rivaroxaban1
≥30 mL/min
SKIP 1 DOSE
Edoxaban2,3
≥30 mL/min
SKIP 1 DOSE
2 Days Before
Apixaban1
≥30 mL/min
SKIP 4 DOSES
Dabigatran1
≥50 mL/min
SKIP 4 DOSES
Rivaroxaban1
≥30 mL/min
SKIP 2 DOSES
Edoxaban2,3
≥30 mL/min
SKIP 2 DOSES
5 Days Before
Dabigatran1
30 to ≤50 mL/min
SKIP 10 DOSES
Timing of LAST Dose Before Procedure
1. Thrombosis Canada. New/Novel Oral Anticoagulants (NOACs): Peri‐operative Management. Available from:
http://thrombosiscanada.ca/wp-content/uploads/2016/07/21_NOACs-Peri-Operative-Management_2016July13-FINAL.pdf ; 2. Edoxaban
(Lixiana) Product Monograph. Progress Therapeutics; 3. Consensus recommendations of the Planning Committee.

Post-operative Management of Patients
Receiving a NOAC
1. Thrombosis Canada. New/Novel Oral Anticoagulants (NOACs): Peri‐operative Management. Available from:
http://thrombosiscanada.ca/wp-content/uploads/2016/07/21_NOACs-Peri-Operative-Management_2016July13-FINAL.pdf; 2. Edoxaban
(Lixiana) Product Monograph. Progress Therapeutics49
Drug Renal Function
Suggested Timing for Resuming NOAC
Low Risk
of Bleeding
Intermediate or High
Risk of Bleeding
Apixaban1 24 hours after surgery 48 hours after surgery
Dabigatran1 24 hours after surgery 48 hours after surgery
Edoxaban2 Once adequate hemostasis has been established
Rivaroxaban1 24 hours after surgery 48 hours after surgery

Bridging Not Required for NOACs
“Bridging (LMWH or UFH) is not required for NVAF patients on
NOAC undergoing elective surgery or invasive procedures
requiring interruption of anticoagulation”
Consider bridging therapy in ANY post-operative patient whose
OAC therapy cannot be restarted within 72 hours2
50LMWH: low molecular weight heparin; NVAF: non-valvular atrial fibrillation; UFH: unfractionated heparin.
1. Macle et al. CJC. 2016;32:1170-85; 2. Douketis et coll. NEJM. 2015;373:823-33.
2016 CCS Guidelines for the Management of AF1
Thrombosis Canada

Xa inhibitors vs. Warfarin for ischemic stroke, intracranial hemorrhage or the combination of both
Apixaban Warfarin HR (95% CI)
apixaban vs. warfarin
HR (95% CI)
apixaban vs. warfarinRate (%/year) Rate (%/year)
ICH 0.38 0.97 0.38 (0.17–0.88)*
Ischemic
stroke0.56 0.51 1.13 (0.49–2.63)
Combined 0.89 1.44 0.63 (0.35–1.12)
0.125 0.25 0.5 1 2 4
Favorsapixaban
Favors warfarin
*p<0.05
Rivaroxaban Warfarin HR (95% CI)
rivaroxaban vs.
warfarin
HR (95% CI)
rivaroxaban vs. warfarinRate (%/year) Rate (%/year)
ICH 0.49 0.96 0.53 (0.35–0.79)*
Ischemic
stroke0.54 0.83 0.71 (0.47–1.07)
Combined 0.95 1.6 0.61 (0.45–0.82)*
0.125 0.25 0.5 1 2 4Favors
rivaroxabanFavors
warfarin
Coleman CI, Antz M, Simard E, et al. Real-world evidence on stroke prevention in patients with atrial fibrillation in the United States.
Presented at: European Cardiac Arrhythmia Society Congress. April 17, 2016. Paris, France.

NOAC adherence clinically-relevant?Dabigatran
0.95
1.00
1.05
1.10
1.15
Mortality/stroke Stroke Non-fatal bleeding event
Ha
zard
ra
tio
/10
% d
ecr
ea
se in
PD
C
1.13
95%CI, 1.08–1.191.13
95%CI, 0.97–1.33
1.04
95%CI, 0.94–1.14
5376 US veterans with NVAF (71.3±9.7 years; 98.3% were men and mean CHADS2 score was 2.4±1.2; mean PDC 84%±22%; 27.8% with a PDC <80%; median follow-up of 244 days) initiated on dabigatran from October 2010 to September 2012
Non-adherence is
associated with worse
outcomes during NVAF
NOAC treatment
Am Heart J. 2014;167:810-7.

XARELTO Product Monograph
XARELTO 10 mg – 100% with or without food
XARELTO 20mg – 66% without food,
39% increase with food
XARELTO 15 mg and 20 mg tablets should be
taken with food

Objectives
54
To determine in stable CV disease, whether:
•Aspirin 100 mg od
•Rivaroxaban 5 mg bid
•Rivaroxaban 2.5 mg bid + aspirin 100 mg od
Outcome: CV death, stroke or myocardial infarction
And whether: Pantoprazole compared with placebo reduces upper GI events (ongoing)

COMPASS design
Aspirin 100 mg od
Rivaroxaban 5 mg bid
RRun-in
(aspirin)
55
Rivaroxaban 2.5 mg bid
+ aspirin 100 mg od
Stable CAD or PAD2200 Events3-4 years

Baseline characteristics
56
CharacteristicRivaroxaban + aspirin Rivaroxaban Aspirin
N=9,152 N=9,117 N=9,126
Age, yr 68 68 68
Blood pressure, mmHg 136/77 136/78 136/78
Total cholesterol, mmol/L 4.2 4.2 4.2
CAD 91% 90% 90%
PAD 27% 27% 27%
Diabetes 38% 38% 38%
Lipid-lowering 90% 90% 89%
ACE-I or ARB 71% 72% 71%

Follow up, adherence
57
• On February 6, 2017 the Data and Safety Monitoring Board recommended discontinuation of rivaroxaban/aspirin arms for clear evidence of efficacy (combination: Z= -4.59, P<0.00001; rivaroxaban: Z= -2.44, P=0.01)
• Close-out between March and June 2017
• Mean follow up 23 months
• Follow up 99.8% complete

Primary: CV death, stroke, MI
58

Primary components
59
Outcome
R + AN=9,152
AN=9,126
Rivaroxaban + Aspirin vs. Aspirin
N(%)
N(%)
HR(95% CI) p
CV death160
(1.7%)203
(2.2%)0.78
(0.64-0.96) 0.02
Stroke83
(0.9%)142
(1.6%)0.58
(0.44-0.76)<0.0001
MI178
(1.9%)205
(2.2%)0.86
(0.70-1.05)0.14

Secondary outcomes
13
Outcome
R + AN=9,152
AN=9,126
Rivaroxaban + Aspirin vs. Aspirin
N(%)
N(%)
HR(95% CI) P*
CHD death, IS, MI, ALI
329(3.6%)
450(4.9%)
0.72(0.63-0.83)
<0.0001
CV death, IS, MI, ALI
389(4.3%)
516(5.7%)
0.74(0.65-0.85)
<0.0001
Mortality313
(3.4%)378
(4.1%)0.82
(0.71-0.96)0.01
* pre-specified threshold P=0.0025

CAD and PAD Subgroups for primary outcome
Outcome
R + AN=9,152
AN=9,126
Rivaroxaban + Aspirin
vs. Aspirin
N (%) N (%) HR (95% CI)
CAD347
(4.2%)
460
(5.6%)
0.74
(0.65-0.86)
PAD126
(5.1%)174
(6.9%)0.72
(0.57-0.90)
14

Major bleeding
62
Outcome
R + AN=9,152
RN=9,117
AN=9,126
Rivaroxaban + Aspirin vs. Aspirin
Rivaroxaban vs. Aspirin
N (%) N (%) N (%) HR (95% CI)P
HR (95% CI)P
Major bleeding288
(3.1%)255
(2.8%)170
(1.9%)1.70
(1.40-2.05) <0.00011.51
(1.25-1.84) <0.0001
Fatal15
(0.2%)14
(0.2%)10
(0.1%)1.49
(0.67-3.33) 0.321.40
(0.62-3.15) 0.41
Non fatal ICH*21
(0.2%)32
(0.4%)19
(0.2%)1.10
(0.59-2.04) 0.771.69
(0.96-2.98) 0.07
Non-fatal othercritical organ*
42(0.5%)
45(0.5%)
29(0.3%)
1.43(0.89-2.29) 0.14
1.57(0.98-2.50) 0.06
* symptomatic

Net clinical benefit
63
Outcome
R + AN=9,152
AN=9,126
Rivaroxaban + Aspirin vs. Aspirin
N (%) N (%) HR (95% CI)P
Net clinical benefit(Primary + Severe bleeding
events)431
(4.7%)534
(5.9%)0.80
(0.70-0.91)0.0005




















![05 KFox Stroke - UCSF CMEhemorrhagic)/systemic embolization –Bleeding risk similar to Warfarin Rivaroxaban[Factor Xainhibitor] ... •20mg/day starting 5-7 days post-ictus •Mechanism](https://img.pdfslide.us/doc/110x75/5e62650ec0efb16de73cadc2/05-kfox-stroke-ucsf-hemorrhagicsystemic-embolization-ableeding-risk-similar.jpg)